Krittin Bunditanukul Pharm.D, BCPS Department of Pharmacy Practice, Faculty of Pharmaceutical Sciences, Chulalongkorn University
|
|
|
- Lynne Gregory
- 6 years ago
- Views:
Transcription




1 Krittin Bunditanukul Pharm.D, BCPS Department of Pharmacy Practice, Faculty of Pharmaceutical Sciences, Chulalongkorn University
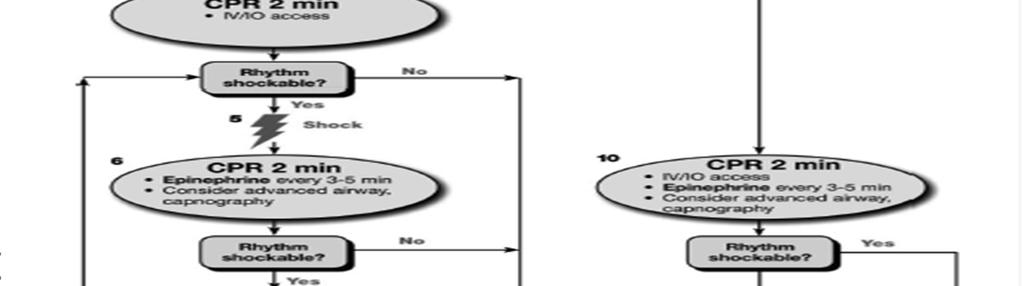
2 Cardiac arrest Cardiac arrest can be caused by 4 rhythms: Ventricular fibrillation (VF) Pulseless ventricular tachycardia (VT) Pulseless electric activity (PEA) Asystole.
3 VF/VT VF represents disorganized electric activity. Pulseless VT represents organized electric activity of the ventricular myocardium. Neither of these rhythms generates significant forward blood flow.
4 PEA PEA encompasses a heterogeneous group of organized electric rhythms that are associated with either absence of mechanical ventricular activity or mechanical ventricular activity that is insufficient to generate a clinically detectable pulse.
5 Asystole Asystole represents absence of detectable ventricular electric activity with or without atrial electric activity.

6 Neumar RW et al. Circulation. 2010;122:S729-S767
7 Management of cardiac arrest During management of cardiac arrest the provider should identify and treat any factor that may have caused the arrest or may be complicating the resuscitative effort
8 Management of cardiac arrest Treatable caused of cardiac arrest - Hypoxia - Toxins - Hypovolemia - Cardiac tamponade - Acidosis (Hydrogen) - Tension Pneumothorax - Hypo/hyper K + - Pulmonary thrombosis - Hypothermia - Coronary thrombosis
9 Drug therapy in VF/VT When VF/pulseless VT persists after at least 1 shock and a 2-minute CPR period, a vasopressor can be given with the primary goal of increasing myocardial blood flow during CPR and achieving return of spontaneous circulation (Class IIb, LOE A). Neumar RW et al. Circulation. 2010;122:S729-S767
10 Drug therapy in VF/VT The peak effect of an IV vasopressor given as a bolus dose during CPR is delayed for at least 1-2 minutes. If a shock fails to generate a perfusing rhythm, then giving a vasopressor soon after the shock will optimize the potential impact of increased myocardial blood flow before the next shock.
11 Drug therapy in VF/VT However, if a shock results in a perfusing rhythm, a bolus dose of vasopressor at any time during the subsequent 2-minute period of CPR could theoretically have detrimental effects on cardiovascular stability.
12 Drug therapy in VF/VT Amiodarone is the first-line antiarrhythmic agent given during cardiac arrest because it has been clinically demonstrated to improve the rate of return of spontaneous circulation and hospital admission in adults with refractory VF/pulseless VT Neumar RW et al. Circulation. 2010;122:S729-S767
13 Drug therapy in VF/VT Amiodarone may be considered when VF/VT is unresponsive to CPR, defibrillation, and vasopressor therapy (Class IIb, LOE A). Neumar RW et al. Circulation. 2010;122:S729-S767
14 Drug therapy in VF/VT If amiodarone is unavailable, lidocaine may be considered, but in clinical studies lidocaine has not been demonstrated to improve rates of return of spontaneous circulation and hospital admission compared with amiodarone (Class IIb, LOE B). Magnesium sulfate should be considered only for torsades de pointes associated with a long QT interval (Class IIb, LOE B). Neumar RW et al. Circulation. 2010;122:S729-S767
15 Drug therapy in VF/VT Fibrinolytic therapy administered during CPR for acute coronary occlusion has not been shown to improve outcome. Bottiger BW et al. N Engl J Med. 2008;359:

16 Bottiger BW et al. N Engl J Med. 2008;359:
17 Drug therapy for PEA/Asystole A vasopressor can be given as soon as feasible with the primary goal of increasing myocardial and cerebral blood flow during CPR and achieving return of spontaneous circulation (Class IIb, LOE A). Neumar RW et al. Circulation. 2010;122:S729-S767
18 Drug therapy for PEA/Asystole Available evidence suggests that the routine use of atropine during PEA or asystole is unlikely to have a therapeutic benefit (Class IIb, LOE B). For this reason atropine has been removed from the cardiac arrest algorithm. Neumar RW et al. Circulation. 2010;122:S729-S767
19 Drug therapy for PEA/Asystole Given the potential association of PEA with hypoxemia, placement of an advanced airway is theoretically more important than during VF/pulseless VT and might be necessary to achieve adequate oxygenation or ventilation.
20 Drug therapy for PEA/Asystole PEA caused by severe volume loss or sepsis will potentially benefit from administration of empirical IV crystalloid. A patient with PEA caused by severe blood loss will potentially benefit from a blood transfusion.
21 Drug therapy for PEA/Asystole When pulmonary embolism is presumed or known to be the cause of cardiac arrest, empirical fibrinolytic therapy can be considered
22 Drug therapy for PEA/Asystole Asystole is commonly the end-stage rhythm that follows prolonged VF or PEA, and for this reason the prognosis is generally much worse.
23 Monitoring during CPR Rate and dept of compression Rate of ventilation EKG Pulse ABG Central venous oxygen saturation Echocardiogram
24 Access of parenteral medication during cardiac arrest There is insufficient evidence to recommend a specific timing or sequence of drug administration and advanced airway placement during cardiac arrest.
25 Access of parenteral medication during cardiac arrest If a resuscitation drug is administered by a peripheral venous route, it should be administered by bolus injection and followed with a 20 ml bolus of IV fluid to facilitate the drug flow from the extremity into the central circulation. Briefly elevating the extremity during and after drug administration theoretically may also recruit the benefit of gravity to facilitate delivery to the central circulation
26 Access of parenteral medication during cardiac arrest The primary advantage of a central line is that peak drug concentrations are higher and drug circulation times shorter compared peripheral IV catheter. A central line extending into the superior vena cava can be used to monitor ScvO2 and estimate CPP during CPR. Central venous catheterization is a relative contraindication for fibrinolytic therapy in patients with ACS.
27 Medication for arrest rhythms The primary goal of pharmacologic therapy during cardiac arrest is to facilitate restoration and maintenance of a perfusing spontaneous rhythm. ACLS drug therapy during CPR is often associated with increased rates of ROSC and hospital admission but not increased rates of long-term survival with good neurologic outcome.
28 Vasopressors To date no placebo-controlled trials have shown that administration of any vasopressor agent at any stage during management of VF, pulseless VT, PEA, or asystole increases the rate of neurologically intact survival to hospital discharge. There is evidence, however, that the use of vasopressor agents is associated with an increased rate of ROSC.
29 Ref 138
30 Ref 137
31 Epinephrine Epinephrine produces beneficial effects in patients during cardiac arrest, primarily because of its α-adrenergic receptorstimulating properties. The a-adrenergic effects of epinephrine can increase CPP and cerebral perfusion pressure during CPR. Michael JR,et al. Circulation. 1984;69:


32 Epinephrine Herlitz J, et al. Resuscitation. 1995;29:
33 Epinephrine Ref 135 Vandycke C, et al. Resuscitation. 2000;45:
34 Epinephrine There are no RCTs that adequately compare epinephrine with placebo in treatment of and outcomes related to out-of-hospital cardiac arrest. It is reasonable to consider administering a 1 mg dose of IV epinephrine every 3 to 5 minutes during adult cardiac arrest (Class IIb, LOE A). Neumar RW et al. Circulation. 2010;122:S729-S767
35 Vasopressin Vasopressin is a non-adrenergic peripheral vasoconstrictor that also causes coronary and renal vasoconstriction.
36 From: Vasopressin for Cardiac Arrest: A Systematic Review and Meta-analysis Arch Intern Med. 2005;165(1): doi: /archinte Figure Legend: Failure of return of spontaneous circulation. CI indicates confidence interval; RR, risk ratio. Vertical lines represent RR of 1; squares, individual study; diamond, pooled effect; arrowhead, the farthermost point of the horizontal line (CI) falls beyond the left margin of the scale. Date of download: 1/9/2014 Copyright 2012 American Medical Association. All rights reserved.
37 From: Vasopressin for Cardiac Arrest: A Systematic Review and Meta-analysis Arch Intern Med. 2005;165(1): doi: /archinte Figure Legend: Death before hospital admission. CI indicates confidence interval; RR, risk ratio. For explanation of symbols, see legend to Figure 2. Date of download: 1/9/2014 Copyright 2012 American Medical Association. All rights reserved.
38 From: Vasopressin for Cardiac Arrest: A Systematic Review and Meta-analysis Arch Intern Med. 2005;165(1): doi: /archinte Figure Legend: Combination of number of deaths and neurologically impaired survivors. CI indicates confidence interval; RR, risk ratio. For explanation of symbols, see legend to Figure 2. Date of download: 1/9/2014 Copyright 2012 American Medical Association. All rights reserved.
39 Vasopressin Because the effects of vasopressin have not been shown to differ from those of epinephrine in cardiac arrest, 1 dose of vasopressin 40 units IV may replace either the first or second dose of epinephrine in the treatment of cardiac arrest (Class IIb, LOE A). Neumar RW et al. Circulation. 2010;122:S729-S767
40 Other vasopressors There are no alternative vasopressors (norepinephrine, phenylephrine) with proven survival benefit compared with epinephrine. Neumar RW et al. Circulation. 2010;122:S729-S767
41 Antiarrhythmics There is no evidence that any antiarrhythmic drug given routinely during human cardiac arrest increases survival to hospital discharge. Neumar RW et al. Circulation. 2010;122:S729-S767
42 Amiodarone IV amiodarone affects sodium, potassium, and calcium channels and has α and β adrenergic blocking properties. It can be considered for treatment of VF or pulseless VT unresponsive to shock delivery, CPR, and a vasopressor.


43 Ref 134 Kudenchank PJ, et al. N Engl J Med. 1999;341:

44 Effect of Treatment with Amiodarone or Lidocaine on the Rate of Survival to Hospital Admission in All Patients and in Selected Subgroups Dorian, P. et al. N Engl J Med 2002;346:
45 Amiodarone Amiodarone may be considered for VF or pulseless VT unresponsive to CPR, defibrillation, and a vasopressor therapy (Class IIb, LOE B). An initial dose of 300 mg IV can be followed by 1 dose of 150 mg IV. A higher incidence of bradycardia and hypotension was reported for amiodarone The adverse hemodynamic effects of the IV formulation of amiodarone are attributed to vasoactive solvents Neumar RW et al. Circulation. 2010;122:S729-S767
46 Lidocaine Lidocaine, however, has no proven short- or longterm efficacy in cardiac arrest. Lidocaine may be considered if amiodarone is not available (Class IIb, LOE B). The initial dose is mg/kg IV. If VF/pulseless VT persists, additional doses of mg/kg IV push may be administered at 5-10 minute intervals to a maximum dose of 3 mg/kg. Neumar RW et al. Circulation. 2010;122:S729-S767
47 Ref 289 Helitz J, et al. Resuscitation. 1997;33:
48 Magnesium sulfate When VF/pulseless VT cardiac arrest is associated with torsades de pointes, providers may administer an IV bolus of magnesium sulfate at a dose of 1-2 g diluted in 10 ml D5W (Class IIb, LOE C). Routine administration of magnesium sulfate in cardiac arrest is not recommended (Class III, LOE A) unless torsades de pointes is present. Neumar RW et al. Circulation. 2010;122:S729-S767
49 Magnesium sulfate Magnesium sulfate is not likely to be effective in terminating irregular/polymorphic VT in patients with a normal QT interval. Tzivoni D, et al. Circulation. 1988;77:
50 Magnesium sulfate Ref 293 Thel MC, et al. Lancet. 1997;350:
51 Atropine Atropine sulfate reverses cholinergic-mediated decreases in heart rate and AV nodal conduction. Available evidence suggests that routine use of atropine during PEA or asystole is unlikely to have a therapeutic benefit (Class IIb, LOE B). Neumar RW et al. Circulation. 2010;122:S729-S767
52 NaHCO 3 Tissue acidosis and resulting acidemia during cardiac arrest and resuscitation are dynamic processes resulting from no blood flow during arrest and low blood flow during CPR. These processes are affected by the duration of cardiac arrest, level of blood flow, and arterial oxygen content during CPR.
53 NaHCO 3 There are few data to support therapy with buffers during cardiac arrest. There is no evidence that bicarbonate improves the likelihood of defibrillation or survival rates in animals with VF cardiac arrest. A wide variety of adverse effects have been linked to administration of bicarbonate during cardiac arrest.



54 NaHCO 3 Vukmir RB, et al. Am J Emerg Med. 2006;24:



55 Delooz HH, et al. Resuscitation. 1989; 17 suppl:s161-s172.
56 NaHCO 3 Disadvantage of NaHCO 3 - Compromise CPP by reducing systemic vascular resistance. Create extracellular alkalosis Hypernatremia Hyperosmolarity Produces excess CO2 and may paradoxically contribute to intracellular acidosis Exacerbate central venous acidosis and may inactivate simultaneously administered catecholamines.
57 NaHCO 3 In some special resuscitation situations, such as preexisting metabolic acidosis, hyperkalemia, or tricyclic antidepressant overdose, bicarbonate can be beneficial However, routine use of NaHCO 3 is not recommended for patients in cardiac arrest (Class III, LOE B). Neumar RW et al. Circulation. 2010;122:S729-S767
58 NaHCO 3 An initial dose of 1 meq/kg is typical. Whenever possible, bicarbonate therapy should be guided by the bicarbonate concentration or calculated base deficit obtained from blood gas analysis or laboratory measurement. To minimize the risk of iatrogenically induced alkalosis, providers should not attempt complete correction of the calculated base deficit.
59 Intervention not recommended for routine use during cardiac arrest Calcium Fibrinolytics IV fluid Neumar RW et al. Circulation. 2010;122:S729-S767
60 Bradycardia Bradycardia is defined as a heart rate of < 60 bpm. However, when bradycardia is the cause of symptoms, the rate is generally < 50 bpm
61 Bradycardia Because hypoxemia is a common cause of bradycardia, initial evaluation of any patient with bradycardia should focus on signs of increased work of breathing and oxyhemoglobin saturation as determined by pulse oximetry
62 Bradycardia If bradycardia produces signs and symptoms of instability, the initial treatment is atropine (Class IIa, LOE B). If bradycardia is unresponsive to atropine, IV infusion of -adrenergic agonists with rateaccelerating effects (dopamine, epinephrine) or transcutaneous pacing can be effective (Class IIa, LOE B). Neumar RW et al. Circulation. 2010;122:S729-S767
63 Atropine Atropine remains the first-line drug for acute symptomatic bradycardia. Clinical trials in adults showed that IV atropine improved heart rate, symptoms, and signs associated with bradycardia. Brady WJ, et al. Resuscitation. 1999;41: Swart G, et al. Am J Emerg Med. 1999;17:
64 Atropine The recommended atropine dose for bradycardia is 0.5 mg IV every 3 to 5 minutes to a maximum total dose of 3 mg. Doses of atropine sulfate of,0.5 mg may paradoxically result in further slowing of the heart rate.
65 Atropine Use atropine cautiously in the presence of acute coronary ischemia or MI; increased heart rate may worsen ischemia or increase infarction size. Atropine will likely be ineffective in patients who have undergone cardiac transplantation because the transplanted heart lacks vagal innervation.
66 Alternative drug Dopamine At lower doses dopamine has a more selective effect on inotropy and heart rate; at higher doses, it also has vasoconstrictive effects. Dopamine infusion may be used for patients with symptomatic bradycardia, particularly if associated with hypotension, in whom atropine may be inappropriate or after atropine fails (Class IIb, LOE B). Begin dopamine infusion at 2 to 10 mcg/kg per minute and titrate to patient response Neumar RW et al. Circulation. 2010;122:S729-S767
67 Alternative drug Epinephrine Epinephrine infusion may be used for patients with symptomatic bradycardia, particularly if associated with hypotension, for whom atropine may be inappropriate or after atropine fails (Class IIb, LOE B). Begin the infusion at 2 to10 mcg/min and titrate to patient response. Neumar RW et al. Circulation. 2010;122:S729-S767
68 Alternative drug Isoproterenol Isoproterenol is a b-adrenergic agent with β-1 and β-2 effects, resulting in an increase in heart rate and vasodilation. The recommended adult dose is 2 to 10 mcg/min by IV infusion, titrated according to heart rate and rhythm response. Neumar RW et al. Circulation. 2010;122:S729-S767




69 Neumar RW et al. Circulation. 2010;122:S729-S767
70 Tachycardia Tachycardia is defined as an arrhythmia with a rate of >100 bpm, although, as with defining bradycardia, the rate of a tachycardia takes on clinical significance at its greater extremes and is more likely attributable to an arrhythmia rate of 150 bpm.
71 Tachycardia If the tachycardic patient is unstable with severe signs and symptoms related to a suspected arrhythmia, immediate cardioversion should be performed (Class I, LOE B). In select cases of regular narrow-complex tachycardia with unstable signs or symptoms (not hypotensive), a trial of adenosine before cardioversion is reasonable to consider (Class IIb, LOE C). Neumar RW et al. Circulation. 2010;122:S729-S767
72 Tachycardia If the patient with tachycardia is stable, determine if the patient has a narrow-complex or wide-complex tachycardia, whether the rhythm is regular or irregular, and for wide complexes whether the QRS morphology is monomorphic or polymorphic. Neumar RW et al. Circulation. 2010;122:S729-S767
73 Regular narrow-complex tachycardia If judged to be sinus tachycardia, no specific drug treatment is required. Instead, therapy is directed toward identification and treatment of the underlying cause. When cardiac function is poor, cardiac output can be dependent on a rapid heart rate. In such compensatory tachycardias, stroke volume is limited, so normalizing the heart rate can be detrimental.
74 Reentry SVT Give 6 mg of IV adenosine as a rapid IV push through a large vein followed by a 20 ml saline flush (Class I, LOE B). If the rhythm does not convert within 1 to 2 mins, give a 12 mg rapid IV push using the method above. The effect of adenosine on other SVTs (such as atrial fibrillation or flutter) is to transiently slow ventricular rate (which may be useful diagnostically) but not afford their termination or meaningful lasting rate control. Neumar RW et al. Circulation. 2010;122:S729-S767
75 Reentry SVT Therapy Vagal maneuvers Adenosine Calcium channel blockers (CCBs) Beta-blockers (BBs)
76 Adenosine Adenosine is safe and effective in pregnancy. Adenosine does have several important drug interactions. Larger doses may be required for patients with a significant blood level of theophylline or caffeine. The initial dose should be reduced to 3 mg in patients taking dipyridamole or carbamazepine, those with transplanted hearts, or if given by central venous access.
77 Adenosine Side effects with adenosine are common but transient; flushing, dyspnea, and chest discomfort are the most frequently observed. Adenosine should not be given to patients with asthma.
78 CCBs and BBs If adenosine fail to convert PSVT, PSVT recurs after such treatment, or these treatments disclose a different form of SVT (such as AF or flutter), it is reasonable to use longer-acting AV nodal blocking agents, such as the nondihydropyridine calcium channel blockers (verapamil and diltiazem) (Class IIa, LOE B) or b-blockers (Class IIa, LOE C). Neumar RW et al. Circulation. 2010;122:S729-S767
79 CCBs and BBs For verapamil, give a mg IV bolus over 2 mins (over 3 mins in older patients). If there is no therapeutic response repeated doses of 5-10 mg may be administered every mins to a total dose of 20 mg. An alternative dosing regimen is to give a 5 mg bolus every 15 mins to a total dose of 30 mg.
80 CCBs and BBs Verapamil should be given only to patients with narrow-complex reentry SVT or arrhythmias known with certainty to be of supraventricular origin. Verapamil should not be given to patients with wide-complex tachycardias. It should not be given to patients with impaired ventricular function or heart failure.
81 CCBs and BBs For diltiazem, give a dose of mg (0.25 mg/kg) IV over 2 mins; if needed, in 15 mins give an additional IV dose of mg (0.35 mg/kg). The maintenance infusion dose is 5-15 mg/hour, titrated to heart rate.
82 CCBs and BBs Like calcium channel blockers, they also have negative inotropic effects and further reduce cardiac output in patients with heart failure. Side effects of b-blockers can include bradycardias, AV conduction delays, and hypotension. β-blockers should be used with caution in patients with obstructive pulmonary disease or congestive heart failure.
83 Wide-complex tachycardia If the etiology of the rhythm cannot be determined, the rate is regular, and the QRS is monomorphic, recent evidence suggests that IV adenosine is relatively safe for both treatment and diagnosis (Class IIb, LOE B). However, adenosine should not be given for unstable or for irregular or polymorphic widecomplex tachycardias, as it may cause degeneration of the arrhythmia to VF (Class III, LOE C). Neumar RW et al. Circulation. 2010;122:S729-S767
84 Wide-complex tachycardia Verapamil is contraindicated for widecomplex tachycardias unless known to be of supraventricular origin (Class III, LOE B). Profound hypotension was reported in patients known to have VT treated with verapamil. Neumar RW et al. Circulation. 2010;122:S729-S767
85 Wide-complex tachycardia For patients who are stable with likely VT, IV antiarrhythmic drugs or elective cardioversion is the preferred treatment strategy. If IV antiarrhythmics are administered: Procainamide (Class IIa, LOE B) Amiodarone (Class IIb, LOE B) Sotalol (Class IIb, LOE B) Procainamide and sotalol should be avoided in patients with prolonged QT. If one of these antiarrhythmic agents is given, a second agent should not be given without expert consultation (Class III, LOE B). Neumar RW et al. Circulation. 2010;122:S729-S767
86 Wide-complex tachycardia Amiodarone is also effective in preventing recurrent monomorphic VT or treating refractory ventricular arrhythmias. It is given 150 mg IV over 10 minutes; dosing should be repeated as needed to a maximum dose of 2.2 g IV per 24 hours. Higher doses (300 mg) were associated with an increased frequency of hypotension,
87 Wide-complex tachycardia Lidocaine is less effective in terminating VT than procainamide, sotalol, and amiodarone. Lidocaine should be considered second-line antiarrhythmic therapy for monomorphic VT. Lidocaine can be administered at a dose of mg/kg IV bolus. Maintenance infusion is 1-4 mg/min (30-50 mcg/kg per minute). Neumar RW et al. Circulation. 2010;122:S729-S767 Somberg JC, et al. Am J Cardiol. 2002;90:




88 Neumar RW et al. Circulation. 2010;122:S729-S767
89 AF and Atrial flutter General management of AF should focus on control of the rapid ventricular rate (rate control), conversion of hemodynamically unstable AF to sinus rhythm (rhythm control), or both. Patients with an AF duration of > 48 hours are at increased risk for cardioembolic events, although shorter durations of AF do not exclude the possibility of such events. Neumar RW et al. Circulation. 2010;122:S729-S767
90 AF and Atrial flutter Electric or pharmacologic cardioversion should not be attempted in these patients unless the patient is unstable. An alternative strategy is to perform cardioversion following anti-coagulation with heparin and performance of TEE to ensure the absence of a left atrial thrombus. Neumar RW et al. Circulation. 2010;122:S729-S767
91

92

93
94
95
Chapter 9. Learning Objectives. Learning Objectives 9/11/2012. Cardiac Arrhythmias. Define electrical therapy
 Chapter 9 Cardiac Arrhythmias Learning Objectives Define electrical therapy Explain why electrical therapy is preferred initial therapy over drug administration for cardiac arrest and some arrhythmias
Chapter 9 Cardiac Arrhythmias Learning Objectives Define electrical therapy Explain why electrical therapy is preferred initial therapy over drug administration for cardiac arrest and some arrhythmias
Management of Cardiac Arrest Based on : 2010 American Heart Association Guidelines
 Management of Cardiac Arrest Based on : 2010 American Heart Association Guidelines www.circ.ahajournals.org Elham Pishbin. M.D Assistant Professor of Emergency Medicine MUMS C H E S Advanced Life Support
Management of Cardiac Arrest Based on : 2010 American Heart Association Guidelines www.circ.ahajournals.org Elham Pishbin. M.D Assistant Professor of Emergency Medicine MUMS C H E S Advanced Life Support
Adenosine. poison/drug induced. flushing, chest pain, transient asystole. Precautions: tachycardia. fibrillation, atrial flutter. Indications: or VT
 Adenosine Indications: 1. Narrow complex PSVT 2. Does not convert atrial fibrillation, atrial flutter or VT 1. Side effects include flushing, chest pain, transient asystole 2. May deteriorate widecomplex
Adenosine Indications: 1. Narrow complex PSVT 2. Does not convert atrial fibrillation, atrial flutter or VT 1. Side effects include flushing, chest pain, transient asystole 2. May deteriorate widecomplex
ACLS Review. Pulse Oximetry to be between 94 99% to avoid hyperoxia (high oxygen tension can lead to tissue death
 ACLS Review BLS CPR BLS CPR changed in 2010. The primary change is from the ABC format to CAB. After establishing unresponsiveness and calling for a code, check for a pulse less than 10 seconds then begin
ACLS Review BLS CPR BLS CPR changed in 2010. The primary change is from the ABC format to CAB. After establishing unresponsiveness and calling for a code, check for a pulse less than 10 seconds then begin
CSI Skills Lab #5: Arrhythmia Interpretation and Treatment
 CSI 202 - Skills Lab #5: Arrhythmia Interpretation and Treatment Origins of the ACLS Approach: CSI 202 - Skills Lab 5 Notes ACLS training originated in Nebraska in the early 1970 s. Its purpose was to
CSI 202 - Skills Lab #5: Arrhythmia Interpretation and Treatment Origins of the ACLS Approach: CSI 202 - Skills Lab 5 Notes ACLS training originated in Nebraska in the early 1970 s. Its purpose was to
Objectives: This presentation will help you to:
 emergency Drugs Objectives: This presentation will help you to: Five rights for medication administration Recognize different cardiac arrhythmias and determine the common drugs used for each one List the
emergency Drugs Objectives: This presentation will help you to: Five rights for medication administration Recognize different cardiac arrhythmias and determine the common drugs used for each one List the
1. Normal sinus rhythm 2. SINUS BRADYCARDIA
 1. Normal sinus rhythm 2. SINUS BRADYCARDIA No signs and symptoms observe There are severe signs or symptoms o What are the signs and symptom Hypotension
1. Normal sinus rhythm 2. SINUS BRADYCARDIA No signs and symptoms observe There are severe signs or symptoms o What are the signs and symptom Hypotension
The ARREST Trial: Amiodarone for Resuscitation After Out-of-Hospital Cardiac Arrest Due to Ventricular Fibrillation
 The ARREST Trial: Amiodarone for Resuscitation After Out-of-Hospital Cardiac Arrest Due to Ventricular Fibrillation Introduction The ARREST (Amiodarone in out-of-hospital Resuscitation of REfractory Sustained
The ARREST Trial: Amiodarone for Resuscitation After Out-of-Hospital Cardiac Arrest Due to Ventricular Fibrillation Introduction The ARREST (Amiodarone in out-of-hospital Resuscitation of REfractory Sustained
Advanced Cardiac Life Support ACLS
 Essential Medical Training, LLC Providing Quality, Professional Training Advanced Cardiac Life Support ACLS Course Study Guide and Agenda 772-781-9249 office 772-382-0607 fax Email: treasurecoastcpr@gmail.com
Essential Medical Training, LLC Providing Quality, Professional Training Advanced Cardiac Life Support ACLS Course Study Guide and Agenda 772-781-9249 office 772-382-0607 fax Email: treasurecoastcpr@gmail.com
INSTITUTE FOR MEDICAL SIMULATION & EDUCATION ACLS PRACTICAL SCENARIOS
 Practical Teaching for Respiratory Arrest with a Pulse (Case 1) You are a medical officer doing a pre-operative round when 60-year old patient started coughing violently and becomes unconscious. Fortunately
Practical Teaching for Respiratory Arrest with a Pulse (Case 1) You are a medical officer doing a pre-operative round when 60-year old patient started coughing violently and becomes unconscious. Fortunately
European Resuscitation Council
 European Resuscitation Council Objectives To know basic elements to evaluate patients with rythm disturbance To know advanced treatment of paediatric cardiac arrest To know emergency treatment of most
European Resuscitation Council Objectives To know basic elements to evaluate patients with rythm disturbance To know advanced treatment of paediatric cardiac arrest To know emergency treatment of most
national CPR committee Saudi Heart Association (SHA). International Liason Commission Of Resuscitation (ILCOR)
. International Liason Commission Of Resuscitation (ILCOR)") 2 It is our pleasure to present to you this work as a result of team work of the national CPR committee at the Saudi Heart Association (SHA). We adapted the 2010 guidelines as per International Liason
2 It is our pleasure to present to you this work as a result of team work of the national CPR committee at the Saudi Heart Association (SHA). We adapted the 2010 guidelines as per International Liason
MICHIGAN. State Protocols. Pediatric Cardiac Table of Contents 6.1 General Pediatric Cardiac Arrest 6.2 Bradycardia 6.
 MICHIGAN State Protocols Protocol Number Protocol Name Pediatric Cardiac Table of Contents 6.1 General Pediatric Cardiac Arrest 6.2 Bradycardia 6.3 Tachycardia PEDIATRIC CARDIAC PEDIATRIC CARDIAC ARREST
MICHIGAN State Protocols Protocol Number Protocol Name Pediatric Cardiac Table of Contents 6.1 General Pediatric Cardiac Arrest 6.2 Bradycardia 6.3 Tachycardia PEDIATRIC CARDIAC PEDIATRIC CARDIAC ARREST
WHAT DO YOU SEE WHEN YOU STIMULATE BETA
 CARDIAC DRUG REVIEW WHAT DO YOU SEE WHEN YOU STIMULATE BETA VASODILATE BRONCHODILATE +CHRONOTROPE +INOTROPE EPI S OTHER NAME? ADRENALIN WHAT DOES EPI DO THAT NOREPI AND DOPAMINE DO NOT DO? BETA 2 BRONCHODILATOR
CARDIAC DRUG REVIEW WHAT DO YOU SEE WHEN YOU STIMULATE BETA VASODILATE BRONCHODILATE +CHRONOTROPE +INOTROPE EPI S OTHER NAME? ADRENALIN WHAT DOES EPI DO THAT NOREPI AND DOPAMINE DO NOT DO? BETA 2 BRONCHODILATOR
PEDIATRIC CARDIAC RHYTHM DISTURBANCES. -Jason Haag, CCEMT-P
 PEDIATRIC CARDIAC RHYTHM DISTURBANCES -Jason Haag, CCEMT-P General: CARDIAC RHYTHM DISTURBANCES - More often the result and not the cause of acute cardiovascular emergencies - Typically the end result
PEDIATRIC CARDIAC RHYTHM DISTURBANCES -Jason Haag, CCEMT-P General: CARDIAC RHYTHM DISTURBANCES - More often the result and not the cause of acute cardiovascular emergencies - Typically the end result
Michigan Pediatric Cardiac Protocols. Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS
 Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
DYSRHYTHMIAS. D. Assess whether or not it is the arrhythmia that is making the patient unstable or symptomatic
 DYSRHYTHMIAS GENERAL CONSIDERATIONS A. The 2015 American Heart Association Guidelines were referred to for this protocol development. Evidence-based science was implemented in those areas where the AHA
DYSRHYTHMIAS GENERAL CONSIDERATIONS A. The 2015 American Heart Association Guidelines were referred to for this protocol development. Evidence-based science was implemented in those areas where the AHA
JUST SAY NO TO DRUGS?
 JUST SAY NO TO DRUGS? THE EVIDENCE BEHIND MEDICATIONS USED IN CARDIAC RESUSCITATION NTI 2014 CLASS CODE 148 Nicole Kupchik RN, MN, CCNS, CCRN, PCCN Objectives 1. Discuss the historical evidence supporting
JUST SAY NO TO DRUGS? THE EVIDENCE BEHIND MEDICATIONS USED IN CARDIAC RESUSCITATION NTI 2014 CLASS CODE 148 Nicole Kupchik RN, MN, CCNS, CCRN, PCCN Objectives 1. Discuss the historical evidence supporting
Post Cardiac Arrest Care 2015 American Heart Association Guideline Update for CPR and Emergency Cardiovascular Care
 Post Cardiac Arrest Care 2015 American Heart Association Guideline Update for CPR and Emergency Cardiovascular Care รศ.ดร.พญ.ต นหยง พ พานเมฆาภรณ ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร มหาว ทยาล ยเช ยงใหม System
Post Cardiac Arrest Care 2015 American Heart Association Guideline Update for CPR and Emergency Cardiovascular Care รศ.ดร.พญ.ต นหยง พ พานเมฆาภรณ ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร มหาว ทยาล ยเช ยงใหม System
ACLS Prep. Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep.
 November, 2013 ACLS Prep Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep. ACLS Prep Preparation is key to a successful ACLS experience.
November, 2013 ACLS Prep Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep. ACLS Prep Preparation is key to a successful ACLS experience.
COUNTY OF SACRAMENTO EMERGENCY MEDICAL SERVICES AGENCY
 COUNTY OF SACRAMENTO EMERGENCY MEDICAL SERVICES AGENCY Document # 8024.31 PROGRAM DOCUMENT: Initial Date: 10/26/94 Cardiac Dysrhythmias Last Approval Date: 11/01/16 Effective Date: 11/01/18 Next Review
COUNTY OF SACRAMENTO EMERGENCY MEDICAL SERVICES AGENCY Document # 8024.31 PROGRAM DOCUMENT: Initial Date: 10/26/94 Cardiac Dysrhythmias Last Approval Date: 11/01/16 Effective Date: 11/01/18 Next Review
Michigan Pediatric Cardiac Protocols. Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS
 Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Pediatric Asystole Section 4-1 Pediatric Bradycardia Section 4-2 Pediatric Cardiac Arrest General Section 4-3 Pediatric Narrow Complex Tachycardia
ACLS Study Guide Key guidelines recommendations for healthcare professionals:
 1 ACLS Study Guide 0.849. Key guidelines recommendations for healthcare professionals: Effective teamwork techniques should be learned and practiced regularly. Professional rescuers should use quantitative
1 ACLS Study Guide 0.849. Key guidelines recommendations for healthcare professionals: Effective teamwork techniques should be learned and practiced regularly. Professional rescuers should use quantitative
Final Written Exam ASHI ACLS
 Final Written Exam ASHI ACLS Instructions: Identify the choice that best completes the statement or answers the question. Questions 1 and 2 pertain to the following scenario: A 54-year-old man has experienced
Final Written Exam ASHI ACLS Instructions: Identify the choice that best completes the statement or answers the question. Questions 1 and 2 pertain to the following scenario: A 54-year-old man has experienced
Evidence for Lidocaine and Amiodarone in Cardiac Arrest Due to VF/Pulseless VT
 Evidence for Lidocaine and Amiodarone in Cardiac Arrest Due to VF/Pulseless VT Introduction Evidence supporting the use of lidocaine and amiodarone for advanced cardiac life support was considered by international
Evidence for Lidocaine and Amiodarone in Cardiac Arrest Due to VF/Pulseless VT Introduction Evidence supporting the use of lidocaine and amiodarone for advanced cardiac life support was considered by international
Preparing for your upcoming PALS course
 IU Health PALS Study Guide Preparing for your upcoming PALS course UPDATED November 2016 Course Curriculum: 2015 American Heart Association (AHA) Guidelines for Pediatric Advanced Life Support (PALS) AHA
IU Health PALS Study Guide Preparing for your upcoming PALS course UPDATED November 2016 Course Curriculum: 2015 American Heart Association (AHA) Guidelines for Pediatric Advanced Life Support (PALS) AHA
ADVANCED CARDIAC LIFE SUPPORT (ACLS) RECERTIFICATION EXAMINATION
 RECERTIFICATION EXAMINATION") ADVANCED CARDIAC LIFE SUPPORT (ACLS) RECERTIFICATION EXAMINATION 1. Ten minutes after an 85 year old woman collapses, paramedics arrive and start CPR for the first time. The monitor shows fine (low amplitude)
ADVANCED CARDIAC LIFE SUPPORT (ACLS) RECERTIFICATION EXAMINATION 1. Ten minutes after an 85 year old woman collapses, paramedics arrive and start CPR for the first time. The monitor shows fine (low amplitude)
Unstable: Hypotension/Shock, Fever, Altered Mental Status, Chest discomfort, Acute Heart Failure Saturation <94%, Systolic BP < 90mmHg
 Bradycardia Heart Rate less than 50/min Stable: Monitor Seek expert help Treat Reversible Causes Unstable Signs and Symptoms: chest pain, shortness of breath, altered mental status, weak, Hypotension,
Bradycardia Heart Rate less than 50/min Stable: Monitor Seek expert help Treat Reversible Causes Unstable Signs and Symptoms: chest pain, shortness of breath, altered mental status, weak, Hypotension,
Adult Advanced Cardiovascular Life Support 2015 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular
 Adult Advanced Cardiovascular Life Support 2015 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care 1 DR. Alireza Abootalebi Assistant Professor Of
Adult Advanced Cardiovascular Life Support 2015 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care 1 DR. Alireza Abootalebi Assistant Professor Of
Atrial fibrillation in the ICU
 Atrial fibrillation in the ICU Atrial fibrillation Preexisting or incident (new onset) among nearly one in three critically ill patients Formation of arrhythogenic substrate usually fibrosis (CHF, hypertension,
Atrial fibrillation in the ICU Atrial fibrillation Preexisting or incident (new onset) among nearly one in three critically ill patients Formation of arrhythogenic substrate usually fibrosis (CHF, hypertension,
Advanced Cardiac Life Support
 Advanced Cardiac Life Support Algorithm Drugs Class I: definitely helpful, excellent Class II: Class II a -probably helpful; good to very good Class II b -possibly helpful; fair to good Class
Advanced Cardiac Life Support Algorithm Drugs Class I: definitely helpful, excellent Class II: Class II a -probably helpful; good to very good Class II b -possibly helpful; fair to good Class
ALS MODULE 7 Pharmacology
 ALS MODULE 7 Pharmacology Relates to HLT404C Apply Advanced Resuscitation Techniques Introduction There are no studies that addressed the order of drug administration. There is inadequate evidence to define
ALS MODULE 7 Pharmacology Relates to HLT404C Apply Advanced Resuscitation Techniques Introduction There are no studies that addressed the order of drug administration. There is inadequate evidence to define
MICHIGAN. State Protocols
 MICHIGAN State Protocols Protocol Number 5.1 5.2 5.3 5.4 5.5 Protocol Name Adult Cardiac Table of Contents General Cardiac Arrest Bradycardia Tachycardia Pulmonary Edema/CHF Chest Pain/Acute Coronary Syndrome
MICHIGAN State Protocols Protocol Number 5.1 5.2 5.3 5.4 5.5 Protocol Name Adult Cardiac Table of Contents General Cardiac Arrest Bradycardia Tachycardia Pulmonary Edema/CHF Chest Pain/Acute Coronary Syndrome
Advanced Resuscitation - Adult
 C02A Resuscitation 2017-03-23 17 years & older Office of the Medical Director Advanced Resuscitation - Adult Intermediate Advanced Critical From PRIMARY ASSESSMENT Known or suspected hypothermia Algorithm
C02A Resuscitation 2017-03-23 17 years & older Office of the Medical Director Advanced Resuscitation - Adult Intermediate Advanced Critical From PRIMARY ASSESSMENT Known or suspected hypothermia Algorithm
The most common. hospitalized patients. hypotension due to. filling time Rate control in ICU patients may be difficult as many drugs cause hypotension
 Arrhythmias in the critically ill ICU patients: Approach for rapid recognition & management Objectives Be able to identify and manage: Atrial fibrillation with a rapid ventricular response Atrial flutter
Arrhythmias in the critically ill ICU patients: Approach for rapid recognition & management Objectives Be able to identify and manage: Atrial fibrillation with a rapid ventricular response Atrial flutter
Emergency treatment to SVT Evidence-based Approach. Tran Thao Giang
 Emergency treatment to SVT Evidence-based Approach Tran Thao Giang Description ECG manifestations: HR is extremely rapid and regular (240bpm ± 40) P wave is: usually invisible When visible: anormal P axis,
Emergency treatment to SVT Evidence-based Approach Tran Thao Giang Description ECG manifestations: HR is extremely rapid and regular (240bpm ± 40) P wave is: usually invisible When visible: anormal P axis,
Adult Basic Life Support
 Adult Basic Life Support UNRESPONSIVE? Shout for help Open airway NOT BREATHING NORMALLY? Call 112* 30 chest compressions 2 rescue breaths 30 compressions *or national emergency number Fig 1.2_Adult BLS
Adult Basic Life Support UNRESPONSIVE? Shout for help Open airway NOT BREATHING NORMALLY? Call 112* 30 chest compressions 2 rescue breaths 30 compressions *or national emergency number Fig 1.2_Adult BLS
Review Packet EKG Competency This packet is a review of the information you will need to know for the proctored EKG competency test.
 Review Packet EKG Competency 2015 This packet is a review of the information you will need to know for the proctored EKG competency test. Normal Sinus Rhythm Rhythm: Regular Ventricular Rate: 60-100 bpm
Review Packet EKG Competency 2015 This packet is a review of the information you will need to know for the proctored EKG competency test. Normal Sinus Rhythm Rhythm: Regular Ventricular Rate: 60-100 bpm
SUMMARY OF MAJOR CHANGES 2010 AHA GUIDELINES FOR CPR & ECC
 SUMMARY OF MAJOR CHANGES 2010 AHA GUIDELINES FOR CPR & ECC The following is a summary of the key issues and changes in the AHA 2010 Guidelines for Cardiopulmonary Resuscitation (CPR) and Emergency Cardiac
SUMMARY OF MAJOR CHANGES 2010 AHA GUIDELINES FOR CPR & ECC The following is a summary of the key issues and changes in the AHA 2010 Guidelines for Cardiopulmonary Resuscitation (CPR) and Emergency Cardiac
Update of CPR AHA Guidelines
 Update of CPR AHA Guidelines Donald Hal Shaffner Course objective is to have an updated understanding of the American Heart Association s treatment algorithms for the management of cardiac decompensation
Update of CPR AHA Guidelines Donald Hal Shaffner Course objective is to have an updated understanding of the American Heart Association s treatment algorithms for the management of cardiac decompensation
ACLS Emergency Cardiac Drug Therapy (bolded = changes based on 2005 AHA ACLS Guidelines) revised 01/18/07
 revised 01/18/07") Oxygen Acute Chest Pain Suspected hypoxemia of any cause or c/o SOB Cardiopulmonary Arrest correct hypoxemia by O2 tension O2 content tissue oxygenation O2 Toxicity with high FIO2s May cause CO2 if a CO2
Oxygen Acute Chest Pain Suspected hypoxemia of any cause or c/o SOB Cardiopulmonary Arrest correct hypoxemia by O2 tension O2 content tissue oxygenation O2 Toxicity with high FIO2s May cause CO2 if a CO2
Advanced Cardiac Life Support G 2010
 Advanced Cardiac Life Support G 2010 Produced by the Advanced Cardiac Life Support Council of the Irish Heart Foundation March 2012 Introduction: The Arrhythmia and ACLS Councils of the Irish Heart Foundation
Advanced Cardiac Life Support G 2010 Produced by the Advanced Cardiac Life Support Council of the Irish Heart Foundation March 2012 Introduction: The Arrhythmia and ACLS Councils of the Irish Heart Foundation
HigHligHts of the 2018 Focused In 2015 Updates to the American Heart Association Guidelines for CPR and ECC: Advanced Cardiovascular Life
 Highlights of the 2018 Focused Updates to the American Heart Association Guidelines for CPR and ECC: Advanced Cardiovascular Life Support and Pediatric Advanced Life Support - Heart and Stroke Foundation
Highlights of the 2018 Focused Updates to the American Heart Association Guidelines for CPR and ECC: Advanced Cardiovascular Life Support and Pediatric Advanced Life Support - Heart and Stroke Foundation
Advanced Resuscitation - Child
 C02C Resuscitation 2017-03-23 1 up to 10 years Office of the Medical Director Advanced Resuscitation - Child Intermediate Advanced Critical From PRIMARY ASSESSMENT Known or suspected hypothermia Algorithm
C02C Resuscitation 2017-03-23 1 up to 10 years Office of the Medical Director Advanced Resuscitation - Child Intermediate Advanced Critical From PRIMARY ASSESSMENT Known or suspected hypothermia Algorithm
Blanchard Valley Hospital Pharmacy Code Blue Overview
 Blanchard Valley Hospital Pharmacy Code Blue Overview Adapted from Gary Spanik, RPh Edited by Kate Reeves, Pharm D, RPh Jon Manocchio, Pharm D, RPh Pharmacist Responsibilities Be aware of basic ACLS tenets
Blanchard Valley Hospital Pharmacy Code Blue Overview Adapted from Gary Spanik, RPh Edited by Kate Reeves, Pharm D, RPh Jon Manocchio, Pharm D, RPh Pharmacist Responsibilities Be aware of basic ACLS tenets
Asystole / PEA (PEDIATRIC)
") FRRCKSBURG MS Asystole / A (ATRC) 1 Check for Responsiveness Check for Breathing Check for Carotid ulse nitiate CR o As soon as a mechanical external compression device (i.e. Lucas 2) (rocedure 11) becomes
FRRCKSBURG MS Asystole / A (ATRC) 1 Check for Responsiveness Check for Breathing Check for Carotid ulse nitiate CR o As soon as a mechanical external compression device (i.e. Lucas 2) (rocedure 11) becomes
ADULT DRUG REFERENCE Drug Indication Adult Dosage Precautions / Comments
 ADENOSINE Paroxysmal SVT 1 st Dose 6 mg rapid IV 2 nd & 3 rd Doses 12 mg rapid IV push Follow each dose with rapid bolus of 20 ml NS May cause transient heart block or asystole. Side effects include chest
ADENOSINE Paroxysmal SVT 1 st Dose 6 mg rapid IV 2 nd & 3 rd Doses 12 mg rapid IV push Follow each dose with rapid bolus of 20 ml NS May cause transient heart block or asystole. Side effects include chest
PALS Case Scenario Testing Checklist Respiratory Case Scenario 1 Upper Airway Obstruction
 Respiratory Case Scenario 1 Upper Airway Obstruction Directs administration of 100% oxygen or supplementary oxygen as needed to support oxygenation Identifies signs and symptoms of upper airway obstruction
Respiratory Case Scenario 1 Upper Airway Obstruction Directs administration of 100% oxygen or supplementary oxygen as needed to support oxygenation Identifies signs and symptoms of upper airway obstruction
Cardiac Arrhythmias & Drugs used in Advanced Life Support and Cardiac Emergencies
 Cardiac Arrhythmias & Drugs used in Advanced Life Support and Cardiac Emergencies CNHE Ballarat Health Services Valid from 1 st March 2016 to 31 st June 2018 1 Supraventricular Tachycardia (SVT) An atrial
Cardiac Arrhythmias & Drugs used in Advanced Life Support and Cardiac Emergencies CNHE Ballarat Health Services Valid from 1 st March 2016 to 31 st June 2018 1 Supraventricular Tachycardia (SVT) An atrial
THE EVIDENCED BASED 2015 CPR GUIDELINES
 SAUDI HEART ASSOCIATION NATIONAL CPR COMMITTEE THE EVIDENCED BASED 2015 CPR GUIDELINES Page 1 Chapter 3 ACLS AND SPECIAL SITUATIONS CHAPTER The International Liaison Committee on Resuscitation (ILCOR)
SAUDI HEART ASSOCIATION NATIONAL CPR COMMITTEE THE EVIDENCED BASED 2015 CPR GUIDELINES Page 1 Chapter 3 ACLS AND SPECIAL SITUATIONS CHAPTER The International Liaison Committee on Resuscitation (ILCOR)
Emergency Cardiovascular Care: EMT-Intermediate Treatment Algorithms. Introduction to the Algorithms
 Emergency Cardiovascular Care: EMT-Intermediate Treatment Algorithms Introduction to the Algorithms Cardiac Arrest Algorithms Prehospital Medication Profiles Perspective regarding the EMT- Intermediate
Emergency Cardiovascular Care: EMT-Intermediate Treatment Algorithms Introduction to the Algorithms Cardiac Arrest Algorithms Prehospital Medication Profiles Perspective regarding the EMT- Intermediate
THE EVIDENCED BASED 2015 CPR GUIDELINES
 SAUDI HEART ASSOCIATION NATIONAL CPR COMMITTEE THE EVIDENCED BASED 2015 CPR GUIDELINES (EXECUTIVE SUMMARY) Page 1 FORWARD Since 2000, the International Liaison Committee on Resuscitation (ILCOR) has published
SAUDI HEART ASSOCIATION NATIONAL CPR COMMITTEE THE EVIDENCED BASED 2015 CPR GUIDELINES (EXECUTIVE SUMMARY) Page 1 FORWARD Since 2000, the International Liaison Committee on Resuscitation (ILCOR) has published
Treatment of Arrhythmias in the Emergency Setting
 Treatment of Arrhythmias in the Emergency Setting Zian H. Tseng, M.D. Assistant Professor of Medicine Cardiac Electrophysiology Section Cardiology Division University of California, San Francisco There
Treatment of Arrhythmias in the Emergency Setting Zian H. Tseng, M.D. Assistant Professor of Medicine Cardiac Electrophysiology Section Cardiology Division University of California, San Francisco There
Advanced Cardiac Life Support (ACLS) Science Update 2015
 Science Update 2015") 1 2 3 4 5 6 7 8 9 Advanced Cardiac Life Support (ACLS) Science Update 2015 What s New in ACLS for 2015? Adult CPR CPR remains (Compressions, Airway, Breathing Chest compressions has priority over all other
1 2 3 4 5 6 7 8 9 Advanced Cardiac Life Support (ACLS) Science Update 2015 What s New in ACLS for 2015? Adult CPR CPR remains (Compressions, Airway, Breathing Chest compressions has priority over all other
Michigan Adult Cardiac Protocols TABLE OF CONTENTS
 Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Asystole Section 2-1 Bradycardia Section 2-2 Cardiac Arrest General Section 2-3 Cardiac Arrest ROSC Section 2-4 Chest Pain Acute Coronary Syndrome
Date: November 15, 2012 Page 1 of 1 TABLE OF CONTENTS Asystole Section 2-1 Bradycardia Section 2-2 Cardiac Arrest General Section 2-3 Cardiac Arrest ROSC Section 2-4 Chest Pain Acute Coronary Syndrome
Advanced Resuscitation - Adolescent
 C02B Resuscitation 2017-03-23 10 up to 17 years Office of the Medical Director Advanced Resuscitation - Adolescent Intermediate Advanced Critical From PRIMARY ASSESSMENT Known or suspected hypothermia
C02B Resuscitation 2017-03-23 10 up to 17 years Office of the Medical Director Advanced Resuscitation - Adolescent Intermediate Advanced Critical From PRIMARY ASSESSMENT Known or suspected hypothermia
Routine Patient Care Guidelines - Adult
 Routine Patient Care Guidelines - Adult All levels of provider will complete an initial & focused assessment on every patient, and as standing order, use necessary and appropriate skills and procedures
Routine Patient Care Guidelines - Adult All levels of provider will complete an initial & focused assessment on every patient, and as standing order, use necessary and appropriate skills and procedures
Requirements to successfully complete PALS:
 The American Heart Association released new resuscitation science and treatment guidelines on October 19, 2010. The new AHA Handbook of Emergency Cardiac Care (ECC) contains these 2010 Guidelines.The 2010
The American Heart Association released new resuscitation science and treatment guidelines on October 19, 2010. The new AHA Handbook of Emergency Cardiac Care (ECC) contains these 2010 Guidelines.The 2010
PEDIATRIC SVT MANAGEMENT
 PEDIATRIC SVT MANAGEMENT 1 INTRODUCTION Supraventricular tachycardia (SVT) can be defined as an abnormally rapid heart rhythm originating above the ventricles, often (but not always) with a narrow QRS
PEDIATRIC SVT MANAGEMENT 1 INTRODUCTION Supraventricular tachycardia (SVT) can be defined as an abnormally rapid heart rhythm originating above the ventricles, often (but not always) with a narrow QRS
Updated Policies and Procedures # s 606, 607, 610, 611, 612, 613, 625, 628, 630, 631, and 633 (ACLS Protocols and Policies)
") SLO County Emergency Medical Services Agency Bulletin 2012-09 PLEASE POST Updated Policies and Procedures # s 606, 607, 610, 611, 612, 613, 625, 628, 630, 631, and 633 (ACLS Protocols and Policies) July
SLO County Emergency Medical Services Agency Bulletin 2012-09 PLEASE POST Updated Policies and Procedures # s 606, 607, 610, 611, 612, 613, 625, 628, 630, 631, and 633 (ACLS Protocols and Policies) July
Don t Forget the Basics
 Scary Arrhythmias in the Hospital Gregory M Marcus, MD, MAS Assistant Professor of Medicine Division of Cardiology University of California, San Francisc Don t Forget the Basics 79 yo man with a history
Scary Arrhythmias in the Hospital Gregory M Marcus, MD, MAS Assistant Professor of Medicine Division of Cardiology University of California, San Francisc Don t Forget the Basics 79 yo man with a history
Acute Arrhythmias in the Hospitalized Patient
 Acute Arrhythmias in the Hospitalized Patient Gregory M Marcus, MD, MAS Associate Professor of Medicine Division of Cardiology University of California, San Francisc Disclosures Medtronic: Research Support
Acute Arrhythmias in the Hospitalized Patient Gregory M Marcus, MD, MAS Associate Professor of Medicine Division of Cardiology University of California, San Francisc Disclosures Medtronic: Research Support
APPROACH TO TACHYARRYTHMIAS
 APPROACH TO TACHYARRYTHMIAS PROF.DR.MD.ZAKIR HOSSAIN PROFESSOR AND HEAD DEPARTMENT OF MEDICINE SZMCH TACHYARRYTHMIA Cardiac arrythmia is a disturbance of electrical rhythm of heart. Cardac arrythmia with
APPROACH TO TACHYARRYTHMIAS PROF.DR.MD.ZAKIR HOSSAIN PROFESSOR AND HEAD DEPARTMENT OF MEDICINE SZMCH TACHYARRYTHMIA Cardiac arrythmia is a disturbance of electrical rhythm of heart. Cardac arrythmia with
Rhythm Control: Is There a Role for the PCP? Blake Norris, MD, FACC BHHI Primary Care Symposium February 28, 2014
 Rhythm Control: Is There a Role for the PCP? Blake Norris, MD, FACC BHHI Primary Care Symposium February 28, 2014 Financial disclosures Consultant Medtronic 3 reasons to evaluate and treat arrhythmias
Rhythm Control: Is There a Role for the PCP? Blake Norris, MD, FACC BHHI Primary Care Symposium February 28, 2014 Financial disclosures Consultant Medtronic 3 reasons to evaluate and treat arrhythmias
1 of 6 1/8/2016 2:51 PM
 Official reprint from UpToDate www.uptodate.com 2016 UpToDate The content on the UpToDate website is not intended nor recommended as a substitute for medical advice, diagnosis, or treatment. Always seek
Official reprint from UpToDate www.uptodate.com 2016 UpToDate The content on the UpToDate website is not intended nor recommended as a substitute for medical advice, diagnosis, or treatment. Always seek
EKG Rhythm Interpretation Exam
 as EKG Rhythm Interpretation Exam Name: Date: ID# Unit Assume each strip is a 6 second strip. Passing is 80%. 1. Identify the following rhythm: a. Asystole b. Ventricular fibrillation c. Atrial fibrillation
as EKG Rhythm Interpretation Exam Name: Date: ID# Unit Assume each strip is a 6 second strip. Passing is 80%. 1. Identify the following rhythm: a. Asystole b. Ventricular fibrillation c. Atrial fibrillation
Cardiopulmonary Resuscitation in Adults
 Cardiopulmonary Resuscitation in Adults Fatma Özdemir, MD Emergency Deparment of Uludag University Faculty of Medicine OVERVIEW Introduction Pathophysiology BLS algorithm ALS algorithm Post resuscitation
Cardiopulmonary Resuscitation in Adults Fatma Özdemir, MD Emergency Deparment of Uludag University Faculty of Medicine OVERVIEW Introduction Pathophysiology BLS algorithm ALS algorithm Post resuscitation
Stayin Alive: Pediatric Advanced Life Support (PALS) Updated Guidelines
 Updated Guidelines") Stayin Alive: Pediatric Advanced Life Support (PALS) Updated Guidelines Margaret Oates, PharmD, BCPPS Pediatric Critical Care Specialist GSHP Summer Meeting July 16, 2016 Disclosures I have nothing to
Stayin Alive: Pediatric Advanced Life Support (PALS) Updated Guidelines Margaret Oates, PharmD, BCPPS Pediatric Critical Care Specialist GSHP Summer Meeting July 16, 2016 Disclosures I have nothing to
ADULT TREATMENT GUIDELINES
 A1 Adult Patient Care A2 Chest Pain / Suspected ACS A3 Cardiac Arrest Initial Care and CPR A4 Ventricular Fibrillation / Ventricular Tachycardia A5 PEA / Asystole A6 Symptomatic Bradycardia A7 Ventricular
A1 Adult Patient Care A2 Chest Pain / Suspected ACS A3 Cardiac Arrest Initial Care and CPR A4 Ventricular Fibrillation / Ventricular Tachycardia A5 PEA / Asystole A6 Symptomatic Bradycardia A7 Ventricular
1. What would you do first to restore oxygenation and ventilation to an unresponsive, breathless, near-drowning victim?
 ACLS Provider Course SAMPLE ACLS PRE-TEST EXAM This is a single-answer multiple-choice examination. There is only one correct answer to each question. 1. What would you do first to restore oxygenation
ACLS Provider Course SAMPLE ACLS PRE-TEST EXAM This is a single-answer multiple-choice examination. There is only one correct answer to each question. 1. What would you do first to restore oxygenation
1 Pediatric Advanced Life Support Science Update What s New for 2010? 3 CPR. 4 4 Steps of BLS Survey 5 CPR 6 CPR.
 1 Pediatric Advanced Life Support Science Update 2010 2 What s New for 2010? 3 CPR Take no longer than seconds for pulse check Rate at least on per minute (instead of around 100 per minute ) Depth change:
1 Pediatric Advanced Life Support Science Update 2010 2 What s New for 2010? 3 CPR Take no longer than seconds for pulse check Rate at least on per minute (instead of around 100 per minute ) Depth change:
4/14/15 HTEC 91. Topics for Today. Guess That Rhythm. Premature Ventricular Contractions (PVCs) Ventricular Rhythms
 Ventricular Rhythms") 4/14/15 Topics for Today HTEC 91 Medical Office Diagnostic Tests Week 5 Ventricular Rhythms PVCs: Premature Ventricular Contractions VT: Ventricular Tachycardia VF: Ventricular Fibrillation Asystole Study
4/14/15 Topics for Today HTEC 91 Medical Office Diagnostic Tests Week 5 Ventricular Rhythms PVCs: Premature Ventricular Contractions VT: Ventricular Tachycardia VF: Ventricular Fibrillation Asystole Study
ACLS: 2015 Update. What s new? Or:
 ACLS: 2015 Update Or: What s new? Mitchell Shulman MDCM FRCPC CSPQ Emergency Department, MUHC Master Instructor ACLS, QHSF Assist Professor, Dept of Surgery CME Faculty Disclosure Dr. Shulman has no affiliation
ACLS: 2015 Update Or: What s new? Mitchell Shulman MDCM FRCPC CSPQ Emergency Department, MUHC Master Instructor ACLS, QHSF Assist Professor, Dept of Surgery CME Faculty Disclosure Dr. Shulman has no affiliation
Chain of Survival. Highlights of 2010 American Heart Guidelines CPR
 Highlights of 2010 American Heart Guidelines CPR Compressions rate of at least 100/min. allow for complete chest recoil Adult CPR depth of at least 2 inches Child/Infant CPR depth of 1/3 anterior/posterior
Highlights of 2010 American Heart Guidelines CPR Compressions rate of at least 100/min. allow for complete chest recoil Adult CPR depth of at least 2 inches Child/Infant CPR depth of 1/3 anterior/posterior
Arrhythmic Complications of MI. Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine
 Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
The ABCs of EKGs/ECGs for HCPs. Al Heuer, PhD, MBA, RRT, RPFT Professor, Rutgers School of Health Related Professions
 The ABCs of EKGs/ECGs for HCPs Al Heuer, PhD, MBA, RRT, RPFT Professor, Rutgers School of Health Related Professions Learning Objectives Review the basic anatomy of the heart Describe the cardiac conducting
The ABCs of EKGs/ECGs for HCPs Al Heuer, PhD, MBA, RRT, RPFT Professor, Rutgers School of Health Related Professions Learning Objectives Review the basic anatomy of the heart Describe the cardiac conducting
MASTER SYLLABUS
 A. Academic Division: Health Sciences B. Discipline: Respiratory Care MASTER SYLLABUS 2018-2019 C. Course Number and Title: RESP 2330 Advanced Life Support Procedures D. Course Coordinator: Tricia Winters,
A. Academic Division: Health Sciences B. Discipline: Respiratory Care MASTER SYLLABUS 2018-2019 C. Course Number and Title: RESP 2330 Advanced Life Support Procedures D. Course Coordinator: Tricia Winters,
Case #1. 73 y/o man with h/o HTN and CHF admitted with dizziness and SOB Treated for CHF exacerbation with Lasix Now HR 136
 Tachycardias Case #1 73 y/o man with h/o HTN and CHF admitted with dizziness and SOB Treated for CHF exacerbation with Lasix Now HR 136 Initial Assessment Check Telemetry screen if pt on tele Telemetry
Tachycardias Case #1 73 y/o man with h/o HTN and CHF admitted with dizziness and SOB Treated for CHF exacerbation with Lasix Now HR 136 Initial Assessment Check Telemetry screen if pt on tele Telemetry
Arrhythmias. Sarah B. Murthi Department of Surgery University of Maryland Medical School R. Adams Cowley Shock Trauma Center
 Arrhythmias Sarah B. Murthi Department of Surgery University of Maryland Medical School R. Adams Cowley Shock Trauma Center 2012 Clinical Congress Presenter Disclosure Slide American College of Surgeons
Arrhythmias Sarah B. Murthi Department of Surgery University of Maryland Medical School R. Adams Cowley Shock Trauma Center 2012 Clinical Congress Presenter Disclosure Slide American College of Surgeons
Adult Drug Reference. Dopamine Drip Chart. Pediatric Drug Reference. Pediatric Drug Dosage Charts DRUG REFERENCES
 Adult Drug Reference Dopamine Drip Chart Pediatric Drug Reference Pediatric Drug Dosage Charts DRUG REFERENCES ADULT DRUG REFERENCE Drug Indication Adult Dosage Precautions / Comments ADENOSINE Paroxysmal
Adult Drug Reference Dopamine Drip Chart Pediatric Drug Reference Pediatric Drug Dosage Charts DRUG REFERENCES ADULT DRUG REFERENCE Drug Indication Adult Dosage Precautions / Comments ADENOSINE Paroxysmal
1 Cardiology Acute Care Day 22 April 2013 Arrhythmia Tutorial Course Material
 1 Cardiology Acute Care Day 22 April 2013 Arrhythmia Tutorial Course Material Arrhythmia recognition This tutorial builds on the ECG lecture and provides a framework for approaching any ECG to allow the
1 Cardiology Acute Care Day 22 April 2013 Arrhythmia Tutorial Course Material Arrhythmia recognition This tutorial builds on the ECG lecture and provides a framework for approaching any ECG to allow the
Antiarrhythmic Drugs
 Antiarrhythmic Drugs DR ATIF ALQUBBANY A S S I S T A N T P R O F E S S O R O F M E D I C I N E / C A R D I O L O G Y C O N S U L T A N T C A R D I O L O G Y & I N T E R V E N T I O N A L E P A C H D /
Antiarrhythmic Drugs DR ATIF ALQUBBANY A S S I S T A N T P R O F E S S O R O F M E D I C I N E / C A R D I O L O G Y C O N S U L T A N T C A R D I O L O G Y & I N T E R V E N T I O N A L E P A C H D /
ANZCOR Guideline 12.4 Medications and Fluids in Paediatric Advanced Life Support
 ANZCOR Guideline 12. Medications and Fluids in Paediatric Advanced Life Support Who does this guideline apply to? This guideline applies to infants and children. Summary Who is the audience for this guideline?
ANZCOR Guideline 12. Medications and Fluids in Paediatric Advanced Life Support Who does this guideline apply to? This guideline applies to infants and children. Summary Who is the audience for this guideline?
Rate and Rhythm Control of Atrial Fibrillation
 Rate and Rhythm Control of Atrial Fibrillation April 21, 2017 춘계심혈관통합학술대회 Jaemin Shim, MD, PhD Arrhythmia Center Korea University Anam Hospital Treatment of AF Goal Reducing symptoms Preventing complication
Rate and Rhythm Control of Atrial Fibrillation April 21, 2017 춘계심혈관통합학술대회 Jaemin Shim, MD, PhD Arrhythmia Center Korea University Anam Hospital Treatment of AF Goal Reducing symptoms Preventing complication
Based on the Guidelines 2000 for Cardiopulmonary Resuscitation & Emergency Cardiovascular Care EMERGENCY PHARMACOLOGY I & II. ADENOSINE (Adenocard)
") EMERGENCY PHARMACOLOGY I & II Advanced Cardiac Life Support Seminole Community College Based on the Guidelines 2000 for Cardiopulmonary Resuscitation & Emergency Cardiovascular Care International Consensus
EMERGENCY PHARMACOLOGY I & II Advanced Cardiac Life Support Seminole Community College Based on the Guidelines 2000 for Cardiopulmonary Resuscitation & Emergency Cardiovascular Care International Consensus
Utah EMS Protocol Guidelines: Cardiac
 Utah EMS Protocol Guidelines: Cardiac Version 1 / November 1, 2013 Cardiac Patient Care Guidelines These guidelines were created to provide direction for each level of certified provider in caring for
Utah EMS Protocol Guidelines: Cardiac Version 1 / November 1, 2013 Cardiac Patient Care Guidelines These guidelines were created to provide direction for each level of certified provider in caring for
The ALS Algorithm and Post Resuscitation Care
 The ALS Algorithm and Post Resuscitation Care CET - Ballarat Health Services Valid from 1 st July 2018 to 30 th June 2020 2 Defibrillation Produces simultaneous mass depolarisation of myocardial cells
The ALS Algorithm and Post Resuscitation Care CET - Ballarat Health Services Valid from 1 st July 2018 to 30 th June 2020 2 Defibrillation Produces simultaneous mass depolarisation of myocardial cells
CRC 431 ECG Basics. Bill Pruitt, MBA, RRT, CPFT, AE-C
 CRC 431 ECG Basics Bill Pruitt, MBA, RRT, CPFT, AE-C Resources White s 5 th ed. Ch 6 Electrocardiography Einthoven s Triangle Chest leads and limb leads Egan s 10 th ed. Ch 17 Interpreting the Electrocardiogram
CRC 431 ECG Basics Bill Pruitt, MBA, RRT, CPFT, AE-C Resources White s 5 th ed. Ch 6 Electrocardiography Einthoven s Triangle Chest leads and limb leads Egan s 10 th ed. Ch 17 Interpreting the Electrocardiogram
Pediatric Advanced Life Support Essentials
 chapter 14 Pediatric Advanced Life Support Essentials Sharon E. Mace, MD, FACEP, FAAP 1Discuss the new developments in resuscitation science. Review new 2010 2 American Heart Association Guidelines for
chapter 14 Pediatric Advanced Life Support Essentials Sharon E. Mace, MD, FACEP, FAAP 1Discuss the new developments in resuscitation science. Review new 2010 2 American Heart Association Guidelines for
Welcome to ACLS with Medical Education Angels!
 Welcome to ACLS with Medical Education Angels! For your greatest success, please be aware that the AHA assumes those taking ACLS have the ability to interpret and determine appropriate treatments for a
Welcome to ACLS with Medical Education Angels! For your greatest success, please be aware that the AHA assumes those taking ACLS have the ability to interpret and determine appropriate treatments for a
THE FOLLOWING QUESTIONS RELATE TO THE RESUSCITATION COUNCIL (UK) RESUSCITATION GUIDELINES 2005
 RESUSCITATION GUIDELINES 2005") THE FOLLOWING QUESTIONS RELATE TO THE RESUSCITATION COUNCIL (UK) RESUSCITATION GUIDELINES 2005 1. The guidelines suggest that in out-of-hospital cardiac arrests, attended but unwitnessed by health care
THE FOLLOWING QUESTIONS RELATE TO THE RESUSCITATION COUNCIL (UK) RESUSCITATION GUIDELINES 2005 1. The guidelines suggest that in out-of-hospital cardiac arrests, attended but unwitnessed by health care
ACLS. Advanced Cardiac Life Support Practice Test Questions. 1. The following is included in the ACLS Survey?
 1. The following is included in the ACLS Survey? a. Airway, Breathing, Circulation, Differential Diagnosis b. Airway, Breathing, Circulation, Defibrillation c. Assessment, Breathing, Circulation, Defibrillation
1. The following is included in the ACLS Survey? a. Airway, Breathing, Circulation, Differential Diagnosis b. Airway, Breathing, Circulation, Defibrillation c. Assessment, Breathing, Circulation, Defibrillation
Heart Failure (HF) Treatment
 Treatment") Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
ACLS: 2015 Update. Anything New?
 ACLS: 2015 Update Anything New? Mitchell Shulman MDCM FRCPC CSPQ Emergency Department, MUHC Master Instructor ACLS, QHSF Assist Professor, Dept of Surgery Copyright 2017 by Sea Courses Inc. All rights
ACLS: 2015 Update Anything New? Mitchell Shulman MDCM FRCPC CSPQ Emergency Department, MUHC Master Instructor ACLS, QHSF Assist Professor, Dept of Surgery Copyright 2017 by Sea Courses Inc. All rights
Atrial Fibrillation 10/2/2018. Depolarization & ECG. Atrial Fibrillation. Hemodynamic Consequences
 Depolarization & ECG Atrial Fibrillation How to make ORDER out of CHAOS Julia Shih, VMD, DACVIM (Cardiology) October 27, 2018 Depolarization & ECG Depolarization & ECG Atrial Fibrillation Hemodynamic Consequences
Depolarization & ECG Atrial Fibrillation How to make ORDER out of CHAOS Julia Shih, VMD, DACVIM (Cardiology) October 27, 2018 Depolarization & ECG Depolarization & ECG Atrial Fibrillation Hemodynamic Consequences
I have nothing to disclose.
 I have nothing to disclose. Antiarrhythmic Therapy in Pregnancy Prof. Ali Oto,MD,FESC,FACC,FHRS Department of Cardiology Hacettepe University,Faculty of Medicine Ankara Arrhythmias in pregnancy An increased
I have nothing to disclose. Antiarrhythmic Therapy in Pregnancy Prof. Ali Oto,MD,FESC,FACC,FHRS Department of Cardiology Hacettepe University,Faculty of Medicine Ankara Arrhythmias in pregnancy An increased
Antiarrhythmic Pharmacology. The Electronics
 Antiarrhythmic Pharmacology Linking Pharmacological Treatment to the Patient and the Rhythm Presented By: Karen Marzlin BSN, RN,C, CCRN-CMC CNEA 2009 1 The Electronics Action Potential of Cardiac Cells
Antiarrhythmic Pharmacology Linking Pharmacological Treatment to the Patient and the Rhythm Presented By: Karen Marzlin BSN, RN,C, CCRN-CMC CNEA 2009 1 The Electronics Action Potential of Cardiac Cells
ACLS & Beyond. Christa Creech, Pharm.D. PGY-2 Emergency Medicine Pharmacy Resident October 7 th, 2018
 ACLS & Beyond Christa Creech, Pharm.D. PGY-2 Emergency Medicine Pharmacy Resident October 7 th, 2018 Objectives List recent changes to ACLS guidelines applicable to pharmacists Recognize reversible causes
ACLS & Beyond Christa Creech, Pharm.D. PGY-2 Emergency Medicine Pharmacy Resident October 7 th, 2018 Objectives List recent changes to ACLS guidelines applicable to pharmacists Recognize reversible causes
Chapter 03: Sinus Mechanisms Test Bank MULTIPLE CHOICE
 Instant download and all chapters Tesst Bank ECGs Made Easy 5th Edition Barbara J Aehlert https://testbanklab.com/download/tesst-bank-ecgs-made-easy-5th-edition-barbara-jaehlert/ Chapter 03: Sinus Mechanisms
Instant download and all chapters Tesst Bank ECGs Made Easy 5th Edition Barbara J Aehlert https://testbanklab.com/download/tesst-bank-ecgs-made-easy-5th-edition-barbara-jaehlert/ Chapter 03: Sinus Mechanisms
Anti arrhythmic drugs. Hilal Al Saffar College of medicine Baghdad University
 Anti arrhythmic drugs Hilal Al Saffar College of medicine Baghdad University Mechanism of Arrhythmia Abnormal heart pulse formation Abnormal heart pulse conduction Classification of Arrhythmia Abnormal
Anti arrhythmic drugs Hilal Al Saffar College of medicine Baghdad University Mechanism of Arrhythmia Abnormal heart pulse formation Abnormal heart pulse conduction Classification of Arrhythmia Abnormal