Priorities in Penetrating Chest Trauma
|
|
|
- Cody Thompson
- 5 years ago
- Views:
Transcription


1 Priorities in Penetrating Chest Trauma K. Inaba, MD FRCSC FACS Division of Trauma Surgery & Critical Care LAC+USC Medical Center University of Southern California
2 ü None. DISCLOSURES
3 OBJECTIVES ü Practical approach ü Heart ü Trans-mediastinal wounds ü Autotransfusion ü Tension Pneumothorax
4 OBJECTIVES ü Practical approach ü Heart ü Trans-mediastinal wounds ü Autotransfusion ü Tension Pneumothorax
5 Penetrating Chest Injury Arresting Unstable Stable
6 Penetrating Chest Injury Arresting Unstable Stable
7 Penetrating Chest Injury Arresting Unstable Stable ED Thoracotomy Right Chest Tube
8 2001 ü 25 year review, 4,620 EDT ü Overall Survival 7.4% ü Normal Neurologic Function 92.4%


9 2001 ü 25 year review, 4,620 EDT ü Overall Survival 7.4% ü Normal Neurologic Function 92.4% ü Really Depends on: Mechanism Location


10 Survival By Mechanism 18% 16% 14% Survival 12% 10% 8% 6% 8.8% 4% 2% 0% 1.4%

11 Survival By Mechanism 18% 16% 16.8% 14% Survival 12% 10% 8% 6% 8.8% 4% 2% 0% 1.4% 4.3%

12 Injury Location 12% 10% 10.7% Survival 8% 6% 4% 2% 0% 4.5% 0.7% Thoracic Abdominal Multiple
13 Injury Location 12% 10% 10.7% Isolated Cardiac = 19.4% Survival 8% 6% 4% 2% 0% 4.5% 0.7% Thoracic Abdominal Multiple
14 2015 ü Pro, 187 trauma arrests ü Survivors 3.2%, Donors 1.6% ü FAST prior to EDT ü Ability of cardiac motion/fluid to detect survivors and donors?

15 2015 ü Cardiac Motion/Fluid Sensitivity 100% Specificity 73.7% ü FAST able to identify all survivors, avoid 59% futile EDTs ü Likelihood of survival if both motion/fluid absent is zero
16 EDT INTERVENTIONS ü Release Tamponade ü Repair Cardiac Injury ü Control Hilar Bleeding ü Cross Clamp Aorta ü Restart Heart

17 EDT INTERVENTIONS ü Release Tamponade ü Repair Cardiac Injury ü Control Hilar Bleeding ü Cross Clamp Aorta ü Restart Heart

18 Penetrating Chest Injury Arresting ER Thoracotomy Right Chest Tube Unstable Stable
19 Stable Critical Actions 1. General ü Airway/Oxygenate ü IV/BW/Monitors 2. What is at risk of injury? ü External wounds. ü Plain radiography for missile localization and trajectory mapping.
20 Stable Critical Actions 1. General ü Airway/Oxygenate ü IV/BW/Monitors 2. What is at risk of injury? ü External wounds. ü Plain radiography for missile localization and trajectory mapping.
21 Don t Forget the Back
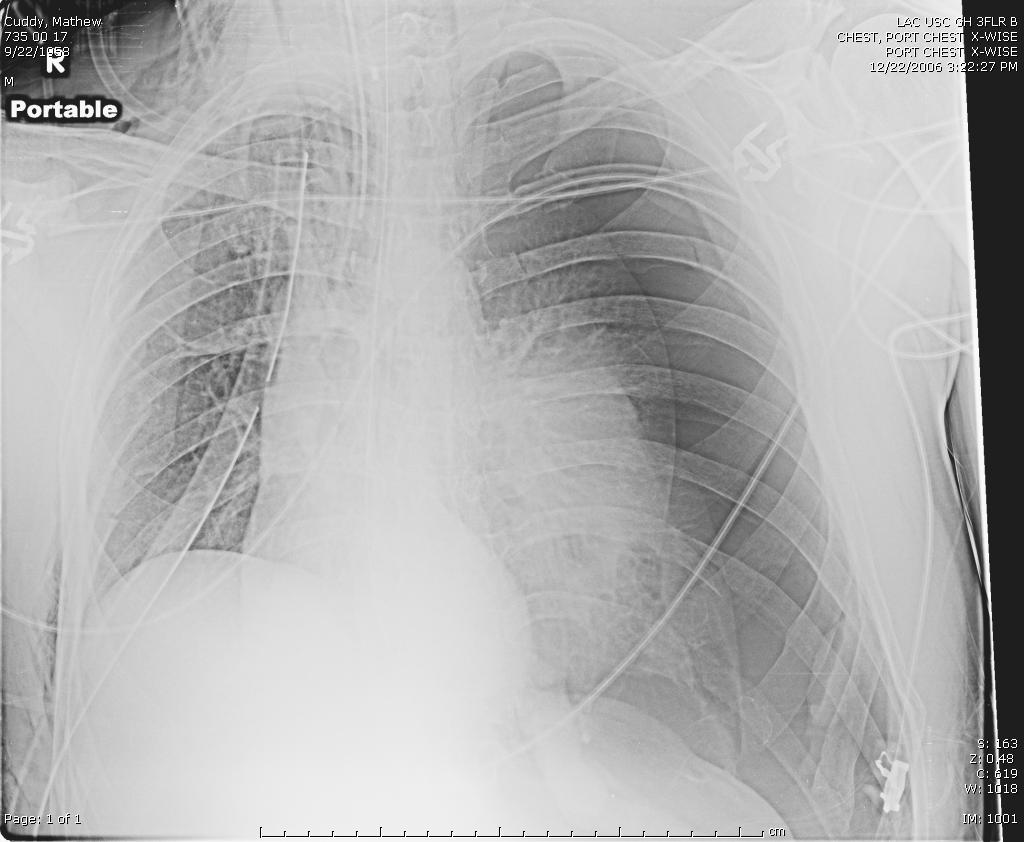
22 For SWs CXR usually sufficient

23 RETAINED FRAGS HEMOTHORAX PNEUMOTHORAX
24 For GSWs also check back
25 For GSWs 1. External holes 2. Internal fragments Everything in between is at risk of injury CT
26 OBJECTIVES ü Practical approach ü Heart ü Trans-mediastinal wounds ü Autotransfusion ü Tension Pneumothorax
27 OBJECTIVES ü Practical approach ü Heart ü Trans-mediastinal wounds ü Autotransfusion ü Tension Pneumothorax
28 Diagnosing Cardiac Injury ü Clinical Exam Restless Shock Tachycardia Beck s triad ü CXR Enlarged heart shadow Pneumopericardium Widened mediastinum ü CVP, ECG ü Pericardiocentesis Unacceptable Sensitivity & Specificity

29 Ultrasound Advantages ü Non-invasive ü Radiation ü Repeatable ü Portable ü Rapid ü Cost effective

30 Heart Video

31 ü Prospective truncal SW or GSW ü No indication for emergent OR ü Non-radiologist performed FAST 1996
32 ü 247 consecutive pts (121 GSW, 126 SW) 100% SENSITIVITY 100% SPECIFICITY ü Pericardium not visualized in one pt Heart Injury No Heart Injury FAST FAST 0 236
33 Summary FN=0 Author Year Journal Design n TN TP FN FP Sensitivity Specificity Rozycki GS 1996 Ann Surg Prospective % 100.0% Rozycki GS 1998 Ann Surg Prospective % 99.3% Rozycki GS 1999 J Trauma Prospective % 97.0% Patel AN 2003 Ann Thorac Surg Retrospective % 99.3% Tayal VS 2004 J Ultrasound Med Prospective % 100.0% TOTAL % 99.0%

34 2009
35 Watch out for ü Large Hemothorax ü Continuous CT output Repeat FAST or do TTE
36 Penetrating Cardiac Injury ü Ultrasound has near perfect sensitivity and specificity ü Positive=sternotomy ü Equivocal=repeat, formal TTE, pericardial window ü Negative=beware the Hemothorax or ongoing CT output
37 Penetrating Cardiac Injury ü Ultrasound has near perfect sensitivity and specificity ü Positive=sternotomy ü Equivocal=repeat, formal TTE, pericardial window ü Negative=beware the Hemothorax or ongoing CT output
38 Penetrating Cardiac Injury ü Ultrasound has near perfect sensitivity and specificity ü Positive=sternotomy ü Equivocal=repeat, formal TTE, pericardial window ü Negative=beware the Hemothorax or ongoing CT output
39 Penetrating Cardiac Injury ü Ultrasound has near perfect sensitivity and specificity ü Positive=sternotomy ü Equivocal=repeat, formal TTE, pericardial window ü Negative=no injury but beware the large Hemothorax or ongoing CT output
40 OBJECTIVES ü Practical approach ü Heart ü Trans-mediastinal wounds ü Autotransfusion ü Tension Pneumothorax
41 Trans-Mediastinal Injury Traditional approach ü Unstable=OR ü Stable=Full Diagnostic Evaluation ü Pan-endoscopy ü Contrast swallow ü Angiography ü Echo
42 Trans-Mediastinal Injury Traditional approach ü Unstable=OR ü Stable=Full Diagnostic Evaluation ü Pan-endoscopy ü Contrast swallow ü Angiography ü Echo TIME CONSUMING AND EXPENSIVE
43 Retrospective, n=22. Stable TM-GSW. CT initial diagnostic test. ü 32% Positive CT, 9% required OR ü 68% Negative CT rate ü 100% NPV

44 Retrospective, n=22. Stable TM-GSW. CT initial diagnostic test. ü 32% Positive CT, 9% required OR ü 68% Negative CT rate ü 100% NPV
45 Trans-Mediastinal GSW? Unstable..OR? Stable..FAST and CTA ü Cardiac FAST ü CT Angiogram
46 Trans-Mediastinal GSW? Unstable..OR? Stable..FAST and CTA ü Cardiac FAST ü CT Angiogram
47 Trans-Mediastinal GSW? Unstable..OR? Stable..FAST and CTA ü Cardiac FAST ü CT Angiogram
48 Trans-Mediastinal GSW? Unstable..OR? Stable..FAST and CTA ü Cardiac FAST Positive=Sternotomy Negative=go to CTA ü CT Angiogram
49 Trans-Mediastinal GSW? Unstable..OR? Stable..FAST and CTA ü Cardiac FAST ü CT Angiogram Trajectory clear=done Injury=OR Equivocal=Bronch/DL, Angio, EGD, Swallow
50 OBJECTIVES ü Practical approach ü Heart ü Trans-mediastinal wounds ü Autotransfusion ü Tension Pneumothorax
51 2012 ü Pro, n=353 acute CT inserted ü 28-32Fr v Fr ü Same blood drainage ü Same duration ü Same complication rate ü Same pneumonia & empyema

52 2012 ü Same RHTx ü Same need for new tube ü Same IR rate ü Same VATS rate ü Same Thoracotomy rate Size did not matter


53 2014 ü RCT, n=40 pneumothorax ü 14Fr pigtail v 28Fr CT ü Pigtail-pain significantly less ü Duration of insertion, success and complications same
54 2012 ü Prospective, n=36 ü 14Fr Pigtail v historic 32-40Fr Chest Tubes ü Ability to drain acute HTx?

55 2012 ü Same initial output ü Same insertion complications ü Same failure rate ü Same tube duration Pigtails effective drains?

56 Chest Autotransfusion ü Cheap. ü Fast. ü Warm. ü Whole blood.
57 Autotransfusion Bacterial contamination? Red cell breakdown products? Inflammatory contents? O2 Delivery Capacity? VS. ü Cheap, fast ü Warm ü Fresh ü Factors ü Virus neutral ü ABO
58 Autotransfusion Bacterial contamination? Red cell breakdown products? Inflammatory contents? O2 Delivery Capacity? VS. Cheap, fast Warm Fresh Factors Virus neutral ABO
59 2015 ü Multicenter, retrospective ü N=272, propensity score ü +/- Autotransfusion with CPD
60 2015 ü ND mortality ü ND complications ü ND 24h INR ü Less RBC required ü Less Platelets required ü Less cost of transfusion
61 2015 ü ND mortality ü ND complications ü ND 24h INR ü Less RBC required ü Less Platelets required ü Less cost of transfusion


62 Autotransfusion ü Citrate phosphate dextrose (CPD) in all collection systems 1mL/7mL blood.
63 DISCHARGING THE STABLE PT
64 DISCHARGING THE STABLE PT ü Stable ü Examinable ü Isolated thoracic injury ü Negative U/S+CXR
65 DISCHARGING THE STABLE PT ü Stable ü Examinable ü Isolated thoracic injury ü Negative U/S+CXR When can we d/c home?
66 ü Prospective ü Penetrating chest injury ü 15 months, n=116 (93SW/23GSW) ü Normal admission CXR and no indication for CT or OR ü Repeat 3 and 6 hrs


67 ü 0.9% developed PTx on 3hr CXR requiring CT insertion ü Follow-up CXR is warranted ü No new findings on 6hr CXR
68 2008 ü Prospective, 36 months ü 100 asymptomatic, normal admission CXR ü 75% SW, 25% GSW

69 2008 ü 2% delayed PTx ü All diagnosed on 3hr CXR ü D/C by 8.8+/-2.6hrs Normal 3hr CXR = D/C home


70 2013 ü 88 prospective sw/gsw chest ü Normal initial CXR ü Repeat ordered 1 & 3hrs ü Done at 1hr 34min: 2.3% PTx ü No new information at 3 hrs Normal 1hr CXR = D/C home
71 Penetrating Chest Injury Arresting Unstable Stable ER Thoracotomy Right Chest Tube Cardiac U/S X-Rays +/- CT +/- L-scope

72 The Unstable Patient
73 Unstable-Critical Actions ü Start crystalloid resuscitation. ü Initiate cross-matching. ü Stabilize ü Arrest ü Remain Unstable
74 Unstable-Critical Actions ü Remain unstable. ü Start uncross-matched or type specific blood. ü Start thawing FFP.
75 Unstable-Critical Actions 1.Localize bleeding. Cardiac U/S Clinically directed chest tube insertion. R/O other areas of blood loss (FAST/DPA). 2. Stop bleeding.
76 Unstable-Critical Actions 1.Localize bleeding. Cardiac U/S Clinically directed chest tube insertion. R/O other areas of blood loss (FAST/DPA). 2. Stop bleeding.
77 Unstable-Critical Actions 1.Localize bleeding. Cardiac U/S - STERNOTOMY Clinically directed chest tube insertion. R/O other areas of blood loss (FAST/DPA). 2. Stop bleeding.
78 Unstable-Critical Actions 1.Localize bleeding. Cardiac U/S Clinically directed chest tube insertion - THORACOTOMY R/O other areas of blood loss (FAST/DPA). 2. Stop bleeding. ü Initial output > 1-1.5L ü Continuous > 2-250cc/hr X 2-4hrs
79 Unstable-Critical Actions 1.Localize bleeding. Cardiac U/S Clinically directed chest tube insertion. R/O other areas of blood loss (FAST/DPA) LAPAROTOMY 2. Stop bleeding.
80 OBJECTIVES ü Practical approach ü Heart ü Trans-mediastinal wounds ü Autotransfusion ü Tension Pneumothorax
81 ü Shortness of Breath ü Chest Pain ü Decreased A/E ü Low O2 Saturation ü Hyper-resonance ü Tactile fremitus
82 ü Shortness of Breath ü Chest Pain ü Decreased A/E ü Low O2 Saturation ü Hyper-resonance ü Tactile fremitus PTX
83 ü Shortness of Breath ü Chest Pain ü Decreased A/E ü Low O2 Saturation ü Hyper-resonance ü Tactile fremitus ü TACHYCARDIA ü HYPOTENSION
84 ü Shortness of Breath ü Chest Pain ü Decreased A/E ü Low O2 Saturation ü Hyper-resonance ü Tactile fremitus ü TACHYCARDIA ü HYPOTENSION TENSION PTX
85 Pleural Air
86 Pleural Air Compresses lung
87 Pleural Air Compresses lung SIMPLE PNEUMOTHORAX
88 Air Increases
89 Air Increases Compresses Lung Even More
90 Air Increases Compresses Lung Even More Shifts Mediastinum
91 Functional Deformation + Impaired Venous Return Decreased CO

92 Functional Deformation + Impaired Venous Return TENSION PNEUMOTHORAX
93 Collapsed Lung
94 Mediastinal Shift

95 ü EXTRINSIC COMPRESSION ü CARDIAC DEFORMATION ü DECREASED VENOUS RETURN
96 NEEDLE DECOMPRESSION

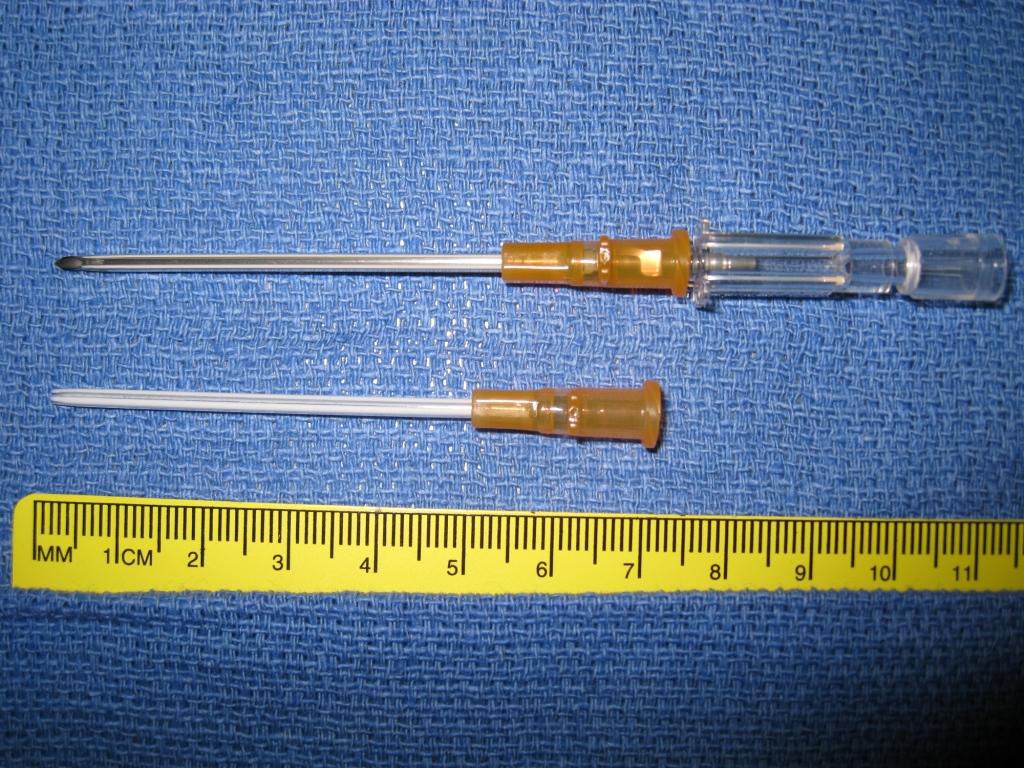
97 NEEDLE DECOMPRESSION ü Emergent procedure for decompression ü ATLS - 2 nd Intercostal space, Mid-clavicular line ü 5 cm catheter
98 Does it work? ü No good data on indications ü No good data on efficacy
99 THE PROBLEM ü Diagnosis is clinical ü Treatment occurs before CXR confirmation ü Never get to know if diagnosis was correct
100 DIFFERENT INSERTION SITE? 5 th Intercostal space, anterior axillary line Potential benefits P Easily accessible supine P Does not impact transport P Experience with CT insertion
101 Studies 1. CADAVERIC MODEL 2. CT BASED HUMAN EVALUATION 3. EMS EVALUATION
102 2011 ü Human cadavers ü Traditional 2 nd v. 5 th ICS ü 5cm standard catheter ü 80 needles into 20 cadavers
103 2011 ü Human cadavers ü Traditional 2 nd v. 5 th ICS ü 5cm standard catheter ü 80 needles into 20 cadavers ü Chest Wall >1cm thicker at 2 nd

104 SUCCESSFUL PENETRATION * * 60% 55%
105 SUCCESSFUL PENETRATION * 70% 15%
106 Cadaver Summary ü Chest thicker at 2 nd v. 5 th ICS ü Especially females ü 42% of 2 nd ICS did not penetrate chest ü 100% at 5 th ICS successful NO cardiac, lung, hilum, aorta, spleen or liver injury
107 2012 ü Evaluate 2 nd v 5 th using Chest CTs of real trauma patients
108 2012 ü Evaluate 2 nd v 5 th using Chest CTs of real trauma patients ü Same findings as cadaver ü Worse as the BMI increases
109 2005 ü 25 EM physicians in Ireland ü 84% ATLS certified ü Do they know where to Needle? ü Can they find it on a live model?

110 2005 ü 88% named 2 nd ICS MCL ü Only 60% able to point out where this was on patient ü 4% pointed out 5 th ICS AAL ü 8% wanted to needle abdomen below & lateral to xiphoid
111 EMS ü 20 Corpsmen, 80 needles ü 25.5+/-3.9 years, 75% male ü 4.4+/-3.3 years experience ü Half previous deployment
112 RESULTS ü Time to insertion SAME ü Ease of finding and inserting needle BETTER ü Accuracy BETTER ü Aggregate distance from correct position BETTER
113 Take Home Points ü Indications for needle decompression not well delineated ü If going to needle, know the following
114 Take Home Points ü Standard Angiocath <5cm ü Chest wall 2 nd ICS >5cm in 40-50% ü Most in upper ¾ of BMIs cannot be decompressed with standard needle
115 Take Home Points ü In controlled experiments, 60% will fail entry ü R and L ü Females > Males ü Worse as BMI increases
116 Take Home Points ü May not be in chest ü If not responding, try again with a different angle ü Especially for females or obese ü May consider alternate positions
117 Arresting Summary ü Resuscitative Thoracotomy. ü Right Sided Chest Tube.
118 Stable Summary ü What areas are at risk? External exam/roll early CXR/Plain Film Survey ü Cardiac U/S ü Negative CXR & U/S & Isolated Chest, Repeat CXR in 1 hour. ü Special Regions Trans-Mediastinal Injuries.
119 Unstable Summary ü Failed volume challenge start blood. ü Localize bleeding. Cardiac U/S. Directed Chest Tube insertion. Check other regions at risk. ü Stop bleeding.
In ESH we usually see blunt chest trauma but penetrating injuries also treated here (usually as single injuries, like stab wound)
") Chest Trauma Dr Csaba Dioszeghy MD PhD FRCEM FFICM FERC East Surrey Hospital Emergency Department Scope Thoracic injuries are common and can be life threatening In ESH we usually see blunt chest trauma
Chest Trauma Dr Csaba Dioszeghy MD PhD FRCEM FFICM FERC East Surrey Hospital Emergency Department Scope Thoracic injuries are common and can be life threatening In ESH we usually see blunt chest trauma
The Management of Chest Trauma. Tom Scaletta, MD FAAEM Immediate Past President, AAEM
 The Management of Chest Trauma Tom Scaletta, MD FAAEM Immediate Past President, AAEM Trichotomizing Rib Fractures Upper 1-3 vascular injuries Middle 4-9 Lower 10-12 12 liver/spleen injuries Management
The Management of Chest Trauma Tom Scaletta, MD FAAEM Immediate Past President, AAEM Trichotomizing Rib Fractures Upper 1-3 vascular injuries Middle 4-9 Lower 10-12 12 liver/spleen injuries Management
The ABC s of Chest Trauma
 The ABC s of Chest Trauma J Bradley Pickhardt MD, FACS Providence St Patrick Hospital What s the Problem? 2/3 of trauma patients have chest trauma Responsible for 25% of all trauma deaths Most injuries
The ABC s of Chest Trauma J Bradley Pickhardt MD, FACS Providence St Patrick Hospital What s the Problem? 2/3 of trauma patients have chest trauma Responsible for 25% of all trauma deaths Most injuries
Trauma. Neck trauma zones. Neck Injuries 1/3/2018. Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure
 Trauma 45 minutes highest points Ahmed Mahmoud, MD Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure Neck trauma zones Airway ;Rapid sequence intubation Breathing ;Needle
Trauma 45 minutes highest points Ahmed Mahmoud, MD Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure Neck trauma zones Airway ;Rapid sequence intubation Breathing ;Needle
Shot Through the Heart (And You re to Blame): Penetrating Cardiac Trauma
: Penetrating Cardiac Trauma") Shot Through the Heart (And You re to Blame): Penetrating Cardiac Trauma Yalaunda M. Thomas, MD, FACS The American College of Osteopathic Emergency Physicians Spring Seminar April 5, 2018 Disclosures I
Shot Through the Heart (And You re to Blame): Penetrating Cardiac Trauma Yalaunda M. Thomas, MD, FACS The American College of Osteopathic Emergency Physicians Spring Seminar April 5, 2018 Disclosures I
(SKILLS/HANDS-ON) Chest Tubes. Rebecca Carman, MSN, ACNP-BC. Amanda Shumway, PA-C. Thomas W. White, MD, FACS, CNSC
 Chest Tubes. Rebecca Carman, MSN, ACNP-BC. Amanda Shumway, PA-C. Thomas W. White, MD, FACS, CNSC") (SKILLS/HANDS-ON) Chest Tubes Rebecca Carman, MSN, ACNP-BC Nurse Practitioner, Trauma Services, Intermountain Medical Center, Intermountain Healthcare Amanda Shumway, PA-C APC Trauma and Critical Care
(SKILLS/HANDS-ON) Chest Tubes Rebecca Carman, MSN, ACNP-BC Nurse Practitioner, Trauma Services, Intermountain Medical Center, Intermountain Healthcare Amanda Shumway, PA-C APC Trauma and Critical Care
Acute Pericardial Tamponade
 Acute Pericardial Tamponade Marx: Rosen's Emergency Medicine: Concepts and Clinical Practice, 5th ed. Epidemiology The reported incidence of acute pericardial tamponade is approximately 2% in patients
Acute Pericardial Tamponade Marx: Rosen's Emergency Medicine: Concepts and Clinical Practice, 5th ed. Epidemiology The reported incidence of acute pericardial tamponade is approximately 2% in patients
Emergency Department Thoracotomy
 Emergency Department Thoracotomy November 3, 2017 North Oaks Shock Trauma Symposium Jeremy R. Timmer, M.D., FACS Objectives Background of RT Indications for RT Contraindications for RT Survival Benefits
Emergency Department Thoracotomy November 3, 2017 North Oaks Shock Trauma Symposium Jeremy R. Timmer, M.D., FACS Objectives Background of RT Indications for RT Contraindications for RT Survival Benefits
Evaluation & Management of Penetrating Wounds to the NECK
 Evaluation & Management of Penetrating Wounds to the NECK Goal Effectively identify patients with a high probability of injury requiring surgical intervention Define the role of diagnostic tests in assessing
Evaluation & Management of Penetrating Wounds to the NECK Goal Effectively identify patients with a high probability of injury requiring surgical intervention Define the role of diagnostic tests in assessing
Algorithms for managing the common trauma patient
 ALGORITHMS Algorithms for managing the common trauma patient J John, MB ChB Department of Urology, Frere Hospital, East London Hospital Complex, East London, South Africa Corresponding author: J John (jeffveenajohn@gmail.com)
ALGORITHMS Algorithms for managing the common trauma patient J John, MB ChB Department of Urology, Frere Hospital, East London Hospital Complex, East London, South Africa Corresponding author: J John (jeffveenajohn@gmail.com)
Damage Control in Abdominal and Pelvic Injuries
 Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
Critical Care Monitoring. Indications. Pleural Space. Chest Drainage. Chest Drainage. Potential space. Contains fluid lubricant
 Critical Care Monitoring Indications 1-2- 2 Pleural Space Potential space Contains fluid lubricant Can fill with air, blood, plasma, serum, lymph, pus 3 1 Pleural Space Problems when contain abnormal substances:
Critical Care Monitoring Indications 1-2- 2 Pleural Space Potential space Contains fluid lubricant Can fill with air, blood, plasma, serum, lymph, pus 3 1 Pleural Space Problems when contain abnormal substances:
CHEST TRAUMA. Dr Naeem Zia FCPS,FACS,FRCS
 CHEST TRAUMA Dr Naeem Zia FCPS,FACS,FRCS Learning objectives Anatomy of chest wall and thoracic viscera Physiology of respiration and nerve pathways for pain Enumerate different thoracic conditions requiring
CHEST TRAUMA Dr Naeem Zia FCPS,FACS,FRCS Learning objectives Anatomy of chest wall and thoracic viscera Physiology of respiration and nerve pathways for pain Enumerate different thoracic conditions requiring
Objectives. The Extended FAST Exam. Focused Assessment e With Sonography In. Trauma (FAST)
") Northern California Emergency Ultrasound Course Objectives The Extended FAST Exam Rimon Bengiamin, MD, RDMS UC SF Discuss the components of the EFAST exam Evaluate the utility of the EFAST Review how to
Northern California Emergency Ultrasound Course Objectives The Extended FAST Exam Rimon Bengiamin, MD, RDMS UC SF Discuss the components of the EFAST exam Evaluate the utility of the EFAST Review how to
The Primary Survey. Clay Cothren Burlew, MD FACS
 The Primary Survey Clay Cothren Burlew, MD FACS Director, Surgical Intensive Care Unit Attending Surgeon, Denver Health Medical Center Associate Professor of Surgery, University of Colorado Outlining the
The Primary Survey Clay Cothren Burlew, MD FACS Director, Surgical Intensive Care Unit Attending Surgeon, Denver Health Medical Center Associate Professor of Surgery, University of Colorado Outlining the
PEDIATRIC TRAUMA: Implications for Respiratory Care
 PEDIATRIC TRAUMA: Implications for Respiratory Care 17 th Annual Rainbow Respiratory Conference - September 4, 2015 Mike Dingeldein, MD Pediatric Surgeon Pediatric Trauma Medical Director Disclosures none
PEDIATRIC TRAUMA: Implications for Respiratory Care 17 th Annual Rainbow Respiratory Conference - September 4, 2015 Mike Dingeldein, MD Pediatric Surgeon Pediatric Trauma Medical Director Disclosures none
Imaging in the Trauma Patient
 Imaging in the Trauma Patient David A. Spain, MD Department of Surgery Stanford University Pan Scan Instead of Clinical Exam? 1 Granted, some patients don t need CT scan Platinum Package Stanford Special
Imaging in the Trauma Patient David A. Spain, MD Department of Surgery Stanford University Pan Scan Instead of Clinical Exam? 1 Granted, some patients don t need CT scan Platinum Package Stanford Special
Cardiac Arrest due to Trauma
 Cardiac Arrest due to Trauma Colonel Michael Reade MBBS MPH DPhil DMedSc DIMCRCSEd AFRACMA FANZCA FCICM ADF Professor of Military Medicine & Surgery University of Queensland & ADF Joint Health Command
Cardiac Arrest due to Trauma Colonel Michael Reade MBBS MPH DPhil DMedSc DIMCRCSEd AFRACMA FANZCA FCICM ADF Professor of Military Medicine & Surgery University of Queensland & ADF Joint Health Command
ED Thoracotomy Left chest opened and extended across sternum with 1000mL blood drained Pericardium opened with 100mL blood drained 1cm laceration in t
 Case Report 39yM stabbed in the left upper chest by wife with kitchen knife. Intubated in the field. Loss of vitals on arrival to hospital while in ambulance. In ED, (-) palpable pulse and (+) organized
Case Report 39yM stabbed in the left upper chest by wife with kitchen knife. Intubated in the field. Loss of vitals on arrival to hospital while in ambulance. In ED, (-) palpable pulse and (+) organized
Emergency Room Resuscitation of the Unstable Trauma Patient
 Emergency Room Resuscitation of the Unstable Trauma Patient Goals of trauma resuscitation Maintain: Systemic oxygenation Systemic perfusion Neurologic function Approach to unstable trauma patient Primary
Emergency Room Resuscitation of the Unstable Trauma Patient Goals of trauma resuscitation Maintain: Systemic oxygenation Systemic perfusion Neurologic function Approach to unstable trauma patient Primary
Guidelines and Protocols
 TITLE: CHEST TRAUMA PURPOSE: Provides a standardized treatment algorithm for patients with chest trauma PROCESS: I. INITIAL ASSESSMENT OF THORACIC TRAUMA A. Penetrating Thoracic Trauma 1. Hemodynamically
TITLE: CHEST TRAUMA PURPOSE: Provides a standardized treatment algorithm for patients with chest trauma PROCESS: I. INITIAL ASSESSMENT OF THORACIC TRAUMA A. Penetrating Thoracic Trauma 1. Hemodynamically
Aggressive Management of Chest Trauma. James Moore Cardiothoracic Anaesthetist & Intensive Care Specialist CCDHB
 Aggressive Management of Chest Trauma James Moore Cardiothoracic Anaesthetist & Intensive Care Specialist CCDHB Outline Why is chest trauma important? Risk Assessment Which patients can go home? Management
Aggressive Management of Chest Trauma James Moore Cardiothoracic Anaesthetist & Intensive Care Specialist CCDHB Outline Why is chest trauma important? Risk Assessment Which patients can go home? Management
The Primary Survey. C. Clay Cothren, MD FACS. Attending Surgeon, Denver Health Medical Center Assistant Professor of Surgery, University of Colorado
 The Primary Survey C. Clay Cothren, MD FACS Attending Surgeon, Denver Health Medical Center Assistant Professor of Surgery, University of Colorado Outlining the ABCs Why do we need such an approach? The
The Primary Survey C. Clay Cothren, MD FACS Attending Surgeon, Denver Health Medical Center Assistant Professor of Surgery, University of Colorado Outlining the ABCs Why do we need such an approach? The
Pre-Hospital and Emergency Department Resuscitative Thoracotomy
 Pre-Hospital and Emergency Department Programme Directors: Mr Jim Connolly Consultant A&E Surgeon Accident and Emergency Department, Royal Victoria Infirmary Dr Paul Wallman Consultant in Emergency Medicine
Pre-Hospital and Emergency Department Programme Directors: Mr Jim Connolly Consultant A&E Surgeon Accident and Emergency Department, Royal Victoria Infirmary Dr Paul Wallman Consultant in Emergency Medicine
Pneumothorax. Defined as air in the pleural space which can occur through a number of mechanisms
 Pneumothorax Defined as air in the pleural space which can occur through a number of mechanisms Traumatic pneumothorax Penetrating chest trauma Common secondary to bullet or knife penetration Chest tube
Pneumothorax Defined as air in the pleural space which can occur through a number of mechanisms Traumatic pneumothorax Penetrating chest trauma Common secondary to bullet or knife penetration Chest tube
Penetrating Cardiac Trauma. Eric Klein, M.D. SUNY Downstate Department of Surgery 6/9/2011
 Penetrating Cardiac Trauma Eric Klein, M.D. SUNY Downstate Department of Surgery 6/9/2011 Case #1 21 y/o male suffered multiple 1cm thoracic stab wounds with an ice pick Left 4th intercostal parasternal
Penetrating Cardiac Trauma Eric Klein, M.D. SUNY Downstate Department of Surgery 6/9/2011 Case #1 21 y/o male suffered multiple 1cm thoracic stab wounds with an ice pick Left 4th intercostal parasternal
PEDIATRIC PENETRATING TRAUMA. Laura Boomer 11/18/15
 PEDIATRIC PENETRATING TRAUMA Laura Boomer 11/18/15 PENETRATING THORACIC TRAUMA Trauma is the major cause of morbidity and mortality in children Penetrating trauma (in general) accounts for only approximately
PEDIATRIC PENETRATING TRAUMA Laura Boomer 11/18/15 PENETRATING THORACIC TRAUMA Trauma is the major cause of morbidity and mortality in children Penetrating trauma (in general) accounts for only approximately
SURGICAL CRITICAL CARE REVIEW TRAUMA K. INABA, MD FACS LAC+USC MEDICAL CENTER
 SURGICAL CRITICAL CARE REVIEW TRAUMA K. INABA, MD FACS LAC+USC MEDICAL CENTER None DISCLOSURES OBJECTIVES CPMT SYNDROME ABDOMEN EXTREMITY OBJECTIVES CPMT SYNDROME ABDOMEN EXTREMITY Abdominal Compartment
SURGICAL CRITICAL CARE REVIEW TRAUMA K. INABA, MD FACS LAC+USC MEDICAL CENTER None DISCLOSURES OBJECTIVES CPMT SYNDROME ABDOMEN EXTREMITY OBJECTIVES CPMT SYNDROME ABDOMEN EXTREMITY Abdominal Compartment
Penetrating Neck Injuries. Jason Levine MD Lutheran Medical Center July 22, 2010
 Penetrating Neck Injuries Jason Levine MD Lutheran Medical Center July 22, 2010 CASE PRESENTATION 19 YO M 3 Stab Wounds Right zone I neck SW 2 SW anterior abdomen Left epigastrium anterior axillary line
Penetrating Neck Injuries Jason Levine MD Lutheran Medical Center July 22, 2010 CASE PRESENTATION 19 YO M 3 Stab Wounds Right zone I neck SW 2 SW anterior abdomen Left epigastrium anterior axillary line
RESUSCITATION IN TRAUMA. Important things I have learnt
 RESUSCITATION IN TRAUMA Important things I have learnt Trauma resuscitation through the decades What was hot and now is not 1970s 1980s 1990s 2000s Now 1977 Fluids Summary Dogs subjected to arterial hemorrhage
RESUSCITATION IN TRAUMA Important things I have learnt Trauma resuscitation through the decades What was hot and now is not 1970s 1980s 1990s 2000s Now 1977 Fluids Summary Dogs subjected to arterial hemorrhage
RCH Trauma Guideline. Management of Traumatic Pneumothorax & Haemothorax. Trauma Service, Division of Surgery
 RCH Trauma Guideline Management of Traumatic Pneumothorax & Haemothorax Trauma Service, Division of Surgery Aim To describe safe and competent management of traumatic pneumothorax and haemothorax at RCH.
RCH Trauma Guideline Management of Traumatic Pneumothorax & Haemothorax Trauma Service, Division of Surgery Aim To describe safe and competent management of traumatic pneumothorax and haemothorax at RCH.
CHEST INJURY PULMONARY CONTUSION
 CHEST INJURY PULMONARY CONTUSION Introduction Pulmonary contusion refers to blunt traumatic lung parenchymal injury which results in oedema and haemorrhaging into alveolar spaces. It may also result in
CHEST INJURY PULMONARY CONTUSION Introduction Pulmonary contusion refers to blunt traumatic lung parenchymal injury which results in oedema and haemorrhaging into alveolar spaces. It may also result in
Gunshot Wounds to the Abdomen: From Bullet to Incision. Patrick M Reilly MD FACS
 Gunshot Wounds to the Abdomen: From Bullet to Incision Patrick M Reilly MD FACS Master? I Do Get The Chance to Practice What Are We Not Discussing? Stab Wounds Prehospital Care Management of Specific Injuries
Gunshot Wounds to the Abdomen: From Bullet to Incision Patrick M Reilly MD FACS Master? I Do Get The Chance to Practice What Are We Not Discussing? Stab Wounds Prehospital Care Management of Specific Injuries
Extended FAST Exam. Goal of Trauma Care. Golden Hour of Trauma
 Extended FAST Exam Goal of Trauma Care Golden Hour of Trauma Best INITIAL screening modality in trauma efast 2014 LLSA Article (ACEP Policy Statement) Level B Recommendation: In hemodynamically unstable
Extended FAST Exam Goal of Trauma Care Golden Hour of Trauma Best INITIAL screening modality in trauma efast 2014 LLSA Article (ACEP Policy Statement) Level B Recommendation: In hemodynamically unstable
Management of Bleeding Pelvic Fractures
 Management of Bleeding Pelvic Fractures Clay Cothren Burlew, MD FACS Professor of Surgery Program Director, SCC and TACS Fellowships Director, Surgical Intensive Care Unit Denver Health Medical Center/University
Management of Bleeding Pelvic Fractures Clay Cothren Burlew, MD FACS Professor of Surgery Program Director, SCC and TACS Fellowships Director, Surgical Intensive Care Unit Denver Health Medical Center/University
Lecture. ALS Algorithm
 Lecture ALS Algorithm 1 Learning outcomes The ALS algorithm Treatment of shockable and non-shockable rhythms Potentially reversible causes of cardiac arrest 2 Adult ALS Algorithm 3 To confirm cardiac arrest
Lecture ALS Algorithm 1 Learning outcomes The ALS algorithm Treatment of shockable and non-shockable rhythms Potentially reversible causes of cardiac arrest 2 Adult ALS Algorithm 3 To confirm cardiac arrest
Imaging of Thoracic Trauma: Tips and Traps. Arun C. Nachiappan, MD Associate Professor of Clinical Radiology University of Pennsylvania
 Imaging of Thoracic Trauma: Tips and Traps Arun C. Nachiappan, MD Associate Professor of Clinical Radiology University of Pennsylvania None Disclosures Objectives Describe blunt and penetrating traumatic
Imaging of Thoracic Trauma: Tips and Traps Arun C. Nachiappan, MD Associate Professor of Clinical Radiology University of Pennsylvania None Disclosures Objectives Describe blunt and penetrating traumatic
Chest X rays and Case Studies. No disclosures. Outline 5/31/2018. Carlo Manalo, M.D. Department of Radiology Loma Linda University Children s Hospital
 Chest X rays and Case Studies Carlo Manalo, M.D. Department of Radiology Loma Linda University Children s Hospital No disclosures. Outline Importance of history Densities delineated on radiography An approach
Chest X rays and Case Studies Carlo Manalo, M.D. Department of Radiology Loma Linda University Children s Hospital No disclosures. Outline Importance of history Densities delineated on radiography An approach
THORACIC TRAUMA: THE ABCs AND BEYOND
 THORACIC TRAUMA: THE ABCs AND BEYOND Walter L. Biffl, M.D. Medical Director, Acute Care Surgery, The Queen s Medical Center Professor and Associate Chair for Research, Department of Surgery, JABSOM/University
THORACIC TRAUMA: THE ABCs AND BEYOND Walter L. Biffl, M.D. Medical Director, Acute Care Surgery, The Queen s Medical Center Professor and Associate Chair for Research, Department of Surgery, JABSOM/University
ASSESSMENT OF DIAGNOSTIC MODALITIES IN PENETRATING CARDIAC TRAUMA FOR THE HAEMODYNAMICALLY STABLE PATIENT
 ASSESSMENT OF DIAGNOSTIC MODALITIES IN PENETRATING CARDIAC TRAUMA FOR THE HAEMODYNAMICALLY STABLE PATIENT DANIEL JOHNATHAN DAVID SURRIDGE A research report submitted to the Faculty of Health Sciences,
ASSESSMENT OF DIAGNOSTIC MODALITIES IN PENETRATING CARDIAC TRAUMA FOR THE HAEMODYNAMICALLY STABLE PATIENT DANIEL JOHNATHAN DAVID SURRIDGE A research report submitted to the Faculty of Health Sciences,
Table 2: Outcomes measured. Table 1: Intrapleural alteplase instillation therapy protocol
 ORIGINAL RESEARCH ARTICLE Intrapleural F brinolytic Therapy with Alteplase in Empyema Thoracis in Children conducted in the Department of Pediatric critical care and Pulmonology unit at our institution
ORIGINAL RESEARCH ARTICLE Intrapleural F brinolytic Therapy with Alteplase in Empyema Thoracis in Children conducted in the Department of Pediatric critical care and Pulmonology unit at our institution
The diagnosis and management of pneumothorax
 Respiratory 131 The diagnosis and management of pneumothorax Pneumothorax is a relatively common presentation in patients under the age of 40 years (approximately, 85% of patients are younger than 40 years).
Respiratory 131 The diagnosis and management of pneumothorax Pneumothorax is a relatively common presentation in patients under the age of 40 years (approximately, 85% of patients are younger than 40 years).
Pan Scan Instead of Clinical Exam? David A. Spain, MD
 Pan Scan Instead of Clinical Exam? David A. Spain, MD Granted, some patients don t t need CT scan Platinum Package Stanford Special CT Scan Head Neck Chest Abdomen Pelvis Takes about 20 minutes to do
Pan Scan Instead of Clinical Exam? David A. Spain, MD Granted, some patients don t t need CT scan Platinum Package Stanford Special CT Scan Head Neck Chest Abdomen Pelvis Takes about 20 minutes to do
Improving Rural Trauma Outcomes: Local Damage Control? R Simons, V Vogt Haines, K McCarroll. Enhanced Surgical Skills Program Banff, January 2018
 Improving Rural Trauma Outcomes: Local Damage Control? R Simons, V Vogt Haines, K McCarroll Enhanced Surgical Skills Program Banff, January 2018 Session Objectives Define problem of high injury mortality
Improving Rural Trauma Outcomes: Local Damage Control? R Simons, V Vogt Haines, K McCarroll Enhanced Surgical Skills Program Banff, January 2018 Session Objectives Define problem of high injury mortality
Chapter 16. Thoracic Injuries
 Thoracic Injuries Chapter 16 Thoracic Injuries Introduction About 15% of war injuries involve the chest. Of those, 10% are superficial (soft tissue only) requiring only basic wound treatment. The remaining
Thoracic Injuries Chapter 16 Thoracic Injuries Introduction About 15% of war injuries involve the chest. Of those, 10% are superficial (soft tissue only) requiring only basic wound treatment. The remaining
Case Presentation Surgery Grand Round. Amid Keshavarzi, MD UCHSC 4/9/2006
 Case Presentation Surgery Grand Round Amid Keshavarzi, MD UCHSC 4/9/2006 Case Presentation 12 y/o female Presented to OSH after accidental swallowing of plastic fork in the bus, CXR/AXR form OSH did not
Case Presentation Surgery Grand Round Amid Keshavarzi, MD UCHSC 4/9/2006 Case Presentation 12 y/o female Presented to OSH after accidental swallowing of plastic fork in the bus, CXR/AXR form OSH did not
ISPUB.COM. Quick Review: GSW to the Chest: The Effect And Impact of High-Velocity Gun Shots. B Phillips CASE REPORT THE OPERATING ROOM
 ISPUB.COM The Internet Journal of Rescue and Disaster Medicine Volume 3 Number 2 Quick Review: GSW to the Chest: The Effect And Impact of High-Velocity Gun Shots B Phillips Citation B Phillips.. The Internet
ISPUB.COM The Internet Journal of Rescue and Disaster Medicine Volume 3 Number 2 Quick Review: GSW to the Chest: The Effect And Impact of High-Velocity Gun Shots B Phillips Citation B Phillips.. The Internet
Point of Care Ultrasound (PoCUS)
") Point of Care Ultrasound (PoCUS) Competency Assessment Forms AORTA Competency A Focussed Assessment of the Aorta (AAA) Guidance Please follow this guidance as closely as possible to ensure consistency
Point of Care Ultrasound (PoCUS) Competency Assessment Forms AORTA Competency A Focussed Assessment of the Aorta (AAA) Guidance Please follow this guidance as closely as possible to ensure consistency
Ultrasound in the ICU
 Ultrasound in the ICU Kristine E. W. Breyer, MD Assistant Professor Anesthesia & Critical Care Medicine UCSF DISCLOSURES: NONE Definition The Ultrasound Exam Types & Uses Training Clinical Examples Objectives
Ultrasound in the ICU Kristine E. W. Breyer, MD Assistant Professor Anesthesia & Critical Care Medicine UCSF DISCLOSURES: NONE Definition The Ultrasound Exam Types & Uses Training Clinical Examples Objectives
Lecture 2: Clinical anatomy of thoracic cage and cavity II
 Lecture 2: Clinical anatomy of thoracic cage and cavity II Dr. Rehan Asad At the end of this session, the student should be able to: Identify and discuss clinical anatomy of mediastinum such as its deflection,
Lecture 2: Clinical anatomy of thoracic cage and cavity II Dr. Rehan Asad At the end of this session, the student should be able to: Identify and discuss clinical anatomy of mediastinum such as its deflection,
Thoracic Trauma The Spectrum
 Thoracic Trauma The Spectrum Joseph Mathew Consultant, s & Emergency dept. 2 Thoracic Trauma Responsible for 20-25% of all deaths attributed to trauma. Contributing cause of death in an additional 25%
Thoracic Trauma The Spectrum Joseph Mathew Consultant, s & Emergency dept. 2 Thoracic Trauma Responsible for 20-25% of all deaths attributed to trauma. Contributing cause of death in an additional 25%
Chest Tube Thoracostomy
 Chest Tube Thoracostomy INTRODUCTION A chest tube thoracostomy is commonly done in the ED to evacuate an abnormal accumulation of fluid (blood, empyema) or air from the pleural space under an elective,
Chest Tube Thoracostomy INTRODUCTION A chest tube thoracostomy is commonly done in the ED to evacuate an abnormal accumulation of fluid (blood, empyema) or air from the pleural space under an elective,
TEVAR for trauma is here to stay: Advances in the Treatment of Blunt Thoracic Aortic Injury
 TEVAR for trauma is here to stay: Advances in the Treatment of Blunt Thoracic Aortic Injury Megan Brenner MD MS RPVI FACS Associate Professor of Surgery Division of Trauma/Surgical Critical Care, RA Cowley
TEVAR for trauma is here to stay: Advances in the Treatment of Blunt Thoracic Aortic Injury Megan Brenner MD MS RPVI FACS Associate Professor of Surgery Division of Trauma/Surgical Critical Care, RA Cowley
PEMSS PROTOCOLS INVASIVE PROCEDURES
 PEMSS PROTOCOLS INVASIVE PROCEDURES Panhandle Emergency Medical Services System SURGICAL AND NEEDLE CRICOTHYROTOMY Inability to intubate is the primary indication for creating an artificial airway. Care
PEMSS PROTOCOLS INVASIVE PROCEDURES Panhandle Emergency Medical Services System SURGICAL AND NEEDLE CRICOTHYROTOMY Inability to intubate is the primary indication for creating an artificial airway. Care
TACO CASE STUDIES RTC JUNE Kerry Dowling Blood Transfusion Laboratory Manager Jonathan Ricks Blood Transfusion Nurse Practitioner
 TACO CASE STUDIES RTC JUNE 2017 Kerry Dowling Blood Transfusion Laboratory Manager Jonathan Ricks Blood Transfusion Nurse Practitioner RISK FACTORS - TACO Age over 70 years although also seen in younger
TACO CASE STUDIES RTC JUNE 2017 Kerry Dowling Blood Transfusion Laboratory Manager Jonathan Ricks Blood Transfusion Nurse Practitioner RISK FACTORS - TACO Age over 70 years although also seen in younger
Shock and Resuscitation: Part II. Patrick M Reilly MD FACS Professor of Surgery
 Shock and Resuscitation: Part II Patrick M Reilly MD FACS Professor of Surgery Trauma Patient 1823 / 18 Police Dropoff Torso GSW Lower Midline / Right Buttock Shock This Monday Trauma Patient 1823 / 18
Shock and Resuscitation: Part II Patrick M Reilly MD FACS Professor of Surgery Trauma Patient 1823 / 18 Police Dropoff Torso GSW Lower Midline / Right Buttock Shock This Monday Trauma Patient 1823 / 18
Emergency Department Thoracotomy. Khalid Al Johani. MD EM & Trauma consultant
 Emergency Department Thoracotomy Khalid Al Johani. MD EM & Trauma consultant Background Thoracic trauma is one of the leading causes of death worldwide in all age groups and accounts for 25-50% of all
Emergency Department Thoracotomy Khalid Al Johani. MD EM & Trauma consultant Background Thoracic trauma is one of the leading causes of death worldwide in all age groups and accounts for 25-50% of all
Damage Control Resuscitation. VGH Trauma Rounds 2018 Harvey Hawes
 Damage Control Resuscitation VGH Trauma Rounds 2018 Harvey Hawes Example Case 25yo F in motor vehicle collision at high speed Picked up at scene by Helicopter EMS unit Initial vital signs: HR 134 BP 88/42
Damage Control Resuscitation VGH Trauma Rounds 2018 Harvey Hawes Example Case 25yo F in motor vehicle collision at high speed Picked up at scene by Helicopter EMS unit Initial vital signs: HR 134 BP 88/42
Ultrasound. FAST Focused Assessment with Sonography in Trauma
 Ultrasound FAST Focused Assessment with Sonography in Trauma Rohit Patel, MD University of Florida Health Director, Critical Care Ultrasound Surgical ICU Center for Intensive Care Gainesville, Florida
Ultrasound FAST Focused Assessment with Sonography in Trauma Rohit Patel, MD University of Florida Health Director, Critical Care Ultrasound Surgical ICU Center for Intensive Care Gainesville, Florida
Session Number 219 A BLUNT REVIEW OF THE PENETRATING ISSUES IN CHEST TRAUMA
 Session Number 219 A BLUNT REVIEW OF THE PENETRATING ISSUES IN CHEST TRAUMA Lisa C. Laphan-Morad, MSN, APN-C Administrative Director of Surgical & Ambulatory Services Nurse Practitioner Virtua Health Marlton,
Session Number 219 A BLUNT REVIEW OF THE PENETRATING ISSUES IN CHEST TRAUMA Lisa C. Laphan-Morad, MSN, APN-C Administrative Director of Surgical & Ambulatory Services Nurse Practitioner Virtua Health Marlton,
Putting it all together: 1. The arrested patient 2. The shocked patient 3. The breathless patient
 Putting it all together: 1. The arrested patient 2. The shocked patient 3. The breathless patient 1 The Arrested Patient Adapted from Lichtenstein's SESAME protocol, with permission 2 Summary 1. (Ongoing
Putting it all together: 1. The arrested patient 2. The shocked patient 3. The breathless patient 1 The Arrested Patient Adapted from Lichtenstein's SESAME protocol, with permission 2 Summary 1. (Ongoing
The FAST Exam! Dr. David Easton MD FRCPC Critical Care and Emergency Medicine University of Manitoba Canada
 The FAST Exam! Dr. David Easton MD FRCPC Critical Care and Emergency Medicine University of Manitoba Canada Dr. David Easton MD FRCPC Assistant Professor Section of Critical Care and Emergency Medicine
The FAST Exam! Dr. David Easton MD FRCPC Critical Care and Emergency Medicine University of Manitoba Canada Dr. David Easton MD FRCPC Assistant Professor Section of Critical Care and Emergency Medicine
A Repeat Case of Idiopathic Spontaneous Hemothorax
 Case Report A Repeat Case of Idiopathic Spontaneous Hemothorax Felix R. Gaw, MD Jack H. Bloch, MD, PhD, FACS Nolan J. Anderson, MD, FACS Spontaneous hemothorax, a collection of blood in the pleural cavity
Case Report A Repeat Case of Idiopathic Spontaneous Hemothorax Felix R. Gaw, MD Jack H. Bloch, MD, PhD, FACS Nolan J. Anderson, MD, FACS Spontaneous hemothorax, a collection of blood in the pleural cavity
CT of Acute Thoracic Aortic Syndromes Stuart S. Sagel, M.D.
 CT of Acute Thoracic Aortic Syndromes Stuart S. Sagel, M.D. Thoracic Aortic Aneurysms Atherosclerotic Dissection Penetrating ulcer Mycotic Inflammatory (vasculitis) Traumatic Aortic Imaging Options Catheter
CT of Acute Thoracic Aortic Syndromes Stuart S. Sagel, M.D. Thoracic Aortic Aneurysms Atherosclerotic Dissection Penetrating ulcer Mycotic Inflammatory (vasculitis) Traumatic Aortic Imaging Options Catheter
STORMY DENGUE with bloody problems. Anand M.Patil PICU MED/SURG TEAM Apollo Childrens Hospitals Chennai
 STORMY DENGUE with bloody problems Anand M.Patil PICU MED/SURG TEAM Apollo Childrens Hospitals Chennai 1 HISTORY 4 ½ years girl Day 1: Fever, Lethargy, Low urine output Hypotension, high PCV,low platelets
STORMY DENGUE with bloody problems Anand M.Patil PICU MED/SURG TEAM Apollo Childrens Hospitals Chennai 1 HISTORY 4 ½ years girl Day 1: Fever, Lethargy, Low urine output Hypotension, high PCV,low platelets
Management of Pelvic Fracture
 Management of Pelvis Fracture with Hemodynamic Instability James W. Davis MD Professor of Clinical Surgery, UCSF/Fresno Chief of Trauma Management of Pelvic Fracture How NOT to do it The basics Evaluation
Management of Pelvis Fracture with Hemodynamic Instability James W. Davis MD Professor of Clinical Surgery, UCSF/Fresno Chief of Trauma Management of Pelvic Fracture How NOT to do it The basics Evaluation
Thoracic Injuries. Chapter 16
 Thoracic Injuries Chapter 16 Thoracic Injuries Introduction About 15% of war injuries involve the torso. Those injuries involving the vasculature of the mediastinum (heart, great vessels, and pulmonary
Thoracic Injuries Chapter 16 Thoracic Injuries Introduction About 15% of war injuries involve the torso. Those injuries involving the vasculature of the mediastinum (heart, great vessels, and pulmonary
Cardiac tamponade and Pericardiocentesis Made Easy
 Cardiac tamponade and Pericardiocentesis Made Easy www.cardiconcept.com Etiology of pericardial diseases. Non Infectious cause Infectious cause European Heart Journal (2015) 36, 2921 2964 Recommendations
Cardiac tamponade and Pericardiocentesis Made Easy www.cardiconcept.com Etiology of pericardial diseases. Non Infectious cause Infectious cause European Heart Journal (2015) 36, 2921 2964 Recommendations
Management of the Trauma Patient. Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015
 Management of the Trauma Patient Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015 Saturday Night 25 yo M s/p high speed MVC Hypotensive in the ED, altered
Management of the Trauma Patient Elizabeth R Benjamin MD PhD Trauma and Surgical Critical Care Critical Care Symposium April 20, 2015 Saturday Night 25 yo M s/p high speed MVC Hypotensive in the ED, altered
Purpose This Operating Procedure provides guidance on the management of blunt thoracic traumatic injury
 Blunt Thoracic Trauma HELI.CLI.09 Purpose This Operating Procedure provides guidance on the management of blunt thoracic traumatic injury Procedure Management of Blunt Thoracic Traumatic Injury For Review
Blunt Thoracic Trauma HELI.CLI.09 Purpose This Operating Procedure provides guidance on the management of blunt thoracic traumatic injury Procedure Management of Blunt Thoracic Traumatic Injury For Review
Thoracic trauma, both in isolation and as part of the. Does size matter? A prospective analysis of versus French chest tube size in trauma
 ORIGINAL ARTICLE Does size matter? A prospective analysis of 28 32 versus 36 40 French chest tube size in trauma Kenji Inaba, MD, Thomas Lustenberger, MD, Gustavo Recinos, MD, Crysanthos Georgiou, MD,
ORIGINAL ARTICLE Does size matter? A prospective analysis of 28 32 versus 36 40 French chest tube size in trauma Kenji Inaba, MD, Thomas Lustenberger, MD, Gustavo Recinos, MD, Crysanthos Georgiou, MD,
CHEST INJURIES. Jacek Piątkowski M.D., Ph. D.
 CHEST INJURIES Jacek Piątkowski M.D., Ph. D. CHEST INJURIES 3-4% of all injuries 8% of patients hospitalized due to injuries 65% of patients who died at the accident place CLASSIFICATION OF THE CHEST INJURIES
CHEST INJURIES Jacek Piątkowski M.D., Ph. D. CHEST INJURIES 3-4% of all injuries 8% of patients hospitalized due to injuries 65% of patients who died at the accident place CLASSIFICATION OF THE CHEST INJURIES
Pulmonary Embolism. Pulmonary Embolism. Pulmonary Embolism. PE - Clinical
 Pulmonary embolus - a practical approach to investigation and treatment Sam Janes Wellcome Senior Fellow and Respiratory Physician, University College London Background Diagnosis Treatment Common: 50 cases
Pulmonary embolus - a practical approach to investigation and treatment Sam Janes Wellcome Senior Fellow and Respiratory Physician, University College London Background Diagnosis Treatment Common: 50 cases
Alexander A Schult, M.D., FCCP. October 21, 2017 Revised 1/10/18
 Alexander A Schult, M.D., FCCP October 21, 2017 Revised 1/10/18 Identifying normal anatomy Identifying various pathologic states Identifying placement of hardware Identifying limitations of portable CXR
Alexander A Schult, M.D., FCCP October 21, 2017 Revised 1/10/18 Identifying normal anatomy Identifying various pathologic states Identifying placement of hardware Identifying limitations of portable CXR
INJURIES CHEST, ABDOMEN, LIMBS. FN Brno November 2011
 INJURIES CHEST, ABDOMEN, LIMBS FN Brno November 2011 Injury Chest Abdomen Limbs Injury to the rib cage Fractured one or more ribs Sharp pain at the site of fracture Pain on taking a deep breath Shallow
INJURIES CHEST, ABDOMEN, LIMBS FN Brno November 2011 Injury Chest Abdomen Limbs Injury to the rib cage Fractured one or more ribs Sharp pain at the site of fracture Pain on taking a deep breath Shallow
Pediatric Trauma Practice. Guideline for Management of the Child in Shock. Background
 Pediatric Trauma Practice Guideline for Management of the Child in Shock Background Guideline for Management Trauma is the leading cause of death in children and adolescents in the United States. Although
Pediatric Trauma Practice Guideline for Management of the Child in Shock Background Guideline for Management Trauma is the leading cause of death in children and adolescents in the United States. Although
Chest Trauma.
 Chest Trauma www.fisiokinesiterapia.biz Objectives Anatomy of Thorax Main Causes of Chest Injuries S/S of Chest Injuries Different Types of Chest Injuries Treatments of Chest Injuries Anatomy of the chest
Chest Trauma www.fisiokinesiterapia.biz Objectives Anatomy of Thorax Main Causes of Chest Injuries S/S of Chest Injuries Different Types of Chest Injuries Treatments of Chest Injuries Anatomy of the chest
Northwest Community EMS System September 2017: Head and Chest Trauma Credit Questions
 NWC EMSS Sept 2017 CE: Head & Chest Trauma. Credit Questions - page 1 Northwest Community EMS System September 2017: Head and Chest Trauma Credit Questions Name: EMS Agency EMSC/Educator reviewer: Date
NWC EMSS Sept 2017 CE: Head & Chest Trauma. Credit Questions - page 1 Northwest Community EMS System September 2017: Head and Chest Trauma Credit Questions Name: EMS Agency EMSC/Educator reviewer: Date
Penetrating Cardiac Injury
 Penetrating Cardiac Injury Getting to the Heart of the Matter Marilyn Ng, MD Dept. of Surgery Conference Downstate Medical Center Aug 11, 2011 Case Presentation 28 yo M with unknown PMHx Level 1 notification
Penetrating Cardiac Injury Getting to the Heart of the Matter Marilyn Ng, MD Dept. of Surgery Conference Downstate Medical Center Aug 11, 2011 Case Presentation 28 yo M with unknown PMHx Level 1 notification
PRE-HOSPITAL EMERGENCY CARE COURSE.
 PRE-HOSPITAL EMERGENCY CARE COURSE www.basics.org.uk Chest Assessment & Management BASICS Education March 2016 Objectives To understand the importance of oxygenation and ventilation To be able to describe
PRE-HOSPITAL EMERGENCY CARE COURSE www.basics.org.uk Chest Assessment & Management BASICS Education March 2016 Objectives To understand the importance of oxygenation and ventilation To be able to describe
MEDIASTINAL STAGING surgical pro
 MEDIASTINAL STAGING surgical pro Paul E. Van Schil, MD, PhD Department of Thoracic and Vascular Surgery University of Antwerp, Belgium Mediastinal staging Invasive techniques lymph node mapping cervical
MEDIASTINAL STAGING surgical pro Paul E. Van Schil, MD, PhD Department of Thoracic and Vascular Surgery University of Antwerp, Belgium Mediastinal staging Invasive techniques lymph node mapping cervical
10/4/2018. Nothing to Disclose. Liz Robertson, MD FACS October 5, 2018 Steven R. Hall Trauma Symposium Big Cedar Lodge, MO
 Nothing to Disclose Liz Robertson, MD FACS October 5, 2018 Steven R. Hall Trauma Symposium Big Cedar Lodge, MO History of IV Resuscitation Review of Data for Fluid Strategies Historical Examples of IV
Nothing to Disclose Liz Robertson, MD FACS October 5, 2018 Steven R. Hall Trauma Symposium Big Cedar Lodge, MO History of IV Resuscitation Review of Data for Fluid Strategies Historical Examples of IV
Disclosures: Image Guided Procedures Pearls, Pitfalls, and Disasters. Central Venous Access. Outline:
 Image Guided Procedures Pearls, Pitfalls, and Disasters Disclosures: I have nothing to disclose Miles B. Conrad MD, MPH Clinical Assoc. Prof of Radiology Section: IR Outline: Image Guided Procedures Pearls,
Image Guided Procedures Pearls, Pitfalls, and Disasters Disclosures: I have nothing to disclose Miles B. Conrad MD, MPH Clinical Assoc. Prof of Radiology Section: IR Outline: Image Guided Procedures Pearls,
We are now going to review the diagnosis and management of pericardial collections and tamponade
 We are now going to review the diagnosis and management of pericardial collections and tamponade FEEL COURSE PAGE 1 Paying particular attention to the difference between a collection and cardiac tamponade
We are now going to review the diagnosis and management of pericardial collections and tamponade FEEL COURSE PAGE 1 Paying particular attention to the difference between a collection and cardiac tamponade
Trauma Workshop! Skills Centre, St George Hospital! Saturday 15 March 2014!
 Trauma Workshop Skills Centre, St George Hospital Saturday 15 March 2014 VMO facilitators: Dr Ricardo Hamilton (Campbelltown Hospital) Dr Mary Langcake (St George Hospital) Dr Anthony Chambers (St George
Trauma Workshop Skills Centre, St George Hospital Saturday 15 March 2014 VMO facilitators: Dr Ricardo Hamilton (Campbelltown Hospital) Dr Mary Langcake (St George Hospital) Dr Anthony Chambers (St George
Low Risk Chest Pain. Objectives. Disclosure. Case 1. Jeffrey Tabas, MD Professor of Emergency Medicine Office of CME UCSF School of Medicine
 Disclosure Low Risk Chest Pain No Financial Relationships to Disclose No significant investments or savings Unlimited Expenses Jeffrey Tabas, MD Professor of Emergency Medicine Office of CME UCSF School
Disclosure Low Risk Chest Pain No Financial Relationships to Disclose No significant investments or savings Unlimited Expenses Jeffrey Tabas, MD Professor of Emergency Medicine Office of CME UCSF School
account for 10% to 15% of all traffic fatalities majority fatal at the scene 50% who survive the initial injury die in the first 24 hours 90% die
 account for 10% to 15% of all traffic fatalities majority fatal at the scene 50% who survive the initial injury die in the first 24 hours 90% die within the first month if aorta not repaired 30-90% overall
account for 10% to 15% of all traffic fatalities majority fatal at the scene 50% who survive the initial injury die in the first 24 hours 90% die within the first month if aorta not repaired 30-90% overall
Adam J. Hansen, MD UHC Thoracic Surgery
 Adam J. Hansen, MD UHC Thoracic Surgery Sometimes seen on Chest X-ray (CXR) Common incidental findings on computed tomography (CT) chest and abdomen done for other reasons Most lung cancers discovered
Adam J. Hansen, MD UHC Thoracic Surgery Sometimes seen on Chest X-ray (CXR) Common incidental findings on computed tomography (CT) chest and abdomen done for other reasons Most lung cancers discovered
ACUTE CLINICAL MANAGEMENT OF TRAUMA Tina Gaarder, MD, PhD
 ACUTE CLINICAL MANAGEMENT OF TRAUMA Tina Gaarder, MD, PhD Trauma represents a leading cause of disability and preventable death and is mainly affecting people between 15 and 40 years of age, accounting
ACUTE CLINICAL MANAGEMENT OF TRAUMA Tina Gaarder, MD, PhD Trauma represents a leading cause of disability and preventable death and is mainly affecting people between 15 and 40 years of age, accounting
Transfusion Requirements and Management in Trauma RACHEL JACK
 Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
Management of the Open Abdomen
 Management of the Open Abdomen Clay Cothren Burlew, MD FACS Director, Surgical Intensive Care Unit Associate Professor of Surgery Denver Health Medical Center / University of Colorado The Open Abdomen
Management of the Open Abdomen Clay Cothren Burlew, MD FACS Director, Surgical Intensive Care Unit Associate Professor of Surgery Denver Health Medical Center / University of Colorado The Open Abdomen
Aurora Health Care EMS Continuing Education Spring 2011 Packet THORACIC TRAUMA THE PREHOSPITAL APPROACH TO CHEST INJURY MANAGEMENT
 Aurora Health Care EMS Continuing Education Spring 2011 Packet THORACIC TRAUMA Chest injuries are significant contributors to death from major trauma and can be difficult to assess adequately in the pre-hospital
Aurora Health Care EMS Continuing Education Spring 2011 Packet THORACIC TRAUMA Chest injuries are significant contributors to death from major trauma and can be difficult to assess adequately in the pre-hospital
EAST MULTICENTER STUDY DATA DICTIONARY. Temporary Intravascular Shunt Study Data Dictionary
 EAST MULTICENTER STUDY DATA DICTIONARY Temporary Intravascular Shunt Study Data Dictionary Data Entry Points and appropriate definitions / clarifications: Entry space Definition / Instructions 1. Specific
EAST MULTICENTER STUDY DATA DICTIONARY Temporary Intravascular Shunt Study Data Dictionary Data Entry Points and appropriate definitions / clarifications: Entry space Definition / Instructions 1. Specific
Iatrogenic Cardiac Injuries. Kings County Hospital Center Verena Liu, MD 9/1/2011
 Iatrogenic Cardiac Injuries Kings County Hospital Center Verena Liu, MD 9/1/2011 Case Presentation 69 year old male recently diagnosed with a 3.8 cm x 4.3 cm hepatocellular CA in the superior segment of
Iatrogenic Cardiac Injuries Kings County Hospital Center Verena Liu, MD 9/1/2011 Case Presentation 69 year old male recently diagnosed with a 3.8 cm x 4.3 cm hepatocellular CA in the superior segment of
Which Blunt Trauma Patients Should Be Studied by Abdominal CT?
 MDCT of Bowel and Mesenteric Injury: How Findings Influence Management 4 th Nordic Trauma Radiology Course 2006 4 th Nordic Trauma Radiology Course 2006 Stuart E. Mirvis, M.D., FACR Department of Radiology
MDCT of Bowel and Mesenteric Injury: How Findings Influence Management 4 th Nordic Trauma Radiology Course 2006 4 th Nordic Trauma Radiology Course 2006 Stuart E. Mirvis, M.D., FACR Department of Radiology
REBOA new snake in the grass?
 REBOA new snake in the grass? Does it have a place in South Africa and other LMICs? Tim Hardcastle Trauma Surgeon IALCH/UKZN Controversies in Surgery 2016 History nothing new under the sun (Solomon = Ecclesiates)
REBOA new snake in the grass? Does it have a place in South Africa and other LMICs? Tim Hardcastle Trauma Surgeon IALCH/UKZN Controversies in Surgery 2016 History nothing new under the sun (Solomon = Ecclesiates)
vel 2 Level 2 3,034 c-spine evaluations with CSR Level 3 detected injury only 53% of the time. Level 3 False (-) rate 47%
 rate 47%") Objectives Blunt and Penetrating Neck Trauma Julie Mayglothling, MD, FACEP Virginia Commonwealth University Richmond, VA Summit to Sound, May 20 th, 2011 Blunt Neck Trauma Evaluation of the low mechanism,
Objectives Blunt and Penetrating Neck Trauma Julie Mayglothling, MD, FACEP Virginia Commonwealth University Richmond, VA Summit to Sound, May 20 th, 2011 Blunt Neck Trauma Evaluation of the low mechanism,
Abdominal Aortic Aneurysm - Part 1. Learning Objectives. Disclosure. University of Toronto Division of Vascular Surgery
 University of Toronto Division of Vascular Surgery Abdominal Aortic Aneurysm - Part 1 Dr Mark Wheatcroft & Dr Elisa Greco Vascular Surgeon, St Michael s Hospital, Toronto & University of Toronto Disclosure
University of Toronto Division of Vascular Surgery Abdominal Aortic Aneurysm - Part 1 Dr Mark Wheatcroft & Dr Elisa Greco Vascular Surgeon, St Michael s Hospital, Toronto & University of Toronto Disclosure
Financial Disclosure. Objectives 9/24/2018
 Hemorrhage and Transfusion Adjuncts in the Setting of Damage Control Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Adjunct Professor of Orthopedics and Neurosurgery, University
Hemorrhage and Transfusion Adjuncts in the Setting of Damage Control Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Adjunct Professor of Orthopedics and Neurosurgery, University
Shedding Light on Neonatal X-rays. Objectives. Indications for X-Rays 5/14/2018
 Shedding Light on Neonatal X-rays Barbara C. Mordue, MSN, NNP-BC Neonatal Nurse Practitioner LLUH Children s Hospital, NICU Objectives Utilize a systematic approach to neonatal x-ray interpretation Identify
Shedding Light on Neonatal X-rays Barbara C. Mordue, MSN, NNP-BC Neonatal Nurse Practitioner LLUH Children s Hospital, NICU Objectives Utilize a systematic approach to neonatal x-ray interpretation Identify