Why Old Blood is Bad. tales from the electronic perfusion record. Molly Marko, BS, BSE, CCP Geisinger Health System Danville, Pennsylvania
|
|
|
- Isaac Johnston
- 5 years ago
- Views:
Transcription


1 Why Old Blood is Bad tales from the electronic perfusion record Molly Marko, BS, BSE, CCP Geisinger Health System Danville, Pennsylvania

2 Disclosure I have no financial relationship with any of the companies whose products or materials are discussed here within.

3 Plan of Attack Why blood has the potential to be good Why old blood can be bad What does the electronic perfusion record tell us? Would washing donor RBC s help?

4 Allogeneic Red Blood Cells

 + (0.")


5 Why Blood Can Be Good Oxygen Carrying Capacity CaO 2 = (1.34 x Hgb x SaO 2 ) + ( x PaO 2 ) 100% Administration of donor RBC s can increase the CaO 2, thereby increasing oxygenation

6 Why Blood Can Be Good 2,3-Diphosphoglycerate (2,3-DPG) Lowers affinity of Hemoglobin molecule for oxygen oxygen released to tissues
 Vasodilator under hypoxic")
7 Why Blood Can Be Good Adenosine Triphosphate (ATP) Intracellular energy source Intracellular signaling molecule RBC s release ATP in response to hypoxia, ph, and mechanical stress Increase production of nitric oxide (NO) Vasodilator under hypoxic conditions


8 Why Blood Can Be Good Red Blood Cell shape Round, elastic, bi-concave discs Large surface area for O 2 diffusion Flexibility allows RBC s to pass through capillaries as narrow as 3mm Rouleaux formation

9 The Storage Lesion (aka Why Old Blood is Bad)


10 Why Old Blood is Bad Loss of 2,3 DPG Decreases quickly in first 2 weeks of storage to almost undetectable levels Increased O 2 affinity Levels appear to recover post-transfusion Up to 72 hours Studies suggest minimal physiological impact


11 Why Old Blood is Bad Decreased Intracellular ATP 40% days Associated with the reduced oxygen-delivery capacity Can induce RBC shape changes Levels recover in-vivo

12 Source: Salzer U, et al. Vesicles generated during storage of red cells are rich in the lipid raft marker stomatin. Transfusion 2008; 48:


13 Why Old Blood is Bad Morphological changes Biconcave discs Echinocytes with protrusions Spheroechinocytes Formation of microvesicles Loss of membrane phospholipids
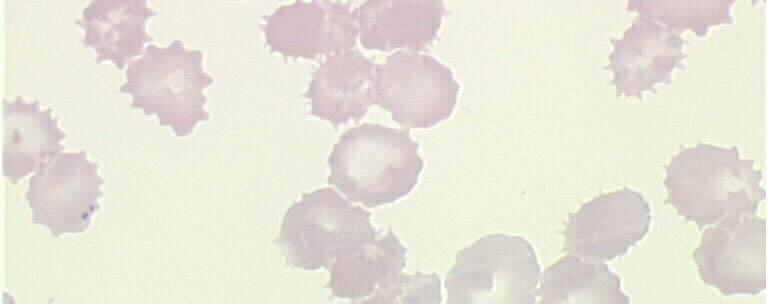
14
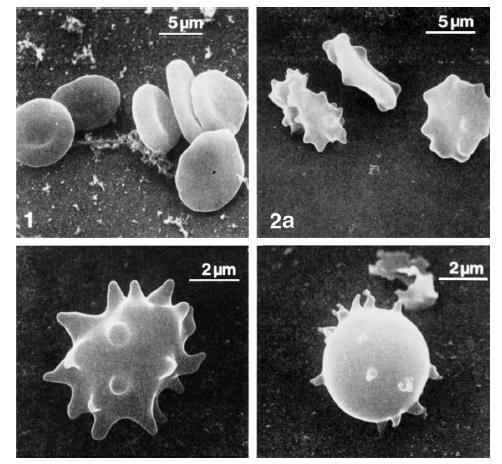
15

16 Why Old Blood is Bad Morphological changes Decreased membrane deformability Increased aggregability Increased adhesion to endothelium Minimizes ability to flow through microcirculation Influences RBC transport of O 2 to tissues Increased osmotic fragility Hemolysis

17 Salzer U, et al


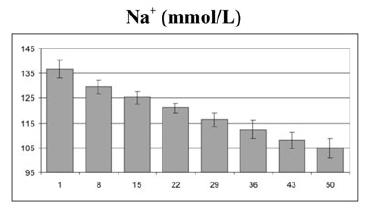
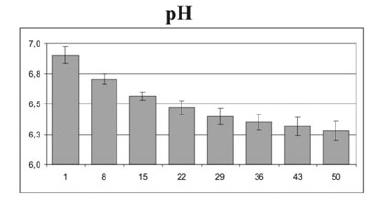
18 Why Old Blood is Bad Other Changes Potassium Sodium ph Lactate Glucose

19 Salzer, et al

20 Salzer U, et al
21 Loss in Membrane Deformability Independent risk factor for MOF 2,3-DPG, ATP & RBC survivability < 80% DAY DAY Steady rise in K + Steady-state K + Alteration in corpuscular shape ( hemolysis) Increased extracellular lactate, K+, pco2 Decreased ph, bicarbonate Deterioration of gastric intramucosal ph

22 The Word on the Street


23 2872 patients who received 8802 units of blood 14 days old 3130 patients who received 10,782 units of blood > 14 days old Blood older than 2 weeks was associated with a significantly increased risk of postoperative complications as well as reduced short-term and long-term survival


24 Four groups based on PRBC age: <10 days days days >19 days Transfusion of RBCs increased cerebral oxygenation except in those transfused with RBCs stored > 19 days.


25 Two groups: blood 5 days old, blood 20 days old Measured gastric ph as index of gastric oxygenation status No change in oxygenation with any transfusion Blood transfusion worthwhile?
26










27 Studies in Cardiac Surgery Patients Author, year Study type RBC Age Vamvakas, 2000 Retrospective Mean d van de Watering, 2006 Retrospective 13 days 24 days Conclusion From the currently available published data, it is difficult to determine whether there is a relationship between the age of transfused RBC s and outcome in adult patients, except possibly in trauma patients receiving massive transfusion. Wasser, 1989 Pro, Randomized < 12 hr vs 2-5d No diff post-op blood loss Vamvakas, 1999 Retrospective 1 41 days Inc risk pneumonia No change in LOS No diff survival or LOS Koch, 2008 Retrospective <14 d, >14 d Inc mortality, LOS Yap, 2008 Retrospective Median 13 days No effect
28 Loss in Membrane Deformability Independent risk factor for MOF 2,3-DPG, ATP & RBC survivability < 80% DAY DAY Steady rise in K + Steady-state K + Alteration in corpuscular shape ( hemolysis) Increased extracellular lactate, K+, pco2 Decreased ph, bicarbonate Deterioration of gastric intramucosal ph

29 Tales from the Electronic Perfusion Record

30

31 SIII INPUT CDI 500 ANESTHESIA MONITOR INVOS

32 Utilization of the EPR Use of the third timer on the Sorin S3 pump allows us to track transfusion time Three time points: Pre-transfusion Transfusion Post-transfusion Data collected every 20 seconds

33 Utilization of the EPR At the end of each case, data is wirelessly exported to a desktop computer That data can then be exported from the DMS program as an Excel file for evaluation

34 Miscellaneous timer started Miscellaneous timer stopped

35 Pre-Transfusion Data Transfusion Data Post-Transfusion Data
 During transfusion (2) Post-transfusion")
36 Data copy and pasted from master Excel file into separate worksheets based on three time points: Pre-transfusion (1) During transfusion (2) Post-transfusion (3)
 But what about the different")
37 We now have information separated by time point (pre-, post-transfusion) But what about the different variables?



38 Data separated into worksheets for 18 different variables Pre-, during, and post-transfusion
 Invos")

39 Variables Cardiac Index MAP Temperature Sweep Rate FiO 2 Hemoglobin Invos (Right) Invos (Left) SVR ph SvO 2 SaO 2 PaCO 2 PaO 2 HCO 3 Oxygen Consumption Oxygen Delivery Oxygen Extraction Ratio
40 Variables Cardiac Index MAP Temperature Sweep Rate FiO 2 Hemoglobin Invos (Right) Invos (Left) SVR ph SvO 2 SaO 2 PaCO 2 PaO 2 HCO 3 Oxygen Consumption Oxygen Delivery Oxygen Extraction Ratio

41 Oxygen Extraction Ratio (O 2 ER) Index of global oxygenation Measure of the fractional tissue uptake of oxygen from the blood at the microcirculation level O 2 ER = VO 2 /DO 2 Normal value 30%

42 Data Analysis Transfusion data separated into 3 groups based on blood age Group 1: 0 15 days old Group 2: days old Group 3: days old Multiple, concurrent transfusions of same age counted as same event Multiple, concurrent transfusions of different ages counted as same event but categorized by oldest unit
43 Percent Oxygen Extraction Ratio Group 1 Group 2 Group :00 0:06 0:13 0:20 0:26 0:03 0:09 0:16 0:23 0:29 Time
44 Percent Oxygen Extraction Ratio Group 1 Group 2 Group :00 0:06 0:13 0:20 0:26 0:03 0:09 0:16 0:23 0:29 Time
45 Percent Oxygen Extraction Ratio Group 1 Group 2 Group :00 0:06 0:13 0:20 0:26 0:03 0:09 0:16 0:23 0:29 Time
46 Percent Oxygen Extraction Ratio Group 1 Group 2 Group :00 0:06 0:13 0:20 0:26 0:03 0:09 0:16 0:23 0:29 Time
47 ml O 2 /min Oxygen Delivery (DO 2 ) Group 1 Group 2 Group 3 0:00 0:06 0:13 0:20 0:26 0:03 0:09 0:16 0:23 0:29 Time DO 2 = Q x [(1.34 x Hgb x SaO 2 )]
48 ml O 2 /min Oxygen Delivery (DO 2 ) Group 1 Group 2 Group 3 0:00 0:06 0:13 0:20 0:26 0:03 0:09 0:16 0:23 0:29 Time DO 2 = Q x [(1.34 x Hgb x SaO 2 )]
49 Cardiac Index L/min/m :00 0:07 0:14 0:22 0:29 0:06 0:13 0:21 0:28 Time Group 1 Group 2 Group 3 DO 2 = Q x [(1.34 x Hgb x SaO 2 )]
50 Cardiac Index L/min/m :00 0:07 0:14 0:22 0:29 0:06 0:13 0:21 0:28 Time Group 1 Group 2 Group 3 DO 2 = Q x [(1.34 x Hgb x SaO 2 )]
51 g/dl Hemoglobin Group 1 Group 2 Group :00 0:06 0:13 0:20 0:26 0:03 0:09 0:16 0:23 0:29 Time DO 2 = Q x [(1.34 x Hgb x SaO 2 )]

52 mmhg PaO Group 1 Group 2 Group :00 0:06 0:13 0:20 0:26 0:03 0:09 0:16 0:23 0:29 Time
53 ml/min Oxygen Consumption (VO 2 ) :00 0:06 0:13 0:20 0:26 0:03 0:09 0:16 0:23 0:29 Time Group 1 Group 2 Group 3

54 Percent Venous Oxygen Saturation (SvO 2 ) Group 1 Group 2 Group :00 0:06 0:13 0:20 0:26 0:03 0:09 0:16 0:23 0:29 Time
55 mmhg Mean Arterial Pressure :00 0:06 0:13 0:20 0:26 0:03 0:09 0:16 0:23 0:29 Group 1 Group 2 Group 3 Time

56 Points of Interest Noticeable and consistent differences between the three groups of blood Oxygen extraction least in oldest blood Venous saturation greatest is oldest blood Strongly suggests decreased ability of old blood to release oxygen to microcirculation

57 Limitations Observational study Cannot isolate storage lesion variables to determine cause and effect Limited power of certain variables due to small sample size
58 Somanetics Group 1 Group 2 Group :00 0:06 0:13 0:20 0:26 0:03 0:09 0:16 0:23 0:29 Time

59 Future Direction Continue to collect and analyze data Data analysis to show statistical significance Compute changes in oxygenation variables Correlate data to outcomes Compare washed RBC s to unwashed RBC s Create a multi-institutional data set among other DMS users

60 To Wash or Not To Wash


61 prbcs 3-21 days old Washing prbcs results in very low levels of K+.


62 Free lactate and potassium siginificantly reduced RBC osmotic resistance improved RBC aggregation capacity reduced Deformability and Free Hgb unchanged


63 Mean age of RBC s ~ 15 days Processed RBC s had significantly higher Hct, and lower levels of blood glucose, [K + ], and lactate

64 To Wash or Not To Wash? Research has demonstrated: Decreased potassium load Decreased lactate load Increased hematocrit Within the Geisinger Health System all donor RBC s are washed prior to transfusion in cases utilizing ATX Exception: emergent need for RBC s Negatives to this practice?

65 Take Home Messages After 15 days of storage: 2,3 DPG, ATP, and RBC survivability decreases Clinical significance is inconclusive based on current studies The Electronic Perfusion Record may assist in elucidating these differences The age of donor RBC s has an effect on oxygenation variables
Dr. Puntarica Suwanprathes. Version 2007
 Dr. Puntarica Suwanprathes Version 2007 O 2 and CO 2 transport in blood Oxyhemoglobin dissociation curve O 2 consumption (VO 2 ) CO 2 production (VCO 2 ) O 2 capacity O 2 content: CaO 2 or CvO 2 %saturation
Dr. Puntarica Suwanprathes Version 2007 O 2 and CO 2 transport in blood Oxyhemoglobin dissociation curve O 2 consumption (VO 2 ) CO 2 production (VCO 2 ) O 2 capacity O 2 content: CaO 2 or CvO 2 %saturation
Critical Care Monitoring. Assessing the Adequacy of Tissue Oxygenation. Tissue Oxygenation - Step 1. Tissue Oxygenation
 Critical Care Monitoring 1 Assessing the Adequacy of Tissue oxygenation is the end-product of many complex steps 2 - Step 1 Oxygen must be made available to alveoli 3 1 - Step 2 Oxygen must cross the alveolarcapillary
Critical Care Monitoring 1 Assessing the Adequacy of Tissue oxygenation is the end-product of many complex steps 2 - Step 1 Oxygen must be made available to alveoli 3 1 - Step 2 Oxygen must cross the alveolarcapillary
Mechanical Ventilation. Assessing the Adequacy of Tissue Oxygenation. Tissue Oxygenation - Step 1. Tissue Oxygenation
 1 Mechanical Ventilation Assessing the Adequacy of 2 Tissue oxygenation is the end-product of many complex steps - Step 1 3 Oxygen must be made available to alveoli 1 - Step 2 4 Oxygen must cross the alveolarcapillary
1 Mechanical Ventilation Assessing the Adequacy of 2 Tissue oxygenation is the end-product of many complex steps - Step 1 3 Oxygen must be made available to alveoli 1 - Step 2 4 Oxygen must cross the alveolarcapillary
3. Which of the following would be inconsistent with respiratory alkalosis? A. ph = 7.57 B. PaCO = 30 mm Hg C. ph = 7.63 D.
 Pilbeam: Mechanical Ventilation, 4 th Edition Test Bank Chapter 1: Oxygenation and Acid-Base Evaluation MULTIPLE CHOICE 1. The diffusion of carbon dioxide across the alveolar capillary membrane is. A.
Pilbeam: Mechanical Ventilation, 4 th Edition Test Bank Chapter 1: Oxygenation and Acid-Base Evaluation MULTIPLE CHOICE 1. The diffusion of carbon dioxide across the alveolar capillary membrane is. A.
How to maintain optimal perfusion during Cardiopulmonary By-pass. Herdono Poernomo, MD
 How to maintain optimal perfusion during Cardiopulmonary By-pass Herdono Poernomo, MD Cardiopulmonary By-pass Target Physiologic condition as a healthy person Everything is in Normal Limit How to maintain
How to maintain optimal perfusion during Cardiopulmonary By-pass Herdono Poernomo, MD Cardiopulmonary By-pass Target Physiologic condition as a healthy person Everything is in Normal Limit How to maintain
Conventional vs. Goal Directed Perfusion (GDP) Management: Decision Making & Challenges
 Management: Decision Making & Challenges") Conventional vs. Goal Directed Perfusion (GDP) Management: Decision Making & Challenges GEORGE JUSTISON CCP MANAGER PERFUSION SERVICES UNIVERSITY OF COLORADO HOSPITAL How do you define adequate perfusion?
Conventional vs. Goal Directed Perfusion (GDP) Management: Decision Making & Challenges GEORGE JUSTISON CCP MANAGER PERFUSION SERVICES UNIVERSITY OF COLORADO HOSPITAL How do you define adequate perfusion?
Introduction. Invasive Hemodynamic Monitoring. Determinants of Cardiovascular Function. Cardiovascular System. Hemodynamic Monitoring
 Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Heinz-Hermann Weitkemper, EBCP. 4th Joint Scandinavian Conference in Cardiothoracic Surgery 2012 Vilnius / Lithuania
 Heinz-Hermann Weitkemper, EBCP Everyone who earnestly practices perfusion is acting with the full belief that what they are doing is in the best interest of their patients. Perfusion can never be normal,
Heinz-Hermann Weitkemper, EBCP Everyone who earnestly practices perfusion is acting with the full belief that what they are doing is in the best interest of their patients. Perfusion can never be normal,
Morris A. Blajchman, MD, FRCP(C) Emeritus Professor, McMaster University Hamilton, Ontario, CANADA
 Emeritus Professor, McMaster University Hamilton, Ontario, CANADA") Morris A. Blajchman, MD, FRCP(C) Emeritus Professor, McMaster University Hamilton, Ontario, CANADA RBC TRANSFUSIONS: GENERAL PRINCIPLES RBCs are usually dispensed on a first-in, first-out basis. Storage
Morris A. Blajchman, MD, FRCP(C) Emeritus Professor, McMaster University Hamilton, Ontario, CANADA RBC TRANSFUSIONS: GENERAL PRINCIPLES RBCs are usually dispensed on a first-in, first-out basis. Storage
EVIDENCE BASED RED CELL TRANSFUSION. Rana Samuel, MD DIRECTOR, PATHOLOGY AND LABORATORY MEDICINE VA WNY Health Care System
 EVIDENCE BASED RED CELL TRANSFUSION Rana Samuel, MD DIRECTOR, PATHOLOGY AND LABORATORY MEDICINE VA WNY Health Care System HISTORY Blood transfusion works (ie: red cell transfusion saves lives). based on
EVIDENCE BASED RED CELL TRANSFUSION Rana Samuel, MD DIRECTOR, PATHOLOGY AND LABORATORY MEDICINE VA WNY Health Care System HISTORY Blood transfusion works (ie: red cell transfusion saves lives). based on
Transfusion Limbo How Low Will You Go? Safely. Nina A. Guzzetta, M.D. Children s Healthcare of Atlanta Emory University School of Medicine
 Transfusion Limbo How Low Will You Go? Safely Nina A. Guzzetta, M.D. Children s Healthcare of Atlanta Emory University School of Medicine Objectives Benefits and risks of RBC administration in pediatric
Transfusion Limbo How Low Will You Go? Safely Nina A. Guzzetta, M.D. Children s Healthcare of Atlanta Emory University School of Medicine Objectives Benefits and risks of RBC administration in pediatric
Alternatives to RBC Transfusion: Erythropoietin and beyond
 Alternatives to RBC Transfusion: Erythropoietin and beyond David Shimabukuro, MDCM Department of Anesthesia and Perioperative Care Medical Director, 13 ICU UC SF 1 Agenda Physiology of Oxygen Transport
Alternatives to RBC Transfusion: Erythropoietin and beyond David Shimabukuro, MDCM Department of Anesthesia and Perioperative Care Medical Director, 13 ICU UC SF 1 Agenda Physiology of Oxygen Transport
Goal Directed Perfusion: theory, clinical results, and key rules
 Goal Directed Perfusion: theory, clinical results, and key rules M. Ranucci Director of Clinical Research Dept of Cardiothoracic and Vascular Anesthesia and Intensive Care IRCCS Policlinico S.Donato Ranuuci,
Goal Directed Perfusion: theory, clinical results, and key rules M. Ranucci Director of Clinical Research Dept of Cardiothoracic and Vascular Anesthesia and Intensive Care IRCCS Policlinico S.Donato Ranuuci,
Defining Optimal Perfusion during CPB. Carlo Alberto Tassi Marketing Manager Eurosets Italy
 Defining Optimal Perfusion during CPB Carlo Alberto Tassi Marketing Manager Eurosets Italy It is a device able to monitor in a real time vital parameters and able to provide information regarding the transport
Defining Optimal Perfusion during CPB Carlo Alberto Tassi Marketing Manager Eurosets Italy It is a device able to monitor in a real time vital parameters and able to provide information regarding the transport
What is. InSpectra StO 2?
 What is InSpectra StO 2? www.htibiomeasurement.com What is InSpectra StO 2? Hemoglobin O 2 saturation is measured in three areas: 1) Arterial (SaO 2, SpO 2 ) Assesses how well oxygen is loading onto hemoglobin
What is InSpectra StO 2? www.htibiomeasurement.com What is InSpectra StO 2? Hemoglobin O 2 saturation is measured in three areas: 1) Arterial (SaO 2, SpO 2 ) Assesses how well oxygen is loading onto hemoglobin
Advanced Monitoring of Cardiovascular and Respiratory Systems in Infants Kuwait 2018 Dr. Yasser Elsayed, MD, PhD Director of the Targeted Neonatal
 Advanced Monitoring of Cardiovascular and Respiratory Systems in Infants Kuwait 2018 Dr. Yasser Elsayed, MD, PhD Director of the Targeted Neonatal Echocardiography, Point of Care and Hemodynamics Program
Advanced Monitoring of Cardiovascular and Respiratory Systems in Infants Kuwait 2018 Dr. Yasser Elsayed, MD, PhD Director of the Targeted Neonatal Echocardiography, Point of Care and Hemodynamics Program
OXYGENATION AND ACID- BASE EVALUATION. Chapter 1
 OXYGENATION AND ACID- BASE EVALUATION Chapter 1 MECHANICAL VENTILATION Used when patients are unable to sustain the level of ventilation necessary to maintain the gas exchange functions Artificial support
OXYGENATION AND ACID- BASE EVALUATION Chapter 1 MECHANICAL VENTILATION Used when patients are unable to sustain the level of ventilation necessary to maintain the gas exchange functions Artificial support
Endpoints of Resuscitation for Circulatory Shock: When Enough is Enough?
 Endpoints of Resuscitation for Circulatory Shock: When Enough is Enough? Emanuel P. Rivers, MD, MPH, IOM Vice Chairman and Research Director Departments of Emergency Medicine and Surgery Henry Ford Hospital
Endpoints of Resuscitation for Circulatory Shock: When Enough is Enough? Emanuel P. Rivers, MD, MPH, IOM Vice Chairman and Research Director Departments of Emergency Medicine and Surgery Henry Ford Hospital
Blood Substitutes. Roy Wang Ellen Quach November 2005
 Blood Substitutes Roy Wang Ellen Quach November 2005 Why Do We Need Blood Substitutes? Provides disease-free alternative to transfusions Universal Compatibility Longer shelf-life than allogeneic blood
Blood Substitutes Roy Wang Ellen Quach November 2005 Why Do We Need Blood Substitutes? Provides disease-free alternative to transfusions Universal Compatibility Longer shelf-life than allogeneic blood
7/4/2015. diffuse lung injury resulting in noncardiogenic pulmonary edema due to increase in capillary permeability
 Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
No Disclosures. Objectives. Objectives 10/10/2018
 Algorithmic Quantification of Prime and Perfusate Composition to Regulate Physiological Variables during Cardiopulmonary Bypass in Neonates and Infants Isaac Chinnappan, MS CCP LCP FPP CPBMT Monroe Carell
Algorithmic Quantification of Prime and Perfusate Composition to Regulate Physiological Variables during Cardiopulmonary Bypass in Neonates and Infants Isaac Chinnappan, MS CCP LCP FPP CPBMT Monroe Carell
Presented by: Indah Dwi Pratiwi
 Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
Presented by: Indah Dwi Pratiwi Normal Fluid Requirements Resuscitation Fluids Goals of Resuscitation Maintain normal body temperature In most cases, elevate the feet and legs above the level of the heart
Module G: Oxygen Transport. Oxygen Transport. Dissolved Oxygen. Combined Oxygen. Topics to Cover
 Topics to Cover Module G: Oxygen Transport Oxygen Transport Oxygen Dissociation Curve Oxygen Transport Studies Tissue Hypoxia Cyanosis Polycythemia Oxygen Transport Oxygen is carried from the lungs to
Topics to Cover Module G: Oxygen Transport Oxygen Transport Oxygen Dissociation Curve Oxygen Transport Studies Tissue Hypoxia Cyanosis Polycythemia Oxygen Transport Oxygen is carried from the lungs to
UTILITY of ScvO 2 and LACTATE
 UTILITY of ScvO 2 and LACTATE Professor Jeffrey Lipman Department of Intensive Care Medicine Royal Brisbane Hospital University of Queensland THIS TRIP SPONSORED AND PAID FOR BY STRUCTURE Physiology -
UTILITY of ScvO 2 and LACTATE Professor Jeffrey Lipman Department of Intensive Care Medicine Royal Brisbane Hospital University of Queensland THIS TRIP SPONSORED AND PAID FOR BY STRUCTURE Physiology -
DEFINING OPTIMAL PERFUSION DURING CPB and MONITORING ECMO
 DEFINING OPTIMAL PERFUSION DURING CPB and MONITORING ECMO CPB OPTIMIZATION & ECMO MONITORING Sweep Gas Flow Oxygen Delivery Oxygen Delivery Index Oxygen Consumption Oxygen Consumption Index Oxygen Extraction
DEFINING OPTIMAL PERFUSION DURING CPB and MONITORING ECMO CPB OPTIMIZATION & ECMO MONITORING Sweep Gas Flow Oxygen Delivery Oxygen Delivery Index Oxygen Consumption Oxygen Consumption Index Oxygen Extraction
Case scenario V AV ECMO. Dr Pranay Oza
 Case scenario V AV ECMO Dr Pranay Oza Case Summary 53 y/m, k/c/o MVP with myxomatous mitral valve with severe Mitral regurgitation underwent Mitral valve replacement with mini thoracotomy Pump time nearly
Case scenario V AV ECMO Dr Pranay Oza Case Summary 53 y/m, k/c/o MVP with myxomatous mitral valve with severe Mitral regurgitation underwent Mitral valve replacement with mini thoracotomy Pump time nearly
Gas Exchange in the Tissues
 Gas Exchange in the Tissues As the systemic arterial blood enters capillaries throughout the body, it is separated from the interstitial fluid by only the thin capillary wall, which is highly permeable
Gas Exchange in the Tissues As the systemic arterial blood enters capillaries throughout the body, it is separated from the interstitial fluid by only the thin capillary wall, which is highly permeable
There are number of parameters which are measured: ph Oxygen (O 2 ) Carbon Dioxide (CO 2 ) Bicarbonate (HCO 3 -) AaDO 2 O 2 Content O 2 Saturation
 Carbon Dioxide (CO 2 ) Bicarbonate (HCO 3 -) AaDO 2 O 2 Content O 2 Saturation") Arterial Blood Gases (ABG) A blood gas is exactly that...it measures the dissolved gases in your bloodstream. This provides one of the best measurements of what is known as the acid-base balance. The body
Arterial Blood Gases (ABG) A blood gas is exactly that...it measures the dissolved gases in your bloodstream. This provides one of the best measurements of what is known as the acid-base balance. The body
Factors influencing the individual effects of blood transfusions on oxygen delivery and oxygen consumption*
 Factors influencing the individual effects of blood transfusions on oxygen delivery and oxygen consumption* Mattias Casutt, MD; Burkhardt Seifert, PhD; Thomas Pasch, MD; Edith R. Schmid, MD; Marko I. Turina,
Factors influencing the individual effects of blood transfusions on oxygen delivery and oxygen consumption* Mattias Casutt, MD; Burkhardt Seifert, PhD; Thomas Pasch, MD; Edith R. Schmid, MD; Marko I. Turina,
Red blood cell transfusions Risks, benefits, and surprises
 SIOP PODC Supportive Care Education Presentation Date: 19 th January 2016 www.cure4kids.org Red blood cell transfusions Risks, benefits, and surprises Scott Howard, MD, MSc Professor, Universidad de Memphis,
SIOP PODC Supportive Care Education Presentation Date: 19 th January 2016 www.cure4kids.org Red blood cell transfusions Risks, benefits, and surprises Scott Howard, MD, MSc Professor, Universidad de Memphis,
Dietary fish oil protects skeletal muscle from hypoxic stress during a bout of contractile fatigue in the rat in vivo hindlimb
 Identifying the primary site(s) of skeletal muscle fatigue Dietary fish oil protects skeletal muscle from hypoxic stress during a bout of contractile fatigue in the rat in vivo hindlimb an inability to
Identifying the primary site(s) of skeletal muscle fatigue Dietary fish oil protects skeletal muscle from hypoxic stress during a bout of contractile fatigue in the rat in vivo hindlimb an inability to
Blood transfusions in sepsis, the elderly and patients with TBI
 Blood transfusions in sepsis, the elderly and patients with TBI Shabbir Alekar MICU, CH Baragwanath Academic Hospital & The University of the Witwatersrand CCSSA Congress 11 June 2015 Packed RBC - complications
Blood transfusions in sepsis, the elderly and patients with TBI Shabbir Alekar MICU, CH Baragwanath Academic Hospital & The University of the Witwatersrand CCSSA Congress 11 June 2015 Packed RBC - complications
DO 2 > VO 2. The amount of oxygen delivered is a product of cardiac output (L/min) and the amount of oxygen in the arterial blood (ml/dl).
 and the amount of oxygen in the arterial blood (ml/dl).") Shock (Part 1): Review and Diagnostic Approach Jeffrey M. Todd, DVM, DACVECC University of Minnesota, St. Paul, MN Overview Shock is the clinical presentation of inadequate oxygen utilization, typically
Shock (Part 1): Review and Diagnostic Approach Jeffrey M. Todd, DVM, DACVECC University of Minnesota, St. Paul, MN Overview Shock is the clinical presentation of inadequate oxygen utilization, typically
Carbon Dioxide Transport. Carbon Dioxide. Carbon Dioxide Transport. Carbon Dioxide Transport - Plasma. Hydrolysis of Water
 Module H: Carbon Dioxide Transport Beachey Ch 9 & 10 Egan pp. 244-246, 281-284 Carbon Dioxide Transport At the end of today s session you will be able to : Describe the relationship free hydrogen ions
Module H: Carbon Dioxide Transport Beachey Ch 9 & 10 Egan pp. 244-246, 281-284 Carbon Dioxide Transport At the end of today s session you will be able to : Describe the relationship free hydrogen ions
Arterial Blood Gases. Dr Mark Young Mater Health Services
 Arterial Blood Gases Dr Mark Young Mater Health Services Why do them? Quick results Bedside test Range of important information Oxygenation Effectiveness of gas exchange Control of ventilation Acid base
Arterial Blood Gases Dr Mark Young Mater Health Services Why do them? Quick results Bedside test Range of important information Oxygenation Effectiveness of gas exchange Control of ventilation Acid base
Lec.2 Medical Physiology Blood Physiology Z.H.Kamil
 Destruction of Red Blood Cells When red blood cells are delivered from the bone marrow into the circulatory system, they normally circulate an average of 120 days before being destroyed. Even though mature
Destruction of Red Blood Cells When red blood cells are delivered from the bone marrow into the circulatory system, they normally circulate an average of 120 days before being destroyed. Even though mature
Early Goal-Directed Therapy
 Early Goal-Directed Therapy Where do we stand? Jean-Daniel Chiche, MD PhD MICU & Dept of Host-Pathogen Interaction Hôpital Cochin & Institut Cochin, Paris-F Resuscitation targets in septic shock 1 The
Early Goal-Directed Therapy Where do we stand? Jean-Daniel Chiche, MD PhD MICU & Dept of Host-Pathogen Interaction Hôpital Cochin & Institut Cochin, Paris-F Resuscitation targets in septic shock 1 The
CCAS CPB Workshop Curriculum Outline Perfusion: What you might not know
 CCAS CPB Workshop Curriculum Outline Perfusion: What you might not know Scott Lawson, CCP Carrie Striker, CCP Disclosure: Nothing to disclose Objectives: * Demonstrate how the cardiopulmonary bypass machine
CCAS CPB Workshop Curriculum Outline Perfusion: What you might not know Scott Lawson, CCP Carrie Striker, CCP Disclosure: Nothing to disclose Objectives: * Demonstrate how the cardiopulmonary bypass machine
Introduction and Overview of Acute Respiratory Failure
 Introduction and Overview of Acute Respiratory Failure Definition: Acute Respiratory Failure Failure to oxygenate Inadequate PaO 2 to saturate hemoglobin PaO 2 of 60 mm Hg ~ SaO 2 of 90% PaO 2 of 50 mm
Introduction and Overview of Acute Respiratory Failure Definition: Acute Respiratory Failure Failure to oxygenate Inadequate PaO 2 to saturate hemoglobin PaO 2 of 60 mm Hg ~ SaO 2 of 90% PaO 2 of 50 mm
a non-trivial challenge for a perfusionist
 DO 2 -guided nephroprotective perfusion - a non-trivial challenge for a perfusionist Dirk Buchwald, Krzysztof Klak xygenium oxygen - Colorless and odorless gas - Most common chemical element on earth atomic
DO 2 -guided nephroprotective perfusion - a non-trivial challenge for a perfusionist Dirk Buchwald, Krzysztof Klak xygenium oxygen - Colorless and odorless gas - Most common chemical element on earth atomic
with their viability and resistance to hemolysis ,19
 A n n a l s o f C l i n i c a l L a b o r a t o r y S c i e n c e, V o l. 1, N o. 2 C o p y r i g h t 1 9 7 1, I n s t i t u t e f o r C l i n i c a l S c i e n c e In Vitro Parameters of the Integrity
A n n a l s o f C l i n i c a l L a b o r a t o r y S c i e n c e, V o l. 1, N o. 2 C o p y r i g h t 1 9 7 1, I n s t i t u t e f o r C l i n i c a l S c i e n c e In Vitro Parameters of the Integrity
BASIC CRITICAL CARE OF THE PATIENT. Hannelisa Callisen PA C February 2017
 BASIC CRITICAL CARE OF THE PATIENT Hannelisa Callisen PA C February 2017 Disclosures Industry: None ECMO is off label Objectives ECMO initiation selection, cannulation Physiology : Review of DO2 on ECMO
BASIC CRITICAL CARE OF THE PATIENT Hannelisa Callisen PA C February 2017 Disclosures Industry: None ECMO is off label Objectives ECMO initiation selection, cannulation Physiology : Review of DO2 on ECMO
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT
 PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
PHYSIOLOGY AND MANAGEMENT OF THE SEPTIC PATIENT Melanie Sanchez, RN, MSNE, OCN, CCRN Clinical Nurse III City of Hope National Medical Center HOW THE EXPERTS TREAT HEMATOLOGIC MALIGNANCIES LAS VEGAS, NV
Goal Directed Therapy : Liberal vs Restrictive Transfusion.. Syafri Kamsul Arif
 Goal Directed Therapy : Liberal vs Restrictive Transfusion. Syafri Kamsul Arif Sepsis Perioperative EGDT PGDT PGDT Protocol Stroke volume optimization with fluid protocol SVV or PPV based GDT Protocol
Goal Directed Therapy : Liberal vs Restrictive Transfusion. Syafri Kamsul Arif Sepsis Perioperative EGDT PGDT PGDT Protocol Stroke volume optimization with fluid protocol SVV or PPV based GDT Protocol
(Peripheral) Temperature and microcirculation
 Temperature and microcirculation") (Peripheral) Temperature and microcirculation Prof. Jan Bakker MD, PhD Chair dept Intensive Care Adults jan.bakker@erasmusmc.nl www.intensivecare.me Intensive Care Med (2005) 31:1316 1326 DOI 10.1007/s00134-005-2790-2
(Peripheral) Temperature and microcirculation Prof. Jan Bakker MD, PhD Chair dept Intensive Care Adults jan.bakker@erasmusmc.nl www.intensivecare.me Intensive Care Med (2005) 31:1316 1326 DOI 10.1007/s00134-005-2790-2
EVALUATION OF CONTEMPORARY OXYGENATOR PERFORMANCE
 EVALUATION OF CONTEMPORARY OXYGENATOR PERFORMANCE ROGER STANZEL CPC, PHD, ADJUNCT PROFESSOR OF MEDICINE, DALHOUSIE UNIVERSITY MARK HENDERSON CPC, CCP BILL O REILLY CPC, CCP AGENDA BACKGROUND/GOALS BENCH-TOP
EVALUATION OF CONTEMPORARY OXYGENATOR PERFORMANCE ROGER STANZEL CPC, PHD, ADJUNCT PROFESSOR OF MEDICINE, DALHOUSIE UNIVERSITY MARK HENDERSON CPC, CCP BILL O REILLY CPC, CCP AGENDA BACKGROUND/GOALS BENCH-TOP
Content Display. - Introduction to Unit 4. Unit 4 - Cardiorespiratory Response to Exercise : Lesson 1. KINE xxxx Exercise Physiology
 Content Display Unit 4 - Cardiorespiratory Response to Exercise : Lesson KINE xxxx Exercise Physiology 5 Unit 4 - Cardiorespiratory Response to Exercise Lesson U4LP - Introduction to Unit 4 The specific
Content Display Unit 4 - Cardiorespiratory Response to Exercise : Lesson KINE xxxx Exercise Physiology 5 Unit 4 - Cardiorespiratory Response to Exercise Lesson U4LP - Introduction to Unit 4 The specific
Lecture 10. Circulatory systems; flow dynamics, flow regulation in response to environmental and internal conditions.
 Lecture 10 Circulatory systems; flow dynamics, flow regulation in response to environmental and internal conditions Professor Simchon Influence of P O2 on Hemoglobin Saturation Hemoglobin saturation plotted
Lecture 10 Circulatory systems; flow dynamics, flow regulation in response to environmental and internal conditions Professor Simchon Influence of P O2 on Hemoglobin Saturation Hemoglobin saturation plotted
Is Timing Everything?
 The Journal of ExtraCorporeal Technology Is Timing Everything? George Justison, CCP University of Colorado Hospital, Perfusion Services, Aurora, Colorado Presented at Goal Directed Therapy Symposium, 54th
The Journal of ExtraCorporeal Technology Is Timing Everything? George Justison, CCP University of Colorado Hospital, Perfusion Services, Aurora, Colorado Presented at Goal Directed Therapy Symposium, 54th
Thinking outside of the box Perfusion management and myocardial protection strategy for a patient with sickle cell disease
 Thinking outside of the box Perfusion management and myocardial protection strategy for a patient with sickle cell disease Shane Buel MS, RRT 1 Nicole Michaud MS CCP PBMT 1 Rashid Ahmad MD 2 1 Vanderbilt
Thinking outside of the box Perfusion management and myocardial protection strategy for a patient with sickle cell disease Shane Buel MS, RRT 1 Nicole Michaud MS CCP PBMT 1 Rashid Ahmad MD 2 1 Vanderbilt
Physiological Causes of Abnormal ABG s
 Physiological Causes of Abnormal ABG s Major Student Performance Objective 1 1. The student will be able to discuss causes for various types of blood gas results. 2. They will also be required to discuss
Physiological Causes of Abnormal ABG s Major Student Performance Objective 1 1. The student will be able to discuss causes for various types of blood gas results. 2. They will also be required to discuss
Maternal and Fetal Physiology
 Background Maternal and Fetal Physiology Anderson Lo, DO Fellow, Maternal-Fetal Medicine Wayne State University School of Medicine SEMCME Fetal Assessment Course July 20, 2018 Oxygen pathway Mother Placenta
Background Maternal and Fetal Physiology Anderson Lo, DO Fellow, Maternal-Fetal Medicine Wayne State University School of Medicine SEMCME Fetal Assessment Course July 20, 2018 Oxygen pathway Mother Placenta
Evidence-Based. Management of Severe Sepsis. What is the BP Target?
 Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
1. I can explain the structure of ATP and how it is used to store energy.
 1. I can explain the structure of ATP and how it is used to store energy. ATP is the primary energy molecule for the cell. It is produced in the mitochondria during cellular respiration, which breaks down
1. I can explain the structure of ATP and how it is used to store energy. ATP is the primary energy molecule for the cell. It is produced in the mitochondria during cellular respiration, which breaks down
Going on Bypass. What happens before, during and after CPB. Perfusion Dept. Royal Children s Hospital Melbourne, Australia
 Going on Bypass What happens before, during and after CPB. Perfusion Dept. Royal Children s Hospital Melbourne, Australia Circulation Brain Liver Kidneys Viscera Muscle Skin IVC, SVC Pump Lungs R.A. L.V.
Going on Bypass What happens before, during and after CPB. Perfusion Dept. Royal Children s Hospital Melbourne, Australia Circulation Brain Liver Kidneys Viscera Muscle Skin IVC, SVC Pump Lungs R.A. L.V.
Factors affecting oxygen dissociation curve
 P a g e 1 Factors affecting oxygen dissociation curve As you know, hemoglobin contains 4 heme molecules that bind 4 oxygen molecules (8 atoms). These 4 heme molecules, however, do not bind oxygen all at
P a g e 1 Factors affecting oxygen dissociation curve As you know, hemoglobin contains 4 heme molecules that bind 4 oxygen molecules (8 atoms). These 4 heme molecules, however, do not bind oxygen all at
Goal-directed vs Flow-guidedresponsive
 Goal-directed vs Flow-guidedresponsive therapy S Magder Department of Critical Care, McGill University Health Centre Flow-directed vs goal directed strategy for management of hemodynamics S Magder Curr
Goal-directed vs Flow-guidedresponsive therapy S Magder Department of Critical Care, McGill University Health Centre Flow-directed vs goal directed strategy for management of hemodynamics S Magder Curr
FIGURE A. The phosphate end of the molecule is polar (charged) and hydrophilic (attracted to water).
 and hydrophilic (attracted to water).") PLASMA MEMBRANE 1. The plasma membrane is the outermost part of a cell. 2. The main component of the plasma membrane is phospholipids. FIGURE 2.18 A. The phosphate end of the molecule is polar (charged)
PLASMA MEMBRANE 1. The plasma membrane is the outermost part of a cell. 2. The main component of the plasma membrane is phospholipids. FIGURE 2.18 A. The phosphate end of the molecule is polar (charged)
Mechanical Ventilation & Cardiopulmonary Interactions: Clinical Application in Non- Conventional Circulations. Eric M. Graham, MD
 Mechanical Ventilation & Cardiopulmonary Interactions: Clinical Application in Non- Conventional Circulations Eric M. Graham, MD Background Heart & lungs work to meet oxygen demands Imbalance between supply
Mechanical Ventilation & Cardiopulmonary Interactions: Clinical Application in Non- Conventional Circulations Eric M. Graham, MD Background Heart & lungs work to meet oxygen demands Imbalance between supply
Transfusion Pitfalls. Objectives. Packed Red Blood Cells. TRICC trial (subgroups): Is transfusion always good? Components
: Is transfusion always good? Components") Objectives Transfusion Pitfalls Gregory W. Hendey, MD, FACEP Professor and Chief UCSF Fresno, Emergency Medicine To list risks and benefits of various blood products To discuss controversy over liberal
Objectives Transfusion Pitfalls Gregory W. Hendey, MD, FACEP Professor and Chief UCSF Fresno, Emergency Medicine To list risks and benefits of various blood products To discuss controversy over liberal
Alternatives to RBC Transfusion:
 Alternatives to RBC Transfusion: beyond Erythropoietin and David Shimabukuro, MDCM Department of Anesthesia and Perioperative Care Medical Director, 13 ICU UC SF 1 Agenda Background Erythropoietin Hemoglobin-based
Alternatives to RBC Transfusion: beyond Erythropoietin and David Shimabukuro, MDCM Department of Anesthesia and Perioperative Care Medical Director, 13 ICU UC SF 1 Agenda Background Erythropoietin Hemoglobin-based
Effects of Increasing FiO 2 on Venous Saturation During Cardiopulmonary Bypass in the Swine Model
 The Journal of The American Society of Extra-Corporeal Technology Effects of Increasing FiO 2 on Venous Saturation During Cardiopulmonary Bypass in the Swine Model Jeffery D. Nichols, MPS, CCP; Alfred
The Journal of The American Society of Extra-Corporeal Technology Effects of Increasing FiO 2 on Venous Saturation During Cardiopulmonary Bypass in the Swine Model Jeffery D. Nichols, MPS, CCP; Alfred
Conflicts of Interest
 Anesthesia for Major Abdominal Cancer Resection John E. Ellis MD Adjunct Professor University of Pennsylvania johnellis1700@gmail.com Conflicts of Interest 1 Upper Abdominal Surgery Focus on oncologic
Anesthesia for Major Abdominal Cancer Resection John E. Ellis MD Adjunct Professor University of Pennsylvania johnellis1700@gmail.com Conflicts of Interest 1 Upper Abdominal Surgery Focus on oncologic
SEPSIS: Seeing Through the. W. Graham Carlos MD, MSCR, ATSF, FACP
 SEPSIS: Seeing Through the W. Graham Carlos MD, MSCR, ATSF, FACP Objectives Forget everything you have known about sepsis Learn new things Objectives Define sepsis Explain why Early Goal Directed Therapy
SEPSIS: Seeing Through the W. Graham Carlos MD, MSCR, ATSF, FACP Objectives Forget everything you have known about sepsis Learn new things Objectives Define sepsis Explain why Early Goal Directed Therapy
Are Patients Hypoperfused in the ED? Rapid Perfusion Assessment in the Emergency Department
 Are Patients Hypoperfused in the ED? Rapid Perfusion Assessment in the Emergency Department R. Benjamin Saldaña DO, FACEP Associate Medical Director Methodist Emergency Care Center, Houston TX Disclosure
Are Patients Hypoperfused in the ED? Rapid Perfusion Assessment in the Emergency Department R. Benjamin Saldaña DO, FACEP Associate Medical Director Methodist Emergency Care Center, Houston TX Disclosure
Chronic Obstructive Pulmonary Disease
 136 PHYSIOLOGY CASES AND PROBLEMS Case 24 Chronic Obstructive Pulmonary Disease Bernice Betweiler is a 73-year-old retired seamstress who has never been married. She worked in the alterations department
136 PHYSIOLOGY CASES AND PROBLEMS Case 24 Chronic Obstructive Pulmonary Disease Bernice Betweiler is a 73-year-old retired seamstress who has never been married. She worked in the alterations department
Chapter 5 Ground Rules of Metabolism Sections 6-10
 Chapter 5 Ground Rules of Metabolism Sections 6-10 5.6 Cofactors in Metabolic Pathways Most enzymes require cofactors Energy in ATP drives many endergonic reactions Table 5-1 p86 Cofactors and Coenzymes
Chapter 5 Ground Rules of Metabolism Sections 6-10 5.6 Cofactors in Metabolic Pathways Most enzymes require cofactors Energy in ATP drives many endergonic reactions Table 5-1 p86 Cofactors and Coenzymes
Exam KEY. NROSCI/BIOSC 1070 and MSNBIO 2070 Exam # 2 October 23, 2015 Total POINTS: % of grade in class
 NROSCI/BIOSC 1070 and MSNBIO 2070 Exam # 2 October 23, 2015 Total POINTS: 100 20% of grade in class 1) Arterial and venous blood samples are taken, and other physiological measures are obtained, from a
NROSCI/BIOSC 1070 and MSNBIO 2070 Exam # 2 October 23, 2015 Total POINTS: 100 20% of grade in class 1) Arterial and venous blood samples are taken, and other physiological measures are obtained, from a
BIOL 2458 CHAPTER 19 Part 1 SI 1. List the types of extracellular fluids. 2. Intracellular fluid makes up of the body fluids. Where is it found?
 BIOL 2458 CHAPTER 19 Part 1 SI 1 1. Extracellular fluid makes up of the body fluids. List the types of extracellular fluids. 2. Intracellular fluid makes up of the body fluids. Where is it found? 3. In
BIOL 2458 CHAPTER 19 Part 1 SI 1 1. Extracellular fluid makes up of the body fluids. List the types of extracellular fluids. 2. Intracellular fluid makes up of the body fluids. Where is it found? 3. In
Chapter 19: The Cardiovascular System: The Blood. Copyright 2009, John Wiley & Sons, Inc.
 Chapter 19: The Cardiovascular System: The Blood Blood Liquid connective tissue 3 general functions 1. Transportation Gases, nutrients, hormones, waste products 2. Regulation ph, body temperature, osmotic
Chapter 19: The Cardiovascular System: The Blood Blood Liquid connective tissue 3 general functions 1. Transportation Gases, nutrients, hormones, waste products 2. Regulation ph, body temperature, osmotic
Acute Changes in Oxyhemoglobin Affinity EFFECTS ON OXYGEN TRANSPORT AND UTILIZATION
 Acute Changes in Oxyhemoglobin Affinity EFFECTS ON OXYGEN TRANSPORT AND UTILIZATION Thomas E. Riggs,, A. William Shafer, Clarence A. Guenter J Clin Invest. 1973;52(10):2660-2663. https://doi.org/10.1172/jci107459.
Acute Changes in Oxyhemoglobin Affinity EFFECTS ON OXYGEN TRANSPORT AND UTILIZATION Thomas E. Riggs,, A. William Shafer, Clarence A. Guenter J Clin Invest. 1973;52(10):2660-2663. https://doi.org/10.1172/jci107459.
The Hemodynamic Puzzle
 The Hemodynamic Puzzle SVV NIRS O 2 ER Lactate Energy Metabolism (Oxygen Consumption) (Ml/min/m 2 ) Oxygen Debt: To Pay or Not to Pay? Full Recovery Possible Delayed Repayment of O 2 Debt Oxygen Deficit
The Hemodynamic Puzzle SVV NIRS O 2 ER Lactate Energy Metabolism (Oxygen Consumption) (Ml/min/m 2 ) Oxygen Debt: To Pay or Not to Pay? Full Recovery Possible Delayed Repayment of O 2 Debt Oxygen Deficit
Objectives. Epidemiology of Sepsis. Review Guidelines for Resuscitation. Tx: EGDT, timing/choice of abx, activated
 Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
Update on Surviving Sepsis 2008 Objectives Epidemiology of Sepsis Definition of Sepsis and Septic Shock Review Guidelines for Resuscitation Dx: Lactate, t cultures, SVO2 Tx: EGDT, timing/choice of abx,
Objective 2/9/2012. Blood Gas Analysis In The Univentricular Patient: The Need For A Different Perspective. VENOARTERIAL CO2 GRADIENT
 Blood Gas Analysis In The Univentricular Patient: The Need For A Different Perspective. Gary Grist RN CCP Chief Perfusionist The Children s Mercy Hospitals and Clinics Kansas City, Mo. Objective The participant
Blood Gas Analysis In The Univentricular Patient: The Need For A Different Perspective. Gary Grist RN CCP Chief Perfusionist The Children s Mercy Hospitals and Clinics Kansas City, Mo. Objective The participant
NIRS of the brain new diagnostic tool
 NIRS of the brain new diagnostic tool Berndt Urlesberger Professor of Neonatology Head, Division of Neonatology, Department of Pediatrics Medical University Graz, Austria Email: berndt.urlesberger@medunigraz.at
NIRS of the brain new diagnostic tool Berndt Urlesberger Professor of Neonatology Head, Division of Neonatology, Department of Pediatrics Medical University Graz, Austria Email: berndt.urlesberger@medunigraz.at
การอบรมว ทยาศาสตร พ นฐานทางศ ลยศาสตร เร อง นพ.ส ณฐ ต โมราก ล ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร โรงพยาบาลรามาธ บด มหาวทยาลยมหดล
 การอบรมว ทยาศาสตร พ นฐานทางศ ลยศาสตร เร อง นพ.ส ณฐ ต โมราก ล ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร โรงพยาบาลรามาธ บด มหาวทยาลยมหดล Distributive shock Severe sepsis and Septic shock Anaphylactic shock Neurogenic
การอบรมว ทยาศาสตร พ นฐานทางศ ลยศาสตร เร อง นพ.ส ณฐ ต โมราก ล ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร โรงพยาบาลรามาธ บด มหาวทยาลยมหดล Distributive shock Severe sepsis and Septic shock Anaphylactic shock Neurogenic
Advances in Transfusion and Blood Conservation
 Advances in Transfusion and Blood Conservation Arman Kilic, MD Division of Cardiac Surgery, Department of Surgery, Johns Hopkins Hospital, Baltimore, MD No relevant financial relationships to disclose.
Advances in Transfusion and Blood Conservation Arman Kilic, MD Division of Cardiac Surgery, Department of Surgery, Johns Hopkins Hospital, Baltimore, MD No relevant financial relationships to disclose.
A. Incorrect! The left ventricle receives oxygenated blood from the lungs via the left atrium.
 DAT Biology - Problem Drill 10: The Circulatory System Question No. 1 of 10 1. What is the flow of deoxygenated blood through the heart as it returns from the body? Question #01 (A) Vena cava; right ventricle;
DAT Biology - Problem Drill 10: The Circulatory System Question No. 1 of 10 1. What is the flow of deoxygenated blood through the heart as it returns from the body? Question #01 (A) Vena cava; right ventricle;
Chapter 14 Blood Vessels, Blood Flow and Pressure Exam Study Questions
 Chapter 14 Blood Vessels, Blood Flow and Pressure Exam Study Questions 14.1 Physical Law Governing Blood Flow and Blood Pressure 1. How do you calculate flow rate? 2. What is the driving force of blood
Chapter 14 Blood Vessels, Blood Flow and Pressure Exam Study Questions 14.1 Physical Law Governing Blood Flow and Blood Pressure 1. How do you calculate flow rate? 2. What is the driving force of blood
CPB pump flow, and effective Flow in patient. 1
 Peter Fast Nielsen ECCP, MCT AUH. Skejby, Denmark. CPB pump flow, and effective Flow in patient. 1 Pump Flow - that s what the Perfusionist controls, right? Well: Does the pump deliver what we expect?
Peter Fast Nielsen ECCP, MCT AUH. Skejby, Denmark. CPB pump flow, and effective Flow in patient. 1 Pump Flow - that s what the Perfusionist controls, right? Well: Does the pump deliver what we expect?
Chapter 9. Body Fluid Compartments. Body Fluid Compartments. Blood Volume. Blood Volume. Viscosity. Circulatory Adaptations to Exercise Part 4
 Body Fluid Compartments Chapter 9 Circulatory Adaptations to Exercise Part 4 Total body fluids (40 L) Intracellular fluid (ICF) 25 L Fluid of each cell (75 trillion) Constituents inside cell vary Extracellular
Body Fluid Compartments Chapter 9 Circulatory Adaptations to Exercise Part 4 Total body fluids (40 L) Intracellular fluid (ICF) 25 L Fluid of each cell (75 trillion) Constituents inside cell vary Extracellular
Energy sources in skeletal muscle
 Energy sources in skeletal muscle Pathway Rate Extent ATP/glucose 1. Direct phosphorylation Extremely fast Very limited - 2. Glycolisis Very fast limited 2-3 3. Oxidative phosphorylation Slow Unlimited
Energy sources in skeletal muscle Pathway Rate Extent ATP/glucose 1. Direct phosphorylation Extremely fast Very limited - 2. Glycolisis Very fast limited 2-3 3. Oxidative phosphorylation Slow Unlimited
Physiological Response to Hypovolemic Shock Dr Khwaja Mohammed Amir MD Assistant Professor(Physiology) Objectives At the end of the session the
 Objectives At the end of the session the") Physiological Response to Hypovolemic Shock Dr Khwaja Mohammed Amir MD Assistant Professor(Physiology) Objectives At the end of the session the students should be able to: List causes of shock including
Physiological Response to Hypovolemic Shock Dr Khwaja Mohammed Amir MD Assistant Professor(Physiology) Objectives At the end of the session the students should be able to: List causes of shock including
Chandra Ramamoorthy MBBS; FRCA (UK) Professor of Anesthesiology, Stanford University. Director of Pediatric Cardiac Anesthesiology
 Professor of Anesthesiology, Stanford University. Director of Pediatric Cardiac Anesthesiology") Should NIRS be Standard Care for Pediatric CPB Chandra Ramamoorthy MBBS; FRCA (UK) Professor of Anesthesiology, Stanford University Director of Pediatric Cardiac Anesthesiology Stanford Children s Hospital
Should NIRS be Standard Care for Pediatric CPB Chandra Ramamoorthy MBBS; FRCA (UK) Professor of Anesthesiology, Stanford University Director of Pediatric Cardiac Anesthesiology Stanford Children s Hospital
Membrane Structure. Membrane Structure. Membranes. Chapter 5
 Membranes Chapter 5 Membrane Structure The fluid mosaic model of membrane structure contends that membranes consist of: -phospholipids arranged in a bilayer -globular proteins inserted in the lipid bilayer
Membranes Chapter 5 Membrane Structure The fluid mosaic model of membrane structure contends that membranes consist of: -phospholipids arranged in a bilayer -globular proteins inserted in the lipid bilayer
Cardiovascular Responses to Exercise
 CARDIOVASCULAR PHYSIOLOGY 69 Case 13 Cardiovascular Responses to Exercise Cassandra Farias is a 34-year-old dietician at an academic medical center. She believes in the importance of a healthy lifestyle
CARDIOVASCULAR PHYSIOLOGY 69 Case 13 Cardiovascular Responses to Exercise Cassandra Farias is a 34-year-old dietician at an academic medical center. She believes in the importance of a healthy lifestyle
RENAL SYSTEM 2 TRANSPORT PROPERTIES OF NEPHRON SEGMENTS Emma Jakoi, Ph.D.
 RENAL SYSTEM 2 TRANSPORT PROPERTIES OF NEPHRON SEGMENTS Emma Jakoi, Ph.D. Learning Objectives 1. Identify the region of the renal tubule in which reabsorption and secretion occur. 2. Describe the cellular
RENAL SYSTEM 2 TRANSPORT PROPERTIES OF NEPHRON SEGMENTS Emma Jakoi, Ph.D. Learning Objectives 1. Identify the region of the renal tubule in which reabsorption and secretion occur. 2. Describe the cellular
Tissue Hypoxia and Oxygen Therapy
 Tissue Hypoxia and Oxygen Therapy ก ก ก ก ก ก 1. ก ก 2. ก ก 3. tissue hypoxia 4. ก ก ก 5. ก ก ก 6. ก กก ก 7. ก ก tissue hypoxia ก ก ก ก 1. Pathway of oxygen transport 2. Causes of tissue hypoxia 3. Effect
Tissue Hypoxia and Oxygen Therapy ก ก ก ก ก ก 1. ก ก 2. ก ก 3. tissue hypoxia 4. ก ก ก 5. ก ก ก 6. ก กก ก 7. ก ก tissue hypoxia ก ก ก ก 1. Pathway of oxygen transport 2. Causes of tissue hypoxia 3. Effect
i. Zone 1 = dead space ii. Zone 2 = ventilation = perfusion (ideal situation) iii. Zone 3 = shunt
 iii. Zone 3 = shunt") Respiratory Review I. Oxygen transport a. Oxygen content of blood i. Dissolved oxygen =.003 x PaO 2, per 100 ml plasma 1. Henry s Law ii. Oxygen on hemoglobin = 1.34 ml x sat x Hgb iii. CaO 2 = Dissolved
Respiratory Review I. Oxygen transport a. Oxygen content of blood i. Dissolved oxygen =.003 x PaO 2, per 100 ml plasma 1. Henry s Law ii. Oxygen on hemoglobin = 1.34 ml x sat x Hgb iii. CaO 2 = Dissolved
Interactions Between Cells and the Extracellular Environment
 Chapter 6 Interactions Between Cells and the Extracellular Environment Et Extracellular lll environment Includes all parts of the body outside of cells Cells receive nourishment Cells release waste Cells
Chapter 6 Interactions Between Cells and the Extracellular Environment Et Extracellular lll environment Includes all parts of the body outside of cells Cells receive nourishment Cells release waste Cells
Oxygen as an ergogenic aid in elite sports. performance at altitude. Juha Peltonen. Why to go to altitude?
 Why to go to altitude? Oxygen as an ergogenic aid in elite sports Olympic Committee, 7.9.2010, Helsinki Juha Peltonen, PhD Senior exercise physiologist Unit for Sports and Exercise Medicine Institute of
Why to go to altitude? Oxygen as an ergogenic aid in elite sports Olympic Committee, 7.9.2010, Helsinki Juha Peltonen, PhD Senior exercise physiologist Unit for Sports and Exercise Medicine Institute of
PBL SEMINAR. HEMOGLOBIN, O 2 -TRANSPORT and CYANOSIS An Overview
 1 University of Papua New Guinea School of Medicine and Health Sciences Division of Basic Medical Sciences Discipline of Biochemistry and Molecular Biology PBL SEMINAR HEMOGLOBIN, O 2 -TRANSPORT and CYANOSIS
1 University of Papua New Guinea School of Medicine and Health Sciences Division of Basic Medical Sciences Discipline of Biochemistry and Molecular Biology PBL SEMINAR HEMOGLOBIN, O 2 -TRANSPORT and CYANOSIS
Acids, Bases, and Salts
 Acid / Base Balance Objectives Define an acid, a base, and the measure of ph. Discuss acid/base balance, the effects of acidosis or alkalosis on the body, and the mechanisms in place to maintain balance
Acid / Base Balance Objectives Define an acid, a base, and the measure of ph. Discuss acid/base balance, the effects of acidosis or alkalosis on the body, and the mechanisms in place to maintain balance
Role of Red Cells in RDCR. Philip C. Spinella, MD, FCCM RDCR Symposium Bergen, Norway 2013
 Role of Red Cells in RDCR Philip C. Spinella, MD, FCCM RDCR Symposium Bergen, Norway 2013 Overview Role of shock in ACT/TIC Methods to reverse shock RBC functions RBC efficacy in reversing shock Storage
Role of Red Cells in RDCR Philip C. Spinella, MD, FCCM RDCR Symposium Bergen, Norway 2013 Overview Role of shock in ACT/TIC Methods to reverse shock RBC functions RBC efficacy in reversing shock Storage
Acid Base Balance by: Susan Mberenga RN, BSN, MSN
 Acid Base Balance by: Susan Mberenga RN, BSN, MSN Acid Base Balance Refers to hydrogen ions as measured by ph Normal range: 7.35-7.45 Acidosis/acidemia: ph is less than 7.35 Alkalosis/alkalemia: ph is
Acid Base Balance by: Susan Mberenga RN, BSN, MSN Acid Base Balance Refers to hydrogen ions as measured by ph Normal range: 7.35-7.45 Acidosis/acidemia: ph is less than 7.35 Alkalosis/alkalemia: ph is
HYPOVOLEMIA AND HEMORRHAGE UPDATE ON VOLUME RESUSCITATION HEMORRHAGE AND HYPOVOLEMIA DISTRIBUTION OF BODY FLUIDS 11/7/2015
 UPDATE ON VOLUME RESUSCITATION HYPOVOLEMIA AND HEMORRHAGE HUMAN CIRCULATORY SYSTEM OPERATES WITH A SMALL VOLUME AND A VERY EFFICIENT VOLUME RESPONSIVE PUMP. HOWEVER THIS PUMP FAILS QUICKLY WITH VOLUME
UPDATE ON VOLUME RESUSCITATION HYPOVOLEMIA AND HEMORRHAGE HUMAN CIRCULATORY SYSTEM OPERATES WITH A SMALL VOLUME AND A VERY EFFICIENT VOLUME RESPONSIVE PUMP. HOWEVER THIS PUMP FAILS QUICKLY WITH VOLUME
Lab 4: Respiratory Physiology and Pathophysiology
 Lab 4: Respiratory Physiology and Pathophysiology This exercise is completed as an in class activity and including the time for the PhysioEx 9.0 demonstration this activity requires ~ 1 hour to complete
Lab 4: Respiratory Physiology and Pathophysiology This exercise is completed as an in class activity and including the time for the PhysioEx 9.0 demonstration this activity requires ~ 1 hour to complete
5. What is the cause of this patient s metabolic acidosis? LACTIC ACIDOSIS SECONDARY TO ANEMIC HYPOXIA (HIGH CO LEVEL)
") Self-Assessment RSPT 2350: Module F - ABG Analysis 1. You are called to the ER to do an ABG on a 40 year old female who is C/O dyspnea but seems confused and disoriented. The ABG on an FiO 2 of.21 show:
Self-Assessment RSPT 2350: Module F - ABG Analysis 1. You are called to the ER to do an ABG on a 40 year old female who is C/O dyspnea but seems confused and disoriented. The ABG on an FiO 2 of.21 show:
ARTERIAL BLOOD GASES PART 1 BACK TO BASICS SSR OLIVIA ELSWORTH SEPT 2017
 ARTERIAL BLOOD GASES PART 1 BACK TO BASICS SSR OLIVIA ELSWORTH SEPT 2017 WHAT INFORMATION DOES AN ABG GIVE US? ph = measure of hydrogen ion concentration (acidity or alkalinity) PaCO2 = partial pressure
ARTERIAL BLOOD GASES PART 1 BACK TO BASICS SSR OLIVIA ELSWORTH SEPT 2017 WHAT INFORMATION DOES AN ABG GIVE US? ph = measure of hydrogen ion concentration (acidity or alkalinity) PaCO2 = partial pressure
Institute of Surgical Research C Module Advance Basic Medical Skills
 Institute of Surgical Research C Module Advance Basic Medical Skills C1-2 MODUL Non-invasive monitoring; Invasive hemodinamic monitoring C3-4 MODUL Laparotomy, enterotomy, Intestinal suture, Diagnostic
Institute of Surgical Research C Module Advance Basic Medical Skills C1-2 MODUL Non-invasive monitoring; Invasive hemodinamic monitoring C3-4 MODUL Laparotomy, enterotomy, Intestinal suture, Diagnostic