Heinz-Hermann Weitkemper, EBCP. 4th Joint Scandinavian Conference in Cardiothoracic Surgery 2012 Vilnius / Lithuania
|
|
|
- Myra Sharp
- 5 years ago
- Views:
Transcription



1 Heinz-Hermann Weitkemper, EBCP
2 Everyone who earnestly practices perfusion is acting with the full belief that what they are doing is in the best interest of their patients. Perfusion can never be normal, only adequate!


3 Flow rate must equal the basal cardiac output to ensure a wide margin of safety in the metabolic support of tissues.
4 Flow affects blood trauma, embolic load, collateral flow, surgical field. Influence of temperature and haemodilution Flow and pressure are inter-related & dynamic? Pulsatile flow What is optimal perfusion?

5 The question of arterial pressure and its relationship to optimal perfusion flow rates is of major importance, but the prevailing opinions are diverse and contradictory. The overwhelming evidence appears to indicate that there is no definite prescribed flow rate, but a range of physiologic parameters within which one can perfuse with a relative margin of safety, dependent on the prevailing circumstances.
6 CARDIAC OUTPUT CPB FLOW Changes based on metabolic needs Usually in the range of 2.8 to 3.0 L/min/m² May increase up to 15 L/min/m² CO with arterial oxygen content, determines the oxygen delivery (DO 2 ) Guaranty oxygen need VO 2 ) Pulsatile flow Adjusted by the perfusionist based on temperature and blood pressure 2.0 to 3.0 L/min/m² Adequacy of the pump flow controlled with SvO 2 monitoring Qb with arterial oxygen content, determines the oxygen delivery (DO 2 ) Should guaranty oxygen need (VO 2 )



7 Flow is 2,4 LPM/m 2 MAP 60 mmhg ABG = normal SvO 2 > 75%

8 Optimal Versus Suboptimal Perfusion During Cardiopulmonary Bypass and the Inflammatory Response F. De Somer, SEMIN CARDIOTHORAC VASC ANESTH 2009

 + (0.003 x PaO2)")
9 The blood oxygen content based on: hemoglobin content, and dissolved O 2 Described by the equation: CaO2 = (1.34 x Hb x SaO2) + (0.003 x PaO2)




10 O 2 delivery = DO 2 = CO x CaO 2 x 10 Usually = ml/min/m 2 dysoxia threshold 270 ml/min/m 2


11 If the Blood-Flow is constantly DO 2 is determinant by Haemoglobin Content



12 Depends of: Cardiac output Difference in oxygen content b/w arterial and venous blood VO 2 = CO x 1.34 x Hb (SaO 2 SvO 2 )10
13 Temperature: VO 2 decrease approx. 7% per 1 0 Cels. Anesthesia: 37 C: 4 ml/kg/min 37 C + Anesthesia: 2-3 ml/kg/min 28 C + Anesthesia: 1-2 ml/kg/min


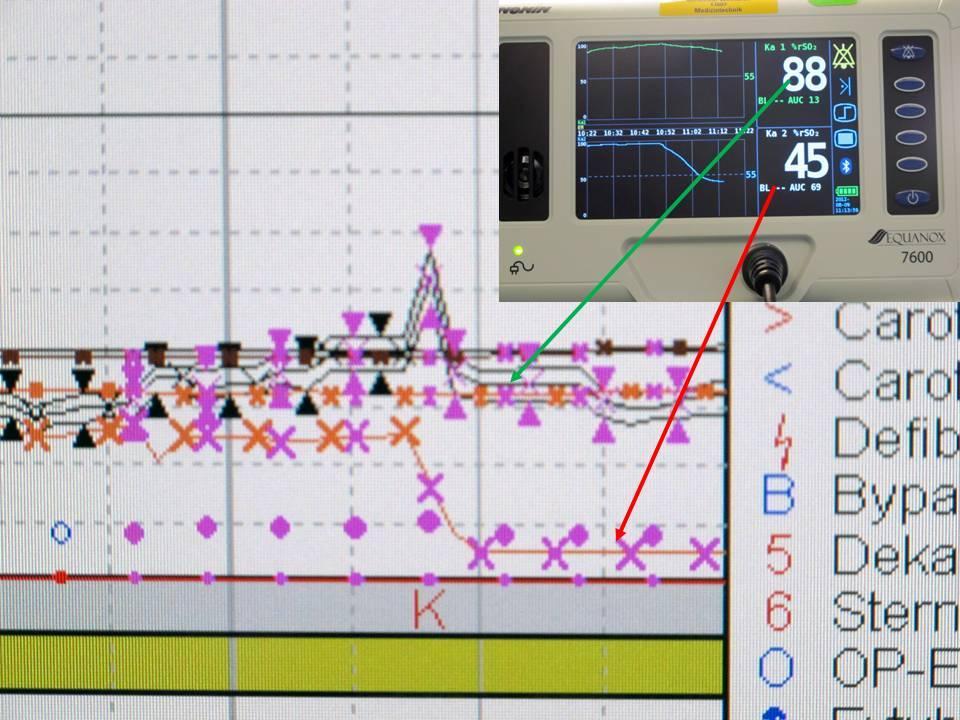
14 Increase: Hypovolemia Hypoperfusion Hyperthermia Anemia Hypoxia Decrease: Decreased Metabolic Rate Alkalosis Anesthesia Hypothermia

15 To keep tissues aerobic metabolism we need oxygen. Allows the conversion of glucose to ATP We get 36 moles ATP per mole glucose
16 Less oxygen = anaerobic metabolism dysoxia threshold 270 ml/min/m 2 Only 2 moles ATP per mole glucose Production of lactate




17 Patients experiencing a single HCT value of 19% or less during CPB had more than twice the mortality as patients with a nadir HCT value of 25%! DeFoe 2001, Multicenter study of 6980 patients undergoing isolated CABG surgery. Hematocrit below 21% is associated with increase of renal failure, stroke and morbidity and mortality.

18 The Influence of Hematocrit Optimal Perfusion During Cardiopulmonary Bypass: An Evidence-Based Approach Glenn S. Murphy, MD 2008 ;ANESTHESIA & ANALGESIA
 the RR-ARF risk is low,")

19 Patients with a low DO 2 have a high risk of RR-ARF regardless of their HCT value; conversely, if the DO 2 is maintained above the critical threshold,(270 ml /min/m 2 ) the RR-ARF risk is low, again regardless of the HCT. Ranucci M, Romitti F, Isgro G, et al. Oxygen delivery during cardiopulmonary bypass and acute renal failure after coronary operations. Ann Thorac Surg. 2005;80:
20 To guarantee sufficient oxygen supply for peripheral tissue a careful coupling of pump-flow and arterial oxygen content is mandatory. Keep the blood-flow high enough to hold DO 2 above the critical level (> 270ml/min/m 2 )

21 Hello Houston. Mhm. We have problems concerning SvO 2 levels!
22 Inline Monitoring (most common) Venous Saturation S v O 2 Venous partial oxygen Tension P V O 2 Did not guarantee optimal tissue oxygenation Did not predict hyperlactatemia. Mixed venous saturation is a weak indicator especially for cerebral and splanchnic venous oxygen saturation. Lindholm L, Hansdottir V, Lundqvist M, Jeppsson A. The relationship between mixed venous and regional venous oxygen saturation during cardiopulmonary bypass. Perfusion. 2002;17:

23 Flow is 2,4 LPM/m 2 MAP 60 mmhg ABG = normal SvO2 > 75% Flow is coupled to HCT to keep DO 2 > 270ml/min/m 2
24 Regional Perfusion is still unknown We must be assured that DO 2 is adequate to the patient. We must monitor the metabolism also = Lactat Several studies describe hyperlactatemia in up to 20% of all patients undergoing cardiac surgery with CPB indicating nonoptimal perfusion.

25 Hyperlactatemia during CPB is due mainly to a DO 2 inadequate to fulfill the metabolic needs of the patient, and this critical value is approximately 270 ml/min/m 2. Therefore, every attempt should be applied to avoid HL during CPB, and the critical DO 2 value of 260 to 270 ml/minute per m 2 should be considered whenever setting the pump flow and the maximum acceptable hemodilution degree. Hyperlactatemia during cardiopulmonary bypass: determinants and impact on postoperative outcome M. Ranucci, Critical Care 2006; Vol 10 No 6.

26 Annals of Thoracic Surgery; 2006
27 Carbon dioxide derived parameters are representative of hyperlactatemia during CPB, as a result of the carbon dioxide produced under anaerobic conditions through the buffering of protons by the bicarbonate system. The carbon dioxide elimination rate measured at the exhaled site of the oxygenator may be used for an indirect assessment of the metabolic state of the patient. Predictor of Hyperlactatemia: If the ratio between oxygen delivery and carbon dioxide production is lower than 5. Anaerobic metabolism during cardiopulmonary bypass: predictive value of carbon dioxide derived parameters. Ranucci M,. Ann Thorac Surg. 2006;81:

28 Correlation between Oxygen Delivery DO 2 and CO 2 production

29 We have to be aware: The interpretation of lactate measurement requires caution. The Lactate concentration depends on balance between production and clearance. Very Rapid production of Lactate but the Clearance depends on the metabolic elimination and is prolonged. Monitoring of Carbon Dioxide derived parameters together with Oxygen delivery can be a considerable aid. To optimize the pump-flow and the arterial oxygen content.





30 Flow is 2.4l / min / m 2 MAP is 60mmHg ABG is normal SvO 2 is > 75% The flow is coupled to the Hct to guarantee a DO 2 > 270 ml / min / m 2 The flow ensures no lactate formation according to the DO 2 / VCO 2 ratio


31 Brain Liver Kidney Muscle Bowel Vascular


32

33 48. If Perfusion ain t happy, ain t nobody happy! Heart Surgeon`s Little Instruction Book

34 Heart-Lung-Bypass: principles and techniques of extracorporeal circulation by Galleti and Brecher 1962 Optimal Perfusion Flow Rates for Cardiopulmonary Bypass. Bennett A. Mitchell. JECT 1991 Optimal Perfusion During Cardiopulmonary Bypass: An Evidence-Based Approach Glenn S. Murphy, MD 2008 ;ANESTHESIA & ANALGESIA The relationship between mixed venous and regional venous oxygen saturation during cardiopulmonary bypass. Lindholm L, Hansdottir V, Lundqvist M, Jeppsson A. Perfusion. 2002;17: Combination of venoarterial PCO2 difference with arteriovenous O2 content difference to detect anaerobic Metabolism in patients. Mekontso-Dessap A, Castelain V, Anguel N, et al. Intensive Care Med. 2002;28: Oxygen delivery during cardiopulmonary bypass and acute renal failure after coronary operations. Ranucci M, Romitti F, Isgro G, et al. Ann Thorac Surg.2005;80: Acute renal injury and lowest hematocrit during cardiopulmonary bypass: Not only a matter of cellular hypoxemia. Ranucci M, Menicanti L, Frigiola A Ann Thorac Surg. 2004;78: Hyperlactatemia during cardiopulmonary bypass: determinants and impact on postoperative outcome. Ranucci M, De Toffol B, Isgro G, Romitti F, Conti D, Vicentini M. Crit Care. 2006;10:R167. Anaerobic metabolism during cardiopulmonary bypass: predictive value of carbon dioxide derived parameters. Ranucci M, Isgro G, Romitti F, Mele S, Biagioli B, Giomarelli P. Ann Thorac Surg. 2006;81: Optimal Versus Suboptimal Perfusion During Cardiopulmonary Bypass and the Inflammatory Response F. De Somer, Seminars in Cardiothoracic and Vascular Anesthesia, 2009;13 :2; What Is Optimal Flow and How to Validate This F.ilip De Somer, JECT. 2007;39:
Conventional vs. Goal Directed Perfusion (GDP) Management: Decision Making & Challenges
 Management: Decision Making & Challenges") Conventional vs. Goal Directed Perfusion (GDP) Management: Decision Making & Challenges GEORGE JUSTISON CCP MANAGER PERFUSION SERVICES UNIVERSITY OF COLORADO HOSPITAL How do you define adequate perfusion?
Conventional vs. Goal Directed Perfusion (GDP) Management: Decision Making & Challenges GEORGE JUSTISON CCP MANAGER PERFUSION SERVICES UNIVERSITY OF COLORADO HOSPITAL How do you define adequate perfusion?
Goal Directed Perfusion: theory, clinical results, and key rules
 Goal Directed Perfusion: theory, clinical results, and key rules M. Ranucci Director of Clinical Research Dept of Cardiothoracic and Vascular Anesthesia and Intensive Care IRCCS Policlinico S.Donato Ranuuci,
Goal Directed Perfusion: theory, clinical results, and key rules M. Ranucci Director of Clinical Research Dept of Cardiothoracic and Vascular Anesthesia and Intensive Care IRCCS Policlinico S.Donato Ranuuci,
Defining Optimal Perfusion during CPB. Carlo Alberto Tassi Marketing Manager Eurosets Italy
 Defining Optimal Perfusion during CPB Carlo Alberto Tassi Marketing Manager Eurosets Italy It is a device able to monitor in a real time vital parameters and able to provide information regarding the transport
Defining Optimal Perfusion during CPB Carlo Alberto Tassi Marketing Manager Eurosets Italy It is a device able to monitor in a real time vital parameters and able to provide information regarding the transport
Anaerobic Metabolism During Cardiopulmonary Bypass: Predictive Value of Carbon Dioxide Derived Parameters
 Anaerobic Metabolism During Cardiopulmonary Bypass: Predictive Value of Carbon Dioxide Derived Parameters Marco Ranucci, MD, Giuseppe Isgrò, MD, Federica Romitti, MD, Sara Mele, MD, Bonizella Biagioli,
Anaerobic Metabolism During Cardiopulmonary Bypass: Predictive Value of Carbon Dioxide Derived Parameters Marco Ranucci, MD, Giuseppe Isgrò, MD, Federica Romitti, MD, Sara Mele, MD, Bonizella Biagioli,
Is Timing Everything?
 The Journal of ExtraCorporeal Technology Is Timing Everything? George Justison, CCP University of Colorado Hospital, Perfusion Services, Aurora, Colorado Presented at Goal Directed Therapy Symposium, 54th
The Journal of ExtraCorporeal Technology Is Timing Everything? George Justison, CCP University of Colorado Hospital, Perfusion Services, Aurora, Colorado Presented at Goal Directed Therapy Symposium, 54th
Variation in Measurement and Reporting of Goal Directed Perfusion Parameters
 The Journal of ExtraCorporeal Technology Variation in Measurement and Reporting of Goal Directed Perfusion Parameters Robert A. Baker Cardiac Surgery Research and Perfusion, Flinders Medical Centre and
The Journal of ExtraCorporeal Technology Variation in Measurement and Reporting of Goal Directed Perfusion Parameters Robert A. Baker Cardiac Surgery Research and Perfusion, Flinders Medical Centre and
Low Oxygen Delivery as a Predictor of Acute Kidney Injury during Cardiopulmonary Bypass
 The Journal of ExtraCorporeal Technology Original Articles Low Oxygen Delivery as a Predictor of Acute Kidney Injury during Cardiopulmonary Bypass Richard F. Newland, BSc, CCP; Robert A. Baker, PhD, CCP
The Journal of ExtraCorporeal Technology Original Articles Low Oxygen Delivery as a Predictor of Acute Kidney Injury during Cardiopulmonary Bypass Richard F. Newland, BSc, CCP; Robert A. Baker, PhD, CCP
Transfusion and Blood Conservation
 Transfusion and Blood Conservation Kenneth G. Shann, CCP Assistant Director, Perfusion Services Senior Advisor, Performance Improvement Department of Cardiovascular and Thoracic Surgery Montefiore Medical
Transfusion and Blood Conservation Kenneth G. Shann, CCP Assistant Director, Perfusion Services Senior Advisor, Performance Improvement Department of Cardiovascular and Thoracic Surgery Montefiore Medical
Risk Factors and Management of Acute Renal Injury in Cardiac Surgery
 Risk Factors and Management of Acute Renal Injury in Cardiac Surgery Robert S Kramer, MD, FACS Clinical Associate Professor of Surgery Tufts University School of Medicine Maine Medical Center, Portland
Risk Factors and Management of Acute Renal Injury in Cardiac Surgery Robert S Kramer, MD, FACS Clinical Associate Professor of Surgery Tufts University School of Medicine Maine Medical Center, Portland
a non-trivial challenge for a perfusionist
 DO 2 -guided nephroprotective perfusion - a non-trivial challenge for a perfusionist Dirk Buchwald, Krzysztof Klak xygenium oxygen - Colorless and odorless gas - Most common chemical element on earth atomic
DO 2 -guided nephroprotective perfusion - a non-trivial challenge for a perfusionist Dirk Buchwald, Krzysztof Klak xygenium oxygen - Colorless and odorless gas - Most common chemical element on earth atomic
Critical Care Monitoring. Assessing the Adequacy of Tissue Oxygenation. Tissue Oxygenation - Step 1. Tissue Oxygenation
 Critical Care Monitoring 1 Assessing the Adequacy of Tissue oxygenation is the end-product of many complex steps 2 - Step 1 Oxygen must be made available to alveoli 3 1 - Step 2 Oxygen must cross the alveolarcapillary
Critical Care Monitoring 1 Assessing the Adequacy of Tissue oxygenation is the end-product of many complex steps 2 - Step 1 Oxygen must be made available to alveoli 3 1 - Step 2 Oxygen must cross the alveolarcapillary
Get connected to optimal data management practices
 CONNECT TM Get connected to optimal data management practices The first innovative and intuitive perfusion data management system designed to improve clinical eff iciency 4 and enable Goal-Directed Perfusion
CONNECT TM Get connected to optimal data management practices The first innovative and intuitive perfusion data management system designed to improve clinical eff iciency 4 and enable Goal-Directed Perfusion
Get connected to optimal data management practices
 TM Get connected to optimal data management practices The first innovative and intuitive perfusion data management system designed to improve clinical eff iciency 4 and enable Goal-Directed Perfusion Therapy
TM Get connected to optimal data management practices The first innovative and intuitive perfusion data management system designed to improve clinical eff iciency 4 and enable Goal-Directed Perfusion Therapy
Dr. Puntarica Suwanprathes. Version 2007
 Dr. Puntarica Suwanprathes Version 2007 O 2 and CO 2 transport in blood Oxyhemoglobin dissociation curve O 2 consumption (VO 2 ) CO 2 production (VCO 2 ) O 2 capacity O 2 content: CaO 2 or CvO 2 %saturation
Dr. Puntarica Suwanprathes Version 2007 O 2 and CO 2 transport in blood Oxyhemoglobin dissociation curve O 2 consumption (VO 2 ) CO 2 production (VCO 2 ) O 2 capacity O 2 content: CaO 2 or CvO 2 %saturation
3. Which of the following would be inconsistent with respiratory alkalosis? A. ph = 7.57 B. PaCO = 30 mm Hg C. ph = 7.63 D.
 Pilbeam: Mechanical Ventilation, 4 th Edition Test Bank Chapter 1: Oxygenation and Acid-Base Evaluation MULTIPLE CHOICE 1. The diffusion of carbon dioxide across the alveolar capillary membrane is. A.
Pilbeam: Mechanical Ventilation, 4 th Edition Test Bank Chapter 1: Oxygenation and Acid-Base Evaluation MULTIPLE CHOICE 1. The diffusion of carbon dioxide across the alveolar capillary membrane is. A.
The Hemodynamic Puzzle
 The Hemodynamic Puzzle SVV NIRS O 2 ER Lactate Energy Metabolism (Oxygen Consumption) (Ml/min/m 2 ) Oxygen Debt: To Pay or Not to Pay? Full Recovery Possible Delayed Repayment of O 2 Debt Oxygen Deficit
The Hemodynamic Puzzle SVV NIRS O 2 ER Lactate Energy Metabolism (Oxygen Consumption) (Ml/min/m 2 ) Oxygen Debt: To Pay or Not to Pay? Full Recovery Possible Delayed Repayment of O 2 Debt Oxygen Deficit
Why Old Blood is Bad. tales from the electronic perfusion record. Molly Marko, BS, BSE, CCP Geisinger Health System Danville, Pennsylvania
 Why Old Blood is Bad tales from the electronic perfusion record Molly Marko, BS, BSE, CCP Geisinger Health System Danville, Pennsylvania Disclosure I have no financial relationship with any of the companies
Why Old Blood is Bad tales from the electronic perfusion record Molly Marko, BS, BSE, CCP Geisinger Health System Danville, Pennsylvania Disclosure I have no financial relationship with any of the companies
12 RANUCCI ET AL Ann Thorac Surg HEMODILUTION DURING CPB AND MORBIDITY RISK 2010;89:11 8 Abbreviations and Acronyms CI confidence interval CPB cardiop
 ORIGINAL ARTICLES: CARDIOTHORACIC ANESTHESIOLOGY: The Annals of Thoracic Surgery CME Program is located online at http://cme.ctsnetjournals.org. To take the CME activity related to this article, you must
ORIGINAL ARTICLES: CARDIOTHORACIC ANESTHESIOLOGY: The Annals of Thoracic Surgery CME Program is located online at http://cme.ctsnetjournals.org. To take the CME activity related to this article, you must
IMPROVE PATIENT OUTCOMES AND SAFETY IN ADULT CARDIAC SURGERY.
 Clinical Evidence Guide IMPROVE PATIENT OUTCOMES AND SAFETY IN ADULT CARDIAC SURGERY. With the INVOS cerebral/somatic oximeter An examination of controlled studies reveals that responding to cerebral desaturation
Clinical Evidence Guide IMPROVE PATIENT OUTCOMES AND SAFETY IN ADULT CARDIAC SURGERY. With the INVOS cerebral/somatic oximeter An examination of controlled studies reveals that responding to cerebral desaturation
Mechanical Ventilation. Assessing the Adequacy of Tissue Oxygenation. Tissue Oxygenation - Step 1. Tissue Oxygenation
 1 Mechanical Ventilation Assessing the Adequacy of 2 Tissue oxygenation is the end-product of many complex steps - Step 1 3 Oxygen must be made available to alveoli 1 - Step 2 4 Oxygen must cross the alveolarcapillary
1 Mechanical Ventilation Assessing the Adequacy of 2 Tissue oxygenation is the end-product of many complex steps - Step 1 3 Oxygen must be made available to alveoli 1 - Step 2 4 Oxygen must cross the alveolarcapillary
UTILITY of ScvO 2 and LACTATE
 UTILITY of ScvO 2 and LACTATE Professor Jeffrey Lipman Department of Intensive Care Medicine Royal Brisbane Hospital University of Queensland THIS TRIP SPONSORED AND PAID FOR BY STRUCTURE Physiology -
UTILITY of ScvO 2 and LACTATE Professor Jeffrey Lipman Department of Intensive Care Medicine Royal Brisbane Hospital University of Queensland THIS TRIP SPONSORED AND PAID FOR BY STRUCTURE Physiology -
How to maintain optimal perfusion during Cardiopulmonary By-pass. Herdono Poernomo, MD
 How to maintain optimal perfusion during Cardiopulmonary By-pass Herdono Poernomo, MD Cardiopulmonary By-pass Target Physiologic condition as a healthy person Everything is in Normal Limit How to maintain
How to maintain optimal perfusion during Cardiopulmonary By-pass Herdono Poernomo, MD Cardiopulmonary By-pass Target Physiologic condition as a healthy person Everything is in Normal Limit How to maintain
Transfusion & Mortality. Philippe Van der Linden MD, PhD
 Transfusion & Mortality Philippe Van der Linden MD, PhD Conflict of Interest Disclosure In the past 5 years, I have received honoraria or travel support for consulting or lecturing from the following companies:
Transfusion & Mortality Philippe Van der Linden MD, PhD Conflict of Interest Disclosure In the past 5 years, I have received honoraria or travel support for consulting or lecturing from the following companies:
Change in the perioperative blood glucose and blood lactate levels of non-diabetic patients undergoing coronary bypass surgery
 1220 Change in the perioperative blood glucose and blood lactate levels of non-diabetic patients undergoing coronary bypass surgery CHUNJIAN SHEN 1,3, TIANXIANG GU 1, LILI GU 2, ZHONGYI XIU 1, ZHIWEI ZHANG
1220 Change in the perioperative blood glucose and blood lactate levels of non-diabetic patients undergoing coronary bypass surgery CHUNJIAN SHEN 1,3, TIANXIANG GU 1, LILI GU 2, ZHONGYI XIU 1, ZHIWEI ZHANG
Arterial Blood Gas Analysis
 Arterial Blood Gas Analysis L Lester www.3bv.org Bones, Brains & Blood Vessels Drawn from radial or femoral arteries. Invasive procedure Caution must be taken with patient on anticoagulants ph: 7.35-7.45
Arterial Blood Gas Analysis L Lester www.3bv.org Bones, Brains & Blood Vessels Drawn from radial or femoral arteries. Invasive procedure Caution must be taken with patient on anticoagulants ph: 7.35-7.45
Intra-operative Echocardiography: When to Go Back on Pump
 Intra-operative Echocardiography: When to Go Back on Pump GREGORIO G. ROGELIO, MD., F.P.C.C. OUTLINE A. Indications for Intraoperative Echocardiography B. Role of Intraoperative Echocardiography C. Criteria
Intra-operative Echocardiography: When to Go Back on Pump GREGORIO G. ROGELIO, MD., F.P.C.C. OUTLINE A. Indications for Intraoperative Echocardiography B. Role of Intraoperative Echocardiography C. Criteria
Advances in Transfusion and Blood Conservation
 Advances in Transfusion and Blood Conservation Arman Kilic, MD Division of Cardiac Surgery, Department of Surgery, Johns Hopkins Hospital, Baltimore, MD No relevant financial relationships to disclose.
Advances in Transfusion and Blood Conservation Arman Kilic, MD Division of Cardiac Surgery, Department of Surgery, Johns Hopkins Hospital, Baltimore, MD No relevant financial relationships to disclose.
Base deficit in the immediate postoperative period of open-heart surgery and patient outcome
 Original Research Medical Journal of the Islamic Republic of Iran.Vol. 21, No. 4, February 2008. pp. 215-222 Base deficit in the immediate postoperative period of open-heart surgery and patient outcome
Original Research Medical Journal of the Islamic Republic of Iran.Vol. 21, No. 4, February 2008. pp. 215-222 Base deficit in the immediate postoperative period of open-heart surgery and patient outcome
CPB pump flow, and effective Flow in patient. 1
 Peter Fast Nielsen ECCP, MCT AUH. Skejby, Denmark. CPB pump flow, and effective Flow in patient. 1 Pump Flow - that s what the Perfusionist controls, right? Well: Does the pump deliver what we expect?
Peter Fast Nielsen ECCP, MCT AUH. Skejby, Denmark. CPB pump flow, and effective Flow in patient. 1 Pump Flow - that s what the Perfusionist controls, right? Well: Does the pump deliver what we expect?
Clinical relevance of perioperative ScvO 2 monitoring
 Risk adapted peri operative haemodynamic management Clinical relevance of perioperative ScvO 2 monitoring Euroanaesthesia 2007 Meeting Munich, Germany, 9.-12. June 2007 Claus-Georg KRENN Dept. of Anaesthesia
Risk adapted peri operative haemodynamic management Clinical relevance of perioperative ScvO 2 monitoring Euroanaesthesia 2007 Meeting Munich, Germany, 9.-12. June 2007 Claus-Georg KRENN Dept. of Anaesthesia
Absolute Cerebral Oximeters for Cardiovascular Surgical Cases
 Absolute Cerebral Oximeters for Cardiovascular Surgical Cases Mary E. Arthur, MD, Associate Professor, Anesthesiology and Perioperative Medicine Medical College of Georgia at Georgia Regents University
Absolute Cerebral Oximeters for Cardiovascular Surgical Cases Mary E. Arthur, MD, Associate Professor, Anesthesiology and Perioperative Medicine Medical College of Georgia at Georgia Regents University
FOLLOW-UP MEDICAL CARE OF SERVICE MEMBERS AND VETERANS CARDIOPULMONARY EXERCISE TESTING
 Cardiopulmonary Exercise Testing Chapter 13 FOLLOW-UP MEDICAL CARE OF SERVICE MEMBERS AND VETERANS CARDIOPULMONARY EXERCISE TESTING WILLIAM ESCHENBACHER, MD* INTRODUCTION AEROBIC METABOLISM ANAEROBIC METABOLISM
Cardiopulmonary Exercise Testing Chapter 13 FOLLOW-UP MEDICAL CARE OF SERVICE MEMBERS AND VETERANS CARDIOPULMONARY EXERCISE TESTING WILLIAM ESCHENBACHER, MD* INTRODUCTION AEROBIC METABOLISM ANAEROBIC METABOLISM
Intensive Care Unit Admission Parameters Improve the Accuracy of Operative Mortality Predictive Models in Cardiac Surgery
 Intensive Care Unit Admission Parameters Improve the Accuracy of Operative Mortality Predictive Models in Cardiac Surgery Marco Ranucci*, Andrea Ballotta, Serenella Castelvecchio, Ekaterina Baryshnikova,
Intensive Care Unit Admission Parameters Improve the Accuracy of Operative Mortality Predictive Models in Cardiac Surgery Marco Ranucci*, Andrea Ballotta, Serenella Castelvecchio, Ekaterina Baryshnikova,
Bicarbonate in the NICU
 OMG Bicarbonate in the NICU A Useless Therapy? At first I thought I was going to have to refute the paper Then I got into it and thought: I m so confused Then I learned a lot HOPEFULLY I CAN LEARN YOU
OMG Bicarbonate in the NICU A Useless Therapy? At first I thought I was going to have to refute the paper Then I got into it and thought: I m so confused Then I learned a lot HOPEFULLY I CAN LEARN YOU
Carbon Dioxide Transport. Carbon Dioxide. Carbon Dioxide Transport. Carbon Dioxide Transport - Plasma. Hydrolysis of Water
 Module H: Carbon Dioxide Transport Beachey Ch 9 & 10 Egan pp. 244-246, 281-284 Carbon Dioxide Transport At the end of today s session you will be able to : Describe the relationship free hydrogen ions
Module H: Carbon Dioxide Transport Beachey Ch 9 & 10 Egan pp. 244-246, 281-284 Carbon Dioxide Transport At the end of today s session you will be able to : Describe the relationship free hydrogen ions
Effects of Increasing FiO 2 on Venous Saturation During Cardiopulmonary Bypass in the Swine Model
 The Journal of The American Society of Extra-Corporeal Technology Effects of Increasing FiO 2 on Venous Saturation During Cardiopulmonary Bypass in the Swine Model Jeffery D. Nichols, MPS, CCP; Alfred
The Journal of The American Society of Extra-Corporeal Technology Effects of Increasing FiO 2 on Venous Saturation During Cardiopulmonary Bypass in the Swine Model Jeffery D. Nichols, MPS, CCP; Alfred
DEFINING OPTIMAL PERFUSION DURING CPB and MONITORING ECMO
 DEFINING OPTIMAL PERFUSION DURING CPB and MONITORING ECMO CPB OPTIMIZATION & ECMO MONITORING Sweep Gas Flow Oxygen Delivery Oxygen Delivery Index Oxygen Consumption Oxygen Consumption Index Oxygen Extraction
DEFINING OPTIMAL PERFUSION DURING CPB and MONITORING ECMO CPB OPTIMIZATION & ECMO MONITORING Sweep Gas Flow Oxygen Delivery Oxygen Delivery Index Oxygen Consumption Oxygen Consumption Index Oxygen Extraction
What is. InSpectra StO 2?
 What is InSpectra StO 2? www.htibiomeasurement.com What is InSpectra StO 2? Hemoglobin O 2 saturation is measured in three areas: 1) Arterial (SaO 2, SpO 2 ) Assesses how well oxygen is loading onto hemoglobin
What is InSpectra StO 2? www.htibiomeasurement.com What is InSpectra StO 2? Hemoglobin O 2 saturation is measured in three areas: 1) Arterial (SaO 2, SpO 2 ) Assesses how well oxygen is loading onto hemoglobin
Objective 2/9/2012. Blood Gas Analysis In The Univentricular Patient: The Need For A Different Perspective. VENOARTERIAL CO2 GRADIENT
 Blood Gas Analysis In The Univentricular Patient: The Need For A Different Perspective. Gary Grist RN CCP Chief Perfusionist The Children s Mercy Hospitals and Clinics Kansas City, Mo. Objective The participant
Blood Gas Analysis In The Univentricular Patient: The Need For A Different Perspective. Gary Grist RN CCP Chief Perfusionist The Children s Mercy Hospitals and Clinics Kansas City, Mo. Objective The participant
Elevated blood lactate levels associated with metabolic
 Outcome With High Blood Lactate Levels During Cardiopulmonary Bypass in Adult Cardiac Operation Philippe Demers, MD, Stéphane Elkouri, MD, Raymond Martineau, MD, André Couturier, MSc, and Raymond Cartier,
Outcome With High Blood Lactate Levels During Cardiopulmonary Bypass in Adult Cardiac Operation Philippe Demers, MD, Stéphane Elkouri, MD, Raymond Martineau, MD, André Couturier, MSc, and Raymond Cartier,
Advanced Monitoring of Cardiovascular and Respiratory Systems in Infants Kuwait 2018 Dr. Yasser Elsayed, MD, PhD Director of the Targeted Neonatal
 Advanced Monitoring of Cardiovascular and Respiratory Systems in Infants Kuwait 2018 Dr. Yasser Elsayed, MD, PhD Director of the Targeted Neonatal Echocardiography, Point of Care and Hemodynamics Program
Advanced Monitoring of Cardiovascular and Respiratory Systems in Infants Kuwait 2018 Dr. Yasser Elsayed, MD, PhD Director of the Targeted Neonatal Echocardiography, Point of Care and Hemodynamics Program
Anesthesiology in advanced radical surgery. Bruno Carrara Ospedali Riuniti di Bergamo
 Anesthesiology in advanced radical surgery Bruno Carrara Ospedali Riuniti di Bergamo Anesthetic considerations Anesthesiology in advanced radical surgery Anesthesiologists's task is to minimize the contribution
Anesthesiology in advanced radical surgery Bruno Carrara Ospedali Riuniti di Bergamo Anesthetic considerations Anesthesiology in advanced radical surgery Anesthesiologists's task is to minimize the contribution
Hell or High Lactate. Charles Bruen, MD. resusreview.com/regionsmar17
 Hell or High Lactate Charles Bruen, MD resusreview.com/regionsmar17 No Disclosures No Off-label Use 3 Positive troponin? Inpatient or Observation? Lactate elevated? Goals What causes lactate production?
Hell or High Lactate Charles Bruen, MD resusreview.com/regionsmar17 No Disclosures No Off-label Use 3 Positive troponin? Inpatient or Observation? Lactate elevated? Goals What causes lactate production?
-Cardiogenic: shock state resulting from impairment or failure of myocardium
 Shock chapter Shock -Condition in which tissue perfusion is inadequate to deliver oxygen, nutrients to support vital organs, cellular function -Affects all body systems -Classic signs of early shock: Tachycardia,tachypnea,restlessness,anxiety,
Shock chapter Shock -Condition in which tissue perfusion is inadequate to deliver oxygen, nutrients to support vital organs, cellular function -Affects all body systems -Classic signs of early shock: Tachycardia,tachypnea,restlessness,anxiety,
Physiological Causes of Abnormal ABG s
 Physiological Causes of Abnormal ABG s Major Student Performance Objective 1 1. The student will be able to discuss causes for various types of blood gas results. 2. They will also be required to discuss
Physiological Causes of Abnormal ABG s Major Student Performance Objective 1 1. The student will be able to discuss causes for various types of blood gas results. 2. They will also be required to discuss
Blood transfusions in sepsis, the elderly and patients with TBI
 Blood transfusions in sepsis, the elderly and patients with TBI Shabbir Alekar MICU, CH Baragwanath Academic Hospital & The University of the Witwatersrand CCSSA Congress 11 June 2015 Packed RBC - complications
Blood transfusions in sepsis, the elderly and patients with TBI Shabbir Alekar MICU, CH Baragwanath Academic Hospital & The University of the Witwatersrand CCSSA Congress 11 June 2015 Packed RBC - complications
Evaluation of a Heads-up Display for Cardiopulmonary Bypass
 Technique Evaluation of a Heads-up Display for Cardiopulmonary Bypass Jon W. Austin, CCP Western Cardiovascular Perfusion, Scottsdale, Arizona Keywords: cardiopulmonary bypass, heads-up display, perfusion
Technique Evaluation of a Heads-up Display for Cardiopulmonary Bypass Jon W. Austin, CCP Western Cardiovascular Perfusion, Scottsdale, Arizona Keywords: cardiopulmonary bypass, heads-up display, perfusion
Continuous monitoring of cardiac output: why and how
 33rd International Symposium of Intensive Care and Emergency Medicine, Brussels 19.03.-22.03.2013 UNIVERSITÄTSKLINIKUM Schleswig-Holstein Continuous monitoring of cardiac output: why and how Berthold Bein,
33rd International Symposium of Intensive Care and Emergency Medicine, Brussels 19.03.-22.03.2013 UNIVERSITÄTSKLINIKUM Schleswig-Holstein Continuous monitoring of cardiac output: why and how Berthold Bein,
7/4/2015. diffuse lung injury resulting in noncardiogenic pulmonary edema due to increase in capillary permeability
 Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
Identification and Treatment of the Patient with Sleep Related Hypoventilation
 Identification and Treatment of the Patient with Sleep Related Hypoventilation Hillary Loomis-King, MD Pulmonary and Critical Care of NW MI Munson Sleep Disorders Center X Conflict of Interest Disclosures
Identification and Treatment of the Patient with Sleep Related Hypoventilation Hillary Loomis-King, MD Pulmonary and Critical Care of NW MI Munson Sleep Disorders Center X Conflict of Interest Disclosures
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE
 Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
The Relationship between Intra-Operative Transfusions and Nadir Hematocrit on Post-Operative Outcomes after Cardiac Surgery
 The Journal of ExtraCorporeal Technology The Relationship between Intra-Operative Transfusions and Nadir Hematocrit on Post-Operative Outcomes after Cardiac Surgery Joshua B. Goldberg, MD;* Kenneth G.
The Journal of ExtraCorporeal Technology The Relationship between Intra-Operative Transfusions and Nadir Hematocrit on Post-Operative Outcomes after Cardiac Surgery Joshua B. Goldberg, MD;* Kenneth G.
Blood Management of the Cardiac Patient in the Postoperative Period
 Blood Management of the Cardiac Patient in the Postoperative Period Al Stammers, MSA, CCP, Eric Tesdahl, PhD Andy Stasko MS, CCP, RRT, Linda Mongero, BS, CCP, Sam Weinstein, MD, MBA Goal To examine the
Blood Management of the Cardiac Patient in the Postoperative Period Al Stammers, MSA, CCP, Eric Tesdahl, PhD Andy Stasko MS, CCP, RRT, Linda Mongero, BS, CCP, Sam Weinstein, MD, MBA Goal To examine the
DO 2 > VO 2. The amount of oxygen delivered is a product of cardiac output (L/min) and the amount of oxygen in the arterial blood (ml/dl).
 and the amount of oxygen in the arterial blood (ml/dl).") Shock (Part 1): Review and Diagnostic Approach Jeffrey M. Todd, DVM, DACVECC University of Minnesota, St. Paul, MN Overview Shock is the clinical presentation of inadequate oxygen utilization, typically
Shock (Part 1): Review and Diagnostic Approach Jeffrey M. Todd, DVM, DACVECC University of Minnesota, St. Paul, MN Overview Shock is the clinical presentation of inadequate oxygen utilization, typically
CCAS CPB Workshop Curriculum Outline Perfusion: What you might not know
 CCAS CPB Workshop Curriculum Outline Perfusion: What you might not know Scott Lawson, CCP Carrie Striker, CCP Disclosure: Nothing to disclose Objectives: * Demonstrate how the cardiopulmonary bypass machine
CCAS CPB Workshop Curriculum Outline Perfusion: What you might not know Scott Lawson, CCP Carrie Striker, CCP Disclosure: Nothing to disclose Objectives: * Demonstrate how the cardiopulmonary bypass machine
Acute Kidney Injury after Cardiac Surgery: Incidence, Risk Factors and Prevention
 Acute Kidney Injury after Cardiac Surgery: Incidence, Risk Factors and Prevention Hong Liu, MD Professor of Clinical Anesthesiology Department of Anesthesiology and Pain Medicine University of California
Acute Kidney Injury after Cardiac Surgery: Incidence, Risk Factors and Prevention Hong Liu, MD Professor of Clinical Anesthesiology Department of Anesthesiology and Pain Medicine University of California
i-stat Alinity v Utilization Guide
 istat Alinity v Utilization Guide The istat Alinity v delivers blood gas, acidbase, electrolyte, chemistry, and hematology measurements in a completely portable, handheld package. Accuracy is ensured by
istat Alinity v Utilization Guide The istat Alinity v delivers blood gas, acidbase, electrolyte, chemistry, and hematology measurements in a completely portable, handheld package. Accuracy is ensured by
OXYGENATION AND ACID- BASE EVALUATION. Chapter 1
 OXYGENATION AND ACID- BASE EVALUATION Chapter 1 MECHANICAL VENTILATION Used when patients are unable to sustain the level of ventilation necessary to maintain the gas exchange functions Artificial support
OXYGENATION AND ACID- BASE EVALUATION Chapter 1 MECHANICAL VENTILATION Used when patients are unable to sustain the level of ventilation necessary to maintain the gas exchange functions Artificial support
Arterial Blood Gases. Dr Mark Young Mater Health Services
 Arterial Blood Gases Dr Mark Young Mater Health Services Why do them? Quick results Bedside test Range of important information Oxygenation Effectiveness of gas exchange Control of ventilation Acid base
Arterial Blood Gases Dr Mark Young Mater Health Services Why do them? Quick results Bedside test Range of important information Oxygenation Effectiveness of gas exchange Control of ventilation Acid base
Content Display. - Introduction to Unit 4. Unit 4 - Cardiorespiratory Response to Exercise : Lesson 1. KINE xxxx Exercise Physiology
 Content Display Unit 4 - Cardiorespiratory Response to Exercise : Lesson KINE xxxx Exercise Physiology 5 Unit 4 - Cardiorespiratory Response to Exercise Lesson U4LP - Introduction to Unit 4 The specific
Content Display Unit 4 - Cardiorespiratory Response to Exercise : Lesson KINE xxxx Exercise Physiology 5 Unit 4 - Cardiorespiratory Response to Exercise Lesson U4LP - Introduction to Unit 4 The specific
Endpoints of Resuscitation for Circulatory Shock: When Enough is Enough?
 Endpoints of Resuscitation for Circulatory Shock: When Enough is Enough? Emanuel P. Rivers, MD, MPH, IOM Vice Chairman and Research Director Departments of Emergency Medicine and Surgery Henry Ford Hospital
Endpoints of Resuscitation for Circulatory Shock: When Enough is Enough? Emanuel P. Rivers, MD, MPH, IOM Vice Chairman and Research Director Departments of Emergency Medicine and Surgery Henry Ford Hospital
Maternal and Fetal Physiology
 Background Maternal and Fetal Physiology Anderson Lo, DO Fellow, Maternal-Fetal Medicine Wayne State University School of Medicine SEMCME Fetal Assessment Course July 20, 2018 Oxygen pathway Mother Placenta
Background Maternal and Fetal Physiology Anderson Lo, DO Fellow, Maternal-Fetal Medicine Wayne State University School of Medicine SEMCME Fetal Assessment Course July 20, 2018 Oxygen pathway Mother Placenta
There are number of parameters which are measured: ph Oxygen (O 2 ) Carbon Dioxide (CO 2 ) Bicarbonate (HCO 3 -) AaDO 2 O 2 Content O 2 Saturation
 Carbon Dioxide (CO 2 ) Bicarbonate (HCO 3 -) AaDO 2 O 2 Content O 2 Saturation") Arterial Blood Gases (ABG) A blood gas is exactly that...it measures the dissolved gases in your bloodstream. This provides one of the best measurements of what is known as the acid-base balance. The body
Arterial Blood Gases (ABG) A blood gas is exactly that...it measures the dissolved gases in your bloodstream. This provides one of the best measurements of what is known as the acid-base balance. The body
Evidence-Based. Management of Severe Sepsis. What is the BP Target?
 Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Physical Education Studies Year 11 ATAR. CHAPTER 5: Exercise Physiology NEXT
 Physical Education Studies Year 11 ATAR CHAPTER 5: Exercise Physiology NEXT Welcome to the quiz for Chapter 5 You will be given 30 multiple choice questions Click on the correct answer Use the links to
Physical Education Studies Year 11 ATAR CHAPTER 5: Exercise Physiology NEXT Welcome to the quiz for Chapter 5 You will be given 30 multiple choice questions Click on the correct answer Use the links to
UPMC Critical Care
 UPMC Critical Care www.ccm.pitt.edu Shock and Monitoring Samuel A. Tisherman, MD, FACS, FCCM Professor Departments of CCM and Surgery University of Pittsburgh Shock Anaerobic metabolism Lactic acidosis
UPMC Critical Care www.ccm.pitt.edu Shock and Monitoring Samuel A. Tisherman, MD, FACS, FCCM Professor Departments of CCM and Surgery University of Pittsburgh Shock Anaerobic metabolism Lactic acidosis
This PDF is available for free download from a site hosted by Medknow Publications
 Indian J Crit Care Med Oct-Dec 006 Vol 10 Issue 4 IJCCM October-December 003 Vol 7 Issue 4 Research Article Correlation of mixed venous and central venous oxygen saturation and its relation to cardiac
Indian J Crit Care Med Oct-Dec 006 Vol 10 Issue 4 IJCCM October-December 003 Vol 7 Issue 4 Research Article Correlation of mixed venous and central venous oxygen saturation and its relation to cardiac
Annals of Cardiac Anaesthesia 2005; 8: Shinde et al. Blood Lactate Levels during CPB 39
 Annals of Cardiac Anaesthesia 2005; 8: 39 44 Shinde et al. Blood Lactate Levels during CPB 39 Blood Lactate Levels During Cardiopulmonary Bypass for Valvular Heart Surgery ORIGINAL ARTICLES Santosh B Shinde,
Annals of Cardiac Anaesthesia 2005; 8: 39 44 Shinde et al. Blood Lactate Levels during CPB 39 Blood Lactate Levels During Cardiopulmonary Bypass for Valvular Heart Surgery ORIGINAL ARTICLES Santosh B Shinde,
Disclosures. Set up audience participation. Test question. Outline. Neuromonitoring What and When? IP for monitoring technology licensed to Medtronic
 Neuromonitoring What and When? Disclosures IP for monitoring technology licensed to Medtronic Ken Brady, MD Pediatrics, Anesthesia, Critical Care Texas Children s Hospital Baylor College of Medicine Set
Neuromonitoring What and When? Disclosures IP for monitoring technology licensed to Medtronic Ken Brady, MD Pediatrics, Anesthesia, Critical Care Texas Children s Hospital Baylor College of Medicine Set
Transfusion Limbo How Low Will You Go? Safely. Nina A. Guzzetta, M.D. Children s Healthcare of Atlanta Emory University School of Medicine
 Transfusion Limbo How Low Will You Go? Safely Nina A. Guzzetta, M.D. Children s Healthcare of Atlanta Emory University School of Medicine Objectives Benefits and risks of RBC administration in pediatric
Transfusion Limbo How Low Will You Go? Safely Nina A. Guzzetta, M.D. Children s Healthcare of Atlanta Emory University School of Medicine Objectives Benefits and risks of RBC administration in pediatric
Perioperative Goal- Protocol Summary
 Perioperative Goal- Directed Therapy Protocol Summary Evidence-based, perioperative Goal-Directed Therapy (GDT) protocols. Several single centre randomized controlled trials, meta-analysis and quality
Perioperative Goal- Directed Therapy Protocol Summary Evidence-based, perioperative Goal-Directed Therapy (GDT) protocols. Several single centre randomized controlled trials, meta-analysis and quality
ARTERIAL BLOOD GASES PART 1 BACK TO BASICS SSR OLIVIA ELSWORTH SEPT 2017
 ARTERIAL BLOOD GASES PART 1 BACK TO BASICS SSR OLIVIA ELSWORTH SEPT 2017 WHAT INFORMATION DOES AN ABG GIVE US? ph = measure of hydrogen ion concentration (acidity or alkalinity) PaCO2 = partial pressure
ARTERIAL BLOOD GASES PART 1 BACK TO BASICS SSR OLIVIA ELSWORTH SEPT 2017 WHAT INFORMATION DOES AN ABG GIVE US? ph = measure of hydrogen ion concentration (acidity or alkalinity) PaCO2 = partial pressure
INVOS System Inservice Guide for Pediatric Use. INVOS System Inservice Guide for Pediatric Use
 INVOS System Inservice Guide for Pediatric Use INVOS System Inservice Guide for Pediatric Use The INVOS System: A Window to Perfusion Adequacy The noninvasive INVOS System reports the venous- weighted
INVOS System Inservice Guide for Pediatric Use INVOS System Inservice Guide for Pediatric Use The INVOS System: A Window to Perfusion Adequacy The noninvasive INVOS System reports the venous- weighted
Module G: Oxygen Transport. Oxygen Transport. Dissolved Oxygen. Combined Oxygen. Topics to Cover
 Topics to Cover Module G: Oxygen Transport Oxygen Transport Oxygen Dissociation Curve Oxygen Transport Studies Tissue Hypoxia Cyanosis Polycythemia Oxygen Transport Oxygen is carried from the lungs to
Topics to Cover Module G: Oxygen Transport Oxygen Transport Oxygen Dissociation Curve Oxygen Transport Studies Tissue Hypoxia Cyanosis Polycythemia Oxygen Transport Oxygen is carried from the lungs to
Alternatives to RBC Transfusion: Erythropoietin and beyond
 Alternatives to RBC Transfusion: Erythropoietin and beyond David Shimabukuro, MDCM Department of Anesthesia and Perioperative Care Medical Director, 13 ICU UC SF 1 Agenda Physiology of Oxygen Transport
Alternatives to RBC Transfusion: Erythropoietin and beyond David Shimabukuro, MDCM Department of Anesthesia and Perioperative Care Medical Director, 13 ICU UC SF 1 Agenda Physiology of Oxygen Transport
Mechanical Ventilation & Cardiopulmonary Interactions: Clinical Application in Non- Conventional Circulations. Eric M. Graham, MD
 Mechanical Ventilation & Cardiopulmonary Interactions: Clinical Application in Non- Conventional Circulations Eric M. Graham, MD Background Heart & lungs work to meet oxygen demands Imbalance between supply
Mechanical Ventilation & Cardiopulmonary Interactions: Clinical Application in Non- Conventional Circulations Eric M. Graham, MD Background Heart & lungs work to meet oxygen demands Imbalance between supply
Conflicts of Interest
 Anesthesia for Major Abdominal Cancer Resection John E. Ellis MD Adjunct Professor University of Pennsylvania johnellis1700@gmail.com Conflicts of Interest 1 Upper Abdominal Surgery Focus on oncologic
Anesthesia for Major Abdominal Cancer Resection John E. Ellis MD Adjunct Professor University of Pennsylvania johnellis1700@gmail.com Conflicts of Interest 1 Upper Abdominal Surgery Focus on oncologic
Whole body oxygen consumption (VO 2 ) is universally
 is universally") Cardiopulmonary Bypass and Oxygen Consumption: Oxygen Delivery and Hemodynamics Alessandro Parolari, MD, PhD, Francesco Alamanni, MD, Tiziano Gherli, MD, Antonella Bertera, CCP, Luca Dainese, MD, Cristina
Cardiopulmonary Bypass and Oxygen Consumption: Oxygen Delivery and Hemodynamics Alessandro Parolari, MD, PhD, Francesco Alamanni, MD, Tiziano Gherli, MD, Antonella Bertera, CCP, Luca Dainese, MD, Cristina
Transfusions in Acute Care Too Little?
 Transfusions in Acute Care Too Little? Keyvan Karkouti MD FRCPC MSc Associate Professor Department of Anesthesia; Department of Health Policy, Management, and Evaluation; University of Toronto Scientist
Transfusions in Acute Care Too Little? Keyvan Karkouti MD FRCPC MSc Associate Professor Department of Anesthesia; Department of Health Policy, Management, and Evaluation; University of Toronto Scientist
Cardiac surgery and acute kidney injury: retrospective study
 Cardiac surgery and acute kidney injury: retrospective study Department of Cardiovascular and Thoracic Surgery University of Liege Hospital (ULg CHU), Belgium MG LAGNY 1, F BLAFFART 1, JO DEFRAIGNE 2,
Cardiac surgery and acute kidney injury: retrospective study Department of Cardiovascular and Thoracic Surgery University of Liege Hospital (ULg CHU), Belgium MG LAGNY 1, F BLAFFART 1, JO DEFRAIGNE 2,
AllinaHealthSystem 1
 : Definition End-organ hypoperfusion secondary to cardiac failure Venoarterial ECMO: Patient Selection Michael A. Samara, MD FACC Advanced Heart Failure, Cardiac Transplant & Mechanical Circulatory Support
: Definition End-organ hypoperfusion secondary to cardiac failure Venoarterial ECMO: Patient Selection Michael A. Samara, MD FACC Advanced Heart Failure, Cardiac Transplant & Mechanical Circulatory Support
Case year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50
 Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
Case 1 65 year old female nursing home resident with a hx CAD, PUD, recent hip fracture Transferred to ED with decreased mental status BP in ED 80/50 Case 1 65 year old female nursing home resident with
Goal Directed Therapy : Liberal vs Restrictive Transfusion.. Syafri Kamsul Arif
 Goal Directed Therapy : Liberal vs Restrictive Transfusion. Syafri Kamsul Arif Sepsis Perioperative EGDT PGDT PGDT Protocol Stroke volume optimization with fluid protocol SVV or PPV based GDT Protocol
Goal Directed Therapy : Liberal vs Restrictive Transfusion. Syafri Kamsul Arif Sepsis Perioperative EGDT PGDT PGDT Protocol Stroke volume optimization with fluid protocol SVV or PPV based GDT Protocol
UNIVERSITY OF BOLTON SCHOOL OF SPORT AND BIOMEDICAL SCIENCES SPORT PATHWAYS WITH FOUNDATION YEAR SEMESTER TWO EXAMINATIONS 2015/2016
 LH8 UNIVERSITY OF BOLTON SCHOOL OF SPORT AND BIOMEDICAL SCIENCES SPORT PATHWAYS WITH FOUNDATION YEAR SEMESTER TWO EXAMINATIONS 2015/2016 INTRODUCTION TO HUMAN PHYSIOLOGY MODULE NO: SRB3008 Date: Monday
LH8 UNIVERSITY OF BOLTON SCHOOL OF SPORT AND BIOMEDICAL SCIENCES SPORT PATHWAYS WITH FOUNDATION YEAR SEMESTER TWO EXAMINATIONS 2015/2016 INTRODUCTION TO HUMAN PHYSIOLOGY MODULE NO: SRB3008 Date: Monday
Use of Blood Lactate Measurements in the Critical Care Setting
 Use of Blood Lactate Measurements in the Critical Care Setting John G Toffaletti, PhD Director of Blood Gas and Clinical Pediatric Labs Professor of Pathology Duke University Medical Center Chief, VAMC
Use of Blood Lactate Measurements in the Critical Care Setting John G Toffaletti, PhD Director of Blood Gas and Clinical Pediatric Labs Professor of Pathology Duke University Medical Center Chief, VAMC
Introduction to Emergency Medical Care 1
 Introduction to Emergency Medical Care 1 OBJECTIVES 6.1 Define key terms introduced in this chapter. Slides 11, 15, 17, 26, 27, 31, 33, 37, 40 42, 44, 45, 51, 58 6.2 Describe the basic roles and structures
Introduction to Emergency Medical Care 1 OBJECTIVES 6.1 Define key terms introduced in this chapter. Slides 11, 15, 17, 26, 27, 31, 33, 37, 40 42, 44, 45, 51, 58 6.2 Describe the basic roles and structures
MiECC AND THE BRAIN Helena Argiriadou
 MiECC AND THE BRAIN Helena Argiriadou Ass. Professor of Anesthesiology Aristotle University of Thessaloniki, Cardiothoracic Department AHEPA University Hospital Thessaloniki, Greece NEUROLOGIC INJURY AND
MiECC AND THE BRAIN Helena Argiriadou Ass. Professor of Anesthesiology Aristotle University of Thessaloniki, Cardiothoracic Department AHEPA University Hospital Thessaloniki, Greece NEUROLOGIC INJURY AND
Preparing for Patients at High Risk of Transfusion
 18/10/2017 Preparing for Patients at High Risk of Transfusion Jane Ottens. B.Sc., CCP ( Aust) Ashford Hospital, South Australia Preparing for Patients at High Risk of Transfusion Jane Ottens. B.Sc., CCP
18/10/2017 Preparing for Patients at High Risk of Transfusion Jane Ottens. B.Sc., CCP ( Aust) Ashford Hospital, South Australia Preparing for Patients at High Risk of Transfusion Jane Ottens. B.Sc., CCP
TOPIC : Cardiogenic Shock
 University of Ferrara Department of Morphology, Surgery and Experimental Medicine. Section of Anaesthesia and Intensive Care Medicine TOPIC : Cardiogenic Shock What is shock? Shock is a condition of inadequate
University of Ferrara Department of Morphology, Surgery and Experimental Medicine. Section of Anaesthesia and Intensive Care Medicine TOPIC : Cardiogenic Shock What is shock? Shock is a condition of inadequate
Interpretation of Arterial Blood Gases. Prof. Dr. W. Vincken Head Respiratory Division Academisch Ziekenhuis Vrije Universiteit Brussel (AZ VUB)
") Interpretation of Arterial Blood Gases Prof. Dr. W. Vincken Head Respiratory Division Academisch Ziekenhuis Vrije Universiteit Brussel (AZ VUB) Before interpretation of ABG Make/Take note of Correct puncture
Interpretation of Arterial Blood Gases Prof. Dr. W. Vincken Head Respiratory Division Academisch Ziekenhuis Vrije Universiteit Brussel (AZ VUB) Before interpretation of ABG Make/Take note of Correct puncture
PERANAN LAKTAT PADA PASIEN KRITIS DI ICU. Prof. Dr. dr. Made Wiryana, SpAn.KIC.KAO
 PERANAN LAKTAT PADA PASIEN KRITIS DI ICU Prof. Dr. dr. Made Wiryana, SpAn.KIC.KAO History of Lactate Karl Scheele, 1780 found in sour milk Joseph Scherer the German physician-chemist after 70 years demonstrate
PERANAN LAKTAT PADA PASIEN KRITIS DI ICU Prof. Dr. dr. Made Wiryana, SpAn.KIC.KAO History of Lactate Karl Scheele, 1780 found in sour milk Joseph Scherer the German physician-chemist after 70 years demonstrate
Sepsis Management Update 2014
 Sepsis Management Update 2014 Laura J. Moore, MD, FACS Associate Professor, Department of Surgery The University of Texas Health Science Center, Houston Medical Director, Shock Trauma ICU Texas Trauma
Sepsis Management Update 2014 Laura J. Moore, MD, FACS Associate Professor, Department of Surgery The University of Texas Health Science Center, Houston Medical Director, Shock Trauma ICU Texas Trauma
Role of PoCT in Goal-Directed Therapy in Critical Care Settings
 Role of PoCT in Goal-Directed Therapy in Critical Care Settings Alessandro Protti Fondazione IRCCS Ca Granda Ospedale Maggiore Policlinico Milan, Italy Sponsored by Instrumentation Laboratory Contents
Role of PoCT in Goal-Directed Therapy in Critical Care Settings Alessandro Protti Fondazione IRCCS Ca Granda Ospedale Maggiore Policlinico Milan, Italy Sponsored by Instrumentation Laboratory Contents
Acid-base management during hypothermic CPB alpha-stat and ph-stat models of blood gas interpretation
 Acid-base management during hypothermic CPB alpha-stat and ph-stat models of blood gas interpretation Michael Kremke Department of Anaesthesiology and Intensive Care Aarhus University Hospital, Denmark
Acid-base management during hypothermic CPB alpha-stat and ph-stat models of blood gas interpretation Michael Kremke Department of Anaesthesiology and Intensive Care Aarhus University Hospital, Denmark
Major Aortic Reconstruction; Cerebral protection and Monitoring
 Major Aortic Reconstruction; Cerebral protection and Monitoring N AT H A E N W E I T Z E L M D A S S O C I AT E P R O F E S S O R O F A N E S T H E S I O LO G Y U N I V E R S I T Y O F C O LO R A D O S
Major Aortic Reconstruction; Cerebral protection and Monitoring N AT H A E N W E I T Z E L M D A S S O C I AT E P R O F E S S O R O F A N E S T H E S I O LO G Y U N I V E R S I T Y O F C O LO R A D O S
University of Groningen. Acute kidney injury after cardiac surgery Loef, Berthus Gerard
 University of Groningen Acute kidney injury after cardiac surgery Loef, Berthus Gerard IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it.
University of Groningen Acute kidney injury after cardiac surgery Loef, Berthus Gerard IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it.
Central venous oxygen saturation and blood lactate levels during cardiopulmonary bypass are associated with outcome after pediatric cardiac surgery
 RESEARCH Open Access Central venous oxygen saturation and blood lactate levels during cardiopulmonary bypass are associated with outcome after pediatric cardiac surgery Marco Ranucci 1*, Giuseppe Isgrò
RESEARCH Open Access Central venous oxygen saturation and blood lactate levels during cardiopulmonary bypass are associated with outcome after pediatric cardiac surgery Marco Ranucci 1*, Giuseppe Isgrò
Introduction. Invasive Hemodynamic Monitoring. Determinants of Cardiovascular Function. Cardiovascular System. Hemodynamic Monitoring
 Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Accepted Manuscript. Avoiding Acute Kidney Injury After Cardiac Operations Searching for the Holy Grail Isn t Easy. Victor A. Ferraris, M.D., Ph.D.
 Accepted Manuscript Avoiding Acute Kidney Injury After Cardiac Operations Searching for the Holy Grail Isn t Easy Victor A. Ferraris, M.D., Ph.D. PII: S0022-5223(18)33205-7 DOI: https://doi.org/10.1016/j.jtcvs.2018.11.078
Accepted Manuscript Avoiding Acute Kidney Injury After Cardiac Operations Searching for the Holy Grail Isn t Easy Victor A. Ferraris, M.D., Ph.D. PII: S0022-5223(18)33205-7 DOI: https://doi.org/10.1016/j.jtcvs.2018.11.078
Gas Exchange in the Tissues
 Gas Exchange in the Tissues As the systemic arterial blood enters capillaries throughout the body, it is separated from the interstitial fluid by only the thin capillary wall, which is highly permeable
Gas Exchange in the Tissues As the systemic arterial blood enters capillaries throughout the body, it is separated from the interstitial fluid by only the thin capillary wall, which is highly permeable