Preload optimisation in severe sepsis and septic shock
|
|
|
- Hilary Cooper
- 5 years ago
- Views:
Transcription


1 Preload optimisation in severe sepsis and septic shock Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris South France
2 Conflicts of interest Member of themedical Advisory Board ofpulsion
3 Decision of starting fluid administration presence of hemodynamic instability/peripheral hypoperfusion (mottled skin, hypotension, oliguria, hyperlactatemia ) and presence of preload responsiveness and limited risks of fluid overload
4 Fluid Challenge Predictors of fluid responsiveness/unresponsiveness
5 Crit Care Med 2006; 34: Rate of infusion: ml crystalloids or ml colloids over 30 mins Goal:reversal of themarker of perfusion failurethat prompted the fluid challenge (ex: hypotension, tachycardia, oliguria, etc) Safety limits:cvpof 15 mmhg measured every 10 mins
6 Crit Care Med 2006; 34: Limitations Fluid challenge cannot serve as a test to predict fluid responsiveness First, it isnot a test but areal therapy ml crystalloids or ml colloids/30 mins Not negligible amounts! Second, by definition, itcannot predictfluid responsiveness Fluid challenge is successful in only 50% cases

7 CHEST 2002, 121:2000-8
8 Crit Care Med 2006; 34: Limitations Fluid challenge cannot serve as a test to predict fluid responsiveness First, it isnot a test but areal therapy ml crystalloids or ml colloids/30 mins Not negligible amounts! Second, by definition, itcannot predictfluid responsiveness Fluid challenge is successful in only 50% cases Fluid challenge is potentiallyrisky Assessing fluid responsiveness is a «every day» issue Repetition of fluid challenges could be harmful
9
10 Tento obrázek nyní nelze zobrazit. Tento obrázek nyní nelze zobrazit.

11

12 Fluid Challenge Predictors of fluid responsiveness/unresponsiveness Can help to choose the best fluid strategy by avoiding to fluid overload patients who would be fluid unresponsive
13 Fluid infusion will increase LV stroke volume only ifboth ventricles arepreload responsive preload unresponsiveness Stroke Volume Fluid responsiveness equivalent to preload responsiveness biventricular preload responsiveness Ventricular preload
14 Fluid Challenge Predictors of fluid responsiveness/unresponsiveness Static markers of preload
15 normal heart Stroke volume preload responsiveness «static» measures ofpreload cannot reliablypredict fluid responsiveness. preload unresponsiveness failing heart Ventricular preload
16 Tento obrázek nyní nelze zobrazit. neither baseline PAOP nor baseline CVP predicted volume responsiveness Responders Nonresponders Responders Nonresponders

17 Tento obrázek nyní nelze zobrazit. Tento obrázek nyní nelze zobrazit. Tento obrázek nyní nelze zobrazit. Tento obrázek nyní nelze zobrazit. Crit Care Med 2013; 41: pts Summary AUC 0.56 Crit Care Med 2013; 41:
18 Tento obrázek nyní nelze zobrazit.???
19 Dynamic indices of preload responsiveness normal heart Stroke volume preload responsiveness failing heart. preload unresponsiveness Ventricular preload
20 Fluid Challenge Predictors of fluid responsiveness/unresponsiveness Static markers of preload Dynamic markers of preload responsiveness o heart-lung interaction tests o variability of stroke volume and of its surrogates
21 MV induces cyclic changes in SV only in pts with biventricular preload responsiveness fluid responsiveness occurs only in pts with biventricular preload responsiveness correlates with the magnitude of the induced by
22 Fluid Challenge Predictors of fluid responsiveness/unresponsiveness Static markers of preload Dynamic markers of preload responsiveness o heart-lung interaction tests o variability of stroke volume and of its surrogates Invasive indices
23 Tento obrázek nyní nelze zobrazit. Stroke volume preload responsiveness preload unresponsiveness A B Ventricular preload

24 Tento obrázek nyní nelze zobrazit. Am J Respir Crit Care Med 2000; 162:134-8 PPV = PPmax- PPmin (PPmax +PPmin) /2 Arterial catheter PPmax PPmin
25 PP (%) before fluid Infusion 13 % non-responders n = responders n = 16
26 PPV Sensitivity CVP PAOP 1 -Specificity








27 Chest 2005;128; Anesth Analg 2011; 113:523-8 Chest 2004, 126: PPV Crit Care Med 2005;33: Tento obrázek ny ní nelze zobrazit. M. Cannesson, J. Slieker, O. Desebbe, F. Fahdi,O. Bastien, JJ. Lehot Tento obrázek ny ní nelze zobrazit. Tento obrázek ny ní nelze zobrazit. X. Monnet1,2*, L. Guerin1,2, M. Jozwiak1,2, A. Bataille1,2, F. Julien1,2, C. Richard1,2, J-L. Teboul1,2 Tento obrázek ny ní nelze zobrazit.

28
29 The larger the PPbeforefluid infusion, the larger the increase in Am CO J Respir Crit after Care Med 2000; fluid 162:134-8 infusion Fluid-induced changes in cardiac index (%) r 2 = The smallerthe PPVbefore fluid infusion, PP (%) before fluid infusion the smaller the increase in CO after fluid infusion





30 Pulse Pressure Variation Calculated automatically and displayed in real-time by usual hemodynamic monitors All thesemonitors aresuitable todisplay PPV in real-time


31 Arterial pressure waveform analysis Stroke volume Arterial Pressure Stroke Volume Variation Calculated automatically anddisplayed inreal-time by new hemodynamic monitors











32 X. Monnet1,2*, L. Guerin1,2, M. Jozwiak1,2, A. Bataille1,2,F. Julien1,2, C. Richard1,2, J-L. Teboul1,2 Assessing fluid responsiveness by stroke volume variation in mechanically ventilated patients with severe sepsis G. Marx, T. Cope, L. McCrossan, S. Swaraj, C. Cowan, SM. Mostafa, R. Wenstone, M. Leuwer European Journal of Anaesthesiology 2004; 21: Chest 2005;128;
33 PPV SVV 685 pts

34 Average cut-off: 12.5%
35 Fluid Challenge Predictors of fluid responsiveness/unresponsiveness Static markers of preload Dynamic markers of preload responsiveness o heart-lung interaction tests o variability of stroke volume and of its surrogates Invasive indices Non invasive indices

36 PPVi PPVni Non-invasive finger blood pressure monitoring device
37 Esophageal Doppler 18% ABF % = ABF max-abf min (ABF max+ ABF min)/2 R NR
 / 2 4 responders non")
38 Doppler-echo Vpeak Vpeak (%) before fluid Vpeak max Vpeak min Vpeak = Vpeak max Vpeak min (Vpeak max + Vpeak min) / 2 4 responders non responders

39 Pulse oximeter

40

41 PPV SVV PVI GEDV
42 NE (-) NE (+)
43 Fluid Challenge Predictors of fluid responsiveness/unresponsiveness Static markers of preload Dynamic markers of preload responsiveness o heart-lung interaction tests o variability of stroke volume and of its surrogates o variability of (inferior or superior) vena cava diameter


44 Subcostal view divcmin divcmax divc% = divcmax-divcmin (divcmax + divcmin)/2


45 66 pts with MV Systematic fluid loading with 10 ml/kg HES
46 36 % 100 SVC collapsibility (AUC: 0.99) 80 PPV 12% (AUC: 0.94) Specificity (%) PPV and SVC collapsibility perform equally for predicting fluid responsiveness Transesophageal approach is required Specificity (%)
47 Limitations of respiratory variability indices impossible to interpret in pts with spontaneous breathing activity
48 PPV (threshold: 12 %) fully adapted to ventilator patients with spontaneous breathing sensitivity PPV 1 -specificity
49 Limitations of respiratory variability indices impossible to interpret in pts with spontaneous breathing activity impossible to interpret in patients with arrhythmias mmhg 110 PPmax PPmin
50 Limitations of respiratory variability indices impossible to interpret in pts with spontaneous breathing activity impossible to interpret in patients with arrhythmias difficult to interpret if tidal volume is too low
51 PPV 12.8 % PPV 8 % Sensitivity Normal TV Low TV 1- Specificity
52 Limitations of respiratory variability indices impossible to interpret in pts with spontaneous breathing activity impossible to interpret in patients with arrhythmias difficult to interpret if tidal volume is too low difficult to interpret if lung compliance is too low
53 Ability of PPV to predict fluid responsiveness in function of lung compliance Crs 40 ml/cmh 2 O Sensitivity Crs < 40 ml/cmh 2 O Crs < 30 ml/cmh 2 O Specificity (%)
54 Limitations of respiratory variability indices impossible to interpret in pts with spontaneous breathing activity impossible to interpret in patients with arrhythmias difficult to interpret if tidal volume is too low difficult to interpret if lung compliance is too low difficult to interpret in case of high frequency ventilation PPV can be not reliable when the heart rate/respiratory rate is> 3.6 De Backer et al Anesthesiology 2009
55 Limitations of respiratory variability indices impossible to interpret in pts with spontaneous breathing activity impossible to interpret in patients with arrhythmias difficult to interpret if tidal volume is too low difficult to interpret if lung compliance is too low difficult to interpret in case of high frequency ventilation difficult to interpret under open-chest conditions difficult to interpret in case of severe RV failure Mahjoub et al Crit Care Med 2009, Wyler von Ballmoos et al Crit Care 2010
56 Limitations of respiratory variability indices impossible to interpret in pts with spontaneous breathing activity impossible to interpret in patients with arrhythmias difficult to interpret if tidal volume is too low difficult to interpret if lung compliance is too low difficult to interpret in case of high frequency ventilation difficult to interpret under open-chest conditions In all these situations and in case of any doubt about interpretation other reliable dynamic tests are required difficult to interpret in case of severe RV failure and are now available
57 Fluid Challenge Predictors of fluid responsiveness/unresponsiveness Static markers of preload Dynamic markers of preload responsiveness o heart-lung interaction tests o variability of stroke volume and of its surrogates o variability of (inferior or superior) vena cava diameter o end-expiratory occlusion test


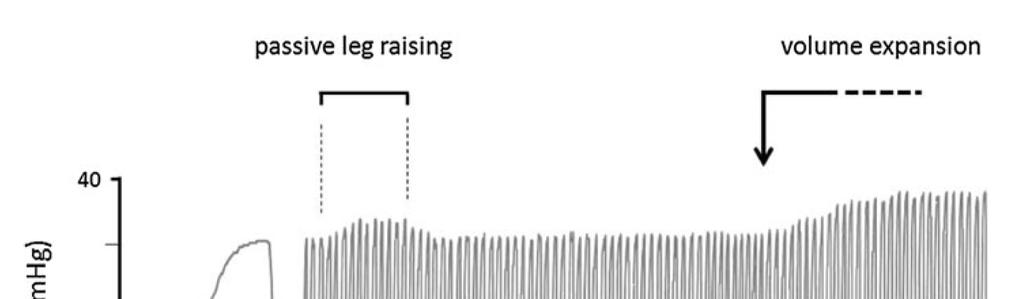
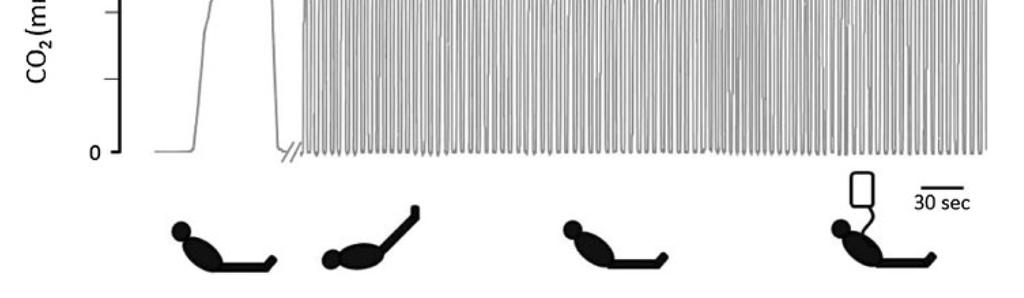
58 End-expiratory occlusion test Cyclic decrease in preload Transient increase in preload and hence in CO in case of preload-dependency Fluid responders should be identified by anincrease of theirco during theend-expiration occlusion test Systemic venous return

59 % 50 effects ofend-expiratory occlusion on Pulse contour CO % 50 effects ofend-expiratory occlusion on pulse pressure Any real-time CO monitor could be suitable A simple arterial catheter could be suitable NR R -10 NR R
60
61 Fluid Challenge Predictors of fluid responsiveness/unresponsiveness Static markers of preload Dynamic markers of preload responsiveness o heart-lung interaction tests o variability of stroke volume and of its surrogates o variability of (inferior or superior) vena cava diameter o end-expiratory occlusion test o passive leg raising test


62
63 Passive Leg Raising: the advantages PLR provides a good prediction of fluid responsiveness Unlike fluid challenge, effects of PLR are rapidly reversible PLR may well assess fluid responsiveness in situations where PPVfails to do it
64
 20")


65 RAP (mmhg) PAOP (mmhg) PLR 0 PLR Base post-plr Base post-plr

66 Stroke Volume PLR mimics fluid challenge preload responsiveness b' a' Unlike fluid challenge, no fluid is infused, preload unresponsiveness and, the effects are reversible and transient b a The hemodynamic response to PLR A PLR B Ventricular preload can predict the hemodynamic response to volume infusion








67 The hemodynamic response to PLR can predict the hemodynamic response to fluid infusion Real-time CO response to PLR

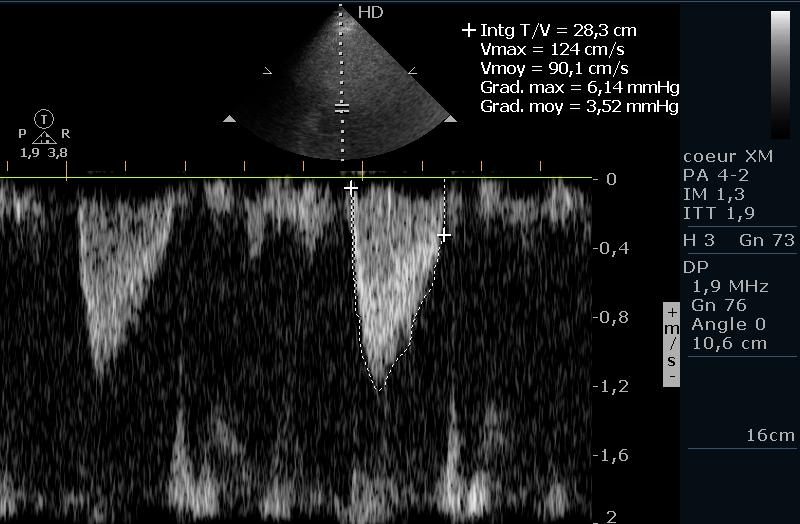
68 VTI VTI +35%



69 24 pts with circulatory failure and SB TTE before and after 500 ml saline PLR-induced change in Velocity-Time Integral PLR-induced changes in VTIAo (%) goodprediction of volume responsiveness VTI * 12% -5 R NR
70
71
72 Passive Leg Raising: the advantages PLR provides a good prediction of fluid responsiveness Unlike fluid challenge, effects of PLR are rapidly reversible PLR may well assess fluid responsiveness in situations where PPVfails to do it


73 reversible hemodynamic effects ABF PLR ABF max 90 sec No risk of pulmonary edema
74 Passive Leg Raising: the advantages PLR provides a good prediction of fluid responsiveness Unlike fluid challenge, effects of PLR are rapidly reversible PLR may well assess fluid responsiveness in situations where PPVfails to do it Spontaneous Breathing activity

75 Pts with spontaneous breathing PLR-induced changes in ABF sensitivity PPV 1 -specificity
76 Passive Leg Raising: The advantages PLR provides a good prediction of fluid responsiveness Unlike fluid challenge, effects of PLR are rapidly reversible PLR may well assess fluid responsiveness in situations where PPVfails to do it Spontaneous Breathing activity Low lung compliance
77 Lung compliance 30 ml/cmh 2 O Lung compliance < 30 ml/cmh 2 O 100 PPV effects of PLR on CO 100 effects of PLR on CO Sensitivity Sensitivity PPV Specificity 100-Specificity
78 Passive Leg Raising: the limits PLRshould notstart from a horizontalpatient s position but from a semi-recumbent position
79 45 45 semi-recumbent position Passive Leg Raising horizontal position 45 Passive Leg Raising
80 37.5 % change in CO from baseline
81 35 patients (all responders to fluid administration) 35 pts correctly classified as responders 20 pts correctly classified as responders 15 pts classified as nonresponders
82 45 45 semi-recumbent position Passive Leg Raising rather than horizontal position 45 Passive Leg Raising
83 Passive Leg Raising: the limits PLRshould notstart from a horizontalpatient s position but from a semi-recumbent position The hemodynamic response to PLR should not be monitored with arterial pressure but with CO measurements

84 PLR-induced changes in CO PLR-induced changes in AP Study name sample size AUC Study name sample size AUC Monnet CCM Lafanéchère CC Lamia ICM Maizel ICM Monnet CCM Thiel CC Biais CC Preau CCM Monnet CCM Monnet CCM Preau CCM
85 80 PLR-induced changes in aortic blood flow PLR-induced changes in pulse pressure 60 % change from Baseline 40 Following thechanges in arterial pressure * * during PLR is not suitable (false negative cases) Falses negative cases A real-time CO monitor is necessary NR R NR R
86 Decision of starting fluid administration presence of hemodynamic instability/peripheral hypoperfusion (mottled skin, hypotension, oliguria, hyperlactatemia ) and presence of preload responsiveness and limited risks of fluid overload
87 Decision of stopping fluid administration disappearance of hemodynamic instability/peripheral hypoperfusion or presence of preload unresponsiveness or high risks of fluid overload or severe hypoxemic lung injury Value ofevlw andpvpi
88 Conclusion Predictors of fluid responsiveness/unresponsiveness Pulse pressure variation orstroke volume variation PLR or end-expiratory occlusion tests Can help to choose the best fluid strategy by identifying patients eligible for fluid infusion and by avoiding to fluid overload patients who would be fluid unresponsive Thank you
Fluid responsiveness and extravascular lung water
 Fluid responsiveness and extravascular lung water Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris-South France Conflicts of interest Member of the Medical Advisory Board of Maquet/Pulsion
Fluid responsiveness and extravascular lung water Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris-South France Conflicts of interest Member of the Medical Advisory Board of Maquet/Pulsion
Hemodynamic monitoring beyond cardiac output
 Hemodynamic monitoring beyond cardiac output Prof Xavier MONNET Medical Intensive Care Unit Bicêtre Hospital Assistance publique Hôpitaux de Paris FRANCE Conflicts of interest Lilly GlaxoSmithKline Pulsion
Hemodynamic monitoring beyond cardiac output Prof Xavier MONNET Medical Intensive Care Unit Bicêtre Hospital Assistance publique Hôpitaux de Paris FRANCE Conflicts of interest Lilly GlaxoSmithKline Pulsion
Jan M. Headley, R.N. BS
 Fluid First: Using PLR & SVV to Optimize Volume Jan M. Headley, R.N. BS Disclosure Director, Clinical Marketing & Professional Education Edwards Lifesciences Does this Patient NEED Fluid?? WE Have a Problem
Fluid First: Using PLR & SVV to Optimize Volume Jan M. Headley, R.N. BS Disclosure Director, Clinical Marketing & Professional Education Edwards Lifesciences Does this Patient NEED Fluid?? WE Have a Problem
Prof. Dr. Iman Riad Mohamed Abdel Aal
 The Use of New Ultrasound Indices to Evaluate Volume Status and Fluid Responsiveness in Septic Shock Patients Thesis Submitted for partial fulfillment of MD degree in Anesthesiology, Surgical Intensive
The Use of New Ultrasound Indices to Evaluate Volume Status and Fluid Responsiveness in Septic Shock Patients Thesis Submitted for partial fulfillment of MD degree in Anesthesiology, Surgical Intensive
FLUIDS AND SOLUTIONS IN THE CRITICALLY ILL. Daniel De Backer Department of Intensive Care Erasme University Hospital Brussels, Belgium
 FLUIDS AND SOLUTIONS IN THE CRITICALLY ILL Daniel De Backer Department of Intensive Care Erasme University Hospital Brussels, Belgium Why do we want to administer fluids? To correct hypovolemia? To increase
FLUIDS AND SOLUTIONS IN THE CRITICALLY ILL Daniel De Backer Department of Intensive Care Erasme University Hospital Brussels, Belgium Why do we want to administer fluids? To correct hypovolemia? To increase
Sepsis Wave II Webinar Series. Sepsis Reassessment
 Sepsis Wave II Webinar Series Sepsis Reassessment Presenters Nova Panebianco, MD Todd Slesinger, MD Fluid Reassessment in Sepsis Todd L. Slesinger, MD, FACEP, FCCM, FCCP, FAAEM Residency Program Director
Sepsis Wave II Webinar Series Sepsis Reassessment Presenters Nova Panebianco, MD Todd Slesinger, MD Fluid Reassessment in Sepsis Todd L. Slesinger, MD, FACEP, FCCM, FCCP, FAAEM Residency Program Director
Using Functional Hemodynamic Indicators to Guide Fluid Therapy
 CE 2.6 HOURS Continuing Education Using Functional Hemodynamic Indicators to Guide Fluid Therapy A more accurate and less invasive way to gauge responsiveness to iv volume replacement. OVERVIEW: Hemodynamic
CE 2.6 HOURS Continuing Education Using Functional Hemodynamic Indicators to Guide Fluid Therapy A more accurate and less invasive way to gauge responsiveness to iv volume replacement. OVERVIEW: Hemodynamic
Hemodynamic Monitoring Pressure or Volumes? Antonio Pesenti University of Milan Italy
 Hemodynamic Monitoring Pressure or Volumes? Antonio Pesenti University of Milan Italy antonio.pesenti@unimi.it CCCF 2017 Is it useful? YES: CVP It is an important diagnostic element! Your best guess CVP
Hemodynamic Monitoring Pressure or Volumes? Antonio Pesenti University of Milan Italy antonio.pesenti@unimi.it CCCF 2017 Is it useful? YES: CVP It is an important diagnostic element! Your best guess CVP
Assessing Preload Responsiveness Using Arterial Pressure Based Technologies. Patricia A. Meehan, RN, MS Education Consultant Edwards Lifesciences, LLC
 Assessing Preload Responsiveness Using Arterial Pressure Based Technologies Patricia A. Meehan, RN, MS Education Consultant Edwards Lifesciences, LLC Content Description : Fluid administration is a first
Assessing Preload Responsiveness Using Arterial Pressure Based Technologies Patricia A. Meehan, RN, MS Education Consultant Edwards Lifesciences, LLC Content Description : Fluid administration is a first
The cornerstone of treating patients with hypotension,
 Does the Central Venous Pressure Predict Fluid Responsiveness? An Updated Meta-Analysis and a Plea for Some Common Sense* Paul E. Marik, MD, FCCM 1 ; Rodrigo Cavallazzi, MD 2 Background: Aim: Data Sources:
Does the Central Venous Pressure Predict Fluid Responsiveness? An Updated Meta-Analysis and a Plea for Some Common Sense* Paul E. Marik, MD, FCCM 1 ; Rodrigo Cavallazzi, MD 2 Background: Aim: Data Sources:
3/14/2017. Disclosures. None. Outline. Fluid Management and Hemodynamic Assessment Paul Marik, MD, FCCP, FCCM
 Fluid Management and Hemodynamic Assessment Paul Marik, MD, FCCP, FCCM Disclosures Stocks Advisory boards Grants Speakers Bureau None Outline Hemodynamic Goals Fluid Resuscitation Historical Perspective
Fluid Management and Hemodynamic Assessment Paul Marik, MD, FCCP, FCCM Disclosures Stocks Advisory boards Grants Speakers Bureau None Outline Hemodynamic Goals Fluid Resuscitation Historical Perspective
The Vigileo monitor by Edwards Lifesciences supports both the FloTrac Sensor for continuous cardiac output and the Edwards PreSep oximetry catheter
 1 2 The Vigileo monitor by Edwards Lifesciences supports both the FloTrac Sensor for continuous cardiac output and the Edwards PreSep oximetry catheter for continuous central venous oximetry (ScvO2) 3
1 2 The Vigileo monitor by Edwards Lifesciences supports both the FloTrac Sensor for continuous cardiac output and the Edwards PreSep oximetry catheter for continuous central venous oximetry (ScvO2) 3
ICU Volume 12 - Issue 4 - Winter 2012/ Matrix Features
 ICU Volume 12 - Issue 4 - Winter 2012/2013 - Matrix Features Fluid Management in Critically Ill Patients: A Guided Approach Prof. Antonio Artigas, MD, PhD ICU Management & Practice Editorial Board Member
ICU Volume 12 - Issue 4 - Winter 2012/2013 - Matrix Features Fluid Management in Critically Ill Patients: A Guided Approach Prof. Antonio Artigas, MD, PhD ICU Management & Practice Editorial Board Member
Shock and hemodynamic monitorization. Nilüfer Yalındağ Öztürk Marmara University Pendik Research and Training Hospital
 Shock and hemodynamic monitorization Nilüfer Yalındağ Öztürk Marmara University Pendik Research and Training Hospital Shock Leading cause of morbidity and mortality Worldwide: dehydration and hypovolemic
Shock and hemodynamic monitorization Nilüfer Yalındağ Öztürk Marmara University Pendik Research and Training Hospital Shock Leading cause of morbidity and mortality Worldwide: dehydration and hypovolemic
Tailored Volume Resuscitation in the Critically Ill is Achievable. Objectives. Clinical Case 2/16/2018
 Tailored Volume Resuscitation in the Critically Ill is Achievable Heath E Latham, MD Associate Professor Fellowship Program Director Pulmonary and Critical Care Objectives Describe the goal of resuscitation
Tailored Volume Resuscitation in the Critically Ill is Achievable Heath E Latham, MD Associate Professor Fellowship Program Director Pulmonary and Critical Care Objectives Describe the goal of resuscitation
Swan Ganz catheter: Does it still have a role? Daniel De Backer Department of Intensive Care Erasme University Hospital Brussels, Belgium
 Swan Ganz catheter: Does it still have a role? Daniel De Backer Department of Intensive Care Erasme University Hospital Brussels, Belgium How can cardiac output be measured? Thermodilution Arterial waveform
Swan Ganz catheter: Does it still have a role? Daniel De Backer Department of Intensive Care Erasme University Hospital Brussels, Belgium How can cardiac output be measured? Thermodilution Arterial waveform
EVOLUCIÓN DE LA MONITORIZACIÓN CARDIOVASCULAR EN LA UCI
 EVOLUCIÓN DE LA MONITORIZACIÓN CARDIOVASCULAR EN LA UCI Antonio Artigas Critical Care Center Sabadell Hospital CIBER Enfermedades Respiratorias Autonomos University of Barcelona Spain aartigas@tauli.cat
EVOLUCIÓN DE LA MONITORIZACIÓN CARDIOVASCULAR EN LA UCI Antonio Artigas Critical Care Center Sabadell Hospital CIBER Enfermedades Respiratorias Autonomos University of Barcelona Spain aartigas@tauli.cat
Goal-directed resuscitation in sepsis; a case-based approach
 Goal-directed resuscitation in sepsis; a case-based approach Jorge A Guzman, MD, FCCM Head, Section Critical Care Medicine Respiratory Institute Cleveland Clinic Foundation The challenges to managing septic
Goal-directed resuscitation in sepsis; a case-based approach Jorge A Guzman, MD, FCCM Head, Section Critical Care Medicine Respiratory Institute Cleveland Clinic Foundation The challenges to managing septic
Disclaimer. Improving MET-based patient care using treatment algorithms. Michael R. Pinsky, MD, Dr hc. Different Environments Demand Different Rules
 Michael R. Pinsky, MD - June 29, 26 Improving MET-based patient care using Michael R. Pinsky, MD, Dr hc Department of Critical Care Medicine University of Pittsburgh Disclaimer Michael R. Pinsky, MD is
Michael R. Pinsky, MD - June 29, 26 Improving MET-based patient care using Michael R. Pinsky, MD, Dr hc Department of Critical Care Medicine University of Pittsburgh Disclaimer Michael R. Pinsky, MD is
ENDPOINTS OF RESUSCITATION
 ENDPOINTS OF RESUSCITATION Fred Pieracci, MD, MPH Acute Care Surgeon Denver Health Medical Center Assistant Professor of Surgery University of Colorado Health Science Center OUTLINE Recognition and characterization
ENDPOINTS OF RESUSCITATION Fred Pieracci, MD, MPH Acute Care Surgeon Denver Health Medical Center Assistant Professor of Surgery University of Colorado Health Science Center OUTLINE Recognition and characterization
Functional Hemodynamic Monitoring and Management A practical Approach
 Functional Hemodynamic Monitoring and Management A practical Approach Daniel A. Reuter Center of Anesthesiology and Intensive Care Medicine Hamburg-Eppendorf University Hospital Hamburg, Germany Euronaesthesia
Functional Hemodynamic Monitoring and Management A practical Approach Daniel A. Reuter Center of Anesthesiology and Intensive Care Medicine Hamburg-Eppendorf University Hospital Hamburg, Germany Euronaesthesia
Sepsis Update: Focus on Early Recognition and Intervention. Disclosures
 Sepsis Update: Focus on Early Recognition and Intervention Jessie Roske, MD October 2017 Disclosures I have no actual or potential conflict of interest in relation to this program/presentation. I will
Sepsis Update: Focus on Early Recognition and Intervention Jessie Roske, MD October 2017 Disclosures I have no actual or potential conflict of interest in relation to this program/presentation. I will
UPMC Critical Care.
 UPMC Critical Care www.ccm.pitt.edu Functional Hemodynamic Monitoring Michael R. Pinsky, MD, Dr hc Department of Critical Care Medicine University of Pittsburgh Important Conflicts of Interest Unimportant
UPMC Critical Care www.ccm.pitt.edu Functional Hemodynamic Monitoring Michael R. Pinsky, MD, Dr hc Department of Critical Care Medicine University of Pittsburgh Important Conflicts of Interest Unimportant
Fluid responsiveness Monitoring in Surgical and Critically Ill Patients
 Fluid responsiveness Monitoring in Surgical and Critically Ill Patients Impact clinique de la Goal-directed-therapy Patrice FORGET, M.D Cliniques universitaires Saint Luc Université catholique de Louvain,
Fluid responsiveness Monitoring in Surgical and Critically Ill Patients Impact clinique de la Goal-directed-therapy Patrice FORGET, M.D Cliniques universitaires Saint Luc Université catholique de Louvain,
Dr. F Javier Belda Dept. Anesthesiology and Critical Care Hospital Clinico Universitario Valencia (Spain) Pulsion MAB
 Pulsion MAB") State of the Art Hemodynamic Monitoring III CO, preload, lung water and ScvO2 The winning combination! Dr. F Javier Belda Dept. Anesthesiology and Critical Care Hospital Clinico Universitario Valencia
State of the Art Hemodynamic Monitoring III CO, preload, lung water and ScvO2 The winning combination! Dr. F Javier Belda Dept. Anesthesiology and Critical Care Hospital Clinico Universitario Valencia
6/5/2014. Sepsis Management and Hemodynamics. 2004: International group of experts,
 Sepsis Management and Hemodynamics Javier Perez-Fernandez, M.D., F.C.C.P. Medical Director Critical Care Services, Baptist t Hospital of Miamii Medical Director Pulmonary Services, West Kendall Baptist
Sepsis Management and Hemodynamics Javier Perez-Fernandez, M.D., F.C.C.P. Medical Director Critical Care Services, Baptist t Hospital of Miamii Medical Director Pulmonary Services, West Kendall Baptist
Echocardiography to guide fluid therapy in critically ill patients: check the heart and take a quick look at the lungs
 Editorial Echocardiography to guide fluid therapy in critically ill patients: check the heart and take a quick look at the lungs Federico Franchi 1 *, Luigi Vetrugno 2 *, Sabino Scolletta 1 1 Department
Editorial Echocardiography to guide fluid therapy in critically ill patients: check the heart and take a quick look at the lungs Federico Franchi 1 *, Luigi Vetrugno 2 *, Sabino Scolletta 1 1 Department
Impedance Cardiography (ICG) Application of ICG in Intensive Care and Emergency
 Application of ICG in Intensive Care and Emergency") Impedance Cardiography (ICG) Application of ICG in Intensive Care and Emergency Aim of haemodynamic monitoring in ICU and ED Detection and therapy of insufficient organ perfusion Answers to common cardiovascular
Impedance Cardiography (ICG) Application of ICG in Intensive Care and Emergency Aim of haemodynamic monitoring in ICU and ED Detection and therapy of insufficient organ perfusion Answers to common cardiovascular
Review Article Echocardiographic Assessment of Preload Responsiveness in Critically Ill Patients
 Cardiology Research and Practice Volume 2012, Article ID 819696, 7 pages doi:10.1155/2012/819696 Review Article Echocardiographic Assessment of Preload Responsiveness in Critically Ill Patients Alexander
Cardiology Research and Practice Volume 2012, Article ID 819696, 7 pages doi:10.1155/2012/819696 Review Article Echocardiographic Assessment of Preload Responsiveness in Critically Ill Patients Alexander
The Use of Dynamic Parameters in Perioperative Fluid Management
 The Use of Dynamic Parameters in Perioperative Fluid Management Gerard R. Manecke Jr., M.D. Chief, Cardiac Anesthesia UCSD Medical Center San Diego, CA, USA Thanks to Tom Higgins, M.D. 1 Goals of today
The Use of Dynamic Parameters in Perioperative Fluid Management Gerard R. Manecke Jr., M.D. Chief, Cardiac Anesthesia UCSD Medical Center San Diego, CA, USA Thanks to Tom Higgins, M.D. 1 Goals of today
Norepinephrine in septic shock
 Norepinephrine in septic shock Prof. Zsolt Molnár zsoltmolna@gmail.com Department of Anaesthesia and Intensive Therapy University of Szeged, Hungary A few months ago should we give it earlier? (Courtesy
Norepinephrine in septic shock Prof. Zsolt Molnár zsoltmolna@gmail.com Department of Anaesthesia and Intensive Therapy University of Szeged, Hungary A few months ago should we give it earlier? (Courtesy
Obligatory joke. The case for why it matters. Sepsis: More is more. Goal-Directed Fluid Resuscitation 6/1/2013
 Obligatory joke Keep your eye on the food. Goal-Directed Fluid Resuscitation Christopher G. Choukalas, MD, MS Department of Anesthesia and Perioperative Care University of California, San Francisco The
Obligatory joke Keep your eye on the food. Goal-Directed Fluid Resuscitation Christopher G. Choukalas, MD, MS Department of Anesthesia and Perioperative Care University of California, San Francisco The
Purist? or Pragmatist? Assessment & Management of ICU Volume Status
 Assessment & Management of ICU Volume Status 9 th Annual Rocky Mountain Hospital Medicine Symposium Denver, Colorado Paula Dennen, MD Assistant Professor of Medicine Nephrology and Critical Care Medicine
Assessment & Management of ICU Volume Status 9 th Annual Rocky Mountain Hospital Medicine Symposium Denver, Colorado Paula Dennen, MD Assistant Professor of Medicine Nephrology and Critical Care Medicine
Patrick C. Cullinan, DO, NBPNS, FCCM, FACOEP, FACOI Associate Clinical Professor, UIWSOM, San Antonio, Texas Adjunct Assistant Professor, University
 Patrick C. Cullinan, DO, NBPNS, FCCM, FACOEP, FACOI Associate Clinical Professor, UIWSOM, San Antonio, Texas Adjunct Assistant Professor, University of Texas Health Science Center, Department of Emergency
Patrick C. Cullinan, DO, NBPNS, FCCM, FACOEP, FACOI Associate Clinical Professor, UIWSOM, San Antonio, Texas Adjunct Assistant Professor, University of Texas Health Science Center, Department of Emergency
FLUID RESUSCITATION AND MONITORING IN SEPSIS PROTOCOLIZED VS USUAL CARE DEEPA BANGALORE GOTUR MD, FCCP ASSISTANT PROFESSOR, WEILL CORNELL MEDICAL
 FLUID RESUSCITATION AND MONITORING IN SEPSIS PROTOCOLIZED VS USUAL CARE DEEPA BANGALORE GOTUR MD, FCCP ASSISTANT PROFESSOR, WEILL CORNELL MEDICAL COLLEGE NOVEMBER 10 TH 2017 TEXAS SCCM SYMPOSIUM Disclosures
FLUID RESUSCITATION AND MONITORING IN SEPSIS PROTOCOLIZED VS USUAL CARE DEEPA BANGALORE GOTUR MD, FCCP ASSISTANT PROFESSOR, WEILL CORNELL MEDICAL COLLEGE NOVEMBER 10 TH 2017 TEXAS SCCM SYMPOSIUM Disclosures
DESIGNER RESUSCITATION: TITRATING TO TISSUE NEEDS
 DESIGNER RESUSCITATION: TITRATING TO TISSUE NEEDS R. Phillip Dellinger MD, MSc, MCCM Professor and Chair of Medicine Cooper Medical School of Rowan University Chief of Medicine Cooper University Hospital
DESIGNER RESUSCITATION: TITRATING TO TISSUE NEEDS R. Phillip Dellinger MD, MSc, MCCM Professor and Chair of Medicine Cooper Medical School of Rowan University Chief of Medicine Cooper University Hospital
Cardiac filling pressures are not appropriate to predict hemodynamic response to volume challenge*
 Cardiac filling pressures are not appropriate to predict hemodynamic response to volume challenge* David Osman, MD; Christophe Ridel, MD; Patrick Ray, MD; Xavier Monnet, MD, PhD; Nadia Anguel, MD; Christian
Cardiac filling pressures are not appropriate to predict hemodynamic response to volume challenge* David Osman, MD; Christophe Ridel, MD; Patrick Ray, MD; Xavier Monnet, MD, PhD; Nadia Anguel, MD; Christian
Shock, Monitoring Invasive Vs. Non Invasive
 Shock, Monitoring Invasive Vs. Non Invasive Paula Ferrada MD Assistant Professor Trauma, Critical Care and Emergency Surgery Virginia Commonwealth University Shock Fluid Pressors Ionotrope Intervention
Shock, Monitoring Invasive Vs. Non Invasive Paula Ferrada MD Assistant Professor Trauma, Critical Care and Emergency Surgery Virginia Commonwealth University Shock Fluid Pressors Ionotrope Intervention
Actualités de la prise en charge hémodynamique initiale Daniel De Backer
 Actualités de la prise en charge hémodynamique initiale Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles Past- President European
Actualités de la prise en charge hémodynamique initiale Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles Past- President European
Comparıng pulse pressure varıatıon and pleth varıabılıty ındex in the semı-recumbent and trendelenburg posıtıon ın crıtıcally ıll septıc patıents
 SIGNA VITAE 2017; 13(2): 91-96 Comparıng pulse pressure varıatıon and pleth varıabılıty ındex in the semı-recumbent and trendelenburg posıtıon ın crıtıcally ıll septıc patıents SELMAN KARADAYI 1, BEYHAN
SIGNA VITAE 2017; 13(2): 91-96 Comparıng pulse pressure varıatıon and pleth varıabılıty ındex in the semı-recumbent and trendelenburg posıtıon ın crıtıcally ıll septıc patıents SELMAN KARADAYI 1, BEYHAN
Bioreactance-based passive leg raising test can predict fluid responsiveness in elderly patients with septic shock
 Original Article Page 1 of 6 Bioreactance-based passive leg raising test can predict fluid responsiveness in elderly patients with septic shock Caibao Hu 1 *, Guolong Cai 1 *, Jing Yan 1, Hongjie Tong
Original Article Page 1 of 6 Bioreactance-based passive leg raising test can predict fluid responsiveness in elderly patients with septic shock Caibao Hu 1 *, Guolong Cai 1 *, Jing Yan 1, Hongjie Tong
Continuous and noninvasive arterial blood pressure monitoring
 Continuous and noninvasive arterial blood pressure monitoring Pr. Jean-Luc Fellahi fellahi-jl@chu-caen.fr Pôle Réanimations-Anesthésie-SAMU, CHU de Caen UFR de Médecine, EA4650, Université de Caen Basse-Normandie
Continuous and noninvasive arterial blood pressure monitoring Pr. Jean-Luc Fellahi fellahi-jl@chu-caen.fr Pôle Réanimations-Anesthésie-SAMU, CHU de Caen UFR de Médecine, EA4650, Université de Caen Basse-Normandie
Online Supplement. Hemodynamic Assessment of Patients With Septic Shock Using Transpulmonary Thermodilution and Critical Care Echocardiography
 Online Supplement Hemodynamic Assessment of Patients With Septic Shock Using Transpulmonary Thermodilution and Critical Care Echocardiography A Comparative Study Philippe Vignon, MD, PhD; Emmanuelle Begot,
Online Supplement Hemodynamic Assessment of Patients With Septic Shock Using Transpulmonary Thermodilution and Critical Care Echocardiography A Comparative Study Philippe Vignon, MD, PhD; Emmanuelle Begot,
Surviving Sepsis Campaign Guidelines 2012 & Update for David E. Tannehill, DO Critical Care Medicine Mercy Hospital St.
 Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
Surviving Sepsis Campaign Guidelines 2012 & Update for 2015 David E. Tannehill, DO Critical Care Medicine Mercy Hospital St. Louis Be appropriately aggressive the longer one delays aggressive metabolic
Fluid Responsiveness Monitoring In Surgical and Critically Ill Patients
 Fluid Responsiveness Monitoring In Surgical and Critically Ill Patients Clinical Impact of Goal-Directed Therapy Release Date: September 1, 2010 Expiration Date: September 30, 2011 Needs Statement Volume
Fluid Responsiveness Monitoring In Surgical and Critically Ill Patients Clinical Impact of Goal-Directed Therapy Release Date: September 1, 2010 Expiration Date: September 30, 2011 Needs Statement Volume
Vasopressors in septic shock
 Vasopressors in septic shock Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris-South France Questions 1- Why do we use vasopressors in septic shock? 2- Which first-line agent? 3- When
Vasopressors in septic shock Prof. Jean-Louis TEBOUL Medical ICU Bicetre hospital University Paris-South France Questions 1- Why do we use vasopressors in septic shock? 2- Which first-line agent? 3- When
CHAPTER 13. Fluid Responsiveness
 CHAPTER 13 Fluid Responsiveness SECTION 1 Introduction Administration of an intravenous fluid challenge is a common medical intervention in the hypotensive or hypovolemic patient. Ideally, a fluid challenge
CHAPTER 13 Fluid Responsiveness SECTION 1 Introduction Administration of an intravenous fluid challenge is a common medical intervention in the hypotensive or hypovolemic patient. Ideally, a fluid challenge
Sepsis: Management ANUPOL PANITCHOTE, MD. Division of Critical Care Medicine Department of Medicine, Khon Kaen University, Thailand
 Sepsis: Management ANUPOL PANITCHOTE, MD. Division of Critical Care Medicine Department of Medicine, Khon Kaen University, Thailand Vital signs Symptoms LAB BT > 38.3 or < 36 ๐ C HR > 90 bpm RR > 20 /min
Sepsis: Management ANUPOL PANITCHOTE, MD. Division of Critical Care Medicine Department of Medicine, Khon Kaen University, Thailand Vital signs Symptoms LAB BT > 38.3 or < 36 ๐ C HR > 90 bpm RR > 20 /min
Hemodynamic monitoring should be kept as simple as possible. But not simpler!
 Hemodynamic monitoring should be kept as simple as possible. But not simpler! Azriel Perel Professor and Chairman Department of Anesthesiology and Intensive Care Sheba Medical Center, Tel Aviv University,
Hemodynamic monitoring should be kept as simple as possible. But not simpler! Azriel Perel Professor and Chairman Department of Anesthesiology and Intensive Care Sheba Medical Center, Tel Aviv University,
The Hemodynamic Puzzle
 The Hemodynamic Puzzle SVV NIRS O 2 ER Lactate Energy Metabolism (Oxygen Consumption) (Ml/min/m 2 ) Oxygen Debt: To Pay or Not to Pay? Full Recovery Possible Delayed Repayment of O 2 Debt Oxygen Deficit
The Hemodynamic Puzzle SVV NIRS O 2 ER Lactate Energy Metabolism (Oxygen Consumption) (Ml/min/m 2 ) Oxygen Debt: To Pay or Not to Pay? Full Recovery Possible Delayed Repayment of O 2 Debt Oxygen Deficit
Invasive Cardiac Output Monitoring and Pulse Contour Analysis. Harshad B. Ranchod Paediatric Intensivist Chris Hani Baragwanath Hospital COPICON 2011
 Invasive Cardiac Output Monitoring and Pulse Contour Analysis Harshad B. Ranchod Paediatric Intensivist Chris Hani Baragwanath Hospital COPICON 2011 Introduction The primary goal of haemodynamic monitoring
Invasive Cardiac Output Monitoring and Pulse Contour Analysis Harshad B. Ranchod Paediatric Intensivist Chris Hani Baragwanath Hospital COPICON 2011 Introduction The primary goal of haemodynamic monitoring
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE
 Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Utility of transthoracic echocardiography (TTE) in assessing fluid responsiveness in critically ill patients a challenge for the bedside sonographer
 in assessing fluid responsiveness in critically ill patients a challenge for the bedside sonographer") Continuing education Med Ultrason 2016, Vol. 18, no. 4, -514 DOI: 10.11152/mu-880 Utility of transthoracic echocardiography (TTE) in assessing fluid responsiveness in critically ill patients a challenge
Continuing education Med Ultrason 2016, Vol. 18, no. 4, -514 DOI: 10.11152/mu-880 Utility of transthoracic echocardiography (TTE) in assessing fluid responsiveness in critically ill patients a challenge
Review Article. Interactive Physiology in Critical Illness : Pulmonary and Cardiovascular Systems. Introduction
 310 Indian Deepak J Physiol Shrivastava Pharmacol 2016; 60(4) : 310 314 Indian J Physiol Pharmacol 2016; 60(4) Review Article Interactive Physiology in Critical Illness : Pulmonary and Cardiovascular Systems
310 Indian Deepak J Physiol Shrivastava Pharmacol 2016; 60(4) : 310 314 Indian J Physiol Pharmacol 2016; 60(4) Review Article Interactive Physiology in Critical Illness : Pulmonary and Cardiovascular Systems
Hemodynamic Monitoring To Guide Volume Resuscitation
 Hemodynamic Monitoring To Guide Volume Resuscitation Nick Johnson, MD Acting Assistant Professor Division of Emergency Medicine Attending Physician, Medical & Neuro-Intensive Care Units Harborview Medical
Hemodynamic Monitoring To Guide Volume Resuscitation Nick Johnson, MD Acting Assistant Professor Division of Emergency Medicine Attending Physician, Medical & Neuro-Intensive Care Units Harborview Medical
Arterial Pulse Pressure Variation During Positive Pressure Ventilation and Passive Leg Raising
 Arterial Pulse Pressure Variation During Positive Pressure Ventilation and Passive Leg Raising J.-L. Teboul, X. Monnet, and C. Richard Introduction Inadequate cardiac preload can play a major role in the
Arterial Pulse Pressure Variation During Positive Pressure Ventilation and Passive Leg Raising J.-L. Teboul, X. Monnet, and C. Richard Introduction Inadequate cardiac preload can play a major role in the
How to resuscitate the patient in early sepsis? A physiological approach. J.G. van der Hoeven, Nijmegen
 How to resuscitate the patient in early sepsis? A physiological approach J.G. van der Hoeven, Nijmegen Disclosure interests speaker (potential) conflict of interest Potentially relevant relationships with
How to resuscitate the patient in early sepsis? A physiological approach J.G. van der Hoeven, Nijmegen Disclosure interests speaker (potential) conflict of interest Potentially relevant relationships with
PCV and PAOP Old habits die hard!
 PCV and PAOP Old habits die hard! F Javier Belda MD, PhD Head of Department Associate Professor Anaesthesia and Critical Care Hospital Clínico Universitario Valencia (SPAIN) An old example TOBACO SMOKING
PCV and PAOP Old habits die hard! F Javier Belda MD, PhD Head of Department Associate Professor Anaesthesia and Critical Care Hospital Clínico Universitario Valencia (SPAIN) An old example TOBACO SMOKING
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014
 December 17, 2014") Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
Patient Safety Safe Table Webcast: Sepsis (Part III and IV) December 17, 2014 Presenters Mark Blaney, RN Regional Nurse Educator CHI Franciscan Health Karen Lautermilch Director, Quality & Performance
Troubleshooting Audio
 Welcome! Audio for this event is available via ReadyTalk Internet Streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
Welcome! Audio for this event is available via ReadyTalk Internet Streaming. No telephone line is required. Computer speakers or headphones are necessary to listen to streaming audio. Limited dial-in lines
Cardiac Output Monitoring - 6
 Cardiac Output Monitoring - 6 How to use Wrexham s Cardiac Output Monitors. Wrexham Maelor Critical Care Version 02.05.16 Introduction Types of Devices: NICOM - Cheetah Oesophageal Doppler +/- Pulse Contour
Cardiac Output Monitoring - 6 How to use Wrexham s Cardiac Output Monitors. Wrexham Maelor Critical Care Version 02.05.16 Introduction Types of Devices: NICOM - Cheetah Oesophageal Doppler +/- Pulse Contour
Fluid optimization strategies in critical care patients
 Perioperative & Critical Care Medicine Page 1 of 5 Fluid optimization strategies in critical care patients X García*, G Gruartmoner, J Mesquida Abstract Introduction Fluid optimization is an important
Perioperative & Critical Care Medicine Page 1 of 5 Fluid optimization strategies in critical care patients X García*, G Gruartmoner, J Mesquida Abstract Introduction Fluid optimization is an important
IN THE NAME OF GOD SHOCK MANAGMENT OMID MORADI MOGHADDAM,MD,FCCM IUMS ASSISTANT PROFESSOR
 IN THE NAME OF GOD SHOCK MANAGMENT OMID MORADI MOGHADDAM,MD,FCCM IUMS ASSISTANT PROFESSOR The ability to evaluate and manage a critically ill patient is one of the most important skills any intensivist
IN THE NAME OF GOD SHOCK MANAGMENT OMID MORADI MOGHADDAM,MD,FCCM IUMS ASSISTANT PROFESSOR The ability to evaluate and manage a critically ill patient is one of the most important skills any intensivist
Perioperative Fluid Management in ERPs
 Perioperative Fluid Management in ERPs Robert H. Thiele, M.D. Assistant Professor University of Virginia First Do No Harm Intravenous fluids should be considered a pharmacotherapeutic agent Just like all
Perioperative Fluid Management in ERPs Robert H. Thiele, M.D. Assistant Professor University of Virginia First Do No Harm Intravenous fluids should be considered a pharmacotherapeutic agent Just like all
Fluid management. Dr. Timothy Miller Assistant Professor of Anesthesiology Duke University Medical Center
 Fluid management Dr. Timothy Miller Assistant Professor of Anesthesiology Duke University Medical Center Disclosure Consultant and research funding Edwards Lifesciences Goals of fluid therapy 1. Maintain
Fluid management Dr. Timothy Miller Assistant Professor of Anesthesiology Duke University Medical Center Disclosure Consultant and research funding Edwards Lifesciences Goals of fluid therapy 1. Maintain
Making the Case For Less Invasive Flow Based Parameters: APCO + SVV. Patricia A. Meehan, RN, MS, CCRN (a) Education Consultant Edwards Lifesciences
 Education Consultant Edwards Lifesciences") Making the Case For Less Invasive Flow Based Parameters: APCO + SVV Patricia A. Meehan, RN, MS, CCRN (a) Education Consultant Edwards Lifesciences A New Gold Standard? How does the system work? Sensor
Making the Case For Less Invasive Flow Based Parameters: APCO + SVV Patricia A. Meehan, RN, MS, CCRN (a) Education Consultant Edwards Lifesciences A New Gold Standard? How does the system work? Sensor
Clinical Applications of The Pleth. Variability Index (PVI):
:") Clinical Applications of The Pleth. Variability Index (PVI): A non invasive and continuous monitoring of fluid responsiveness J.PIRSON, MD 26 nov. 2011 Preoperative hypovolemia after an overnight fasting
Clinical Applications of The Pleth. Variability Index (PVI): A non invasive and continuous monitoring of fluid responsiveness J.PIRSON, MD 26 nov. 2011 Preoperative hypovolemia after an overnight fasting
PiCCO based algorithms
 European Society of Anaesthesiologists Annual Meeting 12.-15. June 2010, Helsinki, Finland PiCCO based algorithms Berthold Bein, MD, PhD, DEAA Department of Anaesthesiology and Intensive Care Medicine
European Society of Anaesthesiologists Annual Meeting 12.-15. June 2010, Helsinki, Finland PiCCO based algorithms Berthold Bein, MD, PhD, DEAA Department of Anaesthesiology and Intensive Care Medicine
How can the PiCCO improve protocolized care?
 How can the PiCCO improve protocolized care? Azriel Perel Professor and Chairman Department of Anesthesiology and Intensive Care Sheba Medical Center, Tel Aviv University, Israel ESICM, Vienna 2009 Disclosure
How can the PiCCO improve protocolized care? Azriel Perel Professor and Chairman Department of Anesthesiology and Intensive Care Sheba Medical Center, Tel Aviv University, Israel ESICM, Vienna 2009 Disclosure
Fluids in Sepsis Less is more. Dr Anand Senthi Joondalup Health Campus ED MBBS, MAppFin, GradCertPubHlth,
 Fluids in Sepsis Less is more Dr Anand Senthi Joondalup Health Campus ED MBBS, MAppFin, GradCertPubHlth, FRACGP @drsenthi Summary Discussion of the evidence for/against fluid resuscitation in septic shock
Fluids in Sepsis Less is more Dr Anand Senthi Joondalup Health Campus ED MBBS, MAppFin, GradCertPubHlth, FRACGP @drsenthi Summary Discussion of the evidence for/against fluid resuscitation in septic shock
Mechanical ventilation induced or exacerbated right ventricular failure
 Mechanical ventilation induced or exacerbated right ventricular failure Toronto 2016 Jesse Hall MD Professor of Medicine, Anesthesia & Critical Care University of Chicago Faculty Disclosures Dr. Hall
Mechanical ventilation induced or exacerbated right ventricular failure Toronto 2016 Jesse Hall MD Professor of Medicine, Anesthesia & Critical Care University of Chicago Faculty Disclosures Dr. Hall
Assessing volume status and fluid responsiveness in the emergency department
 Clin Exp Emerg Med 2014;1(2):67-77 http://dx.doi.org/10.15441/ceem.14.040 Assessing volume status and fluid responsiveness in the emergency department David C. Mackenzie 1, Vicki E. Noble 2 1 Department
Clin Exp Emerg Med 2014;1(2):67-77 http://dx.doi.org/10.15441/ceem.14.040 Assessing volume status and fluid responsiveness in the emergency department David C. Mackenzie 1, Vicki E. Noble 2 1 Department
Index. K Knobology, TTE artifact, image resolution, ultrasound, 14
 A Acute aortic regurgitation (AR), 124 128 Acute aortic syndrome (AAS) classic aortic dissection diagnosis, 251 263 evolutive patterns, 253 255 pathology, 250 251 classifications, 247 248 incomplete aortic
A Acute aortic regurgitation (AR), 124 128 Acute aortic syndrome (AAS) classic aortic dissection diagnosis, 251 263 evolutive patterns, 253 255 pathology, 250 251 classifications, 247 248 incomplete aortic
Nurse Driven Fluid Optimization Using Dynamic Assessments
 Nurse Driven Fluid Optimization Using Dynamic Assessments 2016 1 WHAT WE BELIEVE We believe that clinicians make vital fluid and drug decisions every day with limited and inconclusive information Cheetah
Nurse Driven Fluid Optimization Using Dynamic Assessments 2016 1 WHAT WE BELIEVE We believe that clinicians make vital fluid and drug decisions every day with limited and inconclusive information Cheetah
Cardiovascular Management of Septic Shock
 Cardiovascular Management of Septic Shock R. Phillip Dellinger, MD Professor of Medicine Robert Wood Johnson Medical School/UMDNJ Director, Critical Care Medicine and Med/Surg ICU Cooper University Hospital
Cardiovascular Management of Septic Shock R. Phillip Dellinger, MD Professor of Medicine Robert Wood Johnson Medical School/UMDNJ Director, Critical Care Medicine and Med/Surg ICU Cooper University Hospital
Predicting fluid responsiveness in the intensive care unit: a clinical guide
 review Netherlands Journal of Critical Care Copyright 2008, Nederlandse Vereniging voor Intensive Care. All Rights Reserved. Received June 2008; accepted January 2009 Predicting fluid responsiveness in
review Netherlands Journal of Critical Care Copyright 2008, Nederlandse Vereniging voor Intensive Care. All Rights Reserved. Received June 2008; accepted January 2009 Predicting fluid responsiveness in
Hemodynamic Monitoring in Critically ill Patients in Arthur Simonnet, interne Tuteur : Pr. Raphaël Favory
 Hemodynamic Monitoring in Critically ill Patients in 2017 Arthur Simonnet, interne Tuteur : Pr. Raphaël Favory Rationale for Hemodynamic Monitoring Identify the presence of hemodynamic instability Identify
Hemodynamic Monitoring in Critically ill Patients in 2017 Arthur Simonnet, interne Tuteur : Pr. Raphaël Favory Rationale for Hemodynamic Monitoring Identify the presence of hemodynamic instability Identify
Jarisch A. Kreislauffragen, Dünser et al. Critical Care 2013, 17:326 Sunday, March 30, 14
 It was fatal for the development of our understanding of circulation that blood flow is relatively difficult while blood pressure so easy to measure: This is the reason why the sphygmomanometer has gained
It was fatal for the development of our understanding of circulation that blood flow is relatively difficult while blood pressure so easy to measure: This is the reason why the sphygmomanometer has gained
Echocardiography Volume assessment. Justin Mandeville 2014
 Echocardiography Volume assessment Justin Mandeville 2014 Volume assessment and the intensivist Hypovolaemic shock Fluid tolerance Optimising cardiac output Avoiding overloading Guided fluid removal Add
Echocardiography Volume assessment Justin Mandeville 2014 Volume assessment and the intensivist Hypovolaemic shock Fluid tolerance Optimising cardiac output Avoiding overloading Guided fluid removal Add
福島県立医科大学学術成果リポジトリ. Title laparoscopic adrenalectomy in patie pheochromocytoma. Midori; Iida, Hiroshi; Murakawa, Ma
 福島県立医科大学学術成果リポジトリ Examination of the usefulness of no Title variation monitoring for adjusting laparoscopic adrenalectomy in patie pheochromocytoma Isosu, Tsuyoshi; Obara, Shinju; Oha Author(s) Atsuyuki;
福島県立医科大学学術成果リポジトリ Examination of the usefulness of no Title variation monitoring for adjusting laparoscopic adrenalectomy in patie pheochromocytoma Isosu, Tsuyoshi; Obara, Shinju; Oha Author(s) Atsuyuki;
Fluid Resuscitation and Monitoring in Sepsis. Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS
 Fluid Resuscitation and Monitoring in Sepsis Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS Learning Objectives Compare and contrast fluid resuscitation strategies in septic shock Discuss available
Fluid Resuscitation and Monitoring in Sepsis Deepa Gotur, MD, FCCP Anne Rain T. Brown, PharmD, BCPS Learning Objectives Compare and contrast fluid resuscitation strategies in septic shock Discuss available
Bedside Ultrasound. US Guided Fluid Resuscitation. Michiel J. van Veelen, Emergency Physician, DTM&H
 Bedside Ultrasound US Guided Fluid Resuscitation Michiel J. van Veelen, Emergency Physician, DTM&H Outline Shock and Fluid Resuscitation in ICU Ultrasound in Shock Ultrasound Guided Fluid Resuscitation
Bedside Ultrasound US Guided Fluid Resuscitation Michiel J. van Veelen, Emergency Physician, DTM&H Outline Shock and Fluid Resuscitation in ICU Ultrasound in Shock Ultrasound Guided Fluid Resuscitation
Echocardiography as a diagnostic and management tool in medical emergencies
 Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
SHOCK. Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital
 SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
SHOCK Emergency pediatric PICU division Pediatric Department Medical Faculty, University of Sumatera Utara H. Adam Malik Hospital 1 Definition Shock is an acute, complex state of circulatory dysfunction
EARLY GOAL DIRECTED THERAPY : seminaires iris. Etat des lieux en Daniel De Backer
 EARLY GOAL DIRECTED THERAPY : Etat des lieux en 2017 Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles Past-President European
EARLY GOAL DIRECTED THERAPY : Etat des lieux en 2017 Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles Past-President European
Cardiorespiratory Interactions:
 Cardiorespiratory Interactions: The Heart - Lung Connection Jon N. Meliones, MD, MS, FCCM Professor of Pediatrics Duke University Medical Director PCVICU Optimizing CRI Cardiorespiratory Economics O2:
Cardiorespiratory Interactions: The Heart - Lung Connection Jon N. Meliones, MD, MS, FCCM Professor of Pediatrics Duke University Medical Director PCVICU Optimizing CRI Cardiorespiratory Economics O2:
Effects of mechanical ventilation on organ function. Masterclass ICU nurses
 Effects of mechanical ventilation on organ function Masterclass ICU nurses Case Male, 60 - No PMH - L 1.74 m and W 85 kg Pneumococcal pneumonia Stable hemodynamics - No AKI MV in prone position (PEEP 16
Effects of mechanical ventilation on organ function Masterclass ICU nurses Case Male, 60 - No PMH - L 1.74 m and W 85 kg Pneumococcal pneumonia Stable hemodynamics - No AKI MV in prone position (PEEP 16
Predicting cardiac output responses to passive leg raising by a PEEP-induced increase in central venous pressure, in cardiac surgery patients
 Chapter 10 Predicting cardiac output responses to passive leg raising by a PEEP-induced increase in central venous pressure, in cardiac surgery patients Bart Geerts, Leon Aarts, Johan Groeneveld and Jos
Chapter 10 Predicting cardiac output responses to passive leg raising by a PEEP-induced increase in central venous pressure, in cardiac surgery patients Bart Geerts, Leon Aarts, Johan Groeneveld and Jos
Impedance Cardiography (ICG) Method, Technology and Validity
 Method, Technology and Validity") Method, Technology and Validity Hemodynamic Basics Cardiovascular System Cardiac Output (CO) Mean arterial pressure (MAP) Variable resistance (SVR) Aortic valve Left ventricle Elastic arteries / Aorta
Method, Technology and Validity Hemodynamic Basics Cardiovascular System Cardiac Output (CO) Mean arterial pressure (MAP) Variable resistance (SVR) Aortic valve Left ventricle Elastic arteries / Aorta
NONINVASIVE/MINIMALLY INVASIVE HEMODYNAMIC MONITORING
 DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
Mon patient a une bonne pression artérielle il a a donc un bon débit cardiaque! seminaires iris. Daniel De Backer
 Mon patient a une bonne pression artérielle il a a donc un bon débit cardiaque! Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles
Mon patient a une bonne pression artérielle il a a donc un bon débit cardiaque! Daniel De Backer Head Dept Intensive Care, CHIREC hospitals, Belgium Professor of Intensive Care, Université Libre de Bruxelles
Division of Perioperative and Emergency Medicine, University Medical Center Utrecht, the Netherlands
 04RC1 Advances in cardiovascular monitoring Wolfgang Buhre Division of Perioperative and Emergency Medicine, University Medical Center Utrecht, the Netherlands Saturday, 11 June 2011 13:00-13:45 Room:
04RC1 Advances in cardiovascular monitoring Wolfgang Buhre Division of Perioperative and Emergency Medicine, University Medical Center Utrecht, the Netherlands Saturday, 11 June 2011 13:00-13:45 Room:
SHOCK and the Trauma Victim. JP Pretorius Department of Surgery & SICU Steve Biko Academic Hospital.
 SHOCK and the Trauma Victim JP Pretorius Department of Surgery & SICU Steve Biko Academic Hospital. Classification of Shock Cardiogenic - Myopathic Arrythmic Mechanical Hypovolaemic - Haemorrhagic Non-haemorrhagic
SHOCK and the Trauma Victim JP Pretorius Department of Surgery & SICU Steve Biko Academic Hospital. Classification of Shock Cardiogenic - Myopathic Arrythmic Mechanical Hypovolaemic - Haemorrhagic Non-haemorrhagic
Positive pressure ventilation in cardiogenic shock: friend or foe?
 Positive pressure ventilation in cardiogenic shock: friend or foe? ACCA Masterclass 2017 Josep Masip MD, PhD, FESC Disclosures: Novartis advisor, ThermoFisher consultant, Philips and Orion speaker fees,
Positive pressure ventilation in cardiogenic shock: friend or foe? ACCA Masterclass 2017 Josep Masip MD, PhD, FESC Disclosures: Novartis advisor, ThermoFisher consultant, Philips and Orion speaker fees,
P. Grassi 1, L. Lo Nigro 2, K. Battaglia 1, M. Barone 2, F. Testa 2, G. Berlot 1,2 INTRODUCTION
 ORIGINAL ARTICLE HSR Proc Intensive Care Cardiovasc Anesth. 2013; 5(2): 98-109 98 Pulse pressure variation as a predictor of fluid responsiveness in mechanically ventilated patients with spontaneous breathing
ORIGINAL ARTICLE HSR Proc Intensive Care Cardiovasc Anesth. 2013; 5(2): 98-109 98 Pulse pressure variation as a predictor of fluid responsiveness in mechanically ventilated patients with spontaneous breathing
Sepsis & Beyond Guidelines & Goal-Directed Therapy
 Sepsis & Beyond Guidelines & Goal-Directed Therapy Canadian Association of Critical Care Nurses 2014 Quebec City Presented by: Nicole Kupchik RN, MN, CCNS, CCRN, PCCN Objectives Review the 2012 Surviving
Sepsis & Beyond Guidelines & Goal-Directed Therapy Canadian Association of Critical Care Nurses 2014 Quebec City Presented by: Nicole Kupchik RN, MN, CCNS, CCRN, PCCN Objectives Review the 2012 Surviving
Point-of-Care Ultrasound Closer look at the Inferior Vena Cavae &
 Point-of-Care Ultrasound Closer look at the Inferior Vena Cavae & Brief Introduction to Gross Systolic Function Omar S. Darwish, MS, DO Certified in Point-of-Care Ultrasound Hospitalist University of California,
Point-of-Care Ultrasound Closer look at the Inferior Vena Cavae & Brief Introduction to Gross Systolic Function Omar S. Darwish, MS, DO Certified in Point-of-Care Ultrasound Hospitalist University of California,
An algorithmic approach to the very high risk surgical patient
 An algorithmic approach to the very high risk surgical patient Daniel A. Reuter Center of Anesthesiology and Intensive Care Medicine Hamburg-Eppendorf Universiy Medical Center Disclosures: Member of the
An algorithmic approach to the very high risk surgical patient Daniel A. Reuter Center of Anesthesiology and Intensive Care Medicine Hamburg-Eppendorf Universiy Medical Center Disclosures: Member of the
UPMC Critical Care
 UPMC Critical Care www.ccm.pitt.edu Shock and Monitoring Samuel A. Tisherman, MD, FACS, FCCM Professor Departments of CCM and Surgery University of Pittsburgh Shock Anaerobic metabolism Lactic acidosis
UPMC Critical Care www.ccm.pitt.edu Shock and Monitoring Samuel A. Tisherman, MD, FACS, FCCM Professor Departments of CCM and Surgery University of Pittsburgh Shock Anaerobic metabolism Lactic acidosis
Initial Resuscitation of Sepsis & Septic Shock
 Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known
Initial Resuscitation of Sepsis & Septic Shock Dr. Fatema Ahmed MD (Critical Care Medicine) FCPS (Medicine) Associate professor Dept. of Critical Care Medicine BIRDEM General Hospital Is Sepsis a known