Diagnosis & Management of Kidney Trauma. LAU - Urology Residency Program LOP Urology Residents Meeting
|
|
|
- Theresa Jordan
- 5 years ago
- Views:
Transcription
1 Diagnosis & Management of Kidney Trauma LAU - Urology Residency Program LOP Urology Residents Meeting
2 Outline Introduction Investigation Staging Treatment
3 Introduction The kidneys are the most common genitourinary organs injured from external trauma. 5% of all trauma and 10% of abdominal trauma cases Motor vehicle accidents, falls from heights, and assaults contribute to the majority of blunt renal trauma.
4 Blunt Perhaps the most important information to obtain in the history of the injury is the extent of deceleration involved in high-velocity impact trauma. Retroperitoneal points of fixation such as the renal hilum or UPJ, result in renal artery thrombosis, renal vein disruption, and renal pedicle avulsion.
5 Penetrating Penetrating renal injuries most often come from gunshot and stab wounds. weapon characteristics including caliber and types. Common entry sites including the upper abdomen, flank, and lower chest should alert to possible renal involvement Anterior axillary line hilum Posterior axillary line parenchymal
6 Physical Exam Vital signs Possible renal injury: flank hematoma, abdominal or flank tenderness, rib fractures, and penetrating injuries to the low thorax or flank. Gunshot injuries can be misleading!!!
7 Laboratory Tests Urinalysis Creatinine CBCD and other tests related to trauma
8 Hematuria The degree of hematuria and the severity of the renal injury don t consistently correlate. The presence or absence of hematuria should not be the sole determinant in the assessment of a patient with suspected renal trauma.
9 Hematuria For example, absent in 7% of 420 grade IV renal injuries (Shariat et al, 2008a) 36% of renal vascular injuries from blunt trauma no blood in the urine (Cass, 1989). 50% of injuries to the UPJ no microscopic or gross hematuria.
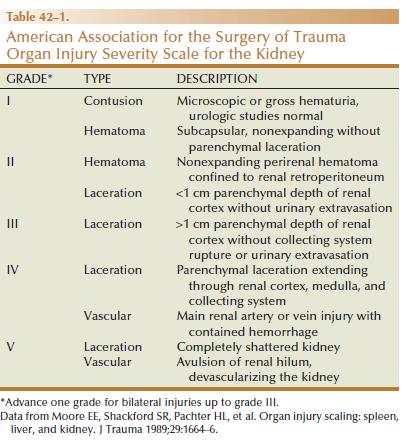
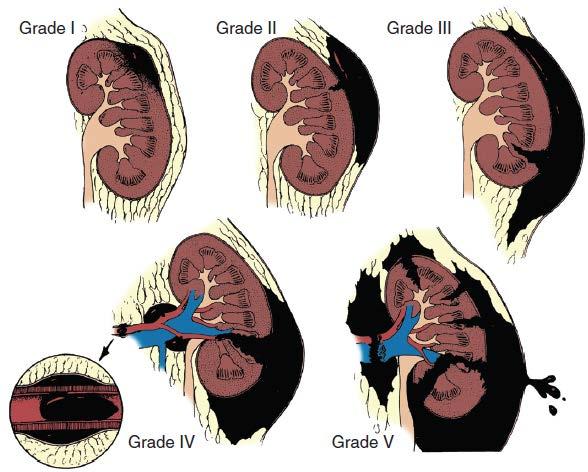
10 Staging To provides maximal guidance for treatment decisions: History (personal + trauma) Physical examination findings Imaging studies
11 Diagnostic Imaging 4-phase CT scan is the gold standard Other modalities: - Ultrasound - IVP/ One-shot Intra-op - MRI - Angiography
12 Indications for Renal Imaging 1. all penetrating trauma patients with a likelihood of renal injury (abdomen, flank, or low chest) who are hemodynamically stable 2. all blunt trauma with significant mechanism of injury, specifically rapid deceleration as would occur in a motor vehicle accident or a fall from heights 3. all blunt trauma with gross hematuria
13 Indications for Renal Imaging 4. all blunt trauma with hypotension defined as a systolic pressure of less than 90 mm Hg at any time during evaluation and resuscitation 5. all pediatric patients with greater than 5 RBCs/HPF
14 Indications for Renal Imaging Patients who are hemodynamically unstable after initial resuscitation require immediate surgical intervention.
15
16
17 Imaging Patients with microscopic hematuria without shock can be observed clinically without imaging studies. these patients rarely have a significant injury. But if high suspicion go for imaging. Penetrating injuries with any degree of hematuria should be imaged.
18 Imaging Technique Contrast-enhanced computed tomography (CT) is the gold standard. Findings on CT that raise suspicion for major injury are: 1. medial hematoma, suggesting vascular injury (may hide an isolated renal vein injury) 2. Medial urinary extravasation, suggesting renal pelvis or UPJ avulsion injury; 3. lack of contrast enhancement of the parenchyma, suggesting arterial injury.

19 Computed tomography scan of a right renal stab wound (grade IV), demonstrating extensive urinary extravasation and large retroperitoneal hematoma
20 IVP Largely replaced by CT, a limited role includes the intraoperative single-shot IVP. single film is taken 10 minutes after intravenous injection (IV push) of 2 ml/kg of contrast material
21 Imaging Ultrasound and Doppler add limited amount of information (hematoma, abdominal fluid ) Arteriography in stable patients diagnostic and therapeutic.

22 Angioembolization of renal laceration: A, Arteriography demonstrating active arterial bleeding. B, Coil embolization used to control bleeding. Note presence of coil and large, triangular area of infarct.
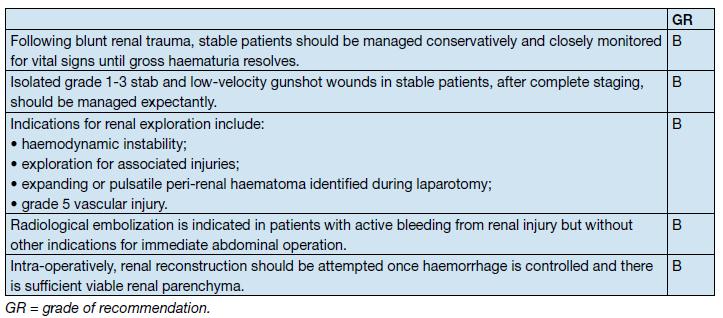
23 Non-operative management Standard of care in stable well-staged patients. I-III non-surgical management IV-V more often require surgical exploration but can be managed non surgically in selected cases especially if no other organ injury. Kidneys heal with conservative management even if high grade injury present. 4/6 grade V kidneys demonstrated satisfactory function after conservative treatment (Altman, 2000).
24 Non-operative management This concept continues into intraop scenarios where the injured kidney demonstrate nonexpanding non-pulsatile hematoma!
25 Non-operative management The management of severe renal lacerations must balance two major issues: the increased incidence of nephrectomy in patients undergoing immediate as opposed to delayed renal exploration the associated morbidity of patients managed expectantly.
26 Non-operative management Serial hematocrit readings. Strict bed rest is mandatory. Urinary extravasation or nonviable parenchyma periodic inpatient imaging, although the authors are aware of no studies to prove it helps in the absence of worrisome symptoms (fever, flank pain, dropping hematocrit).
27 Non-operative management Although most grades II to IV injuries resolve uneventfully, delayed renal bleeding can occur in up to 25% (Wessells et al, 1997). Should bleeding persist or delayed bleeding occur, angiography with selective embolization of bleeding vessels can obviate surgical intervention.
28 Angiography Indications for angiography with embolization therapy: bleeding from a renal segmental artery with or without parenchymal laceration, AVs fistula or pseudoaneurysm, persistent gross hematuria, and/or blood loss exceeding 2 units in 24 hours.
29 Angiography Case reports of renal artery thrombosis treated with stents Main issue in anticoagulation afterwards.
30 Non-operative management Urinary extravasation in solitary injuries can be managed without major intervention and a resolution rate of > 90% If significant urinary extravasation persists, placement of an internal ureteral stent for drainage often prevents prolongation of the extravasation and decreases the chance of perirenal urinoma formation + broad spectrum antibiotics
31 Non-operative management Unilateral main arterial injuries will normally be managed non-operatively in a hemodynamically stable patient Surgical repair reserved for bilateral artery injuries or injuries involving a solitary functional kidney
32 Flow chart for adult renal injuries to serve as a guide for decision making.
33 Operative Management Absolute indications include 1. hemodynamic instability with shock; 2. expanding/pulsatile renal hematoma (usually indicating renal artery avulsion) > 3.5 cm; 3. suspected renal pedicle avulsion (grade 5); 4. ureteropelvic junction disruption. Relative indications are now rare: urinary extravasation together with nonviable tissue renal injury together with colon/pancreatic injury, and a delayed diagnosis of arterial injury (which most likely will need delayed nephrectomy).
34 Operative Management Should nonviable tissue constitute more than 25% in association with a parenchymal laceration or urinary extravasation or both the potential for complications greatly increases and operative management is recommended (Alsikafi et al, 2006).
35 Operative Management If findings are not normal on intra-op IVP, renal exploration provides the opportunity to complete the staging process and reconstruct a significant injury.
36 Operative Management Renal Exploration Transabdominal approach allows complete inspection of intra-abdominal organs and bowel. Obtaining early vascular control before opening Gerota fascia can decrease renal loss: in a comparative series, the total nephrectomy rate was reduced from 56% to 18% (McAninch and Carroll, 1982).

37 The surgical approach to the renal vessels and kidney. A, Retroperitoneal incision over the aorta medial to the inferior mesenteric vein. B, Anatomic relationships of the renal vessels. C, Retroperitoneal incision lateral to the colon, exposing the kidney.
38 Treatment
39 Operative Management Renal Reconstruction The principles of renal reconstruction after trauma include: complete renal exposure, measures for temporary vascular control, debridement of nonviable tissue, hemostasis by individual suture ligation of bleeding vessels, watertight closure of the collecting system if possible, coverage or reapproximation of the parenchymal defect, and judicious use of drains

40 Operative Management Renal Reconstruction Technique for partial nephrectomy: A, total renal exposure; B, sharp removal of nonviable tissue; C, hemostasis obtained and collecting system closed; D, defect covered.

41 Operative Management Renal Reconstruction Technique for renorrhaphy: A, typical injury in midportion of kidney; B, debridement, hemostasis, and collecting system closure; C, approximation of parenchymal margins; D, sutures tied over gelatin sponge bolster.
42 Renovascular Injuries. For major renovascular injuries, speedy nephrectomy is advocated. In rare instances where repair is possible, renal salvage rates are low, (33% for main renal artery reconstruction even in the most expert of hands)(elliott et al, 2007). With delayed diagnosis (>8 hours), the kidney typically cannot be salvaged

43 Vascular injuries. Left, Venous injuries may occur in the main renal vein or the segmental branches. Middle, Repair of main renal vein. Right, Ligation of segmental branch can be done safely.
44 Renovascular Injuries. Main renal artery thrombosis from blunt trauma occurs secondary to deceleration injuries (stretch injury with intimal tear). Outcomes for salvage remain dismally low and nephrectomy is almost always required. When repair is attempted excision with graft. Promising endovascular techniques but anticoagulation remains an issue.

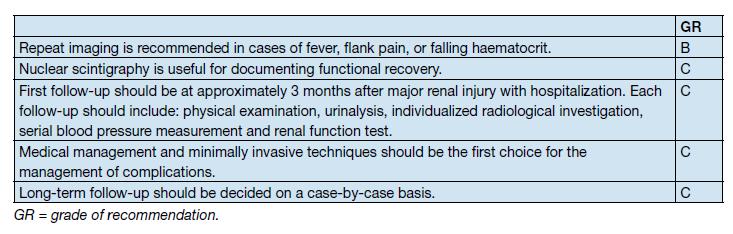
45 A, Movement of the kidney from blunt trauma (deceleration injury) causes stretch on the renal artery, resulting in rupture of the arterial intima and formation of a thrombus.

46 B, Computed tomography of a left kidney with renal artery thrombosis, demonstrating lack of contrast material perfusion to the kidney. C, Arteriography demonstrating complete occlusion of the left renal artery secondary to thrombus formation.
47 Renovascular Injuries. Segmental renal arterial injuries result in ischemic infarction to a segment of the kidney. These should be observed nonoperatively when diagnosed unless associated with a parenchymal laceration with infarction be greater than 20% of the parenchyma careful consideration should be given to endovascular embolization or surgical correction.
48 Operative Management Segmental renal artery injury Concerns include delayed bleeding and urinoma formation. A recent series demonstrated excellent outcomes with only 1 of 18 (6%) patients requiring subsequent intervention during conservative management of segmental renal artery injuries (Elliott et al, 2007).
49 Damage Control Coburn (2002) has noted the benefit of damage control to improve renal salvage. The wound and area around the injured kidney are packed with laparotomy pads to control bleeding with a planned return in 24 hours to explore and evaluate the extent of injury. This approach is commonly used by trauma surgeons in patients with extensive injuries and has long been used by general surgeons. It may well be useful in managing complex renal injuries to avoid total nephrectomy.
50 Complications Early complications (<1 month): bleeding, infection, perinephric abscess, sepsis, urinary fistula, hypertension, urinary extravasation and urinoma Delayed complications include bleeding, calculus formation, chronic pyelonephritis, hypertension, AVF, hydronephrosis and pseudoaneurysms
51 Complications Delayed renal bleeding can occur up to several weeks after injury but usually occurs within 21 days bed rest and hydration +/- embolization Perinephric abscess (rare) drain Hypertension ( injury, compression, AV fistula (Renin-angiotensin))
52 Follow-up The risk of complications in patients who have been treated conservatively increases with grade. Repeat imaging 2-4 days after trauma minimizes the risk of missed complications, especially in grade 3-5 blunt injuries CT scans should always be performed on patients with fever, unexplained decreasing hematocrit or significant flank pain
53 Treatment
54 Summary Expectant management strategies of renal trauma allow for maximal renal preservation. The degree of hematuria and the severity of renal injury do not consistently correlate. Contrast-enhanced computed tomography (CT) is the gold standard for genitourinary imaging in renal trauma. Patients with microscopic hematuria without shock can be observed clinically without imaging studies. Hemodynamically stable, well-staged renal injuries should be conservatively managed (even with severe, high-grade injuries).
55 Summary Selective embolization provides an effective and minimally invasive means to stop active bleeding from parenchymal lacerations and segmental arterial injury. CT findings suspicious for major injury include (1) medial hematoma (vascular injury); (2) medial urinary extravasation (renal pelvis or ureteropelvic junction injury); and (3) lack of contrast enhancement of the parenchyma (arterial injury). Intraoperative one-shot IVP confirms the presence of a contralateral functioning kidney. Early vascular control before opening Gerota fascia can decrease renal loss.
56 Thank you! (questions?)
Question 2. What percentage of abdominal trauma involve the kidney? a) 5 % b) 10% c) 15 % d) 20 %
 5 % b) 10% c) 15 % d) 20 %") Quiz Question 1 After injecting 2ml/kg of contrast for a patient needing a single-shot IVP before kidney exploration, What is the best turnaround time to take the X-ray? a) 3 minutes b) 5 minutes c) 10
Quiz Question 1 After injecting 2ml/kg of contrast for a patient needing a single-shot IVP before kidney exploration, What is the best turnaround time to take the X-ray? a) 3 minutes b) 5 minutes c) 10
Canadian Undergraduate Urology Curriculum (CanUUC): Genitourinary Trauma. Last reviewed June 2014
: Genitourinary Trauma. Last reviewed June 2014") Canadian Undergraduate Urology Curriculum (CanUUC): Genitourinary Trauma Last reviewed June 2014 Session Objectives 1. Recognize hematuria as the cardinal symptom of urinary tract trauma. 1. Outline the
Canadian Undergraduate Urology Curriculum (CanUUC): Genitourinary Trauma Last reviewed June 2014 Session Objectives 1. Recognize hematuria as the cardinal symptom of urinary tract trauma. 1. Outline the
UBC Department of Urologic Sciences Lecture Series. Urological Trauma
 UBC Department of Urologic Sciences Lecture Series Urological Trauma Disclaimer: This is a lot of information to cover and we are unlikely to cover it all today These slides are to be utilized for your
UBC Department of Urologic Sciences Lecture Series Urological Trauma Disclaimer: This is a lot of information to cover and we are unlikely to cover it all today These slides are to be utilized for your
Role of imaging in evaluation of genitourinary i trauma Spectrum of GU injuries Relevance of imaging findings in determining management Focus on MDCT
 Genitourinary Tract Injuries 6 th Nordic Course Scott D. Steenburg, MD Assistant Professor University of Maryland Department of Radiology Division of Trauma and Emergency Radiology R Adams Cowley Shock
Genitourinary Tract Injuries 6 th Nordic Course Scott D. Steenburg, MD Assistant Professor University of Maryland Department of Radiology Division of Trauma and Emergency Radiology R Adams Cowley Shock
Genitourinary Trauma Introduction GU Trauma overlooked
 Genitourinary Trauma Introduction GU Trauma overlooked 10-20% of all injured patients Long term morbidity Impotence Incontinence Life-threatening injuries first Urethral Injury Plan Bladder Injury Kidney
Genitourinary Trauma Introduction GU Trauma overlooked 10-20% of all injured patients Long term morbidity Impotence Incontinence Life-threatening injuries first Urethral Injury Plan Bladder Injury Kidney
Guidelines on Urological Trauma
 Guidelines on Urological Trauma D. Lynch, L. Martinez-Piñeiro, E. Plas, E. Serafetinidis, L. Turkeri, R. Santucci, M. Hohenfellner European Association of Urology 2006 TABLE OF CONTENTS PAGE 1. RENAL TRAUMA
Guidelines on Urological Trauma D. Lynch, L. Martinez-Piñeiro, E. Plas, E. Serafetinidis, L. Turkeri, R. Santucci, M. Hohenfellner European Association of Urology 2006 TABLE OF CONTENTS PAGE 1. RENAL TRAUMA
Bladder Trauma Data Collection Sheet
 Bladder Trauma Data Collection Sheet If there was no traumatic injury with PENETRATION of the bladder DO NOT proceed Date of injury: / / Time of injury: Date of hospital arrival: / / Time of hospital arrival:
Bladder Trauma Data Collection Sheet If there was no traumatic injury with PENETRATION of the bladder DO NOT proceed Date of injury: / / Time of injury: Date of hospital arrival: / / Time of hospital arrival:
Traumatic Renocaval Fistula With Pseudoaneurysm Leading To Renal Atrophy
 ISPUB.COM The Internet Journal of Radiology Volume 6 Number 2 Traumatic Renocaval Fistula With Pseudoaneurysm Leading To Renal Atrophy M Kukkady, A Deena, S Raj, Ramachandra Citation M Kukkady, A Deena,
ISPUB.COM The Internet Journal of Radiology Volume 6 Number 2 Traumatic Renocaval Fistula With Pseudoaneurysm Leading To Renal Atrophy M Kukkady, A Deena, S Raj, Ramachandra Citation M Kukkady, A Deena,
Guidelines on Urological Trauma
 Guidelines on Urological Trauma N. Djakovic, E. Plas, L. Martínez-Piñeiro, Th. Lynch, Y. Mor, R.A. Santucci, E. Serafetinidis, L.N. Turkeri, M. Hohenfellner European Association of Urology 2012 TABLE OF
Guidelines on Urological Trauma N. Djakovic, E. Plas, L. Martínez-Piñeiro, Th. Lynch, Y. Mor, R.A. Santucci, E. Serafetinidis, L.N. Turkeri, M. Hohenfellner European Association of Urology 2012 TABLE OF
Conservative Management of Renal Trauma: Ten Years Experience Reem Al-Bareeq MRCSI, CABU* Kadem Zabar CABS** Mohammed Al-Tantawi CABS***
 Bahrain Medical Bulletin, Vol. 28, No. 3, September 2006 Conservative Management of Renal Trauma: Ten Years Experience Reem Al-Bareeq MRCSI, CABU* Kadem Zabar CABS** Mohammed Al-Tantawi CABS*** Objective:
Bahrain Medical Bulletin, Vol. 28, No. 3, September 2006 Conservative Management of Renal Trauma: Ten Years Experience Reem Al-Bareeq MRCSI, CABU* Kadem Zabar CABS** Mohammed Al-Tantawi CABS*** Objective:
UROLOGIC TRAUMA. Urology Division, Surgery Department Medical Faculty, University of Sumatera Utara
 UROLOGIC TRAUMA Urology Division, Surgery Department Medical Faculty, University of Sumatera Utara UROLOGIC TRAUMA Renal trauma Ureteral injury Bladder injury Urethral injury Injury to external genitalia
UROLOGIC TRAUMA Urology Division, Surgery Department Medical Faculty, University of Sumatera Utara UROLOGIC TRAUMA Renal trauma Ureteral injury Bladder injury Urethral injury Injury to external genitalia
ORIGINAL ARTICLE. Complications Following Renal Trauma
 ORIGINAL ARTICLE Complications Following Renal Trauma Margaret Starnes, MD; Demetrios Demetriades, MD, PhD; Pantelis Hadjizacharia, MD; Kenji Inaba, MD; Charles Best, MD; Linda Chan, PhD Objectives: To
ORIGINAL ARTICLE Complications Following Renal Trauma Margaret Starnes, MD; Demetrios Demetriades, MD, PhD; Pantelis Hadjizacharia, MD; Kenji Inaba, MD; Charles Best, MD; Linda Chan, PhD Objectives: To
2. Blunt abdominal Trauma
 Abdominal Trauma 1. Evaluation and management depends on: a. Mechanism (Blunt versus Penetrating) b. Injury complex in addition to abdomen c. Haemodynamic stability assessment: i. Classically patient s
Abdominal Trauma 1. Evaluation and management depends on: a. Mechanism (Blunt versus Penetrating) b. Injury complex in addition to abdomen c. Haemodynamic stability assessment: i. Classically patient s
Urogenital Injuries The role of radiology
 Urogenital Injuries The role of radiology NORDTER 7 th Nordic Trauma Radiology Course Helsinki, Finland May 21-24, 2012 Johann Baptist Dormagen, MD, PhD Oslo University Hospital, Norway Kidney injuries
Urogenital Injuries The role of radiology NORDTER 7 th Nordic Trauma Radiology Course Helsinki, Finland May 21-24, 2012 Johann Baptist Dormagen, MD, PhD Oslo University Hospital, Norway Kidney injuries
Interventional Radiology in Trauma. Vikash Prasad, MD, FRCPC Vascular and Interventional Radiology The Moncton Hospital
 Interventional Radiology in Trauma Vikash Prasad, MD, FRCPC Vascular and Interventional Radiology The Moncton Hospital Disclosures None relevant to this presentation Shareholder Johnson and Johnson Goal
Interventional Radiology in Trauma Vikash Prasad, MD, FRCPC Vascular and Interventional Radiology The Moncton Hospital Disclosures None relevant to this presentation Shareholder Johnson and Johnson Goal
University of Cape Town
 The copyright of this thesis vests in the author. No quotation from it or information derived from it is to be published without full acknowledgement of the source. The thesis is to be used for private
The copyright of this thesis vests in the author. No quotation from it or information derived from it is to be published without full acknowledgement of the source. The thesis is to be used for private
Medical - Clinical Research & Reviews
 Research Article Research Article Medical - Clinical Research & Reviews ISSN 2575-6087 Management of Kidney in Saiful Anwar General Hospital Malang Indonesia Besut Daryanto, I Made Udiyana Indradiputra,
Research Article Research Article Medical - Clinical Research & Reviews ISSN 2575-6087 Management of Kidney in Saiful Anwar General Hospital Malang Indonesia Besut Daryanto, I Made Udiyana Indradiputra,
ISPUB.COM. Traumatic Uretero-Pelvic Junction Disruption. G Kraushaar, S Harder, K Visvanathan INTRODUCTION CASE REPORT
 ISPUB.COM The Internet Journal of Radiology Volume 4 Number 1 Traumatic Uretero-Pelvic Junction Disruption G Kraushaar, S Harder, K Visvanathan Citation G Kraushaar, S Harder, K Visvanathan. Traumatic
ISPUB.COM The Internet Journal of Radiology Volume 4 Number 1 Traumatic Uretero-Pelvic Junction Disruption G Kraushaar, S Harder, K Visvanathan Citation G Kraushaar, S Harder, K Visvanathan. Traumatic
MDCT Findings of Renal Trauma
 MDT of Renal Trauma Genitourinary Imaging Pictorial Essay Downloaded from www.ajronline.org by 148.251.232.83 on 04/06/18 from IP address 148.251.232.83. opyright RRS. For personal use only; all rights
MDT of Renal Trauma Genitourinary Imaging Pictorial Essay Downloaded from www.ajronline.org by 148.251.232.83 on 04/06/18 from IP address 148.251.232.83. opyright RRS. For personal use only; all rights
Role of Imaging in the evaluation of Renal Trauma
 Role of Imaging in the evaluation of Renal Trauma M. H. Ather,M.A. Noor ( Department of Surgery, The Aga Khan University, Karachi. ) Trauma is the leading cause of morbidity and mortality among young adults
Role of Imaging in the evaluation of Renal Trauma M. H. Ather,M.A. Noor ( Department of Surgery, The Aga Khan University, Karachi. ) Trauma is the leading cause of morbidity and mortality among young adults
Penetrating abdominal trauma clinical view. Ari Leppäniemi, MD Department of Abdominal Surgery Meilahti hospital University of Helsinki Finland
 Penetrating abdominal trauma clinical view Ari Leppäniemi, MD Department of Abdominal Surgery Meilahti hospital University of Helsinki Finland Meilahti hospital - one of Helsinki University hospitals -
Penetrating abdominal trauma clinical view Ari Leppäniemi, MD Department of Abdominal Surgery Meilahti hospital University of Helsinki Finland Meilahti hospital - one of Helsinki University hospitals -
Evaluation and management of renal injuries: consensus statement of the renal trauma subcommittee
 Miscellaneous RENAL TRAUMA CONSENSUS STATEMENT R.A. SANTUCCI ET AL. The first in this series of five papers concerns the evaluation and management of renal injuries. The authors of this paper come from
Miscellaneous RENAL TRAUMA CONSENSUS STATEMENT R.A. SANTUCCI ET AL. The first in this series of five papers concerns the evaluation and management of renal injuries. The authors of this paper come from
Nonoperative Management of Grade 5 Renal Injury in Children: Does It Have a Place?
 EUROPEAN UROLOGY 57 (2010) 154 163 available at www.sciencedirect.com journal homepage: www.europeanurology.com Pediatric Urology Nonoperative Management of Grade 5 Renal Injury in Children: Does It Have
EUROPEAN UROLOGY 57 (2010) 154 163 available at www.sciencedirect.com journal homepage: www.europeanurology.com Pediatric Urology Nonoperative Management of Grade 5 Renal Injury in Children: Does It Have
Management of Blunt Renal Trauma in Srinagarind Hospital: 10-Year Experience
 Management of Blunt Renal Trauma in Srinagarind Hospital: 10-Year Experience Chaiyut Thanapaisal MD*, Wichien Sirithanaphol MD* * Department of Surgery, Faculty of Medicine, Khon Kaen University, Khon
Management of Blunt Renal Trauma in Srinagarind Hospital: 10-Year Experience Chaiyut Thanapaisal MD*, Wichien Sirithanaphol MD* * Department of Surgery, Faculty of Medicine, Khon Kaen University, Khon
Renal injury occurs in up to 1.2% of trauma cases in the
 Renal Arterial Injuries: A Single Center Analysis of Management Strategies and Outcomes Sean P. Elliott, Ephrem O. Olweny and Jack W. McAninch* From the Department of Urologic Surgery, University of Minnesota,
Renal Arterial Injuries: A Single Center Analysis of Management Strategies and Outcomes Sean P. Elliott, Ephrem O. Olweny and Jack W. McAninch* From the Department of Urologic Surgery, University of Minnesota,
Partial Nephrectomy Techniques for Renal Preservation: Historical and Modern Approaches
 Partial Nephrectomy Techniques for Renal Preservation: Historical and Modern Approaches Cary N Robertson MD FACS Associate Professor Division of Urology Associate Director Urologic Oncology Duke Cancer
Partial Nephrectomy Techniques for Renal Preservation: Historical and Modern Approaches Cary N Robertson MD FACS Associate Professor Division of Urology Associate Director Urologic Oncology Duke Cancer
TitleRadiographic evaluation of blunt re. TSUJI, Akira; MATSUZAKI, Shouji; TA. Citation 泌尿器科紀要 (1989), 35(7):
, 35(7):") TitleRadiographic evaluation of blunt re TSUJI, Akira; MATSUZAKI, Shouji; TA Author(s) NAGAKURA, Kazuhiko; MURAI, Masaru; Hiroshi Citation 泌尿器科紀要 (1989), 35(7): 1119-1123 Issue Date 1989-07 URL http://hdl.handle.net/2433/116611
TitleRadiographic evaluation of blunt re TSUJI, Akira; MATSUZAKI, Shouji; TA Author(s) NAGAKURA, Kazuhiko; MURAI, Masaru; Hiroshi Citation 泌尿器科紀要 (1989), 35(7): 1119-1123 Issue Date 1989-07 URL http://hdl.handle.net/2433/116611
Renal trauma: What the radiologist needs to know
 Renal trauma: What the radiologist needs to know Poster No.: C-1519 Congress: ECR 2016 Type: Educational Exhibit Authors: D. Roriz, I. Abreu, P. Belo Soares, F. Caseiro Alves ; 1 1 2 2 3 3 4 4 Guimarães/PT,
Renal trauma: What the radiologist needs to know Poster No.: C-1519 Congress: ECR 2016 Type: Educational Exhibit Authors: D. Roriz, I. Abreu, P. Belo Soares, F. Caseiro Alves ; 1 1 2 2 3 3 4 4 Guimarães/PT,
Genitourinary Tract Injuries
 Genitourinary Tract Injuries Chapter 18 Genitourinary Tract Injuries Introduction Genitourinary injuries constitute approximately 5% of the total injuries encountered in combat. Their treatment adheres
Genitourinary Tract Injuries Chapter 18 Genitourinary Tract Injuries Introduction Genitourinary injuries constitute approximately 5% of the total injuries encountered in combat. Their treatment adheres
Trauma. Neck trauma zones. Neck Injuries 1/3/2018. Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure
 Trauma 45 minutes highest points Ahmed Mahmoud, MD Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure Neck trauma zones Airway ;Rapid sequence intubation Breathing ;Needle
Trauma 45 minutes highest points Ahmed Mahmoud, MD Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure Neck trauma zones Airway ;Rapid sequence intubation Breathing ;Needle
Management of High-grade Blunt Renal Trauma
 ORIGINAL ARTICLE J Trauma Inj 2017;30(4):192-196 http://doi.org/10.20408/jti.2017.30.4.192 JOURNAL OF TRAUMA AND INJURY Management of High-grade Blunt Renal Trauma Min A Lee, M.D., Myung Jin Jang, M.S.,
ORIGINAL ARTICLE J Trauma Inj 2017;30(4):192-196 http://doi.org/10.20408/jti.2017.30.4.192 JOURNAL OF TRAUMA AND INJURY Management of High-grade Blunt Renal Trauma Min A Lee, M.D., Myung Jin Jang, M.S.,
Clinical aspects in urogenital injuries
 Clinical aspects in urogenital injuries Rolf Wahlqvist Oslo Urological University Clinic Aker University Hospital Nordic Rad.2008 1 Urogenital injuries in trauma patients Renal injury Ureteral injury (infrequent/iatrogenic)
Clinical aspects in urogenital injuries Rolf Wahlqvist Oslo Urological University Clinic Aker University Hospital Nordic Rad.2008 1 Urogenital injuries in trauma patients Renal injury Ureteral injury (infrequent/iatrogenic)
Genitourinary. Common Clinical Scenarios Protocoling Module. Patty Ojeda & Mariam Shehata
 The following training module was developed as a quality improvement project to serve as an educational tool for junior radiology residents. The following diagnostic radiology protocoling modules were
The following training module was developed as a quality improvement project to serve as an educational tool for junior radiology residents. The following diagnostic radiology protocoling modules were
Imaging abdominal vascular emergencies. V.Stoynova
 Imaging abdominal vascular emergencies V.Stoynova Abdominal vessels V. Stoynova 2 Acute liver bleeding trauma anticoagulant therapy liver disease : HCC, adenoma, meta, FNH, Hemangioma Diagnosis :CT angiography
Imaging abdominal vascular emergencies V.Stoynova Abdominal vessels V. Stoynova 2 Acute liver bleeding trauma anticoagulant therapy liver disease : HCC, adenoma, meta, FNH, Hemangioma Diagnosis :CT angiography
LIVER INJURIES PROFF. S.FLORET
 LIVER INJURIES PROFF. S.FLORET Abdominal injuries For anatomical consideration: Abdomen can be divided in four areas Intra thoracic abdomen True abdomen Pelvic abdomen Retroperitoneal abdomen ETIOLOGY
LIVER INJURIES PROFF. S.FLORET Abdominal injuries For anatomical consideration: Abdomen can be divided in four areas Intra thoracic abdomen True abdomen Pelvic abdomen Retroperitoneal abdomen ETIOLOGY
EAST MULTICENTER STUDY DATA DICTIONARY. Temporary Intravascular Shunt Study Data Dictionary
 EAST MULTICENTER STUDY DATA DICTIONARY Temporary Intravascular Shunt Study Data Dictionary Data Entry Points and appropriate definitions / clarifications: Entry space Definition / Instructions 1. Specific
EAST MULTICENTER STUDY DATA DICTIONARY Temporary Intravascular Shunt Study Data Dictionary Data Entry Points and appropriate definitions / clarifications: Entry space Definition / Instructions 1. Specific
Oncourology COMPLICATIONS OF PARTIAL NEPHRECTOMY AT OPERATIVE TREATMENT OF RENAL CELL CARCINOMA
 1 Oncourology COMPLICATIONS OF PARTIAL NEPHRECTOMY AT OPERATIVE TREATMENT OF RENAL CELL CARCINOMA Address: Eduard Oleksandrovych Stakhovsky, 03022, Kyiv, Lomonosova Str., 33/43, National Cancer Institute
1 Oncourology COMPLICATIONS OF PARTIAL NEPHRECTOMY AT OPERATIVE TREATMENT OF RENAL CELL CARCINOMA Address: Eduard Oleksandrovych Stakhovsky, 03022, Kyiv, Lomonosova Str., 33/43, National Cancer Institute
Damage Control in Abdominal and Pelvic Injuries
 Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
Uroradiology For Medical Students
 Uroradiology For Medical Students Lesson 4: Cystography & Urethrography - Part 2 American Urological Association Review Cystography is useful in evaluating the bladder, the urethra and the competence of
Uroradiology For Medical Students Lesson 4: Cystography & Urethrography - Part 2 American Urological Association Review Cystography is useful in evaluating the bladder, the urethra and the competence of
ABDOMINAL TRAUMA Lecture Prof. Zbigniew Wlodarczyk
 ABDOMINAL TRAUMA Lecture Prof. Zbigniew Wlodarczyk Epidemiology 2% of all traumas (4% amongst hospitalized patients) 75% M 25% F Average age 35 years 80% close 20% penetrating 40% liver and spleen, 10%
ABDOMINAL TRAUMA Lecture Prof. Zbigniew Wlodarczyk Epidemiology 2% of all traumas (4% amongst hospitalized patients) 75% M 25% F Average age 35 years 80% close 20% penetrating 40% liver and spleen, 10%
Renal Trauma: Management Options
 Renal Trauma: Management Options Immediate surgical repair Nephrectomy Conservative management Alonso RC et al. Kidney in Danger: CT Findings of Blunt and Penetrating Renal Trauma. RadioGraphics 2009;
Renal Trauma: Management Options Immediate surgical repair Nephrectomy Conservative management Alonso RC et al. Kidney in Danger: CT Findings of Blunt and Penetrating Renal Trauma. RadioGraphics 2009;
CT Imaging of Blunt and Penetrating Vascular Trauma DENNIS FOLEY MEDICAL COLLEGE WISCONSIN
 CT Imaging of Blunt and Penetrating Vascular Trauma DENNIS FOLEY MEDICAL COLLEGE WISCONSIN THORACO ABDOMINAL TRAUMA 0 10 20 30 40 50 60 5 cc/sec 30 secs 1.25 mm/ 55 mm Z1.375 2.5 mm/ 55 mm Z 1.375 Grade
CT Imaging of Blunt and Penetrating Vascular Trauma DENNIS FOLEY MEDICAL COLLEGE WISCONSIN THORACO ABDOMINAL TRAUMA 0 10 20 30 40 50 60 5 cc/sec 30 secs 1.25 mm/ 55 mm Z1.375 2.5 mm/ 55 mm Z 1.375 Grade
Urinary tract embolization
 Beograd, 14.10.2012 Urinary tract embolization asist. Peter Popovič, MD, MSc Head of abdominal radiology department, Institute of Radiology, UMC Ljubljana Embolization Who and when procedure: local/general
Beograd, 14.10.2012 Urinary tract embolization asist. Peter Popovič, MD, MSc Head of abdominal radiology department, Institute of Radiology, UMC Ljubljana Embolization Who and when procedure: local/general
Renal Transplant Surgery
 Renal Transplant Surgery Mr Somaiah Aroori MS MD EBS in HPB FRCS Consultant HPB & Renal Transplant Surgeon SWTC, Derriford Hospital, Plymouth Over next few minutes Aim to cover Details of Transplant procedure
Renal Transplant Surgery Mr Somaiah Aroori MS MD EBS in HPB FRCS Consultant HPB & Renal Transplant Surgeon SWTC, Derriford Hospital, Plymouth Over next few minutes Aim to cover Details of Transplant procedure
Abdomen and Genitalia Injuries. Chapter 28
 Abdomen and Genitalia Injuries Chapter 28 Hollow Organs in the Abdominal Cavity Signs of Peritonitis Abdominal pain Tenderness Muscle spasm Diminished bowel sounds Nausea/vomiting Distention Solid Organs
Abdomen and Genitalia Injuries Chapter 28 Hollow Organs in the Abdominal Cavity Signs of Peritonitis Abdominal pain Tenderness Muscle spasm Diminished bowel sounds Nausea/vomiting Distention Solid Organs
already in the operating room.(0 Ultrasonography (US) has also been found to be very useful in the early evaluation
 has also been found to be very useful in the early evaluation") Pictorial Essay Singapore Med J 2010, 51(6) 68 CME Article Computed tomography of blunt renal trauma Razali M R, Azian A A, Am ran A R, Azlin S ABSTRACT Renal injury is observed in 10 percent of cases
Pictorial Essay Singapore Med J 2010, 51(6) 68 CME Article Computed tomography of blunt renal trauma Razali M R, Azian A A, Am ran A R, Azlin S ABSTRACT Renal injury is observed in 10 percent of cases
EAU Guidelines on Urological Trauma
 EAU Guidelines on Urological Trauma N.D. Kitrey (Chair), N. Djakovic, M. Gonsalves, F.E. Kuehhas, N. Lumen, E. Serafetinidis, D.M. Sharma, D.J. Summerton Guidelines Associates: P-J. Elshout, A. Sujenthiran,
EAU Guidelines on Urological Trauma N.D. Kitrey (Chair), N. Djakovic, M. Gonsalves, F.E. Kuehhas, N. Lumen, E. Serafetinidis, D.M. Sharma, D.J. Summerton Guidelines Associates: P-J. Elshout, A. Sujenthiran,
PRACTICE GUIDELINE TITLE: NON-OPERATIVE MANAGEMENT OF LIVER / SPLENIC INJURIES
 PRACTICE GUIDELINE Effective Date: 6-18-04 Manual Reference: Deaconess Trauma Services TITLE: N-OPERATIVE MANAGEMENT OF LIVER / SPLENIC INJURIES PURPOSE: To define when non-operative management of liver
PRACTICE GUIDELINE Effective Date: 6-18-04 Manual Reference: Deaconess Trauma Services TITLE: N-OPERATIVE MANAGEMENT OF LIVER / SPLENIC INJURIES PURPOSE: To define when non-operative management of liver
Treatment of choice for end stage renal disease Imaging to establish baseline and diagnosis of potential complications Review common surgical
 Treatment of choice for end stage renal disease Imaging to establish baseline and diagnosis of potential complications Review common surgical techniques Review normal appearance Discuss US diagnosis of
Treatment of choice for end stage renal disease Imaging to establish baseline and diagnosis of potential complications Review common surgical techniques Review normal appearance Discuss US diagnosis of
A Giant Hydronephrotic Kidney with Ureteropelvic Junction Obstruction with Blunt Renal Trauma in a Boy
 A Giant Hydronephrotic Kidney with Ureteropelvic Junction Obstruction with Blunt Renal Trauma in a Boy BY JUNYA TSURUKIRI, HIDEFUMI SANO, YOSUKE TANAKA, TAKAO SATO, HIROKAZU TAGUCHI Abstract An 18-year-old
A Giant Hydronephrotic Kidney with Ureteropelvic Junction Obstruction with Blunt Renal Trauma in a Boy BY JUNYA TSURUKIRI, HIDEFUMI SANO, YOSUKE TANAKA, TAKAO SATO, HIROKAZU TAGUCHI Abstract An 18-year-old
West Yorkshire Major Trauma Network Clinical Guidelines 2015
 WYMTN: Pelvic fracture with urogenital trauma KEY RECOMMENDATIONS 1. During the initial exploratory survey / secondary survey, a. The external urethral meatus and the transurethral bladder catheter (if
WYMTN: Pelvic fracture with urogenital trauma KEY RECOMMENDATIONS 1. During the initial exploratory survey / secondary survey, a. The external urethral meatus and the transurethral bladder catheter (if
Open Journal of Trauma. Grade V Renal Injury Short and Long Term Outcome. Introduction. Research Article
 Clinical Group Open Journal of Trauma DOI http://dx.doi.org/10.17352/ojt.000005 CC By Rajendra B Nerli 1 *, Vikas Sharma 1, Basavaraj M Kajagar 2, Neeraj S Dixit 1 and Nitin D Pingale 1 1 Department of
Clinical Group Open Journal of Trauma DOI http://dx.doi.org/10.17352/ojt.000005 CC By Rajendra B Nerli 1 *, Vikas Sharma 1, Basavaraj M Kajagar 2, Neeraj S Dixit 1 and Nitin D Pingale 1 1 Department of
Abdominal & retroperitoneal endovascular intervention, Bo Kalin, Karolinska Hospital
 Abdominal & retroperitoneal endovascular intervention, Bo Kalin, Karolinska Hospital What is endovascular therapy. Diagnosing Traumatic Arterial Injury Clinical signs CT / CT-angiography To diminish a
Abdominal & retroperitoneal endovascular intervention, Bo Kalin, Karolinska Hospital What is endovascular therapy. Diagnosing Traumatic Arterial Injury Clinical signs CT / CT-angiography To diminish a
EAU GUIDELINES POCKET EDITION 4
 EAU GUIDELINES POCKET EDITION 4 CONTENTS: UROLOGICAL TRAUMA PAIN MANAGEMENT IN UROLOGY UROGENERIC LUTS RENAL TRANSPLANTATION 2 EAU POCKET GUIDELINES POCKET EDITION 4 Introduction 3 Introduction This is
EAU GUIDELINES POCKET EDITION 4 CONTENTS: UROLOGICAL TRAUMA PAIN MANAGEMENT IN UROLOGY UROGENERIC LUTS RENAL TRANSPLANTATION 2 EAU POCKET GUIDELINES POCKET EDITION 4 Introduction 3 Introduction This is
PONGSASIT SINGHATAS, M.D. Department of Surgery Faculty of Medicine, Ramathibodi Hospital Mahidol University
 PONGSASIT SINGHATAS, M.D. Department of Surgery Faculty of Medicine, Ramathibodi Hospital Mahidol University Patient survive Low morbidity GOOD JUDGMENT COMES FROM EXPERIENCE EXPERIENCE COMES FROM BAD
PONGSASIT SINGHATAS, M.D. Department of Surgery Faculty of Medicine, Ramathibodi Hospital Mahidol University Patient survive Low morbidity GOOD JUDGMENT COMES FROM EXPERIENCE EXPERIENCE COMES FROM BAD
SPECIAL DIAGNOSTIC STUDIES IN BLUNT TRAUMA OLEH : Prof.DR.Dr Abdul Rasyid SpRad (K),Ph.D Dr.Evo Elidar Sp.Rad
,Ph.D Dr.Evo Elidar Sp.Rad") SPECIAL DIAGNOSTIC STUDIES IN BLUNT TRAUMA OLEH : Prof.DR.Dr Abdul Rasyid SpRad (K),Ph.D Dr.Evo Elidar Sp.Rad Trauma Emergency Room layout Ideally the trauma emergency room is centrally located to provide
SPECIAL DIAGNOSTIC STUDIES IN BLUNT TRAUMA OLEH : Prof.DR.Dr Abdul Rasyid SpRad (K),Ph.D Dr.Evo Elidar Sp.Rad Trauma Emergency Room layout Ideally the trauma emergency room is centrally located to provide
AORTIC GRAFT INFECTION
 NURSING CARE Theresa O Keefe NUM Vascular Unit PAH Vascular infections are serious They are associated with high morbidity and mortality The primary cause of surgical wound infections is contamination
NURSING CARE Theresa O Keefe NUM Vascular Unit PAH Vascular infections are serious They are associated with high morbidity and mortality The primary cause of surgical wound infections is contamination
Radiological Investigations of Abdominal Trauma
 76 77 Investigations of Abdominal Trauma Introduction: Trauma to abdominal organs is a common cause of patient morbidity and mortality among trauma patients. Causes of abdominal trauma include blunt injuries,
76 77 Investigations of Abdominal Trauma Introduction: Trauma to abdominal organs is a common cause of patient morbidity and mortality among trauma patients. Causes of abdominal trauma include blunt injuries,
George M Wadie, MD Director Division of Pediatric Surgery Sacred Heart Medical Center. Springfield, OR Adjunct Assistant Professor of Surgery Oregon
 George M Wadie, MD Director Division of Pediatric Surgery Sacred Heart Medical Center. Springfield, OR Adjunct Assistant Professor of Surgery Oregon Health and Sciences University. Portland, OR Outline
George M Wadie, MD Director Division of Pediatric Surgery Sacred Heart Medical Center. Springfield, OR Adjunct Assistant Professor of Surgery Oregon Health and Sciences University. Portland, OR Outline
PROTOCOLS. Lap-belt syndrome. Principal investigator. Background
 Lap-belt syndrome Principal investigator Claude Cyr, MD, Centre hospitalier universitaire de Sherbrooke, 3001 12 e Avenue Nord, Sherbrooke QC J1H 5N4; tel.: (819) 346-1110, ext. 14634; fax: (819) 564-5398;
Lap-belt syndrome Principal investigator Claude Cyr, MD, Centre hospitalier universitaire de Sherbrooke, 3001 12 e Avenue Nord, Sherbrooke QC J1H 5N4; tel.: (819) 346-1110, ext. 14634; fax: (819) 564-5398;
A Case Report of Acute Renal Artery Occlusion Mimicking Acute Appendicitis
 ISPUB.COM The Internet Journal of Surgery Volume 7 Number 1 A Case Report of Acute Renal Artery Occlusion Mimicking Acute Appendicitis S Abouel-Enin, A Douglas, R Morgan Citation S Abouel-Enin, A Douglas,
ISPUB.COM The Internet Journal of Surgery Volume 7 Number 1 A Case Report of Acute Renal Artery Occlusion Mimicking Acute Appendicitis S Abouel-Enin, A Douglas, R Morgan Citation S Abouel-Enin, A Douglas,
Surgery of urogenital trauma in condition of war or precarity
 Surgery of urogenital trauma in condition of war or precarity C. H. Rochat Multi-disciplinary Center for Robotic Surgery, Geneva (www.beaulieu.ch) Geneva Foundation for Medical Education and Research (www.gfmer.ch)
Surgery of urogenital trauma in condition of war or precarity C. H. Rochat Multi-disciplinary Center for Robotic Surgery, Geneva (www.beaulieu.ch) Geneva Foundation for Medical Education and Research (www.gfmer.ch)
Pediatric Abdomen Trauma
 Pediatric Abdomen Trauma Susan D. John, MD, FACR Pediatric Trauma Trauma is leading cause of death and disability in children and adolescents Causes and effects vary between age groups Blunt trauma predominates
Pediatric Abdomen Trauma Susan D. John, MD, FACR Pediatric Trauma Trauma is leading cause of death and disability in children and adolescents Causes and effects vary between age groups Blunt trauma predominates
Delayed Presentation of Traumatic Bladder Injury: A case report and review of current treatment trends
 ISPUB.COM The Internet Journal of Urology Volume 5 Number 1 Delayed Presentation of Traumatic Bladder Injury: A case report and review of current treatment trends S Deem, C Lavender, S Agarwal Citation
ISPUB.COM The Internet Journal of Urology Volume 5 Number 1 Delayed Presentation of Traumatic Bladder Injury: A case report and review of current treatment trends S Deem, C Lavender, S Agarwal Citation
PARA107 Summary. Page 1-3: Page 4-6: Page 7-10: Page 11-13: Page 14-17: Page 18-21: Page 22-25: Page 26-28: Page 29-33: Page 34-36: Page 37-38:
 PARA107 Summary Page 1-3: Page 4-6: Page 7-10: Page 11-13: Page 14-17: Page 18-21: Page 22-25: Page 26-28: Page 29-33: Page 34-36: Page 37-38: Injury, Mechanisms of Injury, Time Critical Guidelines Musculoskeletal
PARA107 Summary Page 1-3: Page 4-6: Page 7-10: Page 11-13: Page 14-17: Page 18-21: Page 22-25: Page 26-28: Page 29-33: Page 34-36: Page 37-38: Injury, Mechanisms of Injury, Time Critical Guidelines Musculoskeletal
A Z OF ABDOMINAL RADIOLOGY
 Z OF BDOMINL RDIOLOGY bdominal trauma to Z of bdominal Radiology Clinical characteristics general discussion, followed by organ-specific summaries, is given below. bdominal trauma is managed as part of
Z OF BDOMINL RDIOLOGY bdominal trauma to Z of bdominal Radiology Clinical characteristics general discussion, followed by organ-specific summaries, is given below. bdominal trauma is managed as part of
Kaiser Oakland Urology
 Kaiser Oakland Urology What is Laparoscopy? Minimally invasive surgical alternative to standard surgery How is Laparoscopy Performed? A laparoscope and video camera are used to visualize internal organs
Kaiser Oakland Urology What is Laparoscopy? Minimally invasive surgical alternative to standard surgery How is Laparoscopy Performed? A laparoscope and video camera are used to visualize internal organs
Long-term functional follow-up after kidney injury in children: Retrospective review of 33 cases
 Mémoire de Maîtrise en médecine No 1839 Long-term functional follow-up after kidney injury in children: Retrospective review of 33 cases Etudiant Roschan Hayoz Tuteur Dr. Nicolas Lutz Dpt de chirurgie
Mémoire de Maîtrise en médecine No 1839 Long-term functional follow-up after kidney injury in children: Retrospective review of 33 cases Etudiant Roschan Hayoz Tuteur Dr. Nicolas Lutz Dpt de chirurgie
A Severely Injured Pediatric Trauma Patient: Case Presentation and Discussion
 A Severely Injured Pediatric Trauma Patient: Case Presentation and Discussion Christopher Butts PhD, DO Surgical Critical Care Fellow Cooper University Hospital H&P 10 year old female presents as a trauma
A Severely Injured Pediatric Trauma Patient: Case Presentation and Discussion Christopher Butts PhD, DO Surgical Critical Care Fellow Cooper University Hospital H&P 10 year old female presents as a trauma
Vascular Surgery Rotation Objectives for Junior Residents (PGY-1 and 2)
") Vascular Surgery Rotation Objectives for Junior Residents (PGY-1 and 2) Definition Vascular surgery is the specialty concerned with the diagnosis and management of congenital and acquired diseases of the
Vascular Surgery Rotation Objectives for Junior Residents (PGY-1 and 2) Definition Vascular surgery is the specialty concerned with the diagnosis and management of congenital and acquired diseases of the
Abdominal Aortic Aneurysms. A Surgeons Perspective Dr. Derek D. Muehrcke
 Abdominal Aortic Aneurysms A Surgeons Perspective Dr. Derek D. Muehrcke Aneurysm Definition The abnormal enlargement or bulging of an artery caused by an injury or weakness in the blood vessel wall A localized
Abdominal Aortic Aneurysms A Surgeons Perspective Dr. Derek D. Muehrcke Aneurysm Definition The abnormal enlargement or bulging of an artery caused by an injury or weakness in the blood vessel wall A localized
RENAL SURGERY. Susanne Åkerblom Chief of Surgery Swedish Specialist in Surgery (Small Animal)
") RENAL SURGERY Susanne Åkerblom Chief of Surgery Swedish Specialist in Surgery (Small Animal) ANATOMY The left kidney is generally more mobile than the right The kidney is covered by a thin fibrous capsule
RENAL SURGERY Susanne Åkerblom Chief of Surgery Swedish Specialist in Surgery (Small Animal) ANATOMY The left kidney is generally more mobile than the right The kidney is covered by a thin fibrous capsule
General Imaging. Imaging modalities. Incremental CT. Multislice CT Multislice CT [ MDCT ]
![General Imaging. Imaging modalities. Incremental CT. Multislice CT Multislice CT [ MDCT ]](/thumbs/76/74079340.jpg "General Imaging. Imaging modalities. Incremental CT. Multislice CT Multislice CT [ MDCT ]") General Imaging Imaging modalities Conventional X-rays Ultrasonography [ US ] Computed tomography [ CT ] Radionuclide imaging Magnetic resonance imaging [ MRI ] Angiography conventional, CT,MRI Interventional
General Imaging Imaging modalities Conventional X-rays Ultrasonography [ US ] Computed tomography [ CT ] Radionuclide imaging Magnetic resonance imaging [ MRI ] Angiography conventional, CT,MRI Interventional
GUIDELINEs ON UROLOGICAL TRAUMA
 GUIDELINEs ON UROLOGICAL TRAUMA (Text update March 2009) N. Djakovic, Th. Lynch, L. Martínez-Piñeiro, Y. Mor, E. Plas, E. Serafetinides, L. Turkeri, R.A. Santucci, M. Hohenfellner Eur Urol 2005;47(1):1-15
GUIDELINEs ON UROLOGICAL TRAUMA (Text update March 2009) N. Djakovic, Th. Lynch, L. Martínez-Piñeiro, Y. Mor, E. Plas, E. Serafetinides, L. Turkeri, R.A. Santucci, M. Hohenfellner Eur Urol 2005;47(1):1-15
GUIDELINEs ON UROLOGICAL TRAUMA
 GUIDELINEs ON UROLOGICAL TRAUMA (Text update March 2009) N. Djakovic, Th. Lynch, L. Martínez-Piñeiro, Y. Mor, E. Plas, E. Serafetinides, L. Turkeri, R.A. Santucci, M. Hohenfellner Eur Urol 2005;47(1):1-15
GUIDELINEs ON UROLOGICAL TRAUMA (Text update March 2009) N. Djakovic, Th. Lynch, L. Martínez-Piñeiro, Y. Mor, E. Plas, E. Serafetinides, L. Turkeri, R.A. Santucci, M. Hohenfellner Eur Urol 2005;47(1):1-15
Abdominal Trauma. Nat Krairojananan M.D., FRCST Department of Trauma and Emergency Medicine Phramongkutklao Hospital
 Abdominal Trauma Nat Krairojananan M.D., FRCST Department of Trauma and Emergency Medicine Phramongkutklao Hospital overview Quick review abdominal anatomy Review of mechanism of injury Review of investigation
Abdominal Trauma Nat Krairojananan M.D., FRCST Department of Trauma and Emergency Medicine Phramongkutklao Hospital overview Quick review abdominal anatomy Review of mechanism of injury Review of investigation
Renal Artery Embolization for the Treatment of Renal Artery Pseudoaneurysm Following Partial Nephrectomy
 The Ochsner Journal 13:259 263, 2013 Ó Academic Division of Ochsner Clinic Foundation Renal Artery Embolization for the Treatment of Renal Artery Pseudoaneurysm Following Partial Nephrectomy Cara Irwine,
The Ochsner Journal 13:259 263, 2013 Ó Academic Division of Ochsner Clinic Foundation Renal Artery Embolization for the Treatment of Renal Artery Pseudoaneurysm Following Partial Nephrectomy Cara Irwine,
Guidelines and Protocols
 TITLE: PELVIC TRAUMA PURPOSE: Develop a protocol of care that will insure rapid identification and treatment of these patients PROCESS: I. CARE OF PATIENTS WITH PELVIC TRAUMA A. Patients in hemorrhagic
TITLE: PELVIC TRAUMA PURPOSE: Develop a protocol of care that will insure rapid identification and treatment of these patients PROCESS: I. CARE OF PATIENTS WITH PELVIC TRAUMA A. Patients in hemorrhagic
Clinical Questions. Clinical Questions. Clinical Questions. Health-Process-Evidencebased Clinical Practice Guidelines Acute Abdomen
 Health-Process-Evidencebased Clinical Practice Guidelines Acute Abdomen 1. What is an operational concept of acute abdomen? any abdominal condition of acute onset from various causes involving the intraabdominal
Health-Process-Evidencebased Clinical Practice Guidelines Acute Abdomen 1. What is an operational concept of acute abdomen? any abdominal condition of acute onset from various causes involving the intraabdominal
Abdominal Compartment Syndrome. Jeff Johnson, MD
 Abdominal Compartment Syndrome Jeff Johnson, MD Acute Care Surgeon, Denver Health Associate Professor of Surgery, University of Colorado Denver The Abdomen A Forgotten Closed Compartment Early Animal Models
Abdominal Compartment Syndrome Jeff Johnson, MD Acute Care Surgeon, Denver Health Associate Professor of Surgery, University of Colorado Denver The Abdomen A Forgotten Closed Compartment Early Animal Models
Case 37 Clinical Presentation
 Case 37 73 Clinical Presentation The patient is a 62-year-old woman with gastrointestinal (GI) bleeding. 74 RadCases Interventional Radiology Imaging Findings () Image from a selective digital subtraction
Case 37 73 Clinical Presentation The patient is a 62-year-old woman with gastrointestinal (GI) bleeding. 74 RadCases Interventional Radiology Imaging Findings () Image from a selective digital subtraction
PENETRATING COLON TRAUMA: THE CURRENT EVIDENCE
 PENETRATING COLON TRAUMA: THE CURRENT EVIDENCE Samuel Hawkins MD CASE PRESENTATION 22M BIBEMS s/p multiple GSW ABCs intact Normotensive, non-tachycardic Secondary Survey: 4 truncal bullet holes L superior
PENETRATING COLON TRAUMA: THE CURRENT EVIDENCE Samuel Hawkins MD CASE PRESENTATION 22M BIBEMS s/p multiple GSW ABCs intact Normotensive, non-tachycardic Secondary Survey: 4 truncal bullet holes L superior
Blunt Renal Trauma in a Pre-Existing Renal Lesion
 Case Study TheScientificWorldJOURNAL (2006) 6, 2334 2338 TSW Urology ISSN 1537-744X; DOI 10.1100/tsw.2006.364 Blunt Renal Trauma in a Pre-Existing Renal Lesion G.V. Soundra Pandyan*, Idris Omo-Adua, Mohammed
Case Study TheScientificWorldJOURNAL (2006) 6, 2334 2338 TSW Urology ISSN 1537-744X; DOI 10.1100/tsw.2006.364 Blunt Renal Trauma in a Pre-Existing Renal Lesion G.V. Soundra Pandyan*, Idris Omo-Adua, Mohammed
Interventional Radiology Case Conferences Massachusetts General Hospital
 Interventional Radiology Case Conferences Massachusetts General Hospital Renal Trauma: Radiologic Evaluation and Percutaneous Treatment of Nonvascular Injuries Ross L. Titton 1, Debra A. Gervais, Giles
Interventional Radiology Case Conferences Massachusetts General Hospital Renal Trauma: Radiologic Evaluation and Percutaneous Treatment of Nonvascular Injuries Ross L. Titton 1, Debra A. Gervais, Giles
The epidemiology of renal trauma
 Original Article The epidemiology of renal trauma Bryan B. Voelzke, Laura Leddy Department of Urology, Harborview Medical Center, University of Washington Medical Center, Seattle, Washington 98104, USA
Original Article The epidemiology of renal trauma Bryan B. Voelzke, Laura Leddy Department of Urology, Harborview Medical Center, University of Washington Medical Center, Seattle, Washington 98104, USA
SSRG International Journal of Medical Science (SSRG-IJMS) volume 1 Issue 2 December 2014
 volume 1 Issue 2 December 2014") Blunt Abdominal Trauma: Making Decision of Management with Conventional and Ultrasonography Evaluation Dr.Naveen K G 1, Dr. Ravi N 2, Dr. Nagaraj B R 3 1(senior resident-department of radiology, Bangalore
Blunt Abdominal Trauma: Making Decision of Management with Conventional and Ultrasonography Evaluation Dr.Naveen K G 1, Dr. Ravi N 2, Dr. Nagaraj B R 3 1(senior resident-department of radiology, Bangalore
Interventional Radiology for Solid Organ Trauma. Case Study 8/17/2017. Diagnosis? Case Study (cont d)
") Interventional Radiology for Solid Organ Trauma Jamie Gallivan RN, BSN Interventional Radiology Case Study 6 y/o boy fell out of 2 nd story window onto concrete Hemodynamically stable at scene Arrival
Interventional Radiology for Solid Organ Trauma Jamie Gallivan RN, BSN Interventional Radiology Case Study 6 y/o boy fell out of 2 nd story window onto concrete Hemodynamically stable at scene Arrival
PERPHERAL ARTERY ANEURYSM. By Pooja Sharma and Susanna Sebastianpillai
 PERPHERAL ARTERY ANEURYSM By Pooja Sharma and Susanna Sebastianpillai Defintions True Aneurysm Involves all three layers of the vessel. Have two basic shapes; Fusiform = symmetric widening of the vessels
PERPHERAL ARTERY ANEURYSM By Pooja Sharma and Susanna Sebastianpillai Defintions True Aneurysm Involves all three layers of the vessel. Have two basic shapes; Fusiform = symmetric widening of the vessels
How to manage TAVI related vascular complications. Paul TL Chiam MBBS, FRCP, FESC, FACC, FSCAI
 How to manage TAVI related vascular complications Paul TL Chiam MBBS, FRCP, FESC, FACC, FSCAI Definition VARC-2 consensus statement Complications caused by: Wire Catheter Anything related to vascular access
How to manage TAVI related vascular complications Paul TL Chiam MBBS, FRCP, FESC, FACC, FSCAI Definition VARC-2 consensus statement Complications caused by: Wire Catheter Anything related to vascular access
Liver lacerations in abdominal trauma management based on anatomical knowledge: A Case report
 American Journal of Advances in Medical Science www.arnaca.com eissn: 2347-2766 Case Report Liver lacerations in abdominal trauma management based on anatomical Ashfaq ul Hassan 1*, Rohul 1, Shifan 2,
American Journal of Advances in Medical Science www.arnaca.com eissn: 2347-2766 Case Report Liver lacerations in abdominal trauma management based on anatomical Ashfaq ul Hassan 1*, Rohul 1, Shifan 2,
Genitourinary Tract Trauma. Wen-xuan Chen Department of urology Tianjin medical university General hospital
 Genitourinary Tract Trauma Wen-xuan Chen Department of urology Tianjin medical university General hospital Introduction About 10% of all injuries in the emergency room are genitourinary injuries. The most
Genitourinary Tract Trauma Wen-xuan Chen Department of urology Tianjin medical university General hospital Introduction About 10% of all injuries in the emergency room are genitourinary injuries. The most
10/2/2018. Acute Management of Pelvic Injuries. Learning Objectives. 17 yo male ped struck by truck
 17 yo male ped struck by truck Acute Management of Pelvic Injuries David Volgas, MD CoxHealth University of Missouri HD unstable Open pelvic wound superior gluteal fold through rectum to scrotum Open rami
17 yo male ped struck by truck Acute Management of Pelvic Injuries David Volgas, MD CoxHealth University of Missouri HD unstable Open pelvic wound superior gluteal fold through rectum to scrotum Open rami
RCH Trauma Guideline. Management of Traumatic Pneumothorax & Haemothorax. Trauma Service, Division of Surgery
 RCH Trauma Guideline Management of Traumatic Pneumothorax & Haemothorax Trauma Service, Division of Surgery Aim To describe safe and competent management of traumatic pneumothorax and haemothorax at RCH.
RCH Trauma Guideline Management of Traumatic Pneumothorax & Haemothorax Trauma Service, Division of Surgery Aim To describe safe and competent management of traumatic pneumothorax and haemothorax at RCH.
To review the incidence and management of penetrating renal injuries in patients with multiorgan trauma during a 6-year period.
 1. Ramchandani P, Buckler PM. Imaging of genitourinary trauma. AJR 2009; 192(6):151-152. 2. Kansas BT, Eddy MJ, Mydlo JH, Uzzo RG. Incidence and management of penetrating renal trauma in with multiorgan
1. Ramchandani P, Buckler PM. Imaging of genitourinary trauma. AJR 2009; 192(6):151-152. 2. Kansas BT, Eddy MJ, Mydlo JH, Uzzo RG. Incidence and management of penetrating renal trauma in with multiorgan
Urologic Surgical Complications In Renal Transplantation
 Urologic Surgical Complications In Renal Transplantation Chris Freise, MD Professor of Surgery UCSF Transplant Division Urologic Complications Review of Bladder Anastomosis Complications and Management
Urologic Surgical Complications In Renal Transplantation Chris Freise, MD Professor of Surgery UCSF Transplant Division Urologic Complications Review of Bladder Anastomosis Complications and Management
TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES
 TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES ALBERTO MAUD, MD ASSOCIATE PROFESSOR TEXAS TECH UNIVERSITY HEALTH SCIENCES CENTER EL PASO PAUL L. FOSTER SCHOOL OF MEDICINE 18TH ANNUAL RIO GRANDE TRAUMA 2017
TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES ALBERTO MAUD, MD ASSOCIATE PROFESSOR TEXAS TECH UNIVERSITY HEALTH SCIENCES CENTER EL PASO PAUL L. FOSTER SCHOOL OF MEDICINE 18TH ANNUAL RIO GRANDE TRAUMA 2017
Pelvic Injuries. Chapter 21
 Chapter 21 Introduction Injuries of the pelvis are an uncommon, but potentially lethal, battlefield injury. Blunt injuries may be associated with major hemorrhage and early mortality. Death within the
Chapter 21 Introduction Injuries of the pelvis are an uncommon, but potentially lethal, battlefield injury. Blunt injuries may be associated with major hemorrhage and early mortality. Death within the
Combat Extremity Vascular Trauma
 Combat Extremity Vascular Trauma Training teams to be a TEAM Chatt A. Johnson LTC, MC, USA 08 March 2010 US Army Trauma Training Center Core Discussion Series Outline: Combat Vascular Injury Physiologic
Combat Extremity Vascular Trauma Training teams to be a TEAM Chatt A. Johnson LTC, MC, USA 08 March 2010 US Army Trauma Training Center Core Discussion Series Outline: Combat Vascular Injury Physiologic
MINIMALLY INVASIVE MANAGEMENT OF RENOVASCULAR COMPLICATIONS AFTER RENAL GRAFT TRANSPLANTATION
 MINIMALLY INVASIVE MANAGEMENT OF RENOVASCULAR COMPLICATIONS AFTER RENAL GRAFT TRANSPLANTATION Gortes, Francisco Javier B.S; Salsamendi, Jason Thomas M.D LEARNING OBJECTIVES Educate physicians on the prompt
MINIMALLY INVASIVE MANAGEMENT OF RENOVASCULAR COMPLICATIONS AFTER RENAL GRAFT TRANSPLANTATION Gortes, Francisco Javier B.S; Salsamendi, Jason Thomas M.D LEARNING OBJECTIVES Educate physicians on the prompt
Case Report Transplantation of Horseshoe Kidney from Living, Genetically Unrelated Donor
 Case Reports in Transplantation Volume 2015, Article ID 390381, 4 pages http://dx.doi.org/10.1155/2015/390381 Case Report Transplantation of Horseshoe Kidney from Living, Genetically Unrelated Donor Kazuro
Case Reports in Transplantation Volume 2015, Article ID 390381, 4 pages http://dx.doi.org/10.1155/2015/390381 Case Report Transplantation of Horseshoe Kidney from Living, Genetically Unrelated Donor Kazuro