2
|
|
|
- Laureen Miles
- 5 years ago
- Views:
Transcription
1 1
2 2
3 3

4 Cystic fibrosis of the pancreas was described in a study of clinical reports with autopsy analysis of the pancreas that aimed to find more reliable criteria for differentiating causes of steatorrhea cases of cystic fibrosis of the pancreas were described Autosomal recessive single-gene defect was postulated as leading to cystic fibrosis of the pancreas based on an analysis of the inheritance characteristics of 105 cases with documented fibrosis of the pancreas out of 365 children (well and sick) from 118 families 2 Defects in both bicarbonate and chloride were shown in a study of 56 patients with CF with a wide range of pancreatic function and 56 non-cf subjects who where healthy (6 subjects), had no evidence of pancreatic disease but had function testing to rule out Schwachmans syndrome (6 subjects) or CF (3 subjects), had Schwachman s syndrome (10 subjects), or had other diagnoses with variable pancreatic dysfunction (31). 3 Pancreatic output samples were obtained by a marker perfusion pancreatic function test, using a double-lumen tube positioned to perfuse a nonabsorbable marker across the ampulla of Vater and aspirate the marker and pancreatic secretions distally. Samples were analyzed for chloride, bicarbonate, and other secretions. Three pivotal papers were published simultaneously in Science in 1989 describing the discovery and description of the CF gene A detailed analysis of 280 kb of contiguous DNA isolated by chromosome jumping and walking permitted the cloning of the locus responsible for cystic fibrosis without prior knowledge of the basic defect. 4 Analysis of cdna clones identified a region of 6.1 kb that was capable of encoding a 1480 amino acid protein. Hybridization experiments localized the protein to pancreas, primary cultures of nasal polyps, lung, colon, and cultured epithelial cells from sweat glands. 5 When CF sequences were compared with normal sequences, a 3-base-pair deletion difference was found that produced F508del. 5 Predicted structure was a protein with resemblance to membrane transporter proteins. 5 Analysis of CF carriers using restriction fragment length polymorphisms were used to study determine the relation of each of the DNA segments isolated from the chromosome walking and jumping experiments to CF. These studies were able to show a relationship between pancreatic sufficiency/insufficiency and severity of mutations in the gene product. 6 Two studies identified the single channel properties of the CFTR protein expressed in cells that do not normally have a camp-regulated chloride conductance, 7 and synthetic phospholipid vesicles, 8 demonstrating unequivocally that CFTR is a membrane ion channel with a chloride conductance that is activated by camp-dependent protein kinase A. A chloride-independent bicarbonate flux was demonstrated using pancreatic duct epithelia from guinea pigs and wild type mice that was absent in CF mice. 9 References 1. Andersen DH. Am J Dis Child 1938; 56: Lowe CU et al. Am J Dis Child. 1949;78: Kopelman H et al. Gastroenterol. 1988;95: Rommens JM et al. Science. 1989;245: Riordan JR et al. Science. 1989;245: Kerem B et al. Science. 1989;245: Berger HA et al. J Clin Invest. 1991;88: Bear CE et al. Cell. 1992;68: Ishiguro H et al. J Gen Physiol. 2009;133:

5 Cystic fibrosis is a rare life-long genetic disease that affects approximately 29,000 people in the United States and about 70,000 worldwide regardless of race or ethnicity but is more common in Caucasians 1,2 CF generally manifests in infancy or early childhood and leads to a shortened lifespan. Availability of multiple treatments and an improved understanding of the course of the disease has led to increased life expectancy; however, the median predicted age of survival was reported to be 39.3 years in the US in Clinical manifestations of CF occur throughout the body and affect many key organs and systems, including lungs, sinuses, pancreas, digestive and reproductive tracts, sweat glands and others 3 References 1. Cystic Fibrosis Foundation (CFF) Patient Registry Annual Data Report. Bethesda, MD: CFF; Sosnay PR et al. Nat Genet. 2013;45(10): O Sullivan BP, Freedman SD. Lancet. 2009;373:

6 CFTR protein channels transport ions, such as chloride and bicarbonate, to regulate fluid and electrolyte balance in epithelial tissues throughout the body Reference MacDonald KD et al. Pediatr Drugs. 2007;9:
7 7

8 The expression of the CF clinical phenotype in a specific patient is affected by total CFTR activity (determined by by CFTR genotype) as well as by modifier genes and environmental factors 1 Generally, 2 mutations with little or no CFTR activity are associated with a more classic phenotype. The presence of a complex allele may also contribute to reduction in CFTR activity 2-3 Ongoing active research identified many modifier genes that have been implicated in modifying function of various organs affected in cystic fibrosis, including those that :4 Are directly involved in CFTR function (β-adrenergic receptor) Encode alternate ion transport pathways (voltage-gated chloride channel 2) Affect immune responses (mannose binding lectin-2, tissue necrosis factor (TNF)-α) Impact lung function/disease course (transforming growth factor-β1, α-1 antitrypsin, TNF-α) Assessing environmental contribution to the CF pulmonary phenotype is challenging due to various components involved and the lack of objective measurements for many components. Despite these limitations, passive cigarette smoking and ambient air pollution have been linked with reduced pulmonary function. Pulmonary colonization with Pseudomonas aeruginosa and Burkholderia cepacia is an environmentally mediated event that is associated with reduced longevity 4 References 1. Cutting GR et al. Nat Rev Genet. 2015;16: DeGracia J et al. Thorax. 2005;60: Castellani C et al. J Cyst Fibros. 2008;7: Cutting GR. Annu Rev Genomics Hum Genet. 2005;6:
9 Studies have shown that the increased chloride level in sweat in patients with cystic fibrosis (CF) is linked to dysfunction or absence of CFTR protein. 1 Generally, the sweat chloride concentration in normal subjects is below 40 mmol/l and in individuals with CF, sweat chloride concentrations are 60 mmol/l 2 CF patients with partial CFTR function and exocrine pancreatic sufficiency tend to have lower sweat chloride levels than patients who have pancreatic insufficiency (PI) 1 Individuals with CF and PI have the lowest level of CFTR protein activity and the highest sweat chloride content 1 Therefore, sweat chloride level is a biomarker of pancreatic status in CF 1 Note for the graph: 3 important assumptions were made: 1) sweat chloride levels are versus predicted CFTR activity; 2) normal individuals are assumed to have 100% CFTR activity; 3) carriers are assumed to have 50% CFTR activity 1 References 1. Rowe SM et al. Proc Am Thorac Soc. 2007;4(4): Farrell PM et al. J Pediatr. 2008;153:S4-S14. 9
10 A single center study in Toronto evaluated 742 patients with a confirmed clinical diagnosis of CF who had been followed between 1990 and 1997; at diagnosis, 610 (82.2%) were exocrine pancreas insufficient (PI), 110 (14.8%) remained exocrine pancreas sufficient (PS), and 22 patients, who were PS at diagnosis, became PI during follow up (PS PI) 1 Among the 569 patients carrying two severe mutations, 546 (96.0%) were PI, while 61/62 (98%) with at least one mild mutation were PS A subset of patients with severe mutations on both alleles were PS at diagnosis but progressed to PI. Only four individuals (0.7%) with two severe mutations remained PS The correlation between CFTR mutation and pancreatic status is, however, incomplete: pancreatic insufficiency has been observed in some patients with CFTR mutations usually associated with pancreatic sufficiency. This may suggest that factors other than CFTR contribute to the maintenance of the PS state, like modifier genes 2 Genetic variation in SLC26A9 modifier gene, which encodes a bicarbonate and chloride transport protein that interacts with CFTR, is associated with cystic fibrosis-related diabetes (CFRD), and 3 additional type 2 diabetes loci also affect CFRD risk. 3 SLC26A9 was also recently shown to be associated with prenatal exocrine pancreatic damage as measured by newborn screened (NBS) immunoreactive trypsinogen (IRT) levels 4 References 1. Ahmed N et al. Gut. 2003;52: Cutting GR. Annu Rev Genomics Hum Genet. 2005;6: Blackman SM et al. Diabetes. 2013;62: Miller MR et al. J Pediatr. 2015;166:
11 11
12 12

13 The exocrine pancreas secretes digestive enzymes and sodium bicarbonate which are ultimately carried through the pancreatic duct into the duodenum 1 Digestive enzymes include α-amylase, lipase, DNase, RNase and the proenzymes trypsinogen, chymotrypsinogen, procarboxypeptidase A, procarboxypeptidase B, prophospholipase, proelastase, and mesotrypsin 1 The endocrine pancreas secretes hormones into the bloodstream, including insulin, somatostatin, and glucagon 2 References 1. Pandol SJ. The Exocrine Pancreas. San Rafael (CA): Morgan & Claypool Life Sciences; Begg DP, Woods SC. Adv Physiol Educ. 2013;37:
: Morgan & Claypool Life Sciences; 2010. Avisse C, Flament JB, Delattre JF. Surg Clin North Am.")
14 Pancreatic gross anatomy is depicted on this slide References Pandol SJ. The Exocrine Pancreas. San Rafael (CA): Morgan & Claypool Life Sciences; Avisse C, Flament JB, Delattre JF. Surg Clin North Am. 2000;80:

15 Acinar cells store digestive enzymes in forms that prevent destruction of intracellular structures and the acinar cells themselves. Some are stored as inactive proenzymes, others are packaged into acidic zymogen granules that are secreted 1 The lumen of the acini is connected to intercalated ducts, which drain into intralobular collecting ducts, which in turn drain into the main pancreatic duct 1 CFTR protein is located in the duct cell membrane and helps regulate ion and fluid secretion 2 References 1. Pandol SJ. The Exocrine Pancreas. San Rafael (CA): Morgan & Claypool Life Sciences; Macdonald KD et al. Pediatr Drugs. 2007;9:
 are the main inorganic constituents of pancreatic secretion; these constituents and their flow during a meal are necessary for")
16 Digestive enzymes include α-amylase, lipase, DNase, RNase and the proenzymes trypsinogen, chymotrypsinogen, procarboxypeptidase A, procarboxypeptidase B, prophospholipase, proelastase, and mesotrypsin Water and ions (sodium, potassium, chloride and bicarbonate) are the main inorganic constituents of pancreatic secretion; these constituents and their flow during a meal are necessary for transporting pancreatic enzymes secreted from the acinar cell to the intestinal lumen Another key function of pancreatic water and ion secretion is neutralization of gastric acid emptied into the duodenum Pancreatic enzymes have optimal activity at neutral ph, and are ineffective at the acid ph of gastric secretions Ductal secretion during the intestinal phase of the meal is much greater in volume than acinar secretion. The flow rate increases from an average rate of 0.2 or 0.3 ml/min in the resting state to 4.0 ml/min during stimulation of a meal. The total daily volume of secretion is about 2.5 L The concentration of bicarbonate increases dramatically during a meal with a reciprocal decrease in chloride; The exocrine pancreatic duct is unique in its ability to secrete a fluid with bicarbonate concentrations as great as 140 mm Reference Pandol SJ. The Exocrine Pancreas. San Rafael (CA): Morgan & Claypool Life Sciences;
17 17
18 Direct harvesting of pancreatic secretions is possible, but invasive and requires duodenal intubation 1 The 72-hour quantitative fecal fat balance study measures pancreatic function by determining coefficient of fat absorption 2 Patients must not be taking pancreatic enzyme supplements (PERT) during the test period. Fat intake must be carefully recorded during the test period 3 Two proxies are often used for pancreatic function: Serum immunoreactive trypsinogen is a useful tool to define PI in patients older than 7 years of age, 4 but the mean age of diagnosis of patients is 3.7 years (median, 4 months) 5 A human monoclonal or polyclonal ELISA test for Fecal Elastase 1 References 1. Daftary A et al. J Cyst Fibros. 2006;5: Borowitz D et al. J Pediatr Gastro Nutr. 2007;44: O Sullivan BP et al. J Pediatr. 2013;162: Durie PR et al. Pediatr Res. 1986;20: CFF Patient Registry 2013 Annual Data Report to the Center Directors. Bethesda, MD: 2014 CFF. 18

19 For research purposes, the 72-hour quantitative fecal fat balance test involves 1 : 3 days of a high-fat diet (100mg fat/d or 60 g fat/m 2 ) controlled and measured by a research dietitian Stool collection between the appearance of 2 orally ingested dye markers to mark the beginning and end of the controlled high-fat diet Fecal fat analysis performed in a central laboratory The formula used to calculate the coefficient of fat absorption is: (grams of fat consumed - grams of fat excreted) X100 grams of fat consumed In a head-to-head comparison, the 72-hour fecal fat balance test was more sensitive and more specific than the fecal elastase and immunoreactive trypsinogen tests for distinguishing between pancreatic insufficiency and pancreatic sufficiency 2 References 1. Borowitz D et al. J Pediatr Gastro Nutr. 2007;44: Weintraub A et al. J Pediatr Gastroenterol Nutr. 2009;48:
20 20

21 Fecal elastase is detected using ELISA using either monoclonal or polyclonal antibodies 1 and levels of fecal elastase below 100 µg/g of stool indicate pancreatic insufficiency 1 Monoclonal antibody test can be performed while patients are taking exogenous PERT because the human monoclonal elastase antibody does not cross-react with porcine elastase 2 Limitations of the fecal elastase test 1 : Polyclonal antibodies react with some as yet unknown antigen associated with elastase. Falsely elevated E1 levels may be detected when using the polyclonal antibody test even in the presence of clinical steatorrhea Care should be taken in interpreting values from diarrheal stools and in the presence of intestinal inflammation or enteropathy as underestimation of true E1 levels may result Intestinal inflammation can cause low enzyme levels, which may take several months to recover It is unable to distinguish primary exocrine pancreatic insufficiency from exocrine insufficiency secondary to intestinal villous damage References 1. Daftary A et al. J Cyst Fibros. 2006;5: Borowitz D et al. J Pediatr Gastro Nutr. 2007;44:
22 To produce active trypsin, the cells that line the duodenum secrete an enzyme, enteropeptidase, that hydrolyzes a unique lysineisoleucine peptide bond in trypsinogen as the zymogen (inactive precursor or proenzyme) enters the duodenum from the pancreas. The small amount of trypsin produced in this way activates more trypsinogen and the other zymogens The digestion of proteins in the duodenum requires the concurrent action of several proteolytic enzymes, because each is specific for a limited number of side chains. Thus, the zymogens must be switched on at the same time Coordinated control is achieved by the action of trypsin as the common activator of all the pancreatic zymogens trypsinogen, chymotrypsinogen, proelastase, procarboxypeptidase, and prolipase, a lipid degrading enzyme Thus, the formation of trypsin by enteropeptidase is the master activation step Reference Berg JM, Tymoczko JL, Stryer L (eds). Chapter 10.5 In: Biochemistry. 5th Edition. New York (NY): W H Freeman;

23 The mechanism by which trypsinogen enters the systemic circulation remains unknown Inspissated protein plugging of small pancreatic ductules is thought to be a consequence of diminished fluid output resulting from protein hyperconcentration, ductal stasis, and protein precipitation. Regurgitant release of trypsinogen into the circulation from obstructed acinar-ductular units may be an end result of this process Alternatively, increased serum levels of cationic trypsinogen may reflect increased ductular concentrations of pancreatic enzymes, with back diffusion into the systemic circulation The high serum trypsinogen levels in infants with PI and CF probably reflect the presence of functional acini proximal to obstructed ductules Reference Couper RT et al. J Pediatr. 1995;127:
24 The IRT test can be done with random blood samples 1 An enzyme immunoassay (EIA) with monoclonal antibodies against human trypsinogen in neonatal bloodspots has been evaluated for screening for neonatal CF, and found to be quicker and less labor intensive than conventional assays for the detection of immunoreactive trypsin 2 References 1. Durie PR et al. Pediatr Res. 1986;20: Bowling FG et al. Lancet. 1987;1:
25 These data came from a study of 381 children with CF and 99 healthy controls conducted at the Hospital for Sick Children, Toronto, between 1981 and 1983 CF patients had known pancreatic status based on fecal fat balance studies or direct pancreatic stimulation Figures show the least squares mean and 95% confidence intervals that were modeled from the data derived from the 314 patients with pancreatic insufficiency. On the left, the data from those patients is plotted. On the right, the data from the pancreatic sufficient patients is plotted The non-cf range ( pg/liter) is shaded The results show that after age 7, the IRT curves distinguished PS from PI patients Reference Durie PR et al. Pediatr Res. 1986;20:
26 Wireless motility capsule (WMC) System Measures ph and transit time Use of ph capsule devise is limited in young children and infants due to its size Reference Bodewes FA et al. J Cyst Fibros. 2015;14:
27 This pilot study was conducted in 10 subjects with CF and pancreatic insufficiency, and 10 controls matched for sex, age, and BMI Subjects swallowed the wireless motility capsule and carried a receiver to track duodenal ph Following an overnight fast, eligible subjects ate a standardized low fat meal bar and swallowed the WMC with water. CF subjects took half their usual enzyme dose with the meal bar Analysis of CF subjects matched to the controls yielded statistically significant results with time required to reach and sustain ph of 5.5 in CF vs. control subjects (17.7 ± 6.8 vs. 6.3 ± 6.4 min, respectively; p<0.001) and time required to reach and sustain ph of 6.0 in CF vs. control subjects (42.2 ± 23.1 vs ± 17.1 min, respectively; p<0.001) Reference Gelfond D et al. Dig Dis Sci. 2013;58:
 are analyzed using ELISA method 2 According to one proposed screening strategy (France), all newborns are tested for IRT. Newborns with IRT > 50 ng/ml are tested for PAP.")
28 PAP is proposed as a less costly and invasive alternative to the DNA testing or IRT retesting after the initial elevated IRT test results in newborns 1,2 Blood from neonatal samples (pinpricks/bloodspots) are analyzed using ELISA method 2 According to one proposed screening strategy (France), all newborns are tested for IRT. Newborns with IRT > 50 ng/ml are tested for PAP. Those with PAP > 1.8 ng/ml and those with PAP >1.0 ng/ml and IRT > 100 ng/ml are recalled for sweat testing 2 References 1. Sarles J et al. Arch Dis Child Fetal Neonatal Ed. 1999;80:F118-F Sarles J. et al. J Pediatr. 2005;147:
29 29
 to maintain a more alkaline ph inside the lumen of the ducts 1 Pancreatic secretions contain digestive enzymes that flow from the pancreatic duct into")
30 Under normal conditions in the pancreas, CFTR channels secrete Cl into the lumen of pancreatic ducts to maintain the appropriate fluid volume of pancreatic secretions. These channels also secrete HCO 3 (bicarbonate) to maintain a more alkaline ph inside the lumen of the ducts 1 Pancreatic secretions contain digestive enzymes that flow from the pancreatic duct into the small intestine to properly break down nutrients 1 In CF disease, dysfunction of CFTR channels leads to defective HCO 3 and Cl secretion into the ducts of the pancreas. This impairs the fluid and ph balance of secretions containing digestive enzymes 1-3 As a result, pancreatic secretions become reduced in volume and more acidic, obstructing the pancreatic ducts. This causes progressive damage to the pancreas and may lead to nutrient malabsorption, malnutrition, failure to thrive, and reliance on enzyme replacement therapy 1,2 Pancreatic damage is thought to occur, in part, because inadequate HCO 3 secretion creates an acid environment inside the pancreatic ducts. This acidic environment, normally reached when the digestive enzymes are secreted into the small intestine, begins to prematurely activate digestive enzymes 3 This causes proteolysis (digestion of pancreatic proteins) and inflammation that destroys the exocrine pancreas 3 References 1. Wilschanski M et al. Gut. 2007;56: Walkowiak J et al. Eur J Gastroenterol Hepatol. 2008;20: Quinton PM. Acta Physiologica Sinica. 2007;59:
, and associated increased protein concentration in secretions 1 As a consequence of secretion precipitation, early pathology of duct plugging and dilatation and inflammation occur.")
31 In the pancreas, loss of CFTR gene can lead to progressive deterioration of structure and function 1 The physiological effects of defective CFTR in pancreas are reduced volume of secretions (fluid and bicarbonate), and associated increased protein concentration in secretions 1 As a consequence of secretion precipitation, early pathology of duct plugging and dilatation and inflammation occur. 1 Later, fibrosis and fatty replacement of tissue and atrophy occur The clinical picture includes pancreatic insufficiency if the damage is severe, pancreatitis, and with sufficient loss of islets, cysticfibrosis related diabetes (CFRD) may develop 2 References 1. Wilschanski M, Novak I. Cold Spring Harb Perspect Med. 2013;3:a Moran A et al. Pediatr Diabetes. 2014;15(Suppl 20):
32 Data on timing of pancreatic insufficiency are from a longitudinal evaluation of pancreatic function in patients with CF based on fecal elastase values measured during the first year of life. 1 The evaluable cohort of 61 infants provided their first stool sample for testing before age 3.5 months and their final sample at age 9 months to ensure that assessment of changes in fecal elastase occurring over the entire first year of life 48 of these infants had an initial fecal elastase value <200 µg/g indicating pancreatic insufficiency, and an additional 3 had a starting value above 200 and ending value <200 µg/g, indicating that about 84% of infants in this study were PI within the first year of life A cutoff of 2% of functioning pancreas for pancreatic sufficiency was shown in a study of 24 patients with steatorrhea (fecal fat excretion > 7% of fat intake) and 54 patients with normal fat absorption. 2 The 24 patients with steatorrhea included 3 patients aged 5-12 yr with Shwachman syndrome (exocrine pancreatic hypoplasia and neutropenia), 1 patient aged 1.5 yr with pancreatic hypoplasia of unknown etiology, and 20 patients aged yr with cystic fibrosis All patients were assessed with direct pancreas stimulation; any pancreatic supplementation was stopped 48 hours before the study Development issues with exocrine pancreas were evaluated in a retrospective study in 60 pancreatic autopsy specimens of infants who died within 4 months of birth, collected over a period of 25 years. 3 Subjects were included in 1 of 3 groups: Group 1: 29 control subjects with no evidence of CF or of any pancreatic involvement in the cause of death Group 2: 24 subjects with a history of meconium ileus and exocrine changes compatible with cystic fibrosis, based on the examination of at least three organ systems Group 3: 7 subjects with pathologic findings compatible with CF and with no history of meconium ileus Control subjects: Ratio of acinar to connective tissue increased 4-fold from birth to 4 months Lumenal volume =0.2% of pancreas volume, not age-dependent CF subjects Ratio of acinar to connective tissue diminished progressively with age 83% of cases had lumenal volume >0.5% of pancreas volume Similar failure of acinar development in CF subjects with meconium ileus and pulmonary failure as cause of death References 1. O Sullivan BP et al. J Pediatr. 2013;162: Gaskin KJ et al. Gastroenterol. 1984;86: Imrie J et al. Am J Path. 1979;95:

33 The study by Augarten et al was an Israeli cohort study of 505 CF patients, 139 of whom were pancreatic sufficient, 366 were pancreatic insufficient, and 4 were PS who converted to PI during the period in their charts 1 Pancreatitis was diagnosed based on episodes of abdominal pain associated with elevation of serum amylase or serum pancreatic lipase levels The study by Ooi et al looked at CF patients from the Canadian Consortium for CF Genetic Studies and Verona CF Centre databases and identified 277 who were PS and met inclusion criteria 2 Pancreatitis was diagnosed by abdominal pain (with no other attributable cause) in association with (1) elevated serum amylase and/or lipase level (>2 x ULN) and/or (2) imaging evidence of acute (such as pancreatic edema, hemorrhage, or necrosis) or chronic (such as calcification or characteristic ductal changes) The study by Durno et al was a cohort study involving 1075 patients with CF in a regional referral center database with acute recurrent or chronic pancreatitis over a 30-year period ( ) 3 Pancreatitis was diagnosed if a patient experienced an acute episode of abdominal pain in association with elevated serum amylase level ( 1.5 x ULN) provided the pain could not be attributed to another cause References 1. Augarten A et al. Eur J Gastroenterol Hepatol. 2008;20: Ooi CY et al. Gastroenterol. 2011;140: Durno G et al. Gastroenterol. 2002;123:
34 34
35 35

36 Anatomic studies demonstrate that the blood flow from the endocrine pancreas enters the capillaries of the exocrine tissue surrounding each of the islets before entering the general circulation This "portal" system provides for the delivery of very high concentrations of hormones from the islets of Langerhans to the exocrine tissue surrounding the Islets The hormones from the islets of Langerhans include insulin, and although the full significance of the effects of these hormones on the exocrine pancreas is not known, the acinar cells of the pancreas have insulin receptors that are involved in regulation of digestive enzyme synthesis of the exocrine pancreas Reference Pandol SJ. The Exocrine Pancreas. San Rafael (CA): Morgan & Claypool Life Sciences;

37 Islet cells include β-cells that secrete insulin and amylin, α-cells that secrete glucagon, δ-cells that secrete somatostatin, ε-cells that secrete ghrelin, and F-cells that secrete pancreatic polypeptide 1 Insulin s best known action is to stimulate glucose transporters in cell membranes of most peripheral tissues to activate glucose uptake into the cells for use as fuel or storage as glycogen 1 Glucagon functions as a counter-regulatory hormone to insulin, increasing blood glucose by stimulating glycogenolysis and gluconeogenesis 2 Amylin produces a reduction in eating, gastric acid and glucagon secretion, and limits the rate of gastric emptying 3 Somatostatin inhibits a wide range of endocrine secretions, from the pituitary (growth hormone, prolactin and thyrotropin), gastrointestinal tract (cholecystokinin, gastric inhibitory peptide, gastrin, motilin, neurotensin and secretin) and pancreas (glucagon, insulin and pancreatic polypeptide). It is also a transmitter and neuromodulator in the nervous system 4 Ghrelin increases growth hormone release and stimulates appetite, and also causes a slight increase in glucose levels and reduction in circulating insulin 5 Pancreatic polypeptide inhibits gastric emptying, which may account for its ability to reduce appetite; it can also inhibit intestinal electrolyte and water secretion, and has an inhibitory action on intestinal motor activity and peristalsis 6 References 1. Begg DP, Woods SC. Adv Physiol Educ. 2013;37: Charron MJ, Vuguin PM. J Endocrinol. 2015;224:R123-R Lutz TA. Am J Physiol Regul Integr Comp Physiol. 2010;298:R1475-R Krantic S et al. Eur J Endocrinol. 2004;151: Lengyel AM. Braz J Med Biol Res. 2006;39: Holzer P et al. Neuropeptides. 2012;46:
38 38
39 The oral glucose tolerance test is preferred for CFRD based on poor performance of other tests in this population, data linking OGTT with clinical outcomes, and the importance of detecting CFRD early, when fasting glucose levels are still normal Hemoglobin A1c is a measure of glycated hemoglobin in the blood, and therefore gives a measure of the average blood glucose level over the past 3 months, based on the turnover time of erythrocytes 2 Hemoglobin A1c is not sensitive enough to use as a screening test for CFRD 3 Low or normal HbA1c levels do not exclude the diagnosis of CFRD because HbA1c is often spuriously low in CF. This has been postulated to be due to increased red blood cell turnover related to inflammation 1 References 1. Moran A et al. Pediatr Diabetes. 2014;15(Suppl 20): National Clearinghouse of Diabetes Information. The A1C Test and Diabetes. Available at Accessed March 17, Moran A et al. Diabetes Care. 2010;33:

40 Testing should be done on 2 separate days to rule out laboratory error unless there are unequivocal symptoms of hyperglycemia (polyuria and polydipsia) A positive FPG or A1c can be used as a confirmatory test, but if it is normal the OGTT should be performed or repeated Reference Moran A et al. Diabetes Care. 2010;33:
41 41

42 Several hypotheses have been proposed for the mechanism of CFRD pathogenesis: Pancreatic destruction leads to loss if islet cells, fibrosis and amyloid deposits in islets 1 Defective CFTR activity led to insufficient depolarization and Ca 2+ mobilization in response to glucose in cultured beta cells 2 β-cells synthesize large amounts of protein. Chronic accumulation of misfolded CFTR may overwhelm the β-cell proteolytic degradation pathways leading to sustained endoplasmic reticulum stress responses (unfolded protein response, endoplasmic reticulum-associated protein degradation) and β-cell apoptosis 3 A chronic inflammatory state produced by oxidative stress, ROS production, 4 elevated pro-inflammatory cytokines, 1 defective fat-soluble antioxidant absorption, and possibly vitamin D deficiency contribute to β-cell destruction and dysfunction and insulin resistance 1,4 Insulin sensitivity is normal in patients with CF in most studies, 1,5 and in studies showing reduced insulin sensitivity, issues of study populations, methods, and interpretation may be factors 5 Insulin resistance in CF may develop because of abnormal localization of the GLUT-4 glucose transporter and/or elevated TNF-α levels 6 References 1. Barrio R. Eur J Endocrinol. 2015;172:R131-R Guo JH et al. Nat Commun. 2014;5: Ali BR. Med Hypotheses. 2009;72: Galli F et al. Biochimica et Biophysica Acta. 2012;1822: Mohan K et al. Diabet Med. 2009;26: Hardin DS et al. Am J Physiol Endocrinol Metab. 2001;281:E1022-E
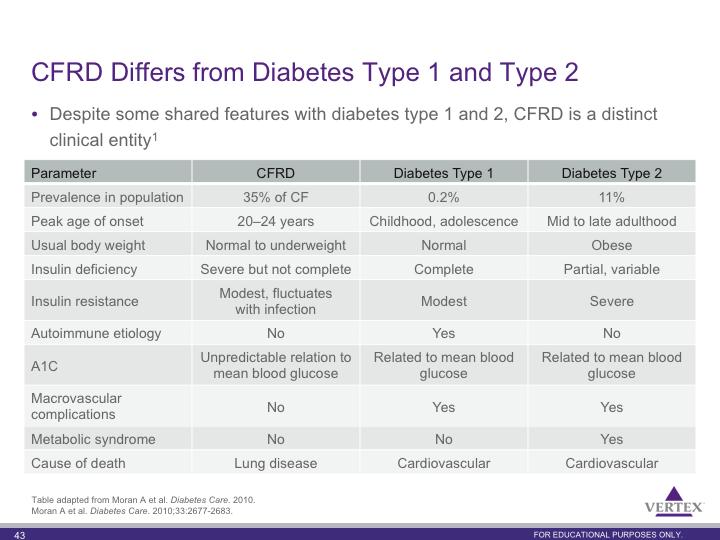
43 43
44 44

45 A number of clinical consequences of pancreatic insufficiency have been documented, including steatorrhea, fat-soluble vitamin deficiency, nutrient malabsorption leading to malnutrition, weight loss and failure to thrive, lung function decline, and increased mortality 1-3 Development of CFRD may also occur, and is associated with protein catabolism, lung function decline and increased mortality such that these conditions will be worse in patients with PI and CFRD 4 References 1. O Sullivan BP, Freedman SD. Lancet. 2009;373: Cystic Fibrosis Foundation. Patient Registry 2013 Annual Data Report to the Center Directors. Bethesda, MD Schaedel C et al. Pediatr Pulmonol. 2002;33: Davis PB et al. Pediatr Pulmonol. 2004;38: Moran A et al. Diabetes Care. 2010;33:
46 Key Points In cystic fibrosis, nutritional deficiency is common due to pancreatic insufficiency and malabsorption. 1 Evidence shows that growth and nutritional status is strongly associated with pulmonary function in children with cystic fibrosis 2,3 Patient Registry data show a strong association between a higher BMI percentile and better lung function in children with CF 2 The graph above on the left shows the association between higher BMI percentile and better lung function in children ages 6 through 19 years. The bar in the middle is the BMI 50th percentile goal for children with CF 2 Shown in the figure on the right, relative weight gain from age 3 to 6 was associated with improved pulmonary function at age 6 (when FEV 1 becomes a reliable measure) 3 Data suggest that early nutritional intervention may improve pulmonary health 2,3 Additional Information A large cohort of patients were prospectively followed and evaluated for growth indexes and pulmonary health measures between age 3 and 6 2 Data revealed that patients with lower growth indexes at age 3 had lower pulmonary function at age 6. This was strongest for measures of weight for age 2 As shown in the figure, relative weight gain from age 3 to 6 was also associated with better pulmonary function at age 6 2 Children whose weight for age was greater than the 10th percentile at age 3 and remained greater than the 10th percentile at age 6 had the highest FEV 1 scores Conversely, patients whose weight for age was less than the 10th percentile at age 3 and remained less than the 10th percentile at age 6 had the lowest FEV 1 scores References 1. O Sullivan BP, Freedman SD. Lancet. 2009;373: Konstan et al. J Pediatr. 2003;142: Cystic Fibrosis Foundation. Patient Registry 2013 Annual Data Report to the Center Directors. Bethesda, MD
47 Occurrence of abnormal glucose and CFRD was assessed in patients recruited during a longitudinal, prospective, multicenter study on Early Diagnosis of Diabetes Mellitus in Patients with Cystic Fibrosis (Trial No. NCT ) carried out between 2001 and 2010 in 43 specialized centers (40 German, 3 Austrian) 1 Standardized OGTTs performed to screen serially for CFRD starting at age 10. In case of a pathological OGTT, testing was repeated: according to study protocol, a diabetic OGTT was to be repeated after 4 to 6 weeks and an OGTT revealing impaired glucose tolerance (IGT) or impaired fasting glucose (IFG) was to be repeated after 6 months The final study population comprised 5,179 oral glucose tolerance tests performed in 1,658 cystic fibrosis patients Prevalence of CFRD was evaluated based on a total of 527 patients followed at the University of Minnesota Cystic Fibrosis Center on 15 September Routine annual OGTT screening has been recommended at the University of Minnesota since the early 1990s for patients aged 6 years (1.75 g/kg glucose [maximum 75g]). OGTTs are performed when patients are in their usual baseline state of health References 1. Scheuing N et al. PLoS ONE. 2013;8:e Moran A et al. Diabetes Care. 2009;32:
48 Key Point Patients with CF and mutations associated with pancreatic sufficiency (PS) have a better survival rate than those homozygous for the F508del mutation, 98% of whom are PI 1,2 Notes The clinical impact of CFTR protein activity can be illustrated by the impact of pancreatic manifestations of CFTR impairment on patient survival. Pancreatic sufficiency is associated with lesser impairment of CFTR protein function, whereas PI is associated with greater impairment. 3 In a study of patients with CF (N=264), those with PS had a significantly better survival rate compared with those who were homozygous for F508del-CFTR (P=0.0083) 2 References 1. CFTR2.org F508del mutation details. Accessed 5/15/ Davis PB et al. Pediatr Pulmonol. 2004;38: Ahmed N et al. Gut. 2003;52:
49 49
Week 3 The Pancreas: Pancreatic ph buffering:
 Week 3 The Pancreas: A gland with both endocrine (secretion of substances into the bloodstream) & exocrine (secretion of substances to the outside of the body or another surface within the body) functions
Week 3 The Pancreas: A gland with both endocrine (secretion of substances into the bloodstream) & exocrine (secretion of substances to the outside of the body or another surface within the body) functions
6.2.1 Exocrine pancreatic insufficiency
 6.2.1 Exocrine pancreatic insufficiency Authors: Jean Louis Frossard, Alain Sauty 1. INTRODUCTION Exocrine pancreatic insufficiency is a biological and clinical condition that is characterized by a progressive
6.2.1 Exocrine pancreatic insufficiency Authors: Jean Louis Frossard, Alain Sauty 1. INTRODUCTION Exocrine pancreatic insufficiency is a biological and clinical condition that is characterized by a progressive
Pancreas Fox Chapter 18 part 2 (also Chapter 19.3 & 19.4)
") Vert Phys PCB3743 Pancreas Fox Chapter 18 part 2 (also Chapter 19.3 & 19.4) T. Houpt, Ph.D. Anatomy of Digestive System Peristalsis Stomach and Acid Secretion Liver and Bile Secretion Pancreas and pancreatic
Vert Phys PCB3743 Pancreas Fox Chapter 18 part 2 (also Chapter 19.3 & 19.4) T. Houpt, Ph.D. Anatomy of Digestive System Peristalsis Stomach and Acid Secretion Liver and Bile Secretion Pancreas and pancreatic
Chapter 15 Gastrointestinal System
 Chapter 15 Gastrointestinal System Dr. LL Wang E-mail: wanglinlin@zju.edu.cn Rm 608, Block B, Research Building, School of Medicine, Zijingang Campus Pancreatic Secretion The exocrine cells in the pancreas
Chapter 15 Gastrointestinal System Dr. LL Wang E-mail: wanglinlin@zju.edu.cn Rm 608, Block B, Research Building, School of Medicine, Zijingang Campus Pancreatic Secretion The exocrine cells in the pancreas
Diseases of exocrine pancreas
 Diseases of exocrine pancreas The exocrine pancreas constitutes 80% to 85% of the organ and is composed of acinar cells that secrete enzymes needed for digestion. the accessory duct of Santorini, the main
Diseases of exocrine pancreas The exocrine pancreas constitutes 80% to 85% of the organ and is composed of acinar cells that secrete enzymes needed for digestion. the accessory duct of Santorini, the main
History of Investigation
 Acini - Pancreatic juice (1º) (2º) Secretions- neuronal and hormonal mechanisms 1) Secretin - bicarbonate rich 2) Cholecystokinin - enzyme rich Islets of Langerhans (contain 4 cell types) Alpha cells (α)-
Acini - Pancreatic juice (1º) (2º) Secretions- neuronal and hormonal mechanisms 1) Secretin - bicarbonate rich 2) Cholecystokinin - enzyme rich Islets of Langerhans (contain 4 cell types) Alpha cells (α)-
Physiology Unit 4 DIGESTIVE PHYSIOLOGY
 Physiology Unit 4 DIGESTIVE PHYSIOLOGY In Physiology Today Functions Motility Ingestion Mastication Deglutition Peristalsis Secretion 7 liters/day! Exocrine/endocrine Digestion Absorption Digestion of
Physiology Unit 4 DIGESTIVE PHYSIOLOGY In Physiology Today Functions Motility Ingestion Mastication Deglutition Peristalsis Secretion 7 liters/day! Exocrine/endocrine Digestion Absorption Digestion of
The Digestive System. What is the advantage of a one-way gut? If you swallow something, is it really inside you?
 The Digestive System What is the advantage of a one-way gut?! If you swallow something, is it really inside you? Functions and Processes of the Digestive System: Move nutrients, water, electrolytes from
The Digestive System What is the advantage of a one-way gut?! If you swallow something, is it really inside you? Functions and Processes of the Digestive System: Move nutrients, water, electrolytes from
Diagnosis of chronic Pancreatitis. Christoph Beglinger, University Hospital Basel, Switzerland
 Diagnosis of chronic Pancreatitis Christoph Beglinger, University Hospital Basel, Switzerland Pancreatitis Pancreas Pancreas - an organ that makes bicarbonate to neutralize gastric acid, enzymes to digest
Diagnosis of chronic Pancreatitis Christoph Beglinger, University Hospital Basel, Switzerland Pancreatitis Pancreas Pancreas - an organ that makes bicarbonate to neutralize gastric acid, enzymes to digest
CYSTIC FIBROSIS (CF) COMPLICATIONS BEYOND THE LUNGS. A Resource for the CF Center Care Team
 COMPLICATIONS BEYOND THE LUNGS. A Resource for the CF Center Care Team") CYSTIC FIBROSIS (CF) COMPLICATIONS BEYOND THE LUNGS A Resource for the CF Center Care Team Vertex Pharmaceuticals Incorporated, 50 Northern Avenue, Boston, MA 02210. Vertex and the Vertex triangle logo
CYSTIC FIBROSIS (CF) COMPLICATIONS BEYOND THE LUNGS A Resource for the CF Center Care Team Vertex Pharmaceuticals Incorporated, 50 Northern Avenue, Boston, MA 02210. Vertex and the Vertex triangle logo
Insulin and the brain. Mary ET Boyle, Ph. D. Department of Cognitive Science UCSD
 Insulin and the brain Mary ET Boyle, Ph. D. Department of Cognitive Science UCSD 1921 Banting & Macleod Nobel Prize 1923 White, M. F. (2003) Science Berg, J. M., Tymoczko, J. L. and Stryer, L. (2007) Biochemistry
Insulin and the brain Mary ET Boyle, Ph. D. Department of Cognitive Science UCSD 1921 Banting & Macleod Nobel Prize 1923 White, M. F. (2003) Science Berg, J. M., Tymoczko, J. L. and Stryer, L. (2007) Biochemistry
1-It is to prevent back flow of fecal content from colon into small intestine.
 Function of the ileocecal valve: 1-It is to prevent back flow of fecal content from colon into small intestine. 2-The wall of the ileum for several centimeters preceding valve has a thickened muscular
Function of the ileocecal valve: 1-It is to prevent back flow of fecal content from colon into small intestine. 2-The wall of the ileum for several centimeters preceding valve has a thickened muscular
Chapter 3 The Role of Nutrition in CF Care
 Chapter 3 The Role of Nutrition in CF Care S. King, N. Saxby & N. Sander Cystic fibrosis is the most common lethal autosomal recessive genetic condition affecting Caucasians 186,187. Over 3500 Australians
Chapter 3 The Role of Nutrition in CF Care S. King, N. Saxby & N. Sander Cystic fibrosis is the most common lethal autosomal recessive genetic condition affecting Caucasians 186,187. Over 3500 Australians
Advances in CF therapies and their effect on GI manifestations. Presenter Disclosure Daniel Gelfond, MD Relationship related to this presentation
 Advances in CF therapies and their effect on GI manifestations Daniel Gelfond, MD University of Rochester WNY Pediatric Gastroenterology Presenter Disclosure Daniel Gelfond, MD Relationship related to
Advances in CF therapies and their effect on GI manifestations Daniel Gelfond, MD University of Rochester WNY Pediatric Gastroenterology Presenter Disclosure Daniel Gelfond, MD Relationship related to
DIGESTIVE. CHAPTER 17 Lecture: Part 1 Part 2 BIO 212: ANATOMY & PHYSIOLOGY II
 BIO 212: ANATOMY & PHYSIOLOGY II CHAPTER 17 Lecture: DIGESTIVE Part 1 Part 2 Dr. Lawrence G. Altman www.lawrencegaltman.com Some illustrations are courtesy of McGraw-Hill. SMALL INTESTINE DUODENUM > JEJUNUM
BIO 212: ANATOMY & PHYSIOLOGY II CHAPTER 17 Lecture: DIGESTIVE Part 1 Part 2 Dr. Lawrence G. Altman www.lawrencegaltman.com Some illustrations are courtesy of McGraw-Hill. SMALL INTESTINE DUODENUM > JEJUNUM
A Quick Guide to the. I507del. Mutation CFTR SCIENCE
 A Quick Guide to the I507del Mutation CFTR SCIENCE 2016 Vertex Pharmaceuticals Incorporated VXR-HQ-02-00045a(1) 03/2016 Loss of CFTR activity is the underlying cause of cystic fibrosis (CF) 1 Spectrum
A Quick Guide to the I507del Mutation CFTR SCIENCE 2016 Vertex Pharmaceuticals Incorporated VXR-HQ-02-00045a(1) 03/2016 Loss of CFTR activity is the underlying cause of cystic fibrosis (CF) 1 Spectrum
THE ROLE OF CFTR MUTATIONS IN CAUSING CYSTIC FIBROSIS (CF)
") THE ROLE OF CFTR MUTATIONS IN CAUSING CYSTIC FIBROSIS (CF) Vertex Pharmaceuticals Incorporated, 50 Northern Avenue, Boston, MA 02210. Vertex and the Vertex triangle logo are registered trademarks for Vertex
THE ROLE OF CFTR MUTATIONS IN CAUSING CYSTIC FIBROSIS (CF) Vertex Pharmaceuticals Incorporated, 50 Northern Avenue, Boston, MA 02210. Vertex and the Vertex triangle logo are registered trademarks for Vertex
Cystic Fibrosis. Jennifer McDaniel, BS, RRT-NPS
 Cystic Fibrosis Jennifer McDaniel, BS, RRT-NPS Overview Cystic fibrosis is the most common fatal, inherited disease in the U. S. CF results from a defective autosomal recessive gene One copy of gene =
Cystic Fibrosis Jennifer McDaniel, BS, RRT-NPS Overview Cystic fibrosis is the most common fatal, inherited disease in the U. S. CF results from a defective autosomal recessive gene One copy of gene =
Respiratory Pharmacology: Treatment of Cystic Fibrosis
 Respiratory Pharmacology: Treatment of Cystic Fibrosis Dr. Tillie-Louise Hackett Department of Anesthesiology, Pharmacology and Therapeutics University of British Columbia Associate Head, Centre of Heart
Respiratory Pharmacology: Treatment of Cystic Fibrosis Dr. Tillie-Louise Hackett Department of Anesthesiology, Pharmacology and Therapeutics University of British Columbia Associate Head, Centre of Heart
Anatomy of the biliary tract
 Harvard-MIT Division of Health Sciences and Technology HST.121: Gastroenterology, Fall 2005 Instructors: Dr. Jonathan Glickman Anatomy of the biliary tract Figure removed due to copyright reasons. Biliary
Harvard-MIT Division of Health Sciences and Technology HST.121: Gastroenterology, Fall 2005 Instructors: Dr. Jonathan Glickman Anatomy of the biliary tract Figure removed due to copyright reasons. Biliary
"Management and Treatment of Patients with Cystic fibrosis (CF)
") "Management and Treatment of Patients with Cystic fibrosis (CF) Dr. Malena Cohen-Cymberknoh Pediatric Pulmonology and CF Center Hadassah Hebrew-University Medical Center Jerusalem, Israel Afula, March
"Management and Treatment of Patients with Cystic fibrosis (CF) Dr. Malena Cohen-Cymberknoh Pediatric Pulmonology and CF Center Hadassah Hebrew-University Medical Center Jerusalem, Israel Afula, March
Ali Yaghi. Yaseen Fatayer. M.Khatatbeh
 6 Ali Yaghi Yaseen Fatayer M.Khatatbeh P a g e 1 pancreatic secretions note: The pancreas has endocrine (secretions are released toward the blood) and exocrine(secretions are released through the canalicular
6 Ali Yaghi Yaseen Fatayer M.Khatatbeh P a g e 1 pancreatic secretions note: The pancreas has endocrine (secretions are released toward the blood) and exocrine(secretions are released through the canalicular
Soft palate elevates, closing off the nasopharynx. Hard palate Tongue Bolus Epiglottis. Glottis Larynx moves up and forward.
 The Cephalic Phase Chemical and mechanical digestion begins in the mouth Saliva is an exocrine secretion Salivary secretion is under autonomic control Softens and lubricates food Chemical digestion: salivary
The Cephalic Phase Chemical and mechanical digestion begins in the mouth Saliva is an exocrine secretion Salivary secretion is under autonomic control Softens and lubricates food Chemical digestion: salivary
18. PANCREATIC FUNCTION AND METABOLISM. Pancreatic secretions ISLETS OF LANGERHANS. Insulin
 18. PANCREATIC FUNCTION AND METABOLISM ISLETS OF LANGERHANS Some pancreatic functions have already been discussed in the digestion section. In this one, the emphasis will be placed on the endocrine function
18. PANCREATIC FUNCTION AND METABOLISM ISLETS OF LANGERHANS Some pancreatic functions have already been discussed in the digestion section. In this one, the emphasis will be placed on the endocrine function
Section Coordinator: Jerome W. Breslin, PhD, Assistant Professor of Physiology, MEB 7208, ,
 IDP Biological Systems Gastrointestinal System Section Coordinator: Jerome W. Breslin, PhD, Assistant Professor of Physiology, MEB 7208, 504-568-2669, jbresl@lsuhsc.edu Overall Learning Objectives 1. Characterize
IDP Biological Systems Gastrointestinal System Section Coordinator: Jerome W. Breslin, PhD, Assistant Professor of Physiology, MEB 7208, 504-568-2669, jbresl@lsuhsc.edu Overall Learning Objectives 1. Characterize
Gastrointestinal Anatomy and Physiology. Bio 219 Napa Valley College Dr. Adam Ross
 Gastrointestinal Anatomy and Physiology Bio 219 Napa Valley College Dr. Adam Ross Functions of digestive system Digestion Breakdown of food (chemically) using enzymes, acid, and water Absorption Nutrients,
Gastrointestinal Anatomy and Physiology Bio 219 Napa Valley College Dr. Adam Ross Functions of digestive system Digestion Breakdown of food (chemically) using enzymes, acid, and water Absorption Nutrients,
ENERGY FROM INGESTED NUTREINTS MAY BE USED IMMEDIATELY OR STORED
 QUIZ/TEST REVIEW NOTES SECTION 1 SHORT TERM METABOLISM [METABOLISM] Learning Objectives: Identify primary energy stores of the body Differentiate the metabolic processes of the fed and fasted states Explain
QUIZ/TEST REVIEW NOTES SECTION 1 SHORT TERM METABOLISM [METABOLISM] Learning Objectives: Identify primary energy stores of the body Differentiate the metabolic processes of the fed and fasted states Explain
Control of Glucose Metabolism
 Glucose Metabolism Control of Glucose Metabolism The pancreas is both an exocrine and endocrine gland. It secretes digestive enzymes into the duodenum (exocrine) and 3 specific hormones into the bloodstream
Glucose Metabolism Control of Glucose Metabolism The pancreas is both an exocrine and endocrine gland. It secretes digestive enzymes into the duodenum (exocrine) and 3 specific hormones into the bloodstream
Focus on Cystic Fibrosis. Cystic Fibrosis. Cystic Fibrosis
 Focus on (Relates to Chapter 29, Nursing Management: Obstructive Pulmonary Diseases, in the textbook) Copyright 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. Autosomal recessive, multisystem
Focus on (Relates to Chapter 29, Nursing Management: Obstructive Pulmonary Diseases, in the textbook) Copyright 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. Autosomal recessive, multisystem
Pediatrics Grand Rounds 18 Sept University of Texas Health Science Center. + Disclosure. + Learning Objectives.
 Disclosure Dr Donna Willey Courand receives research support from Cystic Fibrosis Therapeutics The Cystic Fibrosis Foundation Children with Special Health Care Needs Cystic Fibrosis 05: Improving Survival
Disclosure Dr Donna Willey Courand receives research support from Cystic Fibrosis Therapeutics The Cystic Fibrosis Foundation Children with Special Health Care Needs Cystic Fibrosis 05: Improving Survival
Pancreas composed of 2 parts: 1- exocrine gland 2- endocrine gland
 pancreas Pancreas composed of 2 parts: 1- exocrine gland 2- endocrine gland Acute pancreatitis Inflammation of the pancreas associated with acinar cell injury Clinical features: 1-abdominal pain cardinal
pancreas Pancreas composed of 2 parts: 1- exocrine gland 2- endocrine gland Acute pancreatitis Inflammation of the pancreas associated with acinar cell injury Clinical features: 1-abdominal pain cardinal
Day Date Title Instructor 5 th Ed 6 th Ed. Protein digestion and AA absorption
 Day Date Title Instructor 5 th Ed 6 th Ed 1 Tuesday 18 April 2017 Protein digestion and AA absorption D S Jairajpuri 250 256 250 256 2 Wednesday 19 April 2017 Removal of nitrogen and urea cycle D S Jairajpuri
Day Date Title Instructor 5 th Ed 6 th Ed 1 Tuesday 18 April 2017 Protein digestion and AA absorption D S Jairajpuri 250 256 250 256 2 Wednesday 19 April 2017 Removal of nitrogen and urea cycle D S Jairajpuri
Cystic Fibrosis 8/23/2014 GROWTH DEFICIENCY IN CYSTIC FIBROSIS IS
 8/23/214 GROWTH DEFICIENCY IN CYSTIC FIBROSIS IS OBSERVABLE AT BIRTH AND PREDICTIVE OF EARLY PULMONARY FUNCTION by Rebecca Joan Nelson Case Western Reserve University Cleveland, Ohio Thesis Advisor: Rebecca
8/23/214 GROWTH DEFICIENCY IN CYSTIC FIBROSIS IS OBSERVABLE AT BIRTH AND PREDICTIVE OF EARLY PULMONARY FUNCTION by Rebecca Joan Nelson Case Western Reserve University Cleveland, Ohio Thesis Advisor: Rebecca
Digestive System Module 6: Accessory Organs in Digestion: The Liver, Pancreas, and Gallbladder
 Connexions module: m49293 1 Digestive System Module 6: Accessory Organs in Digestion: The Liver, Pancreas, and Gallbladder Donna Browne Based on Accessory Organs in Digestion: The Liver, Pancreas, and
Connexions module: m49293 1 Digestive System Module 6: Accessory Organs in Digestion: The Liver, Pancreas, and Gallbladder Donna Browne Based on Accessory Organs in Digestion: The Liver, Pancreas, and
Hormonal Regulations Of Glucose Metabolism & DM
 Hormonal Regulations Of Glucose Metabolism & DM What Hormones Regulate Metabolism? What Hormones Regulate Metabolism? Insulin Glucagon Thyroid hormones Cortisol Epinephrine Most regulation occurs in order
Hormonal Regulations Of Glucose Metabolism & DM What Hormones Regulate Metabolism? What Hormones Regulate Metabolism? Insulin Glucagon Thyroid hormones Cortisol Epinephrine Most regulation occurs in order
TIMELINESS IN NEWBORN SCREENING: CONSIDERATIONS FOR CYSTIC FIBROSIS
 TIMELINESS IN NEWBORN SCREENING: CONSIDERATIONS FOR CYSTIC FIBROSIS Susanna A. McColley, MD Northwestern University Feinberg School of Medicine Ann & Robert H. Lurie Children s Hospital of Chicago Stanley
TIMELINESS IN NEWBORN SCREENING: CONSIDERATIONS FOR CYSTIC FIBROSIS Susanna A. McColley, MD Northwestern University Feinberg School of Medicine Ann & Robert H. Lurie Children s Hospital of Chicago Stanley
Pediatrics Grand Rounds 13 November University of Texas Health Science Center at San Antonio. Learning Objectives
 Nationwide Newborn Screening for Cystic Fibrosis: Finally Creating an Opportunity for All Patients to Have Better Outcomes Philip M Farrell, MD, PhD* University of Wisconsin-Madison *No disclosures other
Nationwide Newborn Screening for Cystic Fibrosis: Finally Creating an Opportunity for All Patients to Have Better Outcomes Philip M Farrell, MD, PhD* University of Wisconsin-Madison *No disclosures other
Bio& 242 Unit 1 / Lecture 4
 Bio& 242 Unit 1 / Lecture 4 system: Gastric hormones GASTRIN: Secretion: By enteroendocrine (G) in gastric pits of the mucosa. Stimulus: Stomach distention and acid ph of chyme causes Gastrin. Action:
Bio& 242 Unit 1 / Lecture 4 system: Gastric hormones GASTRIN: Secretion: By enteroendocrine (G) in gastric pits of the mucosa. Stimulus: Stomach distention and acid ph of chyme causes Gastrin. Action:
16 April 2010 Resident Teaching Conference. Pancreatitis. W. H. Nealon, M.D., F.A.C.S. J.J. Smith, M.D., D.W.D.
 16 April 2010 Resident Teaching Conference Pancreatitis W. H. Nealon, M.D., F.A.C.S. J.J. Smith, M.D., D.W.D. Santorini Wirsung anatomy.med.umich.edu/.../ duodenum_ans.html Bud and ductology Ventral pancreatic
16 April 2010 Resident Teaching Conference Pancreatitis W. H. Nealon, M.D., F.A.C.S. J.J. Smith, M.D., D.W.D. Santorini Wirsung anatomy.med.umich.edu/.../ duodenum_ans.html Bud and ductology Ventral pancreatic
Causes of pancreatic insufficiency. Eugen Dumitru
 Causes of pancreatic insufficiency Eugen Dumitru Pancreatic Exocrine Insufficiency (PEI) 1. The Concept 2. The Causes 3. The Consequences Pancreatic Exocrine Insufficiency (PEI) 1. The Concept 2. The Causes
Causes of pancreatic insufficiency Eugen Dumitru Pancreatic Exocrine Insufficiency (PEI) 1. The Concept 2. The Causes 3. The Consequences Pancreatic Exocrine Insufficiency (PEI) 1. The Concept 2. The Causes
Energy, Chemical Reactions and Enzymes
 Phosphorylation Hydrolysis Energy, Chemical Reactions and Enzymes Chapter 2 (selections) What is Energy? Energy is the capacity to do work Potential Energy Kinetic Energy Chemical Bond Energy Like a rechargeable
Phosphorylation Hydrolysis Energy, Chemical Reactions and Enzymes Chapter 2 (selections) What is Energy? Energy is the capacity to do work Potential Energy Kinetic Energy Chemical Bond Energy Like a rechargeable
THE ROLE OF CFTR MUTATIONS IN CAUSING CYSTIC FIBROSIS (CF)
") THE ROLE OF CFTR MUTATIONS IN CAUSING CYSTIC FIBROSIS (CF) Vertex Pharmaceuticals Incorporated, 50 Northern Avenue, Boston, MA 02210. Vertex and the Vertex triangle logo are registered trademarks of Vertex
THE ROLE OF CFTR MUTATIONS IN CAUSING CYSTIC FIBROSIS (CF) Vertex Pharmaceuticals Incorporated, 50 Northern Avenue, Boston, MA 02210. Vertex and the Vertex triangle logo are registered trademarks of Vertex
Pancreatitis. Acute Pancreatitis
 Pancreatitis Pancreatitis is an inflammation of the pancreas. The pancreas is a large gland behind the stomach and close to the duodenum. The duodenum is the upper part of the small intestine. The pancreas
Pancreatitis Pancreatitis is an inflammation of the pancreas. The pancreas is a large gland behind the stomach and close to the duodenum. The duodenum is the upper part of the small intestine. The pancreas
Key Points: References: Canadian data from the Canadian Cystic Fibrosis Registry 2015 Annual Report normal
 1 2 3 Cystic fibrosis is a rare life-long genetic disease that affects approximately 4,000 people in Canada and about 70,000 worldwide regardless of race or ethnicity but is more common in Caucasians 1,2
1 2 3 Cystic fibrosis is a rare life-long genetic disease that affects approximately 4,000 people in Canada and about 70,000 worldwide regardless of race or ethnicity but is more common in Caucasians 1,2
Monosaccharides: Little amounts Don t need any digestion
 Slide 8 Digestion result in mono and disaccharides & alpha-dextrins (oligosaccharides) Alpha1-4 in sequences / alpha1-6 at branches Dietary carbohydrates: Polysaccharides: 1) Containing α(1,4)/ α(1,6)
Slide 8 Digestion result in mono and disaccharides & alpha-dextrins (oligosaccharides) Alpha1-4 in sequences / alpha1-6 at branches Dietary carbohydrates: Polysaccharides: 1) Containing α(1,4)/ α(1,6)
Digestion and Absorption
 Digestion and Absorption Digestion and Absorption Digestion is a process essential for the conversion of food into a small and simple form. Mechanical digestion by mastication and swallowing Chemical digestion
Digestion and Absorption Digestion and Absorption Digestion is a process essential for the conversion of food into a small and simple form. Mechanical digestion by mastication and swallowing Chemical digestion
L1, 2 : Biochemical Aspects of Digestion of Lipids, Proteins, and Carbohydrates
 L1, 2 : Biochemical Aspects of Digestion of Lipids, Proteins, and Carbohydrates OBJECTIVES: Understand the process of digestion of dietary lipids, protein and carbohydrates including, the organs involved,
L1, 2 : Biochemical Aspects of Digestion of Lipids, Proteins, and Carbohydrates OBJECTIVES: Understand the process of digestion of dietary lipids, protein and carbohydrates including, the organs involved,
PHYSIOLOGY OF THE DIGESTIVE SYSTEM
 Student Name CHAPTER 26 PHYSIOLOGY OF THE DIGESTIVE SYSTEM D igestion is the process of breaking down complex nutrients into simpler units suitable for absorption. It involves two major processes: mechanical
Student Name CHAPTER 26 PHYSIOLOGY OF THE DIGESTIVE SYSTEM D igestion is the process of breaking down complex nutrients into simpler units suitable for absorption. It involves two major processes: mechanical
UNDERSTANDING THE EARLY, SYSTEMIC PROGRESSION OF CYSTIC FIBROSIS (CF) A Resource for the CF Center Care Team
 A Resource for the CF Center Care Team") UNDERSTANDING THE EARLY, SYSTEMIC PROGRESSION OF CYSTIC FIBROSIS (CF) A Resource for the CF Center Care Team Vertex Pharmaceuticals Incorporated, 50 Northern Avenue, Boston, MA 02210. Vertex and the Vertex
UNDERSTANDING THE EARLY, SYSTEMIC PROGRESSION OF CYSTIC FIBROSIS (CF) A Resource for the CF Center Care Team Vertex Pharmaceuticals Incorporated, 50 Northern Avenue, Boston, MA 02210. Vertex and the Vertex
AN ANIMAL S DIET MUST SUPPLY CHEMICAL ENERGY, ORGANIC MOLECULES, AND ESSENTIAL NUTRIENTS
 1 ANIMAL NUTRITION 2 3 4 5 6 7 Food is taken in, taken apart, and taken up in the process of animal nutrition In general, animals fall into three categories: Herbivores eat mainly plants and algae Carnivores
1 ANIMAL NUTRITION 2 3 4 5 6 7 Food is taken in, taken apart, and taken up in the process of animal nutrition In general, animals fall into three categories: Herbivores eat mainly plants and algae Carnivores
Insulin and the brain. Mary ET Boyle + Billy + Bree + Alex + Rachael Department of Cognitive Science, UCSD
 Insulin and the brain Mary ET Boyle + Billy + Bree + Alex + Rachael Department of Cognitive Science, UCSD 1921 Banting & Macleod Nobel Prize 1923 White, M. F. (2003) Science Berg, J. M., Tymoczko, J. L.
Insulin and the brain Mary ET Boyle + Billy + Bree + Alex + Rachael Department of Cognitive Science, UCSD 1921 Banting & Macleod Nobel Prize 1923 White, M. F. (2003) Science Berg, J. M., Tymoczko, J. L.
Chapter 14: The Digestive System
 Chapter 14: The Digestive System Digestive system consists of Muscular tube (digestive tract) alimentary canal Accessory organs teeth, tongue, glandular organs 6 essential activities 1. 2. 3. 4. 5. 6.
Chapter 14: The Digestive System Digestive system consists of Muscular tube (digestive tract) alimentary canal Accessory organs teeth, tongue, glandular organs 6 essential activities 1. 2. 3. 4. 5. 6.
Summary of chemical breakdown of food by hydrolytic enzymes (Protein enzymes).
.") Biology 12 Digestive System Digestion Overview: The digestive process can be divided into 4 phases: 1. ingestion - includes swallowing and peristalsis 2. digestion - the physical (by teeth) and chemical
Biology 12 Digestive System Digestion Overview: The digestive process can be divided into 4 phases: 1. ingestion - includes swallowing and peristalsis 2. digestion - the physical (by teeth) and chemical
Evaluation of Patients with Diffuse Bronchiectasis
 Evaluation of Patients with Diffuse Bronchiectasis Dr. Patricia Eshaghian, MD Assistant Clinical Professor of Medicine Director, UCLA Adult Cystic Fibrosis Affiliate Program UCLA Division of Pulmonary
Evaluation of Patients with Diffuse Bronchiectasis Dr. Patricia Eshaghian, MD Assistant Clinical Professor of Medicine Director, UCLA Adult Cystic Fibrosis Affiliate Program UCLA Division of Pulmonary
Hormones and Homeostasis
 Hormones and Homeostasis The endocrine system is a system of organs that releases chemical message molecules, called hormones, into the blood. Unlike the nervous system whose action helps the body react
Hormones and Homeostasis The endocrine system is a system of organs that releases chemical message molecules, called hormones, into the blood. Unlike the nervous system whose action helps the body react
The Players. Liver Thyroid Adrenals Pancreas Reproductive System Pituitary Gut Bacteria
 The Players Part I Quick Review Understanding some of the key systems and their relationship to hormones is the best place to start It will help with some of the hormone interconnections Key to understanding
The Players Part I Quick Review Understanding some of the key systems and their relationship to hormones is the best place to start It will help with some of the hormone interconnections Key to understanding
ESPEN Congress Nice From child to adult nutrition. Cystic fibrosis. A. Munck
 ESPEN Congress Nice 2010 From child to adult nutrition Cystic fibrosis A. Munck Cystic fibrosis nutrition: from child to adulthood -Positive impact of optimizing nutrition -Monitoring nutritional status
ESPEN Congress Nice 2010 From child to adult nutrition Cystic fibrosis A. Munck Cystic fibrosis nutrition: from child to adulthood -Positive impact of optimizing nutrition -Monitoring nutritional status
Cystic Fibrosis. Parkland College. Monica Rahman Parkland College. Recommended Citation
 Parkland College A with Honors Projects Honors Program 2013 Cystic Fibrosis Monica Rahman Parkland College Recommended Citation Rahman, Monica, "Cystic Fibrosis" (2013). A with Honors Projects. 98. http://spark.parkland.edu/ah/98
Parkland College A with Honors Projects Honors Program 2013 Cystic Fibrosis Monica Rahman Parkland College Recommended Citation Rahman, Monica, "Cystic Fibrosis" (2013). A with Honors Projects. 98. http://spark.parkland.edu/ah/98
Cystic Fibrosis as it relates to the neonate MARIANNE MUHLEBACH, MD PROFESSOR, DEPT. PEDIATRICS UNC CHAPEL HILL
 Cystic Fibrosis as it relates to the neonate MARIANNE MUHLEBACH, MD PROFESSOR, DEPT. PEDIATRICS UNC CHAPEL HILL Objectives: At the end of the presentation the listeners will Be able to describe neonatal
Cystic Fibrosis as it relates to the neonate MARIANNE MUHLEBACH, MD PROFESSOR, DEPT. PEDIATRICS UNC CHAPEL HILL Objectives: At the end of the presentation the listeners will Be able to describe neonatal
PANCREATIC BETA CELLS PRODUCE AND SECRETE
 15 March, 2018 PANCREATIC BETA CELLS PRODUCE AND SECRETE Document Filetype: PDF 374.06 KB 0 PANCREATIC BETA CELLS PRODUCE AND SECRETE Among the oldest and cheapest drugs for diabetes are the drugs that
15 March, 2018 PANCREATIC BETA CELLS PRODUCE AND SECRETE Document Filetype: PDF 374.06 KB 0 PANCREATIC BETA CELLS PRODUCE AND SECRETE Among the oldest and cheapest drugs for diabetes are the drugs that
Lecture Overview. ** Digestive System ** (cont d) A&P II Lecture Notes Pages
 A&P II Lecture Notes Pages") ** Digestive System ** (cont d) A&P II Lecture Notes Pages 103-111 Lecture Overview Gall Bladder/Ducts Pancreas GI Tract Movements Chemistry of Digestion Secretion and Absorption Metabolism 2 Liver, Bile
** Digestive System ** (cont d) A&P II Lecture Notes Pages 103-111 Lecture Overview Gall Bladder/Ducts Pancreas GI Tract Movements Chemistry of Digestion Secretion and Absorption Metabolism 2 Liver, Bile
Physiology 12. Overview. The Gastrointestinal Tract. Germann Ch 19
 Physiology 12 The Gastrointestinal Tract Germann Ch 19 Overview 1 Basic functions of the GI tract Digestion Secretion Absorption Motility Basic functions of the GI tract Digestion: : Dissolving and breaking
Physiology 12 The Gastrointestinal Tract Germann Ch 19 Overview 1 Basic functions of the GI tract Digestion Secretion Absorption Motility Basic functions of the GI tract Digestion: : Dissolving and breaking
Chapter 20 The Digestive System Exam Study Questions
 Chapter 20 The Digestive System Exam Study Questions 20.1 Overview of GI Processes 1. Describe the functions of digestive system. 2. List and define the four GI Processes: 20.2 Functional Anatomy of the
Chapter 20 The Digestive System Exam Study Questions 20.1 Overview of GI Processes 1. Describe the functions of digestive system. 2. List and define the four GI Processes: 20.2 Functional Anatomy of the
Diseases of pancreas - Chronic pancreatitis
 Corso di laurea in Medicina e Chirurgia Anno accademico 2015-2016 V Anno di corso- Primo Semestre Corso Integrato : Patologia Sistemica C- Gastroenterologia Prof. Stefano Fiorucci Diseases of pancreas
Corso di laurea in Medicina e Chirurgia Anno accademico 2015-2016 V Anno di corso- Primo Semestre Corso Integrato : Patologia Sistemica C- Gastroenterologia Prof. Stefano Fiorucci Diseases of pancreas
Adrenal gland And Pancreas
 Adrenal gland And Pancreas Structure Cortex Glucocorticoids Effects Control of secretion Mineralocorticoids Effects Control of secretion Sex steroids Medulla Catecholamines Adrenal cortex 80% of an adrenal
Adrenal gland And Pancreas Structure Cortex Glucocorticoids Effects Control of secretion Mineralocorticoids Effects Control of secretion Sex steroids Medulla Catecholamines Adrenal cortex 80% of an adrenal
ESPEN Congress The Hague 2017
 ESPEN Congress The Hague 2017 Meeting nutritional needs of acute care patients Feeding acute pancreatitis patients J. Luttikhold (NL) FEEDING ACUTE PANCREATITIS PATIENTS Joanna Luttikhold, MD PhD Registrar
ESPEN Congress The Hague 2017 Meeting nutritional needs of acute care patients Feeding acute pancreatitis patients J. Luttikhold (NL) FEEDING ACUTE PANCREATITIS PATIENTS Joanna Luttikhold, MD PhD Registrar
Ingestion Digestion- Absorption- Elimination
 DIGESTIVE SYSTEM 1 FUNCTIONS Organization GI tract==mouth anus Accessory organs Salivary glands, liver, pancreas, gallbladder Major Functions: Ingestion-mouth, teeth, tongue Digestion- chemical and mechanical
DIGESTIVE SYSTEM 1 FUNCTIONS Organization GI tract==mouth anus Accessory organs Salivary glands, liver, pancreas, gallbladder Major Functions: Ingestion-mouth, teeth, tongue Digestion- chemical and mechanical
Chapter 20 The Digestive System Exam Study Questions
 Chapter 20 The Digestive System Exam Study Questions 20.1 Overview of GI Processes 1. Describe the functions of digestive system. 2. List and define the four GI Processes: 20.2 Functional Anatomy of the
Chapter 20 The Digestive System Exam Study Questions 20.1 Overview of GI Processes 1. Describe the functions of digestive system. 2. List and define the four GI Processes: 20.2 Functional Anatomy of the
Sphincters heartburn diaphragm The Stomach gastric glands pepsin, chyme The Small Intestine 1-Digestion Is Completed in the Small Intestine duodenum
 Sphincters are muscles that encircle tubes and act as valves. The tubes close when the sphincters contract and they open when the sphincters relax. When food or saliva is swallowed, the sphincter relaxes
Sphincters are muscles that encircle tubes and act as valves. The tubes close when the sphincters contract and they open when the sphincters relax. When food or saliva is swallowed, the sphincter relaxes
NUTRIENT DIGESTION & ABSORPTION
 NUTRIENT DIGESTION & ABSORPTION NUTR 2050: Nutrition for Nursing Professionals Mrs. Deborah A. Hutcheon, MS, RD, LD Lesson Objectives At the end of the lesson, the student will be able to: 1. Differentiate
NUTRIENT DIGESTION & ABSORPTION NUTR 2050: Nutrition for Nursing Professionals Mrs. Deborah A. Hutcheon, MS, RD, LD Lesson Objectives At the end of the lesson, the student will be able to: 1. Differentiate
Includes mouth, pharynx, esophagus, stomach, small intestine, large intestine, rectum, anus. Salivary glands, liver, gallbladder, pancreas
 Chapter 14 The Digestive System and Nutrition Digestive System Brings Nutrients Into the Body The digestive system includes Gastrointestinal (GI) tract (hollow tube) Lumen: space within this tube Includes
Chapter 14 The Digestive System and Nutrition Digestive System Brings Nutrients Into the Body The digestive system includes Gastrointestinal (GI) tract (hollow tube) Lumen: space within this tube Includes
What systems are involved in homeostatic regulation (give an example)?
?") 1 UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY AND MOLECULAR BIOLOGY GLUCOSE HOMEOSTASIS (Diabetes Mellitus Part 1): An Overview
1 UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY AND MOLECULAR BIOLOGY GLUCOSE HOMEOSTASIS (Diabetes Mellitus Part 1): An Overview
STEIN IN-TERM EXAM -- BIOLOGY APRIL 18, PAGE
 STEIN IN-TERM EXAM -- BIOLOGY 3058 -- APRIL 18, 2019 -- PAGE 1 of 9 There are 25 questions in this Biology 3058 exam. All questions are "A, B, C, D, E, F, G, H" questions worth one point each. There is
STEIN IN-TERM EXAM -- BIOLOGY 3058 -- APRIL 18, 2019 -- PAGE 1 of 9 There are 25 questions in this Biology 3058 exam. All questions are "A, B, C, D, E, F, G, H" questions worth one point each. There is
Chapter 20 Endocrine System
 Chapter 20 Endocrine System The endocrine system consists of glands and tissues that secrete Hormones are chemicals that affect other glands or tissues, many times far away from the site of hormone production
Chapter 20 Endocrine System The endocrine system consists of glands and tissues that secrete Hormones are chemicals that affect other glands or tissues, many times far away from the site of hormone production
A review of Cystic Fibrosis
 A review of Cystic Fibrosis Jennifer Landry md F.R.C.P.(C) Pulmonary & Critical Care Medicine McGill University Health Center Cystic Fibrosis One of the most common lethal inherited AR disorders in the
A review of Cystic Fibrosis Jennifer Landry md F.R.C.P.(C) Pulmonary & Critical Care Medicine McGill University Health Center Cystic Fibrosis One of the most common lethal inherited AR disorders in the
Chapter 26 The Digestive System
 Chapter 26 The Digestive System Digestive System Gastroenterology is the study of the stomach and intestine. Digestion Catabolism Absorption Anabolism The actions of the digestive system are controlled
Chapter 26 The Digestive System Digestive System Gastroenterology is the study of the stomach and intestine. Digestion Catabolism Absorption Anabolism The actions of the digestive system are controlled
PATHOLOGY MCQs. The Pancreas
 PATHOLOGY MCQs The Pancreas A patient with cystic fibrosis is characteristically: A. more than 45 years of age B. subject to recurring pulmonary infections C. obese D. subject to spontaneous fractures
PATHOLOGY MCQs The Pancreas A patient with cystic fibrosis is characteristically: A. more than 45 years of age B. subject to recurring pulmonary infections C. obese D. subject to spontaneous fractures
UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY AND MOLECULAR BIOLOGY
 1 UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY AND MOLECULAR BIOLOGY GLUCOSE HOMEOSTASIS An Overview WHAT IS HOMEOSTASIS? Homeostasis
1 UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY AND MOLECULAR BIOLOGY GLUCOSE HOMEOSTASIS An Overview WHAT IS HOMEOSTASIS? Homeostasis
ENDOCRINOLOGY. Dr.AZZA SAJID ALKINANY 2 nd STAGE
 ENDOCRINOLOGY Dr.AZZA SAJID ALKINANY 2 nd STAGE THE RELATIONSHIP AMONG THE HYPOTHALMUS,POSTERIOR PITUITARY AND TARGET TISSUES. The posterior pituitary does not produce its own hormones, but stores and
ENDOCRINOLOGY Dr.AZZA SAJID ALKINANY 2 nd STAGE THE RELATIONSHIP AMONG THE HYPOTHALMUS,POSTERIOR PITUITARY AND TARGET TISSUES. The posterior pituitary does not produce its own hormones, but stores and
10/23/2013 ANIMAL NUTRITION ANIMAL NUTRITION ESSENTIAL NUTRIENTS AN ANIMAL S DIET MUST STUPPLY: AMINO ACIDS
 ANIMAL NUTRITION Food is taken in, taken apart, and taken up in the process of animal nutrition In general, animals fall into three categories: Herbivores Carnivores Omnivores ANIMAL NUTRITION Chapter
ANIMAL NUTRITION Food is taken in, taken apart, and taken up in the process of animal nutrition In general, animals fall into three categories: Herbivores Carnivores Omnivores ANIMAL NUTRITION Chapter
The Small Intestine. The pyloric sphincter at the bottom of the stomach opens, squirting small amounts of food into your small intestine.
 The Small Intestine The pyloric sphincter at the bottom of the stomach opens, squirting small amounts of food into your small intestine. approximately six metres (the longest section of your digestive
The Small Intestine The pyloric sphincter at the bottom of the stomach opens, squirting small amounts of food into your small intestine. approximately six metres (the longest section of your digestive
Nutrition. Autotrophs. plants, some protists & bacteria producers
 Nutrition Autotrophs plants, some protists & bacteria producers Nutrition Heterotrophs animals, fungi, some protists & bacteria consumers Animal Nutrition Most obtain food by ingestion take in their food
Nutrition Autotrophs plants, some protists & bacteria producers Nutrition Heterotrophs animals, fungi, some protists & bacteria consumers Animal Nutrition Most obtain food by ingestion take in their food
KRISHNA TEJA PHARMACY COLLEGE HUMAN ANATOMY AND PHYSIOLOGY. DIGESTIVE SYSTEM Dr.B.Jyothi
 KRISHNA TEJA PHARMACY COLLEGE HUMAN ANATOMY AND PHYSIOLOGY DIGESTIVE SYSTEM Dr.B.Jyothi Prof, Dept. Of Pharmacology KTPC The Digestive System Food undergoes six major processes: 1. Ingestion : process
KRISHNA TEJA PHARMACY COLLEGE HUMAN ANATOMY AND PHYSIOLOGY DIGESTIVE SYSTEM Dr.B.Jyothi Prof, Dept. Of Pharmacology KTPC The Digestive System Food undergoes six major processes: 1. Ingestion : process
PULMONARY SURFACTANT, ALPHA 1 ANTITRYPSIN INHIBITOR DEFICIENCY, AND CYSTIC FIBROSIS DR. NABIL BASHIR BIOCHEMISTRY/RESPIRATORY SYSTEM
 PULMONARY SURFACTANT, ALPHA 1 ANTITRYPSIN INHIBITOR DEFICIENCY, AND CYSTIC FIBROSIS DR. NABIL BASHIR BIOCHEMISTRY/RESPIRATORY SYSTEM Pulmonary surfactant Pulmonary surfactant is (phospholipoprotein) complex
PULMONARY SURFACTANT, ALPHA 1 ANTITRYPSIN INHIBITOR DEFICIENCY, AND CYSTIC FIBROSIS DR. NABIL BASHIR BIOCHEMISTRY/RESPIRATORY SYSTEM Pulmonary surfactant Pulmonary surfactant is (phospholipoprotein) complex
Cystic Fibrosis Foundation Patient Registry 2013
 5/9/2015 Targeting CFTR to Treat Cystic Fibrosis: Small Molecule Therapy Mary Ellen Kleinhenz, MD Director, UCSF Adult Cystic Fibrosis Program Professor of Medicine UCSF Division of Pulmonary, Critical
5/9/2015 Targeting CFTR to Treat Cystic Fibrosis: Small Molecule Therapy Mary Ellen Kleinhenz, MD Director, UCSF Adult Cystic Fibrosis Program Professor of Medicine UCSF Division of Pulmonary, Critical
Station 1. Identify (= name) the spaces or structures labeled 1 9.
 the spaces or structures labeled 1 9.") Station 1. Identify (= name) the spaces or structures labeled 1 9. 1 9 8 2 7 3 4 5 6 Station 2. Identify/name the parts or structures labeled 10 20. 10. Is this the right or left lung? 15 13 14 16 11 12
Station 1. Identify (= name) the spaces or structures labeled 1 9. 1 9 8 2 7 3 4 5 6 Station 2. Identify/name the parts or structures labeled 10 20. 10. Is this the right or left lung? 15 13 14 16 11 12
You Can Observe a Lot By Just Watching. Wayne J. Morgan, MD, CM
 You Can Observe a Lot By Just Watching Wayne J. Morgan, MD, CM Disclosures Genentech Epidemiological Study of Cystic Fibrosis, Scientific Advisory Group CF Foundation Data Safety Monitoring Board Registry/Comparative
You Can Observe a Lot By Just Watching Wayne J. Morgan, MD, CM Disclosures Genentech Epidemiological Study of Cystic Fibrosis, Scientific Advisory Group CF Foundation Data Safety Monitoring Board Registry/Comparative
Hormonal regulation of. Physiology Department Medical School, University of Sumatera Utara
 Hormonal regulation of nutrient metabolism Physiology Department Medical School, University of Sumatera Utara Homeostasis & Controls Successful compensation Homeostasis reestablished Failure to compensate
Hormonal regulation of nutrient metabolism Physiology Department Medical School, University of Sumatera Utara Homeostasis & Controls Successful compensation Homeostasis reestablished Failure to compensate
Study Aid for D1: Nutrition
 Study Aid for D1: Nutrition Essential nutrient Food only source. Ex. Some Amino acids, minerals, calcium, vitamins, water, some fatty acids Non-essential nutrient Can be made in body. Ex. Glucose, starch.
Study Aid for D1: Nutrition Essential nutrient Food only source. Ex. Some Amino acids, minerals, calcium, vitamins, water, some fatty acids Non-essential nutrient Can be made in body. Ex. Glucose, starch.
EAT TO LIVE: THE ROLE OF THE PANCREAS. Felicia V. Nowak, M.D., Ph.D. Ohio University COM 22 January, 2008
 EAT TO LIVE: THE ROLE OF THE PANCREAS Felicia V. Nowak, M.D., Ph.D. Ohio University COM 22 January, 2008 THE ROLE OF THE PANCREAS Exocrine pancreas Endocrine pancreas THE ROLE OF THE PANCREAS EXOCRINE
EAT TO LIVE: THE ROLE OF THE PANCREAS Felicia V. Nowak, M.D., Ph.D. Ohio University COM 22 January, 2008 THE ROLE OF THE PANCREAS Exocrine pancreas Endocrine pancreas THE ROLE OF THE PANCREAS EXOCRINE
Summary break down long chain proteins, polysaccharides and nucleic acids into monomers recall hydrolysis (opposite of dehydration synthesis) (hydro-w
 (hydro-w") Summary break down long chain proteins, polysaccharides and nucleic acids into monomers recall hydrolysis (opposite of dehydration synthesis) (hydro-water lysis-break apart) if not broken down, proteins
Summary break down long chain proteins, polysaccharides and nucleic acids into monomers recall hydrolysis (opposite of dehydration synthesis) (hydro-water lysis-break apart) if not broken down, proteins
2- Minimum toxic concentration (MTC): The drug concentration needed to just produce a toxic effect.
: The drug concentration needed to just produce a toxic effect.") BIOPHARMACEUTICS Drug Product Performance Parameters: 1- Minimum effective concentration (MEC): The minimum concentration of drug needed at the receptors to produce the desired pharmacologic effect. 2-
BIOPHARMACEUTICS Drug Product Performance Parameters: 1- Minimum effective concentration (MEC): The minimum concentration of drug needed at the receptors to produce the desired pharmacologic effect. 2-
Overview. Physiology 1. The Gastrointestinal Tract. Guyton section XI
 Overview Physiology 1 The Gastrointestinal Tract Guyton section XI Basic functions of the GI tract Digestion Secretion Absorption Motility Basic functions of the GI tract Digestion: : Dissolving and breaking
Overview Physiology 1 The Gastrointestinal Tract Guyton section XI Basic functions of the GI tract Digestion Secretion Absorption Motility Basic functions of the GI tract Digestion: : Dissolving and breaking
Ch 7 Nutrition in humans
 Ch 7 Nutrition in humans Think about (Ch 7, p.2) 1. The stomach churns food into smaller pieces physically. The stomach wall secretes proteases to chemically digest proteins. It also releases hydrochloric
Ch 7 Nutrition in humans Think about (Ch 7, p.2) 1. The stomach churns food into smaller pieces physically. The stomach wall secretes proteases to chemically digest proteins. It also releases hydrochloric
Introduction to Human Anatomy & Physiology Chapter 35
 Biology Introduction to Human Anatomy & Physiology Chapter 35 Digestion The breakdown of complex biological molecules into their component parts. Lipids to fatty acids Proteins to individual amino acids
Biology Introduction to Human Anatomy & Physiology Chapter 35 Digestion The breakdown of complex biological molecules into their component parts. Lipids to fatty acids Proteins to individual amino acids
CF: Information for Case Managers. Cindy Capen MSN, RN Pediatric Pulmonary Division University of Florida
 CF: Information for Case Managers Cindy Capen MSN, RN capencl@peds.ufl.edu Pediatric Pulmonary Division University of Florida About your speaker 25+ years in pulmonary Coordinator for CF Center and CF
CF: Information for Case Managers Cindy Capen MSN, RN capencl@peds.ufl.edu Pediatric Pulmonary Division University of Florida About your speaker 25+ years in pulmonary Coordinator for CF Center and CF
Part 1 The Cell and the Cellular Environment
 1 Chapter 3 Anatomy and Physiology Part 1 The Cell and the Cellular Environment 2 The Human Cell The is the fundamental unit of the human body. Cells contain all the necessary for life functions. 3 Cell
1 Chapter 3 Anatomy and Physiology Part 1 The Cell and the Cellular Environment 2 The Human Cell The is the fundamental unit of the human body. Cells contain all the necessary for life functions. 3 Cell
Minimal Enteral Nutrition
 Abstract Minimal Enteral Nutrition Although parenteral nutrition has been used widely in the management of sick very low birth weight infants, a smooth transition to the enteral route is most desirable.
Abstract Minimal Enteral Nutrition Although parenteral nutrition has been used widely in the management of sick very low birth weight infants, a smooth transition to the enteral route is most desirable.
Week 3, Lecture 5a. Pathophysiology of Diabetes. Simin Liu, MD, ScD
 Week 3, Lecture 5a Pathophysiology of Diabetes Simin Liu, MD, ScD General Model of Peptide Hormone Action Hormone Plasma Membrane Activated Nucleus Cellular Trafficking Enzymes Inhibited Receptor Effector
Week 3, Lecture 5a Pathophysiology of Diabetes Simin Liu, MD, ScD General Model of Peptide Hormone Action Hormone Plasma Membrane Activated Nucleus Cellular Trafficking Enzymes Inhibited Receptor Effector
STEIN IN-TERM EXAM -- BIOLOGY APRIL 21, PAGE
 STEIN IN-TERM EXAM -- BIOLOGY 3058 -- APRIL 21, 2016 -- PAGE 1 of 9 There are 25 questions in this Biology 3058 exam. All questions are "A, B, C, D, E, F, G, H" questions worth one point each. There is
STEIN IN-TERM EXAM -- BIOLOGY 3058 -- APRIL 21, 2016 -- PAGE 1 of 9 There are 25 questions in this Biology 3058 exam. All questions are "A, B, C, D, E, F, G, H" questions worth one point each. There is