RECURRENT GN BWG Chairs Nada Alachkar, MD Serena Bagnasco, MD Johns Hopkins University School of Medicine, Baltimore, MD, USA 28 March 2017
|
|
|
- Della Fox
- 5 years ago
- Views:
Transcription
1 RECURRENT GN BWG Chairs Nada Alachkar, MD Serena Bagnasco, MD Johns Hopkins University School of Medicine, Baltimore, MD, USA 28 March 2017
2 Nothing to disclose DISCLOSURE

3 OBJECTIVES Significance of recurrent GN in the transplanted kidney Goal of the GN working group Structure of the work Brief highlights Preliminary data Future work
4 Significance of GN recurrence All primary GN recur highly post transplant Recurrence rate is different for each type Second most common cause of allograft failure after rejection Limited data on the pathology and its significance in the outcome Limited data on de novo GN
5 Goals of this work Establish pathology guidelines in GN diagnosis for pathologists/ clinicians Early signs of recurrence Late manifestation SAVE GLOMERULUS BANFF GN Understanding GN changes when combined with other pathological changes Correlations & predictions pathology with clinical manifestation & outcome Genetic variations biomarkers correlation with pathology
6 GN Banff Working Group Aula Magna Room: March 29 th, 2017; 18:30-20:30 Chairs: Nada Alachkar & Serena Bagnasco Multi international centers; ~ 30 centers: pathology/nephrology/immunology/surgery members Each center: pathologist + clinician Members: 54 showed interest
7 MEMBERS Member Title Institution Alexandre Loupy Nephrology Necker hospital, France Michael Mengel Pathology University of Alberta, Canada Surya V Seshan Pathology Weill Cornell Medicine, USA Darshana Dadhania Nephrology Weill Cornell Medicine, USA Ibrahim Batal Pathology Columbia University, USA Marian C Clahsen-van Groningen Pathology Erasmus University Rotterdam, Netherlands Patricia Campbell Immunology University of Alberta, Edmonton, Canada Davis Massey Pathology Virginia Commonwealth University, USA Alton B. "Brad" Farris Pathology Emory University Hospital, USA Maarten Naesens Nephrology University Hospitals Leuven, Belgium Adnan Sharif Nephrology University Hospitals Birmingham, UK Ajda T Rowshani Nephrology Erasmus University Medical, Netherlands Dana Baran Nephrology McGill University Hospital Centre, Canada Maha Mohamed Nephrology Univ. of Wisconsin, USA Bassam Abu Jawdeh Nephrology Univ. of Cincinnati, USA Gaurav Gupta Nephrology Virginia Commonwealth University, USA Marco Delsante Pathology Johns Hopkins, USA Lorraine Racusen Pathology Johns Hopkins, USA Anke Schwarz Pathology Hannover Medical School, Germany Michael Stokes Pathology Columbia University, USA Nithya Krishnan Nephrology University Hospital (Coventry), UK Nasreen Hasan Mohamed Pathology King Fahad Specialist Hospital-Dammam, Saudi Arabia Emanuele Cozzi Immunology University of Padua, Italy David Rush Nephrology University of Manitoba, Winnipeg, Canada Mark Haas Pathology Cedar s Sinai, USA Ruth Sapir-Pichhadze Nephrology McGill University, Canada Laurine Bow Immunology Yale, USA Diana Taheri Pathology Isfahan University, Iran Jason Kidd Nephrology Virginia Commonwealth University, USA Lynn D Cornell Pathology Mayo Clinic, USA Tarek Alhamad Nephrology Wash. Univ. St. Louis, USA Kevin Wen Nephrology University of Alberta, Canada Cuong Nguyen Nephrology Oklahoma, USA
8 Previous meetings Kickoff meeting: June 13, 2016; Boston, MA (ATC) Starting with IgA in native and transplant; followed by other GN Multi-centers registry Reports of the bx Second meeting: November 17th, 2017; Chicago, IL (ASN) Share single center s data in redcap/other data entry system Grants for data entry and analysis Each center will have internal IRB

9 Main Questions?????? Recurrence rate of GN /Frequency of de novo GN? Manifestations/characteristics of recurrence /de novo in the allograft in each of these glomerulopathies? Clinical and pathological characteristics of NATIVE GN that can predict recurrence in the transplanted kidney? Characteristics of the histological /clinical manifestation in ALLOGRAFT with predictive value for progression/graft survival? What do we need for diagnosis: Light microscopy/if/em/markers?
10 GN in Native Kidney Characterization Clinical Glomerulopathy PATHOLOGY CLINICAL FINDINGS Native disease Light Microscopy: Global glomerulosclerosis (%) Segmental glomerulosclerosis (%) Hyalinosis Podocyte changes Glomerular capillary walls Mesangial matrix expansion Mesangial hypercellularity Endocapillary proliferation Crescents Karyorrhexis/ segmental necrotizing lesions Tubular injury Tubulitis Interstitial inflammation % interstitial fibrosis % Tubular atrophy Arteriosclerosis (cv) Arteriolar hyalinosis (ah) IF: EM: presence of deposits and distribution, Substructures % of podocyte foot process effacement Demographics Age of onset Renal manifestations at onset Renal function egfr Hematuria Proteinuria, UPCR at time of onset Co-morbidities Diabetes, Hypertension at onset Progression of the disease, time from onset to ESRD (egfr, UPCR others) Therapy for glomerulopathy
11 GN in Transplanted Kidney Characterization Clinical Glomerulopathy PATHOLOGY CLINICAL FINDINGS Post Transplant Light Microscopy: Global glomerulosclerosis (%) Segmental glomerulosclerosis (%) Hyalinosis Podocyte changes Glomerular capillary walls Mesangial matrix expansion Mesangial hypercellularity Endocapillary proliferation Crescents Karyorrhexis/ segmental necrotizing lesions Tubular injury Tubulitis Interstitial inflammation % interstitial fibrosis % Tubular atrophy Arteriosclerosis (cv) Arteriolar hyalinosis (ah) IF: EM: presence of deposits and distribution, Substructures % of podocyte foot process effacement Type of donor (Live, Deceased, cpra, HLA mismatches) Desensitization Induction Maintenance immunosuppression Rejection episodes and type of rejections pre- post recurrence Infections pre-post recurrence Time of Onset of the pathological changes from transplantation Renal function at onset of recurrence Treatment of glomerulopathy Effect of treatment Resolution/persistence/progression in FU biopsies
12 Elements to be analyzed Elements Histology Clinical Frequency Histological features at diagnosis Time of onset post transplant Predictors Histological predictors Clinical predictors: Demographics, Age, native dx, characteristics of the transplanted kidney (live/decease, HLA compatibility etc), egfr, Hematuria, UPCR, therapy, episodes and types of rejection Relation to native dx WORKING GROUP Comparison with histological features in the native kidney Demographics, Age, native dx, egfr, Hematuria, UPCR, therapy, Progression of the native dx Copy of Bx Report/Shared scan slides Clinical data of the center s cohort Questionnaire Registry
13 THE HISTORY OF RECURRENT GLOMERULONEPHRITIS "glomerulonephritis" AND "kidney transplantation" 2737 publications



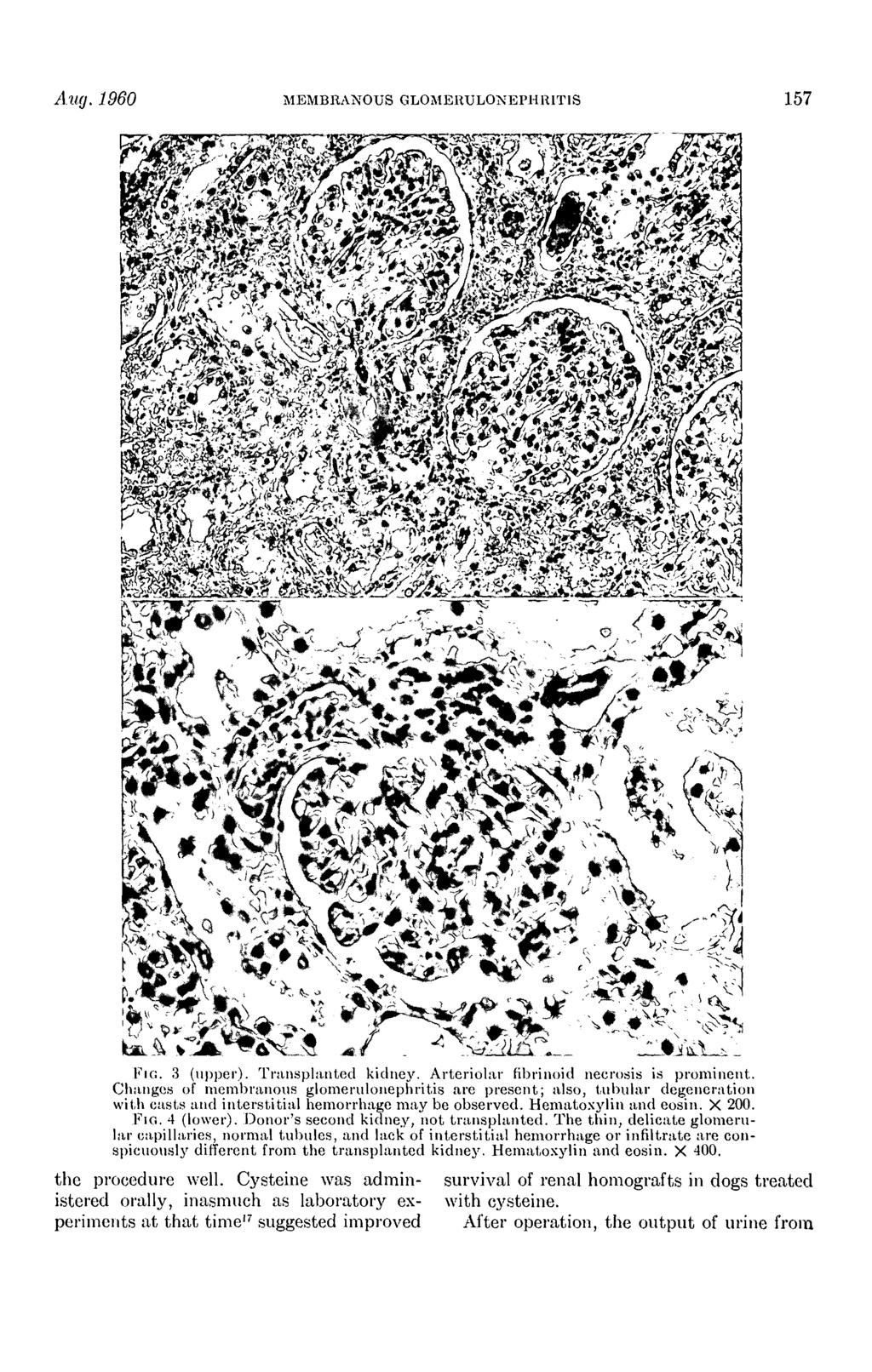

14 Earlier data--- recurrent MN 1960







15 Earlier data--- recurrent MPGN 1970
16 Recurrent Glomerulonephritis After Renal Transplantation 1978 J Hamburger, J Crosnier, and L H Noel Annual Review of Medicine

17 DE NOVO COLLAPSING GLOMERULOPATHY IN RENAL ALLOGRAFTS Meehan, Shane; Pascual, Manuel; Williams, Winn; Tolkoff-Rubin, Nina; Delmonico, Francis; Cosimi, A; Colvin, Robert Transplantation. 65(9): , May 15,
18 RECURRENT AND DE NOVO GLOMERULAR DISEASE AFTER RENAL TRANSPLANTATION: A Report from Renal Allograft Disease Registry (RADR) 1999 Hariharan S et al. Transplantation 1999
19 RECURRENT AND DE NOVO GLOMERULAR DISEASE AFTER RENAL TRANSPLANTATION: A Report from Renal Allograft Disease Registry (RADR) Hariharan S et al. Transplantation 1999

20 FSGS variants in patients native and transplant kidneys IJpelaar et al. JASN 2008;19:
21 Kidney Transplantation Outcomes across GN Subtypes in the United States O Shaughnessy et al. JASN 2016

22 Kidney Transplantation Outcomes across GN Subtypes in the United States O Shaughnessy et al. JASN 2016

23 THE GOAL IS NOT to Reinvent GN recurrence BUT To Connect ALL The Dots
24 Single Center s Experience Johns Hopkins University: IgA, FSGS, MPGN, MN University of Alberta Virginia Commonwealth University Colombia Wisconsin University
25 IgA nephropathy--native Characterization Clinical IgA nephropathy PATHOLOGY CLINICAL FINDINGS Native disease IgA deposits with no histological glomerular changes IgA deposits with histological changes Light Microscopy: Global glomerulosclerosis (%) Segmental glomerulosclerosis (%) Hyalinosis Podocyte changes Glomerular capillary walls Mesangial matrix expansion Mesangial hypercellularity Endocapillary proliferation Crescents Karyorrhexis/ segmental necrotizing lesions Tubular injury Tubulitis Interstitial inflammation % interstitial fibrosis % Tubular atrophy Arteriosclerosis (cv) Arteriolar hyalinosis (ah) IF: EM: presence of deposits and distribution, Substructures % of podocyte foot process effacement Demographics Age of onset Renal manifestations at onset Renal function egfr Hematuria Proteinuria, UPCR at time of onset Co-morbidities Diabetes, Hypertension at onset Progression of the disease, time from onset to ESRD (egfr, UPCR others) Therapy for glomerulopathy
26 IgA nephropathy--transplant Ch Characterization Clinical IgA nephropathy PATHOLOGY CLINICAL FINDINGS Post Transplant IgA deposits with no histological glomerular changes IgA deposits with histological changes Light Microscopy: Global glomerulosclerosis (%) Segmental glomerulosclerosis (%) Hyalinosis Podocyte changes Glomerular capillary walls Mesangial matrix expansion Mesangial hypercellularity Endocapillary proliferation Crescents Karyorrhexis/ segmental necrotizing lesions Tubular injury Tubulitis Interstitial inflammation % interstitial fibrosis % Tubular atrophy Arteriosclerosis (cv) Arteriolar hyalinosis (ah) IF: EM: presence of deposits and distribution, Substructures % of podocyte foot process effacement Type of donor (Live, Deceased, cpra, HLA mismatches) Desensitization Induction Maintenance immunosuppression Rejection episodes and type of rejections pre- post recurrence Infections pre-post recurrence Time of Onset of the pathological changes from transplantation Renal function at onset of recurrence Treatment of glomerulopathy Effect of treatment Resolution/persistence/progression in FU biopsies
27 IgA nephropathy--elements to be analyzed Frequency Histological features at diagnosis Time of onset post transplant Predictors Histological predictors Clinical predictors: Demographics, Age, native dx, characteristics of the transplanted kidney (live/decease, HLA compatibility etc), egfr, Hematuria, UPCR, therapy, episodes and types of rejection Relation to native dx Comparison with histological features in the native kidney Demographics, Age, native dx, egfr, Hematuria, UPCR, therapy, Progression of the native dx Correlation with FSGS FSGS associated with IgA; Podocyte injury Effect on UPC: more if FSGS lesions De Novo IgA post transplant with no native IgA Time/Lab changes







28 IgA Nephropathy Focal proliferative with fibrocellular crescent Focal proliferative GN with cellular crescent Crescent - silver stain IgA stain C3 2+ Fibrinogen stains the crescentic area Mesangial electron-dense deposits

29 IgA Nephropathy, n=105 pts, 122 allografts Clinical characteristic Recurrent group (n=22) Non-recurrent group P value (n=82) Allografts (n=23) Allografts (n=99) Male (% ) 18 (82) 48 (58) 0.07 Mean age at diagnosis, years ± SD 29.4 ± ± Time from diagnosis to ESRD 2.4 ± ± Time from ESRD to transplant 1.4 ± ± UPC at diagnosis, g/g ± SD 4.4 ± ± Parameters Before recurrence At recurrence Most recent p value Mean RBC/ hpf ± SD N/A 27 ± 50 3 ± Mean UPC ratio, g/g ± SD Mean serum creatinine, mg/dl ± SD N/A 2 ± ± ± ± ± Serum albumin at diagnosis, g/dl 4.3 ± ± 0.6 NS Mean age at transplant, years 37.7 ± ± Preemptive transplant (% ) 4 (17) 26 (26) 0.53 Deceased Living related Living unrelated Age at recurrence, years ± SD 44.3 ± Time to recurrence, years ± SD 6.75 ± Therapy after transplant ACEI/ARB (% ) 14 (61) 31 (31) Steroids (% ) 17 (74) 84 (85) NS Cyclophosphamide (% ) 2 (9) 1 (1) NS Rejections (% ) 7 (30) 17 (17) recent serum creatinine, mg/dl 2.7 ± ± Mean most recent UPC ratio, g/g 1.6 ± ± Graft failure (% ) 13 (57) 10 (10) Time to Graft Failure, years ± SD 6.5 ± ± 7.5 < Mean egfr ml/min/1.73 m 2 ± SD 49 ± ± ± Nijim S & Alachkar N. Transplant Proc 2016
30 IgA Nephropathy, n=105 pts, 122 allografts Graft loss was attributed to recurrent IgA nephropathy if the renal allograft biopsy at the time of clinical graft failure demonstrated diffuse mesangial proliferation and glomerular sclerosis due to IgA deposits


31 RISK FACTORS OF RECURRENCE AND GRAFT SURVIVAL (n=62; with follow up of >6 years) Nijim S & Alachkar N. Transplant Proc 2016
32 Causes of ESRD in transplanted patients from Jan 2000 to Nov 2016 (Total Tx 3393) Primary GN Renal involvement in systemic diseases DM HTN ADPKD OTHER UNKNOWN
33 Primary GN (Total 518) FSGS IgAN MN MPGN OTHER
34 Recurrence % % % 15.38% 0 IgA FSGS MPGN MN Non-recurrent Recurrent
35 Glomerular Changes IgA recurrence Normal+IgA Crescentic FSGS+IgA M ± E
36 3 Banff t v i ti g ptc C4d mm ci ct ah cv cg Normal+IgA Mean M ± E Mean FSGS+IgA Mean Crescentic Mean
37 3 Banff ti ti Normal+IgA mean M ± E mean FSGS+IgA mean Crescentic mean
38 40% IFTA % 35% 30% 25% 20% 15% 10% 5% 0% IFTA % Normal+IgA mean M ± E mean FSGS+IgA mean Crescentic mean
39 45% Global Glomerulosclerosis (GS) % 40% 35% 30% 25% 20% 15% 10% 5% 0% GS% Normal+IgA mean M ± E mean FSGS+IgA mean Crescentic mean
40 Number of IgA recurrent cases Time of recurrence post transplant Months from transplant

41
42 Early findings of FSGS Podocytes injury: focal detachment from the GBM Podocytes loose their adhesive phenotype in early FSGS, which may contribute to the detachment of podocytes from the GBM Kemeny E et al. Clin Nephrol Feb;43(2):71-83
43 Retrospective Data, n=25 9 recurrent FSGS had histopathological data available on their primary FSGS: 3 had collapsing, 2 tip, and 4 classic (NOS) 4 had histopathological data also available at the time of recurrence: 3 had concordant FSGS variants, and 1 had primary classic FSGS, had recurrent collapsing FSGS post transplant Alachkar et al. Transplantation 2013
44 Retrospective Data, n=25 24 had bx at time of post-transplant FSGS diagnosis 6 had histopathological changes consistent with FSGS on light microscopy (two with classic FSGS, one with tip and collapsing variant, two with collapsing variant and one with perihilar variants) 18 did not have any FSGS changes on light microscopy Foot process effacement 13% - 100% Alachkar et al. Transplantation 2013

45 Pathological Changes of post transplant FSGS

 vs mild ( 25%) podocyte")
46 Changes in podocyte effacement after therapy with PP+Rituximab Recovery of podocyte effacement after therapy Foot processes effacement Decrease supar level after therapy Resolution of effacement after therapy Alachkar et al. Transplantation 2013 supar levels higher in severe ( 75%) vs mild ( 25%) podocyte effacement (13,030 vs. 4,806 pg/ml; P=0.03)

47 Plasma supar correlations with FSGS lesions in IgA FSGS lesions in IgA nephropathy Guo et al. PLOS ONE.2015
48 rfsgs prospective data, n=66 Serum samples, clinical data and biopsy results Recurrence: 38 patients (59%), 2 de novo Median time to recurrence 1.25 mos (1 day- 30 mos) Mean UPC at recurrence: 5.81 g/g ( g/g)

49 OUR OUTCOME Sensitivity Specificity Score 3: ROC area: Score 2 ROC area: Score 4: ROC area: Reference






50 Segmental thickening + endocapillary proliferation with lobulated appearance MPGN Double contours Duplication of GBM with immunecomplex deposits in between C3: 3-4+ staining IgG granular CW and mesangial staining GBM Duplication with cell interposition + Deposits
51 MPGN n=34, recurrent n=18 Variable Transplants (n=40) 37.4 (15-59) Median age at transplantation- yr (range) Gender (Male) 20 (50%) Independent variable Hazard Ratio (CI) P-value Age at transplantation ( ) 0.65 Race: Caucasian African American Other MPGN type (Old classification*): Type I Type I I Type I II Mixed MPGN type (New classification ): I CGN CGN Donor source: Deceased Living unrelated Living related 28 (70%) 7 (17%) 5 (13%) 65% 9% 21% 5% 88% 12% 10 (25% ) 15 (37% ) 15 (37% ) Gender (Male) 1.00 ( ) 1 Race (Caucasian) 1.5 ( ) 0.1 Allogr aft source (Living related) ( ) Duration of dialysis ( ) Preemptive transplantation ( ) Previous failed transplantation ( ) 0.86 Number of mismatches (2% ) 3 (7% ) 5 (12% ) 10 (25% ) 7 (17% ) 7 (17% ) 6 (15% ) Preemptive kidney transplant 4 (10% ) DGF (In deceased donor) 1.21 ( ) 0.83 Development of rejection ( ) 0.25 Use of ACEi/ARB ( ) Low complement level ( ) Median cumulative ESRD duration for non-preemptive- yr (range) 5.2 (0.2-20) Evidence of monoclonal gammopathy ( ) Alasfar S et al. BMC Nephrology 2016
52 MPGN, n=34 Reason for graft loss Frequency Treatment Number of allografts Response to therapy* MPGN recurrence 6 Antibody-Medicated 2 Rejection Cell-Medicated rejection 2 MPGN recurrence & rejection* 3 ATN 2 Bleeding 1 Thrombosis 1 Recurrence type at time of diagnosis (new classification) Number of cases Probability of remaining free of graft loss Recurrence type at time of diagnosis (old classification) ICGN 15 Type I: 14, Type III:1 CGN 2 Type I: 1, Type II: 1 ICGN-IgA dominant 1 Type I High dose steroids 4 1 Rituximab ± plasmapheresis Number at risk Non Recurrence Recurrence 8 3 Plasmapheresis 1 1 Eculizumab 1 1 No change in therapy 4 3 Kaplan-Meier renal allograft survival Time in year Non-recurrence Recurrence P 0.18 Alasfar et al. Alachkar. BMC Nephrology 2016
53 Other centers experience University of Alberta (Dr. Wen): 182 cases of IgA (1st transplants only, living donor and decease donors) with 50 cases of recurrence, recurrence rate 27% All of these were biopsy proven native IgA nephropathy; able to find the native biopsy reports and/or pathology samples Should be able to access the pathology for the 50 recurrence cases Virginia Commonwealth University (Dr. Gupta): 1. FSGS Membranous glomerulonephritis 29/nephropathy 18 (Total 47) 3. IgA nephropathy 59
54 Other centers experience Colombia University (Dr. Batal): 3 years: IgAN found in 538 native biopsies; of these 22 had transplant: at Columbia (n=19) or other hospitals (n=3), of these 22, 6 show recurrent IgAN in allograft Expect to have~100 cases in Columbia from 2000-now; ~70 from Wisconsin University (Dr. Mohamed): Native kidney diagnosis and already transplanted IgA nephropathy diagnosis: n=306 (2000 to present) Glomerulonephritis diagnosis: n=341 (2000 to present)
55 SUMMARY Limited data on GN pathology: single center s findings Recurrent GN is missing from Banff Unifying characterization of recurrent GN and de novo GN is crucial Identify early findings for therapies/response to therapies Histological prediction and correlation of clinical manifestation and outcome Understanding other glomerulopathies This work will potentially lead to guidelines for clinical practice

56 AKNOWLEDGEMENT BANFF ORGANIZERS GN working group members Serena Bagnasco Marco Delsante
Case # 2 3/27/2017. Disclosure of Relevant Financial Relationships. Clinical history. Clinical history. Laboratory findings
 Case # 2 Christopher Larsen, MD Arkana Laboratories Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content
Case # 2 Christopher Larsen, MD Arkana Laboratories Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content
Classification of Glomerular Diseases and Defining Individual Glomerular Lesions: Developing International Consensus
 Classification of Glomerular Diseases and Defining Individual Glomerular Lesions: Developing International Consensus Mark Haas MD, PhD Department of Pathology & Laboratory Medicine Cedars-Sinai Medical
Classification of Glomerular Diseases and Defining Individual Glomerular Lesions: Developing International Consensus Mark Haas MD, PhD Department of Pathology & Laboratory Medicine Cedars-Sinai Medical
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT. J. H. Helderman,MD,FACP,FAST
 RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT J. H. Helderman,MD,FACP,FAST Vanderbilt University Medical Center Professor of Medicine, Pathology and Immunology Medical Director, Vanderbilt Transplant
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT J. H. Helderman,MD,FACP,FAST Vanderbilt University Medical Center Professor of Medicine, Pathology and Immunology Medical Director, Vanderbilt Transplant
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT
 RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT HISTOPATHOLOGIC DISORDERS AFFECTING THE ALLOGRAFT OTHER THAN REJECTION RECURRENT DISEASE DE NOVO DISEASE TRANSPLANT GLOMERULOPATHY Glomerular Non-glomerular
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT HISTOPATHOLOGIC DISORDERS AFFECTING THE ALLOGRAFT OTHER THAN REJECTION RECURRENT DISEASE DE NOVO DISEASE TRANSPLANT GLOMERULOPATHY Glomerular Non-glomerular
Case 3. ACCME/Disclosure. Laboratory results. Clinical history 4/13/2016
 Case 3 Lynn D. Cornell, M.D. Mayo Clinic, Rochester, MN Cornell.Lynn@mayo.edu USCAP Renal Case Conference March 13, 2016 ACCME/Disclosure Dr. Cornell has nothing to disclose Clinical history 57-year-old
Case 3 Lynn D. Cornell, M.D. Mayo Clinic, Rochester, MN Cornell.Lynn@mayo.edu USCAP Renal Case Conference March 13, 2016 ACCME/Disclosure Dr. Cornell has nothing to disclose Clinical history 57-year-old
Mayo Clinic/ RPS Consensus Report on Classification, Diagnosis, and Reporting of Glomerulonephritis
 Mayo Clinic/ RPS Consensus Report on Classification, Diagnosis, and Reporting of Glomerulonephritis Sanjeev Sethi, MD, PhD Department of Laboratory Medicine and Pathology Disclosure Relevant Financial
Mayo Clinic/ RPS Consensus Report on Classification, Diagnosis, and Reporting of Glomerulonephritis Sanjeev Sethi, MD, PhD Department of Laboratory Medicine and Pathology Disclosure Relevant Financial
RENAL EVENING SPECIALTY CONFERENCE
 RENAL EVENING SPECIALTY CONFERENCE Harsharan K. Singh, MD The University of North Carolina at Chapel Hill Disclosure of Relevant Financial Relationships No conflicts of interest to disclose. CLINICAL HISTORY
RENAL EVENING SPECIALTY CONFERENCE Harsharan K. Singh, MD The University of North Carolina at Chapel Hill Disclosure of Relevant Financial Relationships No conflicts of interest to disclose. CLINICAL HISTORY
The Banff Classification for Diagnosis of Renal Allograft Rejection: Updates from the 2017 Banff Conference
 The Banff Classification for Diagnosis of Renal Allograft Rejection: Updates from the 2017 Banff Conference Mark Haas Cedars-Sinai Medical Center Los Angeles, California, USA Statement of Disclosure Mark
The Banff Classification for Diagnosis of Renal Allograft Rejection: Updates from the 2017 Banff Conference Mark Haas Cedars-Sinai Medical Center Los Angeles, California, USA Statement of Disclosure Mark
Monoclonal Gammopathies and the Kidney. Tibor Nádasdy, MD The Ohio State University, Columbus, OH
 Monoclonal Gammopathies and the Kidney Tibor Nádasdy, MD The Ohio State University, Columbus, OH Monoclonal gammopathy of renal significance (MGRS) Biopsies at OSU (n=475) between 2007 and 2016 AL or AH
Monoclonal Gammopathies and the Kidney Tibor Nádasdy, MD The Ohio State University, Columbus, OH Monoclonal gammopathy of renal significance (MGRS) Biopsies at OSU (n=475) between 2007 and 2016 AL or AH
Statement of Disclosure
 Statement of Disclosure Mark Haas serves as a paid consultant on pathology adjudication committees for two industry-sponsored clinical trials: Shire ViroPharma Treatment of Acute ABMR AstraZeneca Treatment
Statement of Disclosure Mark Haas serves as a paid consultant on pathology adjudication committees for two industry-sponsored clinical trials: Shire ViroPharma Treatment of Acute ABMR AstraZeneca Treatment
CHAPTER 2. Primary Glomerulonephritis
 2nd Report of the PRIMARY GLOMERULONEPHRITIS CHAPTER 2 Primary Glomerulonephritis Sunita Bavanandan Lee Han Wei Lim Soo Kun 21 PRIMARY GLOMERULONEPHRITIS 2nd Report of the 2.1 Introduction This chapter
2nd Report of the PRIMARY GLOMERULONEPHRITIS CHAPTER 2 Primary Glomerulonephritis Sunita Bavanandan Lee Han Wei Lim Soo Kun 21 PRIMARY GLOMERULONEPHRITIS 2nd Report of the 2.1 Introduction This chapter
Ordering Physician. Collected REVISED REPORT. Performed. IgG IF, Renal MCR. Lambda IF, Renal MCR. C1q IF, Renal. MCR Albumin IF, Renal MCR
 RenalPath Level IV Wet Ts IgA I Renal IgM I Renal Kappa I Renal Renal Bx Electron Microscopy IgG I Renal Lambda I Renal C1q I Renal C3 I Renal Albumin I Renal ibrinogen I Renal Mayo Clinic Dept. of Lab
RenalPath Level IV Wet Ts IgA I Renal IgM I Renal Kappa I Renal Renal Bx Electron Microscopy IgG I Renal Lambda I Renal C1q I Renal C3 I Renal Albumin I Renal ibrinogen I Renal Mayo Clinic Dept. of Lab
CHAPTER 2 PRIMARY GLOMERULONEPHRITIS
 CHAPTER 2 Sunita Bavanandan Lim Soo Kun 19 5th Report of the 2.1: Introduction This chapter covers the main primary glomerulonephritis that were reported to the MRRB from the years 2005-2012. Minimal change
CHAPTER 2 Sunita Bavanandan Lim Soo Kun 19 5th Report of the 2.1: Introduction This chapter covers the main primary glomerulonephritis that were reported to the MRRB from the years 2005-2012. Minimal change
Case Presentation Turki Al-Hussain, MD
 Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
C1q nephropathy the Diverse Disease
 C1q nephropathy the Diverse Disease Danica Galešić Ljubanović School of Medicine, University of Zagreb Dubrava University Hospital Zagreb, Croatia Definition Dominant or codominant ( 2+), mesangial staining
C1q nephropathy the Diverse Disease Danica Galešić Ljubanović School of Medicine, University of Zagreb Dubrava University Hospital Zagreb, Croatia Definition Dominant or codominant ( 2+), mesangial staining
Management of Rejection
 Management of Rejection I have no disclosures Disclosures (relevant or otherwise) Deborah B Adey, MD Professor of Medicine University of California, San Francisco Kidney and Pancreas Transplant Center
Management of Rejection I have no disclosures Disclosures (relevant or otherwise) Deborah B Adey, MD Professor of Medicine University of California, San Francisco Kidney and Pancreas Transplant Center
Dr Ian Roberts Oxford. Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust
 Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing proteinuria & haematuria Highlight diagnostic pitfalls Nephrotic
Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing proteinuria & haematuria Highlight diagnostic pitfalls Nephrotic
Membranoproliferative glomerulonephritis recurrence after kidney transplantation: using the new classification
 Alasfar et al. BMC Nephrology (2016) 17:7 DOI 10.1186/s12882-015-0219-x RESEARCH ARTICLE Open Access Membranoproliferative glomerulonephritis recurrence after kidney transplantation: using the new classification
Alasfar et al. BMC Nephrology (2016) 17:7 DOI 10.1186/s12882-015-0219-x RESEARCH ARTICLE Open Access Membranoproliferative glomerulonephritis recurrence after kidney transplantation: using the new classification
Secondary IgA Nephropathy & HSP
 Secondary IgA Nephropathy & HSP Anjali Gupta, MD 1/11/11 AKI sec to Hematuria? 65 cases of ARF after an episode of macroscopic hematuria have been reported in the literature in patients with GN. The main
Secondary IgA Nephropathy & HSP Anjali Gupta, MD 1/11/11 AKI sec to Hematuria? 65 cases of ARF after an episode of macroscopic hematuria have been reported in the literature in patients with GN. The main
Surgical Pathology Report
 Louisiana State University Health Sciences Center Department of Pathology Shreveport, Louisiana Accession #: Collected: Received: Reported: 6/1/2012 09:18 6/2/2012 09:02 6/2/2012 Patient Name: Med. Rec.
Louisiana State University Health Sciences Center Department of Pathology Shreveport, Louisiana Accession #: Collected: Received: Reported: 6/1/2012 09:18 6/2/2012 09:02 6/2/2012 Patient Name: Med. Rec.
Classification of Glomerular Diseases and Defining Individual Glomerular Lesions: Developing International Consensus
 Classification of Glomerular Diseases and Defining Individual Glomerular Lesions: Developing International Consensus Mark Haas MD, PhD Department of Pathology & Laboratory Medicine Cedars-Sinai Medical
Classification of Glomerular Diseases and Defining Individual Glomerular Lesions: Developing International Consensus Mark Haas MD, PhD Department of Pathology & Laboratory Medicine Cedars-Sinai Medical
Review of Rituximab and renal transplantation. Dr.E Nemati. Professor of Nephrology
 Review of Rituximab and renal transplantation Dr.E Nemati Professor of Nephrology Introductio n Rituximab is a chimeric anti-cd20 monoclonal antibody. The CD20 antigen is a transmembrane nonglycosylated
Review of Rituximab and renal transplantation Dr.E Nemati Professor of Nephrology Introductio n Rituximab is a chimeric anti-cd20 monoclonal antibody. The CD20 antigen is a transmembrane nonglycosylated
Kidney Summary. Mark Haas Cedars-Sinai Medical Center Los Angeles, California, USA
 Kidney Summary Mark Haas Cedars-Sinai Medical Center Los Angeles, California, USA Key Issues to Address re: the Classification 1. Incorporation of i-ifta + tubulitis into the TCMR classification - Defining
Kidney Summary Mark Haas Cedars-Sinai Medical Center Los Angeles, California, USA Key Issues to Address re: the Classification 1. Incorporation of i-ifta + tubulitis into the TCMR classification - Defining
Hasan Fattah 3/19/2013
 Hasan Fattah 3/19/2013 AASK trial Rational: HTN is a leading cause of (ESRD) in the US, with no known treatment to prevent progressive declines leading to ESRD. Objective: To compare the effects of 2 levels
Hasan Fattah 3/19/2013 AASK trial Rational: HTN is a leading cause of (ESRD) in the US, with no known treatment to prevent progressive declines leading to ESRD. Objective: To compare the effects of 2 levels
Clinical pathological correlations in AKI
 Clinical pathological correlations in AKI Dr. Rajasekara chakravarthi Director - Nephrology Star Kidney Center, Star Hospitals Renown clinical services India Introduction AKI is common entity Community
Clinical pathological correlations in AKI Dr. Rajasekara chakravarthi Director - Nephrology Star Kidney Center, Star Hospitals Renown clinical services India Introduction AKI is common entity Community
FIBRILLARY GLOMERULONEPHRITIS DIAGNOSTIC CRITERIA, PITFALLS, AND DIFFERENTIAL DIAGNOSIS
 FIBRILLARY GLOMERULONEPHRITIS DIAGNOSTIC CRITERIA, PITFALLS, AND DIFFERENTIAL DIAGNOSIS Guillermo A. Herrera MD Louisiana State University, Shreveport Fibrils in bundles 10-20 nm d Diabetic fibrillosis
FIBRILLARY GLOMERULONEPHRITIS DIAGNOSTIC CRITERIA, PITFALLS, AND DIFFERENTIAL DIAGNOSIS Guillermo A. Herrera MD Louisiana State University, Shreveport Fibrils in bundles 10-20 nm d Diabetic fibrillosis
Glomerular Pathology- 1 Nephrotic Syndrome. Dr. Nisreen Abu Shahin
 Glomerular Pathology- 1 Nephrotic Syndrome Dr. Nisreen Abu Shahin The Nephrotic Syndrome a clinical complex resulting from glomerular disease & includes the following: (1) massive proteinuria (3.5 gm /day
Glomerular Pathology- 1 Nephrotic Syndrome Dr. Nisreen Abu Shahin The Nephrotic Syndrome a clinical complex resulting from glomerular disease & includes the following: (1) massive proteinuria (3.5 gm /day
Rejection or Not? Interhospital Renal Meeting 10 Oct Desmond Yap & Sydney Tang Queen Mary Hospital
 Rejection or Not? Interhospital Renal Meeting 10 Oct 2007 Desmond Yap & Sydney Tang Queen Mary Hospital Case Presentation F/61 End stage renal failure due to unknown cause Received HD in private hospital
Rejection or Not? Interhospital Renal Meeting 10 Oct 2007 Desmond Yap & Sydney Tang Queen Mary Hospital Case Presentation F/61 End stage renal failure due to unknown cause Received HD in private hospital
Case Presentation Turki Al-Hussain, MD
 Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Glomerular diseases mostly presenting with Nephritic syndrome
 Glomerular diseases mostly presenting with Nephritic syndrome 1 The Nephritic Syndrome Pathogenesis: proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls escape of RBCs
Glomerular diseases mostly presenting with Nephritic syndrome 1 The Nephritic Syndrome Pathogenesis: proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls escape of RBCs
Renal Pathology 1: Glomerulus. With many thanks to Elizabeth Angus PhD for EM photographs
 Renal Pathology 1: Glomerulus With many thanks to Elizabeth Angus PhD for EM photographs Anatomy of the Kidney http://www.yalemedicalgroup.org/stw/page.asp?pageid=stw028980 The Nephron http://www.beltina.org/health-dictionary/nephron-function-kidney-definition.html
Renal Pathology 1: Glomerulus With many thanks to Elizabeth Angus PhD for EM photographs Anatomy of the Kidney http://www.yalemedicalgroup.org/stw/page.asp?pageid=stw028980 The Nephron http://www.beltina.org/health-dictionary/nephron-function-kidney-definition.html
Atypical IgA Nephropathy
 Atypical IgA Nephropathy Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA XXXIII Chilean Congress of Nephrology, Hypertension and Transplantation Puerto Varas, Chile October 6, 2016 IgA
Atypical IgA Nephropathy Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA XXXIII Chilean Congress of Nephrology, Hypertension and Transplantation Puerto Varas, Chile October 6, 2016 IgA
C3 GLOMERULOPATHIES. Budapest Nephrology School Zoltan Laszik
 C3 GLOMERULOPATHIES Budapest Nephrology School 8.30.2018. Zoltan Laszik 1 Learning Objectives Familiarize with the pathogenetic mechanisms of glomerular diseases Learn the pathologic landscape and clinical
C3 GLOMERULOPATHIES Budapest Nephrology School 8.30.2018. Zoltan Laszik 1 Learning Objectives Familiarize with the pathogenetic mechanisms of glomerular diseases Learn the pathologic landscape and clinical
Prof. Rosanna Coppo Director of the Nephrology, Dialysis and Transplantation Department Regina Margherita Hospital Turin, Italy. Slide 1.
 ROLE OF PATHOLOGY AND CLINICAL FEATURES IN PREDICTING PROGRESSION OF IGA NEPHROPATHY: RESULTS FROM THE ERA-EDTA RESEARCH VALIGA Rosanna Coppo, Turin, Italy Chairs: François Berthoux, Saint-Etienne, France
ROLE OF PATHOLOGY AND CLINICAL FEATURES IN PREDICTING PROGRESSION OF IGA NEPHROPATHY: RESULTS FROM THE ERA-EDTA RESEARCH VALIGA Rosanna Coppo, Turin, Italy Chairs: François Berthoux, Saint-Etienne, France
Update on Transplant Glomerulopathy
 Update on Transplant Glomerulopathy Miklos Z Molnar, MD, PhD, FEBTM, FERA, FASN Associate Professor of Medicine Division of Nephrology, Department of Medicine University of Tennessee Health Science Center
Update on Transplant Glomerulopathy Miklos Z Molnar, MD, PhD, FEBTM, FERA, FASN Associate Professor of Medicine Division of Nephrology, Department of Medicine University of Tennessee Health Science Center
A clinical syndrome, composed mainly of:
 Nephritic syndrome We will discuss: 1)Nephritic syndrome: -Acute postinfectious (poststreptococcal) GN -IgA nephropathy -Hereditary nephritis 2)Rapidly progressive GN (RPGN) A clinical syndrome, composed
Nephritic syndrome We will discuss: 1)Nephritic syndrome: -Acute postinfectious (poststreptococcal) GN -IgA nephropathy -Hereditary nephritis 2)Rapidly progressive GN (RPGN) A clinical syndrome, composed
IgA Nephropathy: Morphologic Findings Associated with Disease Progression and Therapeutic Response A Working Group Approach
 I IgA Nephropathy: Morphologic Findings Associated with Disease Progression and Therapeutic Response A Working Group Approach Mark Haas Department of Pathology & Lab Medicine Cedars-Sinai Medical Center
I IgA Nephropathy: Morphologic Findings Associated with Disease Progression and Therapeutic Response A Working Group Approach Mark Haas Department of Pathology & Lab Medicine Cedars-Sinai Medical Center
Pathology of Complement Mediated Renal Disease
 Pathology of Complement Mediated Renal Disease Mariam Priya Alexander, MD Associate Professor of Pathology GN Symposium Hong Kong Society of Nephrology July 8 th, 2017 2017 MFMER slide-1 The complement
Pathology of Complement Mediated Renal Disease Mariam Priya Alexander, MD Associate Professor of Pathology GN Symposium Hong Kong Society of Nephrology July 8 th, 2017 2017 MFMER slide-1 The complement
Dr Ian Roberts Oxford. Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust
 Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Plan of attack: Diagnostic approach to the renal biopsy Differential diagnosis of the clinical syndromes of renal disease Microscopy Step
Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Plan of attack: Diagnostic approach to the renal biopsy Differential diagnosis of the clinical syndromes of renal disease Microscopy Step
James E. Cooper, M.D. Assistant Professor, University of Colorado at Denver Division of Renal Disease and Hypertension, Kidney and PancreasTransplant
 James E. Cooper, M.D. Assistant Professor, University of Colorado at Denver Division of Renal Disease and Hypertension, Kidney and PancreasTransplant Program Has no real or apparent conflicts of interest
James E. Cooper, M.D. Assistant Professor, University of Colorado at Denver Division of Renal Disease and Hypertension, Kidney and PancreasTransplant Program Has no real or apparent conflicts of interest
Nephrology Grand Rounds. Mansi Mehta November 24, 2015
 Nephrology Grand Rounds Mansi Mehta November 24, 2015 Case 51yo F with PMH significant for Hypertension referred to renal clinic for evaluation of elevated Cr. no known history of CKD; baseline creatinine
Nephrology Grand Rounds Mansi Mehta November 24, 2015 Case 51yo F with PMH significant for Hypertension referred to renal clinic for evaluation of elevated Cr. no known history of CKD; baseline creatinine
Glomerular diseases with organized deposits
 Glomerular diseases with organized deposits Banu Sis, MD, FRCPC University of Alberta, Edmonton, AB, Canada Ulusal Patoloji Kongresi, Manavgat, Antalya 8/11/2012 What is an organized deposit? A number
Glomerular diseases with organized deposits Banu Sis, MD, FRCPC University of Alberta, Edmonton, AB, Canada Ulusal Patoloji Kongresi, Manavgat, Antalya 8/11/2012 What is an organized deposit? A number
Diabetes, Obesity and Heavy Proteinuria
 Diabetes, Obesity and Heavy Proteinuria Clinical Case 41 yo Black woman with heavy proteinuria History 2014: noted to have proteinuria on routine lab testing (1.1g/g). 1+ edema. Blood pressure has been
Diabetes, Obesity and Heavy Proteinuria Clinical Case 41 yo Black woman with heavy proteinuria History 2014: noted to have proteinuria on routine lab testing (1.1g/g). 1+ edema. Blood pressure has been
Glomerular pathology in systemic disease
 Glomerular pathology in systemic disease Lecture outline Lupus nephritis Diabetic nephropathy Glomerulonephritis Associated with Bacterial Endocarditis and Other Systemic Infections Henoch-Schonlein Purpura
Glomerular pathology in systemic disease Lecture outline Lupus nephritis Diabetic nephropathy Glomerulonephritis Associated with Bacterial Endocarditis and Other Systemic Infections Henoch-Schonlein Purpura
RENAL HISTOPATHOLOGY
 RENAL HISTOPATHOLOGY Peter McCue, M.D. Department of Pathology, Anatomy & Cell Biology Sidney Kimmel Medical College There are no conflicts of interest. 1 Goals and Objectives! Goals Provide introduction
RENAL HISTOPATHOLOGY Peter McCue, M.D. Department of Pathology, Anatomy & Cell Biology Sidney Kimmel Medical College There are no conflicts of interest. 1 Goals and Objectives! Goals Provide introduction
Glomerular pathology-2 Nephritic syndrome. Dr. Nisreen Abu Shahin
 Glomerular pathology-2 Nephritic syndrome Dr. Nisreen Abu Shahin 1 The Nephritic Syndrome Pathogenesis: inflammation proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls
Glomerular pathology-2 Nephritic syndrome Dr. Nisreen Abu Shahin 1 The Nephritic Syndrome Pathogenesis: inflammation proliferation of the cells in glomeruli & leukocytic infiltrate Injured capillary walls
Biopsy Features of Kidney Allograft Rejection Banff B. Ivanyi, MD Department of Pathology, University of Szeged, Szeged, Hungary
 Biopsy Features of Kidney Allograft Rejection Banff 2017 B. Ivanyi, MD Department of Pathology, University of Szeged, Szeged, Hungary Treatment of allograft dysfunction should rely on the biopsy findings
Biopsy Features of Kidney Allograft Rejection Banff 2017 B. Ivanyi, MD Department of Pathology, University of Szeged, Szeged, Hungary Treatment of allograft dysfunction should rely on the biopsy findings
Tuesday Conference 7/23/2013. Hasan Fattah
 Tuesday Conference 7/23/2013 Hasan Fattah 48 AA male, PMH: HTN, proteinuria since 2009, sent from primary clinic for high Cr evaluation (7.1), last known of 1.1 in 2010 associated with sub-nephrotic range
Tuesday Conference 7/23/2013 Hasan Fattah 48 AA male, PMH: HTN, proteinuria since 2009, sent from primary clinic for high Cr evaluation (7.1), last known of 1.1 in 2010 associated with sub-nephrotic range
Histopathology: Glomerulonephritis and other renal pathology
 Histopathology: Glomerulonephritis and other renal pathology These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you
Histopathology: Glomerulonephritis and other renal pathology These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you
Elevated Serum Creatinine, a simplified approach
 Elevated Serum Creatinine, a simplified approach Primary Care Update Creighton University School of Medicine. April 27 th, 2018 Disclosure Slide I have no disclosures and have no conflicts with this presentation.
Elevated Serum Creatinine, a simplified approach Primary Care Update Creighton University School of Medicine. April 27 th, 2018 Disclosure Slide I have no disclosures and have no conflicts with this presentation.
Clinicopathologic Characteristics of IgA Nephropathy with Steroid-responsive Nephrotic Syndrome
 J Korean Med Sci 2009; 24 (Suppl 1): S44-9 ISSN 1011-8934 DOI: 10.3346/jkms.2009.24.S1.S44 Copyright The Korean Academy of Medical Sciences Clinicopathologic Characteristics of IgA Nephropathy with Steroid-responsive
J Korean Med Sci 2009; 24 (Suppl 1): S44-9 ISSN 1011-8934 DOI: 10.3346/jkms.2009.24.S1.S44 Copyright The Korean Academy of Medical Sciences Clinicopathologic Characteristics of IgA Nephropathy with Steroid-responsive
Darshana Dadhania 12 Fritz Diekmann 13 Klemens Budde 14 Fritz Lower 15 Babak J. Orandi 16 Ajda T. Rowshani 17 Lynn Cornell 18 Edward Kraus 19
 Received: 23 February 2018 Revised: 25 May 2018 Accepted: 31 May 2018 DOI: 10.1111/ajt.14979 ORIGINAL ARTICLE Banff survey on antibody mediated rejection clinical practices in kidney transplantation: Diagnostic
Received: 23 February 2018 Revised: 25 May 2018 Accepted: 31 May 2018 DOI: 10.1111/ajt.14979 ORIGINAL ARTICLE Banff survey on antibody mediated rejection clinical practices in kidney transplantation: Diagnostic
Proliferative Glomerulonephritis with Monoclonal IgG Deposits Recurs in the Allograft
 Article Proliferative Glomerulonephritis with Monoclonal IgG Deposits Recurs in the Allograft Samih H. Nasr,* Sanjeev Sethi,* Lynn D. Cornell,* Mary E. Fidler,* Mark Boelkins, Fernando C. Fervenza, Fernando
Article Proliferative Glomerulonephritis with Monoclonal IgG Deposits Recurs in the Allograft Samih H. Nasr,* Sanjeev Sethi,* Lynn D. Cornell,* Mary E. Fidler,* Mark Boelkins, Fernando C. Fervenza, Fernando
Case Report A Clinical and Pathological Variant of Acute Transplant Glomerulopathy
 Case Report A Clinical and Pathological Variant of Acute Transplant Glomerulopathy Miklos Z. Molnar, 1 G. V. Ramesh Prasad, 2 Darren A. Yuen, 2,3 Serge Jothy, 4 and Jeffrey S. Zaltzman 2,5 1 Division of
Case Report A Clinical and Pathological Variant of Acute Transplant Glomerulopathy Miklos Z. Molnar, 1 G. V. Ramesh Prasad, 2 Darren A. Yuen, 2,3 Serge Jothy, 4 and Jeffrey S. Zaltzman 2,5 1 Division of
Recognition and Treatment of Chronic Allograft Dysfunction
 Recognition and Treatment of Chronic Allograft Dysfunction Alexander Wiseman, M.D. Associate Professor, Division of Renal Diseases and Hypertension Medical Director, Kidney and Pancreas Transplant Programs
Recognition and Treatment of Chronic Allograft Dysfunction Alexander Wiseman, M.D. Associate Professor, Division of Renal Diseases and Hypertension Medical Director, Kidney and Pancreas Transplant Programs
Pathology of Kidney Allograft Dysfunction. B. Ivanyi, MD Department of Pathology, University of Szeged, Szeged, Hungary
 Pathology of Kidney Allograft Dysfunction B. Ivanyi, MD Department of Pathology, University of Szeged, Szeged, Hungary The gold standard for exploration of the cause of an allograft dysfunction is to perform
Pathology of Kidney Allograft Dysfunction B. Ivanyi, MD Department of Pathology, University of Szeged, Szeged, Hungary The gold standard for exploration of the cause of an allograft dysfunction is to perform
Familial DDD associated with a gain-of-function mutation in complement C3.
 Familial DDD associated with a gain-of-function mutation in complement C3. Santiago Rodríguez de Córdoba, Centro de investigaciones Biológicas, Madrid Valdés Cañedo F. and Vázquez- Martul E., Complejo
Familial DDD associated with a gain-of-function mutation in complement C3. Santiago Rodríguez de Córdoba, Centro de investigaciones Biológicas, Madrid Valdés Cañedo F. and Vázquez- Martul E., Complejo
IgA Nephropathy - «Maladie de Berger»
 IgA Nephropathy - «Maladie de Berger» B. Vogt, Division de Néphrologie/Consultation d Hypertension CHUV, Lausanne 2011 Montreux CME SGN-SSN IgA Nephropathy 1. Introduction 2. Etiology and Pathogenesis
IgA Nephropathy - «Maladie de Berger» B. Vogt, Division de Néphrologie/Consultation d Hypertension CHUV, Lausanne 2011 Montreux CME SGN-SSN IgA Nephropathy 1. Introduction 2. Etiology and Pathogenesis
Journal of Nephropathology
 www.nephropathol.com DOI: 10.15171/jnp.2017.36 J Nephropathol. 2017;6(3):220-224 Journal of Nephropathology Proliferative glomerulonephritis with monoclonal IgG deposits; an unusual cause of de novo disease
www.nephropathol.com DOI: 10.15171/jnp.2017.36 J Nephropathol. 2017;6(3):220-224 Journal of Nephropathology Proliferative glomerulonephritis with monoclonal IgG deposits; an unusual cause of de novo disease
Clinicopathological analysis of proliferative glomerulonephritis with monoclonal IgG deposits in 5 renal allografts
 Wen et al. BMC Nephrology (2018) 19:173 https://doi.org/10.1186/s12882-018-0969-3 RESEARCH ARTICLE Open Access Clinicopathological analysis of proliferative glomerulonephritis with monoclonal IgG deposits
Wen et al. BMC Nephrology (2018) 19:173 https://doi.org/10.1186/s12882-018-0969-3 RESEARCH ARTICLE Open Access Clinicopathological analysis of proliferative glomerulonephritis with monoclonal IgG deposits
Pathological back-ground of renal transplant pathology and important mile-stones of the Banff classification
 Banff 1 Banff Pathological back-ground of renal transplant pathology and important mile-stones of the Banff classification Department of Nephrology, Japanese Red Cross Nagoya Daini Hospital Morozumi Kunio,
Banff 1 Banff Pathological back-ground of renal transplant pathology and important mile-stones of the Banff classification Department of Nephrology, Japanese Red Cross Nagoya Daini Hospital Morozumi Kunio,
Lupus Related Kidney Diseases. Jason Cobb MD Assistant Professor Renal Division Emory University School of Medicine October 14, 2017
 Lupus Related Kidney Diseases Jason Cobb MD Assistant Professor Renal Division Emory University School of Medicine October 14, 2017 Financial Disclosures MedImmune Lupus Nephritis Kidney Biopsy Biomarkers
Lupus Related Kidney Diseases Jason Cobb MD Assistant Professor Renal Division Emory University School of Medicine October 14, 2017 Financial Disclosures MedImmune Lupus Nephritis Kidney Biopsy Biomarkers
Index. electron microscopy, 81 immunofluorescence microscopy, 80 light microscopy, 80 Amyloidosis clinical setting, 185 etiology/pathogenesis,
 A Acute antibody-mediated rejection (Acute AMR) clinical features, 203 clinicopathologic correlations, 206 pathogenesis, 205 206 204 205 light microscopy, 203 204 Acute cellular rejection (ACR) clinical
A Acute antibody-mediated rejection (Acute AMR) clinical features, 203 clinicopathologic correlations, 206 pathogenesis, 205 206 204 205 light microscopy, 203 204 Acute cellular rejection (ACR) clinical
HLA and Non-HLA Antibodies in Transplantation and their Management
 HLA and Non-HLA Antibodies in Transplantation and their Management Luca Dello Strologo October 29 th, 2016 Hystory I 1960 donor specific antibodies (DSA): first suggestion for a possible role in deteriorating
HLA and Non-HLA Antibodies in Transplantation and their Management Luca Dello Strologo October 29 th, 2016 Hystory I 1960 donor specific antibodies (DSA): first suggestion for a possible role in deteriorating
Glomerular Diseases. Anna Vinnikova, MD Nephrology
 Glomerular Diseases Anna Vinnikova, MD Nephrology Classification of Glomerular Diseases http://what-when-how.com/acp-medicine/glomerular-diseases-part-1/ Classification of pathologic and clinical manifestations
Glomerular Diseases Anna Vinnikova, MD Nephrology Classification of Glomerular Diseases http://what-when-how.com/acp-medicine/glomerular-diseases-part-1/ Classification of pathologic and clinical manifestations
J Nephropharmacol. 2014; 3(2): Journal of Nephropharmacology
: Journal of Nephropharmacology") J Nephropharmacol. 2014; 3(2): 33 37. NPJ Journal of Nephropharmacology Pathological patterns of mesangioproliferative glomerulonephritis seen at a tertiary care center Ghadeer A. Mokhtar 1*, Sawsan Jalalah
J Nephropharmacol. 2014; 3(2): 33 37. NPJ Journal of Nephropharmacology Pathological patterns of mesangioproliferative glomerulonephritis seen at a tertiary care center Ghadeer A. Mokhtar 1*, Sawsan Jalalah
Steroid Minimization: Great Idea or Silly Move?
 Steroid Minimization: Great Idea or Silly Move? Disclosures I have financial relationship(s) within the last 12 months relevant to my presentation with: Astellas Grants ** Bristol Myers Squibb Grants,
Steroid Minimization: Great Idea or Silly Move? Disclosures I have financial relationship(s) within the last 12 months relevant to my presentation with: Astellas Grants ** Bristol Myers Squibb Grants,
The new Banff vision of the role of HLA antibodies in organ transplantation: Improving diagnostic system and design of clinical trials
 The new Banff vision of the role of HLA antibodies in organ transplantation: Improving diagnostic system and design of clinical trials Carmen Lefaucheur 1 2 Banff 2015: Integration of HLA-Ab for improving
The new Banff vision of the role of HLA antibodies in organ transplantation: Improving diagnostic system and design of clinical trials Carmen Lefaucheur 1 2 Banff 2015: Integration of HLA-Ab for improving
CASE OF THE WEEK 1
 www.nephro-pathology.com CASE OF THE WEEK 1 Clinical Presentation: A 17 year old Indian boy presented with anasarca, decreased urine output and episodes of nausea and vomiting over the last three weeks.
www.nephro-pathology.com CASE OF THE WEEK 1 Clinical Presentation: A 17 year old Indian boy presented with anasarca, decreased urine output and episodes of nausea and vomiting over the last three weeks.
Case Report A Case of Proliferative Glomerulonephritis with Monoclonal IgG Deposits That Showed Predominantly Membranous Features
 Hindawi Case Reports in Nephrology Volume 2017, Article ID 1027376, 5 pages https://doi.org/10.1155/2017/1027376 Case Report A Case of Proliferative Glomerulonephritis with Monoclonal IgG Deposits That
Hindawi Case Reports in Nephrology Volume 2017, Article ID 1027376, 5 pages https://doi.org/10.1155/2017/1027376 Case Report A Case of Proliferative Glomerulonephritis with Monoclonal IgG Deposits That
Supplementary appendix
 Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Lefaucheur C, Loupy A, Vernerey D, et al. Antibody-mediated
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Lefaucheur C, Loupy A, Vernerey D, et al. Antibody-mediated
A Case of IgG2 Heavy Chain Deposition Disease in a Patient with Kappa Positive Plasma Cell Dyscrasia
 Published online: August 14, 2014 2296 9705/14/0051 0006$39.50/0 This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial 3.0 Unported license (CC BY-NC)
Published online: August 14, 2014 2296 9705/14/0051 0006$39.50/0 This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial 3.0 Unported license (CC BY-NC)
Pathology of Kidney Allograft Dysfunction. B. Ivanyi, MD Department of Pathology, University of Szeged, Szeged, Hungary
 Pathology of Kidney Allograft Dysfunction B. Ivanyi, MD Department of Pathology, University of Szeged, Szeged, Hungary The renal biopsy is a powerful tool in the diagnostic evaluation of allograft dysfunction
Pathology of Kidney Allograft Dysfunction B. Ivanyi, MD Department of Pathology, University of Szeged, Szeged, Hungary The renal biopsy is a powerful tool in the diagnostic evaluation of allograft dysfunction
Risk Factors in Long Term Immunosuppressive Use and Advagraf. Daniel Serón Nephrology department Hospital Universitari Vall d Hebron
 Risk Factors in Long Term Immunosuppressive Use and Advagraf Daniel Serón Nephrology department Hospital Universitari Vall d Hebron Progressive well defined diseases ABMR GN Polyoma Non-specific Findings
Risk Factors in Long Term Immunosuppressive Use and Advagraf Daniel Serón Nephrology department Hospital Universitari Vall d Hebron Progressive well defined diseases ABMR GN Polyoma Non-specific Findings
POST INFECTIOUS GLOMERULONEPHRITIS (PIGN) Anjali Gupta
 Anjali Gupta") POST INFECTIOUS GLOMERULONEPHRITIS (PIGN) Anjali Gupta PIGN One of the oldest recognized renal diseases. Now less commonly seen in industrialized nations, but in the underprivileged world, the burden remains
POST INFECTIOUS GLOMERULONEPHRITIS (PIGN) Anjali Gupta PIGN One of the oldest recognized renal diseases. Now less commonly seen in industrialized nations, but in the underprivileged world, the burden remains
Dr Ian Roberts Oxford
 Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing renal failure Highlight diagnostic pitfalls. Crescentic GN: renal
Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing renal failure Highlight diagnostic pitfalls. Crescentic GN: renal
STEROID-RESISTANT NEPHROTIC SYNDROME (SRNS)
") MARIO NEGRI INSTITUTE FOR PHARMACOLOGICAL RESEARCH CLINICAL RESEARCH CENTRE FOR RARE DISEASES ALDO E CELE DACCO' Villa Camozzi - 24020 Ranica (Bergamo) Italy Telephone 39-35-4535304 fax 39-35-4535373 STEROID-RESISTANT
MARIO NEGRI INSTITUTE FOR PHARMACOLOGICAL RESEARCH CLINICAL RESEARCH CENTRE FOR RARE DISEASES ALDO E CELE DACCO' Villa Camozzi - 24020 Ranica (Bergamo) Italy Telephone 39-35-4535304 fax 39-35-4535373 STEROID-RESISTANT
The transcriptome of the renal transplant biopsy: the lessons. Philip F Halloran
 The transcriptome of the renal transplant biopsy: the lessons Philip F Halloran Alberta Transplant Applied Genomics Centre April 27 th 2009 Congratulations on your 50 th anniversary ATAGC Learning objectives:
The transcriptome of the renal transplant biopsy: the lessons Philip F Halloran Alberta Transplant Applied Genomics Centre April 27 th 2009 Congratulations on your 50 th anniversary ATAGC Learning objectives:
CJASN epress. Published on September 28, 2010 as doi: /CJN
 CJASN epress. Published on September 28, 2010 as doi: 10.2215/CJN.05750710 Proliferative Glomerulonephritis with Monoclonal IgG Deposits Recurs in the Allograft Samih H. Nasr,* Sanjeev Sethi,* Lynn D.
CJASN epress. Published on September 28, 2010 as doi: 10.2215/CJN.05750710 Proliferative Glomerulonephritis with Monoclonal IgG Deposits Recurs in the Allograft Samih H. Nasr,* Sanjeev Sethi,* Lynn D.
Recurrent Diseases in the Transplant. Simin Goral MD University of Pennsylvania Medical Center Philadelphia, Pennsylvania
 Recurrent Diseases in the Transplant Simin Goral MD University of Pennsylvania Medical Center Philadelphia, Pennsylvania Case #1 21-year-old male, was on hemodialysis since September 2005 History of nephrotic
Recurrent Diseases in the Transplant Simin Goral MD University of Pennsylvania Medical Center Philadelphia, Pennsylvania Case #1 21-year-old male, was on hemodialysis since September 2005 History of nephrotic
Enterprise Interest None
 Enterprise Interest None Lupus Nephritis Ingeborg Bajema Lupus nephritis: the basics Up to 60% of patients with SLE develop lupus nephritis during the course of their disease Lupus nephritis is associated
Enterprise Interest None Lupus Nephritis Ingeborg Bajema Lupus nephritis: the basics Up to 60% of patients with SLE develop lupus nephritis during the course of their disease Lupus nephritis is associated
An unusual association between focal segmental sclerosis and lupus nephritis: a distinct concept from lupus podocytopathy?
 CEN Case Rep (2015) 4:70 75 DOI 10.1007/s13730-014-0142-1 CASE REPORT An unusual association between focal segmental sclerosis and lupus nephritis: a distinct concept from lupus podocytopathy? Hironari
CEN Case Rep (2015) 4:70 75 DOI 10.1007/s13730-014-0142-1 CASE REPORT An unusual association between focal segmental sclerosis and lupus nephritis: a distinct concept from lupus podocytopathy? Hironari
CKD in Other Organ Transplants
 CKD in Other Organ Transplants Alexander Wiseman, M.D. Associate Professor, Division of Renal Diseases and Hypertension Medical Director, Kidney and Pancreas Transplant Programs University of Colorado
CKD in Other Organ Transplants Alexander Wiseman, M.D. Associate Professor, Division of Renal Diseases and Hypertension Medical Director, Kidney and Pancreas Transplant Programs University of Colorado
Future Webinars. Handouts 18/09/ Program-Handouts.aspx
 Transplant Webinar Series: Ep. 9 Bio for Post-Transplant Immune Injury Future Webinars Link to register: https://immucor.webinato.com/register All Content 215 Immucor, Inc. Handouts http://www.immucor.com/en-us/pages/educational-
Transplant Webinar Series: Ep. 9 Bio for Post-Transplant Immune Injury Future Webinars Link to register: https://immucor.webinato.com/register All Content 215 Immucor, Inc. Handouts http://www.immucor.com/en-us/pages/educational-
ACCME/Disclosure. Case #1. Case History. Dr. Bracamonte has nothing to disclose
 Case #1 ACCME/Disclosure Dr. Erika Bracamonte Associate Professor of Pathology University of Arizona, College of Medicine Banner University Medical Center, Tucson Dr. Bracamonte has nothing to disclose
Case #1 ACCME/Disclosure Dr. Erika Bracamonte Associate Professor of Pathology University of Arizona, College of Medicine Banner University Medical Center, Tucson Dr. Bracamonte has nothing to disclose
Transplantation and 6-Month Follow-up of Renal Transplantation from a Donor with Systemic Lupus Erythematosus and Lupus Nephritis
 American Journal of Transplantation 2005; 5: 1772 1776 Blackwell Munksgaard Case Report Copyright C Blackwell Munksgaard 2005 doi: 10.1111/j.1600-6143.2005.00922.x Transplantation and 6-Month Follow-up
American Journal of Transplantation 2005; 5: 1772 1776 Blackwell Munksgaard Case Report Copyright C Blackwell Munksgaard 2005 doi: 10.1111/j.1600-6143.2005.00922.x Transplantation and 6-Month Follow-up
Clinical Findings, Pathology, and Outcomes of C3GN after Kidney Transplantation
 CLINICAL RESEARCH www.jasn.org Clinical Findings, Pathology, and Outcomes of C3GN after Kidney ation Ladan Zand,* Elizabeth C. Lorenz,* Fernando G. Cosio,* Fernando C. Fervenza,* Samih H. Nasr, Manish
CLINICAL RESEARCH www.jasn.org Clinical Findings, Pathology, and Outcomes of C3GN after Kidney ation Ladan Zand,* Elizabeth C. Lorenz,* Fernando G. Cosio,* Fernando C. Fervenza,* Samih H. Nasr, Manish
Nephrotic syndrome minimal change disease vs. IgA nephropathy. Hadar Meringer Internal medicine B Sheba
 Nephrotic syndrome minimal change disease vs. IgA nephropathy Hadar Meringer Internal medicine B Sheba The Case 29 year old man diagnosed with nephrotic syndrome 2 weeks ago and complaining now about Lt.flank
Nephrotic syndrome minimal change disease vs. IgA nephropathy Hadar Meringer Internal medicine B Sheba The Case 29 year old man diagnosed with nephrotic syndrome 2 weeks ago and complaining now about Lt.flank
Transplant Webinar Series: Ep. 9 Biomarkers for Post-Transplant Immune Injury
 Transplant Webinar Series: Ep. 9 Biomarkers for Post-Transplant Immune Injury Future Webinars Link to register: https://immucor.webinato.com/register All Content 2015 Immucor, Inc. Handouts http://www.immucor.com/en-us/pages/educational-
Transplant Webinar Series: Ep. 9 Biomarkers for Post-Transplant Immune Injury Future Webinars Link to register: https://immucor.webinato.com/register All Content 2015 Immucor, Inc. Handouts http://www.immucor.com/en-us/pages/educational-
Lupus Nephritis. Ingeborg Bajema
 Lupus Nephritis Ingeborg Bajema Lupus nephritis: the basics Up to 60% of patients with SLE develop lupus nephritis during the course of their disease Lupus nephritis is associated with considerable morbidity
Lupus Nephritis Ingeborg Bajema Lupus nephritis: the basics Up to 60% of patients with SLE develop lupus nephritis during the course of their disease Lupus nephritis is associated with considerable morbidity
Clinical and pathologic characteristics of focal segmental glomerulosclerosis pathologic variants
 original article http://www.kidney-international.org & 2006 International Society of Nephrology Clinical and pathologic characteristics of focal segmental glomerulosclerosis pathologic variants DB Thomas
original article http://www.kidney-international.org & 2006 International Society of Nephrology Clinical and pathologic characteristics of focal segmental glomerulosclerosis pathologic variants DB Thomas
C3 Glomerulopathy. Jun-Ki Park
 C3 Glomerulopathy Jun-Ki Park 03.08.11 For the last 30 years classification MPGN is based on glomerular findings by light microscopy with further specification on EM and staining for Ig and complement
C3 Glomerulopathy Jun-Ki Park 03.08.11 For the last 30 years classification MPGN is based on glomerular findings by light microscopy with further specification on EM and staining for Ig and complement
Dr Michael Rayment Chelsea and Westminster Hospital, London
 17 TH ANNUAL CONFERENCE OF THE BRITISH HIV ASSOCIATION (BHIVA) Dr Michael Rayment Chelsea and Westminster Hospital, London 6-8 April 2011, Bournemouth International Centre A decade of renal biopsies in
17 TH ANNUAL CONFERENCE OF THE BRITISH HIV ASSOCIATION (BHIVA) Dr Michael Rayment Chelsea and Westminster Hospital, London 6-8 April 2011, Bournemouth International Centre A decade of renal biopsies in
Interesting case seminar: Native kidneys Case Report:
 Interesting case seminar: Native kidneys Case Report: Proximal tubulopathy and light chain deposition disease presented as severe pulmonary hypertension with right-sided cardiac dysfunction and nephrotic
Interesting case seminar: Native kidneys Case Report: Proximal tubulopathy and light chain deposition disease presented as severe pulmonary hypertension with right-sided cardiac dysfunction and nephrotic
Donor-derived Cell-free DNA Improves DSA-informed Diagnosis of ABMR in Kidney Transplant Patients
 Donor-derived Cell-free DNA Improves DSA-informed Diagnosis of ABMR in Kidney Transplant Patients Stanley C. Jordan, MD Director, Division of Nephrology Medical Director, Kidney Transplant Program Medical
Donor-derived Cell-free DNA Improves DSA-informed Diagnosis of ABMR in Kidney Transplant Patients Stanley C. Jordan, MD Director, Division of Nephrology Medical Director, Kidney Transplant Program Medical
THROMBOTIC MICROANGIOPATHY (TMA) BANFF WORKING GROUP. Marjan Afrouzian, Chair
 BANFF WORKING GROUP. Marjan Afrouzian, Chair") THROMBOTIC MICROANGIOPATHY (TMA) BANFF WORKING GROUP Marjan Afrouzian, Chair Assistant Professor Department of Pathology University of Texas Medical Branch (UTMB) USA TMA in renal allograft can be a challenging
THROMBOTIC MICROANGIOPATHY (TMA) BANFF WORKING GROUP Marjan Afrouzian, Chair Assistant Professor Department of Pathology University of Texas Medical Branch (UTMB) USA TMA in renal allograft can be a challenging
Case Report Nephrotic Syndrome Secondary to Proliferative Glomerulonephritis with Monoclonal Immunoglobulin Deposits of Lambda Light Chain
 Hindawi Publishing Corporation Case Reports in Nephrology Volume 214, Article ID 164694, 6 pages http://dx.doi.org/1.1155/214/164694 Case Report Nephrotic Syndrome Secondary to Proliferative Glomerulonephritis
Hindawi Publishing Corporation Case Reports in Nephrology Volume 214, Article ID 164694, 6 pages http://dx.doi.org/1.1155/214/164694 Case Report Nephrotic Syndrome Secondary to Proliferative Glomerulonephritis
Research Article Transplant Outcomes in Patients with Idiopathic Membranous Nephropathy
 International Nephrology Volume 2013, Article ID 818537, 4 pages http://dx.doi.org/10.1155/2013/818537 Research Article Transplant Outcomes in Patients with Idiopathic Membranous Nephropathy Claire Kennedy,
International Nephrology Volume 2013, Article ID 818537, 4 pages http://dx.doi.org/10.1155/2013/818537 Research Article Transplant Outcomes in Patients with Idiopathic Membranous Nephropathy Claire Kennedy,
Recurrent Idiopathic Membranous Glomerulonephritis After Kidney Transplantation and Successful Treatment With Rituximab
 TRANSPLANTATION Recurrent Idiopathic Membranous Glomerulonephritis After Kidney Transplantation and Successful Treatment With Rituximab Khadijeh Makhdoomi, 1,2 Saeed Abkhiz, 1,2 Farahnaz Noroozinia, 1,3
TRANSPLANTATION Recurrent Idiopathic Membranous Glomerulonephritis After Kidney Transplantation and Successful Treatment With Rituximab Khadijeh Makhdoomi, 1,2 Saeed Abkhiz, 1,2 Farahnaz Noroozinia, 1,3
DSA Positive and then To biopsy or not?
 DSA Positive and then To biopsy or not? Banff SCT 2017 29 March 2017 Peter Nickerson, MD, FRCPC, FCAHS Flynn Family Chair in Renal Transplantation Professor of Internal Medicine and Immunology Relevant
DSA Positive and then To biopsy or not? Banff SCT 2017 29 March 2017 Peter Nickerson, MD, FRCPC, FCAHS Flynn Family Chair in Renal Transplantation Professor of Internal Medicine and Immunology Relevant