Surgical Aspects of Kidney and Pancreas Transplant. Hannah Choate, MD
|
|
|
- Preston Reed
- 5 years ago
- Views:
Transcription
1 Surgical Aspects of Kidney and Pancreas Transplant Hannah Choate, MD
2 I have no financial disclosures or conflicts of interest
3 Kidney transplantation Indications ESRD or advancing CKD with GFR less than 20 ml/min Projected survival of > 5 years irrespective of kidney disease
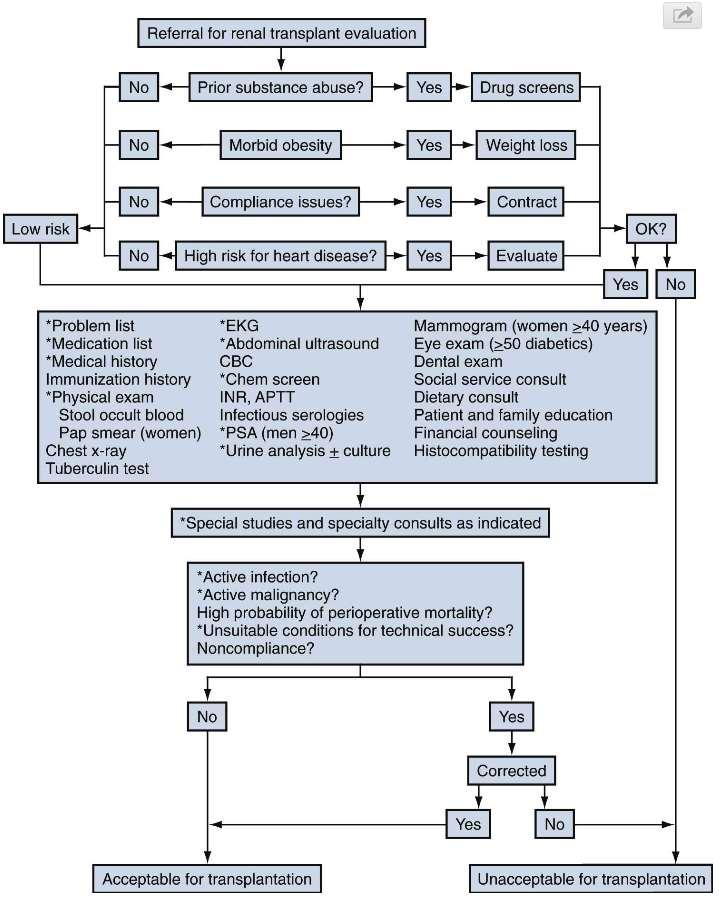
4 Contraindications to Kidney Transplant Active or recent malignancy Reversible renal disease Severe irreversible extra-renal disease Severe functional disability with limited rehabilitation potential Active or recent untreated infection Unmodifiable nonadherence to treatment Psychiatric illness: not remitting with treatment and could affect consent and/or adherence
5
6 Pre-transplant evaluation History Cause of renal disease and pre-esrd treatment Steroids, cytotoxics, immunosuppression Dialysis Duration, modality, access Previous transplants If yes- Induction, complications, compliance, rejection Sensitization Pregnancies, blood transfusions, previous transplants Complete medical history Travel history Exposures to infections, pets/animals Previous surgeries Previous urologic history
7 Pre-transplant evaluation History Medications Anticoagulants, potential interactions with immunosuppressants Allergies Functional status Occupation, exercise tolerance, hobbies Social Smoking, alcohol, drugs, social support Family medical history ESRD, malignancies, CAD
8 Pre-transplant evaluation Physical examination BMI > 40 morbidly obese (Can consider pre-operative bariatric surgery) Vitals Visual and auditory deficits Evaluate for any physical deficits that can impair ability to take medications Heart: murmurs, evidence of heart failure Lungs: Signs of COPD, fluid overload
9 Pre-transplant evaluation Physical examination Abdomen Hepatomegaly, ascites, hernias, bruits, previous incisions Vascular Peripheral pulses, bruits Neurologic Cognitive deficits, sequela of CVA s Cutaneous Skin cancers, infections Musculoskeletal Gait, ability to ambulate, strength, fall risk
10 Pre-transplant evaluation Age and gender appropriate cancer screening Colonoscopy, mammogram, pap smear, PSA Labs CBC, coags, chemistries, LFT s, calcium, phosphorous, PTH UA Infectious disease panel CMV, EBV, VZV, Hepatitis B and C, HIV, PPD (TB Gold), RPR Immunologic profile Imaging ABO, HLA typing, PRA CXR, CT of the abdomen and pelvis or abdominal ultrasound, any additional imaging studies based on patient examination or history
11 Malignancy Recommended wait times Renal cell Incidental: None <5cm : 0-2 years > 5cm : 5 years Prostate : 0-2 years Bladder: 2 years Colorectal/Breast/Uterus/Lung Clinically guided, 2-5 years Melanoma: 5 years
12 Indications for native nephrectomy ADPKD Extending into the pelvis prohibitive of transplant Anorexia/nausea and vomiting/weight loss/recurrent infections or hematuria/pain Suspicious renal mass Obstructing/infected kidney stones Recurrent pyelonephritis Malignant HTN Severe nephrotic syndrome Severe vesicoureteral reflux or hydronephrosis

13 Polycystic kidney disease

14 Polycystic kidney disease
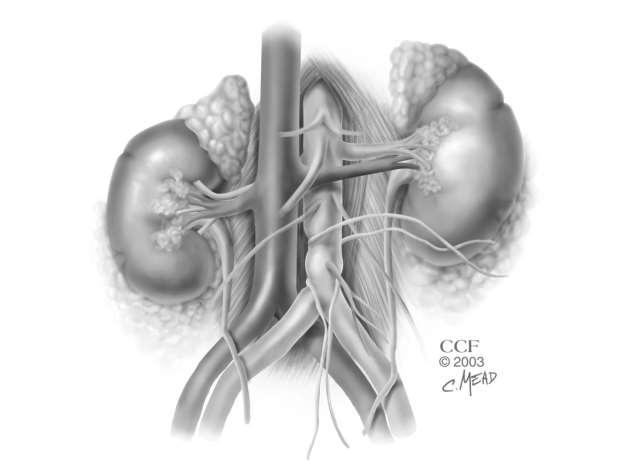
15 Transplant operative technique Backbench preparation of the donor kidney Identification of Renal vein/artery, multiple vessels Reconstruction of the right renal vein to add length using IVC in the setting of a right deceased donor kidney Dissection of the renal artery and vein towards the hilum for mobilization and increased length Ligation of perforating venous branches with silk ties Identification of the ureter Removal of perinephric fat

16 Backbench preparation

17 Backbench preparation

18 Operative technique
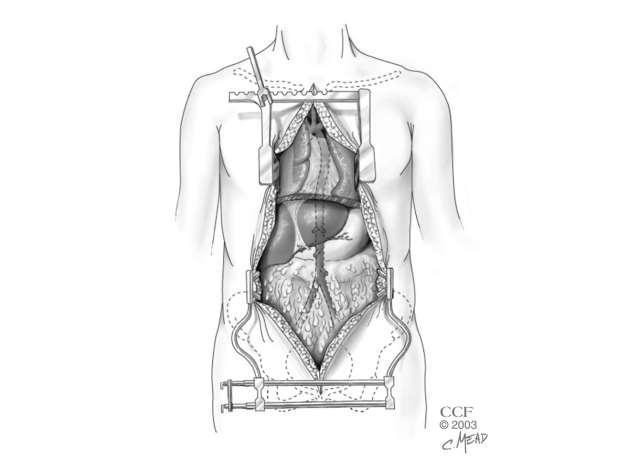
19 Operative technique Gibson (or modified) incision 2cm superior to the pubic symphysis, 2cm medial to the ASIS Retroperitoneal exposure Bookwalter retractor to expose the iliac fossa Dissection of the common/external/internal iliac arteries and vein, depending on the amount of vessel dissection required Vessel loops placed to facilitate clamp placement
20 Operative technique Vascular anastomosis - Venous Typically the vein is performed first -unless the internal iliac artery is used for end to end anastomosis Generally anastomosed end to side to the common, external iliac vein, or IVC Side-biting clamp (Satinsky) placed on the vein Venotomy made with an 11 blade Vessel is irrigated with heparinized saline and venotomy is extended with Potts scissors Running or interrupted, permanent suture (most often 5-0 or 6-0 Prolene) Can apply bulldog clamp but not necessary
21 Operative technique Vascular anastomosis- Arterial Can be performed end to end to the internal iliac artery, or end to side to the common or external iliac artery Proximal and distal clamps applied or may use side-biting arterial clamp Must avoid areas of calcification for clamp placement to avoid lower extremity embolic events Interrupted or running anastomosis with permanent suture, most commonly 5-0 or 6-0 Prolene
22 Operative technique Accessory arteries Upper pole- can ligate if very small, will lose this portion of kidney perfusion, generally a small defect Lower pole- MUST preserve as provides blood supply to the ureter Multiple main renal arteries Can anastomose together on the back table End to side (spatulate smaller artery and anastomose to side of larger artery Side to side (spatulate both arteries and anastomose together Can anastomose separately to the iliac Can keep kidney iced through both anastomoses or can reperfuse the kidney and then anastomose a smaller lower artery Can also anastomose lower artery end to end to inferior epigastric artery
23 Operative technique Reperfusion of the kidney Venous clamp removed first, then the arterial Must inspect perfusion of the kidney, evaluate the venous outflow, inspect for bleeding, and confirm distal arterial pulses May use papaverine externally May inject intra-arterial verapamil

24 Reperfusion

25 Multiple arteries
26 Operative technique Ensure appropriate and adequate flow to the kidney with no immediate vascular complications Ureter is then trimmed and spatulated Bladder is filled with solution, may use methylene blue to aid in identification of the bladder (vs peritoneum)
27 Operative technique Ureteral anastomosis Can be performed in many ways Single layer onlay (running, interrupted) Tunneled with two layers (mucosal followed by second layer of detrusor to tunnel the ureter) Ureteroureterostomy to native ureter only if necessary Stent vs no stent Drain vs no drain Foley left in place for 3-5 days, may require longer duration of foley catheter for more complex anatomy
28 Vascular Complications Kidney Arterial inflow compromise Malpositioning, improper technique, accidental narrowing with anastomosis, inadvertent ligation of multiple vessels Venous outflow compromise Narrowing at the level of the anastomosis, malpositioning of the anastomoses or the kidney renal vein thrombosis Recipient LE compromise from embolic event Clamping calcified artery LE compromise from dissection Clamping calcified artery, dissection at the time of opening the vessel, not including all layers of the arterial wall in the anastomosis Bleeding DVT related to the venous anastomosis

29 Renal vein thrombosis

30 Pancreas Transplantation
31 Indications DM I Very rarely DM II (low insulin requirement, low BMI) Level of renal function determines type of pancreas transplant ESRD main determinant of patient longevity
32 Indications Simultaneous Kidney and Pancreas Transplant (SPK) Approximately 80% of pancreas transplants DM 1 with ESRD or GFR<20 Lifelong immunosuppression for the kidney transplantonly adding surgical risk with pancreas Lower immunologic graft loss than Pancreas After Kidney (PAK) Benefit of concordant nature of rejection (60-70% simultaneous) One operation Shorter wait time than kidney alone Median time to transplant for SPK (SRTR 2016) 16.6 months
33 Indications Pancreas After Kidney (PAK) Approximately 12% of pancreas transplants Patients with labile BG control, previous well-functioning kidney transplant Risk of kidney allograft loss as result of pancreas transplant complications (3-5%) Pancreas transplant can be performed ~3 months after kidney Kidney can be placed on the left if planned previously Median wait time for PAK (SRTR 2016) 18.2 months
34 Indications Isolated pancreas Approximately 8% of all pancreas transplants Brittle DM1 without uremia Uncontrolled, hypoglycemic unawareness, DKA, frequent hospitalizations Adds both surgical risk and risk of lifelong immunosuppression
35 Recipient Evaluation No absolute age (majority <50) Cardiac assessment critical CV disease-majority of waitlist deaths, 30% of recipient deaths Significant lesions present in ~1/3 of patients presenting for pancreas evaluation
36 Recipient Evaluation History and Physical Other complications of DM: limb, vision, GI BMI, hypercoaguable state, anticoagulation Evaluation of vasculature +/- imaging Cancer screening Infectious risk Psychosocial-support, substance abuse history, compliance, financial
37 Donor Evaluation Primary: Age BMI Cause of death Appearance at the time of organ procurement Other factors: Med/Soc history, hemodynamics and lab values, anticipated preservation time
38 Donor Evaluation Donor age-important determinant of graft survival Age thresholds vary <1 % from donors >50 Donor BMI Very few >30-35 used Higher rate of graft failure in overweight donors with death from CVA Death from CVA Worse graft survival
39 Donor Evaluation DMII, pancreatitis, alcoholism, splenectomy not necessarily contraindications Amylase/lipase, insulin administration- minor role Abnormal HbA1c-relative contraindication Trauma to other intra-abdominal organs Social history-risk of transmission of infectious diseases (risk/benefit)
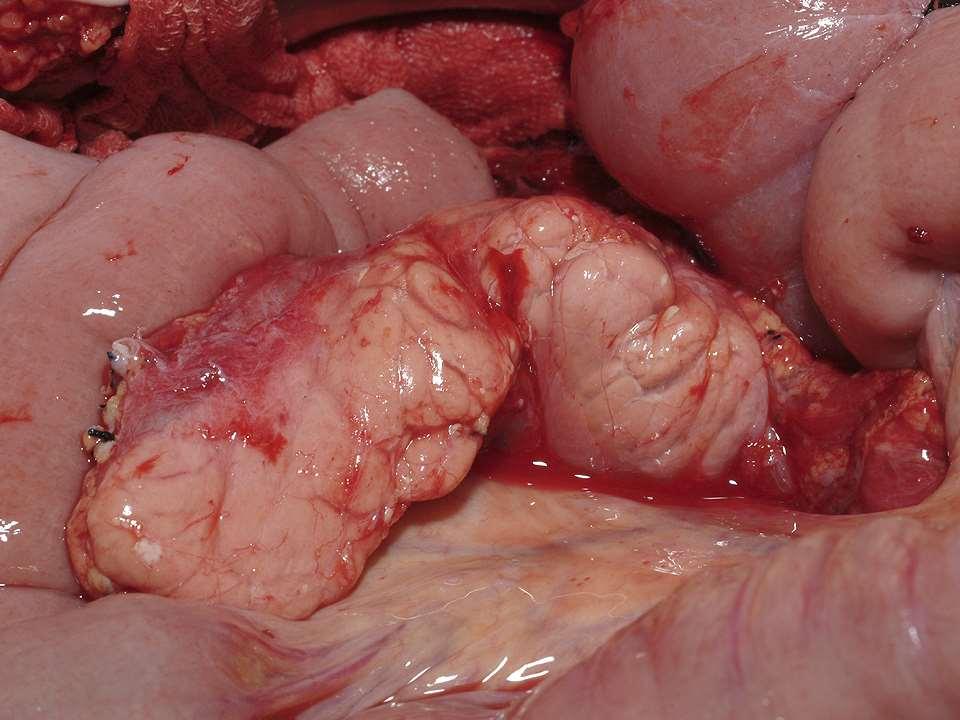
40 Donor Evaluation Intraoperative evaluation-single most important determinant of donor selection Inflammation/fibrosis (firm pancreas) is a contraindication Fatty infiltration Edema Trauma Shorter cold times preferred (>50% of transplants performed in the country with <12 hour CIT)
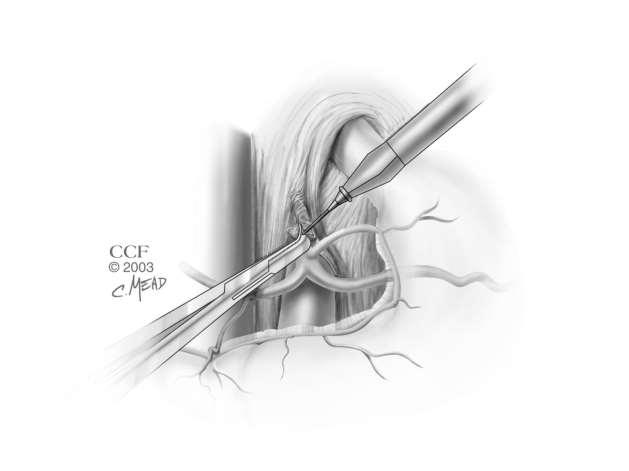
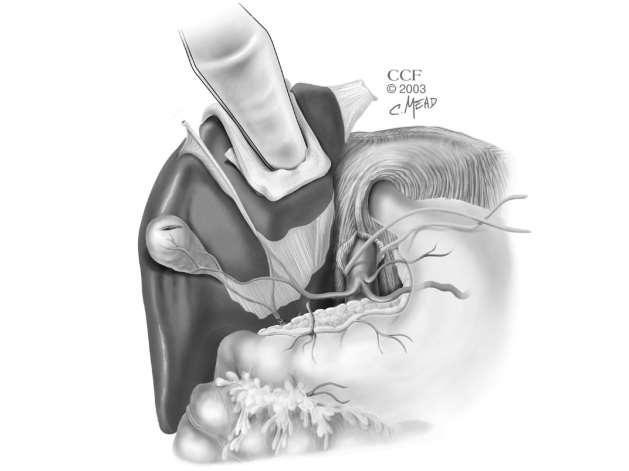
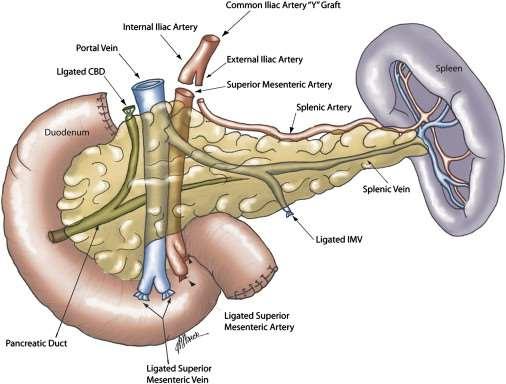
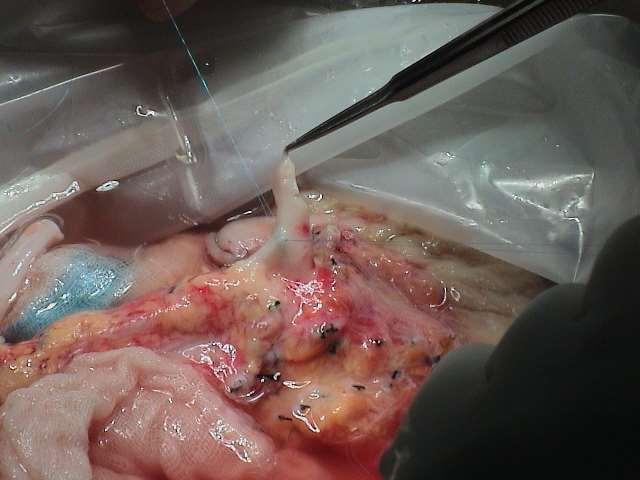
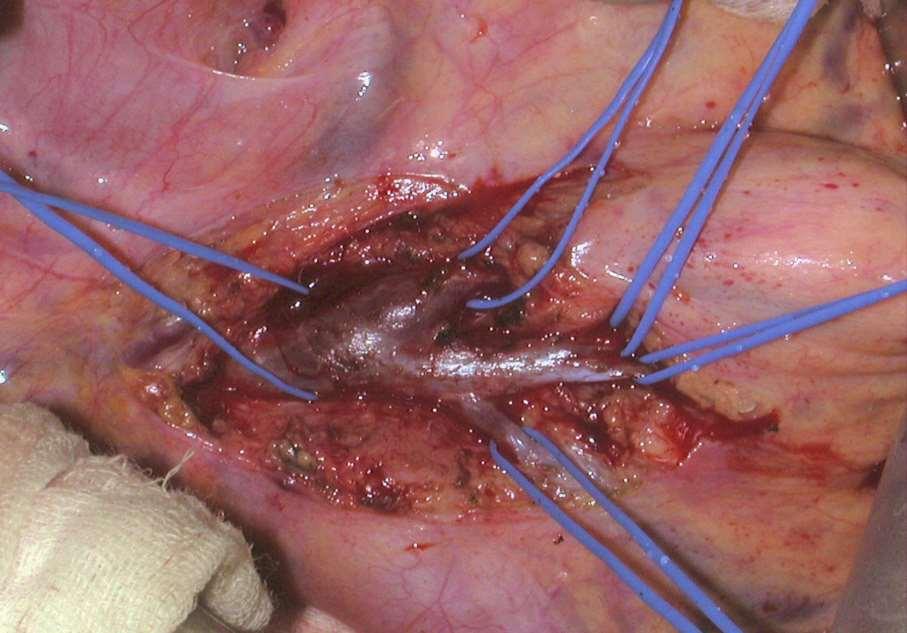
41 Organ Procurement Inspection performed through the lesser sac Majority of the dissection performed in the warm, using the spleen as a handle to minimize manipulation of the pancreas Infrarenal, supraceliac aorta controlled for flushing/crossclamping +/- portal flush via IMV Limit aortic flush Duodenum stapled at the pylorus, then again at the 4 th portion or proximal jejunum
42 Organ Procurement CBD, GDA ligated Portal vein divided halfway between the pancreas and liver (at least 1cm above pancreatic border) Divide splenic artery close to the celiac origin, do not dissect into the pancreas Divide SMA at the aorta. If liver is not being procured, leave SMA and celiac on common aortic cuff Root of the small bowel mesentery stapled >3cm away from head of the pancreas to avoid injury to inferior pancreaticoduodenal arcade Full length of iliac artery (common, internal, external), Iliac vein (in the event of need for portal vein extension)
43 Organ Procurement
44 Organ Procurement
45 Organ Procurement
46 Organ Procurement
47 Organ Procurement
48 Organ Procurement
49 Organ Procurement
50 Organ Procurement
51 Organ Procurement
52

53
54

55

56
57
58
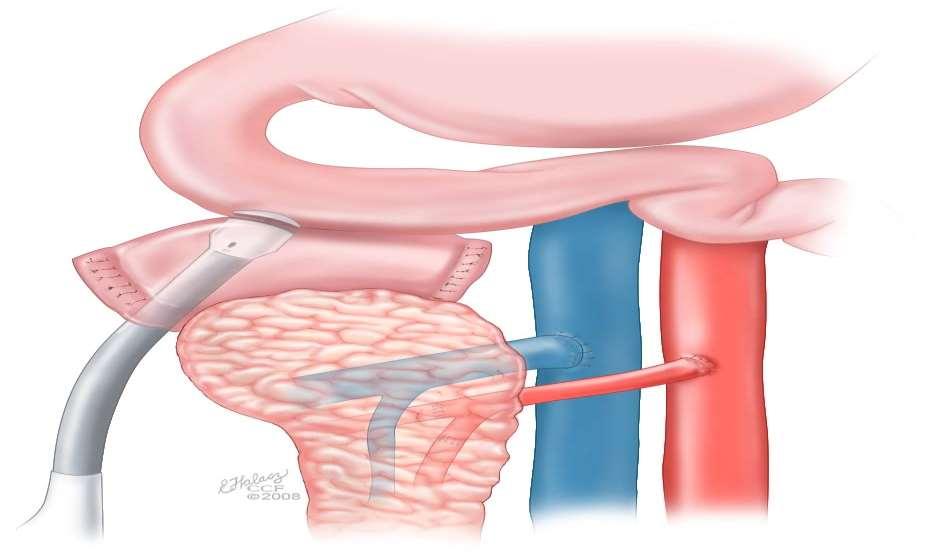
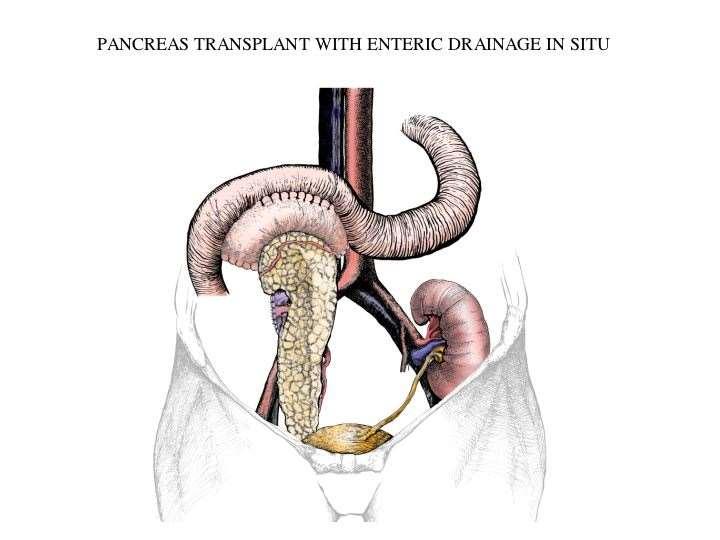
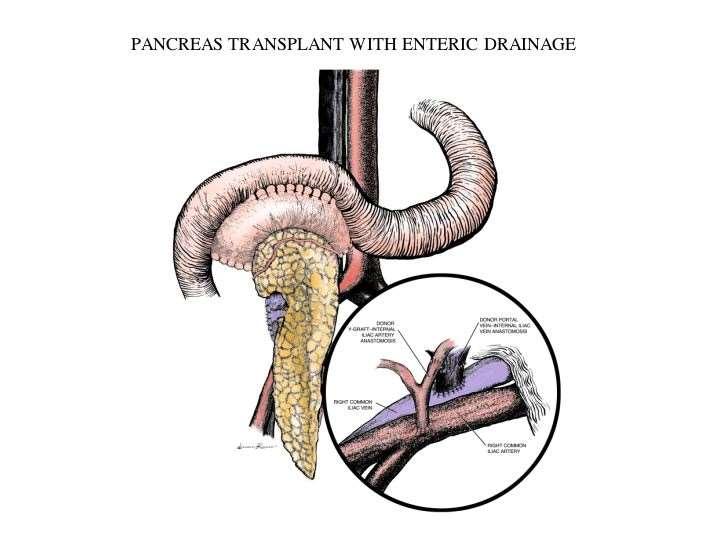
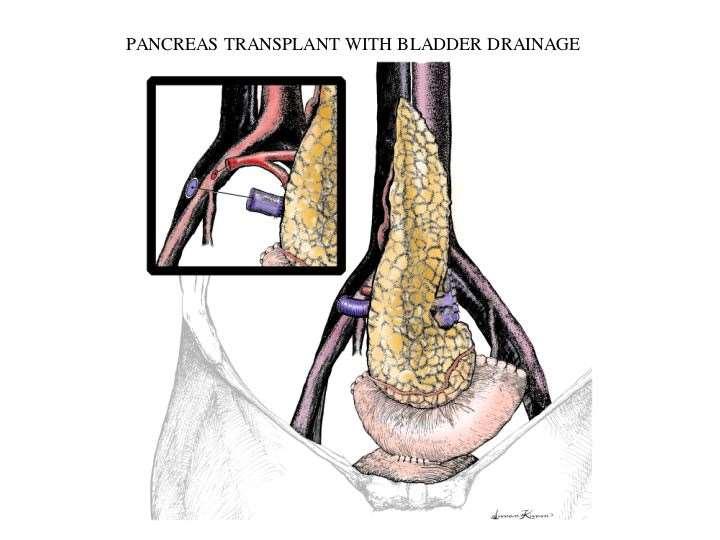
59 Surgical Techniques Exocrine drainage (Donor duodenum) Enteric drainage >80% of all pancreas transplants in the US Donor duodenum anastomosed to recipient jejunum or duodenum More physiologic than bladder drainage Risk of leak Less ability to monitor for rejection Bladder drainage Donor duodenum anastomosed to bladder Allows for better monitoring for rejection No risk of enteric leak/peritonitis Risk of metabolic abnormalities-hyperchloremic metabolic acidosis due to bicarbonate loss in the urine, recurrent UTI, dehydration, cystitis, graft pancreatitis
60
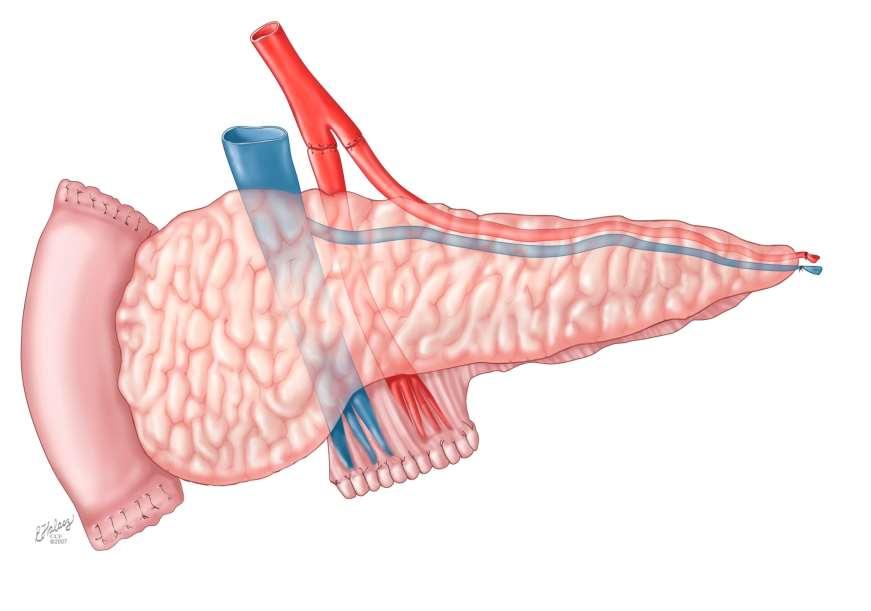
61 Surgical Techniques Venous drainage (Portal vein) Portal vs systemic >90% of pancreas transplants in the US utilize systemic drainage Peripheral hyperinsulinemia with systemic- minimal clinical adverse effects No difference in risk of technical complications or rejection For systemic drainage, the portal vein is typically anastomosed to iliac veins or IVC

62
63

64
65
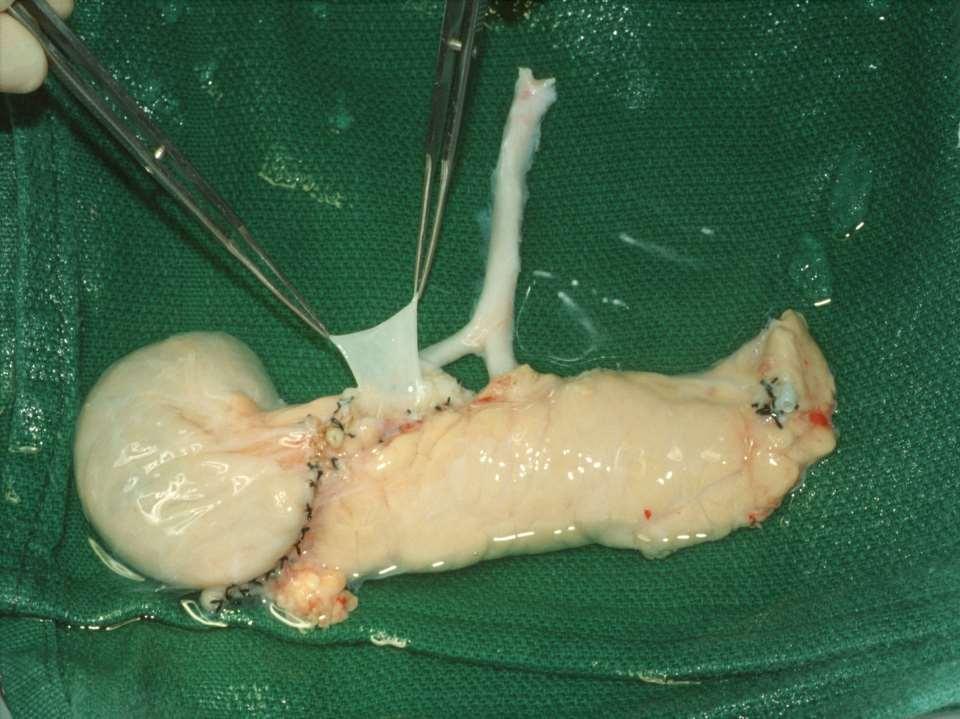
66 Surgical Techniques Arterial supply (SMA, Splenic artery) Most commonly Iliac Y-graft anastomosed end to end on the backtable (External iliac to SMA, Internal Iliac to Splenic) Y-graft typically anastomosed to the right common or external iliac
67 Surgical Techniques
68 Surgical Techniques
69 Surgical Techniques
70 Postoperative course NPO, NGT JP drain x 1 or 2 Foley, stent for SPK Prolonged PACU recovery vs ICU Q1 hour accuchecks first 12 hours NO insulin (BG is evidence of function)
71 Postoperative course Induction with Simulect or Thymoglobulin Maintenance with Prograf, MMF, Prednisone (rapid taper) Length of stay typically dependent upon return of bowel function, average 4-7 days Length of JP drainage dependent upon presence of leak Occasionally require oral hypoglycemics if type II picture
72 Complications Bleeding Enteric complications-bowel leak/intra-abdominal sepsis Ileus/gastroparesis/SBO Pancreatitis Thrombosis
73 Transplant outcomes Significant variation in reporting of graft survival (insulin independence vs continued c peptide production) Early reported pancreas graft losses (SRTR) 8.3% PAK, 9.4 % PTA, 8% SPK Past decade 1, 5 year graft survival SPK 89%, 71% PAK 86%, 65% PA 84%, 58% Estimated half life (50% function) SPK 14 years PAK 7 years PA 7 years 5-year patient survival for pancreas transplants similar between SPK, PAK, PA %

74 Benefits Stabilization/improvement in complications of DM (retinopathy, neuropathy, nephropathy, CAD Restores normal glucagon response from islet alpha cells and symptom recognition of hypoglycemia >50% report significant improvement in quality of life Adding a pancreas transplant to a kidney in a diabetic patient improves survival
75 Survival Benefits SPK-Patient survival significantly higher at 10 years posttransplant compared to deceased donor kidney recipients. SPK with greatest longevity PAK evidence suggests that pancreas transplant improves long-term patient and kidney graft survival rates

76 Questions?
Pancreas and Pancreas-Kidney Transplantation By: Kay R. Brown, CLCP
 Pancreas and Pancreas-Kidney Transplantation By: Kay R. Brown, CLCP Pancreas transplant recipients are usually under age 50. The majority of pancreas transplants are performed on diabetics, who are generally
Pancreas and Pancreas-Kidney Transplantation By: Kay R. Brown, CLCP Pancreas transplant recipients are usually under age 50. The majority of pancreas transplants are performed on diabetics, who are generally
Pancreas Transplantation. Sonia Clarke-Swaby Recipient Kidney/pancreas Transplant Co-ordinator Guy s Hospital
 Pancreas Transplantation Sonia Clarke-Swaby Recipient Kidney/pancreas Transplant Co-ordinator Guy s Hospital Introduction Selection criteria, New innovation Complications, Success rates, Life expectancy
Pancreas Transplantation Sonia Clarke-Swaby Recipient Kidney/pancreas Transplant Co-ordinator Guy s Hospital Introduction Selection criteria, New innovation Complications, Success rates, Life expectancy
DISCHARGE DIAGNOSES: End stage renal disease secondary to rapidly progressive glomerulonephritis.
 DISCHARGE SUMMARY DISCHARGE DIAGNOSES: End stage renal disease secondary to rapidly progressive glomerulonephritis. OPERATIONS/PROCEDURES: Living related renal transplantation. HISTORY: For full details
DISCHARGE SUMMARY DISCHARGE DIAGNOSES: End stage renal disease secondary to rapidly progressive glomerulonephritis. OPERATIONS/PROCEDURES: Living related renal transplantation. HISTORY: For full details
Islet and Pancreas Transplantation
 Islet and Pancreas Transplantation Julie Wardle Specialist Nurse Coordinator Indication for Transplant Treatment option for a select groups of patients with type 1 diabetes Aged 18 years or over Recurrent
Islet and Pancreas Transplantation Julie Wardle Specialist Nurse Coordinator Indication for Transplant Treatment option for a select groups of patients with type 1 diabetes Aged 18 years or over Recurrent
TRANSPLANTATION IN DIABETIC PATIENTS. A.Tarik Kizilisik, MD, MSc, FACS, FICS Director & Primary Transplant Surgeon Lutheran Transplant Center
 TRANSPLANTATION IN DIABETIC PATIENTS A.Tarik Kizilisik, MD, MSc, FACS, FICS Director & Primary Transplant Surgeon Lutheran Transplant Center Diabetes is the pandemic of the new millennium 24 million diabetics
TRANSPLANTATION IN DIABETIC PATIENTS A.Tarik Kizilisik, MD, MSc, FACS, FICS Director & Primary Transplant Surgeon Lutheran Transplant Center Diabetes is the pandemic of the new millennium 24 million diabetics
Overview. Evaluation of Potential Kidney Transplant Recipients. Projected Years of Life in Patients with ESRD
 Evaluation of Potential Kidney Transplant Recipients Donald E. Hricik MD Professor of Medicine and Chief, Division of Nephrology and Hypertension University Hospitals Case Medical Center Conflict of Interest
Evaluation of Potential Kidney Transplant Recipients Donald E. Hricik MD Professor of Medicine and Chief, Division of Nephrology and Hypertension University Hospitals Case Medical Center Conflict of Interest
Renal Transplant Surgery
 Renal Transplant Surgery Mr Somaiah Aroori MS MD EBS in HPB FRCS Consultant HPB & Renal Transplant Surgeon SWTC, Derriford Hospital, Plymouth Over next few minutes Aim to cover Details of Transplant procedure
Renal Transplant Surgery Mr Somaiah Aroori MS MD EBS in HPB FRCS Consultant HPB & Renal Transplant Surgeon SWTC, Derriford Hospital, Plymouth Over next few minutes Aim to cover Details of Transplant procedure
Case Report Transplantation of Horseshoe Kidney from Living, Genetically Unrelated Donor
 Case Reports in Transplantation Volume 2015, Article ID 390381, 4 pages http://dx.doi.org/10.1155/2015/390381 Case Report Transplantation of Horseshoe Kidney from Living, Genetically Unrelated Donor Kazuro
Case Reports in Transplantation Volume 2015, Article ID 390381, 4 pages http://dx.doi.org/10.1155/2015/390381 Case Report Transplantation of Horseshoe Kidney from Living, Genetically Unrelated Donor Kazuro
Pancreas Transplantation
 5 Pancreas Transplantation Abhinav Humar, Khalid O. Khwaja, and David E.R. Sutherland Standard Procedure a) Pretransplant Evaluation b) Surgical Technique c) Postoperative Care d) Results e) Islet Cell
5 Pancreas Transplantation Abhinav Humar, Khalid O. Khwaja, and David E.R. Sutherland Standard Procedure a) Pretransplant Evaluation b) Surgical Technique c) Postoperative Care d) Results e) Islet Cell
The Whipple Operation Illustrations
 The Whipple Operation Illustrations Fig. 1. Illustration of the sixstep pancreaticoduodenectomy (Whipple operation) as described in a number of recent text books by Dr. Evans. The operation is divided
The Whipple Operation Illustrations Fig. 1. Illustration of the sixstep pancreaticoduodenectomy (Whipple operation) as described in a number of recent text books by Dr. Evans. The operation is divided
Records. Adult Kidney Pancreas Transplant Recipient Registration Worksheet. Recipient Information. Provider Information.
 Records Adult Kidney Pancreas Transplant Recipient Registration Worksheet FORM APPROVED: O.M.B. NO. 0915 0157 Expiration Date: 07/31/2020 Note: These worksheets are provided to function as a guide to what
Records Adult Kidney Pancreas Transplant Recipient Registration Worksheet FORM APPROVED: O.M.B. NO. 0915 0157 Expiration Date: 07/31/2020 Note: These worksheets are provided to function as a guide to what
Pediatric Kidney Transplantation
 Pediatric Kidney Transplantation Vikas Dharnidharka, MD, MPH Associate Professor Division of Pediatric Nephrology Conflict of Interest Disclosure Vikas Dharnidharka, MD, MPH Employer: University of Florida
Pediatric Kidney Transplantation Vikas Dharnidharka, MD, MPH Associate Professor Division of Pediatric Nephrology Conflict of Interest Disclosure Vikas Dharnidharka, MD, MPH Employer: University of Florida
Upon completion of the transplant rotation, Residents will understand the basic principles of organ transplantation and immunology.
 Transplantation Rotation Length: 1-2 Months, PGY-4 year Location: University of California at San Francisco, Department of Surgery Primary Supervisor: Ryutaro Hirose, M.D., Associate Program Director Contact
Transplantation Rotation Length: 1-2 Months, PGY-4 year Location: University of California at San Francisco, Department of Surgery Primary Supervisor: Ryutaro Hirose, M.D., Associate Program Director Contact
Pancreas Transplantation From Living Donors: A Single Center Experience of 20 Cases
 American Journal of Transplantation 2016; 16: 2413 2420 Wiley Periodicals Inc. Copyright 2016 The American Society of Transplantation and the American Society of Transplant Surgeons doi: 10.1111/ajt.13738
American Journal of Transplantation 2016; 16: 2413 2420 Wiley Periodicals Inc. Copyright 2016 The American Society of Transplantation and the American Society of Transplant Surgeons doi: 10.1111/ajt.13738
Vascular Remodelling in Pancreas Transplantation
 Vascular Remodelling in Pancreas Transplantation Prof Steve White Consultant HPB/Transplant Surgeon The Freeman Hospital Newcastle President Elect EPITA European Pancreas Transplants Pancreas Transplants
Vascular Remodelling in Pancreas Transplantation Prof Steve White Consultant HPB/Transplant Surgeon The Freeman Hospital Newcastle President Elect EPITA European Pancreas Transplants Pancreas Transplants
Kidney Transplantation
 Kidney Transplantation Current Kidney Transplantation Department of Surgery Yonsei University Wonju College of Medicine Kim Myoung Soo M.D. ysms91@wonju.yonsei.ac.kr http://gs.yonsei.ac.kr Current Kidney
Kidney Transplantation Current Kidney Transplantation Department of Surgery Yonsei University Wonju College of Medicine Kim Myoung Soo M.D. ysms91@wonju.yonsei.ac.kr http://gs.yonsei.ac.kr Current Kidney
Supplementary Online Content
 Supplementary Online Content Smith D, Chudgar A, Daly B, Cooper M. Evaluation of potential renal transplant recipients with computed tomography angiography. Arch Intern Med. doi: 10.1001/archsurg.2012.1466.
Supplementary Online Content Smith D, Chudgar A, Daly B, Cooper M. Evaluation of potential renal transplant recipients with computed tomography angiography. Arch Intern Med. doi: 10.1001/archsurg.2012.1466.
UEMS & EBS: DIVISION OF TRANSPLANT SURGERY
 CURRICULUM AND SYLLABUS TRANSPLANTATION Module 1: Multi-organ retrieval Ability to evaluate donor suitability Ability to retrieve abdominal organs for transplantation Evaluation of donor/ organs suitability
CURRICULUM AND SYLLABUS TRANSPLANTATION Module 1: Multi-organ retrieval Ability to evaluate donor suitability Ability to retrieve abdominal organs for transplantation Evaluation of donor/ organs suitability
Visceral aneurysm. Diagnosis and Interventions M.NEDEVSKA
 Visceral aneurysm Diagnosis and Interventions M.NEDEVSKA History 1953 De Bakeyand Cooley Visceral aneurysm VAAs rare, reported incidence of 0.01 to 0.2% on routine autopsies. Clinically important Potentially
Visceral aneurysm Diagnosis and Interventions M.NEDEVSKA History 1953 De Bakeyand Cooley Visceral aneurysm VAAs rare, reported incidence of 0.01 to 0.2% on routine autopsies. Clinically important Potentially
د. عصام طارق. Objectives:
 GI anatomy Lecture: 5 د. عصام طارق Objectives: To describe anatomy of stomach, duodenum & pancreas. To list their main relations. To define their blood & nerve supply. To list their lymph drainage. To
GI anatomy Lecture: 5 د. عصام طارق Objectives: To describe anatomy of stomach, duodenum & pancreas. To list their main relations. To define their blood & nerve supply. To list their lymph drainage. To
CLINICAL PRESENTATION AND RADIOLOGY QUIZ QUESTION
 Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 6/23/2012 Radiology Quiz of the Week # 78 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 6/23/2012 Radiology Quiz of the Week # 78 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Urologic Surgical Complications In Renal Transplantation
 Urologic Surgical Complications In Renal Transplantation Chris Freise, MD Professor of Surgery UCSF Transplant Division Urologic Complications Review of Bladder Anastomosis Complications and Management
Urologic Surgical Complications In Renal Transplantation Chris Freise, MD Professor of Surgery UCSF Transplant Division Urologic Complications Review of Bladder Anastomosis Complications and Management
Liver Transplantation
 1 Liver Transplantation Department of Surgery Yonsei University Wonju College of Medicine Kim Myoung Soo M.D. ysms91@wonju.yonsei.ac.kr http://gs.yonsei.ac.kr History Development of Liver transplantation
1 Liver Transplantation Department of Surgery Yonsei University Wonju College of Medicine Kim Myoung Soo M.D. ysms91@wonju.yonsei.ac.kr http://gs.yonsei.ac.kr History Development of Liver transplantation
Transplant Surgery. Patient Education Guide to Your Kidney/Pancreas Transplant Page 9-1. For a kidney/pancreas transplant. Before Your Surgery
 Patient Education Page 9-1 Transplant Surgery For a kidney/pancreas transplant By the time you have your transplant surgery, you may have been waiting for some time. Reading this chapter before surgery
Patient Education Page 9-1 Transplant Surgery For a kidney/pancreas transplant By the time you have your transplant surgery, you may have been waiting for some time. Reading this chapter before surgery
Procedure related complications and how to prevent them
 Procedure related complications and how to prevent them Rama Jayanthi, M.D. Section of Urology Nationwide Children s Hospital The Ohio State University Retroperitoneoscopic surgery Inadvertent peritoneal
Procedure related complications and how to prevent them Rama Jayanthi, M.D. Section of Urology Nationwide Children s Hospital The Ohio State University Retroperitoneoscopic surgery Inadvertent peritoneal
When is a child untransplantable?
 When is a child untransplantable? Professor Nizam Mamode Guys and St Thomas Hospital Evelina Children s Hospital Great Ormond Street Hospital Page 2 Median waiting time 286 days v 829 days for adults Upper
When is a child untransplantable? Professor Nizam Mamode Guys and St Thomas Hospital Evelina Children s Hospital Great Ormond Street Hospital Page 2 Median waiting time 286 days v 829 days for adults Upper
JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES
 JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES THE PROBLEM DUODENAL / PANCREATIC INJURIES Difficult to diagnose Not very common Anatomic and physiologic challenges 90% rate of associated
JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES THE PROBLEM DUODENAL / PANCREATIC INJURIES Difficult to diagnose Not very common Anatomic and physiologic challenges 90% rate of associated
Corporate Medical Policy
 Corporate Medical Policy Pancreas Transplant File Name: Origination: Last CAP Review: Next CAP Review: Last Review: pancreas_transplant 1/2000 5/2017 5/2018 8/2017 Description of Procedure or Service Transplantation
Corporate Medical Policy Pancreas Transplant File Name: Origination: Last CAP Review: Next CAP Review: Last Review: pancreas_transplant 1/2000 5/2017 5/2018 8/2017 Description of Procedure or Service Transplantation
For more information about how to cite these materials visit
 Author(s): Silas P. Norman, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author(s): Silas P. Norman, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Abdominal Ultrasound : Aorta, Kidneys, Bladder
 Abdominal Ultrasound : Aorta, Kidneys, Bladder Nilam J. Soni, MD, MSc Associate Professor of Medicine Divisions of Hospital Medicine and Pulmonary/Critical Care Medicine Department of Medicine University
Abdominal Ultrasound : Aorta, Kidneys, Bladder Nilam J. Soni, MD, MSc Associate Professor of Medicine Divisions of Hospital Medicine and Pulmonary/Critical Care Medicine Department of Medicine University
Clinical Policy: Pancreas Transplantation Reference Number: PA.CP.MP.102
 Clinical Policy: Reference Number: PA.CP.MP.102 Effective Date: 01/18 Last Review Date: 03/17 Revision Log Coding Implications Description This policy describes the medical necessity requirements for pancreas
Clinical Policy: Reference Number: PA.CP.MP.102 Effective Date: 01/18 Last Review Date: 03/17 Revision Log Coding Implications Description This policy describes the medical necessity requirements for pancreas
Pancreas Transplantation: A Daring Concept 17 December 1966
 Pancreas Transplantation Pancreas Transplantation: A Daring Concept 17 December 1966 Rutger J. Ploeg, MD PhD Abdominal & Transplant Surgery University Medical Centre Groningen The Netherlands Diabetes
Pancreas Transplantation Pancreas Transplantation: A Daring Concept 17 December 1966 Rutger J. Ploeg, MD PhD Abdominal & Transplant Surgery University Medical Centre Groningen The Netherlands Diabetes
CUAJ Techniques in Urology Techniques: Orthotopic kidney transplantation
 Techniques Orthotopic kidney transplantation in patients with diseased inferior vena cavas E. Chan 1 ; Alp Sener 1,2 ; Vivian C. McAlister 1,2, Patrick P. Luke 1,2 1 Western University Schulich School
Techniques Orthotopic kidney transplantation in patients with diseased inferior vena cavas E. Chan 1 ; Alp Sener 1,2 ; Vivian C. McAlister 1,2, Patrick P. Luke 1,2 1 Western University Schulich School
Bladder Trauma Data Collection Sheet
 Bladder Trauma Data Collection Sheet If there was no traumatic injury with PENETRATION of the bladder DO NOT proceed Date of injury: / / Time of injury: Date of hospital arrival: / / Time of hospital arrival:
Bladder Trauma Data Collection Sheet If there was no traumatic injury with PENETRATION of the bladder DO NOT proceed Date of injury: / / Time of injury: Date of hospital arrival: / / Time of hospital arrival:
UW MEDICINE PATIENT EDUCATION. Benefits and Risks. Of a kidney/pancreas transplant DRAFT. Benefits of a Kidney Transplant
 UW MEDICINE PATIENT EDUCATION Benefits and Risks Of a kidney/pancreas transplant A transplant can greatly improve your life, but it also involves serious risks. This chapter describes the benefits and
UW MEDICINE PATIENT EDUCATION Benefits and Risks Of a kidney/pancreas transplant A transplant can greatly improve your life, but it also involves serious risks. This chapter describes the benefits and
MEDICAL POLICY SUBJECT: KIDNEY TRANSPLANT
 MEDICAL POLICY SUBJECT: KIDNEY TRANSPLANT PAGE: 1 OF: 6 If a product excludes coverage for a service, it is not covered, and medical policy criteria do not apply. If a commercial product, including an
MEDICAL POLICY SUBJECT: KIDNEY TRANSPLANT PAGE: 1 OF: 6 If a product excludes coverage for a service, it is not covered, and medical policy criteria do not apply. If a commercial product, including an
Thanks to our Speakers!
 Thanks to our Speakers! Fizza Naqvi, MD Assistant Professor at the Department of Medicine (Nephrology), Johns Hopkins Attending physician at Johns Hopkins hospital. Involved with kidney recipient evaluation
Thanks to our Speakers! Fizza Naqvi, MD Assistant Professor at the Department of Medicine (Nephrology), Johns Hopkins Attending physician at Johns Hopkins hospital. Involved with kidney recipient evaluation
Renal transplant-recipient surgery
 Surgery Illustrated SURGERY ILLUSTRATED BARRY Renal transplant-recipient surgery John M. Barry Division of Urology and Renal Transplantation, The Oregon Health & Science University, Portland, OR, USA INDICATIONS
Surgery Illustrated SURGERY ILLUSTRATED BARRY Renal transplant-recipient surgery John M. Barry Division of Urology and Renal Transplantation, The Oregon Health & Science University, Portland, OR, USA INDICATIONS
Postoperative monitoring after
 Postoperative monitoring after kidney transplantation Bundit sakulchairungrueng,md Vascular and Transplantation Unit Faculty of Medicine Ramathibodi Hospital Mahidol University Reference Introduction A
Postoperative monitoring after kidney transplantation Bundit sakulchairungrueng,md Vascular and Transplantation Unit Faculty of Medicine Ramathibodi Hospital Mahidol University Reference Introduction A
The jejunum and the Ileum. Prof. Oluwadiya KS
 The jejunum and the Ileum Prof. Oluwadiya KS www.oluwadiya.siteled.com Introduction Introduction The small intestine (SI) comprises of the duodenum, jejunum and the ileum The jejunum is the second part
The jejunum and the Ileum Prof. Oluwadiya KS www.oluwadiya.siteled.com Introduction Introduction The small intestine (SI) comprises of the duodenum, jejunum and the ileum The jejunum is the second part
Prevention of Surgical Injuries in Gynecology
 in Gynecology John K. Chan, M.D. Division of Gynecologic Oncology Overview Review anatomy, etiology, intraoperative, postoperative management, prevention of injuries to: 1. Urinary tract 2. Gastrointestinal
in Gynecology John K. Chan, M.D. Division of Gynecologic Oncology Overview Review anatomy, etiology, intraoperative, postoperative management, prevention of injuries to: 1. Urinary tract 2. Gastrointestinal
CT abdomen and pelvis
 CT abdomen and pelvis General indications: Assessment of vague abdominal symptoms (pain, colics,distenstion,...) Varifecation of a lesion discovered by other diagnostic modalities as US, barium,ivp, Staging
CT abdomen and pelvis General indications: Assessment of vague abdominal symptoms (pain, colics,distenstion,...) Varifecation of a lesion discovered by other diagnostic modalities as US, barium,ivp, Staging
PATIENT SELECTION FOR DECEASED DONOR KIDNEY ONLY TRANSPLANTATION
 PATIENT SELECTION FOR DECEASED DONOR KIDNEY ONLY TRANSPLANTATION This policy has been created by the Kidney Advisory Group on behalf of NHSBT. The policy has been considered and approved by the Organ Donation
PATIENT SELECTION FOR DECEASED DONOR KIDNEY ONLY TRANSPLANTATION This policy has been created by the Kidney Advisory Group on behalf of NHSBT. The policy has been considered and approved by the Organ Donation
Anatomy of the SMALL INTESTINE. Dr. Noman Ullah Wazir PMC
 Anatomy of the SMALL INTESTINE Dr. Noman Ullah Wazir PMC SMALL INTESTINE The small intestine, consists of the duodenum, jejunum, and illium. It extends from the pylorus to the ileocecal junction were the
Anatomy of the SMALL INTESTINE Dr. Noman Ullah Wazir PMC SMALL INTESTINE The small intestine, consists of the duodenum, jejunum, and illium. It extends from the pylorus to the ileocecal junction were the
Abdomen and Retroperitoneum Ultrasound Protocols
 Abdomen and Retroperitoneum Ultrasound Protocols Reviewed By: Anna Ellermeier, MD Last Reviewed: March 2018 Contact: (866) 761-4200, Option 1 **NOTE for all examinations: 1. If documenting possible flow
Abdomen and Retroperitoneum Ultrasound Protocols Reviewed By: Anna Ellermeier, MD Last Reviewed: March 2018 Contact: (866) 761-4200, Option 1 **NOTE for all examinations: 1. If documenting possible flow
The abdominal Esophagus, Stomach and the Duodenum. Prof. Oluwadiya KS
 The abdominal Esophagus, Stomach and the Duodenum Prof. Oluwadiya KS www.oluwadiya.com Viscera of the abdomen Abdominal esophagus: Terminal part of the esophagus The stomach Intestines: Small and Large
The abdominal Esophagus, Stomach and the Duodenum Prof. Oluwadiya KS www.oluwadiya.com Viscera of the abdomen Abdominal esophagus: Terminal part of the esophagus The stomach Intestines: Small and Large
Evaluation Process for Liver Transplant Candidates
 Evaluation Process for Liver Transplant Candidates 2 Objectives Identify components of the liver transplant referral to evaluation Describe the role of the liver transplant coordinator Describe selection
Evaluation Process for Liver Transplant Candidates 2 Objectives Identify components of the liver transplant referral to evaluation Describe the role of the liver transplant coordinator Describe selection
SURGERY, TRANSPLANTATION AND POLYCYSTIC DISEASE. Mr Nick Inston PhD FRCS Consultant Transplant Surgeon Queen Elizabeth Hospital Birmingham
 SURGERY, TRANSPLANTATION AND POLYCYSTIC DISEASE Mr Nick Inston PhD FRCS Consultant Transplant Surgeon Queen Elizabeth Hospital Birmingham What are polycystic kidneys and livers?! Cystic degenerative condition!
SURGERY, TRANSPLANTATION AND POLYCYSTIC DISEASE Mr Nick Inston PhD FRCS Consultant Transplant Surgeon Queen Elizabeth Hospital Birmingham What are polycystic kidneys and livers?! Cystic degenerative condition!
Certified Clinical Transplant Nurse (CCTN) * Detailed Content Outline
 * Detailed Content Outline") I. PRETRANSPLANTATION CARE 9 11 3 23 A. Evaluate End-Stage Organ Failure 1 1 1 3 1. History and physical assessment 2. Vital signs and / or hemodynamic parameters 3. Lab values 4. Diagnostic tests B. Monitor
I. PRETRANSPLANTATION CARE 9 11 3 23 A. Evaluate End-Stage Organ Failure 1 1 1 3 1. History and physical assessment 2. Vital signs and / or hemodynamic parameters 3. Lab values 4. Diagnostic tests B. Monitor
Patient Education Transplant Services. Glossary of Terms. For a kidney/pancreas transplant
 Patient Education Glossary of Terms For a kidney/pancreas transplant Glossary of Terms Page 18-2 Antibody A protein substance made by the body s immune system in response to a foreign substance. Antibodies
Patient Education Glossary of Terms For a kidney/pancreas transplant Glossary of Terms Page 18-2 Antibody A protein substance made by the body s immune system in response to a foreign substance. Antibodies
Surgery. Patient Education Transplant Services. For a kidney/pancreas transplant
 Patient Education Surgery For a kidney/pancreas transplant By the time you have surgery, you may have been waiting for some time. It will help to read this section before surgery so you will know what
Patient Education Surgery For a kidney/pancreas transplant By the time you have surgery, you may have been waiting for some time. It will help to read this section before surgery so you will know what
Transplantation in 2012:
 Transplantation in 2012: Optimizing Outcomes through Seamless Communication Kidney, Pancreas and Islet Breakout Session Kidney Transplantation as a Treatment of Choice for ESRD Uday S. Nori, MD Assistant
Transplantation in 2012: Optimizing Outcomes through Seamless Communication Kidney, Pancreas and Islet Breakout Session Kidney Transplantation as a Treatment of Choice for ESRD Uday S. Nori, MD Assistant
Visceral Artery Aneurysms Endovascular vs. Open?
 Disclosures Visceral Artery Aneurysms Endovascular vs. Open? John S. Lane III, MD Professor and Acting Chief of Vascular Surgery UC San Diego, Department of Surgery None relevant UCSF Vascular Symposium,
Disclosures Visceral Artery Aneurysms Endovascular vs. Open? John S. Lane III, MD Professor and Acting Chief of Vascular Surgery UC San Diego, Department of Surgery None relevant UCSF Vascular Symposium,
Ontario s Referral and Listing Criteria for Adult Pancreas-After- Kidney Transplantation
 Ontario s Referral and Listing Criteria for Adult Pancreas-After- Kidney Transplantation Version 2.0 Trillium Gift of Life Network Adult Pancreas-After-Kidney Transplantation Referral & Listing Criteria
Ontario s Referral and Listing Criteria for Adult Pancreas-After- Kidney Transplantation Version 2.0 Trillium Gift of Life Network Adult Pancreas-After-Kidney Transplantation Referral & Listing Criteria
Ontario s Referral and Listing Criteria for Adult Kidney Transplantation
 Ontario s Referral and Listing Criteria for Adult Kidney Transplantation Version 3.0 Trillium Gift of Life Network Adult Kidney Transplantation Referral & Listing Criteria PATIENT REFERRAL CRITERIA: The
Ontario s Referral and Listing Criteria for Adult Kidney Transplantation Version 3.0 Trillium Gift of Life Network Adult Kidney Transplantation Referral & Listing Criteria PATIENT REFERRAL CRITERIA: The
Pancreas & Biliary System. Dr. Vohra & Dr. Jamila
 Pancreas & Biliary System Dr. Vohra & Dr. Jamila 1 Objectives At the end of the lecture, the student should be able to describe the: Location, surface anatomy, parts, relations & peritoneal reflection
Pancreas & Biliary System Dr. Vohra & Dr. Jamila 1 Objectives At the end of the lecture, the student should be able to describe the: Location, surface anatomy, parts, relations & peritoneal reflection
Patient Education. Transplant Services. Benefits and. Of a kidney/pancreas transplant
 Patient Education Benefits and Risks Of a kidney/pancreas transplant This chapter discusses the benefits as well as the risks of a kidney and/or pancreas transplant. The complications of transplant and
Patient Education Benefits and Risks Of a kidney/pancreas transplant This chapter discusses the benefits as well as the risks of a kidney and/or pancreas transplant. The complications of transplant and
Patient Acknowledgement for Kidney, Pancreas or Kidney-Pancreas Transplant
 Patient Acknowledgement for Kidney, Pancreas or Kidney-Pancreas Transplant This form provides information about having a kidney transplant. It describes the purpose, process, tests, risks, benefits, and
Patient Acknowledgement for Kidney, Pancreas or Kidney-Pancreas Transplant This form provides information about having a kidney transplant. It describes the purpose, process, tests, risks, benefits, and
Definitions. You & Your New Transplant ` 38
 Definitions Acute Short, relatively severe Analgesic Pain medicine Anemia A low number of red blood cells Anesthetic Medication that dulls sensation in order to reduce pain Acute Tubular Necrosis (ATN)
Definitions Acute Short, relatively severe Analgesic Pain medicine Anemia A low number of red blood cells Anesthetic Medication that dulls sensation in order to reduce pain Acute Tubular Necrosis (ATN)
Hybrid Repair of a Complex Thoracoabdominal Aortic Aneurysm
 Hybrid Repair of a Complex Thoracoabdominal Aortic Aneurysm Virendra I. Patel MD MPH Assistant Professor of Surgery Massachusetts General Hospital Division of Vascular and Endovascular Surgery Disclosure
Hybrid Repair of a Complex Thoracoabdominal Aortic Aneurysm Virendra I. Patel MD MPH Assistant Professor of Surgery Massachusetts General Hospital Division of Vascular and Endovascular Surgery Disclosure
Renal transplantation is the preferred treatment method of endstage
 Technical Aspects of Renal Transplantation John M. Barry Renal transplantation is the preferred treatment method of endstage renal disease (ESRD). It is more cost-effective than is maintenance dialysis
Technical Aspects of Renal Transplantation John M. Barry Renal transplantation is the preferred treatment method of endstage renal disease (ESRD). It is more cost-effective than is maintenance dialysis
Vascular Imaging in the Pediatric Abdomen. Jonathan Swanson, MD
 Vascular Imaging in the Pediatric Abdomen Jonathan Swanson, MD Goals and Objectives To understand the imaging approach, appearance, and clinical manifestations of the common pediatric abdominal vascular
Vascular Imaging in the Pediatric Abdomen Jonathan Swanson, MD Goals and Objectives To understand the imaging approach, appearance, and clinical manifestations of the common pediatric abdominal vascular
Kidney Transplant Outcomes In Elderly Patients. Simin Goral MD University of Pennsylvania Medical Center Philadelphia, Pennsylvania
 Kidney Transplant Outcomes In Elderly Patients Simin Goral MD University of Pennsylvania Medical Center Philadelphia, Pennsylvania Case Discussion 70 year old Asian male, neuropsychiatrist, works full
Kidney Transplant Outcomes In Elderly Patients Simin Goral MD University of Pennsylvania Medical Center Philadelphia, Pennsylvania Case Discussion 70 year old Asian male, neuropsychiatrist, works full
Kidney Transplantation
 Kidney Tran nsplantation Historical per rspective and current practice Piyanut Poo otracool, M.D. Departmen nt of Surgery, Ramathibo odi Hospital, Mahidol University Kidney Transplantation DDKT Adult deceased
Kidney Tran nsplantation Historical per rspective and current practice Piyanut Poo otracool, M.D. Departmen nt of Surgery, Ramathibo odi Hospital, Mahidol University Kidney Transplantation DDKT Adult deceased
Allogeneic Pancreas Transplant
 Protocol Allogeneic Pancreas Transplant (70302) Medical Benefit Effective Date: 07/01/14 Next Review Date: 05/15 Preauthorization Yes Review Dates: 09/09, 09/10, 09/11, 07/12, 05/13, 05/14 The following
Protocol Allogeneic Pancreas Transplant (70302) Medical Benefit Effective Date: 07/01/14 Next Review Date: 05/15 Preauthorization Yes Review Dates: 09/09, 09/10, 09/11, 07/12, 05/13, 05/14 The following
ANATOMY OF PELVICAYCEAL SYSTEM -DR. RAHUL BEVARA
 1 ANATOMY OF PELVICAYCEAL SYSTEM -DR. RAHUL BEVARA 2 KIDNEY:ANATOMY OVERVIEW Kidneys are retroperitoneal, in posterior abdominal region, extending from T12 L3 Bean-shaped Right kidney is lower than left
1 ANATOMY OF PELVICAYCEAL SYSTEM -DR. RAHUL BEVARA 2 KIDNEY:ANATOMY OVERVIEW Kidneys are retroperitoneal, in posterior abdominal region, extending from T12 L3 Bean-shaped Right kidney is lower than left
Chapter 4 Section Simultaneous Pancreas-Kidney (SPK), Pancreas-After-Kidney (PAK), And Pancreas-Transplant-Alone (PTA)
, Pancreas-After-Kidney (PAK), And Pancreas-Transplant-Alone (PTA)") Surgery Chapter 4 Section 24.7 Simultaneous Pancreas-Kidney (SPK), Pancreas-After-Kidney (PAK), And Pancreas-Transplant-Alone Issue Date: February 5, 1996 Authority: 32 CFR 199.4(e)(5) 1.0 CPT 1 PROCEDURE
Surgery Chapter 4 Section 24.7 Simultaneous Pancreas-Kidney (SPK), Pancreas-After-Kidney (PAK), And Pancreas-Transplant-Alone Issue Date: February 5, 1996 Authority: 32 CFR 199.4(e)(5) 1.0 CPT 1 PROCEDURE
RPLND: Tips and Tricks
 RPLND: Tips and Tricks Andrew J. Stephenson, MD FACS FRCS(C) Director, Center for Urologic Oncology Glickman Urological & Kidney Institute Cleveland Clinic, Cleveland, OH RPLND: Keys to success Knowledge
RPLND: Tips and Tricks Andrew J. Stephenson, MD FACS FRCS(C) Director, Center for Urologic Oncology Glickman Urological & Kidney Institute Cleveland Clinic, Cleveland, OH RPLND: Keys to success Knowledge
Chronic Kidney Disease (CKD) Stages. CHRONIC KIDNEY DISEASE Treatment Options. Incident counts & adjusted rates, by primary diagnosis Figure 2.
 Stages. CHRONIC KIDNEY DISEASE Treatment Options. Incident counts & adjusted rates, by primary diagnosis Figure 2.") Chronic Kidney Disease (CKD) Stages Stage 1 GFR > 90 (evidence of renal disease) Stage 2 GFR 60-89 Stage 3 GFR 30-59 Stage 4 GFR 15-29 Stage 5 GFR
Chronic Kidney Disease (CKD) Stages Stage 1 GFR > 90 (evidence of renal disease) Stage 2 GFR 60-89 Stage 3 GFR 30-59 Stage 4 GFR 15-29 Stage 5 GFR
Chapter 4 Section 24.7
 Surgery Chapter 4 Section 24.7 Simultaneous Pancreas-Kidney (SPK), Pancreas-After-Kidney (PAK), And Pancreas-Transplant-Alone (PTA), And Pancreatic Islet Cell Transplantation Issue Date: February 5, 1996
Surgery Chapter 4 Section 24.7 Simultaneous Pancreas-Kidney (SPK), Pancreas-After-Kidney (PAK), And Pancreas-Transplant-Alone (PTA), And Pancreatic Islet Cell Transplantation Issue Date: February 5, 1996
Treatment of choice for end stage renal disease Imaging to establish baseline and diagnosis of potential complications Review common surgical
 Treatment of choice for end stage renal disease Imaging to establish baseline and diagnosis of potential complications Review common surgical techniques Review normal appearance Discuss US diagnosis of
Treatment of choice for end stage renal disease Imaging to establish baseline and diagnosis of potential complications Review common surgical techniques Review normal appearance Discuss US diagnosis of
Allogeneic Pancreas Transplant
 Protocol Allogeneic Pancreas Transplant (70302) Medical Benefit Effective Date: 07/01/14 Next Review Date: 05/18 Preauthorization Yes Review Dates: 09/09, 09/10, 09/11, 07/12, 05/13, 05/14, 05/15, 05/16,
Protocol Allogeneic Pancreas Transplant (70302) Medical Benefit Effective Date: 07/01/14 Next Review Date: 05/18 Preauthorization Yes Review Dates: 09/09, 09/10, 09/11, 07/12, 05/13, 05/14, 05/15, 05/16,
Heart Transplant Family Education Class
 Heart Transplant Family Education Class Celebrating 30 years History of Heart Transplantation First successful adult heart transplant in United States- January 6, 1968 First heart transplant at OHSU -
Heart Transplant Family Education Class Celebrating 30 years History of Heart Transplantation First successful adult heart transplant in United States- January 6, 1968 First heart transplant at OHSU -
José Oberholzer, MD. Director Charles O. Strickler Transplant Center. Chief, Division of Transplantation
 José Oberholzer, MD Director Charles O. Strickler Transplant Center Chief, Division of Transplantation Professor of Surgery and Biomedical Engineering DISCLOSURES No consulting for, no payments, no stocks
José Oberholzer, MD Director Charles O. Strickler Transplant Center Chief, Division of Transplantation Professor of Surgery and Biomedical Engineering DISCLOSURES No consulting for, no payments, no stocks
Interventional Radiology in Trauma. Vikash Prasad, MD, FRCPC Vascular and Interventional Radiology The Moncton Hospital
 Interventional Radiology in Trauma Vikash Prasad, MD, FRCPC Vascular and Interventional Radiology The Moncton Hospital Disclosures None relevant to this presentation Shareholder Johnson and Johnson Goal
Interventional Radiology in Trauma Vikash Prasad, MD, FRCPC Vascular and Interventional Radiology The Moncton Hospital Disclosures None relevant to this presentation Shareholder Johnson and Johnson Goal
RENAL SURGERY. Susanne Åkerblom Chief of Surgery Swedish Specialist in Surgery (Small Animal)
") RENAL SURGERY Susanne Åkerblom Chief of Surgery Swedish Specialist in Surgery (Small Animal) ANATOMY The left kidney is generally more mobile than the right The kidney is covered by a thin fibrous capsule
RENAL SURGERY Susanne Åkerblom Chief of Surgery Swedish Specialist in Surgery (Small Animal) ANATOMY The left kidney is generally more mobile than the right The kidney is covered by a thin fibrous capsule
Overall Goals and Objectives for Transplant Hepatology EPAs:
 Overall Goals and Objectives for Transplant Hepatology EPAs: 1. DIAGNOSTIC LIST During the one-year Advanced Pediatric Transplant Hepatology Program, fellows are expected to develop comprehensive skills
Overall Goals and Objectives for Transplant Hepatology EPAs: 1. DIAGNOSTIC LIST During the one-year Advanced Pediatric Transplant Hepatology Program, fellows are expected to develop comprehensive skills
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of robot-assisted kidney transplant A kidney transplant is an effective treatment
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of robot-assisted kidney transplant A kidney transplant is an effective treatment
FIG The inferior and posterior peritoneal reflection is easily
 PSOAS HITCH, BOARI FLAP, AND COMBINATION OF PSOAS 7 HITCH AND BOARI FLAP The psoas hitch procedure, Boari flap, and transureteroureterostomy are useful operative procedures for reestablishing continuity
PSOAS HITCH, BOARI FLAP, AND COMBINATION OF PSOAS 7 HITCH AND BOARI FLAP The psoas hitch procedure, Boari flap, and transureteroureterostomy are useful operative procedures for reestablishing continuity
MEDICAL MANAGEMENT POLICY
 PAGE: 1 of 5 MEDICAL MANAGEMENT POLICY This medical policy is not a guarantee of benefits or coverage, nor should it be deemed as medical advice. In the event of any conflict concerning benefit coverage,
PAGE: 1 of 5 MEDICAL MANAGEMENT POLICY This medical policy is not a guarantee of benefits or coverage, nor should it be deemed as medical advice. In the event of any conflict concerning benefit coverage,
Javier Marquez Graciani, MD Attending Dr F. Joglar
 Javier Marquez Graciani, MD Attending Dr F. Joglar MI is the leading single-organ cause of early and late mortality. Huber and associates- - Multisystem organ failure (MSOF) caused more deaths (57%) than
Javier Marquez Graciani, MD Attending Dr F. Joglar MI is the leading single-organ cause of early and late mortality. Huber and associates- - Multisystem organ failure (MSOF) caused more deaths (57%) than
Diagnosis & Management of Kidney Trauma. LAU - Urology Residency Program LOP Urology Residents Meeting
 Diagnosis & Management of Kidney Trauma LAU - Urology Residency Program LOP Urology Residents Meeting Outline Introduction Investigation Staging Treatment Introduction The kidneys are the most common genitourinary
Diagnosis & Management of Kidney Trauma LAU - Urology Residency Program LOP Urology Residents Meeting Outline Introduction Investigation Staging Treatment Introduction The kidneys are the most common genitourinary
Dr. Zahiri. In the name of God
 Dr. Zahiri In the name of God small intestine = small bowel is the part of the gastrointestinal tract Boundaries: Pylorus Ileosecal junction Function: digestion and absorption of food It receives bile
Dr. Zahiri In the name of God small intestine = small bowel is the part of the gastrointestinal tract Boundaries: Pylorus Ileosecal junction Function: digestion and absorption of food It receives bile
Simultaneous Pancreas Kidney Transplantation:
 Simultaneous Pancreas Kidney Transplantation: What is the added advantage, and for whom? Alexander Wiseman, M.D. Associate Professor, Division of Renal Diseases and Hypertension Medical Director, Kidney
Simultaneous Pancreas Kidney Transplantation: What is the added advantage, and for whom? Alexander Wiseman, M.D. Associate Professor, Division of Renal Diseases and Hypertension Medical Director, Kidney
Successful Application of Supraceliac Aortohepatic Conduit Using Saphenous Venous Graft in Right Lobe Living Donor Liver Transplantation
 LETTERS FROM THE FRONTLINE Successful Application of Supraceliac Aortohepatic Conduit Using Saphenous Venous Graft in Right Lobe Living Donor Liver Transplantation TO THE EDITOR: Hepatic artery (HA) reconstruction
LETTERS FROM THE FRONTLINE Successful Application of Supraceliac Aortohepatic Conduit Using Saphenous Venous Graft in Right Lobe Living Donor Liver Transplantation TO THE EDITOR: Hepatic artery (HA) reconstruction
Eilandjes transplantatie. Eelco de Koning, LUMC 14 februari 2008
 Eilandjes transplantatie Eelco de Koning, LUMC 14 februari 2008 Pancreas or islets? What tissue do we wish to transplant? Is there competition for donor pancreas? How does the islet isolation and transplantation
Eilandjes transplantatie Eelco de Koning, LUMC 14 februari 2008 Pancreas or islets? What tissue do we wish to transplant? Is there competition for donor pancreas? How does the islet isolation and transplantation
Lab Monitor Images Dissection of the Abdominal Vasculature + Lower Digestive System
 Lab Monitor Images Dissection of the Abdominal Vasculature + Lower Digestive System Stomach & Duodenum Frontal (AP) View Nasogastric tube 2 1 3 4 Stomach Pylorus Duodenum 1 Duodenum 2 Duodenum 3 Duodenum
Lab Monitor Images Dissection of the Abdominal Vasculature + Lower Digestive System Stomach & Duodenum Frontal (AP) View Nasogastric tube 2 1 3 4 Stomach Pylorus Duodenum 1 Duodenum 2 Duodenum 3 Duodenum
PANCREAS TRANSPLANTATION WAS first described
 0163-769X/04/$20.00/0 Endocrine Reviews 25(6):919 946 Printed in U.S.A. Copyright 2004 by The Endocrine Society doi: 10.1210/er.2002-0036 Pancreas Transplantation: Indications and Consequences JENNIFER
0163-769X/04/$20.00/0 Endocrine Reviews 25(6):919 946 Printed in U.S.A. Copyright 2004 by The Endocrine Society doi: 10.1210/er.2002-0036 Pancreas Transplantation: Indications and Consequences JENNIFER
Glossary. Anesthesiologist A doctor who puts you or parts of your body to sleep during surgery.
 1-Glossary Glossary Acute rejection A type of rejection that occurs when immune cells from your body attack the transplanted organ(s). Acute rejection may occur at any time after a transplant. But it usually
1-Glossary Glossary Acute rejection A type of rejection that occurs when immune cells from your body attack the transplanted organ(s). Acute rejection may occur at any time after a transplant. But it usually
Johns Hopkins Hospital Comprehensive Transplant Center Informed Consent Form for Thoracic Organ Recipient Evaluation
 Johns Hopkins Hospital Comprehensive Transplant Center Informed Consent Form for Thoracic Organ Recipient Evaluation The decision to undergo transplantation can be extremely difficult and often confusing.
Johns Hopkins Hospital Comprehensive Transplant Center Informed Consent Form for Thoracic Organ Recipient Evaluation The decision to undergo transplantation can be extremely difficult and often confusing.
Diabetes and Kidney Disease: Time to Act. Your Guide to Diabetes and Kidney Disease
 Diabetes and Kidney Disease: Time to Act Your Guide to Diabetes and Kidney Disease Diabetes is fast becoming a world epidemic Diabetes is reaching epidemic proportions worldwide. Every year more people
Diabetes and Kidney Disease: Time to Act Your Guide to Diabetes and Kidney Disease Diabetes is fast becoming a world epidemic Diabetes is reaching epidemic proportions worldwide. Every year more people
Allogeneic Pancreas Transplant
 Allogeneic Pancreas Transplant Policy Number: 7.03.02 Last Review: 8/2014 Origination: 8/2001 Next Review: 8/2015 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for allogeneic
Allogeneic Pancreas Transplant Policy Number: 7.03.02 Last Review: 8/2014 Origination: 8/2001 Next Review: 8/2015 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for allogeneic
Patient Name: MRN: DOB: Treatment Location:
 Page 1 of 5 I. TO (Required) This Section is required to be completed by all patients who undergo kidney transplant surgery. I hereby consent to and authorize Dr. and his/her assistant(s), including supervised
Page 1 of 5 I. TO (Required) This Section is required to be completed by all patients who undergo kidney transplant surgery. I hereby consent to and authorize Dr. and his/her assistant(s), including supervised
Duodenum retroperitoneal
 Duodenum retroperitoneal C shaped Initial region out of stomach into small intestine RETROperitoneal viscus Superior 1 st part duodenal cap ; moves upwards and backwards to lie on the R crura medial to
Duodenum retroperitoneal C shaped Initial region out of stomach into small intestine RETROperitoneal viscus Superior 1 st part duodenal cap ; moves upwards and backwards to lie on the R crura medial to
Pancreas transplants. What you need to know. Information for patients Sheffield Kidney Institute (Renal Unit)
") Pancreas transplants What you need to know Information for patients Sheffield Kidney Institute (Renal Unit) page 2 of 16 What is the pancreas and why is it transplanted? The pancreas is part of the digestive
Pancreas transplants What you need to know Information for patients Sheffield Kidney Institute (Renal Unit) page 2 of 16 What is the pancreas and why is it transplanted? The pancreas is part of the digestive
Case 8038 Renal allograft complicated with renal artery stenosis
 Case 8038 Renal allograft complicated with renal artery stenosis Santiago I, Canelas A, Pinto AP Section: Cardiovascular Published: 2009, Nov. 30 Patient: 61 year(s), male Clinical History A 61-year-old
Case 8038 Renal allograft complicated with renal artery stenosis Santiago I, Canelas A, Pinto AP Section: Cardiovascular Published: 2009, Nov. 30 Patient: 61 year(s), male Clinical History A 61-year-old
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons
 General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: TRANSPLANTATION 7-Nov-2016 DEVELOPED BY: Daryl
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: TRANSPLANTATION 7-Nov-2016 DEVELOPED BY: Daryl