Code Stroke Intervention: Endovascular therapy for asah and management J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY
|
|
|
- Philip Little
- 6 years ago
- Views:
Transcription
1 Code Stroke Intervention: Endovascular therapy for asah and management J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY
2 Disclosures None
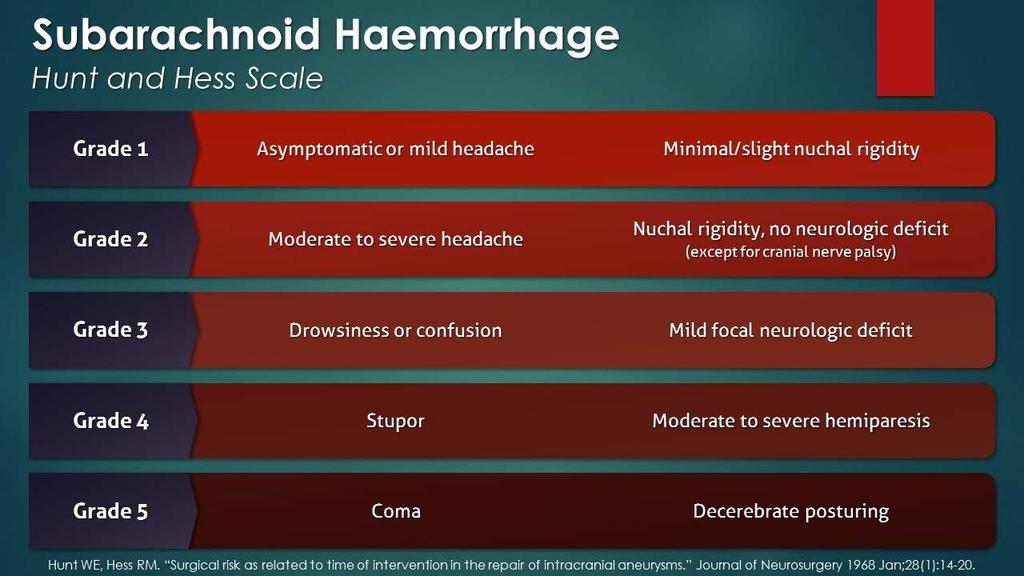
3 Part B. Objectives Epidemiology of asah Concept: What is a brain aneurysm Hunt and Hess grading scale Know about severity of bleed: modified Fisher scale (from CT head) ED management Case Management from RN perspective, after endovascular therapy
4 Introduction Brain aneurysm Definition: Persistent pathologic dilatation of an arterial wall. An estimated 6 million people in the United States have an unruptured brain aneurysm, or 1 in 50 people. Aneurysms are estimated to occur in approximately 2% to 6% of the population (based on autopsy and angiographic studies) Non traumatic SAH represents about 3% of all strokes in the US Worldwide incidence: 2 to 16 per 100,000 people Women are more likely to have SAH 1.24 : 1 Minority groups, particularly AA and Hispanic populations more frequently affected compared to white Americans
5 Introduction Incidence of SAH increases with age Mean onset of > 50 years ~80% of SAH, a ruptured cerebral aneurysm is found No source of bleeding in 15% of cases Other etiologies such as AVM in 5%
6 Introduction asah Mortality rates 8% to 67% Median is 30% in the US Prehospital deaths estimated between 10% to 15% There has been a significant decrease in case-fatality rates of SAH across the globe Likely owing to changes in managements of patients with SAH Neurocritical care Endovascular therapy Refined microsurgical techniques However, despite the decrease in case-fatality rates, about half of survivors experience significant chronic reduction in health-related quality of life
7 Introduction A large proportion of survivors do not return to their previous level of employment, social independence and interactions, or personal or family relationships even 5 years after the event. This may be due to a combination of factors, including Impaired physical functioning Cognitive deficits particularly executive function and memory Mood and emotional symptoms e.g. anxiety, depression and PTSD Personality changes
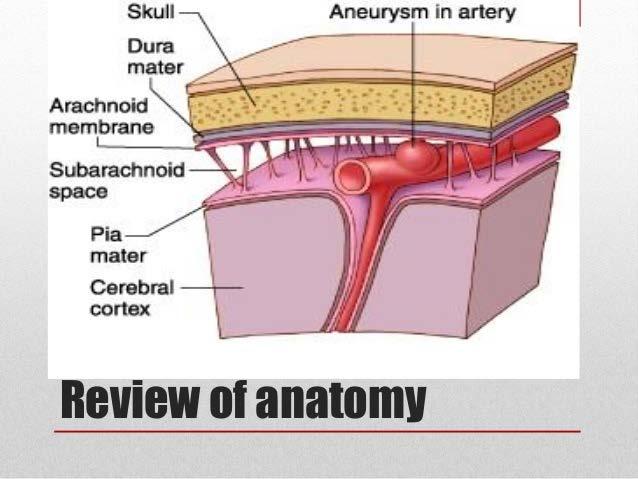
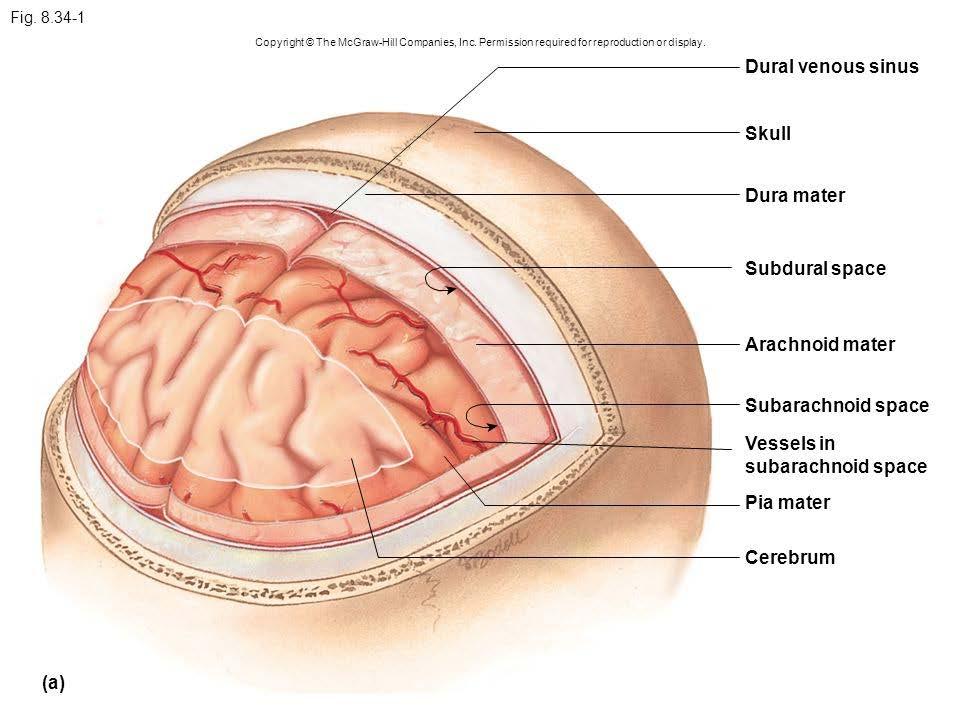
8 Subarachnoid Space

9 Common locations of brain aneurysms ~75% of brain aneurysms In these locations: - Acomm - Pcomm - MCA bifurcation



 Large")


10 Aneurysm Types 10 Aneurysms can be classified by size and by configuration Small (< 10 mm) Large (10-25 mm) Giant (> 25 mm) Saccular Wide- Necke d Fusiform 1
11
12 Main emphasis when caring for patients with SAH Prompt evaluation and diagnosis Immediate transfer to appropriate centers Expeditious diagnosis and treatment of the bleeding source Overall good neurocritical care adhering to available treatment guidelines.
13 Clinical Presentation SAH typically presents with sudden and severe headache Described as the worst headache ever Nausea, vomiting d/t transient elevation in intracranial pressure (ICP) Photophobia Neck pain Loss of consciousness d/t more sustained and severe ICP; can lead to coma and brain death. Physical examination should include Determination of level of consciousness, fundoscopic evaluation Determination of meningeal signs Presence of focal neurologic deficits in about 10% of cases and are associated with worse prognosis when thick SAH clot or parenchymal hemorrhage
14 Clinical presentation Occasionally, patients may present with seizures, acute encephalopathy and concomitant subdural hematoma and head trauma diagnosis of SAH may become more elusive A minority of patients may have a warning sentinel headache days to weeks before an aneurysmal SAH though to represent a small aneurysmal leak Unfortunately this information is only obtained retrospectively as most of the time the headache is transient and head CT scanning is unrevealing in about 50% of cases
15 Step 1: Diagnosis Head CT scan LP Sensitivity of 98%-100% for detection of SAH within 12 hours of symptom onset when compared to LP Sensitivity decreases to 93% at 24 hours Sensitivity only 50% at 7 days Recommended in any patient with suspected SAH and negative or equivocal results on head CT. CSF should be collected in 4 consecutive tubes and RBC count should be determined in tubes #1 and #4. Diagnosis: Elevated opening pressure, elevated RBC count that does not significantly decrease from tube #1 to tube #4, and xanthochromia
16 Initial evaluation Main focus initially is stabilization of airway, breathing and circulation Patients who are unable to protect their airway should be intubated immediately Most common indications: Coma, HCP, seizure, need for sedation for significant agitation Once deemed stable CT brain Avoid hypertension MAP < 110 mmhg or systolic less than 140 mmhg until the ruptured aneurysm is secured Use premorbid baseline blood pressure to refine targets and avoid hypotension Pain control best achieved with short acting opiates I.v. labetalol 5mg to 20 mg pushes Nicardipine 5 to 15 mg/h continuous
17 Step 2: Disease severity scoring What are the strongest predictors of neurologic complications and outcomes after SAH? Severity of neurologic impairment on presentation Amount of SAH on admission
18
19 Step 3: Admission to High-Volume Centers Transfer to high volume center, if not already in one Admit the patient to a dedicated neurocritical care unit Have the patient undergo a multidisciplinary evaluation for the management of an unsecured cerebral aneurysm
20 Case #1 45 y/o right handed woman presented to PSC with sudden onset of severe H/A, N/V and syncope 1 hour prior to presentation while she was moving furniture at her house PMHx of heavy smoking and cocaine use VS; BP 180/100 mmhg, HR 105 an SaO2 97% on room air, T 36.5 C GCS15, Hunt and Hess grade 2, modified Fisher scale score 3
21

22 NORMAL ADULT CT BRAIN


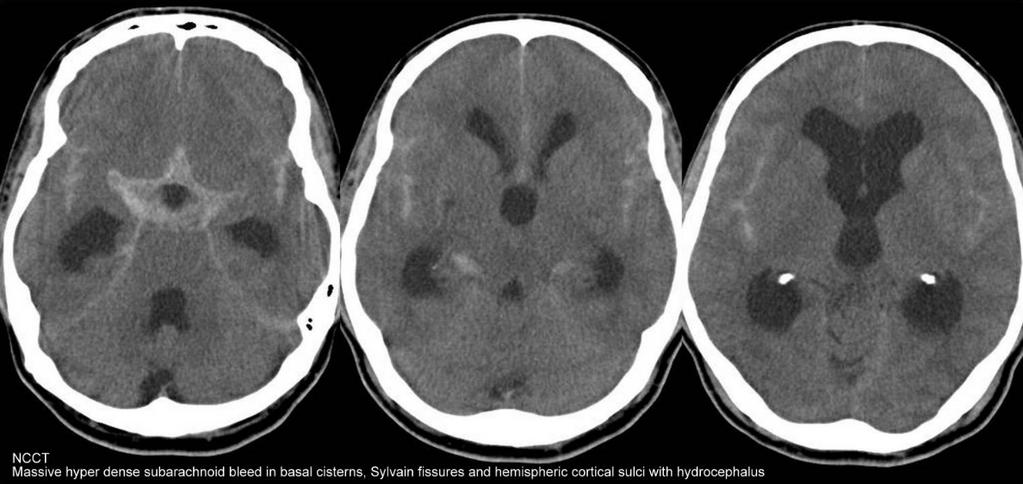
23 Case #1


24 Case #1 She was started on a nicardipine drip to keep her SBP < 140 mmhg Transferred to a CSC DSA demonstrated an irregular, multilobed and wide-neck Acomm aneurysm After discussion with INR, NeuroSx and neuroicu, patient underwent surgical clipping

25 Clipping vs. coiling clipping coiling
26 Rerupture risk Rebleeding in unsecured aneurysms: 1 st 24 hours risk is 4% to 15% 1 st 10 days 2% to 4% per day for the first 10 days 30% during the first 30 days 2-4% per year thereafter Main risk factors associated with rebleeding: Rebleeding rate in secured (treated aneurysms) Coiling: 1-2% Clipping ~ 1% SBP > 160 mmhg Poor neurologic grade Intracerebral or intraventricular hematomas Ruptured posterior circulation aneurysms Aneurysms > 10 mm in size
 Coiling vs.")
27 Best measure to reduced the risk of rebleeding Early treatment of unsecured aneurysms (as seen on previous slides) Coiling vs. clipping
28 Step 4: Treatment of unsecured aneurysms Surgical clipping vs. Endovascular coiling Choice depends on several factors including: Age Aneurysm location Morphology of the aneurysm Relationship to adjacent vessels Because of the complexity of determining the most appropriate treatment for individual patients, it is recommended that a multidisciplinary team made up of cerebrovascular neurosurgeons, endovascular practitioners and neurointensivists confer to reach a consensus Overall, endovascular coiling should be preferred over surgical clipping whenever possible.
29 Step 5: ICU management More than 75% of SAH experience SIRS likely as a result of elevated levels of inflammatory cytokines. SAH patients at higher risk for HCP Cerebral edema Delayed cerebral ischemia (DCI) Rebleeding Seizures Neuroendocrine abnormalities that lead to impaired body regulation of Na+, water and glucose SAH also unleashes hypothalamic-mediated changes, including increased sympathetic and parasympathetic drive, that result in cardiac and pulmonary complications. EKG changes, arrhythmias, impaired cardiac contractility (eg, Takotsubo cardiomyopathy), troponinemia, and myocardial necrosis. Pulmonary complications: Neurogenic pulmonary edema

30 Seizures 20%-26% may present with seizure like episodes Patients with MCA bifurcation aneurysms, concomitant intraparenchymal hematomas, and poor clinical grade are at higher risk for seizures Patients treated with coiling have lower rates of seizures Long term risk for epilepsy is low Prophylactic anticonvulsants, 3 to 7 days. Frequency of subclinical seizure may be high in patients with poor-grade SAH continuous EEG monitoring

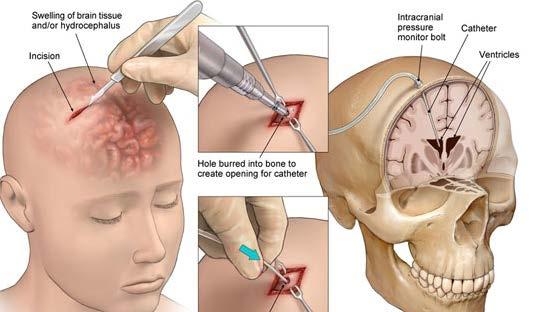
31 Hydrocephalus Acute symptomatic HCP occurs in about 20% of patients with SAH, usually within the first few days after symptom onset What to look for? Decreased level of consciousness Signs of increased ICP such as impaired upward gaze and HTN Immediate f/u CT head is warranted EVD may follow Some centers perform a lumbar drain Weaning the patient of an EVD should begin shortly after aneurysm obliteration or within 48 hours of insertion if patient is neurologically stable ~60% of patients who undergo EVD will have successful weaning; others may require VPS.


32 Hydrocephalus Arachnoid granulations get clogged by subarachnoid blood causing hydrocephalus
33 Hydrocephalus
34 VASOSPASM PROPHYLAXIS(?) Nimodipine 60 mg PO q 4 hours for 21 days Affords neuroprotection without decreasing the frequency of angiographic vasospasm Adverse effects: constipation and hypotension Maintain euvolemia Hypervolemia has not been shown to improve CBF or decrease frequency of vasospasm/dci No established methodology as to how to achieve euvolemia Many intensivist use a combination of methods: strict monitoring of fluid balance, central venous pressure, echocardiogram, and stroke volume variation In practice, euvolemia can be achieved by replacing urine output and even administering fludrocortisone or hydrocortisone in patients with significant diuresis
 SAH, no IVH 33% 4 - Thick SAH, with IVH")
35 Vasospasm and delayed cerebral ischemia (DCI) Modified Fisher Grade 1 - Focal of diffuse thin (<1mm) SAH, no IVH Risk of Vasospasm 24% 2 - Focal or diffuse thin SAH, with IVH 33% 3 - Thick (>1mm) SAH, no IVH 33% 4 - Thick SAH, with IVH 40%
36 Pathophysiology of cerebral vasospasm and DCI Most likely, the main driver is the release of oxyhemoglobin and erythrocyte contents through hemolysis, which unleashes a host of inflammatory and proapoptotic factors The risk of vasospasm increases with Thickness of SAH, density, location, persistence of the SAH Poor clinical grade, loss of consciousness at ictus, cigarette smoking, cocaine use, SIRS, hyperglycemia and HCP However, predicting who will have vasospasm is difficult
37 Vasospasm and delayed cerebral ischemia (DCI)
38 Diagnosis of vasospasm/dci Not easy Frequent neuro checks, at least q 2 hours Suspect DCI if new neurologic impairment of at least 2 points on GCS that lasts for more than 1 hour and cannot be explained by any other cause. Monitoring: Multimodal and includes ICP, CPP, CBF, EEG TCD, DSA, CTA, CT perfusion MR brain, MRA, MR perfusion
39 Delayed Cerebral Ischemia (DCI) Once the diagnosis of cerebral vasospasm is confirmed (after ruling out other neurologic and systemic disorders) treat with: Induced Hypertension Endovascular therapy Goal: Complete resolution of symptoms. Management of DCI is carried out in stepwise fashion Final confirmation and treatment must be done within 2 hours of symptom onset.
40 Treatment I.v. bolus of NS 1 to 2 liters is administered Hypertension is induced with Phenylephrine or Norepinephrine Blood pressure augmentation progresses in stepwise fashion with frequent assessment of neurologic function at each 10 mmhg change in systolic (up to 200 mmhg) or MAP If neurologic deficits persist then patients undergoes CT/CTA/CTP followed by DSA for endovascular therapy Induced hypertension is maintained for at least 72 hours or until stability is achieved and is slowly weaned off after that
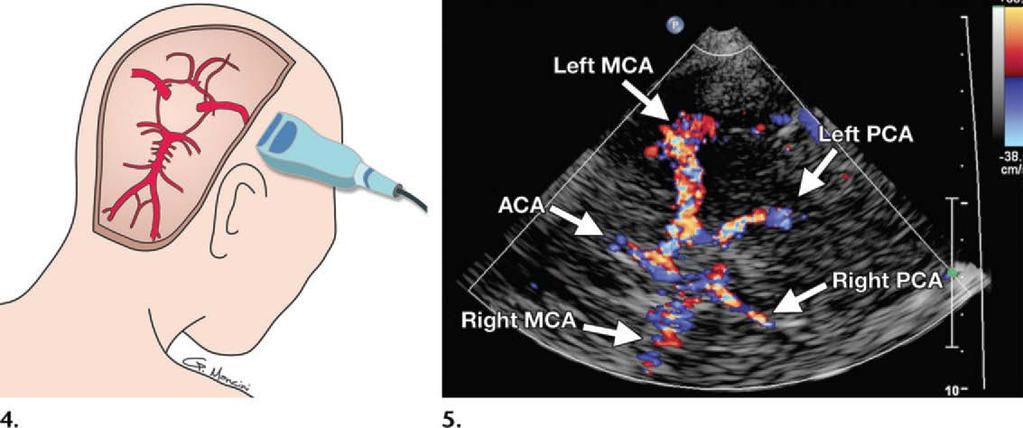
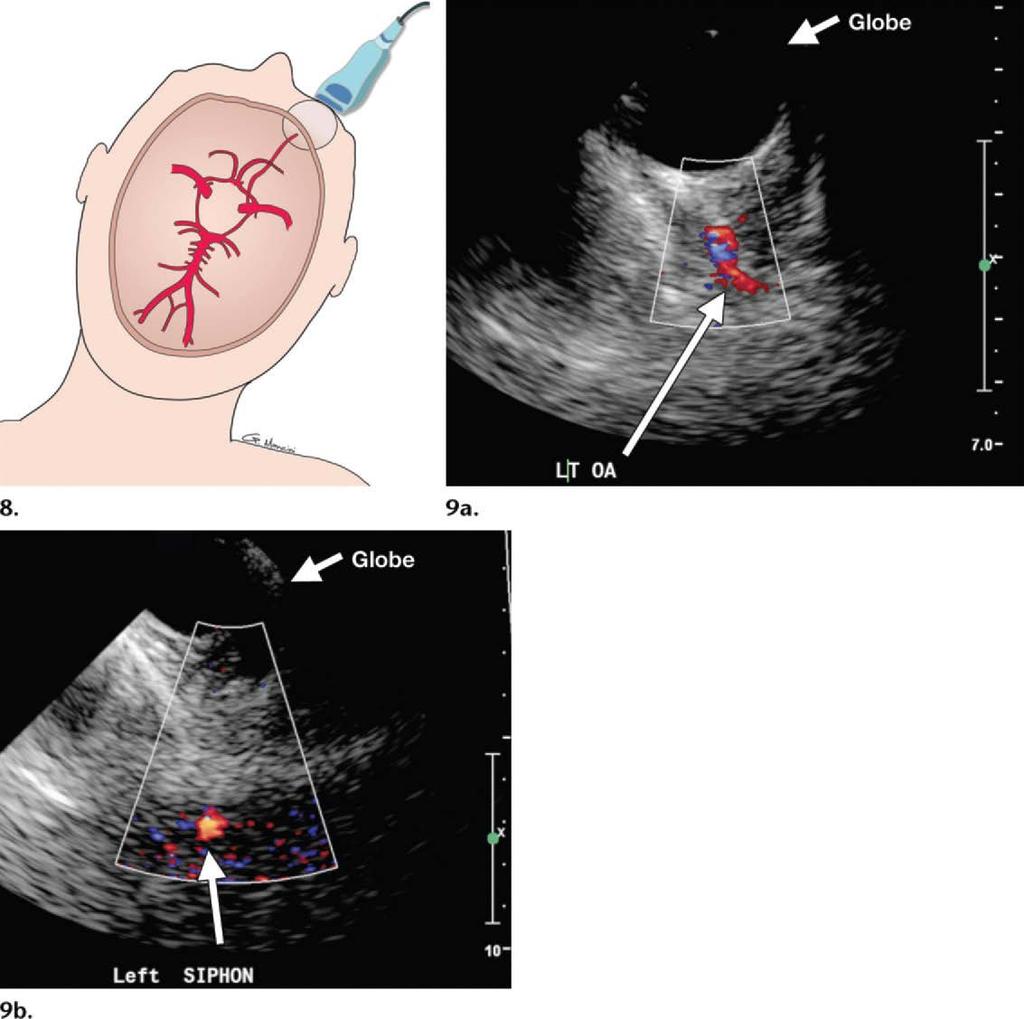
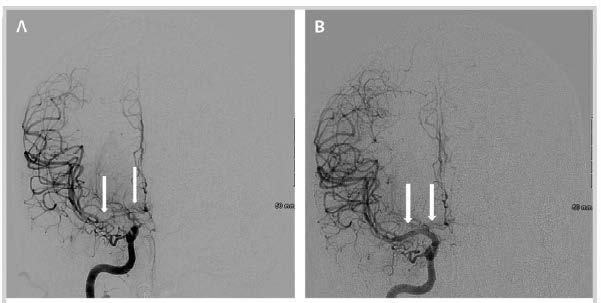
41 Case #1 continued Patient continued to evolve satisfactorily with normal Transcranial Doppler (TCD) On Postbleed day 6, TCD revealed an increase in Mean Flow Velocity (MFV) in the right MCA from 80 cm/s to 180 cm/s
42 Transcranial Doppler (TCD)
43 Case #1 continued Patient continued to evolve satisfactorily with normal Transcranial Doppler (TCD) On Postbleed day 6, TCD revealed an increase in Mean Flow Velocity (MFV) in the right MCA from 80 cm/s to 180 cm/s The next morning the patient developed sudden onset of left hemiparesis and confusion CT brain showed no rebleeding, cerebral edema or HCP She received a bolus of 500 ml of NS via i.v. and was started on norepinephrine drip with some improvement on her left hemiparesis but without resolution BMP was normal, WBC was 14K F/U TCD showed right MCA MFV of 220 cm/s and a Lindegaard ration
44
45 Case #1 continued Her SBP was maintained at greater than 180 mmhg for 3 more days TCD showed improvement in MFV by day 9 to less than 100 cm/s; weaned off norepinephrine by day 10 On day 11 she developed a decreased level of consciousness without focal neurological findings except for limited upward gaze F/U CT showed HCP requiring an EVD

46
47 Case Several #1 attempts continued to wean off the patient from the EVD failed; she underwent a programmable VP shunt placement on day 15 She was transferred to a regular floor Discharged to home on day 17 after clearance by physical and occupational therapies with instructions to continue on oral nimodipine to complete 21 days (for four more days)
48 Medical complications Cardiopulmonary Minor EKG changes to severe dilated cardiomyopathy and ARDS Elevated troponin also frequent up to 30% of patients with SAH Fever Most common non neurologic complication seen in up to 70% of patients Antipyretic medications surface cooling or intravascular devices while avoiding shivering Thromboembolism DVT incidence 2% to 20% SCDS for everyone Heparin SQ 24 hours after aneurysm obliteration
49 Fludrocortisone if diuresis is active Medical complications Glucose abnormalities Hyperglycemia is a common phenomenon. Maintain level between 80 to 200 mg/dl Hyponatremia: The most common electrolyte disorder seen in up to 30% of SAH patients Hyponatremia has been associated with the development of DCI and poor clinical outcomes Can be secondary to cerebral salt wasting or inappropriate secretion of ADH Traditionally the former is treated with volume infusion and the latter with fluid restriction However, hypovolemia is associated with poor outcomes, so fluid restriction should be avoided in patients with SAH Oral free water restriction and maintain euvolemia Continuous infusion of hypertonic saline (1.5% to 3%)
50 Conclusion SHA is a neurologic emergency with high morbidity and mortality SAH is more frequent in women than men More frequent in minority populations Main areas when caring for patients with SAH should be the following: Prompt evaluation and diagnosis Immediate transfer to appropriate centers Expeditious diagnosis and treatment of bleeding source Overall good neurocritical care adhering to available treatment guidelines Main neurologic complications: HCP, seizures, cerebral edema, delayed cerebral ischemia, and neuroendocrine disorders Patients with SAH frequently experience cardiopulmonary complications, which can be life threatening.
Subarachnoid Hemorrhage (SAH) Disclosures/Relationships. Click to edit Master title style. Click to edit Master title style.
 Disclosures/Relationships. Click to edit Master title style. Click to edit Master title style.") Subarachnoid Hemorrhage (SAH) William J. Jones, M.D. Assistant Professor of Neurology Co-Director, UCH Stroke Program Click to edit Master title style Disclosures/Relationships No conflicts of interest
Subarachnoid Hemorrhage (SAH) William J. Jones, M.D. Assistant Professor of Neurology Co-Director, UCH Stroke Program Click to edit Master title style Disclosures/Relationships No conflicts of interest
Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage. Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA
 Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA The traditional view: asah is a bad disease Pre-hospital mortality
Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA The traditional view: asah is a bad disease Pre-hospital mortality
Aneurysmal Subarachnoid Hemorrhage Presentation and Complications
 Aneurysmal Subarachnoid Hemorrhage Presentation and Complications Sherry H-Y. Chou MD MMSc FNCS Department of Critical Care Medicine, Neurology and Neurosurgery University of Pittsburgh School of Medicine
Aneurysmal Subarachnoid Hemorrhage Presentation and Complications Sherry H-Y. Chou MD MMSc FNCS Department of Critical Care Medicine, Neurology and Neurosurgery University of Pittsburgh School of Medicine
4/10/2018. The Surgical Treatment of Cerebral Aneurysms. Aneurysm Locations. Aneurysmal Subarachnoid Hemorrhage. Jerone Kennedy, M.D.
 The Surgical Treatment of Cerebral Aneurysms Aneurysmal Subarachnoid Hemorrhage Jerone Kennedy, M.D. Medical Director, Vascular Neurosurgery CentraCare Health-Neurosciences St. Cloud Hospital Aneurysm
The Surgical Treatment of Cerebral Aneurysms Aneurysmal Subarachnoid Hemorrhage Jerone Kennedy, M.D. Medical Director, Vascular Neurosurgery CentraCare Health-Neurosciences St. Cloud Hospital Aneurysm
The Worst Headache of My Life Hemorrhagic Stroke
 The Worst Headache of My Life Hemorrhagic Stroke Lindsay Trantum ACNP-BC Neurocritical Care Nurse Practitioner Assistant in Anesthesiology, Division of Critical Care Objectives Identify the risk factors
The Worst Headache of My Life Hemorrhagic Stroke Lindsay Trantum ACNP-BC Neurocritical Care Nurse Practitioner Assistant in Anesthesiology, Division of Critical Care Objectives Identify the risk factors
TCD AND VASOSPASM SAH
 CURRENT TREATMENT FOR CEREBRAL ANEURYSMS TCD AND VASOSPASM SAH Michigan Sonographers Society 2 Nd Annual Fall Vascular Conference Larry N. Raber RVT-RDMS Clinical Manager General Ultrasound-Neurovascular
CURRENT TREATMENT FOR CEREBRAL ANEURYSMS TCD AND VASOSPASM SAH Michigan Sonographers Society 2 Nd Annual Fall Vascular Conference Larry N. Raber RVT-RDMS Clinical Manager General Ultrasound-Neurovascular
SAH READMISSIONS TO NCCU
 SAH READMISSIONS TO NCCU Are they preventable? João Amaral Rebecca Gorf Critical Care Outreach Team - NHNN 2015 Total admissions to NCCU =862 Total SAH admitted to NCCU= 104 (93e) (12.0%) Total SAH readmissions=
SAH READMISSIONS TO NCCU Are they preventable? João Amaral Rebecca Gorf Critical Care Outreach Team - NHNN 2015 Total admissions to NCCU =862 Total SAH admitted to NCCU= 104 (93e) (12.0%) Total SAH readmissions=
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
Neurosurgical Management of Stroke
 Overview Hemorrhagic Stroke Ischemic Stroke Aneurysmal Subarachnoid hemorrhage Neurosurgical Management of Stroke Jesse Liu, MD Instructor, Neurological Surgery Initial management In hospital management
Overview Hemorrhagic Stroke Ischemic Stroke Aneurysmal Subarachnoid hemorrhage Neurosurgical Management of Stroke Jesse Liu, MD Instructor, Neurological Surgery Initial management In hospital management
ENDOVASCULAR TREATMENT OF CEREBRAL ANEURYSMS AND MANAGEMENT OF RUPTURED ANEURYSM. Vikram Jadhav MD, PhD. 04/12/2018 CentraCare Health St.
 ENDOVASCULAR TREATMENT OF CEREBRAL ANEURYSMS AND MANAGEMENT OF RUPTURED ANEURYSM Vikram Jadhav MD, PhD 04/12/2018 CentraCare Health St. Cloud, MN OBJECTIVES Understand epidemiology and risk factors for
ENDOVASCULAR TREATMENT OF CEREBRAL ANEURYSMS AND MANAGEMENT OF RUPTURED ANEURYSM Vikram Jadhav MD, PhD 04/12/2018 CentraCare Health St. Cloud, MN OBJECTIVES Understand epidemiology and risk factors for
Disclosures. Objectives. Critical Care Management of Subarachnoid Hemorrhage. Nothing to disclose
 Critical Care Management of Subarachnoid Hemorrhage Nerissa U. Ko, MD, MAS UCSF Department of Neurology September 7, 2013 Nothing to disclose Disclosures Grant funding from American Heart Association,
Critical Care Management of Subarachnoid Hemorrhage Nerissa U. Ko, MD, MAS UCSF Department of Neurology September 7, 2013 Nothing to disclose Disclosures Grant funding from American Heart Association,
Sub-arachnoid haemorrhage
 Sub-arachnoid haemorrhage Dr Mary Newton Consultant Anaesthetist The National Hospital for Neurology and Neurosurgery UCL Hospitals NHS Trust mary.newton@uclh.nhs.uk Kiev, Ukraine September 17 th 2009
Sub-arachnoid haemorrhage Dr Mary Newton Consultant Anaesthetist The National Hospital for Neurology and Neurosurgery UCL Hospitals NHS Trust mary.newton@uclh.nhs.uk Kiev, Ukraine September 17 th 2009
11/27/2017. Stroke Management in the Neurocritical Care Unit. Conflict of interest. Karel Fuentes MD Medical Director of Neurocritical Care
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Current State of the Art
 SAH Current State of the Art Thomas C. Steineke, M.D., Ph.D. Director of Neurovascular Surgery NJ Neuroscience Institute JFK Medical Center Introduction Signs and symptoms of a problem What are aneurysms
SAH Current State of the Art Thomas C. Steineke, M.D., Ph.D. Director of Neurovascular Surgery NJ Neuroscience Institute JFK Medical Center Introduction Signs and symptoms of a problem What are aneurysms
11/23/2015. Disclosures. Stroke Management in the Neurocritical Care Unit. Karel Fuentes MD Medical Director of Neurocritical Care.
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE
 WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE Subarachnoid Hemorrhage is a serious, life-threatening type of hemorrhagic stroke caused by bleeding into the space surrounding the brain,
WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE Subarachnoid Hemorrhage is a serious, life-threatening type of hemorrhagic stroke caused by bleeding into the space surrounding the brain,
Diagnosis of Subarachnoid Hemorrhage (SAH) and Non- Aneurysmal Causes
 and Non- Aneurysmal Causes") Diagnosis of Subarachnoid Hemorrhage (SAH) and Non- Aneurysmal Causes By Sheila Smith, MD Swedish Medical Center 1 Disclosures I have no disclosures 2 Course Objectives Review significance and differential
Diagnosis of Subarachnoid Hemorrhage (SAH) and Non- Aneurysmal Causes By Sheila Smith, MD Swedish Medical Center 1 Disclosures I have no disclosures 2 Course Objectives Review significance and differential
Traumatic Brain Injuries
 Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Standardize comprehensive care of the patient with severe traumatic brain injury
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute
 H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute Memorial Hermann- Texas Medical Center Learning Objectives
H Alex Choi, MD MSc Assistant Professor of Neurology and Neurosurgery The University of Texas Health Science Center Mischer Neuroscience Institute Memorial Hermann- Texas Medical Center Learning Objectives
8/29/2011. Brain Injury Incidence: 200/100,000. Prehospital Brain Injury Mortality Incidence: 20/100,000
 Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Subarachnoid Hemorrhage and Brain Aneurysm
 Subarachnoid Hemorrhage and Brain Aneurysm DIN Department of Interventional Neurology What is SAH? Subarachnoid Haemorrhage is the sudden leaking (haemorrhage) of blood from the blood vessels of brain.
Subarachnoid Hemorrhage and Brain Aneurysm DIN Department of Interventional Neurology What is SAH? Subarachnoid Haemorrhage is the sudden leaking (haemorrhage) of blood from the blood vessels of brain.
THE EFFICACY AND SAFETY OF CILOSTAZOL IN SUBARACHNOID HEMORRHAGE. A META- ANALYSIS OF RANDOMIZED AND NON RANDOMIZED STUDIES DR. MUHAMMAD F.
 THE EFFICACY AND SAFETY OF CILOSTAZOL IN SUBARACHNOID HEMORRHAGE. A META- ANALYSIS OF RANDOMIZED AND NON RANDOMIZED STUDIES DR. MUHAMMAD F. ISHFAQ ZEENAT QURESHI STROKE INSTITUTE AND UNIVERSITY OF TENNESSEE,
THE EFFICACY AND SAFETY OF CILOSTAZOL IN SUBARACHNOID HEMORRHAGE. A META- ANALYSIS OF RANDOMIZED AND NON RANDOMIZED STUDIES DR. MUHAMMAD F. ISHFAQ ZEENAT QURESHI STROKE INSTITUTE AND UNIVERSITY OF TENNESSEE,
CEREBRAL ANEURYSM. Epidemiology. Number of Case per Year 12/15/2008. Wanarak Watcharasakailp M.D.
 Epidemiology CEREBRAL ANEURYSM Wanarak Watcharasakailp M.D. 5-10% of all stroke 6-7 /100,000 persons/yrs, 20/100,000 in Finland and Japan Female predominant Most in anterior circulation Female->ICA 36.8%
Epidemiology CEREBRAL ANEURYSM Wanarak Watcharasakailp M.D. 5-10% of all stroke 6-7 /100,000 persons/yrs, 20/100,000 in Finland and Japan Female predominant Most in anterior circulation Female->ICA 36.8%
Aneurysmal SAH Jenny Fox APN, CCRN, CNRN, ACNP-BC
 Epidemiology of asah Incidence 9.7 to 14.5 per 100,000 in the United States. About 30,000 yearly in North America. Aneurysmal SAH Jenny Fox APN, CCRN, CNRN, ACNP-BC Mean age of onset is 55 years. Most
Epidemiology of asah Incidence 9.7 to 14.5 per 100,000 in the United States. About 30,000 yearly in North America. Aneurysmal SAH Jenny Fox APN, CCRN, CNRN, ACNP-BC Mean age of onset is 55 years. Most
Cerebrovascular Disorders. Blood, Brain, and Energy. Blood Supply to the Brain 2/14/11
 Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
REVIEW. Neurocrit Care (2011) 15: DOI /s Published online: 20 July 2011 Ó Springer Science+Business Media, LLC 2011
 15: DOI /s Published online: 20 July 2011 Ó Springer Science+Business Media, LLC 2011") Neurocrit Care (2011) 15:211 240 DOI 10.1007/s12028-011-9605-9 REVIEW Critical Care Management of Patients Following Aneurysmal Subarachnoid Hemorrhage: from the Neurocritical Care Society s Multidisciplinary
Neurocrit Care (2011) 15:211 240 DOI 10.1007/s12028-011-9605-9 REVIEW Critical Care Management of Patients Following Aneurysmal Subarachnoid Hemorrhage: from the Neurocritical Care Society s Multidisciplinary
Supplement Table 1. Definitions for Causes of Death
 Supplement Table 1. Definitions for Causes of Death 3. Cause of Death: To record the primary cause of death. Record only one answer. Classify cause of death as one of the following: 3.1 Cardiac: Death
Supplement Table 1. Definitions for Causes of Death 3. Cause of Death: To record the primary cause of death. Record only one answer. Classify cause of death as one of the following: 3.1 Cardiac: Death
Subarachnoid Bleeds. Under the Spider via deepthought 1 / 22
 Subarachnoid Bleeds Under the Spider via deepthought 1 / 22 SAH: symptoms worst headache of my life Sudden-onset Severe w max intensity in seconds = thunderclap Sentinel headache in ~10-40% in aneurysmal
Subarachnoid Bleeds Under the Spider via deepthought 1 / 22 SAH: symptoms worst headache of my life Sudden-onset Severe w max intensity in seconds = thunderclap Sentinel headache in ~10-40% in aneurysmal
Pre-hospital Response to Trauma and Brain Injury. Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center
 Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
Intra-arterial nimodipine for the treatment of vasospasm due to aneurysmal subarachnoid hemorrhage
 Romanian Neurosurgery (2016) XXX 4: 461 466 461 DOI: 10.1515/romneu-2016-0074 Intra-arterial nimodipine for the treatment of vasospasm due to aneurysmal subarachnoid hemorrhage A. Chiriac, Georgiana Ion*,
Romanian Neurosurgery (2016) XXX 4: 461 466 461 DOI: 10.1515/romneu-2016-0074 Intra-arterial nimodipine for the treatment of vasospasm due to aneurysmal subarachnoid hemorrhage A. Chiriac, Georgiana Ion*,
Medical Management of Intracranial Hypertension. Joao A. Gomes, MD FAHA Head, Neurointensive Care Unit Cerebrovascular Center
 Medical Management of Intracranial Hypertension Joao A. Gomes, MD FAHA Head, Neurointensive Care Unit Cerebrovascular Center Anatomic and Physiologic Principles Intracranial compartments Brain 80% (1,400
Medical Management of Intracranial Hypertension Joao A. Gomes, MD FAHA Head, Neurointensive Care Unit Cerebrovascular Center Anatomic and Physiologic Principles Intracranial compartments Brain 80% (1,400
Intracranial Hemorrhage. Objectives. What Do Need to Know?
 Intracranial Hemorrhage What Do Need to Know? Kerry Brega, MD Associate Professor of Neurosurgery University of Colorado Objectives Know the common types of ICH. Know how they can be differentiated. Know
Intracranial Hemorrhage What Do Need to Know? Kerry Brega, MD Associate Professor of Neurosurgery University of Colorado Objectives Know the common types of ICH. Know how they can be differentiated. Know
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS. ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS
 FOR THROMBOLYSIS") NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS I. Purpose : A. To reduce morbidity and mortality associated
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS I. Purpose : A. To reduce morbidity and mortality associated
Raw and Quantitative EEG for Identification of Ischemia
 Raw and Quantitative EEG for Identification of Ischemia Susan T. Herman, MD Assistant Professor of Neurology Beth Israel Deaconess Medical Center Harvard Medical School Boston, MA Disclosures None relevant
Raw and Quantitative EEG for Identification of Ischemia Susan T. Herman, MD Assistant Professor of Neurology Beth Israel Deaconess Medical Center Harvard Medical School Boston, MA Disclosures None relevant
Ischemia cerebrale dopo emorragia subaracnoidea Vasospasmo e altri nemici
 Ischemia cerebrale dopo emorragia subaracnoidea Vasospasmo e altri nemici Nino Stocchetti Milan University Neuroscience ICU Ospedale Policlinico IRCCS Milano stocchet@policlinico.mi.it Macdonald RL et
Ischemia cerebrale dopo emorragia subaracnoidea Vasospasmo e altri nemici Nino Stocchetti Milan University Neuroscience ICU Ospedale Policlinico IRCCS Milano stocchet@policlinico.mi.it Macdonald RL et
Stroke Guidelines. November 19, 2011
 Stroke Guidelines November 19, 2011 Clinical Practice Guidelines American Stroke Association Guidelines are comprehensive statements that provide the highest level of scientific evidence for clinical practice.
Stroke Guidelines November 19, 2011 Clinical Practice Guidelines American Stroke Association Guidelines are comprehensive statements that provide the highest level of scientific evidence for clinical practice.
Assessment of Vasospasm and Delayed Cerebral Ischemia after Subarachnoid Hemorrhage: Current concepts and Value of CT Perfusion and CT Angiography
 Assessment of Vasospasm and Delayed Cerebral Ischemia after Subarachnoid Hemorrhage: Current concepts and Value of CT Perfusion and CT Angiography Poster No.: C-2563 Congress: ECR 2012 Type: Educational
Assessment of Vasospasm and Delayed Cerebral Ischemia after Subarachnoid Hemorrhage: Current concepts and Value of CT Perfusion and CT Angiography Poster No.: C-2563 Congress: ECR 2012 Type: Educational
7/18/2018. Cerebral Vasospasm: Current and Emerging Therapies. Disclosures. Objectives
 Cerebral : Current and Emerging Therapies Chad W. Washington MS, MD, MPHS Assistant Professor Department of Neurosurgery Disclosures None Objectives Brief Overview How we got here Review of Trials Meta-analysis
Cerebral : Current and Emerging Therapies Chad W. Washington MS, MD, MPHS Assistant Professor Department of Neurosurgery Disclosures None Objectives Brief Overview How we got here Review of Trials Meta-analysis
Tony L Smith DNP RN ACNP CCRN CFRN EMT-IV Vanderbilt LifeFlight
 Treatment of a Stroke patient: A look at how to care for the Stroke patient in the aeromedical setting Tony L Smith DNP RN ACNP CCRN CFRN EMT-IV Vanderbilt LifeFlight Objectives 1. Discuss the assessment
Treatment of a Stroke patient: A look at how to care for the Stroke patient in the aeromedical setting Tony L Smith DNP RN ACNP CCRN CFRN EMT-IV Vanderbilt LifeFlight Objectives 1. Discuss the assessment
Protocol for IV rtpa Treatment of Acute Ischemic Stroke
 Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Update in Diagnosis and Management of Intracranial Aneurysms for Primary Health Care Providers November 15, 2012 Boston, Massachusetts
 Update in Diagnosis and Management of Intracranial Aneurysms for Primary Health Care Providers November 15, 2012 Boston, Massachusetts Educational Partner: Session 1: Update in Diagnosis and Management
Update in Diagnosis and Management of Intracranial Aneurysms for Primary Health Care Providers November 15, 2012 Boston, Massachusetts Educational Partner: Session 1: Update in Diagnosis and Management
Modern Management of ICH
 Modern Management of ICH Bradley A. Gross, MD Assistant Professor, Dept of Neurosurgery, University of Pittsburgh October 2018 ICH Background Assessment & Diagnosis Medical Management Surgical Management
Modern Management of ICH Bradley A. Gross, MD Assistant Professor, Dept of Neurosurgery, University of Pittsburgh October 2018 ICH Background Assessment & Diagnosis Medical Management Surgical Management
Marcey Osgood, DO Assistant Professor of Neurocritical Care UMASS Medical Center
 Marcey Osgood, DO Assistant Professor of Neurocritical Care UMASS Medical Center Nothing to disclose Review common neurologic emergencies Ischemic Stroke Hemorrhagic Stroke Subarachnoid Hemorrhage Discuss
Marcey Osgood, DO Assistant Professor of Neurocritical Care UMASS Medical Center Nothing to disclose Review common neurologic emergencies Ischemic Stroke Hemorrhagic Stroke Subarachnoid Hemorrhage Discuss
Hemorrhagic Stroke. Team Members: Nawaf Aldarwish, Rawan Alqahtani, Talal AlTukhaim, Fatima Altassan.
 Hemorrhagic Stroke Objectives: Introduction Etiology Pathophysiology Clinical presentation Diagnosis and Imaging Treatment Team Members: Nawaf Aldarwish, Rawan Alqahtani, Talal AlTukhaim, Fatima Altassan.
Hemorrhagic Stroke Objectives: Introduction Etiology Pathophysiology Clinical presentation Diagnosis and Imaging Treatment Team Members: Nawaf Aldarwish, Rawan Alqahtani, Talal AlTukhaim, Fatima Altassan.
CLEAR III TRIAL : UPDATE ON SURGICAL MATTERS THAT MATTER
 CLEAR III TRIAL : UPDATE ON SURGICAL MATTERS THAT MATTER CLEAR Surgical Center Team July 2011 Trial Enrollment Status Updates Insert latest enrollment update chart from most recent CLEAR newsletter Imaging
CLEAR III TRIAL : UPDATE ON SURGICAL MATTERS THAT MATTER CLEAR Surgical Center Team July 2011 Trial Enrollment Status Updates Insert latest enrollment update chart from most recent CLEAR newsletter Imaging
Cerebral Aneurysms. U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Public Health Service National Institutes of Health
 Cerebral Aneurysms U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Public Health Service National Institutes of Health Cerebral Aneurysms What is a cerebral aneurysm? cerebral aneurysm (also known as an
Cerebral Aneurysms U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Public Health Service National Institutes of Health Cerebral Aneurysms What is a cerebral aneurysm? cerebral aneurysm (also known as an
7/22/2016. Navaz Karanjia, MD. FINANCIAL DISCLOSURE: none. UNLABELED/UNAPPROVED USE DISCLOSURE: none
 Navaz Karanjia, MD Director of Neurocritical Care Assistant Professor of Neurosciences, Neurosurgery, and Anesthesiology University of California-San Diego Health System Navaz Karanjia, MD FINANCIAL DISCLOSURE:
Navaz Karanjia, MD Director of Neurocritical Care Assistant Professor of Neurosciences, Neurosurgery, and Anesthesiology University of California-San Diego Health System Navaz Karanjia, MD FINANCIAL DISCLOSURE:
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,900 116,000 120M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,900 116,000 120M Open access books available International authors and editors Downloads Our
Stroke - Intracranial hemorrhage. Dr. Amitesh Aggarwal Associate Professor Department of Medicine
 Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Definition พ.ญ.ส ธ ดา เย นจ นทร. Epidemiology. Definition 5/25/2016. Seizures after stroke Can we predict? Poststroke seizure
 Seizures after stroke Can we predict? พ.ญ.ส ธ ดา เย นจ นทร PMK Epilepsy Annual Meeting 2016 Definition Poststroke seizure : single or multiple convulsive episode(s) after stroke and thought to be related
Seizures after stroke Can we predict? พ.ญ.ส ธ ดา เย นจ นทร PMK Epilepsy Annual Meeting 2016 Definition Poststroke seizure : single or multiple convulsive episode(s) after stroke and thought to be related
Shawke A. Soueidan, MD. Riverside Neurology & Sleep Specialists
 Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
MCHENRY WESTERN LAKE COUNTY EMS SYSTEM Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #7 Strokes
 MCHENRY WESTERN LAKE COUNTY EMS SYSTEM Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #7 Strokes Stroke is the third leading cause of death and the leading cause of adult disability in the
MCHENRY WESTERN LAKE COUNTY EMS SYSTEM Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #7 Strokes Stroke is the third leading cause of death and the leading cause of adult disability in the
Brain AVM with Accompanying Venous Aneurysm with Intracerebral and Intraventricular Hemorrhage
 Cronicon OPEN ACCESS EC PAEDIATRICS Case Report Brain AVM with Accompanying Venous Aneurysm with Intracerebral and Intraventricular Hemorrhage Dimitrios Panagopoulos* Neurosurgical Department, University
Cronicon OPEN ACCESS EC PAEDIATRICS Case Report Brain AVM with Accompanying Venous Aneurysm with Intracerebral and Intraventricular Hemorrhage Dimitrios Panagopoulos* Neurosurgical Department, University
What You Should Know About Cerebral Aneurysms
 American Society of Neuroradiology American Society of Interventional & Therapeutic Neuroradiology What You Should Know About Cerebral Aneurysms From the Cerebrovascular Imaging and Intervention Committee
American Society of Neuroradiology American Society of Interventional & Therapeutic Neuroradiology What You Should Know About Cerebral Aneurysms From the Cerebrovascular Imaging and Intervention Committee
NEUROSURGICAL EMERGENCY GUIDELINE DEVELOPMENT GROUP P3 NEURO CENTER OF NEUROSCIENCE RESEARCH AND SERVICE USM
 NEUROSURGICAL EMERGENCY GUIDELINE DEVELOPMENT GROUP P3 NEURO CENTER OF NEUROSCIENCE RESEARCH AND SERVICE USM Chairperson Professor Dr Zamzuri Idris Head of Department Members Associate Professor Dato Dr
NEUROSURGICAL EMERGENCY GUIDELINE DEVELOPMENT GROUP P3 NEURO CENTER OF NEUROSCIENCE RESEARCH AND SERVICE USM Chairperson Professor Dr Zamzuri Idris Head of Department Members Associate Professor Dato Dr
Hypertensive Urgency and Emergency. Definitions. Emergency or Urgency?
 Hypertensive Urgency and Emergency Joel Handler MD Kaiser Permanente Care Management Institute/ SCal Region Hypertension Lead Definitions Hypertensive Emergency: -Severe elevation in BP with evidence of
Hypertensive Urgency and Emergency Joel Handler MD Kaiser Permanente Care Management Institute/ SCal Region Hypertension Lead Definitions Hypertensive Emergency: -Severe elevation in BP with evidence of
lek Magdalena Puławska-Stalmach
 lek Magdalena Puławska-Stalmach tytuł pracy: Kliniczne i radiologiczne aspekty tętniaków wewnątrzczaszkowych a wybór metody leczenia Summary An aneurysm is a localized, abnormal distended lumen of the
lek Magdalena Puławska-Stalmach tytuł pracy: Kliniczne i radiologiczne aspekty tętniaków wewnątrzczaszkowych a wybór metody leczenia Summary An aneurysm is a localized, abnormal distended lumen of the
Summary of some of the landmark articles:
 Summary of some of the landmark articles: The significance of unruptured intracranial saccular aneurysms: Weibers et al Mayo clinic. 1987 1. 131 patients with 161 aneurysms were followed up at until death,
Summary of some of the landmark articles: The significance of unruptured intracranial saccular aneurysms: Weibers et al Mayo clinic. 1987 1. 131 patients with 161 aneurysms were followed up at until death,
Clinical Prediction of Symptomatic Vasospasm in Aneurysmal Subarachnoid Hemorrhage
 Clinical Prediction of Symptomatic Vasospasm in Aneurysmal Subarachnoid Hemorrhage Hubert Lee A thesis submitted to the Faculty of Graduate and Postdoctoral Studies in partial fulfillment of the requirements
Clinical Prediction of Symptomatic Vasospasm in Aneurysmal Subarachnoid Hemorrhage Hubert Lee A thesis submitted to the Faculty of Graduate and Postdoctoral Studies in partial fulfillment of the requirements
8th Annual NKY TBI Conference 3/28/2014
 Closed Head Injury: Headache to Herniation A N T H O N Y T. K R A M E R U N I V E R S I T Y O F C I N C I N N A T I B L U E A S H E M S T E C H N O L O G Y P R O G R A M Objectives Describe the pathological
Closed Head Injury: Headache to Herniation A N T H O N Y T. K R A M E R U N I V E R S I T Y O F C I N C I N N A T I B L U E A S H E M S T E C H N O L O G Y P R O G R A M Objectives Describe the pathological
Traumatic Brain Injury
 Traumatic Brain Injury Mark J. Harris M.D. Associate Professor University of Utah Salt Lake City USA Overview In US HI responsible for 33% trauma deaths. Closed HI 80% Missile / Penetrating HI 20% Glasgow
Traumatic Brain Injury Mark J. Harris M.D. Associate Professor University of Utah Salt Lake City USA Overview In US HI responsible for 33% trauma deaths. Closed HI 80% Missile / Penetrating HI 20% Glasgow
Recombinant Factor VIIa for Intracerebral Hemorrhage
 Recombinant Factor VIIa for Intracerebral Hemorrhage January 24, 2006 Justin Lee Pharmacy Resident University Health Network Outline 1. Introduction to patient case 2. Overview of intracerebral hemorrhage
Recombinant Factor VIIa for Intracerebral Hemorrhage January 24, 2006 Justin Lee Pharmacy Resident University Health Network Outline 1. Introduction to patient case 2. Overview of intracerebral hemorrhage
Hypertensive Haemorrhagic Stroke. Dr Philip Lam Thuon Mine
 Hypertensive Haemorrhagic Stroke Dr Philip Lam Thuon Mine Intracerebral Haemorrhage Primary ICH Spontaneous rupture of small vessels damaged by HBP Basal ganglia, thalamus, pons and cerebellum Amyloid
Hypertensive Haemorrhagic Stroke Dr Philip Lam Thuon Mine Intracerebral Haemorrhage Primary ICH Spontaneous rupture of small vessels damaged by HBP Basal ganglia, thalamus, pons and cerebellum Amyloid
Stroke: The First Critical Hour. Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP
 Stroke: The First Critical Hour Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP Disclosures We have no actual or potential conflicts of interest in relation to this presentation. Objectives Discuss
Stroke: The First Critical Hour Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP Disclosures We have no actual or potential conflicts of interest in relation to this presentation. Objectives Discuss
Head injuries. Severity of head injuries
 Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Guideline scope Subarachnoid haemorrhage caused by a ruptured aneurysm: diagnosis and management
 0 0 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Subarachnoid haemorrhage caused by a ruptured aneurysm: diagnosis and management The Department of Health and Social Care in England
0 0 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Subarachnoid haemorrhage caused by a ruptured aneurysm: diagnosis and management The Department of Health and Social Care in England
CENTRAL NERVOUS SYSTEM TRAUMA and Subarachnoid Hemorrhage. By: Shifaa AlQa qa
 CENTRAL NERVOUS SYSTEM TRAUMA and Subarachnoid Hemorrhage By: Shifaa AlQa qa Subarachnoid Hemorrhage Causes: Rupture of a saccular (berry) aneurysm Vascular malformation Trauma Hematologic disturbances
CENTRAL NERVOUS SYSTEM TRAUMA and Subarachnoid Hemorrhage By: Shifaa AlQa qa Subarachnoid Hemorrhage Causes: Rupture of a saccular (berry) aneurysm Vascular malformation Trauma Hematologic disturbances
Traumatic brain Injury- An open eye approach
 Traumatic brain Injury- An open eye approach Dr. Sunit Dr Sunit, Apollo children's hospital Blah blah Lots of head injury Lot of ill children Various methods of injury Various mechanisms of brain damage
Traumatic brain Injury- An open eye approach Dr. Sunit Dr Sunit, Apollo children's hospital Blah blah Lots of head injury Lot of ill children Various methods of injury Various mechanisms of brain damage
Pediatric Neurointervention: Vein of Galen Malformations
 Pediatric Neurointervention: Vein of Galen Malformations Johanna T. Fifi, M.D. Assistant Professor of Neurology, Neurosurgery, and Radiology Icahn School of Medicine at Mount Sinai November 9 th, 2014
Pediatric Neurointervention: Vein of Galen Malformations Johanna T. Fifi, M.D. Assistant Professor of Neurology, Neurosurgery, and Radiology Icahn School of Medicine at Mount Sinai November 9 th, 2014
Endovascular Treatment of Cerebral Arteriovenous Malformations. Bs. Nguyễn Ngọc Pi Doanh- Bs Đặng Ngọc Dũng Khoa Ngoại Thần Kinh
 Endovascular Treatment of Cerebral Arteriovenous Malformations Bs. Nguyễn Ngọc Pi Doanh- Bs Đặng Ngọc Dũng Khoa Ngoại Thần Kinh Stroke Vascular Malformations of the Brain Epidemiology: - Incidence: 0.1%,
Endovascular Treatment of Cerebral Arteriovenous Malformations Bs. Nguyễn Ngọc Pi Doanh- Bs Đặng Ngọc Dũng Khoa Ngoại Thần Kinh Stroke Vascular Malformations of the Brain Epidemiology: - Incidence: 0.1%,
SCCEP 2013 LLSA Course Article 10 AHA/ASA Guidelines for the Management of Spontaneous ICH
 SCCEP 2013 LLSA Course Article 10 AHA/ASA Guidelines for the Management of Spontaneous ICH Morgenstern LB, Hemphill JC. Stroke July 2010;41:2108-2129. Article: This article presents guidelines whose "aim
SCCEP 2013 LLSA Course Article 10 AHA/ASA Guidelines for the Management of Spontaneous ICH Morgenstern LB, Hemphill JC. Stroke July 2010;41:2108-2129. Article: This article presents guidelines whose "aim
excellence in care Procedure Neuroprotection For Review Aug 2015
 Neuro Projection HELI.CLI.14 Purpose This procedure outlines the management principles of patients being retrieved with traumatic brain injury (TBI), spontaneous intracranial haemorrhage (including subarachnoid
Neuro Projection HELI.CLI.14 Purpose This procedure outlines the management principles of patients being retrieved with traumatic brain injury (TBI), spontaneous intracranial haemorrhage (including subarachnoid
Management of Severe Traumatic Brain Injury
 Guideline for North Bristol Trust Management of Severe Traumatic Brain Injury This guideline describes the following: Initial assessment and management of the patient with head injury Indications for CT
Guideline for North Bristol Trust Management of Severe Traumatic Brain Injury This guideline describes the following: Initial assessment and management of the patient with head injury Indications for CT
Canadian Best Practice Recommendations for Stroke Care 3.6 Acute Subarachnoid Hemorrhage
 Last Updated: May 21, 2013 Canadian Best Practice Recommendations for Stroke Care Canadian Best Practice Recommendations for Stroke Care 2011-2013 Update Contents Search Strategy... 2 CSN Current Recommendations...Error!
Last Updated: May 21, 2013 Canadian Best Practice Recommendations for Stroke Care Canadian Best Practice Recommendations for Stroke Care 2011-2013 Update Contents Search Strategy... 2 CSN Current Recommendations...Error!
Controversies in Hemorrhagic Stroke Management. Sarah L. Livesay, DNP, RN, ACNP-BC, ACNS-BC Associate Professor Rush University
 Controversies in Hemorrhagic Stroke Management Sarah L. Livesay, DNP, RN, ACNP-BC, ACNS-BC Associate Professor Rush University Disclosures AHA/ASA Outline Blood pressure VTE Coagulopathy Early mobilization
Controversies in Hemorrhagic Stroke Management Sarah L. Livesay, DNP, RN, ACNP-BC, ACNS-BC Associate Professor Rush University Disclosures AHA/ASA Outline Blood pressure VTE Coagulopathy Early mobilization
Acute stroke imaging
 Acute stroke imaging Aims Imaging modalities and differences Why image acute stroke Clinical correlation to imaging appearance What is stroke Classic definition: acute focal injury to the central nervous
Acute stroke imaging Aims Imaging modalities and differences Why image acute stroke Clinical correlation to imaging appearance What is stroke Classic definition: acute focal injury to the central nervous
Management of the Endovascular Patient and Acute Emergencies in the Angio Suite
 Management of the Endovascular Patient and Acute Emergencies in the Angio Suite June 9, 2015 Bridget Cantrell, APN, CNP Endovascular Neurosurgery Advocate Medical Group No Disclosures The human brain is
Management of the Endovascular Patient and Acute Emergencies in the Angio Suite June 9, 2015 Bridget Cantrell, APN, CNP Endovascular Neurosurgery Advocate Medical Group No Disclosures The human brain is
This quiz is being published on behalf of the Education Committee of the SNACC.
 Shobana Rajan, M.D. Assistant professor Anesthesiology, Cleveland Clinic, Cleveland, Ohio Quiz Team; Suneeta Gollapudy M.D, Verghese Cherian M.D This quiz is being published on behalf of the Education
Shobana Rajan, M.D. Assistant professor Anesthesiology, Cleveland Clinic, Cleveland, Ohio Quiz Team; Suneeta Gollapudy M.D, Verghese Cherian M.D This quiz is being published on behalf of the Education
New Frontiers in Intracerebral Hemorrhage
 New Frontiers in Intracerebral Hemorrhage Ryan Hakimi, DO, MS Director, Neuro ICU Director, Inpatient Neurology Services Greenville Health System Clinical Associate Professor Department of Medicine (Neurology)
New Frontiers in Intracerebral Hemorrhage Ryan Hakimi, DO, MS Director, Neuro ICU Director, Inpatient Neurology Services Greenville Health System Clinical Associate Professor Department of Medicine (Neurology)
Subarachnoid Haemorrhage
 2011 Subarachnoid Haemorrhage Subarachnoid Haemorrhage This pamphlet will briefly describe what may happen to a person who has a subarachnoid haemorrhage (SAH). We would like to encourage you to read this
2011 Subarachnoid Haemorrhage Subarachnoid Haemorrhage This pamphlet will briefly describe what may happen to a person who has a subarachnoid haemorrhage (SAH). We would like to encourage you to read this
Traumatic Brain Injury:
 Traumatic Brain Injury: Changes in Management Across the Spectrum of Age and Time Omaha 2018 Trauma Symposium June 15, 2018 Gail T. Tominaga, M.D., F.A.C.S. Scripps Memorial Hospital La Jolla Outline Background
Traumatic Brain Injury: Changes in Management Across the Spectrum of Age and Time Omaha 2018 Trauma Symposium June 15, 2018 Gail T. Tominaga, M.D., F.A.C.S. Scripps Memorial Hospital La Jolla Outline Background
INCREASED INTRACRANIAL PRESSURE
 INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
INCREASED INTRACRANIAL PRESSURE Sheba Medical Center, Acute Medicine Department Irene Frantzis P-Year student SGUL 2013 Normal Values Normal intracranial volume: 1700 ml Volume of brain: 1200-1400 ml CSF:
Neurosurgical Management of Aneurysmal Subarachnoid Hemorrhage
 Neurosurgical Management of Aneurysmal Subarachnoid Hemorrhage PVHMC STROKE SYMPOSIUM 2018 10/27/18 Srinath Samudrala MD, FACS Epidemiology of Subarachnoid Hemorrhage (SAH) Less than 10% of all stroke
Neurosurgical Management of Aneurysmal Subarachnoid Hemorrhage PVHMC STROKE SYMPOSIUM 2018 10/27/18 Srinath Samudrala MD, FACS Epidemiology of Subarachnoid Hemorrhage (SAH) Less than 10% of all stroke
Introduction to Neurosurgical Subspecialties:
 Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
Introduction to Neurosurgical Subspecialties: Trauma and Critical Care Neurosurgery Brian L. Hoh, MD 1, Gregory J. Zipfel, MD 2 and Stacey Q. Wolfe, MD 3 1 University of Florida, 2 Washington University,
Acute stroke update 2016 innovations in managing ischemic and hemorrhagic disease
 Acute stroke update 2016 innovations in managing ischemic and hemorrhagic disease Christopher Koebbe, MD Endovascular Neurosurgeon Florida Spine Institute Director of Neurosciences Northside Hospital Overview
Acute stroke update 2016 innovations in managing ischemic and hemorrhagic disease Christopher Koebbe, MD Endovascular Neurosurgeon Florida Spine Institute Director of Neurosciences Northside Hospital Overview
Traumatic Brain Injury Pathways for Adult ED Patients Being Admitted to Trauma Service
 tic Brain Injury Pathways for Adult ED Patients Being Admitted to Service Revision Team Tyler W. Barrett, MD, MSCI Elizabeth S. Compton, NP Bradley M. Dennis, MD Oscar D. Guillamondegui, MD, MPH Michael
tic Brain Injury Pathways for Adult ED Patients Being Admitted to Service Revision Team Tyler W. Barrett, MD, MSCI Elizabeth S. Compton, NP Bradley M. Dennis, MD Oscar D. Guillamondegui, MD, MPH Michael
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for
 Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
Albumin In SubArachnoid Hemorrhage: The ALISAH Study
 Albumin In SubArachnoid Hemorrhage: The ALISAH Study Jose I Suarez, M.D. Professor of Neurology Neurointensivist and Vascular Neurologist Head Section of Neurocritical Care and Vascular Neurology Department
Albumin In SubArachnoid Hemorrhage: The ALISAH Study Jose I Suarez, M.D. Professor of Neurology Neurointensivist and Vascular Neurologist Head Section of Neurocritical Care and Vascular Neurology Department
Perioperative Management Of Extra-Ventricular Drains (EVD)
") Perioperative Management Of Extra-Ventricular Drains (EVD) Dr. Vijay Tarnal MBBS, FRCA Clinical Assistant Professor Division of Neuroanesthesiology Division of Head & Neck Anesthesiology Michigan Medicine
Perioperative Management Of Extra-Ventricular Drains (EVD) Dr. Vijay Tarnal MBBS, FRCA Clinical Assistant Professor Division of Neuroanesthesiology Division of Head & Neck Anesthesiology Michigan Medicine
Method Hannah Shotton
 #asah Method Hannah Shotton 2 Introduction SAH Rupturing aneurysm Poor outlook Intervention Secure the aneurysm: clipping or coiling Recommended 48 hours Regional Specialist NSC Conservative management
#asah Method Hannah Shotton 2 Introduction SAH Rupturing aneurysm Poor outlook Intervention Secure the aneurysm: clipping or coiling Recommended 48 hours Regional Specialist NSC Conservative management
Case 1. Case 5/30/2013. Traumatic Brain Injury : Review, Update, and Controversies
 Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
Case 1 Traumatic Brain Injury : Review, Update, and Controversies Shirley I. Stiver MD, PhD 32 year old male s/p high speed MVA Difficult extrication Intubated at scene Case BP 75 systolic / palp GCS 3
Neurosurgical decision making in structural lesions causing stroke. Dr Rakesh Ranjan MS, MCh, Dip NB (Neurosurgery)
") Neurosurgical decision making in structural lesions causing stroke Dr Rakesh Ranjan MS, MCh, Dip NB (Neurosurgery) Subarachnoid Hemorrhage Every year, an estimated 30,000 people in the United States experience
Neurosurgical decision making in structural lesions causing stroke Dr Rakesh Ranjan MS, MCh, Dip NB (Neurosurgery) Subarachnoid Hemorrhage Every year, an estimated 30,000 people in the United States experience
A few Neurosurgical Emergencies. Cathrin Parsch Lyell Mc Ewin Hospital SA Ambulance Service SAAS medstar Spring Seminar on Emergency Medicine 2015
 A few Neurosurgical Emergencies Cathrin Parsch Lyell Mc Ewin Hospital SA Ambulance Service SAAS medstar Spring Seminar on Emergency Medicine 2015 Outline Neuroanatomy and physiology (85 slides ) Raised
A few Neurosurgical Emergencies Cathrin Parsch Lyell Mc Ewin Hospital SA Ambulance Service SAAS medstar Spring Seminar on Emergency Medicine 2015 Outline Neuroanatomy and physiology (85 slides ) Raised
ESCMID Online Lecture Library. by author
 Neurologische Klinik und Poliklinik Prof. Dr. M. Dieterich Treatment of community acquired meningitis - ICU and neurologic perspective Izmir 2010 INFECTIOUS FOCI OF COMMUNITY ACQUIRED MENINGITIS The cause
Neurologische Klinik und Poliklinik Prof. Dr. M. Dieterich Treatment of community acquired meningitis - ICU and neurologic perspective Izmir 2010 INFECTIOUS FOCI OF COMMUNITY ACQUIRED MENINGITIS The cause
Hypertensives Emergency and Urgency
 Hypertensives Emergency and Urgency Budi Yuli Setianto Cardiology Divisision Department of Internal Medicine Faculty of Medicine UGM Sardjito Hospital Yogyakarta Background USA: Hypertension is 30% of
Hypertensives Emergency and Urgency Budi Yuli Setianto Cardiology Divisision Department of Internal Medicine Faculty of Medicine UGM Sardjito Hospital Yogyakarta Background USA: Hypertension is 30% of
Guidelines for the management of a patient with a subarachnoid haemorrhage
 Guidelines for the management of a patient with a subarachnoid haemorrhage Item Type Report Authors Health Service Executive (HSE) Citation Health Service Executive. Guidelines for the management of a
Guidelines for the management of a patient with a subarachnoid haemorrhage Item Type Report Authors Health Service Executive (HSE) Citation Health Service Executive. Guidelines for the management of a
Neuroprotective Effects for TBI. Craig Williamson, MD
 Neuroprotective Effects for TBI Craig Williamson, MD Neuroprotection in Traumatic Brain Injury Craig Williamson Clinical Assistant Professor Neurocritical Care Fellowship Director Disclosures I will discuss
Neuroprotective Effects for TBI Craig Williamson, MD Neuroprotection in Traumatic Brain Injury Craig Williamson Clinical Assistant Professor Neurocritical Care Fellowship Director Disclosures I will discuss
TREATMENT OF INTRACRANIAL ANEURYSMS
 TREATMENT OF INTRACRANIAL ANEURYSMS Presented by: Dr Nilesh S. Kurwale Introduction Incidence of aneurysm difficult to estimate Prevalence 0.2-7.9 % Half the aneurysms ruptures 2% present during childhood
TREATMENT OF INTRACRANIAL ANEURYSMS Presented by: Dr Nilesh S. Kurwale Introduction Incidence of aneurysm difficult to estimate Prevalence 0.2-7.9 % Half the aneurysms ruptures 2% present during childhood
UPSTATE Comprehensive Stroke Center. Neurosurgical Interventions Satish Krishnamurthy MD, MCh
 UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic
UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic