Hypertension: 2016 Clinical Update
|
|
|
- Dorcas Hoover
- 5 years ago
- Views:
Transcription

1 PHASE Safety Net Community Benefit Hypertension: 2016 Clinical Update Presented by: Joseph Young, MD Hypertension Clinical Lead Kaiser Permanente Northern California October 6, 2016

2 Dr. Joseph Young Hypertension Clinical Lead, Kaiser Permanente Northern California 2 October 6, 2016 The Permanente Medical Group, Inc. Oakland, CA
3 Speaker s Financial Disclosure I have no financial relationship with any medically related enterprise other than Kaiser Permanente I am not an investigator for a pharmaceutical sponsored trial I am not on a pharmacy sponsored speakers bureau 3 October 6, 2016 The Permanente Medical Group, Inc. Oakland, CA

4 Kaiser Permanente Northern California Northern California (KPNC) More than 3.7 million members Comprehensive inpatient & outpatient services 21 hospitals and 45 medical facilities More than 8,000 Physicians facilities 4 October 6, 2016 The Permanente Medical Group, Inc. Oakland, CA
5 Population With Hypertension (%) Hypertension Affects Approximately 70 Million Americans: 29% of Adults Men Women 10 0 Non-Hispanic White Non-Hispanic Black Mexican American Egan B, et al. NHANES JAMA 2010; 303:

6 Prevalence of High BP in Americans Aged 20 Years and Older by Age and Gender (NHANES IV: )

7 JAMA. 2013;310(7): Select the subtitle text box above, copy, and paste it on to the slide that requires a subtitle Horizontal position setting for subtitle is 0.5" Vertical position setting for subtitle is 1.35" Keep subtitle to one line of text Follow these subtitle placement guidelines to ensure consistent positioning throughout the presentation 7 October 6, 2016 The Permanente Medical Group, Inc. Oakland, CA


8 Leading the Nation in HTN Control Controlling High Blood Pressure HEDIS Trend National Benchmarks 90 th %ile 50 th %ile Commercial Medicare The Permanente Medical Group, Inc. Supported by Quality and Operations Support, Emily Steemers ( ) 8
9 Falling CV Morbidity and Mortality - KPNC Since Year 2000: 30% reduction in mortality from CVD 42% reduction in mortality from stroke 11% reduction in mortality from cancer Sidney S, Jaffe M, Nguyen-Hyunha M, Kushi L, Young J, Sorel M, Selby J, Go A. Closing the Gap Between Cardiovascular and Cancer Mortality in an Integrated Health Care Delivery System, : The Kaiser Permanente Experience. Circulation 2011; 124: A13610 The Permanente Medical Group, Inc. Supported by Quality and Operations Support, Emily Steemers ( ) 9
10 It s All About Implementation It has to work in the real world 10 October 6, 2016 The Permanente Medical Group, Inc. Oakland, CA
11 Key Elements of a Comprehensive Hypertension Control Program Hypertension Registry, Comprehensive Performance Metrics, Transparent and Widely Visible Clinic-level feedback to facilitate operational and system-level change. Treatment Algorithm Evidence-Based Simple, Implementable Single Pill Combination (SPC) pharmacotherapy Medical-Assistant BP Checks Better leverage ancillary staff skills Reduced barriers to patients 11 October 6, 2016 The Permanente Medical Group, Inc. Oakland, CA

12 Speaker s Financial Disclosure I have no financial relationship with any medically related enterprise other than Kaiser Permanente I am not an investigator for a pharmaceutical sponsored trial I am not on a pharmacy sponsored speakers bureau 12 October 6, 2016 The Permanente Medical Group, Inc. Oakland, CA
13 KP HTN Treatment Algorithm 3 Meds to Max Dose in 6 Steps 13 October 6, 2016 The Permanente Medical Group, Inc. Oakland, CA


14 30% of ACEI Rx s dispensed as Fixed Dose Combination Therapy % Of All ACEI Rxs 100% 80% 60% 40% 20% 0% ACEI Only Tablet ACEI + HCTZ Tablet Marc Jaffe, MD The Permanente Medical Group, Inc. Oakland, CA
15 Why Treating HTN Matters? It Saves Lives! Stage 1 HTN + 1 or more CV risk factors and 12 mm drop in SBP for 10 years Prevents 1 death for every 11 pts Ogden LG, et al, Hypertension, 2000;35: The Permanente Medical Group, Inc. Supported by Quality and Operations Support, Emily Steemers ( ) 15
16 Lifestyle Modifications Modification Weight Reduction Adopt DASH eating plan Dietary sodium reduction Physical activity Moderation of alcohol consumption Approximate SBP Reduction (range) 5-10 mmhg/10kg 8-14 mmhg 2-8 mmhg 4-9 mmhg 2 4 mmhg
17 27 ALLHAT Cumulative CHD Event Rate Cumulative Event Rates for the Primary Outcome (Fatal CHD or Nonfatal MI) by ALLHAT Treatment Group A/C L/C RR (95% CI) 0.98 ( ) 0.99 ( ) Chlorthalidone Amlodipine Lisinopril p value Years to CHD Event Number at Risk: Chlorthalidone 15,255 14,477 13,820 13,102 11,362 6,340 2, Amlodipine 9,048 8,576 8,218 7,843 6,824 3,870 1, Lisinopril 9,054 8,535 8,123 7,711 6,662 3,832 1,
18 35 ALLHAT Cumulative Event Rates for Heart Failure by ALLHAT Treatment Group.15 A/C HR (95% CI) 1.38 ( ) p value <.001 L/C 1.19 ( ) <.001 Cumulative CHF Rate Chlorthalidone Amlodipine Lisinopril Years to HF Number at risk: Chlor 15,255 14,528 13,898 13,224 11,511 6,369 3, Amlo 9,048 8,535 8,185 7,801 6,785 3,775 1, Lisin 9,054 8,496 8,096 7,689 6,698 3,789 1,
19 AND Remember: Safety First! ACE / ARB s & Statins May be Teratogenic Avoid ACE-Is, ARBs and Statins in women of child-bearing age unless she is using a highly reliable method of contraception. Cooper, et. Al., NEJM 354;23, June 8, 2006 The Permanente Medical Group, Inc. Supported by Quality and Operations Support, Emily Steemers ( ) 19
20 Why is Spironolactone Now Best 4 th Agent? PATHWAYS-2 RCT: Spironolactone vs Placebo, Doxazosin and Bisoprolol for control of resistant HTN* *Uncontrolled on ACE/ARB + diuretic + CCB. 58% of pts controlled on Spironolactone! Williams B, MacDonald TM, et al., Published online September 21, The Permanente Medical Group, Inc. Supported by Quality and Operations Support, Emily Steemers ( ) 20

21 PATHWAYS-2: Spironolactone is the Best! P S D B The Permanente Medical Group, Inc. Supported by Quality and Operations Support, Emily Steemers ( ) 21
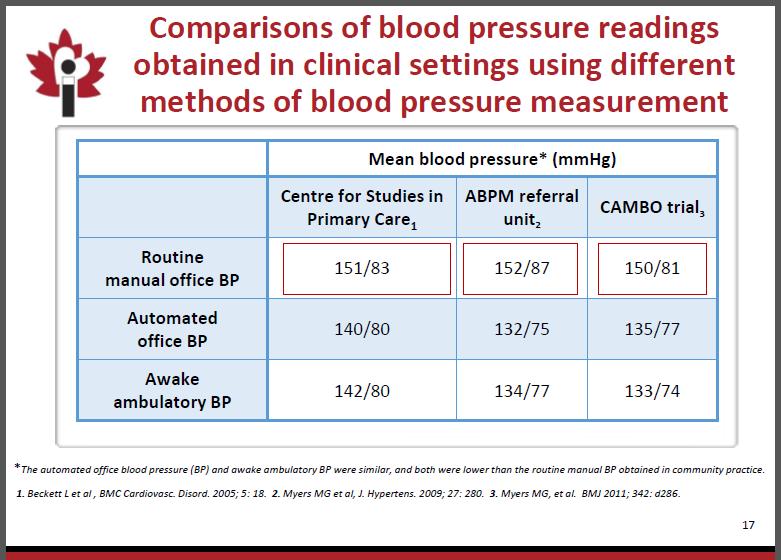
22 AOBPM Technique Oscillometric device Average of three readings: Following 5 minutes of rest Three readings at 1 minute intervals Patient unobserved: Clinic staff prepares patient, pushes button and then leaves patient unattended. Readings and calculated average displayed on device.
23
24 BP Measurement in SPRINT vs. Other Trials Unattended Blood Pressure Measurements in the Systolic, Blood Pressure Intervention Trial Implications for Entry and Achieved Blood Pressure Values Compared With Other Trials BPs taken in SPRINT cannot be directly compared with BPs in other trials and (2) the treatment arm <120 mm Hg in SPRINT compares with a higher SBP value in the other trials. For generalization, the number of mm Hg that should be added must be clarified; suggestions vary from 5 to 10 mm Hg up to mm Hg and a recent study indicates 16 mm Hg. Overall, it means that the lower treatment arm in SPRINT translates into SBP <136 mm Hg, not very different from SBP <140 mm Hg, which is the currently recommended SBP target for most hypertensive people by all hypertension treatment guidelines. Kjeldsen SE et al, Hypertension. 2016; May67(5):
25 BP measurements taken without observing these conditions are likely to overestimate BP and result in overtreatment, with the potential for higher rates of serious adverse effects and greater utilization of resources. This issue should be carefully considered in the development of any practice-based performance measures for BP control in hypertension that are derived from the SPRINT results. Cushman WC, Whelton PK, Fine LJ, Wright JT Jr, Reboussin DM, Johnson KC, Oparil S; SPRINT Study Research Group. SPRINT Trial Results: Latest News in Hypertension Management. Hypertension.2016;67:
 Ambrosius WT et al. Clin. Trials.")
26 SPRINT Research Question Examine effect of more intensive high blood pressure treatment than is currently recommended Randomized Controlled Trial Target Systolic BP Intensive Treatment Goal SBP < 120 mm Hg Standard Treatment Goal SBP < 140 mm Hg SPRINT design details available at: ClinicalTrials.gov (NCT ) Ambrosius WT et al. Clin. Trials. 2014;11:
27 SPRINT Enrollment Criteria INCLUSION CRITERIA > 50 years old SBP 130 to 180 mm Hg SBP < 150 if on 4 meds at enrollment One or more of the following CVD (clinical or subclinical) 20 < egfr < year Framingham Risk > 15% Age > 75 years EXCLUSION CRITERIA Prior Stroke Diabetes Mellitus Standing SBP < 110 mm Hg Polycystic Kidney Disease CHF, symptomatic or with ef < 35% Proteinuria > 1 g / day egfr < 20 Adherence Concerns
28 Primary and Secondary Outcomes Primary Outcomes CVD Composite, 1 st occurrence of: MI ACS (non-mi ACS) Stroke HF, - acute, decompensated CV death Secondary Outcomes All cause mortality Primary Outcomes + All-cause mortality > 50% decline in egfr in patients with CKD > 30% decline in egfr in patients WITHOUT CKD Incident albuminuria
29 Target vs. Achieved BP For any target BP, there will be a distribution of achieved BPs SPRINT is a landmark, federally funded, well designed RCT, analyzed according to pre-specified target BPs Beware of post-hoc analyses based on achieved BPs as these are subject to selection bias, e.g. patients with DM in HOT trial
30 Mean Achieved BPs in SPRINT Intensive Treatment Arm mm Hg Standard Treatment Arm mm Hg BPs as measured (very well) in SPRINT via AOBPM, correlate to higher conventional office readings of 5 mm Hg or more* SPRINT Intensive arm, mean achieved BP corresponds to conventional readings of mid 120s mm Hg or higher *Myers MG et al. Measurement of blood pressure in the office: recognizing the problem and proposing the solution. Hypertension. 2010;55: *Filipovský J et al. Automated compared to manual office blood pressure and to home blood pressure in hypertensive patients. Blood Press Aug;25(4):
31 Systolic BP During Follow-up Year 1 Mean SBP mm Hg Mean SBP mm Hg Standard Intensive Average SBP (During Followup) Standard: mm Hg Intensive: mm Hg Average number of antihypertensive medications Number of participants
32 25% reduction in 1 Outcomes (p < 0.001) The Permanente Medical Group, Inc. Supported by Quality and Operations Support, Emily Steemers ( ) 32
33 Hypotension Consequences in SPRINT are nuanced Statistically Significant Syncope Orthostatic Hypotension LESS frequent in Intensive Treatment Arm. NO Difference Injurious Falls* Dizziness Patient perceived health status VR12 with physical and mental health sub-scores PHQ-9 *Defined as not resulting from Syncope
34 Number Needed to Treat/Harm Relative vs. Absolute Risk Reduction 25% Reduction in Composite Primary Outcome % vs. 5.2% = 1.6% difference NNT Primary Outcome 61; All-cause mortality 90* NNH 45 (2.2%)** On the basis of the SPRINT results, we estimate that for 1000 persons treated over 3.2 years to a systolic BP goal less than 120 mm Hg compared with less than 140 mm Hg, an average of 16 persons will benefit, 22 persons will be seriously harmed, and 962 will not experience benefits or harms * Benefit is typically cited as relative risk reduction (big #) Adverse events are typically cited as absolute risk (small #) * SPRINT Research Group et al. N Engl J Med Nov 26;373(22): ** Ortiz E, James PA. Ann Intern Med May 17;164(10:692-3.
35 Can SPRINT findings be generalized to patients with DM? ACCORD Trial: Also target < 120 mm Hg SBP vs. < 140 mm Hg SBP Primary Composite CV Outcome MI, Stroke, CV Death with trend to benefit in Intensive Arm but not statistically significant Underpowered half the size of SPRINT Effect of antihypertensive treatment at different blood pressure levels in patients with DM: systematic review and meta-analysis. (BMJ 2016:352:1717) If baseline SBP was less than 140 mm Hg, however, further treatment increased the risk of cardiovascular mortality (1.15, 1.00 to 1.32), with a tendency towards an increased risk of all cause mortality (1.05, 0.95 to 1.16).
36 Can SPRINT findings be generalized to patients with h/o Stroke? Secondary Prevention of Small Subcortical Strokes (SPS3) Trial Patients randomized to target SBP < 130 vs. 130 to patients randomized. Mean follow up 3.7 years Primary Endpoint: Reduction in all strokes
37 Recommendations For patients that meet SPRINT enrollment criteria, i.e. age > 75 years, age years with CVD, < 20 egfr < 60 or 10-year Framingham risk of > 15% Pending formal evidence review, shared decision making model of care for target SBP of <130 mm Hg* is appropriate When lower target SPB is used, close monitoring for syncope and renal function is warranted Trial and observational data does not support expansion of SPRINT goals to patients with DM and / or history of stroke * Conventional office SBP < 130 mm Hg is roughly equivalent to AOBPM reading of < 120 mm Hg
38 KP HTN Treatment Algorithm 3 Meds to Max Dose in 6 Steps 38 October 6, 2016 The Permanente Medical Group, Inc. Oakland, CA
39 CASES! The Permanente Medical Group, Inc. Supported by Quality and Operations Support, Emily Steemers ( ) 39
40 Case 1 Non-adherence? 55 year old man, 156/76, HR 84 Lisinopril-HCTZ mg qd Amlodipine 10 mg BP 132/70 on same regimen one year ago Sometimes it s hard to remember to take your medicines. I know I sometimes forget to take a dose of my medicines. Explore possible reasons for non-adherence Forgets would a pillbox help? Side effects? Affordability? The Permanente Medical Group, Inc. Supported by Quality and Operations Support, Emily Steemers ( ) 40
41 Case 2 Don t Under-dose the Thiazide 55 year old man, 142/76, HR 66 Lisinopril-HCTZ mg Amlodipine 10 mg Recommendation Increase lisinopril-hctz to ii qd Remember not to under-dose the thiazide The Permanente Medical Group, Inc. Supported by Quality and Operations Support, Emily Steemers ( ) 41
42 Case 3 Use ARB for ACE-I Cough Intolerance 53 year old woman, 144/64, heart rate 58 Chlorthalidone 25 mg Cough on lisinopril Recommendation: Add losartan 25 mg The Permanente Medical Group, Inc. Supported by Quality and Operations Support, Emily Steemers ( ) 42
43 Case 4 Woman of Child Bearing Potential 38 y/o women. 140/94. Sexually active, uses condoms Chlorthalidone 25 mg daily Recommendation: add amlodipine 2.5 mg qd ACE-Is and ARBs are potentially teratogenic The Permanente Medical Group, Inc. Supported by Quality and Operations Support, Emily Steemers ( ) 43
44 Case 5 Resistant HTN 55 year old man, BP 156/80, HR 78 Lisinopril-HCTZ ii qd Amlodipine 10 i qd K = 4.2, egfr > 60 Recommendation: Add spironolactone 12.5 mg qd Advance to 25 mg qd if needed The Permanente Medical Group, Inc. Supported by Quality and Operations Support, Emily Steemers ( ) 44
45 Case 6 Elderly patient with DM uncontrolled? 72 year old man with DM. 148/64, HR 78 Chlorthalidone 25 mg qd Lisinopril 20 mg qd Amlodipine 5 mg qd Recommendation Stand for two minutes and repeat BP If SBP > 140, increase amlodipine to 10 mg qd The Permanente Medical Group, Inc. Supported by Quality and Operations Support, Emily Steemers ( ) 45


46 Questions?
47 Next Up Don t forget to join us for our next wireside chat! October 26 th at 12pm PT Diabetes 2016: Strategies for Achieving Optimal A1c Control Presented by Dr. Lisa Gilliam from Kaiser Permanente To register, go to:
PHASE Preventing Heart Attacks & Strokes Everyday
 PHASE Preventing Heart Attacks & Strokes Everyday Welcome to the PHASE Learning Community! Joseph D. Young, MD Kaiser Permanente Northern California Jean Nudelman Kaiser Permanente Northern California
PHASE Preventing Heart Attacks & Strokes Everyday Welcome to the PHASE Learning Community! Joseph D. Young, MD Kaiser Permanente Northern California Jean Nudelman Kaiser Permanente Northern California
Objectives. Describe results and implications of recent landmark hypertension trials
 Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014
 HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
Systolic Blood Pressure Intervention Trial (SPRINT)
") 09:30-09:50 2016.4.15 Systolic Blood Pressure Intervention Trial (SPRINT) IN A NEPHROLOGIST S VIEW Sejoong Kim Seoul National University Bundang Hospital Current guidelines for BP control Lowering BP
09:30-09:50 2016.4.15 Systolic Blood Pressure Intervention Trial (SPRINT) IN A NEPHROLOGIST S VIEW Sejoong Kim Seoul National University Bundang Hospital Current guidelines for BP control Lowering BP
Hypertension Management: A Moving Target
 9:45 :30am Hypertension Management: A Moving Target SPEAKER Karol Watson, MD, PhD, FACC Presenter Disclosure Information The following relationships exist related to this presentation: Karol E. Watson,
9:45 :30am Hypertension Management: A Moving Target SPEAKER Karol Watson, MD, PhD, FACC Presenter Disclosure Information The following relationships exist related to this presentation: Karol E. Watson,
The New Hypertension Guidelines
 The New Hypertension Guidelines Joseph Saseen, PharmD Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Disclosure Joseph Saseen reports no conflicts
The New Hypertension Guidelines Joseph Saseen, PharmD Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Disclosure Joseph Saseen reports no conflicts
Hypertension in 2015: SPRINT-ing ahead of JNC-8. MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic
 Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Treating Hypertension in 2018: What Makes the Most Sense Today?
 Treating Hypertension in 2018: What Makes the Most Sense Today? Daniel Blanchard, MD Professor of Medicine UC San Diego Cardiovascular Center La Jolla, California 1 2 Speaker Disclosures Consultant and/or
Treating Hypertension in 2018: What Makes the Most Sense Today? Daniel Blanchard, MD Professor of Medicine UC San Diego Cardiovascular Center La Jolla, California 1 2 Speaker Disclosures Consultant and/or
Management of Lipid Disorders and Hypertension: Implications of the New Guidelines
 Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Hypertension Management Controversies in the Elderly Patient
 Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Preventing and Treating High Blood Pressure
 Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Modern Management of Hypertension
 Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
Managing Hypertension in 2016
 Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
JNC 8 -Controversies. Sagren Naidoo Nephrologist CMJAH
 JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
ALLHAT. Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic
 1 U.S. Department of Health and Human Services National Institutes of Health Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker
1 U.S. Department of Health and Human Services National Institutes of Health Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Modern Management of Hypertension: Where Do We Draw the Line?
 Modern Management of Hypertension: Where Do We Draw the Line? Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Blood Pressure
Modern Management of Hypertension: Where Do We Draw the Line? Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Blood Pressure
HYPERTENSION: UPDATE 2018
 HYPERTENSION: UPDATE 2018 From the Cardiologist point of view Richard C Padgett, MD I have no disclosures HYPERTENSION ALWAYS THE ELEPHANT IN THE EXAM ROOM BUT SOMETIMES IT CHARGES HTN IN US ~78 million
HYPERTENSION: UPDATE 2018 From the Cardiologist point of view Richard C Padgett, MD I have no disclosures HYPERTENSION ALWAYS THE ELEPHANT IN THE EXAM ROOM BUT SOMETIMES IT CHARGES HTN IN US ~78 million
Antihypertensive Trial Design ALLHAT
 1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
Randomized Design of ALLHAT BP Trial
 Outcomes in Hypertensive Black and Nonblack Patients Treated with Chlorthalidone, Amlodipine, and Lisinopril* *Wright JT, Dunn JK, Cutler JA et al. JAMA 2005:293:1595-1608. 42,418 High-risk hypertensive
Outcomes in Hypertensive Black and Nonblack Patients Treated with Chlorthalidone, Amlodipine, and Lisinopril* *Wright JT, Dunn JK, Cutler JA et al. JAMA 2005:293:1595-1608. 42,418 High-risk hypertensive
Hypertension Guidelines: Lessons for Primary Care. Paul A James MD Professor and Chair Department of Family Medicine University of Washington
 Hypertension Guidelines: Lessons for Primary Care Paul A James MD Professor and Chair Department of Family Medicine University of Washington Disclaimer and Financial Disclosure I have no financial interests
Hypertension Guidelines: Lessons for Primary Care Paul A James MD Professor and Chair Department of Family Medicine University of Washington Disclaimer and Financial Disclosure I have no financial interests
Hypertension and Diabetes Should we be SPRINTING or Reaching an ACCORD?
 Hypertension and Diabetes Should we be SPRINTING or Reaching an ACCORD? Suzanne Oparil, MD Distinguished Professor of Medicine, Professor of Cell, Developmental and Integrative Biology Director, Vascular
Hypertension and Diabetes Should we be SPRINTING or Reaching an ACCORD? Suzanne Oparil, MD Distinguished Professor of Medicine, Professor of Cell, Developmental and Integrative Biology Director, Vascular
Hypertension and the SPRINT Trial: Is Lower Better
 Hypertension and the SPRINT Trial: Is Lower Better 8th Annual Orange County Symposium on Cardiovascular Disease Prevention Saturday, October 8, 2016 Keith C. Norris, MD, PhD, FASN Professor of Medicine,
Hypertension and the SPRINT Trial: Is Lower Better 8th Annual Orange County Symposium on Cardiovascular Disease Prevention Saturday, October 8, 2016 Keith C. Norris, MD, PhD, FASN Professor of Medicine,
Hypertension Update Clinical Controversies Regarding Age and Race
 Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Treating Hypertension in Individuals with Diabetes
 Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
DISCLOSURE PHARMACIST OBJECTIVES 9/30/2014 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES. I have nothing to disclose.
 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
Hypertension and Cardiovascular Disease
 Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure. No relevant financial relationships. Blood Pressure and Risk
 MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Blood Pressure Targets: Where are We Now?
 Blood Pressure Targets: Where are We Now? Diana Cao, PharmD, BCPS-AQ Cardiology Assistant Professor Department of Clinical & Administrative Sciences California Northstate University College of Pharmacy
Blood Pressure Targets: Where are We Now? Diana Cao, PharmD, BCPS-AQ Cardiology Assistant Professor Department of Clinical & Administrative Sciences California Northstate University College of Pharmacy
New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets
 New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of
New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of
Evaluation and Management of Hypertension in Women. Vesna D. Garovic, M.D. Moscow, Russia, December 2016
 Evaluation and Management of Hypertension in Women Vesna D. Garovic, M.D. Moscow, Russia, December 2016 2016 MFMER 3508058-1 Women are not small men There is nothing as powerful as an idea whose time has
Evaluation and Management of Hypertension in Women Vesna D. Garovic, M.D. Moscow, Russia, December 2016 2016 MFMER 3508058-1 Women are not small men There is nothing as powerful as an idea whose time has
The Latest Generation of Clinical
 The Latest Generation of Clinical Guidelines: HTN and HLD Dave Brackett Clinical Guideline Purpose Uniform approach Awareness of key details Diagnosis Treatment Monitoring Evidence based approach Inform
The Latest Generation of Clinical Guidelines: HTN and HLD Dave Brackett Clinical Guideline Purpose Uniform approach Awareness of key details Diagnosis Treatment Monitoring Evidence based approach Inform
Hypertension Update 2016 AREEF ISHANI, MD MS CHIEF OF MEDICINE MINNEAPOLIS VA MEDICAL CENTER PROFESSOR OF MEDICINE UNIVERSITY OF MINNESOTA
 Hypertension Update 2016 AREEF ISHANI, MD MS CHIEF OF MEDICINE MINNEAPOLIS VA MEDICAL CENTER PROFESSOR OF MEDICINE UNIVERSITY OF MINNESOTA Case 1 What should be your BP goal for an elderly (> 75 yrs of
Hypertension Update 2016 AREEF ISHANI, MD MS CHIEF OF MEDICINE MINNEAPOLIS VA MEDICAL CENTER PROFESSOR OF MEDICINE UNIVERSITY OF MINNESOTA Case 1 What should be your BP goal for an elderly (> 75 yrs of
Managing Hypertension in 2018
 MANAGING HYPERTENSION IN 2018 How Do We Work With Conflicting Data and Conflicting Guidelines? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School
MANAGING HYPERTENSION IN 2018 How Do We Work With Conflicting Data and Conflicting Guidelines? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School
Evolving Concepts on Hypertension: Implications of Three Guidelines (JNC 8 Panel, ESH/ESC, NICE/BSH)
") Evolving Concepts on Hypertension: Implications of Three Guidelines (JNC 8 Panel, ESH/ESC, NICE/BSH) Sidney C. Smith, Jr. MD, FACC, FAHA, FESC Professor of Medicine/Cardiology University of North Carolina
Evolving Concepts on Hypertension: Implications of Three Guidelines (JNC 8 Panel, ESH/ESC, NICE/BSH) Sidney C. Smith, Jr. MD, FACC, FAHA, FESC Professor of Medicine/Cardiology University of North Carolina
Objectives. Heart failure and Hypertension. Definition & epidemiology of heart failure HEART FAILURE 3/12/2016. Kirsten Bibbins-Domingo, PhD, MD, MAS
 Objectives Heart failure and Hypertension Kirsten Bibbins-Domingo, PhD, MD, MAS Lee Goldman, MD Endowed Chair in Medicine Professor of Medicine and of Epidemiology and Biostatistics University of California,
Objectives Heart failure and Hypertension Kirsten Bibbins-Domingo, PhD, MD, MAS Lee Goldman, MD Endowed Chair in Medicine Professor of Medicine and of Epidemiology and Biostatistics University of California,
New Lipid Guidelines. PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids.
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
Hypertension Update. Mayo Clinic 90 th Annual Clinical Reviews November 2 nd and 16 th, 2016
 Mayo Clinic 90 th Annual Clinical Reviews November 2 nd and 16 th, 2016 Hypertension Update Vincent J. Canzanello, M.D. Consultant, Division of Nephrology and Hypertension Professor or Medicine College
Mayo Clinic 90 th Annual Clinical Reviews November 2 nd and 16 th, 2016 Hypertension Update Vincent J. Canzanello, M.D. Consultant, Division of Nephrology and Hypertension Professor or Medicine College
Hypertension targets: sorting out the confusion. Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town
 Hypertension targets: sorting out the confusion Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town Historical Perspective The most famous casualty of this approach was the
Hypertension targets: sorting out the confusion Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town Historical Perspective The most famous casualty of this approach was the
Hypertension Update 2014:
 GSHTP Webinar Hypertension Update 2014: The Kaiser Permanente Northern California Experience Presented by: Marc Jaffe, MD Associate Clinical Professor of Medicine, UCSF Kaiser Permanente Northern California
GSHTP Webinar Hypertension Update 2014: The Kaiser Permanente Northern California Experience Presented by: Marc Jaffe, MD Associate Clinical Professor of Medicine, UCSF Kaiser Permanente Northern California
Hypertension. Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute
 Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, Financial Disclosures
 Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
ALLHAT Role of Diuretics in the Prevention of Heart Failure - The Antihypertensive and Lipid- Lowering Treatment to Prevent Heart Attack Trial
 1 ALLHAT Role of Diuretics in the Prevention of Heart Failure - The Antihypertensive and Lipid- Lowering Treatment to Prevent Heart Attack Trial Davis BR, Piller LB, Cutler JA, et al. Circulation 2006.113:2201-2210.
1 ALLHAT Role of Diuretics in the Prevention of Heart Failure - The Antihypertensive and Lipid- Lowering Treatment to Prevent Heart Attack Trial Davis BR, Piller LB, Cutler JA, et al. Circulation 2006.113:2201-2210.
Blood Pressure Measurement in SPRINT
 Blood Pressure Measurement in SPRINT Karen C. Johnson, MD, MPH, FAHA Vice Chair, SPRINT Steering Committee University of Tennessee Health Science Center, Department of Preventive Medicine For the SPRINT
Blood Pressure Measurement in SPRINT Karen C. Johnson, MD, MPH, FAHA Vice Chair, SPRINT Steering Committee University of Tennessee Health Science Center, Department of Preventive Medicine For the SPRINT
Hypertension in the Era of ACC/AHA: Practice Changing Evidence and Recommendations
 Hypertension in the Era of ACC/AHA: Practice Changing Evidence and Recommendations Gerald W. Smetana, M.D., MACP Division of General Medicine Beth Israel Deaconess Medical Center Professor of Medicine
Hypertension in the Era of ACC/AHA: Practice Changing Evidence and Recommendations Gerald W. Smetana, M.D., MACP Division of General Medicine Beth Israel Deaconess Medical Center Professor of Medicine
Difficult-to-Control & Resistant Hypertension. Anthony Viera, MD, MPH, FAHA Professor and Chair
 Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
Hypertension 2015: Recent Evidence that Will Change Your Practice
 Hypertension 2015: Recent Evidence that Will Change Your Practice Gerald W. Smetana, M.D. Division of General Medicine Beth Israel Deaconess Medical Center Professor of Medicine Harvard Medical School
Hypertension 2015: Recent Evidence that Will Change Your Practice Gerald W. Smetana, M.D. Division of General Medicine Beth Israel Deaconess Medical Center Professor of Medicine Harvard Medical School
MANAGEMENT OF HYPERTENSION: TREATMENT THRESHOLDS AND MEDICATION SELECTION
 Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
4/4/17 HYPERTENSION TARGETS: WHAT DO WE DO NOW? SET THE STAGE BP IN CLINICAL TRIALS?
 HYPERTENSION TARGETS: WHAT DO WE DO NOW? MICHAEL LEFEVRE, MD, MSPH PROFESSOR AND VICE CHAIR DEPARTMENT OF FAMILY AND COMMUNITY MEDICINE UNIVERSITY OF MISSOURI 4/4/17 DISCLOSURE: MEMBER OF THE JNC 8 PANEL
HYPERTENSION TARGETS: WHAT DO WE DO NOW? MICHAEL LEFEVRE, MD, MSPH PROFESSOR AND VICE CHAIR DEPARTMENT OF FAMILY AND COMMUNITY MEDICINE UNIVERSITY OF MISSOURI 4/4/17 DISCLOSURE: MEMBER OF THE JNC 8 PANEL
Update in Hypertension
 Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
ALLHAT. ALLHAT Antihypertensive Trial Results by Baseline Diabetic & Fasting Glucose Status
 ALLHAT Antihypertensive Trial Results by Baseline Diabetic & Fasting Glucose Status 1 Introduction and Background Clinical trials have reported reduction in CV events with diuretics, CCBs, ACE inhibitors,
ALLHAT Antihypertensive Trial Results by Baseline Diabetic & Fasting Glucose Status 1 Introduction and Background Clinical trials have reported reduction in CV events with diuretics, CCBs, ACE inhibitors,
APPENDIX D: PHARMACOTYHERAPY EVIDENCE
 Página 1 de 7 APPENDIX D: PHARMACOTYHERAPY EVIDENCE Table D1. Outcome Trials of Antihypertensive Agents Study Drug Regimen N Duration Primary Outcomes Remarks Antihypertensive Therapy vs Placebo SHEP 1991
Página 1 de 7 APPENDIX D: PHARMACOTYHERAPY EVIDENCE Table D1. Outcome Trials of Antihypertensive Agents Study Drug Regimen N Duration Primary Outcomes Remarks Antihypertensive Therapy vs Placebo SHEP 1991
The earlier BP control the better cardiovascular outcome. Jin Oh Na Cardiovascular center Korea University Medical College
 The earlier BP control the better cardiovascular outcome Jin Oh Na Cardiovascular center Korea University Medical College Index Introduction HOPE-3 Trial Sprint Study Summary Each 2 mmhg decrease in SBP
The earlier BP control the better cardiovascular outcome Jin Oh Na Cardiovascular center Korea University Medical College Index Introduction HOPE-3 Trial Sprint Study Summary Each 2 mmhg decrease in SBP
Managing Hypertension in Diabetes Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park.
 Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
We are delighted to have Dr. Roetzheim with us today to discuss Managing Hypertension in Older Adult Patients.
 Richard Roetzheim, MD, MSPH is Professor and Chair, Department of Family Medicine at the University of South Florida Morsani College of Medicine. Dr. Roetzheim has considerable experience leading NIH funded
Richard Roetzheim, MD, MSPH is Professor and Chair, Department of Family Medicine at the University of South Florida Morsani College of Medicine. Dr. Roetzheim has considerable experience leading NIH funded
New Hypertension Guidelines: Why the change? Neil Brummond, M.D. Avera Medical Group Internal Medicine Sioux Falls, SD
 New Hypertension Guidelines: Why the change? Neil Brummond, M.D. Avera Medical Group Internal Medicine Sioux Falls, SD None Disclosures Objectives Understand trend in blood pressure clinical practice guidelines
New Hypertension Guidelines: Why the change? Neil Brummond, M.D. Avera Medical Group Internal Medicine Sioux Falls, SD None Disclosures Objectives Understand trend in blood pressure clinical practice guidelines
Hypertension Update 2009
 Hypertension Update 2009 New Drugs, New Goals, New Approaches, New Lessons from Clinical Trials Timothy C Fagan, MD, FACP Professor Emeritus University of Arizona New Drugs Direct Renin Inhibitors Endothelin
Hypertension Update 2009 New Drugs, New Goals, New Approaches, New Lessons from Clinical Trials Timothy C Fagan, MD, FACP Professor Emeritus University of Arizona New Drugs Direct Renin Inhibitors Endothelin
Controlling Hypertension in Primary Care: Hitting a moving target?
 Controlling Hypertension in Primary Care: Hitting a moving target? David J. Hyman, MD,MPH Professor of Medicine and Family & Community Medicine Chief, Section General Medicine Baylor College of Medicine
Controlling Hypertension in Primary Care: Hitting a moving target? David J. Hyman, MD,MPH Professor of Medicine and Family & Community Medicine Chief, Section General Medicine Baylor College of Medicine
Jared Moore, MD, FACP
 Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Objective & Outline. How the JNC Process Has Evolved. Expertise Represented on JNC 8 Panel
 Implementation: Joint National Committee on High Blood Pressure JNC 8 Joel Handler, MD Kaiser Permanente Care Management Institute Hypertension Lead Southern California Permanente Group Objective & Outline
Implementation: Joint National Committee on High Blood Pressure JNC 8 Joel Handler, MD Kaiser Permanente Care Management Institute Hypertension Lead Southern California Permanente Group Objective & Outline
Hypertension Putting the Guidelines into Practice
 Hypertension 2017 Putting the Guidelines into Practice Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or
Hypertension 2017 Putting the Guidelines into Practice Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or
Challenges in Hypertension: Incorporating Evolving Clinical Data Into Practice
 Challenges in Hypertension: Incorporating Evolving Clinical Data Into Practice Faculty Jan Basile, MD Professor of Medicine Seinsheimer Cardiovascular Health Program Division of General Internal Medicine
Challenges in Hypertension: Incorporating Evolving Clinical Data Into Practice Faculty Jan Basile, MD Professor of Medicine Seinsheimer Cardiovascular Health Program Division of General Internal Medicine
Hypertension Pharmacotherapy: A Practical Approach
 Hypertension Pharmacotherapy: A Practical Approach Ronald Victor, MD Burns & Allen Chair in Cardiology Director, The Hypertension Center Associate Director, The Heart Institute Hypertension Center 1. 2.
Hypertension Pharmacotherapy: A Practical Approach Ronald Victor, MD Burns & Allen Chair in Cardiology Director, The Hypertension Center Associate Director, The Heart Institute Hypertension Center 1. 2.
DISCLOSURES OUTLINE OUTLINE 9/29/2014 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE
 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
Blood pressure treatment target in diabetes. Should it be <130 mmhg?
 Blood pressure treatment target in diabetes Should it be
Blood pressure treatment target in diabetes Should it be
None. Disclosure: Relationships with Industry Conflicts of Interests. Learning Objectives: Participants will be able to:
 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults: Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC 8) James W. Shaw, MD Memorial Lecture
2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults: Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC 8) James W. Shaw, MD Memorial Lecture
Update in Outpatient Medicine JNC 8, Hypertension and More
 Update in Outpatient Medicine JNC 8, Hypertension and More March 6 th 2015 Robert Gluckman, MD, FACP CMO Providence Health Plans Disclosures Stock Holdings Abbott Labs Abbvie Bristol Myers Squibb GE Proctor
Update in Outpatient Medicine JNC 8, Hypertension and More March 6 th 2015 Robert Gluckman, MD, FACP CMO Providence Health Plans Disclosures Stock Holdings Abbott Labs Abbvie Bristol Myers Squibb GE Proctor
Update in Cardiology Pharmacologic Management of Cardiovascular Risk. Christopher C. Roe, MSN, ACNP
 Update in Cardiology Pharmacologic Management of Cardiovascular Risk Christopher C. Roe, MSN, ACNP Objectives 1. Verbalize understanding of new pharmacologic guidelines in the treatment of hypertension
Update in Cardiology Pharmacologic Management of Cardiovascular Risk Christopher C. Roe, MSN, ACNP Objectives 1. Verbalize understanding of new pharmacologic guidelines in the treatment of hypertension
Adult Blood Pressure Clinician Guide June 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Adult Blood Pressure Clinician Guide June 2018 Adult Blood Pressure Clinician Guide June 2018 Introduction This Clinician Guide is based on the 2018
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Adult Blood Pressure Clinician Guide June 2018 Adult Blood Pressure Clinician Guide June 2018 Introduction This Clinician Guide is based on the 2018
T. Suithichaiyakul Cardiomed Chula
 T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
Understanding the importance of blood pressure control An overview of new guidelines: How do they impact daily current management?
 Understanding the importance of blood pressure control An overview of new guidelines: How do they impact daily current management? Slides presented during CDMC in Almaty, Kazakhstan on Saturday April 12,
Understanding the importance of blood pressure control An overview of new guidelines: How do they impact daily current management? Slides presented during CDMC in Almaty, Kazakhstan on Saturday April 12,
ALLHAT. U.S. Department of Health and Human Services. National Institutes of Health. National Heart, Lung, and Blood Institute
 U.S. Department of Health and Human Services National Institutes of Health National Heart, Lung, and Blood Institute Review of Heart Failure Events in the Antihypertensive and Lipid Lowering Treatment
U.S. Department of Health and Human Services National Institutes of Health National Heart, Lung, and Blood Institute Review of Heart Failure Events in the Antihypertensive and Lipid Lowering Treatment
2/9/2017. Financial Disclosures/Unapproved Use. Achieving Harmony in Blood Pressure Guidelines Around the Globe. Roger S. Blumenthal, MD.
 Achieving Harmony in Blood Pressure Guidelines Around the Globe Roger S. Blumenthal, MD The Kenneth Jay Pollin Professor of Cardiology Director, The Johns Hopkins Ciccarone Center for the Prevention Of
Achieving Harmony in Blood Pressure Guidelines Around the Globe Roger S. Blumenthal, MD The Kenneth Jay Pollin Professor of Cardiology Director, The Johns Hopkins Ciccarone Center for the Prevention Of
Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension
 Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension Prof. Massimo Volpe, MD, FAHA, FESC, Chair of Cardiology, Department of Clinical and Molecular Medicine
Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension Prof. Massimo Volpe, MD, FAHA, FESC, Chair of Cardiology, Department of Clinical and Molecular Medicine
How do we diagnose hypertension today? Presentation Subtitle
 How do we diagnose hypertension today? Presentation Subtitle Renata Cífková Case 1 JM, a 64-year-old lady referred to our center because of undesirable effects of her antihypertensive medication Personal
How do we diagnose hypertension today? Presentation Subtitle Renata Cífková Case 1 JM, a 64-year-old lady referred to our center because of undesirable effects of her antihypertensive medication Personal
Disclosures. Learning Objectives. Hypertension: a sprint to the finish Ontario Pharmacists Association 1
 Disclosures I have no current or past relationships with commercial entities I have received a speaker s fee from the Ontario Pharmacists Association for this learning activity Laura Tsang PharmD Sunnybrook
Disclosures I have no current or past relationships with commercial entities I have received a speaker s fee from the Ontario Pharmacists Association for this learning activity Laura Tsang PharmD Sunnybrook
New Clinical Trends in Geriatric Medicine. April 8, 2016 Amanda Lathia, MD, MPhil Staff, Center for Geriatric Medicine
 New Clinical Trends in Geriatric Medicine April 8, 2016 Amanda Lathia, MD, MPhil Staff, Center for Geriatric Medicine Objectives Review current guidelines for blood pressure (BP) control in older adults
New Clinical Trends in Geriatric Medicine April 8, 2016 Amanda Lathia, MD, MPhil Staff, Center for Geriatric Medicine Objectives Review current guidelines for blood pressure (BP) control in older adults
Brent M. Egan, MD Professor of Medicine USCSOM Greenville
 Contemporary Management of Uncontrolled and Treatment Resistant Hypertension Brent M. Egan, MD Professor of Medicine USCSOM Greenville Disclosures (past 3 years): Honoraria: BCBSSC, Medtronic Grant Support:
Contemporary Management of Uncontrolled and Treatment Resistant Hypertension Brent M. Egan, MD Professor of Medicine USCSOM Greenville Disclosures (past 3 years): Honoraria: BCBSSC, Medtronic Grant Support:
Management of Hypertension in Women
 Management of Hypertension in Women Eliseo J. Pérez-Stable MD Professor of Medicine DGIM, Department of Medicine July 1, 2013 Declaration of full disclosure: No conflict of interest (I have never been
Management of Hypertension in Women Eliseo J. Pérez-Stable MD Professor of Medicine DGIM, Department of Medicine July 1, 2013 Declaration of full disclosure: No conflict of interest (I have never been
HYPERTENSION MANAGEMENT IN ELDERLY POPULATIONS
 HYPERTENSION MANAGEMENT IN ELDERLY POPULATIONS Michael J. Scalese, PharmD, BCPS, CACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 14, 2018 DISCLOSURE/CONFLICT OF INTEREST
HYPERTENSION MANAGEMENT IN ELDERLY POPULATIONS Michael J. Scalese, PharmD, BCPS, CACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 14, 2018 DISCLOSURE/CONFLICT OF INTEREST
Best Practices in Cardiac Care: Getting with the Guidelines
 Best Practices in Cardiac Care: Getting with the Guidelines December 9, 2014 Agenda Cardiovascular Disease: How do the guidelines fit into an implementation scheme? What the guidelines set out to accomplish
Best Practices in Cardiac Care: Getting with the Guidelines December 9, 2014 Agenda Cardiovascular Disease: How do the guidelines fit into an implementation scheme? What the guidelines set out to accomplish
Hypertension Update. Faculty/Presenter Disclosure
 Hypertension Update Who Gives a CHEP About Targets? Faculty/Presenter Disclosure Presenter: Raj Padwal Relationships that may introduce potential bias and/or conflict of interest: Grants/Research Support:
Hypertension Update Who Gives a CHEP About Targets? Faculty/Presenter Disclosure Presenter: Raj Padwal Relationships that may introduce potential bias and/or conflict of interest: Grants/Research Support:
Update in Outpatient Medicine ACP Scientific Session November 12, 2016
 Update in Outpatient Medicine ACP Scientific Session November 12, 2016 Robert Gluckman MD, MACP Chief Medical Officer Providence Health Plans Disclosures Stock Holdings Abbott Labs Abbvie Bristol Myers
Update in Outpatient Medicine ACP Scientific Session November 12, 2016 Robert Gluckman MD, MACP Chief Medical Officer Providence Health Plans Disclosures Stock Holdings Abbott Labs Abbvie Bristol Myers
Hypertension in the Elderly. John Puxty Division of Geriatrics Center for Studies in Aging and Health, Providence Care
 Hypertension in the Elderly John Puxty Division of Geriatrics Center for Studies in Aging and Health, Providence Care Learning Objectives Review evidence for treatment of hypertension in elderly Consider
Hypertension in the Elderly John Puxty Division of Geriatrics Center for Studies in Aging and Health, Providence Care Learning Objectives Review evidence for treatment of hypertension in elderly Consider
Συμπεράσματα από τις νέες μελέτες για την αρτηριακή υπέρταση (SPRINT,PATHAY 2,HOPE 3)
") Συμπεράσματα από τις νέες μελέτες για την αρτηριακή υπέρταση (SPRINT,PATHAY 2,HOPE 3) Χάρης Γράσσος MD,FESC,PhD,EHS Διευθυντής Καρδιολόγος Γ.Ν.Α ΚΑΤ Visiting Professor University of Bolton U.K New England
Συμπεράσματα από τις νέες μελέτες για την αρτηριακή υπέρταση (SPRINT,PATHAY 2,HOPE 3) Χάρης Γράσσος MD,FESC,PhD,EHS Διευθυντής Καρδιολόγος Γ.Ν.Α ΚΑΤ Visiting Professor University of Bolton U.K New England
Hypertension Controversies: SPRINTing to New Goals
 Hypertension Controversies: SPRINTing to New Goals Diana Isaacs, PharmD, BCPS, BC-ADM, CDE Clinical Pharmacy Specialist Cleveland Clinic Lauren Wolfe, PharmD Primary Care Clinical Specialist Cleveland
Hypertension Controversies: SPRINTing to New Goals Diana Isaacs, PharmD, BCPS, BC-ADM, CDE Clinical Pharmacy Specialist Cleveland Clinic Lauren Wolfe, PharmD Primary Care Clinical Specialist Cleveland
Making Sense of the US Hypertension Guideline in 2018
 Making Sense of the US Hypertension Guideline in 2018 William J. Elliott, M.D., Ph.D. 04 MAY 18 Presenter Disclosure Information William J. Elliott, M.D., Ph.D. Making Sense of the US Hypertension Guideline
Making Sense of the US Hypertension Guideline in 2018 William J. Elliott, M.D., Ph.D. 04 MAY 18 Presenter Disclosure Information William J. Elliott, M.D., Ph.D. Making Sense of the US Hypertension Guideline
Pre-ALLHAT Drug Use. Diuretics. ß-Blockers. ACE Inhibitors. CCBs. Year. % of Treated Patients on Medication. CCBs. Beta Blockers.
 Pre- Drug Use % of Treated Patients on Medication 60 50 40 30 20 10 0 1978 Diuretics ß-Blockers ACE Inhibitors Year CCBs CCBs Beta Blockers Diuretics ACE Inhibitors 1980 1982 1984 1986 1988 1990 1992 IMS
Pre- Drug Use % of Treated Patients on Medication 60 50 40 30 20 10 0 1978 Diuretics ß-Blockers ACE Inhibitors Year CCBs CCBs Beta Blockers Diuretics ACE Inhibitors 1980 1982 1984 1986 1988 1990 1992 IMS
Hypertension: Update
 Hypertension: Update Meenakshi A Bhalla MD,FACC Associate Professor of Medicine Director Preventive Cardiology Advanced Heart Failure and Transplant Cardiology University of Kentucky Faculty Disclosure
Hypertension: Update Meenakshi A Bhalla MD,FACC Associate Professor of Medicine Director Preventive Cardiology Advanced Heart Failure and Transplant Cardiology University of Kentucky Faculty Disclosure
Hypertension Putting the Guidelines into Practice
 Hypertension 2017 Putting the Guidelines into Practice Disclosures Relationships with commercial interests: Grants/Research Support: Speakers Bureau/Honoraria: Consulting Fees: Data Safety and Monitoring:
Hypertension 2017 Putting the Guidelines into Practice Disclosures Relationships with commercial interests: Grants/Research Support: Speakers Bureau/Honoraria: Consulting Fees: Data Safety and Monitoring:
STANDARD treatment algorithm mmHg
 STANDARD treatment algorithm 130-140mmHg (i) At BASELINE, If AVERAGE SBP 1 > 140mmHg If on no antihypertensive drugs: Start 1 drug: If >55 years old / Afro-Caribbean: Calcium channel blocker (CCB) 2 If
STANDARD treatment algorithm 130-140mmHg (i) At BASELINE, If AVERAGE SBP 1 > 140mmHg If on no antihypertensive drugs: Start 1 drug: If >55 years old / Afro-Caribbean: Calcium channel blocker (CCB) 2 If
Masked Hypertension. Why Should We Care? Dr. Peter J. Lin Director Primary Care Initiatives - Canadian Heart Research Centre
 Masked Hypertension Why Should We Care? Dr. Peter J. Lin Director Primary Care Initiatives - Canadian Heart Research Centre PRESENTER DISCLOSURE Faculty: Dr. Peter Lin Relationships with commercial interests:
Masked Hypertension Why Should We Care? Dr. Peter J. Lin Director Primary Care Initiatives - Canadian Heart Research Centre PRESENTER DISCLOSURE Faculty: Dr. Peter Lin Relationships with commercial interests:
Difficult to Treat Hypertension
 Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Blood Pressure Treatment Goals
 Blood Pressure Treatment Goals Kenneth Izuora, MD, MBA, FACE Associate Professor UNLV School of Medicine November 18, 2017 Learning Objectives Discuss the recent studies on treating hypertension Review
Blood Pressure Treatment Goals Kenneth Izuora, MD, MBA, FACE Associate Professor UNLV School of Medicine November 18, 2017 Learning Objectives Discuss the recent studies on treating hypertension Review
Hypertension Update. Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy
 Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
OCTOBER 7-10 PHILADELPHIA, PENNSYLVANIA
 OMED 17 OCTOBER 7-10 PHILADELPHIA, PENNSYLVANIA 29.5 Category 1-A CME credits anticipated ACOFP / AOA s 122 nd Annual Osteopathic Medical Conference & Exposition ACOFP - The Heart of the Matter - An Evidence
OMED 17 OCTOBER 7-10 PHILADELPHIA, PENNSYLVANIA 29.5 Category 1-A CME credits anticipated ACOFP / AOA s 122 nd Annual Osteopathic Medical Conference & Exposition ACOFP - The Heart of the Matter - An Evidence
Don t let the pressure get to you:
 Balanced information for better care Don t let the pressure get to you: Current evidence-based goals for treating hypertension A cornerstone of primary care: Lowering high blood pressure prevents cardiovascular
Balanced information for better care Don t let the pressure get to you: Current evidence-based goals for treating hypertension A cornerstone of primary care: Lowering high blood pressure prevents cardiovascular