WE NEED TO REDISCOVER PHYSIOLOGY!
|
|
|
- Morgan Butler
- 6 years ago
- Views:
Transcription


1 WE NEED TO REDISCOVER PHYSIOLOGY! MERVYN SINGER BLOOMSBURY INSTITUTE OF INTENSIVE CARE MEDICINE UNIVERSITY COLLEGE LONDON, UK
 Deltex Medical")
 Oxford Optronix (manufacturer of bladder")
2 DECLARATIONS OF INTEREST GE Healthcare (manufacturer of Venue ultrasound/echo) Deltex Medical (manufacturer of CardioQ oesophageal Doppler monitor) Oxford Optronix (manufacturer of bladder tissue PO 2 monitor)
3 post-cardiac arrest, 65 y.o. patient has: HR 130, BP 80/50, CVP 8, lactate 5 mmol/l pulmonary oedema on chest x-ray
4 post-cardiac arrest, 65 y.o. patient has: HR 130, BP 80/50, CVP 8, lactate 5 mmol/l pulmonary oedema on chest x-ray

5 post-cardiac arrest, 65 y.o. patient has: HR 130, BP 80/50, CVP 8, lactate 5 mmol/l pulmonary oedema on chest x-ray What would you do? 1. fluid? 2. inotrope? 3. vasodilator? 4. vasoconstrictor?
6 post-cardiac arrest, 65 y.o. patient has: HR 130, BP 80/50, CVP 8, lactate 5 mmol/l pulmonary oedema on chest x-ray cardiac output 2 l/min, evidence of hypovolaemia
7 post-cardiac arrest, 65 y.o. patient has: HR 130, BP 80/50, CVP 8, lactate 5 mmol/l pulmonary oedema on chest x-ray cardiac output 2 l/min, evidence of hypovolaemia What would you do? 1. fluid? 2. inotrope? 3. vasodilator? 4. vasoconstrictor?
8 post-cardiac arrest, 65 y.o. patient has: HR 130, BP 80/50, CVP 8, lactate 5 mmol/l pulmonary oedema on chest x-ray cardiac output 2 l/min, evidence of hypovolaemia What would you do? 1. fluid? 2. inotrope? 3. vasodilator? 4. vasoconstrictor?
9 post-cardiac arrest, 65 y.o. patient has: HR 130, BP 80/50, CVP 8, lactate 5 mmol/l pulmonary oedema on chest x-ray cardiac output 2 l/min, well-filled
10 post-cardiac arrest, 65 y.o. patient has: HR 130, BP 80/50, CVP 8, lactate 5 mmol/l pulmonary oedema on chest x-ray cardiac output 2 l/min, well-filled What would you do? 1. fluid? 2. inotrope? 3. vasodilator? 4. vasoconstrictor?
11 post-cardiac arrest, 65 y.o. patient has: HR 130, BP 80/50, CVP 8, lactate 5 mmol/l pulmonary oedema on chest x-ray cardiac output 2 l/min, well-filled What would you do? 1. fluid? 2. inotrope? 3. vasodilator? 4. vasoconstrictor?
12 post-cardiac arrest, 65 y.o. patient has: HR 130, BP 80/50, CVP 8, lactate 5 mmol/l pulmonary oedema on chest x-ray cardiac output 2 l/min, -filled
13 post-cardiac arrest, 65 y.o. patient has: HR 130, BP 80/50, CVP 8, lactate 5 mmol/l pulmonary oedema on chest x-ray cardiac output 2 l/min, over -filled
14 post-cardiac arrest, 65 y.o. patient has: HR 130, BP 80/50, CVP 8, lactate 5 mmol/l pulmonary oedema on chest x-ray cardiac output 2 l/min, over -filled What would you do? 1. fluid? 2. inotrope? 3. vasodilator? 4. vasoconstrictor?
15 post-cardiac arrest, 65 y.o. patient has: HR 130, BP 80/50, CVP 8, lactate 5 mmol/l pulmonary oedema on chest x-ray cardiac output 2 l/min, over -filled What would you do? 1. fluid? 2. inotrope? 3. vasodilator? 4. vasoconstrictor?
16 post-cardiac arrest, 65 y.o. patient has: HR 130, BP 80/50, CVP 8, lactate 5 mmol/l pulmonary oedema on chest x-ray cardiac output 12 l/min
17 post-cardiac arrest, 65 y.o. patient has: HR 130, BP 80/50, CVP 8, lactate 5 mmol/l pulmonary oedema on chest x-ray cardiac output 12 l/min What would you do? 1. fluid? 2. inotrope? 3. vasodilator? 4. vasoconstrictor?


18 post-cardiac arrest, 65 y.o. patient has: HR 130, BP 80/50, CVP 8, lactate 5 mmol/l pulmonary oedema on chest x-ray cardiac output 12 l/min What would you do? 1. fluid? 2. inotrope? 3. vasodilator? 4. vasoconstrictor?
19 NEED EXTRA INFORMATION TO INFORM CORRECT CHOICE..
20 NEED EXTRA INFORMATION TO INFORM CORRECT CHOICE.. deeper understanding of physiology
21 NEED EXTRA INFORMATION TO INFORM CORRECT CHOICE.. deeper understanding of physiology deeper measurement of physiology

22 NEED EXTRA INFORMATION TO INFORM CORRECT CHOICE.. deeper understanding of physiology deeper measurement of physiology

23 Much of our current practice is empiric.. using inappropriate targets.. with little understanding of physiology... or pharmacology... or biochemistry... or metabolism or...
24 Karl Ludwig ( )

25 " the fundamental problems in the circulation derive from the fact that the supply of adequate amounts of blood to the organs of the body is the main purpose of the circulation and the pressures that are necessary to achieve it are of secondary importance; but the measurement of flow is difficult while that of pressure is easy so that our knowledge of flow is usually derivatory." Karl Ludwig ( )
26
27
28
29
30 BUT THIS IS FOR A POPULATION, NOT AN INDIVIDUAL!!!!!
31 BUT THIS IS FOR A POPULATION, NOT AN INDIVIDUAL!!!!!
32 BUT THIS IS FOR A POPULATION, NOT AN INDIVIDUAL!!!!!




33 BUT THIS IS FOR A POPULATION, NOT AN INDIVIDUAL!!!!!
34
35
36
37
38
39

40
41 DRY OR WET?.. HOW ABOUT ENOUGH?
42 DRY OR WET?.. HOW ABOUT ENOUGH?.. not adapted to individual patient requirement 30 ml/kg is empiric - some patients need more, some less fluid needs to be titrated to a treatment endpoint.. and not an arbitrary amount
43 DRY OR WET?.. HOW ABOUT ENOUGH?.. not adapted to individual patient requirement 30 ml/kg is empiric - some patients need more, some less fluid needs to be titrated to a treatment endpoint.. and not an arbitrary amount BALANCED VS UNBALANCED FLUID? monitor chloride levels.. WHAT S THE ISSUE?.. then can safely give NaCl
44 HOW GOOD ARE YOUR CLINICAL SKILLS?
45 HOW GOOD ARE YOUR CLINICAL SKILLS? Cardiac output LV filling pressure Connors (NEJM 83) ICU pts 44% 42% Eisenberg (CCM 84) ICU pts 50% 33%
46 HOW GOOD ARE YOUR CLINICAL SKILLS? Connors Eisenberg Bayliss (NEJM 83) (CCM 84) (BMJ 83) ICU pts ICU pts CCU pts Cardiac output 44% 50% 71% LV filling pressure 42% 33% 62%
 (CCM 84) (BMJ 83) ICU pts ICU pts CCU pts Cardiac output 44%")
47 HOW GOOD ARE YOUR CLINICAL SKILLS? Connors Eisenberg Bayliss (NEJM 83) (CCM 84) (BMJ 83) ICU pts ICU pts CCU pts Cardiac output 44% 50% 71% LV filling pressure 42% 33% 62% Change in Rx 48% 58% 58%
48 BLOOD PRESSURE AND HEART RATE INSENSITIVE GUIDES TO CIRCULATORY STATUS
49 BLOOD PRESSURE AND HEART RATE INSENSITIVE GUIDES TO CIRCULATORY STATUS a normal (or high) BP may mask a low output state hypotension is a late sign of a low output state a low BP may be due to a high output, vasodilated state tachycardia is an almost universal response to stress
50 BLOOD PRESSURE AND HEART RATE INSENSITIVE GUIDES TO CIRCULATORY STATUS a normal (or high) BP may mask a low output state hypotension is a late sign of a low output state a low BP may be due to a high output, vasodilated state tachycardia is an almost universal response to stress need BETTER monitoring!!!
51 BLOOD PRESSURE AND HEART RATE INSENSITIVE GUIDES TO CIRCULATORY STATUS a normal (or high) BP may mask a low output state hypotension is a late sign of a low output state a low BP may be due to a high output, vasodilated state tachycardia is an almost universal response to stress need BETTER monitoring!!! dynamic challenge rather than static measure


52 J Physiol 1914; 48: Ernest Starling ( )



53 venous pressure J Physiol 1914; 48: cardiac output
54 FRANK-STARLING CURVE

55 FRANK-STARLING CURVE 200 ml 200 ml
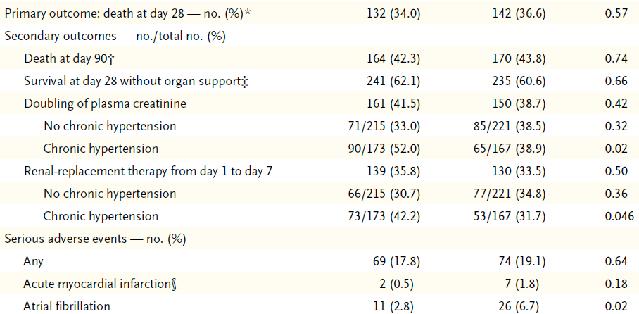
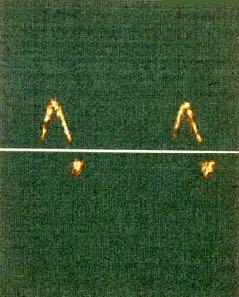
56 DOPPLER FLOW VELOCITY WAVEFORM predominant change
57 DOPPLER FLOW VELOCITY WAVEFORM Preload Reduction Preload Increase predominant change
58 DOPPLER FLOW VELOCITY WAVEFORM Preload Reduction Preload Increase predominant change Myocardial Depression Positive Inotropy
59 DOPPLER FLOW VELOCITY WAVEFORM Preload Reduction Preload Increase predominant change Afterload Increase Afterload Reduction Myocardial Depression Positive Inotropy
60 FRANK-STARLING CURVE STROKE VOLUME END-DIASTOLIC VOL (CVP)
61 FRANK-STARLING CURVE STROKE VOLUME END-DIASTOLIC VOL (CVP)
")
62 FRANK-STARLING CURVE STROKE VOLUME C B A V1 V2 V3 END-DIASTOLIC VOL (P1 P2 P3) (CVP)



63 Stanley J. Sarnoff Chief, Cardiovascular Physiology Lab at the National Heart Institute Physiol Rev 1955; 35:
64 Physiol Rev 1955; 35:123-9
65 Physiol Rev 1955; 35:123-9
66 Physiol Rev 1955; 35:123-9
67 Physiol Rev 1955; 35:123-9


68 Physiol Rev 1955; 35:123-9
69 DOSE RESPONSE CURVE IN HEALTHY VOLUNTEERS TO METHOXAMINE (ALPHA-AGONIST) AND METARAMINOL (ALPHA- AND BETA-AGONIST) [from Singer Crit Care Med. 1991;19: ] mean BP (mmhg) methoxamine metaraminol % change in cardiac output

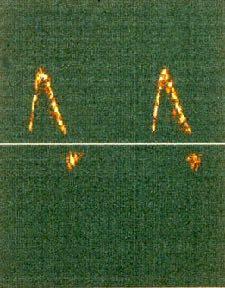
70 pre-metaraminol post-metaraminol
71 go dynamic
72 The physiological challenge fluid dilator posture propofol PEEP..
73




74 PROTOCOLS VS GUIDELINES
75 SUMMARY Physiology is fundamental to good - personalised - patient care Protocols appropriate for processes of care. but not personalised patient management

76 SUMMARY Physiology is fundamental to good - personalised - patient care Protocols appropriate for processes of care. but not personalised patient management
77

78
79
Useful Ectopics: Case Study. Effects of vasodilation and the diagnostic value of ectopic heartbeats
 Effects of vasodilation and the diagnostic value of ectopic heartbeats 83 year old man, weight 66 kg, height 177 cm, BSA 1.82m 2. Closure of colostomy. No cardiac history. Screenshot 1 Baseline at start
Effects of vasodilation and the diagnostic value of ectopic heartbeats 83 year old man, weight 66 kg, height 177 cm, BSA 1.82m 2. Closure of colostomy. No cardiac history. Screenshot 1 Baseline at start
Hemodynamic Monitoring Pressure or Volumes? Antonio Pesenti University of Milan Italy
 Hemodynamic Monitoring Pressure or Volumes? Antonio Pesenti University of Milan Italy antonio.pesenti@unimi.it CCCF 2017 Is it useful? YES: CVP It is an important diagnostic element! Your best guess CVP
Hemodynamic Monitoring Pressure or Volumes? Antonio Pesenti University of Milan Italy antonio.pesenti@unimi.it CCCF 2017 Is it useful? YES: CVP It is an important diagnostic element! Your best guess CVP
FUNDAMENTALS OF HEMODYNAMICS, VASOACTIVE DRUGS AND IABP IN THE FAILING HEART
 FUNDAMENTALS OF HEMODYNAMICS, VASOACTIVE DRUGS AND IABP IN THE FAILING HEART CINDY BITHER, MSN, ANP, ANP, AACC, CHFN CHIEF NP, ADV HF PROGRAM MEDSTAR WASHINGTON HOSPITAL CENTER CONFLICTS OF INTEREST NONE
FUNDAMENTALS OF HEMODYNAMICS, VASOACTIVE DRUGS AND IABP IN THE FAILING HEART CINDY BITHER, MSN, ANP, ANP, AACC, CHFN CHIEF NP, ADV HF PROGRAM MEDSTAR WASHINGTON HOSPITAL CENTER CONFLICTS OF INTEREST NONE
John Park, MD Assistant Professor of Medicine
 John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
John Park, MD Assistant Professor of Medicine Faculty photo will be placed here park.john@mayo.edu 2015 MFMER 3543652-1 Sepsis Out with the Old, In with the New Mayo School of Continuous Professional Development
DESCRIBE THE FACTORS AFFECTING CARDIAC OUTPUT.
 DESCRIBE THE FACTORS AFFECTING CARDIAC OUTPUT. BY: DISHA PRAKASH I MBBS, ROLL NO: 16M069 OBJECTIVES OF LEARNING Terminology and conceptual understanding of Cardiac Output. Factors regulating Cardiac Output.
DESCRIBE THE FACTORS AFFECTING CARDIAC OUTPUT. BY: DISHA PRAKASH I MBBS, ROLL NO: 16M069 OBJECTIVES OF LEARNING Terminology and conceptual understanding of Cardiac Output. Factors regulating Cardiac Output.
FLUIDS AND SOLUTIONS IN THE CRITICALLY ILL. Daniel De Backer Department of Intensive Care Erasme University Hospital Brussels, Belgium
 FLUIDS AND SOLUTIONS IN THE CRITICALLY ILL Daniel De Backer Department of Intensive Care Erasme University Hospital Brussels, Belgium Why do we want to administer fluids? To correct hypovolemia? To increase
FLUIDS AND SOLUTIONS IN THE CRITICALLY ILL Daniel De Backer Department of Intensive Care Erasme University Hospital Brussels, Belgium Why do we want to administer fluids? To correct hypovolemia? To increase
IV fluid administration in sepsis. Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London
 IV fluid administration in sepsis Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London The talk What is septic shock? What are the recommendations? What is the evidence? Do we follow
IV fluid administration in sepsis Dr David Inwald Consultant in PICU St Mary s Hospital, London CATS, London The talk What is septic shock? What are the recommendations? What is the evidence? Do we follow
3/14/2017. Disclosures. None. Outline. Fluid Management and Hemodynamic Assessment Paul Marik, MD, FCCP, FCCM
 Fluid Management and Hemodynamic Assessment Paul Marik, MD, FCCP, FCCM Disclosures Stocks Advisory boards Grants Speakers Bureau None Outline Hemodynamic Goals Fluid Resuscitation Historical Perspective
Fluid Management and Hemodynamic Assessment Paul Marik, MD, FCCP, FCCM Disclosures Stocks Advisory boards Grants Speakers Bureau None Outline Hemodynamic Goals Fluid Resuscitation Historical Perspective
Relax and Learn At the Farm 2012
 Relax and Learn At the Farm Session 9: Invasive Hemodynamic Assessment and What to Do with the Data Carol Jacobson RN, MN Cardiovascular Nursing Education Associates Function of CV system is to deliver
Relax and Learn At the Farm Session 9: Invasive Hemodynamic Assessment and What to Do with the Data Carol Jacobson RN, MN Cardiovascular Nursing Education Associates Function of CV system is to deliver
2.6 Cardiovascular Computer Simulation
 2.6 Cardiovascular Computer Simulation ROOM 23G22 Contents 1. INTRODUCTION... 4 1.1. GENERAL REMARKS... 4 1.2. LEARNING GOALS... 4 1.3. PHYSIOLOGICAL PARAMETERS... 5 1.4. GLOSSARY... 5 2. USING THE COMPUTER
2.6 Cardiovascular Computer Simulation ROOM 23G22 Contents 1. INTRODUCTION... 4 1.1. GENERAL REMARKS... 4 1.2. LEARNING GOALS... 4 1.3. PHYSIOLOGICAL PARAMETERS... 5 1.4. GLOSSARY... 5 2. USING THE COMPUTER
Impedance Cardiography (ICG) Method, Technology and Validity
 Method, Technology and Validity") Method, Technology and Validity Hemodynamic Basics Cardiovascular System Cardiac Output (CO) Mean arterial pressure (MAP) Variable resistance (SVR) Aortic valve Left ventricle Elastic arteries / Aorta
Method, Technology and Validity Hemodynamic Basics Cardiovascular System Cardiac Output (CO) Mean arterial pressure (MAP) Variable resistance (SVR) Aortic valve Left ventricle Elastic arteries / Aorta
Disclaimer. Improving MET-based patient care using treatment algorithms. Michael R. Pinsky, MD, Dr hc. Different Environments Demand Different Rules
 Michael R. Pinsky, MD - June 29, 26 Improving MET-based patient care using Michael R. Pinsky, MD, Dr hc Department of Critical Care Medicine University of Pittsburgh Disclaimer Michael R. Pinsky, MD is
Michael R. Pinsky, MD - June 29, 26 Improving MET-based patient care using Michael R. Pinsky, MD, Dr hc Department of Critical Care Medicine University of Pittsburgh Disclaimer Michael R. Pinsky, MD is
Fluid responsiveness and extravascular lung water
 Fluid responsiveness and extravascular lung water Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris-South France Conflicts of interest Member of the Medical Advisory Board of Maquet/Pulsion
Fluid responsiveness and extravascular lung water Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris-South France Conflicts of interest Member of the Medical Advisory Board of Maquet/Pulsion
Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy
 Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy A 44 year old female undergoing 10 hour Cytoreductive (CRS) procedure followed by Hyperthermic Intraperitoneal Chemotherapy (HIPEC).
Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy A 44 year old female undergoing 10 hour Cytoreductive (CRS) procedure followed by Hyperthermic Intraperitoneal Chemotherapy (HIPEC).
Effects of mechanical ventilation on organ function. Masterclass ICU nurses
 Effects of mechanical ventilation on organ function Masterclass ICU nurses Case Male, 60 - No PMH - L 1.74 m and W 85 kg Pneumococcal pneumonia Stable hemodynamics - No AKI MV in prone position (PEEP 16
Effects of mechanical ventilation on organ function Masterclass ICU nurses Case Male, 60 - No PMH - L 1.74 m and W 85 kg Pneumococcal pneumonia Stable hemodynamics - No AKI MV in prone position (PEEP 16
From PV loop to Starling curve. S Magder Division of Critical Care, McGill University Health Centre
 From PV loop to Starling curve S Magder Division of Critical Care, McGill University Health Centre Otto Frank 1890 s Frank-Starling Relationship ( The Law of the Heart ) The greater the initial stretch
From PV loop to Starling curve S Magder Division of Critical Care, McGill University Health Centre Otto Frank 1890 s Frank-Starling Relationship ( The Law of the Heart ) The greater the initial stretch
Pre-discussion questions
 Amanda Bartlett, PA-C Dustin Bartlett, PA-C Andrea Applegate, PA-C Leslie Yearta Brown, NP CHF Round Table Discussion Objectives ANDREA- Discuss the definition and different categories of CHF DUSTIN- Define
Amanda Bartlett, PA-C Dustin Bartlett, PA-C Andrea Applegate, PA-C Leslie Yearta Brown, NP CHF Round Table Discussion Objectives ANDREA- Discuss the definition and different categories of CHF DUSTIN- Define
Cardiac Output Monitoring - 6
 Cardiac Output Monitoring - 6 How to use Wrexham s Cardiac Output Monitors. Wrexham Maelor Critical Care Version 02.05.16 Introduction Types of Devices: NICOM - Cheetah Oesophageal Doppler +/- Pulse Contour
Cardiac Output Monitoring - 6 How to use Wrexham s Cardiac Output Monitors. Wrexham Maelor Critical Care Version 02.05.16 Introduction Types of Devices: NICOM - Cheetah Oesophageal Doppler +/- Pulse Contour
The Use of Dynamic Parameters in Perioperative Fluid Management
 The Use of Dynamic Parameters in Perioperative Fluid Management Gerard R. Manecke Jr., M.D. Chief, Cardiac Anesthesia UCSD Medical Center San Diego, CA, USA Thanks to Tom Higgins, M.D. 1 Goals of today
The Use of Dynamic Parameters in Perioperative Fluid Management Gerard R. Manecke Jr., M.D. Chief, Cardiac Anesthesia UCSD Medical Center San Diego, CA, USA Thanks to Tom Higgins, M.D. 1 Goals of today
Mechanical ventilation induced or exacerbated right ventricular failure
 Mechanical ventilation induced or exacerbated right ventricular failure Toronto 2016 Jesse Hall MD Professor of Medicine, Anesthesia & Critical Care University of Chicago Faculty Disclosures Dr. Hall
Mechanical ventilation induced or exacerbated right ventricular failure Toronto 2016 Jesse Hall MD Professor of Medicine, Anesthesia & Critical Care University of Chicago Faculty Disclosures Dr. Hall
Standard Operating Procedure (SOP) Management of intervention group patients SOP 001
 Management of intervention group patients SOP 001") ` Standard Operating Procedure (SOP) Management of intervention group patients SOP 001 Authors: Mark Edwards & Rupert Pearse Authorisation: Rupert Pearse (Chief Investigator) Scope To provide guidance
` Standard Operating Procedure (SOP) Management of intervention group patients SOP 001 Authors: Mark Edwards & Rupert Pearse Authorisation: Rupert Pearse (Chief Investigator) Scope To provide guidance
Jan M. Headley, R.N. BS
 Fluid First: Using PLR & SVV to Optimize Volume Jan M. Headley, R.N. BS Disclosure Director, Clinical Marketing & Professional Education Edwards Lifesciences Does this Patient NEED Fluid?? WE Have a Problem
Fluid First: Using PLR & SVV to Optimize Volume Jan M. Headley, R.N. BS Disclosure Director, Clinical Marketing & Professional Education Edwards Lifesciences Does this Patient NEED Fluid?? WE Have a Problem
Sepsis Combine experience and Evidence. Eran Segal, MD Director General ICU, Sheba Medical Center, Israel
 Sepsis Combine experience and Evidence Eran Segal, MD Director General ICU, Sheba Medical Center, Israel The Science of Sepsis A complex and diverse clinical entity Outcome is affected by: Infecting organism
Sepsis Combine experience and Evidence Eran Segal, MD Director General ICU, Sheba Medical Center, Israel The Science of Sepsis A complex and diverse clinical entity Outcome is affected by: Infecting organism
Vasoactive Medications. Matthew J. Korobey Pharm.D., BCCCP Critical Care Clinical Specialist Mercy St. Louis
 Vasoactive Medications Matthew J. Korobey Pharm.D., BCCCP Critical Care Clinical Specialist Mercy St. Louis Objectives List components of physiology involved in blood pressure Review terminology related
Vasoactive Medications Matthew J. Korobey Pharm.D., BCCCP Critical Care Clinical Specialist Mercy St. Louis Objectives List components of physiology involved in blood pressure Review terminology related
Nothing to Disclose. Severe Pulmonary Hypertension
 Severe Ronald Pearl, MD, PhD Professor and Chair Department of Anesthesiology Stanford University Rpearl@stanford.edu Nothing to Disclose 65 year old female Elective knee surgery NYHA Class 3 Aortic stenosis
Severe Ronald Pearl, MD, PhD Professor and Chair Department of Anesthesiology Stanford University Rpearl@stanford.edu Nothing to Disclose 65 year old female Elective knee surgery NYHA Class 3 Aortic stenosis
MANAGEMENT OF CIRCULATORY FAILURE
 MANAGEMENT OF CIRCULATORY FAILURE BACKGROUND AND DEFINITION There is no consensus on the definition of circulatory failure or shock in newborns; it can be defined as global tissue hypoxia secondary to
MANAGEMENT OF CIRCULATORY FAILURE BACKGROUND AND DEFINITION There is no consensus on the definition of circulatory failure or shock in newborns; it can be defined as global tissue hypoxia secondary to
TOPIC : Cardiogenic Shock
 University of Ferrara Department of Morphology, Surgery and Experimental Medicine. Section of Anaesthesia and Intensive Care Medicine TOPIC : Cardiogenic Shock What is shock? Shock is a condition of inadequate
University of Ferrara Department of Morphology, Surgery and Experimental Medicine. Section of Anaesthesia and Intensive Care Medicine TOPIC : Cardiogenic Shock What is shock? Shock is a condition of inadequate
Dr. F Javier Belda Dept. Anesthesiology and Critical Care Hospital Clinico Universitario Valencia (Spain) Pulsion MAB
 Pulsion MAB") State of the Art Hemodynamic Monitoring III CO, preload, lung water and ScvO2 The winning combination! Dr. F Javier Belda Dept. Anesthesiology and Critical Care Hospital Clinico Universitario Valencia
State of the Art Hemodynamic Monitoring III CO, preload, lung water and ScvO2 The winning combination! Dr. F Javier Belda Dept. Anesthesiology and Critical Care Hospital Clinico Universitario Valencia
Cardiovascular Management of Septic Shock
 Cardiovascular Management of Septic Shock R. Phillip Dellinger, MD Professor of Medicine Robert Wood Johnson Medical School/UMDNJ Director, Critical Care Medicine and Med/Surg ICU Cooper University Hospital
Cardiovascular Management of Septic Shock R. Phillip Dellinger, MD Professor of Medicine Robert Wood Johnson Medical School/UMDNJ Director, Critical Care Medicine and Med/Surg ICU Cooper University Hospital
Evolutionary origins of the right ventricle. S Magder Department of Critical Care, McGill University Health Centre
 Evolutionary origins of the right ventricle S Magder Department of Critical Care, McGill University Health Centre Fully separated four chamber heart only evolved in birds and mammals What are the evolutionary
Evolutionary origins of the right ventricle S Magder Department of Critical Care, McGill University Health Centre Fully separated four chamber heart only evolved in birds and mammals What are the evolutionary
Obligatory joke. The case for why it matters. Sepsis: More is more. Goal-Directed Fluid Resuscitation 6/1/2013
 Obligatory joke Keep your eye on the food. Goal-Directed Fluid Resuscitation Christopher G. Choukalas, MD, MS Department of Anesthesia and Perioperative Care University of California, San Francisco The
Obligatory joke Keep your eye on the food. Goal-Directed Fluid Resuscitation Christopher G. Choukalas, MD, MS Department of Anesthesia and Perioperative Care University of California, San Francisco The
Swans and Pressors. Vanderbilt Surgery Summer School Ricky Shinall
 Swans and Pressors Vanderbilt Surgery Summer School Ricky Shinall Shock, Swans, Pressors in 15 minutes 4 Reasons for Shock 4 Swan numbers to know 7 Pressors =15 things to know 4 Reasons for Shock Not enough
Swans and Pressors Vanderbilt Surgery Summer School Ricky Shinall Shock, Swans, Pressors in 15 minutes 4 Reasons for Shock 4 Swan numbers to know 7 Pressors =15 things to know 4 Reasons for Shock Not enough
Swans and Pressors. Vanderbilt Surgery Summer School Ricky Shinall
 Swans and Pressors Vanderbilt Surgery Summer School Ricky Shinall SHOCK Hypotension SHOCK Hypotension SHOCK=Reduction of systemic tissue perfusion, resulting in decreased oxygen delivery to the tissues.
Swans and Pressors Vanderbilt Surgery Summer School Ricky Shinall SHOCK Hypotension SHOCK Hypotension SHOCK=Reduction of systemic tissue perfusion, resulting in decreased oxygen delivery to the tissues.
Goal-directed resuscitation in sepsis; a case-based approach
 Goal-directed resuscitation in sepsis; a case-based approach Jorge A Guzman, MD, FCCM Head, Section Critical Care Medicine Respiratory Institute Cleveland Clinic Foundation The challenges to managing septic
Goal-directed resuscitation in sepsis; a case-based approach Jorge A Guzman, MD, FCCM Head, Section Critical Care Medicine Respiratory Institute Cleveland Clinic Foundation The challenges to managing septic
Swan Ganz catheter: Does it still have a role? Daniel De Backer Department of Intensive Care Erasme University Hospital Brussels, Belgium
 Swan Ganz catheter: Does it still have a role? Daniel De Backer Department of Intensive Care Erasme University Hospital Brussels, Belgium How can cardiac output be measured? Thermodilution Arterial waveform
Swan Ganz catheter: Does it still have a role? Daniel De Backer Department of Intensive Care Erasme University Hospital Brussels, Belgium How can cardiac output be measured? Thermodilution Arterial waveform
Case year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50
 Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
Topics to be Covered. Cardiac Measurements. Distribution of Blood Volume. Distribution of Pulmonary Ventilation & Blood Flow
 Topics to be Covered MODULE F HEMODYNAMIC MONITORING Cardiac Output Determinants of Stroke Volume Hemodynamic Measurements Pulmonary Artery Catheterization Control of Blood Pressure Heart Failure Cardiac
Topics to be Covered MODULE F HEMODYNAMIC MONITORING Cardiac Output Determinants of Stroke Volume Hemodynamic Measurements Pulmonary Artery Catheterization Control of Blood Pressure Heart Failure Cardiac
Using Functional Hemodynamic Indicators to Guide Fluid Therapy
 CE 2.6 HOURS Continuing Education Using Functional Hemodynamic Indicators to Guide Fluid Therapy A more accurate and less invasive way to gauge responsiveness to iv volume replacement. OVERVIEW: Hemodynamic
CE 2.6 HOURS Continuing Education Using Functional Hemodynamic Indicators to Guide Fluid Therapy A more accurate and less invasive way to gauge responsiveness to iv volume replacement. OVERVIEW: Hemodynamic
Introduction. Invasive Hemodynamic Monitoring. Determinants of Cardiovascular Function. Cardiovascular System. Hemodynamic Monitoring
 Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014
 December 17, 2014") Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
Dilemmas in Septic Shock
 Dilemmas in Septic Shock William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center A 62 year-old female presents to the ED with fever,
Dilemmas in Septic Shock William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center A 62 year-old female presents to the ED with fever,
Hemodynamic monitoring should be kept as simple as possible. But not simpler!
 Hemodynamic monitoring should be kept as simple as possible. But not simpler! Azriel Perel Professor and Chairman Department of Anesthesiology and Intensive Care Sheba Medical Center, Tel Aviv University,
Hemodynamic monitoring should be kept as simple as possible. But not simpler! Azriel Perel Professor and Chairman Department of Anesthesiology and Intensive Care Sheba Medical Center, Tel Aviv University,
Assessing Preload Responsiveness Using Arterial Pressure Based Technologies. Patricia A. Meehan, RN, MS Education Consultant Edwards Lifesciences, LLC
 Assessing Preload Responsiveness Using Arterial Pressure Based Technologies Patricia A. Meehan, RN, MS Education Consultant Edwards Lifesciences, LLC Content Description : Fluid administration is a first
Assessing Preload Responsiveness Using Arterial Pressure Based Technologies Patricia A. Meehan, RN, MS Education Consultant Edwards Lifesciences, LLC Content Description : Fluid administration is a first
Sepsis and septic shock Practical hemodynamic consequences. Intensive Care Training Program Radboud University Medical Centre Nijmegen
 Sepsis and septic shock Practical hemodynamic consequences Intensive Care Training Program Radboud University Medical Centre Nijmegen Septic cardiomyopathy Present in > 50% and often masked by low vascular
Sepsis and septic shock Practical hemodynamic consequences Intensive Care Training Program Radboud University Medical Centre Nijmegen Septic cardiomyopathy Present in > 50% and often masked by low vascular
The Pharmacology of Hypotension: Vasopressor Choices for HIE patients. Keliana O Mara, PharmD August 4, 2018
 The Pharmacology of Hypotension: Vasopressor Choices for HIE patients Keliana O Mara, PharmD August 4, 2018 Objectives Review the pathophysiology of hypotension in neonates Discuss the role of vasopressors
The Pharmacology of Hypotension: Vasopressor Choices for HIE patients Keliana O Mara, PharmD August 4, 2018 Objectives Review the pathophysiology of hypotension in neonates Discuss the role of vasopressors
Sepsis Wave II Webinar Series. Sepsis Reassessment
 Sepsis Wave II Webinar Series Sepsis Reassessment Presenters Nova Panebianco, MD Todd Slesinger, MD Fluid Reassessment in Sepsis Todd L. Slesinger, MD, FACEP, FCCM, FCCP, FAAEM Residency Program Director
Sepsis Wave II Webinar Series Sepsis Reassessment Presenters Nova Panebianco, MD Todd Slesinger, MD Fluid Reassessment in Sepsis Todd L. Slesinger, MD, FACEP, FCCM, FCCP, FAAEM Residency Program Director
Goal-directed vs Flow-guidedresponsive
 Goal-directed vs Flow-guidedresponsive therapy S Magder Department of Critical Care, McGill University Health Centre Flow-directed vs goal directed strategy for management of hemodynamics S Magder Curr
Goal-directed vs Flow-guidedresponsive therapy S Magder Department of Critical Care, McGill University Health Centre Flow-directed vs goal directed strategy for management of hemodynamics S Magder Curr
Impedance Cardiography (ICG) Application of ICG for Hypertension Management
 Application of ICG for Hypertension Management") Application of ICG for Hypertension Management 1mA @ 100 khz Impedance Cardiography (ICG) Non-invasive Beat-to-beat Hemodynamic Monitoring Diastole Systole Aortic valve is closed No blood flow in the aorta
Application of ICG for Hypertension Management 1mA @ 100 khz Impedance Cardiography (ICG) Non-invasive Beat-to-beat Hemodynamic Monitoring Diastole Systole Aortic valve is closed No blood flow in the aorta
The Role of the Anaesthesiologist in the Perioperative Management of Preeclampsia. RA Dyer Interlaken 2017
 The Role of the Anaesthesiologist in the Perioperative Management of Preeclampsia RA Dyer Interlaken 2017 6 In preeclampsia - Understanding of pathophysiology Assessment of disease severity Prediction
The Role of the Anaesthesiologist in the Perioperative Management of Preeclampsia RA Dyer Interlaken 2017 6 In preeclampsia - Understanding of pathophysiology Assessment of disease severity Prediction
Tailored Volume Resuscitation in the Critically Ill is Achievable. Objectives. Clinical Case 2/16/2018
 Tailored Volume Resuscitation in the Critically Ill is Achievable Heath E Latham, MD Associate Professor Fellowship Program Director Pulmonary and Critical Care Objectives Describe the goal of resuscitation
Tailored Volume Resuscitation in the Critically Ill is Achievable Heath E Latham, MD Associate Professor Fellowship Program Director Pulmonary and Critical Care Objectives Describe the goal of resuscitation
Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI)
") Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI) Robert W. Schrier, MD University of Colorado School of Medicine Denver, Colorado USA Prevalence of acute renal failure in Intensive
Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI) Robert W. Schrier, MD University of Colorado School of Medicine Denver, Colorado USA Prevalence of acute renal failure in Intensive
Bedside assessment of fluid status
 Bedside assessment of fluid status 2nd AKI Academy October 18 th 2014 David Treacher Guy s & St Thomas NHS Trust Assessing the circulation - the 3 key questions v Is my patient adequately filled? v What
Bedside assessment of fluid status 2nd AKI Academy October 18 th 2014 David Treacher Guy s & St Thomas NHS Trust Assessing the circulation - the 3 key questions v Is my patient adequately filled? v What
Evidence-Based. Management of Severe Sepsis. What is the BP Target?
 Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Permissive hypoxaemia. Mervyn Singer Bloomsbury Institute of Intensive Care Medicine University College London, UK
 Permissive hypoxaemia Mervyn Singer Bloomsbury Institute of Intensive Care Medicine University College London, UK Is mechanical ventilation such a good idea? ventilator-induced lung injury (short- & long-term)
Permissive hypoxaemia Mervyn Singer Bloomsbury Institute of Intensive Care Medicine University College London, UK Is mechanical ventilation such a good idea? ventilator-induced lung injury (short- & long-term)
Case scenario V AV ECMO. Dr Pranay Oza
 Case scenario V AV ECMO Dr Pranay Oza Case Summary 53 y/m, k/c/o MVP with myxomatous mitral valve with severe Mitral regurgitation underwent Mitral valve replacement with mini thoracotomy Pump time nearly
Case scenario V AV ECMO Dr Pranay Oza Case Summary 53 y/m, k/c/o MVP with myxomatous mitral valve with severe Mitral regurgitation underwent Mitral valve replacement with mini thoracotomy Pump time nearly
Wet Lungs Dry lungs Impact on Outcome in ARDS. Charlie Phillips MD Division of PCCM OHSU 2009
 Wet Lungs Dry lungs Impact on Outcome in ARDS Charlie Phillips MD Division of PCCM OHSU 2009 Today s talk Pathophysiology of ARDS The case for dry Targeting EVLW Disclosures Advisor for Pulsion Medical
Wet Lungs Dry lungs Impact on Outcome in ARDS Charlie Phillips MD Division of PCCM OHSU 2009 Today s talk Pathophysiology of ARDS The case for dry Targeting EVLW Disclosures Advisor for Pulsion Medical
Albumina nel paziente critico. Savona 18 aprile 2007
 Albumina nel paziente critico Savona 18 aprile 2007 What Is Unique About Critical Care RCTs patients eligibility is primarily defined by location of care in the ICU rather than by the presence of a specific
Albumina nel paziente critico Savona 18 aprile 2007 What Is Unique About Critical Care RCTs patients eligibility is primarily defined by location of care in the ICU rather than by the presence of a specific
Sepsis and septic shock
 Sepsis and septic shock Practical hemodynamic consequences Intensive Care Training Program Radboud University Medical Centre Nijmegen Septic cardiomyopathy Present in > 50% and often masked by low vascular
Sepsis and septic shock Practical hemodynamic consequences Intensive Care Training Program Radboud University Medical Centre Nijmegen Septic cardiomyopathy Present in > 50% and often masked by low vascular
Heart Pump and Cardiac Cycle. Faisal I. Mohammed, MD, PhD
 Heart Pump and Cardiac Cycle Faisal I. Mohammed, MD, PhD 1 Objectives To understand the volume, mechanical, pressure and electrical changes during the cardiac cycle To understand the inter-relationship
Heart Pump and Cardiac Cycle Faisal I. Mohammed, MD, PhD 1 Objectives To understand the volume, mechanical, pressure and electrical changes during the cardiac cycle To understand the inter-relationship
DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE
 DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE Mefri Yanni, MD Bagian Kardiologi dan Kedokteran Vaskular RS.DR.M.Djamil Padang The 3rd Symcard Padang, Mei 2013 Outline Diagnosis Diagnosis Treatment options
DIAGNOSIS AND MANAGEMENT OF ACUTE HEART FAILURE Mefri Yanni, MD Bagian Kardiologi dan Kedokteran Vaskular RS.DR.M.Djamil Padang The 3rd Symcard Padang, Mei 2013 Outline Diagnosis Diagnosis Treatment options
Percutaneous Mechanical Circulatory Support for Cardiogenic Shock. 24 th Annual San Diego Heart Failure Symposium Ryan R Reeves, MD FSCAI
 Percutaneous Mechanical Circulatory Support for Cardiogenic Shock 24 th Annual San Diego Heart Failure Symposium Ryan R Reeves, MD FSCAI The Need for Circulatory Support Basic Pathophysiologic Problems:
Percutaneous Mechanical Circulatory Support for Cardiogenic Shock 24 th Annual San Diego Heart Failure Symposium Ryan R Reeves, MD FSCAI The Need for Circulatory Support Basic Pathophysiologic Problems:
SHOCK and the Trauma Victim. JP Pretorius Department of Surgery & SICU Steve Biko Academic Hospital.
 SHOCK and the Trauma Victim JP Pretorius Department of Surgery & SICU Steve Biko Academic Hospital. Classification of Shock Cardiogenic - Myopathic Arrythmic Mechanical Hypovolaemic - Haemorrhagic Non-haemorrhagic
SHOCK and the Trauma Victim JP Pretorius Department of Surgery & SICU Steve Biko Academic Hospital. Classification of Shock Cardiogenic - Myopathic Arrythmic Mechanical Hypovolaemic - Haemorrhagic Non-haemorrhagic
A case of post myocardial infarction ventricular septal rupture CHRISTOFOROS KOBOROZOS, MD
 A case of post myocardial infarction ventricular septal rupture CHRISTOFOROS KOBOROZOS, MD NAVAL HOSPITAL OF ATHENS case presentation Female, 81yo Hx: diabetes mellitus, hypertension, chronic anaemia presented
A case of post myocardial infarction ventricular septal rupture CHRISTOFOROS KOBOROZOS, MD NAVAL HOSPITAL OF ATHENS case presentation Female, 81yo Hx: diabetes mellitus, hypertension, chronic anaemia presented
Acute Liver Failure: Supporting Other Organs
 Acute Liver Failure: Supporting Other Organs Michael A. Gropper, MD, PhD Professor of Anesthesia and Physiology Director, Critical Care Medicine University of California San Francisco Acute Liver Failure
Acute Liver Failure: Supporting Other Organs Michael A. Gropper, MD, PhD Professor of Anesthesia and Physiology Director, Critical Care Medicine University of California San Francisco Acute Liver Failure
Impedance Cardiography (ICG) Application of ICG in Intensive Care and Emergency
 Application of ICG in Intensive Care and Emergency") Impedance Cardiography (ICG) Application of ICG in Intensive Care and Emergency Aim of haemodynamic monitoring in ICU and ED Detection and therapy of insufficient organ perfusion Answers to common cardiovascular
Impedance Cardiography (ICG) Application of ICG in Intensive Care and Emergency Aim of haemodynamic monitoring in ICU and ED Detection and therapy of insufficient organ perfusion Answers to common cardiovascular
THE CARDIOVASCULAR SYSTEM
 THE CARDIOVASCULAR SYSTEM AND RESPONSES TO EXERCISE Mr. S. Kelly PSK 4U North Grenville DHS THE HEART: A REVIEW Cardiac muscle = myocardium Heart divided into two sides, 4 chambers (L & R) RS: pulmonary
THE CARDIOVASCULAR SYSTEM AND RESPONSES TO EXERCISE Mr. S. Kelly PSK 4U North Grenville DHS THE HEART: A REVIEW Cardiac muscle = myocardium Heart divided into two sides, 4 chambers (L & R) RS: pulmonary
Radboud University Nijmegen Medical Centre Why measure cardiac output in critically ill children?
 Radboud University Nijmegen Medical Centre Why measure cardiac output in critically ill children? J. Lemson Anesthesiologist/(pediatric)intensivist Case; Girl 2 years, 12 kg, severe meningococcal septic
Radboud University Nijmegen Medical Centre Why measure cardiac output in critically ill children? J. Lemson Anesthesiologist/(pediatric)intensivist Case; Girl 2 years, 12 kg, severe meningococcal septic
Mon patient a une bonne pression artérielle il a a donc un bon débit cardiaque! seminaires iris. Daniel De Backer
 Mon patient a une bonne pression artérielle il a a donc un bon débit cardiaque! Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles
Mon patient a une bonne pression artérielle il a a donc un bon débit cardiaque! Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles
How can the PiCCO improve protocolized care?
 How can the PiCCO improve protocolized care? Azriel Perel Professor and Chairman Department of Anesthesiology and Intensive Care Sheba Medical Center, Tel Aviv University, Israel ESICM, Vienna 2009 Disclosure
How can the PiCCO improve protocolized care? Azriel Perel Professor and Chairman Department of Anesthesiology and Intensive Care Sheba Medical Center, Tel Aviv University, Israel ESICM, Vienna 2009 Disclosure
Cardiac Output (C.O.) Regulation of Cardiac Output
 Regulation of Cardiac Output") Cardiac Output (C.O.) Is the volume of the blood pumped by each ventricle per minute (5 Litre) Stroke volume: Is the volume of the blood pumped by each ventricle per beat. Stroke volume = End diastolic
Cardiac Output (C.O.) Is the volume of the blood pumped by each ventricle per minute (5 Litre) Stroke volume: Is the volume of the blood pumped by each ventricle per beat. Stroke volume = End diastolic
Cardiogenic shock: Current management
 Cardiogenic shock: Current management Janine Pöss Universitätsklinikum des Saarlandes Klinik für Innere Medizin III Kardiologie, Angiologie und internistische Intensivmedizin Homburg/Saar I have nothing
Cardiogenic shock: Current management Janine Pöss Universitätsklinikum des Saarlandes Klinik für Innere Medizin III Kardiologie, Angiologie und internistische Intensivmedizin Homburg/Saar I have nothing
Rounds in the ICU. Eran Segal, MD Director General ICU Sheba Medical Center
 Rounds in the ICU Eran Segal, MD Director General ICU Sheba Medical Center Real Clinical cases (including our mistakes) Emphasis on hemodynamic monitoring Usually no single correct answer We will conduct
Rounds in the ICU Eran Segal, MD Director General ICU Sheba Medical Center Real Clinical cases (including our mistakes) Emphasis on hemodynamic monitoring Usually no single correct answer We will conduct
Surviving Sepsis Campaign Guidelines 2012 & Update for David E. Tannehill, DO Critical Care Medicine Mercy Hospital St.
 Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
The right heart: the Cinderella of heart failure
 The right heart: the Cinderella of heart failure Piotr Ponikowski, MD, PhD, FESC Medical University, Centre for Heart Disease Clinical Military Hospital Wroclaw, Poland none Disclosure Look into the Heart
The right heart: the Cinderella of heart failure Piotr Ponikowski, MD, PhD, FESC Medical University, Centre for Heart Disease Clinical Military Hospital Wroclaw, Poland none Disclosure Look into the Heart
Hemodynamic monitoring beyond cardiac output
 Hemodynamic monitoring beyond cardiac output Prof Xavier MONNET Medical Intensive Care Unit Bicêtre Hospital Assistance publique Hôpitaux de Paris FRANCE Conflicts of interest Lilly GlaxoSmithKline Pulsion
Hemodynamic monitoring beyond cardiac output Prof Xavier MONNET Medical Intensive Care Unit Bicêtre Hospital Assistance publique Hôpitaux de Paris FRANCE Conflicts of interest Lilly GlaxoSmithKline Pulsion
Disclosures. ICU Management of Advanced Lung Disease 5/9/2015. No Disclosures. All pictures from commercial sources
 Disclosures ICU Management of Advanced Lung Disease No Disclosures All pictures from commercial sources Lundy J. Campbell, MD UCSF Department of Anesthesia and Perioperative Care Division of Critical Care
Disclosures ICU Management of Advanced Lung Disease No Disclosures All pictures from commercial sources Lundy J. Campbell, MD UCSF Department of Anesthesia and Perioperative Care Division of Critical Care
Shock Quiz! By Clare Di Bona
 Shock Quiz! By Clare Di Bona Test Question What is Mr Burns full legal name? Answer Charles Montgomery Plantagenet Schicklgruber Burns. (Season 22, episode 11) Question 1. What is the definition of shock?
Shock Quiz! By Clare Di Bona Test Question What is Mr Burns full legal name? Answer Charles Montgomery Plantagenet Schicklgruber Burns. (Season 22, episode 11) Question 1. What is the definition of shock?
HOW LOW CAN YOU GO? HYPOTENSION AND THE ANESTHETIZED PATIENT.
 HOW LOW CAN YOU GO? HYPOTENSION AND THE ANESTHETIZED PATIENT. Donna M. Sisak, CVT, LVT, VTS (Anesthesia/Analgesia) Seattle Veterinary Specialists Kirkland, WA dsisak@svsvet.com THE ANESTHETIZED PATIENT
HOW LOW CAN YOU GO? HYPOTENSION AND THE ANESTHETIZED PATIENT. Donna M. Sisak, CVT, LVT, VTS (Anesthesia/Analgesia) Seattle Veterinary Specialists Kirkland, WA dsisak@svsvet.com THE ANESTHETIZED PATIENT
HAEMODYNAMIC DYSFUNCTION AFTER ABDOMINAL AORTIC ANEURYSM REPAIR
 1 HAEMODYNAMIC DYSFUNCTION AFTER ABDOMINAL AORTIC ANEURYSM REPAIR M Blunt & N Barber CASE SCENARIO A 72-year-old man is admitted directly to the intensive care unit (ICU) following emergency abdominal
1 HAEMODYNAMIC DYSFUNCTION AFTER ABDOMINAL AORTIC ANEURYSM REPAIR M Blunt & N Barber CASE SCENARIO A 72-year-old man is admitted directly to the intensive care unit (ICU) following emergency abdominal
Haemodynamics. Milan Chovanec Department of Physiology 2.LF UK
 Haemodynamics Milan Chovanec Department of Physiology 2.LF UK Major types of blood vessels Blood flow: 50cm/s 0.05cm/s Flow, pressure, resistance Flow, pressure, resistance ΔU = I x R Blood and vessels
Haemodynamics Milan Chovanec Department of Physiology 2.LF UK Major types of blood vessels Blood flow: 50cm/s 0.05cm/s Flow, pressure, resistance Flow, pressure, resistance ΔU = I x R Blood and vessels
Disclosure Information : No conflict of interest
 Intravenous nicorandil improves symptoms and left ventricular diastolic function immediately in patients with acute heart failure : a randomized, controlled trial M. Shigekiyo, K. Harada, A. Okada, N.
Intravenous nicorandil improves symptoms and left ventricular diastolic function immediately in patients with acute heart failure : a randomized, controlled trial M. Shigekiyo, K. Harada, A. Okada, N.
Cardiac Output MCQ. Professor of Cardiovascular Physiology. Cairo University 2007
 Cardiac Output MCQ Abdel Moniem Ibrahim Ahmed, MD Professor of Cardiovascular Physiology Cairo University 2007 90- Guided by Ohm's law when : a- Cardiac output = 5.6 L/min. b- Systolic and diastolic BP
Cardiac Output MCQ Abdel Moniem Ibrahim Ahmed, MD Professor of Cardiovascular Physiology Cairo University 2007 90- Guided by Ohm's law when : a- Cardiac output = 5.6 L/min. b- Systolic and diastolic BP
Echocardiography Volume assessment. Justin Mandeville 2014
 Echocardiography Volume assessment Justin Mandeville 2014 Volume assessment and the intensivist Hypovolaemic shock Fluid tolerance Optimising cardiac output Avoiding overloading Guided fluid removal Add
Echocardiography Volume assessment Justin Mandeville 2014 Volume assessment and the intensivist Hypovolaemic shock Fluid tolerance Optimising cardiac output Avoiding overloading Guided fluid removal Add
Review of Cardiac Mechanics & Pharmacology 10/23/2016. Brent Dunworth, CRNA, MSN, MBA 1. Learning Objectives
 Brent Dunworth, CRNA, MSN, MBA Associate Director of Advanced Practice Division Chief, Nurse Anesthesia Vanderbilt University Medical Center Nashville, Tennessee Learning Objectives Review the principles
Brent Dunworth, CRNA, MSN, MBA Associate Director of Advanced Practice Division Chief, Nurse Anesthesia Vanderbilt University Medical Center Nashville, Tennessee Learning Objectives Review the principles
การอบรมว ทยาศาสตร พ นฐานทางศ ลยศาสตร เร อง นพ.ส ณฐ ต โมราก ล ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร โรงพยาบาลรามาธ บด มหาวทยาลยมหดล
 การอบรมว ทยาศาสตร พ นฐานทางศ ลยศาสตร เร อง นพ.ส ณฐ ต โมราก ล ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร โรงพยาบาลรามาธ บด มหาวทยาลยมหดล Distributive shock Severe sepsis and Septic shock Anaphylactic shock Neurogenic
การอบรมว ทยาศาสตร พ นฐานทางศ ลยศาสตร เร อง นพ.ส ณฐ ต โมราก ล ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร โรงพยาบาลรามาธ บด มหาวทยาลยมหดล Distributive shock Severe sepsis and Septic shock Anaphylactic shock Neurogenic
The Hypotensive Poisoned Patient. Robert S. Hoffman, MD Director, NYC PCC
 The Hypotensive Poisoned Patient Robert S. Hoffman, MD Director, NYC PCC Some Definitions Hypotension = Low blood pressure Failure of macrocirculation Shock = Poor tissue perfusion Failure of microcirculation
The Hypotensive Poisoned Patient Robert S. Hoffman, MD Director, NYC PCC Some Definitions Hypotension = Low blood pressure Failure of macrocirculation Shock = Poor tissue perfusion Failure of microcirculation
Definition- study of blood flow Haemodynamic monitoring refers to monitoring of blood in the cardiovascular system Uses Is NB in the critically ill
 By Craig Definition- study of blood flow Haemodynamic monitoring refers to monitoring of blood in the cardiovascular system Uses Is NB in the critically ill pt Can assist diagnosis and decision making
By Craig Definition- study of blood flow Haemodynamic monitoring refers to monitoring of blood in the cardiovascular system Uses Is NB in the critically ill pt Can assist diagnosis and decision making
SHOCK. Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital
 SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
Sepsis Update: Focus on Early Recognition and Intervention. Disclosures
 Sepsis Update: Focus on Early Recognition and Intervention Jessie Roske, MD October 2017 Disclosures I have no actual or potential conflict of interest in relation to this program/presentation. I will
Sepsis Update: Focus on Early Recognition and Intervention Jessie Roske, MD October 2017 Disclosures I have no actual or potential conflict of interest in relation to this program/presentation. I will
Full Disclosure. The case for why it matters. Goal-directed Fluid Resuscitation
 Goal-directed Fluid Resuscitation Christopher G. Choukalas, MD, MS Department of Anesthesia and Perioperative Care University of California, San Francisco I own no stocks Full Disclosure The case for why
Goal-directed Fluid Resuscitation Christopher G. Choukalas, MD, MS Department of Anesthesia and Perioperative Care University of California, San Francisco I own no stocks Full Disclosure The case for why
9/13/2015. Laboratory. HPI and PE
 Critical Care HPI and PE 74 yo male confused SBP 90/20 MAP50, P 122, RR 34 Ox1 w/o nuchal rigidity S1S2 wo m RLL reduced breath sounds Skin warm dry Laboratory» WBC 15,600 Hgb 8.4 HCt 23%, Plts 95000,
Critical Care HPI and PE 74 yo male confused SBP 90/20 MAP50, P 122, RR 34 Ox1 w/o nuchal rigidity S1S2 wo m RLL reduced breath sounds Skin warm dry Laboratory» WBC 15,600 Hgb 8.4 HCt 23%, Plts 95000,
E/Ea is NOT an essential estimator of LV filling pressures
 Euroecho Kopenhagen Echo in Resynchronization in 2010 E/Ea is NOT an essential estimator of LV filling pressures Wilfried Mullens, MD, PhD December 10, 2010 Ziekenhuis Oost Limburg Genk University Hasselt
Euroecho Kopenhagen Echo in Resynchronization in 2010 E/Ea is NOT an essential estimator of LV filling pressures Wilfried Mullens, MD, PhD December 10, 2010 Ziekenhuis Oost Limburg Genk University Hasselt
Mechanical Ventilation & Cardiopulmonary Interactions: Clinical Application in Non- Conventional Circulations. Eric M. Graham, MD
 Mechanical Ventilation & Cardiopulmonary Interactions: Clinical Application in Non- Conventional Circulations Eric M. Graham, MD Background Heart & lungs work to meet oxygen demands Imbalance between supply
Mechanical Ventilation & Cardiopulmonary Interactions: Clinical Application in Non- Conventional Circulations Eric M. Graham, MD Background Heart & lungs work to meet oxygen demands Imbalance between supply
Organ Donor Management Recommended Guidelines ADULT CARDIAC DEATH (DCD)
") Date: Time: = Always applicable = Check if applicable ADMISSION INSTRUCTIONS Move to Comfort Care Note in chart. Contact initiated with BC Transplant Consent for Organ Donation obtained Code Status: Full
Date: Time: = Always applicable = Check if applicable ADMISSION INSTRUCTIONS Move to Comfort Care Note in chart. Contact initiated with BC Transplant Consent for Organ Donation obtained Code Status: Full
During exercise the heart rate is 190 bpm and the stroke volume is 115 ml/beat. What is the cardiac output?
 The Cardiovascular System Part III: Heart Outline of class lecture After studying part I of this chapter you should be able to: 1. Be able to calculate cardiac output (CO) be able to define heart rate
The Cardiovascular System Part III: Heart Outline of class lecture After studying part I of this chapter you should be able to: 1. Be able to calculate cardiac output (CO) be able to define heart rate
EARLY GOAL DIRECTED THERAPY : seminaires iris. Etat des lieux en Daniel De Backer
 EARLY GOAL DIRECTED THERAPY : Etat des lieux en 2017 Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles Past-President European
EARLY GOAL DIRECTED THERAPY : Etat des lieux en 2017 Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles Past-President European
Impact of Nicorandil on Renal Function in Patients With Acute Heart Failure and Pre-Existing Renal Dysfunction
 Impact of Nicorandil on Renal Function in Patients With Acute Heart Failure and Pre-Existing Renal Dysfunction Masahito Shigekiyo, Kenji Harada, Ayumi Okada, Naho Terada, Hiroyoshi Yoshikawa, Akira Hirono,
Impact of Nicorandil on Renal Function in Patients With Acute Heart Failure and Pre-Existing Renal Dysfunction Masahito Shigekiyo, Kenji Harada, Ayumi Okada, Naho Terada, Hiroyoshi Yoshikawa, Akira Hirono,
Shock and hemodynamic monitorization. Nilüfer Yalındağ Öztürk Marmara University Pendik Research and Training Hospital
 Shock and hemodynamic monitorization Nilüfer Yalındağ Öztürk Marmara University Pendik Research and Training Hospital Shock Leading cause of morbidity and mortality Worldwide: dehydration and hypovolemic
Shock and hemodynamic monitorization Nilüfer Yalındağ Öztürk Marmara University Pendik Research and Training Hospital Shock Leading cause of morbidity and mortality Worldwide: dehydration and hypovolemic
How and why I give IV fluid Disclosures SCA Fluids and public health 4/1/15. Andrew Shaw MB FRCA FCCM FFICM
 How and why I give IV fluid Andrew Shaw MB FRCA FCCM FFICM Professor and Chief Cardiothoracic Anesthesiology Vanderbilt University Medical Center 2015 Disclosures Consultant for Grifols manufacturer of
How and why I give IV fluid Andrew Shaw MB FRCA FCCM FFICM Professor and Chief Cardiothoracic Anesthesiology Vanderbilt University Medical Center 2015 Disclosures Consultant for Grifols manufacturer of