THE IMPACT OF HYPERTENSION GUIDELINES. Daniel Lackland
|
|
|
- Aldous Hodges
- 5 years ago
- Views:
Transcription
1 THE IMPACT OF HYPERTENSION GUIDELINES Daniel Lackland
2 Disclosures Member of NHLBI Risk Assessment Workgroup Member of 2014 Hypertension Guidelines (JNC 8) Member of Evidence Rating Committee for ACC/AHA Hypertension Guidelines No financial disclosures
3 Objectives To describe the population risk of elevated blood pressure To describe the evidence and impact of lowering of elevated blood pressure To describe the process and considerations of target blood pressures for clincal practice guidelines.
4 Stroke. 45(1):315-53, 2014 Stroke. 45(1):315-53,
5 EFFECT OF INTENSIVE BP REDUCTION ON THE RISK OF STROKE Stroke Study HOT, 1998 Adding UKPDS-38, 1998 Adding ABCD (H), 2000 Adding AASK, 2002 Adding ABCD (N), 2002 Adding JATOS, 2008 Adding Cardio-Sis, 2009 Adding ACCORD BP, 2010 Adding VALISH, 2010 Adding HOMED-BP, 2012 Adding SPS3, 2013 Adding Wei et al., 2013 Adding SPRINT, 2015 Cumulative estimate Random effects model Odds Ratio O R 95%-Cl [0.832; 1.363] [0.419; 1.504] [0.516; 1.348] [0.619; 1.204] [0.534; 1.142] [0.632; 1.158] [0.610; 1.110] [0.578; 1.024] [0.591; 0.992] [0.627; 1.022] [0.665; 0.990] [0.648; 0.955] [0.676; 0.952] [0.676; 0.952] Z=2.523; p=0.011 I %; p= More 5 Intensive Better Less Intensive 5 Better Verdecchia et al. Hypertension. 2016;68:
6
7 Systolic and Diastolic Treatment Levels by Guidelines Report Systolic Blood Pressure Diastolic Blood Pressure JNC I No Systolic Level Identified 90 mmhg JNC II No Systolic Level Identified 90 mmhg JNC III 160 mmhg 90 mmhg JNC IV 160 mmhg 90 mmhg JNC V 140 mmhg 90 mmhg JNC VI 140 mmhg 90 mmhg JNC mmhg 90 mmhg JNC 8 Panel 150 mmhg 90 mmhg
8 Population-Based Strategy SBP Distributions After Intervention Before Intervention Reduction in BP JAMA. 2003;289: Reduction in SBP mmhg % Reduction in Mortality Stroke CHD Total
9 Median and 90 th Percentile Systolic BP Declined in years Figure 5c: Smoothed weighted frequency distribution, median, and 90th percentile of SBP: US , age NHES ( ) NHANES I ( ) NHANES II ( ) NHANES III ( ) Stroke. 45(1):315-53, American Heart Association, Inc. All rights reserved. Unauthorized use prohibited. 9
10 Median and 90 th Percentile Systolic BP Declined in years Figure 5d: Smoothed weighted frequency distribution, median, and 90th percentile of SBP: US , age NHES ( ) NHANES I ( ) NHANES II ( ) NHANES III ( ) Stroke. 45(1):315-53, Stroke. Stroke. 45(1):315-53, (1):315-53, 2014 American Heart Association, Inc. All rights reserved. Unauthorized use prohibited. 10
11 Actuaries Report VA Trials JNC I JNC III JNC V JNC 7 JNC II JNC IV JNC VI
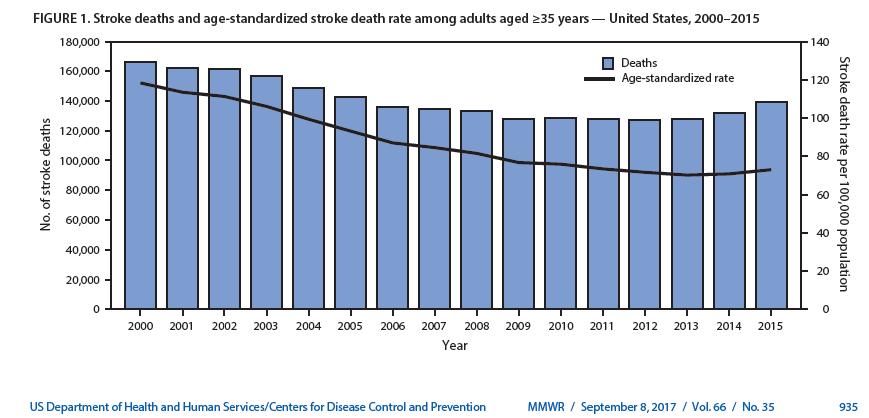
12 Age-Adjusted Death Rates for Cerebrovascular Disease by Year United States, Rates per 100,000 population, standardized to the U.S standard population Diseases were classified to the International Classification of Disease codes in use at the time the deaths were reported American Heart Association, Inc. All rights reserved. Unauthorized use prohibited. 12 Stroke. 45(1):315-53, 2014
13 Mean Systolic Blood Pressure (SBP) by Time Period NHANES I-IV TABLE 1 YEAR SBP (Hg) mm mm mm mm mm mm mm Stroke. 45(1):315-53, American Heart Association, Inc. All rights reserved. Unauthorized use prohibited. 13
14 Mean and 90 th Percentile Systolic Blood Pressure by Time Period and Age Group years years years Median 90 th Percentile Median 90 th Percentile Median 90 th Percentile mmhg 137 mmhg 127 mmhg 155 mmhg 148 mmhg 188 mmhg mmhg 126 mmhg 118 mmhg 138 mmhg 129 mmhg 156 mmhg
15 Age-adjusted Deaths per 100, Source: NVSS. Stroke: I60-I69 US Age-Adjusted Stroke Mortality Rates Actual vs. 20% Impact Goal Scenario Actual 20% Target Scenario Year
16

17 JAMA. 2013;310(7): Select the subtitle text box above, copy, and paste it on to the slide that requires a subtitle Horizontal position setting for subtitle is 0.5" Vertical position setting for subtitle is 1.35" Keep subtitle to one line of text Follow these subtitle placement guidelines to ensure consistent positioning throughout the presentation 17
18 18 KPNC NCQA HEDIS Control Rate vs. National and California Rates
19 Falling CV Morbidity and Mortality - KPNC Since Year 2000: 30% reduction in mortality from CVD 42% reduction in mortality from stroke Sidney S, Jaffe M, Nguyen-Hyunha M, Kushi L, Young J, Sorel M, Selby J, Go A. Closing the Gap Between Cardiovascular and Cancer Mortality in an Integrated Health Care Delivery System, : The Kaiser Permanente Experience. Circulation 2011; 124: A
20 2017 Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults In 2014, a 21 member multidisciplinary Writing Committee appointed to develop the guideline: Cardiologists, epidemiologists, internists, endocrinologist, geriatrician, nephrologist, neurologist, nurse, pharmacist, physician assistant, 2 lay/patient representatives Representation for each of the 11 participating professional organizations No Writing Committee member had a relevant relationship with industry Writing Committee Paul K. Whelton, MB, MD, MSc, FAHA, Chair Robert M. Carey, MD, FAHA, Vice Chair
21 Whelton PK, Carey RM, Aronow WS, Casey DE, Collins KJ, Dennison Himmelfarb C, DePalma SM, Gidding S, Jamerson KA, Jones DW, MacLaughlin EJ, Muntner P, Ovbiagele B, Smith SC, Spencer CC, Stafford RS, Taler SJ, Thomas RJ, Williams KA, Williamson JD, Wright JT ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines.
22 2017 Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults ACC/AHA Guideline Methodology Active participation of all Writing Committee members Comprehensive structured review of the literature Four questions referred to independent Evidence Review Committee for conduct of a systematic review and meta-analysis Evidence Review Committee David M. Rebouissin, PhD, Chair Norinna B. Allen, PhD, MPH, FAHA Edgar (Pete) R Miller III, PhD, MD Michael E. Griswold, PhD Tamar Polonsky, MD, MSCI Eliseo Guallar, MD Angela M Thompson-Paul, PhD, MSPH Yuling Hong, MD, MSc, PhD Suma Vupputuri, PhD, MPH, FAHA Daniel T Lackland, DrPH, FAHA, FASH
23 2017 Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults Number Population, Intervention, Comparator, Outcome, Timing, Setting (PICOTS) formatted Questions 1 Is there evidence that self-directed monitoring of BP and/or ambulatory BP monitoring are superior to office-based measurement of BP by a healthcare worker for 1) preventing adverse outcomes for which high BP is a risk factor and 2) achieving better BP control? 2 What is the optimal target for BP lowering during antihypertensive therapy in adults? 3 In adults with hypertension, do various antihypertensive drug classes differ in their comparative benefits and harms? 4 In adults with hypertension, does initiating treatment with antihypertensive pharmacological monotherapy versus initiating treatment with 2 drugs (including fixed-dose combination therapy), either of which may be followed by the addition of sequential drugs, differ in comparative benefits and/or harms on specific health outcomes? ERC determined data insufficient to answer quest
24 2017 Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults Class (Strength) of Recommendation Level (Quality) of Evidence I Strong: Benefit >>> Risk A High quality evidence from >1 RCT or meta-analysis IIa Moderate: Benefit >> Risk B-R Moderate quality evidence from 1 RCT or meta-analysis (Randomized) IIb III: No Benefit III: Harm Weak: Benefit Risk Moderate: Benefit = Risk Strong: Risk > Benefit B-NR C-LD Moderate quality evidence from 1 well designed/executed non-randomized, observational or registry studies or meta-analyses of such studies (Nonrandomized) Moderate quality evidence from randomized, observational or registry studies, meta-analyses of such studies, or physiological/mechanistic studies in humans (Limited Data) C-EO Consensus of expert opinion (Expert Opinion)
25 2017 Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults Guideline Content 15 sections that provide 106 Recommendations Typical section format List of recommendations Supported by principal references Details of principal and other references in Data Supplement tables Synopsis and recommendation-specific supportive text Complete list of section-specific references accompanying each section
26 2017 Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults BP measurement New BP classification system Selected Highlights New approach to treatment decisions for management of hypertension Lower targets for BP during treatment of hypertension Strategies to improve BP control during treatment of hypertension
27 Blood Pressure (BP) and Cardiovascular Disease (CVD) Risk Systolic Blood Pressure (SBP) Diastolic Blood Pressure (DBP) 256 Age at risk: years 256 Age at risk: years IHD Mortality (Floating Absolute Risk and 95% CI) years years years years IHD Mortality (Floating Absolute Risk and 95% CI) years years years years Usual SBP (mm Hg) Usual DBP (mm Hg) Lewington et al. Lancet. 2002;360:
28 Recommendation Recommendation for Definition of High Blood Pressure (BP) COR LOE Recommendations I B-NR 1. BP should be categorized as normal, elevated, or stages 1 or 2 hypertension in order to prevent and treat high BP
29 Changes in BP Categories from JNC7 to the New Guideline SBP DBP JNC ACC/AHA <120 and <80 Normal BP and <80 Prehypertension or Prehypertension or Stage 1 hypertension 160 or 100 Stage 2 hypertension The categorization of BP should be based on the average of 2 readings on 2 occasions following a standardized protocol.
30 Changes in BP Categories from JNC7 to the New Guideline SBP DBP JNC ACC/AHA <120 and <80 Normal BP Normal BP and <80 Prehypertension Elevated BP or Prehypertension Stage 1 hypertension or Stage 1 hypertension Stage 2 hypertension 160 or 100 Stage 2 hypertension Stage 2 hypertension The categorization of BP should be based on the average of 2 readings on 2 occasions following a standardized protocol.
31 Rationale for BP Categorization in the ACC/AHA Guideline Observational data related to the association between SBP/DBP and CVD risk. Randomized trials of lifestyle modification to lower BP. Treatment with antihypertensive medication to lower BP and prevent CVD.
32 Association between SBP/DBP and CVD risk Several meta-analyses have reported a gradient of progressively higher CVD risk going from normal BP to elevated BP to hypertension. Systolic/Diastolic blood pressure, mm Hg Outcome <120/ / /85-89 Cardiovascular mortality Ref 1.24 ( ) 1.56 ( ) Stroke Ref 1.35 ( ) 1.95 ( ) Coronary heart disease Ref 1.11 ( ) 1.33 ( ) Myocardial infarction Ref 1.43 ( ) 1.99 ( ) Guo et. al. Current Hypertension Reports 2013; 15: Guoet. al. PLoSOne, 2013; 8e Huang et. al. Neurology, 2014; 82: Huang et. al. American Journal of Kidney Diseases, 2014; 63: Lee et. al., Neurology 2011; 77: Shen, American Journal of Cardiology, 2013; 112:
33 Randomized Trials Nonpharmacological interventions Trials have shown the benefit of lowering BP among those with SBP/DBP 130/80 mm Hg through: Weight loss among overweight/obese adults. Heart healthy diet (e.g., DASH diet) Sodium reduction Potassium supplementation Increased physical activity Alcohol reduction Whelton et. al. JAMA, 2002; 288:
34 Randomized Trials Pharmacological interventions Three randomized trials have evaluated pharmacological antihypertensive treatment in adults without hypertension. ECG Index Baseline 18-months Change (95% CI) Sokolow-Lyon Voltage, mm Chlorthalidone/Amiloride 21.8 ± ± (0.45, 1.63) Placebo 21.5 ± ± (-0.61, 0.68) Duration product, µvms Chlorthalidone/Amiloride 229 ± ± (5.7, 25.2) Placebo 223 ± ± (-11.0, 8.2) p-value=0.02 comparing chlorthalidone/amiloride ver Fuchs et. al., Journal of the American Heart Association, 2016; 5: e Julius et. al. New England Journal of Medicine, 2006; 354: Luders et. al., Journal of Hypertension, 2008; 26:
 Muntner, et. al.")
35 Distribution of US adults into BP Categories NHANES Prevalence of hypertension: 45.6% Muntner et. al., Journal of the American College of Cardiology 2017 (in press) Muntner, et. al., Circulation 2017 (in press)
 Muntner, et. al., Circulation 2017 (in press)")
36 Prevalence of Hypertension 2017 ACC/AHA and JN7 Guidelines Prevalence of hypertension, % Number of US adults with hypertension, millions Muntner et. al., Journal of the American College of Cardiology 2017 (in press) Muntner, et. al., Circulation 2017 (in press)
37 Summary The 2017 ACC/AHA guideline uses lower BP thresholds to define hypertension: SBP 130 mm Hg DBP 80 mm Hg The prevalence of hypertension among US adults is 46% using this definition. Approximately 103 million US adults have hypertension according to the new guideline.
38 BP TREATMENT THRESHOLD AND THE USE OF ASCVD RISK ESTIMATION TO GUIDE DRUG TREATMENT OF HYPERTENSION Recommendations for BP Treatment Threshold and Use of ASCVD Risk Estimation* to Guide Drug Treatment of Hypertension COR LOE Recommendations I SBP: A DBP: C-EO 1. Use of BP-lowering medications is recommended for secondary prevention of recurrent CVD events in patients with clinical CVD and an average SBP of 130 mm Hg or higher or an average DBP of 80 mm Hg or higher, and for primary prevention in adults with an estimated 10-year atherosclerotic cardiovascular disease (ASCVD) risk of 10% or higher and an average SBP 130 mm Hg or higher or an average DBP 80 mm Hg or higher. I C-LD 2. Use of BP-lowering medication is recommended for primary prevention of CVD in adults with no history of CVD and with an estimated 10-year ASCVD risk <10% and an SBP of 140 mm Hg or higher or a DBP of 90 mm Hg or higher * ACC/AHA Pooled Cohort Equations to estimate 10-y risk of ASCVD. ASCVD was defined as a first nonfatal MI or CHD death, or fatal or nonfatal stroke among adults free of CVD.
39 ACC/AHA POOLED COHORT EQUATIONS To estimate the 10-year risk of atherosclerotic CVD
40 IS THERE ANY DIFFERENCE IN EXPECTED BENEFIT FROM BP LOWERING ACCORDING TO CVD RISK? Yes Data from the BP Lowering Treatment Trialists Collaboration meta-analysis provided empirical evidence that the absolute benefits achieved with BPlowering therapy are driven by the combination of CVD risk factors determining risk of a CVD event rather than simply the BP level in isolation. Thus, the most intensive BP-lowering therapies should be directed to those at highest CVD risk. Sundstrom J et al. Blood Pressure Lowering Treatment Trialists. Lancet.2014;384;
41 DIFFERENCES IN CVD EVENTS ASSOCIATED WITH ANTIHYPERTENSIVE MEDICATIONS IN 11 TRIALS (>50,000 PATIENTS) Risk Ratios Relative Risk Reduction Absolute Risk Reduction <11% 11%-15% 15%-21% >21% <11% 11%-15% 15%-21% >21% Blood Pressure Lowering Treatment Trialists Collaboration. Lancet.2014;384;
42 TEN-YEAR PREDICTED CVD RISK FOR HYPOTHETICAL LOW, INTERMEDIATE AND HIGH RISK ADULTS 10-Year Predicted CVD Risk 50% 40% 30% 20% 10% 0% Global ASCVD Risk Low Intermediate High 0.8% 12.3% 30.3% Muntner P, Whelton PK. JACC. 2017;69: % 16.2% 110 mm Hg 130 mm Hg Systolic Blood Pressure 38.4%
43 RISK-BASED TREATMENT OF HYPERTENSION Treating 1,000 hypertensuve people Events 5-Y ASCVD Risk (%) Prevented (5Y) NNT* < > * Number needed to treat (NNT) to prevent 1 event: Blood Pressure Lowering Treatment Trialists. Lancet.2014;384;

44 CVD EVENTS AVOIDED BY BASELINE RISK AND MAGNITUDE OF SBP LOWERING Sundstrom et al. Lancet. 2014;384: Cardiovascular events avoided per Systolic blood pressure reduction (mm Hg) > <11
45 BP & PREDICTED CVD RISK IN DRUG TREATMENT DECISION-MAKING The predicted risk of CVD between 2 people with the same SBP can differ by 20-fold based on the individual s global ASCVD risk. The increase in predicted CVD risk with higher BP is small among otherwise low-risk individuals but is much higher in those with higher ASCVD risk scores. Clinical trials and meta-analyses are based on participants with high ASCVD risk. CVD risk can be predicted by equations such as the AHA/ACC 2013 Pooled Cohort CVD Risk Equations** (based on BP, age, history of CVD, diabetes, LDL cholesterol and smoking). Therefore, one can rationalize utilizing ASCVD risk calculations in antihypertensive drug treatment decisions. ** Goff DC Jr et al AHA/ACC guideline on the assessment of cardiovascular risk. J Am Coll Cardiol. 2013;
46 BOTTOM LINE Data from RCTs strongly suggest that patients with higher global ASCVD risk will receive a greater absolute risk reduction benefit from antihypertensive medication. Simulation studies suggest that employing ASCVD risk in conjunction with BP levels would result in treating fewer people with antihypertensive medication while preventing more CVD events and saving more quality-adjusted life years.
47 BP THRESHOLDS AND RECOMMENDATIONS FOR TREATMENT AND FOLLOW UP BP thresholds and recommendations for treatment and follow-up Normal BP (BP <120/80 mm Hg) Elevated BP (BP /<80 mm Hg) Stage 1 Hypertension (BP /80-89 mm Hg) Stage 2 Hypertension (BP >140/90 mm Hg) Promote optimal lifestyle habits (Class I) Non-pharmacologic therapy (Class I) Clinical CVD or estimated 10 y ASCVD risk 10% No Yes Reassess in 1 y (Class IIa) Reassess in 3-6 mo (Class I) Nonpharmacologic therapy (Class I) Non-pharmacologic therapy and BP lowering medication (Class I) Non-pharmacologic therapy and BP lowering medication (Class I) Reassess in 3-6 mo (Class I) Reassess in 1 mo (Class 1)
48 SUMMARY Benefits of using both BP and ASCVD risk assessment in determining BP thresholds for antihypertensive drug therapy Treatment is focused on patients most likely to have events More CVD events are prevented Larger absolute CVD risk reduction with treatment Lower number needed-to-treat to prevent one CVD event More quality-adjusted life years are saved Lower cost of care
49 Blood Pressure Goals for Patients Diagnosed with Hypertension
50 Approach to Determining the Optimal BP Target 1. The question was assigned to an independent evidence review committee for systematic review and meta-analysis in PICOT format. 2. Simultaneously, the writing group conducted a review of the literature
51 Meta Analysis of Trials of Intensive BP Targets Adapted from Thomopolus, Parati, and Zanchetti Journal pf Hypertension 2016
52 More intensive blood pressure lowering significantly reduced CV risk CV Event Relative Risk 95% CI MI Stroke Heart failure CVD composite A target of <130 mm Hg may significantly reduce the risk MI, stroke, heart failure, and major CVD events.
53 Summary Several large RTC s testing intensive BP targets have concluded since the JNC7 Report Systematic review, meta-analysis, and one RTC provide strong evidence for recommending SBP 130 mm Hg DBP 80 mm Hg for those with elevated risk for CVD (10 year risk 10%)
54 Significance of Out of Office BP Readings Guideline calls for greater use of out of office BP measurements (ABPM or HBPM) for both the diagnosis and management of hypertension. A major reason is to identify patients on no antihypertensive medication with: White Coat Hypertension (WCH) with elevated office BPs who may not require drug treatment and Masked Hypertension (MH) with normal office readings who should be considered for drug treatment In addition, in those on antihypertensive medications, to identify White Coat Effect (WCE) where office BPs are significantly higher than out of office readings Masked Uncontrolled Hypertension (MUCH) where office readings indicate adequate BP control but out of office readings are elevated
55 Recommendations for Patients (Not on Antihypertensive Drugs) to Identify WCH COR LOE RECOMMENDATIONS IIa IIa B-NR In adults with an untreated SBP greater than 130 mm Hg but less than 160 mm Hg or DBP greater than 80 mm Hg but less than 100 mm Hg, it is reasonable to screen for the presence of white coat hypertension by using either daytime ambulatory blood pressure monitoring (ABPM) or HBPM before diagnosis of hypertension. C-LD In adults with white coat hypertension, periodic monitoring with either ABPM or HBPM is reasonable to detect transition to sustained hypertension.
56 Cohort, sex, and age-standardized incidence of cardiovascular events in untreated and treated normotensive (NT) and masked hypertensive (MHT) nondiabetic subjects that are derived from an IDACO (International Database on Ambulatory Blood Pressure in Relation to Cardiovascular Outcomes) meta-analysis. 17 Fully adjusted hazard ratios (HRs) for treated vs untreated masked hypertensives are as follows: HR, 2.27 (95% confidence interval, ; P<0.0001). Stanley S. Franklin et al. Hypertension. 2015;65:16-20 Copyright American Heart Association, Inc. All rights reserved.
57 Recommendations for Patients (Not on Antihypertensive Drugs) to Identify MH COR LOE RECOMMENDATIONS IIa B-NR In adults with an untreated SBP greater than 130 mm Hg but less than 160 mm Hg or DBP greater than 80 mm Hg but less than 100 mm Hg, it is reasonable to screen for the presence of white coat hypertension by using either daytime ambulatory blood pressure monitoring (ABPM) or HBPM before diagnosis of hypertension. IIa C-LD In adults with white coat hypertension, periodic monitoring with either ABPM or HBPM is reasonable to detect transition to sustained hypertension.
58 Recommendations for Patients on Antihypertensive Drug Treatment COR LOE RECOMMENDATIONS IIb C-LD In adults on multiple drug therapies for hypertension and office BPs within 10 mm Hg above goal, it may be reasonable to screen for white coat effect with HBPM (or ABPM). IIa C-LD In adults being treated for hypertension with office BP readings not at goal and HBPM readings suggestive of a significant white coat effect, confirmation by ABPM can be useful. IIb C-EO In adults being treated for hypertension with elevated HBPM readings suggestive of masked uncontrolled hypertension, confirmation of the diagnosis by ABPM might be reasonable before intensification of antihypertensive drug treatment.

59 Detection of White Coat Hypertension or Masked Hypertension in Patients not on Drug Therapy

60 Detection of White Coat Hypertension or Masked Hypertension in Patients on Drug Therapy

61 Recommendations for BP Goal for Patients with Hypertension
62 2017 Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults Class (Strength) of Recommendation Level (Quality) of Evidence I Strong: Benefit >>> Risk A High quality evidence from >1 RCT or meta-analysis IIa Moderate: Benefit >> Risk B-R Moderate quality evidence from 1 RCT or meta-analysis (Randomized) IIb III: No Benefit III: Harm Weak: Benefit Risk Moderate: Benefit = Risk Strong: Risk > Benefit B-NR C-LD Moderate quality evidence from 1 well designed/executed non-randomized, observational or registry studies or meta-analyses of such studies (Nonrandomized) Moderate quality evidence from randomized, observational or registry studies, meta-analyses of such studies, or physiological/mechanistic studies in humans (Limited Data) C-EO Consensus of expert opinion (Expert Opinion)
63 2017 Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults BP measurement New BP classification system Selected Highlights New approach to treatment decisions for management of hypertension Lower targets for BP during treatment of hypertension Strategies to improve BP control during treatment of hypertension
64 2017 Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults BP Classification (JNC 7 and ACC/AHA Guidelines) SBP DBP JNC ACC/AHA <120 and <80 Normal BP Normal BP and < or or or 100 Prehypertension Prehypertension Stage 1 hypertension Stage 2 hypertension Elevated BP Stage 1 hypertension Stage 2 hypertension Stage 2 hypertension Blood Pressure should be based on an average of 2 careful readings on 2 occasions Adults with SBP or DBP in two categories should be designated to the higher BP category
65 2017 Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults BP Thresholds for Treatment SBP DBP <120 and < and < or or or or 90 CVD Risk/other circumstances N/A N/A No CVD/10-yr ASCVD risk <10% CVD/10-year ASCVD risk 10% Diabetes or CKD Age 65 years N/A Recommended Treatment Healthy Lifestyle Nonpharmacological therapy Nonpharmacological therapy Antihypertensive drug therapy (plus nonpharmacological therapy) Blood Pressure should be based on an average of 2 careful readings on 2 occasions Adults with SBP or DBP in two categories should be designated to the higher BP category
66 2017 Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults High BP Treatment Target SBP DBP <120 and < and < or or or or CVD Risk N/A N/A No CVD and 10-year ASCVD risk <10% Clinical CVD or 10-year ASCVD risk 10% Diabetes or CKD N/A Age 65 years Recommended Treatment N/A N/A SBP <130 and DBP <80 mm Hg SBP <130 mm Hg
67 Summary 2013: NHLBI transferred responsibility for CVD prevention CPGs to ACC and AHA ACC/AHA partnered with nine professional organizations to sponsor new BP CPG 2014: 21 member multidisciplinary Writing Committee charged to develop the CPG 2017 ACC/AHA BP CPG Comprehensive report 15 sections: 106 recommendations, each characterized by COR and LOE Extensive referencing and provision of 448 supplementary evidence tables Selected areas of interest: BP measurement New system for BP classification New thresholds for initiation of antihypertensive drug therapy In stage1 hypertension, use of ASCVD risk estimation to determine whether to treat with: Nonpharmacological therapy alone ( low risk patients) Antihypertensive drug therapy, in addition to nonpharmacological therapy ( high risk patients) New target for BP control during treatment of hypertension


68 Whelton PK, Carey RM, Aronow WS, Casey DE, Collins KJ, Dennison Himmelfarb C, DePalma SM, Gidding S, Jamerson KA, Jones DW, MacLaughlin EJ, Muntner P, Ovbiagele B, Smith SC, Spencer CC, Stafford RS, Taler SJ, Thomas RJ, Williams KA, Williamson JD, Wright JT ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines.

69 MMWR January 8, 2016 / Vol. 64 / No. 52
70
71 Effect of Sodium Reduction (Higher to Lower) in African-Americans and Non-African-Americans on the Control Diet Change in BP African-Americans P< P< P-interaction < 0.05 Non-African-Americans P< P<.001 Systolic BP Diastolic BP
72 Most Salt Comes from Processed and Restaurant Foods Processed and restaurant foods Naturally occurring 77% 12% While eating 6% Home cooking 5% Source: Mattes, RD. Journal of American College Nutrition, 1991, 10:

73 Most Salt Comes from Processed and Restaurant Foods How much sodium is in a Chicken Cesar Salad at the Costco Food Court? A. 2680mg B. 725 mg C mg D mg

74 Most Salt Comes from Processed and Restaurant Foods How much sodium is an order of PF Chang s, double pan fried noodles with pork? A mg B mg C mg D mg

75 2/3 LB** Double Bacon Cheese Thickburger Serving size (grams) = 462 Calories = 1300 Calories from fat = 860 Total fat = 96 grams Saturated fat = 40 grams Cholesterol = 205 mg Sodium = 2110 mg Total Carbohydrates = 51 grams
76 Diabetes, Black Pooling Project Caucasians African Americans < 50 years years 60+ years
77 Hypertension and Diabetes, Black Pooling Project Percent of Hypertensvies Normal Prehypertension Stage 1 Stage 2 Level of Hypertension
78

79

80 STRIKE OUT STROKE
Summary, Scope, BP Classification, BP thresholds and Targets
 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/ PCNA Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults Summary, Scope, BP Classification, BP thresholds
2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/ PCNA Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults Summary, Scope, BP Classification, BP thresholds
Aquifer Hypertension Guidelines Module
 Aquifer Hypertension Guidelines Module 2018 Aquifer Hypertension Guidelines Module 1 1. Introduction. In 2013 the National Heart Lung and Blood Institute (NHLBI) asked the American College of Cardiology
Aquifer Hypertension Guidelines Module 2018 Aquifer Hypertension Guidelines Module 1 1. Introduction. In 2013 the National Heart Lung and Blood Institute (NHLBI) asked the American College of Cardiology
HYPERTENSION: ARE WE GOING TOO LOW?
 HYPERTENSION: ARE WE GOING TOO LOW? George L. Bakris, M.D.,F.A.S.N.,F.A.S.H., F.A.H.A. Professor of Medicine Director, ASH Comprehensive Hypertension Center University of Chicago Medicine Chicago, IL USA
HYPERTENSION: ARE WE GOING TOO LOW? George L. Bakris, M.D.,F.A.S.N.,F.A.S.H., F.A.H.A. Professor of Medicine Director, ASH Comprehensive Hypertension Center University of Chicago Medicine Chicago, IL USA
Hypertension and the 2017 Guidelines Meeting the Targets in Small Groups. Lisa Ivy APRN
 Hypertension and the 2017 Guidelines Meeting the Targets in Small Groups Lisa Ivy APRN The 2017 Guideline is an Update to JNC7 New information regarding BP related risk of CVD Ambulatory BP monitoring
Hypertension and the 2017 Guidelines Meeting the Targets in Small Groups Lisa Ivy APRN The 2017 Guideline is an Update to JNC7 New information regarding BP related risk of CVD Ambulatory BP monitoring
Using the New Hypertension Guidelines
 Using the New Hypertension Guidelines Kamal Henderson, MD Department of Cardiology, Preventive Medicine, University of North Carolina School of Medicine Kotchen TA. Historical trends and milestones in
Using the New Hypertension Guidelines Kamal Henderson, MD Department of Cardiology, Preventive Medicine, University of North Carolina School of Medicine Kotchen TA. Historical trends and milestones in
Treating Hypertension in 2018: What Makes the Most Sense Today?
 Treating Hypertension in 2018: What Makes the Most Sense Today? Daniel Blanchard, MD Professor of Medicine UC San Diego Cardiovascular Center La Jolla, California 1 2 Speaker Disclosures Consultant and/or
Treating Hypertension in 2018: What Makes the Most Sense Today? Daniel Blanchard, MD Professor of Medicine UC San Diego Cardiovascular Center La Jolla, California 1 2 Speaker Disclosures Consultant and/or
HYPERTENSION: UPDATE 2018
 HYPERTENSION: UPDATE 2018 From the Cardiologist point of view Richard C Padgett, MD I have no disclosures HYPERTENSION ALWAYS THE ELEPHANT IN THE EXAM ROOM BUT SOMETIMES IT CHARGES HTN IN US ~78 million
HYPERTENSION: UPDATE 2018 From the Cardiologist point of view Richard C Padgett, MD I have no disclosures HYPERTENSION ALWAYS THE ELEPHANT IN THE EXAM ROOM BUT SOMETIMES IT CHARGES HTN IN US ~78 million
Managing Hypertension in 2018
 MANAGING HYPERTENSION IN 2018 How Do We Work With Conflicting Data and Conflicting Guidelines? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School
MANAGING HYPERTENSION IN 2018 How Do We Work With Conflicting Data and Conflicting Guidelines? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School
New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets
 New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of
New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of
2/11/2019 CLINICAL IMPLEMENTATION OF THE UPDATED BP GUIDELINES DUALITY OF INTEREST
 CLINICAL IMPLEMENTATION OF THE UPDATED BP GUIDELINES George L. Bakris, M.D.,F.A.S.N., F.A.H.A. Professor of Medicine Director, Am Heart Assoc. Comprehensive Hypertension Center University of Chicago Medicine
CLINICAL IMPLEMENTATION OF THE UPDATED BP GUIDELINES George L. Bakris, M.D.,F.A.S.N., F.A.H.A. Professor of Medicine Director, Am Heart Assoc. Comprehensive Hypertension Center University of Chicago Medicine
New Hypertension Guideline Recommendations for Adults July 7, :45-9:30am
 Advances in Cardiovascular Disease 30 th Annual Convention and Reunion UERM-CMAA, Inc. Annual Convention and Scientific Meeting July 5-8, 2018 New Hypertension Guideline Recommendations for Adults July
Advances in Cardiovascular Disease 30 th Annual Convention and Reunion UERM-CMAA, Inc. Annual Convention and Scientific Meeting July 5-8, 2018 New Hypertension Guideline Recommendations for Adults July
What s In the New Hypertension Guidelines?
 American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
Recent Hypertension Guidelines
 Recent Hypertension Guidelines Lawrence J. Fine, MD, DrPH, FAHA Division of Cardiovascular Sciences NHLBI/NIH February 19, 2014 Disclosures: Member of Panel Appointed to the Eighth Joint National Committee
Recent Hypertension Guidelines Lawrence J. Fine, MD, DrPH, FAHA Division of Cardiovascular Sciences NHLBI/NIH February 19, 2014 Disclosures: Member of Panel Appointed to the Eighth Joint National Committee
The New Hypertension Guidelines
 The New Hypertension Guidelines Joseph Saseen, PharmD Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Disclosure Joseph Saseen reports no conflicts
The New Hypertension Guidelines Joseph Saseen, PharmD Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Disclosure Joseph Saseen reports no conflicts
Potential U.S. Population Impact of the 2017 American College of Cardiology/ American Heart Association High Blood Pressure Guideline
 Accepted Manuscript Potential U.S. Population Impact of the 2017 American College of Cardiology/ American Heart Association High Blood Pressure Guideline Paul Muntner, PhD, Robert M. Carey, MD, Samuel
Accepted Manuscript Potential U.S. Population Impact of the 2017 American College of Cardiology/ American Heart Association High Blood Pressure Guideline Paul Muntner, PhD, Robert M. Carey, MD, Samuel
New Hypertension Guidelines: Why the change? Neil Brummond, M.D. Avera Medical Group Internal Medicine Sioux Falls, SD
 New Hypertension Guidelines: Why the change? Neil Brummond, M.D. Avera Medical Group Internal Medicine Sioux Falls, SD None Disclosures Objectives Understand trend in blood pressure clinical practice guidelines
New Hypertension Guidelines: Why the change? Neil Brummond, M.D. Avera Medical Group Internal Medicine Sioux Falls, SD None Disclosures Objectives Understand trend in blood pressure clinical practice guidelines
Hypertension Guidelines 2017
 Hypertension Guidelines 2017 (American College of Cardiology and the American Heart Association) In 1977, the 1st comprehensive guideline for detection, evaluation, and management of high BP was published,
Hypertension Guidelines 2017 (American College of Cardiology and the American Heart Association) In 1977, the 1st comprehensive guideline for detection, evaluation, and management of high BP was published,
Hypertension Guidelines: Lessons for Primary Care. Paul A James MD Professor and Chair Department of Family Medicine University of Washington
 Hypertension Guidelines: Lessons for Primary Care Paul A James MD Professor and Chair Department of Family Medicine University of Washington Disclaimer and Financial Disclosure I have no financial interests
Hypertension Guidelines: Lessons for Primary Care Paul A James MD Professor and Chair Department of Family Medicine University of Washington Disclaimer and Financial Disclosure I have no financial interests
Using Cardiovascular Risk to Guide Antihypertensive Treatment Implications For The Pre-elderly and Elderly
 Using Cardiovascular Risk to Guide Antihypertensive Treatment Implications For The Pre-elderly and Elderly Paul Muntner, PhD MHS Professor and Vice Chair Department of Epidemiology University of Alabama
Using Cardiovascular Risk to Guide Antihypertensive Treatment Implications For The Pre-elderly and Elderly Paul Muntner, PhD MHS Professor and Vice Chair Department of Epidemiology University of Alabama
Evolving Concepts on Hypertension: Implications of Three Guidelines (JNC 8 Panel, ESH/ESC, NICE/BSH)
") Evolving Concepts on Hypertension: Implications of Three Guidelines (JNC 8 Panel, ESH/ESC, NICE/BSH) Sidney C. Smith, Jr. MD, FACC, FAHA, FESC Professor of Medicine/Cardiology University of North Carolina
Evolving Concepts on Hypertension: Implications of Three Guidelines (JNC 8 Panel, ESH/ESC, NICE/BSH) Sidney C. Smith, Jr. MD, FACC, FAHA, FESC Professor of Medicine/Cardiology University of North Carolina
Blood Pressure LIMBO How Low To Go?
 Blood Pressure LIMBO How Low To Go? Joseph L. Kummer, MD, FACC Bryan Heart Spring Conference April 21 st, 2018 Hypertension Epidemiology Over a billion people have hypertension Major cause of morbidity
Blood Pressure LIMBO How Low To Go? Joseph L. Kummer, MD, FACC Bryan Heart Spring Conference April 21 st, 2018 Hypertension Epidemiology Over a billion people have hypertension Major cause of morbidity
DISCLOSURE PHARMACIST OBJECTIVES 9/30/2014 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES. I have nothing to disclose.
 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
T. Suithichaiyakul Cardiomed Chula
 T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
Hypertension. Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute
 Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
HTN talk_l Davis_ /28/2018
 1 2 GUIDELINES PUBLISHED AHEAD OF PRINT NOV 13, 2017 = SAME DAY AS PUBLIC PRESENTATION LESLIE L DAVIS, PHD, RN, ANP-BC, FPCNA, FAANP, FAHA The New Guidelines Have Been Published! Whelton PK, Carey RM,
1 2 GUIDELINES PUBLISHED AHEAD OF PRINT NOV 13, 2017 = SAME DAY AS PUBLIC PRESENTATION LESLIE L DAVIS, PHD, RN, ANP-BC, FPCNA, FAANP, FAHA The New Guidelines Have Been Published! Whelton PK, Carey RM,
Hypertension and the SPRINT Trial: Is Lower Better
 Hypertension and the SPRINT Trial: Is Lower Better 8th Annual Orange County Symposium on Cardiovascular Disease Prevention Saturday, October 8, 2016 Keith C. Norris, MD, PhD, FASN Professor of Medicine,
Hypertension and the SPRINT Trial: Is Lower Better 8th Annual Orange County Symposium on Cardiovascular Disease Prevention Saturday, October 8, 2016 Keith C. Norris, MD, PhD, FASN Professor of Medicine,
DISCLOSURES OUTLINE OUTLINE 9/29/2014 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE
 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
Pressure Drop: The Latest Guidelines on Treating Hypertension
 Pressure Drop: The Latest Guidelines on Treating Hypertension Eric J MacLaughlin, Pharm.D. Joseph J Saseen, Pharm.D. Target Audience: Pharmacists ACPE#: 0202-0000-18-050-L01-P Activity Type: Application-based
Pressure Drop: The Latest Guidelines on Treating Hypertension Eric J MacLaughlin, Pharm.D. Joseph J Saseen, Pharm.D. Target Audience: Pharmacists ACPE#: 0202-0000-18-050-L01-P Activity Type: Application-based
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
Retour sur le congrès de l AHA 2017
 Retour sur le congrès de l AHA 2017 Paul Poirier MD, PhD, FRCPC, FACC, FAHA, FCCS Professeur Faculté de pharmacie Université Laval Responsable du programme de prévention/réadaptation cardiaque Canagliflozin
Retour sur le congrès de l AHA 2017 Paul Poirier MD, PhD, FRCPC, FACC, FAHA, FCCS Professeur Faculté de pharmacie Université Laval Responsable du programme de prévention/réadaptation cardiaque Canagliflozin
Yuqing Zhang, M.D., FESC Department of Cardiology, Fu Wai Hospital. CAMS & PUMC, Beijing, China
 What Can We Learn from the Observational Studies and Clinical Trials of Prehypertension? Yuqing Zhang, M.D., FESC Department of Cardiology, Fu Wai Hospital. CAMS & PUMC, Beijing, China At ARIC visit 4
What Can We Learn from the Observational Studies and Clinical Trials of Prehypertension? Yuqing Zhang, M.D., FESC Department of Cardiology, Fu Wai Hospital. CAMS & PUMC, Beijing, China At ARIC visit 4
4/4/17 HYPERTENSION TARGETS: WHAT DO WE DO NOW? SET THE STAGE BP IN CLINICAL TRIALS?
 HYPERTENSION TARGETS: WHAT DO WE DO NOW? MICHAEL LEFEVRE, MD, MSPH PROFESSOR AND VICE CHAIR DEPARTMENT OF FAMILY AND COMMUNITY MEDICINE UNIVERSITY OF MISSOURI 4/4/17 DISCLOSURE: MEMBER OF THE JNC 8 PANEL
HYPERTENSION TARGETS: WHAT DO WE DO NOW? MICHAEL LEFEVRE, MD, MSPH PROFESSOR AND VICE CHAIR DEPARTMENT OF FAMILY AND COMMUNITY MEDICINE UNIVERSITY OF MISSOURI 4/4/17 DISCLOSURE: MEMBER OF THE JNC 8 PANEL
New Lipid Guidelines. PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids.
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
None. Disclosure: Relationships with Industry Conflicts of Interests. Learning Objectives: Participants will be able to:
 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults: Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC 8) James W. Shaw, MD Memorial Lecture
2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults: Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC 8) James W. Shaw, MD Memorial Lecture
Objectives. Describe results and implications of recent landmark hypertension trials
 Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
HYPERTENSION: WHAT'S YOUR GOAL?
 HYPERTENSION: WHAT'S YOUR GOAL? SATURDAY/3:15-4:15PM ACPE UAN: 0107-9999-17-243-L01-P 0.1 CEU/1.0 hr Activity Type: Application-Based Learning Objectives for Pharmacists: Upon completion of this CPE activity
HYPERTENSION: WHAT'S YOUR GOAL? SATURDAY/3:15-4:15PM ACPE UAN: 0107-9999-17-243-L01-P 0.1 CEU/1.0 hr Activity Type: Application-Based Learning Objectives for Pharmacists: Upon completion of this CPE activity
Unpacking Recent Hypertension Guidelines
 Unpacking Recent Hypertension Guidelines Lawrence J. Fine, MD, DrPH, FAHA Division of Cardiovascular Sciences NHLBI/NIH August 21, 2014 Disclosures: Member of Panel Appointed to the Eighth Joint National
Unpacking Recent Hypertension Guidelines Lawrence J. Fine, MD, DrPH, FAHA Division of Cardiovascular Sciences NHLBI/NIH August 21, 2014 Disclosures: Member of Panel Appointed to the Eighth Joint National
Pharmacy Updates in Primary Care. Nathan Lamberton Assistant Professor
 Pharmacy Updates in Primary Care January 31 st, 2018 Nathan Lamberton Assistant Professor David N. Ombengi Associate Professor First Metformin, Then? AR is a 57 year old African American male with a PMH
Pharmacy Updates in Primary Care January 31 st, 2018 Nathan Lamberton Assistant Professor David N. Ombengi Associate Professor First Metformin, Then? AR is a 57 year old African American male with a PMH
Hypertension Management Controversies in the Elderly Patient
 Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Disclosure. Instead of JNC 8. Proposed Reasons for Delays. Outline 6/10/2013. Member of JNC 8 panel No other disclosures. Daniel T.
 An Update on The Eighth Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 8): The Evidence-Based Process Disclosure Member of JNC 8
An Update on The Eighth Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 8): The Evidence-Based Process Disclosure Member of JNC 8
12.2. Structured, Team-Based Care Interventions for Hypertension Control
 Downloaded from http://hyper.ahajournals.org/ by guest on November 13, 2017 12.2. Structured, Team-Based Care Interventions for Hypertension Control Recommendation for Structured, Team-Based Care Interventions
Downloaded from http://hyper.ahajournals.org/ by guest on November 13, 2017 12.2. Structured, Team-Based Care Interventions for Hypertension Control Recommendation for Structured, Team-Based Care Interventions
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014
 HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
JNC 8 -Controversies. Sagren Naidoo Nephrologist CMJAH
 JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
2017 High Blood Pressure Clinical Practice Guideline
 2017 High Blood Pressure Clinical Practice Guideline Applying the Latest Hypertension Guideline to Your Practice Carmine D Amico, D.O., F.A.C.C. 2017 ACC / AHA / AAPA / ABC / ACPM / AGS / APhA / ASH /
2017 High Blood Pressure Clinical Practice Guideline Applying the Latest Hypertension Guideline to Your Practice Carmine D Amico, D.O., F.A.C.C. 2017 ACC / AHA / AAPA / ABC / ACPM / AGS / APhA / ASH /
2/10/2014. Hypertension: Highlights of Hypertension Guidelines: Making the Most of Limited Evidence. Issues with contemporary guidelines
 Hypertension: 214 Highlights of Hypertension Guidelines: Making the Most of Limited Evidence Michael A, Weber, MD Editor-in-Chief, The Journal of Clinical Hypertension, Professor of Medicine, Division
Hypertension: 214 Highlights of Hypertension Guidelines: Making the Most of Limited Evidence Michael A, Weber, MD Editor-in-Chief, The Journal of Clinical Hypertension, Professor of Medicine, Division
CONTRIBUTING FACTORS FOR STROKE:
 CONTRIBUTING FACTORS FOR STROKE: HYPERTENSION AND HYPERCHOLESTEROLEMIA Melissa R. Stephens, MD, FAAFP Associate Professor of Clinical Sciences William Carey University College of Osteopathic Medicine LEARNING
CONTRIBUTING FACTORS FOR STROKE: HYPERTENSION AND HYPERCHOLESTEROLEMIA Melissa R. Stephens, MD, FAAFP Associate Professor of Clinical Sciences William Carey University College of Osteopathic Medicine LEARNING
Status Report on the NHLBI-Sponsored CVD Prevention Guidelines
 Status Report on the NHLBI-Sponsored CVD Prevention Guidelines HIGH BLOOD PRESSURE Paul A. James, M.D. Roy J. and Lucille A. Carver College of Medicine The University of Iowa Iowa City IA NHLBI Adult CVD
Status Report on the NHLBI-Sponsored CVD Prevention Guidelines HIGH BLOOD PRESSURE Paul A. James, M.D. Roy J. and Lucille A. Carver College of Medicine The University of Iowa Iowa City IA NHLBI Adult CVD
Hypertension: 2016 Clinical Update
 PHASE Safety Net Community Benefit Hypertension: 2016 Clinical Update Presented by: Joseph Young, MD Hypertension Clinical Lead Kaiser Permanente Northern California October 6, 2016 Dr. Joseph Young Hypertension
PHASE Safety Net Community Benefit Hypertension: 2016 Clinical Update Presented by: Joseph Young, MD Hypertension Clinical Lead Kaiser Permanente Northern California October 6, 2016 Dr. Joseph Young Hypertension
The Latest Generation of Clinical
 The Latest Generation of Clinical Guidelines: HTN and HLD Dave Brackett Clinical Guideline Purpose Uniform approach Awareness of key details Diagnosis Treatment Monitoring Evidence based approach Inform
The Latest Generation of Clinical Guidelines: HTN and HLD Dave Brackett Clinical Guideline Purpose Uniform approach Awareness of key details Diagnosis Treatment Monitoring Evidence based approach Inform
What s the evidence, why do guidelines differ, and what should the GP do?
 What s the evidence, why do guidelines differ, and what should the GP do? Richard McManus Barcelona 2018 Overview What is hypertension? How should blood pressure be measured/diagnosed? What should we be
What s the evidence, why do guidelines differ, and what should the GP do? Richard McManus Barcelona 2018 Overview What is hypertension? How should blood pressure be measured/diagnosed? What should we be
10/21/2014. Disclosures. Introduction. Reasons for the Decline in Stroke Mortality: Implications for Hypertension and Risk Factor Management
 Reasons for the Decline in Stroke Mortality: Implications for Hypertension and Risk Factor Management Daniel T Lackland Disclosures Member of NHLBI Risk Assessment Workgroup Member of 2014 Hypertension
Reasons for the Decline in Stroke Mortality: Implications for Hypertension and Risk Factor Management Daniel T Lackland Disclosures Member of NHLBI Risk Assessment Workgroup Member of 2014 Hypertension
2/9/2017. Financial Disclosures/Unapproved Use. Achieving Harmony in Blood Pressure Guidelines Around the Globe. Roger S. Blumenthal, MD.
 Achieving Harmony in Blood Pressure Guidelines Around the Globe Roger S. Blumenthal, MD The Kenneth Jay Pollin Professor of Cardiology Director, The Johns Hopkins Ciccarone Center for the Prevention Of
Achieving Harmony in Blood Pressure Guidelines Around the Globe Roger S. Blumenthal, MD The Kenneth Jay Pollin Professor of Cardiology Director, The Johns Hopkins Ciccarone Center for the Prevention Of
Blood Pressure Targets: Where are We Now?
 Blood Pressure Targets: Where are We Now? Diana Cao, PharmD, BCPS-AQ Cardiology Assistant Professor Department of Clinical & Administrative Sciences California Northstate University College of Pharmacy
Blood Pressure Targets: Where are We Now? Diana Cao, PharmD, BCPS-AQ Cardiology Assistant Professor Department of Clinical & Administrative Sciences California Northstate University College of Pharmacy
Management of Lipid Disorders and Hypertension: Implications of the New Guidelines
 Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
Hypertension Update 2014:
 GSHTP Webinar Hypertension Update 2014: The Kaiser Permanente Northern California Experience Presented by: Marc Jaffe, MD Associate Clinical Professor of Medicine, UCSF Kaiser Permanente Northern California
GSHTP Webinar Hypertension Update 2014: The Kaiser Permanente Northern California Experience Presented by: Marc Jaffe, MD Associate Clinical Professor of Medicine, UCSF Kaiser Permanente Northern California
2013 ACC/AHA Guidelines on the Assessment of Atherosclerotic Cardiovascular Risk: Overview and Commentary
 2013 ACC/AHA Guidelines on the Assessment of Atherosclerotic Cardiovascular Risk: Overview and Commentary The Johns Hopkins Ciccarone Center for the Prevention of Heart Disease Becky McKibben, MPH; Seth
2013 ACC/AHA Guidelines on the Assessment of Atherosclerotic Cardiovascular Risk: Overview and Commentary The Johns Hopkins Ciccarone Center for the Prevention of Heart Disease Becky McKibben, MPH; Seth
2. Measurement Specifications 3. Patient Messaging 4. Provider Messaging Other Recent Guidelines
 Measure Up/Pressure Down Response to the Release of 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults: Report from the Panel Members Appointed to the Eighth Joint National
Measure Up/Pressure Down Response to the Release of 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults: Report from the Panel Members Appointed to the Eighth Joint National
Atherosclerotic Disease Risk Score
 Atherosclerotic Disease Risk Score Kavita Sharma, MD, FACC Diplomate, American Board of Clinical Lipidology Director of Prevention, Cardiac Rehabilitation and the Lipid Management Clinics September 16,
Atherosclerotic Disease Risk Score Kavita Sharma, MD, FACC Diplomate, American Board of Clinical Lipidology Director of Prevention, Cardiac Rehabilitation and the Lipid Management Clinics September 16,
Prevention of Heart Failure: What s New with Hypertension
 Prevention of Heart Failure: What s New with Hypertension Ali AlMasood Prince Sultan Cardiac Center Riyadh 3ed Saudi Heart Failure conference, Jeddah, 13 December 2014 Background 20-30% of Saudi adults
Prevention of Heart Failure: What s New with Hypertension Ali AlMasood Prince Sultan Cardiac Center Riyadh 3ed Saudi Heart Failure conference, Jeddah, 13 December 2014 Background 20-30% of Saudi adults
Antihypertensive Trial Design ALLHAT
 1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
Blood Pressure Treatment Goals
 Blood Pressure Treatment Goals Kenneth Izuora, MD, MBA, FACE Associate Professor UNLV School of Medicine November 18, 2017 Learning Objectives Discuss the recent studies on treating hypertension Review
Blood Pressure Treatment Goals Kenneth Izuora, MD, MBA, FACE Associate Professor UNLV School of Medicine November 18, 2017 Learning Objectives Discuss the recent studies on treating hypertension Review
MPharmProgramme. Hypertension (HTN)
") MPharmProgramme Hypertension (HTN) Slide 1 of 30 Overview Definition Prevalence Type Causes Diagnosis Management Patients perspective Slide 2 of 30 Definition It is not a disease! So what is it? What two
MPharmProgramme Hypertension (HTN) Slide 1 of 30 Overview Definition Prevalence Type Causes Diagnosis Management Patients perspective Slide 2 of 30 Definition It is not a disease! So what is it? What two
Hypertension targets: sorting out the confusion. Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town
 Hypertension targets: sorting out the confusion Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town Historical Perspective The most famous casualty of this approach was the
Hypertension targets: sorting out the confusion Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town Historical Perspective The most famous casualty of this approach was the
Prevention of Heart Disease: The New Guidelines
 Prevention of Heart Disease: The New Guidelines Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California San Francisco May 18 th 2015
Prevention of Heart Disease: The New Guidelines Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California San Francisco May 18 th 2015
Diabetes Mellitus: A Cardiovascular Disease
 Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Managing HTN in the Elderly: How Low to Go
 Managing HTN in the Elderly: How Low to Go Laxmi S. Mehta, MD, FACC The Ohio State University Medical Center Assistant Professor of Clinical Internal Medicine Clinical Director of the Women s Cardiovascular
Managing HTN in the Elderly: How Low to Go Laxmi S. Mehta, MD, FACC The Ohio State University Medical Center Assistant Professor of Clinical Internal Medicine Clinical Director of the Women s Cardiovascular
24-uur ambulante bloeddrukmeting versus thuisbloedrukmeting
 2017 Dementia 24-uur ambulante bloeddrukmeting versus thuisbloedrukmeting Wat gebruiken in de klinische praktijk? Jan A. Staessen, MD, PhD KU Leuven jan.staessen@kuleuven.be BPM Key messages to be made
2017 Dementia 24-uur ambulante bloeddrukmeting versus thuisbloedrukmeting Wat gebruiken in de klinische praktijk? Jan A. Staessen, MD, PhD KU Leuven jan.staessen@kuleuven.be BPM Key messages to be made
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD
 2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
Int. J. Pharm. Sci. Rev. Res., 36(1), January February 2016; Article No. 06, Pages: JNC 8 versus JNC 7 Understanding the Evidences
, January February 2016; Article No. 06, Pages: JNC 8 versus JNC 7 Understanding the Evidences") Research Article JNC 8 versus JNC 7 Understanding the Evidences Anns Clara Joseph, Karthik MS, Sivasakthi R, Venkatanarayanan R, Sam Johnson Udaya Chander J* RVS College of Pharmaceutical Sciences, Coimbatore,
Research Article JNC 8 versus JNC 7 Understanding the Evidences Anns Clara Joseph, Karthik MS, Sivasakthi R, Venkatanarayanan R, Sam Johnson Udaya Chander J* RVS College of Pharmaceutical Sciences, Coimbatore,
When should blood pressure be lowered? Should treatment be guided by blood pressure values or total cardiovascular risk?
 OF JOURNAL HYPERTENSION JH R RESEARCH Journal of HYPERTENSION RESEARCH www.hypertens.org/jhr Editorial J Hypertens Res (2016) 2(2):47 51 When should blood pressure be lowered? Should treatment be guided
OF JOURNAL HYPERTENSION JH R RESEARCH Journal of HYPERTENSION RESEARCH www.hypertens.org/jhr Editorial J Hypertens Res (2016) 2(2):47 51 When should blood pressure be lowered? Should treatment be guided
Placebo-Controlled Statin Trials EXPLAINING THE DECREASE IN DEATHS FROM CHD! PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN EXPLAINING THE DECREASE IN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline?
 What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline? Salim S. Virani, MD, PhD, FACC, FAHA Associate Professor, Section of Cardiovascular Research Baylor
What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline? Salim S. Virani, MD, PhD, FACC, FAHA Associate Professor, Section of Cardiovascular Research Baylor
Hypertension: JNC-7. Southern California University of Health Sciences Physician Assistant Program
 Hypertension: JNC-7 Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! Reference Card
Hypertension: JNC-7 Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! Reference Card
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, Financial Disclosures
 Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
Observations on US CVD Prevention Guidelines. Donald M. Lloyd-Jones, MD ScM FACC FAHA
 Observations on US CVD Prevention Guidelines Donald M. Lloyd-Jones, MD ScM FACC FAHA What are Guidelines? Evidence Base for Guidelines Tricoci, JAMA 2009 Evidence Base for Guidelines Tricoci, JAMA 2009
Observations on US CVD Prevention Guidelines Donald M. Lloyd-Jones, MD ScM FACC FAHA What are Guidelines? Evidence Base for Guidelines Tricoci, JAMA 2009 Evidence Base for Guidelines Tricoci, JAMA 2009
Hypertension and Cardiovascular Disease
 Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
Hypertension and Diabetes Should we be SPRINTING or Reaching an ACCORD?
 Hypertension and Diabetes Should we be SPRINTING or Reaching an ACCORD? Suzanne Oparil, MD Distinguished Professor of Medicine, Professor of Cell, Developmental and Integrative Biology Director, Vascular
Hypertension and Diabetes Should we be SPRINTING or Reaching an ACCORD? Suzanne Oparil, MD Distinguished Professor of Medicine, Professor of Cell, Developmental and Integrative Biology Director, Vascular
Disclosures. Prevention of Heart Disease: The New Guidelines. Summary of Talk. Four guidelines. No relevant disclosures.
 Disclosures Prevention of Heart Disease: The New Guidelines No relevant disclosures Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California
Disclosures Prevention of Heart Disease: The New Guidelines No relevant disclosures Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California
Blood Pressure Treatment in 2018
 Blood Pressure Treatment in 2018 Jay D. Geoghagan, MD, FACC Disclosures: None 1 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/ APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management
Blood Pressure Treatment in 2018 Jay D. Geoghagan, MD, FACC Disclosures: None 1 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/ APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management
The earlier BP control the better cardiovascular outcome. Jin Oh Na Cardiovascular center Korea University Medical College
 The earlier BP control the better cardiovascular outcome Jin Oh Na Cardiovascular center Korea University Medical College Index Introduction HOPE-3 Trial Sprint Study Summary Each 2 mmhg decrease in SBP
The earlier BP control the better cardiovascular outcome Jin Oh Na Cardiovascular center Korea University Medical College Index Introduction HOPE-3 Trial Sprint Study Summary Each 2 mmhg decrease in SBP
Disclosure of Relationships past 12 months
 HYPERTENSION IN WOMEN: WHAT ARE THE IMPLICATIONS OF THE NEW HYPERTENSION GUIDELINES? ANGELA L. BROWN, MD Associate Professor of Medicine // Cardiovascular Division Washington University School of Medicine
HYPERTENSION IN WOMEN: WHAT ARE THE IMPLICATIONS OF THE NEW HYPERTENSION GUIDELINES? ANGELA L. BROWN, MD Associate Professor of Medicine // Cardiovascular Division Washington University School of Medicine
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Lipid Management 2013 Statin Benefit Groups
 Clinical Integration Steering Committee Clinical Integration Chronic Disease Management Work Group Lipid Management 2013 Statin Benefit Groups Approved by Board Chair Signature Name (Please Print) Date
Clinical Integration Steering Committee Clinical Integration Chronic Disease Management Work Group Lipid Management 2013 Statin Benefit Groups Approved by Board Chair Signature Name (Please Print) Date
Preventing and Treating High Blood Pressure
 Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Modern Management of Hypertension
 Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
Managing Hypertension in 2016
 Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
Lipid Panel Management Refresher Course for the Family Physician
 Lipid Panel Management Refresher Course for the Family Physician Objectives Understand the evidence that was evaluated to develop the 2013 ACC/AHA guidelines Discuss the utility and accuracy of the new
Lipid Panel Management Refresher Course for the Family Physician Objectives Understand the evidence that was evaluated to develop the 2013 ACC/AHA guidelines Discuss the utility and accuracy of the new
Branko N Huisa M.D. Assistant Professor of Neurology UNM Stroke Center
 Branko N Huisa M.D. Assistant Professor of Neurology UNM Stroke Center THE END! CHANGABLE Blood pressure Diabetes Mellitus Hyperlipidemia Atrial fibrillation Nicotine Drug abuse Life style NOT CHANGABLE
Branko N Huisa M.D. Assistant Professor of Neurology UNM Stroke Center THE END! CHANGABLE Blood pressure Diabetes Mellitus Hyperlipidemia Atrial fibrillation Nicotine Drug abuse Life style NOT CHANGABLE
2017 ACC/AHA/AAPA/ABC/ACPM/AGS/
 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/ APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults American College of Cardiology Foundation and
2017 ACC/AHA/AAPA/ABC/ACPM/AGS/ APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults American College of Cardiology Foundation and
Jared Moore, MD, FACP
 Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
4/7/ The stats on heart disease. + Deaths & Age-Adjusted Death Rates for
 + Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
+ Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
Potential U.S. Population Impact of the 2017 American College of. Cardiology/American Heart Association High Blood Pressure Guideline
 Potential U.S. Population Impact of the 2017 American College of Cardiology/American Heart Association High Blood Pressure Guideline Running Title: Muntner et al.; Impact of the 2017 ACC/AHA Guideline
Potential U.S. Population Impact of the 2017 American College of Cardiology/American Heart Association High Blood Pressure Guideline Running Title: Muntner et al.; Impact of the 2017 ACC/AHA Guideline
Systolic Blood Pressure Intervention Trial (SPRINT)
") 09:30-09:50 2016.4.15 Systolic Blood Pressure Intervention Trial (SPRINT) IN A NEPHROLOGIST S VIEW Sejoong Kim Seoul National University Bundang Hospital Current guidelines for BP control Lowering BP
09:30-09:50 2016.4.15 Systolic Blood Pressure Intervention Trial (SPRINT) IN A NEPHROLOGIST S VIEW Sejoong Kim Seoul National University Bundang Hospital Current guidelines for BP control Lowering BP
Placebo-Controlled Statin Trials MANAGEMENT OF HIGH BLOOD CHOLESTEROL MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HYPERTENSION: TREATMENT THRESHOLDS AND MEDICATION SELECTION
 Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Update in Cardiology Pharmacologic Management of Cardiovascular Risk. Christopher C. Roe, MSN, ACNP
 Update in Cardiology Pharmacologic Management of Cardiovascular Risk Christopher C. Roe, MSN, ACNP Objectives 1. Verbalize understanding of new pharmacologic guidelines in the treatment of hypertension
Update in Cardiology Pharmacologic Management of Cardiovascular Risk Christopher C. Roe, MSN, ACNP Objectives 1. Verbalize understanding of new pharmacologic guidelines in the treatment of hypertension
Placebo-Controlled Statin Trials Prevention Of CVD in Women"
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
Update in Hypertension
 Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
The Clinical Unmet need in the patient with Diabetes and ACS
 The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge