Stroke Guidelines. November 19, 2011
|
|
|
- Amice Garrett
- 6 years ago
- Views:
Transcription
1 Stroke Guidelines November 19, 2011
2 Clinical Practice Guidelines American Stroke Association Guidelines are comprehensive statements that provide the highest level of scientific evidence for clinical practice. The 6 flagship or core Guidelines of the Stroke Council are: Primary Prevention of Stroke (2010) Prevention of Stroke in Patients with Stroke or TIA (2010) Early Management of Acute Ischemic Stroke (2007) Management of Spontaneous Intracerebral Hemorrhage (2010) Management of Subarachnoid Hemorrhage (2009) Stroke Rehabilitation (2005)
3 Clinical Practice Guidelines Panel of physicians Vascular neurology Neurocritical care Emergency medicine Neurosurgery Interventional neuroradiology/endovascular neurosurgery Goal: Provide updated recommendations for care w/i first hours of stroke
4 Protocols/Order Sets Thromoblytic Orders Acute Evaluation Orders Discharge Orders Admission Orders NIHSS/tPA Comm form tpa Monitoring Protocol Stroke Alert Process Document Dysphagia Screen DVT Prophylaxis Insulin Orders Interdisciplinary Plan of Care
5 Prehospital Management & Field Treatment Use of 911 system supported to speed access to stroke tx Stroke should be a priority dispatch Public awareness campaigns needed to increase pts who can be treated within time window Education programs for physicians, hospital personnel and EMS personnel to increase pts who are treated Brief but standardized EMS assessments to identify stroke Begin stroke management in field with use of protocols Rapid transport to nearest appropriate facility Telemedicine may facilitate stroke evaluation and treatment Use where lack of expertise prevents access to PSC for tpa eligibility Providers w/ stroke expertise, response time targets, plan for pts disposition Users provide emergency diagnosis & treatment as defined for PSCs
6 Stroke Center Certification Primary Stroke Center development strongly recommended Comprehensive stroke center External certification EMS should bypass hospitals w/o stroke resources to closest treating stroke facility for suspected stroke patients
7 Emergency Evaluation and Diagnosis Organized protocol for the emergency evaluation of patients with suspected stroke Goal to complete evaluation and decide treatment within 60 minutes of arrival Designate an acute stroke team that includes physicians, nurses, and laboratory/ radiology personnel Stroke rating scale is recommended NIHSS Limited number of hematologic, coagulation, and biochemistry tests during the initial emergency evaluation Chest x-ray for selected patients Acute cardiac or pulmonary disease EKG
8 Early Diagnosis: Brain and Vascular Imaging Brain imaging prior to any specific stroke treatment CT adequate in most instances Should be interpreted by physician w/ appropriate expertise Some findings may be associated w/ poor outcome after stroke Advanced imaging may help with stroke diagnosis Except for evidence of hemorrhage, no finding should preclude IV tpa tx w/i 3 hr window Additional imaging needed for IA tap, surgical procedures or endovascular intervention Advanced imaging should not delay tx w/ IV tpa for eligible pts


9 Organized protocol for acute stroke evaluation including time goals for completion of major events

10 Protocol defines role/responsibility for each department involved
11 Priority of LOD vs STAT for stroke alert patients Focus on test results required in assisting w/ early decision making
12 General orders limited and focus on identifying deficits preventing complications during initial evaluation and treatment decision making
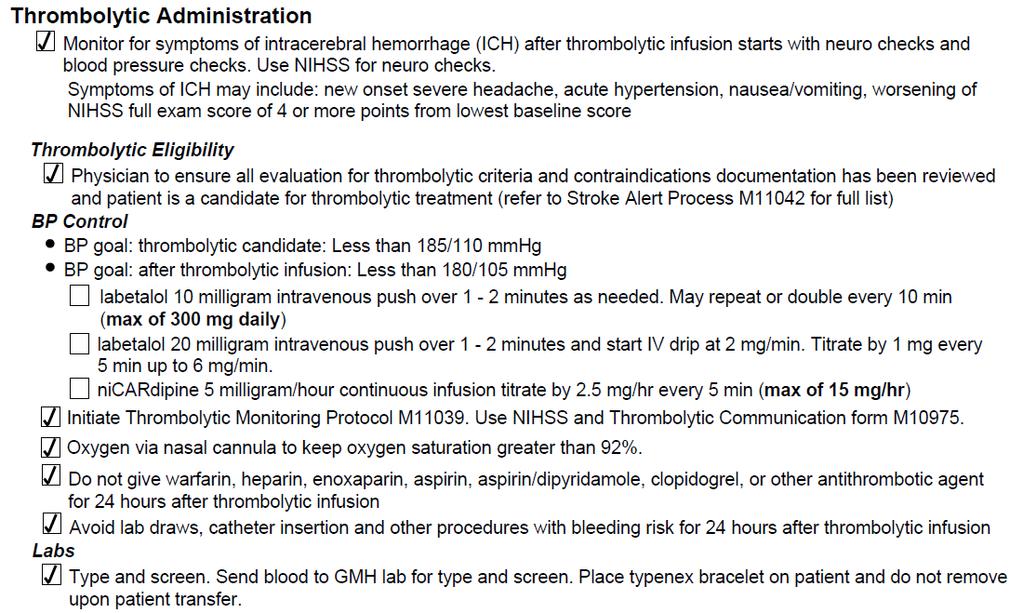
13 Intravenous Thrombolysis IV tpa is recommended for selected pts w/i 3 hr of stroke onset Criteria for eligibility used to determine appropriate candidates Monitoring after treatment should follow recommended regimen Monitoring for sx of hemorrhage and angioedema required BP responsive to treatment may not exclude IV tpa administration Seizure may not exclude patient from IV tpa tx if physician convinced symptoms related to stroke

14 Includes a reference list of IV thrombolytic considerations for neurologist & team review
15
16 Dose weight based Two dose verifications in addition to ordering physician

17 Standardized monitoring protocol Includes instructions for response if ICH suspected

18 Standardized form for monitoring facilitates handoff communication
19 Intra-Arterial Thrombolysis IA thrombolysis an option for selected patients < 6 hrs of onset MCA occlusion Not otherwise eligible for IV tpa Requires access to experienced stroke center Angiography Qualified interventionalists Availability should not preclude IV tap tx for eligible pts
20 General Supportive Care & Treatment of Acute Complications Airway & vent support for pts w/ decreased LOC or airway compromise O2 for hypoxia Treat & avoid fever Cardiac monitoring for a-fib & other arrhythmias for at least 24 hrs Goal for normoglycemia Treat hypoglycemia Hyperglycemia during 1 st 2r hrs associated w/ poor outcomes Treat at >140 to 185 mg/dl
21 If airway compromised, admit to critical care Cardiac monitoring, bedside or telemetry standard Parameters for O2 therapy Meds for fever Regimen 1: Treat for BS > 150
22 General Supportive Care & Treatment of Acute Complications Cautious management of hypertension May spontaneously decline w/i first 24 hrs of stroke onset Treat if other medical indications If eligible for IV tpa treat to goal of <185/110 before tx and then maintain <180/105 for 24 hrs after Same BP parameters for IA tpa Reasonable goal to lower by 15% in first 24 hrs of stroke if markedly elevated (i.e. SBP >220 or DBP >120 Suggested meds include Labetalol 10 to 20 mg IV over 1 to 2 minutes, may repeat 1 Nitropaste 1 to 2 inches Nicardipine infusion, 5 mg/h, titrate up by 2.5 mg/h at 5- to 15-minute intervals, maximum dose 15 mg/h; when desired blood pressure attained, reduce to 3 mg/h
23 General Supportive Care & Treatment of Acute Complications Antihypertensive meds may be restarted at 24 hr if preexisting hypertension and neurologically stable unless otherwise contraindicated Avoid hypotension by correcting hypovolemia and treating cardiac arrhythmias that may reduce cardiac output Hyperbaric oxygen not recommended except for cause due to air embolism Hypothermia for stroke w/o sufficient evidence for recommendation

24 Hypertensive meds for ischemic stroke directly from guidelines Additional meds ICU norm & from hemorrhagic guidelines
25 Anticoagulants Urgent anticoagulation not recommended to: prevent early recurrent stroke halt neurologic worsening improve outcome after AIS Not recommended in lieu of IV tap for otherwise eligible pts Not recommended for moderate to severe strokes due to risk of ICH Anticoagulation w/i 24 hrs after IV tpa not recommended
26 Antiplatelet Agents ASA 325 mg w/i hrs recommended for most pts ASA not a substitute for other acute interventions including IV tap ASA in addition to IV tpa not recommended in 1 st 24 hrs Clopidogrel alone or w/ ASA not rec for AIS treatment IV antiplatelent agents to inhibit gpiib/iiia not recommended outside of clinical trials
27 Antiplatelet Agents Secondary stroke prevention Non-cardioembolic IS or TIA use antiplatelet instead of oral anticoagulants Options for initial therapy include: ASA mg ASA+ER dipyridamole 200 mg BID Clopidogrel 75mg ASA + Clopidogrel increases risk of hemorrhage, routine use for secondary prevention not recommended (Guidelines for the Prevention of Stroke in Patients With Stroke or Transient, Stroke 2011)

28 ASA dosage for acute treatment List from secondary stroke prevention guidelines Oral anticoagulants for cardioembolic strokes
29 Induced Hypertension for the Management of AIS Drug-induced hypertension may be prescribed in exceptional cases Use of neuro & cardiac monitoring needed Not recommended outside of clinical trials for most patients Surgical Interventions Data on the safety and effectiveness of carotid endarterectomy and other operations for treatment of patients with acute ischemic stroke are not sufficient to permit a recommendation. Surgical procedures may have serious risks and may not favorably alter the outcome of the patient.
30 Endovascular Interventions Although the MERCI device is a reasonable intervention for extraction of intra-arterial thrombi in carefully selected patients, the panel also recognizes that the utility of the device in improving outcomes after stroke is unclear (Class IIb, Level of Evidence B). The panel also recommends that the device be studied in additional clinical trials that will define its role in the emergency management of stroke. The usefulness of other mechanical endovascular treatments is not established (Class IIb, Level of Evidence C). These devices should be used in the setting of clinical trials.
31 Combination Reperfusion Therapy in Acute Stroke At present, combinations of interventions to restore perfusion cannot be recommended outside the setting of clinical trials (Class III, Level of Evidence B). Neuroprotective Agents At present, no intervention with putative neuroprotective actions has been established as effective in improving outcomes after stroke, and therefore none currently can be recommended (Class III, Level of Evidence A).
32 Admission to the Hospital and General Acute Treatment Stroke order sets Stroke units recommended Comprehensive specialized stroke care Incorporation of rehabilitation Early mobilization Swallow assessment before any PO Alternate nutrition/hydration via feeding tube while efforts to restore swallowing Nutritional supplements not needed Measures to prevent & treat pneumonia or UTI Prophylactic antibiotics not recommended Avoid indwelling catheters when possible
33 Admission to the Hospital and General Acute Treatment DVT prophlyaxis w/ SQ anticoagulants for immobilized pts ASA less effective than anticoagulants Intermittent external compression devices recommende for those who cannot receive anticoagulants Treatment/management of other medical issues Early interventions to prevent recurrent stroke
34 Updated PSC Recs: Defined group of beds, staff and protocols used for acute stroke care Staffed with by personnel with training and expertise in caring for pts w/ SV disease Many operate as step-down units w/ a 1:3 ratio Multichannel telemetry (BP, P, R, O2) Neuro assessment expertise NIHSS Notification protocol for for changes or worsening in VS and/or neuro status



35 All stroke patients NPO until dysphagia screen Recommends modified diet or NPO until SLP eval
36 Treatment of Acute Neurological Complications Major infarctions higher risk for cerebral edema and increased ICP Measures to decrease risk and monitor for neuro worsening recommended Hydrocephalus secondary to IS affecting cerebellum can be treated w/ ventricular drain Surgical decompression for cerebellar infarction Recurrent seizures should be treated Osmotherapy & hyperventilation unproven and may delay decompressive surgery. Decompressive surgery for malignant edema of the cerebral hemisphere may be life-saving, but the impact of morbidity is unknown Both the age of the patient and the side of the infarction (dominant versus nondominant hemisphere) may affect decisions about surgery.
37 Treatment of Acute Neurological Complications No specific recommendation is made for treatment of patients with asymptomatic hemorrhagic transformation after ischemic stroke Treatment of symptomatic hemorrhagic transformation is addressed in the intracerebral hemorrhage management guideline being issued contemporaneously with this statement Measures to lessen the likelihood of hemorrhagic complications of thrombolytic agents or other interventions to restore or improve perfusion such as careful control of arterial blood pressure are recommended. Corticosteroids are not recommended for treatment of cerebral edema and increased intracranial pressure Prophylactic administration of anticonvulsants to patients with stroke but who have not had seizures is not recommended
38 Palliative Care The family should be given the opportunity to select or withhold medical interventions. In such situation, the medical care may emphasize measures to keep the patient comfortable and to support the family during the terminal aspects of the stroke.
Protocol for IV rtpa Treatment of Acute Ischemic Stroke
 Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข
 Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข Emergency start at community level: Prehospital care Acute stroke
Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข Emergency start at community level: Prehospital care Acute stroke
Team Work in Treatment of Acute Ischemic Stroke
 Diagnosis and Treatment in Acute Ischemic stroke July, 15 th 2016. Bach Mai Hospital Team Work in Treatment of Acute Ischemic Stroke Prof. Pham Minh Thong 1 Time is brain Ischemic stroke: big global burden
Diagnosis and Treatment in Acute Ischemic stroke July, 15 th 2016. Bach Mai Hospital Team Work in Treatment of Acute Ischemic Stroke Prof. Pham Minh Thong 1 Time is brain Ischemic stroke: big global burden
11/27/2017. Stroke Management in the Neurocritical Care Unit. Conflict of interest. Karel Fuentes MD Medical Director of Neurocritical Care
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
11/23/2015. Disclosures. Stroke Management in the Neurocritical Care Unit. Karel Fuentes MD Medical Director of Neurocritical Care.
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Operation Stroke. How to Reduce the Risk of Stroke Complications
 Operation Stroke How to Reduce the Risk of Stroke Complications Objectives Focus on Acute Stroke as an active disease Discuss the most common stroke complications Describe how first 72 hours sets the stage
Operation Stroke How to Reduce the Risk of Stroke Complications Objectives Focus on Acute Stroke as an active disease Discuss the most common stroke complications Describe how first 72 hours sets the stage
2018 Early Management of Acute Ischemic Stroke Guidelines Update
 2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
Stroke in the Rural Setting: How You Can Make A Difference. Susie Fisher, RN, BSN Program Manager Providence Stroke Center Portland, OR
 Stroke in the Rural Setting: How You Can Make A Difference. Susie Fisher, RN, BSN Program Manager Providence Stroke Center Portland, OR Outline State Statistics The Oregon Problem Time & Treatments Steps
Stroke in the Rural Setting: How You Can Make A Difference. Susie Fisher, RN, BSN Program Manager Providence Stroke Center Portland, OR Outline State Statistics The Oregon Problem Time & Treatments Steps
GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE
 2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
Canadian Best Practice Recommendations for Stroke Care. (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management
 Section # 3 Section # 3 Hyperacute Stroke Management") Canadian Best Practice Recommendations for Stroke Care (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management Reorganization of Recommendations 2008 2006 RECOMMENDATIONS: 2008 RECOMMENDATIONS:
Canadian Best Practice Recommendations for Stroke Care (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management Reorganization of Recommendations 2008 2006 RECOMMENDATIONS: 2008 RECOMMENDATIONS:
OHSU Health Care System
 Acute Stroke Practice Standard for the Emergency Department (includes ischemic stroke, TIAs, intracerebral hemorrhage, and non-subarachnoid hemorrhage), PS 01.11 Last Reviewed Date: 2/2/10 STATEMENT OF
Acute Stroke Practice Standard for the Emergency Department (includes ischemic stroke, TIAs, intracerebral hemorrhage, and non-subarachnoid hemorrhage), PS 01.11 Last Reviewed Date: 2/2/10 STATEMENT OF
This publication, Guidelines for the Early Management of
 This publication, Guidelines for the Early Management of Patients With Acute Ischemic Stroke, from the American Heart Association/American Stroke Association (AHA/ASA) is an overview of the current evidence
This publication, Guidelines for the Early Management of Patients With Acute Ischemic Stroke, from the American Heart Association/American Stroke Association (AHA/ASA) is an overview of the current evidence
OHSU HEALTH CARE SYSTEM PRACTICE GUIDELINES
 OHSU HEALTH CARE SYSTEM NEUROSCIENCES (includes ischemic stroke, TIA, intracerebral hemorrhage and non-subarachnoid hemorrhage) Last Reviewed Date: September 2013 POLICY STATEMENT: OHSU hospitals and clinics
OHSU HEALTH CARE SYSTEM NEUROSCIENCES (includes ischemic stroke, TIA, intracerebral hemorrhage and non-subarachnoid hemorrhage) Last Reviewed Date: September 2013 POLICY STATEMENT: OHSU hospitals and clinics
Stroke: The First Critical Hour. Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP
 Stroke: The First Critical Hour Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP Disclosures We have no actual or potential conflicts of interest in relation to this presentation. Objectives Discuss
Stroke: The First Critical Hour Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP Disclosures We have no actual or potential conflicts of interest in relation to this presentation. Objectives Discuss
BY: Ramon Medina EMT-LP/RN
 BY: Ramon Medina EMT-LP/RN Discuss types of strokes Discuss the physical and neurological assessment of stroke patients Discuss pertinent historical findings Discuss pre-hospital and emergency management
BY: Ramon Medina EMT-LP/RN Discuss types of strokes Discuss the physical and neurological assessment of stroke patients Discuss pertinent historical findings Discuss pre-hospital and emergency management
Primary Versus Comprehensive: What is the Difference?
 Primary Versus Comprehensive: What is the Difference? April 26, 2018 Bethann Mercanti, PA-C Director of Clinical Practice Stroke Program Coordinator Cooper Neurological Institute Cooper Bon & Joint Institute
Primary Versus Comprehensive: What is the Difference? April 26, 2018 Bethann Mercanti, PA-C Director of Clinical Practice Stroke Program Coordinator Cooper Neurological Institute Cooper Bon & Joint Institute
Stroke Update. Lacunar 19% Thromboembolic 6% SAH 13% ICH 13% Unknown 32% Hemorrhagic 26% Ischemic 71% Other 3% Cardioembolic 14%
 Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Emergency Treatment of Ischemic Stroke
 Emergency Treatment of Ischemic Stroke JEFFREY BOYLE, M.D., PHD CLINICAL DIRECTOR OF STROKE AT AVERA MCKENNAN AVERA MEDICAL GROUP NEUROLOGY SIOUX FALLS, SD Conflicts of Interest None I will discuss therapies
Emergency Treatment of Ischemic Stroke JEFFREY BOYLE, M.D., PHD CLINICAL DIRECTOR OF STROKE AT AVERA MCKENNAN AVERA MEDICAL GROUP NEUROLOGY SIOUX FALLS, SD Conflicts of Interest None I will discuss therapies
Shawke A. Soueidan, MD. Riverside Neurology & Sleep Specialists
 Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Get With the Guidelines Stroke PMT. Quality Measure Descriptions
 Get With the Guidelines Stroke PMT Quality Measure s Last Updated July 2016 Print Measure s Dysphagia Screen Stroke Education Rehabilitation Considered Time to Intravenous Thrombolytic Therapy 60 min LDL
Get With the Guidelines Stroke PMT Quality Measure s Last Updated July 2016 Print Measure s Dysphagia Screen Stroke Education Rehabilitation Considered Time to Intravenous Thrombolytic Therapy 60 min LDL
Pathophysiology of stroke
 A practical approach to acute stro ke Dr. Sanjith Aaron, M.D., D.M., Professor, Department of Neurosciences, CMC Vellore Stroke is characterized by an abrupt onset of neurological deficit lasting more
A practical approach to acute stro ke Dr. Sanjith Aaron, M.D., D.M., Professor, Department of Neurosciences, CMC Vellore Stroke is characterized by an abrupt onset of neurological deficit lasting more
CEREBRO VASCULAR ACCIDENTS
 CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
Diagnosis: Allergies with reaction type:
 Patient Name: Diagnosis: Allergies with reaction type: ICU Stroke-Ischemic S/P tpa Version 2 5/29/14 This order set is designed to be used with an admission set or for a patient already admitted Nursing
Patient Name: Diagnosis: Allergies with reaction type: ICU Stroke-Ischemic S/P tpa Version 2 5/29/14 This order set is designed to be used with an admission set or for a patient already admitted Nursing
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for
 Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
10/15/ ) Discuss changes in new guidelines for management of acute ischemic stroke patients.
 Discuss changes in new guidelines for management of acute ischemic stroke patients.") 1) Discuss changes in new guidelines for management of acute ischemic stroke patients. Ischemic Stroke Care Erin Brinser, CRNP 2) Evaluate management techniques of complex stroke care. 3) Present current
1) Discuss changes in new guidelines for management of acute ischemic stroke patients. Ischemic Stroke Care Erin Brinser, CRNP 2) Evaluate management techniques of complex stroke care. 3) Present current
Emergency Department Management of Acute Ischemic Stroke
 Emergency Department Management of Acute Ischemic Stroke R. Jason Thurman, MD Associate Professor of Emergency Medicine and Neurosurgery Associate Director, Vanderbilt Stroke Center Vanderbilt University,
Emergency Department Management of Acute Ischemic Stroke R. Jason Thurman, MD Associate Professor of Emergency Medicine and Neurosurgery Associate Director, Vanderbilt Stroke Center Vanderbilt University,
Primary Stroke Center Acute Stroke Transfer Guidelines When to Consider a Transfer:
 When to Consider a Transfer: Hemorrhagic Stroke Large volume intracerebral hematoma greater than 5cm on CT Concern for expanding hematoma Rapidly declining mental status, especially requiring intubation
When to Consider a Transfer: Hemorrhagic Stroke Large volume intracerebral hematoma greater than 5cm on CT Concern for expanding hematoma Rapidly declining mental status, especially requiring intubation
Nuts for Neuro and why I hate EMR
 Nuts for Neuro and why I hate EMR Roberta S Rose, DO private practice in General neurology Staff physician: IRMC and SRMC I have no disclosures, I m just a working stiff Stroke overview: 2018 Guidelines
Nuts for Neuro and why I hate EMR Roberta S Rose, DO private practice in General neurology Staff physician: IRMC and SRMC I have no disclosures, I m just a working stiff Stroke overview: 2018 Guidelines
Stroke Topics. Advances in the Prevention and Treatment of Stroke. Non-Contrast Head CT. Patient 1-68 yo man
 Stroke Topics Advances in the Prevention and Treatment of Stroke August 10, 2009 John W. Engstrom, M.D. Professor of Neurology Acute treatment options for ischemic stroke tpa, clot retraction, future directions
Stroke Topics Advances in the Prevention and Treatment of Stroke August 10, 2009 John W. Engstrom, M.D. Professor of Neurology Acute treatment options for ischemic stroke tpa, clot retraction, future directions
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS. ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS
 FOR THROMBOLYSIS") NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS I. Purpose : A. To reduce morbidity and mortality associated
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS I. Purpose : A. To reduce morbidity and mortality associated
WV Appalachian Stroke Network 2016 State Stroke Conference The Big Decision Packaging the Patient for Transfer
 WV Appalachian Stroke Network 2016 State Stroke Conference The Big Decision Packaging the Patient for Transfer Dr. Jim Kyle, FACSM, FAAFP Regional Medical Director WVOEMS Executive Director, The Kyle Group
WV Appalachian Stroke Network 2016 State Stroke Conference The Big Decision Packaging the Patient for Transfer Dr. Jim Kyle, FACSM, FAAFP Regional Medical Director WVOEMS Executive Director, The Kyle Group
SCCEP 2013 LLSA Course Article 10 AHA/ASA Guidelines for the Management of Spontaneous ICH
 SCCEP 2013 LLSA Course Article 10 AHA/ASA Guidelines for the Management of Spontaneous ICH Morgenstern LB, Hemphill JC. Stroke July 2010;41:2108-2129. Article: This article presents guidelines whose "aim
SCCEP 2013 LLSA Course Article 10 AHA/ASA Guidelines for the Management of Spontaneous ICH Morgenstern LB, Hemphill JC. Stroke July 2010;41:2108-2129. Article: This article presents guidelines whose "aim
Primary Stroke Center Quality & Performance Measures
 Primary Stroke Center Quality & Performance Measures This section of the manual contains information related to the quality performance of Primary Stroke Centers. Brain Attack Coalition Definitions Recognition
Primary Stroke Center Quality & Performance Measures This section of the manual contains information related to the quality performance of Primary Stroke Centers. Brain Attack Coalition Definitions Recognition
Disclosures. Anesthesia for Endovascular Treatment of Acute Ischemic Stroke. Acute Ischemic Stroke. Acute Stroke = Medical Emergency!
 Disclosures Anesthesia for Endovascular Treatment of Acute Ischemic Stroke I have nothing to disclose. Chanhung Lee MD, PhD Associate Professor Anesthesia and perioperative Care Acute Ischemic Stroke 780,000
Disclosures Anesthesia for Endovascular Treatment of Acute Ischemic Stroke I have nothing to disclose. Chanhung Lee MD, PhD Associate Professor Anesthesia and perioperative Care Acute Ischemic Stroke 780,000
Acute Stroke Protocols Modified- What s New in 2013
 Acute Stroke Protocols Modified- What s New in 2013 KUMAR RAJAMANI, MD, DM. Vascular Neurologist-MSN Associate Professor of Neurology WSU School of Medicine. Saturday, September 21, 2013 Crystal Mountain
Acute Stroke Protocols Modified- What s New in 2013 KUMAR RAJAMANI, MD, DM. Vascular Neurologist-MSN Associate Professor of Neurology WSU School of Medicine. Saturday, September 21, 2013 Crystal Mountain
Canadian Stroke Best Practices Initial ED Evaluation of Acute Stroke and Transient Ischemic Attack (TIA) Order Set (Order Set 1)
 Order Set (Order Set 1)") Canadian Best Practice Recommendations for Stroke Care: All patients presenting to an emergency department with suspected stroke or transient ischemic attack must have an immediate clinical evaluation
Canadian Best Practice Recommendations for Stroke Care: All patients presenting to an emergency department with suspected stroke or transient ischemic attack must have an immediate clinical evaluation
Case 1 5/26/2017 ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE
 ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE Rhonda Whiteman Racing Against the Clock Workshop June 1, 2017 Objectives To discuss the hyperacute ischemic stroke management
ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE Rhonda Whiteman Racing Against the Clock Workshop June 1, 2017 Objectives To discuss the hyperacute ischemic stroke management
Antithrombotics: Percent of patients with an ischemic stroke or TIA prescribed antithrombotic therapy at discharge. Corresponding
 Get With The Guidelines -Stroke is the American Heart Association s collaborative performance improvement program, demonstrated to improve adherence to evidence-based care of patients hospitalized with
Get With The Guidelines -Stroke is the American Heart Association s collaborative performance improvement program, demonstrated to improve adherence to evidence-based care of patients hospitalized with
Moving from a Primary Stroke Center to a Comprehensive Stroke Center
 Moving from a Primary Stroke Center to a Comprehensive Stroke Center MJ Hampel, MPH, MBA The Joint Commission October 19, 2012 Presenter Disclosure Information MJ Hampel Moving from a Primary Stroke Center
Moving from a Primary Stroke Center to a Comprehensive Stroke Center MJ Hampel, MPH, MBA The Joint Commission October 19, 2012 Presenter Disclosure Information MJ Hampel Moving from a Primary Stroke Center
William Barr, M.D. January 28, 2017
 William Barr, M.D. January 28, 2017 Types of Stroke Ischemic Stroke Small vessel (20%) Large vessel (31%) Embolic (32%) Hemorrhagic Intracerebral Hemorrhage (10%) Subarachnoid Hemorrhage (7%) The Majority
William Barr, M.D. January 28, 2017 Types of Stroke Ischemic Stroke Small vessel (20%) Large vessel (31%) Embolic (32%) Hemorrhagic Intracerebral Hemorrhage (10%) Subarachnoid Hemorrhage (7%) The Majority
Rural emergency department best practice for treatment of acute ischemic stroke
 Rural emergency department best practice for treatment of acute ischemic stroke Aubrey J. Hoye, DO Ministry Howard Young Medical Center, Woodruff, WI Ministry Eagle River Memorial Hospital, Eagle River,
Rural emergency department best practice for treatment of acute ischemic stroke Aubrey J. Hoye, DO Ministry Howard Young Medical Center, Woodruff, WI Ministry Eagle River Memorial Hospital, Eagle River,
The Importance of Stroke Programs in an Acute Care Setting by Debbie Estes, RN, BSN Stroke Program Coordinator, Medical City of Dallas
 The Importance of Stroke Programs in an Acute Care Setting by Debbie Estes, RN, BSN Stroke Program Coordinator, Medical City of Dallas Objectives Describe the road to the gold Discuss the importance of
The Importance of Stroke Programs in an Acute Care Setting by Debbie Estes, RN, BSN Stroke Program Coordinator, Medical City of Dallas Objectives Describe the road to the gold Discuss the importance of
Hypertensive Urgency and Emergency. Definitions. Emergency or Urgency?
 Hypertensive Urgency and Emergency Joel Handler MD Kaiser Permanente Care Management Institute/ SCal Region Hypertension Lead Definitions Hypertensive Emergency: -Severe elevation in BP with evidence of
Hypertensive Urgency and Emergency Joel Handler MD Kaiser Permanente Care Management Institute/ SCal Region Hypertension Lead Definitions Hypertensive Emergency: -Severe elevation in BP with evidence of
Practical Considerations in the Early Treatment of Acute Stroke
 Practical Considerations in the Early Treatment of Acute Stroke Matthew E. Fink, MD Neurologist-in-Chief Weill Cornell Medical College New York-Presbyterian Hospital mfink@med.cornell.edu Disclosures Consultant
Practical Considerations in the Early Treatment of Acute Stroke Matthew E. Fink, MD Neurologist-in-Chief Weill Cornell Medical College New York-Presbyterian Hospital mfink@med.cornell.edu Disclosures Consultant
CEDR 2018 QCDR Measures for CMS 2018 MIPS Performance Year Reporting
 ACEP19 Emergency Department Utilization of CT for Minor Blunt Head Trauma for Aged 18 Years and Older Percentage of visits for aged 18 years and older who presented with a minor blunt head trauma who had
ACEP19 Emergency Department Utilization of CT for Minor Blunt Head Trauma for Aged 18 Years and Older Percentage of visits for aged 18 years and older who presented with a minor blunt head trauma who had
COMPREHENSIVE SUMMARY OF INSTOR REPORTS
 COMPREHENSIVE SUMMARY OF INSTOR REPORTS Please note that the following chart provides a sampling of INSTOR reports to differentiate this registry s capabilities as a process improvement system. This list
COMPREHENSIVE SUMMARY OF INSTOR REPORTS Please note that the following chart provides a sampling of INSTOR reports to differentiate this registry s capabilities as a process improvement system. This list
Critical Care Management of Acute Ischemic Stroke
 Critical Care Management of Acute Ischemic Stroke Gene Sung, M.D., M.P.H. Past-President, Neurocritical Care Society Neurocritical Care and Stroke Division University of Southern California USC Stroke
Critical Care Management of Acute Ischemic Stroke Gene Sung, M.D., M.P.H. Past-President, Neurocritical Care Society Neurocritical Care and Stroke Division University of Southern California USC Stroke
3. Screening Subject Identification Screening Overview
 3. Screening 3.1 Subject Identification Each site will be responsible for identifying and recruiting participants into the study. It is known that screening methods vary across sites. It is, however, important
3. Screening 3.1 Subject Identification Each site will be responsible for identifying and recruiting participants into the study. It is known that screening methods vary across sites. It is, however, important
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
Intensive Medical Therapy with Therapeutic Hypothermia for Malignant Middle Cerebral Artery Infarction
 Intensive Medical Therapy with Therapeutic Hypothermia for Malignant Middle Cerebral Artery Infarction Kyu sun Lee 1, Sung Eun Lee, 1 Jin Soo Lee 1, Ji Man Hong 1 1 Department of Neurology, Ajou University
Intensive Medical Therapy with Therapeutic Hypothermia for Malignant Middle Cerebral Artery Infarction Kyu sun Lee 1, Sung Eun Lee, 1 Jin Soo Lee 1, Ji Man Hong 1 1 Department of Neurology, Ajou University
Comparison of Five Major Recent Endovascular Treatment Trials
 Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Unclogging The Pipes. Zahraa Rabeeah MD Chief Resident February 9,2018
 Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
UF HEALTH SHANDS CORE POLICY AND PROCEDURE. Stroke Alert Process
 UF HEALTH SHANDS CORE POLICY AND PROCEDURE POLICY NUMBER: CATEGORY: CP02.078 Patient Care TITLE: POLICY: PURPOSE: Stroke Alert Process Patients who present with or develop the cardinal signs of stroke
UF HEALTH SHANDS CORE POLICY AND PROCEDURE POLICY NUMBER: CATEGORY: CP02.078 Patient Care TITLE: POLICY: PURPOSE: Stroke Alert Process Patients who present with or develop the cardinal signs of stroke
Stroke Systems of Care. Sharon Webb, MD, FAANS, FACS, FAHA
 Stroke Systems of Care Sharon Webb, MD, FAANS, FACS, FAHA Disclosures No Disclosures Objectives Describe Systems of Care Describe stroke levels of care Discuss SC stroke council state Initiatives What
Stroke Systems of Care Sharon Webb, MD, FAANS, FACS, FAHA Disclosures No Disclosures Objectives Describe Systems of Care Describe stroke levels of care Discuss SC stroke council state Initiatives What
Guideline scope Stroke and transient ischaemic attack in over 16s: diagnosis and initial management (update)
") NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Stroke and transient ischaemic attack in over s: diagnosis and initial management (update) 0 0 This will update the NICE on stroke and
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Stroke and transient ischaemic attack in over s: diagnosis and initial management (update) 0 0 This will update the NICE on stroke and
PATIENT S NOTES History and Physical Brain Attack Stroke
 UNIVERSITY HOSPITALS OF CLEVELAND PATIENT S NOTES History and Physical Brain Attack Stroke 040527.01 page 1 of 8 Name Hospital # Date Sex Age Dr. Service Division Rm No Date and Time: Current inpatient
UNIVERSITY HOSPITALS OF CLEVELAND PATIENT S NOTES History and Physical Brain Attack Stroke 040527.01 page 1 of 8 Name Hospital # Date Sex Age Dr. Service Division Rm No Date and Time: Current inpatient
ND STROKE Coordinators Case Studies. STEMI and Stroke Conference, Fargo, ND, August 5, 2014
 ND STROKE Coordinators Case Studies STEMI and Stroke Conference, Fargo, ND, August 5, 2014 STROKE Coordinator Case Study Essentia Health, Fargo Essentia Health Stroke Alert Process Within 24 hours of Last
ND STROKE Coordinators Case Studies STEMI and Stroke Conference, Fargo, ND, August 5, 2014 STROKE Coordinator Case Study Essentia Health, Fargo Essentia Health Stroke Alert Process Within 24 hours of Last
ACUTE ISCHEMIC STROKE. Current Treatment Approaches for Acute Ischemic Stroke
 ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
The Joint Commission: Comprehensive Overview of Advanced Stroke & Advance Heart Failure Programs
 The Joint Commission: Comprehensive Overview of Advanced Stroke & Advance Heart Failure Programs WA State Cardiac & Stroke Conference Brian R. Johnson, Ph.D. Associate Director Hospital Business Development
The Joint Commission: Comprehensive Overview of Advanced Stroke & Advance Heart Failure Programs WA State Cardiac & Stroke Conference Brian R. Johnson, Ph.D. Associate Director Hospital Business Development
Blood Pressure Management in Acute Ischemic Stroke
 Blood Pressure Management in Acute Ischemic Stroke Kimberly Clark, PharmD, BCCCP Clinical Pharmacy Specialist Critical Care, Greenville Health System Adjunct Assistant Professor, South Carolina College
Blood Pressure Management in Acute Ischemic Stroke Kimberly Clark, PharmD, BCCCP Clinical Pharmacy Specialist Critical Care, Greenville Health System Adjunct Assistant Professor, South Carolina College
Emergency Department Stroke Registry Indicator Specifications 2018 Report Year (07/01/2017 to 06/30/2018 Discharge Dates)
") 2018 Report Year (07/01/2017 to 06/30/2018 Discharge Dates) Summary of Changes I62.9 added to hemorrhagic stroke ICD-10-CM diagnosis code list (table 3) Measure Description Methodology Rationale Measurement
2018 Report Year (07/01/2017 to 06/30/2018 Discharge Dates) Summary of Changes I62.9 added to hemorrhagic stroke ICD-10-CM diagnosis code list (table 3) Measure Description Methodology Rationale Measurement
Disclosures/Relationships
 Book to Bedside: Develop an Acute Stroke Management Service Ethan Cumbler M.D. Assistant Professor Internal Medicine University of Colorado Hospital UCH Stroke Council 2009 Disclosures/Relationships Research
Book to Bedside: Develop an Acute Stroke Management Service Ethan Cumbler M.D. Assistant Professor Internal Medicine University of Colorado Hospital UCH Stroke Council 2009 Disclosures/Relationships Research
DRUG ALLERGIES WT: KG
 DRUG AND TREATMENT Available at: BMC-B BMC-D BMC-N BMC-S Vital Signs Vital Signs Q4H (DEF)* Q2H Q1H Vital Signs Orthostatic Activity Activity Bedrest, for 12 hours then Up ad lib (DEF)* Bedrest, for 24
DRUG AND TREATMENT Available at: BMC-B BMC-D BMC-N BMC-S Vital Signs Vital Signs Q4H (DEF)* Q2H Q1H Vital Signs Orthostatic Activity Activity Bedrest, for 12 hours then Up ad lib (DEF)* Bedrest, for 24
Standard Precautions Droplet Precautions Standard Precautions Contact Precautions Droplet Precautions Standard Precautions Neutropenic Precautions
 Unique Plan Description: Neurosurgery Subarachnoid Hemorrhage Admission Adult Plan Selection Display: Neurosurgery Subarachnoid Hemorrhage Admission Adult PlanType: Medical Version: 10 Begin Effective
Unique Plan Description: Neurosurgery Subarachnoid Hemorrhage Admission Adult Plan Selection Display: Neurosurgery Subarachnoid Hemorrhage Admission Adult PlanType: Medical Version: 10 Begin Effective
STROKE CARE FROM A NURSING PERSPECTIVE
 STROKE CARE FROM A NURSING PERSPECTIVE Debbie Summers MSN, RN, ACNS-BC, CNRN, SCRN Cardiovascular & Stroke Outcomes Research Saint Luke s Hospital Kansas City, MO OBJECTIVES Participant will: Review nursing
STROKE CARE FROM A NURSING PERSPECTIVE Debbie Summers MSN, RN, ACNS-BC, CNRN, SCRN Cardiovascular & Stroke Outcomes Research Saint Luke s Hospital Kansas City, MO OBJECTIVES Participant will: Review nursing
Mechanical thrombectomy in Plymouth. Will Adams. Will Adams
 Mechanical thrombectomy in Plymouth Will Adams Will Adams History Intra-arterial intervention 1995 (NINDS) iv tpa improved clinical outcome in patients treated within 3 hours of ictus but limited recanalisation
Mechanical thrombectomy in Plymouth Will Adams Will Adams History Intra-arterial intervention 1995 (NINDS) iv tpa improved clinical outcome in patients treated within 3 hours of ictus but limited recanalisation
ENDOVASCULAR THERAPIES FOR ACUTE STROKE
 ENDOVASCULAR THERAPIES FOR ACUTE STROKE Cerebral Arteriogram Cerebral Anatomy Cerebral Anatomy Brain Imaging Acute Ischemic Stroke (AIS) Therapy Main goal is to restore blood flow and improve perfusion
ENDOVASCULAR THERAPIES FOR ACUTE STROKE Cerebral Arteriogram Cerebral Anatomy Cerebral Anatomy Brain Imaging Acute Ischemic Stroke (AIS) Therapy Main goal is to restore blood flow and improve perfusion
Standardize comprehensive care of the patient with severe traumatic brain injury
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Endovascular Treatment for Acute Ischemic Stroke
 ular Treatment for Acute Ischemic Stroke Vishal B. Jani MD Assistant Professor Interventional Neurology, Division of Department of Neurology. Creighton University/ CHI health Omaha NE Disclosure None 1
ular Treatment for Acute Ischemic Stroke Vishal B. Jani MD Assistant Professor Interventional Neurology, Division of Department of Neurology. Creighton University/ CHI health Omaha NE Disclosure None 1
Acute Stroke Treatment Update for 2008
 Acute Stroke Treatment Update for 2008 * Michael R. Dobbs, MD Assistant Professor of Neurology, Preventive Medicine, and Graduate Center for Toxicology University of Kentucky College of Medicine The Stroke
Acute Stroke Treatment Update for 2008 * Michael R. Dobbs, MD Assistant Professor of Neurology, Preventive Medicine, and Graduate Center for Toxicology University of Kentucky College of Medicine The Stroke
Jointly provided by Potomac Center for Medical Education and Rockpointe Supported by an educational grant from Genentech, A Member of the Roche Group
 Jointly provided by Potomac Center for Medical Education and Rockpointe Supported by an educational grant from Genentech, A Member of the Roche Group Faculty Speakers Deepak L. Bhatt, MD, MPH, FACC, FAHA,
Jointly provided by Potomac Center for Medical Education and Rockpointe Supported by an educational grant from Genentech, A Member of the Roche Group Faculty Speakers Deepak L. Bhatt, MD, MPH, FACC, FAHA,
Controversies in Hemorrhagic Stroke Management. Sarah L. Livesay, DNP, RN, ACNP-BC, ACNS-BC Associate Professor Rush University
 Controversies in Hemorrhagic Stroke Management Sarah L. Livesay, DNP, RN, ACNP-BC, ACNS-BC Associate Professor Rush University Disclosures AHA/ASA Outline Blood pressure VTE Coagulopathy Early mobilization
Controversies in Hemorrhagic Stroke Management Sarah L. Livesay, DNP, RN, ACNP-BC, ACNS-BC Associate Professor Rush University Disclosures AHA/ASA Outline Blood pressure VTE Coagulopathy Early mobilization
Managing the Measures: A Serious Look at Key Abstraction Concepts for the Comprehensive Stroke (CSTK) Measure Set Session 2
 Measure Set Session 2") Managing the Measures: A Serious Look at Key Abstraction Concepts for the Comprehensive Stroke (CSTK) Measure Set Session 2 January 28, 2015 1 to 3 PM Central Time Continuing Education Credit This course
Managing the Measures: A Serious Look at Key Abstraction Concepts for the Comprehensive Stroke (CSTK) Measure Set Session 2 January 28, 2015 1 to 3 PM Central Time Continuing Education Credit This course
Advanced Stroke Care in the context of the Cardiovascular Patient
 EASTERN MAINE MEDICAL CENTER Advanced Stroke Care in the context of the Cardiovascular Patient Advancing Science in Cardiovascular Care Samoset Conference NOV 8, 2018 Dr. Gillian Gordon Perue Conflict
EASTERN MAINE MEDICAL CENTER Advanced Stroke Care in the context of the Cardiovascular Patient Advancing Science in Cardiovascular Care Samoset Conference NOV 8, 2018 Dr. Gillian Gordon Perue Conflict
Emergency Room Procedure The first few hours in hospital...
 Emergency Room Procedure The first few hours in hospital... ER 5 level Emergency Severity Index SOP s for Stroke Stroke = Level 2 Target Time = 1 Hour 10 min from door 2 Doctor 25 min from door 2 CT 60
Emergency Room Procedure The first few hours in hospital... ER 5 level Emergency Severity Index SOP s for Stroke Stroke = Level 2 Target Time = 1 Hour 10 min from door 2 Doctor 25 min from door 2 CT 60
Cerebrovascular Disease
 Cerebrovascular Disease I. INTRODUCTION Cerebrovascular disease (CVD) includes all disorders in which an area of the brain is transiently or permanently affected by ischemia or bleeding and one or more
Cerebrovascular Disease I. INTRODUCTION Cerebrovascular disease (CVD) includes all disorders in which an area of the brain is transiently or permanently affected by ischemia or bleeding and one or more
Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase <48h)
") Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase
Antithrombotic therapy in patients with transient ischemic attack / stroke (acute phase
Stroke Systems of Care Claire Corbett, MMS, NRP Manager of Neurodiagnostics and Stroke Center New Hanover Regional Medical Center. What do we know?
 Stroke Systems of Care Claire Corbett, MMS, NRP Manager of Neurodiagnostics and Stroke Center New Hanover Regional Medical Center What do we know? Stroke: Time is Brain Shorter onset to treatment times
Stroke Systems of Care Claire Corbett, MMS, NRP Manager of Neurodiagnostics and Stroke Center New Hanover Regional Medical Center What do we know? Stroke: Time is Brain Shorter onset to treatment times
: STROKE. other pertinent information such as recent trauma, illicit drug use, pertinent medical history or use of oral contraceptives.
 INTRODUCTION A cerebral vascular accident (CVA) or stroke is a lack of blood supply to the brain as a result of either ischemia or hemorrhage. 80% of CVAs are a result of ischemia (embolic or thrombotic)
INTRODUCTION A cerebral vascular accident (CVA) or stroke is a lack of blood supply to the brain as a result of either ischemia or hemorrhage. 80% of CVAs are a result of ischemia (embolic or thrombotic)
Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage. Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA
 Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA The traditional view: asah is a bad disease Pre-hospital mortality
Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA The traditional view: asah is a bad disease Pre-hospital mortality
Dawn Matherne Meyer PhD,RN,FNP-C. Assistant Professor University of California San Diego
 Dawn Matherne Meyer PhD,RN,FNP-C Assistant Professor University of California San Diego Evidence Based Care of the Stroke Patient: A Focus on Acute Treatment, BP Management, & Antiplatelets TIME IS BRAIN
Dawn Matherne Meyer PhD,RN,FNP-C Assistant Professor University of California San Diego Evidence Based Care of the Stroke Patient: A Focus on Acute Treatment, BP Management, & Antiplatelets TIME IS BRAIN
7/22/2016. Navaz Karanjia, MD. FINANCIAL DISCLOSURE: none. UNLABELED/UNAPPROVED USE DISCLOSURE: none
 Navaz Karanjia, MD Director of Neurocritical Care Assistant Professor of Neurosciences, Neurosurgery, and Anesthesiology University of California-San Diego Health System Navaz Karanjia, MD FINANCIAL DISCLOSURE:
Navaz Karanjia, MD Director of Neurocritical Care Assistant Professor of Neurosciences, Neurosurgery, and Anesthesiology University of California-San Diego Health System Navaz Karanjia, MD FINANCIAL DISCLOSURE:
Clinical Guidelines for Stroke Management 2017 Summary Nursing
 Clinical Guidelines for Stroke Management 2017 Summary Nursing This summary is a quick reference to the recommendations in the Clinical Guidelines for Stroke Management 2017 most relevant to nurses. While
Clinical Guidelines for Stroke Management 2017 Summary Nursing This summary is a quick reference to the recommendations in the Clinical Guidelines for Stroke Management 2017 most relevant to nurses. While
New Frontiers in Intracerebral Hemorrhage
 New Frontiers in Intracerebral Hemorrhage Ryan Hakimi, DO, MS Director, Neuro ICU Director, Inpatient Neurology Services Greenville Health System Clinical Associate Professor Department of Medicine (Neurology)
New Frontiers in Intracerebral Hemorrhage Ryan Hakimi, DO, MS Director, Neuro ICU Director, Inpatient Neurology Services Greenville Health System Clinical Associate Professor Department of Medicine (Neurology)
Hypertensive Haemorrhagic Stroke. Dr Philip Lam Thuon Mine
 Hypertensive Haemorrhagic Stroke Dr Philip Lam Thuon Mine Intracerebral Haemorrhage Primary ICH Spontaneous rupture of small vessels damaged by HBP Basal ganglia, thalamus, pons and cerebellum Amyloid
Hypertensive Haemorrhagic Stroke Dr Philip Lam Thuon Mine Intracerebral Haemorrhage Primary ICH Spontaneous rupture of small vessels damaged by HBP Basal ganglia, thalamus, pons and cerebellum Amyloid
Acute Stroke Rescue and Recovery
 Acute Stroke Rescue and Recovery Qaisar A. Shah, MD Director, Neurointerventional and Neurocritical care Nancy Arena Gogal,, RN Manager Cath/EPS/Neuro lab AMH Stroke Program Evolution 1997: Stroke Program
Acute Stroke Rescue and Recovery Qaisar A. Shah, MD Director, Neurointerventional and Neurocritical care Nancy Arena Gogal,, RN Manager Cath/EPS/Neuro lab AMH Stroke Program Evolution 1997: Stroke Program
IDPH EMS Region Five. Stroke Education
 IDPH EMS Region Five Stroke Education Time is Brain!!!!! Time is Brain!!!! Stroke refers to any spontaneous damage to the brain caused by an abnormality of the blood supply by means of a clot or bleed.
IDPH EMS Region Five Stroke Education Time is Brain!!!!! Time is Brain!!!! Stroke refers to any spontaneous damage to the brain caused by an abnormality of the blood supply by means of a clot or bleed.
Alex Abou-Chebl, MD Associate Professor of Neurology and Neurosurgery Director of Neurointerventional Services Director of Vascular and
 Alex Abou-Chebl, MD Associate Professor of Neurology and Neurosurgery Director of Neurointerventional Services Director of Vascular and Interventional Neurology Fellowships University of Louisville School
Alex Abou-Chebl, MD Associate Professor of Neurology and Neurosurgery Director of Neurointerventional Services Director of Vascular and Interventional Neurology Fellowships University of Louisville School
Modern Management of ICH
 Modern Management of ICH Bradley A. Gross, MD Assistant Professor, Dept of Neurosurgery, University of Pittsburgh October 2018 ICH Background Assessment & Diagnosis Medical Management Surgical Management
Modern Management of ICH Bradley A. Gross, MD Assistant Professor, Dept of Neurosurgery, University of Pittsburgh October 2018 ICH Background Assessment & Diagnosis Medical Management Surgical Management
Mark J. Alberts, MD, FAHA, FANA Vice-Chair, Dept of Neurology Professor of Neurology UT Southwestern Medical Center Dallas, TX
 Interventional Therapies for Cerebrovascular Diease: The Good, The Bad, The Needed, and The Few 1 Mark J. Alberts, MD, FAHA, FANA Vice-Chair, Dept of Neurology Professor of Neurology UT Southwestern Medical
Interventional Therapies for Cerebrovascular Diease: The Good, The Bad, The Needed, and The Few 1 Mark J. Alberts, MD, FAHA, FANA Vice-Chair, Dept of Neurology Professor of Neurology UT Southwestern Medical
Stroke Transfer Checklist
 Stroke Transfer Checklist When preparing to transfer an acute stroke patient to the UF Health Shands Comprehensive Stroke Center, please make every attempt to include the following information: Results
Stroke Transfer Checklist When preparing to transfer an acute stroke patient to the UF Health Shands Comprehensive Stroke Center, please make every attempt to include the following information: Results
Department Specific Guideline
 Department Specific Guideline Stroke/TIA Management ED Applicable to: Nursing/Medical staff caring Authorised by: Stroke services team for Acute stroke/tia patients Contact person: Clinical nurse manager,
Department Specific Guideline Stroke/TIA Management ED Applicable to: Nursing/Medical staff caring Authorised by: Stroke services team for Acute stroke/tia patients Contact person: Clinical nurse manager,
Door to Needle Time: Gold Standard of Stroke Treatment Fatima Milfred, MD. Virginia Mason Medical Center March 16, 2018
 Door to Needle Time: Gold Standard of Stroke Treatment Fatima Milfred, MD Virginia Mason Medical Center March 16, 2018 2016 Virginia Mason Medical Center No disclosure 2016 Virginia Mason Medical Center
Door to Needle Time: Gold Standard of Stroke Treatment Fatima Milfred, MD Virginia Mason Medical Center March 16, 2018 2016 Virginia Mason Medical Center No disclosure 2016 Virginia Mason Medical Center
Stroke: What did we learn in the last year?
 Stroke: What did we learn in the last year? J. Claude Hemphill III, MD, MAS Associate Professor of Clinical Neurology and Neurological Surgery University of California, San Francisco Director, Neurocritical
Stroke: What did we learn in the last year? J. Claude Hemphill III, MD, MAS Associate Professor of Clinical Neurology and Neurological Surgery University of California, San Francisco Director, Neurocritical
framework for flow Objectives Acute Stroke Treatment Collaterals in Acute Ischemic Stroke framework & basis for flow
 Acute Stroke Treatment Collaterals in Acute Ischemic Stroke Objectives role of collaterals in acute ischemic stroke collateral therapeutic strategies David S Liebeskind, MD Professor of Neurology & Director
Acute Stroke Treatment Collaterals in Acute Ischemic Stroke Objectives role of collaterals in acute ischemic stroke collateral therapeutic strategies David S Liebeskind, MD Professor of Neurology & Director
Tony L Smith DNP RN ACNP CCRN CFRN EMT-IV Vanderbilt LifeFlight
 Treatment of a Stroke patient: A look at how to care for the Stroke patient in the aeromedical setting Tony L Smith DNP RN ACNP CCRN CFRN EMT-IV Vanderbilt LifeFlight Objectives 1. Discuss the assessment
Treatment of a Stroke patient: A look at how to care for the Stroke patient in the aeromedical setting Tony L Smith DNP RN ACNP CCRN CFRN EMT-IV Vanderbilt LifeFlight Objectives 1. Discuss the assessment
Blood Pressure Management in Acute Stroke. Bradley Molyneaux, M.D., Ph.D. Departments of Neurology & Critical Care Medicine University of Pittsburgh
 Blood Pressure Management in Acute Stroke Bradley Molyneaux, M.D., Ph.D. Departments of Neurology & Critical Care Medicine University of Pittsburgh 80 yo M w/ R MCA syndrome NIHSS 14 A balancing act Cerebral
Blood Pressure Management in Acute Stroke Bradley Molyneaux, M.D., Ph.D. Departments of Neurology & Critical Care Medicine University of Pittsburgh 80 yo M w/ R MCA syndrome NIHSS 14 A balancing act Cerebral
Acute Stroke with Alteplase Administration Order Set
 Review Due Date: 2017 October PATIENT CARE DERS Weight: Adverse Reactions or Intolerances Drug No Yes (list) Food No Yes (list) _ Latex No Yes Admission Admit to Neurology service: Dr. Critical Care Diagnosis:
Review Due Date: 2017 October PATIENT CARE DERS Weight: Adverse Reactions or Intolerances Drug No Yes (list) Food No Yes (list) _ Latex No Yes Admission Admit to Neurology service: Dr. Critical Care Diagnosis:
Management of Acute Ischemic Stroke. Learning Objec=ves. What is a Stroke? Jen Simpson Neurohospitalist
 Management of Acute Ischemic Stroke Jen Simpson Neurohospitalist Learning Objec=ves Iden=fy signs/symptoms of stroke Recognize pa=ents who may be eligible for treatment of acute stroke What is a Stroke?
Management of Acute Ischemic Stroke Jen Simpson Neurohospitalist Learning Objec=ves Iden=fy signs/symptoms of stroke Recognize pa=ents who may be eligible for treatment of acute stroke What is a Stroke?
9/18/16. Management of Ischemic Stroke in the Intensive Care Unit. Outline. Introduction. Kyle B Walsh MD. Phases of Stroke Diagnosis and Treatment
 Management of Ischemic Stroke in the Intensive Care Unit Kyle B Walsh MD Assistant Professor - UC Dept of Emergency Medicine Fellow Physician - Neurocritical Care, Stroke, Research Outline Why ICU care
Management of Ischemic Stroke in the Intensive Care Unit Kyle B Walsh MD Assistant Professor - UC Dept of Emergency Medicine Fellow Physician - Neurocritical Care, Stroke, Research Outline Why ICU care