Dr Nora C Hutajulu,SpJP
|
|
|
- Justina Baker
- 6 years ago
- Views:
Transcription
1 Dr Nora C Hutajulu,SpJP
2 BACKGROUND : Rheumatic heart disease is the most serious complication of rheumatic fever. Acute rheumatic fever follows 0,3 % of cases group A beta hemolytic streptoccal pharyngitis in children. As many as 39 % of patients with acute rheumatic fever may develop varying degrees of pancarditis with associated valve insufficiency,heart failure,pericarditis, and even death.
3 Valve lesions and their abbreviations Valve involved Lesion Abbreviation Mitral valve Aortic valve Mitral stenosis Mitral regurgitation Floppy(prolapsing) p mitral valve Aortic stenosis Aortic regurgitation MS MR MVP AS AR Tricuspid valve Tricuspid regurgitation Tricuspid stenosis TR TS Pulmonary valve Pulmonary stenosis Pulmonary regurgitation PS PR
4 Mitral Valve Competence: Integrated function of several anatomic elements Posterior LA wall Anterior & Posterior valve leaflets Chordae tendineae Papillary muscles Left ventricular wall where the papillary muscles attach
5 Mitral Stenosis Causes The most common cause of mitral stenosis (MS) is rheumatic fever. Other causes are: Congenital (Lutembacher s syndrome-ms associated with an atrial septal defect) Malignant-carcinoid (rare). Systemic lupus erythematosus Left atrial myxoma Rheumatic fever causes fusion of the cusps and commissures and thickening of the cusps, which then become immobile and stenosed in a fish-mouth configuration. An immobile valve cannot close properly and is therefore often regurgitant as well.
6 Mitral Stenosis -Pathophysiology Restriction of blood flow from LA LV during diastole. Normal MVA 4-6cm 2. Mild MS 2-4cm 2. Severe MS < 1.0cm 2. MV Pressure gradient MV grad ~ MV flow//mva. Flow = CO/DFP (diastolic filling gp period). As HR increases, diastole shortens disproportionately and MV gradient increases.
7 Clinical features The main presenting features of MS are: Dyspnoea Haemoptysis Palpitations Systemic emboli a recognized complication of atrial fibrillation.
8 Symptoms that are secondary to effects of left atrial enlargement include : Hoarseness due to stretching t of the recurrent laryngeal nerve. Dysphagia due to oesophageal compression. Left lung collapse due to compression of the left main bronchus.
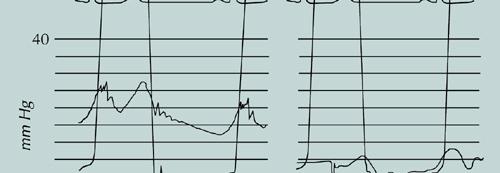
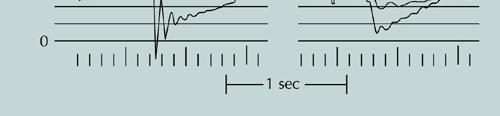
9 On examination The principal clinical findings are: Loud first heart sound (S 1 ) due to the mitral valve slamming shut at the beginning of ventricular systole. A tapping apex beat that is not displaced. opening snap after the second heart sound (S 2 ) followed by a low rumbling mid-diastolic di murmur heard best at the apex with the patients on his or her left side and in expiration. If the patients is in sinus rhythm, the mid-diastolic murmur has a presystolic accentuation; this is absent if the patients has atrial fibrillation. Severity is related to the duration, not the intensity, of the mid-diastolic murmur. If pulmonary hypertension has developed then the pulmonary componentof the second heart sound (P 2 ) is loud and palpable and there may be a right ventricular heave. Tricuspid regurgitation may be present.
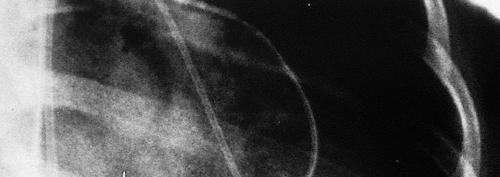
10 Investigations Electrocardiography Chest radiography Echocardiography Cardiac catheterization



11 Mitral Valve Disease Echo findings Mitral Stenosis Thickened, deformed MV leaflets 2D MVA Doppler Gradient Associated LAE, RVH, PHTN, TR,MR, LV function Mitral Regurgitation Determine etiology leaflets, chordae, MVP, MI Doppler severity of MR jet LV function
12 Management Medical management Digoxin or a small dose of a β-blocker (β- adrenoceptor antagonist) t) Anticoagulation with warfarin is recommended in all patients who have MS and atrial fibrillation. Diuretics are used to treat the pulmonary and peripheral p oedema. Surgical management This is indicated in patients who have a mitral valve area of 1 cm 2 or less.
13 Mitral Valve Disease : Treatment Mitral Stenosis Chronic Mitral Regurgitation Medical Rx for Class I & II Medical Rx for mild to mod HR control Dig & BB MR with vasodilators, Anticoagulation diuretics, anticoagulation Afib, >40yrs, LAE, MR, prior embolic event Surgical Rx -Class III &IV Balloon Mitral Valvuloplasty Commissural fusion pliable, noncalcified leaflets No MR of LA thrombus Mitral Valve Surgery Open commissurotomy MV replacement Surgical Rx ideally before LV systolic function declines. MV replacement MV ring & CABG MR repair associated with improved long-term LV funvtion MVP, ruptured chords, infective endocadritis, pap ms rupture.

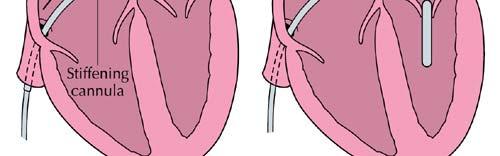

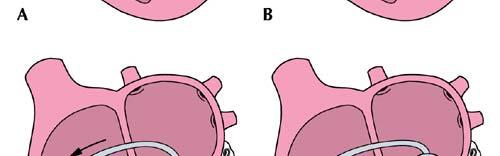
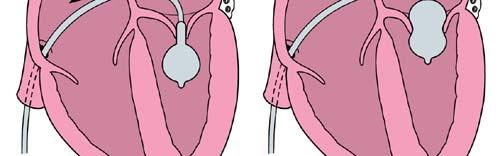
14 Balloon Mitral Commissurotomy
15 Mitral valvuloplasty Mitral valvuloplasty involves the passage of a balloon across the mitral valve and its inflation, so stretching t the stenosed valve. This procedure is carried out via a percutaneous route and only requires a local anaesthetic and light sedation. The following features make a patients unsuitable for this procedure : Marked mitral regurgitation A history of systemic emboli Calcified or thickened rigid mitral valve leaflets.
16 Open mitral valvotomy Open mitral valvotomy is performed under general anaesthetic using a median sternotomy incision and requires cardiopulmonary bypass. It is used in patients who have already had a mitral valvuloplasty or who have mild mitral regurgitation. Closed mitral valvotomy This has now been superseded by mitral valvuloplasty. It does not require cardiopulmonary bypass; a curved incision is made under the left breast. It is worth knowing this because patients in finals examinations may have this scar. Mitral valve replacement
17 Mitral regurgitation The mitral valve may become incompetent for four reasons : Abnormal mitral valve annulus Abnormal mitral valve leaflets Abnormal chordae tendineae Abnormal papillary muscle function
18 Pathophysiology In mitral regurgitation (MR) the regurgitant jet of In mitral regurgitation (MR) the regurgitant jet of blood flows back into the left atrium and with time the left atrium dilates and accommodates the increased backpressure in the pulmonary veins and as the MR worsens pulmonary hypertension develops, which may eventually cause right ventricular hypertrophy and failure.
19 Clinical features Chronic mitral regurgitation develops slowly so allowing the heart to compensate and usually presents with a history of fatigue and dyspnoea. Acute MR presents with severe dyspnoea due to pulmonary oedema.
20 Causes of MR Site of pathology ogy Pathology ogy Mitral annulus Mitral valve leaflets Chordae tendinae Papillary muscle Senile calcification Left ventricular dilatation and enlargement of the annulus Abscess formating during infective endocarditis Infective endocarditis rheumatic fever Prolapsing (floppy) mitral valve Congenital malformation Connective tissue disorders-marfan syndrom, Ehlers- Danlos syndrome Osteogenesis imperfecta, pseudoxanthoma elasticum Idiopathic rupture Myxomatous degeneration Infective endocarditis Connective tissue disorders Myocardial infarction Infiltration-sarcoid, amyloid
21 On examination Atrial fibrillation an irregularly irregular pulse is common, especially in patients who have chronic MR and a dilated left atrium. Jugular venous pressure may be elevated if the patients has developed pulmonary hypertension and right heart failure, or fluid retention The apex is displaced downward and laterally as the left ventricle dilates The murmur of MR is pansystolic and best heard at the apex Signs of congestive cardiac failure P 2 may be loud and there may be a right ventricular heave
22 Floppy mitral valve Investigations Electrocardiography Chest radiography Echocardiography Cardiac catheterization Management Medical management This may consist of diuretics and ACE inhibitors to treat the congestive cardiac failure.
23 Surgical management Patients are considered for surgery if the MR is severe at echocardiography and cardiac catheterization. It is important to act before irreversible left ventricular damage has occurred. Mitral valve repair This may take the form of mitral annuloplasty, repair of a ruptured chorda or reapir of a mitral valve leaflet. These procedures are performed on patients who have mobile non-calcified and nonthickened valves. Mitral valve replacement This is performed if mitral valve repair is not possible. Both repair and replacement of the mitral valve require a median sternotomy incision and cardiopulmonary bypass.
24 Aortic stenosis The most common form of aortic stenosis (AS) is valvular AS; however, aortic stenosis may also occur at the sub-or supravalvular level. Pathophysiology The left ventricular outflow obstruction results in an increased left ventricular pressure. The left ventricle undergoes hypertrophy and more vigorous and prologned contraction to overcome the obstruction and maintain an adequate cardiac output. Myocardial oxygen demand is increased and, because systole is prolonged, diastole is shortened and therefore myocardial blood supply from the coronary arteries is reduced (coronary artery flow occurs during diastole).
25 Causes of AS Type of AS Valvular AS Subvalvular AS Cause Congenital most common, males>females (deformed valve can be uni-, bi-, or tricuspid) Senile calcification Rheumatic fever Severe atherosclerosis Fibrimuscular ring HOCM Supravalvular AS Associated with hypercalcaemia in Williams sydrome, a syndrome associated with elfin facies, mental retardation, strabismus, hypervitaminosis D and hypercalcaemia; the inheritance is autosomal dominant
26 Clinical features Dyspnoea yp may lead to orthopnoea and paroxysmal nocturnal dyspnoea as the left ventricle fails. Angina due to the increased myocardial work and reduced d blood supply (the coronary arteries may be normal). Dizziness and syncope especially on exertion. Sudden death. Systemic emboli.
27 On examination A slow rising, small volume pulse best felt at the carotid pulse. A low blood pressure. Heaving apex beat rarely displaced Ejection systolic murmur at the aortic area radiating to the carotids accompanied by a palpable thrill Signs of left ventricular failure
28 Aortic Stenosis: Physical Findings Severity of AS Mild Moderate Severe Carotid pulse normal Slow rising Parvus et Tardus LV apical impulse normal heaving Heaving & sustained Auscultation S 4 gallop - +/- ++ Systolic + +/- - ejection Click SEM, peaking Early systole midsystole mid-to-late systole S 2 normal Normal or Single or single paradoxical
29 Investigations Electrocardiography Chest radiography Echocardiography Cardiac catheterization Management Medical management Have a negative inotropic effect and result in acute pulmonary oedema Vasodilate the patients, resulting in hypotension because the left ventricle is unable to compensate by increasing cardiac output.
30 Balloon Aortic Valvuloplasty Indications for BAV in critical Aortic Stenosis Younger patients with congenital AS and predominant commissural fusion Bridge to eventual AVR Moderate to severe heart failure/cardiogenic shock Extremely high risk for AVR Urgent/emergent t need for noncardiac surgery Patient with limited lifespan cardiac or noncardiac Patient refuses surgery
31 Surgical management This is considered in all symptomatic patients who have marked stenosis (aortic valve gradient >50 mmhg).without operation the outcome for these patients is very poor. Aortic valve replacement is usually perfomed using a median sternotomy incision and requires cardiopulmonary bypass. Aortic valvuloplasty is performed in children and rarely in the very elderly.
32 Aortic regurgitation Aortic regurgitation (AR) may be due to an abnormality of the valve cusps themselves or dilatation ti of the aortic root and therefore the valve ring. Pathophysiology The regurgitation of blood back into the left ventricle after each systole results in an increased end diastolic volume and an increased stroke volume. The left ventricle works harder and becomes hypertrophied. If the AR worsens the left ventricle may no longer be able to compensate and left ventricular failure will result. If the situation deteriorates further, congestion results. The backpressure from the left ventricle may also cause pulmonary hypertension and right ventricular failure, but this is uncommon.
33 Causes of AR Type of disease Valve disease Aortic root disease Cause Congenital rheumatic fever Infective endocarditis Rheumatoid arthritis SLE Connective tissue disease (e.g. Marfan syndrome, pseudoxanthoma elasticum) Marfan syndrome Osteogenesis imperfecta Type A aortic dissection Ankylosing spondylitis Reiter s syndrome Psoriatic arthritis
34 Clinical features On examination A collapsing high-volume pulse (waterhammer pulse)-due to the increased stroke volume and the rapid run-off of blood back into theleft ventricle after systole. This is better felt at the carotid pulse, but it can also be felt at the radial pulse by lifting the arm and feeling the pulse with the fingers across it. The tapping quality is felt between the examiner s middle and distal interphalangeal joints. A wide pulse pressure on measuring blood pressure. Downward and laterally displaced apex, which has a thrusting nature. Murmur best heard at the left lower sternal edge with the patients sitting forward and in full expiration-it is a soft-pitched early diastolic murmur, which is sometimes difficult to hear, so be sure to listen for it properly with a diaphragm. Increased flow across the aortic valve may produce an ejection systolic murmur. May be signs of left ventricular or congestive failure. Other signs include de Musset s sign (head bobbing with each beat), Quincke s sign (visible capillary pulsation in the nailbed), pistol shot femoral pulses (an audible murmur over the femoral arteries-a to-and-fro sound). The Austin Flint murmur heard when the regurgitant jet causes vibration of the anterior mitral valve leaflet. The murmur is similar to that of MS but with no opening snap.
35 Investigations Electrocardiography Chest radiography Echocardiography Cardiac catheterization
36 Medical management Management The use of diuretics and ACE inhibitors is valuable to treat cardiac failure in these patients. It is, however, important to make the diagnosis and surgically treat this condition before the left ventricle dilates and fails. Surgical management Aortic valve replacement is considered if the patients is symptomatic or if there are signs of progressive left ventricular dilatation. The aortic root may also need to be replaced if it is grossly dilated.
37 Tricuspid regurgitation Causes Most cases of tricuspid regurgitation (TR) are due to dilatation of the tricuspid annulus resulting from dilatation of the right ventricle. This may be due to any cause of right ventricular failure or pulmonary hypertension. Occasionally, the tricuspid valve is affected by infective endocarditis (usually in intravenous drug abusers). Rarer causes include congenital malformations and the carcinoid syndrome.
38 Clinical features The symptoms and signs are due to the backpressure effects of the regurgitant t jet into the right atrium, which h are transmitted to the venous system causing a prominent v wave in the jugular venous waveform. Fatigue and discomfort due to ascites or hepatic congestion are the commonest feature. Patients usually present with symptoms of the disease causing the underlying right ventricular failure;the TR is often an incidental finding. Management The mainstay of management is medical with diuretics and angiotensin-converting enzyme inhibitors to treat the right ventricular failure and fluid overload. Tricuspid valve replacement is considered in very severe cases.
39 Features indicating severity of valve disease Valve disease MS MR AS AR Features Proximity of opening snap to second heart sound and duration of murmur Valve area assessed on echocardiography Evidence of pulmonary hypertension on echocardiography and cardiac catheterization Symptoms and signs of pulmonary oedema Size of regurgitant jet and poor left ventricular function on echocardiography Evidence op pulmonary hypertension on echocardiography and cardiac catheterization Presence of symptoms Low- volume pulse and BP Severity of aortic gradient and poor left venticular function on echocardiography or cardiac catheterization Signs of LVF Left ventricular function and size of regurgitant jet on echocardiography or cardiac catheterization
40 Overview of other valve lesions Valve lesion Cause Clinical features Management Tricuspid stenosis Rheumatic fever; rare Venous congestion JVP raised, large a waves, ascites, hepatomegaly, peripheral oedema, soft deastolic murmur at left lower sternal edge Treat pulmonary hypertension, valve replacement Pulmonary l Congenital If mild asymptomatic, ti if P l l l l t stenosis Pulmonary regurgitation (PR) malformation- Noonan s syndrome, maternal rubella syndrome, carcinoid syndrome Dilatation of the valve ring secondary to pulmonary hypertension, infective endocarditis severe- RVF and cyanosis, ejection systolic murmur in the pulmonary area (second left ICS), wide splittting of second heart sound RVF in severe cases, lowpitched diastolic murmur in pulmonary area, Graham Steel murmur- in severe PR the murmur is high pitched due to the forceful parasternal edge(i.e. similar to that in aortic regurgitation but whith signs of severe pulmonary hypertension and RVF) Pulmonary valvuloplasty or Pulmonary valve replacement Treat underlying disease
41 Types of biological heart disease Type of valve Features Xenograft Manufactured from porcine valve or pericardium and mounted on a frame(on chest x- ray only the mounting ring can be seen) Lasts for about 10 years Homograft Cadaveric valve graft More durable than a xenograft
 between")
42 Normal Valve Function Maintain forward flow and prevent reversal of flow. Valves open and close in response to pressure differences (gradients) between cardiac chambers.
43 Valve Stenosis Abnormal Valve Function Obstruction to valve flow during that phase of the cardiac cycle when the valve is normally open. Hemodynamic hallmark - pressure gradient ~ flow// VA Valve Regurgitation, Insufficiency, Incompetence Inadequate valve closure--- back leakage A single valve can be both stenotic and regurgitant; but both lesions cannot be severe!! Combinations of valve lesions can coexist Single disease process Different disease processes One valve lesion may cause another Certain combinations are particularly burdensome (AS & MR)
44 Mitral Valve Competence: Integrated function of several anatomic elements Posterior LA wall Anterior & Posterior valve leaflets Chordae tendineae Papillary muscles Left ventricular wall where the papillary muscles attach
45 Mitral Valve Disease: Etiology Mitral Stenosis Rheumatic %!!! Congenital Prosthetic valve stenosis Mitral Annular Calcification Left Atrial Myxoma Acute Mitral Regurgitation Infective endocarditis Ischemic Heart disease Papillary ms rupture Mitral valve prolapse Chordal rupture Chest trauma Chronic Mitral Regurgitation Ischemic Heart disease Papillary ms dysfunction Inferior & posterior MI Mitral Valve prolapse Infective endocarditis Rheumatic Prosthetic Mitral annular calcification Cardiomyopathy LV dilatation IHSS
 Forward SV + regurgitant volume LV (LA) dilatation Left Ventricular Volume Overload")
46 Mitral Regurgitation- Pathophysiology h MR: Leakage of blood into LA during systole 1 0 Abnormality -Loss of forward SV into LA Compensatory Mechanisms Increase in SV (& EF) Forward SV + regurgitant volume LV (LA) dilatation Left Ventricular Volume Overload (LVVO)
47 Chronic Mitral Regurgitation - LVVO LVVO LV dilatation Eccentric hypertrophy Increased LA pressure Pulmonary HTN Dyspnea Atrial arrhythmias Low output state
48 Pathophysiology Acute vs Chronic Acute MR Normal (noncompliant) LA Increase LA pressure large V waves Acute Pulmonary Edema Chronic MR Dilated, compliant LA LA pressure normal or slightly increased Fatigue, low output state Atrial arrhythmias- a. fib. Most patients fall between these two extremes!! Mitral Regurgitation ti
49 Mitral Regurgitation: Auscultatory Findings Physical Findings S 1 soft or normal P 2 increased Holosystolic blowing apex MVP mid-systolic click IHSS murmur increases with Valsalva Acute MR descrescendo systolic murmur S 3 gallop & diastolic flow rumble Hyperdynamic Left Ventricle Brisk carotid upstrokes Hyperdynamic LV apical impulse LA lift; RV tap
50 Mitral Stenosis -Pathophysiology Restriction of blood flow from LA LV during diastole. Normal MVA 4-6cm 2. Mild MS 2-4cm 2. Severe MS < 1.0cm 2. MV Pressure gradient MV grad ~ MV flow//mva. Flow = CO/DFP (diastolic filling gp period). As HR increases, diastole shortens disproportionately and MV gradient increases.
51 Relationship between MV gradient and Flow for different Valve Areas Cross hatched area indicates range of normal resting flow. The vertical line represents the threshold for developing pulmonary edema. Pressure gradient increases as flow increases: to a small degree with normal valve area(4-6cm 2 ). to greater degrees with smaller valve areas. in severe stenosis, a significant gradient is present at rest.
52 Mitral Stenosis-Pathophysiology MV gradient Incr LA pr Pulmonary HTN Passive Reactive- 2 nd stenosis RV Pressure Overload RVH RV failure Tricuspid id regurgitation ti Systemic Congestion Paradoxes of MS Disease of Pulm Arts & RV LV unaffected (protected) As RV fails, pulmonary symptoms diminish
53 Mitral Stenosis- Clinical Symptoms Symptoms related to severity of MVA reduction- Symptoms unrelated to severity of MS- Atrial fibrillationill Systemic thromboembolism Symptoms due to Pulmonary HTN and RV failure- Fatigue, low output state Peripheral edema and hepato-splenomegaly Hoarseness recurrent laryngeal nerve palsy
54 Mitral Stenosis: Physical Findings Auscultatory findings S 1 variable intensity; increased early, progressively decreases OS opening snap, variable intensity A 2-OS interval varies inversely with severity of MS; shortens as MVA diminishes Low-pitched diastolic apex Duration of murmur correlates with severity of MS Pre-systolic accentuation Increased P 2 Body habitus thin, asthenic, female Low BP LA lift & RV tap
55 Mitral Valve Disease Echo findings Mitral Stenosis Thickened, deformed MV leaflets 2D MVA Doppler Gradient Associated LAE, RVH, PHTN, TR,MR, LV function Mitral Regurgitation Determine etiology leaflets, chordae, MVP, MI Doppler severity of MR jet LV function
56 Mitral Valve Disease : Treatment Mitral Stenosis Chronic Mitral Regurgitation Medical Rx for Class I & II Medical Rx for mild to mod HR control Dig & BB MR with vasodilators, Anticoagulation diuretics, anticoagulation Afib, >40yrs, LAE, MR, prior embolic event Surgical Rx -Class III &IV Balloon Mitral Valvuloplasty Commissural fusion pliable, noncalcified leaflets No MR of LA thrombus Mitral Valve Surgery Open commissurotomy MV replacement Surgical Rx ideally before LV systolic function declines. MV replacement MV ring & CABG MR repair associated with improved long-term LV funvtion MVP, ruptured chords, infective endocadritis, pap ms rupture.
57 Balloon Mitral Commissurotomy
58 Aortic Valve Disease: Etiology Aortic Stenosis Degenerative calcific (senile) Congenital Uni or bicuspid Rheumatic Prosthetic Acute Aortic Insufficiency Infective endocarditis Acute Aortic Dissection Marfan s Syndrome Chest trauma Chronic Aortic Insufficiency Aortic leaflet disease Infective endocarditis Rheumatic Bicuspid Aortic valve Prolapse & congenital VSD Prosthetic Aortic root disease Aortic aneurysm/dissection Marfan s syndrome Connective tissue disorders Syphilis HTN Annulo-aortic ectasia
59 Aortic Stenosis - Pathophysiology Normal AVA cm 2 Severe AS <1.0cm 2 Critical AS <0.7cm 2 ; <0.5cm 2 /m 2 Hemodynamic Hallmark Systolic pressure gradient AV grad ~ AV flow//ava AV flow = CO/SEP (systolic ejection period) mmHg gradients are common in severe AS
60 Relationship between AV gradient and Flow for different Aortic valve areas. Like Mitral Stenosis as flow increases so does the gradient. Unlike Mitral Stenosis Resting flows are higher smaller AV area shorter SEP Larger gradients Significant (>50mmHg) gradient can be present at rest in asymptomatic individuals.
61 Pathophysiology of Aortic Stenosis- LVPO Chronic LV Pressure Overload Concentric LVH Stiff noncompliant LV Increased LVEDP Increased LV mass Increased MVO 2 Well tolerated for decades LV fails CHF Atrial fibrillation Poorly tolerated Loss of atrial kick Rapid HR Acute pulmonary edema and hypotension.
62 Aortic Stenosis: Natural History & Clinical i l Symptoms Asymptomatic for many Natural History Studiesyears Pts grad 25mmHg 20% Symptoms develop chance of intervention in 15 years when valve is critically narrowed and LV function deteriorates Bicuspid AV 5 th -6 th decade Senile AS 7 th -8 th decades Classic Symptom Triad Angina pectoris 5 years CHF 1-2 years Syncope 2-3 years Sudden Death Pts with asymptomatic severe AS require close f/u Gradient progression 6-10mmHg/yr Risk Factors Age > 70 CAD, hyperlipidemia Chronic renal failure
63 Aortic Stenosis: Physical Findings Severity of AS Mild Moderate Severe Carotid pulse normal Slow rising Parvus et Tardus LV apical impulse normal heaving Heaving & sustained Auscultation S 4 gallop - +/- ++ Systolic + +/- - ejection Click SEM, peaking Early systole midsystole mid-to-late systole S 2 normal Normal or Single or single paradoxical
64 Aortic Insufficiency- Pathophysiology 1 0 abnormality LVVO Severity of LVVO Size of regurgitant orifice Diastolic pressure gradient between Ao & LV HR or duration of diastole Compensatory Mechanisms LV dilatation & eccentric LVH Increased LV diastolic compliance Peripheral vasodilation
65 LV Volume vs Pressure Overload Feature LVPO (AS) LVVO (MR,AI) LV Volume normal Dilated** Wall thickness Conc. LVH Normal to slightly increased LV compliance stiff Increased noncompliant compliance LV diastolic Pr increased Normal to slightly increased LV systolic Pr Increased** Normal to slightly increased LVEF normal increased
66 Acute vs Chronic AR Pathophysiology and Clinical Presentation Acute Aortic Regurgitation Sudden AoV incompetence Noncompliant LV Acute Pulmonary Edema Emergency AVR Chronic Aortic Regurgitation Long asymptomatic phase Progressive LV dilatation DOE, orthopnea, PND Frequent PVC s
67 Chronic Aortic Regurgitation: Physical Findings Widened Pulse Pressure > 70mmHg (170/60) Low diastolic pressure <60mmHg Hyperdynamic LV DeMusset s signs Corrigan s pulse Quincke s pulsations, Durozier s murmur Auscultation: Diminished A 2 Descrescendo diastolic blowing LSB Austin-Flint murmur diastolic flow apex Due to interference with trans-mitral filling by impignement from aortic regurgitant jet. DDx - mitral stenosis(increases intensity with amyl nitrite)
68 Aortic Valve Disease: Diagnostic Testing Aortic Stenosis Aortic regurgitaiton g EKG- NSR, LVH with strain, LAE,LAD CXRay frequently normal 2D-ECHO Aortic cusps thickened, calcified, decreased mobility Assessment of LVH & LV systolic function Concomitant MR, AR Doppler assesment of AoV gradient Planimetry of AV area EKG- LVH without strain CXRay- Chronic AI cor bovinum Acute AI pulmonary edema with nl heart size 2D ECHO Assess Ao valve and root Assess LV function/dilatation LVES dimension>55mm Doppler severity of regurgitant jet
69 Relationship between AV gradient and Flow for different Aortic valve areas. Like Mitral Stenosis as flow increases so does the gradient. Unlike Mitral Stenosis Resting flows are higher smaller AV area shorter SEP Larger gradients Significant (>50mmHg) gradient can be present at rest in asymptomatic individuals.
70 Balloon Aortic Valvuloplasty Indications for BAV in critical Aortic Stenosis Younger patients with congenital AS and predominant commissural fusion Bridge to eventual AVR Moderate to severe heart failure/cardiogenic shock Extremely high risk for AVR Urgent/emergent t need for noncardiac surgery Patient with limited lifespan cardiac or noncardiac Patient refuses surgery




71 Aortic Valve Surgery: Ross Procedure Autotransplant of pulmonic valve to the aortic position Reimplantation of the coronary arteries Homograft valve in the pulmonic position Indications Younger patients No anticoagulation Requires similar sized aortic and pulmonic roots
72 Valvular Heart Disease The End
73
The production of murmurs is due to 3 main factors:
 Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
The production of murmurs is due to 3 main factors:
 Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
Heart murmurs The production of murmurs is due to 3 main factors: high blood flow rate through normal or abnormal orifices forward flow through a narrowed or irregular orifice into a dilated vessel or
What Is Valvular Heart Disease? Heart valve disease occurs when your heart's valves do not work the way they should.
 What Is Valvular Heart Disease? Heart valve disease occurs when your heart's valves do not work the way they should. How Do Heart Valves Work? MAINTAIN ONE-WAY BLOOD FLOW THROUGH YOUR HEART The four heart
What Is Valvular Heart Disease? Heart valve disease occurs when your heart's valves do not work the way they should. How Do Heart Valves Work? MAINTAIN ONE-WAY BLOOD FLOW THROUGH YOUR HEART The four heart
Valvular Heart Disease. Dr. HANAN ALBACKR
 Valvular Heart Disease Dr. HANAN ALBACKR Valvular Heart Disease Format for this lecture IMPORTANT CLINICAL INFO know for boards, tests and clinical practice Spectrum of VHD Aortic Valve Mitral Valve Tricuspid
Valvular Heart Disease Dr. HANAN ALBACKR Valvular Heart Disease Format for this lecture IMPORTANT CLINICAL INFO know for boards, tests and clinical practice Spectrum of VHD Aortic Valve Mitral Valve Tricuspid
Mitral Valve Disease. Prof. Sirchak Yelizaveta Stepanovna
 Mitral Valve Disease Prof. Sirchak Yelizaveta Stepanovna Fall 2008 Mitral Valve Stenosis Lecture Outline Mitral Stenosis Mitral Regurgitation Etiology Pathophysiology Clinical features Diagnostic testing
Mitral Valve Disease Prof. Sirchak Yelizaveta Stepanovna Fall 2008 Mitral Valve Stenosis Lecture Outline Mitral Stenosis Mitral Regurgitation Etiology Pathophysiology Clinical features Diagnostic testing
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease Mitral Stenosis
 Valvular Heart Disease Mitral Stenosis A 75 year old woman with loud first heart sound and mid-diastolic murmur Chronic dyspnea Class 2/4 Fatigue Recent orthopnea/pnd Nocturnal palpitation Pedal edema
Valvular Heart Disease Mitral Stenosis A 75 year old woman with loud first heart sound and mid-diastolic murmur Chronic dyspnea Class 2/4 Fatigue Recent orthopnea/pnd Nocturnal palpitation Pedal edema
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease General Principles Etiology Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease General Principles Etiology Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
MITRAL VALVE DISEASE- ASSESSMENT AND MANAGEMENT. Irene Frantzis P year, SGUL Sheba Medical Center
 MITRAL VALVE DISEASE- ASSESSMENT AND MANAGEMENT Irene Frantzis P year, SGUL Sheba Medical Center MITRAL VALVE DISEASE Mitral Valve Regurgitation Mitral Valve Stenosis Mitral Valve Prolapse MITRAL REGURGITATION
MITRAL VALVE DISEASE- ASSESSMENT AND MANAGEMENT Irene Frantzis P year, SGUL Sheba Medical Center MITRAL VALVE DISEASE Mitral Valve Regurgitation Mitral Valve Stenosis Mitral Valve Prolapse MITRAL REGURGITATION
8/31/2016. Mitraclip in Matthew Johnson, MD
 Mitraclip in 2016 Matthew Johnson, MD 1 Abnormal Valve Function Valve Stenosis Obstruction to valve flow during that phase of the cardiac cycle when the valve is normally open. Hemodynamic hallmark - pressure
Mitraclip in 2016 Matthew Johnson, MD 1 Abnormal Valve Function Valve Stenosis Obstruction to valve flow during that phase of the cardiac cycle when the valve is normally open. Hemodynamic hallmark - pressure
Valvular Heart Disease
 Valvular Heart Disease MITRAL STENOSIS Pathophysiology rheumatic fever. calcific degeneration, malignant carcinoid disease, congenital mitral stenosis. SLE. The increased pressure gradient across the mitral
Valvular Heart Disease MITRAL STENOSIS Pathophysiology rheumatic fever. calcific degeneration, malignant carcinoid disease, congenital mitral stenosis. SLE. The increased pressure gradient across the mitral
Aortic Valve Lesions
 Version 1.0 Valvular Heart Disease 25/03/2012 Aortic Stenosis Aortic Valve Lesions General Most common isolated affected valve, esp elderly 4M:1F Unrecognised can be important cause of anaesthetic & obstetric
Version 1.0 Valvular Heart Disease 25/03/2012 Aortic Stenosis Aortic Valve Lesions General Most common isolated affected valve, esp elderly 4M:1F Unrecognised can be important cause of anaesthetic & obstetric
Cardiac Ausculation in the Elderly
 Cardiac Ausculation in the Elderly 박성하 신촌세브란스병원심장혈관병원심장내과 Anatomy Surface projection of the Heart and Great Vessels Evaluating pulsation Superior vena cava Rt. pulmonary artery Right atrium Right ventricle
Cardiac Ausculation in the Elderly 박성하 신촌세브란스병원심장혈관병원심장내과 Anatomy Surface projection of the Heart and Great Vessels Evaluating pulsation Superior vena cava Rt. pulmonary artery Right atrium Right ventricle
For more information about how to cite these materials visit
 Author: Michael Shea, M.D., 2008 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Share Alike 3.0 License: http://creativecommons.org/licenses/by-sa/3.0/
Author: Michael Shea, M.D., 2008 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Share Alike 3.0 License: http://creativecommons.org/licenses/by-sa/3.0/
Tricuspid and Pulmonic Valve Disease
 Chapter 31 Tricuspid and Pulmonic Valve Disease David A. Tate Acquired disease of the right-sided cardiac valves is much less common than disease of the leftsided counterparts, possibly because of the
Chapter 31 Tricuspid and Pulmonic Valve Disease David A. Tate Acquired disease of the right-sided cardiac valves is much less common than disease of the leftsided counterparts, possibly because of the
TSDA Boot Camp September 13-16, Introduction to Aortic Valve Surgery. George L. Hicks, Jr., MD
 TSDA Boot Camp September 13-16, 2018 Introduction to Aortic Valve Surgery George L. Hicks, Jr., MD Aortic Valve Pathology and Treatment Valvular Aortic Stenosis in Adults Average Course (Post mortem data)
TSDA Boot Camp September 13-16, 2018 Introduction to Aortic Valve Surgery George L. Hicks, Jr., MD Aortic Valve Pathology and Treatment Valvular Aortic Stenosis in Adults Average Course (Post mortem data)
Valvular Heart Disease: Recognition and Management in the Outpatient Setting
 Valvular Heart Disease: Recognition and Management in the Outpatient Setting Ian S. Harris UCSF Division of Cardiology Case 1: 80 year old man with a history of hypertension, complaining of exertional
Valvular Heart Disease: Recognition and Management in the Outpatient Setting Ian S. Harris UCSF Division of Cardiology Case 1: 80 year old man with a history of hypertension, complaining of exertional
Mitral Valve Disease. Chapter 29
 Chapter 29 Mitral Valve Disease Thomas R. Griggs Mitral valve leaflets consist of thin, pliable, fibrous material. The two leaflets anterior and posterior open by unfolding against the ventricular wall
Chapter 29 Mitral Valve Disease Thomas R. Griggs Mitral valve leaflets consist of thin, pliable, fibrous material. The two leaflets anterior and posterior open by unfolding against the ventricular wall
MITRAL STENOSIS. Joanne Cusack
 MITRAL STENOSIS Joanne Cusack BSE Breakdown Recognition of rheumatic mitral stenosis Qualitative description of valve and sub-valve calcification and fibrosis Measurement of orifice area by planimetry
MITRAL STENOSIS Joanne Cusack BSE Breakdown Recognition of rheumatic mitral stenosis Qualitative description of valve and sub-valve calcification and fibrosis Measurement of orifice area by planimetry
Uptofate Study Summary
 CONGENITAL HEART DISEASE Uptofate Study Summary Acyanotic Atrial septal defect Ventricular septal defect Patent foramen ovale Patent ductus arteriosus Aortic coartation Pulmonary stenosis Cyanotic Tetralogy
CONGENITAL HEART DISEASE Uptofate Study Summary Acyanotic Atrial septal defect Ventricular septal defect Patent foramen ovale Patent ductus arteriosus Aortic coartation Pulmonary stenosis Cyanotic Tetralogy
Heart sounds and murmurs. Dr. Szathmári Miklós Semmelweis University First Department of Medicine 15. Oct
 Heart sounds and murmurs Dr. Szathmári Miklós Semmelweis University First Department of Medicine 15. Oct. 2013. Conditions for auscultation of the heart Quiet room Patient comfortable Chest fully exposed
Heart sounds and murmurs Dr. Szathmári Miklós Semmelweis University First Department of Medicine 15. Oct. 2013. Conditions for auscultation of the heart Quiet room Patient comfortable Chest fully exposed
HISTORY. Question: How do you interpret the patient s history? CHIEF COMPLAINT: Dyspnea of two days duration. PRESENT ILLNESS: 45-year-old man.
 HISTORY 45-year-old man. CHIEF COMPLAINT: Dyspnea of two days duration. PRESENT ILLNESS: His dyspnea began suddenly and has been associated with orthopnea, but no chest pain. For two months he has felt
HISTORY 45-year-old man. CHIEF COMPLAINT: Dyspnea of two days duration. PRESENT ILLNESS: His dyspnea began suddenly and has been associated with orthopnea, but no chest pain. For two months he has felt
Ethiology of the disease - What may cause it?: One of the following numerous causes can cause aortic regurgitation:
 AORTIC REGURGITATION Aortic regurgitation is one of the aortic valve diseases, the aorta being the artery that brings oxygenated blood to the systemic circulation. The other one is the aortic valve stenosis.
AORTIC REGURGITATION Aortic regurgitation is one of the aortic valve diseases, the aorta being the artery that brings oxygenated blood to the systemic circulation. The other one is the aortic valve stenosis.
Heart Valve disease: MR. AS tough patient When to echo, When to refer, What s new
 Heart Valve disease: MR. AS tough patient When to echo, When to refer, What s new B. Sonnenberg UAH Cardiology CME Day 5 May 2015 Disclosures Speaker s or Advisory Boards: none Research grants: none (co-investigator
Heart Valve disease: MR. AS tough patient When to echo, When to refer, What s new B. Sonnenberg UAH Cardiology CME Day 5 May 2015 Disclosures Speaker s or Advisory Boards: none Research grants: none (co-investigator
Valvular Stenosis and Regurgitation: Barriers to Flow
 Valvular Stenosis and Regurgitation: Barriers to Flow Presented By: Cynthia Webner BSN, RN,CCRN-CMC www.cardionursing.com CNEA 2009 1 Cardiac Valves Prevent Backward Flow Permit Forward Flow 2 www.cardionursing.com
Valvular Stenosis and Regurgitation: Barriers to Flow Presented By: Cynthia Webner BSN, RN,CCRN-CMC www.cardionursing.com CNEA 2009 1 Cardiac Valves Prevent Backward Flow Permit Forward Flow 2 www.cardionursing.com
By the end of this session, the student should be able to:
 Valvular Heart disease HVD By Dr. Ashraf Abdelfatah Deyab VHD- Objectives By the end of this session, the student should be able to: Define and classify valvular heart disease. Enlist the causes of acquired
Valvular Heart disease HVD By Dr. Ashraf Abdelfatah Deyab VHD- Objectives By the end of this session, the student should be able to: Define and classify valvular heart disease. Enlist the causes of acquired
2) VSD & PDA - Dr. Aso
 VSD & PDA - Dr. Aso") 2) VSD & PDA - Dr. Aso Ventricular Septal Defect (VSD) Most common cardiac malformation 25-30 % Types of VSD: According to position perimembranous, inlet, muscular. According to size small, medium, large.
2) VSD & PDA - Dr. Aso Ventricular Septal Defect (VSD) Most common cardiac malformation 25-30 % Types of VSD: According to position perimembranous, inlet, muscular. According to size small, medium, large.
CARDIAC EXAMINATION MINI-QUIZ
 CARDIAC EXAMINATION MINI-QUIZ 1. Sitting bolt upright, your dyspneic (short of breath) patient has visible jugular venous pulsations to the angle of his jaw, which is 12 cm above his sternal angle. What
CARDIAC EXAMINATION MINI-QUIZ 1. Sitting bolt upright, your dyspneic (short of breath) patient has visible jugular venous pulsations to the angle of his jaw, which is 12 cm above his sternal angle. What
Valvular Heart Disease
 GP Update Refresher 18 th January 2018 Valvular Heart Disease Dr. Alexander Lyon Senior Lecturer and Consultant Cardiologist Clinical Lead in Cardio-Oncology Royal Brompton Hospital, London UK President
GP Update Refresher 18 th January 2018 Valvular Heart Disease Dr. Alexander Lyon Senior Lecturer and Consultant Cardiologist Clinical Lead in Cardio-Oncology Royal Brompton Hospital, London UK President
Physical Exam Part II
 Physical Exam Part II University of Michigan Cardiovascular Center Kim A. Eagle, MD Albion Walter Hewlett Professor Director Physical Exam: Part II Heart Sounds Heart Murmurs HEART SOUNDS S1 MITRAL + TRICUSPID
Physical Exam Part II University of Michigan Cardiovascular Center Kim A. Eagle, MD Albion Walter Hewlett Professor Director Physical Exam: Part II Heart Sounds Heart Murmurs HEART SOUNDS S1 MITRAL + TRICUSPID
Murmur Sounds made by turbulence in the heart or blood stream. 1. Timing. 5. Intensity 2. Shape. 6. Pitch 3. Location of maximum intensity
 Definition Items in description of Timing Shape Location of maximum intensity Murmur Sounds made by turbulence in the heart or blood stream. 1. Timing 5. Intensity 2. Shape 6. Pitch 3. Location of maximum
Definition Items in description of Timing Shape Location of maximum intensity Murmur Sounds made by turbulence in the heart or blood stream. 1. Timing 5. Intensity 2. Shape 6. Pitch 3. Location of maximum
M-Mode Echocardiography Is it still Alive? Itzhak Kronzon, MD,FASE. Sampling Rate M-Mode: 1800 / sec 2D: 30 / sec
 M-Mode Echocardiography Is it still Alive? Itzhak Kronzon, MD,FASE Honoraria: Philips Classical M-mode Echocardiography M-Mode offers better time and image resolution. Sampling Rate M-Mode: 1800 / sec
M-Mode Echocardiography Is it still Alive? Itzhak Kronzon, MD,FASE Honoraria: Philips Classical M-mode Echocardiography M-Mode offers better time and image resolution. Sampling Rate M-Mode: 1800 / sec
Anaesthesia for non-cardiac surgery in patients left ventricular outflow tract obstruction (LVOTO)
") Anaesthesia for non-cardiac surgery in patients left ventricular outflow tract obstruction (LVOTO) Dr. Siân Jaggar Consultant Anaesthetist Royal Brompton Hospital London UK Congenital Cardiac Services
Anaesthesia for non-cardiac surgery in patients left ventricular outflow tract obstruction (LVOTO) Dr. Siân Jaggar Consultant Anaesthetist Royal Brompton Hospital London UK Congenital Cardiac Services
n S2=Aortic valve closure, pulmonic n S3=Very healthy or very sick LV n Children and young athletes, CHF n S4=Stiff LV, incr LVEDP, HTN, hypertrophy
 Cardiac Physical Exam Valvular Heart Disease Susan Schima MD September 29, 2015 S1=mitral valve closure (can t really hear tricuspid component) S2=Aortic valve closure, pulmonic S3=Very healthy or very
Cardiac Physical Exam Valvular Heart Disease Susan Schima MD September 29, 2015 S1=mitral valve closure (can t really hear tricuspid component) S2=Aortic valve closure, pulmonic S3=Very healthy or very
Congenital. Unicuspid Bicuspid Quadricuspid
 David Letterman s Top 10 Aortic Stenosis The victim can be anyone: Echo is the question and the answer!!!! Hilton Head Island Echocardiography Conference 2012 Timothy E. Paterick, MD, JD, MBA Christopher
David Letterman s Top 10 Aortic Stenosis The victim can be anyone: Echo is the question and the answer!!!! Hilton Head Island Echocardiography Conference 2012 Timothy E. Paterick, MD, JD, MBA Christopher
Valvular Heart Disease
 Valvular Heart Disease Objectives: Etiology of valve diseases Pathogenesis Clinical presentation Clinical findings Investigation Management Team Members: Duaa abdulfattah, Basil Almeflh, Jawaher Abanumy,
Valvular Heart Disease Objectives: Etiology of valve diseases Pathogenesis Clinical presentation Clinical findings Investigation Management Team Members: Duaa abdulfattah, Basil Almeflh, Jawaher Abanumy,
Section V VALVULAR HEART T DISEASE. Chapter 27 Aortic Stenosis Chapter 28 Aortic Insufficiency Chapter 29 Mitral Valve Disease...
 Section V VALVULAR HEART T DISEASE Chapter 27 Aortic Stenosis........................... 256 Chapter 28 Aortic Insufficiency....................... 265 Chapter 29 Mitral Valve Disease......................
Section V VALVULAR HEART T DISEASE Chapter 27 Aortic Stenosis........................... 256 Chapter 28 Aortic Insufficiency....................... 265 Chapter 29 Mitral Valve Disease......................
HISTORY. Question: What category of heart disease is suggested by the fact that a murmur was heard at birth?
 HISTORY 23-year-old man. CHIEF COMPLAINT: Decreasing exercise tolerance of several years duration. PRESENT ILLNESS: The patient is the product of an uncomplicated term pregnancy. A heart murmur was discovered
HISTORY 23-year-old man. CHIEF COMPLAINT: Decreasing exercise tolerance of several years duration. PRESENT ILLNESS: The patient is the product of an uncomplicated term pregnancy. A heart murmur was discovered
Aortic stenosis and regurgitation
 1 Aortic stenosis and regurgitation valvuloplasty and replacement Mitral regurgitation and stenosis valvuloplasty and repair/replacement 2 ASD PFO VSD PDA occlusion Left atrial appendage occlusion for
1 Aortic stenosis and regurgitation valvuloplasty and replacement Mitral regurgitation and stenosis valvuloplasty and repair/replacement 2 ASD PFO VSD PDA occlusion Left atrial appendage occlusion for
Adult Cardiac Surgery
 Adult Cardiac Surgery Mahmoud ABU-ABEELEH Associate Professor Department of Surgery Division of Cardiothoracic Surgery School of Medicine University Of Jordan Adult Cardiac Surgery: Ischemic Heart Disease
Adult Cardiac Surgery Mahmoud ABU-ABEELEH Associate Professor Department of Surgery Division of Cardiothoracic Surgery School of Medicine University Of Jordan Adult Cardiac Surgery: Ischemic Heart Disease
See below for descriptions of the waveform
 The internal jugular vein (IJV) connects to the right atrium without any intervening valves. The pulsation of the right atrium therefore causes the column of blood in the IJV to rise and fall this is called
The internal jugular vein (IJV) connects to the right atrium without any intervening valves. The pulsation of the right atrium therefore causes the column of blood in the IJV to rise and fall this is called
Which one of the following echocardiographic profiles most strongly indicates the need for aortic valve replacement? FS [
 Question 46 A 45-year-old asymptomatic man returns for follow-up. He was diagnosed 10 years ago with aortic regurgitation due to a congentia lbicuspid aortic valve, He has never had endocarditis Which
Question 46 A 45-year-old asymptomatic man returns for follow-up. He was diagnosed 10 years ago with aortic regurgitation due to a congentia lbicuspid aortic valve, He has never had endocarditis Which
Clinical significance of cardiac murmurs: Get the sound and rhythm!
 Clinical significance of cardiac murmurs: Get the sound and rhythm! Prof. dr. Gunther van Loon, DVM, PhD, Ass Member ECVDI, Dip ECEIM Dept. of Large Animal Internal Medicine Ghent University, Belgium Murmurs
Clinical significance of cardiac murmurs: Get the sound and rhythm! Prof. dr. Gunther van Loon, DVM, PhD, Ass Member ECVDI, Dip ECEIM Dept. of Large Animal Internal Medicine Ghent University, Belgium Murmurs
PROSTHETIC VALVE BOARD REVIEW
 PROSTHETIC VALVE BOARD REVIEW The correct answer D This two chamber view shows a porcine mitral prosthesis with the typical appearance of the struts although the leaflets are not well seen. The valve
PROSTHETIC VALVE BOARD REVIEW The correct answer D This two chamber view shows a porcine mitral prosthesis with the typical appearance of the struts although the leaflets are not well seen. The valve
HISTORY. Question: What category of heart disease is suggested by this history? CHIEF COMPLAINT: Heart murmur present since early infancy.
 HISTORY 18-year-old man. CHIEF COMPLAINT: Heart murmur present since early infancy. PRESENT ILLNESS: Although normal at birth, a heart murmur was heard at the six week check-up and has persisted since
HISTORY 18-year-old man. CHIEF COMPLAINT: Heart murmur present since early infancy. PRESENT ILLNESS: Although normal at birth, a heart murmur was heard at the six week check-up and has persisted since
Valvular Heart Disease
 Valvular Heart Disease B K Singh, MD, FACC Disclosures: None 1 CARDIAC CYCLE S2 S2=A2P2 S1=M1T1 S4 S1 S3 2 JVP Carotid S1 Slitting of S2 S3 S4 Ejection click Opening snap Dynamic Auscultation What is the
Valvular Heart Disease B K Singh, MD, FACC Disclosures: None 1 CARDIAC CYCLE S2 S2=A2P2 S1=M1T1 S4 S1 S3 2 JVP Carotid S1 Slitting of S2 S3 S4 Ejection click Opening snap Dynamic Auscultation What is the
Congestive Heart Failure Patient Profile. Patient Identity - Mr. Douglas - 72 year old man - No drugs, smokes, moderate social alcohol consumption
 Congestive Heart Failure Patient Profile Patient Identity - Mr. Douglas - 72 year old man - No drugs, smokes, moderate social alcohol consumption Chief Complaint - SOB - When asked: Increasing difficulty
Congestive Heart Failure Patient Profile Patient Identity - Mr. Douglas - 72 year old man - No drugs, smokes, moderate social alcohol consumption Chief Complaint - SOB - When asked: Increasing difficulty
Mitral Stenosis: A Review
 Cardiovascular Innovations and Applications Vol. x No. x (2016) x x ISSN 2009-8618 DOI 10.15212/CVIA.2016.0041 REVIEW Mitral Stenosis: A Review By C. Richard Conti, MD, MACC 1 1 Department of Medicine,
Cardiovascular Innovations and Applications Vol. x No. x (2016) x x ISSN 2009-8618 DOI 10.15212/CVIA.2016.0041 REVIEW Mitral Stenosis: A Review By C. Richard Conti, MD, MACC 1 1 Department of Medicine,
2. The heart sounds are produced by a summed series of mechanical events, as follows:
 Heart Sounds. Phonocardiography 1 Objectives 1. Phonocardiography - Definition 2. What produces the heart sounds 3. Where to listen for the heart sounds 4. How to record a phonocardiogram 5. Normal heart
Heart Sounds. Phonocardiography 1 Objectives 1. Phonocardiography - Definition 2. What produces the heart sounds 3. Where to listen for the heart sounds 4. How to record a phonocardiogram 5. Normal heart
Comprehensive Cardiology: Matters of the Heart Class III SARAH BEANLANDS RN BSCN MSC
 Comprehensive Cardiology: Matters of the Heart Class III SARAH BEANLANDS RN BSCN MSC Overview ACS continued Heart Failure Valvular Disorders and Endocarditis Diagnosis Nuclear stress test- stable angina
Comprehensive Cardiology: Matters of the Heart Class III SARAH BEANLANDS RN BSCN MSC Overview ACS continued Heart Failure Valvular Disorders and Endocarditis Diagnosis Nuclear stress test- stable angina
Cardiology. the Sounds: #7 HCM. LV Outflow Obstruction: Aortic Stenosis. (Coming Soon - HCM)
") A Cardiology HCM LV Outflow Obstruction: Aortic Stenosis (Coming Soon - HCM) the Sounds: #7 Howard J. Sachs, MD www.12daysinmarch.com E-mail: Howard@12daysinmarch.com Aortic Valve Disorders Stenosis Regurgitation
A Cardiology HCM LV Outflow Obstruction: Aortic Stenosis (Coming Soon - HCM) the Sounds: #7 Howard J. Sachs, MD www.12daysinmarch.com E-mail: Howard@12daysinmarch.com Aortic Valve Disorders Stenosis Regurgitation
Cor pulmonale. Dr hamid reza javadi
 1 Cor pulmonale Dr hamid reza javadi 2 Definition Cor pulmonale ;pulmonary heart disease; is defined as dilation and hypertrophy of the right ventricle (RV) in response to diseases of the pulmonary vasculature
1 Cor pulmonale Dr hamid reza javadi 2 Definition Cor pulmonale ;pulmonary heart disease; is defined as dilation and hypertrophy of the right ventricle (RV) in response to diseases of the pulmonary vasculature
Valvular Heart Disease: Volume Versus Pressure and the Hemodynamic Compromise
 Valvular Heart Disease: Volume Versus Pressure and the Hemodynamic Compromise Cynthia Webner BSN, RN, CCRN, CMC www.cardionursing.com NTI 2009 Class Code 112 1 Mastery is not something that strikes in
Valvular Heart Disease: Volume Versus Pressure and the Hemodynamic Compromise Cynthia Webner BSN, RN, CCRN, CMC www.cardionursing.com NTI 2009 Class Code 112 1 Mastery is not something that strikes in
Aortic valve disease. Acknowledgement for slides. Heart Valves 4/28/2018. Adopted from
 Aortic valve disease Senthil Kumar, MD 4.26.2018 28 th Annual Coming Together in Advanced Practice Conference Acknowledgement for slides Adopted from http://www.slideshare.net/ Dr. Anand Chockalingam Dr.
Aortic valve disease Senthil Kumar, MD 4.26.2018 28 th Annual Coming Together in Advanced Practice Conference Acknowledgement for slides Adopted from http://www.slideshare.net/ Dr. Anand Chockalingam Dr.
1. how a careful cardiovascular evaluation can accurately assess pathology and physiology at the bedside, and
 This program will demonstrate: 1. how a careful cardiovascular evaluation can accurately assess pathology and physiology at the bedside, and 2. the importance of integrating this information with selected
This program will demonstrate: 1. how a careful cardiovascular evaluation can accurately assess pathology and physiology at the bedside, and 2. the importance of integrating this information with selected
Congenital Heart Disease Cases
 Congenital Heart Disease Cases Sabrina Phillips, MD FACC FASE Mayo Clinic Congenital Heart Disease Center 2013 MFMER slide-1 No Disclosures 2013 MFMER slide-2 1 CASE 1 2013 MFMER slide-3 63 year old Woman
Congenital Heart Disease Cases Sabrina Phillips, MD FACC FASE Mayo Clinic Congenital Heart Disease Center 2013 MFMER slide-1 No Disclosures 2013 MFMER slide-2 1 CASE 1 2013 MFMER slide-3 63 year old Woman
Cardiac Examination. Pediatrics Clinical Examination
 Pediatrics Clinical Examination Symptoms of Cardiovascular Affection: Cardiac Examination 1. Perinatal history: Maternal DM, cyanosis, respiratory distress 2. Symptoms of lung congestion: Poor interrupted
Pediatrics Clinical Examination Symptoms of Cardiovascular Affection: Cardiac Examination 1. Perinatal history: Maternal DM, cyanosis, respiratory distress 2. Symptoms of lung congestion: Poor interrupted
Case 47 Clinical Presentation
 93 Case 47 C Clinical Presentation 45-year-old man presents with chest pain and new onset of a murmur. Echocardiography shows severe aortic insufficiency. 94 RadCases Cardiac Imaging Imaging Findings C
93 Case 47 C Clinical Presentation 45-year-old man presents with chest pain and new onset of a murmur. Echocardiography shows severe aortic insufficiency. 94 RadCases Cardiac Imaging Imaging Findings C
Index of subjects. effect on ventricular tachycardia 30 treatment with 101, 116 boosterpump 80 Brockenbrough phenomenon 55, 125
 145 Index of subjects A accessory pathways 3 amiodarone 4, 5, 6, 23, 30, 97, 102 angina pectoris 4, 24, 1l0, 137, 139, 140 angulation, of cavity 73, 74 aorta aortic flow velocity 2 aortic insufficiency
145 Index of subjects A accessory pathways 3 amiodarone 4, 5, 6, 23, 30, 97, 102 angina pectoris 4, 24, 1l0, 137, 139, 140 angulation, of cavity 73, 74 aorta aortic flow velocity 2 aortic insufficiency
Bogdan A. Popescu. University of Medicine and Pharmacy Bucharest, Romania. EAE Course, Bucharest, April 2010
 Bogdan A. Popescu University of Medicine and Pharmacy Bucharest, Romania EAE Course, Bucharest, April 2010 This is how it started Mitral stenosis at a glance 2D echo narrow diastolic opening of MV leaflets
Bogdan A. Popescu University of Medicine and Pharmacy Bucharest, Romania EAE Course, Bucharest, April 2010 This is how it started Mitral stenosis at a glance 2D echo narrow diastolic opening of MV leaflets
Echocardiography as a diagnostic and management tool in medical emergencies
 Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
Echocardiography as a diagnostic and management tool in medical emergencies Frank van der Heusen MD Department of Anesthesia and perioperative Care UCSF Medical Center Objective of this presentation Indications
Heart Failure Dr ahmed almutairi Assistant professor internal medicin dept
 Heart Failure Dr ahmed almutairi Assistant professor internal medicin dept (MBBS)(SBMD) Introduction Epidemiology Pathophysiology diastolic/systolic Risk factors Signs and symptoms Classification of HF
Heart Failure Dr ahmed almutairi Assistant professor internal medicin dept (MBBS)(SBMD) Introduction Epidemiology Pathophysiology diastolic/systolic Risk factors Signs and symptoms Classification of HF
Outcomes of Mitral Valve Repair for Mitral Regurgitation Due to Degenerative Disease
 Outcomes of Mitral Valve Repair for Mitral Regurgitation Due to Degenerative Disease TIRONE E. DAVID, MD ; SEMIN THORAC CARDIOVASC SURG 19:116-120c 2007 ELSEVIER INC. PRESENTED BY INTERN 許士盟 Mitral valve
Outcomes of Mitral Valve Repair for Mitral Regurgitation Due to Degenerative Disease TIRONE E. DAVID, MD ; SEMIN THORAC CARDIOVASC SURG 19:116-120c 2007 ELSEVIER INC. PRESENTED BY INTERN 許士盟 Mitral valve
Without echocardiography is
 Diagnosis of valvular heart disease Without echocardiography is like traveling on a horseback or at best on a steam train 1 Echocardiography 2D 2 Diagnosis of valvular heart desease Aortic valve disease
Diagnosis of valvular heart disease Without echocardiography is like traveling on a horseback or at best on a steam train 1 Echocardiography 2D 2 Diagnosis of valvular heart desease Aortic valve disease
Adult Echocardiography Examination Content Outline
 Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Adult Echocardiography Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 Anatomy and Physiology Pathology Clinical Care and Safety Measurement Techniques, Maneuvers,
Congenital heart disease. By Dr Saima Ali Professor of pediatrics
 Congenital heart disease By Dr Saima Ali Professor of pediatrics What is the most striking clinical finding in this child? Learning objectives By the end of this lecture, final year student should be able
Congenital heart disease By Dr Saima Ali Professor of pediatrics What is the most striking clinical finding in this child? Learning objectives By the end of this lecture, final year student should be able
SAMPLE HLTEN610A. TAFE NSW Training and Education Support Industry Skills Unit, Meadowbank. Practise in the cardiovascular nursing environment
 TAFE NSW Training and Education Support Industry Skills Unit, Meadowbank HLTEN610A Practise in the cardiovascular nursing environment Version 1.0 Flexible Learner Resource Product Code: ISO 9001 HLTEN610A
TAFE NSW Training and Education Support Industry Skills Unit, Meadowbank HLTEN610A Practise in the cardiovascular nursing environment Version 1.0 Flexible Learner Resource Product Code: ISO 9001 HLTEN610A
DISCLOSURE. Echocardiography in Systemic Diseases: Questions. Relevant Financial Relationship(s) None. Off Label Usage None 5/7/2018
 None. Off Label Usage None 5/7/2018") Echocardiography in Systemic Diseases: Questions Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate
Echocardiography in Systemic Diseases: Questions Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate
Cardiomyopathy. Jeff Grubbe MD FACP, Chief Medical Director, Allstate Life & Retirement
 Cardiomyopathy Jeff Grubbe MD FACP, Chief Medical Director, Allstate Life & Retirement Nebraska Home Office Life Underwriters Association March 20, 2018 1 Cardiomyopathy A myocardial disorder in which
Cardiomyopathy Jeff Grubbe MD FACP, Chief Medical Director, Allstate Life & Retirement Nebraska Home Office Life Underwriters Association March 20, 2018 1 Cardiomyopathy A myocardial disorder in which
Aortic Stenosis: LVOT Obstruction
 Aortic Stenosis: LVOT Obstruction Raymond Stainback, MD 7 th annual Houston Echo Review 2016: Boot Camp for the Echo Board Murmur: Additional heart or vascular sound due to normal or abnormal turbulent
Aortic Stenosis: LVOT Obstruction Raymond Stainback, MD 7 th annual Houston Echo Review 2016: Boot Camp for the Echo Board Murmur: Additional heart or vascular sound due to normal or abnormal turbulent
How to Assess and Treat Obstructive Lesions
 How to Assess and Treat Obstructive Lesions Erwin Oechslin, MD, FESC, FRCPC, Director, Congenital Cardiac Centre for Adults Peter Munk Cardiac Centre University Health Network/Toronto General Hospital
How to Assess and Treat Obstructive Lesions Erwin Oechslin, MD, FESC, FRCPC, Director, Congenital Cardiac Centre for Adults Peter Munk Cardiac Centre University Health Network/Toronto General Hospital
The Cardiovascular Examination
 The Cardiovascular Examination Contrary to the belief of most candidates, the examination of the cardiovascular system does not end with auscultation of the precordium or the lung bases, but must include,
The Cardiovascular Examination Contrary to the belief of most candidates, the examination of the cardiovascular system does not end with auscultation of the precordium or the lung bases, but must include,
Case # 1. Page: 8. DUKE: Adams
 Case # 1 Page: 8 1. The cardiac output in this patient is reduced because of: O a) tamponade physiology O b) restrictive physiology O c) coronary artery disease O d) left bundle branch block Page: 8 1.
Case # 1 Page: 8 1. The cardiac output in this patient is reduced because of: O a) tamponade physiology O b) restrictive physiology O c) coronary artery disease O d) left bundle branch block Page: 8 1.
Valve Disease Board Review Questions
 Valve Disease Board Review Questions Dennis A. Tighe, MD, FASE University of Massachusetts Medical School Worcester, MA Case 1 History A 61 year-old man Presents to hospital with worsening shortness of
Valve Disease Board Review Questions Dennis A. Tighe, MD, FASE University of Massachusetts Medical School Worcester, MA Case 1 History A 61 year-old man Presents to hospital with worsening shortness of
Etiology, Classification & Management. Sheba Medical Center Cardiology Department Matthew Wright St. George s University of London
 Etiology, Classification & Management Sheba Medical Center Cardiology Department Matthew Wright St. George s University of London Introduction World Health Organization (1995): Diseases of myocardium (heart
Etiology, Classification & Management Sheba Medical Center Cardiology Department Matthew Wright St. George s University of London Introduction World Health Organization (1995): Diseases of myocardium (heart
Notes by Sandra Dankwa 2009 HF- Heart Failure DS- Down Syndrome IE- Infective Endocarditis ET- Exercise Tolerance. Small VSD Symptoms -asymptomatic
 Congenital Heart Disease: Notes. Condition Pathology PC Ix Rx Ventricular septal defect (VSD) L R shuntsdefect anywhere in the ventricle, usually perimembranous (next to the tricuspid valve) 30% 1)small
Congenital Heart Disease: Notes. Condition Pathology PC Ix Rx Ventricular septal defect (VSD) L R shuntsdefect anywhere in the ventricle, usually perimembranous (next to the tricuspid valve) 30% 1)small
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants
 Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
Aortic Stenosis: Spectrum of Disease, Low Flow/Low Gradient and Variants Martin G. Keane, MD, FASE Professor of Medicine Lewis Katz School of Medicine at Temple University Basic root structure Parasternal
Idiopathic Hypertrophic Subaortic Stenosis and Mitral Stenosis
 CASE REPORTS Idiopathic Hypertrophic Subaortic Stenosis and Mitral Stenosis Martin J. Nathan, M.D., Roman W. DeSanctis, M.D., Mortimer J. Buckley, M.D., Charles A. Sanders, M.D., and W. Gerald Austen,
CASE REPORTS Idiopathic Hypertrophic Subaortic Stenosis and Mitral Stenosis Martin J. Nathan, M.D., Roman W. DeSanctis, M.D., Mortimer J. Buckley, M.D., Charles A. Sanders, M.D., and W. Gerald Austen,
The Cardiovascular System Part I: Heart Outline of class lecture After studying part I of this chapter you should be able to:
 The Cardiovascular System Part I: Heart Outline of class lecture After studying part I of this chapter you should be able to: 1. Describe the functions of the heart 2. Describe the location of the heart,
The Cardiovascular System Part I: Heart Outline of class lecture After studying part I of this chapter you should be able to: 1. Describe the functions of the heart 2. Describe the location of the heart,
CCRN Review Cardiovascular
 CCRN Review Cardiovascular Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Angina Definition discomfort that occurs when oxygen demand
CCRN Review Cardiovascular Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Angina Definition discomfort that occurs when oxygen demand
Valvular heart disease : Role of medication ( drug and intervention ) Pol.Col.Dr.Kasem Ratanasumawong
 Pol.Col.Dr.Kasem Ratanasumawong") Valvular heart disease : Role of medication ( drug and intervention ) Pol.Col.Dr.Kasem Ratanasumawong Management of valvular heart disease Accurate diagnosis and disease severity Prevention and treatment
Valvular heart disease : Role of medication ( drug and intervention ) Pol.Col.Dr.Kasem Ratanasumawong Management of valvular heart disease Accurate diagnosis and disease severity Prevention and treatment
Regurgitant Lesions. Bicol Hospital, Legazpi City, Philippines July Gregg S. Pressman MD, FACC, FASE Einstein Medical Center Philadelphia, USA
 Regurgitant Lesions Bicol Hospital, Legazpi City, Philippines July 2016 Gregg S. Pressman MD, FACC, FASE Einstein Medical Center Philadelphia, USA Aortic Insufficiency Valve anatomy and function LVOT and
Regurgitant Lesions Bicol Hospital, Legazpi City, Philippines July 2016 Gregg S. Pressman MD, FACC, FASE Einstein Medical Center Philadelphia, USA Aortic Insufficiency Valve anatomy and function LVOT and
Mitral Valve Diseases
 1 7 Mitral Valve Diseases Maurice L. Enriquez-Sarano and Robert L. Frye The Normal Mitral Valve......................... 397 Mitral Valve Prolapse............................. 402 Mitral Regurgitation.............................
1 7 Mitral Valve Diseases Maurice L. Enriquez-Sarano and Robert L. Frye The Normal Mitral Valve......................... 397 Mitral Valve Prolapse............................. 402 Mitral Regurgitation.............................
Review of Cardiac Mechanics & Pharmacology 10/23/2016. Brent Dunworth, CRNA, MSN, MBA 1. Learning Objectives
 Brent Dunworth, CRNA, MSN, MBA Associate Director of Advanced Practice Division Chief, Nurse Anesthesia Vanderbilt University Medical Center Nashville, Tennessee Learning Objectives Review the principles
Brent Dunworth, CRNA, MSN, MBA Associate Director of Advanced Practice Division Chief, Nurse Anesthesia Vanderbilt University Medical Center Nashville, Tennessee Learning Objectives Review the principles
Heart Disorders. Cardiovascular Disorders (Part B-1) Module 5 -Chapter 8. Overview Heart Disorders Vascular Disorders
 Module 5 -Chapter 8. Overview Heart Disorders Vascular Disorders") Cardiovascular Disorders (Part B-1) Module 5 -Chapter 8 Overview Heart Disorders Vascular Disorders Susie Turner, MD 1/7/13 Heart Disorders Coronary Artery Disease Cardiac Arrhythmias Congestive Heart
Cardiovascular Disorders (Part B-1) Module 5 -Chapter 8 Overview Heart Disorders Vascular Disorders Susie Turner, MD 1/7/13 Heart Disorders Coronary Artery Disease Cardiac Arrhythmias Congestive Heart
Presenter: Steven Brust, HCS-D, HCS-H Product Manager, Home Health Coding Center
 Presenter: Steven Brust, HCS-D, HCS-H Product Manager, Home Health Coding Center Pinpoint & properly assign the appropriate heart failure codes Left- vs. Right-sided Left ventricular failure (LVF) may
Presenter: Steven Brust, HCS-D, HCS-H Product Manager, Home Health Coding Center Pinpoint & properly assign the appropriate heart failure codes Left- vs. Right-sided Left ventricular failure (LVF) may
Pathophysiology: Left To Right Shunts
 Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Skin supplied by T1-4 (medial upper arm and neck) T5-9- epigastrium Visceral afferents from skin and heart are the same dorsal root ganglio
 T5-9- epigastrium Visceral afferents from skin and heart are the same dorsal root ganglio") Cardio 2 ECG... 3 Cardiac Remodelling... 11 Valvular Diseases... 13 Hypertension... 18 Aortic Coarctation... 24 Erythropoiesis... 27 Haemostasis... 30 Anaemia... 36 Atherosclerosis... 44 Angina... 48 Myocardial
Cardio 2 ECG... 3 Cardiac Remodelling... 11 Valvular Diseases... 13 Hypertension... 18 Aortic Coarctation... 24 Erythropoiesis... 27 Haemostasis... 30 Anaemia... 36 Atherosclerosis... 44 Angina... 48 Myocardial
TOP 10 TAKEAWAYS. Jane A. Linderbaum MS, APRN, CNP, AACC Assistant Professor of Medicine Department of cardiovascular disease
 TOP 10 TAKEAWAYS Jane A. Linderbaum MS, APRN, CNP, AACC Assistant Professor of Medicine Department of cardiovascular disease No Disclosures No off-label discussions 73% of survey respondents identified
TOP 10 TAKEAWAYS Jane A. Linderbaum MS, APRN, CNP, AACC Assistant Professor of Medicine Department of cardiovascular disease No Disclosures No off-label discussions 73% of survey respondents identified
Valvular Heart Disease in Pregnancy
 CHAPTER 87 Valvular Heart Disease in Pregnancy M. Panja, S. Basu, D. Kumar Introduction Valvular heart disease in young women is most commonly due to rheumatic heart disease, congenital abnormalities,
CHAPTER 87 Valvular Heart Disease in Pregnancy M. Panja, S. Basu, D. Kumar Introduction Valvular heart disease in young women is most commonly due to rheumatic heart disease, congenital abnormalities,
PATENT DUCTUS ARTERIOSUS (PDA)
") PATENT DUCTUS ARTERIOSUS (PDA) It is a channel that connect the pulmonary artery with the descending aorta (isthumus part). It results from the persistence of patency of the fetal ductus arteriosus after
PATENT DUCTUS ARTERIOSUS (PDA) It is a channel that connect the pulmonary artery with the descending aorta (isthumus part). It results from the persistence of patency of the fetal ductus arteriosus after
RF & RHD Workshop 22 nd March MANAGEMENT of RHEUMATIC HEART DISEASE in PREGNANCY. Dr Dorothy Radford
 RF & RHD Workshop 22 nd March 2016 MANAGEMENT of RHEUMATIC HEART DISEASE in PREGNANCY Dr Dorothy Radford PREGNANCY PHYSIOLOGY Increased cardiac output 30%-50% Increased blood volume 30%-50% Increased heart
RF & RHD Workshop 22 nd March 2016 MANAGEMENT of RHEUMATIC HEART DISEASE in PREGNANCY Dr Dorothy Radford PREGNANCY PHYSIOLOGY Increased cardiac output 30%-50% Increased blood volume 30%-50% Increased heart
Common Codes for ICD-10
 Common Codes for ICD-10 Specialty: Cardiology *Always utilize more specific codes first. ABNORMALITIES OF HEART RHYTHM ICD-9-CM Codes: 427.81, 427.89, 785.0, 785.1, 785.3 R00.0 Tachycardia, unspecified
Common Codes for ICD-10 Specialty: Cardiology *Always utilize more specific codes first. ABNORMALITIES OF HEART RHYTHM ICD-9-CM Codes: 427.81, 427.89, 785.0, 785.1, 785.3 R00.0 Tachycardia, unspecified
LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital
 LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital LV inflow across MV LV LV outflow across AV LV LV geometric changes Pressure overload
LV geometric and functional changes in VHD: How to assess? Mi-Seung Shin M.D., Ph.D. Gachon University Gil Hospital LV inflow across MV LV LV outflow across AV LV LV geometric changes Pressure overload
Valvular defects. Lectures from Pathological Physiology. Study materials from Pathological Physiology, 2017/2018 Oliver Rácz, Eva Sedláková
 Valvular defects Lectures from Pathological Physiology Study materials from Pathological Physiology, 2017/2018 Oliver Rácz, Eva Sedláková 1 2 3 1 Valvular dysfunction - introduction Stenosis block of flow;
Valvular defects Lectures from Pathological Physiology Study materials from Pathological Physiology, 2017/2018 Oliver Rácz, Eva Sedláková 1 2 3 1 Valvular dysfunction - introduction Stenosis block of flow;
Echocardiographic Cardiovascular Risk Stratification: Beyond Ejection Fraction
 Echocardiographic Cardiovascular Risk Stratification: Beyond Ejection Fraction October 4, 2014 James S. Lee, M.D., F.A.C.C. Associates in Cardiology, P.A. Silver Spring, M.D. Disclosures Financial none
Echocardiographic Cardiovascular Risk Stratification: Beyond Ejection Fraction October 4, 2014 James S. Lee, M.D., F.A.C.C. Associates in Cardiology, P.A. Silver Spring, M.D. Disclosures Financial none
Historical perspective R1 黃維立
 Degenerative mitral valve disease refers to a spectrum of conditions in which morphologic changes in the connective tissue of the mitral valve cause structural lesions that prevent normal function of the
Degenerative mitral valve disease refers to a spectrum of conditions in which morphologic changes in the connective tissue of the mitral valve cause structural lesions that prevent normal function of the
Pathophysiology: Left To Right Shunts
 Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
Pathophysiology: Left To Right Shunts Daphne T. Hsu, MD dh17@columbia.edu Learning Objectives Learn the relationships between pressure, blood flow, and resistance Review the transition from fetal to mature
CARDIOVASCULAR PHYSIOLOGY
 CARDIOVASCULAR PHYSIOLOGY LECTURE 4 Cardiac cycle Polygram - analysis of cardiac activity Ana-Maria Zagrean MD, PhD The Cardiac Cycle - definitions: the sequence of electrical and mechanical events that
CARDIOVASCULAR PHYSIOLOGY LECTURE 4 Cardiac cycle Polygram - analysis of cardiac activity Ana-Maria Zagrean MD, PhD The Cardiac Cycle - definitions: the sequence of electrical and mechanical events that
Valvular Heart Disease and Auscultation. Troy L Randle, DO, FACC, FACOI
 Valvular Heart Disease and Auscultation Troy L Randle, DO, FACC, FACOI 2 Normal Structure Mitral Valve Cross-sectional Area 4-6 cm 2 Anterior and Posterior Leaflets Chordae Tendineae Papillary Muscles
Valvular Heart Disease and Auscultation Troy L Randle, DO, FACC, FACOI 2 Normal Structure Mitral Valve Cross-sectional Area 4-6 cm 2 Anterior and Posterior Leaflets Chordae Tendineae Papillary Muscles