Endovascular Treatment of Hepatic Artery Stenosis following Liver Transplantation
|
|
|
- Kelly Harvey
- 6 years ago
- Views:
Transcription

1 Endovascular Treatment of Hepatic Artery Stenosis following Liver Transplantation W. Charles Sternbergh, III, MD Professor and Chief Vascular and Endovascular Surgery Vice Chair for Research Department of Surgery Ochsner Clinic Foundation New Orleans August 30, 2017

2 Disclosure I have no personal or professional financial relationships or interests with any proprietary entity producing healthcare goods/or services
 for Treatment Endovascular technique Results")
3 Outline Endovascular Rx of Hepatic Artery Stenosis Incidence and associated morbidity Etiology Clinical Presentation Diagnostic Evaluation Indications (and contra-indications) for Treatment Endovascular technique Results Complications
4 Top 5 Liver Transplant Centers Volume Ochsner year survival Statistically Higher UCLA As expected Mayo/FL As expected UCSF As Expected Vandy As Expected Source: OPTN/UNOS & Scientific Registry for Transplant Recipients Dec. 2015
 2 Re-transplant required in up to 75% with HAT 3 Hepatic Artery Thrombosis 30-50% risk of Liver failure 4 1. Sabri SS et al.")

5 Hepatic Artery Stenosis Incidence and morbidity Affects 5-11% of orthotopic liver transplants 1 Can Lead to biliary complications (ischemic) Up to 65% chance of progressing to hepatic artery thrombosis (HAT) 2 Re-transplant required in up to 75% with HAT 3 Hepatic Artery Thrombosis 30-50% risk of Liver failure 4 1. Sabri SS et al. Endovascular Therapy for hepatic artery stenosis following liver transplantation. Vasc Endovasc Surg Orons PD et al. HAS in liver transplant recipients: prevalence and cholangiographic appearance of ass. biliary complications. AJR Am J Roentgenol Tucker N. et al. Primer on trasnplantation, 2 nd edition. Mt. Laurel, NJ: American Society of Transplantation Langnas AN et al. Vascular complications after orthotopic liver transplantation. Am J surg 1991.

6 Hepatic Artery Stenosis Common at anastomosis Etiology Less frequently at terminal proper Hepatic/R and L hepatic bifurcation Etiology 1 Technical error Vessel redundancy/kinking Clamp injury Rejection Ischemia of vaso vasorum Gi.jhsps.org 1. Carlos Pulitano et al. Hepatic Artery Stenosis after Liver Transplantation: Is Endovascular Treatment always Necessary? Liver Transplant 2013.
7 Hepatic Artery Stenosis Clinical Presentation Almost always asymptomatic Rarely causes transaminase elevation on its own Other causes of LFT elevation should be aggressively investigated Worsening HAS will frequently be seen in patients with associated sepsis or rejection. Underlying issue should be Rxed first HAS will typically improve/resolve WITHOUT intervention in these circumstances
8 Hepatic Artery Stenosis Diagnostic Evaluation Duplex Ultrasound (Phillips Ochsner) Studies performed: intra-operatively IF there are concerns POD 1 and 7 1,6 and 12 months More frequent for donation after circulatory death (DCD) donors
9 Hepatic Artery Stenosis (HAS) Diagnostic Evaluation Duplex Ultrasound Severe HAS *suggested by: Peak Systolic Velocity (PSV) of > cm/sec Resistive Index (RI) of <0.5 Presence of Tardus Parvus waveforms *Lall NU, Bluth EI, Sternbergh WC III. Ultrasound findings after endovascular stent deployment in transplant liver hepatic artery stenosis. AJR (Am J Roentgenol);202: , 2014




10 Tardus Parvus: HA Stenosis and Post Angioplasty Pre MHA RI =.33 LHA RI =.38 Post Post Angioplasty MHA RI =.63 LHA RI =.65
11 Hepatic Artery Stenosis (HAS) Diagnostic Evaluation Duplex Ultrasound Severe HAS *suggested by: Peak Systolic Velocity (PSV) of > cm/sec Resistive Index (RI) of <0.5 Presence of Tardus Parvus waveforms Rarely, critical HAS has no velocity elevation But has very low RI and + tardus parus waveforms *Lall NU, Bluth EI, Sternbergh WC III. Ultrasound findings after endovascular stent deployment in transplant liver hepatic artery stenosis. AJR (Am J Roentgenol);202: , 2014
 0.35-0.")
12 Duplex: Common hepatic flow not well visualized, possibly thrombosed. R and L hepatic Resistive index (RI) with tardus parvus waveforms 99+% Proper Hepatic Stenosis
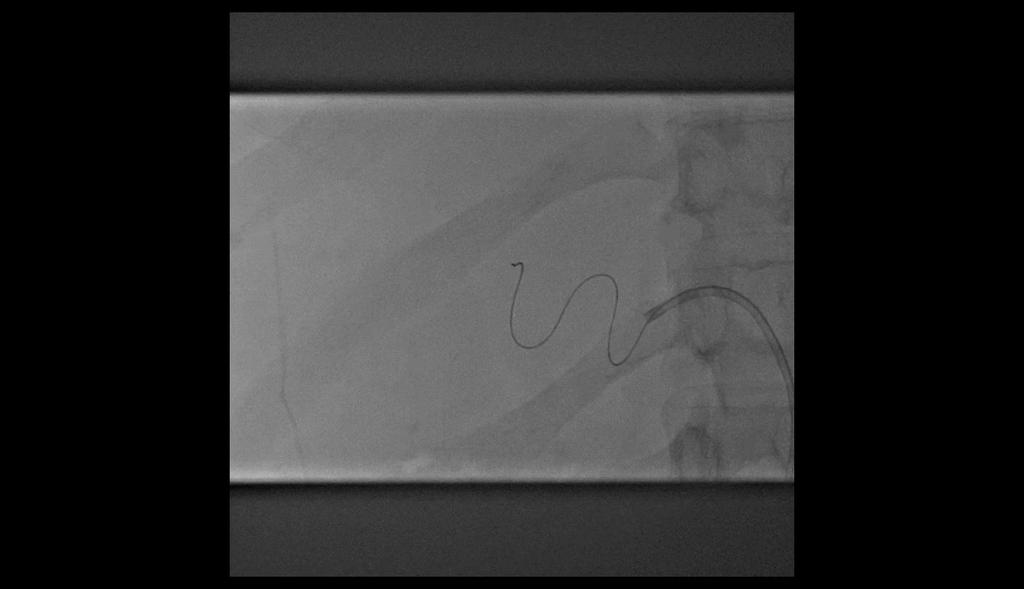
13 Occlusive with wire

14 After 2.75 x 18 DES placement
15 Hepatic Artery Stenosis Diagnostic Evaluation In patients with severe HAS by US, a CTA is usually performed for endovascular case planning (rarely to confirm the Dx) Orientation of celiac Use brachial approach if signif caudal angulation (~30%) Aberrant inflow Recipient hepatic inflow via SMA from replaced R hepatic Unexpected high grade celiac artery stenosis with hepatic inflow through the SMA via retrograde GDA flow Aorta-hepatic conduit
16 Hepatic Artery Stenosis Indications for Endovascular Rx Severe HAS by duplex PSV > , RI <0.5, + tardus parvus waveforms Minimum of 3 wk post-op Completely arbitrary my fear of dilating a fresh anastomosis Peri-operative (typically POD1) HAT is managed surgically Contraindications Concurrent rejection or sepsis (HAS usually improves after Rx of primary issue)
17 Hepatic Artery Stenosis Indications for Endovascular Rx Severe HAS by duplex PSV > , RI <0.5, + tardus parvus waveforms Minimum of 3 wk post-op Completely arbitrary my fear of dilating a fresh anastomosis Peri-operative (typically POD1) HAT is managed surgically Contraindications Concurrent rejection or sepsis (HAS usually improves after Rx of primary issue)
18 Hepatic Artery Stenosis Indications for Endovascular Rx Severe HAS by duplex PSV > , RI <0.5, + tardus parvus waveforms Minimum of 3 wk post-op Completely arbitrary my fear of dilating a fresh anastomosis Peri-operative (typically POD1) HAT is managed surgically Contraindications Concurrent rejection or sepsis (HAS usually improves after Rx of primary issue)

19 Hepatic Artery Stenosis Rx Technique of delivering a stable platform Femoral or Brachial (30%) approach 6 fr RDC-1 guide (femoral), 5 fr multipurpose sheath (brachial) stiff angled glidewire into GDA followed by 5 fr glide catheter Sheath or guide then carefully telescoped into the distal common hepatic over catheter/wire wire and 5 fr catheter removed
20 Hepatic Artery Stenosis Rx Technique for Rx DA imaging (15 fps) frequently better than DSA platform (choice PT regular or extra support my fav) Use the least stiff wire that will allow balloon/stent to track Rapid exchange coronary balloons (2-5 mm) Coronary stents 2-5mm diameter, 8-28mm length Prefer DES if < 3.5mm diameter

21 Technique Main HA 99% Stenosis of proper hepatic artery coronary stent placement

22 Technique Proximal Flaring Balloon expandable coronary stent Completion hepatic angiogram
23 Technique Filling of hepatic vasculature PRE POST

24 Buddy Wire Technique Left HA stenosis Right HA occlusion Main HA


25 Buddy Wire Technique Pre-dilation with buddy wire in left HA Balloon expandable stent in right HA

26 Buddy Wire Technique Stenting of left hepatic artery


27 Buddy Wire Technique PRE POST
28
29 3.5 x 18 DES 2.25 x 12 DES
30
31 Primary stent placement for hepatic artery stenosis after liver transplantation Linda Le, MD, William Terral, MD, Nicolas Zea, MD, Hernan A. Bazan, MD, Taylor A. Smith, MD, George E. Loss, MD, Edward Bluth, MD, and W. Charles Sternbergh III, MD, New Orleans, La Aug 2009 Dec 2013 N=62 interventions in 42 patients 6.4% (42/654 Liver Transplants) need for HAS intervention Most interventions <3 months after transplant J Vasc Surg 2015;62:704-9
32 Results Time to Initial Intervention Mean time = 82.2 ± 56 days /3 within 3 months of transplant 6 Within 30 days Within 3 months After 3 months


33 62 Interventions 42 Initial Interventions 20 Re-interventions 25 initial stent 17 PTA 15 stent 5 PTA 5 Drug-eluting 4 Drug-eluting Median F/U= 19.1 ± 15 months

 2 dissections leading to HAT")
34 Results 95% Technical Success (59/62) 3.2% HAT risk 2.4% 30-day mortality 4.8% Re-transplant Rate (n=3) HAT Recurrent HCC cholangitis 4.8% Complication Rate (n=3) 2 dissections leading to HAT Hepatic artery extravasation, brachial artery thrombosis
35 PTA vs. Stent Patency PTA STENT J Vasc Surg 2015;62:704-9
36 PTA vs. Stent Patency PTA STENT J Vasc Surg 2015;62:704-9
37 Primary Assisted Patency 93% 24 month = 93% J Vasc Surg 2015;62:704-9

38 J Vasc Surg
39 Study Design Retrospective Review: August 2009 March 2016 Tertiary care institution Ochsner Clinic Foundation, New Orleans, LA Largest US volume of OLTx since 2011 Objective Define potential risks associated with early intervention for HAS Describe salvage techniques for endovascular repair IRB Approved
40 Results 79 pts, 1129 OLTx in 6.5 yrs 6.9% HAS Rate 79 Patients Interventions 34 PTA Alone 65 Stent
41 Results 79 pts, 1129 OLTx in 6.5 yrs 6.9% HAS Rate n=106 angiograms 79 Patients Interventions 7 Diagnostic Interventions 34 PTA Alone 65 Stent
 Femoral")
42 Results 79 pts, 1129 OLTx in 6.5 yrs 6.9% HAS Rate n=106 angiograms 79 Patients Interventions 7 Diagnostic Mean Age = 51 yo (Range 11-72) Femoral Approach = 72.6% Median Time to Intervention = 71 days Interventions 34 PTA Alone 65 Stent

43 7 Initial Diagnostic 106 Angiograms for HAS 73 Initial Interventions 26 Re-interventions Initial Stent PTA PTA Stent Diagnostic Re-intervention Rate = 26.5% (21/79) Time to Re-intervention = 97 days

 n=5 >30% Residual")
44 n=2 Major Complication HAS could not be treated Technical Success n=2 Major Complication HAS Aborted 91% (90/99) n=5 >30% Residual Stenosis
45 Major Complications 3 Ruptures, 5 dissections: 7.5% rate (8/106)
46 Major Complications 3 Ruptures, 5 dissections: 7.5% rate (8/106) 6/8 (75%) had successful endovascular Rx Ruptures all successfully Rxed with Jomed covered stent (n=2) or balloon tampanode (n=1) Dissections Rxed with stents if true lumen access could be obtained No open Rx was required
47 Major Complications 3 Ruptures, 5 dissections: 7.5% rate (8/106) 6/8 (75%) had successful endovascular Rx Ruptures all successfully Rxed with Jomed covered stent (n=2) or balloon tampanode (n=1) Dissections Rxed with stents if true lumen access could be obtained No open Rx was required However, 4/8 patients (50%) went on to HAT, compared to 1.4% (1/71) in the noncomplication cohort (P<0.001)
48 Mortality 1 year all cause mortality Complication Cohort: 12.5% (1/8) Non-complication Cohort: 7% (5/71) P =.484
49 Risk Factors for Complications Tortuosity Non-complication Cohort P = % (34/98) interventions had tortuous anatomy Complication Cohort 75% (6/8) interventions had tortuous anatomy 2 fold increase
 patients had 2 liver transplants Complication Cohort 37.")
50 Risk Factors for Complications Re-transplants Non-complication Cohort P = % (9/71) patients had 2 liver transplants Complication Cohort 37.5% (3/8) patients had 2 liver transplants 3 fold increase
51 Hepatic Artery Rupture 11 y/o boy with Budd Chiri 1 st liver Transplant 12/10/13 Open Exploration for hepatic artery thrombosis 2 nd Liver Transplant 12/12/13 Colon perforation/exploration 12/24/13 Severe HAS, angio on 1/13/14 (POD 31)

52 HAS

53 Proper Hepatic Artery Rupture Extravasation

54 3x20 Balloon Tamponade

55
56

57 Jomed 3x16 Covered Stent

58 Resolution of HAS & hepatic rupture
59 Hepatic Artery Dissection
60

61 Proper Hepatic Artery Dissection True Lumen False Lumen

62 Coronary Steerable Catheter
63

64 3.5x33 Bare Metal Stent
65
66 Meta-analysis Stent placement vs angioplasty for HAS after liver transplant: a meta-analysis of case series Rostambeigi et al (U Minnesota), Eur Radiol : interventions from 26 studies 147 PTA, 116 stent
67 Meta-analysis Stent placement vs angioplasty for HAS after liver transplant: a meta-analysis of case series Rostambeigi et al (U Minnesota), Eur Radiol : interventions from 26 studies 147 PTA, 116 stent Procedure success: 89% (PTA) vs 98% (stent) Complication rate: 16% (PTA) vs 19% (stent) Arterial Patency: 76% (PTA) vs 68% (stent) Re-intervention: 22% (PTA) vs 25% (stent) Re-transplantation: 20% (PTA) vs 25% (stent) Conclusion: PTA and stent Rx are equivalent
68 Meta-analysis Stent placement vs angioplasty for HAS after liver transplant: a meta-analysis of case series Rostambeigi et al (U Minnesota), Eur Radiol : interventions from 26 studies 147 PTA, 116 stent Procedure success: 89% (PTA) vs 98% (stent) Complication rate: 16% (PTA) vs 19% (stent) Arterial Patency: 76% (PTA) vs 68% (stent) Re-intervention: 22% (PTA) vs 25% (stent) Re-transplantation: 20% (PTA) vs 25% (stent) Conclusion: PTA and stent Rx are equivalent
69 Meta-analysis Stent placement vs angioplasty for HAS after liver transplant: a meta-analysis of case series Rostambeigi et al (U Minnesota), Eur Radiol : interventions from 26 studies 147 PTA, 116 stent Procedure success: 89% (PTA) vs 98% (stent) Complication rate: 16% (PTA) vs 19% (stent) Arterial Patency: 76% (PTA) vs 68% (stent) Re-intervention: 22% (PTA) vs 25% (stent) Re-transplantation: 20% (PTA) vs 25% (stent) Conclusion: PTA and stent Rx are equivalent
70 Meta-analysis Stent placement vs angioplasty for HAS after liver transplant: a meta-analysis of case series Rostambeigi et al (U Minnesota), Eur Radiol : interventions from 26 studies 147 PTA, 116 stent Procedure success: 89% (PTA) vs 98% (stent) Complication rate: 16% (PTA) vs 19% (stent) Arterial Patency: 76% (PTA) vs 68% (stent) Re-intervention: 22% (PTA) vs 25% (stent) Re-transplantation: 20% (PTA) vs 25% (stent) Conclusion: PTA and stent Rx are equivalent
71 Meta-analysis Stent placement vs angioplasty for HAS after liver transplant: a meta-analysis of case series Rostambeigi et al (U Minnesota), Eur Radiol : interventions from 26 studies 147 PTA, 116 stent Procedure success: 89% (PTA) vs 98% (stent) Complication rate: 16% (PTA) vs 19% (stent) Arterial Patency: 76% (PTA) vs 68% (stent) Re-intervention: 22% (PTA) vs 25% (stent) Re-transplantation: 20% (PTA) vs 25% (stent) Conclusion: PTA and stent Rx are equivalent
72 Meta-analysis Stent placement vs angioplasty for HAS after liver transplant: a meta-analysis of case series Rostambeigi et al (U Minnesota), Eur Radiol : interventions from 26 studies 147 PTA, 116 stent Procedure success: 89% (PTA) vs 98% (stent) Complication rate: 16% (PTA) vs 19% (stent) Arterial Patency: 76% (PTA) vs 68% (stent) Re-intervention: 22% (PTA) vs 25% (stent) Re-transplantation: 20% (PTA) vs 25% (stent) Conclusion: PTA and stent Rx are equivalent
73 Literature, HAS intervention Date N Technical success (%) Complication rate (%) Present Study In press Sommacale Saad Ueno Sabri Rajakannu Kodama
74 Literature, HAS intervention Date N Technical success (%) Complication rate (%) Present Study In press Sommacale Saad Ueno Sabri Rajakannu Kodama
75 Literature, HAS intervention Date N Technical success (%) Complication rate (%) Present Study In press Sommacale Saad Ueno Sabri Rajakannu Kodama
76 Take home clinical pearls Hepatic artery Intervention Only Rx high grade stenosis PSV > , RI <0.5 (usually <0.4), + tardus parvus waveforms Overall, I Rx <50% of cases I m asked to see
77 Take home clinical pearls Hepatic artery Intervention Only Rx high grade stenosis PSV > , RI <0.5 (usually <0.4), + tardus parvus waveforms Overall, I Rx <50% of cases I m asked to see Don t treat in setting of rejection or sepsis
78 Take home clinical pearls Hepatic artery Intervention Only Rx high grade stenosis PSV > , RI <0.5 (usually <0.4), + tardus parvus waveforms Overall, I Rx <50% of cases I m asked to see Don t treat in setting of rejection or sepsis Case plan carefully (femoral vs brachial)
79 Take home clinical pearls Hepatic artery Intervention Only Rx high grade stenosis PSV > , RI <0.5 (usually <0.4), + tardus parvus waveforms Overall, I Rx <50% of cases I m asked to see Don t treat in setting of rejection or sepsis Case plan carefully (femoral vs brachial) Meticulous technique is essential Can be technically challenging/unforgiving Experienced in rapid exchange systems Need availability of bail-out devices
80 Summary Endovascular Rx of Hepatic Artery Stenosis Endovascular Intervention for HAS is effective with excellent primary-assisted patency rates Primary stent placement (particularly DES) appears to reduce the need for secondary intervention in my experience Meta-analysis suggest equivalent results Severe hepatic artery tortuosity and/or retransplantation increase the risk of a major complication by 2-3 fold
81 Summary Endovascular Rx of Hepatic Artery Stenosis Complication rate (7.5%) is acceptable in light of the frequently challenging anatomy While most major complications can be Rxed endovascularly (75%), the subsequent rate of HAT is very high (50% vs 1.4%) Prudent case selection is essential

82
Robert F. Cuff, MD FACS SHMG Vascular Surgery
 Robert F. Cuff, MD FACS SHMG Vascular Surgery Objectives To become familiar with the commercially available fenestrated EVAR graft Discuss techniques to increase success Review available data to determine
Robert F. Cuff, MD FACS SHMG Vascular Surgery Objectives To become familiar with the commercially available fenestrated EVAR graft Discuss techniques to increase success Review available data to determine
DISCLOSURE TEST YOUR WAVEFORM IQ. Partial volume artifact. 86 yo female with right arm swelling, picc line. AVF on left? Dx?
 Deborah Rubens University of Rochester Rochester, NY DISCLOSURE Neither I nor my immediate family have a financial relationship with a commercial organization that may have a direct or indirect interest
Deborah Rubens University of Rochester Rochester, NY DISCLOSURE Neither I nor my immediate family have a financial relationship with a commercial organization that may have a direct or indirect interest
ASDIN 7th Annual Scientific Meeting DISCLOSURES TECHNICAL CONSIDERATIONS TECHNICAL CONSIDERATIONS UTILITY OF ULTRASOUND IN EVALUATING ACCESS
 DISCLOSURES UTILITY OF ULTRASOUND IN EVALUATING ACCESS DYSFUNCTION None Vandana Dua Niyyar, MD Assistant Professor of Medicine, Division of Nephrology, Emory University UTILITY OF ULTRASOUND IN ACCESS
DISCLOSURES UTILITY OF ULTRASOUND IN EVALUATING ACCESS DYSFUNCTION None Vandana Dua Niyyar, MD Assistant Professor of Medicine, Division of Nephrology, Emory University UTILITY OF ULTRASOUND IN ACCESS
Peripheral Arterial Disease: A Practical Approach
 Peripheral Arterial Disease: A Practical Approach Sanjoy Kundu BSc, MD, FRCPC, DABR, FASA, FCIRSE, FSIR The Scarborough Hospital Toronto Endovascular Centre The Vein Institute of Toronto Scarborough Vascular
Peripheral Arterial Disease: A Practical Approach Sanjoy Kundu BSc, MD, FRCPC, DABR, FASA, FCIRSE, FSIR The Scarborough Hospital Toronto Endovascular Centre The Vein Institute of Toronto Scarborough Vascular
The Petticoat Technique Managing Type B Dissection with both Early and Long Term Considerations
 The Petticoat Technique Managing Type B Dissection with both Early and Long Term Considerations Joseph V. Lombardi, MD Professor & Chief, Division of Vascular & Endovascular Surgery Department of Surgery,
The Petticoat Technique Managing Type B Dissection with both Early and Long Term Considerations Joseph V. Lombardi, MD Professor & Chief, Division of Vascular & Endovascular Surgery Department of Surgery,
Step by step Hybrid procedures in peripheral obstructive disease. Holger Staab, MD University Hospital Leipzig, Germany Clinic for Vascular Surgery
 Step by step Hybrid procedures in peripheral obstructive disease Holger Staab, MD University Hospital Leipzig, Germany Clinic for Vascular Surgery Disclosure Speaker name: H.H. Staab I have the following
Step by step Hybrid procedures in peripheral obstructive disease Holger Staab, MD University Hospital Leipzig, Germany Clinic for Vascular Surgery Disclosure Speaker name: H.H. Staab I have the following
Disclosures. Tips and Tricks for Tibial Intervention. Tibial intervention overview
 Tips and Tricks for Tibial Intervention Donald L. Jacobs, MD C Rollins Hanlon Endowed Professor and Chair Chair of Surgery Saint Louis University SSM-STL Saint Louis University Hospital Disclosures Abbott
Tips and Tricks for Tibial Intervention Donald L. Jacobs, MD C Rollins Hanlon Endowed Professor and Chair Chair of Surgery Saint Louis University SSM-STL Saint Louis University Hospital Disclosures Abbott
Challenges. 1. Sizing. 2. Proximal landing zone 3. Distal landing zone 4. Access vessels 5. Spinal cord ischemia 6. Endoleak
 Disclosure I have the following potential conflicts of interest to report: Consulting: Medtronic, Gore Employment in industry Stockholder of a healthcare company Owner of a healthcare company Other(s)
Disclosure I have the following potential conflicts of interest to report: Consulting: Medtronic, Gore Employment in industry Stockholder of a healthcare company Owner of a healthcare company Other(s)
Imaging Strategy For Claudication
 Who are the Debators? Imaging Strategy For Claudication Duplex Ultrasound Alone is Adequate to Select Patients for Endovascular Intervention - Pro: Dennis Bandyk MD No Disclosures PRO - Vascular Surgeon
Who are the Debators? Imaging Strategy For Claudication Duplex Ultrasound Alone is Adequate to Select Patients for Endovascular Intervention - Pro: Dennis Bandyk MD No Disclosures PRO - Vascular Surgeon
Popliteal Artery Aneurysms: Diagnosis and Repair Options
 Deepak N. Deshmukh DO April 27, 2018 Popliteal Artery Aneurysms: Diagnosis and Repair Options No Disclosures Popliteal Artery Aneurysms (PAAs) Male Predominanace Most common peripheral Aneurysm (70%) 30-50%
Deepak N. Deshmukh DO April 27, 2018 Popliteal Artery Aneurysms: Diagnosis and Repair Options No Disclosures Popliteal Artery Aneurysms (PAAs) Male Predominanace Most common peripheral Aneurysm (70%) 30-50%
History of the Powerlink System Design and Clinical Results. Edward B. Diethrich Arizona Heart Hospital Phoenix, AZ
 History of the Powerlink System Design and Clinical Results Edward B. Diethrich Arizona Heart Hospital Phoenix, AZ Powerlink System: Unibody-Bifurcated Design Long Main Body Low-Porosity Proprietary eptfe
History of the Powerlink System Design and Clinical Results Edward B. Diethrich Arizona Heart Hospital Phoenix, AZ Powerlink System: Unibody-Bifurcated Design Long Main Body Low-Porosity Proprietary eptfe
An Overview of Post-EVAR Endoleaks: Imaging Findings and Management. Ravi Shergill BSc Sean A. Kennedy MD Mark O. Baerlocher MD FRCPC
 An Overview of Post-EVAR Endoleaks: Imaging Findings and Management Ravi Shergill BSc Sean A. Kennedy MD Mark O. Baerlocher MD FRCPC Disclosure Slide Mark O. Baerlocher: Current: Consultant for Boston
An Overview of Post-EVAR Endoleaks: Imaging Findings and Management Ravi Shergill BSc Sean A. Kennedy MD Mark O. Baerlocher MD FRCPC Disclosure Slide Mark O. Baerlocher: Current: Consultant for Boston
Obesity, Scaring, Access in EVAR. Kiskinis D, Melas N, Ktenidis K. 1 st Department of Surgery Aristotle University of Thessaloniki, Greece
 Obesity, Scaring, Access in EVAR Kiskinis D, Melas N, Ktenidis K. 1 st Department of Surgery Aristotle University of Thessaloniki, Greece Obesity Decreased radiolucency (visibility) Max weight load < 160
Obesity, Scaring, Access in EVAR Kiskinis D, Melas N, Ktenidis K. 1 st Department of Surgery Aristotle University of Thessaloniki, Greece Obesity Decreased radiolucency (visibility) Max weight load < 160
Contemporary management of brachiocephalic occlusive disease. TM Sullivan Minneapolis, MN
 Contemporary management of brachiocephalic occlusive disease TM Sullivan Minneapolis, MN WL Gore & Associates Disclosures Meeting organizer (SOAR) CR Bard Chair, CEC Bolster trial Veryan National PI, MIMICS
Contemporary management of brachiocephalic occlusive disease TM Sullivan Minneapolis, MN WL Gore & Associates Disclosures Meeting organizer (SOAR) CR Bard Chair, CEC Bolster trial Veryan National PI, MIMICS
SCAI Fall Fellows Course Subclavian/Innominate Case Presentation
 SCAI Fall Fellows Course 2012 Subclavian/Innominate Case Presentation Daniel J. McCormick DO, FACC, FSCAI Director, Cardiovascular Interventional Therapy Pennsylvania Hospital University of Pennsylvania
SCAI Fall Fellows Course 2012 Subclavian/Innominate Case Presentation Daniel J. McCormick DO, FACC, FSCAI Director, Cardiovascular Interventional Therapy Pennsylvania Hospital University of Pennsylvania
CHALLENGING ILIAC ACCESSES AND THROMBOSIS PREVENTION
 CHALLENGING ILIAC ACCESSES AND THROMBOSIS PREVENTION ARMANDO MANSILHA MD, PhD, FEBVS UNIVERSITY HOSPITAL - PORTO Disclosure of Interest Speaker name: ARMANDO MANSILHA I have the following potential conflicts
CHALLENGING ILIAC ACCESSES AND THROMBOSIS PREVENTION ARMANDO MANSILHA MD, PhD, FEBVS UNIVERSITY HOSPITAL - PORTO Disclosure of Interest Speaker name: ARMANDO MANSILHA I have the following potential conflicts
Anatomical challenges in EVAR
 Anatomical challenges in EVAR M.H. EL DESSOKI, MD,FRCS PROFESSOR OF VASCULAR SURGERY CAIRO UNIVERSITY Disclosure Speaker name:... I have the following potential conflicts of interest to report: Consulting
Anatomical challenges in EVAR M.H. EL DESSOKI, MD,FRCS PROFESSOR OF VASCULAR SURGERY CAIRO UNIVERSITY Disclosure Speaker name:... I have the following potential conflicts of interest to report: Consulting
Vascular Surgery Cases: Detours. Brian F. Stull, RDMS, RVT UNC REX Healthcare Vascular Specialists
 Vascular Surgery Cases: Detours Brian F. Stull, RDMS, RVT UNC REX Healthcare Vascular Specialists Brian.Stull@Unchealth.unc.edu Objectives Anatomy of a bypass graft Where does it connect, where does it
Vascular Surgery Cases: Detours Brian F. Stull, RDMS, RVT UNC REX Healthcare Vascular Specialists Brian.Stull@Unchealth.unc.edu Objectives Anatomy of a bypass graft Where does it connect, where does it
Disclosures. Carotid artery stenting. Surveillance after Endovascular Intervention: When to Re-Intervene and What s the Evidence
 Disclosures Surveillance after Endovascular Intervention: When to Re-Intervene and What s the Evidence None 2015 UCSF Vascular Symposium Warren Gasper, MD Assistant Professor of Surgery UCSF Division of
Disclosures Surveillance after Endovascular Intervention: When to Re-Intervene and What s the Evidence None 2015 UCSF Vascular Symposium Warren Gasper, MD Assistant Professor of Surgery UCSF Division of
Percutaneous Axillary Artery Access For Branch Grafting for complex TAAAs and pararenal AAAs: How to do it safely
 Percutaneous Axillary Artery Access For Branch Grafting for complex TAAAs and pararenal AAAs: How to do it safely Daniela Branzan, MD, Department of Vascular Surgery University Hospital Leipzig Disclosure
Percutaneous Axillary Artery Access For Branch Grafting for complex TAAAs and pararenal AAAs: How to do it safely Daniela Branzan, MD, Department of Vascular Surgery University Hospital Leipzig Disclosure
Complex Iliocaval Reconstruction PNEC. Seattle WA. Bill Marston MD Professor, Div of Vascular Surgery University of N.
 Complex Iliocaval Reconstruction 2017 PNEC. Seattle WA Bill Marston MD Professor, Div of Vascular Surgery University of N. Carolina DISCLOSURES William Marston, MD Consultant/Advisory Board: Veniti, Cardinal
Complex Iliocaval Reconstruction 2017 PNEC. Seattle WA Bill Marston MD Professor, Div of Vascular Surgery University of N. Carolina DISCLOSURES William Marston, MD Consultant/Advisory Board: Veniti, Cardinal
FEVAR FIFTEEN YEARS OF EFFICIENCY E.DUCASSE MD PHD FEBVS CHU DE BORDEAUX
 FEVAR FIFTEEN YEARS OF EFFICIENCY E.DUCASSE MD PHD FEBVS CHU DE BORDEAUX 2018 A BIT OF HISTORY First use of F-EVAR : 1990s Park et al. J Vasc Interv Radiol. 1996;7:819-823. Faruqi et al. J Endovasc Surg.
FEVAR FIFTEEN YEARS OF EFFICIENCY E.DUCASSE MD PHD FEBVS CHU DE BORDEAUX 2018 A BIT OF HISTORY First use of F-EVAR : 1990s Park et al. J Vasc Interv Radiol. 1996;7:819-823. Faruqi et al. J Endovasc Surg.
Chimney endovascular aneurysm sealing (ch-evas) for ruptured abdominal aortic aneurysms (AAA) due to type Ia endoleak following failed EVAS
 for ruptured abdominal aortic aneurysms (AAA) due to type Ia endoleak following failed EVAS") Chimney endovascular aneurysm sealing (ch-evas) for ruptured abdominal aortic aneurysms (AAA) due to type Ia endoleak following failed EVAS Saritphat Orrapin MD FRCS (Thailand), Thoetphum Benyakorn, Tunyarat
Chimney endovascular aneurysm sealing (ch-evas) for ruptured abdominal aortic aneurysms (AAA) due to type Ia endoleak following failed EVAS Saritphat Orrapin MD FRCS (Thailand), Thoetphum Benyakorn, Tunyarat
Vascular V12. Covered Stent. The New Standard of Care
 Vascular V12 Covered Stent The New Standard of Care Innovation Novel Thermo-Conformable Covered Stent 316L stainless steel stent completely encapsulated in a proprietary one piece eptfe film cast covering
Vascular V12 Covered Stent The New Standard of Care Innovation Novel Thermo-Conformable Covered Stent 316L stainless steel stent completely encapsulated in a proprietary one piece eptfe film cast covering
Surgical Options for revascularisation P E T E R S U B R A M A N I A M
 Surgical Options for revascularisation P E T E R S U B R A M A N I A M The goal Treat pain Heal ulcer Preserve limb Preserve life The options Conservative Endovascular Surgical bypass Primary amputation
Surgical Options for revascularisation P E T E R S U B R A M A N I A M The goal Treat pain Heal ulcer Preserve limb Preserve life The options Conservative Endovascular Surgical bypass Primary amputation
A Case for Mandatory Routine Graft Surveillance of lower extremity bypass grafts. Avishai Meyer UCHSC resident, Surgery May 8, 2006
 A Case for Mandatory Routine Graft Surveillance of lower extremity bypass grafts Avishai Meyer UCHSC resident, Surgery May 8, 2006 Outline: Definition Background of terms and studies U/S surveillance What
A Case for Mandatory Routine Graft Surveillance of lower extremity bypass grafts Avishai Meyer UCHSC resident, Surgery May 8, 2006 Outline: Definition Background of terms and studies U/S surveillance What
Subclavian Revascularization. Douglas E. Drachman, MD, FSCAI Division of Cardiology Vascular Medicine Section December 9, 2014
 Subclavian Revascularization Douglas E. Drachman, MD, FSCAI Division of Cardiology Vascular Medicine Section December 9, 2014 Disclosure Information Douglas E. Drachman, MD, FACC Abbott Vascular, Inc.:
Subclavian Revascularization Douglas E. Drachman, MD, FSCAI Division of Cardiology Vascular Medicine Section December 9, 2014 Disclosure Information Douglas E. Drachman, MD, FACC Abbott Vascular, Inc.:
Intravascular Ultrasound in the Treatment of Complex Aortic Pathologies. Naixin Kang, M.D. Vascular Surgery Fellow April 26 th, 2018
 Intravascular Ultrasound in the Treatment of Complex Aortic Pathologies Naixin Kang, M.D. Vascular Surgery Fellow April 26 th, 2018 DISCLOSURES Nothing To Disclose 2 ENDOVASCULAR AORTIC INTERVENTION Improved
Intravascular Ultrasound in the Treatment of Complex Aortic Pathologies Naixin Kang, M.D. Vascular Surgery Fellow April 26 th, 2018 DISCLOSURES Nothing To Disclose 2 ENDOVASCULAR AORTIC INTERVENTION Improved
The Ventana Off-the-Shelf Graft for Pararenal AAA. Andrew Holden Associate Professor of Radiology Auckland Hospital
 The Ventana Off-the-Shelf Graft for Pararenal AAA Andrew Holden Associate Professor of Radiology Auckland Hospital Disclosures Andrew Holden, MBChB, FRANZCR Investigator in Nellix and Ventana Trials Clinical
The Ventana Off-the-Shelf Graft for Pararenal AAA Andrew Holden Associate Professor of Radiology Auckland Hospital Disclosures Andrew Holden, MBChB, FRANZCR Investigator in Nellix and Ventana Trials Clinical
Acute dissections of the descending thoracic aorta (Debakey
 Endovascular Treatment of Acute Descending Thoracic Aortic Dissections Nimesh D. Desai, MD, PhD, and Joseph E. Bavaria, MD Acute dissections of the descending thoracic aorta (Debakey type III or Stanford
Endovascular Treatment of Acute Descending Thoracic Aortic Dissections Nimesh D. Desai, MD, PhD, and Joseph E. Bavaria, MD Acute dissections of the descending thoracic aorta (Debakey type III or Stanford
Hybrid Repair of a Complex Thoracoabdominal Aortic Aneurysm
 Hybrid Repair of a Complex Thoracoabdominal Aortic Aneurysm Virendra I. Patel MD MPH Assistant Professor of Surgery Massachusetts General Hospital Division of Vascular and Endovascular Surgery Disclosure
Hybrid Repair of a Complex Thoracoabdominal Aortic Aneurysm Virendra I. Patel MD MPH Assistant Professor of Surgery Massachusetts General Hospital Division of Vascular and Endovascular Surgery Disclosure
The Auckland Experience with the Nellix EVAS System. Andrew Holden, MBChB, FRANZCR
 The Auckland Experience with the Nellix EVAS System Andrew Holden, MBChB, FRANZCR Disclosure Speaker name: Associate Professor Andrew Holden I have the following potential conflicts of interest to report:
The Auckland Experience with the Nellix EVAS System Andrew Holden, MBChB, FRANZCR Disclosure Speaker name: Associate Professor Andrew Holden I have the following potential conflicts of interest to report:
DIFFICULT ACCESS REMAINS A CONTRAINDICATION FOR EVAR APOSTOLOS K. TASSIOPOULOS, MD, FACS PROFESSOR AND CHIEF DIVISION OF VASCULAR SURGERY
 DIFFICULT ACCESS REMAINS A CONTRAINDICATION FOR EVAR APOSTOLOS K. TASSIOPOULOS, MD, FACS PROFESSOR AND CHIEF DIVISION OF VASCULAR SURGERY Disclosures Speaker Bureau: - Medtronic - Cook Medical - Bolton
DIFFICULT ACCESS REMAINS A CONTRAINDICATION FOR EVAR APOSTOLOS K. TASSIOPOULOS, MD, FACS PROFESSOR AND CHIEF DIVISION OF VASCULAR SURGERY Disclosures Speaker Bureau: - Medtronic - Cook Medical - Bolton
Ultrasound Imaging of The Posterior Circulation
 Ultrasound Imaging of The Posterior Circulation Michigan Sonographers Society 2 Nd Annual Fall Vascular Conference Larry N. Raber RDMS-RVT Clinical Manager General Ultrasound/Neurovascular Laboratory Cleveland
Ultrasound Imaging of The Posterior Circulation Michigan Sonographers Society 2 Nd Annual Fall Vascular Conference Larry N. Raber RDMS-RVT Clinical Manager General Ultrasound/Neurovascular Laboratory Cleveland
DEPARTMENT OF HEALTH & HUMAN SERVICES Public Health Service
 M AY. 6. 2011 10:37 A M F D A - C D R H - O D E - P M O N O. 4147 P. 1 DEPARTMENT OF HEALTH & HUMAN SERVICES Public Health Service Food and Drug Administration 10903 New Hampshire Avenue Document Control
M AY. 6. 2011 10:37 A M F D A - C D R H - O D E - P M O N O. 4147 P. 1 DEPARTMENT OF HEALTH & HUMAN SERVICES Public Health Service Food and Drug Administration 10903 New Hampshire Avenue Document Control
Hybrid Procedures for Peripheral Obstructive Disease - Step by Step -
 Hybrid Procedures for Peripheral Obstructive Disease - Step by Step - Holger Staab, MD University Hospital Leipzig, Germany Clinic for Vascular Surgery Disclosure Speaker name:..holger Staab... I have
Hybrid Procedures for Peripheral Obstructive Disease - Step by Step - Holger Staab, MD University Hospital Leipzig, Germany Clinic for Vascular Surgery Disclosure Speaker name:..holger Staab... I have
The Role of US in Chronic Mesenteric Ischemia. Sagar S. Gandhi, MD Vascular Health Alliance Greenville Health System
 The Role of US in Chronic Mesenteric Ischemia Sagar S. Gandhi, MD Vascular Health Alliance Greenville Health System No Disclosures Mesenteric Ischemia Anatomy Presentation Diagnostic tools Treatment Celiac
The Role of US in Chronic Mesenteric Ischemia Sagar S. Gandhi, MD Vascular Health Alliance Greenville Health System No Disclosures Mesenteric Ischemia Anatomy Presentation Diagnostic tools Treatment Celiac
Pre-and Post Procedure Non-Invasive Evaluation of the Patient with Carotid Disease
 Pre-and Post Procedure Non-Invasive Evaluation of the Patient with Carotid Disease Michael R. Jaff, D.O., F.A.C.P., F.A.C.C. Assistant Professor of Medicine Harvard Medical School Director, Vascular Medicine
Pre-and Post Procedure Non-Invasive Evaluation of the Patient with Carotid Disease Michael R. Jaff, D.O., F.A.C.P., F.A.C.C. Assistant Professor of Medicine Harvard Medical School Director, Vascular Medicine
The present status of selfexpanding. for CLI: Why and when to use. Sean P Lyden MD Cleveland Clinic Cleveland, Ohio
 The present status of selfexpanding and balloonexpandable tibial BMS and DES for CLI: Why and when to use Sean P Lyden MD Cleveland Clinic Cleveland, Ohio Disclosure Speaker name: Sean Lyden, MD I have
The present status of selfexpanding and balloonexpandable tibial BMS and DES for CLI: Why and when to use Sean P Lyden MD Cleveland Clinic Cleveland, Ohio Disclosure Speaker name: Sean Lyden, MD I have
Accessi Iliaci Ostili
 Alma Mater Studiorum Bologna University S.Orsola-Malpighi, Bologna, Italy Vascular Surgery Accessi Iliaci Ostili nel trattamento della patologia aortica E. Gallitto Iliac Navigations Alma Mater Studiorum
Alma Mater Studiorum Bologna University S.Orsola-Malpighi, Bologna, Italy Vascular Surgery Accessi Iliaci Ostili nel trattamento della patologia aortica E. Gallitto Iliac Navigations Alma Mater Studiorum
EVAR replaced standard repair in most cases. Why?
 EVAR replaced standard repair in most cases. Why? Initial major steps in endograft evolution Papazoglou O. Konstantinos M.D. The story of a major breakthrough in vascular surgery 1991 Parodi introduces
EVAR replaced standard repair in most cases. Why? Initial major steps in endograft evolution Papazoglou O. Konstantinos M.D. The story of a major breakthrough in vascular surgery 1991 Parodi introduces
Visceral Vascular Ultrasound. Joel Thompson, MD, MPH Borg & Ide Imaging
 Visceral Vascular Ultrasound Joel Thompson, MD, MPH Borg & Ide Imaging Objectives: Review major abdominal vascular structures Identify normal peak systolic velocity (PSV) for major abdominal arteries.
Visceral Vascular Ultrasound Joel Thompson, MD, MPH Borg & Ide Imaging Objectives: Review major abdominal vascular structures Identify normal peak systolic velocity (PSV) for major abdominal arteries.
Treatment options of late failures of EVAS. Michel Reijnen Rijnstate Arnhem The Netherlands
 Treatment options of late failures of EVAS Michel Reijnen Rijnstate Arnhem The Netherlands Disclosure Speaker name: Michel Reijnen I have the following potential conflicts of interest to report: Consulting
Treatment options of late failures of EVAS Michel Reijnen Rijnstate Arnhem The Netherlands Disclosure Speaker name: Michel Reijnen I have the following potential conflicts of interest to report: Consulting
Subclavian artery Stenting
 Subclavian artery Stenting Etiology Atherosclerosis Takayasu s arteritis Fibromuscular dysplasia Giant Cell Arteritis Radiation-induced Vascular Injury Thoracic Outlet Syndrome Neurofibromatosis Incidence
Subclavian artery Stenting Etiology Atherosclerosis Takayasu s arteritis Fibromuscular dysplasia Giant Cell Arteritis Radiation-induced Vascular Injury Thoracic Outlet Syndrome Neurofibromatosis Incidence
Endovascular and Hybrid Treatment of TASC C & D Aortoiliac Occlusive Disease
 Endovascular and Hybrid Treatment of TASC C & D Aortoiliac Occlusive Disease Arash Bornak, MD FACS Vascular & Endovascular Surgery University of Miami Miller School of Medicine No disclosure BACKGROUND
Endovascular and Hybrid Treatment of TASC C & D Aortoiliac Occlusive Disease Arash Bornak, MD FACS Vascular & Endovascular Surgery University of Miami Miller School of Medicine No disclosure BACKGROUND
FLEXIBLE, BALOON EXPANDABLE
 EARLY RESULTS OF A CLINICAL TRIAL OF FLEXIBLE, BALOON EXPANDABLE COVERED STENT GRAFT IN ILIAC OCCLUSIVE DISEASE Chris LeCroy Coastal Vascular and Interventional Pensacola, Florida Clinical Trial WL GORE
EARLY RESULTS OF A CLINICAL TRIAL OF FLEXIBLE, BALOON EXPANDABLE COVERED STENT GRAFT IN ILIAC OCCLUSIVE DISEASE Chris LeCroy Coastal Vascular and Interventional Pensacola, Florida Clinical Trial WL GORE
Accurate Vessel Sizing Drives Clinical Results. IVUS In the Periphery
 Accurate Vessel Sizing Drives Clinical Results IVUS In the Periphery Discussion Iida O, et. al. Study Efficacy of Intravascular Ultrasound in Femoropopliteal Stenting for Peripheral Artery Disease With
Accurate Vessel Sizing Drives Clinical Results IVUS In the Periphery Discussion Iida O, et. al. Study Efficacy of Intravascular Ultrasound in Femoropopliteal Stenting for Peripheral Artery Disease With
11/20/2014. Disclosures. Kissing Balloons and Stents. Treatment of Aortoiliac Occlusive Disease. Data on Patency of Kissing Stents.
 RESULTS FROM A MULTI-CENTER, RETROSPECTIVE REVIEW OF THE AFX ENDOGRAFT FOR USE IN AORTOILIAC OCCLUSIVE DISEASE Disclosures Cook Endologix Medtronic Thomas Maldonado, MD Associate Professor Department of
RESULTS FROM A MULTI-CENTER, RETROSPECTIVE REVIEW OF THE AFX ENDOGRAFT FOR USE IN AORTOILIAC OCCLUSIVE DISEASE Disclosures Cook Endologix Medtronic Thomas Maldonado, MD Associate Professor Department of
Appropriate Device Selection for Endovascular Procedures
 Appropriate Device Selection for Endovascular Procedures Thomas M. Shimshak, MD Florida Hospital Heartland Medical Center Sebring, Florida Disclosures Speaker s Bureau: Abbott Vascular Boston Scientific
Appropriate Device Selection for Endovascular Procedures Thomas M. Shimshak, MD Florida Hospital Heartland Medical Center Sebring, Florida Disclosures Speaker s Bureau: Abbott Vascular Boston Scientific
SAMMPRIS. Stenting and Aggressive Medical Management for Preventing Recurrent Stroke and Intracranial Stenosis. Khalil Zahra, M.D
 SAMMPRIS Stenting and Aggressive Medical Management for Preventing Recurrent Stroke and Intracranial Stenosis Khalil Zahra, M.D Major points Patients with recent TIA or stroke and intra-cranial artery
SAMMPRIS Stenting and Aggressive Medical Management for Preventing Recurrent Stroke and Intracranial Stenosis Khalil Zahra, M.D Major points Patients with recent TIA or stroke and intra-cranial artery
Deb Coghlan AMS (Vascular and General ) Brisbane, Australia
 Brisbane, Australia") Deb Coghlan AMS (Vascular and General ) Brisbane, Australia ANEURYSMAL DIISEASE The infrarenal aorta enlarges with age, and is the commonest site for arterial aneurysms. An aneurysm is a permanent focal
Deb Coghlan AMS (Vascular and General ) Brisbane, Australia ANEURYSMAL DIISEASE The infrarenal aorta enlarges with age, and is the commonest site for arterial aneurysms. An aneurysm is a permanent focal
Hepatic Artery Stenosis After Liver Transplantation: Is Endovascular Treatment Always Necessary?
 LIVER TRANSPLANTATION 21:162 168, 2015 ORIGINAL ARTICLE Hepatic Artery Stenosis After Liver Transplantation: Is Endovascular Treatment Always Necessary? Carlo Pulitano, 1,2 David Joseph, 1 Charbel Sandroussi,
LIVER TRANSPLANTATION 21:162 168, 2015 ORIGINAL ARTICLE Hepatic Artery Stenosis After Liver Transplantation: Is Endovascular Treatment Always Necessary? Carlo Pulitano, 1,2 David Joseph, 1 Charbel Sandroussi,
MESENTERIC ISCHEMIA. Phillip J Bendick, PhD
 MESENTERIC ISCHEMIA Phillip J Bendick, PhD Arterial Celiac - Hepatic - Splenic Superior Mesenteric Artery Inferior Mesenteric Artery Venous Mesenteric system Porto - hepatic system Inferior Vena Cava Acute
MESENTERIC ISCHEMIA Phillip J Bendick, PhD Arterial Celiac - Hepatic - Splenic Superior Mesenteric Artery Inferior Mesenteric Artery Venous Mesenteric system Porto - hepatic system Inferior Vena Cava Acute
Technique and Outcome of Laser Fenestration For Arch Vessels
 Technique and Outcome of Laser Fenestration For Arch Vessels Jean M. Panneton MD, FRCSC, FACS Professor of Surgery Chief & Program Director Division of Vascular Surgery Eastern Virginia Medical School
Technique and Outcome of Laser Fenestration For Arch Vessels Jean M. Panneton MD, FRCSC, FACS Professor of Surgery Chief & Program Director Division of Vascular Surgery Eastern Virginia Medical School
Crossing the Long SFA CTO
 Crossing the Long SFA CTO Techniques and Variables You need to Know Kyoto Katsura Hospital Cardiovascular Center Shigeru Nakamura M.D. Korea Soul 2011.4.28 28 Back ground Superficial femoral artery (SFA)
Crossing the Long SFA CTO Techniques and Variables You need to Know Kyoto Katsura Hospital Cardiovascular Center Shigeru Nakamura M.D. Korea Soul 2011.4.28 28 Back ground Superficial femoral artery (SFA)
Endovascular Management of Thoracic Aortic Pathology Stéphan Haulon, J Sobocinski, B Maurel, T Martin-Gonzalez, R Spear, A Hertault, R Azzaoui
 Endovascular Management of Thoracic Aortic Pathology Stéphan Haulon, J Sobocinski, B Maurel, T Martin-Gonzalez, R Spear, A Hertault, R Azzaoui Aortic Center, Lille University Hospital, France Disclosures
Endovascular Management of Thoracic Aortic Pathology Stéphan Haulon, J Sobocinski, B Maurel, T Martin-Gonzalez, R Spear, A Hertault, R Azzaoui Aortic Center, Lille University Hospital, France Disclosures
US of Renovascular Hypertension. Jonathan R. Dillman, MD, MSc Associate Professor Director, Thoracoabdominal Imaging
 US of Renovascular Hypertension Jonathan R. Dillman, MD, MSc Associate Professor Director, Thoracoabdominal Imaging Disclosures Nothing Relevant Unrelated grant funding Siemens US Toshiba US Objectives
US of Renovascular Hypertension Jonathan R. Dillman, MD, MSc Associate Professor Director, Thoracoabdominal Imaging Disclosures Nothing Relevant Unrelated grant funding Siemens US Toshiba US Objectives
Lessons learned from Ch-EVAR for the treatment of. Miltos Matsagkas MD, PhD, FEBVS Professor of Vascular Surgery University of Thessaly
 Lessons learned from Ch-EVAR for the treatment of pararenal AAAs Miltos Matsagkas MD, PhD, FEBVS Professor of Vascular Surgery University of Thessaly Ch-EVAR Ch-EVAR = Chimney-EVAR Placement of single
Lessons learned from Ch-EVAR for the treatment of pararenal AAAs Miltos Matsagkas MD, PhD, FEBVS Professor of Vascular Surgery University of Thessaly Ch-EVAR Ch-EVAR = Chimney-EVAR Placement of single
Percutaneous Transluminal Angioplasty and Stenting for Hepatic Vessel Stenosis after Orthotopic Liver Transplantation
 Brief Report Acta Cardiol Sin 2015;31:152 157 doi: 10.6515/ACS20140503A Percutaneous Transluminal Angioplasty and Stenting for Hepatic Vessel Stenosis after Orthotopic Liver Transplantation Ming-Yuan Luo,
Brief Report Acta Cardiol Sin 2015;31:152 157 doi: 10.6515/ACS20140503A Percutaneous Transluminal Angioplasty and Stenting for Hepatic Vessel Stenosis after Orthotopic Liver Transplantation Ming-Yuan Luo,
Total Endovascular Repair Type A Dissection. Eric Herget Interventional Radiology
 Total Endovascular Repair Type A Dissection Eric Herget Interventional Radiology 65 year old male Acute Type A Dissection Severe Aortic Regurgitation No co-morbidities Management? Part II Evolving Global
Total Endovascular Repair Type A Dissection Eric Herget Interventional Radiology 65 year old male Acute Type A Dissection Severe Aortic Regurgitation No co-morbidities Management? Part II Evolving Global
(EU), FACC (USA), FSCAI (USA)
, FACC (USA), FSCAI (USA)") How to reduce vascular complications of TAVI Paul TL Chiam MBBS (S pore), MMed, MRCP (UK), FAMS FRCP (Edin), FESC (EU), FACC (USA), FSCAI (USA) Cardiologist Mount Elizabeth Hospital Singapore Definition
How to reduce vascular complications of TAVI Paul TL Chiam MBBS (S pore), MMed, MRCP (UK), FAMS FRCP (Edin), FESC (EU), FACC (USA), FSCAI (USA) Cardiologist Mount Elizabeth Hospital Singapore Definition
UC SF An Algorithm to Choose Which Uncomplicated (Asymptomatic) Acute Type B Dissection Patients Should Undergo TEVAR. Disclosures.
 Acute Type B Dissection Patients Should Undergo TEVAR. Disclosures.") An Algorithm to Choose Which Uncomplicated (Asymptomatic) Acute Type B Dissection Patients Should Undergo TEVAR Disclosures Royalties and research grant support from Cook Medical, Inc. Jade S. Hiramoto,
An Algorithm to Choose Which Uncomplicated (Asymptomatic) Acute Type B Dissection Patients Should Undergo TEVAR Disclosures Royalties and research grant support from Cook Medical, Inc. Jade S. Hiramoto,
MAXIMIZE RADIAL SOLUTIONS TO PERIPHERAL CHALLENGES
 MAXIMIZE RADIAL SOLUTIONS TO PERIPHERAL CHALLENGES PUSHING BOUNDARIES Terumo Interventional Systems is committed to your success with innovative procedural solutions and ongoing support for your most challenging
MAXIMIZE RADIAL SOLUTIONS TO PERIPHERAL CHALLENGES PUSHING BOUNDARIES Terumo Interventional Systems is committed to your success with innovative procedural solutions and ongoing support for your most challenging
Indications: following: embolization. artery that has diseases 5. The evaluation. of suspected. such entities. a cold hand. biopsy
 Peripheral Arterial Ultrasound Protocol Using Color and Spectral Doppler Reviewed by: Mark Yuhasz, MD Last Review Date: January 2015 Contact: (866) 761 4200, Option 1 Indications: The indications for peripheral
Peripheral Arterial Ultrasound Protocol Using Color and Spectral Doppler Reviewed by: Mark Yuhasz, MD Last Review Date: January 2015 Contact: (866) 761 4200, Option 1 Indications: The indications for peripheral
Popliteal Aneurysm: When is surgical therapy indicated? PROF. GRZEGORZ OSZKINIS
 Popliteal Aneurysm: When is surgical therapy indicated? PROF. GRZEGORZ OSZKINIS Asymptomatic mass - 38-40%will develop symptoms at a rate of 14%/yr Intermittent claudic ation (chronic ischemia) - 25%-40%
Popliteal Aneurysm: When is surgical therapy indicated? PROF. GRZEGORZ OSZKINIS Asymptomatic mass - 38-40%will develop symptoms at a rate of 14%/yr Intermittent claudic ation (chronic ischemia) - 25%-40%
Endovascular Repair of Combined Occluded Femoral and Popliteal Arteries
 MEET 2013 Endovascular Repair of Combined Occluded Femoral and Popliteal Arteries ALI AMIN MD, FACS,FACC, RVT CHIEF OF ENDOVASCULAR INTERVENTIONS READING HOSPITAL AND MEDICAL CENTER READING, PA USA Chronic
MEET 2013 Endovascular Repair of Combined Occluded Femoral and Popliteal Arteries ALI AMIN MD, FACS,FACC, RVT CHIEF OF ENDOVASCULAR INTERVENTIONS READING HOSPITAL AND MEDICAL CENTER READING, PA USA Chronic
NON-ATHEROSCLEROTIC PATHOLOGY OF THE CAROTID ARTERIES
 NON-ATHEROSCLEROTIC PATHOLOGY OF THE CAROTID ARTERIES Leslie M. Scoutt, MD, FACR Professor of Diagnostic Radiology & Surgery Vice Chair, Dept of Radiology & Biomedical Imaging Chief, Ultrasound Section
NON-ATHEROSCLEROTIC PATHOLOGY OF THE CAROTID ARTERIES Leslie M. Scoutt, MD, FACR Professor of Diagnostic Radiology & Surgery Vice Chair, Dept of Radiology & Biomedical Imaging Chief, Ultrasound Section
Retrograde Embolization of a Symptomatic Hypogastric Artery Aneurysm
 Retrograde Embolization of a Symptomatic Hypogastric Artery Aneurysm Andrew Unzeitig MD Piedmont Atlanta Hospital Georgia Vascular Society 2017 Annual Meeting Lake Oconee, Georgia Disclosures None Case
Retrograde Embolization of a Symptomatic Hypogastric Artery Aneurysm Andrew Unzeitig MD Piedmont Atlanta Hospital Georgia Vascular Society 2017 Annual Meeting Lake Oconee, Georgia Disclosures None Case
Present & future of below the knee stenting
 Session 5 Below the knee arteries & limb salvage Present & future of below the knee stenting M. Bosiers K. Deloose P. Peeters 1 PRESENT Clinical perspective whom to treat CRITICAL LIMB ISCHEMIA (CLI) 0
Session 5 Below the knee arteries & limb salvage Present & future of below the knee stenting M. Bosiers K. Deloose P. Peeters 1 PRESENT Clinical perspective whom to treat CRITICAL LIMB ISCHEMIA (CLI) 0
John E. Campbell, MD Assistant Professor of Surgery and Medicine Department of Vascular Surgery West Virginia University, Charleston Division
 John E. Campbell, MD Assistant Professor of Surgery and Medicine Department of Vascular Surgery West Virginia University, Charleston Division John Campbell, MD For the 12 months preceding this CME activity,
John E. Campbell, MD Assistant Professor of Surgery and Medicine Department of Vascular Surgery West Virginia University, Charleston Division John Campbell, MD For the 12 months preceding this CME activity,
Bifurcated system Proximal suprarenal stent Modular (aortic main body and two iliac legs) Full thickness woven polyester graft material Fully
 Full thickness woven polyester graft material Fully") Physician Training Bifurcated system Proximal suprarenal stent Modular (aortic main body and two iliac legs) Full thickness woven polyester graft material Fully supported by self-expanding z-stents H&L-B
Physician Training Bifurcated system Proximal suprarenal stent Modular (aortic main body and two iliac legs) Full thickness woven polyester graft material Fully supported by self-expanding z-stents H&L-B
HD Scanning: Velocities and Volume Flow
 HD Scanning: Velocities and Volume Flow Non-Invasive Lab Symposium West Orange, NJ April 27, 2018 Volume Flow Cindy Sturt, MD, FACS, RVT 500,000 Americans on dialysis 20-25% annual mortality 65% 5 year
HD Scanning: Velocities and Volume Flow Non-Invasive Lab Symposium West Orange, NJ April 27, 2018 Volume Flow Cindy Sturt, MD, FACS, RVT 500,000 Americans on dialysis 20-25% annual mortality 65% 5 year
Case 8038 Renal allograft complicated with renal artery stenosis
 Case 8038 Renal allograft complicated with renal artery stenosis Santiago I, Canelas A, Pinto AP Section: Cardiovascular Published: 2009, Nov. 30 Patient: 61 year(s), male Clinical History A 61-year-old
Case 8038 Renal allograft complicated with renal artery stenosis Santiago I, Canelas A, Pinto AP Section: Cardiovascular Published: 2009, Nov. 30 Patient: 61 year(s), male Clinical History A 61-year-old
Copyright HMP Communications
 Ocelot With Wildcat in a Complicated Superficial Femoral Artery Chronic Total Occlusion Soundos K. Moualla, MD, FACC, FSCAI; Richard R. Heuser, MD, FACC, FACP, FESC, FSCAI From Phoenix Heart Center, Phoenix,
Ocelot With Wildcat in a Complicated Superficial Femoral Artery Chronic Total Occlusion Soundos K. Moualla, MD, FACC, FSCAI; Richard R. Heuser, MD, FACC, FACP, FESC, FSCAI From Phoenix Heart Center, Phoenix,
Comparison Of Primary Long Stenting Versus Primary Short Stenting For Long Femoropopliteal Artery Disease (PARADE)
") Comparison Of Primary Long Stenting Versus Primary Short Stenting For Long Femoropopliteal Artery Disease (PARADE) Young-Guk Ko, M.D. Severance Cardiovascular Hospital, Yonsei University Health System,
Comparison Of Primary Long Stenting Versus Primary Short Stenting For Long Femoropopliteal Artery Disease (PARADE) Young-Guk Ko, M.D. Severance Cardiovascular Hospital, Yonsei University Health System,
CAROTID ARTERY ANGIOPLASTY
 CAROTID ARTERY ANGIOPLASTY Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices and
CAROTID ARTERY ANGIOPLASTY Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices and
Malperfusion Syndromes Type B Aortic Dissection with Malperfusion
 Malperfusion Syndromes Type B Aortic Dissection with Malperfusion Jade S. Hiramoto, MD, MAS April 27, 2012 Associated with early mortality Occurs when there is end organ ischemia secondary to aortic branch
Malperfusion Syndromes Type B Aortic Dissection with Malperfusion Jade S. Hiramoto, MD, MAS April 27, 2012 Associated with early mortality Occurs when there is end organ ischemia secondary to aortic branch
BIOLUX P-III Passeo-18 Lux All-comers Registry: 12-month Results for the All-Comers Cohort
 BIOLUX P-III Passeo-18 Lux All-comers Registry: 12-month Results for the All-Comers Cohort Prof. Dr. Gunnar TEPE, Klinikum Rosenheim, Germany CCI on behalf of the BIOLUX P-III Investigators Disclosure
BIOLUX P-III Passeo-18 Lux All-comers Registry: 12-month Results for the All-Comers Cohort Prof. Dr. Gunnar TEPE, Klinikum Rosenheim, Germany CCI on behalf of the BIOLUX P-III Investigators Disclosure
Jean M Panneton, MD Professor of Surgery Program Director Vascular Surgery Chief EVMS. Arch Pathology: The Endovascular Era is here
 Jean M Panneton, MD Professor of Surgery Program Director Vascular Surgery Chief EVMS Arch Pathology: The Endovascular Era is here Disclosures Consultant: Cook Medical, Bolton Medical, Medtronic Inc, Volcano,
Jean M Panneton, MD Professor of Surgery Program Director Vascular Surgery Chief EVMS Arch Pathology: The Endovascular Era is here Disclosures Consultant: Cook Medical, Bolton Medical, Medtronic Inc, Volcano,
Combined Endovascular and Surgical Repair of Thoracoabdominal Aortic Pathology: Hybrid TEVAR
 Combined Endovascular and Surgical Repair of Thoracoabdominal Aortic Pathology: Hybrid TEVAR William J. Quinones-Baldrich MD Professor of Surgery Director UCLA Aortic Center UCLA Medical Center Los Angeles,
Combined Endovascular and Surgical Repair of Thoracoabdominal Aortic Pathology: Hybrid TEVAR William J. Quinones-Baldrich MD Professor of Surgery Director UCLA Aortic Center UCLA Medical Center Los Angeles,
Evaluating the economic value of 5F systems for outpatients
 Evaluating the economic value of 5F systems for outpatients Pr Yann Gouëffic, MD, PhD Department of vascular surgery - University Hospital of Nantes, France Disclosure Speaker's name: Yann Goueffic I have
Evaluating the economic value of 5F systems for outpatients Pr Yann Gouëffic, MD, PhD Department of vascular surgery - University Hospital of Nantes, France Disclosure Speaker's name: Yann Goueffic I have
Visceral aneurysm. Diagnosis and Interventions M.NEDEVSKA
 Visceral aneurysm Diagnosis and Interventions M.NEDEVSKA History 1953 De Bakeyand Cooley Visceral aneurysm VAAs rare, reported incidence of 0.01 to 0.2% on routine autopsies. Clinically important Potentially
Visceral aneurysm Diagnosis and Interventions M.NEDEVSKA History 1953 De Bakeyand Cooley Visceral aneurysm VAAs rare, reported incidence of 0.01 to 0.2% on routine autopsies. Clinically important Potentially
Lower Extremity Peripheral Arterial Disease: Less is Sometimes More. Spence M Taylor, M.D.
 Lower Extremity Peripheral Arterial Disease: Less is Sometimes More Spence M Taylor, M.D. President, Greenville Health System Clinical University Senior Associate Dean for Academic Affairs and Diversity
Lower Extremity Peripheral Arterial Disease: Less is Sometimes More Spence M Taylor, M.D. President, Greenville Health System Clinical University Senior Associate Dean for Academic Affairs and Diversity
The Utility of Atherectomy and the Jetstream Atherectomy System
 The Utility of Atherectomy and the Jetstream Atherectomy System William A. Gray, MD Columbia University Medical Center 2014 Boston Scientific Corporation or its affiliates. All rights reserved. IMPORTANT
The Utility of Atherectomy and the Jetstream Atherectomy System William A. Gray, MD Columbia University Medical Center 2014 Boston Scientific Corporation or its affiliates. All rights reserved. IMPORTANT
1 Year Result Of Stent Graft For Carotid Artery Pseudo- Aneurysm In Behcet s Disease Patients
 1 Year Result Of Stent Graft For Carotid Artery Pseudo- Aneurysm In Behcet s Disease Patients H Lotfy, W Shaalan, A Elemam, A Naga Prof Dr Hassan Lotfy Vascular and Endovascular Consultant Alexandria University
1 Year Result Of Stent Graft For Carotid Artery Pseudo- Aneurysm In Behcet s Disease Patients H Lotfy, W Shaalan, A Elemam, A Naga Prof Dr Hassan Lotfy Vascular and Endovascular Consultant Alexandria University
Recanalization Techniques: Sharp Needle Recanalization. Recanalization Techniques: Sharp Needle Recanalization
 Recanalization of Occluded Central Veins When Conventional Methods Failed: Abigail Falk, MD, FSIR American Access Care New York, NY Conventional Methods of Recanalization Directional 0.035 and 0.018 Guidewires
Recanalization of Occluded Central Veins When Conventional Methods Failed: Abigail Falk, MD, FSIR American Access Care New York, NY Conventional Methods of Recanalization Directional 0.035 and 0.018 Guidewires
CAROTID ARTERY ANGIOPLASTY
 CAROTID ARTERY ANGIOPLASTY Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Medical Coverage Guideline
CAROTID ARTERY ANGIOPLASTY Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Medical Coverage Guideline
Critical limb ischemia due to an occlusion of an aorto-biiliac prothesis step by step case presentation and decision making
 Critical limb ischemia due to an occlusion of an aorto-biiliac prothesis step by step case presentation and decision making Dr. Özgün Sensebat Vascular and general surgeon Vascular Private Clinic Dorsten
Critical limb ischemia due to an occlusion of an aorto-biiliac prothesis step by step case presentation and decision making Dr. Özgün Sensebat Vascular and general surgeon Vascular Private Clinic Dorsten
PATIENT SPECIFIC STRATEGIES IN CRITICAL LIMB ISCHEMIA. Dr. Manar Trab Consultant Vascular Surgeon European Vascular Clinic DMCC Dubai, UAE
 PATIENT SPECIFIC STRATEGIES IN CRITICAL LIMB ISCHEMIA Dr. Manar Trab Consultant Vascular Surgeon European Vascular Clinic DMCC Dubai, UAE Disclosure Speaker name: DR. Manar Trab I have the following potential
PATIENT SPECIFIC STRATEGIES IN CRITICAL LIMB ISCHEMIA Dr. Manar Trab Consultant Vascular Surgeon European Vascular Clinic DMCC Dubai, UAE Disclosure Speaker name: DR. Manar Trab I have the following potential
Management of In-stent Restenosis after Lower Extremity Endovascular Procedures
 Management of In-stent Restenosis after Lower Extremity Endovascular Procedures Piotr Sobieszczyk, MD Associate Director, Cardiac Catheterization Laboratory Cardiovascular Division and Vascular Medicine
Management of In-stent Restenosis after Lower Extremity Endovascular Procedures Piotr Sobieszczyk, MD Associate Director, Cardiac Catheterization Laboratory Cardiovascular Division and Vascular Medicine
Specificities for infrapopliteal stents
 Specificities for infrapopliteal stents Nicolas Diehm, M.D. Swiss Cardiovascular Center Clinical and Interventional Angiology University Hospital Bern, Switzerland Disclosures Speaker`s Bureau: MEDRAD,
Specificities for infrapopliteal stents Nicolas Diehm, M.D. Swiss Cardiovascular Center Clinical and Interventional Angiology University Hospital Bern, Switzerland Disclosures Speaker`s Bureau: MEDRAD,
Chungbuk Regional Cardiovascular Center, Division of Cardiology, Departments of Internal Medicine, Chungbuk National University Hospital Sangmin Kim
 Endovascular Procedures for Isolated Common Iliac and Internal Iliac Aneurysm Chungbuk Regional Cardiovascular Center, Division of Cardiology, Departments of Internal Medicine, Chungbuk National University
Endovascular Procedures for Isolated Common Iliac and Internal Iliac Aneurysm Chungbuk Regional Cardiovascular Center, Division of Cardiology, Departments of Internal Medicine, Chungbuk National University
UC SF. Disclosures. Thoracic Endovascular Aortic Repair 4/24/2009. Management of Acute Dissections: Is There Still a Role for Open Surgery?
 UC SF Management of Acute Dissections: Is There Still a Role for Open Surgery? Darren B. Schneider, M.D. Assistant Professor of Surgery and Radiology Division of Vascular Surgery University of California
UC SF Management of Acute Dissections: Is There Still a Role for Open Surgery? Darren B. Schneider, M.D. Assistant Professor of Surgery and Radiology Division of Vascular Surgery University of California
Preliminary Data from the Gore EXCLUDER Thoracoabdominal Branch Endoprosthesis Early Feasibility Study
 Preliminary Data from the Gore EXCLUDER Thoracoabdominal Branch Endoprosthesis Early Feasibility Study Mark A Farber, MD Professor of Surgery and Radiology Director, UNC Aortic Network University of North
Preliminary Data from the Gore EXCLUDER Thoracoabdominal Branch Endoprosthesis Early Feasibility Study Mark A Farber, MD Professor of Surgery and Radiology Director, UNC Aortic Network University of North
The SplitWire Percutaneous Transluminal Angioplasty Scoring Device. Instructions for Use
 The SplitWire Percutaneous Transluminal Angioplasty Scoring Device Instructions for Use Contents Contains one (1) SplitWire device. Sterile. Sterilized with ethylene oxide gas. Radiopaque. For single use
The SplitWire Percutaneous Transluminal Angioplasty Scoring Device Instructions for Use Contents Contains one (1) SplitWire device. Sterile. Sterilized with ethylene oxide gas. Radiopaque. For single use
Endovascular Abdominal Repair: Technical Tips to Achieve Best Results and Avoid Disaster
 Endovascular Abdominal Repair: Technical Tips to Achieve Best Results and Avoid Disaster RICHARD R. HEUSER, MD, FACC, FACP, FESC, FASCI Director Of Cardiology, St. Luke s Medical Center, Phoenix, Arizona
Endovascular Abdominal Repair: Technical Tips to Achieve Best Results and Avoid Disaster RICHARD R. HEUSER, MD, FACC, FACP, FESC, FASCI Director Of Cardiology, St. Luke s Medical Center, Phoenix, Arizona
Access More Patients. Customize Each Seal.
 Access More. Customize Each Seal. The Least Invasive Path Towards Proven Patency ULTRA LOW PROFILE TO EASE ADVANCEMENT The flexible, ultra-low 12F ID Ovation ix delivery system enables you to navigate
Access More. Customize Each Seal. The Least Invasive Path Towards Proven Patency ULTRA LOW PROFILE TO EASE ADVANCEMENT The flexible, ultra-low 12F ID Ovation ix delivery system enables you to navigate
Postoperative AV Fistula Evaluation. Postoperative examination protocol. Postoperative AVF Protocol. Hemodialysis Access Surveillance
 Hemodialysis Access Surveillance Postoperative AV Fistula Evaluation Failure of maturation Stenosis Perigraft mass/fluid collection Joseph L. Mills, Sr., M.D. Professor of Surgery Chief, Division of Vascular
Hemodialysis Access Surveillance Postoperative AV Fistula Evaluation Failure of maturation Stenosis Perigraft mass/fluid collection Joseph L. Mills, Sr., M.D. Professor of Surgery Chief, Division of Vascular
US clinical trial update on the Gore Excluder iliac branch endoprosthesis (IBE)
") US clinical trial update on the Gore Excluder iliac branch endoprosthesis (IBE) Robert Y. Rhee, MD Chief, Vascular and Endovascular Surgery Director, Maimonides Aortic Center Maimonides Medical Center
US clinical trial update on the Gore Excluder iliac branch endoprosthesis (IBE) Robert Y. Rhee, MD Chief, Vascular and Endovascular Surgery Director, Maimonides Aortic Center Maimonides Medical Center
Christian Wissgott MD, PhD Assistant Director, Radiology Westküstenkliniken Heide
 2-Year Results Of The Tack Optimized Balloon Angioplasty (TOBA) Trial For Fem- Pop Lesions Demonstrates Safety and Efficacy Of The Tack Endovascular System In Repairing Focal Post-PTA Dissections Christian
2-Year Results Of The Tack Optimized Balloon Angioplasty (TOBA) Trial For Fem- Pop Lesions Demonstrates Safety and Efficacy Of The Tack Endovascular System In Repairing Focal Post-PTA Dissections Christian