An Epidemiological Overview
|
|
|
- Maria Amberlynn York
- 5 years ago
- Views:
Transcription

1
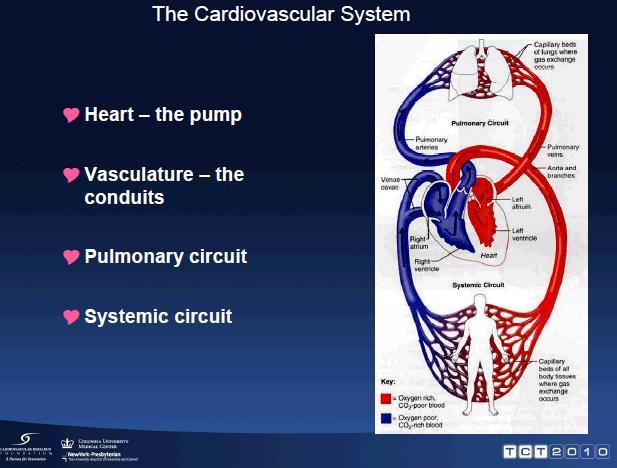
2 An Epidemiological Overview Cardiovascular disease (CVD) is the leading cause of death in the U.S. In 2005 CVD accounted for approximately 38 percent of all deaths CVD has been the number one killer in the U.S. since 1900 except for 1918 (influenza) More that 2,500 Americans die from CVD each day Among women, 1 in 2.6 deaths from CVD

3 Death Rates for Cardiovascular Disease, Including CHD and Stroke for Selected Countries

4 Increasing Prevalence of the Risk Factors for Non Communicable Diseases Globalization Urbanization Poverty Low Education Stress Smoking Unhealthy Diet Phys. Inactivity Blood Sugar Blood Pressure Cholesterol BMI Heart Disease Stroke Cancer Chronic Lung Ds Predisposing Environment Behavioral Risk Factors Biologic Risk factors Chronic NCD Morbidity/Mortality Adopted Preventing Chronic Disease: A Vital Investment. WHO 2005 Lancet 2011; 337:
5
6 Types Of Cardiovascular Disease Atherosclerosis Coronary heart disease (CHD) Irregular heartbeat (arrhythmia) Congestive heart failure (CHF) Congenital and rheumatic heart disease Stroke

7 Percentage Breakdown of Deaths from Cardiovascular Disease in the United States, 2001
8 ATHEROSCLEROSIS

9 Prevention of Cardiovascular Disease is anchored on preventing or slowing the progression of atherosclerosis Foam Cells Fatty Streak Intermediate Lesion Atheroma Fibrous Plaque Complicated Lesion/Rupture Stroke TIA MI Angina High BP Renal failure Endothelial Dysfunction PAD From First Decade From Third Decade From Fourth Decade Growth Mainly by Lipid Accumulation Smooth Muscle and Collagen Thrombosis Hematoma Pepine CJ. Am J Cardiol. 1998;82:23S-27S.
10 Coronary Heart Disease Myocardial infarction (MI) or heart attack blood supplying the heart is disrupted Coronary thrombosis blood clot in the artery Embolus when the blood clot is dislodged and moves through the circulatory system Collateral circulation - if blockage to the heart is minor, an alternative blood flow is selected
11 Arrhythmias
12 Congestive Heart Failure (CHF) Damaged or overworked heart muscle is unable to keep blood circulating normally Affects over 5 million Americans Damage to heart muscle may result from: rheumatic fever, pneumonia, heart attack, or other cardiovascular problem Lack of proper circulation may allow blood to accumulate in the vessels of the legs, ankles, or lungs Diuretics relieve fluid accumulation
13
14
15 Congenital And Rheumatic Heart Disease Congenital heart disease affects 1 out of 125 children born May be due to hereditary factors, maternal diseases, or chemical intake (alcohol) during fetal development Rheumatic heart disease results from rheumatic fever which affects connective tissue
16 Stroke Occurs when the blood supply to the brain is interrupted Thrombus blood clot Embolus free flowing clot Aneurysm bulging or burst blood vessel Transient ischemic attack (TIA) brief interruptions that cause temporary impairment

17 Common Blood Vessel Disorders
18 Reducing Your Risk For Cardiovascular Diseases Risks you CAN control Avoid tobacco Maintain a healthy weight Modify dietary habits Exercise regularly Control diabetes Control blood pressure Systolic Diastolic Control lipid Cut back on saturated fat and cholesterol Manage stress
19 Reducing Your Risk For Cardiovascular Diseases Risks you CANNOT control Heredity Age Gender Race
20 Hypertension is the leading cause of death globally, especially in Asia Ezzati and Riboli. N Engl J Med 2013;369: Deaths attributable to individual risk factors
21 Physiology of Hypertension 3 key physiological mechanism lead to development of hypertension 1. Sodium/Volume 2. Renin Angiotensin Aldosterone System (RAAS) 3. Sympathetic Nervous System (SNS) Studies prove that drugs targeting Sodium/Volume (CCBs and DU) or the RAAS system fare better than SNS blockers in CV outcomes and BP control Even though SNS tone is higher in hypertensive than in normotensives, these results indicates that in most cases the SNS is not a driving force The Journal of Clinical Hypertension 2012;14 (10 );

22 Multiple Interactions among the Mechanisms of Controlling Blood Pressure Kaplan and Opie. Lancet 2006;367:168 76
23 Evolution of Hypertension Younger Pre-hypertensive Hypertensive + Damage Vasoconstriction Increased Peripheral Resistance Vascular remodelling RAAS and SNS Activation Older Hypertensive + Clinical Disease Declining GFR Sodium retention Increased Cardiac output Stiff Aorta systolic hypertension Number of Drugs Plasma Renin B. Williams. 2007

24 Most Hypertensive Patients Have Additional Risk Factors REACH Registry N=67,888 patients aged 45 years or older from 44 countries 81.8% Hypertension a 90.3% with 3 RFs a 140/90 mm Hg at baseline. RFs include: treated diabetes, diabetic nephropathy, ankle-brachial index of <0.9, asymptomatic carotid stenosis 70%, SBP >150 mm Hg, treated hypercholesterolemia, current smoking, men 65 y, women 70 y. REACH, Reduction of Atherothrombosis for Continued Health; RF, risk factor; SBP, systolic blood pressure. Bhatt DL et al. JAMA. 2006;295(2):
25 Risk factors lead to increasing risk of organ damage and clinical events: The cardio-renal continuum The risk associated with hypertension is greatly magnified by other CV risk factors, e.g.: Hyperlipidemia Diabetes LVH Increased arterial stiffness The presence of such risk factors initiates pathological events and processes like oxidative stress and endothelial dysfunction which ultimately lead to overt organ damage and failure Many of these processes leading to CV and renal disease involve the renin-angiotensin system (RAS) and the actions of its most biologically active component angiotensin II Dzau et al. Circulation 2006;114: Mancia et al. J Hypertens 2007;25:


26 From risk factors to organ failure: A continuous development Clinical Disease Diabetes Subclinical Organ Damage Angina IMT Cardiovascular Event TIA LVH Proteinuria Myocardial Infarction Risk Factors Moderate Renal Disease Mild Renal Disease Hypertension Increased LDL End Organ Failure LV remodeling Microalbuminuria Stroke End-Stage Renal Disease Chronic Heart Failure Diabetes/Metabolic Syndrome Smoking Dzau VJ, et al. Circulation. 2006;114:
27 Diagnosis of Hypertension Office BP is recommended for screening and diagnosis of hypertension Diagnosis of hypertension should be based on at least two BP measurements per visit and on at least two visits Out-of-office BP should be considered to confirm the diagnosis of hypertension, identify the type of hypertension, detect hypotensive episodes, and maximize prediction of CV risk For out-of-office BP measurements, ABPM or HBPM may be considered, depending on indication, availability, ease, cost of use, and, if appropriate, patient preference Mancia G et al. J Hypertens. 2013;31(7):
28 Hypertension - JNC BP Classifications: SBP 220 Stage SBP (mm Hg) No recommendations for SBP in JNC I or JNC II ISH ISH Normal Stage 2 Stage 1 Borderline Stage 3 Stage 3 Stage 2 Stage 2 Stage 1 Stage 1 Highnormal Highnormal Normal Normal Optimal Optimal Borderline Prehypertension Normal JNC I JNC II JNC III JNC IV JNC V JNC VI JNC 7 JNC 8 JNC I. JAMA. 1977;237: JNC II. Arch Intern Med. 1980;140: JNC III. Arch Intern Med. 1984;144: JNC IV. Arch Intern Med. 1988;148: JNC V. Arch Intern Med. 1993;153: JNC VI. Arch Intern Med. 1997;157: Chobanian AV et al. JAMA. 2003;289:
29 Hypertension - JNC BP Classifications: DBP Stage 4 DBP (mm Hg) Hypertensive Severe Severe Severe Moderate Moderate Moderate Stage 3 Stage 3 Stage 2 Stage 2 Stage Consider therapy Mild Mild Mild Stage 1 Stage 1 Stage Normal Normal Normal Normal Optimal Optimal JNC I JNC II JNC III JNC IV JNC V JNC VI Highnormal Highnormal Highnormal Highnormal Prehypertension Normal JNC 7 JNC 8 JNC I. JAMA. 1977;237: JNC II. Arch Intern Med. 1980;140: JNC III. Arch Intern Med. 1984;144: JNC IV. Arch Intern Med. 1988;148: JNC V. Arch Intern Med. 1993;153: JNC VI. Arch Intern Med. 1997;157: Chobanian AV et al. JAMA. 2003;289:
30 Increased 24-hour BPV has been associated with CV risk Incidence of mortality and cardiovascular events by fifths of the distributions of the systolic average real variability in 8,938 patients Hansen TW, et al. Hypertension 2010;55: BPV, blood pressure variability; CV, cardiovascular; NCV, non CV.
31 Guidelines on BPV NICE Variability in SBP when measured visit-to-visit is a strong predictor of stroke, independent of mean SBP Whatever the underlying mechanisms, SBP variability appears to be an important independent predictor of clinical outcomes Updated guidance recommends the best available evidence-based treatment options to suppress BPV in people with hypertension ESC/ESH guidelines Consideration should be given to the evidence that visit-to-visit BPV may be a determinant of CV risk, independently of the mean BP levels achieved during long-term treatment, and that, thus, CV protection may be greater in patients with consistent BP control throughout visits BP, blood pressure; CV, cardiovascular; BPV, BP variability; SBP, systolic BP. 1. National Institute for Health and Clinical Excellence (NICE) Clinical Guideline 127. Available at: 2. Mancia G, et al. Eur Heart J 2013;34:

32 Association between CV events and early morning period 18:00 0:00 6:00 12:00 Time of day 1. Muller JE, et al. N Engl J Med 1985;313: Marler JR, et al. Stroke 1989;20: CV, cardiovascular risk; EMBPS, early morning blood pressure surge.
33 MBP surge as a cardiovascular risk Morning surge group (n=46) Non-surge group (n=145) P-value Age (years) NS 24-h systolic BP (mmhg) NS Baseline data Silent cerebral infarct prevalence (%) Number (/person) Multiple cerebral infarcts prevalence (%) Prospective data Stroke incidence (%) (relative risk = 2.7) A 10 mm Hg increase in morning surge in SBP increased clinical stroke risk by 22% Kario K, et al. J Cardiovasc Pharmacol 2003;42 Suppl 1:S87-S91. MBP, morning blood pressure; SBP, systolic blood pressure.



34 BPV and MBP surge are very important and should be targeted Therefore the class of antihypertensive which can control BPV and MBP surge should be the initial treatment of choice Which class of antihyperintensives? CCB, ARB, ACEI, diuretics ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker; BPV, BP variability; CCB, calcium channel blocker.
35 Stratification of Total CV Risk Into Risk Categories According to BP, Risk Factors, and Comorbidities 2013 ESH/ESC Guidelines for the Management of Arterial Hypertension BP, mmhg Other Risk Factors, Asymptomatic OD, or Disease High Normal SBP or DBP Grade 1 Hypertension SBP or DBP Grade 2 Hypertension SBP or DBP Grade 3 Hypertension SBP 180 or DBP 110 No other RF Low risk Moderate risk High risk 1 or 2 RFs Low risk Moderate risk Moderate to high risk High risk 3 RFs Low to moderate risk Moderate to high risk High risk High risk OD, CKD stage 3, or diabetes Moderate to high risk High risk High risk High to very high risk Symptomatic CVD, CKD stage 4, or diabetes with OD/RFs Very high risk Very high risk Very high risk Very high risk CKD, chronic kidney disease; CVD, cardiovascular disease; OD, organ damage. Mancia G et al. J Hypertens. 2013;31(7):
36 JNC 8 Guideline Treatment Recommendations and BP Goals Adult aged 18 years with hypertension Implement lifestyle interventions (continue throughout management) Set BP goal and initiate BP-lowering medication based on age, diabetes, and CKD General population (no diabetes or CKD) Diabetes or CKD present Age 60 y Age <60 y All ages Diabetes present No CKD All ages CKD present with or without diabetes BP goal SBP <150 mm Hg DBP <90 mm Hg BP goal SBP <140 mm Hg DBP <90 mm Hg BP goal SBP <140 mm Hg DBP <90 mm Hg BP goal SBP <140 mm Hg DBP <90 mm Hg Nonblack Black All races Initiate thiazide-type diuretic or ACEI or ARB or CCB alone or in combination a Initiate thiazide-type diuretic or CCB alone or in combination Initiate ACEI or ARB, alone or in combination with other drug class Select a drug treatment titration strategy A. Maximize first medication before adding second or B. Add second medication before reaching maximum dose of first medication or C. Start with 2 medication classes separately or as FDC FDC, fixed-dose combination; a ACEIs and ARBs should not be used in combination James PA et al. JAMA. 2014;311(5):



37 2013 ESH/ESC Hypertension Guidelines ESH/ESC Hypertension Guidelines: Possible Combinations of Antihypertensive Drug Classes Green/continuous: preferred Green/dashed: useful (with some limitations) Man Black/dashed: possible but less well tested Red/continuous: not recommended Only dihydropyridines to be combined with -blockers (except for verapamil or diltiazem for rate control in AF). Thiazides + -blockers increase risk of new onset DM. ACEI + ARB combination is discouraged. Mancia G et al. J Hypertens. 2013;31(7):
38 Different Classes of Drugs have Different Sites of Action BP = Cardiac output = X Total peripheral resistance Heart rate X Stroke volume Arterial pressure Venous pressure β-blockers Diuretics CCBs ARBs ACEIs ACEI = angiotensin-converting enzyme inhibitor; ARB = angiotensin Type II receptor blocker; CCB = calcium channel blocker Different, but complementary mechanism of action Beevers, et al. BMJ 2001;322:912 6; McGhee, et al. Crit Care Nurse 2002;22:60 4; Goodman & Gilman s Pharmacological Basis of Therapeutics. 9 th ed
39 New Weapons Against Heart Disease Techniques for diagnosing heart disease Electrocardiogram (ECG) Angiography Single positron emission color tomography (SPECT) Radionuclide imaging Magnetic resonance imaging (MRI) Ultrafast CT Digital cardiac angiography (DSA)
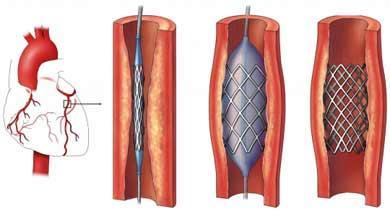
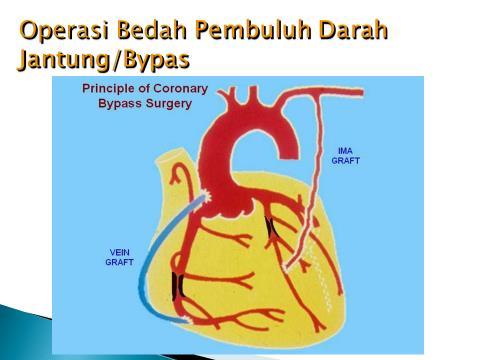
40 Angioplasty Versus Bypass Surgery
41
42
43 Aspirin For Heart Disease? Research shows that 80 milligrams of aspirin every other day is beneficial to heart patients due to its blood thinning properties Some side effects of aspirin: gastrointestinal intolerance and a tendency for difficulty with blood clotting Should only be taken under the advice of your physician
44 Thrombolysis If victim reaches an emergency room and is diagnosed quickly, thrombolysis can be performed Thrombolysis involves injecting an agent such as tissue plasminogen activator (TPA) to dissolve the clot and restore some blood flow
45 Summary CV diseases are the leading cause of deaths globally There are numbers of risk factors that can be controlled to prevent CV diseases Hypertension is one of the important risk factor which could be managed Blood Pressure Variability and Morning BP Surge are associated with CV risk
46
An Epidemiological Overview
 An Epidemiological Overview Cardiovascular disease (CVD) is the leading cause of death in the U.S. In 2005 CVD accounted for approximately 38 percent of all deaths CVD has been the number one killer in
An Epidemiological Overview Cardiovascular disease (CVD) is the leading cause of death in the U.S. In 2005 CVD accounted for approximately 38 percent of all deaths CVD has been the number one killer in
An Epidemiological Overview
 An Epidemiological Overview Cardiovascular disease (CVD) is the leading cause of death in the U.S. In 2005 CVD accounted for approximately 38 percent of all deaths CVD has been the number one killer in
An Epidemiological Overview Cardiovascular disease (CVD) is the leading cause of death in the U.S. In 2005 CVD accounted for approximately 38 percent of all deaths CVD has been the number one killer in
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005
 VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ. Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH
 ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH Hypertension Co-Morbidities HTN Commonly Clusters with Other Risk
ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH Hypertension Co-Morbidities HTN Commonly Clusters with Other Risk
JNC Evidence-Based Guidelines for the Management of High Blood Pressure in Adults
 JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
Hypertension Management Controversies in the Elderly Patient
 Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
DISCLOSURES OUTLINE OUTLINE 9/29/2014 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE
 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
The Evolution To Treatment Of Hypertension With Advanced Formulation
 The Evolution To Treatment Of Hypertension With Advanced Formulation Dr. Donald Ang MBChB (UK) FRCP (Edin) MD (UK) CCST Cardiology (UK) FESC (Europe) Consultant Cardiologist Island Hospital Penang High
The Evolution To Treatment Of Hypertension With Advanced Formulation Dr. Donald Ang MBChB (UK) FRCP (Edin) MD (UK) CCST Cardiology (UK) FESC (Europe) Consultant Cardiologist Island Hospital Penang High
Egyptian Hypertension Guidelines
 Egyptian Hypertension Guidelines 2014 Egyptian Hypertension Guidelines Dalia R. ElRemissy, MD Lecturer of Cardiovascular Medicine Cairo University Why Egyptian Guidelines? Guidelines developed for rich
Egyptian Hypertension Guidelines 2014 Egyptian Hypertension Guidelines Dalia R. ElRemissy, MD Lecturer of Cardiovascular Medicine Cairo University Why Egyptian Guidelines? Guidelines developed for rich
Todd S. Perlstein, MD FIFTH ANNUAL SYMPOSIUM
 Todd S. Perlstein, MD FIFTH ANNUAL SYMPOSIUM Faculty Disclosure I have no financial interest to disclose No off-label use of medications will be discussed FIFTH ANNUAL SYMPOSIUM Recognize changes between
Todd S. Perlstein, MD FIFTH ANNUAL SYMPOSIUM Faculty Disclosure I have no financial interest to disclose No off-label use of medications will be discussed FIFTH ANNUAL SYMPOSIUM Recognize changes between
What s In the New Hypertension Guidelines?
 American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
Lecture 8 Cardiovascular Health Lecture 8 1. Introduction 2. Cardiovascular Health 3. Stroke 4. Contributing Factors
 Lecture 8 Cardiovascular Health 1 Lecture 8 1. Introduction 2. Cardiovascular Health 3. Stroke 4. Contributing Factors 1 Human Health: What s Killing Us? Health in America Health is the U.S Average life
Lecture 8 Cardiovascular Health 1 Lecture 8 1. Introduction 2. Cardiovascular Health 3. Stroke 4. Contributing Factors 1 Human Health: What s Killing Us? Health in America Health is the U.S Average life
10/8/2018. Lecture 9. Cardiovascular Health. Lecture Heart 2. Cardiovascular Health 3. Stroke 4. Contributing Factor
 Lecture 9 Cardiovascular Health 1 Lecture 9 1. Heart 2. Cardiovascular Health 3. Stroke 4. Contributing Factor 1 The Heart Muscular Pump The Heart Receives blood low pressure then increases the pressure
Lecture 9 Cardiovascular Health 1 Lecture 9 1. Heart 2. Cardiovascular Health 3. Stroke 4. Contributing Factor 1 The Heart Muscular Pump The Heart Receives blood low pressure then increases the pressure
hypertension Head of prevention and control of CVD disease office Ministry of heath
 hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
2003 World Health Organization (WHO) / International Society of Hypertension (ISH) Statement on Management of Hypertension.
 / International Society of Hypertension (ISH) Statement on Management of Hypertension.") 2003 World Health Organization (WHO) / International Society of Hypertension (ISH) Statement on Management of Hypertension Writing Group: Background Hypertension worldwide causes 7.1 million premature
2003 World Health Organization (WHO) / International Society of Hypertension (ISH) Statement on Management of Hypertension Writing Group: Background Hypertension worldwide causes 7.1 million premature
 Five chapters 1. What is CVD prevention 2. Why is CVD prevention needed 3. Who needs CVD prevention 4. How is CVD prevention applied 5. Where should CVD prevention be offered Shorter, more adapted to clinical
Five chapters 1. What is CVD prevention 2. Why is CVD prevention needed 3. Who needs CVD prevention 4. How is CVD prevention applied 5. Where should CVD prevention be offered Shorter, more adapted to clinical
Long-Term Care Updates
 Long-Term Care Updates August 2015 By Darren Hein, PharmD Hypertension is a clinical condition in which the force of blood pushing on the arteries is higher than normal. This increases the risk for heart
Long-Term Care Updates August 2015 By Darren Hein, PharmD Hypertension is a clinical condition in which the force of blood pushing on the arteries is higher than normal. This increases the risk for heart
Hypertension Management Focus on new RAAS blocker. Disclosure
 Hypertension Management Focus on new RAAS blocker Rameshkumar Raman M.D Endocrine Associates of The Quad Cities Disclosure Speaker bureau Abbott, Eli Lilly, Novo Nordisk, Novartis, Takeda, Merck, Solvay
Hypertension Management Focus on new RAAS blocker Rameshkumar Raman M.D Endocrine Associates of The Quad Cities Disclosure Speaker bureau Abbott, Eli Lilly, Novo Nordisk, Novartis, Takeda, Merck, Solvay
Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension
 Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension Prof. Massimo Volpe, MD, FAHA, FESC, Chair of Cardiology, Department of Clinical and Molecular Medicine
Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension Prof. Massimo Volpe, MD, FAHA, FESC, Chair of Cardiology, Department of Clinical and Molecular Medicine
Management of Hypertension. M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine
 Division of Nephrology University of Missouri School of Medicine") Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
7/7/ CHD/MI LVH and LV dysfunction Dysrrhythmias Stroke PVD Renal insufficiency and failure Retinopathy. Normal <120 Prehypertension
 Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
Prevalence of Hypertension Hypertension: Diagnosis and Management T. Villela, M.D. Program Director University of California, San Francisco-San Francisco General Hospital Family and Community Medicine
Cardiovascular System and Health. Chapter 15
 Cardiovascular System and Health Chapter 15 Cardiovascular Disease Leading cause of death in U.S. Claims 1 life every 43 seconds Often, the first sign is a fatal heart attack Death Rates #1 CVD #2 Cancer
Cardiovascular System and Health Chapter 15 Cardiovascular Disease Leading cause of death in U.S. Claims 1 life every 43 seconds Often, the first sign is a fatal heart attack Death Rates #1 CVD #2 Cancer
DISCLOSURE PHARMACIST OBJECTIVES 9/30/2014 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES. I have nothing to disclose.
 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
Hypertension in 2015: SPRINT-ing ahead of JNC-8. MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic
 Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Reframe the Paradigm of Hypertension treatment Focus on Diabetes
 Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
Clinical Updates in the Treatment of Hypertension JNC 7 vs. JNC 8. Lauren Thomas, PharmD PGY1 Pharmacy Practice Resident South Pointe Hospital
 Clinical Updates in the Treatment of Hypertension JNC 7 vs. JNC 8 Lauren Thomas, PharmD PGY1 Pharmacy Practice Resident South Pointe Hospital Objectives Review the Eighth Joint National Committee (JNC
Clinical Updates in the Treatment of Hypertension JNC 7 vs. JNC 8 Lauren Thomas, PharmD PGY1 Pharmacy Practice Resident South Pointe Hospital Objectives Review the Eighth Joint National Committee (JNC
Cardiovascular Disease
 Cardiovascular Disease Chapter 15 Introduction Cardiovascular disease (CVD) is the leading cause of death in the U.S. One American dies from CVD every 33 seconds Nearly half of all Americans will die from
Cardiovascular Disease Chapter 15 Introduction Cardiovascular disease (CVD) is the leading cause of death in the U.S. One American dies from CVD every 33 seconds Nearly half of all Americans will die from
Difficult to Treat Hypertension
 Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Vascular disease. Structural evaluation of vascular disease. Goo-Yeong Cho, MD, PhD Seoul National University Bundang Hospital
 Vascular disease. Structural evaluation of vascular disease Goo-Yeong Cho, MD, PhD Seoul National University Bundang Hospital resistance vessels : arteries
Vascular disease. Structural evaluation of vascular disease Goo-Yeong Cho, MD, PhD Seoul National University Bundang Hospital resistance vessels : arteries
Update on Current Trends in Hypertension Management
 Friday General Session Update on Current Trends in Hypertension Management Shawna Nesbitt, MD Associate Dean, Minority Student Affairs Associate Professor, Department of Internal Medicine Office of Student
Friday General Session Update on Current Trends in Hypertension Management Shawna Nesbitt, MD Associate Dean, Minority Student Affairs Associate Professor, Department of Internal Medicine Office of Student
Director of the Israeli Institute for Quality in Medicine Israeli Medical Association July 1st, 2016
 The differential effect of Atherosclerosis on end organ damage in adult and elderly patients with CVRF: New Algorithm for Hypertension Diagnosis and Treatment R. Zimlichman, FAHA, FASH, FESC, FESH Chief
The differential effect of Atherosclerosis on end organ damage in adult and elderly patients with CVRF: New Algorithm for Hypertension Diagnosis and Treatment R. Zimlichman, FAHA, FASH, FESC, FESH Chief
Prevention of Heart Failure: What s New with Hypertension
 Prevention of Heart Failure: What s New with Hypertension Ali AlMasood Prince Sultan Cardiac Center Riyadh 3ed Saudi Heart Failure conference, Jeddah, 13 December 2014 Background 20-30% of Saudi adults
Prevention of Heart Failure: What s New with Hypertension Ali AlMasood Prince Sultan Cardiac Center Riyadh 3ed Saudi Heart Failure conference, Jeddah, 13 December 2014 Background 20-30% of Saudi adults
DEPARTMENT OF GENERAL MEDICINE WELCOMES
 DEPARTMENT OF GENERAL MEDICINE WELCOMES 1 Dr.Mohamed Omar Shariff, 2 nd Year Post Graduate, Department of General Medicine. DR.B.R.Ambedkar Medical College & Hospital. 2 INTRODUCTION Leading cause of global
DEPARTMENT OF GENERAL MEDICINE WELCOMES 1 Dr.Mohamed Omar Shariff, 2 nd Year Post Graduate, Department of General Medicine. DR.B.R.Ambedkar Medical College & Hospital. 2 INTRODUCTION Leading cause of global
Management of Hypertension
 Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Int. J. Pharm. Sci. Rev. Res., 36(1), January February 2016; Article No. 06, Pages: JNC 8 versus JNC 7 Understanding the Evidences
, January February 2016; Article No. 06, Pages: JNC 8 versus JNC 7 Understanding the Evidences") Research Article JNC 8 versus JNC 7 Understanding the Evidences Anns Clara Joseph, Karthik MS, Sivasakthi R, Venkatanarayanan R, Sam Johnson Udaya Chander J* RVS College of Pharmaceutical Sciences, Coimbatore,
Research Article JNC 8 versus JNC 7 Understanding the Evidences Anns Clara Joseph, Karthik MS, Sivasakthi R, Venkatanarayanan R, Sam Johnson Udaya Chander J* RVS College of Pharmaceutical Sciences, Coimbatore,
Cardiovascular Diseases and Diabetes
 Cardiovascular Diseases and Diabetes LEARNING OBJECTIVES Ø Identify the components of the cardiovascular system and the various types of cardiovascular disease Ø Discuss ways of promoting cardiovascular
Cardiovascular Diseases and Diabetes LEARNING OBJECTIVES Ø Identify the components of the cardiovascular system and the various types of cardiovascular disease Ø Discuss ways of promoting cardiovascular
Hypertension Update Clinical Controversies Regarding Age and Race
 Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
T. Suithichaiyakul Cardiomed Chula
 T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
New Antihypertensive Strategies to Improve Blood Pressure Control
 New Antihypertensive Strategies to Improve Blood Pressure Control Antonio Coca, MD, PhD,, FRCP, FESC Hypertension and Vascular Risk Unit Department of Internal Medicine. Hospital Clínic (IDIBAPS) University
New Antihypertensive Strategies to Improve Blood Pressure Control Antonio Coca, MD, PhD,, FRCP, FESC Hypertension and Vascular Risk Unit Department of Internal Medicine. Hospital Clínic (IDIBAPS) University
None. Disclosure: Relationships with Industry Conflicts of Interests. Learning Objectives: Participants will be able to:
 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults: Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC 8) James W. Shaw, MD Memorial Lecture
2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults: Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC 8) James W. Shaw, MD Memorial Lecture
Update in Hypertension
 Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Management of Hypertension in special groups. DR-Mohammed Salah Assistant Lecturer of Cardiology Mansoura University
 Management of Hypertension in special groups BY DR-Mohammed Salah Assistant Lecturer of Cardiology Mansoura University AGENDA SPECIAL GROUPS SPECIFIC DRUDS FOR SPECIAL GROUPS TARGET BP FOR SPECIAL GROUPS:
Management of Hypertension in special groups BY DR-Mohammed Salah Assistant Lecturer of Cardiology Mansoura University AGENDA SPECIAL GROUPS SPECIFIC DRUDS FOR SPECIAL GROUPS TARGET BP FOR SPECIAL GROUPS:
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Long-Term Complications of Diabetes Mellitus Macrovascular Complication
 Long-Term Complications of Diabetes Mellitus Macrovascular Complication Sung Hee Choi MD, PhD Professor, Seoul National University College of Medicine, SNUBH, Bundang Hospital Diabetes = CVD equivalent
Long-Term Complications of Diabetes Mellitus Macrovascular Complication Sung Hee Choi MD, PhD Professor, Seoul National University College of Medicine, SNUBH, Bundang Hospital Diabetes = CVD equivalent
Cardiovascular Disorders. Heart Disorders. Diagnostic Tests for CV Function. Bio 375. Pathophysiology
 Cardiovascular Disorders Bio 375 Pathophysiology Heart Disorders Heart disease is ranked as a major cause of death in the U.S. Common heart diseases include: Congenital heart defects Hypertensive heart
Cardiovascular Disorders Bio 375 Pathophysiology Heart Disorders Heart disease is ranked as a major cause of death in the U.S. Common heart diseases include: Congenital heart defects Hypertensive heart
New Hypertension Guideline Recommendations for Adults July 7, :45-9:30am
 Advances in Cardiovascular Disease 30 th Annual Convention and Reunion UERM-CMAA, Inc. Annual Convention and Scientific Meeting July 5-8, 2018 New Hypertension Guideline Recommendations for Adults July
Advances in Cardiovascular Disease 30 th Annual Convention and Reunion UERM-CMAA, Inc. Annual Convention and Scientific Meeting July 5-8, 2018 New Hypertension Guideline Recommendations for Adults July
Statistical Fact Sheet Populations
 Statistical Fact Sheet Populations At-a-Glance Summary Tables Men and Cardiovascular Diseases Mexican- American Males Diseases and Risk Factors Total Population Total Males White Males Black Males Total
Statistical Fact Sheet Populations At-a-Glance Summary Tables Men and Cardiovascular Diseases Mexican- American Males Diseases and Risk Factors Total Population Total Males White Males Black Males Total
Hypertension and obesity. Dr Wilson Sugut Moi teaching and referral hospital
 Hypertension and obesity Dr Wilson Sugut Moi teaching and referral hospital No conflict of interests to declare Obesity Definition: excessive weight that may impair health BMI Categories Underweight BMI
Hypertension and obesity Dr Wilson Sugut Moi teaching and referral hospital No conflict of interests to declare Obesity Definition: excessive weight that may impair health BMI Categories Underweight BMI
HYPERTENSION: ARE WE GOING TOO LOW?
 HYPERTENSION: ARE WE GOING TOO LOW? George L. Bakris, M.D.,F.A.S.N.,F.A.S.H., F.A.H.A. Professor of Medicine Director, ASH Comprehensive Hypertension Center University of Chicago Medicine Chicago, IL USA
HYPERTENSION: ARE WE GOING TOO LOW? George L. Bakris, M.D.,F.A.S.N.,F.A.S.H., F.A.H.A. Professor of Medicine Director, ASH Comprehensive Hypertension Center University of Chicago Medicine Chicago, IL USA
JNC 8 -Controversies. Sagren Naidoo Nephrologist CMJAH
 JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets
 New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of
New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of
When should you treat blood pressure in the young?
 ESC Stockholm - Dilemmas in Cardiovascular Disease Prevention in the Young: 30 th August 2010 When should you treat blood pressure in the young? Bryan Williams MD FRCP FAHA FESC Professor of Medicine Department
ESC Stockholm - Dilemmas in Cardiovascular Disease Prevention in the Young: 30 th August 2010 When should you treat blood pressure in the young? Bryan Williams MD FRCP FAHA FESC Professor of Medicine Department
MANAGEMENT OF HYPERTENSION: TREATMENT THRESHOLDS AND MEDICATION SELECTION
 Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Hypertension Update Warwick Jaffe Interventional Cardiologist Ascot Hospital
 Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Hypertension Update. Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy
 Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
Hypertension. Risk of cardiovascular disease beginning at 115/75 mmhg doubles with every 20/10mm Hg increase. (Grade B)
") Practice Guidelines and Principles: Guidelines and principles are intended to be flexible. They serve as reference points or recommendations, not rigid criteria. Guidelines and principles should be followed
Practice Guidelines and Principles: Guidelines and principles are intended to be flexible. They serve as reference points or recommendations, not rigid criteria. Guidelines and principles should be followed
Antiplatelet Therapy in Primary CVD Prevention and Stable Coronary Artery Disease. Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν.
 Antiplatelet Therapy in Primary CVD Prevention and Stable Coronary Artery Disease Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν.Κιλκίς Primary CVD Prevention A co-ordinated set of actions,
Antiplatelet Therapy in Primary CVD Prevention and Stable Coronary Artery Disease Καρακώστας Γεώργιος Διευθυντής Καρδιολογικής Κλινικής, Γ.Ν.Κιλκίς Primary CVD Prevention A co-ordinated set of actions,
New Lipid Guidelines. PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids.
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
Combination therapy Giuseppe M.C. Rosano, MD, PhD, MSc, FESC, FHFA St George s Hospitals NHS Trust University of London
 Combination therapy Giuseppe M.C. Rosano, MD, PhD, MSc, FESC, FHFA St George s Hospitals NHS Trust University of London KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email:
Combination therapy Giuseppe M.C. Rosano, MD, PhD, MSc, FESC, FHFA St George s Hospitals NHS Trust University of London KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email:
Using the New Hypertension Guidelines
 Using the New Hypertension Guidelines Kamal Henderson, MD Department of Cardiology, Preventive Medicine, University of North Carolina School of Medicine Kotchen TA. Historical trends and milestones in
Using the New Hypertension Guidelines Kamal Henderson, MD Department of Cardiology, Preventive Medicine, University of North Carolina School of Medicine Kotchen TA. Historical trends and milestones in
Diversity and HTN: Approaches to optimal BP control in AfricanAmericans
 Diversity and HTN: Approaches to optimal BP control in AfricanAmericans Quinn Capers, IV, MD, FACC, FSCAI Assistant Professor of Medicine Associate Dean for Admissions Do Racial Differences Really Exist
Diversity and HTN: Approaches to optimal BP control in AfricanAmericans Quinn Capers, IV, MD, FACC, FSCAI Assistant Professor of Medicine Associate Dean for Admissions Do Racial Differences Really Exist
Slide notes: References:
 1 2 3 Cut-off values for the definition of hypertension are systolic blood pressure (SBP) 135 and/or diastolic blood pressure (DBP) 85 mmhg for home blood pressure monitoring (HBPM) and daytime ambulatory
1 2 3 Cut-off values for the definition of hypertension are systolic blood pressure (SBP) 135 and/or diastolic blood pressure (DBP) 85 mmhg for home blood pressure monitoring (HBPM) and daytime ambulatory
Hypertension (JNC-8)
") Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Evolving Concepts on Hypertension: Implications of Three Guidelines (JNC 8 Panel, ESH/ESC, NICE/BSH)
") Evolving Concepts on Hypertension: Implications of Three Guidelines (JNC 8 Panel, ESH/ESC, NICE/BSH) Sidney C. Smith, Jr. MD, FACC, FAHA, FESC Professor of Medicine/Cardiology University of North Carolina
Evolving Concepts on Hypertension: Implications of Three Guidelines (JNC 8 Panel, ESH/ESC, NICE/BSH) Sidney C. Smith, Jr. MD, FACC, FAHA, FESC Professor of Medicine/Cardiology University of North Carolina
Pathophysiology of Cardiovascular System. Dr. Hemn Hassan Othman, PhD
 Pathophysiology of Cardiovascular System Dr. Hemn Hassan Othman, PhD hemn.othman@univsul.edu.iq What is the circulatory system? The circulatory system carries blood and dissolved substances to and from
Pathophysiology of Cardiovascular System Dr. Hemn Hassan Othman, PhD hemn.othman@univsul.edu.iq What is the circulatory system? The circulatory system carries blood and dissolved substances to and from
Complications of Diabetes mellitus. Dr Bill Young 16 March 2015
 Complications of Diabetes mellitus Dr Bill Young 16 March 2015 Complications of diabetes Multi-organ involvement 2 The extent of diabetes complications At diagnosis as many as 50% of patients may have
Complications of Diabetes mellitus Dr Bill Young 16 March 2015 Complications of diabetes Multi-organ involvement 2 The extent of diabetes complications At diagnosis as many as 50% of patients may have
Incidental Findings; Management of patients presenting with high BP. Phil Swales
 Incidental Findings; Management of patients presenting with high BP Phil Swales Consultant Physician Acute & General Medicine University Hospitals of Leicester NHS Trust Objectives The approach to an incidental
Incidental Findings; Management of patients presenting with high BP Phil Swales Consultant Physician Acute & General Medicine University Hospitals of Leicester NHS Trust Objectives The approach to an incidental
Metoprolol Succinate SelokenZOC
 Metoprolol Succinate SelokenZOC Blood Pressure Control and Far Beyond Mohamed Abdel Ghany World Health Organization - Noncommunicable Diseases (NCD) Country Profiles, 2014. 1 Death Rates From Ischemic
Metoprolol Succinate SelokenZOC Blood Pressure Control and Far Beyond Mohamed Abdel Ghany World Health Organization - Noncommunicable Diseases (NCD) Country Profiles, 2014. 1 Death Rates From Ischemic
Jared Moore, MD, FACP
 Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
VALUE OF ACEI IN THE MANAGEMENT OF HYPERTENSION
 VALUE OF ACEI IN THE MANAGEMENT OF HYPERTENSION Dr Catherine BESEME Paris 6 th December 2005 6 th International Congress of Bangladesh Society of Medicine Hypertension is a risk factor at the source, with
VALUE OF ACEI IN THE MANAGEMENT OF HYPERTENSION Dr Catherine BESEME Paris 6 th December 2005 6 th International Congress of Bangladesh Society of Medicine Hypertension is a risk factor at the source, with
Diabetes and Hypertension
 Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Hypertension with Comorbidities Treatment of Metabolic Risk Factors in Children and Adolescents
 Hypertension with Comorbidities Treatment of Metabolic Risk Factors in Children and Adolescents Stella Stabouli Ass. Professor Pediatrics 1 st Department of Pediatrics Hippocratio Hospital Evaluation of
Hypertension with Comorbidities Treatment of Metabolic Risk Factors in Children and Adolescents Stella Stabouli Ass. Professor Pediatrics 1 st Department of Pediatrics Hippocratio Hospital Evaluation of
Combination Therapy for Hypertension
 Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
1. Albuminuria an early sign of glomerular damage and renal disease. albuminuria
 1. Albuminuria an early sign of glomerular damage and renal disease albuminuria Cardio-renal continuum REGRESS Target organ damage Asymptomatic CKD New risk factors Atherosclerosis Target organ damage
1. Albuminuria an early sign of glomerular damage and renal disease albuminuria Cardio-renal continuum REGRESS Target organ damage Asymptomatic CKD New risk factors Atherosclerosis Target organ damage
Hypertension Update 2009
 Hypertension Update 2009 New Drugs, New Goals, New Approaches, New Lessons from Clinical Trials Timothy C Fagan, MD, FACP Professor Emeritus University of Arizona New Drugs Direct Renin Inhibitors Endothelin
Hypertension Update 2009 New Drugs, New Goals, New Approaches, New Lessons from Clinical Trials Timothy C Fagan, MD, FACP Professor Emeritus University of Arizona New Drugs Direct Renin Inhibitors Endothelin
HYPERTENSION AND HEART FAILURE
 HYPERTENSION AND HEART FAILURE Kenya Cardiac Society Symposium Feb 2017 Dr Jeilan Mohamed No conflict of interests . Geoffrey, 45 yr old hypertensive office worker male from Nairobi, has just watched his
HYPERTENSION AND HEART FAILURE Kenya Cardiac Society Symposium Feb 2017 Dr Jeilan Mohamed No conflict of interests . Geoffrey, 45 yr old hypertensive office worker male from Nairobi, has just watched his
Wellness: Concepts and Applications 8 th Edition Anspaugh, Hamrick, Rosato
 Wellness: Concepts and Applications 8 th Edition Anspaugh, Hamrick, Rosato Preventing Cardiovascular Disease Chapter 2 Cardiovascular Disease the leading cause of death in the U.S. 35.3% of all deaths
Wellness: Concepts and Applications 8 th Edition Anspaugh, Hamrick, Rosato Preventing Cardiovascular Disease Chapter 2 Cardiovascular Disease the leading cause of death in the U.S. 35.3% of all deaths
Antihypertensive Trial Design ALLHAT
 1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
Heart Disease. Signs and Symptoms
 Heart Disease The term "heart disease" refers to several types of heart conditions. The most common type is coronary artery disease, which can cause heart attack, angina, heart failure, and arrhythmias.
Heart Disease The term "heart disease" refers to several types of heart conditions. The most common type is coronary artery disease, which can cause heart attack, angina, heart failure, and arrhythmias.
By Prof. Khaled El-Rabat
 What is The Optimum? By Prof. Khaled El-Rabat Professor of Cardiology - Benha Faculty of Medicine HT. Introduction Despite major worldwide efforts over recent decades directed at diagnosing and treating
What is The Optimum? By Prof. Khaled El-Rabat Professor of Cardiology - Benha Faculty of Medicine HT. Introduction Despite major worldwide efforts over recent decades directed at diagnosing and treating
Atherosclerosis. Atherosclerosis happens when the blood vessels
 Atherosclerosis Atherosclerosis happens when the blood vessels that carry oxygen and nutrients from your heart to the rest of your body (arteries) become thick and stiff sometimes restricting blood flow
Atherosclerosis Atherosclerosis happens when the blood vessels that carry oxygen and nutrients from your heart to the rest of your body (arteries) become thick and stiff sometimes restricting blood flow
Management of Lipid Disorders and Hypertension: Implications of the New Guidelines
 Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Management of Hypertension. Ahmed El Hawary MD Suez Canal University
 Management of Hypertension Ahmed El Hawary MD Suez Canal University Minimal vs. Optimal Care Resources more than science affect type of care and level of management. what is possible (minimal care) and
Management of Hypertension Ahmed El Hawary MD Suez Canal University Minimal vs. Optimal Care Resources more than science affect type of care and level of management. what is possible (minimal care) and
Hypertension. Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute
 Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Stroke 101. Maine Cardiovascular Health Summit. Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013
 Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
Hypertension. Penny Mosley MRPharmS
 Hypertension Penny Mosley MRPharmS Outline of presentation Introduction to hypertension Physiological control of arterial blood pressure What determines our bp? What determines the heart rate? What determines
Hypertension Penny Mosley MRPharmS Outline of presentation Introduction to hypertension Physiological control of arterial blood pressure What determines our bp? What determines the heart rate? What determines
M2 TEACHING UNDERSTANDING PHARMACOLOGY
 M2 TEACHING UNDERSTANDING PHARMACOLOGY USING CVS SYSTEM AS AN EXAMPLE NIGEL FONG 2 JAN 2014 TODAY S OBJECTIVE Pharmacology often seems like an endless list of mechanisms and side effects to memorize. To
M2 TEACHING UNDERSTANDING PHARMACOLOGY USING CVS SYSTEM AS AN EXAMPLE NIGEL FONG 2 JAN 2014 TODAY S OBJECTIVE Pharmacology often seems like an endless list of mechanisms and side effects to memorize. To
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014
 HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
The Failing Heart in Primary Care
 The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs
 Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Hypertension and Heart Disease. Weldon James, MD, Mercy Clinic Family Medicine, Union
 Hypertension and Heart Disease Weldon James, MD, Mercy Clinic Family Medicine, Union The Silent Killer High blood pressure, also known as HBP or hypertension, is a widely misunderstood medical condition
Hypertension and Heart Disease Weldon James, MD, Mercy Clinic Family Medicine, Union The Silent Killer High blood pressure, also known as HBP or hypertension, is a widely misunderstood medical condition
Hypertension JNC 8 (2014)
") Hypertension JNC 8 (2014) Renewed: February 2018 Updated: February 2015 Comparison of Seventh Joint National Committee (JNC 7) vs. Eighth Joint National Committee (JNC 8) Hypertension Guidelines Methodology
Hypertension JNC 8 (2014) Renewed: February 2018 Updated: February 2015 Comparison of Seventh Joint National Committee (JNC 7) vs. Eighth Joint National Committee (JNC 8) Hypertension Guidelines Methodology
Hypertension diagnosis (see detail document) Diabetic. Target less than 130/80mmHg
 Diabetic. Target less than 130/80mmHg") Hypertension diagnosis (see detail document) Non-diabetic Diabetic Very elderly (older than 80 years) Target less than 140/90mmHg Target less than 130/80mmHg Consider SBP target less than 150mmHg Non-diabetic
Hypertension diagnosis (see detail document) Non-diabetic Diabetic Very elderly (older than 80 years) Target less than 140/90mmHg Target less than 130/80mmHg Consider SBP target less than 150mmHg Non-diabetic
Hypertension Update Background
 Hypertension Update Background Overview Aaron J. Friedberg, MD Assistant Professor, Clinical Division of General Internal Medicine The Ohio State University Wexner Medical Center Management Guideline Comparison
Hypertension Update Background Overview Aaron J. Friedberg, MD Assistant Professor, Clinical Division of General Internal Medicine The Ohio State University Wexner Medical Center Management Guideline Comparison
Overview. NOT A REPETION OF LOCAL GUIDELINE Dr Diviash Thakrar
 Overview 1. Why hypertension is important? 2. What are basic principles in treatment? 3. Different ways of measuring 4. Hypercholesterolemia NOT A REPETION OF LOCAL GUIDELINE CVD risk factors? Non modifiable
Overview 1. Why hypertension is important? 2. What are basic principles in treatment? 3. Different ways of measuring 4. Hypercholesterolemia NOT A REPETION OF LOCAL GUIDELINE CVD risk factors? Non modifiable
Valsartan Amlodipine HCT Combination: Control To Goal. Dr. Sameh Shaheen M.B.B.Ch, MSc, MD, FESC, FSCAI. Prof of cardiology Ain Shams University
 Valsartan Amlodipine HCT Combination: Control To Goal Dr. Sameh Shaheen M.B.B.Ch, MSc, MD, FESC, FSCAI Prof of cardiology Ain Shams University Sonesta Hotel Cairo Egypt December 4 th 5 th ; 213 Hypertension
Valsartan Amlodipine HCT Combination: Control To Goal Dr. Sameh Shaheen M.B.B.Ch, MSc, MD, FESC, FSCAI Prof of cardiology Ain Shams University Sonesta Hotel Cairo Egypt December 4 th 5 th ; 213 Hypertension
ALLHAT. Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic
 1 U.S. Department of Health and Human Services National Institutes of Health Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker
1 U.S. Department of Health and Human Services National Institutes of Health Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker
Prevention of Cardiovascular Disease
 Save Thais from Heart Diseases 2019 Prevention of Cardiovascular Disease Orawan Anupraiwan, MD. Central Chest Institute of Thailand ASCVD Prevention Pyramid Risk categories Very high-risk High-risk Documented
Save Thais from Heart Diseases 2019 Prevention of Cardiovascular Disease Orawan Anupraiwan, MD. Central Chest Institute of Thailand ASCVD Prevention Pyramid Risk categories Very high-risk High-risk Documented
Dr Doris M. W Kinuthia
 Dr Doris M. W Kinuthia Objectives Normal blood pressures in children Measurement of blood pressure in children Aetiology of Hypertension in children Evaluation of children with hypertension Treatment of
Dr Doris M. W Kinuthia Objectives Normal blood pressures in children Measurement of blood pressure in children Aetiology of Hypertension in children Evaluation of children with hypertension Treatment of