BMC Pulmonary Medicine
|
|
|
- Gervais Terry
- 5 years ago
- Views:
Transcription

1 BMC Pulmonary Medicine This Provisional PDF corresponds to the article as it appeared upon acceptance. Fully formatted PDF and full text (HTML) versions will be made available soon. Physiological relevance and performance of a minimal lung model -- an experimental study in healthy and acute respiratory distress syndrome model piglets BMC Pulmonary Medicine 2012, 12:59 doi: / Yeong Shiong Chiew (yeong.chiew@pg.canterbury.ac.nz) J.Geoffrey Chase (geoff.chase@canterbury.ac.nz) Bernard Lambermont (b.lambermont@chu.ulg.ac.be) Nathalie Janssen (njanssen@chu.ulg.ac.be) Christoph Schranz (scc@hs-furwangen.de) Knut Moeller (moe@hs-furwangen.de) Geoffrey M Shaw (geoff.shaw@chbd.govt.nz) Thomas Desaive (tdesaive@ulg.ac.be) ISSN Article type Technical advance Submission date 26 June 2012 Acceptance date 19 September 2012 Publication date 21 September 2012 Article URL Like all articles in BMC journals, this peer-reviewed article can be downloaded, printed and distributed freely for any purposes (see copyright notice below). Articles in BMC journals are listed in PubMed and archived at PubMed Central. For information about publishing your research in BMC journals or any BioMed Central journal, go to Chiew et al. ; licensee BioMed Central Ltd. This is an open access article distributed under the terms of the Creative Commons Attribution License ( which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
2 Physiological relevance and performance of a minimal lung model an experimental study in healthy and acute respiratory distress syndrome model piglets Yeong Shiong Chiew 1 yeong.chiew@pg.canterbury.ac.nz J Geoffrey Chase 1 geoff.chase@canterbury.ac.nz Bernard Lambermont 2 b.lambermont@chu.ulg.ac.be Nathalie Janssen 3 njanssen@chu.ulg.ac.be Christoph Schranz 4 scc@hs-furwangen.de Knut Moeller 4 moe@hs-furwangen.de Geoffrey M Shaw 5 geoff.shaw@chbd.govt.nz Thomas Desaive 6* * Corresponding author tdesaive@ulg.ac.be 1 Department of Mechanical Engineering, University of Canterbury, Christchurch, New Zealand 2 Medical Intensive Care Unit, University Hospital of Liege, Liege, Belgium 3 Emergency Department, University Hospital of Liege, Liege, Belgium 4 Institute for Technical Medicine, Furtwangen University, Villingen- Schwenningen, Germany 5 Department of Intensive Care, Christchurch Hospital, Christchurch, New Zealand 6 Thermodynamics of Irreversible Processes, Institute of Physics, University of Liege, Liege, Belgium
3 Abstract Background Mechanical ventilation (MV) is the primary form of support for acute respiratory distress syndrome (ARDS) patients. However, intra- and inter- patient-variability reduce the efficacy of general protocols. Model-based approaches to guide MV can be patient-specific. A physiological relevant minimal model and its patient-specific performance are tested to see if it meets this objective above. Methods Healthy anesthetized piglets weighing 24.0 kg [IQR: ] underwent a step-wise PEEP increase manoeuvre from 5cmH 2 O to 20cmH 2 O. They were ventilated under volume control using Engström Care Station (Datex, General Electric, Finland), with pressure, flow and volume profiles recorded. ARDS was then induced using oleic acid. The data were analyzed with a Minimal Model that identifies patient-specific mean threshold opening and closing pressure (TOP and TCP), and standard deviation (SD) of these TOP and TCP distributions. The trial and use of data were approved by the Ethics Committee of the Medical Faculty of the University of Liege, Belgium. Results and discussions 3 of the 9 healthy piglets developed ARDS, and these data sets were included in this study. Model fitting error during inflation and deflation, in healthy or ARDS state is less than 5.0% across all subjects, indicating that the model captures the fundamental lung mechanics during PEEP increase. Mean TOP was 42.4cmH 2 O [IQR: ] at PEEP = 5cmH 2 O and decreased with PEEP to 25.0cmH 2 O [IQR: ] at PEEP = 20cmH 2 O. In contrast, TCP sees a reverse trend, increasing from 10.2cmH 2 O [IQR: ] to 19.5cmH 2 O [IQR: ]. Mean TOP increased from average cmH 2 O to cmH 2 O between healthy and ARDS subjects, reflecting the higher pressure required to recruit collapsed alveoli. Mean TCP was effectively unchanged. Conclusion The minimal model is capable of capturing physiologically relevant TOP, TCP and SD of both healthy and ARDS lungs. The model is able to track disease progression and the response to treatment. Keywords ARDS, Recruitment Model, Animal Trials, Mechanical Ventilation Background Mechanical ventilation (MV) is extensively used in the intensive care unit (ICU), to support and assist patients diagnosed with acute respiratory distress syndrome (ARDS). These
4 patients have impaired lung function, and are extremely heterogeneous with significant interand intra- patient variation. Thus, patient-specific treatments are required to optimize outcome. Computer modeling can be used to identify and characterize patient-specific condition and guide clinical decisions [1-3]. Thus, the model s physiological relevance corresponding to the patient disease state is crucial for its applicability in clinical decision support. ARDS was first defined by Ashbaugh et al [4], as a consequence of variety of illness. They are characterized by fluid filled lungs (oedema), surfactant denature, causing alveolar instability and collapse, resulting in reduced in lung compliance and gas exchange [5]. A model that characterized the ARDS lung was proposed by Hickling [6]. It describes the lung as a collection of healthy and injured alveoli, distributed in layers subjected to a superimposed pressure. Healthy alveoli are normally open and assume a certain volume. Injured alveoli are collapsed and have no residual volume. They can be opened (recruited) with positive pressure through mechanical ventilation. Once opened, they will assume a volume similar to healthy alveoli. The opening and closing of collapsed alveoli are assumed to be governed by a normally distributed effective threshold opening pressure (TOP) and threshold closing pressure (TCP) [7,8]. Estimating the distribution of these parameters provides unique insight to patient-specific physiological condition, response to different MV treatment, and the opportunity to optimize patient-specific MV settings [9]. A healthy, spontaneously breathing lung normally has no collapsed alveoli. Thus, recruitment models are only considered applicable to characterize lung mechanics in ARDS or similar, which limits its application. A minimal model was proposed by Sundaresan et al using a similar, but modified recruitment concept and it was shown to be capable of monitoring the patient-disease state, predicting recruitment for changes in PEEP, and to guide MV therapy in the ICU [9,10]. It was able to identify physiologically relevant parameters that characterized patient-specific condition. However, the model is only used and tested in ARDS patients, and has yet to be validated for healthy lungs. In this study, an animal trial is carried out to test the model s physiological relevance and performance in both healthy and ARDS lungs. We hypothesize that the minimal model is able to represent both diseased and healthy lungs, as well as being able to monitor the progression of the disease state from the healthy case in a physiologically and clinically expected fashion. More specifically, it is assumed that the open alveoli in a healthy lung will have lower overall threshold opening pressures (lower mean TOP) compared to ARDS lungs, and that difference between healthy and ARDS states will be evident in lowered compliance and greater variability in threshold opening pressures (Higher standard deviation, SD). Satisfying these hypotheses would assist in validating the model s application in MV patient. Methods Subject preparation Experimental piglets were premedicated with tiletamin zolazepam 5 mg/kg and subsequently anaesthetized by a continuous infusion of sufentanil 0.5 μg/kg/h, pentobarbital 5 mg/kg/h and cisatracurium 2 mg/kg/h. They were ventilated through a tracheotomy under volume control (Tidal volume, Vt = 12 ml/kg) with inspired oxygen fraction (FiO 2 ) of 0.5 using Engström Care Station (Datex, General Electric, Finland).
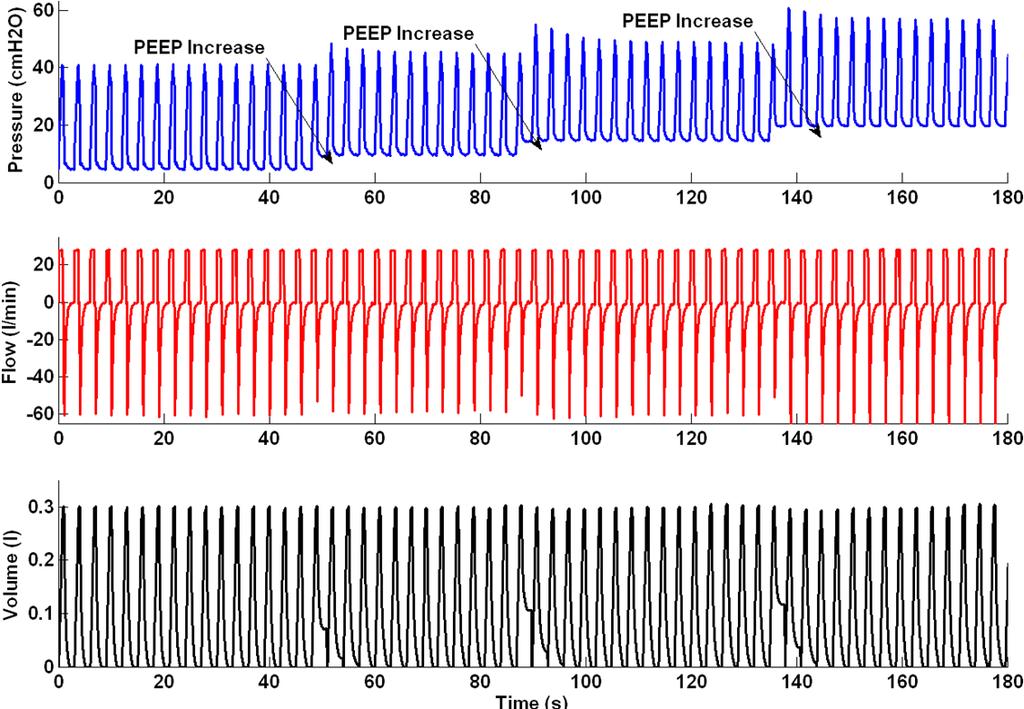
5 Protocol-based recruitment manoeuvre Each subject underwent a protocol-based step-wise PEEP (positive end-expiratory pressure) increase recruitment manoeuvre (RM). Subjects were initially ventilated at baseline PEEP of 5cmH 2 O. During the RM, PEEP was increased with a 5cmH 2 O step until 20cmH 2 O. Other ventilator settings were maintained throughout the RM. Each PEEP level was maintained for 10 ~ 15 breaths before increasing to a higher PEEP level. Figure 1 shows an example of the continuously recorded airway pressure and flow during the RM. Figure 1 Pressure, flow and volume profile during recruitment manoeuvre After the RM, PEEP was decreased step-wise to baseline PEEP at 5cmH 2 O. At this PEEP, the healthy pigs were then injected with oleic acid to induce ARDS. Oleic acid was administrated slowly at 0.1 ml for every 10 minutes interval until 0.1 ml/kg of the subject s weight. Arterial blood gases were monitored hourly, and, once diagnosed with ARDS, the subject underwent a second RM. In this study, ARDS criteria is limited to hypoxemia (PF ratio <200 mmhg). All experimental procedure, protocols and the use of data in this study were reviewed and approved by the Ethics Committee of the University of Liege Medical Faculty. Data processing A representative breath is selected from the last 2 breaths at each PEEP level, with the assumption of viscoelastic stabilization has occurred after PEEP increase. When PEEP increases from a lower to higher level, recruitment occurs and the deflation/unloading of the lung is not complete, with additional air trapped in lung. This recruitment or trapped volume is the estimated lung volume increase for the PEEP increment. Figure 2 shows an example of the estimated lung volume increase, and the associated post-processed pressure volume curve (PV) is shown in Figure 3. Figure 2 Estimation of volume increase during PEEP increment Figure 3 Example of pressure volume curves with volume increase with PEEP Model fitting and data analysis The PV curves were fitted to a minimal model [10] to identify model-based mean TOP and TCP, and the standard deviation (SD) of the TOP and TCP distributions. The minimal model is based on the concept of recruitment, and assumes the lung is a collection of lung units that are either open or collapsed. During inflation, if airway pressure exceeds a lung unit s effective TOP, the lung unit will assume a lung unit volume. Each opened unit volume is added to form the inflation PV curve. Similarly, if the airway pressure during deflation drops below the effective closing pressure, the lung unit collapses and loses the unit volume, which forms the deflation curve. Each lung unit has different effective opening pressure and closing pressure, and they are assumed normally distributed, so only a mean and SD of the distribution needs to be estimated [7,8,11]. The model summary is shown in Equation 1 and the details of the model can be found in [10]
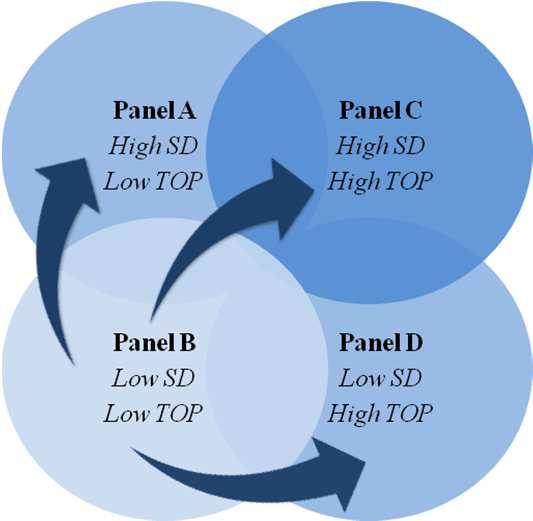
6 1 Pr essure Mean Volume Pressure 1 erf * Total Lung Capacity SD (1) Where erf is the Gaussian Error Function. In a TOP distribution, the mean of the distribution is the pressure when the maximum rate of recruitment occurs. The mean TOP also indicates the mean recruitable total lung units when ventilated at that pressure. Equally, the mean of TCP distribution indicates the maximum rate of derecruitment during deflation and, the mean lung units that will remain recruited during deflation. The SD describes the shape of the TOP/TCP distribution and is an indication of lung heterogeneity. SD reflects compliance and varies for a given subject, depending on the lung condition. Figure 4 shows examples of how different lung conditions affect the TOP distribution. The upper figures are the inspiratory PV curves and the lower figures the corresponding TOP distribution. A collapsed lung requires higher pressure to open/recruit the lung units, therefore, mean TOP thus increases as shown in Figure 4(a). The SD is the spread of the TOP distribution and thus, a heterogeneous lung will result in higher SD, as shown in Figure 4(b). Combination of TOP and SD will thus give the information of overall lung compliance. Similar concepts apply to the TCP distribution. Figure 4 Effect of TOP and SD towards a PV curve. (a) Normal lung to collapse Lung. (b) Normal lung to heterogeneous lung (Top PV curve during inflation, Bottom TOP distribution based on PV curves) In this study, the PV curves were fitted to clinical data using this minimal model [10]. Fitting errors are presented as mean absolute percentage error to indicate model performance. Wilcoxon rank-sum test is used to test for any statistical significance. Model-based mean TOP, TCP and SD in both healthy and ARDS states are compared to examine the effect of ARDS on model parameters, and their physiological and clinical relevance. Disease state grouping (DSG) The estimated patient-specific parameters (mean TOP and SD) can be used to group patients based on their disease state using the 4 panel disease state grouping metric (DSG) shown in Figure 5(a) and 5(b). In general, patients grouped in Panel B (low SD and TOP) are healthier compared to other panels. A decrease of SD or mean TOP indicate a less heterogeneous lung and/or an overall decrease in collapsed lung units. Figure 5(a) showed improvement in lung condition. Conversely, an increase of either of these parameters indicates that lung condition is worsening over time as shown in Figure 5(b). Hard boundaries are deliberately not shown as specific because it may be patient- or group-specific, and hard to define without debate with data available today. Figure 5 Patients-specific disease state grouping and tracking. (a) Lung is recovering over time. (b) Lung condition worsening
7 Results 9 piglets weighing median [Interquartile range (IQR)] 24.0 kg [IQR: ] were included in the study. 3 of 9 subjects reached an ARDS state (Subjects 5, 6 and 9) after oleic acid injection. Individual model parameters are compared between the healthy and ARDS state for these 3 piglets. The summary of model fitting during inflation or deflation for healthy and ARDS subjects is shown in Table 1. The details of Table 1 can be found in the Additional file 1: Table E1-E3. Table 1 Model fitting error (median [IQR]) during Inflation and Deflation at different PEEP levels for healthy and ARDS subjects Inflation Absolute Percentage Fitting Error (%) Median [IQR] PEEP 5 PEEP 10 PEEP 15 PEEP 20 Healthy State Inflation 6.59 [ ] 3.59 [ ] 2.55 [ ] 0.78 [ ] 3.06 [ ] Healthy State Deflation 9.86 [ ] 2.51 [ ] 1.37 [ ] 0.98 [ ] 1.78 [ ] ARDS State* Inflation [ ] ARDS State* Deflation [ ] *Fitting errors for ARDS state at PEEP 5, 10, 15 and 20cmH2O are average values instead of median [IQR] Table 2 shows the model estimated mean TOP and TCP at different PEEP for healthy subjects, and Table 3 for the ARDS subjects (5, 6 and 9). Table 4 shows the SD of the TOP and TCP distribution for the subjects which developed ARDS in both healthy and ARDS state. Table 2 Mean TOP and TCP for healthy subjects Subject Threshold Opening Pressure Threshold Closing Pressure (TOP, cmh 2 O) (TCP, cmh 2 O) PEEP 5 PEEP 10 PEEP 15 PEEP 20 PEEP 5 PEEP 10 PEEP 15 PEEP [ [ [ [ [ [ [ ] 40.0] 33.3] 27.1] 10.4] 13.5] 16.6] Median [IQR] 19.5 [ ] Table 3 Mean TOP and TCP for ARDS subjects Subject Threshold Opening Pressure Threshold Closing Pressure (TOP, cmh 2 O) (TCP, cmh 2 O) PEEP 5 PEEP 10 PEEP 15 PEEP 20 PEEP 5 PEEP 10 PEEP 15 PEEP Average
8 Table 4 SD in healthy and ARDS lung Subject Healthy ARDS Inflation Deflation Inflation Deflation Average Figure 6 shows the model fit to measured PV curves of a healthy subject, and the resulting TOP and TCP distributions at PEEP of 10cmH 2 O and 15cmH 2 O. An example of the PV curve shift from a healthy state to an ARDS state is shown in Figure 7 (Upper). The change in TOP and TCP distributions between healthy and ARDS state for the 3 subjects in Tables 2-3 is shown in Figure 7 (bottom). Figure 8 shows these changes in the disease state grouping (DSG) for Subjects 5, 6 and 9. Figure 6 Model Fitting with TOP and TCP distribution shift for healthy Subject 2. (Top - Model Fitting for PV curve in PEEP 10 and 15cmH 2 O, Bottom - TOP shifts left and TCP shifts right with PEEP increase Figure 7 Pressure-volume curve of Subject 5 and overall TOP and TCP comparison between healthy and ARDS. (Top - Inflation curve right shift from healthy to ARDS, Bottom - TOP in healthy lung is lower than in ARDS. Relatively little change in TCP during healthy and ARDS state) Figure 8 Mean TOP and SD change for healthy subject which later develop ARDS. (a) Subject 5, with slight increase of SD and TOP. (b) Subject 6, large increase of SD. (c) Subject 9, slight increase of SD with high TOP change Discussion The median fitting errors in healthy subjects during inflation and deflation were less than 3.1%. Similar to healthy subjects, the model fits well for ARDS subjects with median absolute percentage error during inflation and deflation less than 4.7%. There is a noticeable high median fitting error for ARDS subject 9 at PEEP 5cmH 2 O, at 27.32% during inflation. The model was not able to capture these specific physiological conditions at low PEEP. In particular, this case can be associated with the effect of Auto-PEEP distorting the actual lung condition [10]. The recruitment model fits better when Subject 9 is ventilated at higher PEEP (P < 0.005) compared to lower PEEP. However, the relatively low median error overall subjects indicates the model is capable of capturing fundamental mechanics of both healthy and ARDS lungs. Tables 2-3 show the estimated mean TOP and TCP for all the healthy and ARDS subjects. In healthy subjects, the overall mean TOP is decreased with increasing PEEP. Mean TCP increases with increasing PEEP. The TOP and TCP distribution shift of a subject during PEEP increase is observed in Figure 6 (Bottom), and are capturing the recruitment as expected. Similar mean TOP and TCP trends are also observed in ARDS subjects. However, an overall higher TOP is observed compared to healthy subjects, which is also expected for an ARDS
9 lung. The overall higher mean TOP indicates that the ARDS lung consists of relatively more collapsed alveoli and higher pressure is needed to recruit the collapsed alveoli. Healthy lungs normally consist of only opened or recruited lung units, and a model based on the concept of recruitment may not be applicable. However, in a healthy anesthetized and sedated subject, pulmonary atelectasis can be observed, but it is less severe compared to an ARDS lung and can be easily recruited [12-14]. Thus, during inflation, relatively lower pressure is needed to ventilate the healthy collapsed lung compared to ARDS lung. Therefore, for a given tidal volume, the area within the PV curve for a healthy lung should be smaller than ARDS lung. Equally, the healthy lung is less heterogeneous and the lower SD will keep the PV loop area smaller. Figure 7 shows a clear comparison of a healthy and ARDS PV curve, in which the ARDS PV curve has greater area than the healthy PV curve and correspondingly higher SD for this Subject 5 in Table 4. The change thus shows the expected higher work of breathing in the heterogeneous ARDS lung. Comparing the healthy and ARDS state, mean TOP for healthy lungs are lower when compared to ARDS lungs in Figure 7 (Bottom Left). A healthy lung is a less heterogeneous lung and the effect of superimposed pressure to alveoli is less detrimental. As suggested earlier, a healthy lung is normally open, which results in a lower mean TOP. Thus, the model captures the fact that, for the same subject at a healthy and ARDS state, higher pressure is required to recruit and open the lung. The inter-subject variability in this behavior is evident in Figure 8. Overall, these model results match clinical observation and expectation, which further validates the model. The deflation curve remains unchanged in ARDS compared to healthy subjects, as shown in Figure 7 (Top), which results in relatively no change in TCP, as seen in Figure 7 (Bottom Right) and Table 3. Hypothetically, mean TCP should be higher in the ARDS state compared to the healthy state [10,11]. ARDS lung units are more unstable and vulnerable to collapse. Thus, higher pressure is required to retain recruitment. However, this hypothesis was neither observed nor apparent in these results. Only a small increase in TCP is observed during ARDS state compared to healthy state as shown in Figure 7. The DSG for the ARDS subjects are shown in Figure 8. It is observed that all 3 subjects experienced different SD and TOP increase when transitioning from healthy to ARDS state. In particular, Subject 5 has a relatively small increase in both SD and TOP between healthy and ARDS state. Subject 6 had very large increase in SD (heterogeneity) but less change in TOP (Collapsed lung units). Subject 9 had a very high TOP change (Lung collapse) but minimal changes in SD (Heterogeneity). These results show the diversity in the impact of the ARDS induced. It is known that ARDS induced in animal model using oleic acid are highly variable [15]. A small variation in ventilation and hemodynamic management during preparation, time and dosage may alter the severity or extensiveness of the lung injury, resulting in different pathophysiological consequences [15-18]. That behavior is clearly evident in these results. Importantly, this research focuses on minimal model performance in healthy and ARDS lungs. Combining the DSG for all 3 subjects, as shown in Figure 8, the healthy subjects have overall lower TOP and SD than in the ARDS state. This finding suggests that the DSG application is not limited to patient-specific disease state tracking, and it is possible to be expanded into population monitoring. Capturing 3 different ARDS respiratory mechanics or
10 pathophysiological consequences, thus encourages the model s application in clinical setting, where the presentation of ARDS and its evolution over time and treatment can be variable. This DSG application is unique and observing DSG shifts should provide useful information for clinical decision support. For example, patients who are grouped in Panel D (High TOP, low SD), have a less heterogeneous lung, but with overall higher lung unit opening pressure. For example, it is hypothesized that a high PEEP can be used in MV to recruit overall collapsed lung units and improve gas exchange [19,20]. For patients who are grouped in Panel A (Low TOP, high SD), ventilation modes with 2 PEEP levels (Bi-Level PEEP ventilation, airway pressure release ventilation (APRV)) can reduce cyclic opening and collapse of lung units and improve patient outcome [21-23]. Tracking patient DSG with time will also show the effect and patient s response to specific treatment. In this research, the effect of oleic acid can be seen in increase of TOP and SD. However, the exact limits of these groupings remain to be determined, although it does not affect the ability to track patient condition and response to therapy as in Figure 8. Overall, the difference of mean TOP and SD between the healthy and ARDS state can be identified using the minimal model. The application of minimal model is not limited to the diseased lung, and allows comparison between healthy and ARDS lungs, and thus encourages its application and future investigation in the ICU to monitor patients-specific condition to guide MV therapy. An overall down shift of mean TOP and/or lowered SD will indicate that the lung recovering for injurious state. In contrast, an up-shift of TOP and/or SD, will show that the lung is more injured. This unique pair of metric thus provides the ability to track the disease state from healthy to injured state and vice-versa. However, mean TCP appears to have little change between healthy and ARDS state, indicating that the TCP parameter was less significant in this clinical use. Limitations ARDS piglets After oleic acid injections, only 3 of 9 subjects successfully developed ARDS. Others experienced hemodynamic failure before ARDS could develop fully or detected. This result shows that oleic acid induced ARDS animals are less reproducible and the subject preparation method should be re-examined [15,24-26]. The estimation and comparison of TOP, TCP and SD during healthy and ARDS state is thus, not conclusive with statistical significance given low subject numbers. However, individual data revealed that subjects that developed ARDS had overall higher TOP compared to subject in a healthy state. This physiologically relevant result is supported by past literature that examines similar clinical conditions [7,8,27]. In addition, all other results follow clinically expected trends. Ventilation tidal volume In this study, tidal volume is set to 12 ml/kg to ventilate the experimental piglets. It is known that such a high tidal volume is injurious with higher mortality [28]. However, the focus of the study is the investigation of the model s performance in healthy and ARDS states. During a healthy state, the recruitment manoeuvre with airway pressure and flow measurements were performed at the very beginning of the trial. This time frame is relatively short and thus, the effect of high tidal volume ventilation was minimal and likely did minimal or no damage.
11 Moreover, a more injurious ventilation strategy would indirectly benefit the overall study goals comparing healthy and damaged lung state. Estimation of the volume change The measurement of volume change was estimated during RM PEEP increase. The calculation method assumes that deflation of the lung is not fully complete and the air remained in the lung due to PEEP. This estimation based on Figure 2 may not be entirely true. However, direct measurement of the lung volume during short PEEP increases is not available at the bedside. In particular, FRC estimation using nitrogen washout requires several breathing cycles and a long stabilization period and thus, was not suitable in this trial or for regular clinical use (1-4 times per day). The volume change estimation is this study is thus a surrogate of the actual lung volume increase. This estimation method can be validated in future studies using nitrogen washin/washout method. However, all trends remain valid, and it is these changes that are critical here. Equally, low fitting errors indicate it did not appear to affect the model. Minimal model and patient DSG The minimal model is a model that estimates TOP, TCP and SD during PEEP titration of the mechanically ventilated. It is unable to predict the alveolar over-distension directly. However, the use of TOP mean shift as proposed by Sundaresan et al [9], it is possible to monitor the recruitability of the lung and thus, indirectly reveal potential over-distension that may cause lung injury. The DSG provides a unique metric to monitor patient s condition and potentially be used to guide ventilator settings. However, there are currently insufficient samples to validate this metric, or to prove the patients outcome for different TOP and SD. In particular, questions such as: what is the actual physiological findings in patients with particular SD/TOP value, what SD or TOP value are considered as high or low need to be addressed. Figure 8 is an example of the metric application, but there is insufficient information to determine which specific TOP/SD is high/low. In addition, the estimated TOP and SD in animals may be different if compared with human subjects. Future clinical trials or clinical PV data from other trials are required to validate this proof of concept. Conclusions The minimal model fits well in both healthy and ARDS lungs, and is capable of capturing the fundamental lung mechanics of the healthy and ARDS lung. The application of minimal model is thus not limited to diseased lung cases, but can be even used for healthy lungs. The model was able to estimate clinically and physiological relevant parameters for healthy and ARDS piglets thus allowing disease state tracking (DSG), which in turn reveals a potential to use this model to assist in clinical decision making. Abbreviations APRV, Airway release pressure ventilation; ARDS, Acute respiratory distress syndrome; DSG, Disease state grouping; FiO 2, Inspired oxygen fraction; ICU, Intensive care unit; IQR, Interquartile range; MV, Mechanical ventilation; PEEP, Positive end expiratory pressure; PV,
12 Pressure volume; RM, Recruitment manoeuvre; SD, Standard deviation; TCP, Threshold closing pressure; TOP, Threshold opening pressure; Vt, Tidal volume Competing interest The authors declare that they have no conflict of interest. Authors contributions YSC, GMS and JGC created and defined the model. BL, NJ and TD implemented trials clinically with input from all others. Every author had input in analysis of results, writing and revising the manuscript. All authors read and approved the final manuscript References 1. Rees S, Allerød C, Murley D, Zhao Y, Smith B, Kjærgaard S, Thorgaard P, Andreassen S: Using physiological models and decision theory for selecting appropriate ventilator settings. J Clin Monit Comput 2006, 20(6): Schranz C, Kno X, Bel C, Kretschmer J, Zhao Z, Mo, ller K: Hierarchical Parameter Identification in Models of Respiratory Mechanics. Biomedical Engineering, IEEE Transactions 2011, 58(11): Chase JG, Le Compte A, Preiser J-C, Shaw G, Penning S, Desaive T: Physiological modeling, tight glycemic control, and the ICU clinician: what are models and how can they affect practice? Annals of Intensive Care 2011, 1: Ashbaugh D, Boyd Bigelow D, Petty T, Levine B: ACUTE RESPIRATORY DISTRESS IN ADULTS. Lancet 1967, 290(7511): The ADTF: Acute respiratory distress syndrome: The berlin definition. JAMA: The Journal of the American Medical Association 2012, 307(23): Hickling Keith G: The Pressure-Volume Curve Is Greatly Modified by Recruitment. A Mathematical Model of ARDS Lungs. Am J Respir Crit Care Med 1998, 158(1): Crotti S, Mascheroni D, Caironi P, Pelosi P, Ronzoni G, Mondino M, Marini JJ, Gattinoni L: Recruitment and Derecruitment during Acute Respiratory Failure. A Clinical Study. Am J Respir Crit Care Med 2001, 164(1): Pelosi P, Goldner M, McKibben A, Adams A, Eccher G, Caironi P, Losappio S, Gattinoni L, Marini JJ: Recruitment and derecruitment during acute respiratory failure: an experimental study. Am J Respir Crit Care Med 2001, 164: Sundaresan A, Chase J, Shaw G, Chiew YS, Desaive T: Model-based optimal PEEP in mechanically ventilated ARDS patients in the Intensive Care Unit. BioMedical Engineering OnLine 2011, 10(1):64.
13 10. Sundaresan A, Yuta T, Hann CE, Geoffrey Chase J, Shaw GM: A minimal model of lung mechanics and model-based markers for optimizing ventilator treatment in ARDS patients. Computer Methods and Programs in Biomedicine 2009, 95(2): Pulletz S, Adler A, Kott M, Elke G, Gawelczyk B, Schädler D, Zick G, Weiler N, Frerichs I: Regional lung opening and closing pressures in patients with acute lung injury. J Crit Care 2012, 27(3):323.e e Tusman G, Böhm SH, de Anda GF V, Do Campo JL, Lachmann B: Alveolar recruitment strategy' improves arterial oxygenation during general anaesthesia. Br J Anaesth 1999, 82(1): Tusman G, Böhm SH, Warner DO, Sprung J: Atelectasis and perioperative pulmonary complications in high-risk patients. Current Opinion in Anesthesiology 2012, 25(1): Rusca M, Proietti S, Schnyder P, Frascarolo P, Hedenstierna G, Spahn DR, Magnusson L: Prevention of Atelectasis Formation During Induction of General Anesthesia. Anesth Analg 2003, 97(6): Schuster D: ARDS: clinical lessons from the oleic acid model of acute lung injury. Am J Respir Crit Care Med 1994, 149(1): Ballard-Croft C, Wang D, Sumpter LR, Zhou X, Zwischenberger JB: Large-Animal Models of Acute Respiratory Distress Syndrome. The Annals of Thoracic Surgery 2012, 93(4): Ware LB: Modeling human lung disease in animals. American Journal of Physiology - Lung Cellular and Molecular Physiology 2008, 294(2):L149 L Bastarache JA, Blackwell TS: Development of animal models for the acute respiratory distress syndrome. Disease Models & Mechanisms 2009, 2(5 6): Takeuchi M, Imanaka H, Tachibana K, Ogino H, Ando M, Nishimura M: Recruitment maneuver and high positive end-expiratory pressure improve hypoxemia in patients after pulmonary thromboendarterectomy for chronic pulmonary thromboembolism *. Crit Care Med 2005, 33(9): /2001.CCM DA. 20. Spieth P, Gama De Abreu M: Lung recruitment in ARDS: We are still confused, but on a higher PEEP level. Crit Care 2012, 16(1): Varpula T, Valta P, Niemi R, Takkunen O, Hynynen M, Pettilä V: Airway pressure release ventilation as a primary ventilatory mode in acute respiratory distress syndrome. Acta Anaesthesiologica Scandinavica 2004, 48(6): Barbas CSV, de Matos GFJ, Pincelli MP, da Rosa Borges E, Antunes T, de Barros JM, Okamoto V, Borges JB, Amato MBP, de Carvalho CR R: Mechanical ventilation in acute respiratory failure: recruitment and high positive end-expiratory pressure are necessary. Curr Opin Crit Care 2005, 11(1):18 28.
14 23. Brower RG, Lanken PN, MacIntyre N, Matthay MA, Morris A, Ancukiewicz M, Schoenfeld D, Thompson BT: Higher versus Lower Positive End-Expiratory Pressures in Patients with the Acute Respiratory Distress Syndrome. N Engl J Med 2004, 351(4): Julien M, Hoeffel JM, Flick MR: Oleic acid lung injury in sheep. J Appl Physiol 1986, 60(2): Grotjohan HP, van der Heijde RMJL, Jansen JRC, Wagenvoort CA, Versprille A: A stable model of respiratory distress by small injections of oleic acid in pigs. Intensive Care Med 1996, 22(4): Rosenthal C, Caronia C, Quinn C, Lugo N, Sagy M: A comparison among animal models of acute lung injury. Crit Care Med 1998, 26(5): Lu Q, Malbouisson LM, Mourgeon E, Goldstein I, Coriat P, Rouby JJ: Assessment of PEEP-induced reopening of collapsed lung regions in acute lung injury: are one or three CT sections representative of the entire lung? Intensive Care Med 2001, 27(9): The Acute Respiratory Distress Syndrome Network: Ventilation with Lower Tidal Volumes as Compared with Traditional Tidal Volumes for Acute Lung Injury and the Acute Respiratory Distress Syndrome. N Engl J Med 2000, 342(18): Additional file Additional_file_1 as DOCX Additional file 1 Table E1, E2 and E3 shows the detail information on model fitting error during inflation, deflation, healthy and ARDS state at different PEEP. Results are presented in median and interquartile range [IQR]. Table E4 shows the peak airway pressure for every subject at different PEEP. Table E5 shows the static compliance for every subject at different PEEP.
15 Figure 1
16 Figure 2
17 Figure 3
18 Figure 4 a b

19 Figure 5 a b
20 Figure 6
21 Figure 7

22 Figure 8 TOP and SD shift from Healthy State to ARDS State
23 Additional files provided with this submission: Additional file 1: _add1.docx, 30K
Physiological Relevance of a Minimal Model in Healthy Pigs Lung
 Physiological Relevance of a Minimal Model in Healthy Pigs Lung Yeong Shiong Chiew*, Thomas Desaive** Bernard Lambermont**, Nathalie Janssen**, Geoffrey M Shaw***, Christoph Schranz****, Knut Möller****,
Physiological Relevance of a Minimal Model in Healthy Pigs Lung Yeong Shiong Chiew*, Thomas Desaive** Bernard Lambermont**, Nathalie Janssen**, Geoffrey M Shaw***, Christoph Schranz****, Knut Möller****,
Analyzing Lung protective ventilation F Javier Belda MD, PhD Sº de Anestesiología y Reanimación. Hospital Clinico Universitario Valencia (Spain)
") Analyzing Lung protective ventilation F Javier Belda MD, PhD Sº de Anestesiología y Reanimación Hospital Clinico Universitario Valencia (Spain) ALI/ARDS Report of the American-European consensus conference
Analyzing Lung protective ventilation F Javier Belda MD, PhD Sº de Anestesiología y Reanimación Hospital Clinico Universitario Valencia (Spain) ALI/ARDS Report of the American-European consensus conference
Refresher Course MYTHS AND REALITY ABOUT LUNG MECHANICS 5 RC 2. European Society of Anaesthesiologists FIGURE 1 STATIC MEASUREMENTS
 European Society of Anaesthesiologists Refresher Course S AND ABOUT LUNG MECHANICS 5 RC 2 Anders LARSSON Gentofte University Hospital Copenhagen University Hellerup, Denmark Saturday May 31, 2003 Euroanaesthesia
European Society of Anaesthesiologists Refresher Course S AND ABOUT LUNG MECHANICS 5 RC 2 Anders LARSSON Gentofte University Hospital Copenhagen University Hellerup, Denmark Saturday May 31, 2003 Euroanaesthesia
APRV Ventilation Mode
 APRV Ventilation Mode Airway Pressure Release Ventilation A Type of CPAP Continuous Positive Airway Pressure (CPAP) with an intermittent release phase. Patient cycles between two levels of CPAP higher
APRV Ventilation Mode Airway Pressure Release Ventilation A Type of CPAP Continuous Positive Airway Pressure (CPAP) with an intermittent release phase. Patient cycles between two levels of CPAP higher
APRV: An Update CHLOE STEINSHOUER, MD PULMONARY & SLEEP CONSULTANTS OF KANSAS 04/06/2017
 APRV: An Update CHLOE STEINSHOUER, MD PULMONARY & SLEEP CONSULTANTS OF KANSAS 04/06/2017 Disclosures No conflicts of interest Objectives Attendees will be able to: Define the mechanism of APRV Describe
APRV: An Update CHLOE STEINSHOUER, MD PULMONARY & SLEEP CONSULTANTS OF KANSAS 04/06/2017 Disclosures No conflicts of interest Objectives Attendees will be able to: Define the mechanism of APRV Describe
Effect of peak inspiratory pressure on the development. of postoperative pulmonary complications.
 Effect of peak inspiratory pressure on the development of postoperative pulmonary complications in mechanically ventilated adult surgical patients: a systematic review protocol Chelsa Wamsley Donald Missel
Effect of peak inspiratory pressure on the development of postoperative pulmonary complications in mechanically ventilated adult surgical patients: a systematic review protocol Chelsa Wamsley Donald Missel
Airway pressure release ventilation (APRV) in PICU: Current evidence. Chor Yek Kee Sarawak General Hospital
 in PICU: Current evidence. Chor Yek Kee Sarawak General Hospital") Airway pressure release ventilation (APRV) in PICU: Current evidence Chor Yek Kee Sarawak General Hospital Outline Brief introduction of APRV History of APRV Common confusion in APRV Features of APRV and
Airway pressure release ventilation (APRV) in PICU: Current evidence Chor Yek Kee Sarawak General Hospital Outline Brief introduction of APRV History of APRV Common confusion in APRV Features of APRV and
Measuring End Expiratory Lung Volume after cardiac surgery
 (Acta Anaesth. Belg., 2012, 63, 115-120) Measuring End Expiratory Lung Volume after cardiac surgery G. MICHIELS (*), V. MARCHAL (**), D. LEDOUX (*) and P. DAMAS (*) Abstract. Background : The aim of this
(Acta Anaesth. Belg., 2012, 63, 115-120) Measuring End Expiratory Lung Volume after cardiac surgery G. MICHIELS (*), V. MARCHAL (**), D. LEDOUX (*) and P. DAMAS (*) Abstract. Background : The aim of this
Biomedical engineer s guide to the clinical aspects of intensive care mechanical ventilation
 https://doi.org/10.1186/s12938-018-0599-9 BioMedical Engineering OnLine REVIEW Open Access Biomedical engineer s guide to the clinical aspects of intensive care mechanical ventilation Vincent J. Major
https://doi.org/10.1186/s12938-018-0599-9 BioMedical Engineering OnLine REVIEW Open Access Biomedical engineer s guide to the clinical aspects of intensive care mechanical ventilation Vincent J. Major
ARDS: an update 6 th March A. Hakeem Al Hashim, MD, FRCP SQUH
 ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
Landmark articles on ventilation
 Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
Respiratory insufficiency in bariatric patients
 Respiratory insufficiency in bariatric patients Special considerations or just more of the same? Weaning and rehabilation conference 6th November 2015 Definition of obesity Underweight BMI< 18 Normal weight
Respiratory insufficiency in bariatric patients Special considerations or just more of the same? Weaning and rehabilation conference 6th November 2015 Definition of obesity Underweight BMI< 18 Normal weight
Protective ventilation for ALL patients
 Protective ventilation for ALL patients PAOLO PELOSI, MD, FERS Department of Surgical Sciences and Integrated Diagnostics (DISC), San Martino Policlinico Hospital IRCCS for Oncology, University of Genoa,
Protective ventilation for ALL patients PAOLO PELOSI, MD, FERS Department of Surgical Sciences and Integrated Diagnostics (DISC), San Martino Policlinico Hospital IRCCS for Oncology, University of Genoa,
Research Article A Patient-Specific Airway Branching Model for Mechanically Ventilated Patients
 Computational and Mathematical Methods in Medicine, Article ID 64573, 1 pages http://dx.doi.org/1.1155/14/64573 Research Article A Patient-Specific Airway Branching Model for Mechanically Ventilated Patients
Computational and Mathematical Methods in Medicine, Article ID 64573, 1 pages http://dx.doi.org/1.1155/14/64573 Research Article A Patient-Specific Airway Branching Model for Mechanically Ventilated Patients
Feasibility of titrating PEEP to minimum elastance for mechanically ventilated patients
 Pilot and Feasibility Studies This Provisional PDF corresponds to the article as it appeared upon acceptance. Fully formatted PDF and full text (HTML) versions will be made available soon. Feasibility
Pilot and Feasibility Studies This Provisional PDF corresponds to the article as it appeared upon acceptance. Fully formatted PDF and full text (HTML) versions will be made available soon. Feasibility
1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation.
 Chapter 1: Principles of Mechanical Ventilation TRUE/FALSE 1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation. F
Chapter 1: Principles of Mechanical Ventilation TRUE/FALSE 1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation. F
Agenda. Mechanical Ventilation in Morbidly Obese Patients. Paolo Pelosi. ESPCOP, Ostend, Belgium Saturday, November 14, 2009.
 Mechanical Ventilation in Morbidly Obese Patients t Paolo Pelosi Department of Ambient, Health and Safety University of Insubria - Varese, ITALY ppelosi@hotmail.com ESPCOP, Ostend, Belgium Saturday, November
Mechanical Ventilation in Morbidly Obese Patients t Paolo Pelosi Department of Ambient, Health and Safety University of Insubria - Varese, ITALY ppelosi@hotmail.com ESPCOP, Ostend, Belgium Saturday, November
Feasibility of titrating PEEP to minimum elastance for mechanically ventilated patients
 Chiew et al. Pilot and Feasibility Studies (2015) 1:9 DOI 10.1186/s40814-015-0006-2 RESEARCH Open Access Feasibility of titrating PEEP to minimum elastance for mechanically ventilated patients Yeong Shiong
Chiew et al. Pilot and Feasibility Studies (2015) 1:9 DOI 10.1186/s40814-015-0006-2 RESEARCH Open Access Feasibility of titrating PEEP to minimum elastance for mechanically ventilated patients Yeong Shiong
Lung Recruitment Strategies in Anesthesia
 Lung Recruitment Strategies in Anesthesia Intraoperative ventilatory management to prevent Post-operative Pulmonary Complications Kook-Hyun Lee, MD, PhD Department of Anesthesiology Seoul National University
Lung Recruitment Strategies in Anesthesia Intraoperative ventilatory management to prevent Post-operative Pulmonary Complications Kook-Hyun Lee, MD, PhD Department of Anesthesiology Seoul National University
Ventilatory Management of ARDS. Alexei Ortiz Milan; MD, MSc
 Ventilatory Management of ARDS Alexei Ortiz Milan; MD, MSc 2017 Outline Ventilatory management of ARDS Protected Ventilatory Strategy Use of NMB Selection of PEEP Driving pressure Lung Recruitment Prone
Ventilatory Management of ARDS Alexei Ortiz Milan; MD, MSc 2017 Outline Ventilatory management of ARDS Protected Ventilatory Strategy Use of NMB Selection of PEEP Driving pressure Lung Recruitment Prone
Dr. Yasser Fathi M.B.B.S, M.Sc, M.D. Anesthesia Consultant, Head of ICU King Saud Hospital, Unaizah
 BY Dr. Yasser Fathi M.B.B.S, M.Sc, M.D Anesthesia Consultant, Head of ICU King Saud Hospital, Unaizah Objectives For Discussion Respiratory Physiology Pulmonary Graphics BIPAP Graphics Trouble Shootings
BY Dr. Yasser Fathi M.B.B.S, M.Sc, M.D Anesthesia Consultant, Head of ICU King Saud Hospital, Unaizah Objectives For Discussion Respiratory Physiology Pulmonary Graphics BIPAP Graphics Trouble Shootings
Should the ART trial change our practice?
 Editorial Should the ART trial change our practice? Jesús Villar 1,2,3, Fernando Suárez-Sipmann 1,4,5, Robert M. Kacmarek 6,7 1 CIBER de Enfermedades Respiratorias, Instituto de Salud Carlos III, Madrid,
Editorial Should the ART trial change our practice? Jesús Villar 1,2,3, Fernando Suárez-Sipmann 1,4,5, Robert M. Kacmarek 6,7 1 CIBER de Enfermedades Respiratorias, Instituto de Salud Carlos III, Madrid,
11 th Annual Congress Turkish Thoracic Society. Mechanical Ventilation in Acute Hypoxemic Respiratory Failure
 11 th Annual Congress Turkish Thoracic Society Mechanical Ventilation in Acute Hypoxemic Respiratory Failure Lluis Blanch MD PhD Senior Critical Care Center Scientific Director Corporació Parc Taulí Universitat
11 th Annual Congress Turkish Thoracic Society Mechanical Ventilation in Acute Hypoxemic Respiratory Failure Lluis Blanch MD PhD Senior Critical Care Center Scientific Director Corporació Parc Taulí Universitat
ARDS Management Protocol
 ARDS Management Protocol February 2018 ARDS Criteria Onset Within 1 week of a known clinical insult or new or worsening respiratory symptoms Bilateral opacities not fully explained by effusions, lobar/lung
ARDS Management Protocol February 2018 ARDS Criteria Onset Within 1 week of a known clinical insult or new or worsening respiratory symptoms Bilateral opacities not fully explained by effusions, lobar/lung
Management of refractory ARDS. Saurabh maji
 Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
Multi-Scale Pulmonary Modelling. and Clinical Applications
 Multi-Scale Pulmonary Modelling and Clinical Applications Nor Salwa Damanhuri A thesis submitted for the degree of Doctor of Philosophy in BioEngineering at the University of Canterbury, Christchurch,
Multi-Scale Pulmonary Modelling and Clinical Applications Nor Salwa Damanhuri A thesis submitted for the degree of Doctor of Philosophy in BioEngineering at the University of Canterbury, Christchurch,
Ventilator ECMO Interactions
 Ventilator ECMO Interactions Lorenzo Del Sorbo, MD CCCF Toronto, October 2 nd 2017 Disclosure Relevant relationships with commercial entities: none Potential for conflicts within this presentation: none
Ventilator ECMO Interactions Lorenzo Del Sorbo, MD CCCF Toronto, October 2 nd 2017 Disclosure Relevant relationships with commercial entities: none Potential for conflicts within this presentation: none
Monitor the patients disease pathology and response to therapy Estimate respiratory mechanics
 Understanding Graphics during Mechanical Ventilation Why Understand Ventilator Graphics? Waveforms are the graphic representation of the data collected by the ventilator and reflect the interaction between
Understanding Graphics during Mechanical Ventilation Why Understand Ventilator Graphics? Waveforms are the graphic representation of the data collected by the ventilator and reflect the interaction between
How ARDS should be treated in 2017
 How ARDS should be treated in 2017 2017, Ostrava Luciano Gattinoni, MD, FRCP Georg-August-Universität Göttingen Germany ARDS 1. Keep the patient alive respiration circulation 2. Cure the disease leading
How ARDS should be treated in 2017 2017, Ostrava Luciano Gattinoni, MD, FRCP Georg-August-Universität Göttingen Germany ARDS 1. Keep the patient alive respiration circulation 2. Cure the disease leading
Tracking lung recruitment and regional tidal volume at the bedside. Antonio Pesenti
 Tracking lung recruitment and regional tidal volume at the bedside Antonio Pesenti Conflicts of Interest Maquet: Received research support and consultation fees Drager: Received research support and consultation
Tracking lung recruitment and regional tidal volume at the bedside Antonio Pesenti Conflicts of Interest Maquet: Received research support and consultation fees Drager: Received research support and consultation
Recruitment Maneuvers and Higher PEEP, the So-Called Open Lung Concept, in Patients with ARDS
 Zee and Gommers Critical Care (2019) 23:73 https://doi.org/10.1186/s13054-019-2365-1 REVIEW Recruitment Maneuvers and Higher PEEP, the So-Called Open Lung Concept, in Patients with ARDS Philip van der
Zee and Gommers Critical Care (2019) 23:73 https://doi.org/10.1186/s13054-019-2365-1 REVIEW Recruitment Maneuvers and Higher PEEP, the So-Called Open Lung Concept, in Patients with ARDS Philip van der
Recognizing and Correcting Patient-Ventilator Dysynchrony
 2019 KRCS Annual State Education Seminar Recognizing and Correcting Patient-Ventilator Dysynchrony Eric Kriner BS,RRT Pulmonary Critical Care Clinical Specialist MedStar Washington Hospital Center Washington,
2019 KRCS Annual State Education Seminar Recognizing and Correcting Patient-Ventilator Dysynchrony Eric Kriner BS,RRT Pulmonary Critical Care Clinical Specialist MedStar Washington Hospital Center Washington,
Cardiorespiratory Physiotherapy Tutoring Services 2017
 VENTILATOR HYPERINFLATION ***This document is intended to be used as an information resource only it is not intended to be used as a policy document/practice guideline. Before incorporating the use of
VENTILATOR HYPERINFLATION ***This document is intended to be used as an information resource only it is not intended to be used as a policy document/practice guideline. Before incorporating the use of
Higher PEEP improves outcomes in ARDS patients with clinically objective positive oxygenation response to PEEP: a systematic review and meta-analysis
 Guo et al. BMC Anesthesiology (2018) 18:172 https://doi.org/10.1186/s12871-018-0631-4 RESEARCH ARTICLE Open Access Higher PEEP improves outcomes in ARDS patients with clinically objective positive oxygenation
Guo et al. BMC Anesthesiology (2018) 18:172 https://doi.org/10.1186/s12871-018-0631-4 RESEARCH ARTICLE Open Access Higher PEEP improves outcomes in ARDS patients with clinically objective positive oxygenation
A Clinician s View of Engineering and Technology in Intensive Care - Modelbased Therapeutics and Patient Outcomes
 A Clinician s View of Engineering and Technology in Intensive Care - Modelbased Therapeutics and Patient Outcomes Shaw GM*, Chase JG**, Hann CE** *Christchurch Hospital Intensive Care Unit, Christchurch,
A Clinician s View of Engineering and Technology in Intensive Care - Modelbased Therapeutics and Patient Outcomes Shaw GM*, Chase JG**, Hann CE** *Christchurch Hospital Intensive Care Unit, Christchurch,
The use of proning in the management of Acute Respiratory Distress Syndrome
 Case 3 The use of proning in the management of Acute Respiratory Distress Syndrome Clinical Problem This expanded case summary has been chosen to explore the rationale and evidence behind the use of proning
Case 3 The use of proning in the management of Acute Respiratory Distress Syndrome Clinical Problem This expanded case summary has been chosen to explore the rationale and evidence behind the use of proning
Outline. Basic principles of lung protective ventilation. The challenging areas. Small tidal volumes Recruitment
 ARDS beyond 6/kg Gordon D. Rubenfeld, MD MSc Professor of Medicine, University of Toronto Chief, Program in Trauma, Emergency, and Critical Care Sunnybrook Health Sciences Centre Outline Basic principles
ARDS beyond 6/kg Gordon D. Rubenfeld, MD MSc Professor of Medicine, University of Toronto Chief, Program in Trauma, Emergency, and Critical Care Sunnybrook Health Sciences Centre Outline Basic principles
Application of Lung Protective Ventilation MUST Begin Immediately After Intubation
 Conflict of Interest Disclosure Robert M Kacmarek Managing Severe Hypoxemia!" 9-28-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts I disclose
Conflict of Interest Disclosure Robert M Kacmarek Managing Severe Hypoxemia!" 9-28-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts I disclose
PULMONARY FUNCTION TESTING. Purposes of Pulmonary Tests. General Categories of Lung Diseases. Types of PF Tests
 PULMONARY FUNCTION TESTING Wyka Chapter 13 Various AARC Clinical Practice Guidelines Purposes of Pulmonary Tests Is lung disease present? If so, is it reversible? If so, what type of lung disease is present?
PULMONARY FUNCTION TESTING Wyka Chapter 13 Various AARC Clinical Practice Guidelines Purposes of Pulmonary Tests Is lung disease present? If so, is it reversible? If so, what type of lung disease is present?
ARDS and Lung Protection
 ARDS and Lung Protection Kristina Sullivan, MD Associate Professor University of California, San Francisco Department of Anesthesia and Perioperative Care Division of Critical Care Medicine Overview Low
ARDS and Lung Protection Kristina Sullivan, MD Associate Professor University of California, San Francisco Department of Anesthesia and Perioperative Care Division of Critical Care Medicine Overview Low
Noninvasive respiratory support:why is it working?
 Noninvasive respiratory support:why is it working? Paolo Pelosi Department of Surgical Sciences and Integrated Diagnostics (DISC) IRCCS San Martino IST University of Genoa, Genoa, Italy ppelosi@hotmail.com
Noninvasive respiratory support:why is it working? Paolo Pelosi Department of Surgical Sciences and Integrated Diagnostics (DISC) IRCCS San Martino IST University of Genoa, Genoa, Italy ppelosi@hotmail.com
Sub-category: Intensive Care for Respiratory Distress
 Course n : Course 3 Title: RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE Sub-category: Intensive Care for Respiratory Distress Topic: Acute Respiratory Distress
Course n : Course 3 Title: RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE Sub-category: Intensive Care for Respiratory Distress Topic: Acute Respiratory Distress
QuickLung Breather Patient Settings
 The QuickLung Breather is capable of simulating a spontaneously breathing patient in a variety of modes and patterns. In response to customer requests, we have compiled five common respiratory cases below.
The QuickLung Breather is capable of simulating a spontaneously breathing patient in a variety of modes and patterns. In response to customer requests, we have compiled five common respiratory cases below.
Estimating afterload, systemic vascular resistance and pulmonary vascular resistance in an intensive care setting
 Estimating afterload, systemic vascular resistance and pulmonary vascular resistance in an intensive care setting David J. Stevenson James Revie Geoffrey J. Chase Geoffrey M. Shaw Bernard Lambermont Alexandre
Estimating afterload, systemic vascular resistance and pulmonary vascular resistance in an intensive care setting David J. Stevenson James Revie Geoffrey J. Chase Geoffrey M. Shaw Bernard Lambermont Alexandre
DESPITE recent advances in treatment strategies introduced during the last decade, adult respiratory distress
 Anesthesiology 2004; 101:620 5 2004 American Society of Anesthesiologists, Inc. Lippincott Williams & Wilkins, Inc. Recruitment Maneuvers after a Positive End-expiratory Pressure Trial Do Not Induce Sustained
Anesthesiology 2004; 101:620 5 2004 American Society of Anesthesiologists, Inc. Lippincott Williams & Wilkins, Inc. Recruitment Maneuvers after a Positive End-expiratory Pressure Trial Do Not Induce Sustained
What is the next best step?
 Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
All rights, in particular the proprietary rights of use and exploitation relating to the following contribution as well as parts thereof (including
 All rights, in particular the proprietary rights of use and exploitation relating to the following contribution as well as parts thereof (including figures and tables) are the exclusive property of Springer
All rights, in particular the proprietary rights of use and exploitation relating to the following contribution as well as parts thereof (including figures and tables) are the exclusive property of Springer
ACUTE RESPIRATORY DISTRESS SYNDROME
 ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
Available online at ScienceDirect. IFAC-PapersOnLine (2015)
") Available online at www.sciencedirect.com ScienceDirect IFAC-PapersOnLine 48-20 (2015) 273 278 Reducing the Length of Mechanical Ventilation with Significance: A Case Study of Sample Size Estimation Trial
Available online at www.sciencedirect.com ScienceDirect IFAC-PapersOnLine 48-20 (2015) 273 278 Reducing the Length of Mechanical Ventilation with Significance: A Case Study of Sample Size Estimation Trial
British Journal of Anaesthesia 104 (5): (2010) doi: /bja/aeq080 Advance Access publication March 30, 2010
: (2010) doi: /bja/aeq080 Advance Access publication March 30, 2010") RESPIRATION AND THE AIRWAY Lung recruitment and positive airway pressure before extubation does not improve oxygenation in the post-anaesthesia care unit: a randomized clinical trial A. B. Lumb 1, S. J.
RESPIRATION AND THE AIRWAY Lung recruitment and positive airway pressure before extubation does not improve oxygenation in the post-anaesthesia care unit: a randomized clinical trial A. B. Lumb 1, S. J.
Efficacy and safety of intrapulmonary percussive ventilation superimposed on conventional ventilation in obese patients with compression atelectasis
 Journal of Critical Care (2006) 21, 328 332 Efficacy and safety of intrapulmonary percussive ventilation superimposed on conventional ventilation in obese patients with compression atelectasis Ryosuke
Journal of Critical Care (2006) 21, 328 332 Efficacy and safety of intrapulmonary percussive ventilation superimposed on conventional ventilation in obese patients with compression atelectasis Ryosuke
Proportional Assist Ventilation (PAV) (NAVA) Younes ARRD 1992;145:114. Ventilator output :Triggering, Cycling Control of flow, rise time and pressure
 (NAVA) Younes ARRD 1992;145:114. Ventilator output :Triggering, Cycling Control of flow, rise time and pressure") Conflict of Interest Disclosure Robert M Kacmarek Unconventional Techniques Using Your ICU Ventilator!" 5-5-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston,
Conflict of Interest Disclosure Robert M Kacmarek Unconventional Techniques Using Your ICU Ventilator!" 5-5-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston,
Ventilation in Paediatric ARDS: extrapolate from adult studies?
 Ventilation in Paediatric ARDS: extrapolate from adult studies? ASMIC 2014 Dr Adrian Plunkett Consultant Paediatric Intensivist Birmingham Children s Hospital, UK Aims of the presentation Ventilation
Ventilation in Paediatric ARDS: extrapolate from adult studies? ASMIC 2014 Dr Adrian Plunkett Consultant Paediatric Intensivist Birmingham Children s Hospital, UK Aims of the presentation Ventilation
Weaning from Mechanical Ventilation. Dr Azmin Huda Abdul Rahim
 Weaning from Mechanical Ventilation Dr Azmin Huda Abdul Rahim Content Definition Classification Weaning criteria Weaning methods Criteria for extubation Introduction Weaning comprises 40% of the duration
Weaning from Mechanical Ventilation Dr Azmin Huda Abdul Rahim Content Definition Classification Weaning criteria Weaning methods Criteria for extubation Introduction Weaning comprises 40% of the duration
Bronchoalveolar lavage (BAL) with surfactant in pediatric ARDS
 with surfactant in pediatric ARDS") Bronchoalveolar lavage (BAL) with surfactant in pediatric ARDS M. Luchetti, E. M. Galassini, A. Galbiati, C. Pagani,, F. Silla and G. A. Marraro gmarraro@picu.it www.picu.it Anesthesia and Intensive Care
Bronchoalveolar lavage (BAL) with surfactant in pediatric ARDS M. Luchetti, E. M. Galassini, A. Galbiati, C. Pagani,, F. Silla and G. A. Marraro gmarraro@picu.it www.picu.it Anesthesia and Intensive Care
The Art and Science of Weaning from Mechanical Ventilation
 The Art and Science of Weaning from Mechanical Ventilation Shekhar T. Venkataraman M.D. Professor Departments of Critical Care Medicine and Pediatrics University of Pittsburgh School of Medicine Some definitions
The Art and Science of Weaning from Mechanical Ventilation Shekhar T. Venkataraman M.D. Professor Departments of Critical Care Medicine and Pediatrics University of Pittsburgh School of Medicine Some definitions
Respiratory Physiology In-Lab Guide
 Respiratory Physiology In-Lab Guide Read Me Study Guide Check Your Knowledge, before the Practical: 1. Understand the relationship between volume and pressure. Understand the three respiratory pressures
Respiratory Physiology In-Lab Guide Read Me Study Guide Check Your Knowledge, before the Practical: 1. Understand the relationship between volume and pressure. Understand the three respiratory pressures
Original Article Effects of prone position on lung function of patients undergoing mechanical ventilation under total intravenous anesthesia
 Int J Clin Exp Med 2017;10(4):6769-6774 www.ijcem.com /ISSN:1940-5901/IJCEM0045140 Original Article Effects of prone position on lung function of patients undergoing mechanical ventilation under total
Int J Clin Exp Med 2017;10(4):6769-6774 www.ijcem.com /ISSN:1940-5901/IJCEM0045140 Original Article Effects of prone position on lung function of patients undergoing mechanical ventilation under total
The Influence of Altered Pulmonarv
 The Influence of Altered Pulmonarv J Mechanics on the Adequacy of Controlled Ventilation Peter Hutchin, M.D., and Richard M. Peters, M.D. W ' hereas during spontaneous respiration the individual determines
The Influence of Altered Pulmonarv J Mechanics on the Adequacy of Controlled Ventilation Peter Hutchin, M.D., and Richard M. Peters, M.D. W ' hereas during spontaneous respiration the individual determines
Estimating afterload, systemic vascular resistance and pulmonary vascular resistance in an intensive care setting
 Estimating afterload, systemic vascular resistance and pulmonary vascular resistance in an intensive care setting David J. Stevenson James Revie Geoffrey J. Chase Geoffrey M. Shaw Bernard Lambermont Alexandre
Estimating afterload, systemic vascular resistance and pulmonary vascular resistance in an intensive care setting David J. Stevenson James Revie Geoffrey J. Chase Geoffrey M. Shaw Bernard Lambermont Alexandre
ARDS & TBI - Trading Off Ventilation Targets
 ARDS & TBI - Trading Off Ventilation Targets Salvatore M. Maggiore, MD, PhD Rome, Italy smmaggiore@rm.unicatt.it Conflict of interest Principal Investigator: RINO trial o Nasal high-flow vs Venturi mask
ARDS & TBI - Trading Off Ventilation Targets Salvatore M. Maggiore, MD, PhD Rome, Italy smmaggiore@rm.unicatt.it Conflict of interest Principal Investigator: RINO trial o Nasal high-flow vs Venturi mask
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv
 Rv") ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ARDS Assisted ventilation and prone position. ICU Fellowship Training Radboudumc
 ARDS Assisted ventilation and prone position ICU Fellowship Training Radboudumc Fig. 1 Physiological mechanisms controlling respiratory drive and clinical consequences of inappropriate respiratory drive
ARDS Assisted ventilation and prone position ICU Fellowship Training Radboudumc Fig. 1 Physiological mechanisms controlling respiratory drive and clinical consequences of inappropriate respiratory drive
Prone Position in ARDS
 Prone Position in ARDS Rich Kallet MS RRT FAARC, FCCM Respiratory Care Services San Francisco General Hospital University of California, San Francisco, Case Study A 39 yo F admitted to SFGH TICU s/p hanging,
Prone Position in ARDS Rich Kallet MS RRT FAARC, FCCM Respiratory Care Services San Francisco General Hospital University of California, San Francisco, Case Study A 39 yo F admitted to SFGH TICU s/p hanging,
Oxygenation Failure. Increase FiO2. Titrate end-expiratory pressure. Adjust duty cycle to increase MAP. Patient Positioning. Inhaled Vasodilators
 Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
WE know that medicine cannot always be a provided
 Acta Anaesthesiol Scand 2004; 48: 267 271 Copyright # Acta Anaesthesiol Scand 2004 Printed in Denmark. All rights reserved ACTA ANAESTHESIOLOGICA SCANDINAVICA Review Article From ventilator-induced lung
Acta Anaesthesiol Scand 2004; 48: 267 271 Copyright # Acta Anaesthesiol Scand 2004 Printed in Denmark. All rights reserved ACTA ANAESTHESIOLOGICA SCANDINAVICA Review Article From ventilator-induced lung
Literature List Electrical Impedance Tomography
 Literature List Electrical Impedance Tomography 2017 Electrical Impedance Tomography (EIT) Literature List 2017 INDEX Writer Subject Publication Page Piraino T, Fan E Acute life-threatening hypoxemia during
Literature List Electrical Impedance Tomography 2017 Electrical Impedance Tomography (EIT) Literature List 2017 INDEX Writer Subject Publication Page Piraino T, Fan E Acute life-threatening hypoxemia during
«Best» PEEP? Physiologic? Therapeutic? Optimal? Super? Preferred? Minimal? Right? Protective? Prophylactic?
 1936-2005 «Best» PEEP? Physiologic? Therapeutic? Optimal? Super? Preferred? Minimal? Right? Protective? Prophylactic? 1990-2000 Post cardiac arrest First day of mechanical ventilation 1990-1991 No patient
1936-2005 «Best» PEEP? Physiologic? Therapeutic? Optimal? Super? Preferred? Minimal? Right? Protective? Prophylactic? 1990-2000 Post cardiac arrest First day of mechanical ventilation 1990-1991 No patient
Fluid restriction is superior in acute lung injury and ARDS
 TAKE-HOME POINTS FROM LECTURES BY CLEVELAND CLINIC AND VISITING FACULTY MEDICAL GRAND ROUNDS CME CREDIT HERBERT P. WIEDEMANN, MD Chairman, Department of Pulmonary, Allergy, and Critical Care Medicine,
TAKE-HOME POINTS FROM LECTURES BY CLEVELAND CLINIC AND VISITING FACULTY MEDICAL GRAND ROUNDS CME CREDIT HERBERT P. WIEDEMANN, MD Chairman, Department of Pulmonary, Allergy, and Critical Care Medicine,
Breathing life into new therapies: Updates on treatment for severe respiratory failure. Whitney Gannon, MSN ACNP-BC
 Breathing life into new therapies: Updates on treatment for severe respiratory failure Whitney Gannon, MSN ACNP-BC Overview Definition of ARDS Clinical signs and symptoms Causes Pathophysiology Management
Breathing life into new therapies: Updates on treatment for severe respiratory failure Whitney Gannon, MSN ACNP-BC Overview Definition of ARDS Clinical signs and symptoms Causes Pathophysiology Management
One Lung Ventilation in Obese patients
 One Lung Ventilation in Obese patients YUSNI PUSPITA DEPARTEMEN ANESTESIOLOGI DAN TERAPI INTENSIF FAKULTAS KEDOKTERAN UNIVERSITAS SRIWIJAYA/RSMH PALEMBANG One Lung Ventilation Lung isolation techniques
One Lung Ventilation in Obese patients YUSNI PUSPITA DEPARTEMEN ANESTESIOLOGI DAN TERAPI INTENSIF FAKULTAS KEDOKTERAN UNIVERSITAS SRIWIJAYA/RSMH PALEMBANG One Lung Ventilation Lung isolation techniques
C h a p t e r 1 4 Ventilator Support
 C h a p t e r 1 4 Ventilator Support Shirish Prayag Ex. Hon. Asst. Prof of Medicine, BJ Medical College and Sassoon Hospital, Pune; Chief Consultant in Internal Medicine and Critical Care, Shree Medical
C h a p t e r 1 4 Ventilator Support Shirish Prayag Ex. Hon. Asst. Prof of Medicine, BJ Medical College and Sassoon Hospital, Pune; Chief Consultant in Internal Medicine and Critical Care, Shree Medical
Computed tomography in adult respiratory distress syndrome: what has it taught us?
 Eur Respir J, 1996, 9, 155 162 DOI: 1.1183/931936.96.95155 Printed in UK - all rights reserved Copyright ERS Journals Ltd 1996 European Respiratory Journal ISSN 93-1936 SERIES 'CLINICAL PHYSIOLOGY IN RESPIRATORY
Eur Respir J, 1996, 9, 155 162 DOI: 1.1183/931936.96.95155 Printed in UK - all rights reserved Copyright ERS Journals Ltd 1996 European Respiratory Journal ISSN 93-1936 SERIES 'CLINICAL PHYSIOLOGY IN RESPIRATORY
APRV for ARDS: the complexities of a mode and how it affects even the best trials
 Editorial APRV for ARDS: the complexities of a mode and how it affects even the best trials Eduardo Mireles-Cabodevila 1,2, Siddharth Dugar 1,2, Robert L. Chatburn 1,2 1 Respiratory Institute, Cleveland
Editorial APRV for ARDS: the complexities of a mode and how it affects even the best trials Eduardo Mireles-Cabodevila 1,2, Siddharth Dugar 1,2, Robert L. Chatburn 1,2 1 Respiratory Institute, Cleveland
Respiratory failure requiring mechanical ventilation
 Current Issues in Mechanical Ventilation for Respiratory Failure* Neil R. MacIntyre, MD The morbidity and mortality associated with respiratory failure is, to a certain extent, iatrogenic. Mechanical ventilation,
Current Issues in Mechanical Ventilation for Respiratory Failure* Neil R. MacIntyre, MD The morbidity and mortality associated with respiratory failure is, to a certain extent, iatrogenic. Mechanical ventilation,
Efficacy and safety of lung recruitment in pediatric patients with acute lung injury
 Efficacy and safety of lung recruitment in pediatric patients with acute lung injury Juan P. Boriosi, MD; Anil Sapru, MD; James H. Hanson, MD; Jeanette Asselin, MS, RT; Ginny Gildengorin, PhD; Vivienne
Efficacy and safety of lung recruitment in pediatric patients with acute lung injury Juan P. Boriosi, MD; Anil Sapru, MD; James H. Hanson, MD; Jeanette Asselin, MS, RT; Ginny Gildengorin, PhD; Vivienne
Principles of Mechanical Ventilation
 47 Principles of Mechanical Ventilation Jonathan E. Sevransky, MD, MHS Objectives Understand the indications for treatment with mechanical ventilation Describe ventilator strategies that will minimize
47 Principles of Mechanical Ventilation Jonathan E. Sevransky, MD, MHS Objectives Understand the indications for treatment with mechanical ventilation Describe ventilator strategies that will minimize
Prone Position in ARDS
 Prone Position in ARDS Rich Kallet MS RRT FAARC, FCCM Respiratory Care Services Department of Anesthesia & Perioperative Care University of California, San Francisco, San Francisco General Hospital Case
Prone Position in ARDS Rich Kallet MS RRT FAARC, FCCM Respiratory Care Services Department of Anesthesia & Perioperative Care University of California, San Francisco, San Francisco General Hospital Case
Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor
 Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Mechanical Ventilation Strategies in Anesthesia
 Mechanical Ventilation Strategies in Anesthesia PAOLO PELOSI, MD, FERS Department of Surgical Sciences and Integrated Diagnostics (DISC), San Martino Policlinico Hospital IRCCS for Oncology, University
Mechanical Ventilation Strategies in Anesthesia PAOLO PELOSI, MD, FERS Department of Surgical Sciences and Integrated Diagnostics (DISC), San Martino Policlinico Hospital IRCCS for Oncology, University
ACUTE RESPIRATORY DISTRESS SYNDROME CHALLENGES FOR TRANSLATIONAL RESEARCH AND OPPORTUNITIES FOR PRECISION MEDICINE
 ACUTE RESPIRATORY DISTRESS SYNDROME CHALLENGES FOR TRANSLATIONAL RESEARCH AND OPPORTUNITIES FOR PRECISION MEDICINE Acute respiratory distress syndrome: challenges for translational research and opportunities
ACUTE RESPIRATORY DISTRESS SYNDROME CHALLENGES FOR TRANSLATIONAL RESEARCH AND OPPORTUNITIES FOR PRECISION MEDICINE Acute respiratory distress syndrome: challenges for translational research and opportunities
Ventilator Waveforms: Interpretation
 Ventilator Waveforms: Interpretation Albert L. Rafanan, MD, FPCCP Pulmonary, Critical Care and Sleep Medicine Chong Hua Hospital, Cebu City Types of Waveforms Scalars are waveform representations of pressure,
Ventilator Waveforms: Interpretation Albert L. Rafanan, MD, FPCCP Pulmonary, Critical Care and Sleep Medicine Chong Hua Hospital, Cebu City Types of Waveforms Scalars are waveform representations of pressure,
Alveolar recruitment maneuver in refractory hypoxemia and lobar atelectasis after cardiac surgery: A case report
 Universidade de São Paulo Biblioteca Digital da Produção Intelectual - BDPI Departamento de Cirurgia - FM/MCG Artigos e Materiais de Revistas Científicas - FM/MCG 2012 Alveolar recruitment maneuver in
Universidade de São Paulo Biblioteca Digital da Produção Intelectual - BDPI Departamento de Cirurgia - FM/MCG Artigos e Materiais de Revistas Científicas - FM/MCG 2012 Alveolar recruitment maneuver in
Provide guidelines for the management of mechanical ventilation in infants <34 weeks gestation.
 Page 1 of 5 PURPOSE: Provide guidelines for the management of mechanical ventilation in infants
Page 1 of 5 PURPOSE: Provide guidelines for the management of mechanical ventilation in infants
Effect of ARDS Severity and Etiology on Short-Term Outcomes
 Effect of ARDS Severity and Etiology on Short-Term Outcomes Haitham El-Haddad MD, Hyejeong Jang MSc, Wei Chen PhD, and Ayman O Soubani MD BACKGROUND: We evaluated the outcome of subjects with ARDS in relation
Effect of ARDS Severity and Etiology on Short-Term Outcomes Haitham El-Haddad MD, Hyejeong Jang MSc, Wei Chen PhD, and Ayman O Soubani MD BACKGROUND: We evaluated the outcome of subjects with ARDS in relation
Transpulmonary pressure measurement
 White Paper Transpulmonary pressure measurement Benefit of measuring transpulmonary pressure in mechanically ventilated patients Dr. Jean-Michel Arnal, Senior Intensivist, Hopital Sainte Musse, Toulon,
White Paper Transpulmonary pressure measurement Benefit of measuring transpulmonary pressure in mechanically ventilated patients Dr. Jean-Michel Arnal, Senior Intensivist, Hopital Sainte Musse, Toulon,
Literature List APRV 2016
 Literature List APRV 2016 APRV Literature List INDEX Writer Subject Publication Page Li JQ. et Yoshihisa Morimoto et Clinical research about airway pressure release ventilation for moderate to severe acute
Literature List APRV 2016 APRV Literature List INDEX Writer Subject Publication Page Li JQ. et Yoshihisa Morimoto et Clinical research about airway pressure release ventilation for moderate to severe acute
Instellen van beademingsparameters bij de obese pa3ent. MDO Nynke Postma
 Instellen van beademingsparameters bij de obese pa3ent MDO 19-1- 2015 Nynke Postma 1. Altered respiratory mechanics in obese pa@ents 2. Transpulmonary pressure 3. Titra@ng PEEP 4. Titra@ng @dal volume
Instellen van beademingsparameters bij de obese pa3ent MDO 19-1- 2015 Nynke Postma 1. Altered respiratory mechanics in obese pa@ents 2. Transpulmonary pressure 3. Titra@ng PEEP 4. Titra@ng @dal volume
Pro - Con Debate APRV vs Conventional Ventilation. Pro Jon Marinaro, MD
 Pro - Con Debate APRV vs Conventional Ventilation Pro Jon Marinaro, MD PRO CON Volume Assist Control Mode ARDS MORTALITY OVER LAST 50 YEARS 53 year old female with 50% Flame Burn to Chest, Flanks & Buttocks
Pro - Con Debate APRV vs Conventional Ventilation Pro Jon Marinaro, MD PRO CON Volume Assist Control Mode ARDS MORTALITY OVER LAST 50 YEARS 53 year old female with 50% Flame Burn to Chest, Flanks & Buttocks
The new ARDS definitions: what does it mean?
 The new ARDS definitions: what does it mean? Richard Beale 7 th September 2012 METHODS ESICM convened an international panel of experts, with representation of ATS and SCCM The objectives were to update
The new ARDS definitions: what does it mean? Richard Beale 7 th September 2012 METHODS ESICM convened an international panel of experts, with representation of ATS and SCCM The objectives were to update
Pulmonary & Extra-pulmonary ARDS: FIZZ or FUSS?
 Pulmonary & Extra-pulmonary ARDS: FIZZ or FUSS? Dr. Rajagopala Srinivas Senior Resident, Dept. Pulmonary Medicine, PGIMER, Chandigarh. The beginning.. "The etiology of this respiratory distress syndrome
Pulmonary & Extra-pulmonary ARDS: FIZZ or FUSS? Dr. Rajagopala Srinivas Senior Resident, Dept. Pulmonary Medicine, PGIMER, Chandigarh. The beginning.. "The etiology of this respiratory distress syndrome
Original Article Ultrasound reaeration scores to assess lung recruitment in rabbits with acute respiratory distress syndrome
 Int J Clin Exp Med 2018;11(8):7761-7769 www.ijcem.com /ISSN:1940-5901/IJCEM0077713 Original Article Ultrasound reaeration scores to assess lung recruitment in rabbits with acute respiratory distress syndrome
Int J Clin Exp Med 2018;11(8):7761-7769 www.ijcem.com /ISSN:1940-5901/IJCEM0077713 Original Article Ultrasound reaeration scores to assess lung recruitment in rabbits with acute respiratory distress syndrome
The Vigileo monitor by Edwards Lifesciences supports both the FloTrac Sensor for continuous cardiac output and the Edwards PreSep oximetry catheter
 1 2 The Vigileo monitor by Edwards Lifesciences supports both the FloTrac Sensor for continuous cardiac output and the Edwards PreSep oximetry catheter for continuous central venous oximetry (ScvO2) 3
1 2 The Vigileo monitor by Edwards Lifesciences supports both the FloTrac Sensor for continuous cardiac output and the Edwards PreSep oximetry catheter for continuous central venous oximetry (ScvO2) 3
Protecting the Lungs
 Protecting the Lungs PGA New York 12/07 Disclosures: Peter Slinger MD, FRCPC University of Toronto 58 y.o. Male, Chronic Gallstone Pancreatitis, Open Cholecystectomy 100 pack/year smoker Dyspnea > 1 block
Protecting the Lungs PGA New York 12/07 Disclosures: Peter Slinger MD, FRCPC University of Toronto 58 y.o. Male, Chronic Gallstone Pancreatitis, Open Cholecystectomy 100 pack/year smoker Dyspnea > 1 block
BioMedical Engineering OnLine. Open Access REVIEW
 https://doi.org/10.1186/s12938-018-0455-y BioMedical Engineering OnLine REVIEW Open Access Next generation, personalised, model based critical care medicine: a state of the art review of in silico virtual
https://doi.org/10.1186/s12938-018-0455-y BioMedical Engineering OnLine REVIEW Open Access Next generation, personalised, model based critical care medicine: a state of the art review of in silico virtual
Bi-Level Therapy: Boosting Comfort & Compliance in Apnea Patients
 Bi-Level Therapy: Boosting Comfort & Compliance in Apnea Patients Objectives Describe nocturnal ventilation characteristics that may indicate underlying conditions and benefits of bilevel therapy for specific
Bi-Level Therapy: Boosting Comfort & Compliance in Apnea Patients Objectives Describe nocturnal ventilation characteristics that may indicate underlying conditions and benefits of bilevel therapy for specific
APPENDIX VI HFOV Quick Guide
 APPENDIX VI HFOV Quick Guide Overall goal: Maintain PH in the target range at the minimum tidal volume. This is achieved by favoring higher frequencies over lower P (amplitude). This goal is also promoted
APPENDIX VI HFOV Quick Guide Overall goal: Maintain PH in the target range at the minimum tidal volume. This is achieved by favoring higher frequencies over lower P (amplitude). This goal is also promoted
Extravascular lung water reflects pulmonary edema F Javier Belda MD, PhD Dept. Anesthesiology and Critical Care
 28 th ISICEM Brussels, 19 March 2008 Monitoring in respiratory failure Extravascular lung water reflects pulmonary edema F Javier Belda MD, PhD Dept. Anesthesiology and Critical Care Hospital Clinico Universitario
28 th ISICEM Brussels, 19 March 2008 Monitoring in respiratory failure Extravascular lung water reflects pulmonary edema F Javier Belda MD, PhD Dept. Anesthesiology and Critical Care Hospital Clinico Universitario
Difficult Ventilation in ARDS Patients
 Thank you for viewing this presentation. We would like to remind you that this material is the property of the author. It is provided to you by the ERS for your personal use only, as submitted by the author.
Thank you for viewing this presentation. We would like to remind you that this material is the property of the author. It is provided to you by the ERS for your personal use only, as submitted by the author.
Steroids for ARDS. Clinical Problem. Management
 Steroids for ARDS James Beck Clinical Problem A 60 year old lady re-presented to ICU with respiratory failure. She had previously been admitted for fluid management and electrolyte correction having presented
Steroids for ARDS James Beck Clinical Problem A 60 year old lady re-presented to ICU with respiratory failure. She had previously been admitted for fluid management and electrolyte correction having presented