Feasibility of titrating PEEP to minimum elastance for mechanically ventilated patients
|
|
|
- Bonnie Berenice Payne
- 6 years ago
- Views:
Transcription
1 Pilot and Feasibility Studies This Provisional PDF corresponds to the article as it appeared upon acceptance. Fully formatted PDF and full text (HTML) versions will be made available soon. Feasibility of titrating PEEP to minimum elastance for mechanically ventilated patients Pilot and Feasibility Studies Sample (2015) 1:9 doi: /s Yeong Shiong Chiew Christopher G Pretty (chris.pretty@canterbury.ac.nz) Geoffrey M Shaw (geoff.shaw@cdhb.health.nz) Yeong Woei Chiew (cyeongwoei@yahoo.com) Bernard Lambermont (b.lambermont@chu.ulg.ac.be) Thomas Desaive (tdesaive@ulg.ac.be) J Geoffrey Chase (geoff.chase@canterbury.ac.nz) Sample ISSN Article type Research Submission date 1 October 2014 Acceptance date 26 February 2015 Article URL For information about publishing your research in BioMed Central journals, go to Chiew et al.; licensee BioMed Central. This is an Open Access article distributed under the terms of the Creative Commons Attribution License ( which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly credited. The Creative Commons Public Domain Dedication waiver ( applies to the data made available in this article, unless otherwise stated.
2 Feasibility of titrating PEEP to minimum elastance for mechanically ventilated patients Yeong Shiong Chiew 1* * Corresponding author yeongshiong.chiew@canterbury.ac.nz Christopher G Pretty 1 chris.pretty@canterbury.ac.nz Geoffrey M Shaw 2 geoff.shaw@cdhb.health.nz Yeong Woei Chiew 3 cyeongwoei@yahoo.com Bernard Lambermont 4 b.lambermont@chu.ulg.ac.be Thomas Desaive 4 tdesaive@ulg.ac.be J Geoffrey Chase 1 geoff.chase@canterbury.ac.nz 1 Department of Mechanical Engineering, University of Canterbury, Private Bag, 8140 Christchurch, New Zealand 2 Department of Intensive Care, Christchurch Hospital, Christchurch, New Zealand 3 Western Medicine Division, Hospital Lam Hua EE, Pulau Penang, Malaysia 4 GIGA Cardiovascular Science, University of Liege, Liege, Belgium Abstract Background Selecting positive end-expiratory pressure (PEEP) during mechanical ventilation is important, as it can influence disease progression and outcome of acute respiratory distress syndrome (ARDS) patients. However, there are no well-established methods for optimizing PEEP selection due to the heterogeneity of ARDS. This research investigates the viability of titrating PEEP to minimum elastance for mechanically ventilated ARDS patients.
3 Methods Ten mechanically ventilated ARDS patients from the Christchurch Hospital Intensive Care Unit were included in this study. Each patient underwent a stepwise PEEP recruitment manoeuvre. Airway pressure and flow data were recorded using a pneumotachometer. Patient-specific respiratory elastance (E rs ) and dynamic functional residual capacity (dfrc) at each PEEP level were calculated and compared. Optimal PEEP for each patient was identified by finding the minima of the PEEP-E rs profile. Results Median E rs and dfrc over all patients and PEEP values were 32.2 cmh 2 O/l [interquartile range (IQR) ] and 0.42 l [IQR ]. These wide ranges reflect patient heterogeneity and variable response to PEEP. The level of PEEP associated with minimum E rs corresponds to a high change of functional residual capacity, representing the balance between recruitment and minimizing the risk of overdistension. Conclusions Monitoring patient-specific E rs can provide clinical insight to patient-specific condition and response to PEEP settings. The level of PEEP associated with minimum-e rs can be identified for each patient using a stepwise PEEP recruitment manoeuvre. This minimum elastance PEEP may represent a patient-specific optimal setting during mechanical ventilation. Trial registration Australian New Zealand Clinical Trials Registry: ACTRN Keywords ARDS, Respiratory elastance, Dynamic functional residual capacity, PEEP, Mechanical ventilation Background Mechanical ventilation (MV) is used in the intensive care unit (ICU) to support the breathing of patients with respiratory failure. MV has evolved from a supporting role to a therapy that affects disease progression and outcome [1-5]. Hence, it is important to have optimal MV management to support patient recovery [5-7]. Positive end-expiratory pressure (PEEP) is one of the important MV settings for patients with acute respiratory distress syndrome (ARDS) [8-10]. PEEP keeps alveoli open and maintains recruitment [11,12]. Several attempts have been made to standardize MV therapy, especially PEEP selection [13-17]. However, these approaches were generalized from large population studies and did not consider intra-patient variability and inter-patient heterogeneity of ARDS. Thus, there is currently no conclusive result on PEEP selection [7,18-21]. Without a standard method for setting patient-specific PEEP, clinicians rely on intuition, experience and/ or
4 methods based on consensus guidelines or cohort-based outcomes [22], leading to more variable care and outcomes. Studies by Suter et al. [23,24] have suggested that patient-specific PEEP selected at maximum compliance (or minimum elastance, where elastance = 1 / compliance) may be beneficial. Similarly, recent animal studies have shown that optimal PEEP can be titrated to minimum respiratory elastance [25-27]. In particular, Carvalho et al., Suarez-Sipmann et al. and Lambermont et al. [25-27] have all reported that pigs with ARDS had minimum elastance at a specific PEEP associated with maximum recruitment, higher functional residual capacity, higher oxygenation and without lung overdistension. While these findings are consistent, the application of this PEEP selection method is limited in clinical practice, and current standard of care remains largely based on clinical intuition or a generalized approach such as using the ARDSNet PEEP-FiO 2 table [13-17,22]. Recently, Pintado et al. [28] conducted a randomized controlled trial (RCT) that demonstrated benefits from selecting PEEP at minimum elastance. However, the results of this trial failed to reach statistical significance, with p = 0.16 [28]. Thus, there is great interest in standardizing patient-specific PEEP selection using the minimum elastance-peep method. In this study, the feasibility of setting PEEP, for mechanically ventilated, intubated ARDS patients, using a patient-specific minimum elastance (E rs ) is investigated. Each patient included in this study underwent a recruitment manoeuvre (RM) with multiple PEEP changes to evaluate the patient-specific E rs -PEEP profile and locate the point of minimum E rs. Clinical implications and feasibility of titrating PEEP to minimum E rs to guide and improve therapy are discussed. Methods Patients The study was conducted in the Christchurch Hospital ICU (New Zealand). Ten patients diagnosed with ARDS using the 1998 consensus [9,29] were recruited to the study on the basis that they had the following conditions: (1) acute onset of respiratory failure, (2) PaO 2 /FiO 2 (PF ratio) between 150 and 300 mmhg, (3) findings of bilateral infiltrates on chest radiograph, and (4) absence of left-sided heart failure. The exclusion criteria for the study were (1) patients who were likely to be discontinued from MV within 24 h, (2) age <16 years, (3) moribund and/or not expected to survive for greater than 72 h, and (4) patient with minimal sedation, where additional sedation may lead to prolonged MV. Written informed consent was obtained from the patient/family members or relatives. These trials and the use of the data were approved by the New Zealand, South Island Regional Ethics Committee. The trial is registered with Australian New Zealand Clinical Trials Registry (ACTRN ). Ventilator settings and measurements All patients were ventilated using Puritan Bennett PB840 ventilators (Covidien, Boulder, CO, USA) with volume control (tidal volume, V t = 6 ~ 8 ml/kg), synchronized intermittent mandatory ventilation (SIMV) mode. Other ventilator settings were not changed during the trial.
5 Airway pressure (P aw ) and flow data (Q) were recorded continuously using a pneumotachometer with Hamilton Medical adult flow sensor (Hamilton Medical, Switzerland) connected to the ventilator circuit Y-piece. A laptop PC (Dell, Austin, TX, USA) was used with a National Instruments USB-6009 data acquisition unit and LabVIEW SignalExpress (National Instruments, Austin, TX, USA) to record the airway pressure and flow data with a sampling frequency of 100 Hz. Analysis was performed using MATLAB (R2014a, The Mathworks, Natick, MA, USA). Clinical protocol Each patient included in the trial underwent a stepwise PEEP RM. Prior to the RM, patients were ventilated at a PEEP selected by the attending clinician, based on their experience. At this clinically selected PEEP, an arterial blood gas analysis was performed to determine PaO 2. Before each RM, patients were sedated and paralyzed with muscle relaxants to prevent spontaneous breathing efforts. The specific protocol for the RM was 1. Decrease PEEP to 0 cmh 2 O (zero end-expiratory pressure, ZEEP) 2. Increase PEEP from 0 cmh 2 O in steps of 5 cmh 2 O until peak airway pressure (PIP) reached the limit of 45 cmh 2 O [30]. 3. Maintain each PEEP level for breathing cycles (~1 min) 4. From the maximum PEEP, reduce PEEP back to a clinically selected value in steps of 5 cmh 2 O. The upper airway pressure was limited to 45 cmh 2 O to ensure patient safety. Further details of the clinical protocol can be found in the Additional file 1 (Section 1.0, Complete clinical protocol). The breathing cycles at each PEEP level provided a period of recruitment and stabilization based on the time frames observed in van Drunen et al. [31]. Patient-specific respiratory system elastance, E rs, for each PEEP level was calculated using the last breathing cycle before a PEEP increase. E rs was identified using a single-compartment lung model [32]. This short time period at each PEEP level was designed to create a clinically feasible and efficient protocol that clinical staff would be more likely to follow. However, some patients may not be fully stabilized by this point. Data analysis Respiratory system elastance, E rs, and resistance, R rs, were identified using the singlecompartment lung model shown in Equation (1). P = E V + R Q+ P0 aw rs rs (1) where P aw is the airway pressure, V is lung volume, Q is flow rate and P0 is offset pressure. E rs is identified from measured data using a multiple regression method [33]. Lung volume increase due to PEEP increase is known as end of expiratory lung volume (EELV) or dynamic functional residual capacity (dfrc) [34] and can be calculated from flow data as the amount of air not expired during PEEP increase.
6 Work of breathing (WOB) consists of two major components: work to overcome respiratory elastance and work to overcome airway resistance [35,36]. Thus, higher elastance requires more work to fill a given lung volume. Hence, minimum elastance is associated with reduced WOB [37-39]. The WOB at each PEEP is calculated using Equation (2) [37]. WOB = ( average inspiratory pressure PEEP) volume (2) Relationships between E rs -WOB and E rs -dfrc were investigated using Pearson s correlation coefficient. Identifying a clinically satisfactory PEEP Initially, as PEEP is increased from ZEEP, E rs falls as new lung volume is recruited faster than pressure builds up in the lung. At some point, little or no further recruitment occurs, and E rs begins to rise with increasing PEEP, indicating that pressure above that PEEP level was unable to recruit significant new lung volume and is, instead, beginning to stretch already recruited lung [40]. Thus, while PEEP at minimum E rs is optimal (minimum-e rs PEEP), a slightly lower value may be more clinically palatable, as it reduces the chances of stretching the lung and causing injury. A value of PEEP lower than minimum-e rs PEEP, where E rs is 5 10% above the observed minima, provides a margin of safety, while retaining the benefits of titrating PEEP to elastance. This point is labelled inflection-e rs PEEP, as it represents a point of diminishing returns in the balance of recruitment safety. It is important to note that for any PEEP that exceeds minimum E rs, there will be a rise in E rs, risking overdistension. Thus, inflection-e rs PEEP is proposed as a safety threshold. The aim of this study is to test the feasibility of titrating PEEP to minimum E rs, by identifying the minimum during an RM. However, as inflection-e rs PEEP provides similar benefits and may be safer and more acceptable, both points are presented in the results, for comparison. Results Demographics and clinical details of patients are shown in Table 1. Figure 1 shows the distribution of respiratory elastance (E rs ) (top panel), peak inspiratory pressure (PIP) (middle panel) and dynamic functional residual capacity (dfrc) (bottom panel) across the cohort for each PEEP. Interestingly, paired PaO 2 measurements, before and 30 min after RM, indicated a statistically non-significant reduction in arterial oxygen by a median 11 mmhg [interquartile range (IQR) 0 15] per patient, following the RM (p = 0.21, Wilcoxon signedrank test). Cohort median PaO 2 values for the cohort were 84.0 mmhg [IQR ] and 77.5 mmhg [IQR ] for before and after RM, respectively.
7 Table 1 Patient demographics and clinical details Patient Sex Age Clinical PF ratio APACHE SAPS FiO 2 Clinically Heart Blood pressure Blood pressure PaO 2 before PaO 2 30 min diagnostic (mmhg) II II selected PEEP rate (bpm) a systolic (mmhg) a diastolic (mmhg) a RM (mmhg) after RM (mmhg) 1 F 61 Peritonitis, COPD M 22 Trauma M 55 Aspiration M 88 Pneumonia, COPD 5 M 59 Pneumonia, COPD 6 M 69 Trauma M 56 Legionnaires F 54 Aspiration M 37 H1N1, COPD M 56 Legionnaires, COPD Median [IQR] 230 [ ] 84.0 [ ] 77.5 [ ] a Values are in median. Abbreviations: APACHE II acute physiology and chronic health evaluation II, bpm beats per minute, COPD chronic obstructive pulmonary disease, FiO 2 fraction of inspired oxygen, IQR interquartile range, PaO 2 partial pressure of oxygen in arterial blood, PEEP positive endexpiratory pressure, PF ratio partial pressure of oxygen in arterial blood/fraction of inspired oxygen, RM recruitment manoeuvre, SAPS II simplified acute physiology score II.
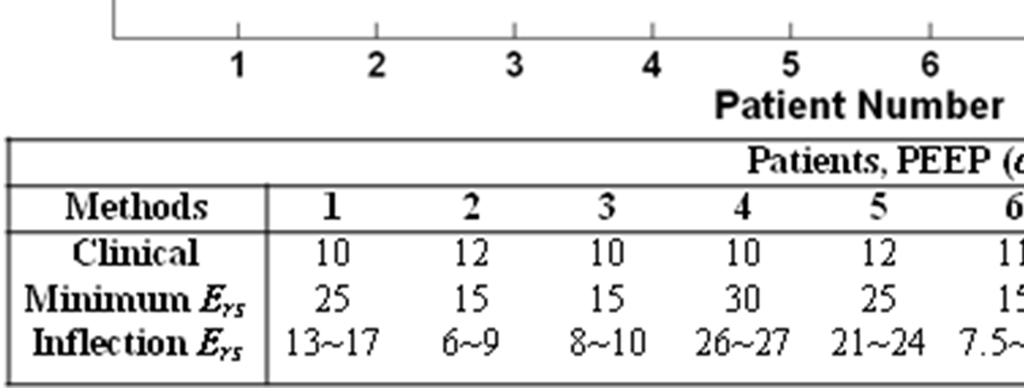
8 Figure 2 shows patient-specific respiratory system elastance (E rs ) and dfrc with increasing PEEP for Patients 2, 6, 8 and 10. The dashed lines shown in Figure 2 are the range where inflection-e rs is located (5 10%, above minimum E rs ). The optimal PEEP using minimum-e rs and inflection-e rs are also indicated. The patient-specific E rs and dfrc with increasing PEEP for all 10 patients are included in the Additional file 1 (Section 2.0, Additional results) provided with the manuscript. Figure 3 presents calculated WOB (left) and dfrc (right) data against E rs. The Pearson correlation of coefficient between E rs and WOB is R = 0.62, and R = 0.62 for dfrc. Figure 1 Cohort respiratory data plotted against positive end-expiratory pressure (PEEP) level. The top panel shows the distribution of patient-specific elastance (E rs ) across the 10 patients at each PEEP level. The middle panel shows peak inspiratory pressure (PIP) and the bottom plot dynamic functional residual capacity (dfrc). Red cross outliers: the outliers in E rs are mainly from patient 5. PEEP levels were classified by rounding to the nearest 5 cmh 2 O. Figure 2 Respiratory mechanics as a function of positive end-expiratory pressure (PEEP). Top left panel, patient 2; top right panel, patient 6; bottom left panel, patient 8; bottom right panel, patient 10. PEEP derived from minimum-e rs and inflection-e rs method are as indicated. The dashed line is the range for inflection-e rs. The dynamic functional residual capacity (dfrc) is also indicated. Figure 3 Pearson s correlation. (Left) Elastance-work of breathing (E rs -WOB), R = (Right) Elastance-dynamic functional residual capacity (E rs -dfrc), R = Figure 4 compares clinically selected PEEP by attending clinicians during MV therapy with minimum-e rs and inflection-e rs values. Across the cohort, these clinical values were within a much narrower range than those selected using patient-specific elastance. Complete patientspecific respiratory mechanics data at each PEEP can be found in the Additional file 1 (Section 2.0, Additional results). Figure 4 Positive end-expiratory pressure (PEEP) selection comparison. Comparison between clinical selection, minimum-e rs and inflection-e rs. Discussion Influence of PEEP in patient s E rs, PIP and dfrc Wide ranges of E rs, PIP and dfrc were observed across all patients and PEEPs. These results reflect the heterogeneity of ARDS patient condition and response to PEEP. It is clear from these results that standardizing PEEP selection is difficult [15], and there is a need for patient-specific approach. Examining the E rs and dfrc across PEEP levels, it was found that all 10 patients included in this study had a different range of E rs, dfrc as well as a patientspecific minimum-e rs PEEP within the tested range (See Additional file 1 (Section 2.0, Additional Results)). At ZEEP, E rs is relatively high and variable across patients (Figure 1). As PEEP is increased, E rs reduces at a rate that is patient-specific (Figure 2). This trend of E rs reduction with PEEP increase matches previous PEEP titration studies in animal subjects [25-27]. This E rs trend
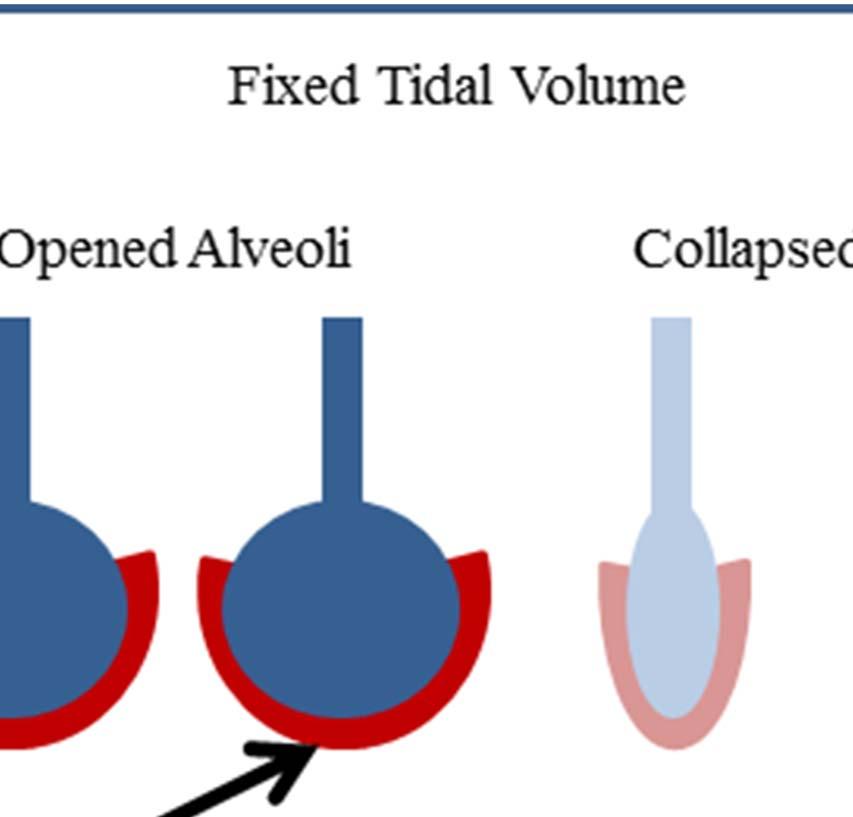
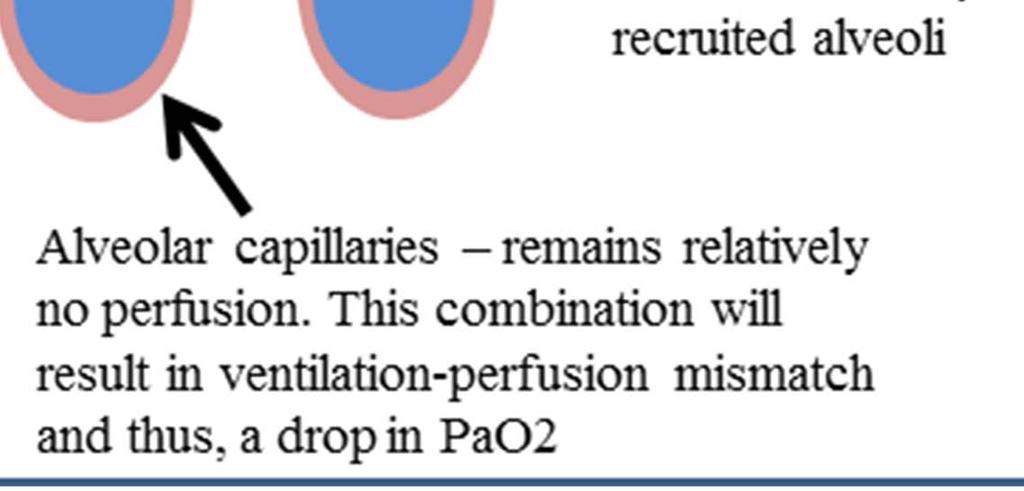
9 with PEEP suggests recruitment, with increase of lung volume outweighing increase in pressure. The dfrc shown in Figure 1 (bottom panel) continued to increase with PEEP, following a sigmoidal curve. This sigmoidal curve indicates overstretching of the lung that occurs at higher PEEP. Increasing PEEP past the minimum-e rs point risks overstretching of healthy lung units even at lower PEEP and airway pressures [19]. In Figure 2, patients 2 and 6 (top panels) show examples of E rs increasing after the minimum, indicating potential stretching of lung units. However, the minimum is not always obvious or present, as was the case for patients 8 and 10, shown in the bottom panels of Figure 2. In this case, E rs -PEEP curve became very flat without further significant reductions in E rs with increases of PEEP from 15 to 30 cmh 2 O. Thus, identifying a point of diminishing returns (inflection-e rs ) is potentially a safer approach to PEEP selection. A moderate correlation between E rs and both WOB and dfrc was observed. This result was expected as elastance relates changes in volume to changes in pressure, and WOB is the product of these two quantities across a breath. Thus, higher elastance requires more work to fill a given lung volume. This result suggests an additional potential benefit to selecting PEEP for minimum E rs to WOB for patients can be minimized if ventilated at the point of minimum elastance. WOB is normally assessed when the patient is spontaneously breathing and may seem pointless in this study where patients were paralyzed. However, these patients slowly resume spontaneous breathing effort as muscle relaxant wears off. Thus, by setting PEEP to minimize a component of WOB could potentially benefit these patients as they regain spontaneous breathing ability. General observations In this study, it was found that PEEP selected using minimum or inflection-e rs were different from clinically selected PEEP. Inflection-E rs selected PEEP was both above and below clinically selected values. This results show a clear variation between these methods. In particular, the clinically selected PEEP was lower than either minimum-e rs or inflection-e rs PEEP in patients with chronic obstructive pulmonary disease (COPD). This result implies that patients with COPD potentially benefit from high PEEP ventilation. It was also found that at higher PEEP of cmh 2 O, the overall maximum PIP remains around 45 cmh 2 O, indicating patients were ventilated at a safe level [30]. However, selecting PEEP is a trade-off in minimizing lung pressure and potential damage versus maximizing recruitment. A total of 7 of 10 patients PaO 2 decreased after the RM by 11 mmhg [IQR 0 15] (p = 0.21, Wilcoxon signed-rank test). While statistically non-significant, this result is worth considering as it is both counterintuitive and contradictory to some studies where significant increases in PaO 2 after RM were observed (p < 0.05) [30,41]. Studies by Tusman et al. [41] and Gattinoni et al. [30] have shown improvement in oxygenation (up to 20%) due to alveolar recruitment. However, other studies have shown no significant differences or reductions in PaO 2 of up to 10% [42-44]. To explain this observed reduction in our trial, we hypothesize that between RM and arterial blood gas analysis, there was insufficient lung perfusion as shown in Figure 5.
10 Figure 5 Ventilation with no perfusion. This condition is due to insufficient blood flow into the newly opened alveoli capillaries. A darker colour shows better perfusion (red) and/or better distribution (blue) of air. Prior to the RM, a fixed tidal volume was distributed between recruited lung units. However, after RM, the same tidal volume would be distributed amongst a larger number of lung units. The newly recruited alveoli are potentially poorly perfused with blood, resulting in a transient lower oxygen transfer to blood and consequently a reduction of observed PaO 2. In addition, the study by Oczenski et al. [42] also showed that maintaining post recruitment manoeuvre PEEP similar to baseline PEEP may not benefit long-term oxygenation improvement, and there is a need to titrate to optimal PEEP. Titrating PEEP The goal of this study is to investigate the feasibility of using an RM to identify patientspecific lung elastance that can be used to titrate a more optimal PEEP. Elastance, E rs, was calculated during the increase-peep section of the RM. Specifically, data from a single inspiration were used, taken from a breath approximately 10 ~ 15 breathing cycles following PEEP increase, to allow stabilization. This procedure is different to the animal studies by Carvalho et al. [25], Suarez-Sipmann et al. [26] and Lambermont et al. [27]. In these studies, elastance (or compliance) was calculated during a PEEP titration manoeuvre after a significant period of time for recruitment [45]. In general, this study has shown that titrating an optimal PEEP for each patient, based on respiratory mechanics, is feasible. Optimal, in this case, is defined as minimum (or nearminimum) elastance, as this point enables maximum recruitment with minimum risk of lung damage. The proposed inflection-e rs is essentially an alternate means of finding a potentially much lower PEEP value that further reduces any unintended potential damage with minimal loss from the optimal minimum E rs. However, the clinical benefit of a patient ventilated at PEEP selected using both inflection-e rs and minimum-e rs was not evaluated in this study and warrants further investigation. Study limitations and recommendations Protocol in hemodynamic management During the RM, there were no standardized protocols for managing hemodynamic stability. Thus, some patients were given hemodynamic therapies such as fluid resuscitation and vasopressors that may have impacted upon the results of this study. However, the responses to these therapies were patient-specific, and the patient numbers were too low in this proofof-concept study to correlate specific elastance responses to the use of these therapies. Equally, it is important to note that the study was primarily focused on proving the metric, capturing the differences across PEEP levels for a range of patients and conditions, which has been shown. For information, Additional file 1 (Section 3.0, Hemodynamic stability) contains the patient-specific details on hemodynamic therapies that were not part of the study protocol.
11 Muscle paralysis Spontaneous breathing efforts can affect the identified respiratory elastance, E rs, as the muscular effort can increase or decrease the apparent mechanical properties. Thus, a muscle relaxant was used in this trial to ensure patients were suitably paralyzed, and E rs could be identified reliably during fully controlled ventilation. However, the use of muscle relaxants for this purpose may be clinically undesirable and could be seen as a limitation of this method. This concern was also raised in the RCT by Pintado et al. [28], in which the authors suggested that finding the maximum compliance PEEP (minimum E rs -PEEP) can be difficult in patients and required muscle relaxants [28]. This potential limitation could be overcome by using oesophageal pressure measurement to remove the spontaneous breathing signal [46]. Monitoring E rs and recruitment manoeuvre design For E rs monitoring, Lambermont et al. [27] allowed 15 min for stabilization time, Suarez- Sipmann et al. [26] allowed 10 min and Carvalho et al. [25] only used 3 min. The clinical study conducted by Suter et al. [23] allowed min for stabilization during increasing PEEP whereas Pintado et al. [28] did not specify the stabilization time period, with the PEEP titration performed during increasing PEEP. Thus, the E rs response observed in this study may be limited to PEEP-induced recruitment and not time-dependent recruitment (if stabilization was not achieved). This limitation is also outlined in the animal trials by van Drunen et al. [47]. The breathing cycles stabilization period allowed for this trial may not be sufficient for all patients as alveoli recruitment is both PEEP- and time-dependent. Thus, E rs and the suggested PEEP from this protocol may be slightly higher than other studies as there is no prior recruitment. The progression of E rs with time and PEEP should be investigated in parallel with a longer stabilization time. An optimal stabilization time period could be established because a shorter stabilization period will significantly reduce the protocol burden, while a longer stabilization may achieve more complete recruitment. A further potential limitation is that several studies have reported that not all patients benefit from RM. In particular, Fan et al. [48], Pelosi et al. [49] and Guerin et al. [44] have reported conflicting results, where the benefit of a RM is dependent of the patient-specific disease state, as well as the design of the RM. Thus, assessing the efficacy of specific forms of RM design should be considered in future clinical trials. In particular, a recruitment manoeuvre of a specific design and its corresponding effect towards cardiovascular, respiratory system and hemodynamic response should be monitored closely with longer period at additional time steps (5, 15, 30, 45, 60, 90 and 120 min after the RM). Equally, the specific design (for example, maximum allowable PEEP or PIP) of RM needs to be adjusted based on the severity of ARDS. Conclusions This study has shown that titrating an optimal PEEP for each patient, based on respiratory mechanics, is feasible. A patient-specific approach is desirable as respiratory mechanics response to PEEP was shown to be quite variable between patients. Minimum-E rs or inflection-e rs PEEP can be found for every patient and thus provide an opportunity to individualize PEEP settings. The patient-specific respiratory elastance, E rs, was shown to be correlated with work of breathing and dynamics functional residual capacity, further
12 indicating its clinical relevance and potential. The approach presented in this proof-ofconcept study offers potential to improve clinical insight and guidance in selecting PEEP. Abbreviations APACHE, Acute physiology and chronic health evaluation; ARDS, Acute respiratory distress syndrome; COPD, Chronic obstructive pulmonary disease; dfrc, Dynamic functional residual capacity; E rs, Patient-specific respiratory elastance; FiO 2, Fraction of inspired oxygen; ICU, Intensive care unit; IQR, Interquartile range; MV, Mechanical ventilation; P0, Offset pressure; PaO 2, Partial pressure of oxygen in arterial blood; P aw, Airway pressure; PEEP, Positive end-expiratory pressure; PF ratio, PaO 2 /FiO 2 ; Q, Flow; RM, Recruitment manoeuvre; R rs, Resistance; SAPS, Simplified acute physiology score; SIMV, Synchronized intermittent mandatory ventilation; V, Volume; VILI, Ventilator-induced lung injury; V t, Tidal volume; WOB, Work of breathing; ZEEP, Zero PEEP Competing interests The authors declare that they have no competing interests. Authors contributions YSC, JGC and GMS created and defined the model. YSC and GMS implemented the clinical trials. YWC, JGC, TD and BL had input to the analysis of results. All authors had input in writing and revising the manuscript. All authors have read and approved the final manuscript. Acknowledgements The authors wish to thank Dr Ashwath Sundaresan for implementing the clinical trials. References 1. Slutsky AS. Lung injury caused by mechanical ventilation*. Chest. 1999;116 suppl 1:9S 15S. 2. Esteban A, Anzueto A, Frutos F, Alia I, Brochard L, Stewart T, et al. Characteristics and outcomes in adult patients receiving mechanical ventilation: a 28-day international study. JAMA. 2002;287(3): Gajic O, Dara SI, Mendez JL, Adesanya AO, Festic E, Caples SM, et al. Ventilatorassociated lung injury in patients without acute lung injury at the onset of mechanical ventilation *. Crit Care Med. 2004;32(9): Gullo A, Berlot G, Garcia CSNB, Rocco PRM, Zin WA. Understanding the mechanism of ventilator-induced lung injury. Perioperative and critical care medicine. Milan: Springer; p Girard TD, Bernard GR. Mechanical ventilation in ARDS. Chest. 2007;131(3):921 9.
13 6. Marini JJ, Gattinoni L. Ventilatory management of acute respiratory distress syndrome: a consensus of two. Crit Care Med. 2004;32: Esteban A, Cook DJ, Anzueto A, Gattinoni L, Chiumello D, Vagginelli F. Management of patients with respiratory failure: an evidence-based approach. In: Vincent J-L, editor. Evidence-based management of patients with respiratory failure. Update in intensive care medicine. Berlin Heidelberg: Springer; p Ashbaugh D, Boyd Bigelow D, Petty T, Levine B. Acute respiratory distress in adults. Lancet. 1967;290(7511): Bernard GR, Artigas A, Brigham KL, Carlet J, Falke K, Hudson L, et al. The American- European consensus conference on ARDS: definitions, mechanisms, relevant outcomes and clinical trial coordination. Am J Respir Crit Care Med. 1994;149: Brandstetter RD, Sharma KC, DellaBadia M, Cabreros LJ, Kabinoff GS. Adult respiratory distress syndrome: a disorder in need of improved outcome. Heart Lung: J Acute Crit Care. 1997;26(1):3 14. doi: 11. Desai A, Deep A. Ventilatory strategies and adjunctive therapy in ARDS. Indian J Pediatr. 2006;73(8): doi: /bf Gattinoni L, Carlesso E, Brazzi L, Caironi P. Positive end-expiratory pressure. Curr Opin Crit Care. 2010;16(1): The Acute Respiratory Distress Syndrome Network. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med. 2000;342(18): Brower RG, Lanken PN, MacIntyre N, Matthay MA, Morris A, Ancukiewicz M, et al. Higher versus lower positive end-expiratory pressures in patients with the acute respiratory distress syndrome. N Engl J Med. 2004;351(4): Mercat A, Richard J-CM, Vielle B, Jaber S, Osman D, Diehl J-L, et al. Positive endexpiratory pressure setting in adults with acute lung injury and acute respiratory distress syndrome: a randomized controlled trial. JAMA. 2008;299(6): doi: /jama Meade MO, Cook DJ, Guyatt GH, Slutsky AS, Arabi YM, Cooper DJ, et al. Ventilation strategy using low tidal volumes, recruitment maneuvers, and high positive end-expiratory pressure for acute lung injury and acute respiratory distress syndrome: a randomized controlled trial. JAMA. 2008;299(6): doi: /jama Briel M, Meade M, Mercat A, Brower RG, Talmor D, Walter SD, et al. Higher vs lower positive end-expiratory pressure in patients with acute lung injury and acute respiratory distress syndrome: systematic review and meta-analysis. JAMA. 2010;303(9): Ware LB, Matthay MA. The acute respiratory distress syndrome. N Engl J Med. 2000;342(18):
14 19. Stenqvist O. Practical assessment of respiratory mechanics. Br J Anaesth. 2003;91(1): doi: /bja/aeg Sundaresan A, Chase JG. Positive end expiratory pressure in patients with acute respiratory distress syndrome - the past, present and future. Biomed Signal Process Control. 2011;7(2): doi: /j.bspc Spieth P, Gama de Abreu M. Lung recruitment in ARDS: we are still confused, but on a higher PEEP level. Crit Care. 2012;16(1): Kallet RH, Branson RD. Do the NIH ARDS Clinical Trials Network PEEP/FIO2 tables provide the best evidence-based guide to balancing PEEP and FIO2 settings in adults? Respir Care. 2007;52(4): Suter P, Fairley B, Isenberg M. Optimum end-expiratory airway pressure in patients with acute pulmonary failure. N Engl J Med. 1975;292(6): Suter PM, Fairley HB, Isenberg MD. Effect of tidal volume and positive end-expiratory pressure on compliance during mechanical ventilation. Chest. 1978;73: Carvalho A, Jandre F, Pino A, Bozza F, Salluh J, Rodrigues R, et al. Positive endexpiratory pressure at minimal respiratory elastance represents the best compromise between mechanical stress and lung aeration in oleic acid induced lung injury. Crit Care. 2007;11(4):R Suarez-Sipmann F, Bohm SH, Tusman G, Pesch T, Thamm O, Reissmann H, et al. Use of dynamic compliance for open lung positive end-expiratory pressure titration in an experimental study. Crit Care Med. 2007;35: Lambermont B, Ghuysen A, Janssen N, Morimont P, Hartstein G, Gerard P, et al. Comparison of functional residual capacity and static compliance of the respiratory system during a positive end-expiratory pressure (PEEP) ramp procedure in an experimental model of acute respiratory distress syndrome. Crit Care. 2008;12(4):R Pintado M-C, de Pablo R, Trascasa M, Milicua J-M, Rogero S, Daguerre M, et al. Individualized PEEP setting in subjects with ARDS: a randomized controlled pilot study. Respir Care. 2013;58(9): doi: /respcare Artigas A, Bernard Gordon R, Carlet J, Dreyfuss D, Gattinoni L, Hudson L, et al. The American-European Consensus Conference on ARDS, Part 2. Ventilatory, pharmacologic, supportive therapy, study design strategies, and issues related to recovery and remodeling. Am J Respir Crit Care Med. 1998;157(4): Gattinoni L, Caironi P, Cressoni M, Chiumello D, Ranieri VM, Quintel M, et al. Lung recruitment in patients with the acute respiratory distress syndrome. N Engl J Med. 2006;354(17): van Drunen E, Chiew YS, Chase J, Shaw G, Lambermont B, Janssen N, et al. Expiratory model-based method to monitor ARDS disease state. Bio Med Eng OnLine. 2013;12(1):57.
15 32. Lucangelo U, Bernabè F, Blanch L. Lung mechanics at the bedside: make it simple. Curr Opin Crit Care. 2007;13(1): doi: /MCC.0b013e df. 33. Peslin R, da Silva JF, Chabot F, Duvivier C. Respiratory mechanics studied by multiple linear regression in unsedated ventilated patients. Eur Respir J. 1992;5(7): Sundaresan A, Geoffrey Chase J, Hann CE, Shaw GM. Dynamic functional residual capacity can be estimated using a stress strain approach. Comput Methods Programs Biomed. 2011;101(2): Otis AB, Fenn WO, Rahn H. Mechanics of breathing in man. J Appl Physiol. 1950;2(11): Marini JJ, Capps JS, Culver BH. The inspiratory work of breathing during assisted mechanical ventilation. Chest. 1985;87(5): doi: /chest Grinnan D, Truwit J. Clinical review: respiratory mechanics in spontaneous and assisted ventilation. Crit Care. 2005;9(5): Kallet RH, Hemphill JC, Dicker RA, Alonso JA, Campbell AR, Mackersie RC, et al. The spontaneous breathing pattern and work of breathing of patients with acute respiratory distress syndrome and acute lung injury. Respir Care. 2007;52(8): Mason RJ, Courtney Broaddus V, Martin TR, King TE, Schraufnagel DE, Murray JF, et al. Murray and Nadel s textbook of respiratory medicine. 5th ed Vieira Silvia RR, Puybasset L, Richecoeur J, Lu QIN, Cluzel P, Gusman Pablo B, et al. A Lung computed tomographic assessment of positive end-expiratory pressure-induced lung overdistension. Am J Respir Crit Care Med. 1998;158(5): Tusman G, Böhm SH, Vazquez de Anda GF, do Campo JL, Lachmann B. Alveolar recruitment strategy improves arterial oxygenation during general anaesthesia. Br J Anaesth. 1999;82(1):8 13. doi: /bja/ Oczenski W, Hörmann C, Keller C, Lorenzl N, Kepka A, Schwarz S, et al. Recruitment maneuvers after a positive end-expiratory pressure trial do not induce sustained effects in early adult respiratory distress syndrome. Anesthesiology. 2004;101(3): Meade MO, Cook DJ, Griffith LE, Hand LE, Lapinsky SE, Stewart TE, et al. A study of the physiologic responses to a lung recruitment maneuver in acute lung injury and acute respiratory distress syndrome. Respir Care. 2008;53(11): Guerin C, Debord S, Leray V, Delannoy B, Bayle F, Bourdin G, et al. Efficacy and safety of recruitment maneuvers in acute respiratory distress syndrome. Ann Intensive Care. 2011;1(1): Suarez-Sipmann F, Bohm S. Recruit the lung before titrating the right positive endexpiratory pressure to protect it. Crit Care. 2009;13(3):134.
16 46. Khirani S, Polese G, Aliverti A, Appendini L, Nucci G, Pedotti A, et al. On-line monitoring of lung mechanics during spontaneous breathing: a physiological study. Respir Med. 2010;104(3): van Drunen E, Chiew YS, Pretty C, Shaw G, Lambermont B, Janssen N, et al. Visualisation of time-varying respiratory system elastance in experimental ARDS animal models. BMC Pulm Med. 2014;14(1): Fan E, Wilcox ME, Brower RG, Stewart TE, Mehta S, Lapinsky SE, et al. Recruitment maneuvers for acute lung injury. Am J Respir Crit Care Med. 2008;178(11): doi: /rccm OC. 49. Pelosi P, Gama de Abreu M, Rocco PR. New and conventional strategies for lung recruitment in acute respiratory distress syndrome. Crit Care. 2010;14:210.
17
18
19
20
21
22 Additional files provided with this submission: Additional file 1. A supplementary document that consist of several information. The information are (1) complete clinical protocol, (2) hemodynamic stability, (3) additional results and (4) independent patient study patient 9 (H1N1) (761kb)
Feasibility of titrating PEEP to minimum elastance for mechanically ventilated patients
 Chiew et al. Pilot and Feasibility Studies (2015) 1:9 DOI 10.1186/s40814-015-0006-2 RESEARCH Open Access Feasibility of titrating PEEP to minimum elastance for mechanically ventilated patients Yeong Shiong
Chiew et al. Pilot and Feasibility Studies (2015) 1:9 DOI 10.1186/s40814-015-0006-2 RESEARCH Open Access Feasibility of titrating PEEP to minimum elastance for mechanically ventilated patients Yeong Shiong
Physiological Relevance of a Minimal Model in Healthy Pigs Lung
 Physiological Relevance of a Minimal Model in Healthy Pigs Lung Yeong Shiong Chiew*, Thomas Desaive** Bernard Lambermont**, Nathalie Janssen**, Geoffrey M Shaw***, Christoph Schranz****, Knut Möller****,
Physiological Relevance of a Minimal Model in Healthy Pigs Lung Yeong Shiong Chiew*, Thomas Desaive** Bernard Lambermont**, Nathalie Janssen**, Geoffrey M Shaw***, Christoph Schranz****, Knut Möller****,
11 th Annual Congress Turkish Thoracic Society. Mechanical Ventilation in Acute Hypoxemic Respiratory Failure
 11 th Annual Congress Turkish Thoracic Society Mechanical Ventilation in Acute Hypoxemic Respiratory Failure Lluis Blanch MD PhD Senior Critical Care Center Scientific Director Corporació Parc Taulí Universitat
11 th Annual Congress Turkish Thoracic Society Mechanical Ventilation in Acute Hypoxemic Respiratory Failure Lluis Blanch MD PhD Senior Critical Care Center Scientific Director Corporació Parc Taulí Universitat
Available online at ScienceDirect. IFAC-PapersOnLine (2015)
") Available online at www.sciencedirect.com ScienceDirect IFAC-PapersOnLine 48-20 (2015) 273 278 Reducing the Length of Mechanical Ventilation with Significance: A Case Study of Sample Size Estimation Trial
Available online at www.sciencedirect.com ScienceDirect IFAC-PapersOnLine 48-20 (2015) 273 278 Reducing the Length of Mechanical Ventilation with Significance: A Case Study of Sample Size Estimation Trial
Protective ventilation for ALL patients
 Protective ventilation for ALL patients PAOLO PELOSI, MD, FERS Department of Surgical Sciences and Integrated Diagnostics (DISC), San Martino Policlinico Hospital IRCCS for Oncology, University of Genoa,
Protective ventilation for ALL patients PAOLO PELOSI, MD, FERS Department of Surgical Sciences and Integrated Diagnostics (DISC), San Martino Policlinico Hospital IRCCS for Oncology, University of Genoa,
Biomedical engineer s guide to the clinical aspects of intensive care mechanical ventilation
 https://doi.org/10.1186/s12938-018-0599-9 BioMedical Engineering OnLine REVIEW Open Access Biomedical engineer s guide to the clinical aspects of intensive care mechanical ventilation Vincent J. Major
https://doi.org/10.1186/s12938-018-0599-9 BioMedical Engineering OnLine REVIEW Open Access Biomedical engineer s guide to the clinical aspects of intensive care mechanical ventilation Vincent J. Major
How ARDS should be treated in 2017
 How ARDS should be treated in 2017 2017, Ostrava Luciano Gattinoni, MD, FRCP Georg-August-Universität Göttingen Germany ARDS 1. Keep the patient alive respiration circulation 2. Cure the disease leading
How ARDS should be treated in 2017 2017, Ostrava Luciano Gattinoni, MD, FRCP Georg-August-Universität Göttingen Germany ARDS 1. Keep the patient alive respiration circulation 2. Cure the disease leading
Higher PEEP improves outcomes in ARDS patients with clinically objective positive oxygenation response to PEEP: a systematic review and meta-analysis
 Guo et al. BMC Anesthesiology (2018) 18:172 https://doi.org/10.1186/s12871-018-0631-4 RESEARCH ARTICLE Open Access Higher PEEP improves outcomes in ARDS patients with clinically objective positive oxygenation
Guo et al. BMC Anesthesiology (2018) 18:172 https://doi.org/10.1186/s12871-018-0631-4 RESEARCH ARTICLE Open Access Higher PEEP improves outcomes in ARDS patients with clinically objective positive oxygenation
Sub-category: Intensive Care for Respiratory Distress
 Course n : Course 3 Title: RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE Sub-category: Intensive Care for Respiratory Distress Topic: Acute Respiratory Distress
Course n : Course 3 Title: RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE Sub-category: Intensive Care for Respiratory Distress Topic: Acute Respiratory Distress
BMC Pulmonary Medicine
 BMC Pulmonary Medicine This Provisional PDF corresponds to the article as it appeared upon acceptance. Fully formatted PDF and full text (HTML) versions will be made available soon. Physiological relevance
BMC Pulmonary Medicine This Provisional PDF corresponds to the article as it appeared upon acceptance. Fully formatted PDF and full text (HTML) versions will be made available soon. Physiological relevance
Dr. Yasser Fathi M.B.B.S, M.Sc, M.D. Anesthesia Consultant, Head of ICU King Saud Hospital, Unaizah
 BY Dr. Yasser Fathi M.B.B.S, M.Sc, M.D Anesthesia Consultant, Head of ICU King Saud Hospital, Unaizah Objectives For Discussion Respiratory Physiology Pulmonary Graphics BIPAP Graphics Trouble Shootings
BY Dr. Yasser Fathi M.B.B.S, M.Sc, M.D Anesthesia Consultant, Head of ICU King Saud Hospital, Unaizah Objectives For Discussion Respiratory Physiology Pulmonary Graphics BIPAP Graphics Trouble Shootings
The use of proning in the management of Acute Respiratory Distress Syndrome
 Case 3 The use of proning in the management of Acute Respiratory Distress Syndrome Clinical Problem This expanded case summary has been chosen to explore the rationale and evidence behind the use of proning
Case 3 The use of proning in the management of Acute Respiratory Distress Syndrome Clinical Problem This expanded case summary has been chosen to explore the rationale and evidence behind the use of proning
ARDS Assisted ventilation and prone position. ICU Fellowship Training Radboudumc
 ARDS Assisted ventilation and prone position ICU Fellowship Training Radboudumc Fig. 1 Physiological mechanisms controlling respiratory drive and clinical consequences of inappropriate respiratory drive
ARDS Assisted ventilation and prone position ICU Fellowship Training Radboudumc Fig. 1 Physiological mechanisms controlling respiratory drive and clinical consequences of inappropriate respiratory drive
Measuring End Expiratory Lung Volume after cardiac surgery
 (Acta Anaesth. Belg., 2012, 63, 115-120) Measuring End Expiratory Lung Volume after cardiac surgery G. MICHIELS (*), V. MARCHAL (**), D. LEDOUX (*) and P. DAMAS (*) Abstract. Background : The aim of this
(Acta Anaesth. Belg., 2012, 63, 115-120) Measuring End Expiratory Lung Volume after cardiac surgery G. MICHIELS (*), V. MARCHAL (**), D. LEDOUX (*) and P. DAMAS (*) Abstract. Background : The aim of this
Should the ART trial change our practice?
 Editorial Should the ART trial change our practice? Jesús Villar 1,2,3, Fernando Suárez-Sipmann 1,4,5, Robert M. Kacmarek 6,7 1 CIBER de Enfermedades Respiratorias, Instituto de Salud Carlos III, Madrid,
Editorial Should the ART trial change our practice? Jesús Villar 1,2,3, Fernando Suárez-Sipmann 1,4,5, Robert M. Kacmarek 6,7 1 CIBER de Enfermedades Respiratorias, Instituto de Salud Carlos III, Madrid,
The new ARDS definitions: what does it mean?
 The new ARDS definitions: what does it mean? Richard Beale 7 th September 2012 METHODS ESICM convened an international panel of experts, with representation of ATS and SCCM The objectives were to update
The new ARDS definitions: what does it mean? Richard Beale 7 th September 2012 METHODS ESICM convened an international panel of experts, with representation of ATS and SCCM The objectives were to update
The ARDS is characterized by increased permeability. Incidence of ARDS in an Adult Population of Northeast Ohio*
 Incidence of ARDS in an Adult Population of Northeast Ohio* Alejandro C. Arroliga, MD, FCCP; Ziad W. Ghamra, MD; Alejandro Perez Trepichio, MD; Patricia Perez Trepichio, RRT; John J. Komara Jr., BA, RRT;
Incidence of ARDS in an Adult Population of Northeast Ohio* Alejandro C. Arroliga, MD, FCCP; Ziad W. Ghamra, MD; Alejandro Perez Trepichio, MD; Patricia Perez Trepichio, RRT; John J. Komara Jr., BA, RRT;
Application of Lung Protective Ventilation MUST Begin Immediately After Intubation
 Conflict of Interest Disclosure Robert M Kacmarek Managing Severe Hypoxemia!" 9-28-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts I disclose
Conflict of Interest Disclosure Robert M Kacmarek Managing Severe Hypoxemia!" 9-28-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts I disclose
Principles of Mechanical Ventilation
 47 Principles of Mechanical Ventilation Jonathan E. Sevransky, MD, MHS Objectives Understand the indications for treatment with mechanical ventilation Describe ventilator strategies that will minimize
47 Principles of Mechanical Ventilation Jonathan E. Sevransky, MD, MHS Objectives Understand the indications for treatment with mechanical ventilation Describe ventilator strategies that will minimize
Recruitment Maneuvers and Higher PEEP, the So-Called Open Lung Concept, in Patients with ARDS
 Zee and Gommers Critical Care (2019) 23:73 https://doi.org/10.1186/s13054-019-2365-1 REVIEW Recruitment Maneuvers and Higher PEEP, the So-Called Open Lung Concept, in Patients with ARDS Philip van der
Zee and Gommers Critical Care (2019) 23:73 https://doi.org/10.1186/s13054-019-2365-1 REVIEW Recruitment Maneuvers and Higher PEEP, the So-Called Open Lung Concept, in Patients with ARDS Philip van der
Research Article A Patient-Specific Airway Branching Model for Mechanically Ventilated Patients
 Computational and Mathematical Methods in Medicine, Article ID 64573, 1 pages http://dx.doi.org/1.1155/14/64573 Research Article A Patient-Specific Airway Branching Model for Mechanically Ventilated Patients
Computational and Mathematical Methods in Medicine, Article ID 64573, 1 pages http://dx.doi.org/1.1155/14/64573 Research Article A Patient-Specific Airway Branching Model for Mechanically Ventilated Patients
Multi-Scale Pulmonary Modelling. and Clinical Applications
 Multi-Scale Pulmonary Modelling and Clinical Applications Nor Salwa Damanhuri A thesis submitted for the degree of Doctor of Philosophy in BioEngineering at the University of Canterbury, Christchurch,
Multi-Scale Pulmonary Modelling and Clinical Applications Nor Salwa Damanhuri A thesis submitted for the degree of Doctor of Philosophy in BioEngineering at the University of Canterbury, Christchurch,
Analyzing Lung protective ventilation F Javier Belda MD, PhD Sº de Anestesiología y Reanimación. Hospital Clinico Universitario Valencia (Spain)
") Analyzing Lung protective ventilation F Javier Belda MD, PhD Sº de Anestesiología y Reanimación Hospital Clinico Universitario Valencia (Spain) ALI/ARDS Report of the American-European consensus conference
Analyzing Lung protective ventilation F Javier Belda MD, PhD Sº de Anestesiología y Reanimación Hospital Clinico Universitario Valencia (Spain) ALI/ARDS Report of the American-European consensus conference
Ventilatory Management of ARDS. Alexei Ortiz Milan; MD, MSc
 Ventilatory Management of ARDS Alexei Ortiz Milan; MD, MSc 2017 Outline Ventilatory management of ARDS Protected Ventilatory Strategy Use of NMB Selection of PEEP Driving pressure Lung Recruitment Prone
Ventilatory Management of ARDS Alexei Ortiz Milan; MD, MSc 2017 Outline Ventilatory management of ARDS Protected Ventilatory Strategy Use of NMB Selection of PEEP Driving pressure Lung Recruitment Prone
Landmark articles on ventilation
 Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
Oxygenation improves during the first 8 h of extended-duration prone positioning in patients with respiratory failure: a retrospective study
 Miyamoto et al. Journal of Intensive Care 2014, 2:52 RESEARCH Open Access Oxygenation improves during the first 8 h of extended-duration prone positioning in patients with respiratory failure: a retrospective
Miyamoto et al. Journal of Intensive Care 2014, 2:52 RESEARCH Open Access Oxygenation improves during the first 8 h of extended-duration prone positioning in patients with respiratory failure: a retrospective
Airway pressure release ventilation (APRV) in PICU: Current evidence. Chor Yek Kee Sarawak General Hospital
 in PICU: Current evidence. Chor Yek Kee Sarawak General Hospital") Airway pressure release ventilation (APRV) in PICU: Current evidence Chor Yek Kee Sarawak General Hospital Outline Brief introduction of APRV History of APRV Common confusion in APRV Features of APRV and
Airway pressure release ventilation (APRV) in PICU: Current evidence Chor Yek Kee Sarawak General Hospital Outline Brief introduction of APRV History of APRV Common confusion in APRV Features of APRV and
The Art and Science of Weaning from Mechanical Ventilation
 The Art and Science of Weaning from Mechanical Ventilation Shekhar T. Venkataraman M.D. Professor Departments of Critical Care Medicine and Pediatrics University of Pittsburgh School of Medicine Some definitions
The Art and Science of Weaning from Mechanical Ventilation Shekhar T. Venkataraman M.D. Professor Departments of Critical Care Medicine and Pediatrics University of Pittsburgh School of Medicine Some definitions
Potential Conflicts of Interest
 Potential Conflicts of Interest Patient Ventilator Synchrony, PAV and NAVA! Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts 4-27-09 WSRC Received research
Potential Conflicts of Interest Patient Ventilator Synchrony, PAV and NAVA! Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts 4-27-09 WSRC Received research
Recognizing and Correcting Patient-Ventilator Dysynchrony
 2019 KRCS Annual State Education Seminar Recognizing and Correcting Patient-Ventilator Dysynchrony Eric Kriner BS,RRT Pulmonary Critical Care Clinical Specialist MedStar Washington Hospital Center Washington,
2019 KRCS Annual State Education Seminar Recognizing and Correcting Patient-Ventilator Dysynchrony Eric Kriner BS,RRT Pulmonary Critical Care Clinical Specialist MedStar Washington Hospital Center Washington,
Spontaneous Breathing Trial and Mechanical Ventilation Weaning Process
 Page 1 of 5 ASSESSMENT INTERVENTION Patient receiving mechanical ventilation Baseline ventilatory mode/ settings RT and RN to assess criteria 1 for SBT Does patient meet criteria? RT to initiate SBT Does
Page 1 of 5 ASSESSMENT INTERVENTION Patient receiving mechanical ventilation Baseline ventilatory mode/ settings RT and RN to assess criteria 1 for SBT Does patient meet criteria? RT to initiate SBT Does
Oxygenation Failure. Increase FiO2. Titrate end-expiratory pressure. Adjust duty cycle to increase MAP. Patient Positioning. Inhaled Vasodilators
 Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
Weaning and extubation in PICU An evidence-based approach
 Weaning and extubation in PICU An evidence-based approach Suchada Sritippayawan, MD. Div. Pulmonology & Crit Care Dept. Pediatrics Faculty of Medicine Chulalongkorn University Kanokporn Udomittipong, MD.
Weaning and extubation in PICU An evidence-based approach Suchada Sritippayawan, MD. Div. Pulmonology & Crit Care Dept. Pediatrics Faculty of Medicine Chulalongkorn University Kanokporn Udomittipong, MD.
Tracking lung recruitment and regional tidal volume at the bedside. Antonio Pesenti
 Tracking lung recruitment and regional tidal volume at the bedside Antonio Pesenti Conflicts of Interest Maquet: Received research support and consultation fees Drager: Received research support and consultation
Tracking lung recruitment and regional tidal volume at the bedside Antonio Pesenti Conflicts of Interest Maquet: Received research support and consultation fees Drager: Received research support and consultation
Outline. Basic principles of lung protective ventilation. The challenging areas. Small tidal volumes Recruitment
 ARDS beyond 6/kg Gordon D. Rubenfeld, MD MSc Professor of Medicine, University of Toronto Chief, Program in Trauma, Emergency, and Critical Care Sunnybrook Health Sciences Centre Outline Basic principles
ARDS beyond 6/kg Gordon D. Rubenfeld, MD MSc Professor of Medicine, University of Toronto Chief, Program in Trauma, Emergency, and Critical Care Sunnybrook Health Sciences Centre Outline Basic principles
Ventilator ECMO Interactions
 Ventilator ECMO Interactions Lorenzo Del Sorbo, MD CCCF Toronto, October 2 nd 2017 Disclosure Relevant relationships with commercial entities: none Potential for conflicts within this presentation: none
Ventilator ECMO Interactions Lorenzo Del Sorbo, MD CCCF Toronto, October 2 nd 2017 Disclosure Relevant relationships with commercial entities: none Potential for conflicts within this presentation: none
Surviving Sepsis Campaign. Guidelines for Management of Severe Sepsis/Septic Shock. An Overview
 Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor
 Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Estimating afterload, systemic vascular resistance and pulmonary vascular resistance in an intensive care setting
 Estimating afterload, systemic vascular resistance and pulmonary vascular resistance in an intensive care setting David J. Stevenson James Revie Geoffrey J. Chase Geoffrey M. Shaw Bernard Lambermont Alexandre
Estimating afterload, systemic vascular resistance and pulmonary vascular resistance in an intensive care setting David J. Stevenson James Revie Geoffrey J. Chase Geoffrey M. Shaw Bernard Lambermont Alexandre
FAILURE OF NONINVASIVE VENTILATION FOR DE NOVO ACUTE HYPOXEMIC RESPIRATORY FAILURE: ROLE OF TIDAL VOLUME
 FAILURE OF NONINVASIVE VENTILATION FOR DE NOVO ACUTE HYPOXEMIC RESPIRATORY FAILURE: ROLE OF TIDAL VOLUME Guillaume CARTEAUX, Teresa MILLÁN-GUILARTE, Nicolas DE PROST, Keyvan RAZAZI, Shariq ABID, Arnaud
FAILURE OF NONINVASIVE VENTILATION FOR DE NOVO ACUTE HYPOXEMIC RESPIRATORY FAILURE: ROLE OF TIDAL VOLUME Guillaume CARTEAUX, Teresa MILLÁN-GUILARTE, Nicolas DE PROST, Keyvan RAZAZI, Shariq ABID, Arnaud
APRV Ventilation Mode
 APRV Ventilation Mode Airway Pressure Release Ventilation A Type of CPAP Continuous Positive Airway Pressure (CPAP) with an intermittent release phase. Patient cycles between two levels of CPAP higher
APRV Ventilation Mode Airway Pressure Release Ventilation A Type of CPAP Continuous Positive Airway Pressure (CPAP) with an intermittent release phase. Patient cycles between two levels of CPAP higher
ARF. 8 8 (PaO 2 / FIO 2 ) NPPV NPPV ( P = 0.37) NPPV NPPV. (PaO 2 / FIO 2 > 200 PaO 2 / FIO 2 NPPV > 100) (P = 0.02) NPPV ( NPPV P = 0.
 NPPV NPPV ( P = 0.37) NPPV NPPV. (PaO 2 / FIO 2 > 200 PaO 2 / FIO 2 NPPV > 100) (P = 0.02) NPPV ( NPPV P = 0.") Monica Rocco, MD; Donatella Dell'Utri, MD; Andrea Morelli, MD; Gustavo Spadetta, MD; Giorgio Conti, MD; Massimo Antonelli, MD; and Paolo Pietropaoli, MD (ARF) (NPPV) 19 ARF ( 8 8 3 ) NPPV 19 (PaO 2 / FIO
Monica Rocco, MD; Donatella Dell'Utri, MD; Andrea Morelli, MD; Gustavo Spadetta, MD; Giorgio Conti, MD; Massimo Antonelli, MD; and Paolo Pietropaoli, MD (ARF) (NPPV) 19 ARF ( 8 8 3 ) NPPV 19 (PaO 2 / FIO
Acute effects of nitric oxide inhalation in ARDS: A dose finding study at steady state kinetics
 Research Article Acute effects of nitric oxide inhalation in ARDS: A dose finding study at steady state kinetics M. S. Hari, A. Trikha*, R. Madan**, H. L. Kaul*** Abstract Background: Inhaled Nitric oxide
Research Article Acute effects of nitric oxide inhalation in ARDS: A dose finding study at steady state kinetics M. S. Hari, A. Trikha*, R. Madan**, H. L. Kaul*** Abstract Background: Inhaled Nitric oxide
Refresher Course MYTHS AND REALITY ABOUT LUNG MECHANICS 5 RC 2. European Society of Anaesthesiologists FIGURE 1 STATIC MEASUREMENTS
 European Society of Anaesthesiologists Refresher Course S AND ABOUT LUNG MECHANICS 5 RC 2 Anders LARSSON Gentofte University Hospital Copenhagen University Hellerup, Denmark Saturday May 31, 2003 Euroanaesthesia
European Society of Anaesthesiologists Refresher Course S AND ABOUT LUNG MECHANICS 5 RC 2 Anders LARSSON Gentofte University Hospital Copenhagen University Hellerup, Denmark Saturday May 31, 2003 Euroanaesthesia
QuickLung Breather Patient Settings
 The QuickLung Breather is capable of simulating a spontaneously breathing patient in a variety of modes and patterns. In response to customer requests, we have compiled five common respiratory cases below.
The QuickLung Breather is capable of simulating a spontaneously breathing patient in a variety of modes and patterns. In response to customer requests, we have compiled five common respiratory cases below.
Ventilation in Paediatric ARDS: extrapolate from adult studies?
 Ventilation in Paediatric ARDS: extrapolate from adult studies? ASMIC 2014 Dr Adrian Plunkett Consultant Paediatric Intensivist Birmingham Children s Hospital, UK Aims of the presentation Ventilation
Ventilation in Paediatric ARDS: extrapolate from adult studies? ASMIC 2014 Dr Adrian Plunkett Consultant Paediatric Intensivist Birmingham Children s Hospital, UK Aims of the presentation Ventilation
RESPIRATORY CARE Paper in Press. Published on January 29, 2013 as DOI: /respcare.02068
 TITLE PAGE: Title: INDIVIDUALIZED POSITIVE END-EXPIRATORY PRESSURE SETTING IN PATIENTS WITH ACUTE RESPIRATORY DISTRESS SYNDROME. A RANDOMIZED CONTROLLED PILOT STUDY. Running title: INDIVIDUALIZED PEEP
TITLE PAGE: Title: INDIVIDUALIZED POSITIVE END-EXPIRATORY PRESSURE SETTING IN PATIENTS WITH ACUTE RESPIRATORY DISTRESS SYNDROME. A RANDOMIZED CONTROLLED PILOT STUDY. Running title: INDIVIDUALIZED PEEP
Ventilator Waveforms: Interpretation
 Ventilator Waveforms: Interpretation Albert L. Rafanan, MD, FPCCP Pulmonary, Critical Care and Sleep Medicine Chong Hua Hospital, Cebu City Types of Waveforms Scalars are waveform representations of pressure,
Ventilator Waveforms: Interpretation Albert L. Rafanan, MD, FPCCP Pulmonary, Critical Care and Sleep Medicine Chong Hua Hospital, Cebu City Types of Waveforms Scalars are waveform representations of pressure,
Comparison of automated and static pulse respiratory mechanics during supported ventilation
 Comparison of automated and static pulse respiratory mechanics during supported ventilation Alpesh R Patel, Susan Taylor and Andrew D Bersten Respiratory system compliance ( ) and inspiratory resistance
Comparison of automated and static pulse respiratory mechanics during supported ventilation Alpesh R Patel, Susan Taylor and Andrew D Bersten Respiratory system compliance ( ) and inspiratory resistance
APRV for ARDS: the complexities of a mode and how it affects even the best trials
 Editorial APRV for ARDS: the complexities of a mode and how it affects even the best trials Eduardo Mireles-Cabodevila 1,2, Siddharth Dugar 1,2, Robert L. Chatburn 1,2 1 Respiratory Institute, Cleveland
Editorial APRV for ARDS: the complexities of a mode and how it affects even the best trials Eduardo Mireles-Cabodevila 1,2, Siddharth Dugar 1,2, Robert L. Chatburn 1,2 1 Respiratory Institute, Cleveland
Noninvasive respiratory support:why is it working?
 Noninvasive respiratory support:why is it working? Paolo Pelosi Department of Surgical Sciences and Integrated Diagnostics (DISC) IRCCS San Martino IST University of Genoa, Genoa, Italy ppelosi@hotmail.com
Noninvasive respiratory support:why is it working? Paolo Pelosi Department of Surgical Sciences and Integrated Diagnostics (DISC) IRCCS San Martino IST University of Genoa, Genoa, Italy ppelosi@hotmail.com
Fluid restriction is superior in acute lung injury and ARDS
 TAKE-HOME POINTS FROM LECTURES BY CLEVELAND CLINIC AND VISITING FACULTY MEDICAL GRAND ROUNDS CME CREDIT HERBERT P. WIEDEMANN, MD Chairman, Department of Pulmonary, Allergy, and Critical Care Medicine,
TAKE-HOME POINTS FROM LECTURES BY CLEVELAND CLINIC AND VISITING FACULTY MEDICAL GRAND ROUNDS CME CREDIT HERBERT P. WIEDEMANN, MD Chairman, Department of Pulmonary, Allergy, and Critical Care Medicine,
Management of Severe ARDS: Current Canadian Practice
 Management of Severe ARDS: Current Canadian Practice Erick Duan MD FRCPC Clinical Scholar, Department of Medicine, Division of Critical Care, McMaster University Intensivist, St. Joseph's Healthcare Hamilton
Management of Severe ARDS: Current Canadian Practice Erick Duan MD FRCPC Clinical Scholar, Department of Medicine, Division of Critical Care, McMaster University Intensivist, St. Joseph's Healthcare Hamilton
Transpulmonary pressure measurement
 White Paper Transpulmonary pressure measurement Benefit of measuring transpulmonary pressure in mechanically ventilated patients Dr. Jean-Michel Arnal, Senior Intensivist, Hopital Sainte Musse, Toulon,
White Paper Transpulmonary pressure measurement Benefit of measuring transpulmonary pressure in mechanically ventilated patients Dr. Jean-Michel Arnal, Senior Intensivist, Hopital Sainte Musse, Toulon,
Efficacy and safety of intrapulmonary percussive ventilation superimposed on conventional ventilation in obese patients with compression atelectasis
 Journal of Critical Care (2006) 21, 328 332 Efficacy and safety of intrapulmonary percussive ventilation superimposed on conventional ventilation in obese patients with compression atelectasis Ryosuke
Journal of Critical Care (2006) 21, 328 332 Efficacy and safety of intrapulmonary percussive ventilation superimposed on conventional ventilation in obese patients with compression atelectasis Ryosuke
Difficult Ventilation in ARDS Patients
 Thank you for viewing this presentation. We would like to remind you that this material is the property of the author. It is provided to you by the ERS for your personal use only, as submitted by the author.
Thank you for viewing this presentation. We would like to remind you that this material is the property of the author. It is provided to you by the ERS for your personal use only, as submitted by the author.
Proportional Assist Ventilation (PAV) (NAVA) Younes ARRD 1992;145:114. Ventilator output :Triggering, Cycling Control of flow, rise time and pressure
 (NAVA) Younes ARRD 1992;145:114. Ventilator output :Triggering, Cycling Control of flow, rise time and pressure") Conflict of Interest Disclosure Robert M Kacmarek Unconventional Techniques Using Your ICU Ventilator!" 5-5-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston,
Conflict of Interest Disclosure Robert M Kacmarek Unconventional Techniques Using Your ICU Ventilator!" 5-5-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston,
1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation.
 Chapter 1: Principles of Mechanical Ventilation TRUE/FALSE 1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation. F
Chapter 1: Principles of Mechanical Ventilation TRUE/FALSE 1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation. F
Estimating afterload, systemic vascular resistance and pulmonary vascular resistance in an intensive care setting
 Estimating afterload, systemic vascular resistance and pulmonary vascular resistance in an intensive care setting David J. Stevenson James Revie Geoffrey J. Chase Geoffrey M. Shaw Bernard Lambermont Alexandre
Estimating afterload, systemic vascular resistance and pulmonary vascular resistance in an intensive care setting David J. Stevenson James Revie Geoffrey J. Chase Geoffrey M. Shaw Bernard Lambermont Alexandre
Respiratory insufficiency in bariatric patients
 Respiratory insufficiency in bariatric patients Special considerations or just more of the same? Weaning and rehabilation conference 6th November 2015 Definition of obesity Underweight BMI< 18 Normal weight
Respiratory insufficiency in bariatric patients Special considerations or just more of the same? Weaning and rehabilation conference 6th November 2015 Definition of obesity Underweight BMI< 18 Normal weight
Effectiveness and safety of a protocolized mechanical ventilation and weaning strategy of COPD patients by respiratory therapists
 Original Article Effectiveness and safety of a protocolized mechanical ventilation and weaning strategy of COPD patients by respiratory therapists Cenk Kirakli, Ozlem Ediboglu, Ilknur Naz, Pinar Cimen,
Original Article Effectiveness and safety of a protocolized mechanical ventilation and weaning strategy of COPD patients by respiratory therapists Cenk Kirakli, Ozlem Ediboglu, Ilknur Naz, Pinar Cimen,
This bibliography is a literature reference for users and represents selected relevant publications, without any claim to completeness.
 Bibliography INTELLiVENT-ASV This bibliography is a literature reference for users and represents selected relevant publications, without any claim to completeness. Table of Contents 1 Closed-loop ventilation
Bibliography INTELLiVENT-ASV This bibliography is a literature reference for users and represents selected relevant publications, without any claim to completeness. Table of Contents 1 Closed-loop ventilation
DESPITE recent advances in treatment strategies introduced during the last decade, adult respiratory distress
 Anesthesiology 2004; 101:620 5 2004 American Society of Anesthesiologists, Inc. Lippincott Williams & Wilkins, Inc. Recruitment Maneuvers after a Positive End-expiratory Pressure Trial Do Not Induce Sustained
Anesthesiology 2004; 101:620 5 2004 American Society of Anesthesiologists, Inc. Lippincott Williams & Wilkins, Inc. Recruitment Maneuvers after a Positive End-expiratory Pressure Trial Do Not Induce Sustained
Effect of peak inspiratory pressure on the development. of postoperative pulmonary complications.
 Effect of peak inspiratory pressure on the development of postoperative pulmonary complications in mechanically ventilated adult surgical patients: a systematic review protocol Chelsa Wamsley Donald Missel
Effect of peak inspiratory pressure on the development of postoperative pulmonary complications in mechanically ventilated adult surgical patients: a systematic review protocol Chelsa Wamsley Donald Missel
Respiratory failure requiring mechanical ventilation
 Current Issues in Mechanical Ventilation for Respiratory Failure* Neil R. MacIntyre, MD The morbidity and mortality associated with respiratory failure is, to a certain extent, iatrogenic. Mechanical ventilation,
Current Issues in Mechanical Ventilation for Respiratory Failure* Neil R. MacIntyre, MD The morbidity and mortality associated with respiratory failure is, to a certain extent, iatrogenic. Mechanical ventilation,
Test Bank Pilbeam's Mechanical Ventilation Physiological and Clinical Applications 6th Edition Cairo
 Instant dowload and all chapters Test Bank Pilbeam's Mechanical Ventilation Physiological and Clinical Applications 6th Edition Cairo https://testbanklab.com/download/test-bank-pilbeams-mechanical-ventilation-physiologicalclinical-applications-6th-edition-cairo/
Instant dowload and all chapters Test Bank Pilbeam's Mechanical Ventilation Physiological and Clinical Applications 6th Edition Cairo https://testbanklab.com/download/test-bank-pilbeams-mechanical-ventilation-physiologicalclinical-applications-6th-edition-cairo/
Steroids for ARDS. Clinical Problem. Management
 Steroids for ARDS James Beck Clinical Problem A 60 year old lady re-presented to ICU with respiratory failure. She had previously been admitted for fluid management and electrolyte correction having presented
Steroids for ARDS James Beck Clinical Problem A 60 year old lady re-presented to ICU with respiratory failure. She had previously been admitted for fluid management and electrolyte correction having presented
Prone Position in ARDS
 Prone Position in ARDS Rich Kallet MS RRT FAARC, FCCM Respiratory Care Services San Francisco General Hospital University of California, San Francisco, Case Study A 39 yo F admitted to SFGH TICU s/p hanging,
Prone Position in ARDS Rich Kallet MS RRT FAARC, FCCM Respiratory Care Services San Francisco General Hospital University of California, San Francisco, Case Study A 39 yo F admitted to SFGH TICU s/p hanging,
NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity
 NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Use of NIV 1998-2010 50 45 40 35 30 25 20 15 10 5 0 1998
NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Use of NIV 1998-2010 50 45 40 35 30 25 20 15 10 5 0 1998
Respiratory Mechanics
 Respiratory Mechanics Critical Care Medicine Specialty Board Tutorial Dr Arthur Chun-Wing LAU Associate Consultant Intensive Care Unit, Pamela Youde Nethersole Eastern Hospital, Hong Kong 17 th June 2014
Respiratory Mechanics Critical Care Medicine Specialty Board Tutorial Dr Arthur Chun-Wing LAU Associate Consultant Intensive Care Unit, Pamela Youde Nethersole Eastern Hospital, Hong Kong 17 th June 2014
Prone Position in ARDS
 Prone Position in ARDS Rich Kallet MS RRT FAARC, FCCM Respiratory Care Services Department of Anesthesia & Perioperative Care University of California, San Francisco, San Francisco General Hospital Case
Prone Position in ARDS Rich Kallet MS RRT FAARC, FCCM Respiratory Care Services Department of Anesthesia & Perioperative Care University of California, San Francisco, San Francisco General Hospital Case
Making sense of the pressure of arterial oxygen to fractional inspired oxygen concentration ratio in patients with acute respiratory distress syndrome
 Page 1 of 6 Optimizing Patient Care Making sense of the pressure of arterial oxygen to fractional inspired oxygen concentration ratio in patients with acute respiratory distress syndrome AF Broccard* Abstract
Page 1 of 6 Optimizing Patient Care Making sense of the pressure of arterial oxygen to fractional inspired oxygen concentration ratio in patients with acute respiratory distress syndrome AF Broccard* Abstract
Weaning from Mechanical Ventilation. Dr Azmin Huda Abdul Rahim
 Weaning from Mechanical Ventilation Dr Azmin Huda Abdul Rahim Content Definition Classification Weaning criteria Weaning methods Criteria for extubation Introduction Weaning comprises 40% of the duration
Weaning from Mechanical Ventilation Dr Azmin Huda Abdul Rahim Content Definition Classification Weaning criteria Weaning methods Criteria for extubation Introduction Weaning comprises 40% of the duration
NIV in hypoxemic patients
 NIV in hypoxemic patients Massimo Antonelli, MD Dept. of Intensive Care & Anesthesiology Università Cattolica del Sacro Cuore Rome - Italy Conflict of interest (research grants and consultations): Maquet
NIV in hypoxemic patients Massimo Antonelli, MD Dept. of Intensive Care & Anesthesiology Università Cattolica del Sacro Cuore Rome - Italy Conflict of interest (research grants and consultations): Maquet
INTELLiVENT -ASV insight. Alexandra Geiger CAS, Dr. Marc Wysocki, Head of Medical Research Hamilton Medical
 INTELLiVENT -ASV insight Alexandra Geiger CAS, Dr. Marc Wysocki, Head of Medical Research Hamilton Medical First Automation of HAMILTON MEDICAL 1998 Adaptive Support Ventilation (ASV) ASV optimize VT and
INTELLiVENT -ASV insight Alexandra Geiger CAS, Dr. Marc Wysocki, Head of Medical Research Hamilton Medical First Automation of HAMILTON MEDICAL 1998 Adaptive Support Ventilation (ASV) ASV optimize VT and
Monitor the patients disease pathology and response to therapy Estimate respiratory mechanics
 Understanding Graphics during Mechanical Ventilation Why Understand Ventilator Graphics? Waveforms are the graphic representation of the data collected by the ventilator and reflect the interaction between
Understanding Graphics during Mechanical Ventilation Why Understand Ventilator Graphics? Waveforms are the graphic representation of the data collected by the ventilator and reflect the interaction between
Neuromuscular Blockade in ARDS
 Neuromuscular Blockade in ARDS Maureen O. Meade, MD, FRCPC Critical care consultant, Hamilton Health Sciences Professor of Medicine, McMaster University www.oscillatetrial.com Disclosures None Possible
Neuromuscular Blockade in ARDS Maureen O. Meade, MD, FRCPC Critical care consultant, Hamilton Health Sciences Professor of Medicine, McMaster University www.oscillatetrial.com Disclosures None Possible
Driving Pressure and Survival in the Acute Respiratory Distress Syndrome
 Special Article Driving Pressure and Survival in the Acute Respiratory Distress Syndrome Marcelo B.P. Amato, M.D., Maureen O. Meade, M.D., Arthur S. Slutsky, M.D., Laurent Brochard, M.D., Eduardo L.V.
Special Article Driving Pressure and Survival in the Acute Respiratory Distress Syndrome Marcelo B.P. Amato, M.D., Maureen O. Meade, M.D., Arthur S. Slutsky, M.D., Laurent Brochard, M.D., Eduardo L.V.
PAOLO PELOSI, LAURA MARIA CHIERICHETTI, PAOLO SEVERGNINI
 MANAGEMENT OF WEANING EUROANESTHESIA 2005 Vienna, Austria 28-31 May 2005 12RC11 PAOLO PELOSI, LAURA MARIA CHIERICHETTI, PAOLO SEVERGNINI Dipartimento Ambiente, Salute e Sicurezza, Universita degli Studi
MANAGEMENT OF WEANING EUROANESTHESIA 2005 Vienna, Austria 28-31 May 2005 12RC11 PAOLO PELOSI, LAURA MARIA CHIERICHETTI, PAOLO SEVERGNINI Dipartimento Ambiente, Salute e Sicurezza, Universita degli Studi
ARDS: an update 6 th March A. Hakeem Al Hashim, MD, FRCP SQUH
 ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
A survey of the use of ventilator hyperinflation in Australian tertiary intensive care units
 A survey of the use of ventilator hyperinflation in Australian tertiary intensive care units Diane M Dennis, Wendy J Jacob and Fiona D Samuel Manual hyperinflation (MHI) or bagging has been used by physiotherapists
A survey of the use of ventilator hyperinflation in Australian tertiary intensive care units Diane M Dennis, Wendy J Jacob and Fiona D Samuel Manual hyperinflation (MHI) or bagging has been used by physiotherapists
MECHANICAL VENTILATION PROTOCOLS
 GENERAL or SURGICAL Initial Ventilator Parameters Ventilator Management (see appendix I) Assess Patient Data (see appendix II) Data Collection Mode: Tidal Volume: FIO2: PEEP: Rate: I:E Ratio: ACUTE PHASE
GENERAL or SURGICAL Initial Ventilator Parameters Ventilator Management (see appendix I) Assess Patient Data (see appendix II) Data Collection Mode: Tidal Volume: FIO2: PEEP: Rate: I:E Ratio: ACUTE PHASE
Effect of ARDS Severity and Etiology on Short-Term Outcomes
 Effect of ARDS Severity and Etiology on Short-Term Outcomes Haitham El-Haddad MD, Hyejeong Jang MSc, Wei Chen PhD, and Ayman O Soubani MD BACKGROUND: We evaluated the outcome of subjects with ARDS in relation
Effect of ARDS Severity and Etiology on Short-Term Outcomes Haitham El-Haddad MD, Hyejeong Jang MSc, Wei Chen PhD, and Ayman O Soubani MD BACKGROUND: We evaluated the outcome of subjects with ARDS in relation
Cardiorespiratory Physiotherapy Tutoring Services 2017
 VENTILATOR HYPERINFLATION ***This document is intended to be used as an information resource only it is not intended to be used as a policy document/practice guideline. Before incorporating the use of
VENTILATOR HYPERINFLATION ***This document is intended to be used as an information resource only it is not intended to be used as a policy document/practice guideline. Before incorporating the use of
GE Healthcare. Non Invasive Ventilation (NIV) For the Engström Ventilator. Relief, Relax, Recovery
 For the Engström Ventilator. Relief, Relax, Recovery") GE Healthcare Non Invasive Ventilation (NIV) For the Engström Ventilator Relief, Relax, Recovery COPD is currently the fourth leading cause of death in the world, and further increases in the prevalence
GE Healthcare Non Invasive Ventilation (NIV) For the Engström Ventilator Relief, Relax, Recovery COPD is currently the fourth leading cause of death in the world, and further increases in the prevalence
Management of refractory ARDS. Saurabh maji
 Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
ARDS: The Evidence. Topics. New definition Breaths: Little or Big? Wet or Dry? Moving or Still? Upside down or Right side up?
 ARDS: The Evidence Todd M Bull MD Professor of Medicine Division of Pulmonary Sciences and Critical Care Division of Cardiology Director Pulmonary Vascular Disease Center Director Center for Lungs and
ARDS: The Evidence Todd M Bull MD Professor of Medicine Division of Pulmonary Sciences and Critical Care Division of Cardiology Director Pulmonary Vascular Disease Center Director Center for Lungs and
Outcomes From Severe ARDS Managed Without ECMO. Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016
 Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
How the Knowledge Proceeds in Intensive Care: the ARDS Example
 How the Knowledge Proceeds in Intensive Care: the ARDS Example 2016, Antalya Luciano Gattinoni, MD, FRCP Georg-August-Universität Göttingen Germany INDUCTION: From particular (application) to general (law/theory)
How the Knowledge Proceeds in Intensive Care: the ARDS Example 2016, Antalya Luciano Gattinoni, MD, FRCP Georg-August-Universität Göttingen Germany INDUCTION: From particular (application) to general (law/theory)
APRV: An Update CHLOE STEINSHOUER, MD PULMONARY & SLEEP CONSULTANTS OF KANSAS 04/06/2017
 APRV: An Update CHLOE STEINSHOUER, MD PULMONARY & SLEEP CONSULTANTS OF KANSAS 04/06/2017 Disclosures No conflicts of interest Objectives Attendees will be able to: Define the mechanism of APRV Describe
APRV: An Update CHLOE STEINSHOUER, MD PULMONARY & SLEEP CONSULTANTS OF KANSAS 04/06/2017 Disclosures No conflicts of interest Objectives Attendees will be able to: Define the mechanism of APRV Describe
VENTILATOR GRAPHICS ver.2.0. Charles S. Williams RRT, AE-C
 VENTILATOR GRAPHICS ver.2.0 Charles S. Williams RRT, AE-C Purpose Graphics are waveforms that reflect the patientventilator system and their interaction. Purposes of monitoring graphics: Allow users to
VENTILATOR GRAPHICS ver.2.0 Charles S. Williams RRT, AE-C Purpose Graphics are waveforms that reflect the patientventilator system and their interaction. Purposes of monitoring graphics: Allow users to
Handling Common Problems & Pitfalls During. Oxygen desaturation in patients receiving mechanical ventilation ACUTE SEVERE RESPIRATORY FAILURE
 Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1.
Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1.
Agenda. Mechanical Ventilation in Morbidly Obese Patients. Paolo Pelosi. ESPCOP, Ostend, Belgium Saturday, November 14, 2009.
 Mechanical Ventilation in Morbidly Obese Patients t Paolo Pelosi Department of Ambient, Health and Safety University of Insubria - Varese, ITALY ppelosi@hotmail.com ESPCOP, Ostend, Belgium Saturday, November
Mechanical Ventilation in Morbidly Obese Patients t Paolo Pelosi Department of Ambient, Health and Safety University of Insubria - Varese, ITALY ppelosi@hotmail.com ESPCOP, Ostend, Belgium Saturday, November
17400 Medina Road, Suite 100 Phone: Minneapolis, MN Fax:
 17400 Medina Road, Suite 100 Phone: 763-398-8300 Minneapolis, MN 55447-1341 Fax: 763-398-8400 www.pulmonetic.com Clinical Bulletin To: Cc: From: Domestic Sales Representatives and International Distributors
17400 Medina Road, Suite 100 Phone: 763-398-8300 Minneapolis, MN 55447-1341 Fax: 763-398-8400 www.pulmonetic.com Clinical Bulletin To: Cc: From: Domestic Sales Representatives and International Distributors
ARDS and Lung Protection
 ARDS and Lung Protection Kristina Sullivan, MD Associate Professor University of California, San Francisco Department of Anesthesia and Perioperative Care Division of Critical Care Medicine Overview Low
ARDS and Lung Protection Kristina Sullivan, MD Associate Professor University of California, San Francisco Department of Anesthesia and Perioperative Care Division of Critical Care Medicine Overview Low
ACUTE RESPIRATORY DISTRESS SYNDROME CHALLENGES FOR TRANSLATIONAL RESEARCH AND OPPORTUNITIES FOR PRECISION MEDICINE
 ACUTE RESPIRATORY DISTRESS SYNDROME CHALLENGES FOR TRANSLATIONAL RESEARCH AND OPPORTUNITIES FOR PRECISION MEDICINE Acute respiratory distress syndrome: challenges for translational research and opportunities
ACUTE RESPIRATORY DISTRESS SYNDROME CHALLENGES FOR TRANSLATIONAL RESEARCH AND OPPORTUNITIES FOR PRECISION MEDICINE Acute respiratory distress syndrome: challenges for translational research and opportunities
Comparison of the SpO 2 /FIO 2 Ratio and the PaO 2 /FIO 2 Ratio in Patients With Acute Lung Injury or ARDS*
 CHEST Original Research Comparison of the SpO 2 /FIO 2 Ratio and the PaO 2 /FIO 2 Ratio in Patients With Acute Lung Injury or ARDS* Todd W. Rice, MD, MSc; Arthur P. Wheeler, MD, FCCP; Gordon R. Bernard,
CHEST Original Research Comparison of the SpO 2 /FIO 2 Ratio and the PaO 2 /FIO 2 Ratio in Patients With Acute Lung Injury or ARDS* Todd W. Rice, MD, MSc; Arthur P. Wheeler, MD, FCCP; Gordon R. Bernard,
Mechanical Ventilation Principles and Practices
 Mechanical Ventilation Principles and Practices Dr LAU Chun Wing Arthur Department of Intensive Care Pamela Youde Nethersole Eastern Hospital 6 October 2009 In this lecture, you will learn Major concepts
Mechanical Ventilation Principles and Practices Dr LAU Chun Wing Arthur Department of Intensive Care Pamela Youde Nethersole Eastern Hospital 6 October 2009 In this lecture, you will learn Major concepts
Biphasic Capnogram in a Single Lung Transplant Recipient A Case Report
 TITLE PAGE Biphasic Capnogram in a Single Lung Transplant Recipient A Case Report Authors: Hardeep S. Rai, MD, Cleveland Clinic, Respiratory Institute, Cleveland, OH 44195 Justin Boehm, RRT, Cleveland
TITLE PAGE Biphasic Capnogram in a Single Lung Transplant Recipient A Case Report Authors: Hardeep S. Rai, MD, Cleveland Clinic, Respiratory Institute, Cleveland, OH 44195 Justin Boehm, RRT, Cleveland
Variation in the Rapid Shallow Breathing Index Associated With Common Measurement Techniques and Conditions
 Variation in the Rapid Shallow Breathing Index Associated With Common Measurement Techniques and Conditions Kapil N Patel MD, Kalpesh D Ganatra MD, Jason HT Bates PhD, and Michael P Young MD BACKGROUND:
Variation in the Rapid Shallow Breathing Index Associated With Common Measurement Techniques and Conditions Kapil N Patel MD, Kalpesh D Ganatra MD, Jason HT Bates PhD, and Michael P Young MD BACKGROUND: