Raw and Quantitative EEG for Identification of Ischemia
|
|
|
- Darlene Simon
- 6 years ago
- Views:
Transcription
1 Raw and Quantitative EEG for Identification of Ischemia Susan T. Herman, MD Assistant Professor of Neurology Beth Israel Deaconess Medical Center Harvard Medical School Boston, MA
2 Disclosures None relevant to this presentation Scientific Advisory Board Eisai Inc. Biotie, Inc. Research UCB Pharma Acorda Therapeutics Epilepsy Therapy Development Project Sage Pharmaceuticals NeuroPace, Inc. Pfizer
3 Detection of Ischemia During and after vascular neurosurgical or interventional neuroradiology procedures After subarachnoid hemorrhage In patients with hemodynamic lesions and borderline flow In other patients at risk for in-hospital acute ischemia Hirsch LJ. J Clin Neurophysiol 2004;21: Herman ST et al. J Clin Neurophysiol 2015; 32:
4 Cerebral Ischemia EEG changes occur within 5 minutes of acute ischemia Superior to current imaging techniques Reversible stage ml/100g/min EEG change Reversibility Normal No injury Loss of beta Reversible Theta slowing Reversible Delta slowing Reversible < 8-10 Suppression Irreversible Astrup et al. Stroke 1981;12: Jordan KG. J Clin Neurophysiol 2004;21:
5 EEG and Cerebral Ischemia Intraoperative monitoring during carotid artery occlusion EEG can detect important changes in CBF Hemispheric EEG slowing Correlates with moderate to severe reductions in CBF on stable Xenon CT Mean dominant EEG frequency 6.5 Hz correlated with CBF 33 to 39 ml/100 g/min 7.8 Hz correlated with CBF 47 ml/100 g/min Vespa et al., EEG Clin Neurophys 1997;103: Sundt et al., Mayo Clin Proc 1981;56:
6 Carotid Endarterectomy: Baseline
7 Carotid Endarterectomy: Intra-op
8 Carotid Endarterectomy: Post-CEA
9 Carotid Endarterectomy: Trends

10 Carotid Endarterectomy: Alpha-Delta

11 Beta Asymmetry

12 Beta Asymmetry

13 Carotid Endarterectomy: Ischemia

14 Carotid Endarterectomy: Ischemia

15 Carotid Endarterectomy, Ischemia
16 Delayed Cerebral Ischemia (DCI) New focal or global neurological deficit and/or new infarction after SAH (exclude rebleeding / hydrocephalus) Days 3 14 after SAH Major cause of cerebral ischemia and morbidity Occurs in 19-46% of patients Infarct in ~ 60% Subclinical in 25%, associated with poor outcome Risk factors Poor Hunt-Hess grade Large amounts of cisternal blood 1. Charpentier et al. Stroke 1999;30: Claassen et al. Stroke 2001;32: Qureshi et al. Crit Care Med 2000;28:
17 Subarachnoid Hemorrhage Pathophysiology Vasospasm of large vessels Microembolism Vasospasm of peripheral arteries and arterioles (as opposed to proximal large vessels) Cortical spreading ischemia DCI is treatable if diagnosed during reversible phase Hypertension Volume expansion Intraarterial nicardipine, papaverine Angioplasty Long window for intervention (2-6 hours) Connolly ES et al. Stroke 2012;43:
18 Monitoring for Vasospasm Clinical examination Patient often sedated, uncooperative Daily Transcranial Dopplers (TCDs) Snapshot in time Only monitors for vasospasm, not other causes of ischemia Mediocre sensitivity and specificity Conventional angiography Performed if above suggestive of ischemia Invasive Brain imaging (CT, CTA, and MRI) Performed if above suggestive of ischemia Diringer MN et al. Neurocrit Care 2011;15:
19 Labar: EEG Monitoring in SAH 21 patients with aneurysmal SAH 2 channel EEG (Cz-T3, Cz-T4) Automatic artifact detection methods (excess of the dynamic range of amplifiers, zero-derivative signals, and excessive 60 Hz interference) Compressed spectral analysis (1-30 Hz) Trend analysis Sum of the power (total power), 1-30 Hz Centroid of the frequency, 1-30 Hz Power Hz / power 1-7 Hz ('alpha ratio ) Power Hz / power 1-30 Hz ('percent delta') Labar DR et al., Electroencephalogr Clin Neurophysiol 1991;78:
20 Labar: EEG Monitoring in SAH EEG Finding EEG Parameter Change in power Change in frequency Focal CT lesions (N) All ischemic events (N) Trend analysis 100% (5) 91% (11) Compressed spectral array 33% (6) 44% (18) Centroid 60% (5) 55% (11) Relative alpha 60% (5) 64% (11) Percent delta 80% (5) 45% (11) Compressed spectral array 17% (6) 39% (18) Labar DR et al., Electroencephalogr Clin Neurophysiol 1991;78:
21 Vespa: EEG Monitoring in SAH 32 patients with aneurysmal SAH Reduction in variability of theta-alpha content (6-14Hz) Ratio of power in 6-14Hz band relative to power in 120Hz band Sensitivity 100% Specificity 50% (increased ICP, recurrent hemorrhage, hydrocephalus, embolic stroke during angio) Preceded clinical onset of vasospasm and elevated TCD velocities in 70% Mean 2.9 days Vespa et al., EEG Clin Neurophys 1997;103:
22 Alpha Variability 1 Excellent 2 Good 3 Fair 4 Poor µv/hz
23 Vespa: EEG Monitoring in SAH Vespa et al., EEG Clin Neurophys 1997;103:

24 Bilateral frontal ischemia - decrease in alpha variability Clinical deterioration Disconnected 2 hrs for angiogram: sedation / intubation Improvement in alpha variability after angio
25
26
27
28 Claassen: EEG Monitoring in SAH 34 of 78 consecutive Hunt-Hess grade 4 or 5 SAH patients Continuous EEG post-op day 2 to post-sah day artifact-free, 1 min EEG-clips after alerting stimulus 10 clips on monitoring day 1 (baseline) 10 clips on days 4-6 (follow-up) In DCI patients, follow-up clips after the onset of deterioration and before infarction Claassen J et al., Clin Neurophysiol 2004;115:
29 Claassen: EEG Monitoring in SAH Nine of 34 patients (26%) developed DCI Alpha/delta ratio (alpha power/delta power; ADR) demonstrated the strongest association with DCI Median decrease of ADR in DCI was 24% Median increase of 3% without DCI (p<0.0001) Clinically useful cut-offs 6 consecutive recordings with >10% decrease in ADR from baseline (sensitivity 100%, specificity 76%) Any single measurement with a >50% decrease (sensitivity 89%, specificity 84%) Claassen J et al., Clin Neurophysiol 2004;115:

30 Claassen et al., J Clin Neurophys 2005;22:92-98
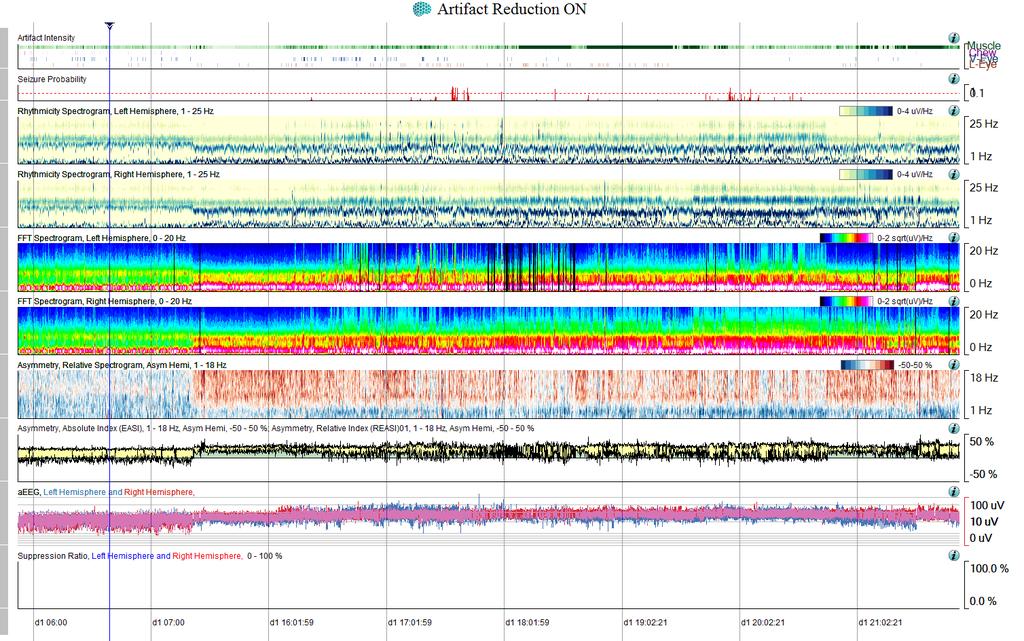
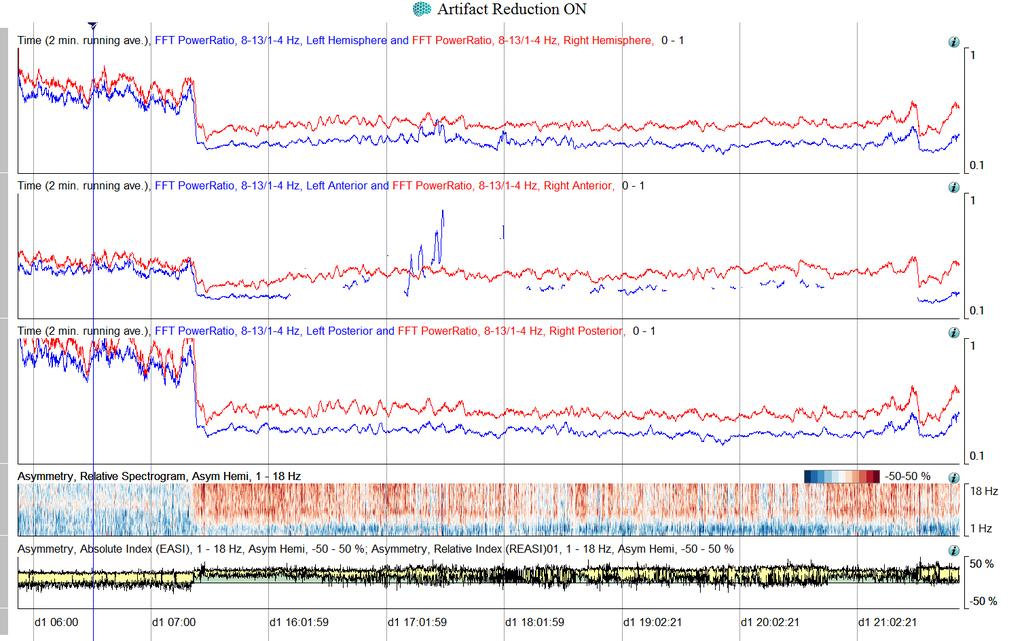
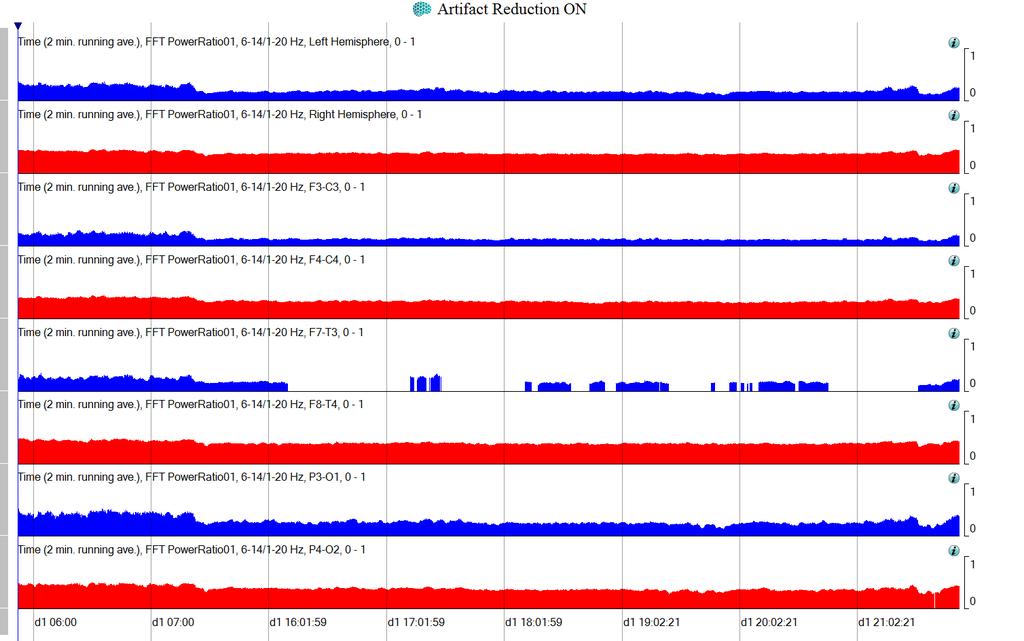
31 SAH: Alpha-Delta Ratio F F T _ P owe rr a tio / / 1-4 F 3 -C 3 F3-C3 F F T _ P owe rr a tio / / 1-4 F 4 -C 4 F4-C4 F F T _ P owe rr a tio / / 1-4 C 3 -T 3 _ a v g C3-T3 F F T _ P owe rr a tio / / 1-4 C 4 -T 4 _ a v g C4-T4 F F T _ P owe rr a tio / / 1-4 P 3 -O 1 P3-O1 F F T _ P owe rr a tio / / 1-4 P 4 -O 2 P4-O2 F F T _ P owe rr a tio / / 1-4 L e ft_ a v g Left F F T _ P owe rr a tio / / 1-4 R ig h t_ a v g Right 12:30 13:30 14:30
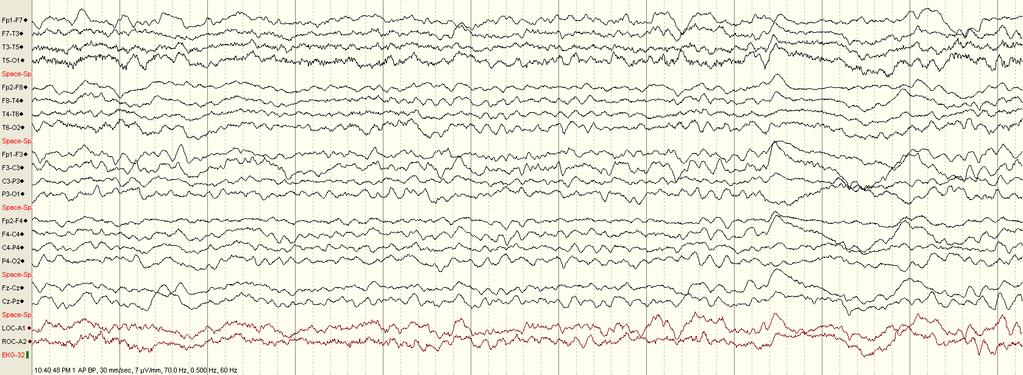
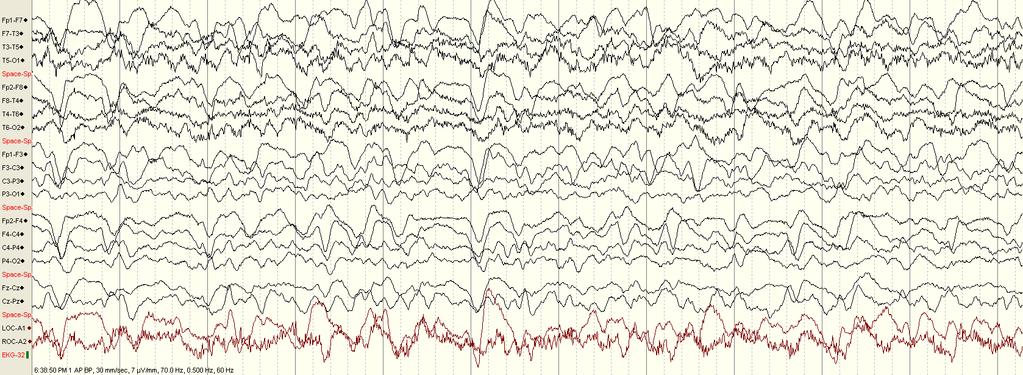
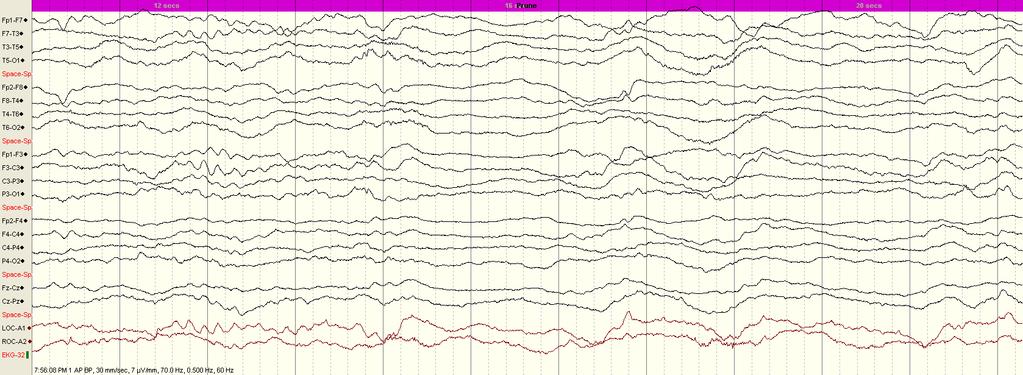
32 FP1-F7 F7-T3 T3-T5 T5-O1 FP2-F8 F8-T4 T4-T6 T6-O2 FP1-F3 F3-C3 C3-P3 P3-O1 FP2-F4 F4-C4 C4-P4 P4-O2 Fz-Cz F3-T3 F4-T4 C3-T3 C4-T4 EKG
33 FP1-F7 F7-T3 T3-T5 T5-O1 FP2-F8 F8-T4 T4-T6 T6-O2 FP1-F3 F3-C3 C3-P3 P3-O1 FP2-F4 F4-C4 C4-P4 P4-O2 Fz-Cz F3-T3 F4-T4 C3-T3 C4-T4 EKG
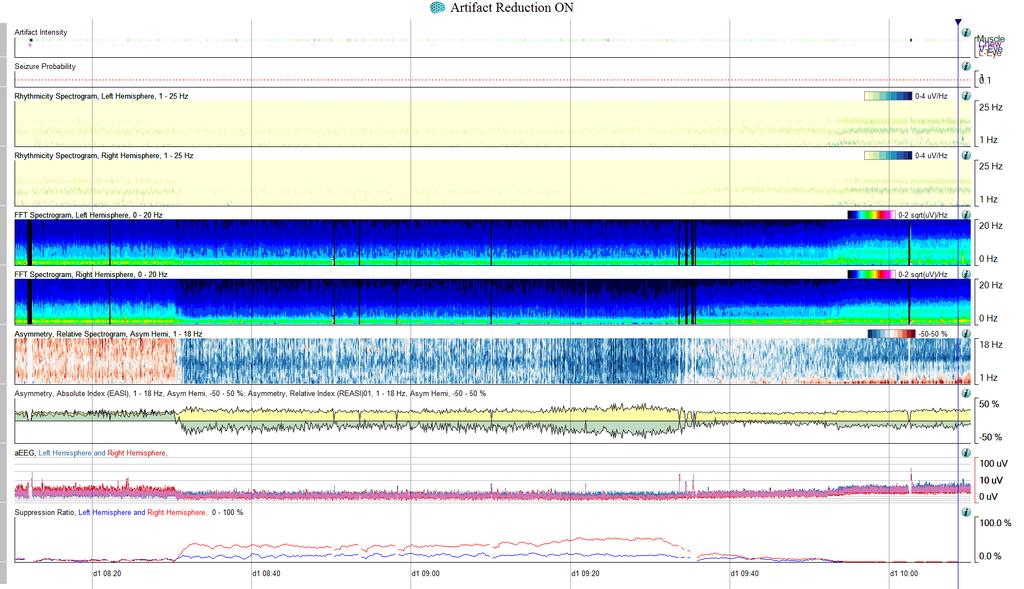
34 Comprehensive Panel
35 Alpha-Delta Ratio
36 Alpha Variability

37 FP1-F7 F7-T3 T3-T5 T5-O1 FP2-F8 F8-T4 T4-T6 T6-O2 FP1-F3 F3-C3 C3-P3 P3-O1 FP2-F4 F4-C4 C4-P4 P4-O2 Fz-Cz F3-T3 F4-T4 C3-T3 C4-T4 EKG
38 FP1-F7 F7-T3 T3-T5 T5-O1 FP2-F8 F8-T4 T4-T6 T6-O2 FP1-F3 F3-C3 C3-P3 P3-O1 FP2-F4 F4-C4 C4-P4 P4-O2 Fz-Cz F3-T3 F4-T4 C3-T3 C4-T4 EKG
39 FP1-F7 F7-T3 T3-T5 T5-O1 FP2-F8 F8-T4 T4-T6 T6-O2 FP1-F3 F3-C3 C3-P3 P3-O1 FP2-F4 F4-C4 C4-P4 P4-O2 Fz-Cz F3-T3 F4-T4 C3-T3 C4-T4 EKG
40 Case 1 56 year old man with SAH Hunt-Hess grade 3 Fisher grade 3 GCS 10 Angiography revealed a 7 mm left AComm aneurysm Aneurysm was clipped uneventfully
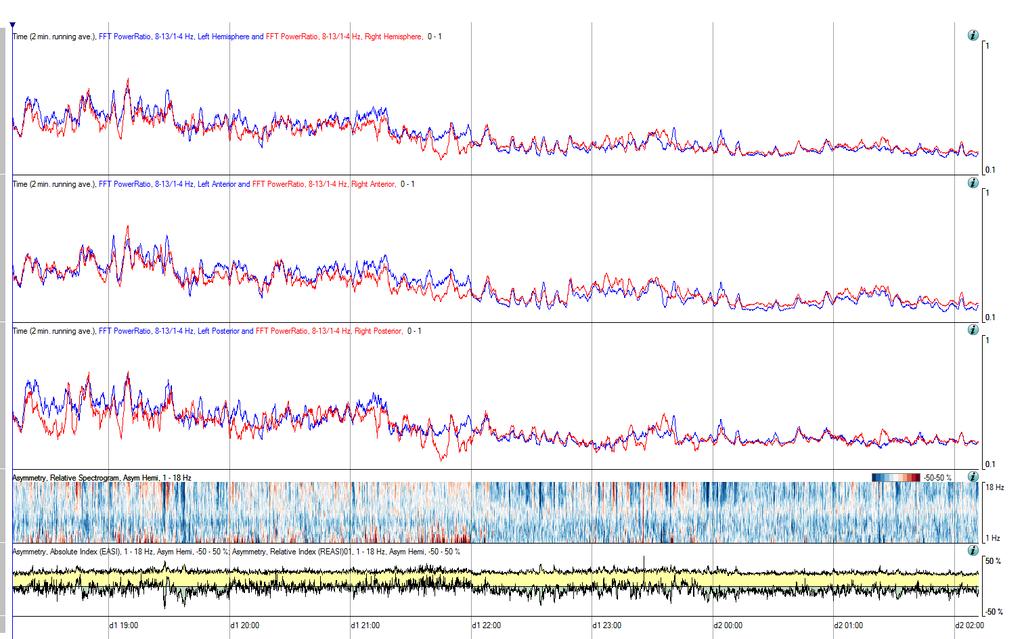
41 Alpha-Delta: 8 hours
42 Raw EEG: 30 minutes
43 Raw EEG: 6 hours

44 Alpha Variability: 8 hours
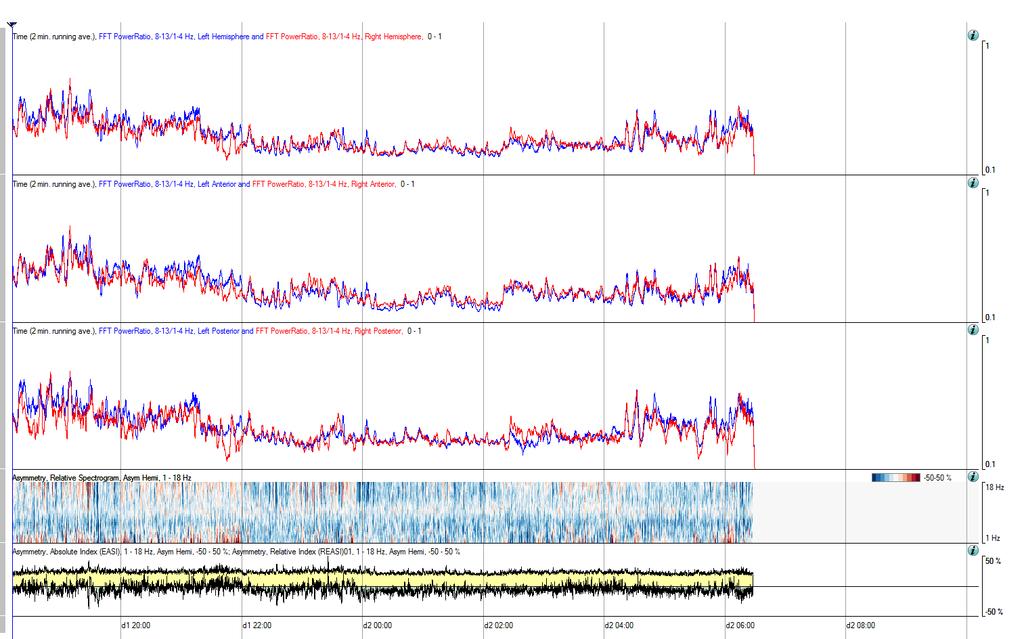
45 Alpha-Delta: 16 hours

46 Alpha Variability: 16 hours
47 Raw EEG: 12 hours
48 Case 2 62-year-old woman with SAH Hunt-Hess grade 2 Fisher grade 3 GCS 14 Angiography revealed a 8 mm right internal carotid supraclinoid aneurysm and a 4 mm left anterior communicating artery/anterior cerebral artery junction aneurysm Both aneurysms were clipped uneventfully
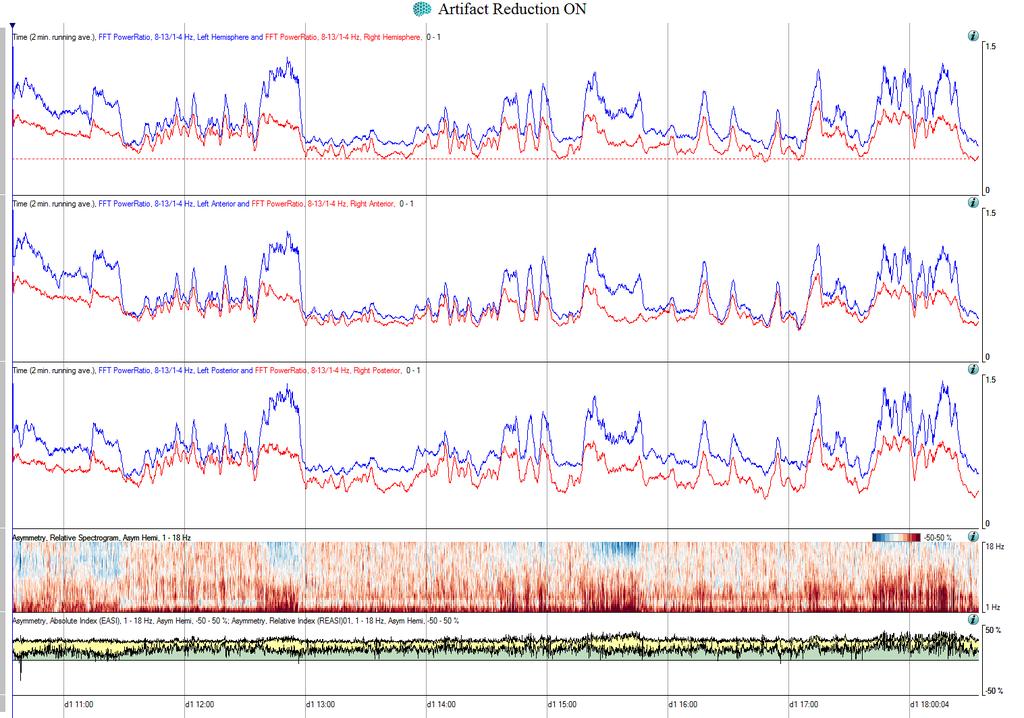
49 Alpha-Delta: 8 hours
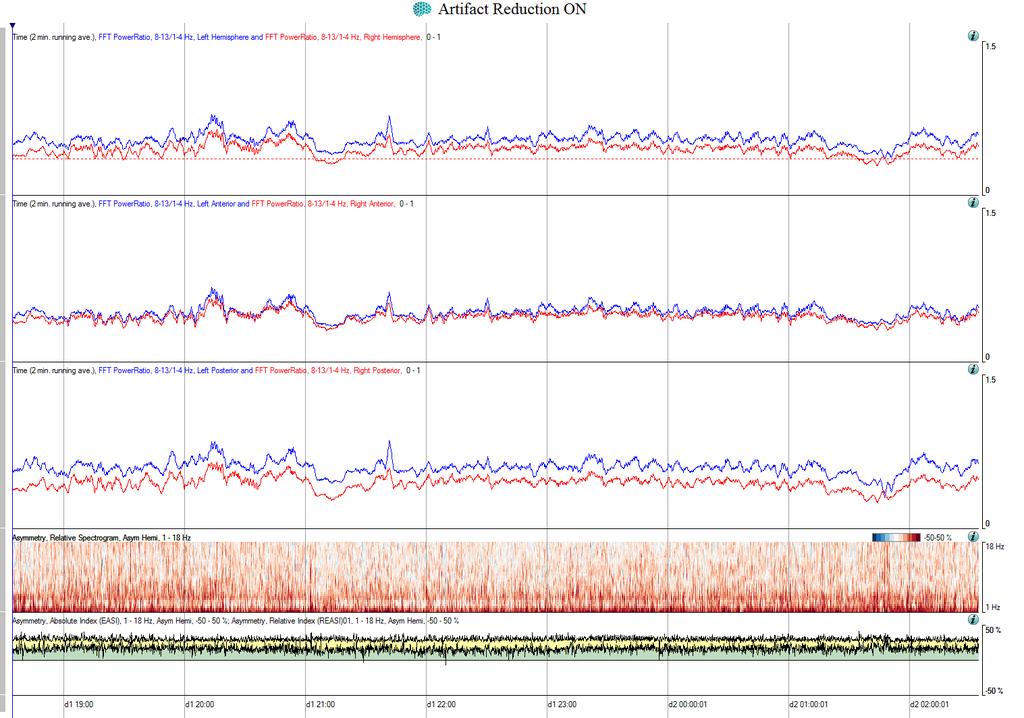
50 Alpha-Delta: 8 hours

51 Alpha Delta: 8 hours, day 4
52 QEEG: Intracortical EEG Improved signal: noise and reduced artifact 5 patients with poor grade SAH (Hunt-Hess grade 4 or 5) 8 contact depth electrode (2.2 mm spacing) QEEG: average over 4-6 hrs baseline vs. prior to angio Alpha/delta ratio (ADR, 8 13 Hz/1 4 Hz) Mean amplitude Suppression percent (percent below 5 uv) Total power (TP, 0 23 Hz) Superior to alpha-delta ratio of scalp EEG Stuart RM et al. Neurocrit Care 2010;13:
53 QEEG: Intracortical EEG 3/5 SAH patients had vasospasm on follow-up angio Mean ICE ADRs prior to angiography Decreased by 42% for those with vasospasm Decreased by 17% for those without vasospasm Dropped by at least 25% for >4 h in all patients with vasospasm 1 3 days before angiographic confirmation of vasospasm No false negatives Surface EEG was limited by significant artifact and poor signal quality, despite application of automated artifact rejection Stuart RM et al. Neurocrit Care 2010;13:
54 Systematic Review 8 publications included from 760 citations All single-center case series, half retrospective All affected by high risk of bias related to patient selection 50% high risk of bias for EEG methodology Kondziella D et al. Neurocrit Care 2015; 22:
55 Systematic Review Reference standard: CT, DSA, and TCD (120 to 140 cm/min) in most but not all studies 4 studies: DCI based on clinical diagnosis, presence of radiological vasospasm or increased TCD flow velocities was supportive but not mandatory Conclusion CEEG monitoring after SAH may predict clinically symptomatic episodes of DCI many hours in advance Unknown if more aggressive treatment alters outcome Kondziella D et al. Neurocrit Care 2015; 22:
56 QEEG for DCI: Confounders Sedation and other medications Increased intracranial pressure Reduced global cerebral perfusion pressure Metabolic changes Hydrocephalus Rebleeding Focal edema Artifacts Large variety of DCI definitions New definition: infarct and functional outcome
57 Summary: CEEG after SAH EEG and QEEG trends on ceeg (performed on days 2 10) correlate with delayed cerebral ischemia QEEG trends designed to detect increased slow and loss of fast frequencies May detect ischemia prior to neurological exam and other diagnostic tests Sensitivity up to 90% Specificity 75% Optimal duration not defined Most studies examined poor grade patients No interventional trials using EEG as detection method Claassen et al. Intensive Care Med 2013;39:
58 Ischemic Stroke 91 patients with acute ischemic stroke 33 (36%) initially had normal CT scans 16 (48%) showed lateralized EEG abnormalities All 16 showed cortical infarctions on follow-up CT scans corresponding to the EEG findings 58 cortical infarctions Lateralized EEG abnormalities 80% of MCA 86% of watershed 12 lacunar infarctions with negative initial CT scans had normal acute EEGs Macdonell RA et al., Arch Neurol 1988;45:
59 Prediction of Malignant Course RAWOD Regional Attenuation WithOut Delta Patients with large acute ischemic stroke Less likely to benefit from thrombolysis Likely to develop cerebral edema Schneider & Jordan. Am J Electroneurodiagnostic Technol 2005;45:
60 RAWOD

61 RAWOD: QEEG
62 Prediction of Malignant Course 25 patients with large (>50%) middle cerebral artery (MCA) infarction 12 malignant, 13 benign course EEG within 24 hours, visual analysis Predictors Benign course: absence of delta activity, presence of theta and fast beta frequencies Malignant course: diffuse slowing (< 8 Hz), slow delta activity (< 1 Hz), loss of fast beta in the ischemic hemisphere Burghaus et al. Clin Neurol Neurosurg 2007;109:45-49
63 Asymmetry Indices Brain Symmetry Index (BSI) Single numerical value: sums absolute values of the differences at each homologous electrode pair for all frequencies 0: perfect symmetry 1: maximal aymmetry Correlates with clinical stroke scales Has been used to follow effect of tpa
64 BSI for Carotid Endarterectomy van Putten MJ, et al. Clin Neurophysiol 2004;115:1189
65 BSI and NIH Stroke Scale van Putten MJ, et al. Stroke 2004;35:
66 BSI: Response to tpa de Vos CC et al. J Clin Neurophysiol 2008;25:77-82
67 Ischemic Stroke: Confounders Spontaneous or provoked state changes Variations in physiological parameters (BP, ICP, cerebral perfusion pressure) Sedative medications Artifacts (EMG, electrode)
68 Ischemic Stroke: Caveats Differential diagnosis of lateralized slowing / loss fast Focal postictal states Hemiplegic migraine Cortical infarctions < 3 cm may not show EEG changes Lacunar infarcts often show normal EEG Medial lesions may produce bilateral rather than focal EEG changes Almost no data on continuous EEG monitoring to detect worsening ischemia in real time
69 Conclusions EEG is a useful monitoring tool for cerebral ischemia Large vessel territorial ischemia Good sensitivity, moderate specificity Retrospective studies have demonstrated helpful QEEG methods in CEA, SAH Limited by Lack of specificity (hydrocephalus, sedatives, etc) Artifacts No prospective real-time analysis Need prospective randomized blinded trials
Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage. Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA
 Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA The traditional view: asah is a bad disease Pre-hospital mortality
Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA The traditional view: asah is a bad disease Pre-hospital mortality
Intra-arterial nimodipine for the treatment of vasospasm due to aneurysmal subarachnoid hemorrhage
 Romanian Neurosurgery (2016) XXX 4: 461 466 461 DOI: 10.1515/romneu-2016-0074 Intra-arterial nimodipine for the treatment of vasospasm due to aneurysmal subarachnoid hemorrhage A. Chiriac, Georgiana Ion*,
Romanian Neurosurgery (2016) XXX 4: 461 466 461 DOI: 10.1515/romneu-2016-0074 Intra-arterial nimodipine for the treatment of vasospasm due to aneurysmal subarachnoid hemorrhage A. Chiriac, Georgiana Ion*,
Assessment of Vasospasm and Delayed Cerebral Ischemia after Subarachnoid Hemorrhage: Current concepts and Value of CT Perfusion and CT Angiography
 Assessment of Vasospasm and Delayed Cerebral Ischemia after Subarachnoid Hemorrhage: Current concepts and Value of CT Perfusion and CT Angiography Poster No.: C-2563 Congress: ECR 2012 Type: Educational
Assessment of Vasospasm and Delayed Cerebral Ischemia after Subarachnoid Hemorrhage: Current concepts and Value of CT Perfusion and CT Angiography Poster No.: C-2563 Congress: ECR 2012 Type: Educational
EEG in the ICU: Part I
 EEG in the ICU: Part I Teneille E. Gofton July 2012 Objectives To outline the importance of EEG monitoring in the ICU To briefly review the neurophysiological basis of EEG To introduce formal EEG and subhairline
EEG in the ICU: Part I Teneille E. Gofton July 2012 Objectives To outline the importance of EEG monitoring in the ICU To briefly review the neurophysiological basis of EEG To introduce formal EEG and subhairline
7/18/2018. Cerebral Vasospasm: Current and Emerging Therapies. Disclosures. Objectives
 Cerebral : Current and Emerging Therapies Chad W. Washington MS, MD, MPHS Assistant Professor Department of Neurosurgery Disclosures None Objectives Brief Overview How we got here Review of Trials Meta-analysis
Cerebral : Current and Emerging Therapies Chad W. Washington MS, MD, MPHS Assistant Professor Department of Neurosurgery Disclosures None Objectives Brief Overview How we got here Review of Trials Meta-analysis
State of the Art Multimodal Monitoring
 State of the Art Multimodal Monitoring Baptist Neurological Institute Mohamad Chmayssani, MD Disclosures I have no financial relationships to disclose with makers of the products here discussed. Outline
State of the Art Multimodal Monitoring Baptist Neurological Institute Mohamad Chmayssani, MD Disclosures I have no financial relationships to disclose with makers of the products here discussed. Outline
TCD AND VASOSPASM SAH
 CURRENT TREATMENT FOR CEREBRAL ANEURYSMS TCD AND VASOSPASM SAH Michigan Sonographers Society 2 Nd Annual Fall Vascular Conference Larry N. Raber RVT-RDMS Clinical Manager General Ultrasound-Neurovascular
CURRENT TREATMENT FOR CEREBRAL ANEURYSMS TCD AND VASOSPASM SAH Michigan Sonographers Society 2 Nd Annual Fall Vascular Conference Larry N. Raber RVT-RDMS Clinical Manager General Ultrasound-Neurovascular
Current State of the Art
 SAH Current State of the Art Thomas C. Steineke, M.D., Ph.D. Director of Neurovascular Surgery NJ Neuroscience Institute JFK Medical Center Introduction Signs and symptoms of a problem What are aneurysms
SAH Current State of the Art Thomas C. Steineke, M.D., Ph.D. Director of Neurovascular Surgery NJ Neuroscience Institute JFK Medical Center Introduction Signs and symptoms of a problem What are aneurysms
Definition พ.ญ.ส ธ ดา เย นจ นทร. Epidemiology. Definition 5/25/2016. Seizures after stroke Can we predict? Poststroke seizure
 Seizures after stroke Can we predict? พ.ญ.ส ธ ดา เย นจ นทร PMK Epilepsy Annual Meeting 2016 Definition Poststroke seizure : single or multiple convulsive episode(s) after stroke and thought to be related
Seizures after stroke Can we predict? พ.ญ.ส ธ ดา เย นจ นทร PMK Epilepsy Annual Meeting 2016 Definition Poststroke seizure : single or multiple convulsive episode(s) after stroke and thought to be related
SAH READMISSIONS TO NCCU
 SAH READMISSIONS TO NCCU Are they preventable? João Amaral Rebecca Gorf Critical Care Outreach Team - NHNN 2015 Total admissions to NCCU =862 Total SAH admitted to NCCU= 104 (93e) (12.0%) Total SAH readmissions=
SAH READMISSIONS TO NCCU Are they preventable? João Amaral Rebecca Gorf Critical Care Outreach Team - NHNN 2015 Total admissions to NCCU =862 Total SAH admitted to NCCU= 104 (93e) (12.0%) Total SAH readmissions=
Acute stroke imaging
 Acute stroke imaging Aims Imaging modalities and differences Why image acute stroke Clinical correlation to imaging appearance What is stroke Classic definition: acute focal injury to the central nervous
Acute stroke imaging Aims Imaging modalities and differences Why image acute stroke Clinical correlation to imaging appearance What is stroke Classic definition: acute focal injury to the central nervous
THE EFFICACY AND SAFETY OF CILOSTAZOL IN SUBARACHNOID HEMORRHAGE. A META- ANALYSIS OF RANDOMIZED AND NON RANDOMIZED STUDIES DR. MUHAMMAD F.
 THE EFFICACY AND SAFETY OF CILOSTAZOL IN SUBARACHNOID HEMORRHAGE. A META- ANALYSIS OF RANDOMIZED AND NON RANDOMIZED STUDIES DR. MUHAMMAD F. ISHFAQ ZEENAT QURESHI STROKE INSTITUTE AND UNIVERSITY OF TENNESSEE,
THE EFFICACY AND SAFETY OF CILOSTAZOL IN SUBARACHNOID HEMORRHAGE. A META- ANALYSIS OF RANDOMIZED AND NON RANDOMIZED STUDIES DR. MUHAMMAD F. ISHFAQ ZEENAT QURESHI STROKE INSTITUTE AND UNIVERSITY OF TENNESSEE,
Stroke: The First Critical Hour. Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP
 Stroke: The First Critical Hour Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP Disclosures We have no actual or potential conflicts of interest in relation to this presentation. Objectives Discuss
Stroke: The First Critical Hour Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP Disclosures We have no actual or potential conflicts of interest in relation to this presentation. Objectives Discuss
Aneurysmal Subarachnoid Hemorrhage Presentation and Complications
 Aneurysmal Subarachnoid Hemorrhage Presentation and Complications Sherry H-Y. Chou MD MMSc FNCS Department of Critical Care Medicine, Neurology and Neurosurgery University of Pittsburgh School of Medicine
Aneurysmal Subarachnoid Hemorrhage Presentation and Complications Sherry H-Y. Chou MD MMSc FNCS Department of Critical Care Medicine, Neurology and Neurosurgery University of Pittsburgh School of Medicine
Disclosures. CREST Trial: Summary. Lecture Outline 4/16/2015. Cervical Atherosclerotic Disease
 Disclosures Your Patient Has Carotid Bulb Stenosis and a Tandem Intracranial Stenosis: How Do SAMMPRIS and Other Evidence Inform Your Treatment? UCSF Vascular Symposium 2015 Steven W. Hetts, MD Associate
Disclosures Your Patient Has Carotid Bulb Stenosis and a Tandem Intracranial Stenosis: How Do SAMMPRIS and Other Evidence Inform Your Treatment? UCSF Vascular Symposium 2015 Steven W. Hetts, MD Associate
ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS. Justin Nolte, MD Assistant Profession Marshall University School of Medicine
 ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS Justin Nolte, MD Assistant Profession Marshall University School of Medicine History of Presenting Illness 64 yo wf with PMHx of COPD, HTN, HLP who was in
ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS Justin Nolte, MD Assistant Profession Marshall University School of Medicine History of Presenting Illness 64 yo wf with PMHx of COPD, HTN, HLP who was in
Occurrence and Risk Factors for Post-traumatic Epilepsy in Civilian Poulations December 2, 2012
 Occurrence and Risk Factors for Post-traumatic Epilepsy in Civilian Poulations December 2, 2012 Dale C Hesdorffer, PhD GH Sergievsky Center Columbia University American Epilepsy Society Annual Meeting
Occurrence and Risk Factors for Post-traumatic Epilepsy in Civilian Poulations December 2, 2012 Dale C Hesdorffer, PhD GH Sergievsky Center Columbia University American Epilepsy Society Annual Meeting
Neurosurgical decision making in structural lesions causing stroke. Dr Rakesh Ranjan MS, MCh, Dip NB (Neurosurgery)
") Neurosurgical decision making in structural lesions causing stroke Dr Rakesh Ranjan MS, MCh, Dip NB (Neurosurgery) Subarachnoid Hemorrhage Every year, an estimated 30,000 people in the United States experience
Neurosurgical decision making in structural lesions causing stroke Dr Rakesh Ranjan MS, MCh, Dip NB (Neurosurgery) Subarachnoid Hemorrhage Every year, an estimated 30,000 people in the United States experience
Quantitative continuous EEG for detecting delayed cerebral ischemia in patients with poor-grade subarachnoid hemorrhage
 Clinical Neurophysiology 115 (2004) 2699 2710 www.elsevier.com/locate/clinph Quantitative continuous EEG for detecting delayed cerebral ischemia in patients with poor-grade subarachnoid hemorrhage Jan
Clinical Neurophysiology 115 (2004) 2699 2710 www.elsevier.com/locate/clinph Quantitative continuous EEG for detecting delayed cerebral ischemia in patients with poor-grade subarachnoid hemorrhage Jan
Spontaneous Recanalization after Complete Occlusion of the Common Carotid Artery with Subsequent Embolic Ischemic Stroke
 Original Contribution Spontaneous Recanalization after Complete Occlusion of the Common Carotid Artery with Subsequent Embolic Ischemic Stroke Abstract Introduction: Acute carotid artery occlusion carries
Original Contribution Spontaneous Recanalization after Complete Occlusion of the Common Carotid Artery with Subsequent Embolic Ischemic Stroke Abstract Introduction: Acute carotid artery occlusion carries
UPSTATE Comprehensive Stroke Center. Neurosurgical Interventions Satish Krishnamurthy MD, MCh
 UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic
UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic
Periodic and Rhythmic Patterns. Suzette M LaRoche, MD Mission Health Epilepsy Center Asheville, North Carolina
 Periodic and Rhythmic Patterns Suzette M LaRoche, MD Mission Health Epilepsy Center Asheville, North Carolina Continuum of EEG Activity Neuronal Injury LRDA GPDs SIRPIDs LPDs + NCS Burst-Suppression LPDs
Periodic and Rhythmic Patterns Suzette M LaRoche, MD Mission Health Epilepsy Center Asheville, North Carolina Continuum of EEG Activity Neuronal Injury LRDA GPDs SIRPIDs LPDs + NCS Burst-Suppression LPDs
Lisa T. Hannegan, MS, CNS, ACNP. Department of Neurological Surgery University of California, San Francisco
 Lisa T. Hannegan, MS, CNS, ACNP Department of Neurological Surgery University of California, San Francisco Era of Clinical Neuro Monitoring Clinical Examination Heart rate Blood Pressure Body temperature
Lisa T. Hannegan, MS, CNS, ACNP Department of Neurological Surgery University of California, San Francisco Era of Clinical Neuro Monitoring Clinical Examination Heart rate Blood Pressure Body temperature
Perils of Mechanical Thrombectomy in Acute Asymptomatic Large Vessel Occlusion
 Perils of Mechanical Thrombectomy in Acute Asymptomatic Large Vessel Occlusion Aman B. Patel, MD Robert & Jean Ojemann Associate Professor Director, Cerebrovascular Surgery Director, Neuroendovascular
Perils of Mechanical Thrombectomy in Acute Asymptomatic Large Vessel Occlusion Aman B. Patel, MD Robert & Jean Ojemann Associate Professor Director, Cerebrovascular Surgery Director, Neuroendovascular
Diagnosis of Middle Cerebral Artery Occlusion with Transcranial Color-Coded Real-Time Sonography
 Diagnosis of Middle Cerebral Artery Occlusion with Transcranial Color-Coded Real-Time Sonography Kazumi Kimura, Yoichiro Hashimoto, Teruyuki Hirano, Makoto Uchino, and Masayuki Ando PURPOSE: To determine
Diagnosis of Middle Cerebral Artery Occlusion with Transcranial Color-Coded Real-Time Sonography Kazumi Kimura, Yoichiro Hashimoto, Teruyuki Hirano, Makoto Uchino, and Masayuki Ando PURPOSE: To determine
Code Stroke Intervention: Endovascular therapy for asah and management J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY
 Code Stroke Intervention: Endovascular therapy for asah and management J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY Disclosures None Part B. Objectives Epidemiology of asah Concept: What is a brain
Code Stroke Intervention: Endovascular therapy for asah and management J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY Disclosures None Part B. Objectives Epidemiology of asah Concept: What is a brain
Comparison of Five Major Recent Endovascular Treatment Trials
 Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Monitoring of Regional Cerebral Blood Flow Using an Implanted Cerebral Thermal Perfusion Probe Archived Medical Policy
 Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Mapping of the brain in unconscious patients Quantitative EEG
 Mapping of the brain in unconscious patients Quantitative EEG Jan Claassen, MD, PhD Division of Critical Care Neurology Columbia University College of Physicians & Surgeons New York, NY 10032 Disclosures:
Mapping of the brain in unconscious patients Quantitative EEG Jan Claassen, MD, PhD Division of Critical Care Neurology Columbia University College of Physicians & Surgeons New York, NY 10032 Disclosures:
Effect of early operation for ruptured aneurysms on prevention of delayed ischemic symptoms
 J Neurosurg 57:622-628, 1982 Effect of early operation for ruptured aneurysms on prevention of delayed ischemic symptoms MAMORU TANEDA, M.D. Department of Neurosurgery, Hanwa Memorial Hospital, Osaka,
J Neurosurg 57:622-628, 1982 Effect of early operation for ruptured aneurysms on prevention of delayed ischemic symptoms MAMORU TANEDA, M.D. Department of Neurosurgery, Hanwa Memorial Hospital, Osaka,
TIA: Updates and Management 2008
 TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine
 Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
Cryptogenic Strokes: Evaluation and Management
 Cryptogenic Strokes: Evaluation and Management 77 yo man with hypertension and hyperlipidemia developed onset of left hemiparesis and right gaze preference, last seen normal at 10:00 AM Brought to ZSFG
Cryptogenic Strokes: Evaluation and Management 77 yo man with hypertension and hyperlipidemia developed onset of left hemiparesis and right gaze preference, last seen normal at 10:00 AM Brought to ZSFG
UPDATES IN INTRACRANIAL INTERVENTION Jordan Taylor DO Metro Health Neurology 2015
 UPDATES IN INTRACRANIAL INTERVENTION Jordan Taylor DO Metro Health Neurology 2015 NEW STUDIES FOR 2015 MR CLEAN ESCAPE EXTEND-IA REVASCAT SWIFT PRIME RECOGNIZED LIMITATIONS IV Alteplase proven benefit
UPDATES IN INTRACRANIAL INTERVENTION Jordan Taylor DO Metro Health Neurology 2015 NEW STUDIES FOR 2015 MR CLEAN ESCAPE EXTEND-IA REVASCAT SWIFT PRIME RECOGNIZED LIMITATIONS IV Alteplase proven benefit
Background. Recommendations for Imaging of Acute Ischemic Stroke: A Scientific Statement From the American Heart Association
 for Imaging of Acute Ischemic Stroke: A Scientific Statement From the American Heart Association An Scientific Statement from the Stroke Council, American Heart Association and American Stroke Association
for Imaging of Acute Ischemic Stroke: A Scientific Statement From the American Heart Association An Scientific Statement from the Stroke Council, American Heart Association and American Stroke Association
Disclosures. Anesthesia for Endovascular Treatment of Acute Ischemic Stroke. Acute Ischemic Stroke. Acute Stroke = Medical Emergency!
 Disclosures Anesthesia for Endovascular Treatment of Acute Ischemic Stroke I have nothing to disclose. Chanhung Lee MD, PhD Associate Professor Anesthesia and perioperative Care Acute Ischemic Stroke 780,000
Disclosures Anesthesia for Endovascular Treatment of Acute Ischemic Stroke I have nothing to disclose. Chanhung Lee MD, PhD Associate Professor Anesthesia and perioperative Care Acute Ischemic Stroke 780,000
MEDICAL POLICY EFFECTIVE DATE: 12/18/08 REVISED DATE: 12/17/09, 03/17/11, 05/19/11, 05/24/12, 05/23/13, 05/22/14
 MEDICAL POLICY SUBJECT: CT (COMPUTED TOMOGRAPHY) PAGE: 1 OF: 5 If the member's subscriber contract excludes coverage for a specific service it is not covered under that contract. In such cases, medical
MEDICAL POLICY SUBJECT: CT (COMPUTED TOMOGRAPHY) PAGE: 1 OF: 5 If the member's subscriber contract excludes coverage for a specific service it is not covered under that contract. In such cases, medical
Advances in Neuro-Endovascular Care for Acute Stroke
 Advances in Neuro-Endovascular Care for Acute Stroke Ciarán J. Powers, MD, PhD, FAANS Associate Professor Program Director Department of Neurological Surgery Surgical Director Comprehensive Stroke Center
Advances in Neuro-Endovascular Care for Acute Stroke Ciarán J. Powers, MD, PhD, FAANS Associate Professor Program Director Department of Neurological Surgery Surgical Director Comprehensive Stroke Center
ACUTE STROKE IMAGING
 ACUTE STROKE IMAGING Mahesh V. Jayaraman M.D. Director, Inter ventional Neuroradiology Associate Professor Depar tments of Diagnostic Imaging and Neurosurger y Alper t Medical School at Brown University
ACUTE STROKE IMAGING Mahesh V. Jayaraman M.D. Director, Inter ventional Neuroradiology Associate Professor Depar tments of Diagnostic Imaging and Neurosurger y Alper t Medical School at Brown University
4/10/2018. The Surgical Treatment of Cerebral Aneurysms. Aneurysm Locations. Aneurysmal Subarachnoid Hemorrhage. Jerone Kennedy, M.D.
 The Surgical Treatment of Cerebral Aneurysms Aneurysmal Subarachnoid Hemorrhage Jerone Kennedy, M.D. Medical Director, Vascular Neurosurgery CentraCare Health-Neurosciences St. Cloud Hospital Aneurysm
The Surgical Treatment of Cerebral Aneurysms Aneurysmal Subarachnoid Hemorrhage Jerone Kennedy, M.D. Medical Director, Vascular Neurosurgery CentraCare Health-Neurosciences St. Cloud Hospital Aneurysm
QEEG markers in stroke, ageing and cognitive decline
 QEEG markers in stroke, ageing and cognitive decline When is theta actually alpha? Simon Finnigan Senior Research Fellow UQ Centre for Clinical Research & Royal Brisbane Clinical Unit University of Queensland,
QEEG markers in stroke, ageing and cognitive decline When is theta actually alpha? Simon Finnigan Senior Research Fellow UQ Centre for Clinical Research & Royal Brisbane Clinical Unit University of Queensland,
ICU EEG MONITORING: WHY, WHEN AND FOR WHOM
 ICU EEG MONITORING: WHY, WHEN AND FOR WHOM Aatif M. Husain, MD Duke University Veterans Affairs Medical Center Durham, NC In the last two decades much has been learned about the frequency with which seizures
ICU EEG MONITORING: WHY, WHEN AND FOR WHOM Aatif M. Husain, MD Duke University Veterans Affairs Medical Center Durham, NC In the last two decades much has been learned about the frequency with which seizures
How Low Should You Go? Management of Blood Pressure in Intracranial Hemorrhage
 How Low Should You Go? Management of Blood Pressure in Intracranial Hemorrhage Rachael Scott, Pharm.D. PGY2 Critical Care Pharmacy Resident Pharmacy Grand Rounds August 21, 2018 2018 MFMER slide-1 Patient
How Low Should You Go? Management of Blood Pressure in Intracranial Hemorrhage Rachael Scott, Pharm.D. PGY2 Critical Care Pharmacy Resident Pharmacy Grand Rounds August 21, 2018 2018 MFMER slide-1 Patient
02/08/53. ** Thanks you to. Dr. Lawrence J. Hirsch, M.D Susan T. Herman, M.D. Jed A. Hartings, Ph.D. Thomas P. Bleck MD Denis Azzopardi
 ** Thanks you to Dr. Lawrence J. Hirsch, M.D Susan T. Herman, M.D. Jed A. Hartings, Ph.D. Thomas P. Bleck MD Denis Azzopardi 1 Why do we need ICU-EEG? Residual electrographic SE after control of visible
** Thanks you to Dr. Lawrence J. Hirsch, M.D Susan T. Herman, M.D. Jed A. Hartings, Ph.D. Thomas P. Bleck MD Denis Azzopardi 1 Why do we need ICU-EEG? Residual electrographic SE after control of visible
Michael Horowitz, MD Pittsburgh, PA
 Michael Horowitz, MD Pittsburgh, PA Introduction Cervical Artery Dissection occurs by a rupture within the arterial wall leading to an intra-mural Hematoma. A possible consequence is an acute occlusion
Michael Horowitz, MD Pittsburgh, PA Introduction Cervical Artery Dissection occurs by a rupture within the arterial wall leading to an intra-mural Hematoma. A possible consequence is an acute occlusion
TRANSCRANIAL DOPPLER ULTRASOUND INTRODUCTION TO TCD INTERPRETATION
 TRANSCRANIAL DOPPLER ULTRASOUND INTRODUCTION TO TCD INTERPRETATION ---Rune Aaslid First TCD Publication 1982 WHAT IS TCD? Uses 2 MHz pulsed Doppler ultrasound Passes through cranial windows Provides information
TRANSCRANIAL DOPPLER ULTRASOUND INTRODUCTION TO TCD INTERPRETATION ---Rune Aaslid First TCD Publication 1982 WHAT IS TCD? Uses 2 MHz pulsed Doppler ultrasound Passes through cranial windows Provides information
11/1/2018. Disclosure. Imaging in Acute Ischemic Stroke 2018 Neuro Symposium. Is NCCT good enough? Keystone Heart Consultant, Stock Options
 Disclosure Imaging in Acute Ischemic Stroke 2018 Neuro Symposium Keystone Heart Consultant, Stock Options Kevin Abrams, M.D. Chief of Radiology Medical Director of Neuroradiology Baptist Hospital, Miami,
Disclosure Imaging in Acute Ischemic Stroke 2018 Neuro Symposium Keystone Heart Consultant, Stock Options Kevin Abrams, M.D. Chief of Radiology Medical Director of Neuroradiology Baptist Hospital, Miami,
IMAGING IN ACUTE ISCHEMIC STROKE
 IMAGING IN ACUTE ISCHEMIC STROKE Timo Krings MD, PhD, FRCP (C) Professor of Radiology & Surgery Braley Chair of Neuroradiology, Chief and Program Director of Diagnostic and Interventional Neuroradiology;
IMAGING IN ACUTE ISCHEMIC STROKE Timo Krings MD, PhD, FRCP (C) Professor of Radiology & Surgery Braley Chair of Neuroradiology, Chief and Program Director of Diagnostic and Interventional Neuroradiology;
ACUTE ISCHEMIC STROKE. Current Treatment Approaches for Acute Ischemic Stroke
 ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
Sub-arachnoid haemorrhage
 Sub-arachnoid haemorrhage Dr Mary Newton Consultant Anaesthetist The National Hospital for Neurology and Neurosurgery UCL Hospitals NHS Trust mary.newton@uclh.nhs.uk Kiev, Ukraine September 17 th 2009
Sub-arachnoid haemorrhage Dr Mary Newton Consultant Anaesthetist The National Hospital for Neurology and Neurosurgery UCL Hospitals NHS Trust mary.newton@uclh.nhs.uk Kiev, Ukraine September 17 th 2009
Stroke School for Internists Part 1
 Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Imaging Stroke: Is There a Stroke Equivalent of the ECG? Albert J. Yoo, MD Director of Acute Stroke Intervention Massachusetts General Hospital
 Imaging Stroke: Is There a Stroke Equivalent of the ECG? Albert J. Yoo, MD Director of Acute Stroke Intervention Massachusetts General Hospital Disclosures Penumbra, Inc. research grant (significant) for
Imaging Stroke: Is There a Stroke Equivalent of the ECG? Albert J. Yoo, MD Director of Acute Stroke Intervention Massachusetts General Hospital Disclosures Penumbra, Inc. research grant (significant) for
Number: Policy *Please see amendment for Pennsylvania Medicaid at the end of this CPB.
 Number: 0789 Policy *Please see amendment for Pennsylvania Medicaid at the end of this CPB. Aetna considers endovascular therapy with a retrievable stent (e.g., Solitaire FR (Flow Restoration stent retriever,
Number: 0789 Policy *Please see amendment for Pennsylvania Medicaid at the end of this CPB. Aetna considers endovascular therapy with a retrievable stent (e.g., Solitaire FR (Flow Restoration stent retriever,
Stroke Guidelines. November 19, 2011
 Stroke Guidelines November 19, 2011 Clinical Practice Guidelines American Stroke Association Guidelines are comprehensive statements that provide the highest level of scientific evidence for clinical practice.
Stroke Guidelines November 19, 2011 Clinical Practice Guidelines American Stroke Association Guidelines are comprehensive statements that provide the highest level of scientific evidence for clinical practice.
occlusions. Cerebral perfusion is driven fundamentally by regional cerebral
 Appendix Figures Figure A1. Hemodynamic changes that may occur in major anterior circulation occlusions. Cerebral perfusion is driven fundamentally by regional cerebral perfusion pressure (CPP). In response
Appendix Figures Figure A1. Hemodynamic changes that may occur in major anterior circulation occlusions. Cerebral perfusion is driven fundamentally by regional cerebral perfusion pressure (CPP). In response
Neuro Quiz 29 Transcranial Doppler Monitoring
 Verghese Cherian, MD, FFARCSI Penn State Hershey Medical Center, Hershey Quiz Team Shobana Rajan, M.D Suneeta Gollapudy, M.D Angele Marie Theard, M.D Neuro Quiz 29 Transcranial Doppler Monitoring This
Verghese Cherian, MD, FFARCSI Penn State Hershey Medical Center, Hershey Quiz Team Shobana Rajan, M.D Suneeta Gollapudy, M.D Angele Marie Theard, M.D Neuro Quiz 29 Transcranial Doppler Monitoring This
Interventions in the Management of Acute Stroke. Dr Md Shafiqul Islam Associate Professor Neurosurgery Dhaka Medical College Hospital
 Interventions in the Management of Acute Stroke Dr Md Shafiqul Islam Associate Professor Neurosurgery Dhaka Medical College Hospital Acute stroke intervention Number of stroke patients increasing day by
Interventions in the Management of Acute Stroke Dr Md Shafiqul Islam Associate Professor Neurosurgery Dhaka Medical College Hospital Acute stroke intervention Number of stroke patients increasing day by
11/23/2015. Disclosures. Stroke Management in the Neurocritical Care Unit. Karel Fuentes MD Medical Director of Neurocritical Care.
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Diagnostic and Therapeutic Consequences of Repeat Brain Imaging and Follow-up Vascular Imaging in Stroke Patients
 AJNR Am J Neuroradiol 0:7, January 999 Diagnostic and Therapeutic Consequences of Repeat Brain Imaging and Follow-up Vascular Imaging in Stroke Patients Birgit Ertl-Wagner, Tobias Brandt, Christina Seifart,
AJNR Am J Neuroradiol 0:7, January 999 Diagnostic and Therapeutic Consequences of Repeat Brain Imaging and Follow-up Vascular Imaging in Stroke Patients Birgit Ertl-Wagner, Tobias Brandt, Christina Seifart,
Brain Attack. Strategies in the Management of Acute Ischemic Stroke: Neuroscience Clerkship. Case Medical Center
 Brain Attack Strategies in the Management of Acute Ischemic Stroke: Neuroscience Clerkship Stroke is a common and devastating disorder Third leading antecedent of death in American men, and second among
Brain Attack Strategies in the Management of Acute Ischemic Stroke: Neuroscience Clerkship Stroke is a common and devastating disorder Third leading antecedent of death in American men, and second among
Basilar artery stenosis with bilateral cerebellar strokes on coumadin
 Qaisar A. Shah, MD Patient Profile 68 years old female with a history of; Basilar artery stenosis with bilateral cerebellar strokes on coumadin Diabetes mellitus Hyperlipidemia Hypertension She developed
Qaisar A. Shah, MD Patient Profile 68 years old female with a history of; Basilar artery stenosis with bilateral cerebellar strokes on coumadin Diabetes mellitus Hyperlipidemia Hypertension She developed
Utility of computed tomography perfusion in detection of cerebral vasospasm in patients with subarachnoid hemorrhage
 Neurosurg Focus 21 (3):E6, 2006 Utility of computed tomography perfusion in detection of cerebral vasospasm in patients with subarachnoid hemorrhage ROHAM MOFTAKHAR, M.D., HOWARD A. ROWLEY, M.D., AQUILLA
Neurosurg Focus 21 (3):E6, 2006 Utility of computed tomography perfusion in detection of cerebral vasospasm in patients with subarachnoid hemorrhage ROHAM MOFTAKHAR, M.D., HOWARD A. ROWLEY, M.D., AQUILLA
Carotid Revascularization
 Options for Carotid Disease Carotid Revascularization Wayne Causey, MD 2 nd Year Vascular Surgery Fellow Best medical therapy, Carotid Endarterectomy, and Carotid Stenting Who benefits from best medical
Options for Carotid Disease Carotid Revascularization Wayne Causey, MD 2 nd Year Vascular Surgery Fellow Best medical therapy, Carotid Endarterectomy, and Carotid Stenting Who benefits from best medical
framework for flow Objectives Acute Stroke Treatment Collaterals in Acute Ischemic Stroke framework & basis for flow
 Acute Stroke Treatment Collaterals in Acute Ischemic Stroke Objectives role of collaterals in acute ischemic stroke collateral therapeutic strategies David S Liebeskind, MD Professor of Neurology & Director
Acute Stroke Treatment Collaterals in Acute Ischemic Stroke Objectives role of collaterals in acute ischemic stroke collateral therapeutic strategies David S Liebeskind, MD Professor of Neurology & Director
Subarachnoid Hemorrhage (SAH) Disclosures/Relationships. Click to edit Master title style. Click to edit Master title style.
 Disclosures/Relationships. Click to edit Master title style. Click to edit Master title style.") Subarachnoid Hemorrhage (SAH) William J. Jones, M.D. Assistant Professor of Neurology Co-Director, UCH Stroke Program Click to edit Master title style Disclosures/Relationships No conflicts of interest
Subarachnoid Hemorrhage (SAH) William J. Jones, M.D. Assistant Professor of Neurology Co-Director, UCH Stroke Program Click to edit Master title style Disclosures/Relationships No conflicts of interest
Acute stroke. Ischaemic stroke. Characteristics. Temporal classification. Clinical features. Interpretation of Emergency Head CT
 Ischaemic stroke Characteristics Stroke is the third most common cause of death in the UK, and the leading cause of disability. 80% of strokes are ischaemic Large vessel occlusive atheromatous disease
Ischaemic stroke Characteristics Stroke is the third most common cause of death in the UK, and the leading cause of disability. 80% of strokes are ischaemic Large vessel occlusive atheromatous disease
HEART AND SOUL STUDY OUTCOME EVENT - MORBIDITY REVIEW FORM
 REVIEW DATE REVIEWER'S ID HEART AND SOUL STUDY OUTCOME EVENT - MORBIDITY REVIEW FORM : DISCHARGE DATE: RECORDS FROM: Hospitalization ER Please check all that may apply: Myocardial Infarction Pages 2, 3,
REVIEW DATE REVIEWER'S ID HEART AND SOUL STUDY OUTCOME EVENT - MORBIDITY REVIEW FORM : DISCHARGE DATE: RECORDS FROM: Hospitalization ER Please check all that may apply: Myocardial Infarction Pages 2, 3,
Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective
 Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective Cathy Sila MD George M Humphrey II Professor and Vice Chair of Neurology Director, Comprehensive Stroke Center
Starting or Resuming Anticoagulation or Antiplatelet Therapy after ICH: A Neurology Perspective Cathy Sila MD George M Humphrey II Professor and Vice Chair of Neurology Director, Comprehensive Stroke Center
Imaging Acute Stroke and Cerebral Ischemia
 Department of Radiology University of California San Diego Imaging Acute Stroke and Cerebral Ischemia John R. Hesselink, M.D. Causes of Stroke Arterial stenosis Thrombosis Embolism Dissection Hypotension
Department of Radiology University of California San Diego Imaging Acute Stroke and Cerebral Ischemia John R. Hesselink, M.D. Causes of Stroke Arterial stenosis Thrombosis Embolism Dissection Hypotension
COMPREHENSIVE SUMMARY OF INSTOR REPORTS
 COMPREHENSIVE SUMMARY OF INSTOR REPORTS Please note that the following chart provides a sampling of INSTOR reports to differentiate this registry s capabilities as a process improvement system. This list
COMPREHENSIVE SUMMARY OF INSTOR REPORTS Please note that the following chart provides a sampling of INSTOR reports to differentiate this registry s capabilities as a process improvement system. This list
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for
 Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
Recent Advances in Neurology Difficult Cases
 Patient X: History Part 1 Recent Advances in Neurology Difficult Cases Heather J. Fullerton, MD, MAS Professor of Neurology & Pediatrics Director, Pediatric Brain Center Previously healthy 14-year old
Patient X: History Part 1 Recent Advances in Neurology Difficult Cases Heather J. Fullerton, MD, MAS Professor of Neurology & Pediatrics Director, Pediatric Brain Center Previously healthy 14-year old
11/27/2017. Stroke Management in the Neurocritical Care Unit. Conflict of interest. Karel Fuentes MD Medical Director of Neurocritical Care
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
/ / / / / / Hospital Abstraction: Stroke/TIA. Participant ID: Hospital Code: Multi-Ethnic Study of Atherosclerosis
 Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Carotid Embolectomy and Endarterectomy for Symptomatic Complete Occlusion of the Carotid Artery as a Rescue Therapy in Acute Ischemic Stroke
 This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivs 3.0 License (www.karger.com/oa-license), applicable to the online version of the article
This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivs 3.0 License (www.karger.com/oa-license), applicable to the online version of the article
CT Perfusion is Essential for Stroke Triage. Maarten Lansberg, MD PhD Associate Professor of Neurology Stanford University, Stanford Stroke Center
 CT Perfusion is Essential for Stroke Triage Maarten Lansberg, MD PhD Associate Professor of Neurology Stanford University, Stanford Stroke Center CT Perfusion is Essential for Stroke Triage Disclosures:
CT Perfusion is Essential for Stroke Triage Maarten Lansberg, MD PhD Associate Professor of Neurology Stanford University, Stanford Stroke Center CT Perfusion is Essential for Stroke Triage Disclosures:
The rupture of an intracranial
 Controversies in the management of aneurysmal subarachnoid hemorrhage* Neeraj S. Naval, MD; Robert D. Stevens, MD; Marek A. Mirski, MD, PhD; Anish Bhardwaj, MD, FCCM Background: The care of patients with
Controversies in the management of aneurysmal subarachnoid hemorrhage* Neeraj S. Naval, MD; Robert D. Stevens, MD; Marek A. Mirski, MD, PhD; Anish Bhardwaj, MD, FCCM Background: The care of patients with
IMAGING IN ACUTE ISCHEMIC STROKE
 IMAGING IN ACUTE ISCHEMIC STROKE Timo Krings MD, PhD, FRCP (C) Professor of Radiology & Surgery Braley Chair of Neuroradiology, Chief and Program Director of Diagnostic and Interventional Neuroradiology;
IMAGING IN ACUTE ISCHEMIC STROKE Timo Krings MD, PhD, FRCP (C) Professor of Radiology & Surgery Braley Chair of Neuroradiology, Chief and Program Director of Diagnostic and Interventional Neuroradiology;
acute-onset, severe, recurrent reversible vasoconstriction
 1 RCVS A clinical and radiologic syndrome Characterized by acute-onset, severe, recurrent headache and reversible vasoconstriction of the cerebral arteries RCVS accounts for most benign thunderclap headaches"
1 RCVS A clinical and radiologic syndrome Characterized by acute-onset, severe, recurrent headache and reversible vasoconstriction of the cerebral arteries RCVS accounts for most benign thunderclap headaches"
Practical Considerations in the Early Treatment of Acute Stroke
 Practical Considerations in the Early Treatment of Acute Stroke Matthew E. Fink, MD Neurologist-in-Chief Weill Cornell Medical College New York-Presbyterian Hospital mfink@med.cornell.edu Disclosures Consultant
Practical Considerations in the Early Treatment of Acute Stroke Matthew E. Fink, MD Neurologist-in-Chief Weill Cornell Medical College New York-Presbyterian Hospital mfink@med.cornell.edu Disclosures Consultant
Stroke Clinical Trials Update Transitioning to an Anatomic Diagnosis in Ischemic Stroke
 Stroke Clinical Trials Update Transitioning to an Anatomic Diagnosis in Ischemic Stroke Alexander A. Khalessi MD MS Director of Endovascular Neurosurgery Surgical Director of NeuroCritical Care University
Stroke Clinical Trials Update Transitioning to an Anatomic Diagnosis in Ischemic Stroke Alexander A. Khalessi MD MS Director of Endovascular Neurosurgery Surgical Director of NeuroCritical Care University
Diagnosis of Subarachnoid Hemorrhage (SAH) and Non- Aneurysmal Causes
 and Non- Aneurysmal Causes") Diagnosis of Subarachnoid Hemorrhage (SAH) and Non- Aneurysmal Causes By Sheila Smith, MD Swedish Medical Center 1 Disclosures I have no disclosures 2 Course Objectives Review significance and differential
Diagnosis of Subarachnoid Hemorrhage (SAH) and Non- Aneurysmal Causes By Sheila Smith, MD Swedish Medical Center 1 Disclosures I have no disclosures 2 Course Objectives Review significance and differential
8/29/2011. Brain Injury Incidence: 200/100,000. Prehospital Brain Injury Mortality Incidence: 20/100,000
 Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
2/7/
 Disclosure Intracranial Atherosclerosis an update None Mai N. Nguyen-Huynh, MD, MAS Assistant Professor of Neurology UCSF Neurovascular Service February 7, 2009 Case #1 60 y.o. Chinese-speaking speaking
Disclosure Intracranial Atherosclerosis an update None Mai N. Nguyen-Huynh, MD, MAS Assistant Professor of Neurology UCSF Neurovascular Service February 7, 2009 Case #1 60 y.o. Chinese-speaking speaking
Emergency EC-IC bypass for symptomatic atherosclerotic ischemic stroke
 Emergency EC-IC bypass for symptomatic atherosclerotic ischemic stroke Tetsuyoshi Horiuchi, Junpei Nitta, Shigetoshi Ishizaka, Kohei Kanaya, Takao Yanagawa, and Kazuhiro Hongo. Department of Neurosurgery,
Emergency EC-IC bypass for symptomatic atherosclerotic ischemic stroke Tetsuyoshi Horiuchi, Junpei Nitta, Shigetoshi Ishizaka, Kohei Kanaya, Takao Yanagawa, and Kazuhiro Hongo. Department of Neurosurgery,
(aneurysmal subarachnoid hemorrhage, 17%~60% :SAH. ,asah , 22%~49% : Willis. :1927 Moniz ;(3) 2. ischemic neurological deficit,dind) SAH) SAH ;(6)
 2. ischemic neurological deficit,dind) SAH) SAH ;(6)") ,, 2. : ;,, :(1), (delayed ;(2) ischemic neurological deficit,dind) ;(3) 2. :SAH ;(4) 5-10 10 HT -1-1 ;(5), 10 SAH ;(6) - - 27%~50%, ( cerebral vasospasm ) Glasgow (Glasgow Coma Scale,GCS), [1],, (aneurysmal
,, 2. : ;,, :(1), (delayed ;(2) ischemic neurological deficit,dind) ;(3) 2. :SAH ;(4) 5-10 10 HT -1-1 ;(5), 10 SAH ;(6) - - 27%~50%, ( cerebral vasospasm ) Glasgow (Glasgow Coma Scale,GCS), [1],, (aneurysmal
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
Ancillary Testing in Death
 Ancillary Testing in Death MICHAËL CHASSÉ, MD, PHD, FRCPC ASSISTANT PROFESSOR, DEPARTMENT OF ANESTHESIOLOGY AND CRITICAL CARE, UNIVERSITÉ LAVAL INTENSIVIST, DEPARTMENT OF ANESTHESIOLOGY, DIVISION OF CRITICAL
Ancillary Testing in Death MICHAËL CHASSÉ, MD, PHD, FRCPC ASSISTANT PROFESSOR, DEPARTMENT OF ANESTHESIOLOGY AND CRITICAL CARE, UNIVERSITÉ LAVAL INTENSIVIST, DEPARTMENT OF ANESTHESIOLOGY, DIVISION OF CRITICAL
Early detection of vasospasm after acute subarachnoid hemorrhage using continuous EEG ICU monitoring
 ELSEVIER Electroencephalography and clinical Neurophysiology 103 (1997) 607-615 Early detection of vasospasm after acute subarachnoid hemorrhage using continuous EEG ICU monitoring Paul M. Vespa a'*, Marc
ELSEVIER Electroencephalography and clinical Neurophysiology 103 (1997) 607-615 Early detection of vasospasm after acute subarachnoid hemorrhage using continuous EEG ICU monitoring Paul M. Vespa a'*, Marc
Blood Pressure Management in Acute Ischemic Stroke
 Blood Pressure Management in Acute Ischemic Stroke Kimberly Clark, PharmD, BCCCP Clinical Pharmacy Specialist Critical Care, Greenville Health System Adjunct Assistant Professor, South Carolina College
Blood Pressure Management in Acute Ischemic Stroke Kimberly Clark, PharmD, BCCCP Clinical Pharmacy Specialist Critical Care, Greenville Health System Adjunct Assistant Professor, South Carolina College
Nicolas Bianchi M.D. May 15th, 2012
 Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
Essentials of Clinical MR, 2 nd edition. 14. Ischemia and Infarction II
 14. Ischemia and Infarction II Lacunar infarcts are small deep parenchymal lesions involving the basal ganglia, internal capsule, thalamus, and brainstem. The vascular supply of these areas includes the
14. Ischemia and Infarction II Lacunar infarcts are small deep parenchymal lesions involving the basal ganglia, internal capsule, thalamus, and brainstem. The vascular supply of these areas includes the
WHI Form Report of Cardiovascular Outcome Ver (For items 1-11, each question specifies mark one or mark all that apply.
 WHI Form - Report of Cardiovascular Outcome Ver. 6. COMMENTS To be completed by Physician Adjudicator Date Completed: - - (M/D/Y) Adjudicator Code: OMB# 095-044 Exp: 4/06 -Affix label here- Clinical Center/ID:
WHI Form - Report of Cardiovascular Outcome Ver. 6. COMMENTS To be completed by Physician Adjudicator Date Completed: - - (M/D/Y) Adjudicator Code: OMB# 095-044 Exp: 4/06 -Affix label here- Clinical Center/ID:
Medical Policy. MP Computed Tomography Perfusion Imaging of the Brain
 Medical Policy MP 6.01.49 BCBSA Ref. Policy: 6.01.49 Last Review: 09/28/2017 Effective Date: 09/28/2017 Section: Radiology Related Policies 2.01.54 Endovascular Procedures for Intracranial Arterial Disease
Medical Policy MP 6.01.49 BCBSA Ref. Policy: 6.01.49 Last Review: 09/28/2017 Effective Date: 09/28/2017 Section: Radiology Related Policies 2.01.54 Endovascular Procedures for Intracranial Arterial Disease
ISPUB.COM. Transcranial Doppler: An Overview of its Clinical Applications. A Alexandrov, M Joseph INTRODUCTION SICKLE CELL DISEASE
 ISPUB.COM The Internet Journal of Neuromonitoring Volume 1 Number 1 Transcranial Doppler: An Overview of its Clinical Applications A Alexandrov, M Joseph Citation A Alexandrov, M Joseph. Transcranial Doppler:
ISPUB.COM The Internet Journal of Neuromonitoring Volume 1 Number 1 Transcranial Doppler: An Overview of its Clinical Applications A Alexandrov, M Joseph Citation A Alexandrov, M Joseph. Transcranial Doppler:
Carotid Endarterectomy for Symptomatic Complete Occlusion of the Internal Carotid Artery
 2011 65 4 239 245 Carotid Endarterectomy for Symptomatic Complete Occlusion of the Internal Carotid Artery a* a b a a a b 240 65 4 2011 241 9 1 60 10 2 62 17 3 67 2 4 64 7 5 69 5 6 71 1 7 55 13 8 73 1
2011 65 4 239 245 Carotid Endarterectomy for Symptomatic Complete Occlusion of the Internal Carotid Artery a* a b a a a b 240 65 4 2011 241 9 1 60 10 2 62 17 3 67 2 4 64 7 5 69 5 6 71 1 7 55 13 8 73 1
Perioperative Management Of Extra-Ventricular Drains (EVD)
") Perioperative Management Of Extra-Ventricular Drains (EVD) Dr. Vijay Tarnal MBBS, FRCA Clinical Assistant Professor Division of Neuroanesthesiology Division of Head & Neck Anesthesiology Michigan Medicine
Perioperative Management Of Extra-Ventricular Drains (EVD) Dr. Vijay Tarnal MBBS, FRCA Clinical Assistant Professor Division of Neuroanesthesiology Division of Head & Neck Anesthesiology Michigan Medicine
INSTITUTE OF NEUROSURGERY & DEPARTMENT OF PICU
 CEREBRAL BYPASS An Innovative Treatment for Arteritis INSTITUTE OF NEUROSURGERY & DEPARTMENT OF PICU CASE 1 q 1 year old girl -recurrent seizure, right side limb weakness, excessive cry and irritability.
CEREBRAL BYPASS An Innovative Treatment for Arteritis INSTITUTE OF NEUROSURGERY & DEPARTMENT OF PICU CASE 1 q 1 year old girl -recurrent seizure, right side limb weakness, excessive cry and irritability.
CEA and cerebral protection Volodymyr labinskyy, MD
 CEA and cerebral protection Volodymyr labinskyy, MD VA Hospital 7/26/2012 63 year old male presents for the vascular evaluation s/p TIA in January 2012 PMH: HTN, long term active smoker, Hep C PSH: None
CEA and cerebral protection Volodymyr labinskyy, MD VA Hospital 7/26/2012 63 year old male presents for the vascular evaluation s/p TIA in January 2012 PMH: HTN, long term active smoker, Hep C PSH: None
Carotid Artery Stenting
 Carotid Artery Stenting JESSICA MITCHELL, ACNP CENTRAL ILLINOIS RADIOLOGICAL ASSOCIATES External Carotid Artery (ECA) can easily be identified from Internal Carotid Artery (ICA) by noticing the branches.
Carotid Artery Stenting JESSICA MITCHELL, ACNP CENTRAL ILLINOIS RADIOLOGICAL ASSOCIATES External Carotid Artery (ECA) can easily be identified from Internal Carotid Artery (ICA) by noticing the branches.