Neurosurgical Management of Aneurysmal Subarachnoid Hemorrhage
|
|
|
- Virginia Lambert
- 5 years ago
- Views:
Transcription
1 Neurosurgical Management of Aneurysmal Subarachnoid Hemorrhage PVHMC STROKE SYMPOSIUM /27/18 Srinath Samudrala MD, FACS
")
2 Epidemiology of Subarachnoid Hemorrhage (SAH) Less than 10% of all stroke annually Acute mortality 25-50%; 30-50% morbidity Stroke subtype and incidence Incidence of aneurysms ~5% general population Most SAH traumatic, but of non traumatic, majority due to aneurysm rupture (85%) Spontaneous SAH
3 Risk Factors and Epidemiology of Aneurysmal SAH Females greater than males Peak age May be higher amongst blacks Smoking, hypertension, heavy alcohol use (Note, these are not the same risk factors for aneurysms development which may include collagen-vascular disease and co-associated conditions such as polycystic kidney disease



4 Types of Cerebral aneurysms DISSECTING SACCULAR FUSIFORM


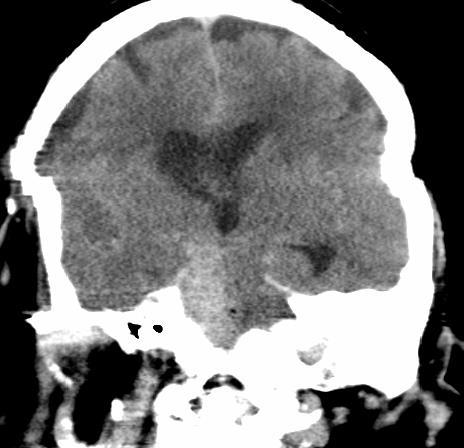

5 Focal peripontine SAH and possible Vertebral artery dissection
6 Clinical features Sudden, severe headache thunderclap headache; Nuchal rigidity; Nausea/vomiting Subhyaloid vitreous hemorrhage Cranial nerve palsies, particularly IIIrd nerve palsy with PCOM aneurysms or other ocular cranial nerve palsies with giant cavernous carotid artery aneurysms Coma, convulsions at onset
7 Diagnosis Computed tomography: hyperdensity in SAS Fisher rating scale: 1: minimal or no blood 2: diffuse thin 3: thick layering in basal cisterns 4: IVH or ICH out of proportion to basal cisternal blood Lumbar puncture: xanthochromia, constant red cell count b/w first and last tube FLAIR MRI increased signal on T2 FLAIR in SAS



8 Fisher grade on CT Fisher 2 Diffuse thin Fisher 3 Thick cisternal clot Fisher 4 ICH, IVH > SAH
9 Clinical Grading Scales Hunt Hess grade 1: mild headache* 2: severe headache OR mild headache with cranial nerve palsy (e.g. dilated pupil) 3: lethargy or focal neurological sign 4: stupor 5: coma World Federation of Neurological Surgeons (combination of GCS and presence or absence of focal symptoms) Occasional reference to H-H grade 0 (unruptured aneurysm), though technically this
10 Natural history of ruptured aneurysms Very high incidence of early rebleeding, upto 50% within first 6 months with 30% of that risk being within first 2 weeks Second bleed is often fatal sentinel bleed : initial asymptomatic or mildly symptomatic bleed followed by subsequent bleed of increased clinical severity
11 Clinical Management of SAH Pre-aneurysm repair: Prevent rerupture Control BP Maintenance fluids Avoidance of anticoagulants Supportive therapy Treatment of hydro if present Nimodipine 60 mg q4 Secure aneurysm Post aneurysm repair: Prevent/treat VSP permissive HTN Fluid augmentation +/- pharm. VTE prophylaxis Supportive therapy Treatment of hydro/vsp if present/occurs Nimodipine x 21 days
12 Deciding on Repair procedure Decision based on aneurysm location, morphology, patient comorbidity factors Ex: basilar tip endovascular treatment, vs MCA bifurcation surgical clipping Wide necked clipping Older patients, cardiopulmonary issues, etc endovascular treatment
13 Clinical trials of aneurysm repair procedures International Surgical Aneurysm Trial (ISAT) Good grade SAH patients clinical equipoise Barrow Ruptured Aneurysm Trial (BRAT) Single center study not blinded Significant crossover from endovasc to surg arm
14 ISAT 2143 patients, 22 UK centers 1 year Death/dependency ~24 vs 31% (EVE vs MSC) 10 years: 83% coiled pts alive vs 79% clipped; 82% coiled vs 78% clipped pts independent Combined OR 1.34,, 95% CI, Slightly higher rate rehemorrhage endo group
15 Barrow Ruptured Aneurysm Trial 700 screened 500 eligible 403 eval 358 patients underwent treatment (remainder died pre-tx or angio negative) 1 year data: Poor outcome in 33.7% clipped vs 23.2% coiled. OR 1.68, 95% CI , p= years: fav outcome, 5.8% absolute difference for coiled groups, P=0.25
16 Aneurysm Repair ENDOVASCULAR ANEURYSM TREATMENT
 Flow diversion Neck coverage")
17 Endovascular Aneurysm Intrasaccular treatments Coil embolization Liquid embolic embolization Extrasaccular (neck treatments) Flow diversion Neck coverage Treatment


18 Development of Neurovascular Coils Guglielmi & Vinuela, UCLA, FDA approved 1995, Target Therapeutics Numerous manufacturers since then bioactive vs bare platinum coils
19 Other general considerations Coils are MRI compatible Stents/Flow diverters are MRI compatible
20 OPEN NEUROSURGICAL ANEURYSM TREATMENT
21 Efficacy and risk factors of surgery More than 90% complete occlusion rate Mortality 0-3% in various series Morbidity 2-11% quoted in large studies Risk of surgery exceeds the 7.5 year risk of bleed in those aneurysm which are <10mm
22 Factors affecting surgical outcome Aneurysm related factors Aneurysm size (>2.5). Location (A comm, ICA bifurcation). Orientation Patient related factors Age Ischemic cerebrovascular diseases Diabetes mellitus
23 RUPTURED ANEURYSMS Sixty percent of patients either die or disabled % rebleed in 30 days. 4% rebleed rate on day 1. more than 70% who rebleed, die. Aneurysm occlusion either surgical or endovascular is the only answer.
24 Options for definitive treatment Surgery. Simple Clipping Wrapping Parent vessel occlusion Revascularization procedures Endovascular methods. Destructive procedures Reconstructive procedures Endoscopy Conservative
25 Timing of surgery: Anterior circulation: early surgery has good results compared to late Posterior circulations: Easy aneurysms: early surgery Difficult aneurysms : after two weeks (Haley EC jr et al the international cooperative study on the timing of aneurysm surgery; the north American experience. Stroke 23: ;1992)
26 Early surgery Virtually eliminates re-bleed Facilitates treatment of vasospasm Allows removal of vasospasmogenic material Though operative mortality higher, but overall outcome is better Factors favoring early surgery: Good medical condition of patient Good neurologic condition Large clot, blood Early rebleed, multiple episodes Imminent rebleed signs
27 Disadvantages Inflammation and brain edema causes more difficult and traumatic retraction Acute clot makes dissection difficult Risk of intraoperative rupture is high Vessel injury may aggravate vasospasm Factors favoring late surgery: Poor medical neurological condition Difficult aneurysms Significant edema on CT Active vasospasm

28 Technical considerations of aneurysm surgery Intraoperative objectives prevent rupture Further enlargement Preserve normal vessels Minimize injury to the brain
29 Technical considerations of aneurysm surgery Clip too low- may occlude parent vessel Distal placement- aneurysmal rest Aneurysmal rest expand in future and may rebleed Surgical exposure: avoid retraction Brain relaxation- hyperventilation, CSF drainage, lumbar spinal drainage, cisternal drainage drugs
30 POST ANEURYSM REPAIR CONSIDERATIONS NEUROLOGICAL SEQUELAE OF SAH AND CLINICAL MANAGEMENT
31 Brain Injury and Neuro sequelae post SAH Ultra-early injury (initial hours) ICP crisis, cerebral circulatory arrest Microthrombosis Cortical spreading ischemia Early injury (first few days) Vasospasm hydrocephalus Late/subacute (first 6-12 months) Depression Fatigue Cognitive problems Delayed complications (remote from incident event) Normal pressure hydrocephalus

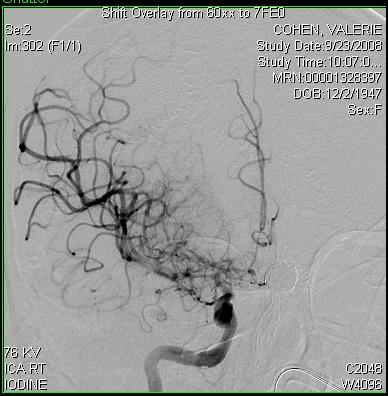
32 34 M with sudden LOC, L vertebral artery aneurysm 6:30 AM 2:17 PM
33 Vasospasm and HHT Constriction of blood vessels due to inflammatory effect of blood breakdown products Peak incidence days 3-10 post SAH Diagnosed by TCD with MFV in major intracranial vessels > 120 cm/sec Treated by triple H therapy (hypertension, hypervolemia, hemodilution) or first two arms, intra-arterial vasodilator administration, intracranial angioplasty


34
35 HHT Many patients auto-hypertense Induced hypertension with vasoactive medications, inotropes In extreme cases IABP Hypervolemic therapy to maintain CVP > 8 mm Hg with albumin, NS, 3% HTS Early move to definitive therapy for refractory cases (no improvement w/in 1 hour of HHT, or despite max HHT)
36 Magnesium therapy Experience with eclampsia patients Neuroprotectant (glutamate antagonist) 5 g bolus MgSO4 2 gm/250 cc NS at 23 cc/hr
37 Endovascular Tx of VSP IA vasodilators: papaverine (very short duration of action), verapamil, nicardipine, NTG Intracranial angioplasty more durable, with low or no incidence of recurrence of VSP at angioplastied segment



38

39 Global cerebral edema More common in poor grade patients Extension of white matter hypodensity to cortical surface on HCT May be exacerbated by HHT therapy
40 Ischemia in Subarachnoid Hemorrhage VASOSPASM Acute and delayed ischemic neurological deficit SILENT CEREBRAL ISCHEMIA 0% angiographic VSP DELAYED CEREBRAL ISCHEMIA?3-20% 30%
41 Prevention/Treatment of Cerebral Ischemia in SAH Detection/treatment of vasospasm Nimodipine Negative/equivocal trials: clozasentan, cilostazol, dantrolene, albumin, statins, magnesium, intra-thecal nimodipine
42 POST ANEURYSM REPAIR CONSIDERATIONS MEDICAL COMPLICATIONS OF SAH
 Prolonged QT interval Torsade de")
43 EKG changes in SAH T wave inversions Diffuse ST elevations or depressions (changes that do not respect coronary artery territory) Prolonged QT interval Torsade de pointes

44 32 M sudden seizure, SAH
45 Neurogenic stunned myocardium Sympathetic surge leads to catecholamine release and global depressed cardiac function More common among middle aged women Echocardiography may show hypokinesis which does not follow pattern of coronary artery distribution May have elevation of cardiac enzymes Can be reversible
46 Differentiating Etiology of Myocardial Dysfunction Neurogenic Age<50 F>M Diffuse/global dysfunction Cardiogenic Older M>F Regional wall motion abnormalities

47 Neurogenic pulmonary edema Can develop within minutes of CNS injury Causes: changes in pulmonary capillary hydrostatic pressure and permeability due to catecholamine surge Lower PCWP than with nonneurological causes of pulmonary edema repo/viz/full/4664/ jpg; accessed 6/4/08
48 Fever in SAH May be more common in poorer grade SAH patients and those with IVH Mees et al, Stroke, 2008: 42% patients experienced fever, 34% infections Fernandez et al, Neurology, 2007: for every 1 C over 37, 9x inc risk of death, 3x inc risk disability Circuit controlled temperature regulatory mechanisms Acetaminophen, NSAIDs, cyproheptadine
49 Cerebral Salt Wasting Sodium derangements (hyponatremia) common initially thought to be due to SIADH, now understood to be far more commonly due to cerebral natriuresis Hypervolemic therapy rather than fluid restriction Hypertonic saline in refractory cases PO salt tabs (not very effective) Avoidance of hypotonic fluids
50 Standard ICU orders for SAH patients (pre-tx) Hourly neurological checks A-line, maintenance of BP </=140/90 mm Hg Ventilatory support for lethargic patients EVD drainage for lethargic patients, pts with hydrocephalus, EVD at 15 cm H20 to tragus Dilantin/leviteracetam or other AED through first few days
51 Pre-Tx orders ctd Nimodipine 60 mg q4 (can give 30 mg q4 for lower BP) IVF (NS, no hypotonic fluids) Stool softener PPI Non medical DVT prophylaxis
52 ICU orders (post Tx) Liberalization of BP parameters Consider starting SQ heparin for DVT prophylaxis consider lower EVD reservoir level Consider D/Cing AEDs at day 7-14 for grades 1 and 2 without intraparenchymal clot Steroids not routine, but may alleviate chemical meningitis pain
53 Differential of Worsening Neurological Rebleeding Status in SAH Worsening hydrocephalus vasospasm Developing edema or other mass effect Seizures (up to 30% poor grade patients with SAH may have subclinical status epilepticus) Worsening of medical comorbidites/ dysfunction
54 Management of Neurological Decline in SAH Treatment of medical comorbidities Clinical assessment, pupillary exam, look for clinical signs of herniation, if present treat as for ICP crisis Early CT scan If rebleeding or concern for VSP, angiography and treatment additional monitoring (EEG)
55 Management of ICP crisis Osmotic therapy (mannitol, hypertonic saline) Hyperventilation to PCO 2 35 mm Hg Sedation (propofol, extreme cases, barbiturates) CSF diversion or other surgical therapy
56 Predictors of Poor Outcome McDonald et al, Toronto, Canada: Worse Hunt and Hess/WFNS scores Leukocytosis at presentation Hemodynamic instability Mayer et al, Columbia, NY, NY Hypoxemia, Aa gradient>125 mm Hg HCO 3 <20 mmol/l Glucose>180 mg/dl MAP <70, > 130 mm Hg
57 Which Unruptured Aneurysms Should be Treated? All newly discovered aneurysms should be referred for further evaluation ISUIA: Low annual risk of hemorrhage for anterior circulation aneurysms < 7 mm, and posterior/pcom < 5 mm In patients with prior SAH and multiple aneuryms, higher risk of hemorrhage for small aneurysms compared with other pts 2+ Family history 25% lifetime risk SAH
58 Common Intracranial Aneurysm Locations
59 PVHMC pt Intracranial Aneurysm Locations 2, 7.4% 8, 29% 1, 3.7% 0 4, 14.8% 3, 11.1% Dural AVF: 1, 3.7% Angio neg: 4, 14.8% Post circ. 4, 14.8% (1 with assoc. AVM)

60 Mortality by Intracranial Aneurysm Locations 1/2, 3.7/12.5/50% 1/8, 3.7/12.5/12.5% 1/1, 3.7/12.5/100% 0 1/3, 3.7/12.5/33% Post circ. 4/4, 14.8/50/100% % of total # of SAH patients/% of expired patients/% w/in this ANEU group
61 PVHMC SAH Data Total (27) Mort. 8, 29.6% Age Female HH 1-2 HH 3-5 misdx Delay hosp. arr , 59% 8, 29.6% 46 5, 62.5% 1, 12.5% 19, 70.4% 7, 87.5% 3, 11.1% 1, 12.5% 9, 33.3% 4, 50% >1 aneu 3, 11% 1, 12.5


62 65 F H/A, prior R cerebellar infarction,?? R VAD, expired SAH day 7, sepsis, cardiopulmonary arrest Severe atherosclerosis with dense calcification of R VA Inflammatory thrombus of the R VA associated with focal vasculitis
63 Conclusion SAH highly morbid subset of stroke, mortality rates 40% Early aneurysm repair Treatment of concomitant hydrocephalus Close ICU observation during vasospasm period and treatment if it occurs essential Treatment of other medical comorbidities
Current State of the Art
 SAH Current State of the Art Thomas C. Steineke, M.D., Ph.D. Director of Neurovascular Surgery NJ Neuroscience Institute JFK Medical Center Introduction Signs and symptoms of a problem What are aneurysms
SAH Current State of the Art Thomas C. Steineke, M.D., Ph.D. Director of Neurovascular Surgery NJ Neuroscience Institute JFK Medical Center Introduction Signs and symptoms of a problem What are aneurysms
Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage. Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA
 Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA The traditional view: asah is a bad disease Pre-hospital mortality
Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA The traditional view: asah is a bad disease Pre-hospital mortality
TREATMENT OF INTRACRANIAL ANEURYSMS
 TREATMENT OF INTRACRANIAL ANEURYSMS Presented by: Dr Nilesh S. Kurwale Introduction Incidence of aneurysm difficult to estimate Prevalence 0.2-7.9 % Half the aneurysms ruptures 2% present during childhood
TREATMENT OF INTRACRANIAL ANEURYSMS Presented by: Dr Nilesh S. Kurwale Introduction Incidence of aneurysm difficult to estimate Prevalence 0.2-7.9 % Half the aneurysms ruptures 2% present during childhood
4/10/2018. The Surgical Treatment of Cerebral Aneurysms. Aneurysm Locations. Aneurysmal Subarachnoid Hemorrhage. Jerone Kennedy, M.D.
 The Surgical Treatment of Cerebral Aneurysms Aneurysmal Subarachnoid Hemorrhage Jerone Kennedy, M.D. Medical Director, Vascular Neurosurgery CentraCare Health-Neurosciences St. Cloud Hospital Aneurysm
The Surgical Treatment of Cerebral Aneurysms Aneurysmal Subarachnoid Hemorrhage Jerone Kennedy, M.D. Medical Director, Vascular Neurosurgery CentraCare Health-Neurosciences St. Cloud Hospital Aneurysm
TCD AND VASOSPASM SAH
 CURRENT TREATMENT FOR CEREBRAL ANEURYSMS TCD AND VASOSPASM SAH Michigan Sonographers Society 2 Nd Annual Fall Vascular Conference Larry N. Raber RVT-RDMS Clinical Manager General Ultrasound-Neurovascular
CURRENT TREATMENT FOR CEREBRAL ANEURYSMS TCD AND VASOSPASM SAH Michigan Sonographers Society 2 Nd Annual Fall Vascular Conference Larry N. Raber RVT-RDMS Clinical Manager General Ultrasound-Neurovascular
ENDOVASCULAR TREATMENT OF CEREBRAL ANEURYSMS AND MANAGEMENT OF RUPTURED ANEURYSM. Vikram Jadhav MD, PhD. 04/12/2018 CentraCare Health St.
 ENDOVASCULAR TREATMENT OF CEREBRAL ANEURYSMS AND MANAGEMENT OF RUPTURED ANEURYSM Vikram Jadhav MD, PhD 04/12/2018 CentraCare Health St. Cloud, MN OBJECTIVES Understand epidemiology and risk factors for
ENDOVASCULAR TREATMENT OF CEREBRAL ANEURYSMS AND MANAGEMENT OF RUPTURED ANEURYSM Vikram Jadhav MD, PhD 04/12/2018 CentraCare Health St. Cloud, MN OBJECTIVES Understand epidemiology and risk factors for
Sub-arachnoid haemorrhage
 Sub-arachnoid haemorrhage Dr Mary Newton Consultant Anaesthetist The National Hospital for Neurology and Neurosurgery UCL Hospitals NHS Trust mary.newton@uclh.nhs.uk Kiev, Ukraine September 17 th 2009
Sub-arachnoid haemorrhage Dr Mary Newton Consultant Anaesthetist The National Hospital for Neurology and Neurosurgery UCL Hospitals NHS Trust mary.newton@uclh.nhs.uk Kiev, Ukraine September 17 th 2009
Subarachnoid Hemorrhage (SAH) Disclosures/Relationships. Click to edit Master title style. Click to edit Master title style.
 Disclosures/Relationships. Click to edit Master title style. Click to edit Master title style.") Subarachnoid Hemorrhage (SAH) William J. Jones, M.D. Assistant Professor of Neurology Co-Director, UCH Stroke Program Click to edit Master title style Disclosures/Relationships No conflicts of interest
Subarachnoid Hemorrhage (SAH) William J. Jones, M.D. Assistant Professor of Neurology Co-Director, UCH Stroke Program Click to edit Master title style Disclosures/Relationships No conflicts of interest
Aneurysmal Subarachnoid Hemorrhage Presentation and Complications
 Aneurysmal Subarachnoid Hemorrhage Presentation and Complications Sherry H-Y. Chou MD MMSc FNCS Department of Critical Care Medicine, Neurology and Neurosurgery University of Pittsburgh School of Medicine
Aneurysmal Subarachnoid Hemorrhage Presentation and Complications Sherry H-Y. Chou MD MMSc FNCS Department of Critical Care Medicine, Neurology and Neurosurgery University of Pittsburgh School of Medicine
Neurosurgical Management of Stroke
 Overview Hemorrhagic Stroke Ischemic Stroke Aneurysmal Subarachnoid hemorrhage Neurosurgical Management of Stroke Jesse Liu, MD Instructor, Neurological Surgery Initial management In hospital management
Overview Hemorrhagic Stroke Ischemic Stroke Aneurysmal Subarachnoid hemorrhage Neurosurgical Management of Stroke Jesse Liu, MD Instructor, Neurological Surgery Initial management In hospital management
Code Stroke Intervention: Endovascular therapy for asah and management J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY
 Code Stroke Intervention: Endovascular therapy for asah and management J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY Disclosures None Part B. Objectives Epidemiology of asah Concept: What is a brain
Code Stroke Intervention: Endovascular therapy for asah and management J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY Disclosures None Part B. Objectives Epidemiology of asah Concept: What is a brain
Summary of some of the landmark articles:
 Summary of some of the landmark articles: The significance of unruptured intracranial saccular aneurysms: Weibers et al Mayo clinic. 1987 1. 131 patients with 161 aneurysms were followed up at until death,
Summary of some of the landmark articles: The significance of unruptured intracranial saccular aneurysms: Weibers et al Mayo clinic. 1987 1. 131 patients with 161 aneurysms were followed up at until death,
Diagnosis of Subarachnoid Hemorrhage (SAH) and Non- Aneurysmal Causes
 and Non- Aneurysmal Causes") Diagnosis of Subarachnoid Hemorrhage (SAH) and Non- Aneurysmal Causes By Sheila Smith, MD Swedish Medical Center 1 Disclosures I have no disclosures 2 Course Objectives Review significance and differential
Diagnosis of Subarachnoid Hemorrhage (SAH) and Non- Aneurysmal Causes By Sheila Smith, MD Swedish Medical Center 1 Disclosures I have no disclosures 2 Course Objectives Review significance and differential
Neurosurgical decision making in structural lesions causing stroke. Dr Rakesh Ranjan MS, MCh, Dip NB (Neurosurgery)
") Neurosurgical decision making in structural lesions causing stroke Dr Rakesh Ranjan MS, MCh, Dip NB (Neurosurgery) Subarachnoid Hemorrhage Every year, an estimated 30,000 people in the United States experience
Neurosurgical decision making in structural lesions causing stroke Dr Rakesh Ranjan MS, MCh, Dip NB (Neurosurgery) Subarachnoid Hemorrhage Every year, an estimated 30,000 people in the United States experience
Update in Diagnosis and Management of Intracranial Aneurysms for Primary Health Care Providers November 15, 2012 Boston, Massachusetts
 Update in Diagnosis and Management of Intracranial Aneurysms for Primary Health Care Providers November 15, 2012 Boston, Massachusetts Educational Partner: Session 1: Update in Diagnosis and Management
Update in Diagnosis and Management of Intracranial Aneurysms for Primary Health Care Providers November 15, 2012 Boston, Massachusetts Educational Partner: Session 1: Update in Diagnosis and Management
CEREBRO VASCULAR ACCIDENTS
 CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
7/18/2018. Cerebral Vasospasm: Current and Emerging Therapies. Disclosures. Objectives
 Cerebral : Current and Emerging Therapies Chad W. Washington MS, MD, MPHS Assistant Professor Department of Neurosurgery Disclosures None Objectives Brief Overview How we got here Review of Trials Meta-analysis
Cerebral : Current and Emerging Therapies Chad W. Washington MS, MD, MPHS Assistant Professor Department of Neurosurgery Disclosures None Objectives Brief Overview How we got here Review of Trials Meta-analysis
/ / / / / / Hospital Abstraction: Stroke/TIA. Participant ID: Hospital Code: Multi-Ethnic Study of Atherosclerosis
 Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Subarachnoid Hemorrhage and Brain Aneurysm
 Subarachnoid Hemorrhage and Brain Aneurysm DIN Department of Interventional Neurology What is SAH? Subarachnoid Haemorrhage is the sudden leaking (haemorrhage) of blood from the blood vessels of brain.
Subarachnoid Hemorrhage and Brain Aneurysm DIN Department of Interventional Neurology What is SAH? Subarachnoid Haemorrhage is the sudden leaking (haemorrhage) of blood from the blood vessels of brain.
Definition พ.ญ.ส ธ ดา เย นจ นทร. Epidemiology. Definition 5/25/2016. Seizures after stroke Can we predict? Poststroke seizure
 Seizures after stroke Can we predict? พ.ญ.ส ธ ดา เย นจ นทร PMK Epilepsy Annual Meeting 2016 Definition Poststroke seizure : single or multiple convulsive episode(s) after stroke and thought to be related
Seizures after stroke Can we predict? พ.ญ.ส ธ ดา เย นจ นทร PMK Epilepsy Annual Meeting 2016 Definition Poststroke seizure : single or multiple convulsive episode(s) after stroke and thought to be related
Acute stroke update 2016 innovations in managing ischemic and hemorrhagic disease
 Acute stroke update 2016 innovations in managing ischemic and hemorrhagic disease Christopher Koebbe, MD Endovascular Neurosurgeon Florida Spine Institute Director of Neurosciences Northside Hospital Overview
Acute stroke update 2016 innovations in managing ischemic and hemorrhagic disease Christopher Koebbe, MD Endovascular Neurosurgeon Florida Spine Institute Director of Neurosciences Northside Hospital Overview
Intra-arterial nimodipine for the treatment of vasospasm due to aneurysmal subarachnoid hemorrhage
 Romanian Neurosurgery (2016) XXX 4: 461 466 461 DOI: 10.1515/romneu-2016-0074 Intra-arterial nimodipine for the treatment of vasospasm due to aneurysmal subarachnoid hemorrhage A. Chiriac, Georgiana Ion*,
Romanian Neurosurgery (2016) XXX 4: 461 466 461 DOI: 10.1515/romneu-2016-0074 Intra-arterial nimodipine for the treatment of vasospasm due to aneurysmal subarachnoid hemorrhage A. Chiriac, Georgiana Ion*,
Multi-modality management of intracranial aneurysms
 Multi-modality management of intracranial aneurysms Christopher Koebbe, Maj, USAF, MC Staff Neurosurgeon San Antonio Military Medical Consortium Clinical Assistant Professor Department of Neurological
Multi-modality management of intracranial aneurysms Christopher Koebbe, Maj, USAF, MC Staff Neurosurgeon San Antonio Military Medical Consortium Clinical Assistant Professor Department of Neurological
Ischemia cerebrale dopo emorragia subaracnoidea Vasospasmo e altri nemici
 Ischemia cerebrale dopo emorragia subaracnoidea Vasospasmo e altri nemici Nino Stocchetti Milan University Neuroscience ICU Ospedale Policlinico IRCCS Milano stocchet@policlinico.mi.it Macdonald RL et
Ischemia cerebrale dopo emorragia subaracnoidea Vasospasmo e altri nemici Nino Stocchetti Milan University Neuroscience ICU Ospedale Policlinico IRCCS Milano stocchet@policlinico.mi.it Macdonald RL et
WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE
 WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE Subarachnoid Hemorrhage is a serious, life-threatening type of hemorrhagic stroke caused by bleeding into the space surrounding the brain,
WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE Subarachnoid Hemorrhage is a serious, life-threatening type of hemorrhagic stroke caused by bleeding into the space surrounding the brain,
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
Small UIAs, <7 mm in diameter, uncommonly cause aneurysmal symptoms and are the most frequently detected incidentally.
 Research grant from Stryker Neurovascular Research grant from Covidien/ Medtronic Consultant and proctor for Stryker Neurovascular Consultant and proctor for Covidien/ Medtronic Consultant for Codman Neurovascular
Research grant from Stryker Neurovascular Research grant from Covidien/ Medtronic Consultant and proctor for Stryker Neurovascular Consultant and proctor for Covidien/ Medtronic Consultant for Codman Neurovascular
Comparison of Five Major Recent Endovascular Treatment Trials
 Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
SAH READMISSIONS TO NCCU
 SAH READMISSIONS TO NCCU Are they preventable? João Amaral Rebecca Gorf Critical Care Outreach Team - NHNN 2015 Total admissions to NCCU =862 Total SAH admitted to NCCU= 104 (93e) (12.0%) Total SAH readmissions=
SAH READMISSIONS TO NCCU Are they preventable? João Amaral Rebecca Gorf Critical Care Outreach Team - NHNN 2015 Total admissions to NCCU =862 Total SAH admitted to NCCU= 104 (93e) (12.0%) Total SAH readmissions=
Modern Management of ICH
 Modern Management of ICH Bradley A. Gross, MD Assistant Professor, Dept of Neurosurgery, University of Pittsburgh October 2018 ICH Background Assessment & Diagnosis Medical Management Surgical Management
Modern Management of ICH Bradley A. Gross, MD Assistant Professor, Dept of Neurosurgery, University of Pittsburgh October 2018 ICH Background Assessment & Diagnosis Medical Management Surgical Management
Subarachnoid Bleeds. Under the Spider via deepthought 1 / 22
 Subarachnoid Bleeds Under the Spider via deepthought 1 / 22 SAH: symptoms worst headache of my life Sudden-onset Severe w max intensity in seconds = thunderclap Sentinel headache in ~10-40% in aneurysmal
Subarachnoid Bleeds Under the Spider via deepthought 1 / 22 SAH: symptoms worst headache of my life Sudden-onset Severe w max intensity in seconds = thunderclap Sentinel headache in ~10-40% in aneurysmal
11/27/2017. Stroke Management in the Neurocritical Care Unit. Conflict of interest. Karel Fuentes MD Medical Director of Neurocritical Care
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Stroke - Intracranial hemorrhage. Dr. Amitesh Aggarwal Associate Professor Department of Medicine
 Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
CENTRAL NERVOUS SYSTEM TRAUMA and Subarachnoid Hemorrhage. By: Shifaa AlQa qa
 CENTRAL NERVOUS SYSTEM TRAUMA and Subarachnoid Hemorrhage By: Shifaa AlQa qa Subarachnoid Hemorrhage Causes: Rupture of a saccular (berry) aneurysm Vascular malformation Trauma Hematologic disturbances
CENTRAL NERVOUS SYSTEM TRAUMA and Subarachnoid Hemorrhage By: Shifaa AlQa qa Subarachnoid Hemorrhage Causes: Rupture of a saccular (berry) aneurysm Vascular malformation Trauma Hematologic disturbances
Acute stroke imaging
 Acute stroke imaging Aims Imaging modalities and differences Why image acute stroke Clinical correlation to imaging appearance What is stroke Classic definition: acute focal injury to the central nervous
Acute stroke imaging Aims Imaging modalities and differences Why image acute stroke Clinical correlation to imaging appearance What is stroke Classic definition: acute focal injury to the central nervous
[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]
![[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]](/thumbs/89/98619893.jpg "[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]") 2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
Interventions in the Management of Acute Stroke. Dr Md Shafiqul Islam Associate Professor Neurosurgery Dhaka Medical College Hospital
 Interventions in the Management of Acute Stroke Dr Md Shafiqul Islam Associate Professor Neurosurgery Dhaka Medical College Hospital Acute stroke intervention Number of stroke patients increasing day by
Interventions in the Management of Acute Stroke Dr Md Shafiqul Islam Associate Professor Neurosurgery Dhaka Medical College Hospital Acute stroke intervention Number of stroke patients increasing day by
Management of the Endovascular Patient and Acute Emergencies in the Angio Suite
 Management of the Endovascular Patient and Acute Emergencies in the Angio Suite June 9, 2015 Bridget Cantrell, APN, CNP Endovascular Neurosurgery Advocate Medical Group No Disclosures The human brain is
Management of the Endovascular Patient and Acute Emergencies in the Angio Suite June 9, 2015 Bridget Cantrell, APN, CNP Endovascular Neurosurgery Advocate Medical Group No Disclosures The human brain is
The Worst Headache of My Life Hemorrhagic Stroke
 The Worst Headache of My Life Hemorrhagic Stroke Lindsay Trantum ACNP-BC Neurocritical Care Nurse Practitioner Assistant in Anesthesiology, Division of Critical Care Objectives Identify the risk factors
The Worst Headache of My Life Hemorrhagic Stroke Lindsay Trantum ACNP-BC Neurocritical Care Nurse Practitioner Assistant in Anesthesiology, Division of Critical Care Objectives Identify the risk factors
North Oaks Trauma Symposium Friday, November 3, 2017
 Traumatic Intracranial Hemorrhage Aaron C. Sigler, DO, MS Neurosurgery Tulane Neurosciences None Disclosures Overview Anatomy Epidural hematoma Subdural hematoma Cerebral contusions Outline Traumatic ICH
Traumatic Intracranial Hemorrhage Aaron C. Sigler, DO, MS Neurosurgery Tulane Neurosciences None Disclosures Overview Anatomy Epidural hematoma Subdural hematoma Cerebral contusions Outline Traumatic ICH
CLEAR III TRIAL : UPDATE ON SURGICAL MATTERS THAT MATTER
 CLEAR III TRIAL : UPDATE ON SURGICAL MATTERS THAT MATTER CLEAR Surgical Center Team July 2011 Trial Enrollment Status Updates Insert latest enrollment update chart from most recent CLEAR newsletter Imaging
CLEAR III TRIAL : UPDATE ON SURGICAL MATTERS THAT MATTER CLEAR Surgical Center Team July 2011 Trial Enrollment Status Updates Insert latest enrollment update chart from most recent CLEAR newsletter Imaging
Hypertensive Haemorrhagic Stroke. Dr Philip Lam Thuon Mine
 Hypertensive Haemorrhagic Stroke Dr Philip Lam Thuon Mine Intracerebral Haemorrhage Primary ICH Spontaneous rupture of small vessels damaged by HBP Basal ganglia, thalamus, pons and cerebellum Amyloid
Hypertensive Haemorrhagic Stroke Dr Philip Lam Thuon Mine Intracerebral Haemorrhage Primary ICH Spontaneous rupture of small vessels damaged by HBP Basal ganglia, thalamus, pons and cerebellum Amyloid
Protocol for IV rtpa Treatment of Acute Ischemic Stroke
 Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Alessandro Della Puppa
 Intraoperative measurement of arterial blood flow in complex cerebral aneurysms surgery Studio flussimetrico intra-operatorio nel clipping degli aneurismi complessi Alessandro Della Puppa NEUROSURGERY
Intraoperative measurement of arterial blood flow in complex cerebral aneurysms surgery Studio flussimetrico intra-operatorio nel clipping degli aneurismi complessi Alessandro Della Puppa NEUROSURGERY
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for
 Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine
 Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
Small and medium size intracranial aneurysms - a 5 years retrospective analysis trial and multimodal treatment
 Romanian Neurosurgery (2015) XXIX 4: 417-426 417 DOI: 10.1515/romneu-2015-0057 Small and medium size intracranial aneurysms - a 5 years retrospective analysis trial and multimodal treatment Valentin Munteanu
Romanian Neurosurgery (2015) XXIX 4: 417-426 417 DOI: 10.1515/romneu-2015-0057 Small and medium size intracranial aneurysms - a 5 years retrospective analysis trial and multimodal treatment Valentin Munteanu
AEROMEDICAL DECISION MAKING IN CEREBRAL ANEURYSMS. Pooshan Navāthé Michael Drane Peter Clem David Fitzgerald
 AEROMEDICAL DECISION MAKING IN CEREBRAL ANEURYSMS Pooshan Navāthé Michael Drane Peter Clem David Fitzgerald Disclaimer I receive a salary from the Commonwealth of Australia. I have no financial relationships
AEROMEDICAL DECISION MAKING IN CEREBRAL ANEURYSMS Pooshan Navāthé Michael Drane Peter Clem David Fitzgerald Disclaimer I receive a salary from the Commonwealth of Australia. I have no financial relationships
Case 1. Case 5/30/2013. Traumatic Brain Injury : Review, Update, and Controversies
 Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
11/23/2015. Disclosures. Stroke Management in the Neurocritical Care Unit. Karel Fuentes MD Medical Director of Neurocritical Care.
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Classification of Stroke. CNA Neuroscience Nursing Course: Cerebrovascular Disorders. Stroke in Canada
 CNA Neuroscience Nursing Course: Cerebrovascular Disorders Breeda O Farrell RN(EC), MScN, CNN(C) Nurse Practitioner Neurology University Hospital, London Health Science Centre London, ON Deb Bisnaire RN(EC),
CNA Neuroscience Nursing Course: Cerebrovascular Disorders Breeda O Farrell RN(EC), MScN, CNN(C) Nurse Practitioner Neurology University Hospital, London Health Science Centre London, ON Deb Bisnaire RN(EC),
The Endovascular Treatment of Cerebral Aneurysms
 The Endovascular Treatment of Cerebral Aneurysms George P. Teitelbaum, M.D., FSIR Regional Director, Neurointerventional Surgery Providence, California Types of Stroke and Their Causes Ischemic (87%):
The Endovascular Treatment of Cerebral Aneurysms George P. Teitelbaum, M.D., FSIR Regional Director, Neurointerventional Surgery Providence, California Types of Stroke and Their Causes Ischemic (87%):
Paul Gigante HMS IV Gillian Lieberman, MD. Sept Mr. T s T s Headache. Paul Gigante,, Harvard Medical School Year IV Gillian Lieberman, MD
 Sept 2005 Mr. T s T s Headache Paul Gigante,, Harvard Medical School Year IV Mr. T s T s Presentation 45 year-old welder complains of sudden severe headache and witnessed seizure with loss of consciousness
Sept 2005 Mr. T s T s Headache Paul Gigante,, Harvard Medical School Year IV Mr. T s T s Presentation 45 year-old welder complains of sudden severe headache and witnessed seizure with loss of consciousness
Disclosures. Objectives. Critical Care Management of Subarachnoid Hemorrhage. Nothing to disclose
 Critical Care Management of Subarachnoid Hemorrhage Nerissa U. Ko, MD, MAS UCSF Department of Neurology September 7, 2013 Nothing to disclose Disclosures Grant funding from American Heart Association,
Critical Care Management of Subarachnoid Hemorrhage Nerissa U. Ko, MD, MAS UCSF Department of Neurology September 7, 2013 Nothing to disclose Disclosures Grant funding from American Heart Association,
TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES
 TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES ALBERTO MAUD, MD ASSOCIATE PROFESSOR TEXAS TECH UNIVERSITY HEALTH SCIENCES CENTER EL PASO PAUL L. FOSTER SCHOOL OF MEDICINE 18TH ANNUAL RIO GRANDE TRAUMA 2017
TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES ALBERTO MAUD, MD ASSOCIATE PROFESSOR TEXAS TECH UNIVERSITY HEALTH SCIENCES CENTER EL PASO PAUL L. FOSTER SCHOOL OF MEDICINE 18TH ANNUAL RIO GRANDE TRAUMA 2017
Supplement Table 1. Definitions for Causes of Death
 Supplement Table 1. Definitions for Causes of Death 3. Cause of Death: To record the primary cause of death. Record only one answer. Classify cause of death as one of the following: 3.1 Cardiac: Death
Supplement Table 1. Definitions for Causes of Death 3. Cause of Death: To record the primary cause of death. Record only one answer. Classify cause of death as one of the following: 3.1 Cardiac: Death
H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute
 H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute Memorial Hermann- Texas Medical Center Learning Objectives
H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute Memorial Hermann- Texas Medical Center Learning Objectives
lek Magdalena Puławska-Stalmach
 lek Magdalena Puławska-Stalmach tytuł pracy: Kliniczne i radiologiczne aspekty tętniaków wewnątrzczaszkowych a wybór metody leczenia Summary An aneurysm is a localized, abnormal distended lumen of the
lek Magdalena Puławska-Stalmach tytuł pracy: Kliniczne i radiologiczne aspekty tętniaków wewnątrzczaszkowych a wybór metody leczenia Summary An aneurysm is a localized, abnormal distended lumen of the
Oltre la terapia medica nelle dissezioni carotidee
 Oltre la terapia medica nelle dissezioni carotidee Rodolfo Pini Chirurgia Vascolare Università di bologna Alma Mater Studiorum Carotid and Vertebral Artery Dissection What we know from the literature Epidemiology
Oltre la terapia medica nelle dissezioni carotidee Rodolfo Pini Chirurgia Vascolare Università di bologna Alma Mater Studiorum Carotid and Vertebral Artery Dissection What we know from the literature Epidemiology
CEREBRAL ANEURYSM. Epidemiology. Number of Case per Year 12/15/2008. Wanarak Watcharasakailp M.D.
 Epidemiology CEREBRAL ANEURYSM Wanarak Watcharasakailp M.D. 5-10% of all stroke 6-7 /100,000 persons/yrs, 20/100,000 in Finland and Japan Female predominant Most in anterior circulation Female->ICA 36.8%
Epidemiology CEREBRAL ANEURYSM Wanarak Watcharasakailp M.D. 5-10% of all stroke 6-7 /100,000 persons/yrs, 20/100,000 in Finland and Japan Female predominant Most in anterior circulation Female->ICA 36.8%
Shawke A. Soueidan, MD. Riverside Neurology & Sleep Specialists
 Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery
 Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery 2 Stroke Stroke kills almost 130,000 Americans each year. - Third cause of all deaths in Arkansas. - Death Rate is highest in
Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery 2 Stroke Stroke kills almost 130,000 Americans each year. - Third cause of all deaths in Arkansas. - Death Rate is highest in
Index. C Capillary telangiectasia, intracerebral hemorrhage in, 295 Carbon monoxide, formation of, in intracerebral hemorrhage, edema due to,
 Neurosurg Clin N Am 13 (2002) 395 399 Index Note: Page numbers of article titles are in boldface type. A Age factors, in intracerebral hemorrhage outcome, 344 Albumin, for intracerebral hemorrhage, 336
Neurosurg Clin N Am 13 (2002) 395 399 Index Note: Page numbers of article titles are in boldface type. A Age factors, in intracerebral hemorrhage outcome, 344 Albumin, for intracerebral hemorrhage, 336
ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS. Justin Nolte, MD Assistant Profession Marshall University School of Medicine
 ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS Justin Nolte, MD Assistant Profession Marshall University School of Medicine History of Presenting Illness 64 yo wf with PMHx of COPD, HTN, HLP who was in
ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS Justin Nolte, MD Assistant Profession Marshall University School of Medicine History of Presenting Illness 64 yo wf with PMHx of COPD, HTN, HLP who was in
ISCHEMIC STROKE IMAGING
 ISCHEMIC STROKE IMAGING ผศ.พญ พญ.จ ร ร ตน ธรรมโรจน ภาคว ชาร งส ว ทยา คณะแพทยศาสตร มหาว ทยาล ยขอนแก น A case of acute hemiplegia Which side is the abnormality, right or left? Early Right MCA infarction
ISCHEMIC STROKE IMAGING ผศ.พญ พญ.จ ร ร ตน ธรรมโรจน ภาคว ชาร งส ว ทยา คณะแพทยศาสตร มหาว ทยาล ยขอนแก น A case of acute hemiplegia Which side is the abnormality, right or left? Early Right MCA infarction
Traumatic Brain Injury:
 Traumatic Brain Injury: Changes in Management Across the Spectrum of Age and Time Omaha 2018 Trauma Symposium June 15, 2018 Gail T. Tominaga, M.D., F.A.C.S. Scripps Memorial Hospital La Jolla Outline Background
Traumatic Brain Injury: Changes in Management Across the Spectrum of Age and Time Omaha 2018 Trauma Symposium June 15, 2018 Gail T. Tominaga, M.D., F.A.C.S. Scripps Memorial Hospital La Jolla Outline Background
State of the Art Multimodal Monitoring
 State of the Art Multimodal Monitoring Baptist Neurological Institute Mohamad Chmayssani, MD Disclosures I have no financial relationships to disclose with makers of the products here discussed. Outline
State of the Art Multimodal Monitoring Baptist Neurological Institute Mohamad Chmayssani, MD Disclosures I have no financial relationships to disclose with makers of the products here discussed. Outline
Supplementary material 1. Definitions of study endpoints (extracted from the Endpoint Validation Committee Charter) 1.
 1.") Rationale, design, and baseline characteristics of the SIGNIFY trial: a randomized, double-blind, placebo-controlled trial of ivabradine in patients with stable coronary artery disease without clinical
Rationale, design, and baseline characteristics of the SIGNIFY trial: a randomized, double-blind, placebo-controlled trial of ivabradine in patients with stable coronary artery disease without clinical
Repair of Intracranial Vessel Perforation with Onyx-18 Using an Exovascular Retreating Catheter Technique
 Repair of Intracranial Vessel Perforation with Onyx-18 Using an Exovascular Retreating Catheter Technique Michael Horowitz M.D. Pittsburgh, Pennsylvania Background Iatrogenic intraprocedural rupture rates
Repair of Intracranial Vessel Perforation with Onyx-18 Using an Exovascular Retreating Catheter Technique Michael Horowitz M.D. Pittsburgh, Pennsylvania Background Iatrogenic intraprocedural rupture rates
Cerebral Vascular Diseases. Nabila Hamdi MD, PhD
 Cerebral Vascular Diseases Nabila Hamdi MD, PhD Outline I. Stroke statistics II. Cerebral circulation III. Clinical symptoms of stroke IV. Pathogenesis of cerebral infarcts (Stroke) 1. Ischemic - Thrombotic
Cerebral Vascular Diseases Nabila Hamdi MD, PhD Outline I. Stroke statistics II. Cerebral circulation III. Clinical symptoms of stroke IV. Pathogenesis of cerebral infarcts (Stroke) 1. Ischemic - Thrombotic
Disclosures. Take Home Points 9/6/2014. Endovascular Treatment of Aneurysms and Pseudoaneurysms
 Endovascular Treatment of Aneurysms and Pseudoaneurysms UCSF Stroke and Aneurysm Update CME Saturday September 6, 2014 Steven W. Hetts, MD Associate Professor of Radiology Interventional Neuroradiology
Endovascular Treatment of Aneurysms and Pseudoaneurysms UCSF Stroke and Aneurysm Update CME Saturday September 6, 2014 Steven W. Hetts, MD Associate Professor of Radiology Interventional Neuroradiology
A Less Invasive Approach for Ruptured Aneurysm with Intracranial Hematoma: Coil Embolization Followed by Clot Evacuation
 A Less Invasive Approach for Ruptured Aneurysm with Intracranial Hematoma: Coil Embolization Followed by Clot Evacuation Je Hoon Jeong, MD 1 Jun Seok Koh, MD 1 Eui Jong Kim, MD 2 Index terms: Endovascular
A Less Invasive Approach for Ruptured Aneurysm with Intracranial Hematoma: Coil Embolization Followed by Clot Evacuation Je Hoon Jeong, MD 1 Jun Seok Koh, MD 1 Eui Jong Kim, MD 2 Index terms: Endovascular
Standardize comprehensive care of the patient with severe traumatic brain injury
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Non-Traumatic Neuro Emergencies
 Department of Radiology University of California San Diego Non-Traumatic Neuro Emergencies John R. Hesselink, M.D. Nontraumatic Neuroemergencies 1. Acute focal neurological deficit 2. Worst headache of
Department of Radiology University of California San Diego Non-Traumatic Neuro Emergencies John R. Hesselink, M.D. Nontraumatic Neuroemergencies 1. Acute focal neurological deficit 2. Worst headache of
Moyamoya Syndrome with contra lateral DACA aneurysm: First Case report with review of literature
 Romanian Neurosurgery Volume XXXI Number 3 2017 July-September Article Moyamoya Syndrome with contra lateral DACA aneurysm: First Case report with review of literature Ashish Kumar Dwivedi, Pradeep Kumar,
Romanian Neurosurgery Volume XXXI Number 3 2017 July-September Article Moyamoya Syndrome with contra lateral DACA aneurysm: First Case report with review of literature Ashish Kumar Dwivedi, Pradeep Kumar,
Fundus findings in spontaneous subarachnoid hemorrhage and their correlation with neurologic characteristics
 European Journal of Ophthalmology / Vol. 19 no. 3, 2009 / pp. 460-465 Fundus findings in spontaneous subarachnoid hemorrhage and their correlation with neurologic characteristics MORTEZA ENTEZARI 1, SHIRZAD
European Journal of Ophthalmology / Vol. 19 no. 3, 2009 / pp. 460-465 Fundus findings in spontaneous subarachnoid hemorrhage and their correlation with neurologic characteristics MORTEZA ENTEZARI 1, SHIRZAD
Cerebrovascular Disease
 Neuropathology lecture series Cerebrovascular Disease Physiology of cerebral blood flow Brain makes up only 2% of body weight Percentage of cardiac output: 15-20% Percentage of O 2 consumption (resting):
Neuropathology lecture series Cerebrovascular Disease Physiology of cerebral blood flow Brain makes up only 2% of body weight Percentage of cardiac output: 15-20% Percentage of O 2 consumption (resting):
Management of Cerebral Aneurysms in Polycystic Kidney Disease. Dr H Stockley Consultant Neuroradiologist Greater Manchester Neuroscience Centre
 Management of Cerebral Aneurysms in Polycystic Kidney Disease Dr H Stockley Consultant Neuroradiologist Greater Manchester Neuroscience Centre What is a cerebral aneurysm? Developmental degenerative arterial
Management of Cerebral Aneurysms in Polycystic Kidney Disease Dr H Stockley Consultant Neuroradiologist Greater Manchester Neuroscience Centre What is a cerebral aneurysm? Developmental degenerative arterial
Introduction to Neurosurgical Subspecialties:
 Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
TRANSCRANIAL DOPPLER ULTRASOUND INTRODUCTION TO TCD INTERPRETATION
 TRANSCRANIAL DOPPLER ULTRASOUND INTRODUCTION TO TCD INTERPRETATION ---Rune Aaslid First TCD Publication 1982 WHAT IS TCD? Uses 2 MHz pulsed Doppler ultrasound Passes through cranial windows Provides information
TRANSCRANIAL DOPPLER ULTRASOUND INTRODUCTION TO TCD INTERPRETATION ---Rune Aaslid First TCD Publication 1982 WHAT IS TCD? Uses 2 MHz pulsed Doppler ultrasound Passes through cranial windows Provides information
Case Report 1. CTA head. (c) Tele3D Advantage, LLC
 Tele3D Advantage, LLC") Case Report 1 CTA head 1 History 82 YEAR OLD woman with signs and symptoms of increased intra cranial pressure in setting of SAH. CT Brain was performed followed by CT Angiography of head. 2 CT brain Extensive
Case Report 1 CTA head 1 History 82 YEAR OLD woman with signs and symptoms of increased intra cranial pressure in setting of SAH. CT Brain was performed followed by CT Angiography of head. 2 CT brain Extensive
Michael Horowitz, MD Pittsburgh, PA
 Michael Horowitz, MD Pittsburgh, PA Introduction Cervical Artery Dissection occurs by a rupture within the arterial wall leading to an intra-mural Hematoma. A possible consequence is an acute occlusion
Michael Horowitz, MD Pittsburgh, PA Introduction Cervical Artery Dissection occurs by a rupture within the arterial wall leading to an intra-mural Hematoma. A possible consequence is an acute occlusion
GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE
 2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
2. Subarachnoid Hemorrhage
 Causes: 2. Subarachnoid Hemorrhage A. Saccular (berry) aneurysm - Is the most frequent cause of clinically significant subarachnoid hemorrhage is rupture of a saccular (berry) aneurysm. B. Vascular malformation
Causes: 2. Subarachnoid Hemorrhage A. Saccular (berry) aneurysm - Is the most frequent cause of clinically significant subarachnoid hemorrhage is rupture of a saccular (berry) aneurysm. B. Vascular malformation
(aneurysmal subarachnoid hemorrhage, 17%~60% :SAH. ,asah , 22%~49% : Willis. :1927 Moniz ;(3) 2. ischemic neurological deficit,dind) SAH) SAH ;(6)
 2. ischemic neurological deficit,dind) SAH) SAH ;(6)") ,, 2. : ;,, :(1), (delayed ;(2) ischemic neurological deficit,dind) ;(3) 2. :SAH ;(4) 5-10 10 HT -1-1 ;(5), 10 SAH ;(6) - - 27%~50%, ( cerebral vasospasm ) Glasgow (Glasgow Coma Scale,GCS), [1],, (aneurysmal
,, 2. : ;,, :(1), (delayed ;(2) ischemic neurological deficit,dind) ;(3) 2. :SAH ;(4) 5-10 10 HT -1-1 ;(5), 10 SAH ;(6) - - 27%~50%, ( cerebral vasospasm ) Glasgow (Glasgow Coma Scale,GCS), [1],, (aneurysmal
UPSTATE Comprehensive Stroke Center. Neurosurgical Interventions Satish Krishnamurthy MD, MCh
 UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic
UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic
Subclavian artery Stenting
 Subclavian artery Stenting Etiology Atherosclerosis Takayasu s arteritis Fibromuscular dysplasia Giant Cell Arteritis Radiation-induced Vascular Injury Thoracic Outlet Syndrome Neurofibromatosis Incidence
Subclavian artery Stenting Etiology Atherosclerosis Takayasu s arteritis Fibromuscular dysplasia Giant Cell Arteritis Radiation-induced Vascular Injury Thoracic Outlet Syndrome Neurofibromatosis Incidence
Coiling of ruptured and unruptured intracranial aneurysms
 ORIGINAL RESEARCH W.J. van Rooij G.J. Keeren J.P.P. Peluso M. Sluzewski Clinical and Angiographic Results of Coiling of 196 Very Small (< 3 mm) Intracranial Aneurysms BACKGROUND AND PURPOSE: Coiling of
ORIGINAL RESEARCH W.J. van Rooij G.J. Keeren J.P.P. Peluso M. Sluzewski Clinical and Angiographic Results of Coiling of 196 Very Small (< 3 mm) Intracranial Aneurysms BACKGROUND AND PURPOSE: Coiling of
8/29/2011. Brain Injury Incidence: 200/100,000. Prehospital Brain Injury Mortality Incidence: 20/100,000
 Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Medical Management of Intracranial Hypertension. Joao A. Gomes, MD FAHA Head, Neurointensive Care Unit Cerebrovascular Center
 Medical Management of Intracranial Hypertension Joao A. Gomes, MD FAHA Head, Neurointensive Care Unit Cerebrovascular Center Anatomic and Physiologic Principles Intracranial compartments Brain 80% (1,400
Medical Management of Intracranial Hypertension Joao A. Gomes, MD FAHA Head, Neurointensive Care Unit Cerebrovascular Center Anatomic and Physiologic Principles Intracranial compartments Brain 80% (1,400
Disclosures. CREST Trial: Summary. Lecture Outline 4/16/2015. Cervical Atherosclerotic Disease
 Disclosures Your Patient Has Carotid Bulb Stenosis and a Tandem Intracranial Stenosis: How Do SAMMPRIS and Other Evidence Inform Your Treatment? UCSF Vascular Symposium 2015 Steven W. Hetts, MD Associate
Disclosures Your Patient Has Carotid Bulb Stenosis and a Tandem Intracranial Stenosis: How Do SAMMPRIS and Other Evidence Inform Your Treatment? UCSF Vascular Symposium 2015 Steven W. Hetts, MD Associate
Daniel A Capen MD Downey Orthopedic Group COMPLICATIONS IN CERVICAL AND LUMBAR SPINAL SURGERY
 Daniel A Capen MD Downey Orthopedic Group COMPLICATIONS IN CERVICAL AND LUMBAR SPINAL SURGERY Complications in Spinal Surgery Positioning Complications Approach Complications Procedure Complications Post-surgical
Daniel A Capen MD Downey Orthopedic Group COMPLICATIONS IN CERVICAL AND LUMBAR SPINAL SURGERY Complications in Spinal Surgery Positioning Complications Approach Complications Procedure Complications Post-surgical
Pre-hospital Response to Trauma and Brain Injury. Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center
 Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
Coil Embolization for Intracranial Aneurysms
 Ontario Health Technology Assessment Series 2006; Vol. 6, No. 1 Coil Embolization for Intracranial Aneurysms An Evidence-Based Analysis January 2006 Medical Advisory Secretariat Ministry of Health and
Ontario Health Technology Assessment Series 2006; Vol. 6, No. 1 Coil Embolization for Intracranial Aneurysms An Evidence-Based Analysis January 2006 Medical Advisory Secretariat Ministry of Health and
Nicolas Bianchi M.D. May 15th, 2012
 Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
NIH Public Access Author Manuscript J Am Coll Radiol. Author manuscript; available in PMC 2013 June 24.
 NIH Public Access Author Manuscript Published in final edited form as: J Am Coll Radiol. 2010 January ; 7(1): 73 76. doi:10.1016/j.jacr.2009.06.015. Cerebral Aneurysms Janet C. Miller, DPhil, Joshua A.
NIH Public Access Author Manuscript Published in final edited form as: J Am Coll Radiol. 2010 January ; 7(1): 73 76. doi:10.1016/j.jacr.2009.06.015. Cerebral Aneurysms Janet C. Miller, DPhil, Joshua A.
THE EFFICACY AND SAFETY OF CILOSTAZOL IN SUBARACHNOID HEMORRHAGE. A META- ANALYSIS OF RANDOMIZED AND NON RANDOMIZED STUDIES DR. MUHAMMAD F.
 THE EFFICACY AND SAFETY OF CILOSTAZOL IN SUBARACHNOID HEMORRHAGE. A META- ANALYSIS OF RANDOMIZED AND NON RANDOMIZED STUDIES DR. MUHAMMAD F. ISHFAQ ZEENAT QURESHI STROKE INSTITUTE AND UNIVERSITY OF TENNESSEE,
THE EFFICACY AND SAFETY OF CILOSTAZOL IN SUBARACHNOID HEMORRHAGE. A META- ANALYSIS OF RANDOMIZED AND NON RANDOMIZED STUDIES DR. MUHAMMAD F. ISHFAQ ZEENAT QURESHI STROKE INSTITUTE AND UNIVERSITY OF TENNESSEE,
What You Should Know About Cerebral Aneurysms
 American Society of Neuroradiology American Society of Interventional & Therapeutic Neuroradiology What You Should Know About Cerebral Aneurysms From the Cerebrovascular Imaging and Intervention Committee
American Society of Neuroradiology American Society of Interventional & Therapeutic Neuroradiology What You Should Know About Cerebral Aneurysms From the Cerebrovascular Imaging and Intervention Committee
Cerebral Aneurysms. U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Public Health Service National Institutes of Health
 Cerebral Aneurysms U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Public Health Service National Institutes of Health Cerebral Aneurysms What is a cerebral aneurysm? cerebral aneurysm (also known as an
Cerebral Aneurysms U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Public Health Service National Institutes of Health Cerebral Aneurysms What is a cerebral aneurysm? cerebral aneurysm (also known as an
Hypertensives Emergency and Urgency
 Hypertensives Emergency and Urgency Budi Yuli Setianto Cardiology Divisision Department of Internal Medicine Faculty of Medicine UGM Sardjito Hospital Yogyakarta Background USA: Hypertension is 30% of
Hypertensives Emergency and Urgency Budi Yuli Setianto Cardiology Divisision Department of Internal Medicine Faculty of Medicine UGM Sardjito Hospital Yogyakarta Background USA: Hypertension is 30% of