Fluid Resuscitation in Sepsis. A Literature Review
|
|
|
- Lindsey Hardy
- 6 years ago
- Views:
Transcription
1 Fluid Resuscitation in Sepsis A Literature Review
2 "On the floor lay a girl of slender make and juvenile height, but with the face of a superannuated hag... The colour of her countenance was that of lead - a silver blue, ghastly tint; her eyes were sunk deep into sockets, as though they had been driven an inch behind their natural position; her mouth was squared; her features flattened; her eyelids black; her fingers shrunk, bent, and inky in their hue
3


4 The Pioneers
5 Dr Latta s Saline Solution Two to three drachms of muriate of soda (NaCl), two scruples of the bicarbonate of soda in six pints of water and injected it at temperature 112 Fah ( approximately 58mmol/l Na +, 49mmol/l Cl -, 9mmol/l HCO 3- ) Ten of the first fifteen patients died

6 180 years on..
7 Current controversies in fluid therapy in septic patients When to give fluid How much fluid to give Which fluid to use
8 Definitions SIRS: widespread inflammatory response that may or may not be associated with infection: 2 or more of Temperature, tachycardia, tachypnoea and WCC Sepsis: SIRS in the presence of or as a result of suspected or proven infection Septic shock: Sepsis with cardiovascular dysfunction despite the administration of >40ml/kg isotonic fluid in one hour
9 Epidemiology Angus et al. Epidemiology of severe sepsis in the United States: Analysis of incidence, outcome and associated costs of care. Critical Care Med 2001; 29: Estimated 750,000 cases of severe sepsis annually in US Mortality of 28.6% $22,100 per case Starship Hospital cases of sepsis/septic shock
10 Pathophysiology

11 The Evidence When to give fluid How much fluid should we give
12 Early Paediatric Practices Early 1980 s Slow cautious fluid bolus: 10-20ml/kg over minutes Era of limited paediatric ventilators/picu Awareness of SIADH in patients with sepsis and meningitis 1988 The AHA s Textbook of PALS Rapid 20ml/kg fluid boluses to a total of 60ml/kg or more in the first hour of resuscitation
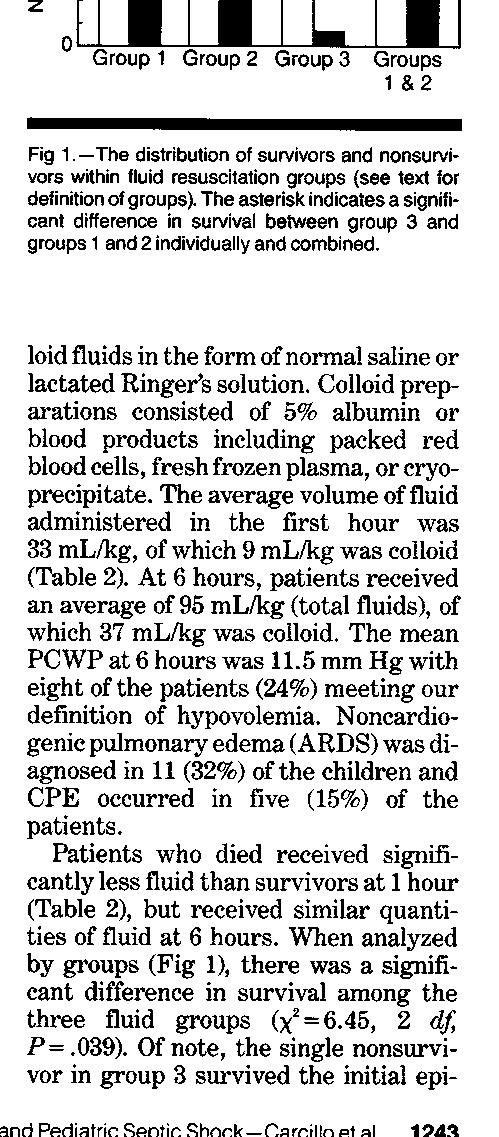
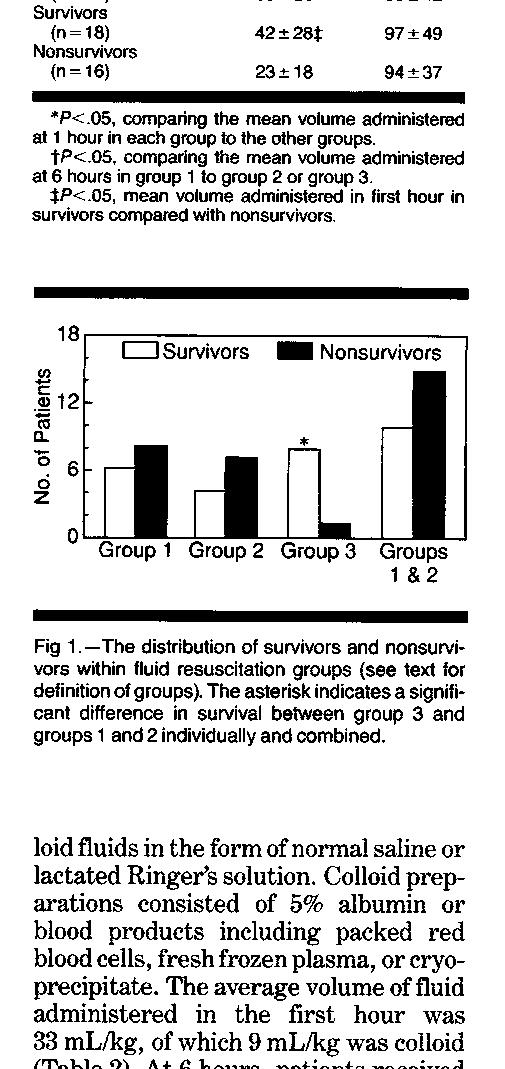
13 Carcillo et al. Role of Early Fluid Resuscitation in Pediatric Septic Shock. JAMA 1991; 266 (9): Children s Hospital National Medical Centre All patients with septic shock with a PAC at 6 hours Group 1: up to 20ml/kg Group 2: 20-40ml/kg and Group 3: >40ml/kg in first hour End points: survival, ARDS, hypovolaemia at 6 hours 34 patients Median age 13.5 months Pre-existing chronic disease in 31% 82% required ventilation 100% required inotropic support Fluid resuscitation Crystalloids (0.9% or lactated Ringer s) Colloids: 5% albumin or blood products (RBC, FFP, cryoprecipitate)
14
15
16

17
18 Carcillo et al. Role of Early Fluid Resuscitation in Pediatric Septic Shock. JAMA 1991; 266 (9): Criticisms Treatment groups assigned non-randomly Treatment based on clinical criteria Criteria determined by different individuals But.findings suggested current PALS guidelines may improve survival in children with septic shock

19 Rivers et al. Early Goal-Directed Therapy in the Treatment of Severe Sepsis and Septic Shock. NEJM 2001; 345: To evaluate the efficacy of EGDT before admission to ICU Single center: Detroit Hospital Emergency Department 263 patients: severe sepsis or septic shock Randomly assigned 6 hours of standard versus EGT End points: MOF, mortality,
20
21
22 Rivers et al. Early Goal-Directed Therapy in the Treatment of Severe Sepsis and Septic Shock. NEJM 2001; 345: Results 263 patients 8.7% excluded or did not consent Similar baseline characteristics including adequacy and duration of antibiotic therapy Standard patients in ED 6.3 hours v 8 hours (p<0.001) No difference in HR or CVP MAP s significantly lower
23
24
25 Rivers et al. Early Goal-Directed Therapy in the Treatment of Severe Sepsis and Septic Shock. NEJM 2001; 345: Criticisms Single center Single physician Treatment group mortality similar across centers

26 Carcillo et al. Clinical practice parameters for haemodynamic support of paediatric and neonatal patients in septic shock. Critical Care Med 2002; 30:
27 St. Mary s Hospital, London Specialist Tertiary Referral Centre, 2002 High rates of meningococcal disease Consultant led retrieval service Telephone advice throughout the south of England Centralization of meningococcal disease care Early aggressive fluid resuscitation 4% Albumin
28 deoliveira et al. ACCM/PALS haemodynamic support guidelines for paediatric septic shock: an outcomes comparison with and without monitoring central venous saturation. Intensive Care Medicine 2008; 34: children with severe sepsis or fluid refractory septic shock Randomly assigned to ACCM/PALS with or without ScvO2 goal-directed resuscitation for 72 hours Control group ACCM/PALS therapies without continuous ScvO2 Fluid resuscitation (crystalloid or colloid), RBC or CVS drugs Maintain normal perfusion pressure for age, UO >1ml/kg/hour, CRT of 2 seconds and normal pulses Intervention group Endpoint of ScvO2 >70% using continuous monitoring If <70% then more fluid, RBC (if Hb<10g/l) or inotropes were given Other supportive therapies: CMV, nutrition, antibiotics and RRT decided by medical team
29 deoliveira et al. ACCM/PALS haemodynamic support guidelines for paediatric septic shock: an outcomes comparison with and without monitoring central venous saturation. Intensive Care Medicine 2008; 34: Intervention Group 28 day mortality (11.8% v 39.2%) More crystalloid (28 v 5mls/kg) RBC transfusion (45.1% v 15.7%) More inotropic support (29.4% v 7.8%) Fewer new organ dysfunctions Support of the current ACCM/PALS guidelines Goal-directed therapy using the endpoint of ScvO2 >70% provided a significant impact on the outcome of children
30 Guideline Update Brierly et al. Clinical practice parameters for haemodynamic support of pediatric and neonatal septic shock: 2007 update from the American College of Critical Care Medicine CCM 2009;37: Surviving Sepsis Campaign guidelines for the management of severe sepsis and septic shock. Critical Care Med (1):
31 Improved outcomes in paediatric septic shock Han et al. Early reversal of pediatric-neonatal septic shock by community physicians is associated with improved outcome. Pediatrics 2003; 112:793-9 Inwald et al. Emergency management of children with severe sepsis in the UK: the results of the Paediatric Intensive Care Society sepsis audit. Arch Disease in Childhood 2009;94:348-53
32
33 Background Early aggressive fluid resuscitation in patients with shock sub-saharan Africa Malaria, sepsis and other infectious disease High early mortality Fluid resuscitation not practiced unless severe anaemia WHO recommends fluid resuscitation in advanced shock only CRT > 3 seconds Weak and fast pulse Cold extremities
34 Aims FEAST trial designed to investigate the practice of: Early resuscitation with a saline bolus as compared with no bolus (control) With an albumin bolus as compared with a saline bolus
35 Study Design 2 stratum, multi-center, open, randomised controlled study January Age between 60 days and 12 years 6 clinical centers: 1 Kenya; 1 Tanzania; 4 Uganda Stratum A Children without severe hypotension Stratum B Children with severe hypotension SBP <50mmHg if <12 months; <60mmHg if 1-5 years; < 70mmHg >5 years
36 Study Design Stratum A Randomly assigned 1:1:1 Rapid volume expansion over 1 hour 20mls/kg (40ml/kg June 2010) % NaCl (saline-bolus group) 2. 5% HAS (albumin-bolus group) 3. none (control group) Additional 20ml/kg bolus at 1 hour if impaired perfusion (not in control group) Severe hypotension: 40ml/kg of study fluid (saline in control group) Stratum B Randomly assigned 1:1 Rapid volume expansion over 1 hour 40ml/kg (60ml/kg June 2010) % or (saline-bolus) 2. 5% HAS (albumin-bolus) Additional 20ml/kg bolus at 1 hour if impaired perfusion Severe hypotension: 40ml/kg of study fluid
37 Study Population Inclusions Age 60 days to 12 years Severe febrile illness complicated by Impaired consciousness Respiratory distress Impaired perfusion 1. CRT >3 seconds 2. Lower limb temperature gradient 3. Weak radial-pulse volume 4. Severe tachycardia Severe malnutrition Gastroenteritis Exclusions Non-infectious causes of shock 1. Trauma 2. Surgery 3. Burns Conditions for which volume expansion is contraindicated
38 End Points Primary End Point Mortality at 48 hours Secondary End Points Mortality at 4 weeks Neurologic sequelae at 4 & 24 weeks Episodes of hypotensive shock within 48 hours after randomisation Adverse events potentially related to fluid resuscitation Pulmonary oedema Increased ICP Severe allergic reaction
39 Study Procedures Treated on general paediatric ward Assisted ventilation bag-mask only Provided with monitors for saturations and blood pressure Training in triage & emergency paediatric life support Supportive management IV maintenance fluids (2.5 4ml/kg/hour) Antibiotics, anti-malarials, anti-pyretics, anticonvulsant drugs Treated for hypoglycaemia (<2.5mmol/L) RBC transfusion at 20ml/kg over 4 hours if Hb <5g/dl
40 Study Procedures Clinical case-report form completed at 1,4, 8, 24 and 48 hours Hypovolaemia, neurologic and cardiorespiratory status Adverse events were reported Neurological assessment at 4 weeks Reviewed by independent clinician Reassessed at 24 weeks if neurological sequelae present
41
42
43
44
45
46 Administered Fluids Adherence to protocol 99.5% in albumin group 99.4% in saline group 99.9% in control group Median volume of all fluids (including blood): Albumin Bolus Group: First hour: 20ml/kg; Second hour: 4.5ml/kg Saline Bolus Group: First hour: 20ml/kg; Second hour: 5ml/kg Control Group: First hour: 1.2ml/kg; Second hour: 2.9ml/kg
47 Fluid Administered Over course of 8 hours Median cumulative volume of fluid Albumin-bolus group: 40ml/kg (30-50) Saline-bolus group: 40ml/kg ( ) Control: 10.1 ml/kg ( ) RBC transfusion in 1408 children 45% in albumin; 47% in saline; 43% in control Initiated earlier in control group but proportions and volumes similar across all groups
48
49
50
51 Good Points Large numbers of children enrolled Multinational nature of sample Small numbers lost to follow up Blinding of treatment assignments High rate of adherence to assigned treatment Confirmed what we know about saline versus albumin
52 Limitations Setting Limited access to diagnostics Different pattern of disease e.g. cerebral malaria Exclusions: gastroenteritis, severe malnutrition or noninfectious causes of shock Few children recruited to stratum B Definitions of shock
53 Restricted Fluid Strategy Adult Literature ARDS Colorectal Surgery Penetrating Trauma
54 What type of fluid?
55 Types of IV Fluids Crystalloids Colloids Isotonic 0.9% Saline Plasma-Lyte Hartman s solution Lactated Ringer s Solution Hypertonic 3% Saline Natural 4% Albumin (iso-oncotic) 20% Albumn (hyper-oncotic) Synthetic Colloids Dextrans: 6% dextran 70; 10% dextran 40 Gelatins: Gelofusin, Haemaccel, gelofundiol HES preparations: Tetrastarch, Pentastarch, Voluven
56 Crystalloid versus Colloid Crystalloids Colloids Cheap Readily available Hyperchloraemia Expensive Anaphylaxis Coagulopathy Exposure to blood products Pruritis

57
58 Albumin Human albumin Natural colloid, MW 69kDa Accounts for 80% plasma oncotic pressure Drug & hormone transport Anti-oxidant and anti-inflammatory properties Hypoalbuminaemic critically ill patients have a worse prognosis Albumin solutions Safe, natural, well tolerated Iso-oncotic (4% or 5%) or hyper-oncotic (20-25%)
59 Levin et al. Improved survival in children admitted to intensive care with meningococcal disease. 2 nd Annual Spring Meeting of the RCPCH. University of York. 1998
60 The Colloid versus Crystalloid Debate Cochrane Injuries Group Albumin Reviewers Human albumin administration in critically ill patients: Systematic review of randomised controlled trials. BMJ 1998; 317: RCT including 1419 randomised patients Burns, hypoalbuminaemia or hypovolaemia 6% increased risk of death with albumin
61 Booy et al. Reduction in case fatality rate from meningococcal disease associated with improved healthcare delivery. Arch Dis Child 2001; 85: children with MD admitted to PICU Case fatality rate 23% (1992/93) to 2% (1997) A significant improvement in outcome for children admitted with MD to a PICU as a result of improvements in the use of their algorithm: 4% albumin boluses Initial management at referring hospitals Use of a mobile intensive care service Centralization of care in a specialist unit
62 Finfer et al. A Comparison of Albumin and Saline for Fluid Resuscitation in the ICU NEJM 2004; 350: The SAFE Study Multicenter, randomised, double-blind trial Primary outcome: death from any cause/28 days Eligible patients Anyone for whom fluid resuscitation required Exclusions: cardiac surgery, liver transplant, burns 4% albumin versus 0.9% saline
63 The SAFE Study 6997 patients Similar baseline characteristics Fluids Administered Albumin group: significantly less study fluid Saline: Albumin of 1: 1.4 Haemodynamics No differences in MAP Albumin group: lower HR & higher CVP
64 Total Fluids Administered Albumin Saline Ratio 2247ml 3096ml 1:1.4
65 The SAFE Study 28 day mortality 726 deaths (20.9%; albumin) v 729 deaths (21.1% saline) Single organ and multiple-organ failure similar No differences in ICU days, hospital days, days of mechanical ventilation, days of RRT
66 The SAFE Study Sub group analysis in severe sepsis Improved outcomes with albumin Saline group 35.3% died Albumin group 30.7% died RR of death 0.87 amongst those in the albumin group RR of death 1.05 without severe sepsis
67 Paediatric Albumin Trials Maitland et al. Randomized trial of volume expansion with albumin or saline in children with severe malaria: preliminary evidence of albumin benefit. Clin Infect Dis 2005; 40(4): Maitland et al. Mortality after fluid bolus in African children. NEJM Jun 30;364(26):
68 Current Trials The PRECISE Trial Evolution of an Early Septic Shock Fluid Resuscitation Trial Canadian Critical Care Trials Group. 5% albumin versus 0.9% NaCl on 90 day mortality ALBIOS Trial The Volume Replacement with Albumin in Severe Sepsis 1350 Italian ICU patients 28- and 90-day mortality; organ dysfunction (secondary end-point) Albumin plus crystalloid versus crystalloid only
69 Surviving Sepsis Campaign guidelines for the management of severe sepsis and septic shock. Critical Care Med (1): Dellinger et al. Surviving Sepsis Campaign: International guidelines for management of severe sepsis and septic shock: Intensive Care Med 2008; 34:17-60 Recommends the use of either crystalloid or colloid for the early resuscitation of patients with sepsis
70 Gelatins Synthetic colloid Hydrosylates of connective tissue of animal origin MW limited to kda Tendency to gel at higher molecular weights Much lower than albumin Limited oncotic effects; intravascular persistence 2-3 hours
71 Gelatins Upadhyay et al. Randomized evaluation of fluid resuscitation with crystalloid (saline) and colloid (polymer from degraded gelatin in saline) in pediatric septic shock. Indian Pediatr 2005; 42(3): children with septic shock 20ml/kg boluses of saline or gelatin Equally effective as a resuscitation fluid
72 Gelatin Acute Kidney Injury Schabinski et al. Effects of a predominantly HES based and a predominantly non HES based fluid therapy on renal function in surgical ICU patients. Intensive Care Medicine 2009; 35: % HES 130/0.4 versus gelatin Gelatin exposure independent RF for ARF (OR 1.99) Anaphylactoid reactions reported
73 Hydroxyethyl Starch Commonest colloid used in European ICU s HES 58%; gelatin 35%; albumin 5% Synthesised by partial hydrolysis of maize or potato starch, amylopectin 4 Elements Concentration: 6% or 10% Molecular weight: kDa Degree of substitution: 0.4 (tetrastarch), 0.7 (hetastarch) C2/C6 ratio 3 Generations
74 HES & Bleeding Cardiac surgery RCT s HES 120/0.7, 130/0.4, 200/0.5, 450/0.7 impaired TEG assessed clotting compared with albumin Blood loss increased with HES 130/0.4 and 450/0.7 (greater blood transfusion) compared with albumin General paediatric surgery patients HES 130/0.4 caused deterioration in TEG parameters in a RCT compared with albumin
75 Acute Kidney Injury Schortgen et al. Effects of hydroxyethylstarch and gelatin on renal function in severe sepsis: a multicentre randomised study. Lancet 2001;357: French patients with severe sepsis 6% HES 200/0.6 increased risk of RF by 2.57 compared with gelatin Brunkhorst et al. Intensive insulin therapy and pentastarch resuscitation in severe sepsis. NEJM 2008:358: % HES, 200kDa versus Ringer s lactate Higher incidence of renal failure and RRT
76 Acute Kidney Injury Consensus statement of the ESICM task force on colloid volume therapy in critically ill patients. Intensive Care Medicine 2012; 38(3):368 Recommend against using HES>200kDa and/or degree of substitution of 0.4 in patients with severe sepsis or risk of AKI Suggest not using 6% HES 130/0.4 in these populations
77 Anaphylactoid Reaction Wills et al. Comparison of three fluid solutions for resuscitation in dengue shock syndrome. NEJM 2005:353: RCT of 383 children Severe allergic reactions more frequent after Dextran 70>HES 200/0.5>Ringer s lactate Case reports described in patients exposed to gelatins, HES and albumin
78 Pruritis Bork et al. Pruritus precipitated by hydroxyethyl starch: a review. Br J Dematol. 2005; 152:3-12 Systematic review of 18 clinical studies; 3239 patients All HES solutions of all molecular weights, substitutions and C2/C6 ratios Incidence 13-34% in ICU 22% in cardiac surgery 3-54% in stroke
79 Current Trials The CHEST Trial Crystalloid Versus Hydroxyethyl Starch Trial 7000 ANZ ICU patients HES 130/0.4 versus saline 90 day mortality; need for RRT (secondary end-point) The Scandinavian Starch for Severe Sepsis/Septic Shock Trial 800 ICU patients HES 130/0.4 or Ringer s acetate Mortality or dialysis dependence at 90 days after infusion

80 Time to put it all together
81 Summary When should fluid be given: Fluid should be given in a time-sensitive manner How much fluid to give Directed toward the goal of improved stroke volume as evidenced by return of HR to normal, CRT <2 second, peripheral pulses and BP as well as correction of Hb and ScvO2>70% Crystalloid or albumin? Probably doesn t matter No place for HES, gelatins or dextrans in paediatric septic shock
Fluid Treatments in Sepsis: Meta-Analyses
 Fluid Treatments in Sepsis: Recent Trials and Meta-Analyses Lauralyn McIntyre MD, FRCP(C), MSc Scientist, Ottawa Hospital Research Institute Assistant Professor, University of Ottawa Department of Epidemiology
Fluid Treatments in Sepsis: Recent Trials and Meta-Analyses Lauralyn McIntyre MD, FRCP(C), MSc Scientist, Ottawa Hospital Research Institute Assistant Professor, University of Ottawa Department of Epidemiology
IV fluid administration in sepsis. Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London
 IV fluid administration in sepsis Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London The talk What is septic shock? What are the recommendations? What is the evidence? Do we follow
IV fluid administration in sepsis Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London The talk What is septic shock? What are the recommendations? What is the evidence? Do we follow
Evidence- Based Medicine Fluid Therapy
 Evidence- Based Medicine Fluid Therapy Ndidi Musa M.D. Assosciate Professor of Pediatrics Medical College of Wisconsin/ Children s Hospital of Wisconsin Disclosures A. I have no relevant financial relationships
Evidence- Based Medicine Fluid Therapy Ndidi Musa M.D. Assosciate Professor of Pediatrics Medical College of Wisconsin/ Children s Hospital of Wisconsin Disclosures A. I have no relevant financial relationships
Respiratory problems with severe malaria: an opportunity to talk about fluid trials!!! Kathryn Maitland
 Respiratory problems with severe malaria: an opportunity to talk about fluid trials!!! Kathryn Maitland Severe malaria-the numbers Up to 1 million deaths in African children
Respiratory problems with severe malaria: an opportunity to talk about fluid trials!!! Kathryn Maitland Severe malaria-the numbers Up to 1 million deaths in African children
towards early goal directed therapy
 Paediatric Septic Shock- towards early goal directed therapy Elliot Long Paediatric Acute Care 2011 Conference Outline Emergency Department Rivers Protocol (EGDT) ACCM Sepsis Protocol Evidence Barriers
Paediatric Septic Shock- towards early goal directed therapy Elliot Long Paediatric Acute Care 2011 Conference Outline Emergency Department Rivers Protocol (EGDT) ACCM Sepsis Protocol Evidence Barriers
Staging Sepsis for the Emergency Department: Physician
 Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Staging Sepsis for the Emergency Department: Physician Sepsis Continuum 1 Sepsis Continuum SIRS = 2 or more clinical criteria, resulting in Systemic Inflammatory Response Syndrome Sepsis = SIRS + proven/suspected
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE
 Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Managing Patients with Sepsis
 Managing Patients with Sepsis Diagnosis; Initial Resuscitation; ARRT Initiation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum
Managing Patients with Sepsis Diagnosis; Initial Resuscitation; ARRT Initiation Prof. Achim Jörres, M.D. Dept. of Nephrology and Medical Intensive Care Charité University Hospital Campus Virchow Klinikum
What is the Role of Albumin in Sepsis? An Evidenced Based Affair. Justin Belsky MD PGY3 2/6/14
 What is the Role of Albumin in Sepsis? An Evidenced Based Affair Justin Belsky MD PGY3 2/6/14 Microcirculation https://www.youtube.com/watch?v=xao1gsyur7q Capillary Leak in Sepsis Asking the RIGHT Question
What is the Role of Albumin in Sepsis? An Evidenced Based Affair Justin Belsky MD PGY3 2/6/14 Microcirculation https://www.youtube.com/watch?v=xao1gsyur7q Capillary Leak in Sepsis Asking the RIGHT Question
Sepsis overview. Dr. Tsang Hin Hung MBBS FHKCP FRCP
 Sepsis overview Dr. Tsang Hin Hung MBBS FHKCP FRCP Epidemiology Sepsis, severe sepsis, septic shock Pathophysiology of sepsis Recent researches and advances From bench to bedside Sepsis bundle Severe sepsis
Sepsis overview Dr. Tsang Hin Hung MBBS FHKCP FRCP Epidemiology Sepsis, severe sepsis, septic shock Pathophysiology of sepsis Recent researches and advances From bench to bedside Sepsis bundle Severe sepsis
Fluid resuscitation in specific patient populations: sepsis and traumatic brain injury
 Fluid resuscitation in specific patient populations: sepsis and traumatic brain injury John A Myburgh MBBCh PhD FCICM UNSW Professor of Critical Care Medicine The George Institute for Global Health University
Fluid resuscitation in specific patient populations: sepsis and traumatic brain injury John A Myburgh MBBCh PhD FCICM UNSW Professor of Critical Care Medicine The George Institute for Global Health University
Modern fluid therapy. Anders Perner. Dept of Intensive Care, Rigshospitalet, University of Copenhagen
 Modern fluid therapy Anders Perner Dept of Intensive Care, Rigshospitalet, University of Copenhagen Scandinavian Critical Care Trials Group www.ssai.info/research/scctg Intensive Care Medicine www.icmjournal.esicm.org
Modern fluid therapy Anders Perner Dept of Intensive Care, Rigshospitalet, University of Copenhagen Scandinavian Critical Care Trials Group www.ssai.info/research/scctg Intensive Care Medicine www.icmjournal.esicm.org
Sepsis Management: Past, Present, and Future
 Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Evidence-Based. Management of Severe Sepsis. What is the BP Target?
 Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Update in Critical Care Medicine
 Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Claire Fraser P.Ramnarayan Author Position tanp CATS Consultant Document Owner E. Polke Document
John Park, MD Assistant Professor of Medicine
 John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
Dr. Nai Shun Tsoi Department of Paediatric and Adolescent Medicine Queen Mary Hospital Hong Kong SAR
 Dr. Nai Shun Tsoi Department of Paediatric and Adolescent Medicine Queen Mary Hospital Hong Kong SAR A very important aspect in paediatric intensive care and deserve more attention Basic principle is to
Dr. Nai Shun Tsoi Department of Paediatric and Adolescent Medicine Queen Mary Hospital Hong Kong SAR A very important aspect in paediatric intensive care and deserve more attention Basic principle is to
Presented by: Indah Dwi Pratiwi
 Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
INTENSIVE CARE MEDICINE CPD EVENING. Dr Alastair Morgan Wednesday 13 th September 2017
 INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
INTENSIVE CARE MEDICINE CPD EVENING Dr Alastair Morgan Wednesday 13 th September 2017 WHAT IS NEW IN ICU? (RELEVANT TO ANAESTHETISTS) Not much! SURVIVING SEPSIS How many deaths in England were thought
Fluids and Lactate. A/Prof Peter Morley
 Fluids and Lactate A/Prof Peter Morley RCTs Other evidence 5 6 Plan Background information Crystalloids Which crystalloid? Colloids Crystalloids v colloids Once that s settled, how much fluid Plan Background
Fluids and Lactate A/Prof Peter Morley RCTs Other evidence 5 6 Plan Background information Crystalloids Which crystalloid? Colloids Crystalloids v colloids Once that s settled, how much fluid Plan Background
Sepsis Management Update 2014
 Sepsis Management Update 2014 Laura J. Moore, MD, FACS Associate Professor, Department of Surgery The University of Texas Health Science Center, Houston Medical Director, Shock Trauma ICU Texas Trauma
Sepsis Management Update 2014 Laura J. Moore, MD, FACS Associate Professor, Department of Surgery The University of Texas Health Science Center, Houston Medical Director, Shock Trauma ICU Texas Trauma
Objectives. Management of Septic Shock. Definitions Progression of sepsis. Epidemiology of severe sepsis. Major goals of therapy
 Objectives Management of Septic Shock Review of the Evidence and Implementation of Pediatric Guidelines at Christus Santa Rosa Manish Desai, M.D. PL 5 2 nd year Pediatric Critical Care Fellow Review of
Objectives Management of Septic Shock Review of the Evidence and Implementation of Pediatric Guidelines at Christus Santa Rosa Manish Desai, M.D. PL 5 2 nd year Pediatric Critical Care Fellow Review of
3/14/2017. Pediatric Sepsis: From Goal Directed Therapy to Protocolized Care. Objectives. Developmental Response to Sepsis
 Pediatric Sepsis: From Goal Directed Therapy to Protocolized Care March 20, 2017 Reid WD Farris, MS MD Objectives Review the evolution & current state of the pediatric septic shock treatment guidelines
Pediatric Sepsis: From Goal Directed Therapy to Protocolized Care March 20, 2017 Reid WD Farris, MS MD Objectives Review the evolution & current state of the pediatric septic shock treatment guidelines
Fluids in Sepsis Less is more. Dr Anand Senthi Joondalup Health Campus ED MBBS, MAppFin, GradCertPubHlth,
 Fluids in Sepsis Less is more Dr Anand Senthi Joondalup Health Campus ED MBBS, MAppFin, GradCertPubHlth, FRACGP @drsenthi Summary Discussion of the evidence for/against fluid resuscitation in septic shock
Fluids in Sepsis Less is more Dr Anand Senthi Joondalup Health Campus ED MBBS, MAppFin, GradCertPubHlth, FRACGP @drsenthi Summary Discussion of the evidence for/against fluid resuscitation in septic shock
Early Goal Directed Therapy in 2015: What Did the Big Trials Teach us?
 Early Goal Directed Therapy in 2015: What Did the Big Trials Teach us? Mitchell M. Levy MD, FCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care Warren Alpert Medical School
Early Goal Directed Therapy in 2015: What Did the Big Trials Teach us? Mitchell M. Levy MD, FCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care Warren Alpert Medical School
INTRAVENOUS FLUID THERAPY. Tom Heaps Consultant Acute Physician
 INTRAVENOUS FLUID THERAPY Tom Heaps Consultant Acute Physician LEARNING OBJECTIVES 1. Crystalloids vs colloids 2. Balanced vs non-balanced solutions 3. Composition of various IV fluids 4. What is normal
INTRAVENOUS FLUID THERAPY Tom Heaps Consultant Acute Physician LEARNING OBJECTIVES 1. Crystalloids vs colloids 2. Balanced vs non-balanced solutions 3. Composition of various IV fluids 4. What is normal
Albumina nel paziente critico. Savona 18 aprile 2007
 Albumina nel paziente critico Savona 18 aprile 2007 What Is Unique About Critical Care RCTs patients eligibility is primarily defined by location of care in the ICU rather than by the presence of a specific
Albumina nel paziente critico Savona 18 aprile 2007 What Is Unique About Critical Care RCTs patients eligibility is primarily defined by location of care in the ICU rather than by the presence of a specific
HYPOVOLEMIA AND HEMORRHAGE UPDATE ON VOLUME RESUSCITATION HEMORRHAGE AND HYPOVOLEMIA DISTRIBUTION OF BODY FLUIDS 11/7/2015
 UPDATE ON VOLUME RESUSCITATION HYPOVOLEMIA AND HEMORRHAGE HUMAN CIRCULATORY SYSTEM OPERATES WITH A SMALL VOLUME AND A VERY EFFICIENT VOLUME RESPONSIVE PUMP. HOWEVER THIS PUMP FAILS QUICKLY WITH VOLUME
UPDATE ON VOLUME RESUSCITATION HYPOVOLEMIA AND HEMORRHAGE HUMAN CIRCULATORY SYSTEM OPERATES WITH A SMALL VOLUME AND A VERY EFFICIENT VOLUME RESPONSIVE PUMP. HOWEVER THIS PUMP FAILS QUICKLY WITH VOLUME
Fluids in ICU. JMO teaching 5th July 2016
 Fluids in ICU JMO teaching 5th July 2016 Objectives Physiology of fluid infusion History of fluid resuscitation Physiology of fluid resuscitation Types of resuscitation fluid The ideal resuscitation fluid
Fluids in ICU JMO teaching 5th July 2016 Objectives Physiology of fluid infusion History of fluid resuscitation Physiology of fluid resuscitation Types of resuscitation fluid The ideal resuscitation fluid
Nothing to disclose 9/25/2017
 Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Nothing to disclose 1 Explain
Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Nothing to disclose 1 Explain
Albumin: rationale, use and evidence
 Albumin: rationale, use and evidence Michaël Chassé, MD, MSc, FRCPC Intensivist, CHU de Québec PhD Candidate, Epidemiology, uottawa Research Fellow, Clinical Epidemiology Program Ottawa Hospital Research
Albumin: rationale, use and evidence Michaël Chassé, MD, MSc, FRCPC Intensivist, CHU de Québec PhD Candidate, Epidemiology, uottawa Research Fellow, Clinical Epidemiology Program Ottawa Hospital Research
9/25/2017. Nothing to disclose
 Nothing to disclose Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Explain
Nothing to disclose Jessie O Neal, PharmD, BCCCP Critical Care Clinical Pharmacist University of New Mexico Hospital New Mexico Society of Health-System Pharmacists 2017 Balloon Fiesta Symposium Explain
Early-goal-directed therapy and protocolised treatment in septic shock
 CAT reviews Early-goal-directed therapy and protocolised treatment in septic shock Journal of the Intensive Care Society 2015, Vol. 16(2) 164 168! The Intensive Care Society 2014 Reprints and permissions:
CAT reviews Early-goal-directed therapy and protocolised treatment in septic shock Journal of the Intensive Care Society 2015, Vol. 16(2) 164 168! The Intensive Care Society 2014 Reprints and permissions:
Shock and hemodynamic monitorization. Nilüfer Yalındağ Öztürk Marmara University Pendik Research and Training Hospital
 Shock and hemodynamic monitorization Nilüfer Yalındağ Öztürk Marmara University Pendik Research and Training Hospital Shock Leading cause of morbidity and mortality Worldwide: dehydration and hypovolemic
Shock and hemodynamic monitorization Nilüfer Yalındağ Öztürk Marmara University Pendik Research and Training Hospital Shock Leading cause of morbidity and mortality Worldwide: dehydration and hypovolemic
Resuscitation fluids in critical care
 Resuscitation fluids in critical care John A Myburgh MBBCh PhD FCICM UNSW Professor of Critical Care Medicine The George Institute for Global Health University of New South Wales St George Hospitals, Sydney
Resuscitation fluids in critical care John A Myburgh MBBCh PhD FCICM UNSW Professor of Critical Care Medicine The George Institute for Global Health University of New South Wales St George Hospitals, Sydney
The Septic Patient. Dr Arunraj Navaratnarajah. Renal SpR Imperial College NHS Healthcare Trust
 The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
Sepsis: Identification and Management in an Acute Care Setting
 Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
What is the right fluid to use?
 What is the right fluid to use? L McIntyre Associate Professor, University of Ottawa Senior Scientist, Ottawa Hospital Research Institute Centre for Transfusion Research CCCF, November 2, 2016 Disclosures
What is the right fluid to use? L McIntyre Associate Professor, University of Ottawa Senior Scientist, Ottawa Hospital Research Institute Centre for Transfusion Research CCCF, November 2, 2016 Disclosures
Fluid balance and clinically relevant outcomes
 Fluid balance and clinically relevant outcomes Rui Moreno, MD, PhD, Professor UCINC, Hospital de São José Centro Hospitalar de Lisboa Central, E.P.E. INSULT PRIMARY MODS SIRS SECONDARY MODS OUTCOME RECOVERY
Fluid balance and clinically relevant outcomes Rui Moreno, MD, PhD, Professor UCINC, Hospital de São José Centro Hospitalar de Lisboa Central, E.P.E. INSULT PRIMARY MODS SIRS SECONDARY MODS OUTCOME RECOVERY
JOURNAL CLUB: THE FLUIDS DEBATE. Veronica Ueckermann
 JOURNAL CLUB: THE FLUIDS DEBATE Veronica Ueckermann INTRODUCTION The selection and use of resuscitation fluids should be based on physiological principles. However, historically, clinical practice has
JOURNAL CLUB: THE FLUIDS DEBATE Veronica Ueckermann INTRODUCTION The selection and use of resuscitation fluids should be based on physiological principles. However, historically, clinical practice has
BREAK 11:10-11:
 1. Sepsis Tom Heaps 09:30-10:20 2. Oncological Emergencies Clare Pollard 10:20-11:10 ------------------------ BREAK 11:10-11:30 ------------------------ 3. Diabetic Ketoacidosis Tom Heaps 11:30-12:20 4.
1. Sepsis Tom Heaps 09:30-10:20 2. Oncological Emergencies Clare Pollard 10:20-11:10 ------------------------ BREAK 11:10-11:30 ------------------------ 3. Diabetic Ketoacidosis Tom Heaps 11:30-12:20 4.
Date written: April 2014 Review date: April 2016 Related documents: Paediatric Sepsis 6
 Scottish Paediatric Retrieval Service (Edinburgh) www.paedsretrieval.com Clinical Guideline SEPSIS Date written: April 2014 Review date: April 2016 Related documents: Paediatric Sepsis 6 Author: Steve
Scottish Paediatric Retrieval Service (Edinburgh) www.paedsretrieval.com Clinical Guideline SEPSIS Date written: April 2014 Review date: April 2016 Related documents: Paediatric Sepsis 6 Author: Steve
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Shruti Dholakia L Chigaru Author Position Fellow CATS Consultant Document Owner E. Polke Document
Children s Acute Transport Service Clinical Guidelines Septic Shock Document Control Information Author Shruti Dholakia L Chigaru Author Position Fellow CATS Consultant Document Owner E. Polke Document
Sepsis Update: Focus on Early Recognition and Intervention. Disclosures
 Sepsis Update: Focus on Early Recognition and Intervention Jessie Roske, MD October 2017 Disclosures I have no actual or potential conflict of interest in relation to this program/presentation. I will
Sepsis Update: Focus on Early Recognition and Intervention Jessie Roske, MD October 2017 Disclosures I have no actual or potential conflict of interest in relation to this program/presentation. I will
Year in Review 2014: Critical Care Medicine
 Disclosures Year in Review 2014: Critical Care Medicine I receive laboratory support from CytoVale Diagnostics for research on early sepsis diagnostics Eric J. Seeley, M.D., F.C.C.P. Assistant Professor
Disclosures Year in Review 2014: Critical Care Medicine I receive laboratory support from CytoVale Diagnostics for research on early sepsis diagnostics Eric J. Seeley, M.D., F.C.C.P. Assistant Professor
Sepsis Story At Intermountain Healthcare Intensive Medicine Clinical Program
 Sepsis Story At Intermountain Healthcare 2004-2012 Intensive Medicine Clinical Program The International Surviving Sepsis Campaign Was Organized In 2002 During The ESICM International Meeting In Barcelona,
Sepsis Story At Intermountain Healthcare 2004-2012 Intensive Medicine Clinical Program The International Surviving Sepsis Campaign Was Organized In 2002 During The ESICM International Meeting In Barcelona,
Comment on infusion solutions containing HES
 Comment on infusion solutions containing HES The European Medicines Agency (EMA) published on 14 June 2013 Pharmacovigilance Risk Assessment Committee (PRAC) recommends suspending marketing authorisations
Comment on infusion solutions containing HES The European Medicines Agency (EMA) published on 14 June 2013 Pharmacovigilance Risk Assessment Committee (PRAC) recommends suspending marketing authorisations
Objectives. Epidemiology of Sepsis. Review Guidelines for Resuscitation. Tx: EGDT, timing/choice of abx, activated
 Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
Advancements in Sepsis
 Objectives Advancements in Sepsis Brian Gilbert, PharmD PGY-1 Pharmacy Resident Jackson Memorial Hospital 3/13/2016 www.fshp.org Pharmacist objectives Review recent updates in resuscitation strategies
Objectives Advancements in Sepsis Brian Gilbert, PharmD PGY-1 Pharmacy Resident Jackson Memorial Hospital 3/13/2016 www.fshp.org Pharmacist objectives Review recent updates in resuscitation strategies
Current issues in Volume therapy
 CCM Inter-Hospital Grand Round Hong Kong, May 22, 2012 Current issues in Volume therapy Dr. Hrishikesh Kulkarni Medical Director Fresenius Kabi Asia Pacific, Hong Kong Controversies in Intravenous fluids
CCM Inter-Hospital Grand Round Hong Kong, May 22, 2012 Current issues in Volume therapy Dr. Hrishikesh Kulkarni Medical Director Fresenius Kabi Asia Pacific, Hong Kong Controversies in Intravenous fluids
Early Goal-Directed Therapy
 Early Goal-Directed Therapy Where do we stand? Jean-Daniel Chiche, MD PhD MICU & Dept of Host-Pathogen Interaction Hôpital Cochin & Institut Cochin, Paris-F Resuscitation targets in septic shock 1 The
Early Goal-Directed Therapy Where do we stand? Jean-Daniel Chiche, MD PhD MICU & Dept of Host-Pathogen Interaction Hôpital Cochin & Institut Cochin, Paris-F Resuscitation targets in septic shock 1 The
2016 Sepsis Update: Pearls, Pitfalls, and Core Measure Quicksand
 2016 Sepsis Update: Pearls, Pitfalls, and Core Measure Quicksand Jack Perkins, MD FACEP, FAAEM, FACP Assistant Professor of Emergency and Internal Medicine Virginia Tech Carilion School of Medicine Why
2016 Sepsis Update: Pearls, Pitfalls, and Core Measure Quicksand Jack Perkins, MD FACEP, FAAEM, FACP Assistant Professor of Emergency and Internal Medicine Virginia Tech Carilion School of Medicine Why
SHOCK. Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital
 SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
Surviving Sepsis Campaign. Guidelines for Management of Severe Sepsis/Septic Shock. An Overview
 Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
R2R: Severe sepsis/septic shock. Surat Tongyoo Critical care medicine Siriraj Hospital
 R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
R2R: Severe sepsis/septic shock Surat Tongyoo Critical care medicine Siriraj Hospital Diagnostic criteria ACCP/SCCM consensus conference 1991 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
Maria B. ALBUJA-CRUZ, MD ALBUMIN: OVERRATED. Surgical Grand Rounds
 Maria B. ALBUJA-CRUZ, MD ALBUMIN: OVERRATED Surgical Grand Rounds ALBUMIN Most abundant plasma protein 1/3 intravascular 50% of interstitial SKIN Synthesized in hepatocytes Transcapillary escape rate COP
Maria B. ALBUJA-CRUZ, MD ALBUMIN: OVERRATED Surgical Grand Rounds ALBUMIN Most abundant plasma protein 1/3 intravascular 50% of interstitial SKIN Synthesized in hepatocytes Transcapillary escape rate COP
How and why I give IV fluid Disclosures SCA Fluids and public health 4/1/15. Andrew Shaw MB FRCA FCCM FFICM
 How and why I give IV fluid Andrew Shaw MB FRCA FCCM FFICM Professor and Chief Cardiothoracic Anesthesiology Vanderbilt University Medical Center 2015 Disclosures Consultant for Grifols manufacturer of
How and why I give IV fluid Andrew Shaw MB FRCA FCCM FFICM Professor and Chief Cardiothoracic Anesthesiology Vanderbilt University Medical Center 2015 Disclosures Consultant for Grifols manufacturer of
Kristan Staudenmayer, MD Stanford University, Stanford, CA
 Kristan Staudenmayer, MD Stanford University, Stanford, CA Fluid resuscitation Variety of fluids How to administer What you do DOES matter WWII 1942 North Africa high mortality from hemorrhaghic shock
Kristan Staudenmayer, MD Stanford University, Stanford, CA Fluid resuscitation Variety of fluids How to administer What you do DOES matter WWII 1942 North Africa high mortality from hemorrhaghic shock
The ABC of CAB- Circulation, Airway, Breathing: PALS/Resuscitation Update
 The ABC of CAB- Circulation, Airway, Breathing: PALS/Resuscitation Update Jennifer K. Lee, MD Johns Hopkins University Dept. of Anesthesia, Division of Pediatric Anesthesia Disclosures I have research
The ABC of CAB- Circulation, Airway, Breathing: PALS/Resuscitation Update Jennifer K. Lee, MD Johns Hopkins University Dept. of Anesthesia, Division of Pediatric Anesthesia Disclosures I have research
Hydroxyethyl starch and bleeding
 Hydroxyethyl starch and bleeding Anders Perner Dept. of Intensive Care, Rigshospitalet University of Copenhagen Scandinavian Critical Care Trials Group Intensive Care Medicine COIs Ferring, LFB - Honoraria
Hydroxyethyl starch and bleeding Anders Perner Dept. of Intensive Care, Rigshospitalet University of Copenhagen Scandinavian Critical Care Trials Group Intensive Care Medicine COIs Ferring, LFB - Honoraria
Chapter 3 MAKING THE DECISION TO TRANSFUSE
 Chapter 3 MAKING THE DECISION TO TRANSFUSE PRACTICE POINTS Determine the best treatment for the patient which may include transfusion. Treat the cause of cytopenia (anaemia or thrombocytopenia) or plasma
Chapter 3 MAKING THE DECISION TO TRANSFUSE PRACTICE POINTS Determine the best treatment for the patient which may include transfusion. Treat the cause of cytopenia (anaemia or thrombocytopenia) or plasma
Out Line OF Lecture. Dr S Manimala Rao
 CHOICE OF FLUID, IMPACT ON RENAL FUNCTION Dr. MANIMALA RAO HOD CRITICAL CARE MEDICINE YASHODA HOSPITALS FORMERLY DEAN AND HOD ANAESTHESIOLOGY AND CRITICAL CARE NIMS HYDERABAD Out Line OF Lecture Basics
CHOICE OF FLUID, IMPACT ON RENAL FUNCTION Dr. MANIMALA RAO HOD CRITICAL CARE MEDICINE YASHODA HOSPITALS FORMERLY DEAN AND HOD ANAESTHESIOLOGY AND CRITICAL CARE NIMS HYDERABAD Out Line OF Lecture Basics
VI.2 ELEMENTS FOR A PUBLIC SUMMARY (VOLUVEN 10%)
") VI.2 ELEMENTS FOR A PUBLIC SUMMARY (VOLUVEN 10%) VI.2.1 OVERVIEW OF DISEASE EPIDEMIOLOGY Hypovolaemia is a state of decreased or reduced circulating blood volume which can be caused by a number of medical
VI.2 ELEMENTS FOR A PUBLIC SUMMARY (VOLUVEN 10%) VI.2.1 OVERVIEW OF DISEASE EPIDEMIOLOGY Hypovolaemia is a state of decreased or reduced circulating blood volume which can be caused by a number of medical
Early goal-directed therapy Where to from here? Rinaldo Bellomo ANZIC Research Centre Melbourne, Australia
 Early goal-directed therapy Where to from here? Rinaldo Bellomo ANZIC Research Centre Melbourne, Australia Early goal-directed therapy in septic shock 2001 Proof-of-concept EGDT trial published NEJM 16%
Early goal-directed therapy Where to from here? Rinaldo Bellomo ANZIC Research Centre Melbourne, Australia Early goal-directed therapy in septic shock 2001 Proof-of-concept EGDT trial published NEJM 16%
SEPSIS SYNDROME
 INTRODUCTION Sepsis has been defined as a life threatening condition that arises when the body s response to an infection injures its own tissues and organs. Sepsis may lead to shock, multiple organ failure
INTRODUCTION Sepsis has been defined as a life threatening condition that arises when the body s response to an infection injures its own tissues and organs. Sepsis may lead to shock, multiple organ failure
IV Fluids. I.V. Fluid Osmolarity Composition 0.9% NaCL (Normal Saline Solution, NSS) Uses/Clinical Considerations
 Uses/Clinical Considerations") IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
Sepsis is an important issue. Clinician s decision-making capability. Guideline recommendations
 Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock: 2012 Clinicians decision-making capability Guideline recommendations Sepsis is an important issue 8.7%
I Suggest Abnormal Saline
 I Suggest Abnormal Saline Sean M Bagshaw, MD, MSc Division of Critical Care Medicine University of Alberta CCCF Oct 27, 2015 2015 Disclosures Salary support: Canada/Alberta government Grant support: Canada/Alberta
I Suggest Abnormal Saline Sean M Bagshaw, MD, MSc Division of Critical Care Medicine University of Alberta CCCF Oct 27, 2015 2015 Disclosures Salary support: Canada/Alberta government Grant support: Canada/Alberta
Getting smart with fluids in the critically ill. NOR AZIM MOHD YUNOS Jeffrey Cheah School of Medicine & Health Sciences Monash University Malaysia
 Getting smart with fluids in the critically ill NOR AZIM MOHD YUNOS Jeffrey Cheah School of Medicine & Health Sciences Monash University Malaysia Isotonic Solutions and Major Adverse Renal Events Trial
Getting smart with fluids in the critically ill NOR AZIM MOHD YUNOS Jeffrey Cheah School of Medicine & Health Sciences Monash University Malaysia Isotonic Solutions and Major Adverse Renal Events Trial
Approach to Severe Sepsis. Jan Hau Lee, MBBS, MRCPCH. MCI Children s Intensive Care Unit KK Women s and Children's Hospital, Singapore
 Approach to Severe Sepsis Jan Hau Lee, MBBS, MRCPCH. MCI Children s Intensive Care Unit KK Women s and Children's Hospital, Singapore 1 2 No conflict of interest Overview Epidemiology of Pediatric Severe
Approach to Severe Sepsis Jan Hau Lee, MBBS, MRCPCH. MCI Children s Intensive Care Unit KK Women s and Children's Hospital, Singapore 1 2 No conflict of interest Overview Epidemiology of Pediatric Severe
Surgical Resuscitation Management in Poly-Trauma Patients
 Surgical Resuscitation Management in Poly-Trauma Patients Andrew Bernard, MD FACS Paul Kearney MD Chair of Trauma Surgery Associate Professor Medical Director of Trauma and Acute Care Surgery UK Healthcare
Surgical Resuscitation Management in Poly-Trauma Patients Andrew Bernard, MD FACS Paul Kearney MD Chair of Trauma Surgery Associate Professor Medical Director of Trauma and Acute Care Surgery UK Healthcare
Fluid assessment, monitoring and therapy for the acute nurse
 Fluid assessment, monitoring and therapy for the acute nurse Kelly Wright Lead Nurse for AKI King s College Hospital Aims and objectives Aims and objectives Why do we worry about volume assessment? Completing
Fluid assessment, monitoring and therapy for the acute nurse Kelly Wright Lead Nurse for AKI King s College Hospital Aims and objectives Aims and objectives Why do we worry about volume assessment? Completing
Fluid Resuscitation and Monitoring in Sepsis. Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS
 Fluid Resuscitation and Monitoring in Sepsis Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS Learning Objectives Compare and contrast fluid resuscitation strategies in septic shock Discuss available
Fluid Resuscitation and Monitoring in Sepsis Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS Learning Objectives Compare and contrast fluid resuscitation strategies in septic shock Discuss available
Reverse (fluid) resuscitation Should we be doing it? NAHLA IRTIZA ISMAIL
 resuscitation Should we be doing it? NAHLA IRTIZA ISMAIL") Reverse (fluid) resuscitation Should we be doing it? NAHLA IRTIZA ISMAIL 65 Male, 60 kg D1 in ICU Admitted from OT intubated Diagnosis : septic shock secondary to necrotising fasciitis of the R lower limb
Reverse (fluid) resuscitation Should we be doing it? NAHLA IRTIZA ISMAIL 65 Male, 60 kg D1 in ICU Admitted from OT intubated Diagnosis : septic shock secondary to necrotising fasciitis of the R lower limb
Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI)
") Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI) Robert W. Schrier, MD University of Colorado School of Medicine Denver, Colorado USA Prevalence of acute renal failure in Intensive
Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI) Robert W. Schrier, MD University of Colorado School of Medicine Denver, Colorado USA Prevalence of acute renal failure in Intensive
Critical Care Treatment Guidelines
 Critical Care Treatment Guidelines West Virginia Office of Emergency Medical Services CCT Guidelines CCT Guidelines TABLE OF CONTENTS Preface Acknowledgments Using the Guidelines INITIAL TREATMENT / UNIVERSAL
Critical Care Treatment Guidelines West Virginia Office of Emergency Medical Services CCT Guidelines CCT Guidelines TABLE OF CONTENTS Preface Acknowledgments Using the Guidelines INITIAL TREATMENT / UNIVERSAL
SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP
 SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP OBJECTIVES Arise, ProMISE, ProCESS Key points in sepsis management The CMS sepsis core measure COST OF SEPSIS CARE IN US Most
SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP OBJECTIVES Arise, ProMISE, ProCESS Key points in sepsis management The CMS sepsis core measure COST OF SEPSIS CARE IN US Most
Sepsis. From EMS to ER to ICU. What we need to be doing
 Sepsis From EMS to ER to ICU What we need to be doing NEHAL BHATT, MD ATHENS PULMONARY, CRITICAL CARE AND SLEEP Objectives 1. Define the changes to the definition of Sepsis 2. Describe the assessment,
Sepsis From EMS to ER to ICU What we need to be doing NEHAL BHATT, MD ATHENS PULMONARY, CRITICAL CARE AND SLEEP Objectives 1. Define the changes to the definition of Sepsis 2. Describe the assessment,
Bedside assessment of fluid status
 Bedside assessment of fluid status 2nd AKI Academy October 18 th 2014 David Treacher Guy s & St Thomas NHS Trust Assessing the circulation - the 3 key questions v Is my patient adequately filled? v What
Bedside assessment of fluid status 2nd AKI Academy October 18 th 2014 David Treacher Guy s & St Thomas NHS Trust Assessing the circulation - the 3 key questions v Is my patient adequately filled? v What
Updates in Sepsis 2017
 Mortality Cases Total U.S. Population/1,000 Updates in 2017 Joshua Solomon, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Background New Definition of New Trials
Mortality Cases Total U.S. Population/1,000 Updates in 2017 Joshua Solomon, M.D. Associate Professor of Medicine National Jewish Health University of Colorado Denver Background New Definition of New Trials
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016
 Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Tailored Volume Resuscitation in the Critically Ill is Achievable. Objectives. Clinical Case 2/16/2018
 Tailored Volume Resuscitation in the Critically Ill is Achievable Heath E Latham, MD Associate Professor Fellowship Program Director Pulmonary and Critical Care Objectives Describe the goal of resuscitation
Tailored Volume Resuscitation in the Critically Ill is Achievable Heath E Latham, MD Associate Professor Fellowship Program Director Pulmonary and Critical Care Objectives Describe the goal of resuscitation
EARLY GOAL DIRECTED THERAPY : seminaires iris. Etat des lieux en Daniel De Backer
 EARLY GOAL DIRECTED THERAPY : Etat des lieux en 2017 Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles Past-President European
EARLY GOAL DIRECTED THERAPY : Etat des lieux en 2017 Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles Past-President European
SURVIVING SEPSIS: Early Management Saves Lives
 SURVIVING SEPSIS: Early Management Saves Lives Pat Posa RN, BSN, MSA System Performance Improvement Leader St. Joseph Mercy Health System Ann Arbor, MI Patricia.posa@stjoeshealth.org Objectives a. Understand
SURVIVING SEPSIS: Early Management Saves Lives Pat Posa RN, BSN, MSA System Performance Improvement Leader St. Joseph Mercy Health System Ann Arbor, MI Patricia.posa@stjoeshealth.org Objectives a. Understand
Transfusion Requirements and Management in Trauma RACHEL JACK
 Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
Transfusion Requirements and Management in Trauma RACHEL JACK Overview Haemostatic resuscitation Massive Transfusion Protocol Overview of NBA research guidelines Haemostatic resuscitation Permissive hypotension
SEPSIS: IT ALL BEGINS WITH INFECTION. Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft.
 SEPSIS: IT ALL BEGINS WITH INFECTION Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft. Worth 1 2 3 OBJECTIVES Review the new Sepsis 3 definitions of sepsis
SEPSIS: IT ALL BEGINS WITH INFECTION Theresa Posani, MS, RN, ACNS-BC, CCRN M/S CNS/Sepsis Coordinator Texas Health Harris Methodist Ft. Worth 1 2 3 OBJECTIVES Review the new Sepsis 3 definitions of sepsis
Sepsis: Management ANUPOL PANITCHOTE, MD. Division of Critical Care Medicine Department of Medicine, Khon Kaen University, Thailand
 Sepsis: Management ANUPOL PANITCHOTE, MD. Division of Critical Care Medicine Department of Medicine, Khon Kaen University, Thailand Vital signs Symptoms LAB BT > 38.3 or < 36 ๐ C HR > 90 bpm RR > 20 /min
Sepsis: Management ANUPOL PANITCHOTE, MD. Division of Critical Care Medicine Department of Medicine, Khon Kaen University, Thailand Vital signs Symptoms LAB BT > 38.3 or < 36 ๐ C HR > 90 bpm RR > 20 /min
Immunomodulation and Sepsis in Oncological Patients. Imad Haddad, M.D. Medical Director, PICU Banner Children s Hospital at BDMC
 Immunomodulation and Sepsis in Oncological Patients Imad Haddad, M.D. Medical Director, PICU Banner Children s Hospital at BDMC 1 Objectives Immune dys-regulation in oncological septic patients Implementation
Immunomodulation and Sepsis in Oncological Patients Imad Haddad, M.D. Medical Director, PICU Banner Children s Hospital at BDMC 1 Objectives Immune dys-regulation in oncological septic patients Implementation
Surviving Sepsis Campaign Guidelines 2012 & Update for David E. Tannehill, DO Critical Care Medicine Mercy Hospital St.
 Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
Frank Sebat, MD - June 29, 2006
 Types of Shock Hypovolemic Shock Low blood volume decreasing cardiac output. AN INTEGRATED SYSTEM OF CARE FOR PATIENTS AT RISK SHOCK TEAM and RAPID RESPONSE TEAM Septic or Distributive Shock Decrease in
Types of Shock Hypovolemic Shock Low blood volume decreasing cardiac output. AN INTEGRATED SYSTEM OF CARE FOR PATIENTS AT RISK SHOCK TEAM and RAPID RESPONSE TEAM Septic or Distributive Shock Decrease in
Guidelines are the Future of Sepsis Management Pro
 Guidelines are the Future of Sepsis Management Pro R. Phillip Dellinger MD, MCCM Professor and Chair of Medicine Director Adult Health Institute Senior Critical Care Attending Camden NJ USA Objectives
Guidelines are the Future of Sepsis Management Pro R. Phillip Dellinger MD, MCCM Professor and Chair of Medicine Director Adult Health Institute Senior Critical Care Attending Camden NJ USA Objectives
Initial Resuscitation of Sepsis & Septic Shock
 Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
Core Measures SEPSIS UPDATES
 Patricia Walker, RN-BC, BSN Evidence Based Practice Manager Quality Management Services UCLA Health System, Ronald Reagan Medical Center Core Measures SEPSIS UPDATES Severe Sepsis and Septic Shock Based
Patricia Walker, RN-BC, BSN Evidence Based Practice Manager Quality Management Services UCLA Health System, Ronald Reagan Medical Center Core Measures SEPSIS UPDATES Severe Sepsis and Septic Shock Based
Sepsis. National Clinical Guideline Centre. Sepsis: the recognition, diagnosis and management of sepsis. NICE guideline <number> January 2016
 National Clinical Guideline Centre Consultation Sepsis Sepsis: the recognition, diagnosis and management of sepsis NICE guideline Appendices I-O January 2016 Draft for consultation Commissioned
National Clinical Guideline Centre Consultation Sepsis Sepsis: the recognition, diagnosis and management of sepsis NICE guideline Appendices I-O January 2016 Draft for consultation Commissioned
Intravenous Fluid Therapy in Critical Illness
 Intravenous Fluid Therapy in Critical Illness GINA HURST, MD DIVISION OF EMERGENCY CRITICAL CARE HENRY FORD HOSPITAL DETROIT, MI Objectives Establish goals of IV fluid therapy Review fluid types and availability
Intravenous Fluid Therapy in Critical Illness GINA HURST, MD DIVISION OF EMERGENCY CRITICAL CARE HENRY FORD HOSPITAL DETROIT, MI Objectives Establish goals of IV fluid therapy Review fluid types and availability
Fluid resuscitation in the ICU/sepsis. The use of albumin
 Fluid resuscitation in the ICU/sepsis The use of albumin Overview Introduction to the ICU and sepsis Albumin: rationale for use in the ICU and severe sepsis Albumin: effects on mortality in sepsis and
Fluid resuscitation in the ICU/sepsis The use of albumin Overview Introduction to the ICU and sepsis Albumin: rationale for use in the ICU and severe sepsis Albumin: effects on mortality in sepsis and
Impact of Fluids in Children with Acute Lung Injury
 Impact of Fluids in Children with Acute Lung Injury Canadian Critical Care Forum Toronto, Canada October 27 th, 2015 Adrienne G. Randolph, MD, MSc Critical Care Division, Department of Anesthesia, Perioperative
Impact of Fluids in Children with Acute Lung Injury Canadian Critical Care Forum Toronto, Canada October 27 th, 2015 Adrienne G. Randolph, MD, MSc Critical Care Division, Department of Anesthesia, Perioperative