3/14/2017. Disclosures. None. Outline. Fluid Management and Hemodynamic Assessment Paul Marik, MD, FCCP, FCCM
|
|
|
- Bertina Ward
- 6 years ago
- Views:
Transcription


1 Fluid Management and Hemodynamic Assessment Paul Marik, MD, FCCP, FCCM Disclosures Stocks Advisory boards Grants Speakers Bureau None Outline Hemodynamic Goals Fluid Resuscitation Historical Perspective Fluid responsiveness and the 6 Guiding principles of fluid resuscitation Techniques for assessment of fluid responsiveness Static CVP Dangers of a high CVP Dynamic Heart-lung interactions Passive leg raising Fluid Challenge Do I give fluid? The effects of a fluid bolus are short lived 1


2 Science Politics Money Religion Chest 2007;132:2020 2
3 Crit Care Med 2013; 41:34 n= Walsh M et al. Anesth 2013:119:507 n= Walsh M et al. Anesth 2013:119:507 3


4 Target Target NEJM 2014;370:1853 NEJM 2014;370:1853 Initial HR > 106 /min Heart rate 24 hours > 95 /min Highly predictive of death 4


5 N Engl J Med 1994; 330:1717 Goals of Hemodynamic Support MAP > 65 mmhg HR < 95 /min Adequate tissue perfusion Clinical examination CI > 2.0 l/min/m 2 CVP < 8 mmhg Fluid Resuscitation Reaching the hemodynamic goals 5




6 Historical Perspective Blue Stage of the Spasmodic Cholera Sketch of girl who died of cholera in Sunderland, November 1831 Lancet, Feb
7 His first patient was an elderly women who had reached the last moments of her earthly existence. Having no precedent to guide me I proceeded with much caution His first patient was an elderly women who had reached the last moments of her earthly existence. Having no precedent to guide me I proceeded with much caution Latta inserted a tube into the basilic vein and injected ounce after ounce of fluid, closely observing the patient. His first patient was an elderly women who had reached the last moments of her earthly existence. Having no precedent to guide me I proceeded with much caution Latta inserted a tube into the basilic vein and injected ounce after ounce of fluid, closely observing the patient. Ounce after ounce of fluid, closely observing the patient. 7




8 His first patient was an elderly women who had reached the last moments of her earthly existence. Having no precedent to guide me I proceeded with much caution Latta inserted a tube into the basilic vein and injected ounce after ounce of fluid, closely observing the patient. Ounce after ounce of fluid, closely observing the patient. the sunken eyes and fallen jaw, pale and cold extremities bearing the manifest imprint of deaths signet, began to glow with returning animation; the pulse returned to the wrist From this to. The Rivers Protocol The Not No evidence 8



9 Fluid overload in patients with severe sepsis and septic shock treated with EGDT Kelm DJ, et al. SHOCK 2015;43: patients with severe sepsis and septic shock At 24 hours, 67% pts had clinical evidence of fluid overload At 72 hours, 48% pts had clinical evidence of fluid overload Fluid overload associated increased hospital mortality OR 1.92 ( ) Crit Care 2015; 19:251 9

 2.")
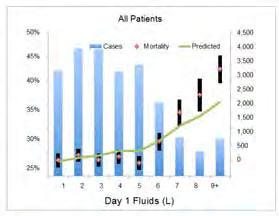
10 Day 1 Fluid Administration in Pts with Severe Sepsis and Septic Shock - Analysis of a large National Database (n=23 513) Day 1 Fluid Administration in Pts with Severe Sepsis and Septic Shock - Analysis of a large National Database (n=23 513) Day 1 fluid < 5 liters Day 1 fluid > 5 liters 0.7% per liter (95% CI 1.0%, 0.4%; p=0.02) 2.3% per liter (95% CI 2.0, 2.5%; p=0.0003) 10


11 Dry, Wet or Something Else Surviving Sepsis Campaign Acta Anaesth Scand 2009;53:843 Dry, Wet or Something Else Surviving Sepsis Campaign Acta Anaesth Scand 2009;53:843 Fluid Restrictive Strategy 11
 current practice and evaluation of fluid management in critically ill patients seems to be arbitrary is not evidence-based and is likely")
12 High Filling Pressures High venous & pulmonary capillary pressures Release of ANP/BNP Shearing of glycocalyx + Decreased Lymphatic flow Organ edema/pulmonary edema Humans evolved to deal with hypovolemia and NOT hypervolemia (311 centers, 46 countries) current practice and evaluation of fluid management in critically ill patients seems to be arbitrary is not evidence-based and is likely harmful 12



13 Fluid resuscitation Give them as much as they need and not a drop more. PRO/CON Series 13
14 Six Principles of Fluid Resuscitation Fluid responsiveness is defined as a >10% increase in SV following a fluid challenge. Only 50% of hemodynamically unstable patients are fluid responsive Six Principles of Fluid Resuscitation Fluid responsiveness is defined as a >10% increase in SV following a fluid challenge. Only 50% of hemodynamically unstable patients are fluid responsive Clinical signs, CXR, CVP, ultrasonography CANNOT be used to determine fluid responsiveness Six Principles of Fluid Resuscitation Fluid responsiveness is defined as a >10% increase in SV following a fluid challenge. Only 50% of hemodynamically unstable patients are fluid responsive Clinical signs, CXR, CVP, ultrasonography CANNOT be used to determine fluid responsiveness The PLR or fluid challenge coupled with real-time SV monitoring are the only accurate methods for determining fluid responsiveness 14
15 Six Principles of Fluid Resuscitation Fluid responsiveness is defined as a >10% increase in SV following a fluid challenge. Only 50% of hemodynamically unstable patients are fluid responsive Clinical signs, CXR, CVP, ultrasonography CANNOT be used to determine fluid responsiveness The PLR or fluid challenge coupled with real-time SV monitoring are the only accurate methods for determining fluid responsiveness The hemodynamic response to a fluid challenge is short lived - usually less than an hour Six Principles of Fluid Resuscitation Fluid responsiveness is defined as a >10% increase in SV following a fluid challenge. Only 50% of hemodynamically unstable patients are fluid responsive Clinical signs, CXR, CVP, ultrasonography CANNOT be used to determine fluid responsiveness The PLR or fluid challenge coupled with real-time SV monitoring are the only accurate methods for determining fluid responsiveness The hemodynamic response to a fluid challenge is short lived - usually less than an hour Fluid responsiveness does not equate to the need for fluid boluses Six Principles of Fluid Resuscitation Fluid responsiveness is defined as a >10% increase in SV following a fluid challenge. Only 50% of hemodynamically unstable patients are fluid responsive Clinical signs, CXR, CVP, ultrasonography CANNOT be used to determine fluid responsiveness The PLR or fluid challenge coupled with real-time SV monitoring are the only accurate methods for determining fluid responsiveness The hemodynamic response to a fluid challenge is short lived - usually less than an hour Fluid responsiveness does not equate to the need for fluid boluses A high CVP is a major factor compromising organ perfusion 15
 across a wide spectrum of patients demonstrated that only 52.")
16 Fluid Responsiveness The only reason to give a patient fluid (fluid bolus) is to increase stroke volume (SV) and cardiac output (CO) A fluid bolus (fluid challenge) is most frequently given for hypotension or oliguria An analysis of 71 clinical studies (3617 pts) across a wide spectrum of patients demonstrated that only 52.7% of patients were fluid responsive Volume expansion cannot be regarded as the cornerstone of resuscitation The Frank-Starling & Marik-Phillips Curves SV EVLW Sepsis Large increase in EVLW Large inc in filling pressures Small increase in CO Large increase in CO Small increase in EVLW Small increase in filling pressures Inc.gradient between MCFP and CVP MCFP= Mean Circulating Filling Pressure Preload Ognibene FP et al. Chest 1988;93:903 16
 RVEDV/LVEDA/GEDI IVC/SVC - respiratory variation PPV/SVV/PVI Aortic blood flow - respiratory variation Passive Leg Raising (PLR) Volume Challenge Non calibrated pulse contour Bioimpedance")
17 Techniques to Assess Fluid Responsiveness ROC Curves & Diagnostic Accuracy Excellent Fair-Good Worthless Assessment of fluid responsiveness Technique Technology CVP/PAOP CVP/PAC IVC/SVC diameter FTc (LVETc) RVEDV/LVEDA/GEDI IVC/SVC - respiratory variation PPV/SVV/PVI Aortic blood flow - respiratory variation Passive Leg Raising (PLR) Volume Challenge Non calibrated pulse contour Bioimpedance Ultrasound (IVC/SVC) Ultrasound (IVC/SVC resp. variability) Pleth waveform (PVI) ECHO- Aortic Doppler (resp. variability) Calibrated pulse contour (PPV/SVV) Esophageal Doppler / USCOM (PLR & volume) Calibrated pulse contour (PLR & volume) NICOM (PLR & volume) 17
 ICU - AUC 0.56 (95% CI; 0.52 to 0.60) OR AUC 0.56 (95% CI; 0.54 to 0.58) There is no data in any group of patients to support using the CVP to guide fluid therapy.")

18 43 studies: healthy controls (n=1), ICU (n=22) and operating room (n=20) patients 57 ± 13% of patients were fluid responders AUC was 0.56 (95% CI; 0.54 to 0.58) ICU - AUC 0.56 (95% CI; 0.52 to 0.60) OR AUC 0.56 (95% CI; 0.54 to 0.58) There is no data in any group of patients to support using the CVP to guide fluid therapy. This approach to fluid resuscitation is potentially dangerous and must be abandoned. Crit Care Med 2013;41:1774 Mean CVP = 9 AUC 0.57 for CVP < 8 AUC 0.54 for CVP 8-12 AUC 0.56 for CVP > 12 Intensive Care Med 2016; epub 18



19 The Not High pressure transmitted backwards MCFP J. Physiol 1931;72:49 19
20 Association between systemic hemodynamics and AKI in patients with sepsis High CVP only factor predictive of AKI Legrund M, et al. Crit Care 2013;17:R278 High CVP only factor predictive of impaired microcirculatory flow BMC Anesthesiol 2013; 13:17 CVP - ARISE 20


21 Measuring the CVP.. leads to volume overload A normal CVP is between 0-2 mmhg this is necessary to ensure adequate venous return and cardiac output (venous return = MCFP CVP). Clinicians seem compelled to give fluid when the CVP is less than 8 mmhg The only solution to this pervasive problem is to stop measuring the CVP Crit Care Resus 2014; 16:245 The Swan is dead. PAC does not improve outcome PAC provides misleading data PAC provides data physician/nurses don t understand PAC is inaccurate 21
 RVEDV/LVEDA/GEDI")

22 The GOLD STANDARD The closest the PAC comes to being a Gold Standard is the color of the catheter!! Assessment of fluid responsiveness Technique CVP/PAOP IVC/SVC diameter FTc (LVETc) RVEDV/LVEDA/GEDI IVC/SVC PPV/SVV/PVI Aortic blood flow Heart-lung interactions during mechanical ventilation PLR Volume Challenge Using heart-lung interactions to assess fluid responsiveness during mechanical ventilation 22
23 Using heart-lung interactions to assess fluid responsiveness during mechanical ventilation Limitations of PPV/SVV Sinus Rhythm Volume cycled ventilation with Vt of 8ml/kg IBW No ventilator-patient dyssynchrony Heart rate/respiratory rate ratio > 3.6 Chest wall compliance (Δ intra-pleural pressure) Cor pulmonale- pulmonary hypertension Increased intra-abdominal pressure Low pulmonary compliance Mechanical ventilation without spontaneous breathing Regular cardiac rhythm Vt 8 ml/kg ideal body weight Heart rate/respiratory rate ratio > 3.6 Total resp. system compliance 30ml/cmH 2 O Tricuspid annular peak systolic velocity 0.15 m/s Only 6 (2%) of the 311 patients satisfied all validity criteria MajoubY, BJA 2014;112:681 23
 RVEDV/LVEDA/GEDI IVC/SVC PPV/SVV/PVI Aortic blood flow PLR Volume Challenge Hemodynamic response to a real or")
24 IVC Collapsibility Index An Indirect measure of RA pressure ROC Assessment of fluid responsiveness Technique CVP/PAOP IVC/SVC diameter FTc (LVETc) RVEDV/LVEDA/GEDI IVC/SVC PPV/SVV/PVI Aortic blood flow PLR Volume Challenge Hemodynamic response to a real or virtual fluid challenge Assessment of fluid responsiveness Technique PLR Volume Challenge Technology Esophageal Doppler/USCOM Calibrated pulse contour NICOM - Bioreactance 24
25 Fluid Responsiveness & Passive Leg Raising Fluid Responsiveness & Passive Leg Raising Stroke Volume preload responsiveness b' a' preload unresponsiveness b a A PLR B Ventricular preload Fluid Responsiveness & Passive Leg Raising Stroke Volume PLR mimics fluid challenge preload responsiveness b' a' preload unresponsiveness b a Unlike fluid challenge, no fluid is infused, and, the effects are reversible and transient A PLR B Ventricular preload 25

26 The volume challenge has to be given rapidly or most is lost from the intravascular space Blood Starch 26

 Give")

27 Crit Care Med 2016 (in press) Fluid Responsive. What Next! Nothing Do not need to increase CO Increased lung water Fluid bolus (500cc LR) Give vasoconstrictor increase venous return secondary to α-agonist mediated decrease in venous capacitance Where's the Blood Volume? 27



28 Venodilation Venoconstriction Increase in MAP following Fluid Bolus mmhg 01 30min min Crit Care 2014;18:


29 Fluid Responsiveness in the FACCT trial Fluid bolus for hypotension, deceased UO 569 boluses in 127 patients 23% of patients were fluid responders At 1 hour MAP increased by 2 mmhg NO change in urine output Lammi MR, et al. Chest 2015; 148: postoperative patients 250 cc crystalloid bolus over 5 minutes 50% fluid responders Maximal change in CO occurred at 1.2 minutes At 10 minutes CO returned to baseline Crit Care Med 2016; 44:880 Hemodynamic Assessment 29





30 Hemodynamic Assessment 30
Tailored Volume Resuscitation in the Critically Ill is Achievable. Objectives. Clinical Case 2/16/2018
 Tailored Volume Resuscitation in the Critically Ill is Achievable Heath E Latham, MD Associate Professor Fellowship Program Director Pulmonary and Critical Care Objectives Describe the goal of resuscitation
Tailored Volume Resuscitation in the Critically Ill is Achievable Heath E Latham, MD Associate Professor Fellowship Program Director Pulmonary and Critical Care Objectives Describe the goal of resuscitation
Sepsis Wave II Webinar Series. Sepsis Reassessment
 Sepsis Wave II Webinar Series Sepsis Reassessment Presenters Nova Panebianco, MD Todd Slesinger, MD Fluid Reassessment in Sepsis Todd L. Slesinger, MD, FACEP, FCCM, FCCP, FAAEM Residency Program Director
Sepsis Wave II Webinar Series Sepsis Reassessment Presenters Nova Panebianco, MD Todd Slesinger, MD Fluid Reassessment in Sepsis Todd L. Slesinger, MD, FACEP, FCCM, FCCP, FAAEM Residency Program Director
Fluid responsiveness and extravascular lung water
 Fluid responsiveness and extravascular lung water Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris-South France Conflicts of interest Member of the Medical Advisory Board of Maquet/Pulsion
Fluid responsiveness and extravascular lung water Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris-South France Conflicts of interest Member of the Medical Advisory Board of Maquet/Pulsion
FLUID RESUSCITATION AND MONITORING IN SEPSIS PROTOCOLIZED VS USUAL CARE DEEPA BANGALORE GOTUR MD, FCCP ASSISTANT PROFESSOR, WEILL CORNELL MEDICAL
 FLUID RESUSCITATION AND MONITORING IN SEPSIS PROTOCOLIZED VS USUAL CARE DEEPA BANGALORE GOTUR MD, FCCP ASSISTANT PROFESSOR, WEILL CORNELL MEDICAL COLLEGE NOVEMBER 10 TH 2017 TEXAS SCCM SYMPOSIUM Disclosures
FLUID RESUSCITATION AND MONITORING IN SEPSIS PROTOCOLIZED VS USUAL CARE DEEPA BANGALORE GOTUR MD, FCCP ASSISTANT PROFESSOR, WEILL CORNELL MEDICAL COLLEGE NOVEMBER 10 TH 2017 TEXAS SCCM SYMPOSIUM Disclosures
Nurse Driven Fluid Optimization Using Dynamic Assessments
 Nurse Driven Fluid Optimization Using Dynamic Assessments 2016 1 WHAT WE BELIEVE We believe that clinicians make vital fluid and drug decisions every day with limited and inconclusive information Cheetah
Nurse Driven Fluid Optimization Using Dynamic Assessments 2016 1 WHAT WE BELIEVE We believe that clinicians make vital fluid and drug decisions every day with limited and inconclusive information Cheetah
Hemodynamic monitoring beyond cardiac output
 Hemodynamic monitoring beyond cardiac output Prof Xavier MONNET Medical Intensive Care Unit Bicêtre Hospital Assistance publique Hôpitaux de Paris FRANCE Conflicts of interest Lilly GlaxoSmithKline Pulsion
Hemodynamic monitoring beyond cardiac output Prof Xavier MONNET Medical Intensive Care Unit Bicêtre Hospital Assistance publique Hôpitaux de Paris FRANCE Conflicts of interest Lilly GlaxoSmithKline Pulsion
Hemodynamic Monitoring Pressure or Volumes? Antonio Pesenti University of Milan Italy
 Hemodynamic Monitoring Pressure or Volumes? Antonio Pesenti University of Milan Italy antonio.pesenti@unimi.it CCCF 2017 Is it useful? YES: CVP It is an important diagnostic element! Your best guess CVP
Hemodynamic Monitoring Pressure or Volumes? Antonio Pesenti University of Milan Italy antonio.pesenti@unimi.it CCCF 2017 Is it useful? YES: CVP It is an important diagnostic element! Your best guess CVP
IN THE NAME OF GOD SHOCK MANAGMENT OMID MORADI MOGHADDAM,MD,FCCM IUMS ASSISTANT PROFESSOR
 IN THE NAME OF GOD SHOCK MANAGMENT OMID MORADI MOGHADDAM,MD,FCCM IUMS ASSISTANT PROFESSOR The ability to evaluate and manage a critically ill patient is one of the most important skills any intensivist
IN THE NAME OF GOD SHOCK MANAGMENT OMID MORADI MOGHADDAM,MD,FCCM IUMS ASSISTANT PROFESSOR The ability to evaluate and manage a critically ill patient is one of the most important skills any intensivist
Fluids in Sepsis Less is more. Dr Anand Senthi Joondalup Health Campus ED MBBS, MAppFin, GradCertPubHlth,
 Fluids in Sepsis Less is more Dr Anand Senthi Joondalup Health Campus ED MBBS, MAppFin, GradCertPubHlth, FRACGP @drsenthi Summary Discussion of the evidence for/against fluid resuscitation in septic shock
Fluids in Sepsis Less is more Dr Anand Senthi Joondalup Health Campus ED MBBS, MAppFin, GradCertPubHlth, FRACGP @drsenthi Summary Discussion of the evidence for/against fluid resuscitation in septic shock
Goal-directed vs Flow-guidedresponsive
 Goal-directed vs Flow-guidedresponsive therapy S Magder Department of Critical Care, McGill University Health Centre Flow-directed vs goal directed strategy for management of hemodynamics S Magder Curr
Goal-directed vs Flow-guidedresponsive therapy S Magder Department of Critical Care, McGill University Health Centre Flow-directed vs goal directed strategy for management of hemodynamics S Magder Curr
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE
 Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
The Use of Dynamic Parameters in Perioperative Fluid Management
 The Use of Dynamic Parameters in Perioperative Fluid Management Gerard R. Manecke Jr., M.D. Chief, Cardiac Anesthesia UCSD Medical Center San Diego, CA, USA Thanks to Tom Higgins, M.D. 1 Goals of today
The Use of Dynamic Parameters in Perioperative Fluid Management Gerard R. Manecke Jr., M.D. Chief, Cardiac Anesthesia UCSD Medical Center San Diego, CA, USA Thanks to Tom Higgins, M.D. 1 Goals of today
Preload optimisation in severe sepsis and septic shock
 Preload optimisation in severe sepsis and septic shock Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris South France Conflicts of interest Member of themedical Advisory Board ofpulsion
Preload optimisation in severe sepsis and septic shock Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris South France Conflicts of interest Member of themedical Advisory Board ofpulsion
Sepsis Management: Past, Present, and Future
 Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
Sepsis Management: Past, Present, and Future Benjamin Ferrell, MD Tennessee ACP Meeting October 28, 2017 Learning Objectives Identify the most updated definition and clinical criteria for sepsis Describe
FLUIDS AND SOLUTIONS IN THE CRITICALLY ILL. Daniel De Backer Department of Intensive Care Erasme University Hospital Brussels, Belgium
 FLUIDS AND SOLUTIONS IN THE CRITICALLY ILL Daniel De Backer Department of Intensive Care Erasme University Hospital Brussels, Belgium Why do we want to administer fluids? To correct hypovolemia? To increase
FLUIDS AND SOLUTIONS IN THE CRITICALLY ILL Daniel De Backer Department of Intensive Care Erasme University Hospital Brussels, Belgium Why do we want to administer fluids? To correct hypovolemia? To increase
Sepsis Update: Focus on Early Recognition and Intervention. Disclosures
 Sepsis Update: Focus on Early Recognition and Intervention Jessie Roske, MD October 2017 Disclosures I have no actual or potential conflict of interest in relation to this program/presentation. I will
Sepsis Update: Focus on Early Recognition and Intervention Jessie Roske, MD October 2017 Disclosures I have no actual or potential conflict of interest in relation to this program/presentation. I will
Prof. Dr. Iman Riad Mohamed Abdel Aal
 The Use of New Ultrasound Indices to Evaluate Volume Status and Fluid Responsiveness in Septic Shock Patients Thesis Submitted for partial fulfillment of MD degree in Anesthesiology, Surgical Intensive
The Use of New Ultrasound Indices to Evaluate Volume Status and Fluid Responsiveness in Septic Shock Patients Thesis Submitted for partial fulfillment of MD degree in Anesthesiology, Surgical Intensive
Fluid management. Dr. Timothy Miller Assistant Professor of Anesthesiology Duke University Medical Center
 Fluid management Dr. Timothy Miller Assistant Professor of Anesthesiology Duke University Medical Center Disclosure Consultant and research funding Edwards Lifesciences Goals of fluid therapy 1. Maintain
Fluid management Dr. Timothy Miller Assistant Professor of Anesthesiology Duke University Medical Center Disclosure Consultant and research funding Edwards Lifesciences Goals of fluid therapy 1. Maintain
Purist? or Pragmatist? Assessment & Management of ICU Volume Status
 Assessment & Management of ICU Volume Status 9 th Annual Rocky Mountain Hospital Medicine Symposium Denver, Colorado Paula Dennen, MD Assistant Professor of Medicine Nephrology and Critical Care Medicine
Assessment & Management of ICU Volume Status 9 th Annual Rocky Mountain Hospital Medicine Symposium Denver, Colorado Paula Dennen, MD Assistant Professor of Medicine Nephrology and Critical Care Medicine
Radboud University Nijmegen Medical Centre Why measure cardiac output in critically ill children?
 Radboud University Nijmegen Medical Centre Why measure cardiac output in critically ill children? J. Lemson Anesthesiologist/(pediatric)intensivist Case; Girl 2 years, 12 kg, severe meningococcal septic
Radboud University Nijmegen Medical Centre Why measure cardiac output in critically ill children? J. Lemson Anesthesiologist/(pediatric)intensivist Case; Girl 2 years, 12 kg, severe meningococcal septic
Fluid Resuscitation and Monitoring in Sepsis. Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS
 Fluid Resuscitation and Monitoring in Sepsis Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS Learning Objectives Compare and contrast fluid resuscitation strategies in septic shock Discuss available
Fluid Resuscitation and Monitoring in Sepsis Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS Learning Objectives Compare and contrast fluid resuscitation strategies in septic shock Discuss available
Disclaimer. Improving MET-based patient care using treatment algorithms. Michael R. Pinsky, MD, Dr hc. Different Environments Demand Different Rules
 Michael R. Pinsky, MD - June 29, 26 Improving MET-based patient care using Michael R. Pinsky, MD, Dr hc Department of Critical Care Medicine University of Pittsburgh Disclaimer Michael R. Pinsky, MD is
Michael R. Pinsky, MD - June 29, 26 Improving MET-based patient care using Michael R. Pinsky, MD, Dr hc Department of Critical Care Medicine University of Pittsburgh Disclaimer Michael R. Pinsky, MD is
Full Disclosure. The case for why it matters. Goal-directed Fluid Resuscitation
 Goal-directed Fluid Resuscitation Christopher G. Choukalas, MD, MS Department of Anesthesia and Perioperative Care University of California, San Francisco I own no stocks Full Disclosure The case for why
Goal-directed Fluid Resuscitation Christopher G. Choukalas, MD, MS Department of Anesthesia and Perioperative Care University of California, San Francisco I own no stocks Full Disclosure The case for why
Surviving Sepsis Campaign Guidelines 2012 & Update for David E. Tannehill, DO Critical Care Medicine Mercy Hospital St.
 Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
Cardiac Output Monitoring - 6
 Cardiac Output Monitoring - 6 How to use Wrexham s Cardiac Output Monitors. Wrexham Maelor Critical Care Version 02.05.16 Introduction Types of Devices: NICOM - Cheetah Oesophageal Doppler +/- Pulse Contour
Cardiac Output Monitoring - 6 How to use Wrexham s Cardiac Output Monitors. Wrexham Maelor Critical Care Version 02.05.16 Introduction Types of Devices: NICOM - Cheetah Oesophageal Doppler +/- Pulse Contour
Jan M. Headley, R.N. BS
 Fluid First: Using PLR & SVV to Optimize Volume Jan M. Headley, R.N. BS Disclosure Director, Clinical Marketing & Professional Education Edwards Lifesciences Does this Patient NEED Fluid?? WE Have a Problem
Fluid First: Using PLR & SVV to Optimize Volume Jan M. Headley, R.N. BS Disclosure Director, Clinical Marketing & Professional Education Edwards Lifesciences Does this Patient NEED Fluid?? WE Have a Problem
The cornerstone of treating patients with hypotension,
 Does the Central Venous Pressure Predict Fluid Responsiveness? An Updated Meta-Analysis and a Plea for Some Common Sense* Paul E. Marik, MD, FCCM 1 ; Rodrigo Cavallazzi, MD 2 Background: Aim: Data Sources:
Does the Central Venous Pressure Predict Fluid Responsiveness? An Updated Meta-Analysis and a Plea for Some Common Sense* Paul E. Marik, MD, FCCM 1 ; Rodrigo Cavallazzi, MD 2 Background: Aim: Data Sources:
Perioperative Fluid Management in ERPs
 Perioperative Fluid Management in ERPs Robert H. Thiele, M.D. Assistant Professor University of Virginia First Do No Harm Intravenous fluids should be considered a pharmacotherapeutic agent Just like all
Perioperative Fluid Management in ERPs Robert H. Thiele, M.D. Assistant Professor University of Virginia First Do No Harm Intravenous fluids should be considered a pharmacotherapeutic agent Just like all
PiCCO based algorithms
 European Society of Anaesthesiologists Annual Meeting 12.-15. June 2010, Helsinki, Finland PiCCO based algorithms Berthold Bein, MD, PhD, DEAA Department of Anaesthesiology and Intensive Care Medicine
European Society of Anaesthesiologists Annual Meeting 12.-15. June 2010, Helsinki, Finland PiCCO based algorithms Berthold Bein, MD, PhD, DEAA Department of Anaesthesiology and Intensive Care Medicine
Dr. F Javier Belda Dept. Anesthesiology and Critical Care Hospital Clinico Universitario Valencia (Spain) Pulsion MAB
 Pulsion MAB") State of the Art Hemodynamic Monitoring III CO, preload, lung water and ScvO2 The winning combination! Dr. F Javier Belda Dept. Anesthesiology and Critical Care Hospital Clinico Universitario Valencia
State of the Art Hemodynamic Monitoring III CO, preload, lung water and ScvO2 The winning combination! Dr. F Javier Belda Dept. Anesthesiology and Critical Care Hospital Clinico Universitario Valencia
Shock and hemodynamic monitorization. Nilüfer Yalındağ Öztürk Marmara University Pendik Research and Training Hospital
 Shock and hemodynamic monitorization Nilüfer Yalındağ Öztürk Marmara University Pendik Research and Training Hospital Shock Leading cause of morbidity and mortality Worldwide: dehydration and hypovolemic
Shock and hemodynamic monitorization Nilüfer Yalındağ Öztürk Marmara University Pendik Research and Training Hospital Shock Leading cause of morbidity and mortality Worldwide: dehydration and hypovolemic
EVOLUCIÓN DE LA MONITORIZACIÓN CARDIOVASCULAR EN LA UCI
 EVOLUCIÓN DE LA MONITORIZACIÓN CARDIOVASCULAR EN LA UCI Antonio Artigas Critical Care Center Sabadell Hospital CIBER Enfermedades Respiratorias Autonomos University of Barcelona Spain aartigas@tauli.cat
EVOLUCIÓN DE LA MONITORIZACIÓN CARDIOVASCULAR EN LA UCI Antonio Artigas Critical Care Center Sabadell Hospital CIBER Enfermedades Respiratorias Autonomos University of Barcelona Spain aartigas@tauli.cat
Bedside assessment of fluid status
 Bedside assessment of fluid status 2nd AKI Academy October 18 th 2014 David Treacher Guy s & St Thomas NHS Trust Assessing the circulation - the 3 key questions v Is my patient adequately filled? v What
Bedside assessment of fluid status 2nd AKI Academy October 18 th 2014 David Treacher Guy s & St Thomas NHS Trust Assessing the circulation - the 3 key questions v Is my patient adequately filled? v What
Using Functional Hemodynamic Indicators to Guide Fluid Therapy
 CE 2.6 HOURS Continuing Education Using Functional Hemodynamic Indicators to Guide Fluid Therapy A more accurate and less invasive way to gauge responsiveness to iv volume replacement. OVERVIEW: Hemodynamic
CE 2.6 HOURS Continuing Education Using Functional Hemodynamic Indicators to Guide Fluid Therapy A more accurate and less invasive way to gauge responsiveness to iv volume replacement. OVERVIEW: Hemodynamic
DESIGNER RESUSCITATION: TITRATING TO TISSUE NEEDS
 DESIGNER RESUSCITATION: TITRATING TO TISSUE NEEDS R. Phillip Dellinger MD, MSc, MCCM Professor and Chair of Medicine Cooper Medical School of Rowan University Chief of Medicine Cooper University Hospital
DESIGNER RESUSCITATION: TITRATING TO TISSUE NEEDS R. Phillip Dellinger MD, MSc, MCCM Professor and Chair of Medicine Cooper Medical School of Rowan University Chief of Medicine Cooper University Hospital
Goal-directed resuscitation in sepsis; a case-based approach
 Goal-directed resuscitation in sepsis; a case-based approach Jorge A Guzman, MD, FCCM Head, Section Critical Care Medicine Respiratory Institute Cleveland Clinic Foundation The challenges to managing septic
Goal-directed resuscitation in sepsis; a case-based approach Jorge A Guzman, MD, FCCM Head, Section Critical Care Medicine Respiratory Institute Cleveland Clinic Foundation The challenges to managing septic
6/5/2014. Sepsis Management and Hemodynamics. 2004: International group of experts,
 Sepsis Management and Hemodynamics Javier Perez-Fernandez, M.D., F.C.C.P. Medical Director Critical Care Services, Baptist t Hospital of Miamii Medical Director Pulmonary Services, West Kendall Baptist
Sepsis Management and Hemodynamics Javier Perez-Fernandez, M.D., F.C.C.P. Medical Director Critical Care Services, Baptist t Hospital of Miamii Medical Director Pulmonary Services, West Kendall Baptist
Obligatory joke. The case for why it matters. Sepsis: More is more. Goal-Directed Fluid Resuscitation 6/1/2013
 Obligatory joke Keep your eye on the food. Goal-Directed Fluid Resuscitation Christopher G. Choukalas, MD, MS Department of Anesthesia and Perioperative Care University of California, San Francisco The
Obligatory joke Keep your eye on the food. Goal-Directed Fluid Resuscitation Christopher G. Choukalas, MD, MS Department of Anesthesia and Perioperative Care University of California, San Francisco The
Assessing Preload Responsiveness Using Arterial Pressure Based Technologies. Patricia A. Meehan, RN, MS Education Consultant Edwards Lifesciences, LLC
 Assessing Preload Responsiveness Using Arterial Pressure Based Technologies Patricia A. Meehan, RN, MS Education Consultant Edwards Lifesciences, LLC Content Description : Fluid administration is a first
Assessing Preload Responsiveness Using Arterial Pressure Based Technologies Patricia A. Meehan, RN, MS Education Consultant Edwards Lifesciences, LLC Content Description : Fluid administration is a first
ICU Volume 12 - Issue 4 - Winter 2012/ Matrix Features
 ICU Volume 12 - Issue 4 - Winter 2012/2013 - Matrix Features Fluid Management in Critically Ill Patients: A Guided Approach Prof. Antonio Artigas, MD, PhD ICU Management & Practice Editorial Board Member
ICU Volume 12 - Issue 4 - Winter 2012/2013 - Matrix Features Fluid Management in Critically Ill Patients: A Guided Approach Prof. Antonio Artigas, MD, PhD ICU Management & Practice Editorial Board Member
The Hemodynamic Puzzle
 The Hemodynamic Puzzle SVV NIRS O 2 ER Lactate Energy Metabolism (Oxygen Consumption) (Ml/min/m 2 ) Oxygen Debt: To Pay or Not to Pay? Full Recovery Possible Delayed Repayment of O 2 Debt Oxygen Deficit
The Hemodynamic Puzzle SVV NIRS O 2 ER Lactate Energy Metabolism (Oxygen Consumption) (Ml/min/m 2 ) Oxygen Debt: To Pay or Not to Pay? Full Recovery Possible Delayed Repayment of O 2 Debt Oxygen Deficit
How can the PiCCO improve protocolized care?
 How can the PiCCO improve protocolized care? Azriel Perel Professor and Chairman Department of Anesthesiology and Intensive Care Sheba Medical Center, Tel Aviv University, Israel ESICM, Vienna 2009 Disclosure
How can the PiCCO improve protocolized care? Azriel Perel Professor and Chairman Department of Anesthesiology and Intensive Care Sheba Medical Center, Tel Aviv University, Israel ESICM, Vienna 2009 Disclosure
Wet Lungs Dry lungs Impact on Outcome in ARDS. Charlie Phillips MD Division of PCCM OHSU 2009
 Wet Lungs Dry lungs Impact on Outcome in ARDS Charlie Phillips MD Division of PCCM OHSU 2009 Today s talk Pathophysiology of ARDS The case for dry Targeting EVLW Disclosures Advisor for Pulsion Medical
Wet Lungs Dry lungs Impact on Outcome in ARDS Charlie Phillips MD Division of PCCM OHSU 2009 Today s talk Pathophysiology of ARDS The case for dry Targeting EVLW Disclosures Advisor for Pulsion Medical
Hemodynamic Monitoring To Guide Volume Resuscitation
 Hemodynamic Monitoring To Guide Volume Resuscitation Nick Johnson, MD Acting Assistant Professor Division of Emergency Medicine Attending Physician, Medical & Neuro-Intensive Care Units Harborview Medical
Hemodynamic Monitoring To Guide Volume Resuscitation Nick Johnson, MD Acting Assistant Professor Division of Emergency Medicine Attending Physician, Medical & Neuro-Intensive Care Units Harborview Medical
Shock, Monitoring Invasive Vs. Non Invasive
 Shock, Monitoring Invasive Vs. Non Invasive Paula Ferrada MD Assistant Professor Trauma, Critical Care and Emergency Surgery Virginia Commonwealth University Shock Fluid Pressors Ionotrope Intervention
Shock, Monitoring Invasive Vs. Non Invasive Paula Ferrada MD Assistant Professor Trauma, Critical Care and Emergency Surgery Virginia Commonwealth University Shock Fluid Pressors Ionotrope Intervention
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016
 Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care
Hemodynamic Monitoring in Critically ill Patients in Arthur Simonnet, interne Tuteur : Pr. Raphaël Favory
 Hemodynamic Monitoring in Critically ill Patients in 2017 Arthur Simonnet, interne Tuteur : Pr. Raphaël Favory Rationale for Hemodynamic Monitoring Identify the presence of hemodynamic instability Identify
Hemodynamic Monitoring in Critically ill Patients in 2017 Arthur Simonnet, interne Tuteur : Pr. Raphaël Favory Rationale for Hemodynamic Monitoring Identify the presence of hemodynamic instability Identify
SHOCK. Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital
 SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy
 Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy A 44 year old female undergoing 10 hour Cytoreductive (CRS) procedure followed by Hyperthermic Intraperitoneal Chemotherapy (HIPEC).
Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy A 44 year old female undergoing 10 hour Cytoreductive (CRS) procedure followed by Hyperthermic Intraperitoneal Chemotherapy (HIPEC).
towards early goal directed therapy
 Paediatric Septic Shock- towards early goal directed therapy Elliot Long Paediatric Acute Care 2011 Conference Outline Emergency Department Rivers Protocol (EGDT) ACCM Sepsis Protocol Evidence Barriers
Paediatric Septic Shock- towards early goal directed therapy Elliot Long Paediatric Acute Care 2011 Conference Outline Emergency Department Rivers Protocol (EGDT) ACCM Sepsis Protocol Evidence Barriers
How to resuscitate the patient in early sepsis? A physiological approach. J.G. van der Hoeven, Nijmegen
 How to resuscitate the patient in early sepsis? A physiological approach J.G. van der Hoeven, Nijmegen Disclosure interests speaker (potential) conflict of interest Potentially relevant relationships with
How to resuscitate the patient in early sepsis? A physiological approach J.G. van der Hoeven, Nijmegen Disclosure interests speaker (potential) conflict of interest Potentially relevant relationships with
IV fluid administration in sepsis. Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London
 IV fluid administration in sepsis Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London The talk What is septic shock? What are the recommendations? What is the evidence? Do we follow
IV fluid administration in sepsis Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London The talk What is septic shock? What are the recommendations? What is the evidence? Do we follow
ENDPOINTS OF RESUSCITATION
 ENDPOINTS OF RESUSCITATION Fred Pieracci, MD, MPH Acute Care Surgeon Denver Health Medical Center Assistant Professor of Surgery University of Colorado Health Science Center OUTLINE Recognition and characterization
ENDPOINTS OF RESUSCITATION Fred Pieracci, MD, MPH Acute Care Surgeon Denver Health Medical Center Assistant Professor of Surgery University of Colorado Health Science Center OUTLINE Recognition and characterization
Fluid responsiveness Monitoring in Surgical and Critically Ill Patients
 Fluid responsiveness Monitoring in Surgical and Critically Ill Patients Impact clinique de la Goal-directed-therapy Patrice FORGET, M.D Cliniques universitaires Saint Luc Université catholique de Louvain,
Fluid responsiveness Monitoring in Surgical and Critically Ill Patients Impact clinique de la Goal-directed-therapy Patrice FORGET, M.D Cliniques universitaires Saint Luc Université catholique de Louvain,
Impedance Cardiography (ICG) Application of ICG in Intensive Care and Emergency
 Application of ICG in Intensive Care and Emergency") Impedance Cardiography (ICG) Application of ICG in Intensive Care and Emergency Aim of haemodynamic monitoring in ICU and ED Detection and therapy of insufficient organ perfusion Answers to common cardiovascular
Impedance Cardiography (ICG) Application of ICG in Intensive Care and Emergency Aim of haemodynamic monitoring in ICU and ED Detection and therapy of insufficient organ perfusion Answers to common cardiovascular
WE NEED TO REDISCOVER PHYSIOLOGY!
 WE NEED TO REDISCOVER PHYSIOLOGY! MERVYN SINGER BLOOMSBURY INSTITUTE OF INTENSIVE CARE MEDICINE UNIVERSITY COLLEGE LONDON, UK DECLARATIONS OF INTEREST GE Healthcare (manufacturer of Venue ultrasound/echo)
WE NEED TO REDISCOVER PHYSIOLOGY! MERVYN SINGER BLOOMSBURY INSTITUTE OF INTENSIVE CARE MEDICINE UNIVERSITY COLLEGE LONDON, UK DECLARATIONS OF INTEREST GE Healthcare (manufacturer of Venue ultrasound/echo)
Troubleshooting Audio
 Welcome! Audio for this event is available via ReadyTalk Internet Streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
Welcome! Audio for this event is available via ReadyTalk Internet Streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
Reverse (fluid) resuscitation Should we be doing it? NAHLA IRTIZA ISMAIL
 resuscitation Should we be doing it? NAHLA IRTIZA ISMAIL") Reverse (fluid) resuscitation Should we be doing it? NAHLA IRTIZA ISMAIL 65 Male, 60 kg D1 in ICU Admitted from OT intubated Diagnosis : septic shock secondary to necrotising fasciitis of the R lower limb
Reverse (fluid) resuscitation Should we be doing it? NAHLA IRTIZA ISMAIL 65 Male, 60 kg D1 in ICU Admitted from OT intubated Diagnosis : septic shock secondary to necrotising fasciitis of the R lower limb
Invasive Cardiac Output Monitoring and Pulse Contour Analysis. Harshad B. Ranchod Paediatric Intensivist Chris Hani Baragwanath Hospital COPICON 2011
 Invasive Cardiac Output Monitoring and Pulse Contour Analysis Harshad B. Ranchod Paediatric Intensivist Chris Hani Baragwanath Hospital COPICON 2011 Introduction The primary goal of haemodynamic monitoring
Invasive Cardiac Output Monitoring and Pulse Contour Analysis Harshad B. Ranchod Paediatric Intensivist Chris Hani Baragwanath Hospital COPICON 2011 Introduction The primary goal of haemodynamic monitoring
Actualités sur le remplissage peropératoire. Philippe Van der Linden MD, PhD
 Actualités sur le remplissage peropératoire Philippe Van der Linden MD, PhD Fees for lectures, advisory board and consultancy: Fresenius Kabi GmbH B Braun Medical SA Perioperative Fluid Volume Administration
Actualités sur le remplissage peropératoire Philippe Van der Linden MD, PhD Fees for lectures, advisory board and consultancy: Fresenius Kabi GmbH B Braun Medical SA Perioperative Fluid Volume Administration
CARDIAC OUTPUT Monitoring ANDY CAMPBELL JOURNAL CLUB NOV 2011
 CARDIAC OUTPUT Monitoring ANDY CAMPBELL JOURNAL CLUB NOV 2011 Is keeping up the pressure enough? It is a source of regret that the measurement of flow is so much more difficult than the measurement of
CARDIAC OUTPUT Monitoring ANDY CAMPBELL JOURNAL CLUB NOV 2011 Is keeping up the pressure enough? It is a source of regret that the measurement of flow is so much more difficult than the measurement of
Jarisch A. Kreislauffragen, Dünser et al. Critical Care 2013, 17:326 Sunday, March 30, 14
 It was fatal for the development of our understanding of circulation that blood flow is relatively difficult while blood pressure so easy to measure: This is the reason why the sphygmomanometer has gained
It was fatal for the development of our understanding of circulation that blood flow is relatively difficult while blood pressure so easy to measure: This is the reason why the sphygmomanometer has gained
L : Line and Tube อ นตรายป องก นได จากการให สารน า
 L : Line and Tube อ นตรายป องก นได จากการให สารน า รศ.นพ.กว ศ กด จ ตตว ฒนร ตน ภาคว ชาศ ลยศาสตร คณะแพทยศาสตร มหาว ทยาล ยเช ยงใหม 3 rd Mini Conference: ความปลอดภ ยในผ ป วย ร วมด วย ช วยได ท กคน ว นท 13-14
L : Line and Tube อ นตรายป องก นได จากการให สารน า รศ.นพ.กว ศ กด จ ตตว ฒนร ตน ภาคว ชาศ ลยศาสตร คณะแพทยศาสตร มหาว ทยาล ยเช ยงใหม 3 rd Mini Conference: ความปลอดภ ยในผ ป วย ร วมด วย ช วยได ท กคน ว นท 13-14
EARLY GOAL DIRECTED THERAPY : seminaires iris. Etat des lieux en Daniel De Backer
 EARLY GOAL DIRECTED THERAPY : Etat des lieux en 2017 Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles Past-President European
EARLY GOAL DIRECTED THERAPY : Etat des lieux en 2017 Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles Past-President European
Impedance Cardiography (ICG) Method, Technology and Validity
 Method, Technology and Validity") Method, Technology and Validity Hemodynamic Basics Cardiovascular System Cardiac Output (CO) Mean arterial pressure (MAP) Variable resistance (SVR) Aortic valve Left ventricle Elastic arteries / Aorta
Method, Technology and Validity Hemodynamic Basics Cardiovascular System Cardiac Output (CO) Mean arterial pressure (MAP) Variable resistance (SVR) Aortic valve Left ventricle Elastic arteries / Aorta
What you need. When you need it. EV1000 Clinical Platform
 What you need. When you need it. EV1000 Clinical Platform EV1000 Clinical Platform The EV1000 clinical platform from Edwards Lifesciences presents the physiologic status of the patient in an intuitive
What you need. When you need it. EV1000 Clinical Platform EV1000 Clinical Platform The EV1000 clinical platform from Edwards Lifesciences presents the physiologic status of the patient in an intuitive
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014
 December 17, 2014") Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
Vasopressors in septic shock
 Vasopressors in septic shock Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris-South France Questions 1- Why do we use vasopressors in septic shock? 2- Which first-line agent? 3- When
Vasopressors in septic shock Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris-South France Questions 1- Why do we use vasopressors in septic shock? 2- Which first-line agent? 3- When
Making the Case For Less Invasive Flow Based Parameters: APCO + SVV. Patricia A. Meehan, RN, MS, CCRN (a) Education Consultant Edwards Lifesciences
 Education Consultant Edwards Lifesciences") Making the Case For Less Invasive Flow Based Parameters: APCO + SVV Patricia A. Meehan, RN, MS, CCRN (a) Education Consultant Edwards Lifesciences A New Gold Standard? How does the system work? Sensor
Making the Case For Less Invasive Flow Based Parameters: APCO + SVV Patricia A. Meehan, RN, MS, CCRN (a) Education Consultant Edwards Lifesciences A New Gold Standard? How does the system work? Sensor
PCV and PAOP Old habits die hard!
 PCV and PAOP Old habits die hard! F Javier Belda MD, PhD Head of Department Associate Professor Anaesthesia and Critical Care Hospital Clínico Universitario Valencia (SPAIN) An old example TOBACO SMOKING
PCV and PAOP Old habits die hard! F Javier Belda MD, PhD Head of Department Associate Professor Anaesthesia and Critical Care Hospital Clínico Universitario Valencia (SPAIN) An old example TOBACO SMOKING
Rounds in the ICU. Eran Segal, MD Director General ICU Sheba Medical Center
 Rounds in the ICU Eran Segal, MD Director General ICU Sheba Medical Center Real Clinical cases (including our mistakes) Emphasis on hemodynamic monitoring Usually no single correct answer We will conduct
Rounds in the ICU Eran Segal, MD Director General ICU Sheba Medical Center Real Clinical cases (including our mistakes) Emphasis on hemodynamic monitoring Usually no single correct answer We will conduct
How and why I give IV fluid Disclosures SCA Fluids and public health 4/1/15. Andrew Shaw MB FRCA FCCM FFICM
 How and why I give IV fluid Andrew Shaw MB FRCA FCCM FFICM Professor and Chief Cardiothoracic Anesthesiology Vanderbilt University Medical Center 2015 Disclosures Consultant for Grifols manufacturer of
How and why I give IV fluid Andrew Shaw MB FRCA FCCM FFICM Professor and Chief Cardiothoracic Anesthesiology Vanderbilt University Medical Center 2015 Disclosures Consultant for Grifols manufacturer of
Sepsis and septic shock: can we win the battle against this hidden crisis?
 REVIEW ARTICLE Sepsis and septic shock: can we win the battle against this hidden crisis? V.G. Dassanayake Department of Surgery, Faculty of Medicine, University of Colombo, Sri Lanka Key words : Sepsis;
REVIEW ARTICLE Sepsis and septic shock: can we win the battle against this hidden crisis? V.G. Dassanayake Department of Surgery, Faculty of Medicine, University of Colombo, Sri Lanka Key words : Sepsis;
Sepsis and septic shock Practical hemodynamic consequences. Intensive Care Training Program Radboud University Medical Centre Nijmegen
 Sepsis and septic shock Practical hemodynamic consequences Intensive Care Training Program Radboud University Medical Centre Nijmegen Septic cardiomyopathy Present in > 50% and often masked by low vascular
Sepsis and septic shock Practical hemodynamic consequences Intensive Care Training Program Radboud University Medical Centre Nijmegen Septic cardiomyopathy Present in > 50% and often masked by low vascular
Relax and Learn At the Farm 2012
 Relax and Learn At the Farm Session 9: Invasive Hemodynamic Assessment and What to Do with the Data Carol Jacobson RN, MN Cardiovascular Nursing Education Associates Function of CV system is to deliver
Relax and Learn At the Farm Session 9: Invasive Hemodynamic Assessment and What to Do with the Data Carol Jacobson RN, MN Cardiovascular Nursing Education Associates Function of CV system is to deliver
Sepsis: Identification and Management in an Acute Care Setting
 Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Sepsis: Identification and Management in an Acute Care Setting Dr. Barbara M. Mills DNP Director Rapid Response Team/ Code Resuscitation Stony Brook University Medical Center SEPSIS LECTURE NPA 2018 OBJECTIVES
Review Article Echocardiographic Assessment of Preload Responsiveness in Critically Ill Patients
 Cardiology Research and Practice Volume 2012, Article ID 819696, 7 pages doi:10.1155/2012/819696 Review Article Echocardiographic Assessment of Preload Responsiveness in Critically Ill Patients Alexander
Cardiology Research and Practice Volume 2012, Article ID 819696, 7 pages doi:10.1155/2012/819696 Review Article Echocardiographic Assessment of Preload Responsiveness in Critically Ill Patients Alexander
The Septic Patient. Dr Arunraj Navaratnarajah. Renal SpR Imperial College NHS Healthcare Trust
 The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
The Septic Patient Dr Arunraj Navaratnarajah Renal SpR Imperial College NHS Healthcare Trust Objectives of this session Define SIRS / sepsis / severe sepsis / septic shock Early recognition of Sepsis The
Cardiovascular Management of Septic Shock
 Cardiovascular Management of Septic Shock R. Phillip Dellinger, MD Professor of Medicine Robert Wood Johnson Medical School/UMDNJ Director, Critical Care Medicine and Med/Surg ICU Cooper University Hospital
Cardiovascular Management of Septic Shock R. Phillip Dellinger, MD Professor of Medicine Robert Wood Johnson Medical School/UMDNJ Director, Critical Care Medicine and Med/Surg ICU Cooper University Hospital
Sepsis Management Update 2014
 Sepsis Management Update 2014 Laura J. Moore, MD, FACS Associate Professor, Department of Surgery The University of Texas Health Science Center, Houston Medical Director, Shock Trauma ICU Texas Trauma
Sepsis Management Update 2014 Laura J. Moore, MD, FACS Associate Professor, Department of Surgery The University of Texas Health Science Center, Houston Medical Director, Shock Trauma ICU Texas Trauma
Topics to be Covered. Cardiac Measurements. Distribution of Blood Volume. Distribution of Pulmonary Ventilation & Blood Flow
 Topics to be Covered MODULE F HEMODYNAMIC MONITORING Cardiac Output Determinants of Stroke Volume Hemodynamic Measurements Pulmonary Artery Catheterization Control of Blood Pressure Heart Failure Cardiac
Topics to be Covered MODULE F HEMODYNAMIC MONITORING Cardiac Output Determinants of Stroke Volume Hemodynamic Measurements Pulmonary Artery Catheterization Control of Blood Pressure Heart Failure Cardiac
Swan Ganz catheter: Does it still have a role? Daniel De Backer Department of Intensive Care Erasme University Hospital Brussels, Belgium
 Swan Ganz catheter: Does it still have a role? Daniel De Backer Department of Intensive Care Erasme University Hospital Brussels, Belgium How can cardiac output be measured? Thermodilution Arterial waveform
Swan Ganz catheter: Does it still have a role? Daniel De Backer Department of Intensive Care Erasme University Hospital Brussels, Belgium How can cardiac output be measured? Thermodilution Arterial waveform
SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP
 SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP OBJECTIVES Arise, ProMISE, ProCESS Key points in sepsis management The CMS sepsis core measure COST OF SEPSIS CARE IN US Most
SEPSIS UPDATE WHY DO WE NEED A CORE MEASURE CHAD M. KOVALA DO, FACOEP, FACEP OBJECTIVES Arise, ProMISE, ProCESS Key points in sepsis management The CMS sepsis core measure COST OF SEPSIS CARE IN US Most
Sepsis Awareness and Education
 Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Sepsis Awareness and Education Meets the updated New York State Department of Health (NYSDOH) requirements for Infection Control and Barrier Precautions coursework Element VII: Sepsis Awareness and Education
Patrick C. Cullinan, DO, NBPNS, FCCM, FACOEP, FACOI Associate Clinical Professor, UIWSOM, San Antonio, Texas Adjunct Assistant Professor, University
 Patrick C. Cullinan, DO, NBPNS, FCCM, FACOEP, FACOI Associate Clinical Professor, UIWSOM, San Antonio, Texas Adjunct Assistant Professor, University of Texas Health Science Center, Department of Emergency
Patrick C. Cullinan, DO, NBPNS, FCCM, FACOEP, FACOI Associate Clinical Professor, UIWSOM, San Antonio, Texas Adjunct Assistant Professor, University of Texas Health Science Center, Department of Emergency
Early Goal Directed Therapy in 2015: What Did the Big Trials Teach us?
 Early Goal Directed Therapy in 2015: What Did the Big Trials Teach us? Mitchell M. Levy MD, FCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care Warren Alpert Medical School
Early Goal Directed Therapy in 2015: What Did the Big Trials Teach us? Mitchell M. Levy MD, FCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care Warren Alpert Medical School
Sepsis or Severe Sepsis? Is there a right thing, and how do we do it?
 Sepsis or Severe Sepsis? Is there a right thing, and how do we do it? Steven Q Simpson, MD, FCCP, FACP Professor of Medicine Division of Pulmonary and Critical Care University of Kansas Disclosures No
Sepsis or Severe Sepsis? Is there a right thing, and how do we do it? Steven Q Simpson, MD, FCCP, FACP Professor of Medicine Division of Pulmonary and Critical Care University of Kansas Disclosures No
Actualités de la prise en charge hémodynamique initiale Daniel De Backer
 Actualités de la prise en charge hémodynamique initiale Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles Past- President European
Actualités de la prise en charge hémodynamique initiale Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles Past- President European
Introduction. Invasive Hemodynamic Monitoring. Determinants of Cardiovascular Function. Cardiovascular System. Hemodynamic Monitoring
 Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Sepsis and septic shock
 Sepsis and septic shock Practical hemodynamic consequences Intensive Care Training Program Radboud University Medical Centre Nijmegen Septic cardiomyopathy Present in > 50% and often masked by low vascular
Sepsis and septic shock Practical hemodynamic consequences Intensive Care Training Program Radboud University Medical Centre Nijmegen Septic cardiomyopathy Present in > 50% and often masked by low vascular
Early Goal-Directed Therapy
 Early Goal-Directed Therapy Where do we stand? Jean-Daniel Chiche, MD PhD MICU & Dept of Host-Pathogen Interaction Hôpital Cochin & Institut Cochin, Paris-F Resuscitation targets in septic shock 1 The
Early Goal-Directed Therapy Where do we stand? Jean-Daniel Chiche, MD PhD MICU & Dept of Host-Pathogen Interaction Hôpital Cochin & Institut Cochin, Paris-F Resuscitation targets in septic shock 1 The
Venous / Arterial Compliance Ratio Calculation. Conflict of Interest
 Venous / Arterial Compliance Ratio Calculation Kirk H. Shelley, M.D., Ph.D. Professor of Anesthesiology Yale University STA 13 Conflict of Interest Twenty plus year history of research on this and related
Venous / Arterial Compliance Ratio Calculation Kirk H. Shelley, M.D., Ph.D. Professor of Anesthesiology Yale University STA 13 Conflict of Interest Twenty plus year history of research on this and related
Sepsis: Management ANUPOL PANITCHOTE, MD. Division of Critical Care Medicine Department of Medicine, Khon Kaen University, Thailand
 Sepsis: Management ANUPOL PANITCHOTE, MD. Division of Critical Care Medicine Department of Medicine, Khon Kaen University, Thailand Vital signs Symptoms LAB BT > 38.3 or < 36 ๐ C HR > 90 bpm RR > 20 /min
Sepsis: Management ANUPOL PANITCHOTE, MD. Division of Critical Care Medicine Department of Medicine, Khon Kaen University, Thailand Vital signs Symptoms LAB BT > 38.3 or < 36 ๐ C HR > 90 bpm RR > 20 /min
Functional Hemodynamic Monitoring and Management A practical Approach
 Functional Hemodynamic Monitoring and Management A practical Approach Daniel A. Reuter Center of Anesthesiology and Intensive Care Medicine Hamburg-Eppendorf University Hospital Hamburg, Germany Euronaesthesia
Functional Hemodynamic Monitoring and Management A practical Approach Daniel A. Reuter Center of Anesthesiology and Intensive Care Medicine Hamburg-Eppendorf University Hospital Hamburg, Germany Euronaesthesia
Index. K Knobology, TTE artifact, image resolution, ultrasound, 14
 A Acute aortic regurgitation (AR), 124 128 Acute aortic syndrome (AAS) classic aortic dissection diagnosis, 251 263 evolutive patterns, 253 255 pathology, 250 251 classifications, 247 248 incomplete aortic
A Acute aortic regurgitation (AR), 124 128 Acute aortic syndrome (AAS) classic aortic dissection diagnosis, 251 263 evolutive patterns, 253 255 pathology, 250 251 classifications, 247 248 incomplete aortic
CATCH A WAVE.. INTRODUCTION NONINVASIVE HEMODYNAMIC MONITORING 4/12/2018
 WAVES CATCH A WAVE.. W I S C O N S I N P A R A M E D I C S E M I N A R A P R I L 2 0 1 8 K E R I W Y D N E R K R A U S E R N, C C R N, E M T - P Have you considered that if you don't make waves, nobody
WAVES CATCH A WAVE.. W I S C O N S I N P A R A M E D I C S E M I N A R A P R I L 2 0 1 8 K E R I W Y D N E R K R A U S E R N, C C R N, E M T - P Have you considered that if you don't make waves, nobody
Sepsis and Hemodynamic Support in September 15, 2017 Carleen Risaliti
 Sepsis and Hemodynamic Support in 2017 September 15, 2017 Carleen Risaliti Objectives Review fluid resuscitation guidelines in septic shock Discuss volume assessment v. fluid responsiveness Evaluate pros
Sepsis and Hemodynamic Support in 2017 September 15, 2017 Carleen Risaliti Objectives Review fluid resuscitation guidelines in septic shock Discuss volume assessment v. fluid responsiveness Evaluate pros
SHOCK and the Trauma Victim. JP Pretorius Department of Surgery & SICU Steve Biko Academic Hospital.
 SHOCK and the Trauma Victim JP Pretorius Department of Surgery & SICU Steve Biko Academic Hospital. Classification of Shock Cardiogenic - Myopathic Arrythmic Mechanical Hypovolaemic - Haemorrhagic Non-haemorrhagic
SHOCK and the Trauma Victim JP Pretorius Department of Surgery & SICU Steve Biko Academic Hospital. Classification of Shock Cardiogenic - Myopathic Arrythmic Mechanical Hypovolaemic - Haemorrhagic Non-haemorrhagic
Point-of-Care Ultrasound Closer look at the Inferior Vena Cavae &
 Point-of-Care Ultrasound Closer look at the Inferior Vena Cavae & Brief Introduction to Gross Systolic Function Omar S. Darwish, MS, DO Certified in Point-of-Care Ultrasound Hospitalist University of California,
Point-of-Care Ultrasound Closer look at the Inferior Vena Cavae & Brief Introduction to Gross Systolic Function Omar S. Darwish, MS, DO Certified in Point-of-Care Ultrasound Hospitalist University of California,