Management of refractory ARDS. Saurabh maji
|
|
|
- Claire Cobb
- 5 years ago
- Views:
Transcription
1 Management of refractory ARDS Saurabh maji
2 Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma oxygenation index 30 Chest 2013;137(5):
3 In another study it has been defined as ARDS patient with Pao2/Fio2 is less than 100 mm Hg for 12 to 24 hrs on a PEEP more than 10 cm H2O and FiO2 greater than 0.5 Am J Respir Crit Care Med Nov 15;172(10):1241-5
4 Lung-Recruitment Maneuvers Prone Positioning Extracorporeal Membrane Oxygenation Inhaled Vasodilators: Nitric Oxide and Prostacyclin
5 Lung-Recruitment Maneuvers There are three 'compartments' in ARDSaffected lungs: 1. aerated normal lung susceptible to barotrauma induced by inappropriate ventilation; 2. air spaces that are filled with exudate and not recruitable; 3. areas that are collapsed due to interstitial infiltration and are potentially recruitable
6 There is an increasing perception that mechanical ventilation may further compromise the sick lung. Compromise may be due to: Overinflation of normal lung tissue, due to high transpulmonary pressures, causing increased permeability, worsening compliance, and a vicious cycle of progressive lung injury; Inadequate levels of positive end-expiratory pressure (PEEP), promoting regional collapse of lung tissue (atelectasis), and also causing alveolar injury due to cyclical closing and opening of airways with ventilation.
7 Recruitment Manoeuvres An administration of high ventilation pressure to a patient for a brief period of time Aim is to reinflate collapsed lung tissue, thus recruiting that tissue Aim is also to prevent de-recruitment by applying PEEP after the manoeuvre The desired outcome is improved oxygenation
8 Indications for RM ARDS / Acute Lung Injury Patients with secondary ARDS (eg from abdominal sepsis) seem to respond better than those with primary ARDS eg. from pneumonia Bilateral pulmonary infiltrates PaO2/FiO2* <300 = ALI PaO2/FiO2 <200 = ARDS Atelectasis during general anaesthesia Desaturation After suctioning the ETT Annals of Intensive Care 2011, 1:9
9 Contraindications for RM Hemodynamic compromise: recruitment manoeuvres cause a transient loss of venous return, compromising cardiac output. Existing barotrauma Increased intracranial pressure Predisposition to barotrauma: Apical bullous lung disease Focal lung pathology eg. lobar pneumonia Crit Care Med 2010,38:
10 Types of Recruitment Manoeuvres CPAP with increased pressures Pressure-controlled ventilation on high PEEP Advanced recruitment manoeuvres: Prone ventilation to recruit dorsal lung units High frequency oscillatory ventilation (lung protective) Airway pressure release ventilation, low PEEP and low tidal volume, with I:E of 4:1
11 Some basic RM protocols CPAP 40cmH2O for 40 seconds CPAP 40cmH2O for 30 seconds Crit Care Med 2005,33:54-61 Anesth Analg.2007 Feb;104(2): Pressure controlled ventilation with Pplat 45cm H2O, PEEP of 5, I:E 1:1 and rate of 10 Anesthesiology 2002, 96:
12 PEEP after recruitment Generally, it is recommended (Hickling 2001) to gradually decrease PEEP until there is a fall in PO2; this is a decremental PEEP trial PEEP is decreased by 2cmH2O every 4 minutes A fall in PO2 by over 10% indicates that there is derecruitment PEEP is then set to just above the level at which derecruitment occurs Am J Respir Crit Care Med Jan;163(1):69-78
13 Consequences of Recruitment Manoeuvres Increased oxygenation Stretch reflex of the alveoli, which causes Type II respiratory cells to release more surfactant Increased intrapulmonary shunt Barotrauma; overdistension of already well-ventilated lung regions VILI due to the above Increased pulmonary arterial pressure Decreased cardiac output Increased intracranial pressure The hemodynamic consequences seem to normalise 10-20mintues after the manoeuvre
14
15
16
17 Prone ventilation Effect of prone ventilation: Prone positioning improves gas exchange via its effect on pleural pressure and lung compression Increased functional residual capacity (FRC) has also been proposed, but changes in FRC have not been a dominant finding in most studies of prone ventilation Am Rev Respir Dis. 1977;115(4):559 Am J Respir Crit Care Med. 1998;157(2):387
18 Trans pulmonary pressure (Ptp) is defined as the difference between the airway pressure (Paw) and pleural pressure (Ppl): Ptp = Paw Ppl In supine position, the dorsal pleural pressure is greater than ventral pleural pressure So, the ventral trans pulmonary pressure exceeds the dorsal transpulmonary pressure and greater expansion of the ventral alveoli than the dorsal alveoli Eur Respir J. 2008;20(4):1017. Intensive Care Med. 1986;12(3):137
19 Exaggerated in supine patients with acute respiratory distress syndrome (ARDS), probably because the difference between the dorsal and ventral pleural pressures is increased by the excess lung weight The result is a tendency towards overinflation of the ventral alveoli and atelectasis of the dorsal alveoli
20 Prone positioning reduces the difference between the dorsal and ventral pleural pressures Making ventilation more homogeneous Leading to a decrease in alveolar overinflation and alveolar collapse. Minimize stress and strain on alveoli, limiting ventilatorassociated lung injury from overdistention and cyclic atelectasis Anesth Analg. 2009;83(6):1206
21 Compression: in supine position: Heart compresses the medial posterior lung parenchyma and the diaphragm compresses the posterior-caudal lung parenchyma Compression by either the heart or the diaphragm may exaggerate dependent lung collapse in the supine position, increasing hypoxemia and ventilator-associated lung injury Am J Respir Crit Care Med. 2008;158(5 Pt 1):1644
22 During prone ventilation, the heart becomes dependent, decreasing medial posterior lung compression The diaphragm is displaced caudally (especially in non-obese patients and when the abdomen is left unsupported), decreasing compression of the posterior-caudal lung parenchyma Improve ventilation and oxygenation
23 Cardiac output: Increase in lung recruitment and reduction in hypoxic pulmonary vasoconstriction Increases in cardiac output by Increases in right ventricular preload, and decreased right ventricular afterload Am J Respir Crit Care Med. 2007;157(2):387
24 Perfusion: In ARDS, there is substantial ventilation-perfusion mismatch in the supine position, since blood flow and alveolar collapse are both greatest in the dependent portions of the lung In prone position as the previously dependent lung continues to receive the majority of the blood flow (independent of the gravitational gradient) as alveoli reopen, while the newly dependent lung continues to receive the minority of the blood flow as alveoli begin to collapse
25 Clinical outcome prone ventilation increases arterial oxygen tension (PaO2) a reduction in the fraction of inspired oxygen (Fio2) Among patients whose oxygenation improves during prone ventilation, some continue to have improved oxygenation for hours after they return to the supine position and many improve each time prone ventilation is repeated N Engl J Med. 2013;368(23):2159
26 Predictor The best predictor of a sustained increase in PaO2 during prone ventilation is 10 mmhg increase in PaO2 over the first 30 minutes of prone ventilation predicted a sustained increase in PaO2 over the next two hours Patients whose PaO2 did not increase during the first 30 minutes of prone ventilation showed no subsequent improvement in their oxygenation Chest. 1988;94(1):103
27
28 Trend of principal parameter throughout the study
29
30 Patients with diffuse pulmonary edema and dependent alveolar collapse appear more likely to improve their PaO2 during prone ventilation than patients with predominantly anterior abnormalities, marked consolidation, and/or fibrosis Extrapulmonary cause for their ARDS seem more likely to increase their PaO2 during prone ventilation than patients with a pulmonary cause Am J Respir Crit Care Med. 2012;157(6 Pt 1):1785
31 Patients with elevated intraabdominal pressure appear more likely to increase their PaO2 during prone ventilation than patients with normal intraabdominal pressure Patients whose chest wall compliance decreases when moving from the supine to the prone position are likely to improve their PaO2 during prone ventilation
32 Hu et al. Critical Care 2014, 18:R109
33 Meta-analysis of the effect of prone positioning on 28- to 30-day mortality in acute respiratory distress syndrome patients related to the ratio of partial pressure of arterial oxygen/fraction of inspired oxygen

34 Prone position with high peep and mortality Meta-analysis of the effect of prone positioning on 28- to 30-day mortality related to positive end-expiratory pressure in acute respiratory distress syndrome patients
35 Meta-analysis of the effect of prone positioning on 90-day mortality in acute respiratory distress syndrome patients related to positive end-expiratory pressure

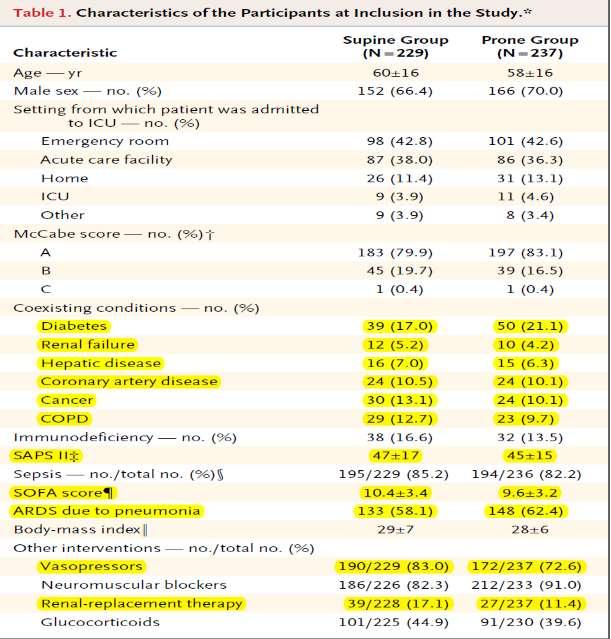
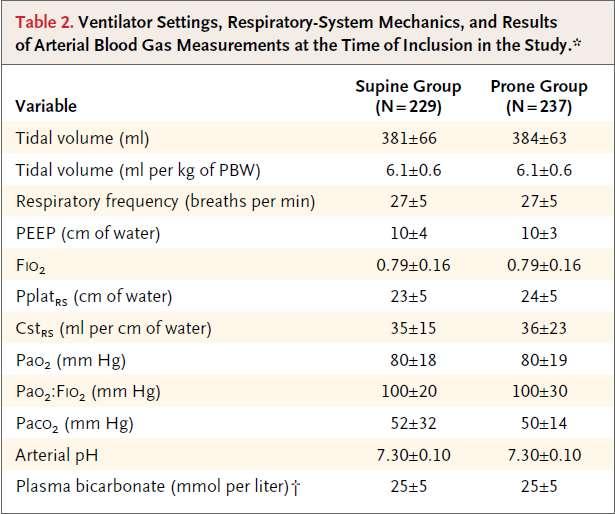
36 Multicenter, prospective, randomized, controlled trial 466 patients with severe ARDS to undergo prone-positioning sessions of at least 16 hours or to be left in the supine position Severe ARDS was defined as Pao2/Fio2 is less than150 mm Hg, with an Fio2 of at least 0.6, a PEEP of at least 5 cm of water, and a tidal volume close to 6 ml per kilogram of predicted body weight After stabilization period of 12 to 24 hours patients were proned for at least 16 hours The primary outcome was the proportion of patients who died from any cause within 28 days after inclusion
37
38
39 First prone-positioning done within 55±55 minutes after randomization The average number of sessions was 4±4 per patient Mean duration per session was 17±3 hours All the patients in this group underwent at least one pronepositioning session patients were ventilated in the prone position for 73% of the 22,334 patient-hours spent in the ICU from the start of the first session to the end of the last session
40 Result
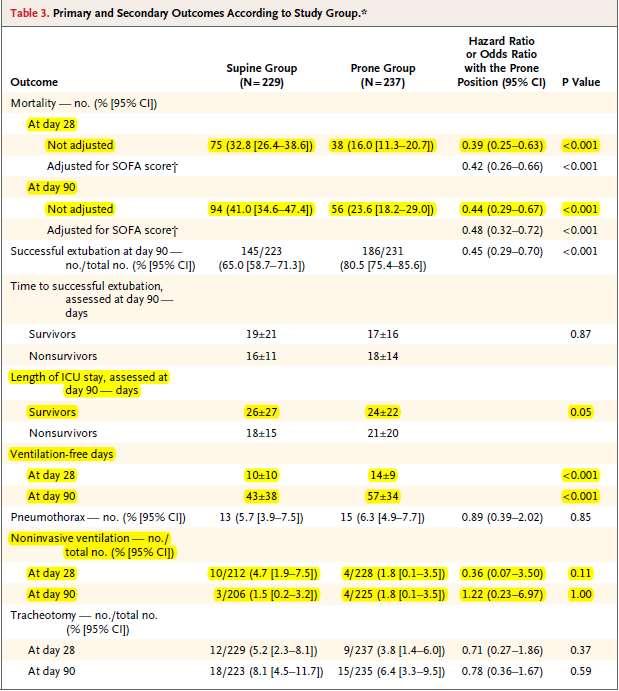
41 Result
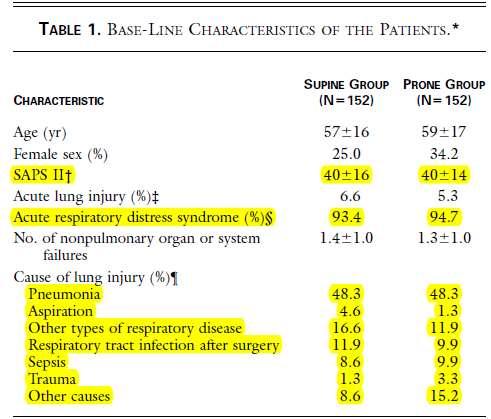
42 Multicenter, randomized trial compared conventional treatment (in the supine position) of patients with acute lung injury or the acute respiratory distress syndrome with a predefined strategy of placing patients in a prone position for six or more hours daily for 10 days Enrolled 304 patients, 152 in each group JAMA. 2006;302(18):
43 The primary end point was death at 10 days At the time of discharge from the intensive care unit 6 months mortality after randomization Secondary end points were Improvement in respiratory failure and improvement in organ dysfunction at 10 days
44
45
46
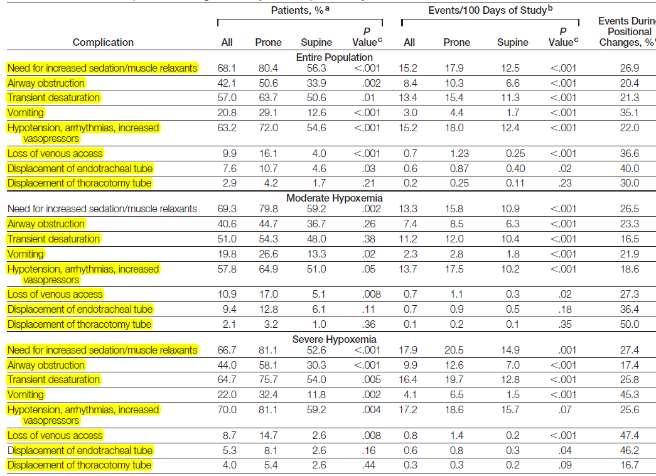
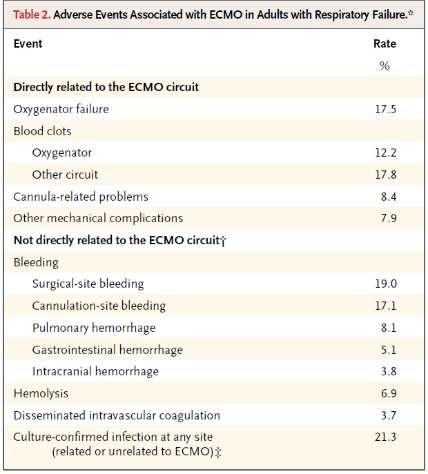
47 complication JAMA. 2009;302(18):
48 ECMO Extracorporeal lung support technologies [i.e., Interventional Lung Assist (ILA) and extracorporeal membrane oxygenation (ECMO)] have been advocated for use in the treatment of patients with respiratory failure These techniques do not treat the underlying lung condition; rather, they improve gas exchange while enabling the implantation of a protective ventilation strategy to prevent further damage to the lung tissues imposed by the ventilator Am J Emerg Med. 2014;32(10):1300 e1 2. doi: /j.
49 ECMO has become a general term encompassing a range of methods for extracorporeal blood oxygenation and CO2 removal In the 1970 s, ECMO referred to a high-flow venoarterial bypass system aimed primarily at blood oxygenation. By the 1980 s, the term extracorporeal CO2 removal (ECCO2R) was used to cover a low-flow venovenous bypass technique and replaced ECMO Later in the mid-1980 s, partial extracorporeal CO2 removal (PECO2R) emerged with the development of a technique used to eliminate only part of the body s CO2 for patients with chronic lung disease. In 1987, a Japanese working group then introduced the term extracorporeal lung assist (ECLA) to describe a venovenous low-flow bypass system. Extracorporeal life support was then introduced to describe techniques that provide prolonged but temporary support for the lungs and heart Ontario Health Technology Assessment Series 2010; Vol. 10, No. 5
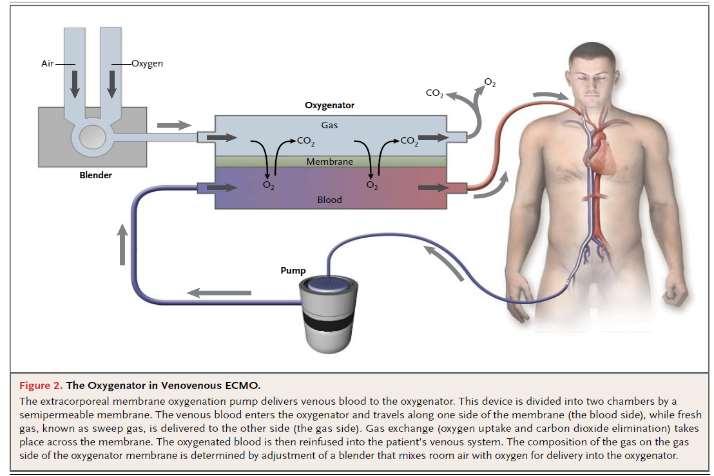
50 The ECMO system consists of a centrifugal pump, a membrane oxygenator, inlet and outlet cannulas, and tubing The exchange of oxygen and CO2 then takes place in the oxygenator, which delivers the reoxygenated blood back into one of the patient s veins or arteries Additional ports may be added for haemodialysis or ultrafiltration
51 Two different techniques may be used to introduce ECMO venoarterial and venovenous venoarterial technique, cannulation is through either the femoral artery and the femoral vein, or through the carotid artery and the internal jugular vein
52 venovenous technique cannulation is through both femoral veins or a femoral vein and internal jugular vein Venovenous ECMO will not provide adequate support if a patient has pulmonary hypertension or right heart failure Venovenous ECMO can be either two site approach or single site approach
53

54 Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine (2015) 23:30
55 Problems associated with cannulation during the procedure include bleeding around the cannulation site and limb ischemia distal to the cannulation site The system is characterized by a novel, low-resistance gas exchange device with a diffusion membrane composed of polymethylpentene (PMP) fibres
56 These fibres are woven into a complex configuration that maximizes the exchange of oxygen and CO2 by simple diffusion system is also designed to operate without the help of an external pump, though one can be added if higher blood flow is required Depending on the size of the cannula used and the mean systemic venous pressure, a blood flow of up to 2.5 L/min can be achieved (up to 5.5 L/min with an external pump). Intensive Care Med 2009;35:

57 pros and cons of double lumen cannula and femoro-jugular cannulation N Engl J Med 2011;365:

58 OHTAS 2010; 10(5)
59
60
61
62
63
64
65 N Engl J Med 2011;365:
66 N Engl J Med 2011;365:
67 CESAR trial was conducted to assess the effectiveness and cost of ECMO therapy for severe, acute respiratory failure. The trial protocol were published in 2006 and details of the methods used for the economic evaluation were published in The study itself was a pragmatic trial (similar to a UK trial of neonatal ECMO), in which best standard practice was compared with an ECMO protocol.
68 The trial involved 180 patients with acute but potentially reversible respiratory failure, with each also Murray score of 3.0 or uncompensated hypercapnia at a ph of < 7.2. Randomized in a 1:1 ratio to receive either conventional ventilation treatment or ECMO while on Conventional management included intermittent positive pressure ventilation, high frequency oscillatory ventilation, or both. As a pragmatic trial, a specific management protocol was not followed; rather the treatment centres were advised to follow a low volume low pressure ventilation strategy. A tidal volume of 4 to 8 ml/kg body weight and a plateau pressure of < 30 cm H2O were recommended
69 Out come measurement The primary outcome measure was death or severe disability at 6 months The secondary outcomes included a range of hospital indices: duration of ventilation, use of high frequency/oscillation/jet ventilation, use of nitric oxide, prone positioning, use of steroids, length of ICU stay, and length of hospital stay and (for ECMO patients only) mode (VV/VA), duration of ECMO.
70
71
72
73 Primary outcome
74
75 Inhaled vasodialator Inhaled vasodilator can result in important physiologic benefits (eg, improved hypoxemia, lower pulmonary arterial pressure, and improved right-ventricular function and cardiac output) without systemic hemodynamic effects. Inhaled nitric oxide (INO) and aerosolized prostacyclins are currently the most frequently used inhaled vasodilators. Inhaled prostacyclins are as effective physiologically as INO and cost less. Randomized controlled trials of INO in the treatment of ARDS have shown short-term physiologic benefits, but no benefit in long-term outcomes. No outcome studies have been reported on the use of prostacyclin in patients with ARDS. There is no role for the routine use of inhaled vasodilators in patients with ARDS. Inhaled vasodilator as a rescue therapy for severe refractory hypoxemia in patients with ARDS may be reasonable, but is controversial Respir Care2014;Feb;55(2):144-5
76
77
78
ARDS: an update 6 th March A. Hakeem Al Hashim, MD, FRCP SQUH
 ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
Landmark articles on ventilation
 Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
ARDS Management Protocol
 ARDS Management Protocol February 2018 ARDS Criteria Onset Within 1 week of a known clinical insult or new or worsening respiratory symptoms Bilateral opacities not fully explained by effusions, lobar/lung
ARDS Management Protocol February 2018 ARDS Criteria Onset Within 1 week of a known clinical insult or new or worsening respiratory symptoms Bilateral opacities not fully explained by effusions, lobar/lung
Ventilatory Management of ARDS. Alexei Ortiz Milan; MD, MSc
 Ventilatory Management of ARDS Alexei Ortiz Milan; MD, MSc 2017 Outline Ventilatory management of ARDS Protected Ventilatory Strategy Use of NMB Selection of PEEP Driving pressure Lung Recruitment Prone
Ventilatory Management of ARDS Alexei Ortiz Milan; MD, MSc 2017 Outline Ventilatory management of ARDS Protected Ventilatory Strategy Use of NMB Selection of PEEP Driving pressure Lung Recruitment Prone
ACUTE RESPIRATORY DISTRESS SYNDROME
 ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
Breathing life into new therapies: Updates on treatment for severe respiratory failure. Whitney Gannon, MSN ACNP-BC
 Breathing life into new therapies: Updates on treatment for severe respiratory failure Whitney Gannon, MSN ACNP-BC Overview Definition of ARDS Clinical signs and symptoms Causes Pathophysiology Management
Breathing life into new therapies: Updates on treatment for severe respiratory failure Whitney Gannon, MSN ACNP-BC Overview Definition of ARDS Clinical signs and symptoms Causes Pathophysiology Management
ARDS Assisted ventilation and prone position. ICU Fellowship Training Radboudumc
 ARDS Assisted ventilation and prone position ICU Fellowship Training Radboudumc Fig. 1 Physiological mechanisms controlling respiratory drive and clinical consequences of inappropriate respiratory drive
ARDS Assisted ventilation and prone position ICU Fellowship Training Radboudumc Fig. 1 Physiological mechanisms controlling respiratory drive and clinical consequences of inappropriate respiratory drive
Oxygenation Failure. Increase FiO2. Titrate end-expiratory pressure. Adjust duty cycle to increase MAP. Patient Positioning. Inhaled Vasodilators
 Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
What s New About Proning?
 1 What s New About Proning? J. Brady Scott, MSc, RRT-ACCS, AE-C, FAARC Director of Clinical Education and Assistant Professor Department of Cardiopulmonary Sciences Division of Respiratory Care Rush University
1 What s New About Proning? J. Brady Scott, MSc, RRT-ACCS, AE-C, FAARC Director of Clinical Education and Assistant Professor Department of Cardiopulmonary Sciences Division of Respiratory Care Rush University
Outcomes From Severe ARDS Managed Without ECMO. Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016
 Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate. Carolyn Calfee, MD MAS Mark Eisner, MD MPH
 ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate Carolyn Calfee, MD MAS Mark Eisner, MD MPH June 3, 2010 Case Presentation Setting: Community hospital, November 2009 29 year old woman with
ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate Carolyn Calfee, MD MAS Mark Eisner, MD MPH June 3, 2010 Case Presentation Setting: Community hospital, November 2009 29 year old woman with
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv
 Rv") ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
7/4/2015. diffuse lung injury resulting in noncardiogenic pulmonary edema due to increase in capillary permeability
 Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
One Lung Ventilation in Obese patients
 One Lung Ventilation in Obese patients YUSNI PUSPITA DEPARTEMEN ANESTESIOLOGI DAN TERAPI INTENSIF FAKULTAS KEDOKTERAN UNIVERSITAS SRIWIJAYA/RSMH PALEMBANG One Lung Ventilation Lung isolation techniques
One Lung Ventilation in Obese patients YUSNI PUSPITA DEPARTEMEN ANESTESIOLOGI DAN TERAPI INTENSIF FAKULTAS KEDOKTERAN UNIVERSITAS SRIWIJAYA/RSMH PALEMBANG One Lung Ventilation Lung isolation techniques
ECMO/ECCO 2 R in Acute Respiratory Failure
 ECMO/ECCO 2 R in Acute Respiratory Failure Alain Combes, MD, PhD, Hôpital Pitié-Salpêtrière, AP-HP Inserm UMRS 1166, ican, Institute of Cardiometabolism and Nutrition Sorbonne Pierre et Marie Curie University,
ECMO/ECCO 2 R in Acute Respiratory Failure Alain Combes, MD, PhD, Hôpital Pitié-Salpêtrière, AP-HP Inserm UMRS 1166, ican, Institute of Cardiometabolism and Nutrition Sorbonne Pierre et Marie Curie University,
Respiratory insufficiency in bariatric patients
 Respiratory insufficiency in bariatric patients Special considerations or just more of the same? Weaning and rehabilation conference 6th November 2015 Definition of obesity Underweight BMI< 18 Normal weight
Respiratory insufficiency in bariatric patients Special considerations or just more of the same? Weaning and rehabilation conference 6th November 2015 Definition of obesity Underweight BMI< 18 Normal weight
9/5/2018. Conflicts of Interests. Pediatric Acute Respiratory Distress Syndrome. Objectives ARDS ARDS. Definitions. None
 Pediatric Acute Respiratory Distress Syndrome Conflicts of Interests Diane C Lipscomb, MD Director Inpatient Pediatric Medical Director Mercy Springfield Associate Clerkship Clinical Director University
Pediatric Acute Respiratory Distress Syndrome Conflicts of Interests Diane C Lipscomb, MD Director Inpatient Pediatric Medical Director Mercy Springfield Associate Clerkship Clinical Director University
Veno-Venous ECMO Support. Chris Cropsey, MD Sept. 21, 2015
 Veno-Venous ECMO Support Chris Cropsey, MD Sept. 21, 2015 Objectives List indications and contraindications for ECMO Describe hemodynamics and oxygenation on ECMO Discuss evidence for ECMO outcomes Identify
Veno-Venous ECMO Support Chris Cropsey, MD Sept. 21, 2015 Objectives List indications and contraindications for ECMO Describe hemodynamics and oxygenation on ECMO Discuss evidence for ECMO outcomes Identify
Acute Respiratory Distress Syndrome (ARDS) An Update
 An Update") Acute Respiratory Distress Syndrome (ARDS) An Update Prof. A.S.M. Areef Ahsan FCPS(Medicine) MD(Critical Care Medicine) MD ( Chest) Head, Dept. of Critical Care Medicine BIRDEM General Hospital INTRODUCTION
Acute Respiratory Distress Syndrome (ARDS) An Update Prof. A.S.M. Areef Ahsan FCPS(Medicine) MD(Critical Care Medicine) MD ( Chest) Head, Dept. of Critical Care Medicine BIRDEM General Hospital INTRODUCTION
ARDS: MANAGEMENT UPDATE
 ARDS: MANAGEMENT UPDATE Tanıl Kendirli, Assoc. Prof. Ankara University School of Medicine, Pediatric Critical Care Medicine The AECC Definition Timing Acute onset, within 48-72 hours Oxygenation ALI PaO2/FiO2
ARDS: MANAGEMENT UPDATE Tanıl Kendirli, Assoc. Prof. Ankara University School of Medicine, Pediatric Critical Care Medicine The AECC Definition Timing Acute onset, within 48-72 hours Oxygenation ALI PaO2/FiO2
Prone Position in ARDS
 Prone Position in ARDS Rich Kallet MS RRT FAARC, FCCM Respiratory Care Services San Francisco General Hospital University of California, San Francisco, Case Study A 39 yo F admitted to SFGH TICU s/p hanging,
Prone Position in ARDS Rich Kallet MS RRT FAARC, FCCM Respiratory Care Services San Francisco General Hospital University of California, San Francisco, Case Study A 39 yo F admitted to SFGH TICU s/p hanging,
ARDS and Lung Protection
 ARDS and Lung Protection Kristina Sullivan, MD Associate Professor University of California, San Francisco Department of Anesthesia and Perioperative Care Division of Critical Care Medicine Overview Low
ARDS and Lung Protection Kristina Sullivan, MD Associate Professor University of California, San Francisco Department of Anesthesia and Perioperative Care Division of Critical Care Medicine Overview Low
INTRODUCTION The effect of CPAP works on lung mechanics to improve oxygenation (PaO 2
 2 Effects of CPAP INTRODUCTION The effect of CPAP works on lung mechanics to improve oxygenation (PaO 2 ). The effect on CO 2 is only secondary to the primary process of improvement in lung volume and
2 Effects of CPAP INTRODUCTION The effect of CPAP works on lung mechanics to improve oxygenation (PaO 2 ). The effect on CO 2 is only secondary to the primary process of improvement in lung volume and
ECMO and refractory Hypoxemia
 ECMO and refractory Hypoxemia Dr. Vinay Dhingra MD FRCPC Clinical Associate Professor of Medicine Clinical Lead Critical Care BCPSQC Medical Director Quality VGH Disclosures ARDS Lancet 1967; 2:319-323
ECMO and refractory Hypoxemia Dr. Vinay Dhingra MD FRCPC Clinical Associate Professor of Medicine Clinical Lead Critical Care BCPSQC Medical Director Quality VGH Disclosures ARDS Lancet 1967; 2:319-323
The use of proning in the management of Acute Respiratory Distress Syndrome
 Case 3 The use of proning in the management of Acute Respiratory Distress Syndrome Clinical Problem This expanded case summary has been chosen to explore the rationale and evidence behind the use of proning
Case 3 The use of proning in the management of Acute Respiratory Distress Syndrome Clinical Problem This expanded case summary has been chosen to explore the rationale and evidence behind the use of proning
Analyzing Lung protective ventilation F Javier Belda MD, PhD Sº de Anestesiología y Reanimación. Hospital Clinico Universitario Valencia (Spain)
") Analyzing Lung protective ventilation F Javier Belda MD, PhD Sº de Anestesiología y Reanimación Hospital Clinico Universitario Valencia (Spain) ALI/ARDS Report of the American-European consensus conference
Analyzing Lung protective ventilation F Javier Belda MD, PhD Sº de Anestesiología y Reanimación Hospital Clinico Universitario Valencia (Spain) ALI/ARDS Report of the American-European consensus conference
Application of Lung Protective Ventilation MUST Begin Immediately After Intubation
 Conflict of Interest Disclosure Robert M Kacmarek Managing Severe Hypoxemia!" 9-28-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts I disclose
Conflict of Interest Disclosure Robert M Kacmarek Managing Severe Hypoxemia!" 9-28-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts I disclose
Experience with Low Flow ECCO2R device on a CRRT platform : CO2 removal
 Experience with Low Flow ECCO2R device on a CRRT platform : CO2 removal Alain Combes, MD, PhD, Hôpital Pitié-Salpêtrière, AP-HP Inserm UMRS 1166, ican, Institute of Cardiometabolism and Nutrition Pierre
Experience with Low Flow ECCO2R device on a CRRT platform : CO2 removal Alain Combes, MD, PhD, Hôpital Pitié-Salpêtrière, AP-HP Inserm UMRS 1166, ican, Institute of Cardiometabolism and Nutrition Pierre
THE ACUTE RESPIRATORY DISTRESS SYNDROME. Daniel Brockman, DO
 THE ACUTE RESPIRATORY DISTRESS SYNDROME Daniel Brockman, DO Objectives Describe the history and evolution of the diagnosis of ARDS Review the diagnostic criteria for ARDS Discuss the primary interventions
THE ACUTE RESPIRATORY DISTRESS SYNDROME Daniel Brockman, DO Objectives Describe the history and evolution of the diagnosis of ARDS Review the diagnostic criteria for ARDS Discuss the primary interventions
Sub-category: Intensive Care for Respiratory Distress
 Course n : Course 3 Title: RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE Sub-category: Intensive Care for Respiratory Distress Topic: Acute Respiratory Distress
Course n : Course 3 Title: RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE Sub-category: Intensive Care for Respiratory Distress Topic: Acute Respiratory Distress
I. Subject: Continuous Positive Airway Pressure CPAP by Continuous Flow Device
 I. Subject: Continuous Positive Airway Pressure CPAP by Continuous Flow Device II. Policy: Continuous Positive Airway Pressure CPAP by the Down's system will be instituted by Respiratory Therapy personnel
I. Subject: Continuous Positive Airway Pressure CPAP by Continuous Flow Device II. Policy: Continuous Positive Airway Pressure CPAP by the Down's system will be instituted by Respiratory Therapy personnel
Case discussion Acute severe asthma during pregnancy. J.G. van der Hoeven
 Case discussion Acute severe asthma during pregnancy J.G. van der Hoeven Case (1) 32-year-old female - gravida 3 - para 2 Previous medical history - asthma Pregnant (33 w) Acute onset fever with wheezing
Case discussion Acute severe asthma during pregnancy J.G. van der Hoeven Case (1) 32-year-old female - gravida 3 - para 2 Previous medical history - asthma Pregnant (33 w) Acute onset fever with wheezing
Part 2 of park s Ventilator and ARDS slides for syllabus
 Part 2 of park s Ventilator and ARDS slides for syllabus Early Neuromuscular Blockade Question 4 The early use of cis-atracurium in severe ARDS is: A. Contraindicated in patients with diabetes B. Associated
Part 2 of park s Ventilator and ARDS slides for syllabus Early Neuromuscular Blockade Question 4 The early use of cis-atracurium in severe ARDS is: A. Contraindicated in patients with diabetes B. Associated
Instellen van beademingsparameters bij de obese pa3ent. MDO Nynke Postma
 Instellen van beademingsparameters bij de obese pa3ent MDO 19-1- 2015 Nynke Postma 1. Altered respiratory mechanics in obese pa@ents 2. Transpulmonary pressure 3. Titra@ng PEEP 4. Titra@ng @dal volume
Instellen van beademingsparameters bij de obese pa3ent MDO 19-1- 2015 Nynke Postma 1. Altered respiratory mechanics in obese pa@ents 2. Transpulmonary pressure 3. Titra@ng PEEP 4. Titra@ng @dal volume
Lung Recruitment Strategies in Anesthesia
 Lung Recruitment Strategies in Anesthesia Intraoperative ventilatory management to prevent Post-operative Pulmonary Complications Kook-Hyun Lee, MD, PhD Department of Anesthesiology Seoul National University
Lung Recruitment Strategies in Anesthesia Intraoperative ventilatory management to prevent Post-operative Pulmonary Complications Kook-Hyun Lee, MD, PhD Department of Anesthesiology Seoul National University
Prone Position in ARDS
 Prone Position in ARDS Rich Kallet MS RRT FAARC, FCCM Respiratory Care Services Department of Anesthesia & Perioperative Care University of California, San Francisco, San Francisco General Hospital Case
Prone Position in ARDS Rich Kallet MS RRT FAARC, FCCM Respiratory Care Services Department of Anesthesia & Perioperative Care University of California, San Francisco, San Francisco General Hospital Case
Ventilator ECMO Interactions
 Ventilator ECMO Interactions Lorenzo Del Sorbo, MD CCCF Toronto, October 2 nd 2017 Disclosure Relevant relationships with commercial entities: none Potential for conflicts within this presentation: none
Ventilator ECMO Interactions Lorenzo Del Sorbo, MD CCCF Toronto, October 2 nd 2017 Disclosure Relevant relationships with commercial entities: none Potential for conflicts within this presentation: none
Management of Severe ARDS: Current Canadian Practice
 Management of Severe ARDS: Current Canadian Practice Erick Duan MD FRCPC Clinical Scholar, Department of Medicine, Division of Critical Care, McMaster University Intensivist, St. Joseph's Healthcare Hamilton
Management of Severe ARDS: Current Canadian Practice Erick Duan MD FRCPC Clinical Scholar, Department of Medicine, Division of Critical Care, McMaster University Intensivist, St. Joseph's Healthcare Hamilton
RESCUE VENTILATION SUMMARY
 DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
Protective ventilation for ALL patients
 Protective ventilation for ALL patients PAOLO PELOSI, MD, FERS Department of Surgical Sciences and Integrated Diagnostics (DISC), San Martino Policlinico Hospital IRCCS for Oncology, University of Genoa,
Protective ventilation for ALL patients PAOLO PELOSI, MD, FERS Department of Surgical Sciences and Integrated Diagnostics (DISC), San Martino Policlinico Hospital IRCCS for Oncology, University of Genoa,
Surviving Sepsis Campaign. Guidelines for Management of Severe Sepsis/Septic Shock. An Overview
 Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
«Best» PEEP? Physiologic? Therapeutic? Optimal? Super? Preferred? Minimal? Right? Protective? Prophylactic?
 1936-2005 «Best» PEEP? Physiologic? Therapeutic? Optimal? Super? Preferred? Minimal? Right? Protective? Prophylactic? 1990-2000 Post cardiac arrest First day of mechanical ventilation 1990-1991 No patient
1936-2005 «Best» PEEP? Physiologic? Therapeutic? Optimal? Super? Preferred? Minimal? Right? Protective? Prophylactic? 1990-2000 Post cardiac arrest First day of mechanical ventilation 1990-1991 No patient
Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye
 Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye Steroids in ARDS: conclusion Give low-dose steroids if indicated for another problem
Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye Steroids in ARDS: conclusion Give low-dose steroids if indicated for another problem
ARDS A Brief Overview. Lucas Pitts, M.D. Assistant Professor of Medicine Pulmonary and Critical Care Medicine University of Kansas School of Medicine
 ARDS A Brief Overview Lucas Pitts, M.D. Assistant Professor of Medicine Pulmonary and Critical Care Medicine University of Kansas School of Medicine Outline Definition of ARDS Epidemiology of ARDS Pathophysiology
ARDS A Brief Overview Lucas Pitts, M.D. Assistant Professor of Medicine Pulmonary and Critical Care Medicine University of Kansas School of Medicine Outline Definition of ARDS Epidemiology of ARDS Pathophysiology
The new ARDS definitions: what does it mean?
 The new ARDS definitions: what does it mean? Richard Beale 7 th September 2012 METHODS ESICM convened an international panel of experts, with representation of ATS and SCCM The objectives were to update
The new ARDS definitions: what does it mean? Richard Beale 7 th September 2012 METHODS ESICM convened an international panel of experts, with representation of ATS and SCCM The objectives were to update
C h a p t e r 1 4 Ventilator Support
 C h a p t e r 1 4 Ventilator Support Shirish Prayag Ex. Hon. Asst. Prof of Medicine, BJ Medical College and Sassoon Hospital, Pune; Chief Consultant in Internal Medicine and Critical Care, Shree Medical
C h a p t e r 1 4 Ventilator Support Shirish Prayag Ex. Hon. Asst. Prof of Medicine, BJ Medical College and Sassoon Hospital, Pune; Chief Consultant in Internal Medicine and Critical Care, Shree Medical
1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation.
 Chapter 1: Principles of Mechanical Ventilation TRUE/FALSE 1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation. F
Chapter 1: Principles of Mechanical Ventilation TRUE/FALSE 1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation. F
Adult Extracorporeal Life Support (ECLS)
") Adult Extracorporeal Life Support (ECLS) Steven Scott, M.D., F.A.C.S. Piedmont Heart Institute Cardiothoracic Surgery Disclosures None ECMO = ECLS A technique of life support that involves a continuous
Adult Extracorporeal Life Support (ECLS) Steven Scott, M.D., F.A.C.S. Piedmont Heart Institute Cardiothoracic Surgery Disclosures None ECMO = ECLS A technique of life support that involves a continuous
ECMO: a breakthrough in care for respiratory failure. PD Dr. Thomas Müller Regensburg no conflict of interest
 ECMO: a breakthrough in care for respiratory failure? PD Dr. Thomas Müller Regensburg no conflict of interest 1 Overview Mortality of severe ARDS Indication for ECMO PaO 2 /FiO 2 Efficiency of ECMO: gas
ECMO: a breakthrough in care for respiratory failure? PD Dr. Thomas Müller Regensburg no conflict of interest 1 Overview Mortality of severe ARDS Indication for ECMO PaO 2 /FiO 2 Efficiency of ECMO: gas
USE OF INHALED NITRIC OXIDE IN THE NICU East Bay Newborn Specialists Guideline Prepared by P Joe, G Dudell, A D Harlingue Revised 7/9/2014
 USE OF INHALED NITRIC OXIDE IN THE NICU East Bay Newborn Specialists Guideline Prepared by P Joe, G Dudell, A D Harlingue Revised 7/9/2014 ino for Late Preterm and Term Infants with Severe PPHN Background:
USE OF INHALED NITRIC OXIDE IN THE NICU East Bay Newborn Specialists Guideline Prepared by P Joe, G Dudell, A D Harlingue Revised 7/9/2014 ino for Late Preterm and Term Infants with Severe PPHN Background:
Does proning patients with refractory hypoxaemia improve mortality?
 Does proning patients with refractory hypoxaemia improve mortality? Clinical problem and domain I selected this case because although this was the second patient we had proned in our unit within a week,
Does proning patients with refractory hypoxaemia improve mortality? Clinical problem and domain I selected this case because although this was the second patient we had proned in our unit within a week,
Author: Thomas Sisson, MD, 2009
 Author: Thomas Sisson, MD, 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Non-commercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author: Thomas Sisson, MD, 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Non-commercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Effects of mechanical ventilation on organ function. Masterclass ICU nurses
 Effects of mechanical ventilation on organ function Masterclass ICU nurses Case Male, 60 - No PMH - L 1.74 m and W 85 kg Pneumococcal pneumonia Stable hemodynamics - No AKI MV in prone position (PEEP 16
Effects of mechanical ventilation on organ function Masterclass ICU nurses Case Male, 60 - No PMH - L 1.74 m and W 85 kg Pneumococcal pneumonia Stable hemodynamics - No AKI MV in prone position (PEEP 16
Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor
 Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Clinical syndrome of severe dyspnea of rapid onset, hypoxemia, and diffuse pulmonary infiltrates leading to respiratory failure.
 Yuanlin Song, M.D. Clinical syndrome of severe dyspnea of rapid onset, hypoxemia, and diffuse pulmonary infiltrates leading to respiratory failure. Pneumonia Trauma SARS PaO2/fiO2
Yuanlin Song, M.D. Clinical syndrome of severe dyspnea of rapid onset, hypoxemia, and diffuse pulmonary infiltrates leading to respiratory failure. Pneumonia Trauma SARS PaO2/fiO2
Cardiorespiratory Physiotherapy Tutoring Services 2017
 VENTILATOR HYPERINFLATION ***This document is intended to be used as an information resource only it is not intended to be used as a policy document/practice guideline. Before incorporating the use of
VENTILATOR HYPERINFLATION ***This document is intended to be used as an information resource only it is not intended to be used as a policy document/practice guideline. Before incorporating the use of
Cardiorespiratory Interactions:
 Cardiorespiratory Interactions: The Heart - Lung Connection Jon N. Meliones, MD, MS, FCCM Professor of Pediatrics Duke University Medical Director PCVICU Optimizing CRI Cardiorespiratory Economics O2:
Cardiorespiratory Interactions: The Heart - Lung Connection Jon N. Meliones, MD, MS, FCCM Professor of Pediatrics Duke University Medical Director PCVICU Optimizing CRI Cardiorespiratory Economics O2:
Extracorporeal Membrane Oxygenation (ECMO)
") Extracorporeal Membrane Oxygenation (ECMO) Policy Number: Original Effective Date: MM.12.006 05/16/2006 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 01/01/2017 Section: Other/Miscellaneous
Extracorporeal Membrane Oxygenation (ECMO) Policy Number: Original Effective Date: MM.12.006 05/16/2006 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 01/01/2017 Section: Other/Miscellaneous
How ARDS should be treated in 2017
 How ARDS should be treated in 2017 2017, Ostrava Luciano Gattinoni, MD, FRCP Georg-August-Universität Göttingen Germany ARDS 1. Keep the patient alive respiration circulation 2. Cure the disease leading
How ARDS should be treated in 2017 2017, Ostrava Luciano Gattinoni, MD, FRCP Georg-August-Universität Göttingen Germany ARDS 1. Keep the patient alive respiration circulation 2. Cure the disease leading
Ventilation in Paediatric ARDS: extrapolate from adult studies?
 Ventilation in Paediatric ARDS: extrapolate from adult studies? ASMIC 2014 Dr Adrian Plunkett Consultant Paediatric Intensivist Birmingham Children s Hospital, UK Aims of the presentation Ventilation
Ventilation in Paediatric ARDS: extrapolate from adult studies? ASMIC 2014 Dr Adrian Plunkett Consultant Paediatric Intensivist Birmingham Children s Hospital, UK Aims of the presentation Ventilation
9/17/2014. Good Morning! 14th Annual Western Kansas Respiratory Care Seminar. 14th Annual Western Kansas Respiratory Care Seminar 28th
 Good Morning! 14th Annual Western Kansas Respiratory Care Seminar Current Status of Extracorporeal Membrane Oxygenation (ECMO) in Infants and Adults Kelly D. Hedlund, MS, CCP Chief Perfusionist Michael
Good Morning! 14th Annual Western Kansas Respiratory Care Seminar Current Status of Extracorporeal Membrane Oxygenation (ECMO) in Infants and Adults Kelly D. Hedlund, MS, CCP Chief Perfusionist Michael
Case scenario V AV ECMO. Dr Pranay Oza
 Case scenario V AV ECMO Dr Pranay Oza Case Summary 53 y/m, k/c/o MVP with myxomatous mitral valve with severe Mitral regurgitation underwent Mitral valve replacement with mini thoracotomy Pump time nearly
Case scenario V AV ECMO Dr Pranay Oza Case Summary 53 y/m, k/c/o MVP with myxomatous mitral valve with severe Mitral regurgitation underwent Mitral valve replacement with mini thoracotomy Pump time nearly
APPENDIX VI HFOV Quick Guide
 APPENDIX VI HFOV Quick Guide Overall goal: Maintain PH in the target range at the minimum tidal volume. This is achieved by favoring higher frequencies over lower P (amplitude). This goal is also promoted
APPENDIX VI HFOV Quick Guide Overall goal: Maintain PH in the target range at the minimum tidal volume. This is achieved by favoring higher frequencies over lower P (amplitude). This goal is also promoted
ARDS and Ventilators PG26 Update in Surgical Critical Care October 9, 2013
 ARDS and Ventilators PG26 Update in Surgical Critical Care October 9, 2013 Pauline K. Park MD, FACS, FCCM University of Michigan School of Medicine Ann Arbor, MI OVERVIEW New Berlin definition of ARDS
ARDS and Ventilators PG26 Update in Surgical Critical Care October 9, 2013 Pauline K. Park MD, FACS, FCCM University of Michigan School of Medicine Ann Arbor, MI OVERVIEW New Berlin definition of ARDS
11 th Annual Congress Turkish Thoracic Society. Mechanical Ventilation in Acute Hypoxemic Respiratory Failure
 11 th Annual Congress Turkish Thoracic Society Mechanical Ventilation in Acute Hypoxemic Respiratory Failure Lluis Blanch MD PhD Senior Critical Care Center Scientific Director Corporació Parc Taulí Universitat
11 th Annual Congress Turkish Thoracic Society Mechanical Ventilation in Acute Hypoxemic Respiratory Failure Lluis Blanch MD PhD Senior Critical Care Center Scientific Director Corporació Parc Taulí Universitat
Section: Therapy Effective Date: October 15, 2016 Subsection: Original Policy Date: June 19, 2015 Subject:
 Last Review Status/Date: September 2016 Page: 1 of 30 Summary Extracorporeal membrane oxygenation (ECMO) provides extracorporeal circulation and physiologic gas exchange for temporary cardiorespiratory
Last Review Status/Date: September 2016 Page: 1 of 30 Summary Extracorporeal membrane oxygenation (ECMO) provides extracorporeal circulation and physiologic gas exchange for temporary cardiorespiratory
ECMO BASICS CHLOE STEINSHOUER, MD PULMONARY AND SLEEP CONSULTANTS OF KANSAS
 ECMO BASICS CHLOE STEINSHOUER, MD PULMONARY AND SLEEP CONSULTANTS OF KANSAS DISCLOSURES No financial disclosures or conflicts of interest OBJECTIVES Define ECMO/ECLS and be able to identify the main types
ECMO BASICS CHLOE STEINSHOUER, MD PULMONARY AND SLEEP CONSULTANTS OF KANSAS DISCLOSURES No financial disclosures or conflicts of interest OBJECTIVES Define ECMO/ECLS and be able to identify the main types
Wanchai Wongkornrat Cardiovascular Thoracic Surgery Siriraj Hospital Mahidol University
 Wanchai Wongkornrat Cardiovascular Thoracic Surgery Siriraj Hospital Mahidol University Assess adequacy of ventilation and oxygenation Aids in establishing a diagnosis and severity of respiratory failure
Wanchai Wongkornrat Cardiovascular Thoracic Surgery Siriraj Hospital Mahidol University Assess adequacy of ventilation and oxygenation Aids in establishing a diagnosis and severity of respiratory failure
INDEPENDENT LUNG VENTILATION
 INDEPENDENT LUNG VENTILATION Giuseppe A. Marraro, MD Director Anaesthesia and Intensive Care Department Paediatric Intensive Care Unit Fatebenefratelli and Ophthalmiatric Hospital Milan, Italy gmarraro@picu.it
INDEPENDENT LUNG VENTILATION Giuseppe A. Marraro, MD Director Anaesthesia and Intensive Care Department Paediatric Intensive Care Unit Fatebenefratelli and Ophthalmiatric Hospital Milan, Italy gmarraro@picu.it
Pulmonary & Extra-pulmonary ARDS: FIZZ or FUSS?
 Pulmonary & Extra-pulmonary ARDS: FIZZ or FUSS? Dr. Rajagopala Srinivas Senior Resident, Dept. Pulmonary Medicine, PGIMER, Chandigarh. The beginning.. "The etiology of this respiratory distress syndrome
Pulmonary & Extra-pulmonary ARDS: FIZZ or FUSS? Dr. Rajagopala Srinivas Senior Resident, Dept. Pulmonary Medicine, PGIMER, Chandigarh. The beginning.. "The etiology of this respiratory distress syndrome
APRV Ventilation Mode
 APRV Ventilation Mode Airway Pressure Release Ventilation A Type of CPAP Continuous Positive Airway Pressure (CPAP) with an intermittent release phase. Patient cycles between two levels of CPAP higher
APRV Ventilation Mode Airway Pressure Release Ventilation A Type of CPAP Continuous Positive Airway Pressure (CPAP) with an intermittent release phase. Patient cycles between two levels of CPAP higher
Seminar. Current Concepts
 Seminar Current Concepts In ARDS What I think is possible to cover in 40 minutes- Definition Management Ventilatory strategies Conventional LPV Rescue therapy Non Ventilatory strategies Definition and
Seminar Current Concepts In ARDS What I think is possible to cover in 40 minutes- Definition Management Ventilatory strategies Conventional LPV Rescue therapy Non Ventilatory strategies Definition and
APRV: An Update CHLOE STEINSHOUER, MD PULMONARY & SLEEP CONSULTANTS OF KANSAS 04/06/2017
 APRV: An Update CHLOE STEINSHOUER, MD PULMONARY & SLEEP CONSULTANTS OF KANSAS 04/06/2017 Disclosures No conflicts of interest Objectives Attendees will be able to: Define the mechanism of APRV Describe
APRV: An Update CHLOE STEINSHOUER, MD PULMONARY & SLEEP CONSULTANTS OF KANSAS 04/06/2017 Disclosures No conflicts of interest Objectives Attendees will be able to: Define the mechanism of APRV Describe
Recruitment Maneuvers and Higher PEEP, the So-Called Open Lung Concept, in Patients with ARDS
 Zee and Gommers Critical Care (2019) 23:73 https://doi.org/10.1186/s13054-019-2365-1 REVIEW Recruitment Maneuvers and Higher PEEP, the So-Called Open Lung Concept, in Patients with ARDS Philip van der
Zee and Gommers Critical Care (2019) 23:73 https://doi.org/10.1186/s13054-019-2365-1 REVIEW Recruitment Maneuvers and Higher PEEP, the So-Called Open Lung Concept, in Patients with ARDS Philip van der
Extracorporeal Membrane Oxygenation (ECMO)
") Extracorporeal Membrane Oxygenation (ECMO) Policy Number: Original Effective Date: MM.12.006 05/16/2006 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 11/01/2014 Section: Other/Miscellaneous
Extracorporeal Membrane Oxygenation (ECMO) Policy Number: Original Effective Date: MM.12.006 05/16/2006 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 11/01/2014 Section: Other/Miscellaneous
Pulmonary Problems of the Neonate. Jon Palmer, VMD, DACVIM Chief, Neonatal Intensive Care Service New Bolton Center, University of Pennsylvania, USA
 Pulmonary Problems of the Neonate Jon Palmer, VMD, DACVIM Chief, Neonatal Intensive Care Service New Bolton Center, University of Pennsylvania, USA Lower Respiratory Diseases Ventilation/Perfusion Abnormalities
Pulmonary Problems of the Neonate Jon Palmer, VMD, DACVIM Chief, Neonatal Intensive Care Service New Bolton Center, University of Pennsylvania, USA Lower Respiratory Diseases Ventilation/Perfusion Abnormalities
Weaning from Mechanical Ventilation. Dr Azmin Huda Abdul Rahim
 Weaning from Mechanical Ventilation Dr Azmin Huda Abdul Rahim Content Definition Classification Weaning criteria Weaning methods Criteria for extubation Introduction Weaning comprises 40% of the duration
Weaning from Mechanical Ventilation Dr Azmin Huda Abdul Rahim Content Definition Classification Weaning criteria Weaning methods Criteria for extubation Introduction Weaning comprises 40% of the duration
Dr. Yasser Fathi M.B.B.S, M.Sc, M.D. Anesthesia Consultant, Head of ICU King Saud Hospital, Unaizah
 BY Dr. Yasser Fathi M.B.B.S, M.Sc, M.D Anesthesia Consultant, Head of ICU King Saud Hospital, Unaizah Objectives For Discussion Respiratory Physiology Pulmonary Graphics BIPAP Graphics Trouble Shootings
BY Dr. Yasser Fathi M.B.B.S, M.Sc, M.D Anesthesia Consultant, Head of ICU King Saud Hospital, Unaizah Objectives For Discussion Respiratory Physiology Pulmonary Graphics BIPAP Graphics Trouble Shootings
What is Acute Respiratory Distress Syndrome? Acute Respiratory Distress Syndrome (ARDS)
") Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Acute Respiratory Distress Syndrome (ARDS) What is Acute Respiratory Distress Syndrome?
 What is Acute Respiratory Distress Syndrome?") Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Agenda. Mechanical Ventilation in Morbidly Obese Patients. Paolo Pelosi. ESPCOP, Ostend, Belgium Saturday, November 14, 2009.
 Mechanical Ventilation in Morbidly Obese Patients t Paolo Pelosi Department of Ambient, Health and Safety University of Insubria - Varese, ITALY ppelosi@hotmail.com ESPCOP, Ostend, Belgium Saturday, November
Mechanical Ventilation in Morbidly Obese Patients t Paolo Pelosi Department of Ambient, Health and Safety University of Insubria - Varese, ITALY ppelosi@hotmail.com ESPCOP, Ostend, Belgium Saturday, November
Pulmonary circulation. Lung Blood supply : lungs have a unique blood supply system :
 Dr. Ali Naji Pulmonary circulation Lung Blood supply : lungs have a unique blood supply system : 1. Pulmonary circulation 2. Bronchial circulation 1- Pulmonary circulation : receives the whole cardiac
Dr. Ali Naji Pulmonary circulation Lung Blood supply : lungs have a unique blood supply system : 1. Pulmonary circulation 2. Bronchial circulation 1- Pulmonary circulation : receives the whole cardiac
ECMO Experience from ECMO-ICU, Karolinska
 ECMO Experience from ECMO-ICU, Karolinska X Curso de Ventilacion Mecanica en Anestesia, Cuidados Criticos y Transplantes Madrid 2012 International numbers Totally since 1989; 46500 patients as of July
ECMO Experience from ECMO-ICU, Karolinska X Curso de Ventilacion Mecanica en Anestesia, Cuidados Criticos y Transplantes Madrid 2012 International numbers Totally since 1989; 46500 patients as of July
Prone ventilation revisited in H1N1 patients
 International Journal of Advanced Multidisciplinary Research ISSN: 2393-8870 www.ijarm.com DOI: 10.22192/ijamr Volume 5, Issue 10-2018 Case Report DOI: http://dx.doi.org/10.22192/ijamr.2018.05.10.005 Prone
International Journal of Advanced Multidisciplinary Research ISSN: 2393-8870 www.ijarm.com DOI: 10.22192/ijamr Volume 5, Issue 10-2018 Case Report DOI: http://dx.doi.org/10.22192/ijamr.2018.05.10.005 Prone
Case Scenarios. Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC. Consultant, Critical Care Medicine Medanta, The Medicity
 Case Scenarios Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Case 1 A 36 year male with cirrhosis and active GI bleeding is intubated to protect his airway,
Case Scenarios Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Case 1 A 36 year male with cirrhosis and active GI bleeding is intubated to protect his airway,
Artificial Lung: A New Inspiration
 Artificial Lung: A New Inspiration Joseph B. Zwischenberger MD Johnston-Wright Professor and Chairman: Department of Surgery j.zwische@uky.edu The University of Kentucky Lexington, Kentucky Presenter Disclosure
Artificial Lung: A New Inspiration Joseph B. Zwischenberger MD Johnston-Wright Professor and Chairman: Department of Surgery j.zwische@uky.edu The University of Kentucky Lexington, Kentucky Presenter Disclosure
ARDS - a must know. Page 1 of 14
 ARDS - a must know Poster No.: C-1683 Congress: ECR 2016 Type: Authors: Keywords: DOI: Educational Exhibit M. Cristian; Turda/RO Education and training, Edema, Acute, Localisation, Education, Digital radiography,
ARDS - a must know Poster No.: C-1683 Congress: ECR 2016 Type: Authors: Keywords: DOI: Educational Exhibit M. Cristian; Turda/RO Education and training, Edema, Acute, Localisation, Education, Digital radiography,
NIV use in ED. Dr. Khalfan AL Amrani Emergency Resuscitation Symposium 2 nd May 2016 SQUH
 NIV use in ED Dr. Khalfan AL Amrani Emergency Resuscitation Symposium 2 nd May 2016 SQUH Outline History & Introduction Overview of NIV application Review of proven uses of NIV History of Ventilation 1940
NIV use in ED Dr. Khalfan AL Amrani Emergency Resuscitation Symposium 2 nd May 2016 SQUH Outline History & Introduction Overview of NIV application Review of proven uses of NIV History of Ventilation 1940
Charisma High-flow CPAP solution
 Charisma High-flow CPAP solution Homecare PNEUMOLOGY Neonatology Anaesthesia INTENSIVE CARE VENTILATION Sleep Diagnostics Service Patient Support charisma High-flow CPAP solution Evidence CPAP therapy
Charisma High-flow CPAP solution Homecare PNEUMOLOGY Neonatology Anaesthesia INTENSIVE CARE VENTILATION Sleep Diagnostics Service Patient Support charisma High-flow CPAP solution Evidence CPAP therapy
Extracorporeal support in acute respiratory failure. Dr Anthony Bastin Consultant in critical care Royal Brompton Hospital, London
 Extracorporeal support in acute respiratory failure Dr Anthony Bastin Consultant in critical care Royal Brompton Hospital, London Objectives By the end of this session, you will be able to: Describe different
Extracorporeal support in acute respiratory failure Dr Anthony Bastin Consultant in critical care Royal Brompton Hospital, London Objectives By the end of this session, you will be able to: Describe different
New Strategies in the Management of Patients with Severe Sepsis
 New Strategies in the Management of Patients with Severe Sepsis Michael Zgoda, MD, MBA President, Medical Staff Medical Director, ICU CMC-University, Charlotte, NC Factors of increases in the dx. of severe
New Strategies in the Management of Patients with Severe Sepsis Michael Zgoda, MD, MBA President, Medical Staff Medical Director, ICU CMC-University, Charlotte, NC Factors of increases in the dx. of severe
Learning Objectives. 1. Indications versus contra-indications 2. CPAP versus NiVS 3. Clinical evidence
 Learning Objectives 1. Indications versus contra-indications 2. CPAP versus NiVS 3. Clinical evidence Pre-hospital Non-invasive vventilatory support Marc Gillis, MD Imelda Bonheiden Our goal out there
Learning Objectives 1. Indications versus contra-indications 2. CPAP versus NiVS 3. Clinical evidence Pre-hospital Non-invasive vventilatory support Marc Gillis, MD Imelda Bonheiden Our goal out there
UPMC Critical Care
 UPMC Critical Care www.ccm.pitt.edu Cardiovascular insufficiency with Initiation and Withdrawal of Mechanical Ventilation Michael R. Pinsky, MD, Dr hc Department of Critical Care Medicine University of
UPMC Critical Care www.ccm.pitt.edu Cardiovascular insufficiency with Initiation and Withdrawal of Mechanical Ventilation Michael R. Pinsky, MD, Dr hc Department of Critical Care Medicine University of
Acute respiratory distress syndrome
 20 Acute respiratory distress syndrome Introduction i Key points Acute respiratory distress syndrome is triggered by injury to the alveolar capillary barrier from any of a variety of causes, resulting
20 Acute respiratory distress syndrome Introduction i Key points Acute respiratory distress syndrome is triggered by injury to the alveolar capillary barrier from any of a variety of causes, resulting
Pro: Early use of VV ECMO for ARDS
 Pro: Early use of VV ECMO for ARDS Kyle J. Rehder, MD, FCCP Associate Professor Division of Pediatric Critical Care Medicine Department of Pediatrics Duke Children s Hospital The ventilator is slowly killing
Pro: Early use of VV ECMO for ARDS Kyle J. Rehder, MD, FCCP Associate Professor Division of Pediatric Critical Care Medicine Department of Pediatrics Duke Children s Hospital The ventilator is slowly killing
Lecture Notes. Chapter 2: Introduction to Respiratory Failure
 Lecture Notes Chapter 2: Introduction to Respiratory Failure Objectives Define respiratory failure, ventilatory failure, and oxygenation failure List the causes of respiratory failure Describe the effects
Lecture Notes Chapter 2: Introduction to Respiratory Failure Objectives Define respiratory failure, ventilatory failure, and oxygenation failure List the causes of respiratory failure Describe the effects
Acute Respiratory Failure. Respiratory Failure. Respiratory Failure. Acute Respiratory Failure. Ventilatory Failure. Type 1 Respiratory Failure
 Acute Respiratory Failure Physiologic Classification Acute Respiratory Failure Type 1 Hypoxemic Type 2 Ventilatory Type 3 Post-op Type 4 Shock Mechanism Shunt Va Atelectasis Cardiac Output Phil Factor,
Acute Respiratory Failure Physiologic Classification Acute Respiratory Failure Type 1 Hypoxemic Type 2 Ventilatory Type 3 Post-op Type 4 Shock Mechanism Shunt Va Atelectasis Cardiac Output Phil Factor,
Best of Pulmonary Jennifer R. Hucks, MD University of South Carolina School of Medicine
 Best of Pulmonary 2012-2013 Jennifer R. Hucks, MD University of South Carolina School of Medicine Topics ARDS- Berlin Definition Prone Positioning For ARDS Lung Protective Ventilation In Patients Without
Best of Pulmonary 2012-2013 Jennifer R. Hucks, MD University of South Carolina School of Medicine Topics ARDS- Berlin Definition Prone Positioning For ARDS Lung Protective Ventilation In Patients Without
Extracorporeal Life Support Organization (ELSO) Guidelines for Pediatric Respiratory Failure
 Guidelines for Pediatric Respiratory Failure") Extracorporeal Life Support Organization (ELSO) Guidelines for Pediatric Respiratory Failure Introduction This pediatric respiratory failure guideline is a supplement to ELSO s General Guidelines for all
Extracorporeal Life Support Organization (ELSO) Guidelines for Pediatric Respiratory Failure Introduction This pediatric respiratory failure guideline is a supplement to ELSO s General Guidelines for all