Paediatric Lung Transplantation
|
|
|
- Gerard Daniels
- 5 years ago
- Views:
Transcription
1 Paediatric Lung Transplantation Cross Canada Rounds Dr. Lucy Perrem Respiratory Medicine Fellow Dec 21 st 2017
2 Objectives 1. Overview of paediatric lung transplantation 2. Discuss acute management and complications in context of recent cases in HSC
3 Incidence Goldfarb S et al, J Heart Lung Transplant, 2015; Sweet S, Resp Care 2017

4 Indications ISHLT registry data Sweet S, Respiratory Care, 2017
5 Contraindications Faro et al, Am J Transplant 2007; Sweet S, Resp Care 2017

6 Contraindications Faro et al, Am J Transplant 2007; Sweet S, Resp Care 2017
7 Survival Goldfarb S et al, J Heart Lung Transplant, 2015
8 Case 1

9 NS 12 year old Idiopathic pulmonary arterial hypertension (dx age 6)
 Group 5 PH due to unclear multifactorial")
10 Pulmonary Hypertension mean pulmonary artery pressure 25 mmhg at rest (WHO) Group 1 Pulmonary arterial hypertension (PAH) Group 2 PH due to left heart disease Group 3 PH due to chronic lung disease and/or hypoxemia Group 4 Chronic thromboembolic pulmonary hypertension (CTEPH) Group 5 PH due to unclear multifactorial mechanisms
11
12
13 NS 12 year old Idiopathic pulmonary arterial hypertension Rx: Treprostinil (Remodulin ) s/c continuous infusion Tadalafil (Adcirca ) 40mg daily Macitentan (Opsumit ) 10mg PO daily Oxygen 1.5L/min (nocturnal + with exercise) Listed Feb 2016
14 NS 12 year old Symptoms++ Echo: Severely dilated and severely reduced RV systolic fxn. RVSp > 2/3 rd systemic pressure (78mmHg) ECG: : Biatrial enlargement. right ventricular hypertrophy.


15 NS 12 year old Transplanted Aug 2017 Pre-op exam: HR108 RR18 BP96/57 SpO2 96% CVS: Increased JVP, Loud P2. Normal pulses, CRT<2sec, no peripheral edema Resp: equal a/e bilat, no adventitious sounds GIT: SNT, no HSM

16 Double Lung Transplant Bilateral sequential lung transplant with end-toend bronchial to bronchial anastomosis - on ECMO
17 Double Lung Transplant Bilateral sequential lung transplant with end-to-end bronchial to bronchial anastomosis - on ECMO Virtual crossmatch positive, high PRAs
18 Preventing hyperacute rejection Step 1 - Virtual crossmatch screening for the presence of recipient pre-formed anti-hla antibodies to the prospective donor HLA type. decision to proceed with transplant Step 2 - An actual crossmatch with donor cells and recipient serum (flow cytometry) Usually resulted AFTER transplant
19 Double Lung Transplant Bilateral sequential lung transplant with end-to-end bronchial to bronchial anastomosis - on ECMO Virtual crossmatch positive, high PRAs Receives plasmapheresis in OR Receives plasmapheresis in ICU Then actual crossmatch negative. No DSAs detected


20 Double Lung Transplant Triple immunosuppression: IS: Prednisone, tacrolimus, MMF
21 Double Lung Transplant Treated with pip-tazobactam for donor +ve staph aureus and E. Coli RLL consolidation - donor consolidation EBV: D+/R+ and CMV: D-/R- Candida prophylaxis

22 Double Lung Transplant Leaves hospital on day 14.

23 Complications

24 Sweet S et al. Pediatric Lung Transplantation. In Kendig and Chernick s Disorders of the Respiratory Tract in Children. 8th Ed. 2006
25 Post-transplant phase 1) Surgical Bleeding anastomotic and non-anastomotic airway stenosis anastomotic dehiscence lobar torsion Pneumothorax Nerve injury Phrenic nerve Recurrent laryngeal nerve Vagus nerve Tejwani V, et al.. Chest Grasemann H, et al. Springer International (in press)
26 Immediate/Early Complications 1) Surgical Bleeding anastomotic and non-anastomotic airway stenosis anastomotic dehiscence lobar torsion pneumothorax Phrenic nerve injury Vagus nerve injury 2) Primary Graft Dysfunction w/i 72h ischemia-reperfusion injury dx exclusion Tejwani V, et al.. Chest Grasemann H, et al. Springer International (in press)
27 Immediate/Early Complications 3) Immunological complications Hyperacute rejection Acute cellular rejection Antibody mediated rejection Tejwani V, et al.. Chest Grasemann H, et al. Early Postoperative Management, Springer International (in press)
28 Immediate/Early Complications 3) Immunological complications Hyperacute rejection Acute cellular rejection Antibody mediated rejection 4) Infectious complications Bacterial/ Viral CMV EBV Herpes Fungal Aspergillus Candida PCP Tejwani V, et al.. Chest Grasemann H, et al. Early Postoperative Management, Springer International (in press) Sweet C, Resp Care. 2017
29 Immediate/Early Complications 5) Iatrogenic Transfusion related acute lung injury Medication SE Diabetes Renal impairment Neurological complications Leukopenia De Perrot et al, Am J Crit Care Med. 2003
30 Immediate/Early Complications 5) Iatrogenic Transfusion related acute lung injury Medication SE 6) Other Pulmonary edema pulmonary arterial or venous thrombus Donor lung injury Pulmonary aspiration Gastroparesis/GIT dysmotility SVT De Perrot et al, Am J Crit Care Med. 2003
 Respiratory distress Reduce air entry on the right WCC 46 x 10^9/L CRP 32 mg/l Rx: Pip/taz &")
31 Sept 5 Returns to clinic 5 days post discharge: c/o SOB, cough, chest pain, asking for oxygen O/E: Hypoxemia 78% room air (SpO2 90% in 100% O2) Respiratory distress Reduce air entry on the right WCC 46 x 10^9/L CRP 32 mg/l Rx: Pip/taz & Vancomycin
32 Sept 5 Chest tube placed Bronchoscopy: Yellow secretions in right main stem bronchus Anastomosis in tact BAL sent (x1 dose abx before BAL)
33 Sept 6 Intubated in the ICU FiO2 100% BAL from Sept 5 still negative for infection
34 Question: Next steps? A) Empirical treatment with Pulse IV Methylprednisolone B) Trans-bronchial biopsies and then Pulse IV MP for ACR C) Plasmapheresis D) Continue current management while awaiting complete BAL cultures
35 Question: Next step? A) Empirical treatment with IV Methylprednisolone B) Transbronchial biopsies and then IV Methylprednisolone for ACR C) Plasmapheresis D) Continue current management while awaiting complete BAL cultures

36 Sept 6 Once stabilized: Insertion of surgical chesttube Vancomycin stopped, Pip/taz continued
37 Sept 7-8 Initial response to treatment with decreased FiO2 from 100% to 60% Extubated but requiring BIPAP and increasing FIO2 requirement Preliminary tbbx report suggestive of infection with ++neutrophils in airways EBV/CMV/fungal/adeno stains negative Antibiotics coverage broadened vancomycin, meropenam, azithromycin

38 Sept 9-10 Clinical deterioration PRAs sent urgently Received Plasmapheresis while waiting results Clinical response FiO2 90%, decreased to 60%
39 +DSAs A1 and A24 saturated (had historic weak A24) Path report Diffuse and organizing alveolar damage. Multiple distinct foci of dense perivascular mononuclear infiltrates, no capillaritis. indicative of grade A4 acute cellular rejection. Mucopururlent exudate in large airways and large airway inflammation suspicious for co-existing infection In the presence of DSAs the biopsy findings could be consistent with antibody-mediated rejection. (despite negative C4d staining)

40 5 day course of plasmapheresis with IVIG at end Increased dose of MMF Improving bilateral airspace opacification Monthly IVIg and rituximab Ongoing close monitoring of PRAs

41 REJECTION
42 Hyperacute rejection Hyperacute rejection within hours Rare, potentially catastrophic Circulating pre-formed recipient antibodies that bind to donor human leukocyte antigen (HLA) molecules on vascular endothelium, leading to vascular damage, obstruction and severe graft ischemia. Pre-op screening with virtual cross-match Sweet S and Noyes B Paediatric Lung Transplantation. In Kendig and Cherneck s Disorders of the Respiratory Tract in Children. 8th Ed.
43 Acute Cellular Rejection ACR occurs when recipient lymphocytes react with donor antigens Majority of lung transplant recipients, most common in first 3m Low early mortality but most significant RF for CLAD Non-specific clinical presentation hypoxia, fever, cough, new infiltrates, obstructive pattern on PFTs Can occur as early as one week and up to 2-3 years post Surveillance bronchs for subclinical rejection controversial Grade A2 and above Rx: Pulse Methylprednisolone x3 days Husain AN et al. Archives of pathology & laboratory medicine. 2016
 to severe (A4) Husain AN et al.")
44 Histologically perivascular lymphocytic infiltrates with or without airway inflammation standardized scoring none (A0) to severe (A4) Husain AN et al. Archives of pathology & laboratory medicine. 2016
45 Antibody Mediated Rejection Development of DSA s can lead to AMR AMR vs. ACR vs infection?? multidisciplinary approach to diagnosis: Clinical allograft dysfunction (can be subclinical) Circulating DSA s Pathological findings (TBBx) +/- complement 4d within the graft (C4d staining) AMR = driver of both acute and chronic lung allograft dysfunction (CLAD). No consensus on treatment strategies
46 Case 2 Consent
47 EE 3 year old boy B/G 1. Ex 37/40, MAS and NAIT in neonatal period 2. Group A Sepsis (age 2) 3. Recurrent RTI 4. Asthma 5. Mild Developmental delay

48 EE Aug 2016 Presented to ED with haematemesis GI scope In PACU frank blood in ETT Transferred to PICU I+V Bronchoscopy confirmed blood in airways
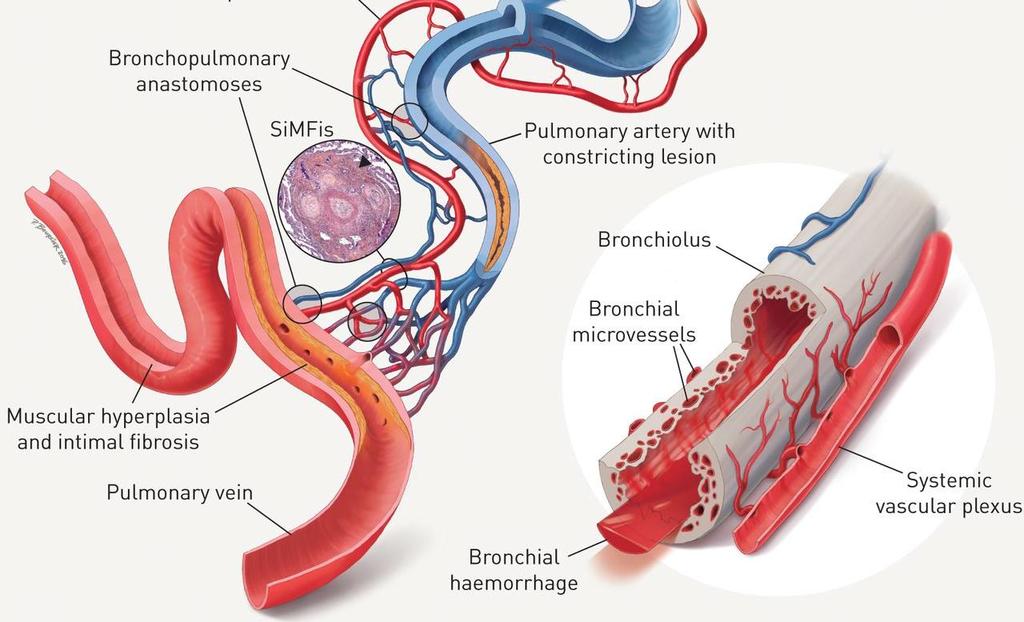
49 EE 3 year old boy CT Chest severe PVS, dilated pulmonary arteries and right ventricular hypertrophy. Ground glass opacities in RLL?fibrosing mediastinitis?primary or secondary PVS Echo: Pulmonary HTN, mildly dilated RV, RVH Good BV function (no PHTn on echo in 2015)

 limited")

50 EE 3 year old boy Rx: multiple catheter interventions with balloon dilations, ASD creation Listed for Lung transplant Jan 2017 Sutureless repair of the R pulmonary veins ( ). Residual pulmonary vein stenosis post repair on CT ( ) limited response to procedures Relisted for lung transplant Treated with daily corticosteroids for unknown but potentially inflammatory aetiology July RVSp 61% systemic measured

51 EE Day 0 Donor: RLL consolidation Donor lungs underwent EVLP for borderline status CMV neg, EBV neg Transplant Uneventful ECMO - 3h Stable vascular and bronchial anastomosis on intra-op bronchoscopy Chest tubes x6

52 ACTIVATION OF INFLAMMATORY PARMAMETERS De Perrot et al. Am J Crit Care Med. 2003
 compared to 30%")
 Transplantation of high-risk donor lungs that were physiologically stable during 4 hours of ex vivo perfusion led to")
53 Lungs perfused and ventilated ex-vivo at body temperature to mimic physiological conditions for 4hours If PaO2:FIO2 ratio >=350mmHg lungs considered suitable for transplant The incidence of Grade 2 or 3 PGD at 72h was 15% (n=20) compared to 30% (n=116) in the control group (p=0.11) Transplantation of high-risk donor lungs that were physiologically stable during 4 hours of ex vivo perfusion led to results similar to those obtained with conventionally selected lungs. Cypel M et al. NEJM, 2011
 Immunosuppression with IV Methylprednisolone, tacrolimus and")
54 EE Day 1 Hemodynamic instability inotropes Hypoxia PS18 PEEP 10cmH20 50% ino Donor BAL growing Staph Aureus (Rx Pip/taz & Vanco) Immunosuppression with IV Methylprednisolone, tacrolimus and MMF
55 Worsening pulmonary infiltrates Day 2 Day 3
56 Aetiology of pulmonary infiltrates? A) Pulmonary edema B) Infection C) Donor lung injury D) Right ventricular dysfunction E) Hyperacute cellular rejection

57 EE Day 4 Aggressive diuresis and fluid restriction Echo - RVSp 18mmHg + CVP 15cmH20 Inotropes stopped ino weaned and discontinued Vancomycin stopped (MSSA)
58 Aetiology of pulmonary infiltrates? A) Pulmonary edema B) Infection C) Donor lung injury D) Primary graft dysfunction E) Acute cellular rejection
59 Pulmonary edema Pulmonary edema common occurrence due to increased vascular permeability and severed lymphatics Management Minimize pulmonary capillary wedge pressure and central venous pressure Fluid restriction, diuresis, ino, milrinone Balanced with need to maintain systemic pressure inotropes Yeung JC et al. Cold Spring Harbor perspectives in medicine. 2014; 4:a015628
60 Primary Graft Dysfunction The expression of all the injury in the donor through to the time of reperfusion. Manifests as hypoxemia in the presence of radiographic infiltrates Typically airspace consolidation or interstitial opacities in the perihilar or basilar regions Clinically defined - ISHLT Syndrome occurring within 72 hours post lung transplant, characterized clinically by pulmonary edema and pathologically by non-specific diffuse alveolar damage Christie JD et al. The Journal of heart and lung transplantation. 2005; 24: De Perrot M et al. Am Jour Cri Care Med ;
61 Mimics Diagnosis of exclusion Cardiac dysfunction Pulmonary aspiration Infection Fluid overload Pulmonary venous outflow obstruction obstruction Antibody mediated rejection
62 PGD Overall incidence approximately 10% Grading system Graded 0-3 by the presence of radiographic infiltrates consistent with pulmonary edema and reduced oxygenation index (Pa)2/fraction of inspired O2) <300 or <200 depending on severity Christie JD et al. The Journal of heart and lung transplantation. 2005; 24:1454-9
63 PGD Treatment is supportive Intensified mechanical ventilation Inhaled Nitric Oxide Improves V/Q mismatch as NO delivered to ventilated alveoli Anti-inflammatory properties Extra-corporeal life support (ECLS) / interventional lung assist (ila) bridge to recovery Yeung JC, et al. Cold Spring Harbor perspectives in medicine. 2014; 4:a015628
64 PGD - Prognosis Significance Decreased 30 day mortality - 42% versus 6% for patients without PGD PGD contributes to nearly half of the short-term mortality after lung transplantation. Survivors of primary graft dysfunction have increased risk of death extending beyond the first post-transplant year. Increased risk of chronic allograft dysfunction Samano M, et al. Elsevier; 2012 Yeung JC, et al Cold Spring Harbor perspectives in medicine Christie JD, et al. American journal of respiratory and critical care medicine. 2005
65 EE multiple pulmonary complications Donor Lung injury (RLL consolidation) Infection (donor BAL +) Pulmonary edema Presumed acute cellular rejection Pulmonary aspiration Phrenic nerve injury
66 Summary Viable option for treatment of end-stage lung disease despite multiple complications many of which can occur in the same patient The donor pool is a limiting factor but can be improved by EVLP
Antibody-Mediated Rejection in the Lung Allograft. Gerald J Berry, MD Dept of Pathology Stanford University Stanford, CA 94305
 Antibody-Mediated Rejection in the Lung Allograft Gerald J Berry, MD Dept of Pathology Stanford University Stanford, CA 94305 Gerald J Berry, MD Professor of Pathology Stanford University, Stanford, CA
Antibody-Mediated Rejection in the Lung Allograft Gerald J Berry, MD Dept of Pathology Stanford University Stanford, CA 94305 Gerald J Berry, MD Professor of Pathology Stanford University, Stanford, CA
ACUTE RESPIRATORY DISTRESS SYNDROME
 ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
Marcelo Cypel MD MSc
 Ex vivo Organ Repair Marcelo Cypel MD MSc Canada Research Chair in Lung Transplantation Surgical Director ECLS Program UHN Assistant Professor of Surgery Division of Thoracic Surgery University Health
Ex vivo Organ Repair Marcelo Cypel MD MSc Canada Research Chair in Lung Transplantation Surgical Director ECLS Program UHN Assistant Professor of Surgery Division of Thoracic Surgery University Health
Antibody Mediated Rejection (AMR) in LUNG TRANSPLANT Recipients
 in LUNG TRANSPLANT Recipients") Antibody Mediated Rejection (AMR) in LUNG TRANSPLANT Recipients Lorriana Leard, MD UCSF Transplant Pulmonologist Associate Professor of Clinical Medicine Vice Chief of Clinical Activities Pulmonary, Critical
Antibody Mediated Rejection (AMR) in LUNG TRANSPLANT Recipients Lorriana Leard, MD UCSF Transplant Pulmonologist Associate Professor of Clinical Medicine Vice Chief of Clinical Activities Pulmonary, Critical
ARDS: an update 6 th March A. Hakeem Al Hashim, MD, FRCP SQUH
 ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
Optimizing the Donor Lung with EVLP
 Optimizing the Donor Lung with EVLP Marcelo Cypel MD MSc FRCSC Canada Research Chair in Lung Transplantation Surgical Director ECLS Lung Program UHN Associate Professor of Surgery Division of Thoracic
Optimizing the Donor Lung with EVLP Marcelo Cypel MD MSc FRCSC Canada Research Chair in Lung Transplantation Surgical Director ECLS Lung Program UHN Associate Professor of Surgery Division of Thoracic
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv
 Rv") ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
Transplant in Pediatric Heart Failure
 Transplant in Pediatric Heart Failure Francis Fynn-Thompson, MD Co-Director, Center for Airway Disorders Surgical Director, Pediatric Mechanical Support Program Surgical Director, Heart and Lung Transplantation
Transplant in Pediatric Heart Failure Francis Fynn-Thompson, MD Co-Director, Center for Airway Disorders Surgical Director, Pediatric Mechanical Support Program Surgical Director, Heart and Lung Transplantation
06/04/2013 ISHLT. 2 International Conference on Respiratory Physiotherapy ARIR Genova, March 21 23, 2013
 LUNG TRANSPLANTS The Journal of Heart and Lung Transplantation, 2012 2 International Conference on Respiratory Physiotherapy ARIR Genova, March 21 23, 2013 LUNG TRANSPLANTATION:STATE OF THE ART L. Santambrogio
LUNG TRANSPLANTS The Journal of Heart and Lung Transplantation, 2012 2 International Conference on Respiratory Physiotherapy ARIR Genova, March 21 23, 2013 LUNG TRANSPLANTATION:STATE OF THE ART L. Santambrogio
Topics to Cover. Post-op Management of Heart and Lung Transplants. Graft Dysfunction (Heart) Hemodynamic Instability. Hemodynamic Instability
 Hemodynamic Instability. Hemodynamic Instability") Topics to Cover Post-op Management of Heart and Lung Transplants Lundy J. Campbell MD Hemodynamic Instability Causes / treatment Pulmonary HTN / RV failure Pulmonary vasodilators Mechanical ventilation
Topics to Cover Post-op Management of Heart and Lung Transplants Lundy J. Campbell MD Hemodynamic Instability Causes / treatment Pulmonary HTN / RV failure Pulmonary vasodilators Mechanical ventilation
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Cypel M, Yeung JC, Liu M, et al. Normothermic ex vivo lung
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Cypel M, Yeung JC, Liu M, et al. Normothermic ex vivo lung
Lung Allograft Dysfunction
 Lung Allograft Dysfunction Carlos S. Restrepo M.D. Ameya Baxi M.D. Department of Radiology University of Texas Health San Antonio Disclaimer: We do not have any conflict of interest or financial gain to
Lung Allograft Dysfunction Carlos S. Restrepo M.D. Ameya Baxi M.D. Department of Radiology University of Texas Health San Antonio Disclaimer: We do not have any conflict of interest or financial gain to
CASE PRESENTATION VV ECMO
 CASE PRESENTATION VV ECMO Joshua Huelster, MD Fellow in Critical Care Medicine Department of Pulmonary and Critical Care Medicine Hennepin County Medical Center Disclosure There are no conflicts of interest
CASE PRESENTATION VV ECMO Joshua Huelster, MD Fellow in Critical Care Medicine Department of Pulmonary and Critical Care Medicine Hennepin County Medical Center Disclosure There are no conflicts of interest
Case Study #2. Case Study #1 cont 9/28/2011. CAPA 2011 Christy Wilson PA C. LH is 78 yowf with PMHx of metz breast CA presents
 Case Study #1 CAPA 2011 Christy Wilson PA C 46 yo female presents with community acquired PNA (CAP). Her condition worsened and she was transferred to the ICU and placed on mechanical ventilation. Describe
Case Study #1 CAPA 2011 Christy Wilson PA C 46 yo female presents with community acquired PNA (CAP). Her condition worsened and she was transferred to the ICU and placed on mechanical ventilation. Describe
ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate. Carolyn Calfee, MD MAS Mark Eisner, MD MPH
 ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate Carolyn Calfee, MD MAS Mark Eisner, MD MPH June 3, 2010 Case Presentation Setting: Community hospital, November 2009 29 year old woman with
ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate Carolyn Calfee, MD MAS Mark Eisner, MD MPH June 3, 2010 Case Presentation Setting: Community hospital, November 2009 29 year old woman with
The multidisciplinary approach to AMR in lung transplantation: Reaching a consensus. Deborah Jo Levine Professor of Medicine University of Texas
 The multidisciplinary approach to AMR in lung transplantation: Reaching a consensus Deborah Jo Levine Professor of Medicine University of Texas Disclosures I have no financial relations with any relevant
The multidisciplinary approach to AMR in lung transplantation: Reaching a consensus Deborah Jo Levine Professor of Medicine University of Texas Disclosures I have no financial relations with any relevant
9/5/2018. Conflicts of Interests. Pediatric Acute Respiratory Distress Syndrome. Objectives ARDS ARDS. Definitions. None
 Pediatric Acute Respiratory Distress Syndrome Conflicts of Interests Diane C Lipscomb, MD Director Inpatient Pediatric Medical Director Mercy Springfield Associate Clerkship Clinical Director University
Pediatric Acute Respiratory Distress Syndrome Conflicts of Interests Diane C Lipscomb, MD Director Inpatient Pediatric Medical Director Mercy Springfield Associate Clerkship Clinical Director University
Solid Organ Transplant
 Solid Organ Transplant Lee R. Goldberg, MD, MPH, FACC Associate Professor of Medicine Medical Director, Heart Failure and CardiacTransplant Program University of Pennsylvania Disclosures Thoratec Consulting
Solid Organ Transplant Lee R. Goldberg, MD, MPH, FACC Associate Professor of Medicine Medical Director, Heart Failure and CardiacTransplant Program University of Pennsylvania Disclosures Thoratec Consulting
EDUCATIONAL COMMENTARY TRANSFUSION-RELATED ACUTE LUNG INJURY
 EDUCATIONAL COMMENTARY TRANSFUSION-RELATED ACUTE LUNG INJURY Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE
EDUCATIONAL COMMENTARY TRANSFUSION-RELATED ACUTE LUNG INJURY Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE
Acute Respiratory Distress Syndrome (ARDS) An Update
 An Update") Acute Respiratory Distress Syndrome (ARDS) An Update Prof. A.S.M. Areef Ahsan FCPS(Medicine) MD(Critical Care Medicine) MD ( Chest) Head, Dept. of Critical Care Medicine BIRDEM General Hospital INTRODUCTION
Acute Respiratory Distress Syndrome (ARDS) An Update Prof. A.S.M. Areef Ahsan FCPS(Medicine) MD(Critical Care Medicine) MD ( Chest) Head, Dept. of Critical Care Medicine BIRDEM General Hospital INTRODUCTION
Managing an Organ - New Therapies
 Managing an Organ - New Therapies Marcelo Cypel MD MSc Canada Research Chair in Lung Transplantation Surgical Director, ECLS program UHN Assistant Professor of Surgery Division of Thoracic Surgery University
Managing an Organ - New Therapies Marcelo Cypel MD MSc Canada Research Chair in Lung Transplantation Surgical Director, ECLS program UHN Assistant Professor of Surgery Division of Thoracic Surgery University
Index. Note: Page numbers of article titles are in boldface type
 Index Note: Page numbers of article titles are in boldface type A Acute coronary syndrome, perioperative oxygen in, 599 600 Acute lung injury (ALI). See Lung injury and Acute respiratory distress syndrome.
Index Note: Page numbers of article titles are in boldface type A Acute coronary syndrome, perioperative oxygen in, 599 600 Acute lung injury (ALI). See Lung injury and Acute respiratory distress syndrome.
Evolution of Surgical Therapies for End-Stage Cardiopulmonary Failure. Heart Failure at the Shoe XI October 5, 2012
 Evolution of Surgical Therapies for End-Stage Cardiopulmonary Failure Heart Failure at the Shoe XI October 5, 2012 Robert S.D. Higgins, MD, MSHA Executive Director, Comprehensive Transplant Center Evolution
Evolution of Surgical Therapies for End-Stage Cardiopulmonary Failure Heart Failure at the Shoe XI October 5, 2012 Robert S.D. Higgins, MD, MSHA Executive Director, Comprehensive Transplant Center Evolution
3/6/2017. Prevention of Complement Activation and Antibody Development: Results from the Duet Trial
 Prevention of Complement Activation and Antibody Development: Results from the Duet Trial Jignesh Patel MD PhD FACC FRCP Medical Director, Heart Transplant Cedars-Sinai Heart Institute Disclosures Name:
Prevention of Complement Activation and Antibody Development: Results from the Duet Trial Jignesh Patel MD PhD FACC FRCP Medical Director, Heart Transplant Cedars-Sinai Heart Institute Disclosures Name:
No evidence of C4d association with AMR However, C3d and AMR correlated well
 C4d positivity Poor prognostic factor Reversal to C4d negativity did not change prognosis, with current therapy Prognostic factor for CAV Variable time line for CAV/death No correlation with cellular rejection
C4d positivity Poor prognostic factor Reversal to C4d negativity did not change prognosis, with current therapy Prognostic factor for CAV Variable time line for CAV/death No correlation with cellular rejection
CONGENITAL TRACHEAL STENOSIS PRESENTING IN THE NEONATAL PERIOD
 CONGENITAL TRACHEAL STENOSIS PRESENTING IN THE NEONATAL PERIOD J Reiter, C Springer, E Erez Israel Society of Pediatric Pulmonolgy Jerusalem, September 2 nd, 2015 Topics Case Presentation Surgical Intervention
CONGENITAL TRACHEAL STENOSIS PRESENTING IN THE NEONATAL PERIOD J Reiter, C Springer, E Erez Israel Society of Pediatric Pulmonolgy Jerusalem, September 2 nd, 2015 Topics Case Presentation Surgical Intervention
Outcomes From Severe ARDS Managed Without ECMO. Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016
 Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
Progression pattern of restrictive allograft syndrome after lung transplantation
 http://www.jhltonline.org FEATURED ARTICLES Progression pattern of restrictive allograft syndrome after lung transplantation Masaaki Sato, MD, PhD, a,b David M. Hwang, MD, PhD, a Thomas K. Waddell, MD,
http://www.jhltonline.org FEATURED ARTICLES Progression pattern of restrictive allograft syndrome after lung transplantation Masaaki Sato, MD, PhD, a,b David M. Hwang, MD, PhD, a Thomas K. Waddell, MD,
5/15/2018. Background. Disclosure Statement
 5/15/218 Efficacy of Bronchoscopically-Administered in the Setting of Primary Graft Dysfunction after Lung Transplantation Primary Investigator: Sana Ahmed, PharmD Research Associates: Matthew Soto-Arenall,
5/15/218 Efficacy of Bronchoscopically-Administered in the Setting of Primary Graft Dysfunction after Lung Transplantation Primary Investigator: Sana Ahmed, PharmD Research Associates: Matthew Soto-Arenall,
ECLS as Bridge to Transplant
 ECLS as Bridge to Transplant Marcelo Cypel MD, MSc Assistant Professor of Surgery Division of Thoracic Surgery Toronto General Hospital University of Toronto Application of ECLS Bridge to lung recovery
ECLS as Bridge to Transplant Marcelo Cypel MD, MSc Assistant Professor of Surgery Division of Thoracic Surgery Toronto General Hospital University of Toronto Application of ECLS Bridge to lung recovery
Heart-lung transplantation: adult indications and outcomes
 Brief Report Heart-lung transplantation: adult indications and outcomes Yoshiya Toyoda, Yasuhiro Toyoda 2 Temple University, USA; 2 University of Pittsburgh, USA Correspondence to: Yoshiya Toyoda, MD,
Brief Report Heart-lung transplantation: adult indications and outcomes Yoshiya Toyoda, Yasuhiro Toyoda 2 Temple University, USA; 2 University of Pittsburgh, USA Correspondence to: Yoshiya Toyoda, MD,
Extracorporeal Life Support Organization (ELSO) Guidelines for Pediatric Respiratory Failure
 Guidelines for Pediatric Respiratory Failure") Extracorporeal Life Support Organization (ELSO) Guidelines for Pediatric Respiratory Failure Introduction This pediatric respiratory failure guideline is a supplement to ELSO s General Guidelines for all
Extracorporeal Life Support Organization (ELSO) Guidelines for Pediatric Respiratory Failure Introduction This pediatric respiratory failure guideline is a supplement to ELSO s General Guidelines for all
NON INVASIVE LIFE SAVERS. Non Invasive Ventilation (NIV)
") Table 1. NIV: Mechanisms Of Action Decreases work of breathing Increases functional residual capacity Recruits collapsed alveoli Improves respiratory gas exchange Reverses hypoventilation Maintains upper
Table 1. NIV: Mechanisms Of Action Decreases work of breathing Increases functional residual capacity Recruits collapsed alveoli Improves respiratory gas exchange Reverses hypoventilation Maintains upper
Pulmonary Hypertension: Another Use for Viagra
 Pulmonary Hypertension: Another Use for Viagra Kathleen Tong, MD Director, Heart Failure Program Assistant Clinical Professor University of California, Davis Disclosures I have no financial conflicts A
Pulmonary Hypertension: Another Use for Viagra Kathleen Tong, MD Director, Heart Failure Program Assistant Clinical Professor University of California, Davis Disclosures I have no financial conflicts A
THE ACUTE RESPIRATORY DISTRESS SYNDROME. Daniel Brockman, DO
 THE ACUTE RESPIRATORY DISTRESS SYNDROME Daniel Brockman, DO Objectives Describe the history and evolution of the diagnosis of ARDS Review the diagnostic criteria for ARDS Discuss the primary interventions
THE ACUTE RESPIRATORY DISTRESS SYNDROME Daniel Brockman, DO Objectives Describe the history and evolution of the diagnosis of ARDS Review the diagnostic criteria for ARDS Discuss the primary interventions
Hospital-acquired Pneumonia
 Hospital-acquired Pneumonia Hospital-acquired pneumonia (HAP) Pneumonia that occurs at least 2 days after hospital admission. The second most common and the leading cause of death due to hospital-acquired
Hospital-acquired Pneumonia Hospital-acquired pneumonia (HAP) Pneumonia that occurs at least 2 days after hospital admission. The second most common and the leading cause of death due to hospital-acquired
Best of Pulmonary Jennifer R. Hucks, MD University of South Carolina School of Medicine
 Best of Pulmonary 2012-2013 Jennifer R. Hucks, MD University of South Carolina School of Medicine Topics ARDS- Berlin Definition Prone Positioning For ARDS Lung Protective Ventilation In Patients Without
Best of Pulmonary 2012-2013 Jennifer R. Hucks, MD University of South Carolina School of Medicine Topics ARDS- Berlin Definition Prone Positioning For ARDS Lung Protective Ventilation In Patients Without
Case Scenarios. Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC. Consultant, Critical Care Medicine Medanta, The Medicity
 Case Scenarios Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Case 1 A 36 year male with cirrhosis and active GI bleeding is intubated to protect his airway,
Case Scenarios Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Case 1 A 36 year male with cirrhosis and active GI bleeding is intubated to protect his airway,
Sample Case Study. The patient was a 77-year-old female who arrived to the emergency room on
 Sample Case Study The patient was a 77-year-old female who arrived to the emergency room on February 25 th with a chief complaint of shortness of breath and a deteriorating pulmonary status along with
Sample Case Study The patient was a 77-year-old female who arrived to the emergency room on February 25 th with a chief complaint of shortness of breath and a deteriorating pulmonary status along with
SCVMC RESPIRATORY CARE PROCEDURE
 Page 1 of 7 New: 12/08 R: 4/11 R NC: 7/11, 7/12 B7180-63 Definitions: Inhaled nitric oxide (i) is a medical gas with selective pulmonary vasodilator properties. Vaso-reactivity is the evidence of acute
Page 1 of 7 New: 12/08 R: 4/11 R NC: 7/11, 7/12 B7180-63 Definitions: Inhaled nitric oxide (i) is a medical gas with selective pulmonary vasodilator properties. Vaso-reactivity is the evidence of acute
Index. Crit Care Clin 19 (2003)
") Crit Care Clin 19 (2003) 331 335 Index A ACVECC. See American College of Veterinary Emergency and Critical Care (ACVECC). Aging. See also Elderly; Geriatric critical care. respiratory function effects
Crit Care Clin 19 (2003) 331 335 Index A ACVECC. See American College of Veterinary Emergency and Critical Care (ACVECC). Aging. See also Elderly; Geriatric critical care. respiratory function effects
Pulmonary AMR Therapeutic Options & Strategies: The Old and the New. Ramsey Hachem, MD March 28, 2017
 Pulmonary AMR Therapeutic Options & Strategies: The Old and the New Ramsey Hachem, MD March 28, 2017 Disclosures Ramsey Hachem I have no financial relations with any relevant commercial interests I will
Pulmonary AMR Therapeutic Options & Strategies: The Old and the New Ramsey Hachem, MD March 28, 2017 Disclosures Ramsey Hachem I have no financial relations with any relevant commercial interests I will
Clinical syndrome of severe dyspnea of rapid onset, hypoxemia, and diffuse pulmonary infiltrates leading to respiratory failure.
 Yuanlin Song, M.D. Clinical syndrome of severe dyspnea of rapid onset, hypoxemia, and diffuse pulmonary infiltrates leading to respiratory failure. Pneumonia Trauma SARS PaO2/fiO2
Yuanlin Song, M.D. Clinical syndrome of severe dyspnea of rapid onset, hypoxemia, and diffuse pulmonary infiltrates leading to respiratory failure. Pneumonia Trauma SARS PaO2/fiO2
ino in neonates with cardiac disorders
 ino in neonates with cardiac disorders Duncan Macrae Paediatric Critical Care Terminology PAP Pulmonary artery pressure PVR Pulmonary vascular resistance PHT Pulmonary hypertension - PAP > 25, PVR >3,
ino in neonates with cardiac disorders Duncan Macrae Paediatric Critical Care Terminology PAP Pulmonary artery pressure PVR Pulmonary vascular resistance PHT Pulmonary hypertension - PAP > 25, PVR >3,
Cystic Fibrosis Complications ANDRES ZIRLINGER, MD STANFORD UNIVERSITY MEDICAL CENTER MARCH 3, 2012
 Cystic Fibrosis Complications ANDRES ZIRLINGER, MD STANFORD UNIVERSITY MEDICAL CENTER MARCH 3, 2012 INTRODUCTION PNEUMOTHORAX HEMOPTYSIS RESPIRATORY FAILURE Cystic Fibrosis Autosomal Recessive Genetically
Cystic Fibrosis Complications ANDRES ZIRLINGER, MD STANFORD UNIVERSITY MEDICAL CENTER MARCH 3, 2012 INTRODUCTION PNEUMOTHORAX HEMOPTYSIS RESPIRATORY FAILURE Cystic Fibrosis Autosomal Recessive Genetically
2/28/2017. Adult Heart Transplants Donor and Recipient Characteristics UNOS, Retransplant VCM. Other /2015 (N = 24,474)
") 1 46% 2% 3% 4% 0% 2% 2% CHD HCM ICM NICM RCM 49% 3% 3% 3% 1% 3% 3% Retransplant VCM 42% Other 35% 1/1982 6/2015 1/2009 6/2015 2016 JHLT. 2016 Oct; 35(10): 1149-1205 UNOS, 2017 Adult Heart Transplants Donor
1 46% 2% 3% 4% 0% 2% 2% CHD HCM ICM NICM RCM 49% 3% 3% 3% 1% 3% 3% Retransplant VCM 42% Other 35% 1/1982 6/2015 1/2009 6/2015 2016 JHLT. 2016 Oct; 35(10): 1149-1205 UNOS, 2017 Adult Heart Transplants Donor
Management of Rejection
 Management of Rejection I have no disclosures Disclosures (relevant or otherwise) Deborah B Adey, MD Professor of Medicine University of California, San Francisco Kidney and Pancreas Transplant Center
Management of Rejection I have no disclosures Disclosures (relevant or otherwise) Deborah B Adey, MD Professor of Medicine University of California, San Francisco Kidney and Pancreas Transplant Center
All I Need Is The Air That I Breathe: A Case Study of Immunotherapy and Severe Pneumonitis
 All I Need Is The Air That I Breathe: A Case Study of Immunotherapy and Severe Pneumonitis Presenter Disclosure Faculty/Speaker: Dr. Brett Finney BSc MD CCFP Relationships with financial sponsors: Grants/Research
All I Need Is The Air That I Breathe: A Case Study of Immunotherapy and Severe Pneumonitis Presenter Disclosure Faculty/Speaker: Dr. Brett Finney BSc MD CCFP Relationships with financial sponsors: Grants/Research
PEEP recruitment maneuver
 Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF Case 1: 40 yo Male restrained driver high speed MVA P 140, RR 40 labored, BP 100/70, O 2 sat 70 Chest wheeze, crackles
Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF Case 1: 40 yo Male restrained driver high speed MVA P 140, RR 40 labored, BP 100/70, O 2 sat 70 Chest wheeze, crackles
Lung Injury after HCT
 Lung Injury after HCT J. Douglas Rizzo, MD, MS Financial Disclosure None SCS06_1.ppt Background HCT an important therapeutic modality for malignant and non-malignant diseases Pulmonary Toxicity common
Lung Injury after HCT J. Douglas Rizzo, MD, MS Financial Disclosure None SCS06_1.ppt Background HCT an important therapeutic modality for malignant and non-malignant diseases Pulmonary Toxicity common
Breathing life into new therapies: Updates on treatment for severe respiratory failure. Whitney Gannon, MSN ACNP-BC
 Breathing life into new therapies: Updates on treatment for severe respiratory failure Whitney Gannon, MSN ACNP-BC Overview Definition of ARDS Clinical signs and symptoms Causes Pathophysiology Management
Breathing life into new therapies: Updates on treatment for severe respiratory failure Whitney Gannon, MSN ACNP-BC Overview Definition of ARDS Clinical signs and symptoms Causes Pathophysiology Management
Management of refractory ARDS. Saurabh maji
 Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
AMR in Liver Transplantation: Incidence
 AMR in Liver Transplantation: Incidence Primary AMR 1/3 to 1/2 of ABO-incompatible transplants Uncommon with ABO-compatible transplant Secondary AMR Unknown incidence: rarely tested Why is AMR uncommon
AMR in Liver Transplantation: Incidence Primary AMR 1/3 to 1/2 of ABO-incompatible transplants Uncommon with ABO-compatible transplant Secondary AMR Unknown incidence: rarely tested Why is AMR uncommon
HLA and Non-HLA Antibodies in Transplantation and their Management
 HLA and Non-HLA Antibodies in Transplantation and their Management Luca Dello Strologo October 29 th, 2016 Hystory I 1960 donor specific antibodies (DSA): first suggestion for a possible role in deteriorating
HLA and Non-HLA Antibodies in Transplantation and their Management Luca Dello Strologo October 29 th, 2016 Hystory I 1960 donor specific antibodies (DSA): first suggestion for a possible role in deteriorating
Lecture Notes. Chapter 16: Bacterial Pneumonia
 Lecture Notes Chapter 16: Bacterial Pneumonia Objectives Explain the epidemiology Identify the common causes Explain the pathological changes in the lung Identify clinical features Explain the treatment
Lecture Notes Chapter 16: Bacterial Pneumonia Objectives Explain the epidemiology Identify the common causes Explain the pathological changes in the lung Identify clinical features Explain the treatment
11/10/2014. Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective. Radiology
 Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective Radiology Pathology Clinical 1 Role of HRCT Diagnosis Fibrosis vs. inflammation Next step in management Response to treatment
Multi-disciplinary Approach to Diffuse Lung Disease: The Imager s Perspective Radiology Pathology Clinical 1 Role of HRCT Diagnosis Fibrosis vs. inflammation Next step in management Response to treatment
SCLERODERMA LUNG DISEASE: WHAT THE PATIENT SHOULD KNOW
 SCLERODERMA LUNG DISEASE: WHAT THE PATIENT SHOULD KNOW Lung disease can be a serious complication of scleroderma. The two most common types of lung disease in patients with scleroderma are interstitial
SCLERODERMA LUNG DISEASE: WHAT THE PATIENT SHOULD KNOW Lung disease can be a serious complication of scleroderma. The two most common types of lung disease in patients with scleroderma are interstitial
ECLS Bridge to Lung Transplantation Optimizing and Ambulating the Recipient
 ECLS Bridge to Lung Transplantation Optimizing and Ambulating the Recipient Shaf Keshavjee MD MSc FRCSC FACS Surgeon-in-Chief, University Health Network James Wallace McCutcheon Chair in Surgery Director,
ECLS Bridge to Lung Transplantation Optimizing and Ambulating the Recipient Shaf Keshavjee MD MSc FRCSC FACS Surgeon-in-Chief, University Health Network James Wallace McCutcheon Chair in Surgery Director,
The Pulmonary Pathology of Iatrogenic Immunosuppression. Kevin O. Leslie, M.D. Mayo Clinic Scottsdale
 The Pulmonary Pathology of Iatrogenic Immunosuppression Kevin O. Leslie, M.D. Mayo Clinic Scottsdale The indications for iatrogenic immunosuppression Autoimmune/inflammatory disease Chemotherapy for malignant
The Pulmonary Pathology of Iatrogenic Immunosuppression Kevin O. Leslie, M.D. Mayo Clinic Scottsdale The indications for iatrogenic immunosuppression Autoimmune/inflammatory disease Chemotherapy for malignant
Paramedic Rounds. Pre-Hospital Continuous Positive Airway Pressure (CPAP)
") Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
Treatment of Coccidioidomycosis-associated Eosinophilic Pneumonia with Corticosteroids
 Treatment of Coccidioidomycosis-associated Eosinophilic Pneumonia with Corticosteroids Joshua Malo, MD Yuval Raz, MD Linda Snyder, MD Kenneth Knox, MD University of Arizona Medical Center Department of
Treatment of Coccidioidomycosis-associated Eosinophilic Pneumonia with Corticosteroids Joshua Malo, MD Yuval Raz, MD Linda Snyder, MD Kenneth Knox, MD University of Arizona Medical Center Department of
Extracorporeal Life Support (ECLS) as a Bridge to Decision in Lung Transplantation
 as a Bridge to Decision in Lung Transplantation") Extracorporeal Life Support (ECLS) as a Bridge to Decision in Lung Transplantation Gabriel Loor, MD Baylor St. Lukes Medical Center Surgical Director Lung Transplantation Co-chief Section of Adult Cardiac
Extracorporeal Life Support (ECLS) as a Bridge to Decision in Lung Transplantation Gabriel Loor, MD Baylor St. Lukes Medical Center Surgical Director Lung Transplantation Co-chief Section of Adult Cardiac
Extracorporeal Membrane Oxygenation (ECMO) Referrals
 Referrals") Children s Acute Transport Service Clinical Guideline Extracorporeal Membrane Oxygenation (ECMO) Referrals Document Control Information Author ECMO/CATS Author Position Service Coordinator Document Owner
Children s Acute Transport Service Clinical Guideline Extracorporeal Membrane Oxygenation (ECMO) Referrals Document Control Information Author ECMO/CATS Author Position Service Coordinator Document Owner
Patient Management Code Blue in the CT Suite
 Patient Management Code Blue in the CT Suite David Stultz, MD November 28, 2001 Case Presentation A 53-year-old woman experienced acute respiratory distress during an IV contrast enhanced CT scan of the
Patient Management Code Blue in the CT Suite David Stultz, MD November 28, 2001 Case Presentation A 53-year-old woman experienced acute respiratory distress during an IV contrast enhanced CT scan of the
ESCMID Online Lecture Library. by author. CASE PRESENTATION ECCMID clinical grand round May Anat Stern, MD Rambam medical center Haifa, Israel
 CASE PRESENTATION ECCMID clinical grand round May 2014 Anat Stern, MD Rambam medical center Haifa, Israel An 18 years old Female, from Ukraine, diagnosed with acute lymphoblastic leukemia (ALL) in 2003.
CASE PRESENTATION ECCMID clinical grand round May 2014 Anat Stern, MD Rambam medical center Haifa, Israel An 18 years old Female, from Ukraine, diagnosed with acute lymphoblastic leukemia (ALL) in 2003.
Surgical indications: Non-malignant pulmonary diseases. Punnarerk Thongcharoen
 Surgical indications: Non-malignant pulmonary diseases Punnarerk Thongcharoen Non-malignant Malignant as a pathological term: Cancer Non-malignant = not cancer Malignant as an adjective: Disposed to cause
Surgical indications: Non-malignant pulmonary diseases Punnarerk Thongcharoen Non-malignant Malignant as a pathological term: Cancer Non-malignant = not cancer Malignant as an adjective: Disposed to cause
CPAP. Pre-Hospital Treatment Using The Respironics Whisperflow CPAP Device. Charlottesville Albemarle Rescue Squad - CPAP
 CPAP Pre-Hospital Treatment Using The Respironics Whisperflow CPAP Device CPAP What Is It? C ontinuous P ositive A irway P ressure Anatomy Review Anatomy Review Anatomy Review Alveoli Anatomy Review Chest
CPAP Pre-Hospital Treatment Using The Respironics Whisperflow CPAP Device CPAP What Is It? C ontinuous P ositive A irway P ressure Anatomy Review Anatomy Review Anatomy Review Alveoli Anatomy Review Chest
Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye
 Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye Steroids in ARDS: conclusion Give low-dose steroids if indicated for another problem
Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye Steroids in ARDS: conclusion Give low-dose steroids if indicated for another problem
Disclosures. ICU Management of Advanced Lung Disease 5/9/2015. No Disclosures. All pictures from commercial sources
 Disclosures ICU Management of Advanced Lung Disease No Disclosures All pictures from commercial sources Lundy J. Campbell, MD UCSF Department of Anesthesia and Perioperative Care Division of Critical Care
Disclosures ICU Management of Advanced Lung Disease No Disclosures All pictures from commercial sources Lundy J. Campbell, MD UCSF Department of Anesthesia and Perioperative Care Division of Critical Care
Stabilization and Transportation guidelines for Neonates and infants with Heart disease:
 Stabilization and Transportation guidelines for Neonates and infants with Heart disease: Background: Referral Pediatric Cardiac Units, frequently receive neonates and infants referred and transported from
Stabilization and Transportation guidelines for Neonates and infants with Heart disease: Background: Referral Pediatric Cardiac Units, frequently receive neonates and infants referred and transported from
9/15/11. Dr. Vivien Hsu Director, UMDNJ Scleroderma Program New Brunswick, NJ September Scleroderma. Hard skin
 Dr. Vivien Hsu Director, UMDNJ Scleroderma Program New Brunswick, NJ September 2011 Scleroderma Hard skin 1 No diagnostic test for scleroderma Pathogenesis is unknown prominent features of disease reflect
Dr. Vivien Hsu Director, UMDNJ Scleroderma Program New Brunswick, NJ September 2011 Scleroderma Hard skin 1 No diagnostic test for scleroderma Pathogenesis is unknown prominent features of disease reflect
Hemodynamic Monitoring
 Perform Procedure And Interpret Results Hemodynamic Monitoring Tracheal Tube Cuff Pressure Dean R. Hess PhD RRT FAARC Hemodynamic Monitoring Cardiac Rate and Rhythm Arterial Blood Pressure Central Venous
Perform Procedure And Interpret Results Hemodynamic Monitoring Tracheal Tube Cuff Pressure Dean R. Hess PhD RRT FAARC Hemodynamic Monitoring Cardiac Rate and Rhythm Arterial Blood Pressure Central Venous
Lung diseases of Vascular Origin. By: Shefaa Qa qqa
 Lung diseases of Vascular Origin By: Shefaa Qa qqa Pulmonary Hypertension Pulmonary hypertension is defined as a mean pulmonary artery pressure greater than or equal to 25 mm Hg at rest. Based on underlying
Lung diseases of Vascular Origin By: Shefaa Qa qqa Pulmonary Hypertension Pulmonary hypertension is defined as a mean pulmonary artery pressure greater than or equal to 25 mm Hg at rest. Based on underlying
Pulmonary Problems of the Neonate. Jon Palmer, VMD, DACVIM Chief, Neonatal Intensive Care Service New Bolton Center, University of Pennsylvania, USA
 Pulmonary Problems of the Neonate Jon Palmer, VMD, DACVIM Chief, Neonatal Intensive Care Service New Bolton Center, University of Pennsylvania, USA Lower Respiratory Diseases Ventilation/Perfusion Abnormalities
Pulmonary Problems of the Neonate Jon Palmer, VMD, DACVIM Chief, Neonatal Intensive Care Service New Bolton Center, University of Pennsylvania, USA Lower Respiratory Diseases Ventilation/Perfusion Abnormalities
Wanchai Wongkornrat Cardiovascular Thoracic Surgery Siriraj Hospital Mahidol University
 Wanchai Wongkornrat Cardiovascular Thoracic Surgery Siriraj Hospital Mahidol University Assess adequacy of ventilation and oxygenation Aids in establishing a diagnosis and severity of respiratory failure
Wanchai Wongkornrat Cardiovascular Thoracic Surgery Siriraj Hospital Mahidol University Assess adequacy of ventilation and oxygenation Aids in establishing a diagnosis and severity of respiratory failure
Maternal Cardiac Disease In Pregnancy. August 25, 2017 PREGNANCY ECHO CONFERENCE
 Maternal Cardiac Disease In Pregnancy August 25, 2017 PREGNANCY ECHO CONFERENCE Maternal Physiology Cardiac Output = HR x SV Non-pregnant: 4.5 L/min Pregnant: 6.0 L/min Increase most acute in first 10
Maternal Cardiac Disease In Pregnancy August 25, 2017 PREGNANCY ECHO CONFERENCE Maternal Physiology Cardiac Output = HR x SV Non-pregnant: 4.5 L/min Pregnant: 6.0 L/min Increase most acute in first 10
Certified Clinical Transplant Nurse (CCTN) * Detailed Content Outline
 * Detailed Content Outline") I. PRETRANSPLANTATION CARE 9 11 3 23 A. Evaluate End-Stage Organ Failure 1 1 1 3 1. History and physical assessment 2. Vital signs and / or hemodynamic parameters 3. Lab values 4. Diagnostic tests B. Monitor
I. PRETRANSPLANTATION CARE 9 11 3 23 A. Evaluate End-Stage Organ Failure 1 1 1 3 1. History and physical assessment 2. Vital signs and / or hemodynamic parameters 3. Lab values 4. Diagnostic tests B. Monitor
Oxygenation Failure. Increase FiO2. Titrate end-expiratory pressure. Adjust duty cycle to increase MAP. Patient Positioning. Inhaled Vasodilators
 Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
ECMO: a breakthrough in care for respiratory failure. PD Dr. Thomas Müller Regensburg no conflict of interest
 ECMO: a breakthrough in care for respiratory failure? PD Dr. Thomas Müller Regensburg no conflict of interest 1 Overview Mortality of severe ARDS Indication for ECMO PaO 2 /FiO 2 Efficiency of ECMO: gas
ECMO: a breakthrough in care for respiratory failure? PD Dr. Thomas Müller Regensburg no conflict of interest 1 Overview Mortality of severe ARDS Indication for ECMO PaO 2 /FiO 2 Efficiency of ECMO: gas
Pediatric Pulmonary Hypertension: Inside Out
 Pediatric Pulmonary Hypertension: Inside Out Asma Razavi, MD Assistant Professor Pediatric Critical Care Medicine Loma Linda University Children s Hopsital Disclosures I have no conflicts of interest to
Pediatric Pulmonary Hypertension: Inside Out Asma Razavi, MD Assistant Professor Pediatric Critical Care Medicine Loma Linda University Children s Hopsital Disclosures I have no conflicts of interest to
Perioperative Management of TAPVC
 Perioperative Management of TAPVC Professor Andrew Wolf Rush University Medical Center,Chicago USA Bristol Royal Children s Hospital UK I have no financial disclosures relevant to this presentation TAPVC
Perioperative Management of TAPVC Professor Andrew Wolf Rush University Medical Center,Chicago USA Bristol Royal Children s Hospital UK I have no financial disclosures relevant to this presentation TAPVC
Is severe re-expansion pulmonary edema still a lethal complication of closed thoracostomy or thoracic surgery?
 Original Article Page 1 of 6 Is severe re-expansion pulmonary edema still a lethal complication of closed thoracostomy or thoracic surgery? Sang Kwon Lee 1, Jung Joo Hwang 2, Mi Hee Lim 1, Joo Hyung Son
Original Article Page 1 of 6 Is severe re-expansion pulmonary edema still a lethal complication of closed thoracostomy or thoracic surgery? Sang Kwon Lee 1, Jung Joo Hwang 2, Mi Hee Lim 1, Joo Hyung Son
Oxygen and ABG. Dr Will Dooley
 Oxygen and ABG G Dr Will Dooley Oxygen and ABGs Simply in 10 cases Recap of: ABG interpretation Oxygen management Some common concerns A-a gradient Base Excess Anion Gap COPD patients CPAP/BiPAP First
Oxygen and ABG G Dr Will Dooley Oxygen and ABGs Simply in 10 cases Recap of: ABG interpretation Oxygen management Some common concerns A-a gradient Base Excess Anion Gap COPD patients CPAP/BiPAP First
Nothing to Disclose. Severe Pulmonary Hypertension
 Severe Ronald Pearl, MD, PhD Professor and Chair Department of Anesthesiology Stanford University Rpearl@stanford.edu Nothing to Disclose 65 year old female Elective knee surgery NYHA Class 3 Aortic stenosis
Severe Ronald Pearl, MD, PhD Professor and Chair Department of Anesthesiology Stanford University Rpearl@stanford.edu Nothing to Disclose 65 year old female Elective knee surgery NYHA Class 3 Aortic stenosis
The new ARDS definitions: what does it mean?
 The new ARDS definitions: what does it mean? Richard Beale 7 th September 2012 METHODS ESICM convened an international panel of experts, with representation of ATS and SCCM The objectives were to update
The new ARDS definitions: what does it mean? Richard Beale 7 th September 2012 METHODS ESICM convened an international panel of experts, with representation of ATS and SCCM The objectives were to update
You Won t Believe What I Saw on. Disclosures. Goals. Dimensions 2013 October 18 th Michael Pfeiffer, MD. No Financial Disclosures
 You Won t Believe What I Saw on that ECHO! Dimensions 2013 October 18 th Michael Pfeiffer, MD Disclosures No Financial Disclosures Goals Review unusual and unique echocardiographic images. Briefly present
You Won t Believe What I Saw on that ECHO! Dimensions 2013 October 18 th Michael Pfeiffer, MD Disclosures No Financial Disclosures Goals Review unusual and unique echocardiographic images. Briefly present
Lung Cancer - Suspected
 Lung Cancer - Suspected Shared Decision Making Lung Cancer: http://www.enhertsccg.nhs.uk/ Patient presents with abnormal CXR Lung cancer - clinical presentation History and Examination Incidental finding
Lung Cancer - Suspected Shared Decision Making Lung Cancer: http://www.enhertsccg.nhs.uk/ Patient presents with abnormal CXR Lung cancer - clinical presentation History and Examination Incidental finding
Veno-Venous ECMO Support. Chris Cropsey, MD Sept. 21, 2015
 Veno-Venous ECMO Support Chris Cropsey, MD Sept. 21, 2015 Objectives List indications and contraindications for ECMO Describe hemodynamics and oxygenation on ECMO Discuss evidence for ECMO outcomes Identify
Veno-Venous ECMO Support Chris Cropsey, MD Sept. 21, 2015 Objectives List indications and contraindications for ECMO Describe hemodynamics and oxygenation on ECMO Discuss evidence for ECMO outcomes Identify
INDEPENDENT LUNG VENTILATION
 INDEPENDENT LUNG VENTILATION Giuseppe A. Marraro, MD Director Anaesthesia and Intensive Care Department Paediatric Intensive Care Unit Fatebenefratelli and Ophthalmiatric Hospital Milan, Italy gmarraro@picu.it
INDEPENDENT LUNG VENTILATION Giuseppe A. Marraro, MD Director Anaesthesia and Intensive Care Department Paediatric Intensive Care Unit Fatebenefratelli and Ophthalmiatric Hospital Milan, Italy gmarraro@picu.it
Transfusion Reactions
 Transfusion Reactions From A to T Provincial Blood Coordinating Program Daphne Osborne MN PANC (C) RN We want you to know Definition Appropriate actions Classification Complete case studies Transfusion
Transfusion Reactions From A to T Provincial Blood Coordinating Program Daphne Osborne MN PANC (C) RN We want you to know Definition Appropriate actions Classification Complete case studies Transfusion
PULMONARY HYPERTENSION
 PULMONARY HYPERTENSION REVIEW & UPDATE Olga M. Fortenko, M.D. Pulmonary & Critical Care Medicine Pulmonary Vascular Diseases Sequoia Hospital 650-216-9000 Olga.Fortenko@dignityhealth.org Disclosures None
PULMONARY HYPERTENSION REVIEW & UPDATE Olga M. Fortenko, M.D. Pulmonary & Critical Care Medicine Pulmonary Vascular Diseases Sequoia Hospital 650-216-9000 Olga.Fortenko@dignityhealth.org Disclosures None
OLB (Open Lung Biopsy) in ARDS
 in ARDS") OLB (Open Lung Biopsy) in ARDS Claude GUERIN MD PhD Réanimation Médicale Hôpital de la Croix-Rousse Université de Lyon Lyon, France CCF Toronto October 28 th 2012 CCF 2012 1 Disclosure No conflict of interest
OLB (Open Lung Biopsy) in ARDS Claude GUERIN MD PhD Réanimation Médicale Hôpital de la Croix-Rousse Université de Lyon Lyon, France CCF Toronto October 28 th 2012 CCF 2012 1 Disclosure No conflict of interest
Case discussion Acute severe asthma during pregnancy. J.G. van der Hoeven
 Case discussion Acute severe asthma during pregnancy J.G. van der Hoeven Case (1) 32-year-old female - gravida 3 - para 2 Previous medical history - asthma Pregnant (33 w) Acute onset fever with wheezing
Case discussion Acute severe asthma during pregnancy J.G. van der Hoeven Case (1) 32-year-old female - gravida 3 - para 2 Previous medical history - asthma Pregnant (33 w) Acute onset fever with wheezing
Lecture Notes. Chapter 3: Asthma
 Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
Pulmonary veno-occlusive disease
 Disclosure Objectives Pulmonary veno-occlusive disease Tilman Humpl The Hospital for Sick Children University of Toronto, Canada Advisor/Research Grants Actelion Pfizer Historical aspects Epidemiology/Genetics
Disclosure Objectives Pulmonary veno-occlusive disease Tilman Humpl The Hospital for Sick Children University of Toronto, Canada Advisor/Research Grants Actelion Pfizer Historical aspects Epidemiology/Genetics
Severe β-lactam allergy. Alternative (use for mild-moderate β-lactam allergy) therapy
 therapy") Recommended Empirical Antibiotic Regimens for MICU Patients Notes: The antibiotic regimens shown are general guidelines and should not replace clinical judgment. Always assess for antibiotic allergies.
Recommended Empirical Antibiotic Regimens for MICU Patients Notes: The antibiotic regimens shown are general guidelines and should not replace clinical judgment. Always assess for antibiotic allergies.
Sub-category: Intensive Care for Respiratory Distress
 Course n : Course 3 Title: RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE Sub-category: Intensive Care for Respiratory Distress Topic: Acute Respiratory Distress
Course n : Course 3 Title: RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE Sub-category: Intensive Care for Respiratory Distress Topic: Acute Respiratory Distress
Specific Basic Standards for Osteopathic Fellowship Training in Pulmonary / Critical Care Medicine
 Specific Basic Standards for Osteopathic Fellowship Training in Pulmonary / Critical Care Medicine American Osteopathic Association and American College of Osteopathic Internists BOT Rev. 2/2011 These
Specific Basic Standards for Osteopathic Fellowship Training in Pulmonary / Critical Care Medicine American Osteopathic Association and American College of Osteopathic Internists BOT Rev. 2/2011 These
7/4/2015. diffuse lung injury resulting in noncardiogenic pulmonary edema due to increase in capillary permeability
 Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
To ECMO Or Not To ECMO Challenges of venous arterial ECMO. Dr Emily Granger St Vincent s Hospital Darlinghurst NSW
 To ECMO Or Not To ECMO Challenges of venous arterial ECMO Dr Emily Granger St Vincent s Hospital Darlinghurst NSW The Start: 1972 St Vincent s Hospital The Turning Point ECMO program restarted in 2004
To ECMO Or Not To ECMO Challenges of venous arterial ECMO Dr Emily Granger St Vincent s Hospital Darlinghurst NSW The Start: 1972 St Vincent s Hospital The Turning Point ECMO program restarted in 2004