Telemedicine. Gabriel A. Vidal, MD
|
|
|
- Maria Rosamund White
- 6 years ago
- Views:
Transcription

1 Telemedicine Gabriel A. Vidal, MD Director Comprehensive Stroke Center Ochsner Medical Center, New Orleans Vascular and Interventional Neurology Gulf States Chapter of the Society of Hospital Medicine 12 th Annual Conference July 8 th, 2016
2 Disclosures Consultant Stryker Speaker s bureau Stryker Penumbra Inc. Genentech Inc.
3 Objectives Clinical problem Description of telestroke networks and models Clinical outcomes and effectiveness Review of Ochsner s telestroke network
4 Burden of stroke US has ~ 4 neurologists per 100,000 persons Caring for more than 795,000 strokes per year Many parts of US are without access to acute services entirely Neurologists across the country are opting out of call coverage for stroke and other neurologic emergencies Direct and indirect costs of stroke are estimated to be $62.7 billion annually in the US
5 Burden of stroke Rapid recognition and accurate diagnosis are critical Many conditions can mimic stroke Misdiagnosis rate by primary care and emergency physicians may be as high as 30% Delays in diagnosis and misdiagnosis limit the use of proven therapies Evidence concerning litigation involving stroke therapy with IV rtpa indicates liability is predominantly associated with failure to provide treatment rather than adverse events
6 Stroke/TIA Mimickers Seizure Migraine Hypoglycemia Bell s Palsy Vestibulopathy Tumor Multiple sclerosis Encephalitis Intracranial (e.g., subdural or epidural) hematoma Intoxication or other encephalopathy Conversion disorder









7 Options for Patients Experiencing an Ischemic Stroke IV tpa Gold-standard in ischemic stroke care. Drug is designed to break apart the clot. Bridging Therapy Endovascular Clot Removal Mechanical disruption or removal of the clot using standard endovascular approaches Medical Management Monitor vitals and provide secondary stroke prevention.
8 Meta-analysis Shows a Strong Correlation Between Revascularization and Good Patient Outcomes 70% 60% 50% 40% 30% 20% 10% 0% 58.1% 24.8% Good Outcome (mrs 0-2) Revascularized 41.6% 14.4% 13.7% 90-Day Mortality SICH Non-revascularized 12.5% * *Differences in sich were not statistically significant between the revascularized and non-revascularized groups Rha JH, Saver JL. The impact of recanalization on ischemic stroke outcome: a meta-analysis. Stroke Mar;38(3):
9 IV tpa, the Gold Standard Systemic Clot Buster FDA Approved for the treatment of AIS in 1996 Only 8% of ischemic stroke patients are eligible for IV tpa Narrow time window Risk of cerebral and systemic hemorrhage *Non FDA-Approved Therapies Achieves early reperfusion in only 13-50% of large vessel occlusions National Institute of Neurological Disorders and Stroke rt-pa Stroke Study Group. Tissue plasminogen activator for acute ischemic stroke. N Engl J Med. 1995;333: Emergency department arrival times after acute ischemic stroke during the 1990s. Neurocrit Care. 2007;7(1):31-5. Recombinant tissue plasminogen activator in acute thrombotic and embolic stroke. Ann Neurol 1992;32: Low rates of acute recanalization with intravenous recombinant tissue plasminogen activator in ischemic stroke: realworld experience and a call for action. Stroke 2010;41:
10 Treatment window Treatment within the first 3 hours only IV t-pa Treatment within the first 4.5 hours IV t-pa
11 Number of patients who benefit and are harmed per 100 patients treated with t-pa in each time window Lansberg M G et al. Stroke 2009;40:
12 t-pa For Acute Stroke Contraindications Suspected SAH Recent significant head trauma (3 mos) or stroke (3 mos) Recent intracranial or intraspinal surgery History of intracranial hemorrhage Heparin w/in 48 hrs and elevated PTT INR > 1.7 PLT count <100,000 Direct thrombin inhibitor or direct factor Xa inhibitor within 2 days Glucose < 50mg/dL Intracranial neoplasm, AVM or aneurysm Uncontrolled hypertension (>185/110) Multilobar hypodensity on CT (> 1/3 hemisphere) Active internal bleeding Arterial puncture at non-compressible site in previous 7 days Relative exclusion criteria Only mild or rapidly improving symptoms Seizure with postictal impairment Pregnancy Major surgery or serious trauma within previous 14 days Recent GI or GU bleed (within 21 days) Recent MI (within 3 mos) Jauch et al. Stroke 2013;44
13 Selected, Updated tpa Guidelines (Class IIb; LOE C) Treatment of patients with non-disabling symptoms w/in 3 hours may be considered Treatment of moderate to severe stroke in pregnancy may be considered Treatment of carefully selected patients who have undergone major surgery w/in 14 days may be considered Treatment of selected patients with recent trauma (<14 days) may be carefully considered Treatment of patients with aneurysms <10mm is reasonable Treatment of patients with severe stroke and unruptured AVM may be considered Demaerschalk et al. Stroke

14





15 Goal of treatment 60 yo female Presentation NIHSS = 18 Puncture ~ 5 hours from LKN TICI 3 in 31 minutes Discharge NIHSS = 0 home



16 Goal of treatment 2 74 yo male Presentation NIHSS = 22 Puncture ~ 15 hours from LKN TICI 3 in 20 minutes Discharge NIHSS = 2 rehab
17 Selected 2015 Endovascular Guidelines Criteria for endovascular therapy with a stent retriever (Class I; Level of Evidence A) Prestroke mrs score 0 to 1 Receiving tpa within 4.5 hrs Causative occlusion of ICA or proximal MCA (M1) 18 yrs of age NIHSS 6 ASPECTS 6 Treatment initiated within 6 hrs of symptom onset Effectiveness of treatment beyond 6 hrs is uncertain (Class IIb; Level of Evidence C) Powers et al. Stroke
18 Selected 2015 Endovascular Guidelines Endovascular therapy within 6 hrs in carefully selected patients with contraindications to tpa is reasonable; inadequate data to determine efficacy (Class IIb; Level of Evidence C) Treatment within 6 hours of patients with M2 or M3, ACA, VA, basilar, or PCA is reasonable although benefits uncertain (Class IIb; Level of Evidence C) Powers et al. Stroke
19 Challenges in acute stroke care Intravenous thrombolysis reduces long-term disability and is cost-effective in acute ischemic stroke (AIS) Intravenous thrombolysis must be delivered within a narrow time window in order for the treatment to be effective Lack of stroke specialists and lack of access to endovascular revascularization therapies, especially in rural areas, account for low utilization of intravenous thrombolysis Rate of intravenous thrombolysis is < 5% of AIS cases
20 POSSIBLE SOLUTION? Telestroke

21 The dawn of telestroke 21

22 The dawn of telestroke 22

23 The dawn of telestroke 23

24 The dawn of telestroke 24
25 Telemedicine Defined as the use of telecommunications technologies to provide medical information and services First reported to be used for stroke in early 1990 s Term telestroke first used in 1999
26 Telestroke Interactive videoconferencing by bidirecitonal audiovisual systems Characterized by dedicated, high-quality, interactive equipment Coupled with the use of teleradiology for remote review of brain images Allows for patient and/or family and both the bedside and distant healthcare provider to see and hear each other in full color
27 Quality requirements > 20 frames per second of bidirectional synchronized audio and video at a resolution capable of being displayed on monitors of 13 Teleradiology is the ability to obtain radiographic images at 1 location and transmit them remotely to another location for diagnostic and consultative purposes Stroke Jul;40(7): doi: /STROKEAHA Epub 2009 May 7.
28 Telestroke advantages Helps solve shortage of neurologists and radiologists Allows hospitals to become acute stroke ready Enhances stroke diagnosis Increases IV thrombolysis administration rates Overcomes geographic barriers to acute stroke care Improves long-term outcomes A study published in 2011 found that hub-and-spoke telestroke networks were cost-effective in the long term from a societal perspective Source: Nelson RE, Saltzmann GM, Skalabrin EJ, Demaerschalk BM, Majersik JJ, The cost-effectiveness of telestroke in the treatment of acute ischemic stroke. Neurology. 2011; 77:
29 Telestroke models Hub-and-spoke model Hub Usually a Comprehensive Stroke Center = Primary Stroke Center with advanced neurological capabilities 24 x 7 support with in-house neurology providers Spoke 1 Typically smaller hospitals with less extensive neurology coverage Underserved hospitals in rural or sub-urban areas Third party provider Spoke hospital contracts with a third party provider for neurologist coverage Third-party provider employs neurologists to be on call to provide telestroke services 2 Spoke hospitals transfer more complicated patients to a tertiary hospital 2 1. Demaerschalk BM, Miley ML, Kiernan T-EJ, et al; for STARR Coinvestigators. Stroke telemedicine. Mayo Clin Proc. 2009;84: Massaro L, Morrison K. An overview of telestroke models: what's right for your hospital. April 6, 2015.

30 Telestroke Models Gisele S. Silva et al. Stroke. 2012;43:
31 Patient flow in hub & spoke network Hub No changes in patient flow Spoke Fewer patients transferred out More patients receiving IV thrombolysis and/or endovascular therapy Research study conducted in 2012 assessed costeffectiveness of telestroke networks from individual hospitals perspectives Study population Telestroke network with 1 hub and 7 spoke hospitals Total of 1,112 unique AIS patients presenting to the emergency departments in the network hospitals per year Clinical outcomes About 114 fewer AIS patients would be admitted to the hub hospital each year, whereas approximately 16 more patients would be admitted to each spoke hospital compared with a no network setting 45 more patients would be treated with IV thrombolysis & 20 more with endovascular stroke therapy in a telestroke network per year Switzer JA, Demaerschalk BM, Xie J, Fan L, Villa KF, Wu EQ. Cost-effectiveness of hub-and-spoke telestroke networks for the management of acute ischemic stroke from the hospitals perspectives. Circ Cardiovasc Qual Outcomes. 2013;6:18-26.
32 Barriers to telestroke Infrastructure funding Regulatory changes to promote development of acute stroke-capable or PSC s Reimbursement for services Promoting physician adoption and participation Physician licensure and credentialing Technology assessment and deployment Medical liability Compliance with privacy and security laws
33 Best practices A program leader to champion the effort Support from emergency departments (ED) at spoke hospitals 20 On-site visits between hub leaders and spoke sites Standardized protocols at all sites throughout the network (hub and spoke) Availability of Activase Personnel trained in Activase administration Spoke hospital training Transfer agreements in place Ongoing educational planning for hub and spoke personnel Schwamm LH, Audebert HJ, Amarenco P, et al. Recommendations for the implementation of telemedicine within stroke systems of care: a policy statement from the American Heart Association. Stroke. 2009;40:
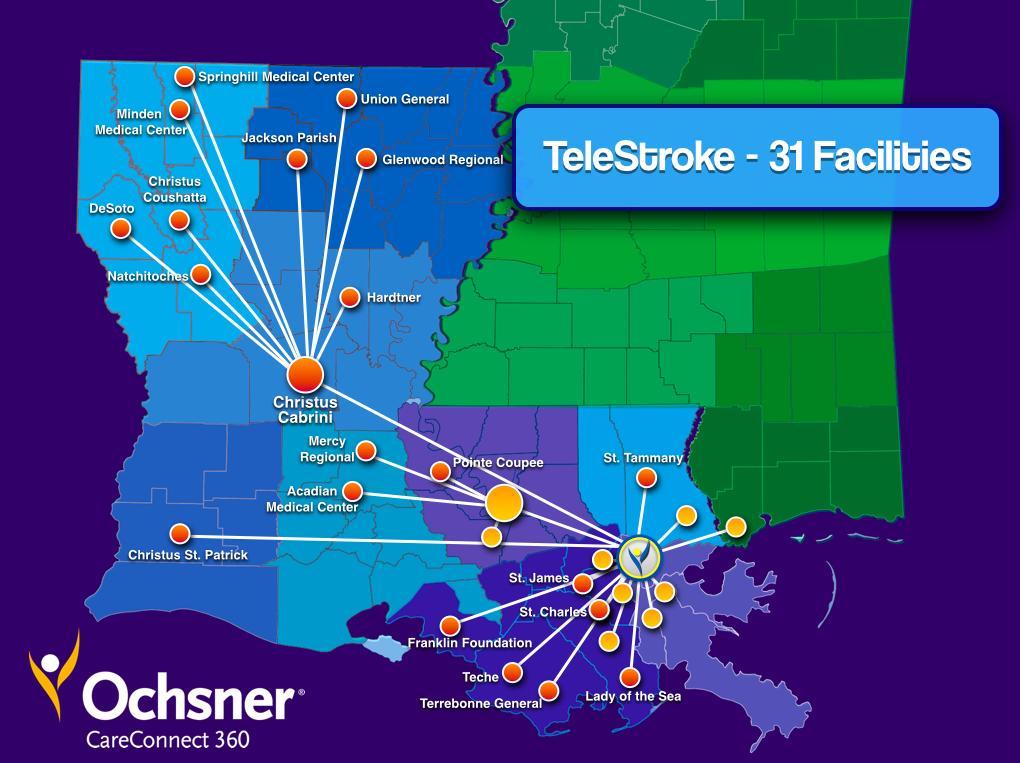
34 ASSERT: Acute Stroke System for Emergent Regional Telestroke Ochsner Tele-stroke Network
35

36

 15% 153 doses in")
 15% 216 doses in")
37 Ochsner telestroke numbers Total # TPA administrations (as of ) doses in doses in 2012 (842 consults) 15% 153 doses in 2013 (956 consults) 16% 190 doses in 2014 (1267 consults) 15% 216 doses in 2015 (1817 consults) 12%
38 2015 TeleStroke Consult Volume O T H E R T R A N S I E N T I S C H E M I C A T T A C K M I M I C T O T A L C O N S U L T S 875 A C U T E I S C H E M I C S TR O K E I N T R A C E R E B R A L H E M O R R H A G E 18 M PAGE 38


39 TeleStroke Network Outcomes Reporting period: August 2009 March 2016 Total consults: 6,254 Diagnosis of AIS: 3,178


40 Disposition by Hospital Type 70% of Patients Stay Local 90% 80% 70% 60% 64% 77% 89% 50% 40% 75% 30% 20% 35% 10% 0% 0% Pre-Telestroke Post-Telestroke

41 Increase in use of tpa 60% 40% 20% 0% HS1 HS2 HS3 HS4 (CAH) HS5 HS6 HUB CH1 CH2 CH3 CAH1 6 mos Prior Most Recent 6 months CAH2 CAH3 CAH4
42 ASSERT Telestroke Network 31 sites currently Projected 45 sites by late total telemedicine consults in 2015 IV tpa initiations in 216 patients in total doses initiated by our team Site expansion: Mississippi & Alabama Future proposed sites: Saudi Arabia & Caribbean Transfer rate ~30%
43 Transfers to OMC Goal: Patients stay local when possible Goal: Make appropriate level of care available for all stroke related patients Who is transferred to OMC-NOLA? Critical care patients High complexity Endovascular candidates How are patients transferred? Distance and weather dependent Ochsner Flight Care (helicopter/fixed wing) Critical Care ground transport
44 Summary Telestroke can satisfy requirements for around-the-clock acute stroke coverage and allow for highly efficient dissemination of expertise to neighboring and distant communities for acute stroke treatment and education
45 Benefits of telestroke Optimization of the use of IV rtpa Decrease in time to initiate IV rtpa Providing treatment with similar safety as Primary Stroke Centers Immediate access to specialty consultation Reliable neurologic exams and NIHSS scores High use rates of IV rtpa without increase in complications or hemorrhages
Disclosures. Outline. Updated Recommendations for Using Alteplase (TPA) in Acute Ischemic Stroke
 in Acute Ischemic Stroke") Updated Recommendations for Using Alteplase (TPA) in Acute Ischemic Stroke Mark J. Alberts, MD, FAHA Chief of Neurology Hartford Hospital Hartford, CT Disclosures Dr. Alberts is a speaker and consultant
Updated Recommendations for Using Alteplase (TPA) in Acute Ischemic Stroke Mark J. Alberts, MD, FAHA Chief of Neurology Hartford Hospital Hartford, CT Disclosures Dr. Alberts is a speaker and consultant
GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE
 2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
Acute brain vessel thrombectomie: when? Why? How?
 Acute brain vessel thrombectomie: when? Why? How? Didier Payen, MD, Ph D Université Paris 7 Département Anesthesiologie-Réanimation Univ Paris 7; Unité INSERM 1160 Hôpital Lariboisière AP-HParis current
Acute brain vessel thrombectomie: when? Why? How? Didier Payen, MD, Ph D Université Paris 7 Département Anesthesiologie-Réanimation Univ Paris 7; Unité INSERM 1160 Hôpital Lariboisière AP-HParis current
Acute Stroke Protocols Modified- What s New in 2013
 Acute Stroke Protocols Modified- What s New in 2013 KUMAR RAJAMANI, MD, DM. Vascular Neurologist-MSN Associate Professor of Neurology WSU School of Medicine. Saturday, September 21, 2013 Crystal Mountain
Acute Stroke Protocols Modified- What s New in 2013 KUMAR RAJAMANI, MD, DM. Vascular Neurologist-MSN Associate Professor of Neurology WSU School of Medicine. Saturday, September 21, 2013 Crystal Mountain
ACUTE ISCHEMIC STROKE. Current Treatment Approaches for Acute Ischemic Stroke
 ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
ACUTE ISCHEMIC STROKE Current Treatment Approaches for Acute Ischemic Stroke EARLY MANAGEMENT OF ACUTE ISCHEMIC STROKE Rapid identification of a stroke Immediate EMS transport to nearest stroke center
Stroke Clinical Trials Update Transitioning to an Anatomic Diagnosis in Ischemic Stroke
 Stroke Clinical Trials Update Transitioning to an Anatomic Diagnosis in Ischemic Stroke Alexander A. Khalessi MD MS Director of Endovascular Neurosurgery Surgical Director of NeuroCritical Care University
Stroke Clinical Trials Update Transitioning to an Anatomic Diagnosis in Ischemic Stroke Alexander A. Khalessi MD MS Director of Endovascular Neurosurgery Surgical Director of NeuroCritical Care University
Unclogging The Pipes. Zahraa Rabeeah MD Chief Resident February 9,2018
 Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
Unclogging The Pipes Zahraa Rabeeah MD Chief Resident February 9,2018 Please join Polleverywhere by texting: ZRABEEAH894 to 37607 Disclosures None Objectives Delineate the differences between TPA vs thrombectomy
ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist
 ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist Pharmacy Grand Rounds 26 July 2016 2015 MFMER slide-1 Learning
ENCHANTED Era: Is it time to rethink treatment of acute ischemic stroke? Kristin J. Scherber, PharmD, BCPS Emergency Medicine Clinical Pharmacist Pharmacy Grand Rounds 26 July 2016 2015 MFMER slide-1 Learning
Update on Early Acute Ischemic Stroke Interventions
 Update on Early Acute Ischemic Stroke Interventions Diana Goodman MD Lead Neurohospitalist Maine Medical Center Assistant Professor of Neurology, Tufts University School of Medicine I have no disclosures
Update on Early Acute Ischemic Stroke Interventions Diana Goodman MD Lead Neurohospitalist Maine Medical Center Assistant Professor of Neurology, Tufts University School of Medicine I have no disclosures
Disclosure. Advances in Interventional Neurology. Disclosure. Natural History of Disease 3/15/2018. Vishal B. Jani MD
 Advances in Interventional Neurology Disclosure Vishal B. Jani MD Medical Director Vascular Neurology Consultant Interventional Neurology CHI Health Assistant Professor, Creighton University School of
Advances in Interventional Neurology Disclosure Vishal B. Jani MD Medical Director Vascular Neurology Consultant Interventional Neurology CHI Health Assistant Professor, Creighton University School of
Endovascular Treatment for Acute Ischemic Stroke
 ular Treatment for Acute Ischemic Stroke Vishal B. Jani MD Assistant Professor Interventional Neurology, Division of Department of Neurology. Creighton University/ CHI health Omaha NE Disclosure None 1
ular Treatment for Acute Ischemic Stroke Vishal B. Jani MD Assistant Professor Interventional Neurology, Division of Department of Neurology. Creighton University/ CHI health Omaha NE Disclosure None 1
Emergency Department Management of Acute Ischemic Stroke
 Emergency Department Management of Acute Ischemic Stroke R. Jason Thurman, MD Associate Professor of Emergency Medicine and Neurosurgery Associate Director, Vanderbilt Stroke Center Vanderbilt University,
Emergency Department Management of Acute Ischemic Stroke R. Jason Thurman, MD Associate Professor of Emergency Medicine and Neurosurgery Associate Director, Vanderbilt Stroke Center Vanderbilt University,
Interventional Stroke Treatment
 Interventional Stroke Treatment Vishal B. Jani MD Medical Director Vascular Neurology Consultant Interventional Neurology CHI Health Assistant Professor, Creighton University School of Medicine Omaha,
Interventional Stroke Treatment Vishal B. Jani MD Medical Director Vascular Neurology Consultant Interventional Neurology CHI Health Assistant Professor, Creighton University School of Medicine Omaha,
Door to Needle Time: Gold Standard of Stroke Treatment Fatima Milfred, MD. Virginia Mason Medical Center March 16, 2018
 Door to Needle Time: Gold Standard of Stroke Treatment Fatima Milfred, MD Virginia Mason Medical Center March 16, 2018 2016 Virginia Mason Medical Center No disclosure 2016 Virginia Mason Medical Center
Door to Needle Time: Gold Standard of Stroke Treatment Fatima Milfred, MD Virginia Mason Medical Center March 16, 2018 2016 Virginia Mason Medical Center No disclosure 2016 Virginia Mason Medical Center
Endovascular Treatment Updates in Stroke Care
 Endovascular Treatment Updates in Stroke Care Autumn Graham, MD April 6-10, 2017 Phoenix, AZ Endovascular Treatment Updates in Stroke Care Autumn Graham, MD Associate Professor of Clinical Emergency Medicine
Endovascular Treatment Updates in Stroke Care Autumn Graham, MD April 6-10, 2017 Phoenix, AZ Endovascular Treatment Updates in Stroke Care Autumn Graham, MD Associate Professor of Clinical Emergency Medicine
Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข
 Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข Emergency start at community level: Prehospital care Acute stroke
Updated Ischemic Stroke Guidelines นพ.ส ชาต หาญไชยพ บ ลย ก ล นายแพทย ทรงค ณว ฒ สาขาประสาทว ทยา สถาบ นประสาทว ทยา กรมการแพทย กระทรวงสาธารณส ข Emergency start at community level: Prehospital care Acute stroke
Primary Stroke Center Acute Stroke Transfer Guidelines When to Consider a Transfer:
 When to Consider a Transfer: Hemorrhagic Stroke Large volume intracerebral hematoma greater than 5cm on CT Concern for expanding hematoma Rapidly declining mental status, especially requiring intubation
When to Consider a Transfer: Hemorrhagic Stroke Large volume intracerebral hematoma greater than 5cm on CT Concern for expanding hematoma Rapidly declining mental status, especially requiring intubation
Stroke, Stroke, Stroke Where Do We Stop on the River? Comprehensive vs. Primary Stroke Centers
 Stroke, Stroke, Stroke Where Do We Stop on the River? Comprehensive vs. Primary Stroke Centers Peter D. Panagos, MD, FAHA, FACEP Departments of Neurology and Emergency Medicine Washington University School
Stroke, Stroke, Stroke Where Do We Stop on the River? Comprehensive vs. Primary Stroke Centers Peter D. Panagos, MD, FAHA, FACEP Departments of Neurology and Emergency Medicine Washington University School
Neurology Telemedicine Systems. Telestroke: Expanding the Reach of Coordinated Stroke Care CAHP. October 16, 2012
 Neurology Telemedicine Systems Telestroke: Expanding the Reach of Coordinated Stroke Care CAHP October 16, 2012 Bart M. Demaerschalk, MD, MSc, FRCP(C) Professor of Neurology Director, Cerebrovascular Diseases
Neurology Telemedicine Systems Telestroke: Expanding the Reach of Coordinated Stroke Care CAHP October 16, 2012 Bart M. Demaerschalk, MD, MSc, FRCP(C) Professor of Neurology Director, Cerebrovascular Diseases
Practical Considerations in the Early Treatment of Acute Stroke
 Practical Considerations in the Early Treatment of Acute Stroke Matthew E. Fink, MD Neurologist-in-Chief Weill Cornell Medical College New York-Presbyterian Hospital mfink@med.cornell.edu Disclosures Consultant
Practical Considerations in the Early Treatment of Acute Stroke Matthew E. Fink, MD Neurologist-in-Chief Weill Cornell Medical College New York-Presbyterian Hospital mfink@med.cornell.edu Disclosures Consultant
Stroke Update. Lacunar 19% Thromboembolic 6% SAH 13% ICH 13% Unknown 32% Hemorrhagic 26% Ischemic 71% Other 3% Cardioembolic 14%
 Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Stroke Update Michel Torbey, MD, MPH, FAHA, FNCS Medical Director, Neurovascular Stroke Center Professor Department of Neurology and Neurosurgery The Ohio State University Wexner Medical Center Objectives
Updated tpa Guidelines: Expanding the opportunity for good outcomes. Benjamin Morrow, MSN RN UPMC Stroke Institute
 Updated tpa Guidelines: Expanding the opportunity for good outcomes Benjamin Morrow, MSN RN UPMC Stroke Institute 1 Outline History Current State Review Exclusions: Minor stroke symptoms Severe strokes
Updated tpa Guidelines: Expanding the opportunity for good outcomes Benjamin Morrow, MSN RN UPMC Stroke Institute 1 Outline History Current State Review Exclusions: Minor stroke symptoms Severe strokes
Comparison of Five Major Recent Endovascular Treatment Trials
 Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
11/1/2018. Disclosure. Imaging in Acute Ischemic Stroke 2018 Neuro Symposium. Is NCCT good enough? Keystone Heart Consultant, Stock Options
 Disclosure Imaging in Acute Ischemic Stroke 2018 Neuro Symposium Keystone Heart Consultant, Stock Options Kevin Abrams, M.D. Chief of Radiology Medical Director of Neuroradiology Baptist Hospital, Miami,
Disclosure Imaging in Acute Ischemic Stroke 2018 Neuro Symposium Keystone Heart Consultant, Stock Options Kevin Abrams, M.D. Chief of Radiology Medical Director of Neuroradiology Baptist Hospital, Miami,
The Importance of Stroke Programs in an Acute Care Setting by Debbie Estes, RN, BSN Stroke Program Coordinator, Medical City of Dallas
 The Importance of Stroke Programs in an Acute Care Setting by Debbie Estes, RN, BSN Stroke Program Coordinator, Medical City of Dallas Objectives Describe the road to the gold Discuss the importance of
The Importance of Stroke Programs in an Acute Care Setting by Debbie Estes, RN, BSN Stroke Program Coordinator, Medical City of Dallas Objectives Describe the road to the gold Discuss the importance of
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS. ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS
 FOR THROMBOLYSIS") NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS I. Purpose : A. To reduce morbidity and mortality associated
NURSING DEPARTMENT CRITICAL CARE POLICY MANUAL CRITICAL CARE PROTOCOLS ACUTE CEREBROVASCULAR ACCIDENT TPA (ACTIVASE /alteplase) FOR THROMBOLYSIS I. Purpose : A. To reduce morbidity and mortality associated
ENDOVASCULAR THERAPIES FOR ACUTE STROKE
 ENDOVASCULAR THERAPIES FOR ACUTE STROKE Cerebral Arteriogram Cerebral Anatomy Cerebral Anatomy Brain Imaging Acute Ischemic Stroke (AIS) Therapy Main goal is to restore blood flow and improve perfusion
ENDOVASCULAR THERAPIES FOR ACUTE STROKE Cerebral Arteriogram Cerebral Anatomy Cerebral Anatomy Brain Imaging Acute Ischemic Stroke (AIS) Therapy Main goal is to restore blood flow and improve perfusion
Mechanical thrombectomy in Plymouth. Will Adams. Will Adams
 Mechanical thrombectomy in Plymouth Will Adams Will Adams History Intra-arterial intervention 1995 (NINDS) iv tpa improved clinical outcome in patients treated within 3 hours of ictus but limited recanalisation
Mechanical thrombectomy in Plymouth Will Adams Will Adams History Intra-arterial intervention 1995 (NINDS) iv tpa improved clinical outcome in patients treated within 3 hours of ictus but limited recanalisation
The DAWN of a New Era for Wake-up Stroke
 The DAWN of a New Era for Wake-up Stroke Alan H. Yee, D.O. Stroke and Critical Care Neurology Department of Neurology University of California Davis Medical Center Objectives Review Epidemiology and Natural
The DAWN of a New Era for Wake-up Stroke Alan H. Yee, D.O. Stroke and Critical Care Neurology Department of Neurology University of California Davis Medical Center Objectives Review Epidemiology and Natural
Antithrombotics: Percent of patients with an ischemic stroke or TIA prescribed antithrombotic therapy at discharge. Corresponding
 Get With The Guidelines -Stroke is the American Heart Association s collaborative performance improvement program, demonstrated to improve adherence to evidence-based care of patients hospitalized with
Get With The Guidelines -Stroke is the American Heart Association s collaborative performance improvement program, demonstrated to improve adherence to evidence-based care of patients hospitalized with
EVOLUTION IN SYSTEMS OF STROKE CARE RIDWAN LIN, MD, PHD STROKE & INTERVENTIONAL NEUROLOGY BROWARD HEALTH
 EVOLUTION IN SYSTEMS OF STROKE CARE RIDWAN LIN, MD, PHD STROKE & INTERVENTIONAL NEUROLOGY BROWARD HEALTH STROKE SYSTEMS OF CARE: 7. Secondary prevention 1. Primary prevention Patient 3. Emergency transport
EVOLUTION IN SYSTEMS OF STROKE CARE RIDWAN LIN, MD, PHD STROKE & INTERVENTIONAL NEUROLOGY BROWARD HEALTH STROKE SYSTEMS OF CARE: 7. Secondary prevention 1. Primary prevention Patient 3. Emergency transport
Rural emergency department best practice for treatment of acute ischemic stroke
 Rural emergency department best practice for treatment of acute ischemic stroke Aubrey J. Hoye, DO Ministry Howard Young Medical Center, Woodruff, WI Ministry Eagle River Memorial Hospital, Eagle River,
Rural emergency department best practice for treatment of acute ischemic stroke Aubrey J. Hoye, DO Ministry Howard Young Medical Center, Woodruff, WI Ministry Eagle River Memorial Hospital, Eagle River,
Endovascular Treatment of Ischemic Stroke
 Endovascular Treatment of Ischemic Stroke William Thorell, MD Associate Professor Neurosurgery UNMC Co-Director Stroke and Neurovascular Center Nebraska Medicine Overview Definitions of terms Review basic
Endovascular Treatment of Ischemic Stroke William Thorell, MD Associate Professor Neurosurgery UNMC Co-Director Stroke and Neurovascular Center Nebraska Medicine Overview Definitions of terms Review basic
Intravenous thrombolysis State of Art. Carlos A. Molina Stroke Unit. Hospital Vall d Hebron Barcelona
 Intravenous thrombolysis State of Art Carlos A. Molina Stroke Unit. Hospital Vall d Hebron Barcelona Independent predictors of good outcome after iv tpa Factor SE OR(95%CI) p Constant 0.467(0.69) Recanalization
Intravenous thrombolysis State of Art Carlos A. Molina Stroke Unit. Hospital Vall d Hebron Barcelona Independent predictors of good outcome after iv tpa Factor SE OR(95%CI) p Constant 0.467(0.69) Recanalization
Code Stroke Intervention: Endovascular Therapies for Stroke J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY
 Code Stroke Intervention: Endovascular Therapies for Stroke J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY Disclosures None Part A. Objectives Epidemiology of AIS and of ELVO Concept: Acute Ischemic
Code Stroke Intervention: Endovascular Therapies for Stroke J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY Disclosures None Part A. Objectives Epidemiology of AIS and of ELVO Concept: Acute Ischemic
Advances in Neuro-Endovascular Care for Acute Stroke
 Advances in Neuro-Endovascular Care for Acute Stroke Ciarán J. Powers, MD, PhD, FAANS Associate Professor Program Director Department of Neurological Surgery Surgical Director Comprehensive Stroke Center
Advances in Neuro-Endovascular Care for Acute Stroke Ciarán J. Powers, MD, PhD, FAANS Associate Professor Program Director Department of Neurological Surgery Surgical Director Comprehensive Stroke Center
Stroke Systems of Care Claire Corbett, MMS, NRP Manager of Neurodiagnostics and Stroke Center New Hanover Regional Medical Center. What do we know?
 Stroke Systems of Care Claire Corbett, MMS, NRP Manager of Neurodiagnostics and Stroke Center New Hanover Regional Medical Center What do we know? Stroke: Time is Brain Shorter onset to treatment times
Stroke Systems of Care Claire Corbett, MMS, NRP Manager of Neurodiagnostics and Stroke Center New Hanover Regional Medical Center What do we know? Stroke: Time is Brain Shorter onset to treatment times
Mechanical Endovascular Reperfusion Therapy
 Get With the Guidelines Stroke Mechanical Endovascular Reperfusion Therapy February 1, 2017 Speaker Lee H. Schwamm, MD Executive Vice Chairman and Director of Stroke/TeleStroke Services, Department of
Get With the Guidelines Stroke Mechanical Endovascular Reperfusion Therapy February 1, 2017 Speaker Lee H. Schwamm, MD Executive Vice Chairman and Director of Stroke/TeleStroke Services, Department of
Pathophysiology of stroke
 A practical approach to acute stro ke Dr. Sanjith Aaron, M.D., D.M., Professor, Department of Neurosciences, CMC Vellore Stroke is characterized by an abrupt onset of neurological deficit lasting more
A practical approach to acute stro ke Dr. Sanjith Aaron, M.D., D.M., Professor, Department of Neurosciences, CMC Vellore Stroke is characterized by an abrupt onset of neurological deficit lasting more
ACCESS CENTER:
 ACCESS CENTER: 1-877-367-8855 Emergency Specialty Services: BRAIN ATTACK Criteria: Stroke symptom onset time less than 6 hours Referring Emergency Department Patient Information Data: Time last known normal:
ACCESS CENTER: 1-877-367-8855 Emergency Specialty Services: BRAIN ATTACK Criteria: Stroke symptom onset time less than 6 hours Referring Emergency Department Patient Information Data: Time last known normal:
Acute Stroke Management Conference 2019: Stroke Clinical Vignettes
 Acute Stroke Management Conference 2019: Stroke Clinical Vignettes Cynthia Kenmuir MD PhD Director of Stroke Program, UPMC Altoona Director of Neurointerventional Program, UPMC Altoona 2015 Guideline for
Acute Stroke Management Conference 2019: Stroke Clinical Vignettes Cynthia Kenmuir MD PhD Director of Stroke Program, UPMC Altoona Director of Neurointerventional Program, UPMC Altoona 2015 Guideline for
COMPREHENSIVE SUMMARY OF INSTOR REPORTS
 COMPREHENSIVE SUMMARY OF INSTOR REPORTS Please note that the following chart provides a sampling of INSTOR reports to differentiate this registry s capabilities as a process improvement system. This list
COMPREHENSIVE SUMMARY OF INSTOR REPORTS Please note that the following chart provides a sampling of INSTOR reports to differentiate this registry s capabilities as a process improvement system. This list
Mechanical thrombectomy beyond the 6 hours. Mahmoud Rayes, MD Medical Director, Stroke program Greenville Memorial Hospital
 Mechanical thrombectomy beyond the 6 hours Mahmoud Rayes, MD Medical Director, Stroke program Greenville Memorial Hospital Disclosures None Worldwide statistics 1 IN 6 people will have a stroke at some
Mechanical thrombectomy beyond the 6 hours Mahmoud Rayes, MD Medical Director, Stroke program Greenville Memorial Hospital Disclosures None Worldwide statistics 1 IN 6 people will have a stroke at some
Team Work in Treatment of Acute Ischemic Stroke
 Diagnosis and Treatment in Acute Ischemic stroke July, 15 th 2016. Bach Mai Hospital Team Work in Treatment of Acute Ischemic Stroke Prof. Pham Minh Thong 1 Time is brain Ischemic stroke: big global burden
Diagnosis and Treatment in Acute Ischemic stroke July, 15 th 2016. Bach Mai Hospital Team Work in Treatment of Acute Ischemic Stroke Prof. Pham Minh Thong 1 Time is brain Ischemic stroke: big global burden
Case 1 5/26/2017 ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE
 ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE Rhonda Whiteman Racing Against the Clock Workshop June 1, 2017 Objectives To discuss the hyperacute ischemic stroke management
ENDOVASCULAR MECHANICAL THROMBECTOMY IN PATIENTS WITH ACUTE ISCHEMIC STROKE Rhonda Whiteman Racing Against the Clock Workshop June 1, 2017 Objectives To discuss the hyperacute ischemic stroke management
Interventional Treatment of Stroke
 Interventional Treatment of Stroke Andrew F. Ducruet, MD Barrow Neurological Institute 2018 BNI Stroke Rehab Symposium October 13, 2018 Disclosures Consultant: Medtronic, Penumbra, Cerenovus Lecture Overview
Interventional Treatment of Stroke Andrew F. Ducruet, MD Barrow Neurological Institute 2018 BNI Stroke Rehab Symposium October 13, 2018 Disclosures Consultant: Medtronic, Penumbra, Cerenovus Lecture Overview
Mechanical Thrombectomy of Large Vessel Occlusions Using Stent Retriever Devices
 Mechanical Thrombectomy of Large Vessel Occlusions Using Stent Retriever Devices Joey English MD, PhD Medical Director, Neurointerventional Services California Pacific Medical Center Hospitals, San Francisco,
Mechanical Thrombectomy of Large Vessel Occlusions Using Stent Retriever Devices Joey English MD, PhD Medical Director, Neurointerventional Services California Pacific Medical Center Hospitals, San Francisco,
Stroke Belt Consortium
 Field Triage And Diversion of Acute Stroke Charles Sand, MD Stroke Belt Consortium 10/26/12 WCF EMS Acute Stroke Advisory Committee Formed 2001 5 Original members Now > 100 members interdisciplinary expertise
Field Triage And Diversion of Acute Stroke Charles Sand, MD Stroke Belt Consortium 10/26/12 WCF EMS Acute Stroke Advisory Committee Formed 2001 5 Original members Now > 100 members interdisciplinary expertise
Managing the Measures: A Serious Look at Key Abstraction Concepts for the Comprehensive Stroke (CSTK) Measure Set Session 2
 Measure Set Session 2") Managing the Measures: A Serious Look at Key Abstraction Concepts for the Comprehensive Stroke (CSTK) Measure Set Session 2 January 28, 2015 1 to 3 PM Central Time Continuing Education Credit This course
Managing the Measures: A Serious Look at Key Abstraction Concepts for the Comprehensive Stroke (CSTK) Measure Set Session 2 January 28, 2015 1 to 3 PM Central Time Continuing Education Credit This course
Drano vs. MR CLEAN Review of New Endovascular Therapy for Acute Ischemic Stroke Patients
 Drano vs. MR CLEAN Review of New Endovascular Therapy for Acute Ischemic Stroke Patients Peter Panagos, MD, FACEP, FAHA Associate Professor Emergency Medicine and Neurology Washington University School
Drano vs. MR CLEAN Review of New Endovascular Therapy for Acute Ischemic Stroke Patients Peter Panagos, MD, FACEP, FAHA Associate Professor Emergency Medicine and Neurology Washington University School
Stroke: The First Critical Hour. Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP
 Stroke: The First Critical Hour Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP Disclosures We have no actual or potential conflicts of interest in relation to this presentation. Objectives Discuss
Stroke: The First Critical Hour Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP Disclosures We have no actual or potential conflicts of interest in relation to this presentation. Objectives Discuss
UPDATES IN INTRACRANIAL INTERVENTION Jordan Taylor DO Metro Health Neurology 2015
 UPDATES IN INTRACRANIAL INTERVENTION Jordan Taylor DO Metro Health Neurology 2015 NEW STUDIES FOR 2015 MR CLEAN ESCAPE EXTEND-IA REVASCAT SWIFT PRIME RECOGNIZED LIMITATIONS IV Alteplase proven benefit
UPDATES IN INTRACRANIAL INTERVENTION Jordan Taylor DO Metro Health Neurology 2015 NEW STUDIES FOR 2015 MR CLEAN ESCAPE EXTEND-IA REVASCAT SWIFT PRIME RECOGNIZED LIMITATIONS IV Alteplase proven benefit
Acute Stroke Treatment: Current Trends 2010
 Acute Stroke Treatment: Current Trends 2010 Helmi L. Lutsep, MD Oregon Stroke Center Oregon Health & Science University Overview Ischemic Stroke Neuroprotectant trials to watch for IV tpa longer treatment
Acute Stroke Treatment: Current Trends 2010 Helmi L. Lutsep, MD Oregon Stroke Center Oregon Health & Science University Overview Ischemic Stroke Neuroprotectant trials to watch for IV tpa longer treatment
Emergency Treatment of Ischemic Stroke
 Emergency Treatment of Ischemic Stroke JEFFREY BOYLE, M.D., PHD CLINICAL DIRECTOR OF STROKE AT AVERA MCKENNAN AVERA MEDICAL GROUP NEUROLOGY SIOUX FALLS, SD Conflicts of Interest None I will discuss therapies
Emergency Treatment of Ischemic Stroke JEFFREY BOYLE, M.D., PHD CLINICAL DIRECTOR OF STROKE AT AVERA MCKENNAN AVERA MEDICAL GROUP NEUROLOGY SIOUX FALLS, SD Conflicts of Interest None I will discuss therapies
Stroke in the Rural Setting: How You Can Make A Difference. Susie Fisher, RN, BSN Program Manager Providence Stroke Center Portland, OR
 Stroke in the Rural Setting: How You Can Make A Difference. Susie Fisher, RN, BSN Program Manager Providence Stroke Center Portland, OR Outline State Statistics The Oregon Problem Time & Treatments Steps
Stroke in the Rural Setting: How You Can Make A Difference. Susie Fisher, RN, BSN Program Manager Providence Stroke Center Portland, OR Outline State Statistics The Oregon Problem Time & Treatments Steps
Updates on Endovascular Therapy
 Updates on Endovascular Therapy 5 th Annual Intermountain Stroke Conference October 16, 2017 M. Shazam Hussain, MD, FRCP(C), FAHA Director, Cerebrovascular Center Associate Professor, CCLCM Staff, Vascular
Updates on Endovascular Therapy 5 th Annual Intermountain Stroke Conference October 16, 2017 M. Shazam Hussain, MD, FRCP(C), FAHA Director, Cerebrovascular Center Associate Professor, CCLCM Staff, Vascular
Role of recombinant tissue plasminogen activator in the updated stroke approach
 Role of recombinant tissue plasminogen activator in the updated stroke approach Joshua Z. Willey, MD, MS Assistant Professor of Neurology Division of Stroke, Columbia University October 2015 jzw2@columbia.edu
Role of recombinant tissue plasminogen activator in the updated stroke approach Joshua Z. Willey, MD, MS Assistant Professor of Neurology Division of Stroke, Columbia University October 2015 jzw2@columbia.edu
2018 Early Management of Acute Ischemic Stroke Guidelines Update
 2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
2018 Early Management of Acute Ischemic Stroke Guidelines Update Brandi Bowman, PhC, Pharm.D. April 17, 2018 Pharmacist Objectives Describe the recommendations for emergency medical services and hospital
Primary Stroke Center Quality & Performance Measures
 Primary Stroke Center Quality & Performance Measures This section of the manual contains information related to the quality performance of Primary Stroke Centers. Brain Attack Coalition Definitions Recognition
Primary Stroke Center Quality & Performance Measures This section of the manual contains information related to the quality performance of Primary Stroke Centers. Brain Attack Coalition Definitions Recognition
Table 1. Specific changes to the FDA labeling for recombinant tissue plasminogen activator (Alteplase, Activase, Genentech, inc).
.") Acute Ischemic Stroke Controversies Steven R. Messé, MD, FAAN Associate professor of Neurology, Pereleman School of Medicine at the University of Pennsylvania, Philadelphia, PA Using the term controversy
Acute Ischemic Stroke Controversies Steven R. Messé, MD, FAAN Associate professor of Neurology, Pereleman School of Medicine at the University of Pennsylvania, Philadelphia, PA Using the term controversy
Advancing Stroke Systems of Care to Improve Outcomes Update on Target: Stroke Phase II
 Advancing Stroke Systems of Care to Improve Outcomes Update on Target: Stroke Phase II Gregg C. Fonarow MD, Eric E. Smith MD, MPH, Jeffrey L. Saver MD, Lee H. Schwamm, MD UCLA Division of Cardiology; Department
Advancing Stroke Systems of Care to Improve Outcomes Update on Target: Stroke Phase II Gregg C. Fonarow MD, Eric E. Smith MD, MPH, Jeffrey L. Saver MD, Lee H. Schwamm, MD UCLA Division of Cardiology; Department
Thrombolytic therapy should be the first line treatment in acute ishchemic stroke. We are against it!!
 Thrombolytic therapy should be the first line treatment in acute ishchemic stroke We are against it!! 85% of strokes are ischaemic, and related to blockage of an artery by a blood clot, so potential treatments
Thrombolytic therapy should be the first line treatment in acute ishchemic stroke We are against it!! 85% of strokes are ischaemic, and related to blockage of an artery by a blood clot, so potential treatments
Parameter Optimized Treatment for Acute Ischemic Stroke
 Heart & Stroke Barnett Memorial Lectureship and Visiting Professorship Parameter Optimized Treatment for Acute Ischemic Stroke December 2, 2016, Thunder Bay, Ontario Adnan I. Qureshi MD Professor of Neurology,
Heart & Stroke Barnett Memorial Lectureship and Visiting Professorship Parameter Optimized Treatment for Acute Ischemic Stroke December 2, 2016, Thunder Bay, Ontario Adnan I. Qureshi MD Professor of Neurology,
Ischemic Stroke Therapies: Resource Guide
 Ischemic Stroke Therapies: Resource Guide Ischemic Stroke Therapies Table of Contents Introduction...1 Stroke Protocol Roadmap...2 Public Awareness...3-4 Emergency Medical Services... 5-6 Emergency Department
Ischemic Stroke Therapies: Resource Guide Ischemic Stroke Therapies Table of Contents Introduction...1 Stroke Protocol Roadmap...2 Public Awareness...3-4 Emergency Medical Services... 5-6 Emergency Department
Stroke Treatment Beyond Traditional Time Windows. Rishi Gupta, MD, MBA
 Stroke Treatment Beyond Traditional Time Windows Rishi Gupta, MD, MBA Director, Stroke and Neurocritical Care Endovascular Neurosurgery Wellstar Health System THE PAST THE PRESENT 2015 American Heart Association/American
Stroke Treatment Beyond Traditional Time Windows Rishi Gupta, MD, MBA Director, Stroke and Neurocritical Care Endovascular Neurosurgery Wellstar Health System THE PAST THE PRESENT 2015 American Heart Association/American
ND STROKE Coordinators Case Studies. STEMI and Stroke Conference, Fargo, ND, August 5, 2014
 ND STROKE Coordinators Case Studies STEMI and Stroke Conference, Fargo, ND, August 5, 2014 STROKE Coordinator Case Study Essentia Health, Fargo Essentia Health Stroke Alert Process Within 24 hours of Last
ND STROKE Coordinators Case Studies STEMI and Stroke Conference, Fargo, ND, August 5, 2014 STROKE Coordinator Case Study Essentia Health, Fargo Essentia Health Stroke Alert Process Within 24 hours of Last
Acute Ischemic Stroke Imaging. Ronald L. Wolf, MD, PhD Associate Professor of Radiology
 Acute Ischemic Stroke Imaging Ronald L. Wolf, MD, PhD Associate Professor of Radiology Title of First Slide of Substance An Illustrative Case 2 Disclosures No financial disclosures Off-label uses of some
Acute Ischemic Stroke Imaging Ronald L. Wolf, MD, PhD Associate Professor of Radiology Title of First Slide of Substance An Illustrative Case 2 Disclosures No financial disclosures Off-label uses of some
Protocol for IV rtpa Treatment of Acute Ischemic Stroke
 Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Recent Changes in IV TPA Recommendations. Ashish Masih, M.D Vascular Neurology
 Recent Changes in IV TPA Recommendations Ashish Masih, M.D Vascular Neurology Disclosures none 4 th leading cause of death Nearly 800,000 cases of stroke annually Statistics Leading cause of disability
Recent Changes in IV TPA Recommendations Ashish Masih, M.D Vascular Neurology Disclosures none 4 th leading cause of death Nearly 800,000 cases of stroke annually Statistics Leading cause of disability
Interventional Neuroradiology. & Stroke INR PROCEDURES INR PROCEDURES. Dr Steve Chryssidis. 25-Sep-17. Interventional Neuroradiology
 Interventional Neuroradiology Interventional Neuroradiology & Stroke Dr Steve Chryssidis Interventional Neuroradiology (INR) is a subspecialty within Radiology INR -- broadly defined as treatment by endovascular
Interventional Neuroradiology Interventional Neuroradiology & Stroke Dr Steve Chryssidis Interventional Neuroradiology (INR) is a subspecialty within Radiology INR -- broadly defined as treatment by endovascular
Mark J. Alberts, MD, FAHA, FANA Vice-Chair, Dept of Neurology Professor of Neurology UT Southwestern Medical Center Dallas, TX
 Interventional Therapies for Cerebrovascular Diease: The Good, The Bad, The Needed, and The Few 1 Mark J. Alberts, MD, FAHA, FANA Vice-Chair, Dept of Neurology Professor of Neurology UT Southwestern Medical
Interventional Therapies for Cerebrovascular Diease: The Good, The Bad, The Needed, and The Few 1 Mark J. Alberts, MD, FAHA, FANA Vice-Chair, Dept of Neurology Professor of Neurology UT Southwestern Medical
Stroke Coordinator: ROI. Author: Debbie Roper, RN, MSN (d.r. Stroke) Vice President of Roper Resources, Inc.
 Vice President of Roper Resources, Inc.") Stroke Coordinator: ROI Author: Debbie Roper, RN, MSN (d.r. Stroke) Vice President of Roper Resources, Inc. debbie@roper-resources.com 214-864-8993 Disclosure Debbie Roper is a speaker for: Genentech Activase
Stroke Coordinator: ROI Author: Debbie Roper, RN, MSN (d.r. Stroke) Vice President of Roper Resources, Inc. debbie@roper-resources.com 214-864-8993 Disclosure Debbie Roper is a speaker for: Genentech Activase
framework for flow Objectives Acute Stroke Treatment Collaterals in Acute Ischemic Stroke framework & basis for flow
 Acute Stroke Treatment Collaterals in Acute Ischemic Stroke Objectives role of collaterals in acute ischemic stroke collateral therapeutic strategies David S Liebeskind, MD Professor of Neurology & Director
Acute Stroke Treatment Collaterals in Acute Ischemic Stroke Objectives role of collaterals in acute ischemic stroke collateral therapeutic strategies David S Liebeskind, MD Professor of Neurology & Director
Lessons Learned from IMS III: Implications for the Future
 Lessons Learned from IMS III: Implications for the Future Pooja Khatri, MD, MSc Professor, Dept of Neurology Director of Acute Stroke, UC Stroke Team University of Cincinnati Disclosures Univ of Cincinnati
Lessons Learned from IMS III: Implications for the Future Pooja Khatri, MD, MSc Professor, Dept of Neurology Director of Acute Stroke, UC Stroke Team University of Cincinnati Disclosures Univ of Cincinnati
Stroke Update Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center
 Stroke Update 2015 Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center Objectives 1. Review successes in systems of care approach to acute ischemic stroke
Stroke Update 2015 Elaine J. Skalabrin MD Medical Director and Neurohospitalist Sacred Heart Medical Center Stroke Center Objectives 1. Review successes in systems of care approach to acute ischemic stroke
Stroke Systems of Care
 Comprehensive Stroke and Cerebrovascular Center Stroke Systems of Care Dana Stradling RN MSN CNRN UC Irvine Stroke Manager dstradli@uci.edu Why Stroke Systems? No. 4 th 5 th cause of death in the U.S.
Comprehensive Stroke and Cerebrovascular Center Stroke Systems of Care Dana Stradling RN MSN CNRN UC Irvine Stroke Manager dstradli@uci.edu Why Stroke Systems? No. 4 th 5 th cause of death in the U.S.
Endovascular Treatment for Acute Ischemic Stroke: Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington
 Endovascular Treatment for Acute Ischemic Stroke: Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington Disclosures: SWIFT PRIME site (Medtronic) Physician Proctor
Endovascular Treatment for Acute Ischemic Stroke: Curtis A. Given II, MD Co-Director, Neurointerventional Services Baptist Physician Lexington Disclosures: SWIFT PRIME site (Medtronic) Physician Proctor
Maximising Delivery of Thrombectomy
 Maximising Delivery of Thrombectomy Professor Gary Ford Chief Executive Officer, Oxford Academic Health Science Network Consultant Stroke Physician, Oxford University Hospitals Visiting Professor of Clinical
Maximising Delivery of Thrombectomy Professor Gary Ford Chief Executive Officer, Oxford Academic Health Science Network Consultant Stroke Physician, Oxford University Hospitals Visiting Professor of Clinical
5/31/2018. Interventional Therapies that Expand Time Windows for Acute Ischemic Stroke Treatment. Disclosures. Impact of clot burden
 Good Outcome (%) Rankin 0-2 at 90 days 5/31/2018 Interventional Therapies that Expand Time Windows for Acute Ischemic Stroke Treatment Disclosures Cerenovus: I am on Executive Committee for ARISE2 Trial
Good Outcome (%) Rankin 0-2 at 90 days 5/31/2018 Interventional Therapies that Expand Time Windows for Acute Ischemic Stroke Treatment Disclosures Cerenovus: I am on Executive Committee for ARISE2 Trial
ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS. Justin Nolte, MD Assistant Profession Marshall University School of Medicine
 ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS Justin Nolte, MD Assistant Profession Marshall University School of Medicine History of Presenting Illness 64 yo wf with PMHx of COPD, HTN, HLP who was in
ACUTE STROKE TREATMENT IN LARGE NIHSS PATIENTS Justin Nolte, MD Assistant Profession Marshall University School of Medicine History of Presenting Illness 64 yo wf with PMHx of COPD, HTN, HLP who was in
Acute Stroke Systems of Care Optimizing Patient Care and Improving Outcomes
 Acute Stroke Systems of Care Optimizing Patient Care and Improving Outcomes Laurie Paletz, BSN PHN RN-BC SCRN Cedars-Sinai Medical Center Stroke Program Coordinator Disclosures Speaker s Bureau: Genentech
Acute Stroke Systems of Care Optimizing Patient Care and Improving Outcomes Laurie Paletz, BSN PHN RN-BC SCRN Cedars-Sinai Medical Center Stroke Program Coordinator Disclosures Speaker s Bureau: Genentech
DISCLOSURES OBJECTIVES 11/18/2014. Stroke Network Update. None. Discuss
 Stroke Network Update MOUHAMMAD A. JUMAA MD ASSISTANT PROFESSOR VASCULAR & INTERVENTIONAL NEUROLOGY UNIVERSITY OF TOLEDO DISCLOSURES None OBJECTIVES Discuss Regional stroke systems of care in NW OHIO Evolution
Stroke Network Update MOUHAMMAD A. JUMAA MD ASSISTANT PROFESSOR VASCULAR & INTERVENTIONAL NEUROLOGY UNIVERSITY OF TOLEDO DISCLOSURES None OBJECTIVES Discuss Regional stroke systems of care in NW OHIO Evolution
Code Stroke!! Amit Kansara, MD, FAHA. Joint EMS Conference Providence Brain and Spine Institute Providence Heart and Vascular Institute
 Code Stroke!! Amit Kansara, MD, FAHA Joint EMS Conference Providence Brain and Spine Institute Providence Heart and Vascular Institute February 22, 2019 Patient History: Dispatch 20:45: You are dispatched
Code Stroke!! Amit Kansara, MD, FAHA Joint EMS Conference Providence Brain and Spine Institute Providence Heart and Vascular Institute February 22, 2019 Patient History: Dispatch 20:45: You are dispatched
Imaging Stroke: Is There a Stroke Equivalent of the ECG? Albert J. Yoo, MD Director of Acute Stroke Intervention Massachusetts General Hospital
 Imaging Stroke: Is There a Stroke Equivalent of the ECG? Albert J. Yoo, MD Director of Acute Stroke Intervention Massachusetts General Hospital Disclosures Penumbra, Inc. research grant (significant) for
Imaging Stroke: Is There a Stroke Equivalent of the ECG? Albert J. Yoo, MD Director of Acute Stroke Intervention Massachusetts General Hospital Disclosures Penumbra, Inc. research grant (significant) for
Code Stroke for Hospital Medicine: Clinical Challenges in Inpatient Care
 Code Stroke for Hospital Medicine: Clinical Challenges in Inpatient Care William J. Hicks II, MD Co-Director, Comprehensive Stroke Program Riverside Methodist Hospital Columbus, OH What s the big deal?
Code Stroke for Hospital Medicine: Clinical Challenges in Inpatient Care William J. Hicks II, MD Co-Director, Comprehensive Stroke Program Riverside Methodist Hospital Columbus, OH What s the big deal?
Thrombolytic Therapy in Acute Ischemic Stroke: Time is Brain -How to Move the Needle on Door-to-Needle
 Thrombolytic Therapy in Acute Ischemic Stroke: Time is Brain -How to Move the Needle on Door-to-Needle Alissa Rich, Pharm.D., M.B.A. Robyn Stakley, Pharm.D. Oct. 12, 2017 2 Disclosures The presenters have
Thrombolytic Therapy in Acute Ischemic Stroke: Time is Brain -How to Move the Needle on Door-to-Needle Alissa Rich, Pharm.D., M.B.A. Robyn Stakley, Pharm.D. Oct. 12, 2017 2 Disclosures The presenters have
Moving from a Primary Stroke Center to a Comprehensive Stroke Center
 Moving from a Primary Stroke Center to a Comprehensive Stroke Center MJ Hampel, MPH, MBA The Joint Commission October 19, 2012 Presenter Disclosure Information MJ Hampel Moving from a Primary Stroke Center
Moving from a Primary Stroke Center to a Comprehensive Stroke Center MJ Hampel, MPH, MBA The Joint Commission October 19, 2012 Presenter Disclosure Information MJ Hampel Moving from a Primary Stroke Center
KPNC Stroke EXPRESS EXpediting the PRocess of Evaluating & Stopping Stroke
 KPNC Stroke EXPRESS EXpediting the PRocess of Evaluating & Stopping Stroke Jeffrey G. Klingman, MD 1 Disclosures None 75% DTN < 60 50% DTN < 45 Why should we care about DTN?: Time is brain 2 million nerve
KPNC Stroke EXPRESS EXpediting the PRocess of Evaluating & Stopping Stroke Jeffrey G. Klingman, MD 1 Disclosures None 75% DTN < 60 50% DTN < 45 Why should we care about DTN?: Time is brain 2 million nerve
Sentinel Stroke National Audit Programme (SSNAP) Based on stroke patients admitted to hospital for thrombectomy between April 2016 and March 2017
 Based on stroke patients admitted to hospital for thrombectomy between April 2016 and March 2017") Thrombectomy Sentinel Stroke National Audit Programme (SSNAP) Thrombectomy Report for April 2016 - March 2017 National results July 2017 Based on stroke patients admitted to hospital for between April
Thrombectomy Sentinel Stroke National Audit Programme (SSNAP) Thrombectomy Report for April 2016 - March 2017 National results July 2017 Based on stroke patients admitted to hospital for between April
Thrombectomy with the preset stent-retriever. Insights from the ARTESp* trial
 Thrombectomy with the preset stent-retriever Insights from the ARTESp* trial Wiebke Kurre, MD Klinikum Stuttgart - Germany * Acute Recanalization of Thrombo-Embolic Ischemic Stroke with preset (ARTESp)
Thrombectomy with the preset stent-retriever Insights from the ARTESp* trial Wiebke Kurre, MD Klinikum Stuttgart - Germany * Acute Recanalization of Thrombo-Embolic Ischemic Stroke with preset (ARTESp)
Acute Stroke Identification and Treatment
 Acute Stroke Identification and Treatment James S. McKinney, MD, FAHA Medical Director, NHRMC Stroke Center SE NC is located in the buckle of the Stroke Belt, seeing the highest stroke incidence and mortality
Acute Stroke Identification and Treatment James S. McKinney, MD, FAHA Medical Director, NHRMC Stroke Center SE NC is located in the buckle of the Stroke Belt, seeing the highest stroke incidence and mortality
Canadian Best Practice Recommendations for Stroke Care. (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management
 Section # 3 Section # 3 Hyperacute Stroke Management") Canadian Best Practice Recommendations for Stroke Care (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management Reorganization of Recommendations 2008 2006 RECOMMENDATIONS: 2008 RECOMMENDATIONS:
Canadian Best Practice Recommendations for Stroke Care (Updated 2008) Section # 3 Section # 3 Hyperacute Stroke Management Reorganization of Recommendations 2008 2006 RECOMMENDATIONS: 2008 RECOMMENDATIONS:
Advances in Acute stroke Management
 Advances in Acute stroke Management Sandra Ripper-Brown, DNP Neuroscience Nurse Practitioner St. Mary s Medical Center WPB, FL Palm Beach County Nurse Practitioner Council Annual Conference APRNs: Agents
Advances in Acute stroke Management Sandra Ripper-Brown, DNP Neuroscience Nurse Practitioner St. Mary s Medical Center WPB, FL Palm Beach County Nurse Practitioner Council Annual Conference APRNs: Agents
Building a Stroke Portfolio. June 28, 2018
 Building a Stroke Portfolio June 28, 2018 1 Forward-Looking Statements This presentation contains forward-looking statements, including statements relating to: the potential benefits, safety and efficacy
Building a Stroke Portfolio June 28, 2018 1 Forward-Looking Statements This presentation contains forward-looking statements, including statements relating to: the potential benefits, safety and efficacy
Journal Club. 1. Develop a PICO (Population, Intervention, Comparison, Outcome) question for this study
 question for this study") Journal Club Articles for Discussion Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-pa Stroke Study Group. N Engl J Med. 1995 Dec
Journal Club Articles for Discussion Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-pa Stroke Study Group. N Engl J Med. 1995 Dec
William Barr, M.D. January 28, 2017
 William Barr, M.D. January 28, 2017 Types of Stroke Ischemic Stroke Small vessel (20%) Large vessel (31%) Embolic (32%) Hemorrhagic Intracerebral Hemorrhage (10%) Subarachnoid Hemorrhage (7%) The Majority
William Barr, M.D. January 28, 2017 Types of Stroke Ischemic Stroke Small vessel (20%) Large vessel (31%) Embolic (32%) Hemorrhagic Intracerebral Hemorrhage (10%) Subarachnoid Hemorrhage (7%) The Majority
Broadening the Stroke Window in Light of the DAWN Trial
 Broadening the Stroke Window in Light of the DAWN Trial South Jersey Neurovascular and Stroke Symposium April 26, 2018 Rohan Chitale, MD Assistant Professor of Neurological Surgery Vanderbilt University
Broadening the Stroke Window in Light of the DAWN Trial South Jersey Neurovascular and Stroke Symposium April 26, 2018 Rohan Chitale, MD Assistant Professor of Neurological Surgery Vanderbilt University
Acute stroke update 2016 innovations in managing ischemic and hemorrhagic disease
 Acute stroke update 2016 innovations in managing ischemic and hemorrhagic disease Christopher Koebbe, MD Endovascular Neurosurgeon Florida Spine Institute Director of Neurosciences Northside Hospital Overview
Acute stroke update 2016 innovations in managing ischemic and hemorrhagic disease Christopher Koebbe, MD Endovascular Neurosurgeon Florida Spine Institute Director of Neurosciences Northside Hospital Overview
How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular Clot Retrieval
 How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular Clot Retrieval Peter Howard MD FRCPC Disclosures No conflicts to disclose How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular
How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular Clot Retrieval Peter Howard MD FRCPC Disclosures No conflicts to disclose How to Interpret CT/CTA for Acute Stroke in the Age of Endovascular
Mark J. Alberts, MD. Turning the Wheels of Stroke Care
 Mark J. Alberts, MD Vice-Chair, Clinical Affairs Professor of Neurology Department of Neurology and Neurotherapeutics University of Texas Southwestern Medical Center Dallas, Texas Turning the Wheels of
Mark J. Alberts, MD Vice-Chair, Clinical Affairs Professor of Neurology Department of Neurology and Neurotherapeutics University of Texas Southwestern Medical Center Dallas, Texas Turning the Wheels of