Medical Management of Intracranial Hypertension. Joao A. Gomes, MD FAHA Head, Neurointensive Care Unit Cerebrovascular Center
|
|
|
- Lesley Richardson
- 5 years ago
- Views:
Transcription
1 Medical Management of Intracranial Hypertension Joao A. Gomes, MD FAHA Head, Neurointensive Care Unit Cerebrovascular Center
2 Anatomic and Physiologic Principles
 CSF 75-150 cc (10%): 50%")
: 70%")
3 Intracranial compartments Brain 80% (1,400 cc) CSF cc (10%): 50% intraventricular and 50% subarachnoid compartment Blood cc (10%): 70% venous, 30% arterial

4 Monro-Kelly doctrine An increase in the volume of one compartment must be accompanied by an approximately equal decrease in the volume of the other compartments to maintain normal ICP

5 Compensation Shift of CSF from the intracranial to the spinal thecal compartment Dural sinus collapse and arterial vasoconstriction: decreased CBV Brain herniation
6
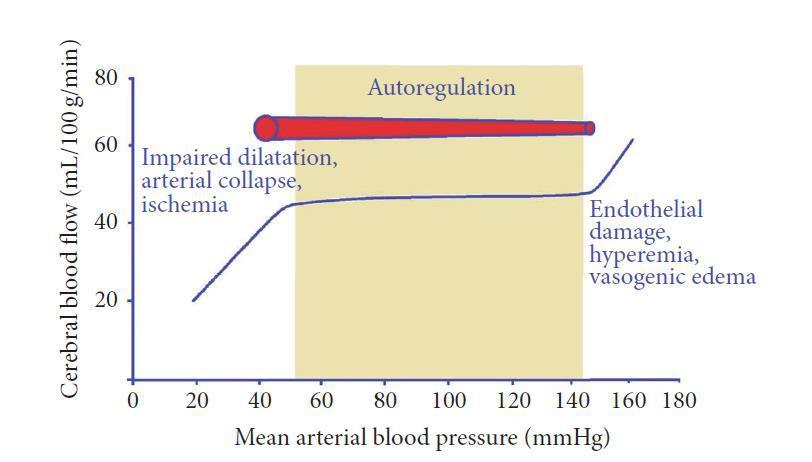
7 Cerebral Perfusion Pressure CBF determinations difficult to perform. CPP is a helpful guide to estimate adequacy of cerebral circulation. CPP is the blood pressure of the brain CPP= MAP - ICP Normal CPP CPP < typically leads to ischemia
8
9 Compliance: pressure-volume response CSF added to the craniospinal space Pressure-volume curve follows a hyperbolic function (rather than linear) Reflection of the elastic properties of the craniospinal system (elastance)
 Measure of the distensibility of the intracranial cavity Zone II: normal ICP, poor")
10 Compliance: zones I, II, III Ratio of the change in volume to the resulting change in pressure (ΔV/ΔP) Measure of the distensibility of the intracranial cavity Zone II: normal ICP, poor compliance
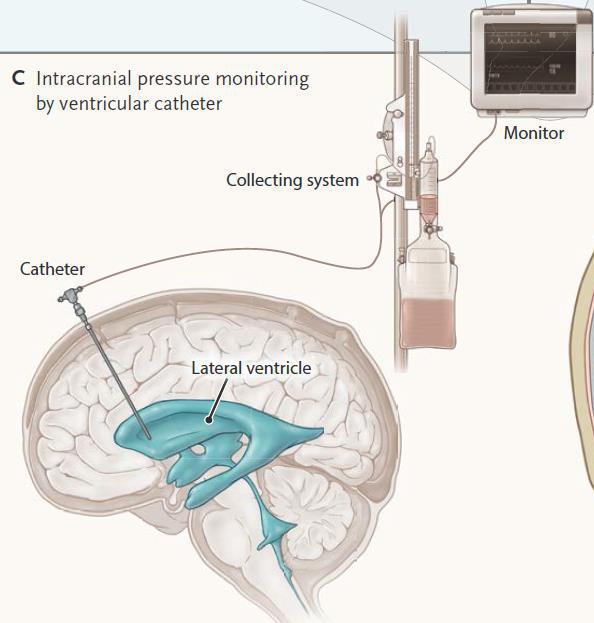
11 ICP Monitoring
12
13 The choroid plexus is credited as the site of transfer of the arterial pulse to the CSF Pressure gradient exists along the craniospinal axis in a rostro-causal fashion (about 60% lower in the lumbar space) Facilitates the movement of CSF from the ventricles into the subarachnoid space ICP waveforms
14 Intraventricular monitoring Percussive wave (P1): choroidal plexus pulse Tidal wave (P2): intracranial compliance Dicrotic wave (P3):closure of aortic valve Poor compliance: peaked P2
15
16
17
18 Pathophysiology
19
20
21 Treatment
22
23 Principles of Treatment General - Avoid shivering, agitation or fever - Euvolemia to slight hypervolemia - Pressors as needed to maintain CPP - Facilitate venous outflow (head elevation > 30 degrees, midline position)
24 Specific - Controlled hyperventilation (PaCO mmhg) - External CSF drainage - Osmotic therapy - Metabolic suppression (propofol, barbiturates) - Decompressive surgery - Hypothermia
25 ICP Treatment Algorithm Insert ICP monitor and maintain CPP >65 mm Hg (ventriculostomy preferred) Consider repeat CT scan Yes Yes Yes CSF drainage (if available) Sedation/Analgesia Consider mild hyperventilation (P a CO mm Hg); further sedation; neuromuscular blockade Yes ICP >20-25 mm Hg? Yes ICP >20-25 mm Hg? Yes No No Hypertonic saline (23.4% 30 cc bolus) Mannitol bolus ( g/kg) ICP >20-25 mm Hg? Yes ICP >20-25 mm Hg? Yes No No Stepwise withdrawal of ICP therapies Second-tier therapies such as hypothermia, decompressive craniectomy, barbiturate coma.
26
27
28 23.4% Hypertonic Saline Bullet Standard dose: 30 ml (120 meq mosm/l) given over minutes May repeat once at discretion of MD (i.e. another dose of 30 ml) MD or APRN/PA may administer 23.4% slow via central line if indicated at 2 cc/min Appropriate for initial or adjunct emergency treatment of acute intracranial hypertensive crisis or herniation
29
 in Patients with Elevated ICP Samer Abubakr 1, MD, Riane Ghamrawi 2, PharmD, Simon Lam 2, PharmD, Christine L.")
 is used for treatment of elevated intracranial pressure (ICP). Pharmacokinetic/pharmacodynamic studies are limited and dose-response curves in humans have not been reported.")
30 ICP mmhg ICP mmhg Efficacy and Dose-Response Relationship of 23.4% Hypertonic Saline Administration and Intracranial Pressure (ICP) in Patients with Elevated ICP Samer Abubakr 1, MD, Riane Ghamrawi 2, PharmD, Simon Lam 2, PharmD, Christine L. Ahrens 2, PharmD, Joao A. Gomes 1, MD 1 Cerebrovascular Center; 2 Department of Pharmacy. Cleveland Clinic, Cleveland, OH, United States #188 Background Results Conclusions 23.4% hypertonic saline (HTS) is used for treatment of elevated intracranial pressure (ICP). Pharmacokinetic/pharmacodynamic studies are limited and dose-response curves in humans have not been reported. HTS 23.4% is traditionally dosed in 30 cc increments rather than based on patient s weight regardless of disease severity. We hypothesize that there is a correlation between weight-based dosing (mosm/kg) and ICP reduction. Study Objectives Total number of patients N=19 Male gender, n (%) 9 (47) Age (years)* 52 ± 18 Weight (kg)* 98 ± 26 ICU LOS (days)* 20 ± 28 GCS Pre* 6.6 ± 3 GCS Post* 8.7 ± 4 GCS change* 2 ± 2 Concomitant hypothermia 13 (68) and pentobarbital coma, n (%) Sodium pre 136 ± 6 Sodium post 146 ± 6 Dose Response Curve n= 18 doses 23.4% HTS was associated with a 67% reduction in ICP values in critically ill neurology/neurosurgery patients Time to clinical endpoint of ICP <20 mmhg was 41 minutes and in 75% of patients the duration of action was 127 minutes An improvement of 2 points in GCS was also observed The first description of a dose-response curve for 23.4% HTS in humans is reported While most patients received 2-4 mosm/kg of HTS, additional benefit may be derived from doses as high as 7 mosm/kg Primary Objective: Describe the onset, duration of action and maximum ICP lowering effect following administration of 23.4% HTS in critically ill patients with ICP crisis. Secondary Objectives: Develop a dose-response curve for 23.4% HTS. Research Design and Methods Retrospective chart review of patients admitted to the Neurocritical care unit from August 2010 to August 2011 who developed ICP crisis (>20 mm Hg sustained for >5 minutes) and were treated with 23.4% HTS. Only data for the first ever treatment with HTS were collected. Patient demographics, onset and duration of action, lowest ICP achieved and use of adjunctive therapies were recorded. Descriptive statistics and correlation analysis were performed. IRB approval and granted per institution policy. Admission diagnosis, n (%) *Data represented as mean + SD SAH 10 (52) 29.5 ± 11.5 pre ICH 6 (32) Other 3 (16) Absolute ICP Reduction ICP 10±12.5 Post P= ICP Change Over Time Time in minutes Limitations Retrospective study Small number of patients. Confounding factors: hypothermia, hyperventilation, pentobarbital therapy Heterogeneous group of patients with different severities Some patients received concomitant hyperosmolar therapy (i.e. mannitol) within few hours prior to HTS Lack of continuous ICP documentation Bibliography Mayer SA, Chong J: Critical care management of increased intracranial pressure. J Intensive Care Med 2002;17:55-67 Qureshi AI, Wilson DA, Traystman RJ. Treatment of elevated intracranial pressure in experimental intracerebral hemorrhage: comparison between mannitol and hypertonic saline. Neurosurgery 1999;44: Suarez JI, Qureshi AI, Bhardwaj A, et al. Treatment of refractory intracranial hypertension with 23.4% saline. Critical Care Medicine Author Disclosures: None 1998;26:
31 23.4% HTS was associated with a 67% reduction in ICP values in critically ill neurology/neurosurgery patients Time to clinical endpoint of ICP <20 mmhg was 41 minutes and in 75% of patients the duration of action was 127 minutes An improvement of 2 points in GCS was also observed The first description of a dose-response curve for 23.4% HTS in humans is reported While most patients received 2-4 mosm/kg of HTS, additional benefit may be derived from doses as high as 7 mosm/kg
32 HTS: side effects CPM SDH CHF Acid-base abnormalities Coagulopathies Hypotension with rapid infusion (decreases SVR)
33 Multimodal Monitoring

34 Partial Pressure of O 2 Brain Tissue It is a closed polarographic p bt O 2 probe with reversible electrochemical reactions. This new type of chemistry virtually eliminates drifting of the probe s sensitivity and zero point

35 Partial Pressure Oxygen in Brain What are we measuring? Licox Microvascular delivery and local cellular consumption

36 ICP/CPP Management Unrelated to oxygenation

37

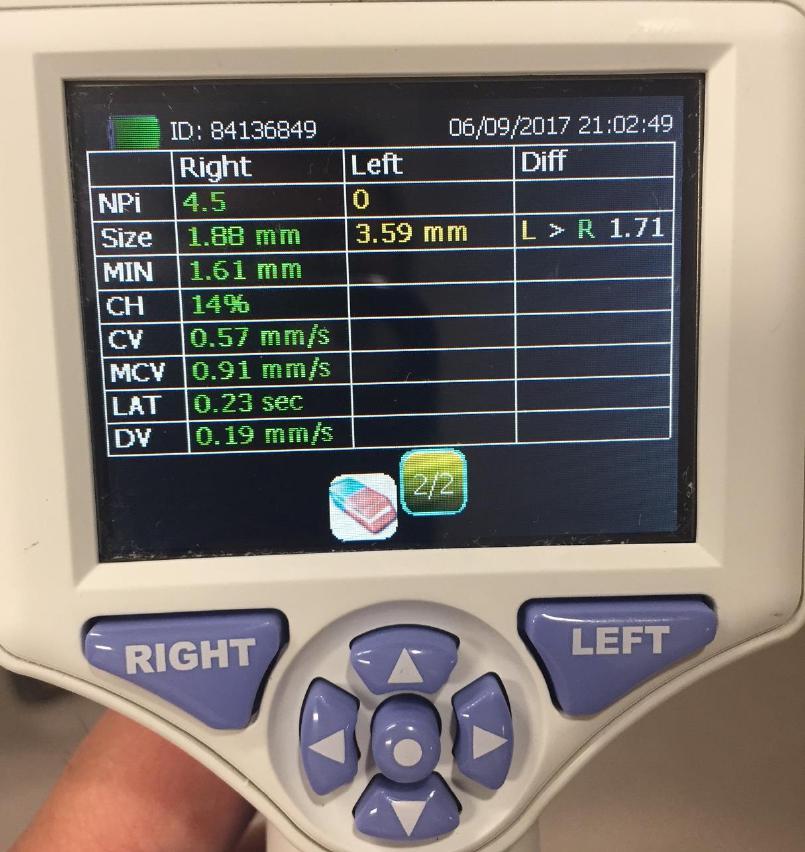
38 Pupillometer
39
40
41 Decompressive Hemicraniectomy

42

43
44 L_ Multimodal Monitoring: the key?

45
ICP. A Stepwise Approach. Stephan A. Mayer, MD Professor, Neurology & Neurosurgery Director, Neurocritical Care, Mount Sinai Health System
 ICP A Stepwise Approach Stephan A. Mayer, MD Professor, Neurology & Neurosurgery Director, Neurocritical Care, Mount Sinai Health System ICP: Basic Concepts Monroe-Kellie doctrine: skull = fixed volume
ICP A Stepwise Approach Stephan A. Mayer, MD Professor, Neurology & Neurosurgery Director, Neurocritical Care, Mount Sinai Health System ICP: Basic Concepts Monroe-Kellie doctrine: skull = fixed volume
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
Management of Traumatic Brain Injury (and other neurosurgical emergencies)
") Management of Traumatic Brain Injury (and other neurosurgical emergencies) Laurel Moore, M.D. University of Michigan 22 nd Annual Review February 7, 2019 Greetings from Michigan! Objectives for Today s
Management of Traumatic Brain Injury (and other neurosurgical emergencies) Laurel Moore, M.D. University of Michigan 22 nd Annual Review February 7, 2019 Greetings from Michigan! Objectives for Today s
Standardize comprehensive care of the patient with severe traumatic brain injury
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Linee guida sul trauma cranico: sempre attuali? Leonardo Bussolin AOU Meyer
 Linee guida sul trauma cranico: sempre attuali? Leonardo Bussolin AOU Meyer Vavilala MS, et al Retrospective multicenter cohort study Prehospital Arena ED OR - ICU Each 1% increase in adherence was associated
Linee guida sul trauma cranico: sempre attuali? Leonardo Bussolin AOU Meyer Vavilala MS, et al Retrospective multicenter cohort study Prehospital Arena ED OR - ICU Each 1% increase in adherence was associated
Case 1. Case 5/30/2013. Traumatic Brain Injury : Review, Update, and Controversies
 Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
Traumatic Brain Injury:
 Traumatic Brain Injury: Changes in Management Across the Spectrum of Age and Time Omaha 2018 Trauma Symposium June 15, 2018 Gail T. Tominaga, M.D., F.A.C.S. Scripps Memorial Hospital La Jolla Outline Background
Traumatic Brain Injury: Changes in Management Across the Spectrum of Age and Time Omaha 2018 Trauma Symposium June 15, 2018 Gail T. Tominaga, M.D., F.A.C.S. Scripps Memorial Hospital La Jolla Outline Background
Moron General Hospital Ciego de Avila Cuba. Department of Neurological Surgery
 Moron General Hospital Ciego de Avila Cuba Department of Neurological Surgery Early decompressive craniectomy in severe head injury with intracranial hypertension Angel J. Lacerda MD PhD, Daisy Abreu MD,
Moron General Hospital Ciego de Avila Cuba Department of Neurological Surgery Early decompressive craniectomy in severe head injury with intracranial hypertension Angel J. Lacerda MD PhD, Daisy Abreu MD,
Neuroprotective Effects for TBI. Craig Williamson, MD
 Neuroprotective Effects for TBI Craig Williamson, MD Neuroprotection in Traumatic Brain Injury Craig Williamson Clinical Assistant Professor Neurocritical Care Fellowship Director Disclosures I will discuss
Neuroprotective Effects for TBI Craig Williamson, MD Neuroprotection in Traumatic Brain Injury Craig Williamson Clinical Assistant Professor Neurocritical Care Fellowship Director Disclosures I will discuss
Traumatic Brain Injuries
 Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Evaluation & Management of Elevated Intracranial Pressure in Adults. Dr. Tawfiq Almezeiny
 Evaluation & Management of Elevated Intracranial Pressure in Adults Dr. Tawfiq Almezeiny Objectives Pathophsiology of elevated intracranial pressure. Clinical features and sequences. Management : Investigations
Evaluation & Management of Elevated Intracranial Pressure in Adults Dr. Tawfiq Almezeiny Objectives Pathophsiology of elevated intracranial pressure. Clinical features and sequences. Management : Investigations
ICP. A Stepwise Protocol
 ICP A Stepwise Protocol Stephan A. Mayer, MD Neurological Intensive Care Unit Neurological Institute of New York Columbia-Presbyterian Medical Center New York, NY ICP: Basic Concepts Monroe-Kellie doctrine:
ICP A Stepwise Protocol Stephan A. Mayer, MD Neurological Intensive Care Unit Neurological Institute of New York Columbia-Presbyterian Medical Center New York, NY ICP: Basic Concepts Monroe-Kellie doctrine:
Any closer to evidence based practice? Asma Salloo Chris Hani Baragwantah Academic Hospital University of Witwatersrand
 Any closer to evidence based practice? Asma Salloo Chris Hani Baragwantah Academic Hospital University of Witwatersrand Evidence Pathophysiology Why? Management Non-degenerative, Non-congenital insult
Any closer to evidence based practice? Asma Salloo Chris Hani Baragwantah Academic Hospital University of Witwatersrand Evidence Pathophysiology Why? Management Non-degenerative, Non-congenital insult
Update on Guidelines for Traumatic Brain Injury
 Update on Guidelines for Traumatic Brain Injury Current TBI Guidelines Shirley I. Stiver MD, PhD Department of Neurosurgery Guidelines for the management of traumatic brain injury Journal of Neurotrauma
Update on Guidelines for Traumatic Brain Injury Current TBI Guidelines Shirley I. Stiver MD, PhD Department of Neurosurgery Guidelines for the management of traumatic brain injury Journal of Neurotrauma
INCREASED INTRACRANIAL PRESSURE
 INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
Neurocritical Care Monitoring. Academic Half Day Critical Care Fellows
 Neurocritical Care Monitoring Academic Half Day Critical Care Fellows Clinical Scenarios for CNS monitoring No Universally accepted Guidelines Traumatic Brain Injury Intracerebral Hemorrhage Subarachnoid
Neurocritical Care Monitoring Academic Half Day Critical Care Fellows Clinical Scenarios for CNS monitoring No Universally accepted Guidelines Traumatic Brain Injury Intracerebral Hemorrhage Subarachnoid
Stroke & Neurovascular Center of New Jersey. Jawad F. Kirmani, MD Director, Stroke and Neurovascular Center
 Stroke & Neurovascular Center of New Jersey Jawad F. Kirmani, MD Director, Stroke and Neurovascular Center Past, present and future Past, present and future Cerebral Blood Flow Past, present and future
Stroke & Neurovascular Center of New Jersey Jawad F. Kirmani, MD Director, Stroke and Neurovascular Center Past, present and future Past, present and future Cerebral Blood Flow Past, present and future
Perioperative Management of Traumatic Brain Injury. C. Werner
 Perioperative Management of Traumatic Brain Injury C. Werner Perioperative Management of TBI Pathophysiology Monitoring Oxygenation CPP Fluid Management Glycemic Control Temperature Management Surgical
Perioperative Management of Traumatic Brain Injury C. Werner Perioperative Management of TBI Pathophysiology Monitoring Oxygenation CPP Fluid Management Glycemic Control Temperature Management Surgical
HEAD INJURY. Dept Neurosurgery
 HEAD INJURY Dept Neurosurgery INTRODUCTION PATHOPHYSIOLOGY CLINICAL CLASSIFICATION MANAGEMENT - INVESTIGATIONS - TREATMENT INTRODUCTION Most head injuries are due to an impact between the head and another
HEAD INJURY Dept Neurosurgery INTRODUCTION PATHOPHYSIOLOGY CLINICAL CLASSIFICATION MANAGEMENT - INVESTIGATIONS - TREATMENT INTRODUCTION Most head injuries are due to an impact between the head and another
8/29/2011. Brain Injury Incidence: 200/100,000. Prehospital Brain Injury Mortality Incidence: 20/100,000
 Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
INTRACRANIAL PRESSURE -!!
 INTRACRANIAL PRESSURE - Significance raised ICP main cause of death in severe head injury main cause of morbidity in moderate and mild head injury main target and prognostic indicator in the ITU setting
INTRACRANIAL PRESSURE - Significance raised ICP main cause of death in severe head injury main cause of morbidity in moderate and mild head injury main target and prognostic indicator in the ITU setting
11/27/2017. Stroke Management in the Neurocritical Care Unit. Conflict of interest. Karel Fuentes MD Medical Director of Neurocritical Care
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
12/4/2017. Disclosure. Educational Objectives. Has been consultant for Bard, Chiesi
 Temperature Management in Neuro ICU Kiwon Lee, MD, FACP, FAHA, FCCM Professor of Neurology, RWJ Medical School Chief of Neurology, RWJ University Hospital Director, RWJ Comprehensive Stroke Center Director,
Temperature Management in Neuro ICU Kiwon Lee, MD, FACP, FAHA, FCCM Professor of Neurology, RWJ Medical School Chief of Neurology, RWJ University Hospital Director, RWJ Comprehensive Stroke Center Director,
11/23/2015. Disclosures. Stroke Management in the Neurocritical Care Unit. Karel Fuentes MD Medical Director of Neurocritical Care.
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
CEREBRAL DECONGESTANTS. Dr. Dwarakanath Srinivas Additional Professor Neurosurgery, NIMHANS
 CEREBRAL DECONGESTANTS Dr. Dwarakanath Srinivas Additional Professor Neurosurgery, NIMHANS Cerebral Oedema Increase in brain water content above normal (80%) in response to primary brain insult. Intracranial
CEREBRAL DECONGESTANTS Dr. Dwarakanath Srinivas Additional Professor Neurosurgery, NIMHANS Cerebral Oedema Increase in brain water content above normal (80%) in response to primary brain insult. Intracranial
H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute
 H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute Memorial Hermann- Texas Medical Center Learning Objectives
H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute Memorial Hermann- Texas Medical Center Learning Objectives
UAMS MEDICAL CENTER TRAUMA and CRITICAL CARE SERVICES MANUAL. SUPERSEDES: New PAGE: 1 of 5. RECOMMENDATION(S): Drs. Bill Beck/J.R.
: Drs. Bill Beck/J.R.") SUPERSEDES: New PAGE: 1 of 5 Purpose: To provide recommendations for the treatment and management of patients with traumatic brain injury. Definitions: Severe TBI - Glasgow Coma Scale (GCS) of 3 to 8 without
SUPERSEDES: New PAGE: 1 of 5 Purpose: To provide recommendations for the treatment and management of patients with traumatic brain injury. Definitions: Severe TBI - Glasgow Coma Scale (GCS) of 3 to 8 without
10. Severe traumatic brain injury also see flow chart Appendix 5
 10. Severe traumatic brain injury also see flow chart Appendix 5 Introduction Severe traumatic brain injury (TBI) is the leading cause of death in children in the UK, accounting for 15% of deaths in 1-15
10. Severe traumatic brain injury also see flow chart Appendix 5 Introduction Severe traumatic brain injury (TBI) is the leading cause of death in children in the UK, accounting for 15% of deaths in 1-15
Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage. Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA
 Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA The traditional view: asah is a bad disease Pre-hospital mortality
Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA The traditional view: asah is a bad disease Pre-hospital mortality
Raised Intracranial Pressure (ICP): Management in Emergency Department
: Management in Emergency Department") Raised Intracranial Pressure (ICP): Management in Emergency Department Author: Dr. Shruti Sangani*, Dr. Samira Parikh** INTRODUCTION: Elevated intracranial pressure (ICP) is a potentially devastating complication
Raised Intracranial Pressure (ICP): Management in Emergency Department Author: Dr. Shruti Sangani*, Dr. Samira Parikh** INTRODUCTION: Elevated intracranial pressure (ICP) is a potentially devastating complication
Mannitol versus Hypertonic Saline for Management of Elevated Intracranial Pressure Jerry Altshuler, PharmD; Diana Esaian, PharmD, BCPS
 Mannitol versus Hypertonic Saline for Management of Elevated Intracranial Pressure Jerry Altshuler, PharmD; Diana Esaian, PharmD, BCPS The intracranial compartment consists of predominantly brain parenchyma
Mannitol versus Hypertonic Saline for Management of Elevated Intracranial Pressure Jerry Altshuler, PharmD; Diana Esaian, PharmD, BCPS The intracranial compartment consists of predominantly brain parenchyma
State of the Art Multimodal Monitoring
 State of the Art Multimodal Monitoring Baptist Neurological Institute Mohamad Chmayssani, MD Disclosures I have no financial relationships to disclose with makers of the products here discussed. Outline
State of the Art Multimodal Monitoring Baptist Neurological Institute Mohamad Chmayssani, MD Disclosures I have no financial relationships to disclose with makers of the products here discussed. Outline
Management of Traumatic Brain Injury. Olaide O. Ajayi, MD
 Management of Traumatic Brain Injury Olaide O. Ajayi, MD Traumatic Brain Injury (TBI) A bump, blow or jolt to the head that disrupts the normal function of the brain 1 Mild: Brief change in mental status
Management of Traumatic Brain Injury Olaide O. Ajayi, MD Traumatic Brain Injury (TBI) A bump, blow or jolt to the head that disrupts the normal function of the brain 1 Mild: Brief change in mental status
SUBJECT: Clinical Practice Guideline for the Management of Severe Traumatic Brain Injury
 ASPIRUS WAUSAU HOSPITAL, INC. Passion for excellence. Compassion for people. Effective Date: December 1, 2005 Proposed By: Samuel Picone III, MD, Trauma Medical Director Approval and Dates: Dr. Bunch,
ASPIRUS WAUSAU HOSPITAL, INC. Passion for excellence. Compassion for people. Effective Date: December 1, 2005 Proposed By: Samuel Picone III, MD, Trauma Medical Director Approval and Dates: Dr. Bunch,
Traumatic brain Injury- An open eye approach
 Traumatic brain Injury- An open eye approach Dr. Sunit Dr Sunit, Apollo children's hospital Blah blah Lots of head injury Lot of ill children Various methods of injury Various mechanisms of brain damage
Traumatic brain Injury- An open eye approach Dr. Sunit Dr Sunit, Apollo children's hospital Blah blah Lots of head injury Lot of ill children Various methods of injury Various mechanisms of brain damage
Traumatic Brain Injury Pathway, GCS 15 Closed head injury
 Traumatic Brain Injury Pathway, GCS 15 Closed head injury Plus Any One of the Following Mild TBI 2010 Consensus Definition of TBI from CDC, NINDS, NIDDR, VA, DVBIC, DCoE Plus Any One of the Following New
Traumatic Brain Injury Pathway, GCS 15 Closed head injury Plus Any One of the Following Mild TBI 2010 Consensus Definition of TBI from CDC, NINDS, NIDDR, VA, DVBIC, DCoE Plus Any One of the Following New
Michael Avant, M.D. The Children s Hospital of GHS
 Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
Michael Avant, M.D. The Children s Hospital of GHS OVERVIEW ER to ICU Transition Early Management Priorities the First 48 hours Organ System Support Complications THE FIRST 48 HOURS Communication Damage
Blood Brain Barrier (BBB)
") Cerebral Blood Flow, Cerebral Spinal Fluid, and Brain Metabolism Part Two Guyton Chapter 61 Morgan & Mikhail, 4 th ed, Chapter 25 (or Morgan & Mikhail 5 th ed, Chapter 26) Blood Brain Barrier (BBB) Cerebral
Cerebral Blood Flow, Cerebral Spinal Fluid, and Brain Metabolism Part Two Guyton Chapter 61 Morgan & Mikhail, 4 th ed, Chapter 25 (or Morgan & Mikhail 5 th ed, Chapter 26) Blood Brain Barrier (BBB) Cerebral
Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth. Objectives 11/7/2017
 Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth Objectives 1. Be able to discuss brain anatomy and physiology as it applies to
Pediatric Subdural Hematoma and Traumatic Brain Injury J. Charles Mace MD FACS Springfield Neurological Institute CoxHealth Objectives 1. Be able to discuss brain anatomy and physiology as it applies to
11 th Annual Cerebrovascular Symposium 5/11-12/2017. Hypertonic Use D E R E K C L A R K
 Hypertonic Use D E R E K C L A R K 1 Outline Types of hyperosmolar therapy Review Cerebral Na Physiology Differences between periphery and BBB Acute phase Subacute phase Chronic changes Hypertonic Saline
Hypertonic Use D E R E K C L A R K 1 Outline Types of hyperosmolar therapy Review Cerebral Na Physiology Differences between periphery and BBB Acute phase Subacute phase Chronic changes Hypertonic Saline
Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery
 Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery 2 Stroke Stroke kills almost 130,000 Americans each year. - Third cause of all deaths in Arkansas. - Death Rate is highest in
Surgical Management of Stroke Brandon Evans, MD Department of Neurosurgery 2 Stroke Stroke kills almost 130,000 Americans each year. - Third cause of all deaths in Arkansas. - Death Rate is highest in
Controversy in the Care of Those with Severe TBI: Can t We All Just Get Along?
 Controversy in the Care of Those with Severe TBI: Can t We All Just Get Along? Disclosure Statement Faculty/Presenters/Authors/Content Reviewers/Planners disclose no conflict of interest relative to this
Controversy in the Care of Those with Severe TBI: Can t We All Just Get Along? Disclosure Statement Faculty/Presenters/Authors/Content Reviewers/Planners disclose no conflict of interest relative to this
Introduction to Neurosurgical Subspecialties:
 Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
Recent trends in the management of head injury
 Recent trends in the management of head injury Contents: Current concepts of management in TBI Blood pressure and oxygenation Intracranial pressure monitoring Cerebral perfusion pressure Body temperature
Recent trends in the management of head injury Contents: Current concepts of management in TBI Blood pressure and oxygenation Intracranial pressure monitoring Cerebral perfusion pressure Body temperature
Severe traumatic brain injury. Fellowship Training Intensive Care Radboud University Nijmegen Medical Centre
 Severe traumatic brain injury Fellowship Training Intensive Care Radboud University Nijmegen Medical Centre Primary focus of care Prevent ischemia, hypoxia and hypoglycemia Nutrient & oxygen supply Limited
Severe traumatic brain injury Fellowship Training Intensive Care Radboud University Nijmegen Medical Centre Primary focus of care Prevent ischemia, hypoxia and hypoglycemia Nutrient & oxygen supply Limited
 www.yassermetwally.com MANAGEMENT OF CEREBRAL HAEMORRHAGE (ICH): A QUICK GUIDE Overview 10% of strokes is caused by ICH. Main Causes: Less than 40 years old: vascular malformations and illicit drug use.
www.yassermetwally.com MANAGEMENT OF CEREBRAL HAEMORRHAGE (ICH): A QUICK GUIDE Overview 10% of strokes is caused by ICH. Main Causes: Less than 40 years old: vascular malformations and illicit drug use.
PATHOPHYSIOLOGY OF ACUTE TRAUMATIC BRAIN INJURY. Dr Nick Taylor MBBS FACEM
 PATHOPHYSIOLOGY OF ACUTE TRAUMATIC BRAIN INJURY Dr Nick Taylor MBBS FACEM The Monro Kellie Doctrine CPP= MAP-ICP PRIMARY DAMAGE TBI is a heterogeneous disorder Brain damage results from external forces,
PATHOPHYSIOLOGY OF ACUTE TRAUMATIC BRAIN INJURY Dr Nick Taylor MBBS FACEM The Monro Kellie Doctrine CPP= MAP-ICP PRIMARY DAMAGE TBI is a heterogeneous disorder Brain damage results from external forces,
SAH READMISSIONS TO NCCU
 SAH READMISSIONS TO NCCU Are they preventable? João Amaral Rebecca Gorf Critical Care Outreach Team - NHNN 2015 Total admissions to NCCU =862 Total SAH admitted to NCCU= 104 (93e) (12.0%) Total SAH readmissions=
SAH READMISSIONS TO NCCU Are they preventable? João Amaral Rebecca Gorf Critical Care Outreach Team - NHNN 2015 Total admissions to NCCU =862 Total SAH admitted to NCCU= 104 (93e) (12.0%) Total SAH readmissions=
Angel J. Lacerda MD PhD, Daisy Abreu MD, Julio A. Díaz MD, Sandro Perez MD, Julio C Martin MD, Daiyan Martin MD.
 Angel J. Lacerda MD PhD, Daisy Abreu MD, Julio A. Díaz MD, Sandro Perez MD, Julio C Martin MD, Daiyan Martin MD. Introduction: Spontaneous intracerebral haemorrhage (SICH) represents one of the most severe
Angel J. Lacerda MD PhD, Daisy Abreu MD, Julio A. Díaz MD, Sandro Perez MD, Julio C Martin MD, Daiyan Martin MD. Introduction: Spontaneous intracerebral haemorrhage (SICH) represents one of the most severe
Brain under pressure Managing ICP. Giuseppe
 Brain under pressure Managing ICP Giuseppe Citerio giuseppe.citerio@unimib.it @Dr_Cit Intro Thresholds Treating HICP Conclusions NO COI for this presentation Produces pressure gradients: herniation HIGH
Brain under pressure Managing ICP Giuseppe Citerio giuseppe.citerio@unimib.it @Dr_Cit Intro Thresholds Treating HICP Conclusions NO COI for this presentation Produces pressure gradients: herniation HIGH
Traumatic Brain Injury Pathways for Adult ED Patients Being Admitted to Trauma Service
 tic Brain Injury Pathways for Adult ED Patients Being Admitted to Service Revision Team Tyler W. Barrett, MD, MSCI Elizabeth S. Compton, NP Bradley M. Dennis, MD Oscar D. Guillamondegui, MD, MPH Michael
tic Brain Injury Pathways for Adult ED Patients Being Admitted to Service Revision Team Tyler W. Barrett, MD, MSCI Elizabeth S. Compton, NP Bradley M. Dennis, MD Oscar D. Guillamondegui, MD, MPH Michael
7/22/2016. Navaz Karanjia, MD. FINANCIAL DISCLOSURE: none. UNLABELED/UNAPPROVED USE DISCLOSURE: none
 Navaz Karanjia, MD Director of Neurocritical Care Assistant Professor of Neurosciences, Neurosurgery, and Anesthesiology University of California-San Diego Health System Navaz Karanjia, MD FINANCIAL DISCLOSURE:
Navaz Karanjia, MD Director of Neurocritical Care Assistant Professor of Neurosciences, Neurosurgery, and Anesthesiology University of California-San Diego Health System Navaz Karanjia, MD FINANCIAL DISCLOSURE:
Chapter 8: Cerebral protection Stephen Lo
 Chapter 8: Cerebral protection Stephen Lo Introduction There will be a variety of neurological pathologies that you will see within the intensive care. The purpose of this chapter is not to cover all neurological
Chapter 8: Cerebral protection Stephen Lo Introduction There will be a variety of neurological pathologies that you will see within the intensive care. The purpose of this chapter is not to cover all neurological
Postanesthesia Care of the Patient Suffering From Traumatic Brain Injury
 Postanesthesia Care of the Patient Suffering From Traumatic Brain Injury By: Susan Letvak, PhD, RN Rick Hand, CRNA, DNSc Letvak, S. & Hand, R. (2003). Postanesthesia care of the traumatic brain injured
Postanesthesia Care of the Patient Suffering From Traumatic Brain Injury By: Susan Letvak, PhD, RN Rick Hand, CRNA, DNSc Letvak, S. & Hand, R. (2003). Postanesthesia care of the traumatic brain injured
Hypertensive Haemorrhagic Stroke. Dr Philip Lam Thuon Mine
 Hypertensive Haemorrhagic Stroke Dr Philip Lam Thuon Mine Intracerebral Haemorrhage Primary ICH Spontaneous rupture of small vessels damaged by HBP Basal ganglia, thalamus, pons and cerebellum Amyloid
Hypertensive Haemorrhagic Stroke Dr Philip Lam Thuon Mine Intracerebral Haemorrhage Primary ICH Spontaneous rupture of small vessels damaged by HBP Basal ganglia, thalamus, pons and cerebellum Amyloid
Reducing intracranial pressure in patients with traumatic brain injury
 Reducing intracranial pressure in patients with traumatic brain injury Learn how to identify rising intracranial pressure early to promote appropriate interventions. By Cindy L. Zerfoss, MSN, RN, ACNP-CS
Reducing intracranial pressure in patients with traumatic brain injury Learn how to identify rising intracranial pressure early to promote appropriate interventions. By Cindy L. Zerfoss, MSN, RN, ACNP-CS
Process Measures Toolkit for 2016 Admissions
 Process Measures Toolkit for 2016 Admissions Collection Criterion #1 Collect on all patients The following data fields should be reported using the listed field value option(s), or relevant value, as indicated
Process Measures Toolkit for 2016 Admissions Collection Criterion #1 Collect on all patients The following data fields should be reported using the listed field value option(s), or relevant value, as indicated
12/1/2017. Disclosure. When I was invited to give a talk in Tokyo 2011 at the 4 th International. Hypothermia Symposium
 Disclosure Different Levels of Hypothermia: Is Cooler Better? Nothing to disclose (wish I did) Absolutely no conflict of interest for this lecture Kiwon Lee, MD, FACP, FAHA, FCCM Vice Chairman of Neurology
Disclosure Different Levels of Hypothermia: Is Cooler Better? Nothing to disclose (wish I did) Absolutely no conflict of interest for this lecture Kiwon Lee, MD, FACP, FAHA, FCCM Vice Chairman of Neurology
Intracranial volume-pressure relationships during
 Journial of Neurology, Neurosurgery, and Psychiatry, 1974, 37, 115-1111 Intracranial volume-pressure relationships during experimental brain compression in primates 3. Effect of mannitol and hyperventilation
Journial of Neurology, Neurosurgery, and Psychiatry, 1974, 37, 115-1111 Intracranial volume-pressure relationships during experimental brain compression in primates 3. Effect of mannitol and hyperventilation
Shobana Rajan, M.D. Associate staff Anesthesiologist, Cleveland Clinic, Cleveland, Ohio
 Shobana Rajan, M.D. Associate staff Anesthesiologist, Cleveland Clinic, Cleveland, Ohio Shaheen Shaikh, M.D. Assistant Professor of Anesthesiology, University of Massachusetts Medical center, Worcester,
Shobana Rajan, M.D. Associate staff Anesthesiologist, Cleveland Clinic, Cleveland, Ohio Shaheen Shaikh, M.D. Assistant Professor of Anesthesiology, University of Massachusetts Medical center, Worcester,
R Adams Cowley Founder of the R Adams Cowley Shock Trauma Center and Maryland EMS System in Baltimore, Maryland.
 R Adams Cowley 1917 -- 1991 Founder of the R Adams Cowley Shock Trauma Center and Maryland EMS System in Baltimore, Maryland. ...That the primary purpose of medicine was to save lives, that every critically
R Adams Cowley 1917 -- 1991 Founder of the R Adams Cowley Shock Trauma Center and Maryland EMS System in Baltimore, Maryland. ...That the primary purpose of medicine was to save lives, that every critically
UPSTATE Comprehensive Stroke Center. Neurosurgical Interventions Satish Krishnamurthy MD, MCh
 UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic
UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic
Improving TBI outcome
 Improving TBI outcome Dr Peter Smielewski ps10011@cam.ac.uk 20/10/2017 Division of Neurosurgery, Department of Clinical Neurosciences Background Stein, S. C., Georgoff, P., et al. (2010). Journal of Neurotrauma
Improving TBI outcome Dr Peter Smielewski ps10011@cam.ac.uk 20/10/2017 Division of Neurosurgery, Department of Clinical Neurosciences Background Stein, S. C., Georgoff, P., et al. (2010). Journal of Neurotrauma
9/18/16. Management of Ischemic Stroke in the Intensive Care Unit. Outline. Introduction. Kyle B Walsh MD. Phases of Stroke Diagnosis and Treatment
 Management of Ischemic Stroke in the Intensive Care Unit Kyle B Walsh MD Assistant Professor - UC Dept of Emergency Medicine Fellow Physician - Neurocritical Care, Stroke, Research Outline Why ICU care
Management of Ischemic Stroke in the Intensive Care Unit Kyle B Walsh MD Assistant Professor - UC Dept of Emergency Medicine Fellow Physician - Neurocritical Care, Stroke, Research Outline Why ICU care
8th Annual NKY TBI Conference 3/28/2014
 Closed Head Injury: Headache to Herniation A N T H O N Y T. K R A M E R U N I V E R S I T Y O F C I N C I N N A T I B L U E A S H E M S T E C H N O L O G Y P R O G R A M Objectives Describe the pathological
Closed Head Injury: Headache to Herniation A N T H O N Y T. K R A M E R U N I V E R S I T Y O F C I N C I N N A T I B L U E A S H E M S T E C H N O L O G Y P R O G R A M Objectives Describe the pathological
Conflict of Interest Disclosure J. Claude Hemphill III, MD,MAS. Difficult Diagnosis and Treatment: New Onset Obtundation
 Difficult Diagnosis and Treatment: New Onset Obtundation J. Claude Hemphill III, MD, MAS Kenneth Rainin Chair in Neurocritical Care Professor of Neurology and Neurological Surgery University of California,
Difficult Diagnosis and Treatment: New Onset Obtundation J. Claude Hemphill III, MD, MAS Kenneth Rainin Chair in Neurocritical Care Professor of Neurology and Neurological Surgery University of California,
How Low Should You Go? Management of Blood Pressure in Intracranial Hemorrhage
 How Low Should You Go? Management of Blood Pressure in Intracranial Hemorrhage Rachael Scott, Pharm.D. PGY2 Critical Care Pharmacy Resident Pharmacy Grand Rounds August 21, 2018 2018 MFMER slide-1 Patient
How Low Should You Go? Management of Blood Pressure in Intracranial Hemorrhage Rachael Scott, Pharm.D. PGY2 Critical Care Pharmacy Resident Pharmacy Grand Rounds August 21, 2018 2018 MFMER slide-1 Patient
Intracranial hypertension and cerebral edema are cardinal
 High-Osmolarity Saline in Neurocritical Care: Systematic Review and Meta-Analysis* Christos Lazaridis, MD 1,,3 ; Ron Neyens, PharmD 1,4 ; Jeffrey Bodle, MD ; Stacia M. DeSantis, PhD 5 Background and Purpose:
High-Osmolarity Saline in Neurocritical Care: Systematic Review and Meta-Analysis* Christos Lazaridis, MD 1,,3 ; Ron Neyens, PharmD 1,4 ; Jeffrey Bodle, MD ; Stacia M. DeSantis, PhD 5 Background and Purpose:
Malignant Edema and Hemicraniectomy After Stroke
 Malignant Edema and Hemicraniectomy After Stroke Sherri A. Braksick, MD March 29, 2017 No Financial Disclosures No Discussion of Off-Label Usage Objectives 1. Review the pathophysiology of edema after
Malignant Edema and Hemicraniectomy After Stroke Sherri A. Braksick, MD March 29, 2017 No Financial Disclosures No Discussion of Off-Label Usage Objectives 1. Review the pathophysiology of edema after
Neurocritical Care Basics. Tapan Kavi, MD Christina Fox, RN
 Neurocritical Care Basics Tapan Kavi, MD Christina Fox, RN GOAL 1: DON T LET THE PATIENT DIE Not unique ACLS, ATLS, ENLS, other strategies common to all emergency medical care ABCs MORE not less important
Neurocritical Care Basics Tapan Kavi, MD Christina Fox, RN GOAL 1: DON T LET THE PATIENT DIE Not unique ACLS, ATLS, ENLS, other strategies common to all emergency medical care ABCs MORE not less important
9/19/2011. Damien Beilman, RRT Adult Clinical Specialist Wesley Medical Center. Epidural Hematoma: Lens Shaped.
 Damien Beilman, RRT Adult Clinical Specialist Wesley Medical Center Epidural Hematoma: Lens Shaped. 1 Epidural Hematoma Subdural Hematoma: Crescent-shaped Subdural Hematoma 2 Cerebral Contusion Cause of
Damien Beilman, RRT Adult Clinical Specialist Wesley Medical Center Epidural Hematoma: Lens Shaped. 1 Epidural Hematoma Subdural Hematoma: Crescent-shaped Subdural Hematoma 2 Cerebral Contusion Cause of
Mechanisms of Headache in Intracranial Hypotension
 Mechanisms of Headache in Intracranial Hypotension Stephen D Silberstein, MD Jefferson Headache Center Thomas Jefferson University Hospital Philadelphia, PA Stephen D. Silberstein, MD, FACP Director, Jefferson
Mechanisms of Headache in Intracranial Hypotension Stephen D Silberstein, MD Jefferson Headache Center Thomas Jefferson University Hospital Philadelphia, PA Stephen D. Silberstein, MD, FACP Director, Jefferson
Perioperative Management Of Extra-Ventricular Drains (EVD)
") Perioperative Management Of Extra-Ventricular Drains (EVD) Dr. Vijay Tarnal MBBS, FRCA Clinical Assistant Professor Division of Neuroanesthesiology Division of Head & Neck Anesthesiology Michigan Medicine
Perioperative Management Of Extra-Ventricular Drains (EVD) Dr. Vijay Tarnal MBBS, FRCA Clinical Assistant Professor Division of Neuroanesthesiology Division of Head & Neck Anesthesiology Michigan Medicine
Raised intracranial pressure (ICP) is a common problem in neurosurgical and neurological
 is a common problem in neurosurgical and neurological") Correspondence to: Mr Laurence T Dunn, Department of Neurosurgery, Institute of Neurological Sciences, Southern General Hospital, Glasgow G51 4TF, UK; ltd1x@udcf.gla.ac.uk RAISED INTRACRANIAL PRESSURE
Correspondence to: Mr Laurence T Dunn, Department of Neurosurgery, Institute of Neurological Sciences, Southern General Hospital, Glasgow G51 4TF, UK; ltd1x@udcf.gla.ac.uk RAISED INTRACRANIAL PRESSURE
NEUROMONITORING AND ANESTHESIA CONSIDERATIONS. Martha Richter, MSN, CRNA
 NEUROMONITORING AND ANESTHESIA CONSIDERATIONS Martha Richter, MSN, CRNA OBJECTIVES The student will 1. Review the types of neuromonitoring currently in use 2. Identify possible procedural applications
NEUROMONITORING AND ANESTHESIA CONSIDERATIONS Martha Richter, MSN, CRNA OBJECTIVES The student will 1. Review the types of neuromonitoring currently in use 2. Identify possible procedural applications
Optimum sodium levels in children with brain injury. Professor Sunit Singhi, Head, Department of Pediatrics, Head, Pediatric
 India Optimum sodium levels in children with brain injury Professor Sunit Singhi, Head, Department of Pediatrics, Head, Pediatric Sodium and brain Sodium - the major extracellular cation and most important
India Optimum sodium levels in children with brain injury Professor Sunit Singhi, Head, Department of Pediatrics, Head, Pediatric Sodium and brain Sodium - the major extracellular cation and most important
INTRACRANIAL PRESSURE MONITORING
 INTRACRANIAL PRESSURE MONITORING A Handbook for the Nursing Professional 2 Why do we care about measuring intracranial pressure (ICP)? The intracranial compartment is very different from other regions
INTRACRANIAL PRESSURE MONITORING A Handbook for the Nursing Professional 2 Why do we care about measuring intracranial pressure (ICP)? The intracranial compartment is very different from other regions
PACT module. Traumatic Brain Injury. Intensive Care Training Program Radboud University Medical Centre Nijmegen
 PACT module Traumatic Brain Injury Intensive Care Training Program Radboud University Medical Centre Nijmegen Severe traumatic brain injury Leading cause of morbidity/mortality among young individuals
PACT module Traumatic Brain Injury Intensive Care Training Program Radboud University Medical Centre Nijmegen Severe traumatic brain injury Leading cause of morbidity/mortality among young individuals
FOCUS Annual Fall Classic Respiratory Care of the Patient with Traumatic Brain Injury
 FOCUS Annual Fall Classic 2018 Respiratory Care of the Patient with Traumatic Brain Injury Daniel W. Chipman, BS, RRT Assistant Director of Respiratory Care Massachusetts General Hospital Boston, Massachusetts
FOCUS Annual Fall Classic 2018 Respiratory Care of the Patient with Traumatic Brain Injury Daniel W. Chipman, BS, RRT Assistant Director of Respiratory Care Massachusetts General Hospital Boston, Massachusetts
Head injuries. Severity of head injuries
 Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Monitoring of Cerebral and Spinal Haemodynamics during Neurosurgery
 Monitoring of Cerebral and Spinal Haemodynamics during Neurosurgery Bearbeitet von Georg E Cold, Niels Juul 1. Auflage 2008. Buch. XX, 332 S. Hardcover ISBN 978 3 540 77872 1 Format (B x L): 15,5 x 23,5
Monitoring of Cerebral and Spinal Haemodynamics during Neurosurgery Bearbeitet von Georg E Cold, Niels Juul 1. Auflage 2008. Buch. XX, 332 S. Hardcover ISBN 978 3 540 77872 1 Format (B x L): 15,5 x 23,5
UPDATE OF NEUROCRITICAL CARE PHARMACOTHERAPY. Vera Wilson, PharmD, BCPS Emergency Services Clinical Pharmacy Specialist Johnson City Medical Center
 UPDATE OF NEUROCRITICAL CARE PHARMACOTHERAPY Vera Wilson, PharmD, BCPS Emergency Services Clinical Pharmacy Specialist Johnson City Medical Center DISCLOSURE STATEMENT OF FINANCIAL INTEREST I, Vera Wilson,
UPDATE OF NEUROCRITICAL CARE PHARMACOTHERAPY Vera Wilson, PharmD, BCPS Emergency Services Clinical Pharmacy Specialist Johnson City Medical Center DISCLOSURE STATEMENT OF FINANCIAL INTEREST I, Vera Wilson,
Pediatric Head Injury:
 Pediatric Head Injury: Part I Basic Principles Jogi V. Pattisapu, MD FAAP FACS Emeritus Medical Director Arnold Palmer Medical Center College of Medicine University of Central Florida Orlando FL USA JogiP@mail.UCF.edu
Pediatric Head Injury: Part I Basic Principles Jogi V. Pattisapu, MD FAAP FACS Emeritus Medical Director Arnold Palmer Medical Center College of Medicine University of Central Florida Orlando FL USA JogiP@mail.UCF.edu
Cosa chiedo alla PtO 2
 Cosa chiedo alla PtO 2 Pr Mauro Oddo Department of Medical-Surgical Intensive Care Medicine CHUV-Lausanne University Hospital Faculty of Biology and Medicine, University of Lausanne, Switzerland NEURO
Cosa chiedo alla PtO 2 Pr Mauro Oddo Department of Medical-Surgical Intensive Care Medicine CHUV-Lausanne University Hospital Faculty of Biology and Medicine, University of Lausanne, Switzerland NEURO
Management of head injury in the intensive-care unit
 Management of head injury in the intensive-care unit Keith Girling Key points Head injuries are common and have a major impact predominantly on young individuals. Key principles of head-injury management
Management of head injury in the intensive-care unit Keith Girling Key points Head injuries are common and have a major impact predominantly on young individuals. Key principles of head-injury management
Changing Demographics in Death After Devastating Brain Injury
 Changing Demographics in Death After Devastating Brain Injury Andreas H. Kramer MD MSc FRCPC Departments of Critical Care Medicine & Clinical Neurosciences Foothills Medical Center, University of Calgary
Changing Demographics in Death After Devastating Brain Injury Andreas H. Kramer MD MSc FRCPC Departments of Critical Care Medicine & Clinical Neurosciences Foothills Medical Center, University of Calgary
What is elevated ICP?
 What is elevated ICP? and When should it be treated? David Menon Professor of Anaesthesia, University of Cambridge ICP monitoring recommended to reduce inhospital & 2-wk mortality Rx ICP > 22 mm Hg as
What is elevated ICP? and When should it be treated? David Menon Professor of Anaesthesia, University of Cambridge ICP monitoring recommended to reduce inhospital & 2-wk mortality Rx ICP > 22 mm Hg as
Severe Traumatic Brain Injury Protocol
 Severe Traumatic Brain Injury Protocol PROTOCOL I. Objective II. Definition of Severe TBI III. Patient Care: Parameters IV. Patient Care: Management Timeline (First 7 days of TBI) V. Nursing Care: Communication
Severe Traumatic Brain Injury Protocol PROTOCOL I. Objective II. Definition of Severe TBI III. Patient Care: Parameters IV. Patient Care: Management Timeline (First 7 days of TBI) V. Nursing Care: Communication
BRAIN TRAUMA THERAPEUTIC RECOMMENDATIONS
 1 BRAIN TRAUMA THERAPEUTIC RECOMMENDATIONS Richard A. LeCouteur, BVSc, PhD, Dip ACVIM (Neurology), Dip ECVN Professor Emeritus, University of California, Davis, California, USA Definitions Hemorrhage:
1 BRAIN TRAUMA THERAPEUTIC RECOMMENDATIONS Richard A. LeCouteur, BVSc, PhD, Dip ACVIM (Neurology), Dip ECVN Professor Emeritus, University of California, Davis, California, USA Definitions Hemorrhage:
Feeling the Pressure
 Feeling the Pressure (as in Intracranial Pressure.) Liz Kim, MSN, ACNS-BC, FAHA Advanced Practice Provider Neurocritical Care Stanford Health Care May 15, 2017 World Live Neurovascular Conference Disclosures
Feeling the Pressure (as in Intracranial Pressure.) Liz Kim, MSN, ACNS-BC, FAHA Advanced Practice Provider Neurocritical Care Stanford Health Care May 15, 2017 World Live Neurovascular Conference Disclosures
Lisa T. Hannegan, MS, CNS, ACNP. Department of Neurological Surgery University of California, San Francisco
 Lisa T. Hannegan, MS, CNS, ACNP Department of Neurological Surgery University of California, San Francisco Era of Clinical Neuro Monitoring Clinical Examination Heart rate Blood Pressure Body temperature
Lisa T. Hannegan, MS, CNS, ACNP Department of Neurological Surgery University of California, San Francisco Era of Clinical Neuro Monitoring Clinical Examination Heart rate Blood Pressure Body temperature
5/15/2018. Reduced Platelet Activity
 ASSOCIATION OF DESMOPRESSIN ACETATE ON OUTCOMES IN ACUTE INTRACRANIAL HEMORRHAGE IN PATIENTS ON ANTIPLATELET THERAPY Jessica McManus, Pharm. D. PGY2 Critical Care Pharmacy Resident UF Health Jacksonville
ASSOCIATION OF DESMOPRESSIN ACETATE ON OUTCOMES IN ACUTE INTRACRANIAL HEMORRHAGE IN PATIENTS ON ANTIPLATELET THERAPY Jessica McManus, Pharm. D. PGY2 Critical Care Pharmacy Resident UF Health Jacksonville
Mannitol for Resuscitation in Acute Head Injury: Effects on Cerebral Perfusion and Osmolality
 Original articles Mannitol for Resuscitation in Acute Head Injury: Effects on Cerebral Perfusion and Osmolality J. A. MYBURGH*, S. B. LEWIS *Intensive Care Unit, Royal Adelaide Hospital, Adelaide, SOUTH
Original articles Mannitol for Resuscitation in Acute Head Injury: Effects on Cerebral Perfusion and Osmolality J. A. MYBURGH*, S. B. LEWIS *Intensive Care Unit, Royal Adelaide Hospital, Adelaide, SOUTH
Continuous cerebral autoregulation monitoring
 Continuous cerebral autoregulation monitoring Dr Peter Smielewski ps10011@cam.ac.uk 20/10/2017 Division of Neurosurgery, Department of Clinical Neurosciences Determinants of cerebral blood flow Thanks
Continuous cerebral autoregulation monitoring Dr Peter Smielewski ps10011@cam.ac.uk 20/10/2017 Division of Neurosurgery, Department of Clinical Neurosciences Determinants of cerebral blood flow Thanks
Decompressive Hemicraniectomy in Acute Neurological Diseases
 Decompressive Hemicraniectomy in Acute Neurological Diseases Angela Crudele, MD 1 ; Syed Omar Shah, MD 1 ; Barak Bar, MD 1,2 Department of Neurology, Thomas Jefferson University, Philadelphia, PA, Department
Decompressive Hemicraniectomy in Acute Neurological Diseases Angela Crudele, MD 1 ; Syed Omar Shah, MD 1 ; Barak Bar, MD 1,2 Department of Neurology, Thomas Jefferson University, Philadelphia, PA, Department
Increased Intracranial Pressure 2.0 Contact Hours Presented by: CEU Professor
 Increased Intracranial Pressure 2.0 Contact Hours Presented by: CEU Professor 7 www.ceuprofessoronline.com Copyright 8 2007 The Magellan Group, LLC All Rights Reserved. Reproduction and distribution of
Increased Intracranial Pressure 2.0 Contact Hours Presented by: CEU Professor 7 www.ceuprofessoronline.com Copyright 8 2007 The Magellan Group, LLC All Rights Reserved. Reproduction and distribution of
Case Report Forms. Hospital Variables TBI Patients
 Case Report Forms Hospital Variables TBI Patients Table of Contents Clinical Protocol Grid... Hospital Admission and Discharge... Surgeries... Monitoring Devices... Complications... 9 Scheduled Medications...
Case Report Forms Hospital Variables TBI Patients Table of Contents Clinical Protocol Grid... Hospital Admission and Discharge... Surgeries... Monitoring Devices... Complications... 9 Scheduled Medications...
A Study to Describe Cerebral Perfusion Pressure Optimization Practice among ICU Patients of Tertiary Hospital of South India
 International Journal of Caring Sciences January-April 2018 Volume 11 Issue 1 Page 296 Original Article A Study to Describe Cerebral Perfusion Pressure Optimization Practice among ICU Patients of Tertiary
International Journal of Caring Sciences January-April 2018 Volume 11 Issue 1 Page 296 Original Article A Study to Describe Cerebral Perfusion Pressure Optimization Practice among ICU Patients of Tertiary
ESCMID Online Lecture Library. by author
 Neurologische Klinik und Poliklinik Prof. Dr. M. Dieterich Treatment of community acquired meningitis - ICU and neurologic perspective Izmir 2010 INFECTIOUS FOCI OF COMMUNITY ACQUIRED MENINGITIS The cause
Neurologische Klinik und Poliklinik Prof. Dr. M. Dieterich Treatment of community acquired meningitis - ICU and neurologic perspective Izmir 2010 INFECTIOUS FOCI OF COMMUNITY ACQUIRED MENINGITIS The cause
Pediatric Head Trauma August 2016
 PEDIATRIC HEAD TRAUMA AUGUST 2016 Pediatric Head Trauma August 2016 EDUCATION COMMITTEE PEER EDUCATION Quick Review of Pathophysiology of TBI Nuggets of knowledge to keep in mind with TBI Intracranial
PEDIATRIC HEAD TRAUMA AUGUST 2016 Pediatric Head Trauma August 2016 EDUCATION COMMITTEE PEER EDUCATION Quick Review of Pathophysiology of TBI Nuggets of knowledge to keep in mind with TBI Intracranial