Title. CitationSurgical Endoscopy, 26(6): Issue Date Doc URL. Rights. Type. File Information. surgery
|
|
|
- Easter Clark
- 6 years ago
- Views:
Transcription
1 Title Endoscopic ultrasound-guided transmural drainage for surgery Onodera, Manabu; Kawakami, Hiroshi; Kuwatani, Masaki Author(s) Eto, Kazunori; Nasu, Yuya; Tanaka, Eiichi; Hirano, S CitationSurgical Endoscopy, 26(6): Issue Date Doc URL Rights The original publication is available at Type article (author version) File Information SE26-6_ pdf Instructions for use Hokkaido University Collection of Scholarly and Aca
2 Endoscopic ultrasound-guided transmural drainage for pancreatic fistula or pancreatic duct dilatation after pancreatic surgery Manabu Onodera 1), Hiroshi Kawakami 1), Masaki Kuwatani 1), Taiki Kudo 1), Shin Haba 1), Yoko Abe 1), Shuhei Kawahata 1), Kazunori Eto 1), Yuya Nasu 2), Eiichi Tanaka 2), Satoshi Hirano 2), and Masahiro Asaka 1) 1) Department of Gastroenterology, Hokkaido University Graduate School of Medicine 2) Department of Surgical Oncology, Hokkaido University Graduate School of Medicine Author contributions: Onodera M and Kawakami H contributed equally to this work Address correspondence to: Hiroshi Kawakami, MD, PhD. Department of Gastroenterology, Hokkaido University Graduate School of Medicine, Sapporo, , Japan Tel: Fax: (ext.5918) hiropon@med.hokudai.ac.jp Running title: EUS-TD of pancreatic fistula Key words: EUS-guided drainage, EUS-guided transmural drainage, pancreatic fistula, stasis of pancreatic juice, pancreatic surgery
3 Abstract Background Endoscopic ultrasound (EUS)-guided drainage is widely used to manage pancreatic pseudocysts. Several studies have reported the use of EUS-guided drainage for pancreatic fistula and stasis of pancreatic juice caused by stricture of the pancreatic duct after pancreatic resection. Methods In total, 262 patients underwent surgery involving pancreatic resection in our hospital from April 2005 to March Ninety patients (34%) developed a grade B or C postoperative pancreatic fistula (POPF) that required additional treatment. We performed EUS-guided transmural drainage (EUS-TD) for six patients (2.1%) with a pancreatic fistula or dilatation of the main pancreatic duct visible by EUS. Eighteen patients (6.8%) received percutaneous drainage. The success rates of EUS-TD and percutaneous drainage were compared in a retrospective analysis. Results EUS-TD was successfully performed without complications in all six cases, with five of the six patients being successfully treated with only one trial of EUS-TD. The final technical success rate was 100% for EUS-TD and for percutaneous drainage. Both the short-term and long-term clinical success rates of EUS-TD were 100%, and those of percutaneous drainage were 61.1% and 83%, respectively. The differences in these rates were not significant (short-term success, P = 0.091; long-term success, P = 0.403). However, the period to clinical success was significantly shorter with EUS-TD (5.8 days) than with percutaneous drainage (30.4 days; P = ) in our series. Conclusions EUS-TD appears to be a safe and technically feasible alternative to percutaneous drainage and may be considered a first-line therapy for pancreatic fistulas visible by EUS.
4 Abbreviations: CT, computed tomography; EUS, endoscopic ultrasound; EUS-TD, EUS-guided transmural drainage; MPD, main pancreatic duct; POPF, postoperative pancreatic fistula; US, ultrasound; DPDS, Disconnected pancreatic duct syndrome
5 Introduction Postoperative pancreatic fistula (POPF), a serious and potentially lethal complication, is the main unsolved problem in pancreatic surgery. The principle underlying this treatment is drainage of the pancreatic fluid that has collected within the abdominal cavity. The surgeon usually places the drainage tube near the pancreatic stump or the anastomotic site of pancreatoenterostomy to drain the collected fluid in cases of leakage (pancreatic fistula). However, additional drainage may be needed when the drainage work during the operation is inadequate. Despite the expansive growth pattern of pancreatic pseudocysts followed by acute or chronic pancreatitis, the POPF space extends to the peritoneal cavity between visceral organs. This space is usually located deep in the peritoneal cavity and it has an irregular and complex shape. These caused treatment with both surgical and interventional ultrasound (US) or computed tomography (CT)-guided drainage procedures to be problematic. The incidence of postoperative pancreatic fistula (POPF) has been reported to be 5 20% after pancreaticoduodenectomy and is associated with high mortality [1]. The Japanese Society of Hepato-Biliary-Pancreatic Surgery reported that the rate of POPF after pancreaticoduodenectomy was 30.2% [1]. Even with recent advances in pancreatic surgery, POPF remains the major contributor to morbidity after pancreatic resection. The treatment of choice for POPF is external or internal drainage of pancreatic juice, which can be accomplished by surgical drainage, image-guided percutaneous drainage, or endoscopic drainage. A surgical cyst-enteric anastomosis has traditionally been performed, with high morbidity rates ranging from 7 to 37% [2, 3]. Percutaneous drainage offers satisfying results, but it requires a long therapy period (several weeks to months) owing to the indwelling catheter and is occasionally associated with the formation of an external fistula [4, 5]. Furthermore,
6 cutaneopancreatic fistulas that form after percutaneous drainage are usually intractable. Endoscopic drainage has been performed increasingly during the last 10 years [6 8]. Two approaches have been used for endoscopic access: through the gastrointestinal wall by creating a cystogastrostomy/cystoduodenostomy (transmural drainage) or via the papilla (transpapillary drainage). Both approaches, which usually require the insertion of one or more plastic stents [9], have success rates of 70 87% and complication rates of 11 34% [10, 11]. Recently, endoscopic ultrasound (EUS)-guided transmural drainage (EUS-TD) has been widely used to manage pancreatic pseudocysts, and its applications have been extended gradually with the development of more innovative techniques and devices. Several reports have indicated the feasibility of EUS-guided drainage of pancreatic fistulae and stasis of pancreatic juice caused by a pancreatic duct stricture after pancreatic resection [12, 13]. However, no detailed reports are available comparing EUS-TD and percutaneous drainage of a pancreatic fistula after pancreatic resection. To examine the utility and efficacy of EUS-TD, we report six consecutive successful pancreatic fistula and pancreatic duct dilatation cases treated by EUS-TD through the gastrointestinal tract and compare the outcomes with those of cases treated by conventional percutaneous drainage. Patients and methods In total, 262 patients underwent surgery involving pancreatic resection at our hospital from April, 2005 to March, A total of 172 patients (65%) did not have POPF and did not undergo additional treatment. Ninety patients (34%) developed POPF and required additional interventional treatment because they had symptoms such as fever and abdominal pain. Sixty-six patients have been cured by conservative therapies, while 24 have not since a convex
7 array echo endoscope was introduced to our institute in April When POPFs were visible by EUS, EUS-TD was the first choice for their treatment. Percutaneous drainage was the second choice for treatment of refractory POPFs with symptoms or if they were not visible by EUS. As a result, POPFs in five patients (2.1%) and dilatation of the main pancreatic duct (MPD) caused by a stricture of the anastomosis in one, were detected by EUS and treated by EUS-TD, and patients with a POPF not visible by EUS were treated with percutaneous drainage (18 cases, 6.8%) or with a surgical drain followed by primary surgery (66 cases, 25%) for the duration above. In the six patients treated with EUS-TD (Table 1), initial surgical indications were pancreatic carcinoma in three, bile duct carcinoma in two, and ampullary carcinoma in one. Pancreatoduodenectomy had been performed in three cases; hepatopancreatoduodenectomy, in two; and distal pancreatectomy, in one. After surgery, five patients (cases 1 5) developed a POPF, and one (case 6) developed dilatation of the MPD. Three patients (cases 1, 2, and 6) experienced fever, abdominal pain, or general fatigue as signs of a pancreatic fistula infection or stasis of pancreatic juice. Of the 18 POPF patients treated with percutaneous drainage (Table 1), seven with a clinical diagnosis of bile duct carcinoma, three with pancreatic carcinoma, two with intraductal papillary mucinous neoplasm, and one each with ampullary carcinoma, gallbladder cancer, and mucinous cystic neoplasm had initially undergone pancreaticoduodenectomy or distal pancreatectomy. Hepatopancreatoduodenectomy had been performed in three patients diagnosed with bile duct carcinoma (Fig. 1). Data were collected from our endoscopic database and hospital records. Figure 1 shows a flow diagram of the study participants.
8 Endoscopic therapy All EUS-guided procedures were performed with the patient in the lateral or prone position and under conscious sedation with midazolam and fentanyl. A convex array echo endoscope (GF-UCT240; Olympus Medical Systems, Tokyo, Japan), an ultrasound system (ProSound SSD-5000; ALOKA, Tokyo, Japan), and a fluoroscope (CUREVISTA; Hitachi Medical Corp., Tokyo, Japan) were used for all procedures. All POPF or dilatation of MPD were visible by EUS, and all punctures were performed through the stomach wall. With regard to EUS-TD of POPF, first, an internal fistula was created between the POPF and the stomach by introducing a 19-gauge needle (Echo Tip Ultra; Cook Endoscopy, Osaka, Japan). Successful POPF access was demonstrated by injection of contrast medium defining a POPF. Next, a inch guidewire (Jagwire; Boston Scientific, Tokyo, Japan) was passed through the needle, introduced into the cavity of the POPF, and coiled within the POPF under fluoroscopic guidance. The tract was sequentially dilated with an over-the-wire biliary balloon dilator (6 mm, Hurricane RX; Boston Scientific), a Soehendra biliary dilatation catheter (SBDC-6, -7, -8.5; Cook Endoscopy), or a Soehendra stent retriever (7 Fr; Cook Endoscopy). After dilatation, a double-pigtail stent (7 Fr, 40 mm; Olympus Medical Systems) was deployed into the fluid-filled space. Regarding EUS-TD of the dilated MPD, after the pancreatic duct was identified and regional recurrence was confirmed by color Doppler imaging, the MPD was punctured with a 19-gauge needle (Echo Tip Ultra; Cook Endoscopy), and an internal fistula was created between the MPD and the stomach as the initial step. Successful pancreatic duct access was demonstrated by injection of contrast medium defining a pancreatogram. Next, a inch guidewire (Jagwire; Boston Scientific) was passed through the needle and introduced into the cavity of the MPD under fluoroscopic guidance. The tract was sequentially
9 dilated with a Soehendra dilatation catheter (SBDC-6; Cook Endoscopy). After dilatation, a pancreatic stent (5 Fr, 50 mm; Cook Endoscopy) was deployed into the MPD. Representative images of EUS-TD for POPF associated with the treatment of case 1 are shown in Fig. 2. Percutaneous drainage of pancreatic fistulas Percutaneous drainage was performed by an interventional radiologist and a surgeon, who punctured the pancreatic fistula by inserting a inch guidewire into the fistula space and then placed an indwelling drainage catheter (7.2 Fr strait catheter; O-HIRATA TM, Medico s Hirata, Osaka, Japan, or 8.5 Fr pigtail catheter; Ultrathane TM, Cook Endoscopy) under fluoroscopy, US, or CT guidance. Technical and clinical success of EUS-TD and percutaneous drainage Technical success of EUS-TD was defined as the successful placement of a transmural stent or percutaneous catheter into the POPF. Short-term clinical success was defined as a 50% decrease in the POPF or an improvement in the dilated MPD on CT images, and a decrease in serum amylase level in the drainage fluid 1 week after treatment. Long-term clinical success was defined as the resolution of the POPF or improvement of the dilated MPD on CT images 1 month after treatment. Statistical analysis Non-normally distributed variables are expressed as medians (range), and nonparametric tests (Mann-Whitney U test) were employed for statistical comparisons. Nominal variables are expressed as frequencies and percentages. The χ 2 test with Yates continuity correction for the
10 two-way contingency table was used for statistical comparisons. Fisher s exact test was used in the case of a small expected frequency. Data were considered significant at a P value <0.05. Results The mean period between the onset of POPF and endoscopic therapy was 7.1 months (range, 1 24 months). EUS-TD was successfully performed without complications in all six cases (rate of technical success, 100%) (Table 2). The size of the fistula decreased remarkably (average reduction rate, 81.2%; range, %) in the five POPF patients. The MPD diameter in case 6 improved after MPD stenting. In all six cases, the serum amylase level was lower after drainage (before drainage: 413 U/L; 1 week after drainage: 65 U/L), reflecting decreased pancreatic duct pressure. One patient (case 1) developed a growth in the cavity by occlusion of the indwelling stent 2 months after the first drainage; this case underwent a stent exchange using a conventional endoscopic approach. No recurrences (mean follow-up, 7.5 months; range, 1 27 months) were observed in the remaining five cases. Table 3 compares the characteristics of the patient treated by EUS-TD and percutaneous drainage. EUS-TD and percutaneous drainage each had a final technical success rate of 100%. The short- and long-term clinical success rates of EUS-TD were both 100%, and those of percutaneous drainage were 61.1% and 83%, respectively. These rates did not differ significantly between techniques (short-term clinical success rate, P = 0.091; long-term clinical success rate, P = 0.403). However, the time until clinical success was significantly shorter with EUS-TD (5.8 days) than with percutaneous drainage (30.4 days; P = ). Follow-up
11 After discharge, all patients were followed-up by laboratory investigations and CT. Transmural stents were not retrieved, even after fluid collection was completed. Endoscopic treatment was repeated in the event of stent occlusion. No POPF recurrence was observed during the follow-up time (mean follow-up, 17.7 months; range, 1 47 months). Discussion A pancreatic fistula is as an abnormal communication between the pancreatic duct and another non-epithelized cavity containing pancreas-derived, enzyme-rich fluid [3, 12], which occurs mainly after pancreatic resection and trauma. Pancreatic juice may spread throughout the pleura or peritoneum and induce severe inflammation and autodigestion of peripancreatic and retroperitoneal tissues. A pancreatic pseudocyst, which develops after acute pancreatitis or accompanying chronic pancreatitis, is a localized collection of fluid rich in amylase and other pancreatic enzymes and enclosed by a non-epithelized, hard and thick wall [3, 12]. However, differentiating a POPF from a pancreatic pseudocyst is difficult in some situations. A POPF represents failure of healing and/or sealing of a pancreatic-enteric anastomosis and a leak of pancreatic juice into the peritoneal or retroperitoneal cavity. POPF is treatable by endoscopic, surgical, and/or percutaneous drainage. Endoscopic transpapillary drainage of the MPD for a pancreatic fistula communicating with the MPD is a relatively easy, well established, first-step for patients with POPFs [14, 15]. However, the transpapillary approach can occasionally be difficult owing to distortion of the duodenum caused by postoperative changes. When distal pancreatectomy is performed, a transpapillary approach should be considered. However, we did not undertake any endoscopic transpapillary approaches during the period of this retrospective study. Of the six cases, cases 1 3, 5 and 6
12 underwent pancreaticoduodenectomy or hepatopancreatoduodenectomy. Although only case 4 underwent a distal pancretectomy, we performed EUS-TD because POPF were readily visualized by EUS. EUS-TD has been successfully performed for POPFs associated with a complete MPD rupture caused by trauma, pancreatoenteric anastomotic breakdown, and occlusion of a pancreatoenteric anastomosis after pancreatic surgery [13, 16, 17]. The present report demonstrates that drainage of pancreatic fistulas and MPD by EUS-TD through the gastrointestinal tract was effective and safe in all six cases. EUS-TD allows access to relatively small and non-bulging pancreatic fistulas and provides visualization of the blood vessels to reduce the risk of bleeding [18, 19]. EUS-TD also permits internal drainage of pancreatic fluid into the gut, and direct fistula formation between the POPF space and the gut can facilitate POPF closure in one step. In contrast, percutaneous drainage may lead to the formation of a permanent external fistula in 5 10% of cases [4]. Percutaneous drainage also sometimes requires two or more procedures in a multistep conversion from external to internal drainage and necessitates a longer hospital stay compared with EUS-TD. Disconnected pancreatic duct syndrome (DPDS) is an anatomic situation defined by a lack of ductal continuity between viable secreting pancreatic tissue and the gastrointestinal tract. The visible upstream pancreas continues secretion without an intact drainage system. The physiologic abnormality of DPDS results in myriad complications, including pancreatic pseudocysts, pancreatic ascites, pancreatic fistula, and others [20]. In our study, we believed that differences in the mechanism of POPF were caused by the methods of surgical anastomosis used. The patients with pancreatojejunostomy would demonstrate POPFs caused by anastomotic breakdown (case 1 3,5) or complete rupture (case 4), whereas a case with pancratogastrostomy would develop stasis of the pancreatic juice caused by occlusion of the anastomosis (case 6). EUS-TD to the
13 dilatation of the MPD was successful in our study. However, Kahaleh et al. [21] reported that EUS-TD of the MPD dilatation failed in 28.5% of postsurgical patients. Therefore, EUS-guided pancreatic duct drainage remains difficult, especially in the postoperative situation. If recurrence develops after EUS-TD of the dilated MPD, surgery should be considered, despite its higher morbidity and mortality than nonsurgical approaches [22]. Only one patient (case 1) developed a relapse of pancreatic fluid collection due to stent occlusion and underwent a second EUS-TD for a stent exchange. Although several reports have indicated the recurrence of pancreatic fluid accumulation following stent removal after endoscopic transmural drainage, in most patients with a pancreatic fistula who undergo EUS-TD, stent removal is performed routinely within 2 weeks of fistula resolution on imaging [6, 23]. The recurrence rate of a pancreatic fistula that requires further endoscopic, surgical, or percutaneous drainage varies from 10% to 30%, and recurrence often occurs within 1 year after treatment [6, 7, 10]. A previous randomized controlled trial regarding stent removal after successful endoscopic transmural drainage of a pancreatic fistula caused by acute pancreatitis or chronic pancreatitis showed that stent retrieval was associated with a higher recurrence rate [24]. In this study, during a median follow-up period of 14 months, no patients in the persistent stent placement group had POPF recurrence, whereas five of the 13 patients (38.4%) in the stent retrieval group did have POPF recurrence. This result suggests that by maintaining the stent in place, the cystenterostomy tract may remain patent. This patency could be caused by the stent, which acts as a wick and maintains communication between the pancreatic fistula and the stomach. Prolonged transmural stent placement has been adapted as a strategy to prevent recurrence of POPF [24, 25]. Although Varadarajulu et al. pointed out the risk of stent migration, they reported placement of a permanent indwelling stent by EUS-TD [26].
14 Furthermore, the appropriate period for stent placement and optimal stent diameter are controversial and yet to be determined. Nevertheless, we consider that a stent remaining in its proper position reduces the recurrence rate. In our study, the period to clinical success was significantly shorter with EUS-TD than with percutaneous drainage. In two previous studies [27, 28], a higher failure rate was associated with percutaneous drainage of pancreatic pseudocysts (58%) compared with surgical treatment (7%) [27], and surgical and endoscopic interventions for pancreatic pseudocysts were equally safe and effective compared with percutaneous drainage [28]. Thus, EUS-TD can be considered a first-line therapy for a pancreatic fistula detectable by EUS when conservative management is ineffective. When EUS-TD cannot be performed, percutaneous drainage or surgical drainage can be considered to manage POPF. No major complications following EUS-TD were noted in our study. Previous studies have reported complications such as perforation, bleeding, and pancreatitis, although most were not serious [10, 11]. As major hemorrhage, a rare occurrence during EUS-TD, would require surgery, EUS-TD should be performed only in tertiary care centers [17]. The limitations of the present study include its retrospective design, the small number of patients studied, and the evaluation of subjects from a single center. Larger studies are needed to further understand the current situation of POPF drainage. In conclusion, EUS-TD is a technically feasible and apparently safe alternative to percutaneous or surgical drainage for POPF. EUS-TD can be considered as a first-line therapy for POPFs visible by EUS.
15 Acknowledgments The authors declare that there was no grant support and that there are no financial disclosures or conflicts of interest. We are deeply grateful to Professor Satoshi Kondo (formerly of the Department of Surgical Oncology, Hokkaido University Graduate School of Medicine), who provided support during the preparation of this manuscript, but who passed away before its submission.
16 References 1. Le Moine O, Matos C, Closset J, Devière J (2004) Endoscopic management of pancreatic fistula after pancreatic and other abdominal surgery. Best Pract Res Clin Gastroenterol 18: Kawai M, Kondo S, Yamaue H, Wada K, Sano K, Motoi F, et al. (2011) Predictive risk factors for clinically relevant pancreatic fistula analyzed in 1,239 patients with pancreaticoduodenectomy: multicenter data collection as a project study of pancreatic surgery by the Japanese Society of Hepato-Biliary-Pancreatic Surgery. J Hepatobiliary Pancreat Sci 18: Lehman GA (1999) Pseudocysts. Gastrointest Endosc 49:S81 S84 4. Boerma D, van Gulik TM, Obertop H, Gouma DJ (1999) Internal drainage of infected pancreatic pseudocysts: safe or sorry? Dig Surg 16: Neff R (2001) Pancreatic pseudocysts and fluid collections: percutaneous approaches. Surg Clin North Am 81: Sohn TA, Yeo CJ, Cameron JL, Geschwind JF, Mitchell SE, Venbrux AC, et al. (2003) Pancreaticoduodenectomy: role of interventional radiologists in managing patients and complications. J Gastrointest Surg 7: Baron TH, Harewood GC, Morgan DE, Yates MR (2002) Outcome differences after endoscopic drainage of pancreatic necrosis, acute pancreatic pseudocysts, and chronic pancreatic pseudocysts. Gastrointest Endosc 56: Binmoeller KF, Seifert H, Walter A, Soehendra N (1995) Transpapillary and transmural drainage of pancreatic pseudocysts. Gastrointest Endosc 42: Harewood GC, Wright CA, Baron TH (2003) Impact on patient outcomes of experience in
17 the performance of endoscopic pancreatic fluid collection drainage. Gastrointest Endosc 58: Delhaye M, Matos C, Devière J (2003) Endoscopic management of chronic pancreatitis. Gastrointest Endosc Clin N Am 13: Cahen D, Rauws E, Fockens P, Weverling G, Huibregtse K, Bruno M (2005) Endoscopic drainage of pancreatic pseudocysts: long-term outcome and procedural factors associated with safe and successful treatment. Endoscopy 37: Hookey LC, Debroux S, Delhaye M, Arvanitakis M, Le Moine O, Devière J (2006) Endoscopic drainage of pancreatic-fluid collections in 116 patients: a comparison of etiologies, drainage techniques, and outcomes. Gastrointest Endosc 63: Arvanitakis M, Delhaye M, Bali MA, Matos C, Le Moine O, Devière J (2007) Endoscopic treatment of external pancreatic fistulas: when draining the main pancreatic duct is not enough. Am J Gastroenterol 102: Devière J, Bueso H, Baize M, Azar C, Love J, Moreno E, et al. (1995) Complete disruption of the main pancreatic duct-endoscopic management. Gastrointest Endosc 42: Varadarajulu S, Noone TC, Tutuian R, Hawes RH, Cotton PB (2005) Predictors of outcome in pancreatic duct disruption managed by endoscopic transpapillary stent placement. Gastrointest Endosc 61: Katanuma A, Maguchi H, Fukazawa M, Kurita A, Ichiya T, Kin T, et al. (2009) Endoscopic ultrasonography-guided pancreaticogastrostomy for a case of occlusion of gastro-pancreatic anastomosis after pancreaticoduodenectomy. Dig Endosc 21:S87 S Cavallini A, Butturini G, Malleo G, Bertuzzo F, Angelini G, Abu Hilal M, et al. (2011) Endoscopic transmural drainage of pseudocysts associated with pancreatic resections or
18 pancreatitis a comparative study. Surg Endosc 25: Giovannini M, Binmoeller K, Seifert H (2003) Endoscopic ultrasound-guided cystogastrostomy. Endoscopy 35: Krüger M, Schneider AS, Manns MP, Meier PN (2006) Endoscopic management of pancreatic pseudocysts or abscesses after an EUS-guided 1-step procedure for initial access. Gastrointest Endosc 63: Lawrence C, Howell DA, Stefan AM, Conklin DE, Lukens FJ, Martin RF, Landes A, Benz B (2008) Disconnected pancreatic tail syndrome: potential for endoscopic therapy and results of long-term follow-up. Gastrointest Endosc 67: Kahaleh M, Hernandez AJ, Tokar J, Adams RB, Shami VM, Yeaton P (2007) EUS guided pancreaticogastrostomy: analysis of its efficacy to drain inaccessible pancreatic ducts. Gastrointest Endosc 65: Szentes MJ, Traverso LW, Kozarek RA, Freeny PC (1991) Invasive treatment of pancreatic fluid collection with surgical and non surgical methods. Am J Surg 161: Cahen D, Rauws E, Fockens P, Weverling G, Huibregtse K, Bruno M (2005) Endoscopic drainage of pancreatic pseudocysts: long-term outcome and procedural factors associated with safe and successful treatment. Endoscopy 37: Arvanitakis M, Delhaye M, Bali MA, Matos C, De Maertelaer V, Le Moine O, Devière J (2007) Pancreatic-fluid collections: a randomized controlled trial regarding stent removal after endoscopic transmural drainage. Gastrointest Endosc 65: Devière J, Bueso H, Baize M, Azar C, Love J, Moreno E, Cremer M. (1995) Complete disruption of the main pancreatic duct: endoscopic management. Gastrointest Endosc 42:
19 26. Varadarajulu S, Wilcox CM. (2011) Endoscopic placement of permanent indwelling transmural stents in disconnected pancreatic duct syndrome: does benefit outweigh the risks? Gastrointest Endosc. (in press) 27. Heider R, Meyer AA, Galanko JA, Behrns KE (1999) Percutaneous drainage of pancreatic pseudocysts is associated with a higher failure rate than surgical treatment in unselected patients. Ann Surg 229: Johnson MD, Walsh RM, Henderson JM, Brown N, Ponsky J, Dumot J, et al. (2009) Surgical versus nonsurgical management of pancreatic pseudocysts. J Clin Gastroenterol 43:
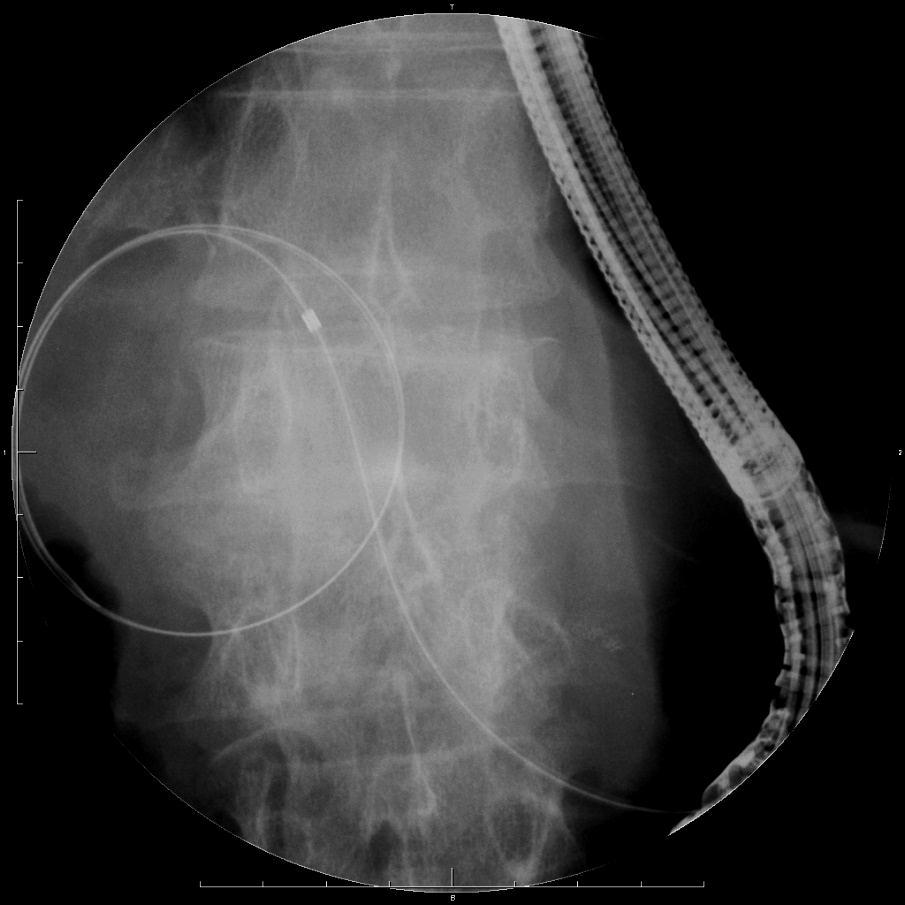
20 Figure legends Fig. 1. Flow diagram of the study participants. Abbreviations: AC, ampullary carcinoma; BDC, bile duct carcinoma; DP, distal pancreatectomy; EUS-TD, endoscopic ultrasound-guided transmural drainage; GBC, gallbladder cancer; HPD, hepatopancreaticoduodenectomy; IPMN, intraductal papillary mucinous neoplasm; MCN, mucinous cystic neoplasm; NET, neuroendocrine tumor; PC, pancreatic carcinoma; PD, pancreaticoduodenectomy; POPF, postoperative pancreatic fistula; SPR, segmental pancreatic resection. Fig. 2 Endoscopic ultrasound-guided transmural drainage (EUS-TD) technique. A Computed tomography scan of the abdomen showing a postoperative pancreatic fistula (arrowhead) that developed 24 months after surgical resection. B EUS image of a pancreatic fistula (arrowhead) showing a 71-mm hypoechoic area and introduction of a needle (dotted arrowhead). C, D, E, F Fluoroscopic images of EUS-TD. A fine aspiration needle was used to puncture the fistula under EUS guidance. A guidewire was introduced through the needle and was coiled within the fistula cavity under fluoroscopic guidance. Dilatation was performed using a dilatation catheter. After dilatation, a 7 Fr double-pigtail stent was inserted into the fistula.
21 Table 1. Characteristics of patients with a postoperative pancreatic fistula before endoscopic treatment. Case Age (yr)/gender Disease Operation Reconstruction Location of POPF POPF grade Size of POPF (mm) Duration from Operation to EUS-TD (months) 1 50/M PC PD PJ Anastomosis of PJ B /M PC PD PJ Anastomosis of PJ B /M BDC HPD PJ Anastomosis of PJ B /M PC DP ( ) Pancreatic body (cut end) B /M BDC HPD PJ Anastomosis of PJ B /M AC PD PG Dilatation of MPD* B 6 3 AC, ampullary carcinoma; BDC, bile duct carcinoma; DP, distal pancreatectomy; EUS-TD, endoscopic ultrasound-guided transmural drainage; HPD, hepatopancreaticoduodenectomy; MPD, main pancreatic duct; PC, pancreatic carcinoma; PD, pancreaticoduodenectomy; PG, pancreatogastrostomy; PJ, pancreatojejunostomy; POPF, postoperative pancreatic fistula. * Case 6 had a dilatation of the pancreatic duct by occlusion of pancreatogastrostomy. The value indicates the MPD diameter.
22 Table 2. Clinical course of patients with a postoperative pancreatic fistula before and after EUS-TD. Case Indwelling stent size Number of EUS-TD procedures Resolution of POPF Period of clinical success (days) Recurrence of POPF Size of POPF or MPD (mm) Before 1 week after drainage drainage Serum amylase (U/l) Before 1 week after drainage drainage Follow up (months) 1 7 Fr-40 mm 2 Yes 4 Yes* Fr-40 mm 1 Yes 5 No Fr-40 mm 1 Yes 7 No Fr-40 mm 1 Yes 7 No Fr-40 mm 1 Yes 7 No Fr-50 mm 1 Yes 5 No 6** 2.5** EUS-TD, endoscopic ultrasound-guided transmural drainage; MPD, main pancreatic duct; POPF, postoperative pancreatic fistula. *Case 1 developed a growth in the cavity by occlusion of the indwelling stent 2 months after the first drainage and underwent stent exchange by a conventional endoscopic approach. **The value of case 6 indicates the MPD diameter.
23 Table 3. Characteristics of the patients with a postoperative pancreatic fistula treated with EUS-TD and percutaneous drainage Characteristic EUS-TD Percutaneous drainage P value Number of cases, n 6 18 NS Male/Female, n 6/0 11/7 NS Mean age, years NS Initial operation, n PD/HPD 3/2 10/3 NS DP 1 5 NS PF location, n Anastomosis of PJ 4 16 NS Pancreatic body 2 2 NS POPF grade/no. of cases B/6 B/11, C/7 Median PF diameter (range), cm 4.9 ( ) 7 (3 14.7) NS Technical success, n (%) 6 (100) 18 (100) NS Short-term clinical success, n (%) 6 (100) 11 (61.1) NS Long-term clinical success, n (%) 6 (100) 15 (83) NS Time till clinical success (range), days 5.8 (4 7) 30.4 (15 57) Complications, n 0 0 NS
24 DP, distal pancreatectomy; HPD, hepatopancreaticoduodenectomy; NS, not significant; PD, pancreaticoduodenectomy; PJ, pancreatojejunostomy; POPF, postoperative pancreatic fistula.
25 Total n=262 POPF (-) or POPF, gradea n=172 POPF grade B or C n=90 Conservative treatment (n=172) Conservative treatment by surgical drain (n=66) Percutaneous drainage (n=18) EUS-TD (n=6) Disease PC 102 BDC 32 NET 13 GBC 5 IPMN 4 AC 4 Others 6 Benign disease 6 Disease BDC 26 PC 23 NET 5 IPMN 4 AC 2 Others 4 Benign disease 2 Disease BDC 10 PC 3 IPMN 2 AC 1 GBC 1 MCN 1 Disease PC 3 BDC 2 AC 1 Surgery PD 116 HPD 8 DP 48 Surgery PD 34 HPD 10 DP 19 SPR 3 Surgery PD 10 HPD 3 DP 5 Surgery PD 3 HPD 2 DP 1




26 A C D B E F
Management of Pancreatic Fistulae
 Management of Pancreatic Fistulae Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Fistula definition A Fistula is a permanent abnormal passageway between two organs (epithelial
Management of Pancreatic Fistulae Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Fistula definition A Fistula is a permanent abnormal passageway between two organs (epithelial
PANCREATIC PSEUDOCYSTS: Optimal therapeutic strategies. Jacques DEVIERE, MD, PhD Erasme University Hospital Brussels
 PANCREATIC PSEUDOCYSTS: Optimal therapeutic strategies Jacques DEVIERE, MD, PhD Erasme University Hospital Brussels 1. Diagnosis. 2. Multidisciplinary approach. 3. Therapeutic planning. 4. How? 5. Follow-up
PANCREATIC PSEUDOCYSTS: Optimal therapeutic strategies Jacques DEVIERE, MD, PhD Erasme University Hospital Brussels 1. Diagnosis. 2. Multidisciplinary approach. 3. Therapeutic planning. 4. How? 5. Follow-up
PANCREATIC PSEUDOCYSTS. Madhuri Rao MD PGY-5 Kings County Hospital Center
 PANCREATIC PSEUDOCYSTS Madhuri Rao MD PGY-5 Kings County Hospital Center 34 yo M Case Presentation PMH: Chronic pancreatitis (ETOH related) PSH: Nil Meds: Nil NKDA www.downstatesurgery.org Symptoms o Chronic
PANCREATIC PSEUDOCYSTS Madhuri Rao MD PGY-5 Kings County Hospital Center 34 yo M Case Presentation PMH: Chronic pancreatitis (ETOH related) PSH: Nil Meds: Nil NKDA www.downstatesurgery.org Symptoms o Chronic
Endoscopic ultrasound-guided drainage of postoperative intra-abdominal abscesses
 Submit a Manuscript: http://www.wjgnet.com/esps/ Help Desk: http://www.wjgnet.com/esps/helpdesk.aspx DOI: 10.3748/wjg.v21.i11.3402 World J Gastroenterol 2015 March 21; 21(11): 3402-3408 ISSN 1007-9327
Submit a Manuscript: http://www.wjgnet.com/esps/ Help Desk: http://www.wjgnet.com/esps/helpdesk.aspx DOI: 10.3748/wjg.v21.i11.3402 World J Gastroenterol 2015 March 21; 21(11): 3402-3408 ISSN 1007-9327
The role of ERCP in chronic pancreatitis
 The role of ERCP in chronic pancreatitis Marianna Arvanitakis Erasme University Hospital, ULB, Brussels, Belgium 10 th Nottingham Endoscopy Masterclass SPEAKER DECLARATIONS This presenter has the following
The role of ERCP in chronic pancreatitis Marianna Arvanitakis Erasme University Hospital, ULB, Brussels, Belgium 10 th Nottingham Endoscopy Masterclass SPEAKER DECLARATIONS This presenter has the following
PANCREATIC PSEUDOCYST DRAINAGE: ENDOSCOPIC APPROACHES & THE NURSING ROLE. PRESENTED BY: Susan DePasquale, CGRN, MSN
 PANCREATIC PSEUDOCYST DRAINAGE: ENDOSCOPIC APPROACHES & THE NURSING ROLE PRESENTED BY: Susan DePasquale, CGRN, MSN Pancreatic Fluid Collection (PFC) A result of pancreatic duct (PD) and side branch disruption,
PANCREATIC PSEUDOCYST DRAINAGE: ENDOSCOPIC APPROACHES & THE NURSING ROLE PRESENTED BY: Susan DePasquale, CGRN, MSN Pancreatic Fluid Collection (PFC) A result of pancreatic duct (PD) and side branch disruption,
Endoscopic Management of Acute Pancreatitis. Theo Doukides, MD Gastroenterology and Therapeutic Endoscopy February 13, 2018
 Endoscopic Management of Acute Pancreatitis Theo Doukides, MD Gastroenterology and Therapeutic Endoscopy February 13, 2018 Objectives Assessment of acute pancreatitis Early management Who needs an ERCP
Endoscopic Management of Acute Pancreatitis Theo Doukides, MD Gastroenterology and Therapeutic Endoscopy February 13, 2018 Objectives Assessment of acute pancreatitis Early management Who needs an ERCP
Research Article Risk Factors for Migration, Fracture, and Dislocation of Pancreatic Stents
 Gastroenterology Research and Practice Volume 2015, Article ID 365457, 6 pages http://dx.doi.org/10.1155/2015/365457 Research Article Risk Factors for Migration, Fracture, and Dislocation of Pancreatic
Gastroenterology Research and Practice Volume 2015, Article ID 365457, 6 pages http://dx.doi.org/10.1155/2015/365457 Research Article Risk Factors for Migration, Fracture, and Dislocation of Pancreatic
EUS-Guided Transduodenal Biliary Drainage in Unresectable Pancreatic Cancer with Obstructive Jaundice
 CASE REPORT EUS-Guided Transduodenal Biliary Drainage in Unresectable Pancreatic Cancer with Obstructive Jaundice Tiing Leong Ang, Eng Kiong Teo, Kwong Ming Fock Division of Gastroenterology, Department
CASE REPORT EUS-Guided Transduodenal Biliary Drainage in Unresectable Pancreatic Cancer with Obstructive Jaundice Tiing Leong Ang, Eng Kiong Teo, Kwong Ming Fock Division of Gastroenterology, Department
and Transmural Drainage
 HPB Surgery, 2000, Vol. 11, pp. 333-338 Reprints available directly from the publisher Photocopying permitted by license only (C) 2000 OPA (Overseas Publishers Association) N.V. Published by license under
HPB Surgery, 2000, Vol. 11, pp. 333-338 Reprints available directly from the publisher Photocopying permitted by license only (C) 2000 OPA (Overseas Publishers Association) N.V. Published by license under
Original Article INTRODUCTION
 Original Article A retrospective study evaluating endoscopic ultrasound guided drainage of pancreatic fluid collections using a novel lumen apposing metal stent on an electrocautery enhanced delivery system
Original Article A retrospective study evaluating endoscopic ultrasound guided drainage of pancreatic fluid collections using a novel lumen apposing metal stent on an electrocautery enhanced delivery system
Clinical evaluation of endoscopic ultrasonography-guided drainage using a novel flared-type biflanged metal stent for pancreatic fluid collection
 Original Article Clinical evaluation of endoscopic ultrasonography-guided drainage using a novel flared-type biflanged metal stent for pancreatic fluid collection Shuntaro Mukai, Takao Itoi, Atsushi Sofuni,
Original Article Clinical evaluation of endoscopic ultrasonography-guided drainage using a novel flared-type biflanged metal stent for pancreatic fluid collection Shuntaro Mukai, Takao Itoi, Atsushi Sofuni,
Endoscopic pancreatic necrosectomy in 2017
 Endoscopic pancreatic necrosectomy in 2017 Mouen Khashab, MD Associate Professor of Medicine Director of Therapeutic Endoscopy The Johns Hopkins Hospital Revised Atlanta Classification Entity Acute fluid
Endoscopic pancreatic necrosectomy in 2017 Mouen Khashab, MD Associate Professor of Medicine Director of Therapeutic Endoscopy The Johns Hopkins Hospital Revised Atlanta Classification Entity Acute fluid
Chronic pancreatitis mimicking intraductal papillary mucinous neoplasm of the pancreas; Report of tow cases
 Jichi Medical University Journal Chronic pancreatitis mimicking intraductal papillary mucinous neoplasm of the pancreas; Report of tow cases Noritoshi Mizuta, Hiroshi Noda, Nao Kakizawa, Nobuyuki Toyama,
Jichi Medical University Journal Chronic pancreatitis mimicking intraductal papillary mucinous neoplasm of the pancreas; Report of tow cases Noritoshi Mizuta, Hiroshi Noda, Nao Kakizawa, Nobuyuki Toyama,
Does it matter what we drain?
 Endoscopic Management of Pancreatic Fluid Collections Shyam Varadarajulu, MD Medical Director Center for Interventional Endoscopy Florida Hospital, Orlando Does it matter what we drain? Makes all the difference!
Endoscopic Management of Pancreatic Fluid Collections Shyam Varadarajulu, MD Medical Director Center for Interventional Endoscopy Florida Hospital, Orlando Does it matter what we drain? Makes all the difference!
Endoscopic Management of the Iatrogenic CBD Injury
 The Liver Week 2014, Jeju, Korea Endoscopic Management of the Iatrogenic CBD Injury Jong Ho Moon, MD, PhD Department of Internal Medicine Soon Chun Hyang University School of Medicine Bucheon/Seoul, KOREA
The Liver Week 2014, Jeju, Korea Endoscopic Management of the Iatrogenic CBD Injury Jong Ho Moon, MD, PhD Department of Internal Medicine Soon Chun Hyang University School of Medicine Bucheon/Seoul, KOREA
Yoshitsugu; Kanematsu, Takashi; Kur
 NAOSITE: Nagasaki University's Ac Title Author(s) Citation Laparoscopic Middle Pancreatectomy Surgery Kitasato, Amane; Adachi, Tomohiko; Yoshitsugu; Kanematsu, Takashi; Kur Hepato-Gastroenterology, 59(120),
NAOSITE: Nagasaki University's Ac Title Author(s) Citation Laparoscopic Middle Pancreatectomy Surgery Kitasato, Amane; Adachi, Tomohiko; Yoshitsugu; Kanematsu, Takashi; Kur Hepato-Gastroenterology, 59(120),
Reinterventions belong to complications
 Reinterventions belong to complications Pancreatic surgery is the archetypus of complex abdominal surgery Mortality (1-4%) and morbidity (7-60%) rates are relevant even at high volume centres Reinterventions
Reinterventions belong to complications Pancreatic surgery is the archetypus of complex abdominal surgery Mortality (1-4%) and morbidity (7-60%) rates are relevant even at high volume centres Reinterventions
ACUTE CHOLANGITIS AS a result of an occluded
 Digestive Endoscopy 2017; 29 (Suppl. 2): 88 93 doi: 10.1111/den.12836 Current status of biliary drainage strategy for acute cholangitis Endoscopic treatment for acute cholangitis with common bile duct
Digestive Endoscopy 2017; 29 (Suppl. 2): 88 93 doi: 10.1111/den.12836 Current status of biliary drainage strategy for acute cholangitis Endoscopic treatment for acute cholangitis with common bile duct
EUS Guided Pancreatic Duct Drainage: When? How?
 PBS-IV Beyond the Horizon of Interventional EUS EUS Guided Pancreatic Duct Drainage: When? How? Uzma D. Siddiqui, M.D. Center for Endoscopic Research and Therapeutics (CERT), University of Chicago Medicine,
PBS-IV Beyond the Horizon of Interventional EUS EUS Guided Pancreatic Duct Drainage: When? How? Uzma D. Siddiqui, M.D. Center for Endoscopic Research and Therapeutics (CERT), University of Chicago Medicine,
A LEADER IN ADVANCED ENDOSCOPY AND HEPATOBILIARY SURGERY
 A LEADER IN ADVANCED ENDOSCOPY AND HEPATOBILIARY SURGERY St. Peter s Hospital Advanced Endoscopy & Hepatobiliary Center Welcome The St. Peter s Hospital Advanced Endoscopy & Hepatobiliary Center is a leader
A LEADER IN ADVANCED ENDOSCOPY AND HEPATOBILIARY SURGERY St. Peter s Hospital Advanced Endoscopy & Hepatobiliary Center Welcome The St. Peter s Hospital Advanced Endoscopy & Hepatobiliary Center is a leader
Evaluation of a new stent for EUS-guided pancreatic duct drainage: long-term follow-up outcome
 Evaluation of a new stent for EUS-guided pancreatic duct drainage: long-term follow-up outcome Authors Yukitoshi Matsunami 1,TakaoItoi 1, Atsushi Sofuni 1, Takayoshi Tsuchiya 1,KentaroKamada 1, Reina Tanaka
Evaluation of a new stent for EUS-guided pancreatic duct drainage: long-term follow-up outcome Authors Yukitoshi Matsunami 1,TakaoItoi 1, Atsushi Sofuni 1, Takayoshi Tsuchiya 1,KentaroKamada 1, Reina Tanaka
Chronic Pancreatitis: When to Scope? Gregory A. Cote, MD, MS Assistant Professor of Medicine Indiana University School of Medicine
 Chronic Pancreatitis: When to Scope? Gregory A. Cote, MD, MS Assistant Professor of Medicine Indiana University School of Medicine Endoscopy & Chronic Pancreatitis Diagnosis EUS ERCP Exocrine Function
Chronic Pancreatitis: When to Scope? Gregory A. Cote, MD, MS Assistant Professor of Medicine Indiana University School of Medicine Endoscopy & Chronic Pancreatitis Diagnosis EUS ERCP Exocrine Function
Endoscopic Ultrasound-Guided Treatment of Pancreaticocutaneous Fistulas
 ACG CASE REPORTS JOURNAL CASE REPORT ENDOSCOPY Endoscopic Ultrasound-Guided Treatment of Pancreaticocutaneous Fistulas Abdul Haseeb, MD, Barham K. Abu Dayyeh, MD, Michael J. Levy, MD, Larissa L. Fujii,
ACG CASE REPORTS JOURNAL CASE REPORT ENDOSCOPY Endoscopic Ultrasound-Guided Treatment of Pancreaticocutaneous Fistulas Abdul Haseeb, MD, Barham K. Abu Dayyeh, MD, Michael J. Levy, MD, Larissa L. Fujii,
Lumen Apposing Metal Stents: Expanding the Role of the Interventional Endoscopist. Alireza Sedarat, MD UCLA Division of Digestive Diseases
 Lumen Apposing Metal Stents: Expanding the Role of the Interventional Endoscopist Alireza Sedarat, MD UCLA Division of Digestive Diseases Disclosures Consultant for Boston Scientific and Olympus Corporation
Lumen Apposing Metal Stents: Expanding the Role of the Interventional Endoscopist Alireza Sedarat, MD UCLA Division of Digestive Diseases Disclosures Consultant for Boston Scientific and Olympus Corporation
Endoscopic Ultrasound-Guided Pancreatic Duct Intervention
 FOCUSED REVIEW SERIES: EUS-Guided Therapeutic Interventions Clin Endosc 2017;50:112-116 https://doi.org/10.5946/ce.2017.046 Print ISSN 2234-2400 On-line ISSN 2234-2443 Open Access Endoscopic Ultrasound-Guided
FOCUSED REVIEW SERIES: EUS-Guided Therapeutic Interventions Clin Endosc 2017;50:112-116 https://doi.org/10.5946/ce.2017.046 Print ISSN 2234-2400 On-line ISSN 2234-2443 Open Access Endoscopic Ultrasound-Guided
M. Ellrichmann; C. Jürgensen; A. Arlt; A. Fritscher-Ravens
 Randomized multicenter study on pancreatic duct stenting in disrupted or obstructed ducts in context with endoscopic treatment of pancreatic pseudocysts. M. Ellrichmann; C. Jürgensen; A. Arlt; A. Fritscher-Ravens
Randomized multicenter study on pancreatic duct stenting in disrupted or obstructed ducts in context with endoscopic treatment of pancreatic pseudocysts. M. Ellrichmann; C. Jürgensen; A. Arlt; A. Fritscher-Ravens
Citation Hepato-Gastroenterology, 55(86-87),
,") NAOSITE: Nagasaki University's Ac Title Author(s) Combined pancreatic resection and p multiple lesions of the pancreas: i of the pancreas concomitant with du Kuroki, Tamotsu; Tajima, Yoshitsugu Tomohiko;
NAOSITE: Nagasaki University's Ac Title Author(s) Combined pancreatic resection and p multiple lesions of the pancreas: i of the pancreas concomitant with du Kuroki, Tamotsu; Tajima, Yoshitsugu Tomohiko;
Review Article Fully Covered Self-Expandable Metal Stents for Treatment of Both Benign and Malignant Biliary Disorders
 Hindawi Publishing Corporation Diagnostic and Therapeutic Endoscopy Volume 2012, Article ID 498617, 5 pages doi:10.1155/2012/498617 Review Article Fully Covered Self-Expandable Metal Stents for Treatment
Hindawi Publishing Corporation Diagnostic and Therapeutic Endoscopy Volume 2012, Article ID 498617, 5 pages doi:10.1155/2012/498617 Review Article Fully Covered Self-Expandable Metal Stents for Treatment
Outcome of pancreatic ascites in patients with tropical calcific pancreatitis managed using a uniform treatment protocol
 Indian J Gastroenterol 2009(May June):28(3):102 106 CASE SERIES Outcome of pancreatic ascites in patients with tropical calcific pancreatitis managed using a uniform treatment protocol Prakash Kurumboor
Indian J Gastroenterol 2009(May June):28(3):102 106 CASE SERIES Outcome of pancreatic ascites in patients with tropical calcific pancreatitis managed using a uniform treatment protocol Prakash Kurumboor
Title. region. Author(s) Citation Surgery, 145(3), pp ; Issue Date
 Citation Surgery, 145(3), pp ; Issue Date") NAOSITE: Nagasaki University's Ac Title Author(s) Huge pancreatic pseudocyst migratin region. Tajima, Yoshitsugu; Mishima, Takehi Taiichiro; Adachi, Tomohiko; Tsuneo Citation Surgery, 145(3), pp.341-342;
NAOSITE: Nagasaki University's Ac Title Author(s) Huge pancreatic pseudocyst migratin region. Tajima, Yoshitsugu; Mishima, Takehi Taiichiro; Adachi, Tomohiko; Tsuneo Citation Surgery, 145(3), pp.341-342;
UvA-DARE (Digital Academic Repository)
") UvA-DARE (Digital Academic Repository) Endosonographic imaging of pancreatic pseudocysts before endoscopic transmural drainage Fockens, P.; Johnson, T.G.; van Dullemen, H.M.; Huibregtse, K.; Tytgat, G.N.J.
UvA-DARE (Digital Academic Repository) Endosonographic imaging of pancreatic pseudocysts before endoscopic transmural drainage Fockens, P.; Johnson, T.G.; van Dullemen, H.M.; Huibregtse, K.; Tytgat, G.N.J.
Safety and Efficacy of Endoscopic Ultrasound-Guided Drainage of Pancreatic Fluid Collections With Lumen-Apposing Covered Self-Expanding Metal Stents
 All studies published in Clinical Gastroenterology and Hepatology are embargoed until 3PM ET of the day they are published as corrected proofs on-line. Studies cannot be publicized as accepted manuscripts
All studies published in Clinical Gastroenterology and Hepatology are embargoed until 3PM ET of the day they are published as corrected proofs on-line. Studies cannot be publicized as accepted manuscripts
Post-operative complications following hepatobiliary surgery: imaging findings and current radiological treatment options
 Post-operative complications following hepatobiliary surgery: imaging findings and current radiological treatment options Poster No.: C-1501 Congress: ECR 2015 Type: Educational Exhibit Authors: A. Hadjivassiliou,
Post-operative complications following hepatobiliary surgery: imaging findings and current radiological treatment options Poster No.: C-1501 Congress: ECR 2015 Type: Educational Exhibit Authors: A. Hadjivassiliou,
Naoyuki Toyota, Tadahiro Takada, Hodaka Amano, Masahiro Yoshida, Fumihiko Miura, and Keita Wada
 J Hepatobiliary Pancreat Surg (2006) 13:80 85 DOI 10.1007/s00534-005-1062-4 Endoscopic naso-gallbladder drainage in the treatment of acute cholecystitis: alleviates inflammation and fixes operator s aim
J Hepatobiliary Pancreat Surg (2006) 13:80 85 DOI 10.1007/s00534-005-1062-4 Endoscopic naso-gallbladder drainage in the treatment of acute cholecystitis: alleviates inflammation and fixes operator s aim
Mild. Moderate. Severe
 2012 Revised Atlanta Classification Acute pancreatitis Classified based on absence or presence of local and/or systemic complications Mild Acute Pancreatits Moderate Severe P. A. Banks, T. L. Bollen, C.
2012 Revised Atlanta Classification Acute pancreatitis Classified based on absence or presence of local and/or systemic complications Mild Acute Pancreatits Moderate Severe P. A. Banks, T. L. Bollen, C.
EUS-Guided Multitransgastric Endoscopic Necrosectomy for Infected Pancreatic Necrosis with Noncontagious Retroperitoneal and Peritoneal Extension
 Gut and Liver, Vol. 4, No. 1, March 2010, pp. 140-145 Case report EUS-Guided Multitransgastric Endoscopic Necrosectomy for Infected Pancreatic Necrosis with Noncontagious Retroperitoneal and Peritoneal
Gut and Liver, Vol. 4, No. 1, March 2010, pp. 140-145 Case report EUS-Guided Multitransgastric Endoscopic Necrosectomy for Infected Pancreatic Necrosis with Noncontagious Retroperitoneal and Peritoneal
Endoscopic ultrasound guided gastrojejunostomy
 Review Article Endoscopic ultrasound guided gastrojejunostomy Enad Dawod 1, Jose M. Nieto 2 1 Weill Cornell Medicine, Department of Gastroenterology and Hepatology, New York, NY, USA; 2 Borland Groover
Review Article Endoscopic ultrasound guided gastrojejunostomy Enad Dawod 1, Jose M. Nieto 2 1 Weill Cornell Medicine, Department of Gastroenterology and Hepatology, New York, NY, USA; 2 Borland Groover
Making ERCP Easy: Tips From A Master
 Making ERCP Easy: Tips From A Master Raj J. Shah, M.D., FASGE Associate Professor of Medicine University of Colorado School of Medicine Co-Director, Endoscopy Director, Pancreaticobiliary Endoscopy Services
Making ERCP Easy: Tips From A Master Raj J. Shah, M.D., FASGE Associate Professor of Medicine University of Colorado School of Medicine Co-Director, Endoscopy Director, Pancreaticobiliary Endoscopy Services
Endoscopic treatment for chronic pancreatitis: indications, technique, results
 J Hepatobiliary Pancreat Sci (2010) 17:770 775 DOI 10.1007/s00534-009-0182-7 TOPICS Chronic pancreatitis: current treatment strategies Endoscopic treatment for chronic pancreatitis: indications, technique,
J Hepatobiliary Pancreat Sci (2010) 17:770 775 DOI 10.1007/s00534-009-0182-7 TOPICS Chronic pancreatitis: current treatment strategies Endoscopic treatment for chronic pancreatitis: indications, technique,
Clinical Study Endoscopic Ultrasound-Guided Drainage without Fluoroscopic Guidance for Extraluminal Complicated Cysts
 Gastroenterology Research and Practice Volume 2016, Article ID 1249064, 8 pages http://dx.doi.org/10.1155/2016/1249064 Clinical Study Endoscopic Ultrasound-Guided Drainage without Fluoroscopic Guidance
Gastroenterology Research and Practice Volume 2016, Article ID 1249064, 8 pages http://dx.doi.org/10.1155/2016/1249064 Clinical Study Endoscopic Ultrasound-Guided Drainage without Fluoroscopic Guidance
Clinical Study Covered Metal Stenting for Malignant Lower Biliary Stricture with Pancreatic Duct Obstruction: Is Endoscopic Sphincterotomy Needed?
 Gastroenterology Research and Practice Volume 2013, Article ID 375613, 6 pages http://dx.doi.org/10.1155/2013/375613 Clinical Study Covered Metal Stenting for Malignant Lower Biliary Stricture with Pancreatic
Gastroenterology Research and Practice Volume 2013, Article ID 375613, 6 pages http://dx.doi.org/10.1155/2013/375613 Clinical Study Covered Metal Stenting for Malignant Lower Biliary Stricture with Pancreatic
Primary acinar cell carcinoma of the ampulla of Vate. The original publication is available at Instructions for use
 Title Primary acinar cell carcinoma of the ampulla of Vate Kawakami, Hiroshi; Kuwatani, Masaki; Onodera, Manabu Author(s) Itoh, Tomoo; Asaka, Masahiro CitationJournal of gastroenterology, 42(8): 694-697
Title Primary acinar cell carcinoma of the ampulla of Vate Kawakami, Hiroshi; Kuwatani, Masaki; Onodera, Manabu Author(s) Itoh, Tomoo; Asaka, Masahiro CitationJournal of gastroenterology, 42(8): 694-697
The Pancreas. Basic Anatomy. Endocrine pancreas. Exocrine pancreas. Pancreas vasculature. Islets of Langerhans. Acinar cells Ductal System
 SGNA: Back to Basics Rogelio G. Silva, MD Assistant Clinical Professor of Medicine University of Illinois at Chicago Department of Medicine Division of Gastroenterology Advocate Christ Medical Center GI
SGNA: Back to Basics Rogelio G. Silva, MD Assistant Clinical Professor of Medicine University of Illinois at Chicago Department of Medicine Division of Gastroenterology Advocate Christ Medical Center GI
Vascular complications in percutaneous biliary interventions: A series of 111 procedures
 Vascular complications in percutaneous biliary interventions: A series of 111 procedures Poster No.: C-0744 Congress: ECR 2013 Type: Educational Exhibit Authors: A. BHARADWAZ; AARHUS, Re/DK Keywords: Obstruction
Vascular complications in percutaneous biliary interventions: A series of 111 procedures Poster No.: C-0744 Congress: ECR 2013 Type: Educational Exhibit Authors: A. BHARADWAZ; AARHUS, Re/DK Keywords: Obstruction
6/17/2016. ERCP in June 26, Kenneth M. Sigman, M.D. Birmingham Gastroenterology Associates
 ERCP in 2016 June 26, 2016 Kenneth M. Sigman, M.D. Birmingham Gastroenterology Associates 1 2 3 Diagnostic/Therapeutic ERCP Biliary Obstruction Benign stricture Malignant Stones Ductal injuries Cholangitis
ERCP in 2016 June 26, 2016 Kenneth M. Sigman, M.D. Birmingham Gastroenterology Associates 1 2 3 Diagnostic/Therapeutic ERCP Biliary Obstruction Benign stricture Malignant Stones Ductal injuries Cholangitis
The Use of Pancreatoscopy in the Diagnosis of Intraductal Papillary Mucinous Tumor Lesions of the Pancreas
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2005;3:S53 S57 The Use of Pancreatoscopy in the Diagnosis of Intraductal Papillary Mucinous Tumor Lesions of the Pancreas KENJIRO YASUDA, MUNEHIRO SAKATA, MOOSE
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2005;3:S53 S57 The Use of Pancreatoscopy in the Diagnosis of Intraductal Papillary Mucinous Tumor Lesions of the Pancreas KENJIRO YASUDA, MUNEHIRO SAKATA, MOOSE
THE CRITICAL COMPLCATIONS AND MANAGEMENTS AFTER PANCREATIC SURGERY 2013/12/21
 THE CRITICAL COMPLCATIONS AND MANAGEMENTS AFTER PANCREATIC SURGERY Tsann-Long Hwang, MD, FACS Department of Surgery Chang Gung Memorial Hospital Chang Gung University Taipei, TAIWAN 2013/12/21 THE DIFFICULTY
THE CRITICAL COMPLCATIONS AND MANAGEMENTS AFTER PANCREATIC SURGERY Tsann-Long Hwang, MD, FACS Department of Surgery Chang Gung Memorial Hospital Chang Gung University Taipei, TAIWAN 2013/12/21 THE DIFFICULTY
Endoscopic Management of Biliary Strictures. Sammy Ho, MD Director of Pancreaticobiliary Services and Endoscopic Ultrasound Montefiore Medical Center
 Endoscopic Management of Biliary Strictures Sammy Ho, MD Director of Pancreaticobiliary Services and Endoscopic Ultrasound Montefiore Medical Center Malignant Biliary Strictures Etiologies: Pancreatic
Endoscopic Management of Biliary Strictures Sammy Ho, MD Director of Pancreaticobiliary Services and Endoscopic Ultrasound Montefiore Medical Center Malignant Biliary Strictures Etiologies: Pancreatic
Pancreatoscopy-Directed Electrohydraulic Lithotripsy for Pancreatic Ductal Stones in Painful
 Pancreatoscopy-Directed Electrohydraulic Lithotripsy for Pancreatic Ductal Stones in Painful Chronic Pancreatitis Using SpyGlass Short title: EHL for Pancreatic Ductal Stones Noor LH Bekkali 1, MD, PhD;
Pancreatoscopy-Directed Electrohydraulic Lithotripsy for Pancreatic Ductal Stones in Painful Chronic Pancreatitis Using SpyGlass Short title: EHL for Pancreatic Ductal Stones Noor LH Bekkali 1, MD, PhD;
Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds
 Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds Imaging in jaundice and 2ww pathway Image protocol Staging Limitations Pancreatic cancer 1.2.4 Refer people using a suspected
Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds Imaging in jaundice and 2ww pathway Image protocol Staging Limitations Pancreatic cancer 1.2.4 Refer people using a suspected
CHRONIC PANCREATITIS CONSERVATIVE TREATMENT, ENDOSCOPY OR SURGERY?
 Endoscopy 2006 Update and Live Demonstration Berlin, 04. 05. Mai 2006 CHRONIC PANCREATITIS CONSERVATIVE TREATMENT, ENDOSCOPY OR SURGERY? J. F. Riemann A. Rosenbaum Medizinische Klinik C, Klinikum Ludwigshafen
Endoscopy 2006 Update and Live Demonstration Berlin, 04. 05. Mai 2006 CHRONIC PANCREATITIS CONSERVATIVE TREATMENT, ENDOSCOPY OR SURGERY? J. F. Riemann A. Rosenbaum Medizinische Klinik C, Klinikum Ludwigshafen
ACG Clinical Guideline: Diagnosis and Management of Pancreatic Cysts
 ACG Clinical Guideline: Diagnosis and Management of Pancreatic Cysts Grace H. Elta, MD, FACG 1, Brintha K. Enestvedt, MD, MBA 2, Bryan G. Sauer, MD, MSc, FACG (GRADE Methodologist) 3 and Anne Marie Lennon,
ACG Clinical Guideline: Diagnosis and Management of Pancreatic Cysts Grace H. Elta, MD, FACG 1, Brintha K. Enestvedt, MD, MBA 2, Bryan G. Sauer, MD, MSc, FACG (GRADE Methodologist) 3 and Anne Marie Lennon,
A tale of two LAMS: a report of benign tissue ingrowth resulting in recurrent gastric outlet obstruction
 A tale of two LAMS: a report of benign tissue ingrowth resulting in recurrent gastric outlet obstruction Authors Parth J. Parekh, Mohammad H. Shakhatreh, Paul Yeaton Institution Department of Internal
A tale of two LAMS: a report of benign tissue ingrowth resulting in recurrent gastric outlet obstruction Authors Parth J. Parekh, Mohammad H. Shakhatreh, Paul Yeaton Institution Department of Internal
The role of endoscopy in the diagnosis and treatment of cystic pancreatic neoplasms
 The role of endoscopy in the diagnosis and treatment of cystic pancreatic neoplasms CYSTIC LESIONS AND FLUID COLLECTIONS OF THE PANCREAS Their pathology ranges from pseudocysts and pancreatic necrosis
The role of endoscopy in the diagnosis and treatment of cystic pancreatic neoplasms CYSTIC LESIONS AND FLUID COLLECTIONS OF THE PANCREAS Their pathology ranges from pseudocysts and pancreatic necrosis
Citation American Journal of Surgery, 196(5)
") NAOSITE: Nagasaki University's Ac Title Author(s) Multifocal branch-duct pancreatic i neoplasms Tajima, Yoshitsugu; Kuroki, Tamotsu Amane; Adachi, Tomohiko; Mishima, T Kanematsu, Takashi Citation American
NAOSITE: Nagasaki University's Ac Title Author(s) Multifocal branch-duct pancreatic i neoplasms Tajima, Yoshitsugu; Kuroki, Tamotsu Amane; Adachi, Tomohiko; Mishima, T Kanematsu, Takashi Citation American
Endoscopic Treatment of Luminal Perforations and Leaks
 Endoscopic Treatment of Luminal Perforations and Leaks Ali A. Siddiqui, MD Professor of Medicine Director of Interventional Endoscopy Jefferson Medical College Philadelphia, PA When Do You Suspect a Luminal
Endoscopic Treatment of Luminal Perforations and Leaks Ali A. Siddiqui, MD Professor of Medicine Director of Interventional Endoscopy Jefferson Medical College Philadelphia, PA When Do You Suspect a Luminal
Стенты «Ella-cs» Уважаемые коллеги! Высылаем очередной выпуск «Issue of ELLA Abstracts»
 Уважаемые коллеги! Высылаем очередной выпуск «Issue of ELLA Abstracts» A. Esophageal Stenting and related topics 1 AMJG 2009; 104:1329 1330 Letters to Editor Early Tracheal Stenosis Post Esophageal Stent
Уважаемые коллеги! Высылаем очередной выпуск «Issue of ELLA Abstracts» A. Esophageal Stenting and related topics 1 AMJG 2009; 104:1329 1330 Letters to Editor Early Tracheal Stenosis Post Esophageal Stent
Principles of ERCP: papilla cannulation, indications/contraindications and risks. Dr. med. Henrik Csaba Horváth PhD
 Principles of ERCP: papilla cannulation, indications/contraindications and risks Dr. med. Henrik Csaba Horváth PhD Evolution of ERCP 1968. 1970s ECPG Endoscopic CholangioPancreatoGraphy Japan 1974 Biliary
Principles of ERCP: papilla cannulation, indications/contraindications and risks Dr. med. Henrik Csaba Horváth PhD Evolution of ERCP 1968. 1970s ECPG Endoscopic CholangioPancreatoGraphy Japan 1974 Biliary
Outcomes associated with robotic approach to pancreatic resections
 Short Communication (Management of Foregut Malignancies and Hepatobiliary Tract and Pancreas Malignancies) Outcomes associated with robotic approach to pancreatic resections Caitlin Takahashi 1, Ravi Shridhar
Short Communication (Management of Foregut Malignancies and Hepatobiliary Tract and Pancreas Malignancies) Outcomes associated with robotic approach to pancreatic resections Caitlin Takahashi 1, Ravi Shridhar
Imaging Guided Biopsy. Edited & Presented by ; Hussien A.B ALI DINAR. Msc Lecturer,Reporting Sonographer
 Imaging Guided Biopsy Edited & Presented by ; Hussien A.B ALI DINAR. Msc Lecturer,Reporting Sonographer Objective By the End of this lessons you should : Define what biopsy Justify Aim to perform biopsy
Imaging Guided Biopsy Edited & Presented by ; Hussien A.B ALI DINAR. Msc Lecturer,Reporting Sonographer Objective By the End of this lessons you should : Define what biopsy Justify Aim to perform biopsy
Endoscopic Ultrasonography Assessment for Ampullary and Bile Duct Malignancy
 Diagnostic and Therapeutic Endoscopy, Vol. 3, pp. 35-40 Reprints available directly from the publisher Photocopying permitted by license only (C) 1996 OPA (Overseas Publishers Association) Amsterdam B.V.
Diagnostic and Therapeutic Endoscopy, Vol. 3, pp. 35-40 Reprints available directly from the publisher Photocopying permitted by license only (C) 1996 OPA (Overseas Publishers Association) Amsterdam B.V.
Information Technology Solutions
 2016 2014 CPT Esophagoscopy Changes - Gastroenterology CPT Changes Information Technology Solutions ASGE LOGO AND INFO Esophagogastroduodenoscopy CPT Codes 43235-43270 The American Society for Gastrointestinal
2016 2014 CPT Esophagoscopy Changes - Gastroenterology CPT Changes Information Technology Solutions ASGE LOGO AND INFO Esophagogastroduodenoscopy CPT Codes 43235-43270 The American Society for Gastrointestinal
Endoscopic Management of Perforations
 Endoscopic Management of Perforations Gregory G. Ginsberg, MD Professor of Medicine University of Pennsylvania Perelman School of Medicine Gastroenterology Division Executive Director of Endoscopic Services
Endoscopic Management of Perforations Gregory G. Ginsberg, MD Professor of Medicine University of Pennsylvania Perelman School of Medicine Gastroenterology Division Executive Director of Endoscopic Services
Performance of novel tissue harmonic echo imaging using endoscopic ultrasound for pancreatic diseases
 E Performance of novel tissue harmonic echo imaging using endoscopic ultrasound for pancreatic diseases Authors Kazuyuki Matsumoto, *, Akio Katanuma, *, Hiroyuki Maguchi, Kuniyuki Takahashi, Manabu Osanai,
E Performance of novel tissue harmonic echo imaging using endoscopic ultrasound for pancreatic diseases Authors Kazuyuki Matsumoto, *, Akio Katanuma, *, Hiroyuki Maguchi, Kuniyuki Takahashi, Manabu Osanai,
Surgical Management of Chronic Pancreatitis VERENA LIU, MD KINGS COUNTY HOSPITAL CENTER SURGERY GRAND ROUNDS 4/1/2013
 Surgical Management of Chronic Pancreatitis VERENA LIU, MD KINGS COUNTY HOSPITAL CENTER SURGERY GRAND ROUNDS 4/1/2013 Case Report 42F with h/o chronic pancreatitis due to alcohol use with chronic upper
Surgical Management of Chronic Pancreatitis VERENA LIU, MD KINGS COUNTY HOSPITAL CENTER SURGERY GRAND ROUNDS 4/1/2013 Case Report 42F with h/o chronic pancreatitis due to alcohol use with chronic upper
Diagnosis of tumor extension in biliary carcinoma has. Differential Diagnosis and Treatment of Biliary Strictures
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2009;7:S79 S83 Differential Diagnosis and Treatment of Biliary Strictures KAZUO INUI, JUNJI YOSHINO, and HIRONAO MIYOSHI Department of Internal Medicine, Second
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2009;7:S79 S83 Differential Diagnosis and Treatment of Biliary Strictures KAZUO INUI, JUNJI YOSHINO, and HIRONAO MIYOSHI Department of Internal Medicine, Second
Diagnostic performance of endoscopic ultrasound-guided fine-needle aspiration in pancreatic lesions
 European Review for Medical and Pharmacological Sciences 2018; 22: 1397-1401 Diagnostic performance of endoscopic in pancreatic lesions Q.-M. WU 1, Y.-N. GUO 1, Y.-Q. XU 1 Digestive Department of Beijing
European Review for Medical and Pharmacological Sciences 2018; 22: 1397-1401 Diagnostic performance of endoscopic in pancreatic lesions Q.-M. WU 1, Y.-N. GUO 1, Y.-Q. XU 1 Digestive Department of Beijing
An investigation of pancreatic volume by disease using pancreatic volumetry
 Yamagata Med J (ISSN 0288-030X)2015;33(2):71-76 DOI 10.15022/00003469 An investigation of pancreatic volume by disease using pancreatic volumetry Tsuyoshi Fukumoto, Toshihiro Watanabe, Koji Tezuka, Akiko
Yamagata Med J (ISSN 0288-030X)2015;33(2):71-76 DOI 10.15022/00003469 An investigation of pancreatic volume by disease using pancreatic volumetry Tsuyoshi Fukumoto, Toshihiro Watanabe, Koji Tezuka, Akiko
Comparative evaluation of structural and functional changes in pancreas after endoscopic and surgical management of pancreatic necrosis
 ORIGINAL ARTICLE Annals of Gastroenterology (2014) 27, 162-166 Comparative evaluation of structural and functional changes in pancreas after endoscopic and surgical management of pancreatic necrosis Surinder
ORIGINAL ARTICLE Annals of Gastroenterology (2014) 27, 162-166 Comparative evaluation of structural and functional changes in pancreas after endoscopic and surgical management of pancreatic necrosis Surinder
Endoscopic management of postoperative bile duct injuries: a single center experience.
 1- Endoscopic management of postoperative bile duct injuries: a single center experience. BACKGROUND/AIM: Biliary endoscopic procedures may be less invasive than surgery for management of postoperative
1- Endoscopic management of postoperative bile duct injuries: a single center experience. BACKGROUND/AIM: Biliary endoscopic procedures may be less invasive than surgery for management of postoperative
MATERIALS AND METHODS Patients
 Yonago Acta medica 216;59:232 236 Original Article Usefulness of T-Shaped Gauze for Precise Dissection of Supra-Pancreatic Lymph Nodes and for Reduced Postoperative Pancreatic Fistula in Patients Undergoing
Yonago Acta medica 216;59:232 236 Original Article Usefulness of T-Shaped Gauze for Precise Dissection of Supra-Pancreatic Lymph Nodes and for Reduced Postoperative Pancreatic Fistula in Patients Undergoing
Therapeutic EUS: today & tomorrow Pietro Fusaroli
 Therapeutic EUS: today & tomorrow Pietro Fusaroli Gastroenterologia Università di Bologna AUSL di Imola, Castel S. Pietro Terme (BO) Direttore Prof. G. Caletti EUS FNA: CONVEX ARRAY Olympus, Pentax, Toshiba
Therapeutic EUS: today & tomorrow Pietro Fusaroli Gastroenterologia Università di Bologna AUSL di Imola, Castel S. Pietro Terme (BO) Direttore Prof. G. Caletti EUS FNA: CONVEX ARRAY Olympus, Pentax, Toshiba
STRICTURES OF THE BILE DUCTS Session No.: 5. Andrea Tringali Digestive Endoscopy Unit Catholic University Rome - Italy
 STRICTURES OF THE BILE DUCTS Session No.: 5 Andrea Tringali Digestive Endoscopy Unit Catholic University Rome - Italy Drainage of biliary strictures. The history before 1980 Surgical bypass Percutaneous
STRICTURES OF THE BILE DUCTS Session No.: 5 Andrea Tringali Digestive Endoscopy Unit Catholic University Rome - Italy Drainage of biliary strictures. The history before 1980 Surgical bypass Percutaneous
Complex pancreatico- duodenal injuries. Elmin Steyn Head, Division of Surgery Faculty of Health Sciences Stellenbosch University
 Complex pancreatico- duodenal injuries Elmin Steyn Head, Division of Surgery Faculty of Health Sciences Stellenbosch University Pancreatic and duodenal trauma: daunting or simply confusing? 2-4% of abdominal
Complex pancreatico- duodenal injuries Elmin Steyn Head, Division of Surgery Faculty of Health Sciences Stellenbosch University Pancreatic and duodenal trauma: daunting or simply confusing? 2-4% of abdominal
Original article. Introduction!
 382 Original article Peritoneal seeding in intraductal papillary mucinous neoplasm of the pancreas patients who underwent endoscopic ultrasound-guided fine-needle aspiration: The PIPE Study Authors Won
382 Original article Peritoneal seeding in intraductal papillary mucinous neoplasm of the pancreas patients who underwent endoscopic ultrasound-guided fine-needle aspiration: The PIPE Study Authors Won
Jennifer Hsieh 1, Amar Thosani 1, Matthew Grunwald 2, Satish Nagula 1, Juan Carlos Bucobo 1, Jonathan M. Buscaglia 1. Introduction
 How We Do It Serial insertion of bilateral uncovered metal stents for malignant hilar obstruction using an 8 Fr biliary system: a case series of 17 consecutive patients Jennifer Hsieh 1, Amar Thosani 1,
How We Do It Serial insertion of bilateral uncovered metal stents for malignant hilar obstruction using an 8 Fr biliary system: a case series of 17 consecutive patients Jennifer Hsieh 1, Amar Thosani 1,
Title: The endoscopic ultrasound-assisted Rendez-Vous technique for treatment of recurrent pancreatitis due to pancreas divisum and ansa pancreatica
 Title: The endoscopic ultrasound-assisted Rendez-Vous technique for treatment of recurrent pancreatitis due to pancreas divisum and ansa pancreatica Authors: Sergio López-Durán, Celia Zaera, Juan Ángel
Title: The endoscopic ultrasound-assisted Rendez-Vous technique for treatment of recurrent pancreatitis due to pancreas divisum and ansa pancreatica Authors: Sergio López-Durán, Celia Zaera, Juan Ángel
Esophageal seeding after endoscopic ultrasound-guided fine-needle aspiration of a mediastinal tumor
 Esophageal seeding after endoscopic ultrasound-guided fine-needle aspiration of a mediastinal tumor Authors Kensuke Yokoyama 1,JunUshio 1,NorikatsuNumao 1, Kiichi Tamada 1, Noriyoshi Fukushima 2, Alan
Esophageal seeding after endoscopic ultrasound-guided fine-needle aspiration of a mediastinal tumor Authors Kensuke Yokoyama 1,JunUshio 1,NorikatsuNumao 1, Kiichi Tamada 1, Noriyoshi Fukushima 2, Alan
Anatomical and Functional MRI of the Pancreas
 Anatomical and Functional MRI of the Pancreas MA Bali, MD, T Metens, PhD Erasme Hospital Free University of Brussels Belgium mbali@ulb.ac.be Introduction The use of MRI to investigate the pancreas has
Anatomical and Functional MRI of the Pancreas MA Bali, MD, T Metens, PhD Erasme Hospital Free University of Brussels Belgium mbali@ulb.ac.be Introduction The use of MRI to investigate the pancreas has
Evaluation of AGA and Fukuoka Guidelines for EUS and surgical resection of incidental pancreatic cysts
 Evaluation of AGA and Fukuoka Guidelines for EUS and surgical resection of incidental pancreatic cysts Authors Alexander Lee 1, Vivek Kadiyala 2,LindaS.Lee 3 Institutions 1 Texas Digestive Disease Consultants,
Evaluation of AGA and Fukuoka Guidelines for EUS and surgical resection of incidental pancreatic cysts Authors Alexander Lee 1, Vivek Kadiyala 2,LindaS.Lee 3 Institutions 1 Texas Digestive Disease Consultants,
Tomonari, Akiko; Katanuma, Akio; Ma Author(s)
") Resected tumor seeding in stomach w Titleultrasonography-guided fine needle adenocarcinoma Tomonari, Akiko; Katanuma, Akio; Ma Author(s) Yamazaki, Hajime; Sano, Itsuki; Min Manabu; Ikarashi, Satoshi; Kin,
Resected tumor seeding in stomach w Titleultrasonography-guided fine needle adenocarcinoma Tomonari, Akiko; Katanuma, Akio; Ma Author(s) Yamazaki, Hajime; Sano, Itsuki; Min Manabu; Ikarashi, Satoshi; Kin,
The first stents designed for use in the biliary tree and
 Imaging and Advanced Technology Michael B. Wallace, Section Editor Expandable Gastrointestinal Stents TODD H. BARON Department of Medicine, Division of Gastroenterology & Hepatology, Mayo Clinic, Rochester,
Imaging and Advanced Technology Michael B. Wallace, Section Editor Expandable Gastrointestinal Stents TODD H. BARON Department of Medicine, Division of Gastroenterology & Hepatology, Mayo Clinic, Rochester,
Successful Endoscopic Treatment of Severe Pancreaticojejunostomy Strictures by Puncturing the Anastomotic Site with an EUS-guided Guidewire
 doi: 10.2169/internalmedicine.9133-17 http://internmed.jp CASE REPORT Successful Endoscopic Treatment of Severe Pancreaticojejunostomy Strictures by Puncturing the Anastomotic Site with an EUS-guided Guidewire
doi: 10.2169/internalmedicine.9133-17 http://internmed.jp CASE REPORT Successful Endoscopic Treatment of Severe Pancreaticojejunostomy Strictures by Puncturing the Anastomotic Site with an EUS-guided Guidewire
Correspondence should be addressed to Justin Cochrane;
 Case Reports in Gastrointestinal Medicine Volume 2015, Article ID 794282, 4 pages http://dx.doi.org/10.1155/2015/794282 Case Report Acute on Chronic Pancreatitis Causing a Highway to the Colon with Subsequent
Case Reports in Gastrointestinal Medicine Volume 2015, Article ID 794282, 4 pages http://dx.doi.org/10.1155/2015/794282 Case Report Acute on Chronic Pancreatitis Causing a Highway to the Colon with Subsequent
Endoscopic Ultrasonography Clinical Impact. Giancarlo Caletti. Gastroenterologia Università di Bologna. Caletti
 Clinical Impact Giancarlo Gastroenterologia Università di Bologna AUSL di Imola,, Castel S. Pietro Terme (BO) 1982 Indications Diagnosis of Submucosal Tumors (SMT) Staging of Neoplasms Evaluation of Pancreato-Biliary
Clinical Impact Giancarlo Gastroenterologia Università di Bologna AUSL di Imola,, Castel S. Pietro Terme (BO) 1982 Indications Diagnosis of Submucosal Tumors (SMT) Staging of Neoplasms Evaluation of Pancreato-Biliary
P resently, pancreaticoduodenectomy is widely accepted as the standard surgical procedure for patients with
 OPEN SUBJECT AREAS: CANCER THERAPY PANCREATIC CANCER GASTROINTESTINAL CANCER OUTCOMES RESEARCH Received 13 May 2013 Accepted 3 June 2013 Published 25 June 2013 Correspondence and requests for materials
OPEN SUBJECT AREAS: CANCER THERAPY PANCREATIC CANCER GASTROINTESTINAL CANCER OUTCOMES RESEARCH Received 13 May 2013 Accepted 3 June 2013 Published 25 June 2013 Correspondence and requests for materials
Management of the Mucin Filled Bile Duct. A Complication of Intraductal Papillary Mucinous Tumor of the Pancreas
 CASE REPORT Management of the Mucin Filled Bile Duct. A Complication of Intraductal Papillary Mucinous Tumor of the Pancreas Anand Patel, Louis Lambiase, Antonio Decarli, Ali Fazel Division of Gastroenterology
CASE REPORT Management of the Mucin Filled Bile Duct. A Complication of Intraductal Papillary Mucinous Tumor of the Pancreas Anand Patel, Louis Lambiase, Antonio Decarli, Ali Fazel Division of Gastroenterology
An Approach to Pancreatic Cysts. Introduction
 An Approach to Pancreatic Cysts Nalini M. Guda, MD Aurora St. Luke s Medical Center, Milwaukee Clinical Adjunct Professor of Medicine, University of Wisconsin School of Medicine and Public Health Introduction
An Approach to Pancreatic Cysts Nalini M. Guda, MD Aurora St. Luke s Medical Center, Milwaukee Clinical Adjunct Professor of Medicine, University of Wisconsin School of Medicine and Public Health Introduction
Keywords. Abstract. Introduction
 The Safety of Endoscopic Ultrasonography-Guided Drainage of Pancreatic Fluid Collections Without Fluoroscopic Control: a Single Tertiary Center Experience Andrada Seicean 1, Roxana Stan-Iuga 1, Radu Badea
The Safety of Endoscopic Ultrasonography-Guided Drainage of Pancreatic Fluid Collections Without Fluoroscopic Control: a Single Tertiary Center Experience Andrada Seicean 1, Roxana Stan-Iuga 1, Radu Badea
An Intra-Hepatic Pancreatic Pseudocyst Successfully Treated by Endoscopic Transpapillary Drainage Alone
 CASE REPORT An Intra-Hepatic Pancreatic Pseudocyst Successfully Treated by Endoscopic Transpapillary Drainage Alone Deepak Kumar Bhasin, Surinder Singh Rana, Vijant Singh Chandail, Mohit Nanda, Nikhil
CASE REPORT An Intra-Hepatic Pancreatic Pseudocyst Successfully Treated by Endoscopic Transpapillary Drainage Alone Deepak Kumar Bhasin, Surinder Singh Rana, Vijant Singh Chandail, Mohit Nanda, Nikhil
Congenital dilatation of the common bile duct and pancreaticobiliary maljunction clinical implications
 Langenbecks Arch Surg (2009) 394:209 213 DOI 10.1007/s00423-008-0330-6 CURRENT CONCEPT IN CLINICAL SURGERY Congenital dilatation of the common bile duct and pancreaticobiliary maljunction clinical implications
Langenbecks Arch Surg (2009) 394:209 213 DOI 10.1007/s00423-008-0330-6 CURRENT CONCEPT IN CLINICAL SURGERY Congenital dilatation of the common bile duct and pancreaticobiliary maljunction clinical implications
Sreeni Jonnalagadda, MD., FASGE Professor of Medicine, UMKC Director of Interventional Endoscopy Saint Luke s Hospital, Kansas City
 Sreeni Jonnalagadda, MD., FASGE Professor of Medicine, UMKC Director of Interventional Endoscopy Saint Luke s Hospital, Kansas City Peptic stricture Shtki Schatzki s ring Esophageal cancer Radiation therapy
Sreeni Jonnalagadda, MD., FASGE Professor of Medicine, UMKC Director of Interventional Endoscopy Saint Luke s Hospital, Kansas City Peptic stricture Shtki Schatzki s ring Esophageal cancer Radiation therapy
The Risk Factors for Acute Pancreatitis after Endoscopic Ultrasound Guided Biopsy
 Korean J Gastroenterol Vol. 72 No. 3, 135-140 https://doi.org/10.4166/kjg.2018.72.3.135 pissn 1598-9992 eissn 2233-6869 ORIGINAL ARTICLE The Risk Factors for Acute Pancreatitis after Endoscopic Ultrasound
Korean J Gastroenterol Vol. 72 No. 3, 135-140 https://doi.org/10.4166/kjg.2018.72.3.135 pissn 1598-9992 eissn 2233-6869 ORIGINAL ARTICLE The Risk Factors for Acute Pancreatitis after Endoscopic Ultrasound
ESPEN Congress Brussels 2005
 ESPEN Congress Brussels 2005 Therapeutic endoscopy of pancreatic diseases. How endoscopy may improve nutrition? Myriam Delhaye Therapeutic endoscopy of pancreatic diseases. How endoscopy may improve nutrition?
ESPEN Congress Brussels 2005 Therapeutic endoscopy of pancreatic diseases. How endoscopy may improve nutrition? Myriam Delhaye Therapeutic endoscopy of pancreatic diseases. How endoscopy may improve nutrition?
Chronic pancreatitis is a fibroinflammatory disease of the
 Session 2C: Pancreaticobiliary Disease CHRONIC PANCREATITIS: WHEN TO SCOPE? Gregory A. Coté, MD, MS Chronic pancreatitis is a fibroinflammatory disease of the pancreas that presents with several distinct
Session 2C: Pancreaticobiliary Disease CHRONIC PANCREATITIS: WHEN TO SCOPE? Gregory A. Coté, MD, MS Chronic pancreatitis is a fibroinflammatory disease of the pancreas that presents with several distinct
Title. CitationHepato-Gastroenterology, 61(135): Issue Date Doc URL. Type. File Information. IgG4-Related Sclerosing Cholangitis
: Issue Date Doc URL. Type. File Information. IgG4-Related Sclerosing Cholangitis") Title Difference from Bile Duct Cancer and Relationship be IgG4-Related Sclerosing Cholangitis Kuwatani, Masaki; Kawakami, Hiroshi; Zen, Yoh; Kawak Author(s) Sakamoto, Naoya CitationHepato-Gastroenterology,
Title Difference from Bile Duct Cancer and Relationship be IgG4-Related Sclerosing Cholangitis Kuwatani, Masaki; Kawakami, Hiroshi; Zen, Yoh; Kawak Author(s) Sakamoto, Naoya CitationHepato-Gastroenterology,
5/17/2013. Pancreatic Cancer. Postgraduate Course in General Surgery CASE 1: CASE 1: Overview. Case presentation. Differential diagnosis
 Overview Case presentation Postgraduate Course in General Surgery Differential diagnosis Diagnosis and therapy Eric K. Nakakura Koloa, HI March 26, 2013 Outcomes CASE 1: CASE 1: A 78-year-old man developed
Overview Case presentation Postgraduate Course in General Surgery Differential diagnosis Diagnosis and therapy Eric K. Nakakura Koloa, HI March 26, 2013 Outcomes CASE 1: CASE 1: A 78-year-old man developed
Best of UEG week 2017 (Pancreas-biliary)
") Best of UEG week 2017 (Pancreas-biliary) Marianna Arvanitakis Erasme University Hospital, ULB, Brussels, Belgium 10 th Nottingham Endoscopy Masterclass SPEAKER DECLARATIONS This presenter has the following
Best of UEG week 2017 (Pancreas-biliary) Marianna Arvanitakis Erasme University Hospital, ULB, Brussels, Belgium 10 th Nottingham Endoscopy Masterclass SPEAKER DECLARATIONS This presenter has the following
MM* - RN - TMo - TMi - * Corresponding author
 Open Access Case report Pancreatic pseudocyst with pancreatolithiasis and intracystic hemorrhage treated with distal pancreatectomy: a case report Masato Maeda 1 *, Ryota Nomura 1, Toshiaki Moriki 2 and
Open Access Case report Pancreatic pseudocyst with pancreatolithiasis and intracystic hemorrhage treated with distal pancreatectomy: a case report Masato Maeda 1 *, Ryota Nomura 1, Toshiaki Moriki 2 and