INTRAVENOUS FLUIDS. Ahmad AL-zu bi
|
|
|
- Julie Parker
- 5 years ago
- Views:
Transcription
1 INTRAVENOUS FLUIDS Ahmad AL-zu bi
2 Types of IV fluids Crystalloids colloids
3 Crystalloids Crystalloids are aqueous solutions of low molecular weight ions,with or without glucose. Isotonic, Hypotonic, & Hypertonic Fluids
4 Isotonic Iso: same/equal Tonic: concentration of a solution Isotonic fluids 0.9% Saline 5% dextrose in water (D5W)**also used as a hypotonic solution after it is administered because the body absorbs the dextrose BUT it is considered isotonic) 5% Dextrose in 0.225% saline (D5W1/4NS) Lactated Ringer s
5 Hypotonic Hypo: under/beneath Tonic: concentration of a solution The cell has a low amount of solute extracellularly and it wants to shift inside the cell to get everything back to normal via osmosis. This will cause CELL SWELLING which can cause the cell to burst or lyses. Hypotonic solutions 0.45% Saline (1/2 NS) 0.225% Saline (1/4 NS) 0.33% saline (1/3 NS) Hypotonic solutions are used when the cell is dehydrated and fluids need to be put back intracellularly. This happens when patients develop diabetic ketoacidosis (DKA) or hyperosmolar hyperglycemia. Important: Watch out for depleting the circulatory system of fluid since you are trying to push extracellular fluid into the cell to re-hydrate it. Never give hypotonic solutions to patient who are at risk for increased cranial pressure (can cause fluid to shift to brain tissue), extensive burns, trauma (already hypovolemic) etc. because you can deplete their fluid volume
6 Hypertonic solutions 3% Saline 5% Saline 10% Dextrose in Water (D10W) 5% Dextrose in 0.9% Saline 5% Dextrose in 0.45% saline 5% Dextrose in Lactated Ringer s When hypertonic solutions are used (very cautiously.most likely to be given in the ICU due to quickly arising side effects of pulmonary edema/fluid over load). In addition, it is prefered to give hypertonic solutions via a central line due to the hypertonic solution being vesicant on the veins and the risk of infiltration.
7
8 Solutions are chosen according to the type of fluid loss being replaced : For losses primarily involving water, replacement is hypotonic solutions also known as maintenance type solutions like: Dextrose solution 5% If losses involve both water and electrolytes replacement is with isotonic electrolytes solutions or replacement type solutions like: ringer s lactate
9 Normal saline or sodium chloride 0.9% is a mixture of sodium chloride in water that is slightly hypertonic and contains more chloride than ECF aggressive volume resuscitation with normal saline >>? Normal saline is the preferred solution for 1. hypochloremic metabolic alkalosis 2. diluting packed red blood cells prior to transfusion
10 Five percent dextrose in water (D5W) It is a hypotonic,isosmotic solution that doesn t contain electrolytes Dextrose solution is equivalent to administering water that s why 1. It is used for replacement of pure water deficits 2. as a maintenance fluid for patients on sodium restriction (hypernatremia) 3. It prevents the catabolic state (hypoglycemia and ketosis ) that follows prolonged fasting 4.More concentrated dextrose solutions (10%,20% and 50%) are available but their use is limited to the management of diabetic patients and patients of hypoglycemia
11 lactated Ringer s solution Ringer's lactate solution or (Hartmann's solution), is a mixture of sodium chloride, sodium lactate, potassium chloride, and calcium chloride in water Uses of ringer lactate 1. It is used for replacing fluids and electrolytes in those who have low blood volume or low blood pressure. 2. It may also be used to treat metabolic acidosis in cases other than those caused by lactic acidosis 3. And to wash the eye following a chemical burn
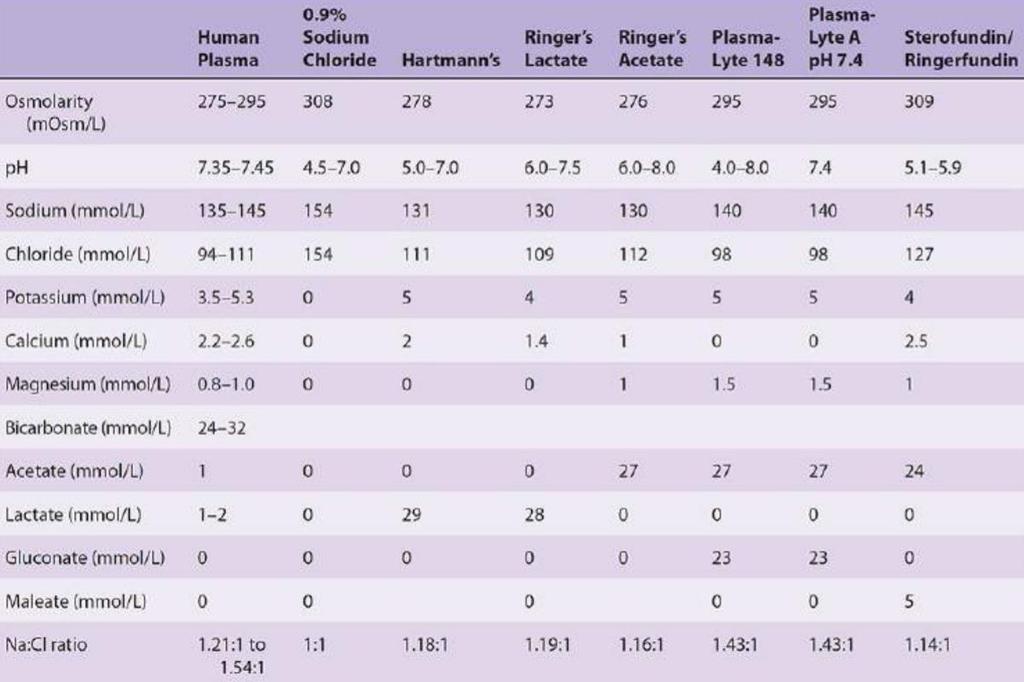
12 Other types of solutions: Plasmalyte : is a family of balanced crystalloid solutions with multiple different formulations available It closely mimics human plasma in content of electrolytes, osmolality and ph that s why it is a replacement type solution Hypertonic 3% saline is employed in therapy of severe symptomatic hyponatremia
13 colloids Are those containing high mw substances that exert an oncotic pressure indications for colloids include 1. fluid resuscitation in patients with severe intravascular fluid deficits (eg, hemorrhagic shock) prior to the arrival of blood for transfusion 2. fluid resuscitation in the presence of severe hypoalbuminemia or conditions associated with large protein losses such as burns. (Replacing an intravascular volume deficit with crystalloids generally requires three to four times the volume needed when using colloids, this justifies their indication for the use where more than 3_4 liters of crystalloid solution has been injected
14 colloids Natural (human albumin) Artificial (gelatins, dextrans and hydroxyethyl starches)
15 Albumin Half life =1.6 hours in plasma Stays in intravascular space 5% solution isotonic 10% and 25% hypertonic Expands volume 5x in 30 minutes and its effect lasts 1-2 days Side effects : 1. volume overload 2. Fever 3. Defects in hemostasis
16 Advantages: Natural colloid: As albumin is a natural colloid it is associated with lesser side-effects like pruritus, anaphylactic reactions and coagulation abnormalities compared to synthetic colloids. Degree of volume expansion: 25%Albumin has a greater degree of volume expansion as compared to rest of colloids. 5% albumin solution has a similar degree of volume expansion as compared to hetastarch but greater than gelatins and dextrans. Other benefits: Albumin acts a principal binding protein of endogenous and exogenous substances. It also possesses antioxidant effects. Albumin being negatively charged protein contributes to the formation of normal anion gap, influencing the acid-base status.
17 Synthetic colloids gelatins dextrose starches Dextran High molecular weight polysaccharide (40000 >coagulation effect than dextran ) 10% solution in NS or D5W SE: anaphylaxis, coagulopathy,renal failure is used as a volume expander but also reduces blood viscosity, von Willebrand factor antigen, platelet adhesion, and red blood cell aggregation,that s why it is used by microsurgeons to improve microcirculatory flow and decrease risk of microthrombus formation
18 hydroxyethyl starch is highly effective as a plasma expander and is less expensive than albumin. Allergic reactions are rare, but anaphylactic reactions have been reported Hetastarch can decrease von Willebrand factor antigen levels, may prolong the prothrombin time, and has been associated with hemorrhagic complications. It is potentially nephrotoxic
19 Differences Colloids are more expensive than crystalloids Colloids have higher molecular weight Half life of crystalloids is between 15 to 20 minutes while colloids last 2-3hrs Colloids act as plasma expanders
20 Intraoperative fluid requirements Optimal perioperative fluid therapy requires an understanding of the changes that occur in the volume and composition of the body fluid compartments.. Intravenous fluids are used to replenish fluid losses while maintaning : ** intravascular volume ( which is essential for adequate perfusion of vital organs ) ** cardiac preload ** oxygen-carrying capacity ** coagulation status ** acid-base balance ** electrolyte balance
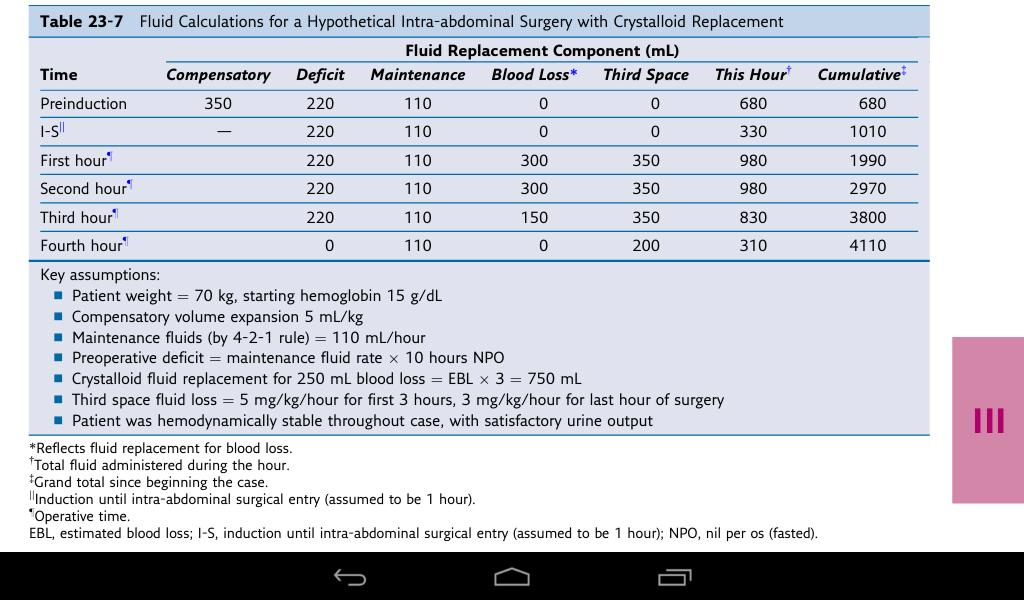
21 The total fluid requirement is composed of : compensatory intravascular volume expansion (CVE).. maintenance fluids.. preoperative deficits ( NPO,, GI losses,, blood loss ) ongoing surgical Losses ( evaporation,, blood loss,, 3de space loss )..
22 compensatory intravascular volume expansion Intravascular volume must usually be supplemented to compensate for the venodilation and cardiac depression caused by anesthesia.. Increasing cardiac preload by infusing fluid intravascularly to return stroke volume to an acceptable range.. 5 ml/kg of balanced salt solution (Ringer's lactate) should be introduced before or simultaneous with the onset of anesthesia.. Postoperatively ; venodilation and cardiac depression rapidly subside when administration of the anesthetic is stopped.. ** Note : Patients with impaired cardiac or renal responses may then become acutely hypervolemic!!
23 Maintenance fluids Maintenance fluid requirements for any body weight can be calculated using the : "4-2-1" rule for hourly fluid requirements or the " " rule for daily fluid requirements For example, a 75 kg adult will require: Per hour: 10 kg x 4 ml/hr = 40 ml/hr 10 kg x 2 ml/hr = 20 ml/hr 55 x 1 ml/hr = 55 ml/hr Total : 75 kg 115 ml/hr Per day: 10 kg x 100 ml/day = 1000 ml/day 10 kg x 50 ml/day = 500 ml/day 55 x 20 ml/day = 1100 ml/day Total : 75 kg 2600 ml/day
24 Preoperative deficits 1. as a result of a period of fasting ( NPO deficit ) : In the absence of oral intake ; fluid and electrolyte deficits can rapidly develop as a result of continued urine formation, gastrointestinal secretions, and insensible losses ( from the skin and lungs ).. can be calculated by multiplying the patient's hourly maintenance requirements by the number of hours fasted ---> Maintenance requirements / hour x number of hours fasted $ 75 kg 115 ml/hr $ = = 920 ml ** in surgery that takes 4 hrs for ex. we give half deficit in 1 st hour ( 920/2 = 460) & other half divided by 3hrs ( 460/3 ) per hr ** 2. preoperative losses from the gastrointestinal tract ( eg. vomitting or diarrhea ),, best replaced with a crystalloid of similar composition (0.9% NS or Ringer s lactate )
25 intraoperative deficits 3. Blood loss** < 15% blood loss we use crystlloids ; If 1000 ml of NS is infused intravenously ; only 1/3 (approx. 300 ml) will remain in the intravascular compartment,, the remaining 2/3 ( 700 ml) will move into the interstitial and intracellular compartments 3 times the volume of blood lost must be infused when crystalloids (NS or RL) are used to maintain the intravascular volume ( 3:1volume basis ) % blood loss use colloids ; given in a volume similar to the estimated deficit to maintain the circulating volume (1:1 volume basis)..
26 intraoperative deficits > 30% start to transfuse blood (unit-for-unit) esp in young patients.. in children we start blood transfusion at 10% blood loss.. in elderly & preexisting medical condition as in IHD start blood transusion at 20% blood loss..
27 Blood loss we prefer to start with crystalloids in replacement of blood loss bcz they're safer.. we don't prefer to use colloids bcz of the side effects ( eg. coagulopathy,, anaphylaxis.. ).. we don't prefer to transfuse blood bcz of the complications until the danger of anemia outweighs the risks of transfusion ( transfusion point )then we should transfuse blood ( red blood cells to maintain hemoglobin concentration or hematocrit at certian level ).. usually we start the procedure when Hb >10g/dl esp in elderly and sicker patients with cardiac or pulmonary disease but could be acceptalble >7-8 g/dl in younger & medically free patient
28 Blood loss The transfusion point can be determined preoperatively from the hematocrit and by estimating blood volume.. hematocrit : volume percentage (%) of red blood cells in blood in (Men= 42-52%,, Women= 37-47%) blood volume : can be either calculated in formula ( plasma volume/ 1-hematocrit ) or generally estimated as in table below : Age group Average blood volume (ml/kg) Premature neonates 95 Full-term neonates 85 Infants 80 Adult male 75 Adult female 65
29 ** the amount of blood loss necessary for the hematocrit to fall to 30% can be calculated as follows : 1. Estimate blood volume from. 2. Estimate the red blood cell volume (RBCV) at the preoperative hematocrit (RBCV preop ). 3. Estimate RBCV at a hematocrit of 30% (RBCV 30% ), assuming normal blood volume is maintained. 4. Calculate the RBCV lost when the hematocrit is 30%; RBCV lost = RBCV preop RBCV 30%. 5. Allowable blood loss = RBCV lost 3
30 example : An 85-kg woman has a preoperative hematocrit of 35% How much blood loss will decrease her hematocrit to 30%? Estimated blood volume = 65 ml/kg 85 kg = 5525 ml. RBCV 35% = % = 1934 ml. RBCV 30% = % = 1658 ml. Red cell loss at 30% = = 276 ml. Allowable blood loss = ml = 828 ml.
31 <4> ongoing surgical Losses 1. Evaporation : This can occur during body cavity surgery or when large areas of tissues are exposed,, and here evaporation from exposed viscera is entirely water, but the electrolyte is left behind, leading to a need for free water.. 2. Blood loss : Depends upon the type and site of surgery.. 3. Third space loss : -->
32 third space first ( intravascular ) and second ( interstitial ) spaces are the constituents of the ECF which are normal physiological compartments.. "third space" is a space in the body where fluid does not normally collect in larger amounts,, it's related to and formed from the ECF,, examples : ** peritoneal cavity ( eg. ascites ).. ** pleural cavity ( eg. pleural effusion ).. ** lumen of the gastrointestinal tract ( as in a patient with ileus ).. ** swelling of the tissues after surgical trauma or burns.. Replacing third space fluid losses is a ( ml/kg/hr ) rule ; 4 for minor trauma ( eg. hernia, tonsilictomy ), 6 for moderate trauma ( eg. hysterectomy), 8 for major trauma ( eg. AAA repair)
33
34 Liberal versus Restrictive Fluid Management routine intraoperative fluid management strategy has been criticized,, ex. in lung surgery ; the risk of postpneumonectomy pulmonary edema is clearly associated with the amount of administered fluid,, ** As a result ; fluid-conservative or dry fluid strategies are now commonly employed for patients undergoing lung surgery.. another ex. gastrointestinal surgery Excessive perioperative fluid administration may also lead to edema of the gastrointestinal tract contributing to ileus,, ** perioperative fluid restriction can lead to improved outcomes after major elective gastrointestinal surgery..
35 Restrictive Fluid Management There are several approaches to fluid restriction : ** Replacement of blood loss on a ml per ml basis with colloid.. ** No replacement of third space loss during surgery.. ** No fluid loading prior to general anesthesia.. ** Postoperative restriction of fluids with administration of diuretics..
36 Monitoring Adequacy of Fluid Replacement ** Vital Signs : BP and HR if patient get hypotensive during surgery most likely cause is hypovolemia and 1st sign is tachycardia,, but,, Anesthetic drugs can cause hypotension and mask traditional signs of hypovolemia such as tachycardia.. ** Urine output : Nl --> 1.0 ml/kg/hr Decreased intraoperative urine output does not necessarily indicate hypovolemia but could be of help.. ** periodic monitoring of hemoglobin and hematocrit.. ** Invasive monitoring : - central venous pressure (It is a good approximation of right atrial pressure,, used as a surrogate for preload,, changes in CVP in response to infusions of intravenous fluid have been used to predict volume-responsiveness ) - transesophageal echocardiography
IV Fluids. I.V. Fluid Osmolarity Composition 0.9% NaCL (Normal Saline Solution, NSS) Uses/Clinical Considerations
 Uses/Clinical Considerations") IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
KASHVET VETERINARIAN RESOURCES FLUID THERAPY AND SELECTION OF FLUIDS
 KASHVET VETERINARIAN RESOURCES FLUID THERAPY AND SELECTION OF FLUIDS INTRODUCTION Formulating a fluid therapy plan for the critical small animal patient requires careful determination of the current volume
KASHVET VETERINARIAN RESOURCES FLUID THERAPY AND SELECTION OF FLUIDS INTRODUCTION Formulating a fluid therapy plan for the critical small animal patient requires careful determination of the current volume
HYPOVOLEMIA AND HEMORRHAGE UPDATE ON VOLUME RESUSCITATION HEMORRHAGE AND HYPOVOLEMIA DISTRIBUTION OF BODY FLUIDS 11/7/2015
 UPDATE ON VOLUME RESUSCITATION HYPOVOLEMIA AND HEMORRHAGE HUMAN CIRCULATORY SYSTEM OPERATES WITH A SMALL VOLUME AND A VERY EFFICIENT VOLUME RESPONSIVE PUMP. HOWEVER THIS PUMP FAILS QUICKLY WITH VOLUME
UPDATE ON VOLUME RESUSCITATION HYPOVOLEMIA AND HEMORRHAGE HUMAN CIRCULATORY SYSTEM OPERATES WITH A SMALL VOLUME AND A VERY EFFICIENT VOLUME RESPONSIVE PUMP. HOWEVER THIS PUMP FAILS QUICKLY WITH VOLUME
FLUID THERAPY: IT S MORE THAN JUST LACTATED RINGERS
 FLUID THERAPY: IT S MORE THAN JUST LACTATED RINGERS Elisa M. Mazzaferro, MS, DVM, PhD, DACVECC Cornell University Veterinary Specialists, Stamford, CT, USA Total body water constitutes approximately 60%
FLUID THERAPY: IT S MORE THAN JUST LACTATED RINGERS Elisa M. Mazzaferro, MS, DVM, PhD, DACVECC Cornell University Veterinary Specialists, Stamford, CT, USA Total body water constitutes approximately 60%
Principles of Infusion Therapy: Fluids
 Principles of Infusion Therapy: Fluids Christie Heinzman, MSN, APRN-CNP Acute Care Pediatric Nurse Practitioner Cincinnati Children s Hospital Medical Center May 22, 2018 Conflict of Interest Disclosure
Principles of Infusion Therapy: Fluids Christie Heinzman, MSN, APRN-CNP Acute Care Pediatric Nurse Practitioner Cincinnati Children s Hospital Medical Center May 22, 2018 Conflict of Interest Disclosure
Presented by: Indah Dwi Pratiwi
 Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
Basic Fluid and Electrolytes
 Basic Fluid and Electrolytes Chapter 22 Basic Fluid and Electrolytes Introduction Infants and young children have a greater need for water and are more vulnerable to alterations in fluid and electrolyte
Basic Fluid and Electrolytes Chapter 22 Basic Fluid and Electrolytes Introduction Infants and young children have a greater need for water and are more vulnerable to alterations in fluid and electrolyte
Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES
 Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES Body Water Content Water Balance: Normal 2500 2000 1500 1000 500 Metab Food Fluids Stool Breath Sweat Urine
Amjad Bani Hani Ass.Prof. of Cardiac Surgery & Intensive Care FLUIDS AND ELECTROLYTES Body Water Content Water Balance: Normal 2500 2000 1500 1000 500 Metab Food Fluids Stool Breath Sweat Urine
Dr. Dafalla Ahmed Babiker Jazan University
 Dr. Dafalla Ahmed Babiker Jazan University objectives Overview Definition of dehydration Causes of dehydration Types of dehydration Diagnosis, signs and symptoms Management of dehydration Complications
Dr. Dafalla Ahmed Babiker Jazan University objectives Overview Definition of dehydration Causes of dehydration Types of dehydration Diagnosis, signs and symptoms Management of dehydration Complications
INTRAVENOUS FLUID THERAPY. Tom Heaps Consultant Acute Physician
 INTRAVENOUS FLUID THERAPY Tom Heaps Consultant Acute Physician LEARNING OBJECTIVES 1. Crystalloids vs colloids 2. Balanced vs non-balanced solutions 3. Composition of various IV fluids 4. What is normal
INTRAVENOUS FLUID THERAPY Tom Heaps Consultant Acute Physician LEARNING OBJECTIVES 1. Crystalloids vs colloids 2. Balanced vs non-balanced solutions 3. Composition of various IV fluids 4. What is normal
How and why I give IV fluid Disclosures SCA Fluids and public health 4/1/15. Andrew Shaw MB FRCA FCCM FFICM
 How and why I give IV fluid Andrew Shaw MB FRCA FCCM FFICM Professor and Chief Cardiothoracic Anesthesiology Vanderbilt University Medical Center 2015 Disclosures Consultant for Grifols manufacturer of
How and why I give IV fluid Andrew Shaw MB FRCA FCCM FFICM Professor and Chief Cardiothoracic Anesthesiology Vanderbilt University Medical Center 2015 Disclosures Consultant for Grifols manufacturer of
12/29/2014. IV/IO Therapy & Fluid Administration. Objectives. Cleansing of the soul
 IV/IO Therapy & Fluid Administration Gary Hoertz, EMT-P Spokane County EMS Indications for IV Access Types of Intravenous Access IV fluids Flow Rates Fluid resuscitation Objectives Cleansing of the soul
IV/IO Therapy & Fluid Administration Gary Hoertz, EMT-P Spokane County EMS Indications for IV Access Types of Intravenous Access IV fluids Flow Rates Fluid resuscitation Objectives Cleansing of the soul
Proceeding of the LAVC Latin American Veterinary Conference Oct , 2011 Lima, Peru
 Close this window to return to IVIS www.ivis.org Proceeding of the LAVC Latin American Veterinary Conference Oct. 24-26, 2011 Lima, Peru Next LAVC Conference: Apr. 24-26, 2012 Lima, Peru Reprinted in the
Close this window to return to IVIS www.ivis.org Proceeding of the LAVC Latin American Veterinary Conference Oct. 24-26, 2011 Lima, Peru Next LAVC Conference: Apr. 24-26, 2012 Lima, Peru Reprinted in the
Water (Dysnatremia) & Sodium (Dysvolemia) Disorders Ahmad Raed Tarakji, MD, MSPH, PGCertMedEd, FRCPC, FACP, FASN, FNKF, FISQua
 & Sodium (Dysvolemia) Disorders Ahmad Raed Tarakji, MD, MSPH, PGCertMedEd, FRCPC, FACP, FASN, FNKF, FISQua") Water (Dysnatremia) & Sodium (Dysvolemia) Disorders Ahmad Raed Tarakji, MD, MSPH, PGCertMedEd, FRCPC, FACP, FASN, FNKF, FISQua Assistant Professor Nephrology Unit, Department of Medicine College of Medicine,
Water (Dysnatremia) & Sodium (Dysvolemia) Disorders Ahmad Raed Tarakji, MD, MSPH, PGCertMedEd, FRCPC, FACP, FASN, FNKF, FISQua Assistant Professor Nephrology Unit, Department of Medicine College of Medicine,
Principles of Fluid Balance
 Principles of Fluid Balance I. The Cellular Environment: Fluids and Electrolytes A. Water 1. Total body water (TBW) = 60% of total body weight 2. Fluid Compartments in the Body a. Intracellular Compartment
Principles of Fluid Balance I. The Cellular Environment: Fluids and Electrolytes A. Water 1. Total body water (TBW) = 60% of total body weight 2. Fluid Compartments in the Body a. Intracellular Compartment
Fluid & Electrolyte Therapy. Prof. Soliman Ali Hassan Prof. of Surgery Taibah university
 Fluid & Electrolyte Therapy By Prof. Soliman Ali Hassan Prof. of Surgery Taibah university Fluid and electrolyte therapy Learning objectives At the end of this lecture, 1-The student should have an idea
Fluid & Electrolyte Therapy By Prof. Soliman Ali Hassan Prof. of Surgery Taibah university Fluid and electrolyte therapy Learning objectives At the end of this lecture, 1-The student should have an idea
What would be the response of the sympathetic system to this patient s decrease in arterial pressure?
 CASE 51 A 62-year-old man undergoes surgery to correct a herniated disc in his spine. The patient is thought to have an uncomplicated surgery until he complains of extreme abdominal distention and pain
CASE 51 A 62-year-old man undergoes surgery to correct a herniated disc in his spine. The patient is thought to have an uncomplicated surgery until he complains of extreme abdominal distention and pain
Fluids and Lactate. A/Prof Peter Morley
 Fluids and Lactate A/Prof Peter Morley RCTs Other evidence 5 6 Plan Background information Crystalloids Which crystalloid? Colloids Crystalloids v colloids Once that s settled, how much fluid Plan Background
Fluids and Lactate A/Prof Peter Morley RCTs Other evidence 5 6 Plan Background information Crystalloids Which crystalloid? Colloids Crystalloids v colloids Once that s settled, how much fluid Plan Background
Body fluids. Lecture 13:
 Lecture 13: Body fluids Body fluids are distributed in compartments: A. Intracellular compartment: inside the cells of the body (two thirds) B. Extracellular compartment: (one third) it is divided into
Lecture 13: Body fluids Body fluids are distributed in compartments: A. Intracellular compartment: inside the cells of the body (two thirds) B. Extracellular compartment: (one third) it is divided into
Maria B. ALBUJA-CRUZ, MD ALBUMIN: OVERRATED. Surgical Grand Rounds
 Maria B. ALBUJA-CRUZ, MD ALBUMIN: OVERRATED Surgical Grand Rounds ALBUMIN Most abundant plasma protein 1/3 intravascular 50% of interstitial SKIN Synthesized in hepatocytes Transcapillary escape rate COP
Maria B. ALBUJA-CRUZ, MD ALBUMIN: OVERRATED Surgical Grand Rounds ALBUMIN Most abundant plasma protein 1/3 intravascular 50% of interstitial SKIN Synthesized in hepatocytes Transcapillary escape rate COP
Proceeding of the LAVECCS
 Close this window to return to IVIS Proceeding of the LAVECCS Congreso Latinoamericano de Emergencia y Cuidados Intensivos Ju1. 28-30, 2011 Santiago de Chile, Chile www.laveccs.org Reprinted in IVIS with
Close this window to return to IVIS Proceeding of the LAVECCS Congreso Latinoamericano de Emergencia y Cuidados Intensivos Ju1. 28-30, 2011 Santiago de Chile, Chile www.laveccs.org Reprinted in IVIS with
-Cardiogenic: shock state resulting from impairment or failure of myocardium
 Shock chapter Shock -Condition in which tissue perfusion is inadequate to deliver oxygen, nutrients to support vital organs, cellular function -Affects all body systems -Classic signs of early shock: Tachycardia,tachypnea,restlessness,anxiety,
Shock chapter Shock -Condition in which tissue perfusion is inadequate to deliver oxygen, nutrients to support vital organs, cellular function -Affects all body systems -Classic signs of early shock: Tachycardia,tachypnea,restlessness,anxiety,
SLCOA National Guidelines
 SLCOA National Guidelines Peri - operative Fluid & Electrolyte Management SLCOA National Guidelines Contents List of Contributors 92 Paediatric fasting guidelines for elective procedures 93 Guidelines
SLCOA National Guidelines Peri - operative Fluid & Electrolyte Management SLCOA National Guidelines Contents List of Contributors 92 Paediatric fasting guidelines for elective procedures 93 Guidelines
Dr. Nai Shun Tsoi Department of Paediatric and Adolescent Medicine Queen Mary Hospital Hong Kong SAR
 Dr. Nai Shun Tsoi Department of Paediatric and Adolescent Medicine Queen Mary Hospital Hong Kong SAR A very important aspect in paediatric intensive care and deserve more attention Basic principle is to
Dr. Nai Shun Tsoi Department of Paediatric and Adolescent Medicine Queen Mary Hospital Hong Kong SAR A very important aspect in paediatric intensive care and deserve more attention Basic principle is to
12/1/2009. Chapter 19: Hemorrhage. Hemorrhage and Shock Occurs when there is a disruption or leak in the vascular system Internal hemorrhage
 Chapter 19: Hemorrhage Hemorrhage and Shock Occurs when there is a disruption or leak in the vascular system External hemorrhage Internal hemorrhage Associated with higher morbidity and mortality than
Chapter 19: Hemorrhage Hemorrhage and Shock Occurs when there is a disruption or leak in the vascular system External hemorrhage Internal hemorrhage Associated with higher morbidity and mortality than
Fluids and electrolytes: the basics
 Fluids and electrolytes: the basics This document is based on the handout from the Surgery for Finals course. The notes provided here summarise key aspects, focusing on areas that are popular in clinical
Fluids and electrolytes: the basics This document is based on the handout from the Surgery for Finals course. The notes provided here summarise key aspects, focusing on areas that are popular in clinical
Body fluid compartments Fluid Pharmacology Phases of fluid therapy. Fluid therapy during anesthesia Subcutaneous fluids
 Edward Cooper, VMD, MS, DACVECC Professor, Emergency and Critical Care The Ohio State University Body fluid compartments Fluid Pharmacology Phases of fluid therapy Resuscitation Replacement Maintenance
Edward Cooper, VMD, MS, DACVECC Professor, Emergency and Critical Care The Ohio State University Body fluid compartments Fluid Pharmacology Phases of fluid therapy Resuscitation Replacement Maintenance
Burn Resuscitation Formulas. John P. Sabra, MD Seton Surgical Group Department of Surgery Dell Medical School Austin, TX
 Burn Resuscitation Formulas John P. Sabra, MD Seton Surgical Group Department of Surgery Dell Medical School Austin, TX BURN INJURY % Physiologic Change % TBSA burn Stasis BURN VASCULAR PERMEABILITY
Burn Resuscitation Formulas John P. Sabra, MD Seton Surgical Group Department of Surgery Dell Medical School Austin, TX BURN INJURY % Physiologic Change % TBSA burn Stasis BURN VASCULAR PERMEABILITY
MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE
 MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE CONTENTS Definition Indications Transfusion trigger Massive transfusion protocol Complications DEFINITION Massive transfusion:
MASSIVE TRANSFUSION DR.K.HITESH KUMAR FINAL YEAR PG DEPT. OF TRANSFUSION MEDICINE CONTENTS Definition Indications Transfusion trigger Massive transfusion protocol Complications DEFINITION Massive transfusion:
L : Line and Tube อ นตรายป องก นได จากการให สารน า
 L : Line and Tube อ นตรายป องก นได จากการให สารน า รศ.นพ.กว ศ กด จ ตตว ฒนร ตน ภาคว ชาศ ลยศาสตร คณะแพทยศาสตร มหาว ทยาล ยเช ยงใหม 3 rd Mini Conference: ความปลอดภ ยในผ ป วย ร วมด วย ช วยได ท กคน ว นท 13-14
L : Line and Tube อ นตรายป องก นได จากการให สารน า รศ.นพ.กว ศ กด จ ตตว ฒนร ตน ภาคว ชาศ ลยศาสตร คณะแพทยศาสตร มหาว ทยาล ยเช ยงใหม 3 rd Mini Conference: ความปลอดภ ยในผ ป วย ร วมด วย ช วยได ท กคน ว นท 13-14
Division 1 Introduction to Advanced Prehospital Care
 Division 1 Introduction to Advanced Prehospital Care Topics Fluids & fluid imbalances IV Therapy Hypoperfusion Shock Fluids and Fluid Imbalances 1 Water is the most abundant substance in the human body.
Division 1 Introduction to Advanced Prehospital Care Topics Fluids & fluid imbalances IV Therapy Hypoperfusion Shock Fluids and Fluid Imbalances 1 Water is the most abundant substance in the human body.
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE
 Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Nursing Process Focus: Patients Receiving Dextran 40 (Gentran 40)
") Assess for presence/history of hypovolemia, shock, venous thrombosis. Assess vital signs: Hypovolemic shock secondary to surgery, burns, hemorrhage, other serious condition PT and PTT abnormalities Venous
Assess for presence/history of hypovolemia, shock, venous thrombosis. Assess vital signs: Hypovolemic shock secondary to surgery, burns, hemorrhage, other serious condition PT and PTT abnormalities Venous
Salty Solutions or Salty Problems? Outline. Outline 29/04/2013
 Salty Solutions or Salty Problems? 18 th October 2012 Richard Seigne Anaesthetist 1 - Non fluid 40% T o t a l b o d y f l u i d 60% NaCl NaCl Intra-cellular fluid 2/3 KCl Interstitial fluid 3/4 of ECF
Salty Solutions or Salty Problems? 18 th October 2012 Richard Seigne Anaesthetist 1 - Non fluid 40% T o t a l b o d y f l u i d 60% NaCl NaCl Intra-cellular fluid 2/3 KCl Interstitial fluid 3/4 of ECF
Hypo/Hypernatremia. Stuart L. Goldstein MD. Director, Center for Acute Care Nephrology Cincinnati Children s Hospital
 Hypo/Hypernatremia Stuart L. Goldstein MD Director, Center for Acute Care Nephrology Cincinnati Children s Hospital Objectives Understand Fluid cellular shifts Understand maintenance fluid and calculations
Hypo/Hypernatremia Stuart L. Goldstein MD Director, Center for Acute Care Nephrology Cincinnati Children s Hospital Objectives Understand Fluid cellular shifts Understand maintenance fluid and calculations
Fluids in ICU. JMO teaching 5th July 2016
 Fluids in ICU JMO teaching 5th July 2016 Objectives Physiology of fluid infusion History of fluid resuscitation Physiology of fluid resuscitation Types of resuscitation fluid The ideal resuscitation fluid
Fluids in ICU JMO teaching 5th July 2016 Objectives Physiology of fluid infusion History of fluid resuscitation Physiology of fluid resuscitation Types of resuscitation fluid The ideal resuscitation fluid
Physiology of the body fluids, Homeostasis
 Physiology of the body fluids, Homeostasis Tamas Banyasz The Body as an open system 1. Open system: The body exchanges material and energy with its environment 2. Homeostasis: The process through which
Physiology of the body fluids, Homeostasis Tamas Banyasz The Body as an open system 1. Open system: The body exchanges material and energy with its environment 2. Homeostasis: The process through which
SHOCK. Pathophysiology
 SHOCK Dr. Ahmed Saleem FICMS TUCOM / 3rd Year / 2015 Shock is the most common and therefore the most important cause of death of surgical patients. Death may occur rapidly due to a profound state of shock,
SHOCK Dr. Ahmed Saleem FICMS TUCOM / 3rd Year / 2015 Shock is the most common and therefore the most important cause of death of surgical patients. Death may occur rapidly due to a profound state of shock,
Chapter 3 MAKING THE DECISION TO TRANSFUSE
 Chapter 3 MAKING THE DECISION TO TRANSFUSE PRACTICE POINTS Determine the best treatment for the patient which may include transfusion. Treat the cause of cytopenia (anaemia or thrombocytopenia) or plasma
Chapter 3 MAKING THE DECISION TO TRANSFUSE PRACTICE POINTS Determine the best treatment for the patient which may include transfusion. Treat the cause of cytopenia (anaemia or thrombocytopenia) or plasma
Pare. Blalock. Shires. shock caused by circulating toxins treatment with phlebotomy. shock caused by hypovolemia treatment with plasma replacement
 Pare shock caused by circulating toxins treatment with phlebotomy Blalock shock caused by hypovolemia treatment with plasma replacement Shires deficit in functional extracellular volume treatment with
Pare shock caused by circulating toxins treatment with phlebotomy Blalock shock caused by hypovolemia treatment with plasma replacement Shires deficit in functional extracellular volume treatment with
CHAPTER 27 LECTURE OUTLINE
 CHAPTER 27 LECTURE OUTLINE I. INTRODUCTION A. Body fluid refers to body water and its dissolved substances. B. Regulatory mechanisms insure homeostasis of body fluids since their malfunction may seriously
CHAPTER 27 LECTURE OUTLINE I. INTRODUCTION A. Body fluid refers to body water and its dissolved substances. B. Regulatory mechanisms insure homeostasis of body fluids since their malfunction may seriously
Vasoactive Medications. Matthew J. Korobey Pharm.D., BCCCP Critical Care Clinical Specialist Mercy St. Louis
 Vasoactive Medications Matthew J. Korobey Pharm.D., BCCCP Critical Care Clinical Specialist Mercy St. Louis Objectives List components of physiology involved in blood pressure Review terminology related
Vasoactive Medications Matthew J. Korobey Pharm.D., BCCCP Critical Care Clinical Specialist Mercy St. Louis Objectives List components of physiology involved in blood pressure Review terminology related
Actualités sur le remplissage peropératoire. Philippe Van der Linden MD, PhD
 Actualités sur le remplissage peropératoire Philippe Van der Linden MD, PhD Fees for lectures, advisory board and consultancy: Fresenius Kabi GmbH B Braun Medical SA Perioperative Fluid Volume Administration
Actualités sur le remplissage peropératoire Philippe Van der Linden MD, PhD Fees for lectures, advisory board and consultancy: Fresenius Kabi GmbH B Braun Medical SA Perioperative Fluid Volume Administration
Pediatric Sodium Disorders
 Pediatric Sodium Disorders Guideline developed by Ron Sanders, Jr., MD, MS, in collaboration with the ANGELS team. Last reviewed by Ron Sanders, Jr., MD, MS on May 20, 2016. Definitions, Physiology, Assessment,
Pediatric Sodium Disorders Guideline developed by Ron Sanders, Jr., MD, MS, in collaboration with the ANGELS team. Last reviewed by Ron Sanders, Jr., MD, MS on May 20, 2016. Definitions, Physiology, Assessment,
Unit 11. Objectives. Indications for IV Therapy. Intravenous Access Devices & Common IV Fluids. 3 categories. Maintenance Replacement Restoration
 Unit 11 Fluids, Electrolytes and Acid Base Imbalances Intravenous Access Devices & Common IV Fluids Objectives Review the purpose and types of intravenous (IV) therapy. Recall the nursing care related
Unit 11 Fluids, Electrolytes and Acid Base Imbalances Intravenous Access Devices & Common IV Fluids Objectives Review the purpose and types of intravenous (IV) therapy. Recall the nursing care related
Albumina nel paziente critico. Savona 18 aprile 2007
 Albumina nel paziente critico Savona 18 aprile 2007 What Is Unique About Critical Care RCTs patients eligibility is primarily defined by location of care in the ICU rather than by the presence of a specific
Albumina nel paziente critico Savona 18 aprile 2007 What Is Unique About Critical Care RCTs patients eligibility is primarily defined by location of care in the ICU rather than by the presence of a specific
Electrolytes Solution
 Electrolytes Solution Substances that are not dissociated in solution are called nonelectrolytes, and those with varying degrees of dissociation are called electrolytes. Urea and dextrose are examples
Electrolytes Solution Substances that are not dissociated in solution are called nonelectrolytes, and those with varying degrees of dissociation are called electrolytes. Urea and dextrose are examples
Blood products and plasma substitutes
 Blood products and plasma substitutes Plasma substitutes Dextran 70 and polygeline are macromolecular substances which are metabolized slowly; they may be used to expand and maintain blood volume in shock
Blood products and plasma substitutes Plasma substitutes Dextran 70 and polygeline are macromolecular substances which are metabolized slowly; they may be used to expand and maintain blood volume in shock
I.V. fluids. What nurses. Fluid and Electrolyte Series. 30 l Nursing2011 l May
 Fluid and Electrolyte Series I.V. fluids What nurses 30 l Nursing2011 l May www.nursing2011.com 2.8 ANCC CONTACT HOURS need to know By Ann Crawford, PhD, RN, and Helene Harris, MSN, RN This is the first
Fluid and Electrolyte Series I.V. fluids What nurses 30 l Nursing2011 l May www.nursing2011.com 2.8 ANCC CONTACT HOURS need to know By Ann Crawford, PhD, RN, and Helene Harris, MSN, RN This is the first
How Normal Body Processes Are Altered By Disease and Injury
 1 Chapter 4, GENERAL PRINCIPLES OF PATHOPHYSIOLOGY. Part 1 How Normal Body Processes Are Altered By Disease and Injury 2 How Cells Respond to Change and Injury 3 Pathology & Pathophysiology : the study
1 Chapter 4, GENERAL PRINCIPLES OF PATHOPHYSIOLOGY. Part 1 How Normal Body Processes Are Altered By Disease and Injury 2 How Cells Respond to Change and Injury 3 Pathology & Pathophysiology : the study
Fundamentals of Pharmacology for Veterinary Technicians Chapter 19
 Figure 19-1 Figure 19-2A Figure 19-2B Figure 19-3 Figure 19-4A1 Figure 19-4A2 Figure 19-4B Figure 19-4C Figure 19-4D Figure 19-5 Figure 19-6A Figure 19-6B A Figure 19-7A B Figure 19-7B C Figure 19-7C D
Figure 19-1 Figure 19-2A Figure 19-2B Figure 19-3 Figure 19-4A1 Figure 19-4A2 Figure 19-4B Figure 19-4C Figure 19-4D Figure 19-5 Figure 19-6A Figure 19-6B A Figure 19-7A B Figure 19-7B C Figure 19-7C D
Chapter 26 Fluid, Electrolyte, and Acid- Base Balance
 Chapter 26 Fluid, Electrolyte, and Acid- Base Balance 1 Body Water Content Infants: 73% or more water (low body fat, low bone mass) Adult males: ~60% water Adult females: ~50% water (higher fat content,
Chapter 26 Fluid, Electrolyte, and Acid- Base Balance 1 Body Water Content Infants: 73% or more water (low body fat, low bone mass) Adult males: ~60% water Adult females: ~50% water (higher fat content,
Pediatric Dehydration and Oral Rehydration. May 16/17
 Pediatric Dehydration and Oral Rehydration May 16/17 Volume Depletion (hypovolemia): refers to any condition in which the effective circulating volume is reduced. It can be produced by salt and water loss
Pediatric Dehydration and Oral Rehydration May 16/17 Volume Depletion (hypovolemia): refers to any condition in which the effective circulating volume is reduced. It can be produced by salt and water loss
How Normal Body Processes Are Altered By Disease and Injury
 1 Chapter 4, General Principles of Pathophysiology Part 1 How Normal Body Processes Are Altered By Disease and Injury 2 How Cells Respond to Change and Injury 3 Pathology & Pathophysiology : the study
1 Chapter 4, General Principles of Pathophysiology Part 1 How Normal Body Processes Are Altered By Disease and Injury 2 How Cells Respond to Change and Injury 3 Pathology & Pathophysiology : the study
NORMOSOL -R MULTIPLE ELECTROLYTES INJECTION TYPE 1, USP For Replacing Acute Losses of Extracellular Fluid Flexible Plastic Container
 NORMOSOL -R MULTIPLE ELECTROLYTES INJECTION TYPE 1, USP For Replacing Acute Losses of Extracellular Fluid Flexible Plastic Container R x only DESCRIPTION Normosol-R is a sterile, nonpyrogenic isotonic
NORMOSOL -R MULTIPLE ELECTROLYTES INJECTION TYPE 1, USP For Replacing Acute Losses of Extracellular Fluid Flexible Plastic Container R x only DESCRIPTION Normosol-R is a sterile, nonpyrogenic isotonic
Fluid and Electrolytes: Parenteral
 Article fluid & electrolytes Fluid and Electrolytes: Parenteral Fluid Therapy Kenneth B. Roberts, MD* Objectives After completing this article, readers should be able to: 1. Relate maintenance fluid and
Article fluid & electrolytes Fluid and Electrolytes: Parenteral Fluid Therapy Kenneth B. Roberts, MD* Objectives After completing this article, readers should be able to: 1. Relate maintenance fluid and
OT Exam 3, August 19, 2002 Page 1 of 6. Occupational Therapy Physiology, Summer Examination 3. August 19, 2002
 Page 1 of 6 Occupational Therapy Physiology, Summer 2002 Examination 3 August 19, 2002 There are 20 questions and each question is worth 5 points for a total of 100 points. Dr. Heckman's section is questions
Page 1 of 6 Occupational Therapy Physiology, Summer 2002 Examination 3 August 19, 2002 There are 20 questions and each question is worth 5 points for a total of 100 points. Dr. Heckman's section is questions
I have no financial disclosures
 Athina Sikavitsas DO Children's Emergency Services University of Michigan Discuss DKA Presentation Assessment Treatment I have no financial disclosures 1 6 Y/O male presents with vomiting and abdominal
Athina Sikavitsas DO Children's Emergency Services University of Michigan Discuss DKA Presentation Assessment Treatment I have no financial disclosures 1 6 Y/O male presents with vomiting and abdominal
Goal-Directed Fluid Therapy: A New Way of Thinking. Ji Su Jenny Kim & Logan D. MacLean SRNA, BSN, CCRN DNP Candidates
 Goal-Directed Fluid Therapy: A New Way of Thinking Ji Su Jenny Kim & Logan D. MacLean SRNA, BSN, CCRN DNP Candidates Goal-Directed Fluid Therapy Map History of Fluid Management Significance of Fluid Management
Goal-Directed Fluid Therapy: A New Way of Thinking Ji Su Jenny Kim & Logan D. MacLean SRNA, BSN, CCRN DNP Candidates Goal-Directed Fluid Therapy Map History of Fluid Management Significance of Fluid Management
CSL Behring LLC Albuminar -25 US Package Insert Albumin (Human) USP, 25% Revised: 01/2008 Page 1
 USP, 25% Revised: 01/2008 Page 1") Page 1 CSL Behring Albuminar -25 Albumin (Human) USP, 25% R x only DESCRIPTION Albuminar -25, Albumin (Human) 25%, is a sterile aqueous solution of albumin obtained from large pools of adult human venous
Page 1 CSL Behring Albuminar -25 Albumin (Human) USP, 25% R x only DESCRIPTION Albuminar -25, Albumin (Human) 25%, is a sterile aqueous solution of albumin obtained from large pools of adult human venous
Normosol -R and 5% Dextrose Injection MULTIPLE ELECTROLYTES AND 5% DEXTROSE INJECTION TYPE 1, USP For Replacing Acute Losses of Extracellular Fluid
 Normosol -R and 5% Dextrose Injection MULTIPLE ELECTROLYTES AND 5% DEXTROSE INJECTION TYPE 1, USP For Replacing Acute Losses of Extracellular Fluid R x only Flexible Plastic Container DESCRIPTION Normosol-R
Normosol -R and 5% Dextrose Injection MULTIPLE ELECTROLYTES AND 5% DEXTROSE INJECTION TYPE 1, USP For Replacing Acute Losses of Extracellular Fluid R x only Flexible Plastic Container DESCRIPTION Normosol-R
Dr. Carlos Fernando Estrada Garzona. Departamento de Farmacología Universidad de Costa Rica
 Dr. Carlos Fernando Estrada Garzona Departamento de Farmacología Universidad de Costa Rica OBJETIVOS FISIOLOGIA LIQUIDOS CORPORALES SOLUCIONES PARENTERALES PRINCIPIOS DE FLUIDOTERAPIA CRISTALOIDE VS COLOIDE
Dr. Carlos Fernando Estrada Garzona Departamento de Farmacología Universidad de Costa Rica OBJETIVOS FISIOLOGIA LIQUIDOS CORPORALES SOLUCIONES PARENTERALES PRINCIPIOS DE FLUIDOTERAPIA CRISTALOIDE VS COLOIDE
Fluid assessment, monitoring and therapy for the acute nurse
 Fluid assessment, monitoring and therapy for the acute nurse Kelly Wright Lead Nurse for AKI King s College Hospital Aims and objectives Aims and objectives Why do we worry about volume assessment? Completing
Fluid assessment, monitoring and therapy for the acute nurse Kelly Wright Lead Nurse for AKI King s College Hospital Aims and objectives Aims and objectives Why do we worry about volume assessment? Completing
Fine-tuning Management in Dengue Fever
 Fine-tuning Management in Dengue Fever Annual Scientific Meeting On Intensive Care 16 August 2014 Eg Kah Peng University of Malaya Medical Centre Rise In Dengue Infection New Straits Times 8 July 2014
Fine-tuning Management in Dengue Fever Annual Scientific Meeting On Intensive Care 16 August 2014 Eg Kah Peng University of Malaya Medical Centre Rise In Dengue Infection New Straits Times 8 July 2014
SUMMARY OF PRODUCT CHARACTERISTICS 1 NAME OF THE MEDICINAL PRODUCT 2 QUALITATIVE AND QUANTITATIVE COMPOSITION
 SUMMARY OF PRODUCT CHARACTERISTICS 1 NAME OF THE MEDICINAL PRODUCT Albunorm 20%, 200 g/l, solution for infusion 2 QUALITATIVE AND QUANTITATIVE COMPOSITION Albunorm 20% is a solution containing 200 g/l
SUMMARY OF PRODUCT CHARACTERISTICS 1 NAME OF THE MEDICINAL PRODUCT Albunorm 20%, 200 g/l, solution for infusion 2 QUALITATIVE AND QUANTITATIVE COMPOSITION Albunorm 20% is a solution containing 200 g/l
بسم اهلل الرحمن الرحيم
 بسم اهلل الرحمن الرحيم o Always we try to maintain a Homeostasis mechanism. Homeostasis : maintenance of internal environment. How?! The environment,that cells live in it,must be in a constant natural
بسم اهلل الرحمن الرحيم o Always we try to maintain a Homeostasis mechanism. Homeostasis : maintenance of internal environment. How?! The environment,that cells live in it,must be in a constant natural
Body Water Content Infants have low body fat, low bone mass, and are 73% or more water Total water content declines throughout life Healthy males are
 Fluid, Electrolyte, and Acid-Base Balance Body Water Content Infants have low body fat, low bone mass, and are 73% or more water Total water content declines throughout life Healthy males are about 60%
Fluid, Electrolyte, and Acid-Base Balance Body Water Content Infants have low body fat, low bone mass, and are 73% or more water Total water content declines throughout life Healthy males are about 60%
Wales Critical Care & Trauma Network (North) Management of Hyponatraemia in Intensive Care Guidelines
 Management of Hyponatraemia in Intensive Care Guidelines") Wales Critical Care & Trauma Network (North) Management of Hyponatraemia in Intensive Care Guidelines Author: Richard Pugh June 2015 Guideline for management of hyponatraemia in intensive care Background
Wales Critical Care & Trauma Network (North) Management of Hyponatraemia in Intensive Care Guidelines Author: Richard Pugh June 2015 Guideline for management of hyponatraemia in intensive care Background
No Disclosures. Objectives. Objectives 10/10/2018
 Algorithmic Quantification of Prime and Perfusate Composition to Regulate Physiological Variables during Cardiopulmonary Bypass in Neonates and Infants Isaac Chinnappan, MS CCP LCP FPP CPBMT Monroe Carell
Algorithmic Quantification of Prime and Perfusate Composition to Regulate Physiological Variables during Cardiopulmonary Bypass in Neonates and Infants Isaac Chinnappan, MS CCP LCP FPP CPBMT Monroe Carell
Calcium (Ca 2+ ) mg/dl
 mg/dl") Quick Guide to Laboratory Values Use this handy cheat-sheet to help you monitor laboratory values related to fluid and electrolyte status. Remember, normal values may vary according to techniques used
Quick Guide to Laboratory Values Use this handy cheat-sheet to help you monitor laboratory values related to fluid and electrolyte status. Remember, normal values may vary according to techniques used
Disorders of water and sodium homeostasis. Prof A. Pomeranz 2017
 Disorders of water and sodium homeostasis Prof A. Pomeranz 2017 Pediatric (Nephrology) Tool Box Disorders of water and sodium homeostasis Pediatric Nephrology Tool Box Hyponatremiaand and Hypernatremia
Disorders of water and sodium homeostasis Prof A. Pomeranz 2017 Pediatric (Nephrology) Tool Box Disorders of water and sodium homeostasis Pediatric Nephrology Tool Box Hyponatremiaand and Hypernatremia
Fluid and Electrolytes P A R T 2
 Fluid and Electrolytes P A R T 2 Fluid Shifts Extracellular fluid distribution is dynamic Interstitial fluid formation is continuous Venous system Large veins (capacitance vessels) Small veins (capacitance
Fluid and Electrolytes P A R T 2 Fluid Shifts Extracellular fluid distribution is dynamic Interstitial fluid formation is continuous Venous system Large veins (capacitance vessels) Small veins (capacitance
Fluid & Elyte Case Discussion. Hooman N IUMS 2013
 Fluid & Elyte Case Discussion Hooman N IUMS 2013 Objectives Know maintenance water and electrolyte requirements. Assess hydration status. Determine replacement fluids (oral and iv) Know how to approach
Fluid & Elyte Case Discussion Hooman N IUMS 2013 Objectives Know maintenance water and electrolyte requirements. Assess hydration status. Determine replacement fluids (oral and iv) Know how to approach
Neonatal Fluid Therapy Not my mother s physiology!!
 Neonatal Fluid Therapy Not my mother s physiology!! Physiologic Approach to Neonatal Fluid Therapy General principles of fluid balance Fetal physiology of fluid balance Neonatal physiology of fluid balance
Neonatal Fluid Therapy Not my mother s physiology!! Physiologic Approach to Neonatal Fluid Therapy General principles of fluid balance Fetal physiology of fluid balance Neonatal physiology of fluid balance
Kristan Staudenmayer, MD Stanford University, Stanford, CA
 Kristan Staudenmayer, MD Stanford University, Stanford, CA Fluid resuscitation Variety of fluids How to administer What you do DOES matter WWII 1942 North Africa high mortality from hemorrhaghic shock
Kristan Staudenmayer, MD Stanford University, Stanford, CA Fluid resuscitation Variety of fluids How to administer What you do DOES matter WWII 1942 North Africa high mortality from hemorrhaghic shock
Correction of hypervolaemic hypernatraemia by inducing negative Na + and K + balance in excess of negative water balance: a new quantitative approach
 Nephrol Dial Transplant (2008) 23: 2223 2227 doi: 10.1093/ndt/gfm932 Advance Access publication 18 February 2008 Original Article Correction of hypervolaemic hypernatraemia by inducing negative Na + and
Nephrol Dial Transplant (2008) 23: 2223 2227 doi: 10.1093/ndt/gfm932 Advance Access publication 18 February 2008 Original Article Correction of hypervolaemic hypernatraemia by inducing negative Na + and
(human albumin solution) POM SUMMARY OF PRODUCT CHARACTERISTICS
 POM SUMMARY OF PRODUCT CHARACTERISTICS") albunorm TM 20% (human albumin solution) POM SUMMARY OF PRODUCT CHARACTERISTICS UK IRELAND and Ireland Octapharma Limited The Zenith Building, 26 Spring Gardens Manchester M2 1AB United Kingdom 1. Name
albunorm TM 20% (human albumin solution) POM SUMMARY OF PRODUCT CHARACTERISTICS UK IRELAND and Ireland Octapharma Limited The Zenith Building, 26 Spring Gardens Manchester M2 1AB United Kingdom 1. Name
AS - EXPERT
 AS - EXPERT 204-009-361 AS - EXPERT 204-009-362 AS - EXPERT 204-009-363 AS - EXPERT 204-009-364 AS - EXPERT 204-009-365 AS - EXPERT 204-009-366 AS - EXPERT 204-009-367 AS - EXPERT 204-009-368 AS - EXPERT
AS - EXPERT 204-009-361 AS - EXPERT 204-009-362 AS - EXPERT 204-009-363 AS - EXPERT 204-009-364 AS - EXPERT 204-009-365 AS - EXPERT 204-009-366 AS - EXPERT 204-009-367 AS - EXPERT 204-009-368 AS - EXPERT
Feedback. Objectives:
 Objectives: 1-Review basics of fluid & electrolytes physiology in surgical patient 2-Be familiar with different types of commonly used IV fluids 3-Be able to calculate fluid & electrolytes requirement
Objectives: 1-Review basics of fluid & electrolytes physiology in surgical patient 2-Be familiar with different types of commonly used IV fluids 3-Be able to calculate fluid & electrolytes requirement
INTRODUCTION. Dengue is one of the ten leading. Globally 20 million cases/yr. 24,000 deaths/yr. It is important to know the typical and atypical
 DENGUE IN CHILDREN INTRODUCTION Dengue is one of the ten leading causes of hospitalization and death in children. Globally 20 million cases/yr. 24,000 deaths/yr. It is important to know the typical and
DENGUE IN CHILDREN INTRODUCTION Dengue is one of the ten leading causes of hospitalization and death in children. Globally 20 million cases/yr. 24,000 deaths/yr. It is important to know the typical and
Dengue Fever & Dengue Shock Syndrome. 07-May-18 PLES / SLCP 1
 Dengue Fever & Dengue Shock Syndrome 07-May-18 PLES / SLCP 1 Objectives Early diagnosis Pathophysiology of DHF Proper management How to avoid complications Case 07-May-18 PLES / SLCP 2 Febrile Phase High
Dengue Fever & Dengue Shock Syndrome 07-May-18 PLES / SLCP 1 Objectives Early diagnosis Pathophysiology of DHF Proper management How to avoid complications Case 07-May-18 PLES / SLCP 2 Febrile Phase High
Fluids, Electrolytes, and Nutrition
 Fluids, Electrolytes, and Nutrition Leslie A. Hamilton, Pharm.D., BCPS, BCCCP University of Tennessee Health Science Center College of Pharmacy Knoxville, Tennessee Fluids, Electrolytes, and Nutrition
Fluids, Electrolytes, and Nutrition Leslie A. Hamilton, Pharm.D., BCPS, BCCCP University of Tennessee Health Science Center College of Pharmacy Knoxville, Tennessee Fluids, Electrolytes, and Nutrition
DRUGS FOR VIVA. IAP UG Teaching slides
 DRUGS FOR VIVA 1 Q:1 INJ SODIUM BICARBONATE 1. What all strengths are available? 2. What are the clinical indications for IV sodium bicarbonate? 3. How do you administer this drug? 2 ANS: 1. Available
DRUGS FOR VIVA 1 Q:1 INJ SODIUM BICARBONATE 1. What all strengths are available? 2. What are the clinical indications for IV sodium bicarbonate? 3. How do you administer this drug? 2 ANS: 1. Available
SUMMARY OF PRODUCT CHARACTERISTICS. Flexbumin 200 g/l is a solution containing 200 g/l (20%) of total protein of which at least 95% is human albumin.
 of total protein of which at least 95% is human albumin.") SUMMARY OF PRODUCT CHARACTERISTICS 1. NAME OF THE MEDICINAL PRODUCT Flexbumin 200g/l solution for infusion 2. QUALITATIVE AND QUANTITATIVE COMPOSITION Flexbumin 200 g/l is a solution containing 200 g/l
SUMMARY OF PRODUCT CHARACTERISTICS 1. NAME OF THE MEDICINAL PRODUCT Flexbumin 200g/l solution for infusion 2. QUALITATIVE AND QUANTITATIVE COMPOSITION Flexbumin 200 g/l is a solution containing 200 g/l
Supplemental Information
 FROM THE AMERICAN ACADEMY OF PEDIATRICS Supplemental Information SUPPLEMENTAL FIGURE 2 Forest plot of all included RCTs using a random-effects model and M-H statistics with the outcome of hyponatremia
FROM THE AMERICAN ACADEMY OF PEDIATRICS Supplemental Information SUPPLEMENTAL FIGURE 2 Forest plot of all included RCTs using a random-effects model and M-H statistics with the outcome of hyponatremia
Fluid Management in Dengue Fever and Dengue Haemorrhagic Fever
 Fluid Management in Dengue Fever and Dengue Haemorrhagic Fever Dengue infection Dr. A LakKumar Fernando, Consultant Paediatrician Dengue is a disease which is silently transmitted in the community. For
Fluid Management in Dengue Fever and Dengue Haemorrhagic Fever Dengue infection Dr. A LakKumar Fernando, Consultant Paediatrician Dengue is a disease which is silently transmitted in the community. For
Care of the Critically Unwell Patient. fluids
 Care of the Critically Unwell Patient fluids Are we made of water? YES! Humans are like cucumbers Water content at least half of body weight in healty adults (60%) blood volume 7% bw males 6% bw females
Care of the Critically Unwell Patient fluids Are we made of water? YES! Humans are like cucumbers Water content at least half of body weight in healty adults (60%) blood volume 7% bw males 6% bw females
CCRN Review - Renal. CCRN Review - Renal 10/16/2014. CCRN Review Renal. Sodium Critical Value < 120 meq/l > 160 meq/l
 CCRN Review Renal Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Sodium 136-145 Critical Value < 120 meq/l > 160 meq/l Sodium Etiology
CCRN Review Renal Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Sodium 136-145 Critical Value < 120 meq/l > 160 meq/l Sodium Etiology
Out Line OF Lecture. Dr S Manimala Rao
 CHOICE OF FLUID, IMPACT ON RENAL FUNCTION Dr. MANIMALA RAO HOD CRITICAL CARE MEDICINE YASHODA HOSPITALS FORMERLY DEAN AND HOD ANAESTHESIOLOGY AND CRITICAL CARE NIMS HYDERABAD Out Line OF Lecture Basics
CHOICE OF FLUID, IMPACT ON RENAL FUNCTION Dr. MANIMALA RAO HOD CRITICAL CARE MEDICINE YASHODA HOSPITALS FORMERLY DEAN AND HOD ANAESTHESIOLOGY AND CRITICAL CARE NIMS HYDERABAD Out Line OF Lecture Basics
Fluid Therapy What, when and how much? Michael Ethier DVM, DVSc, DACVECC Toronto Veterinary Emergency Hospital
 Fluid Therapy What, when and how much? Michael Ethier DVM, DVSc, DACVECC Toronto Veterinary Emergency Hospital Intravenous fluids are one of the most common therapies administered to hospitalized patients,
Fluid Therapy What, when and how much? Michael Ethier DVM, DVSc, DACVECC Toronto Veterinary Emergency Hospital Intravenous fluids are one of the most common therapies administered to hospitalized patients,
Fluids and electrolytes
 Body Water Content Fluids and electrolytes Infants have low body fat, low bone mass, and are 73% or more water Total water content declines throughout life Healthy males are about 60% water; healthy females
Body Water Content Fluids and electrolytes Infants have low body fat, low bone mass, and are 73% or more water Total water content declines throughout life Healthy males are about 60% water; healthy females
INTRAVENOUS FLUIDS PRINCIPLES
 INTRAVENOUS FLUIDS PRINCIPLES Postnatal physiological weight loss is approximately 5-10% Postnatal diuresis is delayed in Respiratory Distress Syndrome (RDS) Preterm babies have limited capacity to excrete
INTRAVENOUS FLUIDS PRINCIPLES Postnatal physiological weight loss is approximately 5-10% Postnatal diuresis is delayed in Respiratory Distress Syndrome (RDS) Preterm babies have limited capacity to excrete
HEAT STROKE. Lindsay VaughLindsay Vaughn, DVM, DACVECCDVM, DACVECC
 HEAT STROKE Lindsay VaughLindsay Vaughn, DVM, DACVECCDVM, DACVECC Heat Stroke More Preventable Than Treatable Heat Stroke A form of hyperthermia associated with a systemic inflammatory response leading
HEAT STROKE Lindsay VaughLindsay Vaughn, DVM, DACVECCDVM, DACVECC Heat Stroke More Preventable Than Treatable Heat Stroke A form of hyperthermia associated with a systemic inflammatory response leading
EUROANESTHESIA 2008 Copenhagen, Denmark, 31 May - 3 June RC2
 PERI-OPERATIVE FLUID THERAPY IN PAEDIATRIC PRACTICE EUROANESTHESIA 2008 Copenhagen, Denmark, 31 May - 3 June 2008 10RC2 ISABELLE MURAT, MARIE-CLAUDE DUBOIS Department of Anesthesia, Hôpital Armand Trousseau
PERI-OPERATIVE FLUID THERAPY IN PAEDIATRIC PRACTICE EUROANESTHESIA 2008 Copenhagen, Denmark, 31 May - 3 June 2008 10RC2 ISABELLE MURAT, MARIE-CLAUDE DUBOIS Department of Anesthesia, Hôpital Armand Trousseau
Standard Operating Procedure (SOP) Management of intervention group patients SOP 001
 Management of intervention group patients SOP 001") ` Standard Operating Procedure (SOP) Management of intervention group patients SOP 001 Authors: Mark Edwards & Rupert Pearse Authorisation: Rupert Pearse (Chief Investigator) Scope To provide guidance
` Standard Operating Procedure (SOP) Management of intervention group patients SOP 001 Authors: Mark Edwards & Rupert Pearse Authorisation: Rupert Pearse (Chief Investigator) Scope To provide guidance
Intravenous Fluid Therapy in Critical Illness
 Intravenous Fluid Therapy in Critical Illness GINA HURST, MD DIVISION OF EMERGENCY CRITICAL CARE HENRY FORD HOSPITAL DETROIT, MI Objectives Establish goals of IV fluid therapy Review fluid types and availability
Intravenous Fluid Therapy in Critical Illness GINA HURST, MD DIVISION OF EMERGENCY CRITICAL CARE HENRY FORD HOSPITAL DETROIT, MI Objectives Establish goals of IV fluid therapy Review fluid types and availability
Name: Lab Time: The Cell Physiology Study Guide, Chapter 3 List of medical roots, suffixes and prefixes Term Meaning Example Term Meaning Example
 Name: Lab Time: The Cell Physiology Study Guide, Chapter 3 List of medical roots, suffixes and prefixes Term Meaning Example Term Meaning Example a- without atrophy meta- after, beyond metastasis auto-
Name: Lab Time: The Cell Physiology Study Guide, Chapter 3 List of medical roots, suffixes and prefixes Term Meaning Example Term Meaning Example a- without atrophy meta- after, beyond metastasis auto-
INTRAVENOUS FLUID THERAPY
 INTRAVENOUS FLUID THERAPY PRINCIPLES Postnatal physiological weight loss is approximately 5 10% in first week of life Preterm neonates have more total body water and may lose 10 15% of their weight in
INTRAVENOUS FLUID THERAPY PRINCIPLES Postnatal physiological weight loss is approximately 5 10% in first week of life Preterm neonates have more total body water and may lose 10 15% of their weight in
Evidence- Based Medicine Fluid Therapy
 Evidence- Based Medicine Fluid Therapy Ndidi Musa M.D. Assosciate Professor of Pediatrics Medical College of Wisconsin/ Children s Hospital of Wisconsin Disclosures A. I have no relevant financial relationships
Evidence- Based Medicine Fluid Therapy Ndidi Musa M.D. Assosciate Professor of Pediatrics Medical College of Wisconsin/ Children s Hospital of Wisconsin Disclosures A. I have no relevant financial relationships
Disclaimer. Chapter 3 Disorder of Water, Electrolyte and Acid-base Professor A. S. Alhomida. Disorder of Water and Electrolyte
 Disclaimer King Saud University College of Science Department of Biochemistry The texts, tables, figures and images contained in this course presentation (BCH 376) are not my own, they can be found on:
Disclaimer King Saud University College of Science Department of Biochemistry The texts, tables, figures and images contained in this course presentation (BCH 376) are not my own, they can be found on: