Emergency Department Thoracotomy. Khalid Al Johani. MD EM & Trauma consultant
|
|
|
- Emily Nichols
- 5 years ago
- Views:
Transcription

1 Emergency Department Thoracotomy Khalid Al Johani. MD EM & Trauma consultant
2 Background Thoracic trauma is one of the leading causes of death worldwide in all age groups and accounts for 25-50% of all traumatic injuries. EDT intruduced in 1900 Intense debate It is adrastic,last effort to save life
3 Background Cont d Survival rates following Emergency Department Thoracotomy (EDT) for penetrating thoracic trauma is 9-12% (up to 38% with signs of life); where as for blunt trauma survival rates are 1-2% regardless of clinical signs.
4 Remains contraversial, survival rate up to 60% others have argued that EDT is futile and expensive procedure that put the health care providers at risk
5 Definitions Emergency Department Thoracotomy (EDT): Occurring immediately in the emergency department as an integral part of the initial resuscitation process shortly after presentation. Urgent Thoracotomy: Thoracotomy performed in the operating theatre.
6 Signs Of Life (SOL) Increased EDT Survival rates are associated with signs of life in the E D, including the followings Pupillary response to light Respiratory effort Cardiac activity on the ECG Spontaneous Movement Palpable pulse
7 Best Survival Rate EDT for stab injuries who arrived with SOL

8 Factors associated with increased survival rate High blood pressure High respiratory rate High GCS
9 Low Survival Rates Multitrauma No SOL in the field Blunt trauma due to conditions like cardiac contusion, aortic rupture cardiac rupture
10 GSW injuries survival rate USUALLY are un able to seal spontaneously because of the large nature of the missile injury pattern
11 EDT - Accepted Indications Penetrating Thoracic Trauma : Traumatic arrest with previously witnessed cardiac activity Patient with < 5 mins of CPR on arrival Patient in extremis (BP <60 not responding to fluid resuscitation) on arrival to ED Witnessed cardiac arrest in the ED Blunt Thoracic Trauma : Witnessed cardiac arrest in the ED. Patients age and co-morbidity needs to be taken into account when making a decision to undertake an EDT Rapid exsanguinations from chest tube (>1500ml)
12 EDT - Relative Indications Penetrating Thoracic Trauma Traumatic arrest without previously witnessed cardiac activity Penetrating Non-Thoracic Trauma : Traumatic arrest with previously witnessed cardiac activity Blunt Thoracic Trauma: Traumatic arrest with previously witnessed cardiac activity
13 EDT decision should be made case by case basis
14 EDT - Contraindications Blunt Trauma: Blunt thoracic injuries with no witnessed cardiac activity Multiple blunt trauma Severe head injury Non traumatic arrest Improperly trained team Insufficient equipments
15 Prospective multi centre study EDT doesnot yield survival if the follwoings are noted Blunt trauma with more than 10 minutes CPR in prehospital without response Pentrating trauma with more than 15 CPR with no rsponse Asystole without cardiac tamponade

16 The EDT Procedure
17 Aims of an EDT Resuscitation of a patient in extremis with a penetrating injury by: Release cardiac tamponade Control hemorrhage Perform open cardiac massage Cross clamp the descending thoracic aorta Control air embolism
18 Equipment Personal protective equipment and preparation Gloves Sterile gloves Gown Face shield Povidone iodine (Betadine) Sterile drapes
19 To enter the chest cavity Scalpel, No. 10 or No. 20 blade Mayo scissors (alternatively, Metzenbaum scissors) Rib spreaders (eg, Finochietto) Trauma shears or saw (eg, Gigli)
20 EDT Tray Cont d
21 EDT Tray
, 2-0 or larger, on large round-body needle Cardiovascular Ethibond sutures, 3-0 Teflon pledgets Suture scissors Kelly")
22 To control hemorrhage and repair injury Tissue/tooth forceps Satinsky vascular clamps (large and small) Long and short needle holders (eg, Hegar) Nonabsorbable sutures (silk), 2-0 or larger, on large round-body needle Cardiovascular Ethibond sutures, 3-0 Teflon pledgets Suture scissors Kelly clamp
23 Skin stapler High-volume suction device Laparotomy packs Tonsil clamps Aortic clamp instrument Foley catheter, 20F with 30-mL balloon Laparotomy pads Teflon patches Internal defibrillator
24 Approach A supine anterolateral thoracotomy Raise the patient left arm above the head left sided approach is used in all patients and with injuries to the left chest Patients who are not arrested but with profound hypotension and right sided injuries have their right chest opened first.
25 Prepare the patient left and right side with iodine Drape the area with sterile towels Airway control for all, if the thoracic organs are suspected do selective right main bronchus by pushing the tube to 30 cm
26 # Stop ventilation momentarily when you enter the pleural cavity to allow the lung to collapse # The rib spreader should be placed with the handle downward to allow for extenesion # In both cases it may become necessary to extend the incision across the sternum. # Skin incision is made in the 4th intercostal space above the fifth rib, from sternal border to the mid axillary line.
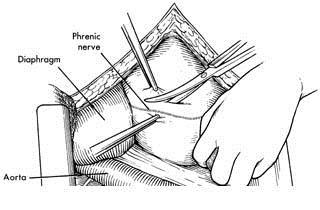
27 Relief of Tamponade : The pericardium is opened longitudinally to avoid damage to the phrenic nerve, the pericardium should always be opened to assess for retro cardiac blood. The operator can use his fingers to disect after the initial incision If cardiac lacerations are seen, digital occlussion,intterrupted sutures, or clamps (satinsky) to repair
28 EDT - Operative Technique
29 Control of Hemorrhage : Cardiac wounds : controlled initially with direct finger pressure. sutured using non-absorbable 3/0 sutures mattress sutures are used to avoid obstructing coronary flow Pulmonary & Hilar injuries. temporarily controlled with finger pressure at the pulmonary hilum.
30 EDT - Operative Technique Cont d
31 Control of Hemorrhage: Cont d Pulmonary & Hilar injuries : (Cont d) This may be augmented by placement of a Satinsky clamp across the hilum Lesser haemorrhage from the lung parenchymas can be controlled with a temporary clamp Great vessel injuries : Small aortic injuries can be sutured directly using the 3/0 Larger injuries, especially to the arch may require temporary digital occlusion and insitution of cardiac bypass.
32 Aortic cross-clamping : The rationale for clamping the aorta is to redistribute blood flow to the coronary vessels, lungs and brain, Clamp time should ideally be 30 minutes or less. Cross-clamping is done ideally distal to the level of the diaphragm, to maximise spinal cord perfusion Near the level of the diaphragm to control bleeding in abdominal vascular injuries.

33 EDT - Operative Technique
34 Retaract the left lung superiorly to expose the aorta, the aorta lies anterior to vertebra wherase the esophagus lies anterior and medial to the aorta The aorta feels rubbery, firm and pulsatile In hypotensive pt NGT inserted to distinguish the esophagus from aorta
35 EDT - Operative Technique Cont d
36 Internal cardiac massage internal cardiac massage should be started as soon as possible A two-handed technique produces a better cardiac output. Compared with standard CPR,which delivers up to 20% of the cardiac output, internal CPR produces up to 55% of the body perfusion
37 EDT - Operative Technique Cont d
38 Internal defibrillation begins at 20 joules and increased to j Avoid touching the coronaries with plades Fluid resuscitation should start after bleeding control, warmed fluid, blood and clotting factors Inotrope support after fluid resus
39 Pitfalls Anoxic brain death ocurrs in 50% of survivors Peroperative Heart Injury Suture Over Coronary Artery Peroperative Lung Injury Peroperative Oesophageal Injury Damage to phrenic nerve Damage to esophagus Recurrent bleeding from chest wall or mammary artery
40 Pearls Blunt trauma survival rate much lower than penetrating injury Airway control is standard NGT to distinguish the esophagus from aorta Immediate surgical consult
41 Left anterolateral approach when the site of injury is unknown Incision over the 5 th rib, 4 th intercostal spase Consider potential organs donor rescue after EDT arrest
42 Indications Stab wounds Deep shock (BP<70 mmhg) Non responder Cardiac arrest in the ED 10 min CPR SUMMARY Emergency procedure now! 1 out of 4 can be saved EDT is part of damage control
43 References 1.Hunt P, Greaves I, Owens W. Emergency thoracotomy in thoracic trauma -a review. Injury. 2006; 37: IATSIC. Manual of Definitive Surgical Trauma Care. 2nd ed. Great Britian: Hodder Arnold; 2007: Pages. 3.Soreide K, Petrone P, Asensio JA. Emergency thoracotomy in trauma: rationale, risks and realities. Scandinavian Journal of Surgery. 2007; 96: American College of Surgeons. Working Group AHCo. Practice Management Guidelines for Emergency Department Thoracotomy. Journal American College of Surgeons. 2001; 193: Rhee PM, Acosta J, Bridgeman A, Wang D, Jordon M, Rich N. Survival after emergency department thoracotomy: Review of the published data from the past 25 years. Journal American College of Surgeons. 2000; 190(3): Feliciano D. Thoracotomy in the Emergency Department Mejia J, Stewart R, Cohn S. Emergency Department Thoracotomy. Thoracic and Cardiovascular Surgery. 2008; 20: ATLS. Advanced Trauma Life Support : Program for Doctors. 8th ed. Chicago: American College of Surgeons; 2008: Pages. 9.Doll D, Bonanno F, Smith M, Deginannis E. Emergency Department Thoracotomy (EDT). Trauma. 2005; 7: Grove C, Lemmon G, Anderson G, McCarthy M. Emergency Thoracotomy: Appropriate Use in Resusitation of Trauma Patients. The American Surgeon. 2002; 68(4): Biffl W, Moore E, Harken A. Emergency Department Thoracotomy. In: Mattox K, Feliciano D, Moore E, eds. Trauma. 4th ed. New York: McGraw-Hill; 2000: 245.
44 THANKS, TASHUKURAT, SHUKRAN
Emergency Department Thoracotomy
 Emergency Department Thoracotomy November 3, 2017 North Oaks Shock Trauma Symposium Jeremy R. Timmer, M.D., FACS Objectives Background of RT Indications for RT Contraindications for RT Survival Benefits
Emergency Department Thoracotomy November 3, 2017 North Oaks Shock Trauma Symposium Jeremy R. Timmer, M.D., FACS Objectives Background of RT Indications for RT Contraindications for RT Survival Benefits
ED Thoracotomy Left chest opened and extended across sternum with 1000mL blood drained Pericardium opened with 100mL blood drained 1cm laceration in t
 Case Report 39yM stabbed in the left upper chest by wife with kitchen knife. Intubated in the field. Loss of vitals on arrival to hospital while in ambulance. In ED, (-) palpable pulse and (+) organized
Case Report 39yM stabbed in the left upper chest by wife with kitchen knife. Intubated in the field. Loss of vitals on arrival to hospital while in ambulance. In ED, (-) palpable pulse and (+) organized
Pre-Hospital and Emergency Department Resuscitative Thoracotomy
 Pre-Hospital and Emergency Department Programme Directors: Mr Jim Connolly Consultant A&E Surgeon Accident and Emergency Department, Royal Victoria Infirmary Dr Paul Wallman Consultant in Emergency Medicine
Pre-Hospital and Emergency Department Programme Directors: Mr Jim Connolly Consultant A&E Surgeon Accident and Emergency Department, Royal Victoria Infirmary Dr Paul Wallman Consultant in Emergency Medicine
Trauma. Neck trauma zones. Neck Injuries 1/3/2018. Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure
 Trauma 45 minutes highest points Ahmed Mahmoud, MD Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure Neck trauma zones Airway ;Rapid sequence intubation Breathing ;Needle
Trauma 45 minutes highest points Ahmed Mahmoud, MD Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure Neck trauma zones Airway ;Rapid sequence intubation Breathing ;Needle
Acute Pericardial Tamponade
 Acute Pericardial Tamponade Marx: Rosen's Emergency Medicine: Concepts and Clinical Practice, 5th ed. Epidemiology The reported incidence of acute pericardial tamponade is approximately 2% in patients
Acute Pericardial Tamponade Marx: Rosen's Emergency Medicine: Concepts and Clinical Practice, 5th ed. Epidemiology The reported incidence of acute pericardial tamponade is approximately 2% in patients
M-AFRAKHTEH. MD OCT.2017 SHOHADA HOSPITAL TAJRISH
 Unrestricted M-AFRAKHTEH. MD OCT.2017 SHOHADA HOSPITAL TAJRISH Patients at imminent risk of exsanguination Manual aortic compression Resuscitative endovascular balloon occlusion of the aorta Uterine tourniquet
Unrestricted M-AFRAKHTEH. MD OCT.2017 SHOHADA HOSPITAL TAJRISH Patients at imminent risk of exsanguination Manual aortic compression Resuscitative endovascular balloon occlusion of the aorta Uterine tourniquet
RCH Trauma Guideline. Management of Traumatic Pneumothorax & Haemothorax. Trauma Service, Division of Surgery
 RCH Trauma Guideline Management of Traumatic Pneumothorax & Haemothorax Trauma Service, Division of Surgery Aim To describe safe and competent management of traumatic pneumothorax and haemothorax at RCH.
RCH Trauma Guideline Management of Traumatic Pneumothorax & Haemothorax Trauma Service, Division of Surgery Aim To describe safe and competent management of traumatic pneumothorax and haemothorax at RCH.
The ABC s of Chest Trauma
 The ABC s of Chest Trauma J Bradley Pickhardt MD, FACS Providence St Patrick Hospital What s the Problem? 2/3 of trauma patients have chest trauma Responsible for 25% of all trauma deaths Most injuries
The ABC s of Chest Trauma J Bradley Pickhardt MD, FACS Providence St Patrick Hospital What s the Problem? 2/3 of trauma patients have chest trauma Responsible for 25% of all trauma deaths Most injuries
Chest Tube Thoracostomy
 Chest Tube Thoracostomy INTRODUCTION A chest tube thoracostomy is commonly done in the ED to evacuate an abnormal accumulation of fluid (blood, empyema) or air from the pleural space under an elective,
Chest Tube Thoracostomy INTRODUCTION A chest tube thoracostomy is commonly done in the ED to evacuate an abnormal accumulation of fluid (blood, empyema) or air from the pleural space under an elective,
CHEST INJURIES. Jacek Piątkowski M.D., Ph. D.
 CHEST INJURIES Jacek Piątkowski M.D., Ph. D. CHEST INJURIES 3-4% of all injuries 8% of patients hospitalized due to injuries 65% of patients who died at the accident place CLASSIFICATION OF THE CHEST INJURIES
CHEST INJURIES Jacek Piątkowski M.D., Ph. D. CHEST INJURIES 3-4% of all injuries 8% of patients hospitalized due to injuries 65% of patients who died at the accident place CLASSIFICATION OF THE CHEST INJURIES
CHEST DRAIN PROTOCOL
 CHEST DRAIN PROTOCOL Rationale The pleural membranes have an important role in effective lung expansion. The visceral pleura is a thin, smooth, serous membrane covering the surface of the lungs and is
CHEST DRAIN PROTOCOL Rationale The pleural membranes have an important role in effective lung expansion. The visceral pleura is a thin, smooth, serous membrane covering the surface of the lungs and is
The Primary Survey. C. Clay Cothren, MD FACS. Attending Surgeon, Denver Health Medical Center Assistant Professor of Surgery, University of Colorado
 The Primary Survey C. Clay Cothren, MD FACS Attending Surgeon, Denver Health Medical Center Assistant Professor of Surgery, University of Colorado Outlining the ABCs Why do we need such an approach? The
The Primary Survey C. Clay Cothren, MD FACS Attending Surgeon, Denver Health Medical Center Assistant Professor of Surgery, University of Colorado Outlining the ABCs Why do we need such an approach? The
Procedure: Chest Tube Placement (Tube Thoracostomy)
") Procedure: Chest Tube Placement (Tube Thoracostomy) Basic Information: The insertion and placement of a chest tube into the pleural cavity for the purpose of removing air, blood, purulent drainage, or
Procedure: Chest Tube Placement (Tube Thoracostomy) Basic Information: The insertion and placement of a chest tube into the pleural cavity for the purpose of removing air, blood, purulent drainage, or
(SKILLS/HANDS-ON) Chest Tubes. Rebecca Carman, MSN, ACNP-BC. Amanda Shumway, PA-C. Thomas W. White, MD, FACS, CNSC
 Chest Tubes. Rebecca Carman, MSN, ACNP-BC. Amanda Shumway, PA-C. Thomas W. White, MD, FACS, CNSC") (SKILLS/HANDS-ON) Chest Tubes Rebecca Carman, MSN, ACNP-BC Nurse Practitioner, Trauma Services, Intermountain Medical Center, Intermountain Healthcare Amanda Shumway, PA-C APC Trauma and Critical Care
(SKILLS/HANDS-ON) Chest Tubes Rebecca Carman, MSN, ACNP-BC Nurse Practitioner, Trauma Services, Intermountain Medical Center, Intermountain Healthcare Amanda Shumway, PA-C APC Trauma and Critical Care
PEMSS PROTOCOLS INVASIVE PROCEDURES
 PEMSS PROTOCOLS INVASIVE PROCEDURES Panhandle Emergency Medical Services System SURGICAL AND NEEDLE CRICOTHYROTOMY Inability to intubate is the primary indication for creating an artificial airway. Care
PEMSS PROTOCOLS INVASIVE PROCEDURES Panhandle Emergency Medical Services System SURGICAL AND NEEDLE CRICOTHYROTOMY Inability to intubate is the primary indication for creating an artificial airway. Care
Cardiac Arrest due to Trauma
 Cardiac Arrest due to Trauma Colonel Michael Reade MBBS MPH DPhil DMedSc DIMCRCSEd AFRACMA FANZCA FCICM ADF Professor of Military Medicine & Surgery University of Queensland & ADF Joint Health Command
Cardiac Arrest due to Trauma Colonel Michael Reade MBBS MPH DPhil DMedSc DIMCRCSEd AFRACMA FANZCA FCICM ADF Professor of Military Medicine & Surgery University of Queensland & ADF Joint Health Command
Imaging of Thoracic Trauma: Tips and Traps. Arun C. Nachiappan, MD Associate Professor of Clinical Radiology University of Pennsylvania
 Imaging of Thoracic Trauma: Tips and Traps Arun C. Nachiappan, MD Associate Professor of Clinical Radiology University of Pennsylvania None Disclosures Objectives Describe blunt and penetrating traumatic
Imaging of Thoracic Trauma: Tips and Traps Arun C. Nachiappan, MD Associate Professor of Clinical Radiology University of Pennsylvania None Disclosures Objectives Describe blunt and penetrating traumatic
PATCHING AND SECTION OF THE PULMONARY ORIFICE OF THE HEART.*
 Published Online: 1 July, 1914 Supp Info: http://doi.org/10.1084/jem.20.1.3 Downloaded from jem.rupress.org on December 24, 2018 PATCHING AND SECTION OF THE PULMONARY ORIFICE OF THE HEART.* BY THEODORE
Published Online: 1 July, 1914 Supp Info: http://doi.org/10.1084/jem.20.1.3 Downloaded from jem.rupress.org on December 24, 2018 PATCHING AND SECTION OF THE PULMONARY ORIFICE OF THE HEART.* BY THEODORE
The Management of Chest Trauma. Tom Scaletta, MD FAAEM Immediate Past President, AAEM
 The Management of Chest Trauma Tom Scaletta, MD FAAEM Immediate Past President, AAEM Trichotomizing Rib Fractures Upper 1-3 vascular injuries Middle 4-9 Lower 10-12 12 liver/spleen injuries Management
The Management of Chest Trauma Tom Scaletta, MD FAAEM Immediate Past President, AAEM Trichotomizing Rib Fractures Upper 1-3 vascular injuries Middle 4-9 Lower 10-12 12 liver/spleen injuries Management
Title of Guideline (must include the word Guideline (not. Guidelines. Contact Name and Job Title (author)
") Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Contact Name and Job Title (author) Directorate & Speciality Date of submission Date on which guideline must be
Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Contact Name and Job Title (author) Directorate & Speciality Date of submission Date on which guideline must be
Chapter 29 - Chest Injuries
 1 2 3 4 5 6 7 8 9 National EMS Education Standard Competencies (1 of 5) Trauma Applies fundamental knowledge to provide basic emergency care and transportation based on assessment findings for an acutely
1 2 3 4 5 6 7 8 9 National EMS Education Standard Competencies (1 of 5) Trauma Applies fundamental knowledge to provide basic emergency care and transportation based on assessment findings for an acutely
Chapter 16. Thoracic Injuries
 Thoracic Injuries Chapter 16 Thoracic Injuries Introduction About 15% of war injuries involve the chest. Of those, 10% are superficial (soft tissue only) requiring only basic wound treatment. The remaining
Thoracic Injuries Chapter 16 Thoracic Injuries Introduction About 15% of war injuries involve the chest. Of those, 10% are superficial (soft tissue only) requiring only basic wound treatment. The remaining
In ESH we usually see blunt chest trauma but penetrating injuries also treated here (usually as single injuries, like stab wound)
") Chest Trauma Dr Csaba Dioszeghy MD PhD FRCEM FFICM FERC East Surrey Hospital Emergency Department Scope Thoracic injuries are common and can be life threatening In ESH we usually see blunt chest trauma
Chest Trauma Dr Csaba Dioszeghy MD PhD FRCEM FFICM FERC East Surrey Hospital Emergency Department Scope Thoracic injuries are common and can be life threatening In ESH we usually see blunt chest trauma
Penetrating Cardiac Injury
 Penetrating Cardiac Injury Getting to the Heart of the Matter Marilyn Ng, MD Dept. of Surgery Conference Downstate Medical Center Aug 11, 2011 Case Presentation 28 yo M with unknown PMHx Level 1 notification
Penetrating Cardiac Injury Getting to the Heart of the Matter Marilyn Ng, MD Dept. of Surgery Conference Downstate Medical Center Aug 11, 2011 Case Presentation 28 yo M with unknown PMHx Level 1 notification
Thoracic Injuries. Chapter 16
 Thoracic Injuries Chapter 16 Thoracic Injuries Introduction About 15% of war injuries involve the torso. Those injuries involving the vasculature of the mediastinum (heart, great vessels, and pulmonary
Thoracic Injuries Chapter 16 Thoracic Injuries Introduction About 15% of war injuries involve the torso. Those injuries involving the vasculature of the mediastinum (heart, great vessels, and pulmonary
Critical Care Monitoring. Indications. Pleural Space. Chest Drainage. Chest Drainage. Potential space. Contains fluid lubricant
 Critical Care Monitoring Indications 1-2- 2 Pleural Space Potential space Contains fluid lubricant Can fill with air, blood, plasma, serum, lymph, pus 3 1 Pleural Space Problems when contain abnormal substances:
Critical Care Monitoring Indications 1-2- 2 Pleural Space Potential space Contains fluid lubricant Can fill with air, blood, plasma, serum, lymph, pus 3 1 Pleural Space Problems when contain abnormal substances:
Trust Guidelines. Title: Guidelines for chest drain insertion
 Trust Guidelines Title: Guidelines for chest drain insertion Authors: Dr JCT Pepperell; Dr J Tipping; J Hansford Ratified by: Planned Care and Emergency & Urgent Care Divisional Governance Committees Active
Trust Guidelines Title: Guidelines for chest drain insertion Authors: Dr JCT Pepperell; Dr J Tipping; J Hansford Ratified by: Planned Care and Emergency & Urgent Care Divisional Governance Committees Active
Chapter 29 - Chest_and_Abdominal_Trauma
 Introduction to Emergency Medical Care 1 OBJECTIVES 29.1 Define key terms introduced in this chapter. Slides 11, 15, 18, 27 29.2 Describe mechanisms of injury commonly associated with chest injuries. Slides
Introduction to Emergency Medical Care 1 OBJECTIVES 29.1 Define key terms introduced in this chapter. Slides 11, 15, 18, 27 29.2 Describe mechanisms of injury commonly associated with chest injuries. Slides
Evaluation & Management of Penetrating Wounds to the NECK
 Evaluation & Management of Penetrating Wounds to the NECK Goal Effectively identify patients with a high probability of injury requiring surgical intervention Define the role of diagnostic tests in assessing
Evaluation & Management of Penetrating Wounds to the NECK Goal Effectively identify patients with a high probability of injury requiring surgical intervention Define the role of diagnostic tests in assessing
The Primary Survey. Clay Cothren Burlew, MD FACS
 The Primary Survey Clay Cothren Burlew, MD FACS Director, Surgical Intensive Care Unit Attending Surgeon, Denver Health Medical Center Associate Professor of Surgery, University of Colorado Outlining the
The Primary Survey Clay Cothren Burlew, MD FACS Director, Surgical Intensive Care Unit Attending Surgeon, Denver Health Medical Center Associate Professor of Surgery, University of Colorado Outlining the
Lecture 2: Clinical anatomy of thoracic cage and cavity II
 Lecture 2: Clinical anatomy of thoracic cage and cavity II Dr. Rehan Asad At the end of this session, the student should be able to: Identify and discuss clinical anatomy of mediastinum such as its deflection,
Lecture 2: Clinical anatomy of thoracic cage and cavity II Dr. Rehan Asad At the end of this session, the student should be able to: Identify and discuss clinical anatomy of mediastinum such as its deflection,
RESUSCITATION IN TRAUMA. Important things I have learnt
 RESUSCITATION IN TRAUMA Important things I have learnt Trauma resuscitation through the decades What was hot and now is not 1970s 1980s 1990s 2000s Now 1977 Fluids Summary Dogs subjected to arterial hemorrhage
RESUSCITATION IN TRAUMA Important things I have learnt Trauma resuscitation through the decades What was hot and now is not 1970s 1980s 1990s 2000s Now 1977 Fluids Summary Dogs subjected to arterial hemorrhage
Priorities in Penetrating Chest Trauma
 Priorities in Penetrating Chest Trauma K. Inaba, MD FRCSC FACS Division of Trauma Surgery & Critical Care LAC+USC Medical Center University of Southern California ü None. DISCLOSURES OBJECTIVES ü Practical
Priorities in Penetrating Chest Trauma K. Inaba, MD FRCSC FACS Division of Trauma Surgery & Critical Care LAC+USC Medical Center University of Southern California ü None. DISCLOSURES OBJECTIVES ü Practical
CHEST TRAUMA. Dr Naeem Zia FCPS,FACS,FRCS
 CHEST TRAUMA Dr Naeem Zia FCPS,FACS,FRCS Learning objectives Anatomy of chest wall and thoracic viscera Physiology of respiration and nerve pathways for pain Enumerate different thoracic conditions requiring
CHEST TRAUMA Dr Naeem Zia FCPS,FACS,FRCS Learning objectives Anatomy of chest wall and thoracic viscera Physiology of respiration and nerve pathways for pain Enumerate different thoracic conditions requiring
Background & Indications Probe Selection
 Teresa S. Wu, MD, FACEP Director, EM Ultrasound Program & Fellowship Co-Director, Simulation Based Training Program & Fellowship Associate Program Director, EM Residency Program Maricopa Medical Center
Teresa S. Wu, MD, FACEP Director, EM Ultrasound Program & Fellowship Co-Director, Simulation Based Training Program & Fellowship Associate Program Director, EM Residency Program Maricopa Medical Center
Esophageal Perforation
 Esophageal Perforation Dr. Carmine Simone Thoracic Surgeon, Division of General Surgery Head, Division of Critical Care May 15, 2006 Overview Case presentation Radiology Pre-operative management Operative
Esophageal Perforation Dr. Carmine Simone Thoracic Surgeon, Division of General Surgery Head, Division of Critical Care May 15, 2006 Overview Case presentation Radiology Pre-operative management Operative
Right lung. -fissures:
 -Right lung is shorter and wider because it is compressed by the right copula of the diaphragm by the live.. 2 fissure, 3 lobes.. hilum : 2 bronchi ( ep-arterial, hyp-arterial ), one artery mediastinal
-Right lung is shorter and wider because it is compressed by the right copula of the diaphragm by the live.. 2 fissure, 3 lobes.. hilum : 2 bronchi ( ep-arterial, hyp-arterial ), one artery mediastinal
PEDIATRIC TRAUMA: Implications for Respiratory Care
 PEDIATRIC TRAUMA: Implications for Respiratory Care 17 th Annual Rainbow Respiratory Conference - September 4, 2015 Mike Dingeldein, MD Pediatric Surgeon Pediatric Trauma Medical Director Disclosures none
PEDIATRIC TRAUMA: Implications for Respiratory Care 17 th Annual Rainbow Respiratory Conference - September 4, 2015 Mike Dingeldein, MD Pediatric Surgeon Pediatric Trauma Medical Director Disclosures none
Trauma operating room
 Section 1 Chapter 1 Operating Room General Conduct Trauma operating room Kenji Inaba and Lisa L. Schlitzkus Operating room A large operating room (OR) situated near the emergency department, elevators,
Section 1 Chapter 1 Operating Room General Conduct Trauma operating room Kenji Inaba and Lisa L. Schlitzkus Operating room A large operating room (OR) situated near the emergency department, elevators,
Emergency Approach to the Subclavian and Innominate Vessels
 Emergency Approach to the Subclavian and Innominate Vessels Joseph J. Amato, M.D., Robert M. Vanecko, M.D., See Tao Yao, M.D., and Milton Weinberg, Jr., M.D. T he operative approach to an acutely injured
Emergency Approach to the Subclavian and Innominate Vessels Joseph J. Amato, M.D., Robert M. Vanecko, M.D., See Tao Yao, M.D., and Milton Weinberg, Jr., M.D. T he operative approach to an acutely injured
University of Florida Department of Surgery. CardioThoracic Surgery VA Learning Objectives
 University of Florida Department of Surgery CardioThoracic Surgery VA Learning Objectives This service performs coronary revascularization, valve replacement and lung cancer resections. There are 2 faculty
University of Florida Department of Surgery CardioThoracic Surgery VA Learning Objectives This service performs coronary revascularization, valve replacement and lung cancer resections. There are 2 faculty
Thoracic Trauma The Spectrum
 Thoracic Trauma The Spectrum Joseph Mathew Consultant, s & Emergency dept. 2 Thoracic Trauma Responsible for 20-25% of all deaths attributed to trauma. Contributing cause of death in an additional 25%
Thoracic Trauma The Spectrum Joseph Mathew Consultant, s & Emergency dept. 2 Thoracic Trauma Responsible for 20-25% of all deaths attributed to trauma. Contributing cause of death in an additional 25%
Contributors. First Publication Date: 28 Jul 2007 Publication Date: 18 Jul 2018 Supersedes CPG dated 11 Jun 2012 TABLE OF CONTENTS
 JOINT TRAUMA SYSTEM CLINICAL PRACTICE GUIDELINE (JTS CPG) Emergent Resuscitative Thoracotomy (ERT) (CPG ID: 20) Summarizes recommendations and technique for ERT in a Military Treatment Facility (MTF) in
JOINT TRAUMA SYSTEM CLINICAL PRACTICE GUIDELINE (JTS CPG) Emergent Resuscitative Thoracotomy (ERT) (CPG ID: 20) Summarizes recommendations and technique for ERT in a Military Treatment Facility (MTF) in
LESSON ASSIGNMENT. After completing this lesson, you should be able to:
 LESSON ASSIGNMENT LESSON 3 Cricothyroidotomy LESSON ASSIGNMENT Paragraphs 3-1 through 3-7. LESSON OBJECTIVES After completing this lesson, you should be able to: 3-1. Define cricothyroidotomy. 3-2. Identify
LESSON ASSIGNMENT LESSON 3 Cricothyroidotomy LESSON ASSIGNMENT Paragraphs 3-1 through 3-7. LESSON OBJECTIVES After completing this lesson, you should be able to: 3-1. Define cricothyroidotomy. 3-2. Identify
SEMINOLE COUNTY EMS PROVISIONAL EMT SKILLS VERIFICATION
 The following individual has completed the Seminole County EMS Provisional EMT Skills Verification check in the following areas: Oxygen, Airway and Ventilation Skills ALS Assistance Trauma Management Medical
The following individual has completed the Seminole County EMS Provisional EMT Skills Verification check in the following areas: Oxygen, Airway and Ventilation Skills ALS Assistance Trauma Management Medical
Lesson 4-3: Cardiac Emergencies. CARDIAC EMERGENCIES Angina, AMI, CHF and AED
 Lesson 4-3: Cardiac Emergencies CARDIAC EMERGENCIES Angina, AMI, CHF and AED THREE FAMILIAR CARDIAC CONDITIONS Angina Pectoris Acute Myocardial Infarction Congestive Heart Failure ANGINA PECTORIS Chest
Lesson 4-3: Cardiac Emergencies CARDIAC EMERGENCIES Angina, AMI, CHF and AED THREE FAMILIAR CARDIAC CONDITIONS Angina Pectoris Acute Myocardial Infarction Congestive Heart Failure ANGINA PECTORIS Chest
Hemorrhage Control. Chapter 6
 Chapter 6 The hemorrhage that take[s] place when a main artery is divided is usually so rapid and so copious that the wounded man dies before help can reach him. Colonel H. M. Gray, 1919 Stop the Bleeding!
Chapter 6 The hemorrhage that take[s] place when a main artery is divided is usually so rapid and so copious that the wounded man dies before help can reach him. Colonel H. M. Gray, 1919 Stop the Bleeding!
Traumatic Cardiac Arrest Protocol
 Traumatic Cardiac Arrest Protocol Background: Major Trauma continues to be the leading worldwide cause of death in young adults. Mortality remains high but there are reports of good neurological outcomes
Traumatic Cardiac Arrest Protocol Background: Major Trauma continues to be the leading worldwide cause of death in young adults. Mortality remains high but there are reports of good neurological outcomes
Appropriate Use of Emergency Department Thoracotomy: Implications for the Thoracic Surgeon
 Appropriate Use of Emergency Department Thoracotomy: Implications for the Thoracic Surgeon Nathan M. Mollberg, DO, Cavin Glenn, MD, Jobin John, MD, Stephen R. Wise, MD, Ryan Sullivan, MD, Amir Vafa, MD,
Appropriate Use of Emergency Department Thoracotomy: Implications for the Thoracic Surgeon Nathan M. Mollberg, DO, Cavin Glenn, MD, Jobin John, MD, Stephen R. Wise, MD, Ryan Sullivan, MD, Amir Vafa, MD,
PEDIATRIC PENETRATING TRAUMA. Laura Boomer 11/18/15
 PEDIATRIC PENETRATING TRAUMA Laura Boomer 11/18/15 PENETRATING THORACIC TRAUMA Trauma is the major cause of morbidity and mortality in children Penetrating trauma (in general) accounts for only approximately
PEDIATRIC PENETRATING TRAUMA Laura Boomer 11/18/15 PENETRATING THORACIC TRAUMA Trauma is the major cause of morbidity and mortality in children Penetrating trauma (in general) accounts for only approximately
Large veins of the thorax Brachiocephalic veins
 Large veins of the thorax Brachiocephalic veins Right brachiocephalic vein: formed at the root of the neck by the union of the right subclavian & the right internal jugular veins. Left brachiocephalic
Large veins of the thorax Brachiocephalic veins Right brachiocephalic vein: formed at the root of the neck by the union of the right subclavian & the right internal jugular veins. Left brachiocephalic
EVAR and TEVAR: Extending Their Use for Rupture and Traumatic Injury. Conflict of Interest. Hypotensive shock 5/5/2014. none
 EVAR and TEVAR: Extending Their Use for Rupture and Traumatic Injury Bruce H. Gray, DO MSVM FSCAI Professor of Surgery/Vascular Medicine USC SOM-Greenville Greenville, South Carolina none Conflict of Interest
EVAR and TEVAR: Extending Their Use for Rupture and Traumatic Injury Bruce H. Gray, DO MSVM FSCAI Professor of Surgery/Vascular Medicine USC SOM-Greenville Greenville, South Carolina none Conflict of Interest
Fetal Pig Dissection Day 2 Circulatory and Respiratory Systems
 Name: Date: Period: Fetal Pig Dissection Day 2 Circulatory and Respiratory Systems Dissection Roles (choose a different role from Day 1): Recorder reads directions out loud to group and records answers
Name: Date: Period: Fetal Pig Dissection Day 2 Circulatory and Respiratory Systems Dissection Roles (choose a different role from Day 1): Recorder reads directions out loud to group and records answers
Central Venous Line Insertion
 Central Venous Line Insertion Understand the indications and risks of CVC insertion Understand and troubleshoot the seldinger technique Understand available sites and select the appropriate site for clinical
Central Venous Line Insertion Understand the indications and risks of CVC insertion Understand and troubleshoot the seldinger technique Understand available sites and select the appropriate site for clinical
Maternal Collapse Guideline
 Maternal Collapse Guideline Guideline Number: 664 Supersedes: Classification Clinical Version No: Date of EqIA: Approved by: Date Approved: Date made active: Review Date: 1 Obstetric Written Documentation
Maternal Collapse Guideline Guideline Number: 664 Supersedes: Classification Clinical Version No: Date of EqIA: Approved by: Date Approved: Date made active: Review Date: 1 Obstetric Written Documentation
FIRST AID WRITTEN EXAM. Team Name: 1. Participation in a critical incident stress debriefing (CISD) is mandatory. a. TRUE b. FALSE
 is mandatory. a. TRUE b. FALSE") 2015 NEW IBERIA MINE RESCUE CONTEST FIRST AID WRITTEN EXAM Name: Date: 1. Participation in a critical incident stress debriefing (CISD) is mandatory. 2. The use of accessory muscles in the chest, abdomen
2015 NEW IBERIA MINE RESCUE CONTEST FIRST AID WRITTEN EXAM Name: Date: 1. Participation in a critical incident stress debriefing (CISD) is mandatory. 2. The use of accessory muscles in the chest, abdomen
Point of Care Ultrasound (PoCUS)
") Point of Care Ultrasound (PoCUS) Competency Assessment Forms AORTA Competency A Focussed Assessment of the Aorta (AAA) Guidance Please follow this guidance as closely as possible to ensure consistency
Point of Care Ultrasound (PoCUS) Competency Assessment Forms AORTA Competency A Focussed Assessment of the Aorta (AAA) Guidance Please follow this guidance as closely as possible to ensure consistency
PONGSASIT SINGHATAS, M.D. Department of Surgery Faculty of Medicine, Ramathibodi Hospital Mahidol University
 PONGSASIT SINGHATAS, M.D. Department of Surgery Faculty of Medicine, Ramathibodi Hospital Mahidol University Patient survive Low morbidity GOOD JUDGMENT COMES FROM EXPERIENCE EXPERIENCE COMES FROM BAD
PONGSASIT SINGHATAS, M.D. Department of Surgery Faculty of Medicine, Ramathibodi Hospital Mahidol University Patient survive Low morbidity GOOD JUDGMENT COMES FROM EXPERIENCE EXPERIENCE COMES FROM BAD
THE DESCENDING THORACIC AORTA
 Intercostal Arteries and Veins Each intercostal space contains a large single posterior intercostal artery and two small anterior intercostal arteries. The anterior intercostal arteries of the lower spaces
Intercostal Arteries and Veins Each intercostal space contains a large single posterior intercostal artery and two small anterior intercostal arteries. The anterior intercostal arteries of the lower spaces
Medical NREMT-PTE. NREMT Paramedic Trauma Exam.
 Medical NREMT-PTE NREMT Paramedic Trauma Exam https://killexams.com/pass4sure/exam-detail/nremt-pte Question: 41 Which of the following most accurately describes the finding of jugular venous distension
Medical NREMT-PTE NREMT Paramedic Trauma Exam https://killexams.com/pass4sure/exam-detail/nremt-pte Question: 41 Which of the following most accurately describes the finding of jugular venous distension
Minimal access aortic valve surgery has become one of
 Minimal Access Aortic Valve Surgery Through an Upper Hemisternotomy Approach Prem S. Shekar, MD Minimal access aortic valve surgery has become one of the accepted forms of surgical therapy for patients
Minimal Access Aortic Valve Surgery Through an Upper Hemisternotomy Approach Prem S. Shekar, MD Minimal access aortic valve surgery has become one of the accepted forms of surgical therapy for patients
Northwest Community EMS System September 2017: Head and Chest Trauma Credit Questions
 NWC EMSS Sept 2017 CE: Head & Chest Trauma. Credit Questions - page 1 Northwest Community EMS System September 2017: Head and Chest Trauma Credit Questions Name: EMS Agency EMSC/Educator reviewer: Date
NWC EMSS Sept 2017 CE: Head & Chest Trauma. Credit Questions - page 1 Northwest Community EMS System September 2017: Head and Chest Trauma Credit Questions Name: EMS Agency EMSC/Educator reviewer: Date
Anatomy and Physiology. The airways can be divided in to parts namely: The upper airway. The lower airway.
 Airway management Anatomy and Physiology The airways can be divided in to parts namely: The upper airway. The lower airway. Non-instrumental airway management Head Tilt and Chin Lift Jaw Thrust Advanced
Airway management Anatomy and Physiology The airways can be divided in to parts namely: The upper airway. The lower airway. Non-instrumental airway management Head Tilt and Chin Lift Jaw Thrust Advanced
Chest Trauma.
 Chest Trauma www.fisiokinesiterapia.biz Objectives Anatomy of Thorax Main Causes of Chest Injuries S/S of Chest Injuries Different Types of Chest Injuries Treatments of Chest Injuries Anatomy of the chest
Chest Trauma www.fisiokinesiterapia.biz Objectives Anatomy of Thorax Main Causes of Chest Injuries S/S of Chest Injuries Different Types of Chest Injuries Treatments of Chest Injuries Anatomy of the chest
1 Chapter 40 Advanced Airway Management 2 Advanced Airway Management The advanced airway management techniques discussed in this chapter are to
 1 Chapter 40 Advanced Airway Management 2 Advanced Airway Management The advanced airway management techniques discussed in this chapter are to introduce the EMT-B student to these procedures only. In
1 Chapter 40 Advanced Airway Management 2 Advanced Airway Management The advanced airway management techniques discussed in this chapter are to introduce the EMT-B student to these procedures only. In
Chapter 40 Advanced Airway Management
 1 2 3 4 5 Chapter 40 Advanced Airway Management Advanced Airway Management The advanced airway management techniques discussed in this chapter are to introduce the EMT-B student to these procedures only.
1 2 3 4 5 Chapter 40 Advanced Airway Management Advanced Airway Management The advanced airway management techniques discussed in this chapter are to introduce the EMT-B student to these procedures only.
LESSON ASSIGNMENT. Emergency Surgical Procedures. After completing this lesson, you should be able to:
 LESSON ASSIGNMENT LESSON 3 Emergency Surgical Procedures. LESSON ASSIGNMENT Paragraphs 3-1 through 3-6. LESSON OBJECTIVES After completing this lesson, you should be able to: 3-1. Identify the steps in
LESSON ASSIGNMENT LESSON 3 Emergency Surgical Procedures. LESSON ASSIGNMENT Paragraphs 3-1 through 3-6. LESSON OBJECTIVES After completing this lesson, you should be able to: 3-1. Identify the steps in
ISPUB.COM. Quick Review: GSW to the Chest: The Effect And Impact of High-Velocity Gun Shots. B Phillips CASE REPORT THE OPERATING ROOM
 ISPUB.COM The Internet Journal of Rescue and Disaster Medicine Volume 3 Number 2 Quick Review: GSW to the Chest: The Effect And Impact of High-Velocity Gun Shots B Phillips Citation B Phillips.. The Internet
ISPUB.COM The Internet Journal of Rescue and Disaster Medicine Volume 3 Number 2 Quick Review: GSW to the Chest: The Effect And Impact of High-Velocity Gun Shots B Phillips Citation B Phillips.. The Internet
LIVER INJURIES PROFF. S.FLORET
 LIVER INJURIES PROFF. S.FLORET Abdominal injuries For anatomical consideration: Abdomen can be divided in four areas Intra thoracic abdomen True abdomen Pelvic abdomen Retroperitoneal abdomen ETIOLOGY
LIVER INJURIES PROFF. S.FLORET Abdominal injuries For anatomical consideration: Abdomen can be divided in four areas Intra thoracic abdomen True abdomen Pelvic abdomen Retroperitoneal abdomen ETIOLOGY
Don t let your patients turn blue! Isn t it about time you used etco 2?
 Don t let your patients turn blue! Isn t it about time you used etco 2? American Association of Critical Care Nurses National Teaching Institute Expo Ed 2013 Susan Thibeault MS, CRNA, APRN, CCRN, EMT-P
Don t let your patients turn blue! Isn t it about time you used etco 2? American Association of Critical Care Nurses National Teaching Institute Expo Ed 2013 Susan Thibeault MS, CRNA, APRN, CCRN, EMT-P
10/14/2018 Dr. Shatarat
 2018 Objectives To discuss mediastina and its boundaries To discuss and explain the contents of the superior mediastinum To describe the great veins of the superior mediastinum To describe the Arch of
2018 Objectives To discuss mediastina and its boundaries To discuss and explain the contents of the superior mediastinum To describe the great veins of the superior mediastinum To describe the Arch of
Pneumothorax. Defined as air in the pleural space which can occur through a number of mechanisms
 Pneumothorax Defined as air in the pleural space which can occur through a number of mechanisms Traumatic pneumothorax Penetrating chest trauma Common secondary to bullet or knife penetration Chest tube
Pneumothorax Defined as air in the pleural space which can occur through a number of mechanisms Traumatic pneumothorax Penetrating chest trauma Common secondary to bullet or knife penetration Chest tube
1. The 2010 AHA Guidelines for CPR recommended BLS sequence of steps are:
 BLS Basic Life Support Practice Test Questions 1. The 2010 AHA Guidelines for CPR recommended BLS sequence of steps are: a. Airway, Breathing, Check Pulse b. Chest compressions, Airway, Breathing c. Airway,
BLS Basic Life Support Practice Test Questions 1. The 2010 AHA Guidelines for CPR recommended BLS sequence of steps are: a. Airway, Breathing, Check Pulse b. Chest compressions, Airway, Breathing c. Airway,
Endovascular Trauma Management. Thomas Larzon, MD, PhD Dep of Cardiothoracic and Vascular Surgery Örebro University Hospital, Sweden
 Endovascular Trauma Management Thomas Larzon, MD, PhD Dep of Cardiothoracic and Vascular Surgery Örebro University Hospital, Sweden Medtronic Symposium, LINC 2016 Disclosures I have the following potential
Endovascular Trauma Management Thomas Larzon, MD, PhD Dep of Cardiothoracic and Vascular Surgery Örebro University Hospital, Sweden Medtronic Symposium, LINC 2016 Disclosures I have the following potential
Haemodynamic deterioration in lateral compression pelvic fracture after prehospital pelvic circumferential compression device application
 Haemodynamic deterioration in lateral compression pelvic fracture after prehospital pelvic circumferential compression device application Authors Alan A Garner Retrieval consultant CareFlight Northmead,
Haemodynamic deterioration in lateral compression pelvic fracture after prehospital pelvic circumferential compression device application Authors Alan A Garner Retrieval consultant CareFlight Northmead,
Trauma Life Support Pre-Hospital (TLS-P) Preparatory Materials
 Preparatory Materials") Trauma Life Support Pre-Hospital (TLS-P) Preparatory Materials 1 1. A high-risk bodily fluid for spreading infection is blood. 2. Items that can reduce the spread of infection include masks, gloves, and
Trauma Life Support Pre-Hospital (TLS-P) Preparatory Materials 1 1. A high-risk bodily fluid for spreading infection is blood. 2. Items that can reduce the spread of infection include masks, gloves, and
Traumatic Cardiac Arrest
 HELICOPTER OPERATING PROCEDURE Traumatic Cardiac Arrest HOP No: C/06 Issued: April 2013 Page: 1 of 5 Revision No: 2 TRIM No: 09/300 Document No: D13/5679 Distribution: Sydney X Illawarra X Orange X Helicopter
HELICOPTER OPERATING PROCEDURE Traumatic Cardiac Arrest HOP No: C/06 Issued: April 2013 Page: 1 of 5 Revision No: 2 TRIM No: 09/300 Document No: D13/5679 Distribution: Sydney X Illawarra X Orange X Helicopter
Images have been removed from the PowerPoint slides in this handout due to copyright restrictions.
 Percutaneous Coronary Intervention https://www.youtube.com/watch?v=bssqnhylvma Types of PCI Procedures Balloon Angioplasty Rotational Atherectomy Coronary Stent Balloon Inflation Rotational Atherectomy
Percutaneous Coronary Intervention https://www.youtube.com/watch?v=bssqnhylvma Types of PCI Procedures Balloon Angioplasty Rotational Atherectomy Coronary Stent Balloon Inflation Rotational Atherectomy
Chapter 13. Injuries to the Thorax and Abdomen
 Chapter 13 Injuries to the Thorax and Abdomen Anatomy Review Thoracic cage has 12 pairs of ribs. The first 7 pairs connect directly to sternum. Pairs 8 through 10 connect via common costal cartilage. Pairs
Chapter 13 Injuries to the Thorax and Abdomen Anatomy Review Thoracic cage has 12 pairs of ribs. The first 7 pairs connect directly to sternum. Pairs 8 through 10 connect via common costal cartilage. Pairs
CHANHASSEN FIRE DEPARTMENT MEDICAL / RESCUE SKILLS
 CHANHASSEN FIRE DEPARTMENT MEDICAL / RESCUE SKILLS PRACTICAL STATIONS CHANHASSEN FIRE DEPARTMENT MEDICAL / RESCUE SKILLS 1. CARDIAC ARREST MANAGEMENT 2. AIRWAY & RESPIRATORY MANAGEMENT 3. SPINAL IMMOBILIZATION
CHANHASSEN FIRE DEPARTMENT MEDICAL / RESCUE SKILLS PRACTICAL STATIONS CHANHASSEN FIRE DEPARTMENT MEDICAL / RESCUE SKILLS 1. CARDIAC ARREST MANAGEMENT 2. AIRWAY & RESPIRATORY MANAGEMENT 3. SPINAL IMMOBILIZATION
Damage Control in Abdominal and Pelvic Injuries
 Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
INTERCOSTAL CATHETER (ICC) & UNDERWATER SEAL DRAINAGE (UWSD) Self-Directed Learning Package
 & UNDERWATER SEAL DRAINAGE (UWSD) Self-Directed Learning Package") INTERCOSTAL CATHETER (ICC) & UNDERWATER SEAL DRAINAGE (UWSD) Self-Directed Learning Package Name: Belmore ID: Date: Intercostal Catheters and UWSD Updated 27/11/2010 Page 1 of 22 TABLE OF CONTENTS INTRODUCTION...
INTERCOSTAL CATHETER (ICC) & UNDERWATER SEAL DRAINAGE (UWSD) Self-Directed Learning Package Name: Belmore ID: Date: Intercostal Catheters and UWSD Updated 27/11/2010 Page 1 of 22 TABLE OF CONTENTS INTRODUCTION...
Chapter 28. Objectives. Objectives 01/09/2013. Bleeding and Soft-Tissue Trauma
 Chapter 28 Bleeding and Soft-Tissue Trauma Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define
Chapter 28 Bleeding and Soft-Tissue Trauma Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights reserved. Objectives 1. Define
You Are the Emergency Medical Responder
 Lesson 32: Injuries to the Chest, Abdomen and Genitalia You Are the Emergency Medical Responder Your police unit responds to a call in a part of town plagued by violence. When you arrive, you find the
Lesson 32: Injuries to the Chest, Abdomen and Genitalia You Are the Emergency Medical Responder Your police unit responds to a call in a part of town plagued by violence. When you arrive, you find the
Interventional Radiology in Trauma. Vikash Prasad, MD, FRCPC Vascular and Interventional Radiology The Moncton Hospital
 Interventional Radiology in Trauma Vikash Prasad, MD, FRCPC Vascular and Interventional Radiology The Moncton Hospital Disclosures None relevant to this presentation Shareholder Johnson and Johnson Goal
Interventional Radiology in Trauma Vikash Prasad, MD, FRCPC Vascular and Interventional Radiology The Moncton Hospital Disclosures None relevant to this presentation Shareholder Johnson and Johnson Goal
Life-Saving Treatment by Fluid Resuscitation and a Thoracotomy in a Case of Deep Pulmonary Laceration
 Tokai J Exp Clin Med., Vol. 31, No. 2, pp. 55-59, 2006 Life-Saving Treatment by Fluid Resuscitation and a Thoracotomy in a Case of Deep Pulmonary Laceration Noboru NISHIUMI, Haruka TAKEICHI, Hiroyuki OTSUKA,
Tokai J Exp Clin Med., Vol. 31, No. 2, pp. 55-59, 2006 Life-Saving Treatment by Fluid Resuscitation and a Thoracotomy in a Case of Deep Pulmonary Laceration Noboru NISHIUMI, Haruka TAKEICHI, Hiroyuki OTSUKA,
Endoscopy. Pulmonary Endoscopy
 Pulmonary 1 Direct visualization of TB tree Developed in 1890 s to remove foreign bodies - rigid metal tube Advances added light system, Sx Flexible fiberoptic scopes introduced in early 1960 s 2 Used
Pulmonary 1 Direct visualization of TB tree Developed in 1890 s to remove foreign bodies - rigid metal tube Advances added light system, Sx Flexible fiberoptic scopes introduced in early 1960 s 2 Used
2017 Northern Mine Rescue Contest Written Exam (First Aid Competition)
") 2017 Northern Mine Rescue Contest Written Exam (First Aid Competition) 2017 2010 June 5, 2017 Findley Lake, New York 2017 Northern Mine Rescue Contest Written Exam First Aid Competition Directions: Fill
2017 Northern Mine Rescue Contest Written Exam (First Aid Competition) 2017 2010 June 5, 2017 Findley Lake, New York 2017 Northern Mine Rescue Contest Written Exam First Aid Competition Directions: Fill
Shot Through the Heart (And You re to Blame): Penetrating Cardiac Trauma
: Penetrating Cardiac Trauma") Shot Through the Heart (And You re to Blame): Penetrating Cardiac Trauma Yalaunda M. Thomas, MD, FACS The American College of Osteopathic Emergency Physicians Spring Seminar April 5, 2018 Disclosures I
Shot Through the Heart (And You re to Blame): Penetrating Cardiac Trauma Yalaunda M. Thomas, MD, FACS The American College of Osteopathic Emergency Physicians Spring Seminar April 5, 2018 Disclosures I
May Clinical Director, Peninsula Trauma Network (Edited for PTN)
") Network Policy Traumatic vascular injuries Guidelines Purpose Date May 2015 Version Following the national introduction of Regional Trauma Networks, Major Trauma Networks (MTN s) are required to have a
Network Policy Traumatic vascular injuries Guidelines Purpose Date May 2015 Version Following the national introduction of Regional Trauma Networks, Major Trauma Networks (MTN s) are required to have a
CT of Acute Thoracic Aortic Syndromes Stuart S. Sagel, M.D.
 CT of Acute Thoracic Aortic Syndromes Stuart S. Sagel, M.D. Thoracic Aortic Aneurysms Atherosclerotic Dissection Penetrating ulcer Mycotic Inflammatory (vasculitis) Traumatic Aortic Imaging Options Catheter
CT of Acute Thoracic Aortic Syndromes Stuart S. Sagel, M.D. Thoracic Aortic Aneurysms Atherosclerotic Dissection Penetrating ulcer Mycotic Inflammatory (vasculitis) Traumatic Aortic Imaging Options Catheter
OB HEMORRHAGE: CARTS, KITS AND TRAYS
 OBSTETRIC HEMORRHAGE CARE GUIDELINES AND COMPENDIUM OF BEST PRACTICES REVIEWED BY CADPH-MCAH: 12/1/09 OB HEMORRHAGE: CARTS, KITS AND TRAYS Leslie Casper, MD, San Diego Medical Center, Southern California
OBSTETRIC HEMORRHAGE CARE GUIDELINES AND COMPENDIUM OF BEST PRACTICES REVIEWED BY CADPH-MCAH: 12/1/09 OB HEMORRHAGE: CARTS, KITS AND TRAYS Leslie Casper, MD, San Diego Medical Center, Southern California
EMT. Chapter 14 Review
 EMT Chapter 14 Review Review 1. All of the following are common signs and symptoms of cardiac ischemia, EXCEPT: A. headache. B. chest pressure. C. shortness of breath. D. anxiety or restlessness. Review
EMT Chapter 14 Review Review 1. All of the following are common signs and symptoms of cardiac ischemia, EXCEPT: A. headache. B. chest pressure. C. shortness of breath. D. anxiety or restlessness. Review
EAST MULTICENTER STUDY DATA DICTIONARY. Temporary Intravascular Shunt Study Data Dictionary
 EAST MULTICENTER STUDY DATA DICTIONARY Temporary Intravascular Shunt Study Data Dictionary Data Entry Points and appropriate definitions / clarifications: Entry space Definition / Instructions 1. Specific
EAST MULTICENTER STUDY DATA DICTIONARY Temporary Intravascular Shunt Study Data Dictionary Data Entry Points and appropriate definitions / clarifications: Entry space Definition / Instructions 1. Specific
Peel-Apart Percutaneous Introducer Kits for
 Bard Access Systems Peel-Apart Percutaneous Introducer Kits for Table of Contents Contents Page Bard Implanted Ports Hickman*, Leonard*, Broviac*, Tenckhoff*, and Groshong* Catheters Introduction....................................
Bard Access Systems Peel-Apart Percutaneous Introducer Kits for Table of Contents Contents Page Bard Implanted Ports Hickman*, Leonard*, Broviac*, Tenckhoff*, and Groshong* Catheters Introduction....................................
Penetrating wounds of the heart and great vessels
 Thorax (1973), 28, 142. Penetrating wounds of the heart and great vessels A report of 30 patients C. E. ANAGNOSTOPOULOS and C. FREDERICK KITTLE Department of Surgery, Section of Thoracic and Cardiovascular
Thorax (1973), 28, 142. Penetrating wounds of the heart and great vessels A report of 30 patients C. E. ANAGNOSTOPOULOS and C. FREDERICK KITTLE Department of Surgery, Section of Thoracic and Cardiovascular
Gunshot Wounds to the Abdomen: From Bullet to Incision. Patrick M Reilly MD FACS
 Gunshot Wounds to the Abdomen: From Bullet to Incision Patrick M Reilly MD FACS Master? I Do Get The Chance to Practice What Are We Not Discussing? Stab Wounds Prehospital Care Management of Specific Injuries
Gunshot Wounds to the Abdomen: From Bullet to Incision Patrick M Reilly MD FACS Master? I Do Get The Chance to Practice What Are We Not Discussing? Stab Wounds Prehospital Care Management of Specific Injuries
Adult Intubation Skill Sheet
 Adult Intubation 2. Opens the airway manually and inserts an oral airway *** 3. Ventilates the patient with BVM attached to oxygen at 15 lpm *** 4. Directs assistant to oxygenate the patient 5. Selects
Adult Intubation 2. Opens the airway manually and inserts an oral airway *** 3. Ventilates the patient with BVM attached to oxygen at 15 lpm *** 4. Directs assistant to oxygenate the patient 5. Selects
3. D Objective: Chapter 4, Objective 4 Page: 79 Rationale: A carbon dioxide level below 35 mmhg indicates hyperventilation.
 1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the
1. A Objective: Chapter 1, Objective 3 Page: 14 Rationale: The sudden increase in acceleration produces posterior displacement of the occupants and possible hyperextension of the cervical spine if the