Treatment of diabetic kidney disease: landmark studies and tribulations
|
|
|
- Magnus Maxwell
- 6 years ago
- Views:
Transcription

1 Division of Nephrology, Department of Medicine, The University of Hong Kong Treatment of diabetic kidney disease: landmark studies and tribulations Sydney C.W. TANG APSN/JSN Continuing Medical Education (CME) Course 2016, 16 Jun 2016
 11.5% 10.8% Zhang L, et al. Lancet 2012 Levey AS, et al. JAMA 2007 11.5 13.4% White SL, et al.")
2 Chronic kidney disease is a global public health problem Estimated CKD Burden: 8 16% worldwide (Jha V, et al. Lancet 2013) 11.5% 10.8% Zhang L, et al. Lancet 2012 Levey AS, et al. JAMA % White SL, et al. Am J Kidney Dis


3 Chronic kidney disease (CKD): an increasingly common cause of death: 1990 to 2013 Top 50 Causes of death: a systematic analysis for the Global Burden of Disease Study 19 Chronic kidney disease 36 Chronic kidney disease 3


4 The number of people with type 2 diabetes is increasing in every country


5 The Diabetes Epidemic The million greatest people number with have of diabetes; people with by diabetes 2035 this are will rise between undiagnosed to million and 59 years of age IDF Diabetes Atlas 2014
6 Outline The burden of diabetic kidney disease in Asia Landmark clinical trials on treatment and tribulations Recent clinical trials Investigational Novel Future perspectives


7 Population: 127 million Japan
8 Chronic Kidney Disease Japan Cohort Study CKD-JAC N=2977 No diabetes Diabetes No CGN CGN No nephropathy % % % nephropathy % Imai et al. Clin Exp Nephrol 2010

9 Causes of incipient dialysis JSDT Diabetic nephropathy 43.8% Chronic glomerulonephritis 18.8% Hypertensive nephrosclerosis
10

11 China has a high prevalence of chronic kidney disease (CKD); an increasing prevalence of hypertension, obesity and type 2 diabetes mellitus, and an ageing population will exacerbate the burden of CKD The current leading cause of CKD in China is glomerular disease, followed by diabetic nephropathy, and hypertension; IgA nephropathy is the most common glomerular disease
12 DN Taiwan


13 Treated ESRD mortality Taiwan Society of Nephrology data

14 Other developed Asian Countries ESRD Registry Committee, Korean Society of Nephrology
15 Singapore Renal Registry Annual Registry Report


16 What about in developing Asian Countries? Phillippine Society of Nephrology 21ST REPORT OF THE MALAYSIAN DIALYSIS AND TRANSPLANT REGISTRY 2013
 : Over one-half of Cambodians with DM had a reduced egfr (60 ml/min/1.73 m2)")
17 Cambodia So far, no reliable data on the incidence and prevalence of ESRD & CKD in Cambodia In a recent study carried out in MoPoTsyo (an NGO Health Center in the Takeo province of Cambodia) : Over one-half of Cambodians with DM had a reduced egfr (60 ml/min/1.73 m2)
18 CKD population in Sri Lanka Estimates only >75% due to DM,HT and CGN DM alone 36% Diabetic population in SL 12%= 2.5 million by 2030-? 5 million DBN 30% to 50% will develop CKD (all stages) =0.81 million Estimated prevalence of HT in SL= 2 million

19 The Indian CKD registry confirms the emergence of DN as the pre-eminent cause of CKD in the country as a whole
20 Nepal No formal registry in Nepal in relation to CKD and ESRD. So, very little is known about the pattern of the ESRD. It is presumed that diabetes mellitus is the commonest cause of ESRD, followed by CGN and hypertension. (Sharma et al. Journal of Nepal Medical Association 2001; Adhikary Land Simkhada R. Kathmandu Medical college Journal 2005) A single hospital based retrospective study from the capital city (Kathmandu) from 1990 to 1999 found that three most common causes of ESRD were Glomerulonephritis (36%), Diabetes mellitus (16.8%), and hypertension (13.7%). (Khakhurel S et al. Journal of Nepal Medical Association 2009). Personal communication with Sharma S, Nepal Society of Nephrology
21
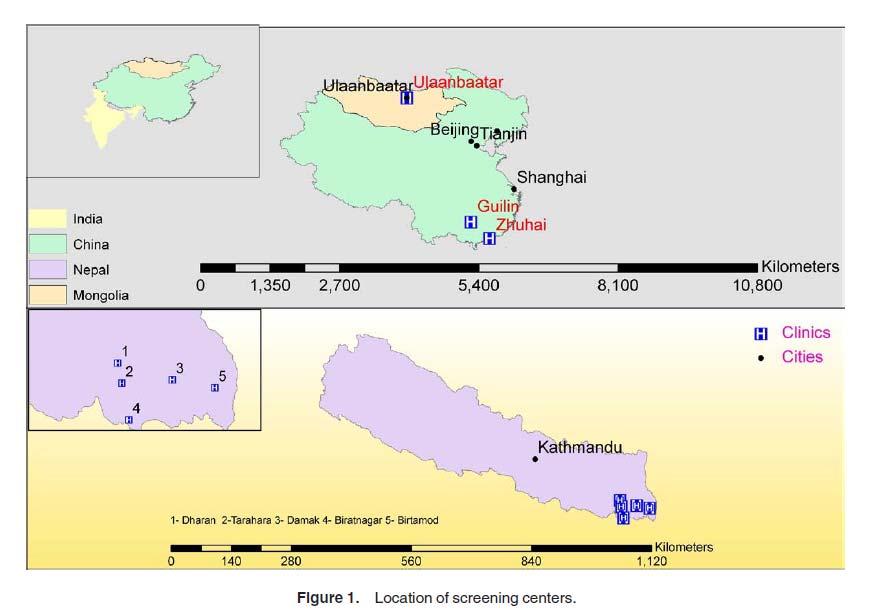
22 AJKD 2010
23 Key messages: Total screened: 11,394 participants Decreased egfr (60 ml/min/1.73 m2): 7.3%-14% Proteinuria on dipstick: 2.4%-10% Hypertension: 26%-36% Diabetes: 3%-8% Obesity (body mass index> 30 kg/m2): 2%-20% Sharma SK, et al. AJKD 2010
24



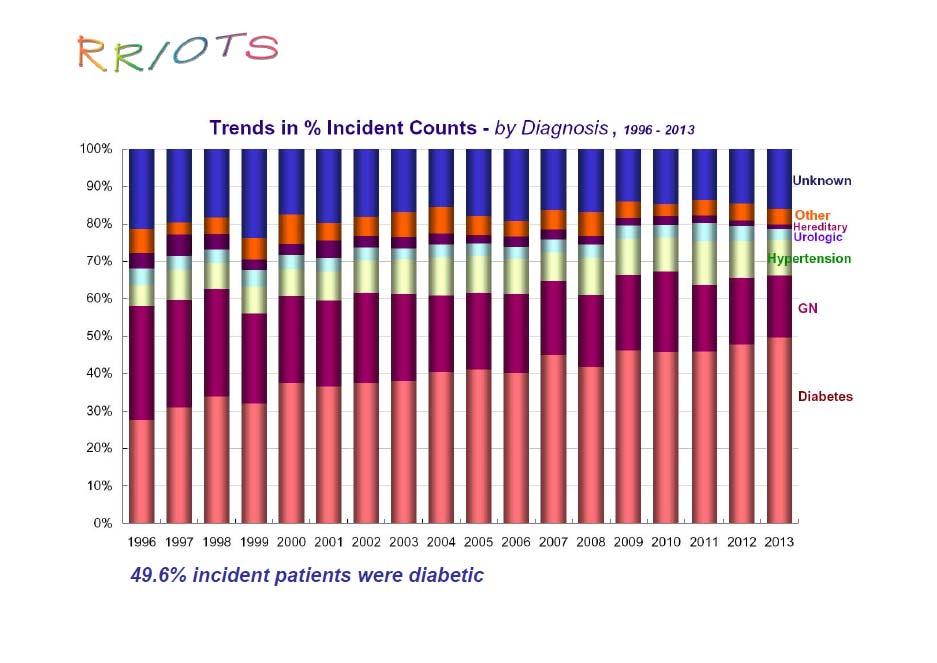
25 USRDS 2014 Report DM: 43.5% 40-50% ~60%


26 DN as the etiology of dialysis therapy
27 Outline The burden of diabetic kidney disease in Asia Landmark clinical trials on treatment and tribulations Recent clinical trials Investigational Novel Future perspectives
28 ARB ACEi ARB/ACEi ARB/DRI MRA
29 ARB: RENAAL & IDNT End stage renal disease (%) Risk reduction, 28% P=0.002 Brenner B, et al. N Engl J Med 2001 Vilayur et al.nat Rev Nephrol (2009) Lewis EJ, N Eng J Med 2001

30 ACE inhibitors in diabetic nephropathy Strippoli GF, BMJ 2004
31 ONTARGET Renal composite Mann JF, et al. Lancet 2008 Mann JF, J Hypertens 2013

32 VA NEPHRON-D
33 VA-NEPHRON-D: Significantly increased SAE Acute Kidney Injury Hyperkalemia HR 1.7 (95% CI ) HR 2.8 (95% CI ) Fried L et al,. N Engl J Med November 2013
34 Dual blockade in patients with DN Catala-Lopez F, Rev Esp Cardiol 2013
35 ALTITUDE: Outcomes Trial terminated in 2011 due to efficacy and safety concerns. Increased nonfatal stroke, hyperkalaemia. Despite lower urinary protein and lower BP Parving, N Eng J Med 2012 (ALTITUDE study)
36 Aldosterone antagonists Aldo antagonist +ACEi/ARB Vs ACEi /ARB alone Aldo antagonist +ACEi/ARB Vs ACEi /ARB alone Aldo antagonist +ACEi/ARB Vs ACEi /ARB alone Spironolactone Eplerenone Total Proteinuria Change in GFR Incidence of hyperkalaemia Navaneethan et al, Clinical JASN 2009
37 What did the guidelines say? KDIGO 2012
38 Finerenone Finerenone (BAY ) is a novel nonsteroidal MRA that has greater receptor selectivity than spironolactone and better receptor affinity than eplerenone in vitro Lower incidence of hyperkalemia than spironolactone. [Pitt B, et al. Eur Heart J 2013] May be able to address the unmet medical need of safely managing albuminuria without adversely affecting serum K in patients with type 2 DN

39 Inclusion: T2DM,UACR 30mg/g, egfr > 30 (30-45: on a non-k sparing diuretic); on an RAS blocker, serum potassium </= 4.8 mmol/l. Primary outcome variable: UACR at day 90 vs at baseline N = ~ 90+ / Rx group (1.25, 2.5, 7.5, 10, 15, 20 mg daily) N = 94 in matching control group

40 Change in Least Squares Mean UACR Weir MR. Nat Rev Nephrol Oct 13, 2015 Bakris G, et al. JAMA 2015

41 Demographic Characteristics of Patients Treated With Placebo or Finerenone, mg/d Bakris G, et al. JAMA 2015

42 Serial egfr and serum K levels 60% had egfr >60 ml/min 2/3 on loop/thiazide Modest BP reduction Bakris G, et al. JAMA 2015
43 The role of glycemic control



44 Glomerulocentric view: Cellular mechanisms of diabetic glomerulosclerosis Adapted from Masaon RM. J Am Soc Nephrol 2003
45 Diabetic substrates Proteins Glucose Glycated proteins Growth factors AGEs Ang II Pathways / molecules NK- B ( ) STAT-1 ( ) The PTEC PKC ( ) TLRs ( ) ERK1/2 ( ) ROS ( ) p38 ( ) Smad ( ) CDK ( ) KKS ( ) Downstream events promulgated Cell cycle arrest, cell hypertrophy and senescence Upregulated inflammatory chemokines/ cytokines Secretion of profibrotic cytokines and ECM proteins EMT (debatable) Tang SC & Lai KN: Nephrol Dial Transplant 2012
46 Standard Intensive Cumulative incidence (%) HR=0.35 (CI ) p=0.017 HbA1c 7.3% HbA1c 6.5% Follow-up (months)
47
48 ADVANCE: New or worsening nephropathy Hazard ratios Annual event rate % BP arm Favours Per-Ind Favours Placebo Relative risk reduction (95% CI) All participants 18% (-1 to 32) 1.2 Standard 18% (-7 to 37) Intensive 17% (-12 to 38) Glucose arm Hazard ratio Favours Intensive Favours Standard Relative risk reduction (95% CI) All participants 19% (2 to 34) Placebo 20% (-4 to 39) Per-Ind 18% (-9 to 39) Hazard ratio Standard Glucose P for interaction= RRR 33%, P= Intensive Per-Ind 0.82 Placebo BP Perkovic, J Am Soc Nephrol. 2009
49 Role of statin in diabetic patients with nephropathy
50 SHARP :CV events 25 Proportion suffering event (%) Risk ratio 0.83 ( ) Logrank 2P= Placebo Eze/simv Years of follow-up Baigent, et al. Lancet 2011
51 SHARP- subgroup analyses Baigent, et al. Lancet 2011

 34 (24):")
52 Statins in CKD- meta analysis Risk of CV events by kidney function Statin better PBO better Hou et al. Eur Heart J (2013) 34 (24):
53
54 Albuminuria reduction in patients with diabetic kidney disease
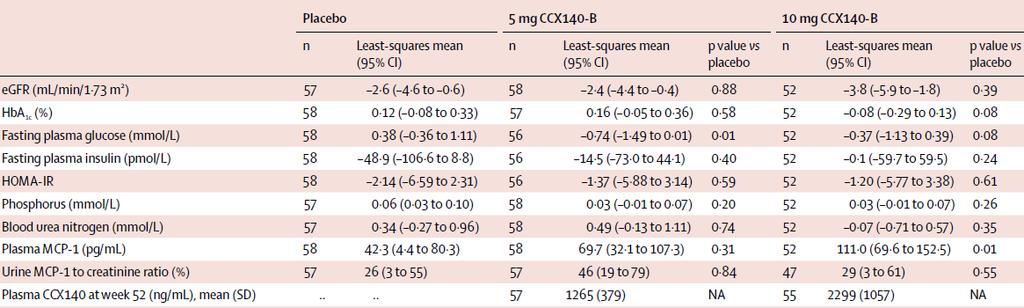
55 Stages of nephropathy in diabetes Annual transition rate in T2DM Annual risk of all-cause death in T2DM Normoalbuminuria 1.4% 2.0% Microalbuminuria 3.0% 2.8% Macroalbuminuria 4.6% 2.3% S-creat. >175 μmol/l or ESKD 19.2% Adapted from: UKPDS 64. Kidney Int 2003; 63:

56 Activation of inflammatory and fibrogenic pathways in proximal tubular epithelial cells by ultrafiltered proteins Glomerular compartment Glomerular filtration barrier Tubulointersitial compartment



57 Activation of inflammatory and fibrogenic pathways in proximal tubular epithelial cells by ultrafiltered proteins Inflammation and T cell recruitment Accumulation of fibroblasts Fibrosis Lai KN, et al. Kidney Int 2007
58 Reduction in albuminuria and protection from renal endpoint - RENAAL De Zeeuw, Kidney Int, 2004

59 Meta-analysis of 1.2 M subjects from 21 studies

60 Medline and EMBASE Mean FU > 1,000 patient-yrs Reported ESRD outcomes with longitud UACR measured 21 trials with 78,342 pts and 4,183 ESRD events for each 30% reduction in albuminuria, the risk of ESRD decreased by 23.7% (95% confidence interval, 11.4% to 34.2%; P=0.001)
61 Outline The burden of diabetic kidney disease in Asia Landmark clinical trials on treatment and tribulations Recent clinical trials Investigational Novel Future perspectives
62

63 The Chemokine and Cytokine storm in the diabetic kidney e.g. CCL2 Tang SC, et al. JASN 2006 Tang SC, et al. Contrib Nephrol 2011 Tang SC, et al. NDT 2013

64
65 Primary Endpoint UACR changes from baseline during 52 weeks were 2% for placebo (95% CI 11% to 9%), 18% for 5 mg CCX140-B ( 26% to 8%), and 11% for 10 mg CCX140-B ( 20% to 1%).
66
67 Primary endpoint: UACR over time % Geometric Mean Change Placebo 0.75 mg atrasentan 1.25 mg atrasentan Days off Time, Weeks p<0.001 for both doses vs. placebo (repeated measures analysis 12 weeks) UACR is reduced by 36% and 44% in the 0.75 mg and 1.25 mg groups compared to a 2% increase in the placebo group De Zeeuw, et al. JASN 2014

68
69 Change in UACR from baseline to the last measurement during treatment Change in UACR and egfr
70
71 Renal glucose handling in humans In normal individuals: Approximately 900mmol (180g) of glucose is filtered by the kidneys daily. 1 In animal models, ~90% reabsorbed in the S1 and S2 segments of the proximal tubule via SGLT2. 2 Remainder reclaimed in the S3 segment 1,3 Minimal glucose is excreted by the kidney In hyperglycaemic individuals: glucose reabsorption by the kidney effectively doubles 1 Am J Physiol Renal Physiol 2001;280:F10 8; 2 Kidney Int Suppl 2007;106:S27 35; 3 J Inherit Metab Dis 2000;23: ;
72 600 Filtered Excreted Tm Reabsorbed T m Rate of glucose filtration / reabsorption /excretion (mg/min) Threshold Plasma glucose (mg/dl) Renal glucose handling in humans
73 Enhanced renal tubular glucose reabsorption contributes to hyperglycaemia in T2DM Hyperglycaemia results in increased glucose filtered at the glomerulus and glucose reabsorption operates at the transport maximum (i.e. if normal glucose is 5 mm/l glucose and Tm is 10 mm/l glucose then twice the amount of glucose is reabsorbed if BSL is 10 mm/l or above) SGLT2 and GLUT transporter numbers are increased, thus Tm is increased
 Hyperfiltration in the early stages of diabetic nephropathy delivers more")
 is the Bowman's capsule (2 and 3). The pink structure is the glomerulus with its capillaries.")
74 Enhanced renal tubular glucose reabsorption contributes to hyperfiltration in diabetes Reduced Na+ delivery to the distal nephron Leading to activation of the macula densa within the JG apparatus to adjust the tone of the afferent glomerular arterioles to increase glomerular filtration (tubuloglomerular feedback mechanism) Hyperfiltration in the early stages of diabetic nephropathy delivers more glucose to the tubule and hence more available to be reabsorbed Renal corpuscle:the structure on the left in blue and pink is the renal corpuscle. The structure on the right is the renal tubule. The blue structure (A) is the Bowman's capsule (2 and 3). The pink structure is the glomerulus with its capillaries. At the left, blood flows from the afferent arteriole (9), through the capillaries (10), and out the efferent arteriole (11). The mesangium is the pink structure inside the glomerulus between the capillaries (5a) and extending outside the glomerulus (5b). Macula densa is #7. Guyton & Hall. Textbook Of Physiology, 11th Edition 2006
 20 0 5 10 15 20 25 30 Years after diabetes onset Williams ME.")
75 Onset of diabetes Pathophysiology of type 2 diabetes: deterioration over 20 years Primary prevention Secondary prevention Tertiary prevention GFR 160 ESRD 6 5 GFR (ml/min) Onset nephropathy Hyperfiltration Glomerulomegaly Renal hypertrophy Urine protein excretion (g/24 h) Years after diabetes onset Williams ME. Am J Nephrol 2005;25:77 94.
76
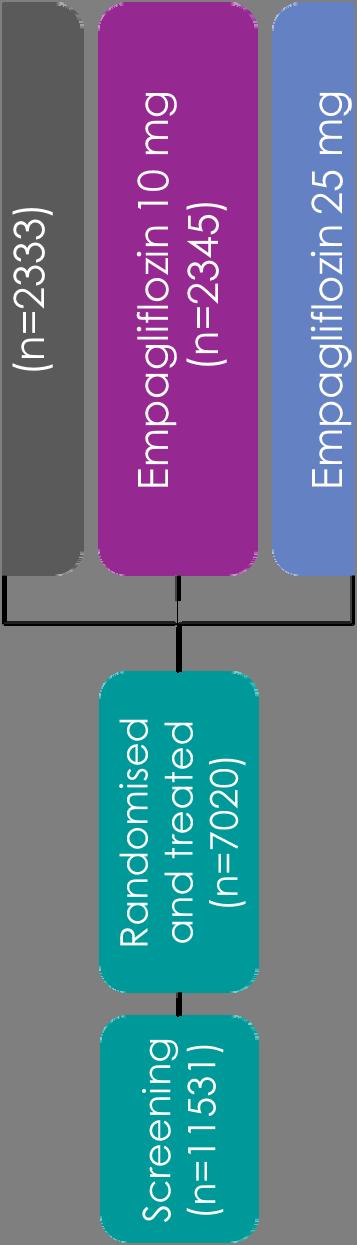
77 Key inclusion and exclusion criteria Key inclusion criteria Adults with type 2 diabetes BMI 45 kg/m 2 HbA1c 7 10%* Established cardiovascular disease Prior myocardial infarction, coronary artery disease, stroke, unstable angina or occlusive peripheral arterial disease Key exclusion criteria egfr <30 ml/min/1.73m 2 (MDRD)
78 Baseline characteristics Placebo (n=2333) Empagliflozin 10 mg (n=2345) Empagliflozin 25 mg (n=2342) HbA1c, % 8.08 (0.84) 8.07 (0.86) 8.06 (0.84) Time since diagnosis of type 2 diabetes, years (18.1) 406 (17.3) 434 (18.6) >5 to (24.5) 585 (24.9) 590 (25.2) > (57.4) 1354 (57.7) 1318 (56.3) LDL cholesterol, mg/dl 84.9 (35.3) 86.3 (36.7) 85.5 (35.2) egfr, ml/min/1.73m 2 (MDRD) 73.8 (21.1) 74.3 (21.8) 74.0 (21.4) 90 ml/min/1.73m (20.9%) 519 (22.1%) 531 (22.7%) 60 to <90 ml/min/1.73m (53.1%) 1221 (52.1%) 1204 (51.4%) <60 ml/min/1.73m (26.0%) 605 (25.8%) 607 (25.9%) Data are n (%) or mean (SD) in patients treated with 1 dose of study drug.


79 HbA1c Placebo Empagliflozin 10 mg Empagliflozin 25 mg


80 Weight Placebo Empagliflozin 10 mg Empagliflozin 25 mg Placebo Empagliflozin 10 mg Empagliflozin 25 mg


81 Systolic blood pressure Placebo Empagliflozin 25 mg Empagliflozin 10 mg Placebo Empagliflozin 10 mg Empagliflozin 25 mg
82 3-point MACE Empagliflozin 10 mg HR 0.85 (95% CI 0.72, 1.01) p= Empagliflozin 25 mg HR 0.86 (95% CI 0.73, 1.02) p= Cumulative incidence function. MACE, Major Adverse Cardiovascular Event; HR, hazard ratio
83 CV death HR 0.62 (95% CI 0.49, 0.77) p< Cumulative incidence function. HR, hazard ratio
84 Hospitalisation for heart failure HR 0.65 (95% CI 0.50, 0.85) p= Cumulative incidence function. HR, hazard ratio
85 All-cause mortality HR 0.68 (95% CI 0.57, 0.82) p< Kaplan-Meier estimate. HR, hazard ratio
86 Adverse events consistent with genital infection Placebo (n=2333) Empagliflozin 10 mg (n=2345) Empagliflozin 25 mg (n=2342) n (%) Rate n (%) Rate n (%) Rate Events consistent with genital infection 42 (1.8%) (6.5%) (6.3%) 2.55 Serious events 3 (0.1%) (0.2%) (0.2%) 0.07 Events leading to discontinuation 2 (0.1%) (0.8%) (0.6%) 0.23 By sex Male 25 (1.5%) (5.4%) (4.6%) 1.78 Female 17 (2.6%) (9.2%) (10.8%) 4.81 Rate = per100 patient-years
87
88 egfr over time Empa (10 or 25 mg daily) dropped egfr by around 4 ml/min (from 74 to 70 71) over the initial 4 weeks, which became stable over the 4-year treatment period The placebo group pursued a steady decline in egfr from 74 to 67 ml/min at the end of the trial 89
89 Worsening nephopathy 90
90 Doubling of scr, initiation of RRT or death from renal disease
91 New onset or worsening of nephropathy N with event Empa N with event Placebo HR 525/ / < P New onset 459/ / < albuminuria 2x scr 70/ / RRT 13/ /
92 FDA Drug Safety Communication: FDA strengthens kidney warnings for diabetes medicines canagliflozin and dapagliflozin 14 Jun 2016 From March 2013, when canagliflozin was approved, to October 2015, FDA received reports of 101 confirmable cases of AKI, some requiring hospitalization/dialysis, with canagliflozin or dapagliflozin use. In half of the cases, AKI occurred within 1 month of starting the drug, and most patients improved after stopping it. Some cases occurred in patients who were younger than 65 years. Some patients were dehydrated, had low BP, or were taking other medicines that can affect the kidneys.
93 Recommendations from FDA Consider factors that may predispose patients to AKI prior to starting SGLT2i, e.g. decreased blood volume; CKD; CHF; and taking other medications such as diuretics, ACE, ARBs, and NSAIDs. Assess kidney function prior to starting SGLT2i and monitor periodically thereafter. If AKI occurs, promptly discontinue the drug and treat the kidney impairment.
94 Evidence based treatments in people with diabetic nephropathy 1. Risk factor modification / Patient education 2. RAS blockade ARB or ACEI DRI: no evidence MRA: possibly the newer compounds 3. BP lowering 4. Glycaemic control 5. Lipid lowering 6. Novel approaches for albuminuria reduction ET antagonist: short term: albuminuria; 4-year trial ongoing CCR2 inhibition: initial data encouraging VDR activator: cost 7. SGLT2 inhibition: CV events;? renoprotective


95 Into the future DPP4i SGLT2i ETARi?TCM Fernandez-Fernandez B, et al. Nat Rev Nephrol 2014
Managing patients with renal disease
 Managing patients with renal disease Hiddo Lambers Heerspink, MD University Medical Centre Groningen, The Netherlands Asian Cardio Diabetes Forum April 23 24, 216 Kuala Lumpur, Malaysia Prevalent cases,
Managing patients with renal disease Hiddo Lambers Heerspink, MD University Medical Centre Groningen, The Netherlands Asian Cardio Diabetes Forum April 23 24, 216 Kuala Lumpur, Malaysia Prevalent cases,
SGLT2 inhibition in diabetes: extending from glycaemic control to renal and cardiovascular protection
 SGLT2 inhibition in diabetes: extending from glycaemic control to renal and cardiovascular protection Hiddo Lambers Heerspink Department of Clinical Pharmacy and Pharmacology University Medical Center
SGLT2 inhibition in diabetes: extending from glycaemic control to renal and cardiovascular protection Hiddo Lambers Heerspink Department of Clinical Pharmacy and Pharmacology University Medical Center
SLOWING PROGRESSION OF KIDNEY DISEASE. Mark Rosenberg MD University of Minnesota
 SLOWING PROGRESSION OF KIDNEY DISEASE Mark Rosenberg MD University of Minnesota OUTLINE 1. Epidemiology of progression 2. Therapy to slow progression a. Blood Pressure control b. Renin-angiotensin-aldosterone
SLOWING PROGRESSION OF KIDNEY DISEASE Mark Rosenberg MD University of Minnesota OUTLINE 1. Epidemiology of progression 2. Therapy to slow progression a. Blood Pressure control b. Renin-angiotensin-aldosterone
The EMPA-REG OUTCOME trial: Design and results. David Fitchett, MD University of Toronto, Canada
 The EMPA-REG OUTCOME trial: Design and results David Fitchett, MD University of Toronto, Canada Asian Cardio Diabetes Forum April 23 24, 2016 Kuala Lumpur, Malaysia Life Expectancy Is Reduced by ~12 Years
The EMPA-REG OUTCOME trial: Design and results David Fitchett, MD University of Toronto, Canada Asian Cardio Diabetes Forum April 23 24, 2016 Kuala Lumpur, Malaysia Life Expectancy Is Reduced by ~12 Years
Chronic Kidney Disease Management for Primary Care Physicians. Dr. Allen Liu Consultant Nephrologist KTPH 21 November 2015
 Chronic Kidney Disease Management for Primary Care Physicians Dr. Allen Liu Consultant Nephrologist KTPH 21 November 2015 Singapore Renal Registry 2012 Incidence of Patients on Dialysis by Mode of Dialysis
Chronic Kidney Disease Management for Primary Care Physicians Dr. Allen Liu Consultant Nephrologist KTPH 21 November 2015 Singapore Renal Registry 2012 Incidence of Patients on Dialysis by Mode of Dialysis
Morbidity & Mortality from Chronic Kidney Disease
 Morbidity & Mortality from Chronic Kidney Disease Dr. Lam Man-Fai ( 林萬斐醫生 ) Honorary Clinical Assistant Professor MBBS, MRCP, FHKCP, FHKAM, PDipID (HK), FRCP (Edin, Glasg) Hong Kong Renal Registry Report
Morbidity & Mortality from Chronic Kidney Disease Dr. Lam Man-Fai ( 林萬斐醫生 ) Honorary Clinical Assistant Professor MBBS, MRCP, FHKCP, FHKAM, PDipID (HK), FRCP (Edin, Glasg) Hong Kong Renal Registry Report
Prevention And Treatment of Diabetic Nephropathy. MOH Clinical Practice Guidelines 3/2006 Dr Stephen Chew Tec Huan
 Prevention And Treatment of Diabetic Nephropathy MOH Clinical Practice Guidelines 3/2006 Dr Stephen Chew Tec Huan Prevention Tight glucose control reduces the development of diabetic nephropathy Progression
Prevention And Treatment of Diabetic Nephropathy MOH Clinical Practice Guidelines 3/2006 Dr Stephen Chew Tec Huan Prevention Tight glucose control reduces the development of diabetic nephropathy Progression
1. Albuminuria an early sign of glomerular damage and renal disease. albuminuria
 1. Albuminuria an early sign of glomerular damage and renal disease albuminuria Cardio-renal continuum REGRESS Target organ damage Asymptomatic CKD New risk factors Atherosclerosis Target organ damage
1. Albuminuria an early sign of glomerular damage and renal disease albuminuria Cardio-renal continuum REGRESS Target organ damage Asymptomatic CKD New risk factors Atherosclerosis Target organ damage
Management of New-Onset Proteinuria in the Ambulatory Care Setting. Akinlolu Ojo, MD, PhD, MBA
 Management of New-Onset Proteinuria in the Ambulatory Care Setting Akinlolu Ojo, MD, PhD, MBA Urine dipstick results Negative Trace between 15 and 30 mg/dl 1+ between 30 and 100 mg/dl 2+ between 100 and
Management of New-Onset Proteinuria in the Ambulatory Care Setting Akinlolu Ojo, MD, PhD, MBA Urine dipstick results Negative Trace between 15 and 30 mg/dl 1+ between 30 and 100 mg/dl 2+ between 100 and
The hypertensive kidney and its Management
 The hypertensive kidney and its Management Dr H0 Chung Ping Hypertension Management Seminar 20061124 Hypertensive kidney Kidney damage asymptomatic till late stage Viscous cycle to augment renal damage
The hypertensive kidney and its Management Dr H0 Chung Ping Hypertension Management Seminar 20061124 Hypertensive kidney Kidney damage asymptomatic till late stage Viscous cycle to augment renal damage
Diabetic Nephropathy. Objectives:
 There are, in truth, no specialties in medicine, since to know fully many of the most important diseases a man must be familiar with their manifestations in many organs. William Osler 1894. Objectives:
There are, in truth, no specialties in medicine, since to know fully many of the most important diseases a man must be familiar with their manifestations in many organs. William Osler 1894. Objectives:
Interventions to reduce progression of CKD what is the evidence? John Feehally
 Interventions to reduce progression of CKD what is the evidence? John Feehally Interventions to reduce progression of CKD what is the evidence? CHALLENGES Understanding what we know. NOT.what we think
Interventions to reduce progression of CKD what is the evidence? John Feehally Interventions to reduce progression of CKD what is the evidence? CHALLENGES Understanding what we know. NOT.what we think
Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin
 Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin Disclosures I have no financial relationship with the manufacturers of any commercial product discussed during this
Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin Disclosures I have no financial relationship with the manufacturers of any commercial product discussed during this
Diabetes and kidney disease.
 Diabetes and kidney disease. What are the implications? Can it be prevented? Nice 18 june 2010 Lars G Weiss. M.D. Ph.D. Department of Neprology Central Hospital Karlstad Sweden Diabetic nephropathy vs
Diabetes and kidney disease. What are the implications? Can it be prevented? Nice 18 june 2010 Lars G Weiss. M.D. Ph.D. Department of Neprology Central Hospital Karlstad Sweden Diabetic nephropathy vs
New Treatment Options for Diabetic Nephropathy patients. Prof. M. Burnier, Service of Nephrology and Hypertension CHUV, Lausanne, Switzerland
 New Treatment Options for Diabetic Nephropathy patients Prof. M. Burnier, Service of Nephrology and Hypertension CHUV, Lausanne, Switzerland Diabetes and nephropathy Diabetic nephropathy is the most common
New Treatment Options for Diabetic Nephropathy patients Prof. M. Burnier, Service of Nephrology and Hypertension CHUV, Lausanne, Switzerland Diabetes and nephropathy Diabetic nephropathy is the most common
SGLT2-inhibition: A New Strategy to Protect the Heart and the Kidney?
 SGLT2-inhibition: A New Strategy to Protect the Heart and the Kidney? Hiddo Lambers Heerspink Department of Clinical Pharmacy and Pharmacology University Medical Center Groningen The Netherlands Disclosures:
SGLT2-inhibition: A New Strategy to Protect the Heart and the Kidney? Hiddo Lambers Heerspink Department of Clinical Pharmacy and Pharmacology University Medical Center Groningen The Netherlands Disclosures:
egfr > 50 (n = 13,916)
") Saxagliptin and Cardiovascular Risk in Patients with Type 2 Diabetes Mellitus and Moderate or Severe Renal Impairment: Observations from the SAVOR-TIMI 53 Trial Supplementary Table 1. Characteristics according
Saxagliptin and Cardiovascular Risk in Patients with Type 2 Diabetes Mellitus and Moderate or Severe Renal Impairment: Observations from the SAVOR-TIMI 53 Trial Supplementary Table 1. Characteristics according
Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin
 Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin Disclosures I have no financial relationship with the manufacturers of any commercial product discussed during this
Diabetic Kidney Disease Tripti Singh MD Department of Nephrology University of Wisconsin Disclosures I have no financial relationship with the manufacturers of any commercial product discussed during this
Diabetic Nephropathy
 Diabetic Nephropathy Larry Lehrner, Ph.D.,M.D. llehrner@ksosn.com Commercial Support Acknowledgement: There is no outside support for this activity Financial Disclosure: stocks > 50,000 Bayer, J&J, Norvartis,Novo
Diabetic Nephropathy Larry Lehrner, Ph.D.,M.D. llehrner@ksosn.com Commercial Support Acknowledgement: There is no outside support for this activity Financial Disclosure: stocks > 50,000 Bayer, J&J, Norvartis,Novo
6/10/2014. Chronic Kidney Disease - General management and standard of care. Management of CKD according to stage (KDOQI 2002)
") Chronic Kidney Disease - General management and standard of care Dr Nathalie Demoulin, Prof Michel Jadoul Cliniques universitaires Saint-Luc Université Catholique de Louvain What should and can be done
Chronic Kidney Disease - General management and standard of care Dr Nathalie Demoulin, Prof Michel Jadoul Cliniques universitaires Saint-Luc Université Catholique de Louvain What should and can be done
Disclosures. Outline. Outline 5/23/17 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Diabetic Nephropathy
 Diabetic Nephropathy Objectives: Know what Diabetic Nephropathy means. Know how common is Diabetic nephropathy in Saudi Arabia and to appreciate how bad are this complications. Know the risk factors of
Diabetic Nephropathy Objectives: Know what Diabetic Nephropathy means. Know how common is Diabetic nephropathy in Saudi Arabia and to appreciate how bad are this complications. Know the risk factors of
Disclosures. Outline. Outline 7/27/2017 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Outline. Outline CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW. Question 1: Which of these patients has CKD?
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Launch Meeting 3 rd April 2014, Lucas House, Birmingham
 Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Launch Meeting 3 rd April 2014, Lucas House, Birmingham Prof Sunil Bhandari
Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Launch Meeting 3 rd April 2014, Lucas House, Birmingham Prof Sunil Bhandari
Diabetic Nephropathy Larry Lehrner, Ph.D.,M.D.
 Diabetic Nephropathy Larry Lehrner, Ph.D.,M.D. llehrner@ksosn.com Commercial Support Acknowledgement: There is no outside support for this activity Financial Disclosure: stocks > 50,000 Bayer, J&J, Norvartis,Novo
Diabetic Nephropathy Larry Lehrner, Ph.D.,M.D. llehrner@ksosn.com Commercial Support Acknowledgement: There is no outside support for this activity Financial Disclosure: stocks > 50,000 Bayer, J&J, Norvartis,Novo
Managing Chronic Kidney Disease: Reducing Risk for CKD Progression
 Managing Chronic Kidney Disease: Reducing Risk for CKD Progression Arasu Gopinath, MD Clinical Nephrologist, Medical Director, Jordan Landing Dialysis Center Objectives: Identify the most important risks
Managing Chronic Kidney Disease: Reducing Risk for CKD Progression Arasu Gopinath, MD Clinical Nephrologist, Medical Director, Jordan Landing Dialysis Center Objectives: Identify the most important risks
Aggressive blood pressure reduction and renin angiotensin system blockade in chronic kidney disease: time for re-evaluation?
 http://www.kidney-international.org & 2013 International Society of Nephrology Aggressive blood pressure reduction and renin angiotensin system blockade in chronic kidney disease: time for re-evaluation?
http://www.kidney-international.org & 2013 International Society of Nephrology Aggressive blood pressure reduction and renin angiotensin system blockade in chronic kidney disease: time for re-evaluation?
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Wanner C, Inzucchi SE, Lachin JM, et al. Empagliflozin and
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Wanner C, Inzucchi SE, Lachin JM, et al. Empagliflozin and
Reducing proteinuria
 Date written: May 2005 Final submission: October 2005 Author: Adrian Gillin Reducing proteinuria GUIDELINES a. The beneficial effect of treatment regimens that include angiotensinconverting enzyme inhibitors
Date written: May 2005 Final submission: October 2005 Author: Adrian Gillin Reducing proteinuria GUIDELINES a. The beneficial effect of treatment regimens that include angiotensinconverting enzyme inhibitors
Invokana (canagliflozin) NEW INDICATION REVIEW
 NEW INDICATION REVIEW") Invokana (canagliflozin) NEW INDICATION REVIEW Introduction Brand name: Invokana Generic name: Canagliflozin Pharmacological class: Sodium-glucose cotransporter 2 (SGLT2) inhibitor Strength and Formulation:
Invokana (canagliflozin) NEW INDICATION REVIEW Introduction Brand name: Invokana Generic name: Canagliflozin Pharmacological class: Sodium-glucose cotransporter 2 (SGLT2) inhibitor Strength and Formulation:
Management of Early Kidney Disease: What to do Before Referring to the Nephrologist
 Management of Early Kidney Disease: What to do Before Referring to the Nephrologist Andrew S. Narva, MD, NIDDK Saturday, February 18, 2017 8:45 a.m. 9:30 a.m. Although evidence-based guidelines for managing
Management of Early Kidney Disease: What to do Before Referring to the Nephrologist Andrew S. Narva, MD, NIDDK Saturday, February 18, 2017 8:45 a.m. 9:30 a.m. Although evidence-based guidelines for managing
Diabetic Kidney Disease in the Primary Care Clinic
 Diabetic Kidney Disease in the Primary Care Clinic Jess Wheeler, DO Nephrology 2015 Outline: 1. CKD/DKD is a growing problem 2. Diagnosis of Chronic Kidney Disease (CKD) 3. Diagnosis of Diabetic Kidney
Diabetic Kidney Disease in the Primary Care Clinic Jess Wheeler, DO Nephrology 2015 Outline: 1. CKD/DKD is a growing problem 2. Diagnosis of Chronic Kidney Disease (CKD) 3. Diagnosis of Diabetic Kidney
Kidney Disease, Hypertension and Cardiovascular Risk
 1 Kidney Disease, Hypertension and Cardiovascular Risk George Bakris, MD, FAHA, FASN Professor of Medicine Director, Hypertensive Diseases Unit The University of Chicago-Pritzker School of Medicine Chicago,
1 Kidney Disease, Hypertension and Cardiovascular Risk George Bakris, MD, FAHA, FASN Professor of Medicine Director, Hypertensive Diseases Unit The University of Chicago-Pritzker School of Medicine Chicago,
Addressing Chronic Kidney Disease in People with Multiple Chronic Conditions
 Addressing Chronic Kidney Disease in People with Multiple Chronic Conditions Andrew S Narva, MD Na/onal Kidney Disease Educa/on Program U.S. Department of Health and Human Services National Institute of
Addressing Chronic Kidney Disease in People with Multiple Chronic Conditions Andrew S Narva, MD Na/onal Kidney Disease Educa/on Program U.S. Department of Health and Human Services National Institute of
Hypertension in Geriatrics. Dr. Allen Liu Consultant Nephrologist 10 September 2016
 Hypertension in Geriatrics Dr. Allen Liu Consultant Nephrologist 10 September 2016 Annual mortality (%) Cardiovascular Mortality Rates are Higher among Dialysis Patients 100 10 1 0.1 0.01 0.001 25-34
Hypertension in Geriatrics Dr. Allen Liu Consultant Nephrologist 10 September 2016 Annual mortality (%) Cardiovascular Mortality Rates are Higher among Dialysis Patients 100 10 1 0.1 0.01 0.001 25-34
Outline. Outline CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW 7/23/2013. Question 1: Which of these patients has CKD?
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH SCIENTIFIC DIRECTOR KIDNEY HEALTH RESEARCH COLLABORATIVE - UCSF CHIEF - GENERAL INTERNAL MEDICINE, SAN FRANCISCO
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH SCIENTIFIC DIRECTOR KIDNEY HEALTH RESEARCH COLLABORATIVE - UCSF CHIEF - GENERAL INTERNAL MEDICINE, SAN FRANCISCO
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
23-Jun-15. Albuminuria Renal and Cardiovascular Consequences A history of progress since ,490,000. Kidney Center, UMC Groningen
 Kidney function (egfr in ml/min) Albuminuria (mg/hr) Incidentie ESRD (%) 3-Jun- Number of patients worldwide that receives kidney replacement therapy Albuminuria Renal and Cardiovascular Consequences A
Kidney function (egfr in ml/min) Albuminuria (mg/hr) Incidentie ESRD (%) 3-Jun- Number of patients worldwide that receives kidney replacement therapy Albuminuria Renal and Cardiovascular Consequences A
Cedars Sinai Diabetes. Michael A. Weber
 Cedars Sinai Diabetes Michael A. Weber Speaker Disclosures I disclose that I am a Consultant for: Ablative Solutions, Boston Scientific, Boehringer Ingelheim, Eli Lilly, Forest, Medtronics, Novartis, ReCor
Cedars Sinai Diabetes Michael A. Weber Speaker Disclosures I disclose that I am a Consultant for: Ablative Solutions, Boston Scientific, Boehringer Ingelheim, Eli Lilly, Forest, Medtronics, Novartis, ReCor
Cardiovascular Protection and the RAS
 Cardiovascular Protection and the RAS Katalin Kauser, MD, PhD, DSc Senior Associate Director, Boehringer Ingelheim Pharmaceutical Inc. Micardis Product Pipeline Scientific Support Ridgefield, CT, USA Cardiovascular
Cardiovascular Protection and the RAS Katalin Kauser, MD, PhD, DSc Senior Associate Director, Boehringer Ingelheim Pharmaceutical Inc. Micardis Product Pipeline Scientific Support Ridgefield, CT, USA Cardiovascular
Updates in Chronic Kidney Disease Management. Delphine S. Tuot, MDCM, MAS Associate Professor of Medicine UCSF-ZSFG
 Updates in Chronic Kidney Disease Management Delphine S. Tuot, MDCM, MAS Associate Professor of Medicine UCSF-ZSFG No disclosures Research Funding: NIH, Blue Shield of California Foundation Objectives
Updates in Chronic Kidney Disease Management Delphine S. Tuot, MDCM, MAS Associate Professor of Medicine UCSF-ZSFG No disclosures Research Funding: NIH, Blue Shield of California Foundation Objectives
Optimal blood pressure targets in chronic kidney disease
 Optimal blood pressure targets in chronic kidney disease Pr. Michel Burnier Service of Nephrology and Hypertension University Hospital Lausanne Switzerland Evidence-Based Guideline for the Management
Optimal blood pressure targets in chronic kidney disease Pr. Michel Burnier Service of Nephrology and Hypertension University Hospital Lausanne Switzerland Evidence-Based Guideline for the Management
 www.usrds.org www.usrds.org 1 1,749 + (2,032) 1,563 to
www.usrds.org www.usrds.org 1 1,749 + (2,032) 1,563 to Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease
 / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease") Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Investigator Meeting 12 th September 2017 - Sheffield Prof Sunil Bhandari Consultant
Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Investigator Meeting 12 th September 2017 - Sheffield Prof Sunil Bhandari Consultant
Chronic kidney disease-what can you do and when to refer?
 Chronic kidney disease-what can you do and when to refer? Dr Goh Heong Keong www.passpaces.com/kidney.htm Outline of Lecture Introduction Epidemiology of CKD in Malaysia/ World Complications of CKD What
Chronic kidney disease-what can you do and when to refer? Dr Goh Heong Keong www.passpaces.com/kidney.htm Outline of Lecture Introduction Epidemiology of CKD in Malaysia/ World Complications of CKD What
Variability in drug response: towards more personalized diabetes care Petrykiv, Sergei
 University of Groningen Variability in drug response: towards more personalized diabetes care Petrykiv, Sergei IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you
University of Groningen Variability in drug response: towards more personalized diabetes care Petrykiv, Sergei IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you
Chronic Kidney Disease for the Primary Care Physician in What do the Kidneys do? CKD in the US
 1:25-2:25pm Managing Chronic Kidney Disease in 2019 SPEAKERS Adriana Dejman, MD Chronic Kidney Disease for the Primary Care Physician in 2019 Adriana Dejman, MD Assistant Professor of Clinical Medicine
1:25-2:25pm Managing Chronic Kidney Disease in 2019 SPEAKERS Adriana Dejman, MD Chronic Kidney Disease for the Primary Care Physician in 2019 Adriana Dejman, MD Assistant Professor of Clinical Medicine
Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease
 / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease") Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Investigator Meetings 1 st and 2 nd September 2016 - London and Leeds Prof Sunil
Angiotensin Converting Enzyme inhibitor (ACEi) / Angiotensin Receptor Blocker (ARB) To STOP OR Not in Advanced Renal Disease Investigator Meetings 1 st and 2 nd September 2016 - London and Leeds Prof Sunil
Uric acid and CKD. Sunil Badve Conjoint Associate Professor, UNSW Staff Specialist, St George
 Uric acid and CKD Sunil Badve Conjoint Associate Professor, UNSW Staff Specialist, St George Hospital @Badves Case Mr J, 52 Male, referred in June 2015 DM type 2 (4 years), HTN, diabetic retinopathy, diabetic
Uric acid and CKD Sunil Badve Conjoint Associate Professor, UNSW Staff Specialist, St George Hospital @Badves Case Mr J, 52 Male, referred in June 2015 DM type 2 (4 years), HTN, diabetic retinopathy, diabetic
Guest Speaker Evaluations Viewer Call-In Thanks to our Sponsors: Phone: Fax: Public Health Live T 2 B 2
 Public Health Live T 2 B 2 Chronic Kidney Disease in Diabetes: Early Identification and Intervention Guest Speaker Joseph Vassalotti, MD, FASN Chief Medical Officer National Kidney Foundation Thanks to
Public Health Live T 2 B 2 Chronic Kidney Disease in Diabetes: Early Identification and Intervention Guest Speaker Joseph Vassalotti, MD, FASN Chief Medical Officer National Kidney Foundation Thanks to
Hypertension and diabetic nephropathy
 Hypertension and diabetic nephropathy Elisabeth R. Mathiesen Professor, Chief Physician, Dr sci Dep. Of Endocrinology Rigshospitalet, University of Copenhagen Denmark Hypertension Brain Eye Heart Kidney
Hypertension and diabetic nephropathy Elisabeth R. Mathiesen Professor, Chief Physician, Dr sci Dep. Of Endocrinology Rigshospitalet, University of Copenhagen Denmark Hypertension Brain Eye Heart Kidney
MANAGEMENT CALL TO DISCUSS LONGER-TERM IMPROVEMENTS IN KIDNEY FUNCTION WITH BARDOXOLONE
 MANAGEMENT CALL TO DISCUSS LONGER-TERM IMPROVEMENTS IN KIDNEY FUNCTION WITH BARDOXOLONE Introduction Substantial body of prior CKD clinical data characterizes Bard s unique profile Bard has demonstrated
MANAGEMENT CALL TO DISCUSS LONGER-TERM IMPROVEMENTS IN KIDNEY FUNCTION WITH BARDOXOLONE Introduction Substantial body of prior CKD clinical data characterizes Bard s unique profile Bard has demonstrated
Avances en nefroprotección en la enfermedad renal diabética Cómo prevenir sus complicaciones y cómo tratarlas
 Avances en nefroprotección en la enfermedad renal diabética Cómo prevenir sus complicaciones y cómo tratarlas Jesus Egido, MD, PhD Catedrático y Director, Departamento de Medicina. Universidad Autónoma
Avances en nefroprotección en la enfermedad renal diabética Cómo prevenir sus complicaciones y cómo tratarlas Jesus Egido, MD, PhD Catedrático y Director, Departamento de Medicina. Universidad Autónoma
QUICK REFERENCE FOR HEALTHCARE PROVIDERS
 KEY MESSAGES 1 SCREENING CRITERIA Screen: Patients with DM and/or hypertension at least yearly. Consider screening patients with: Age >65 years old Family history of stage 5 CKD or hereditary kidney disease
KEY MESSAGES 1 SCREENING CRITERIA Screen: Patients with DM and/or hypertension at least yearly. Consider screening patients with: Age >65 years old Family history of stage 5 CKD or hereditary kidney disease
CARDIO-RENAL SYNDROME
 CARDIO-RENAL SYNDROME Luis M Ruilope Athens, October 216 DISCLOSURES: ADVISOR/SPEAKER for Astra-Zeneca, Bayer, BMS, Daiichi-Sankyo, Esteve, GSK Janssen, Lacer, Medtronic, MSD, Novartis, Pfizer, Relypsa,
CARDIO-RENAL SYNDROME Luis M Ruilope Athens, October 216 DISCLOSURES: ADVISOR/SPEAKER for Astra-Zeneca, Bayer, BMS, Daiichi-Sankyo, Esteve, GSK Janssen, Lacer, Medtronic, MSD, Novartis, Pfizer, Relypsa,
Chronic Kidney Disease
 Chronic Kidney Disease Chronic Kidney Disease (CKD) Educational Objectives Outline Demographics Propose Strategies to slow progression and improve outcomes Plan for treatment of CKD Chronic Kidney Disease
Chronic Kidney Disease Chronic Kidney Disease (CKD) Educational Objectives Outline Demographics Propose Strategies to slow progression and improve outcomes Plan for treatment of CKD Chronic Kidney Disease
Faculty/Presenter Disclosure
 CSI for CKD Unravelling the myths surrounding chronic kidney disease Practical Evidence for Informed Practice Oct 21 2016 Dr. Scott Klarenbach University of Alberta Slide 1: Option B (Presenter with NO
CSI for CKD Unravelling the myths surrounding chronic kidney disease Practical Evidence for Informed Practice Oct 21 2016 Dr. Scott Klarenbach University of Alberta Slide 1: Option B (Presenter with NO
Lessons learned from AASK (African-American Study of Kidney Disease and Hypertension)
") Lessons learned from AASK (African-American Study of Kidney Disease and Hypertension) Janice P. Lea, MD, MSc, FASN Professor of Medicine Chief Medical Director of Emory Dialysis ASH Clinical Specialist
Lessons learned from AASK (African-American Study of Kidney Disease and Hypertension) Janice P. Lea, MD, MSc, FASN Professor of Medicine Chief Medical Director of Emory Dialysis ASH Clinical Specialist
Outline. Outline 10/14/2014 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW. Question 1: Which of these patients has CKD?
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Complications of Diabetes: Screening and Prevention
 Complications of Diabetes: Screening and Prevention Dr Steve Cleland Consultant Physician GGH and QEUH Diabetes Staff Education Course June 17 Diabetic Complications Microvascular: Retinopathy Nephropathy
Complications of Diabetes: Screening and Prevention Dr Steve Cleland Consultant Physician GGH and QEUH Diabetes Staff Education Course June 17 Diabetic Complications Microvascular: Retinopathy Nephropathy
(renoprotective (end-stage renal disease, ESRD) therapies) (JAMA)
 therapies) (JAMA)") [1], 1., 2. 3. (renoprotective (end-stage renal disease, ESRD) therapies) (JAMA) (multiple risk (renal replacement therapy, RRT) factors intervention treatment MRFIT) [2] ( 1) % (ESRD) ( ) ( 1) 2001 (120
[1], 1., 2. 3. (renoprotective (end-stage renal disease, ESRD) therapies) (JAMA) (multiple risk (renal replacement therapy, RRT) factors intervention treatment MRFIT) [2] ( 1) % (ESRD) ( ) ( 1) 2001 (120
Outline. Introduction. Outline CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW 6/26/2012
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
Systolic Blood Pressure Intervention Trial (SPRINT)
") 09:30-09:50 2016.4.15 Systolic Blood Pressure Intervention Trial (SPRINT) IN A NEPHROLOGIST S VIEW Sejoong Kim Seoul National University Bundang Hospital Current guidelines for BP control Lowering BP
09:30-09:50 2016.4.15 Systolic Blood Pressure Intervention Trial (SPRINT) IN A NEPHROLOGIST S VIEW Sejoong Kim Seoul National University Bundang Hospital Current guidelines for BP control Lowering BP
Hypertension targets: sorting out the confusion. Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town
 Hypertension targets: sorting out the confusion Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town Historical Perspective The most famous casualty of this approach was the
Hypertension targets: sorting out the confusion Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town Historical Perspective The most famous casualty of this approach was the
TREAT THE KIDNEY TO SAVE THE HEART. Leanna Tyshler, MD Chronic Kidney Disease Medical Advisor Northwest Kidney Centers February 2 nd, 2009
 TREAT THE KIDNEY TO SAVE THE HEART Leanna Tyshler, MD Chronic Kidney Disease Medical Advisor Northwest Kidney Centers February 2 nd, 2009 1 ESRD Prevalent Rates in 1996 per million population December
TREAT THE KIDNEY TO SAVE THE HEART Leanna Tyshler, MD Chronic Kidney Disease Medical Advisor Northwest Kidney Centers February 2 nd, 2009 1 ESRD Prevalent Rates in 1996 per million population December
Hot Topics in Diabetic Kidney Disease a primary care perspective
 Hot Topics in Diabetic Kidney Disease a primary care perspective DR SARAH DAVIES GP PARTNER WITH SPECIAL INTEREST IN DIABETES, CARDIFF DUK CLINICAL CHAMPION NB MEDICAL HOT TOPICS PRESENTER AND DIABETES
Hot Topics in Diabetic Kidney Disease a primary care perspective DR SARAH DAVIES GP PARTNER WITH SPECIAL INTEREST IN DIABETES, CARDIFF DUK CLINICAL CHAMPION NB MEDICAL HOT TOPICS PRESENTER AND DIABETES
Outline. Outline. Introduction CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW 8/11/2011
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
01/09/2017. Outline. SGLT 2 inhibitor? Diabetes Patients: Complex and Heterogeneous. Association between diabetes and cardiovascular events
 MICROVASCULAR COMPLICATIONS Incidence of outcome g 1 Cardioprotective Effects of SGLT2s Relevant for Which T2 Diabetes Patient? SGLT 2 inhibitor? 58 year old, waist circumference 5 cm, PMH: IHD On statin,
MICROVASCULAR COMPLICATIONS Incidence of outcome g 1 Cardioprotective Effects of SGLT2s Relevant for Which T2 Diabetes Patient? SGLT 2 inhibitor? 58 year old, waist circumference 5 cm, PMH: IHD On statin,
Protecting the heart and kidney: implications from the SHARP trial
 Cardiology Update, Davos, 2013: Satellite Symposium Protecting the heart and kidney: implications from the SHARP trial Colin Baigent Professor of Epidemiology CTSU, University of Oxford S1 First CTT cycle:
Cardiology Update, Davos, 2013: Satellite Symposium Protecting the heart and kidney: implications from the SHARP trial Colin Baigent Professor of Epidemiology CTSU, University of Oxford S1 First CTT cycle:
Top HF Trials to Impact Your Practice
 Top HF Trials to Impact Your Practice Biykem Bozkurt, MD, FACC The Mary and Gordon Cain Chair & Professor of Medicine Medical Care Line Executive, DeBakey VA Medical Center, Director, Winters Center for
Top HF Trials to Impact Your Practice Biykem Bozkurt, MD, FACC The Mary and Gordon Cain Chair & Professor of Medicine Medical Care Line Executive, DeBakey VA Medical Center, Director, Winters Center for
This clinical study synopsis is provided in line with Boehringer Ingelheim s Policy on Transparency and Publication of Clinical Study Data.
 abcd Clinical Study Synopsis for Public Disclosure This clinical study synopsis is provided in line with s Policy on Transparency and Publication of Clinical Study Data. The synopsis which is part of the
abcd Clinical Study Synopsis for Public Disclosure This clinical study synopsis is provided in line with s Policy on Transparency and Publication of Clinical Study Data. The synopsis which is part of the
Predicting and changing the future for people with CKD
 Predicting and changing the future for people with CKD I. David Weiner, M.D. Co-holder, C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University
Predicting and changing the future for people with CKD I. David Weiner, M.D. Co-holder, C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University
ROLE OF ANGIOTENSIN CONVERTING ENZYME INHIBITORS AND ANGIOTENSIN RECEPTOR BLOCKERS IN TYPE I DIABETIC NEPHROPATHY DR.NASIM MUSA
 ROLE OF ANGIOTENSIN CONVERTING ENZYME INHIBITORS AND ANGIOTENSIN RECEPTOR BLOCKERS IN TYPE I DIABETIC NEPHROPATHY DR.NASIM MUSA Type I IDDM is characterized by The abrupt onset of symptoms Insulinopenia
ROLE OF ANGIOTENSIN CONVERTING ENZYME INHIBITORS AND ANGIOTENSIN RECEPTOR BLOCKERS IN TYPE I DIABETIC NEPHROPATHY DR.NASIM MUSA Type I IDDM is characterized by The abrupt onset of symptoms Insulinopenia
SPRINT: Consequences for CKD patients
 SPRINT: Consequences for CKD patients 29 e Workshop Nierziekten Papendal 2018 December 12, 2018 MICHAEL ROCCO, MD, MSCE VARDAMAN M. BUCKALEW JR. PROFESSOR OF MEDICINE PROFESSOR OF PUBLIC HEALTH SCIENCES
SPRINT: Consequences for CKD patients 29 e Workshop Nierziekten Papendal 2018 December 12, 2018 MICHAEL ROCCO, MD, MSCE VARDAMAN M. BUCKALEW JR. PROFESSOR OF MEDICINE PROFESSOR OF PUBLIC HEALTH SCIENCES
Paolo Fornengo SCDU Medicina Interna 3 AOU Città della Salute e della Scienza di Torino
 Paolo Fornengo SCDU Medicina Interna 3 AOU Città della Salute e della Scienza di Torino The KID-ney behind the curtain Altered Renal Glucose Control in Diabetes Gluconeogenesis is increased in postprandial
Paolo Fornengo SCDU Medicina Interna 3 AOU Città della Salute e della Scienza di Torino The KID-ney behind the curtain Altered Renal Glucose Control in Diabetes Gluconeogenesis is increased in postprandial
The CARI Guidelines Caring for Australasians with Renal Impairment. Blood Pressure Control role of specific antihypertensives
 Blood Pressure Control role of specific antihypertensives Date written: May 2005 Final submission: October 2005 Author: Adrian Gillian GUIDELINES a. Regimens that include angiotensin-converting enzyme
Blood Pressure Control role of specific antihypertensives Date written: May 2005 Final submission: October 2005 Author: Adrian Gillian GUIDELINES a. Regimens that include angiotensin-converting enzyme
Diabetes and New Meds for Cardiovascular Risk Reduction. F. Dwight Chrisman, MD, FACC. Disclosures: BI Boehringer Ingelheim speaker
 Diabetes and New Meds for Cardiovascular Risk Reduction F. Dwight Chrisman, MD, FACC Disclosures: BI Boehringer Ingelheim speaker 1 Prevalence of DM DM state specific prevalence 2006 4%-6% 6-8% 8-10% 10-12%
Diabetes and New Meds for Cardiovascular Risk Reduction F. Dwight Chrisman, MD, FACC Disclosures: BI Boehringer Ingelheim speaker 1 Prevalence of DM DM state specific prevalence 2006 4%-6% 6-8% 8-10% 10-12%
Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol
 Inhibitors Drug Class Prior Authorization Protocol") Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has
Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has
hyperlipidemia in CKD DR MOJGAN MORTAZAVI ASSOCIATE PROFESSOR OF NEPHROLOGY ISFAHAN KIDNEY DISEASES RESEARCH CENTER
 Management of hyperlipidemia in CKD DR MOJGAN MORTAZAVI ASSOCIATE PROFESSOR OF NEPHROLOGY ISFAHAN KIDNEY DISEASES RESEARCH CENTER Background on Dyslipidemia in CKD In advanced chronic kidney disease (CKD),
Management of hyperlipidemia in CKD DR MOJGAN MORTAZAVI ASSOCIATE PROFESSOR OF NEPHROLOGY ISFAHAN KIDNEY DISEASES RESEARCH CENTER Background on Dyslipidemia in CKD In advanced chronic kidney disease (CKD),
DISCLOSURES OUTLINE OUTLINE 9/29/2014 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE
 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
The Clinical Unmet need in the patient with Diabetes and ACS
 The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
Diabetes and Hypertension
 Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Metabolic Syndrome and Chronic Kidney Disease
 Metabolic Syndrome and Chronic Kidney Disease Definition of Metabolic Syndrome National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) III Abdominal obesity, defined as a waist circumference
Metabolic Syndrome and Chronic Kidney Disease Definition of Metabolic Syndrome National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) III Abdominal obesity, defined as a waist circumference
Chronic Kidney Disease. Paul Cockwell Queen Elizabeth Hospital Birmingham
 Chronic Kidney Disease Paul Cockwell Queen Elizabeth Hospital Birmingham Paradigms for chronic disease 1. Acute and chronic disease is closely linked 2. Stratify risk and tailor interventions around failure
Chronic Kidney Disease Paul Cockwell Queen Elizabeth Hospital Birmingham Paradigms for chronic disease 1. Acute and chronic disease is closely linked 2. Stratify risk and tailor interventions around failure
ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour
 ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour Dr Indranil Dasgupta Rationale No national practical
ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour Dr Indranil Dasgupta Rationale No national practical
Treating Hypertension in Individuals with Diabetes
 Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
CANVAS Program Independent commentary
 CANVAS Program Independent commentary Cliff Bailey Aston University, Birmingham, UK 2017 Disclosures and disclaimers Clifford J Bailey CJB has attended advisory boards, undertaken ad hoc consultancy, received
CANVAS Program Independent commentary Cliff Bailey Aston University, Birmingham, UK 2017 Disclosures and disclaimers Clifford J Bailey CJB has attended advisory boards, undertaken ad hoc consultancy, received
Stages of Chronic Kidney Disease (CKD)
") Early Treatment is the Key Stages of Chronic Kidney Disease (CKD) Stage Description GFR (ml/min/1.73 m 2 ) >90 1 Kidney damage with normal or GFR 2 Mild decrease in GFR 60-89 3 Moderate decrease in GFR
Early Treatment is the Key Stages of Chronic Kidney Disease (CKD) Stage Description GFR (ml/min/1.73 m 2 ) >90 1 Kidney damage with normal or GFR 2 Mild decrease in GFR 60-89 3 Moderate decrease in GFR
Cardiovascular Risk Reduction in Kidney Transplant Recipients
 Cardiovascular Risk Reduction in Kidney Transplant Recipients Rainer Oberbauer R.O. AUG 2010 CV Mortality in ESRD compared to the general population R.O.2/32 Modified from Foley et al. AJKD 32 (suppl3):
Cardiovascular Risk Reduction in Kidney Transplant Recipients Rainer Oberbauer R.O. AUG 2010 CV Mortality in ESRD compared to the general population R.O.2/32 Modified from Foley et al. AJKD 32 (suppl3):
The Link Between Acute and Chronic Kidney Disease. John Arthur, MD, PhD
 The Link Between Acute and Chronic Kidney Disease John Arthur, MD, PhD Conventional Dogma Conventional dogma was that if a patient survived and recovered from AKI, he was unlikely to have long-term sequela.
The Link Between Acute and Chronic Kidney Disease John Arthur, MD, PhD Conventional Dogma Conventional dogma was that if a patient survived and recovered from AKI, he was unlikely to have long-term sequela.
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014
 HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
Primary Care Approach to Management of CKD
 Primary Care Approach to Management of CKD This PowerPoint was developed through a collaboration between the National Kidney Foundation and ASCP. Copyright 2018 National Kidney Foundation and ASCP Low
Primary Care Approach to Management of CKD This PowerPoint was developed through a collaboration between the National Kidney Foundation and ASCP. Copyright 2018 National Kidney Foundation and ASCP Low
Transforming Diabetes Care
 Transforming Diabetes Care Diabetic Kidney Disease: Prevention, Detection and Treatment Alexis Chettiar, ACNP-BC, PhD(c) 1 Polling Question - 1 What is your role as a healthcare provider? a) Dietitian
Transforming Diabetes Care Diabetic Kidney Disease: Prevention, Detection and Treatment Alexis Chettiar, ACNP-BC, PhD(c) 1 Polling Question - 1 What is your role as a healthcare provider? a) Dietitian
PROTEZIONE DAL DANNO RENALE NEL DIABETE TIPO 2: RUOLO DEI NUOVI FARMACI. Massimo Boemi UOC Malattie Metaboliche e Diabetologia IRCCS INRCA Ancona
 PROTEZIONE DAL DANNO RENALE NEL DIABETE TIPO 2: RUOLO DEI NUOVI FARMACI Massimo Boemi UOC Malattie Metaboliche e Diabetologia IRCCS INRCA Ancona Disclosure Dr Massimo Boemi has been granted as speaker
PROTEZIONE DAL DANNO RENALE NEL DIABETE TIPO 2: RUOLO DEI NUOVI FARMACI Massimo Boemi UOC Malattie Metaboliche e Diabetologia IRCCS INRCA Ancona Disclosure Dr Massimo Boemi has been granted as speaker
Faculty. Disclosures. Learning Objectives. Definitions. Definitions (cont) The Role of the Kidney in Cardiometabolic Disease
 The Role of the Kidney in Cardiometabolic Disease") Faculty The Role of the Kidney in Cardiometabolic Disease Christian W. Mende, MD, FACP, FACN, FASN, FASH Clinical Professor of Medicine University of California at San Diego San Diego, California Disclosures
Faculty The Role of the Kidney in Cardiometabolic Disease Christian W. Mende, MD, FACP, FACN, FASN, FASH Clinical Professor of Medicine University of California at San Diego San Diego, California Disclosures
Drug Class Monograph
 Drug Class Monograph Class: Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drugs: Farxiga (dapagliflozin), Invokamet (canagliflozin/metformin), Invokana (canagliflozin), Jardiance (empagliflozin),
Drug Class Monograph Class: Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drugs: Farxiga (dapagliflozin), Invokamet (canagliflozin/metformin), Invokana (canagliflozin), Jardiance (empagliflozin),
Dapagliflozin and cardiovascular outcomes in type 2
 EARN 3 FREE CPD POINTS diabetes Leader in digital CPD for Southern African healthcare professionals Dapagliflozin and cardiovascular outcomes in type 2 diabetes Introduction People with type 2 diabetes
EARN 3 FREE CPD POINTS diabetes Leader in digital CPD for Southern African healthcare professionals Dapagliflozin and cardiovascular outcomes in type 2 diabetes Introduction People with type 2 diabetes
ADVANCE post trial ObservatioNal Study
 Hot Topics in Diabetes 50 th EASD, Vienna 2014 ADVANCE post trial ObservatioNal Study Sophia Zoungas The George Institute The University of Sydney Rationale and Study Design Sophia Zoungas The George Institute
Hot Topics in Diabetes 50 th EASD, Vienna 2014 ADVANCE post trial ObservatioNal Study Sophia Zoungas The George Institute The University of Sydney Rationale and Study Design Sophia Zoungas The George Institute