Wayne Ruppert and Dr. James Irwin, St Joseph s Hospital, Tampa, FL 2006
|
|
|
- Lorraine Madison Webb
- 5 years ago
- Views:
Transcription




1 The EMS 12 Lead 101 Wayne W Ruppert, CVT, CCCC, NREMT-P Interventional Cardiovascular Technologist Cardiovascular Coordinator Bayfront Health Seven Rivers
2 Welcome!

3

4 Wayne Ruppert and Dr. James Irwin, St Joseph s Hospital, Tampa, FL 2006

5 Cardiac Cath Lab
 Tracing and for Pace-mapping, an integral component")

6 Electrophysiology Lab EP Catheters within the heart used for obtaining the Electrogram (the internal ECG ) Tracing and for Pace-mapping, an integral component of an EP study Author Wayne Ruppert conducting Pacemapping during EP study at the St Joseph s Hospital Heart Institute, Pediatric Electrophysiology Program, Tampa, FL in 2004

7
8 Wayne Ruppert bio: Cardiovascular Coordinator 2012-present (coordinated 5 successful accreditations) Interventional Cardiovascular / Electrophysiology Technologist, 1995-Present. Author of: 12 Lead ECG Interpretation in Acute Coronary Syndrome with Case Studies from the Cardiac Cath Lab, 2010, TriGen publishing / Ingram Books Author of: STEMI Assistant, 2014, TriGen publishing / Ingram Books Florida Nursing CE Provider # Lead ECG Instructor, 1994-present (multiple hospitals, USF College of Medicine 1994) Website:

9 BarnesandNoble.com Amazon.com

10 BarnesandNoble.com Amazon.com
11 STEMI Assistant: an Emergency Crash Cart Interactive Reference Manual - free Download STEMI Assistant Information Video
12 STEMI Assistant Editorial Board: Barbra Backus, MD, PhD Inventor of The HEART Score, University Medical Center, Utrech, Netherlands Michael R. Gunderson, National Director, Clinical and Health IT, American Heart Association Anna Ek, AACC, BSN, RN Accreditation Review Specialist, The American College of Cardiology William Parker, PharmD, CGP, Director of Pharmacy, Bayfront Dade City Printed and Marketed Worldwide by The Ingram Book Company Current
13 Copyright 2010, 2011, 2015, 2019 All cardiovascular subject-related images, graphics and diagrams were created by the author, Wayne Ruppert, and have been taken from his two published textbooks, STEMI Assistant and 12 Lead ECG Interpretation in ACS with Case Studies from the Cardiac Cath Lab, are Copyright protected, and may not be removed from this PowerPoint presentation. This presentation may not be used as part of a profitgenerating program without prior written consent from the author. Wayneruppert@aol.com

14 American College of Cardiology 20 th Congress 2017 Red Rock Resort, Las Vegas October 25 & 26, 2017 Advanced Telemetry & 12 Lead ECG Workshop Part 1 Observation Medicine Tract By: Wayne W Ruppert, CVT, CCCC, NREMT-P
15
16 Download Today s Presentation To go: from the MENU BAR at left side of screen, select Downloads PDF, and then select: EMS 12 Lead 101

17 Go to:
18 Single Lead ECG vs 12 Leads Single lead rhythm strips are obtained to see what rhythm the patient is currently in (e.g.: NSR, atrial fibrillation, heart blocks, etc). 12 Lead ECG is used to see if any part of the heart is not getting adequate blood supply (i.e.: ischemia, infarction). Plus, it aids in the diagnosis of many other conditions...
19 .Other 12 Lead ECG Diagnoses: Bundle Branch Blocks* and Fascicular Blocks Necrosis (old MI, evolving MI*) V-Tach vs SVT with aberrancy Hypertrophy (enlargement of 1 or more chambers) Electrolyte imbalances Sudden Arrhythmia Death Syndromes: Brugada, Long QT*, ARVD, CPVT, HCM, Wolff-Parkinson-White Syndrome Acute Myocarditis / Pericarditis And many more * Covered in this course

20 EMS 12 Lead ECG
21 OBTAINING THE 12 LEAD ECG

22 10 wires... 4 limb leads 6 chest ( V ) leads

23

24

25
26

27

28 Obtaining the 12 Lead ECG
29 Obtaining the 12 Lead ECG Limb leads should be on the limbs.
30 Obtaining the 12 Lead ECG Recent AHA/ACC/HRS literature indicates QRS AMPLITUDE, Q WAVE DURATION, AXIS and WAVEFORM DEFLECTION can be altered when limb leads are placed on the patient's torso (Mason-Likar lead placement). Therefore every effort should be made to place limb leads on the limbs.

31
32
33 Obtaining the 12 Lead ECG Limb leads should be on the limbs. When emergency circumstances dictate that limb leads be placed on patient's torso, the words "LIMB LEADS ON PATIENT'S TORSO" should be noted on the ECG.
34 Obtaining the 12 Lead ECG Limb leads should be on the limbs. When emergency circumstances dictate that limb leads be placed on patient's torso, the words "LIMB LEADS ON PATIENT'S TORSO" should be noted on the ECG. However in the field, it may not be possible or practical to put limb leads on limbs!

35 Limb leads field ECG
36 Remember this... White to the Right Smoke over Fire Green Grass below the White Clouds
37
38

39

40

41
42 Leads V1 & V2 on 12 Lead ECG: Proper lead placement of precordial Leads V1 and V2 are 4th intercostal space on opposite sides of the sternum. Incorrect placement of Leads V1 and V2 will result in: reduction of R wave amplitude (resulting in poor R wave progression) leading to misdiagnosis of previous anterior / septal infarction.

43
44 Obtaining the 12 Lead ECG, etc Patient should lay as flat as possible If you see too much artifact on the ECG, you may have to coach patient to relax all of your muscles... Arms Legs Chest Abdomen, etc.
45 To help you understand what part of the heart each lead of a 12 Lead ECG sees....

46
47

48 What each of the 12 Leads sees, in more detail....
49

50
51
52

53

54

55
56 A 12 Lead ECG sees MOST of the Heart, but it has some BLIND SPOTS!!....
57 THE 12 LEAD ECG HAS TWO MAJOR BLIND SPOTS..
58 Regarding the POSTERIOR WALL, the Standard 12 Lead will give you some good clues that there s a PROBLEM by displaying what we call RECIPROCAL CHANGES.kind of like seeing reflected changes in a mirror
59
60
61

62 ST DEPRESSION can be from any other these conditions:
63 THE 12 LEAD ECG HAS TWO MAJOR BLIND SPOTS..

64 THE 18 LEAD ECG COVERS THE ENTIRE HEART..

65 To do 18 Lead ECG with 12 Lead machine after you obtain 12 Lead, reposition CHEST LEADS to this configuration, then print!

66 RIGHT SIDED ECG is indicated whenever you see INFERIOR WALL STEMI!!
67 POSTERIOR ECG is indicated whenever you see ST DEPRESSION In Leads V1-V4
68 ST Depression in V1 V4....
69 INDICATIONS for 18 Lead ECG include: - INFERIOR WALL MI F Right sided ECG - ST Depression V1-V4 F Posterior ECG
70 Practical application of 18 Lead ECGs is presented in the CASE STUDIES section of this curriculum.
71 Before we go any farther, you should know...
72 Sometimes, ECGs LIE to us!

73 ECGs and USED CAR SALESMEN often have MUCH in common!

74
75 PROBLEMS WITH SENSITIVITY... NORMAL ECG. But..... LETHAL TRIPLE VESSEL DISEASE

76 PROBLEMS WITH SPECIFICITY...

77 PROBLEMS WITH SPECIFICITY...

78

79 Patient: Asymptomatic Troponin normal Cardiac Cath angiography = no obstructive CAD. Discharge diagnosis: EARLY REPOLARIZATION. This degree of ST Elevation in early repolarization is VERY RARE: The only such ECG I have seen in approximately 13,000 cardiac catheterizations.
80 Despite the ECG s problematic issues with Lack of Sensitivity & Lack of Specificity, The 12 Lead ECG remains one of our QUICKEST, most costefficient front-line Triage Tools that we have today.

81 So how do we know when the ECG is telling us the truth???

82
83 In the hospital we utilize ACS Risk Stratification tools such as The HEART Score. We also have Troponins, Echo, CT and Cardiac Cath. In the field, you have far fewer resources!!

84 What do you have in the field? Symptoms Risk Factors ECG Physical Exam

85
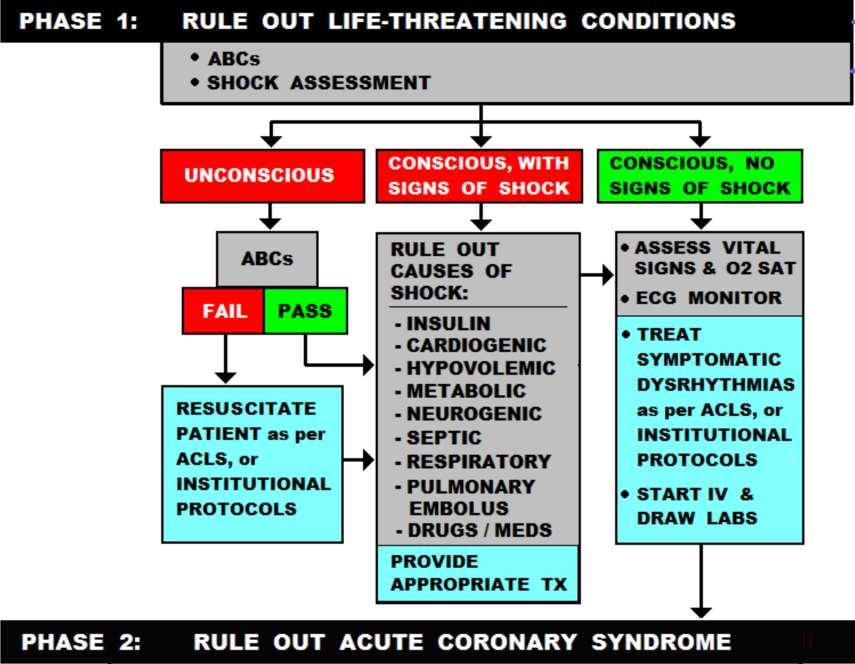
86 You arrive at a patient s residence. The scene is safe, and you re led into the living room by the patient s daughter... The instant you see the patient, you assess for: CAB (pulse, breathing) the patient is awake, to you know he has a pulse and you see him breathing Shock Assessment....

87

88
89 FAIL the SHOCK SURVEY? F RAPIDLY FIND AND TREAT THE ROOT CAUSE... WORK TO RAPIDLY IDENTIFY THE CAUSE OF SHOCK.
90
91
92 CHIEF COMPLAINT KEY WORDS: CHEST: PAIN / HEAVINESS / PRESSURE/ FUNNY FEELING IN, etc. SHORTNESS BREATH DIZZINESS / LIGHTHEADEDNESS ETC. ETC. ETC.
93

94
95 BEWARE of the patient with INTERMITTENT CHEST PAIN.... M
96 ATYPICAL SYMPTOMS of ACS???


97 BOOK PAGE: 70

98


99
100 Physical Exam Clues of MI: Skin may be PALE, CLAMMY SWEATING! (Diaphoresis) Clutching /Rubbing chest BP can be high, normal or low Anxiety / look of impending doom.
101
102 3 or more major RISK FACTORS gets you a checkmark in the RISK FACTOR box!

103
104 Here is the HEART Score! Let s see what the score is for our patient with the NORMAL ECG.who had Critical Triple Vessel Disease and needed STAT Bypass Surgery!...



105 PROBLEMS WITH SENSITIVITY... NORMAL ECG. But..... LETHAL TRIPLE VESSEL DISEASE

106 H = chest pain = 2 E = ECG normal = 0 A = 63 = 1 R = 3 risk factors = 2 T = Trop. NL = 0 HEART Score: = 5
107

108
109 Some Basic Vocabulary: Ischemia = Inadequate blood supply to cells, but cells are still getting blood. Cellular Oxygen Demand is HIGHER than the Oxygen Supply. Infarction = blood supply to cells has been cut off. Cells are no longer receiving oxygen or glucose. Cells survive by consuming available glycogen reserves, convert to ANAEROBIC metabolism. Unless blood supply is restored, cells die when glycogen reserves are depleted.
110 Some Basic Vocabulary: Acute Coronary Syndrome (ACS) is made up of the following cardiac conditions: Unstable Angina Non-ST Segment Elevation Myocardial Infarction (NSTEMI) ST Segment Elevation Myocardial Infarction (STEMI) Low Risk Chest Pain

111 Unstable Angina

112 Non-STEMI (NSTEMI) Non-ST Segment Elevation Myocardial Infarction. sub-endocardial MI... partial wall thickness
113 Non-STEMI (NSTEMI) Non-ST Segment Elevation Myocardial Infarction. sub-endocardial MI... partial wall thickness The 12 Lead ECG may show: - ST Depression - Other ST Segment changes - Inverted T wave - THE ECG MAY BE TOTALLY NORMAL.
114 Non-STEMI (NSTEMI) Non-ST Segment Elevation Myocardial Infarction. sub-endocardial MI... partial wall thickness This is a Partial Wall Thickness MI, heart cells are dying, and the Troponin becomes detectable in the patient s bloodstream. Usually less severe than a STEMI, patient needs blood thinners and to get to the cath lab in hours.

115 STEMI ST Segment Elevation Myocardial Infarction.
116 Non-STEMI (NSTEMI) ST Segment Elevation Myocardial Infarction. ( full-wall thickness, Transmural event) This is a life-threatening emergency. Part of the patient s heart is dying. Blood flow must be restored within 90 minutes or less in order to preserve heart muscle. Based on the region of the heart affected, critical and often lethal complications may rapidly develop.
117 A quick review of some very basic ECG concepts: When you turn on the ECG machine, it defaults to normal values.. Records at 25mm/ second (horizontal axis) Amplitude (vertical axis) is set so 1 mv = 10 small (1mm) boxes.

118

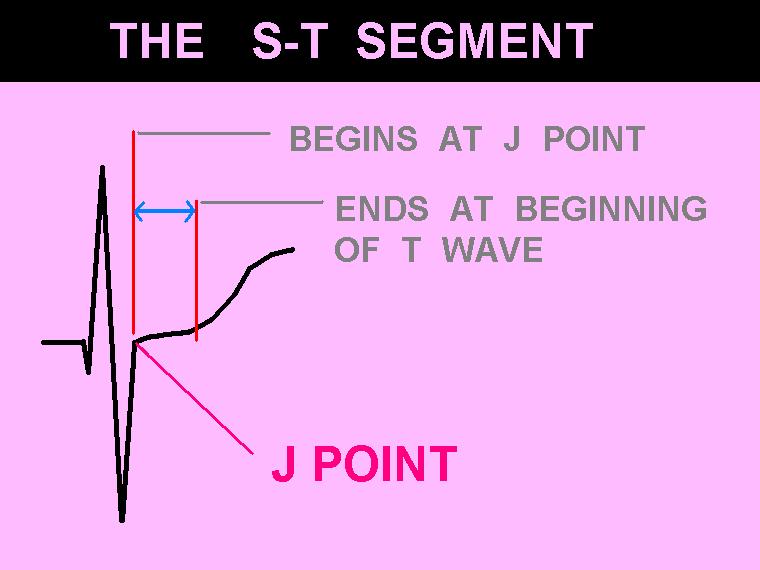
119
120 P WAVE = ATRIAL DEPOLARIZATION QRS COMPLEX = VENTRICULAR DEPOLARIZATION (contracting) T WAVE = VENTRICULAR REPOLARIZATION (recharging)
121 Q: To evaluate the patient for ischemia or infarction, what part of the ECG do we look at?
122 Q: To evaluate the patient for ischemia or infarction, what part of the ECG do we look at? A: We evaluate the J Points ST Segments & T Waves.. in each lead!
123 Evaluating the ECG for ACS:
124 Evaluating the ECG for ACS: Patients with Normal Width QRS (QRSd < 120ms)
125 Q: Why is QRS width an issue when we look at J Points, ST Segments and T Waves??
126 Q: Why is QRS width an issue when we look at J Points, ST Segments and T Waves?? A: When the QRS is abnormally wide (> 120ms), it ALTERS the J Points, ST Segements and T Waves.
127 Defining NORMAL QRS <120ms:

128
129
130

131

132 ...the flat line between ECG complexes, when there is no detectable electrical activity...

133 The Isoelectric Line - it s not always isoelectric!
134
135 Use the P-Q junction as a reference point for measuring the J Point and ST-Segment when iso-electric line is not isoelectric!

136 Defining NORMAL:
137

138
139

140

141
142

143

144 Normal Variants: T Wave Inversion

145
146 The next slide shows an ECG waveform with normal J Points, ST Segments and T waves THINK OF THIS AS YOUR MEASURING STICK of what NORMAL is!!!
")
147 Patients with normal QRS duration ( QRS < 120 ms ) :
148 Q: If the previous slide showed what normal J Points, ST Segments and T waves look like, what is ABNORMAL?
149 Q: If the previous slide showed what normal J Points, ST Segments and T waves look like, what is ABNORMAL? A: EVERYTHING ELSE!!!
150 Up Next: ECG Indicators of ABNORMAL PERFUSION (possible ischemia / infarction) in Patients with Normal Width QRS Complexes (QRS duration < 120 ms)
151
152
153 Some less common, less reliable possible indicators of ACS:
154 LET S START HERE....
155

156

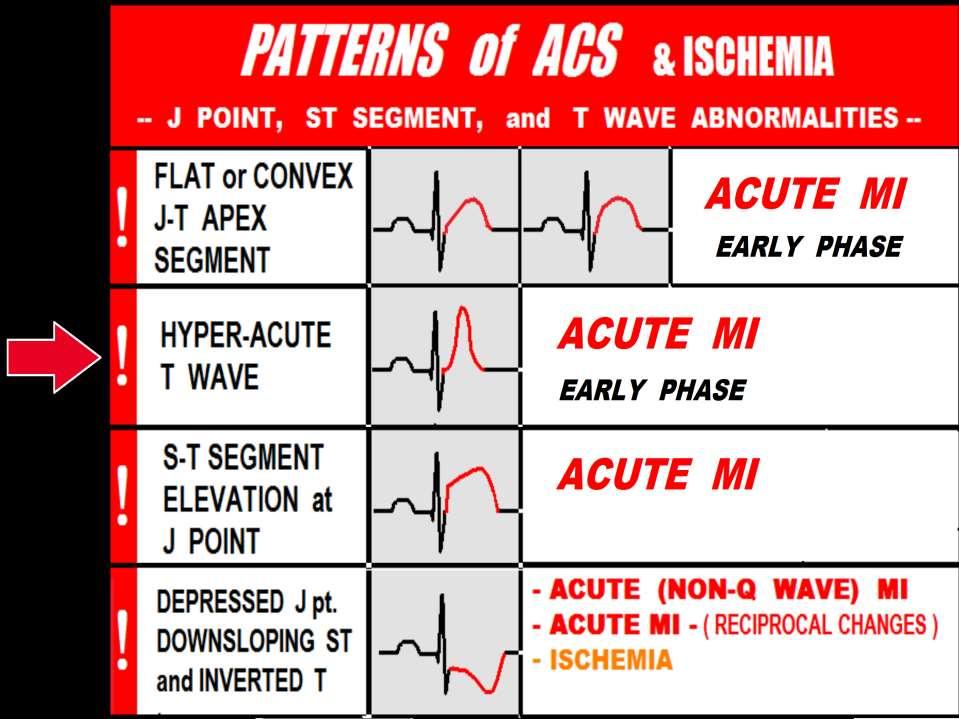
157


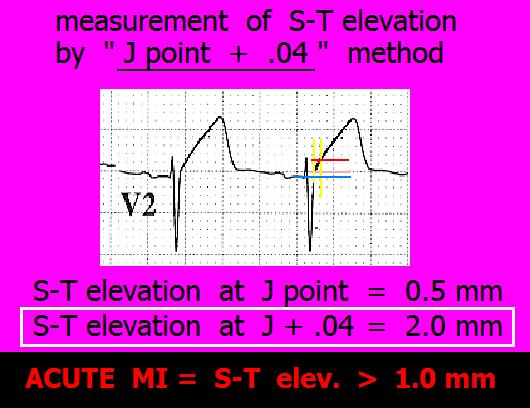
158 WHEN EVALUATING for ST SEGMENT ELEVATION From: AMERICAN HEART ASSOCIATION ACLS 2005 REVISIONS


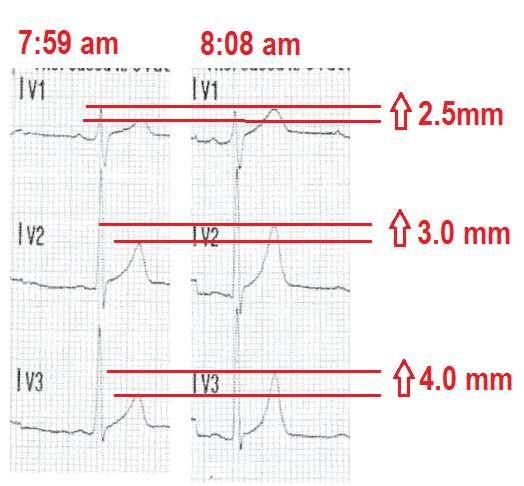
159


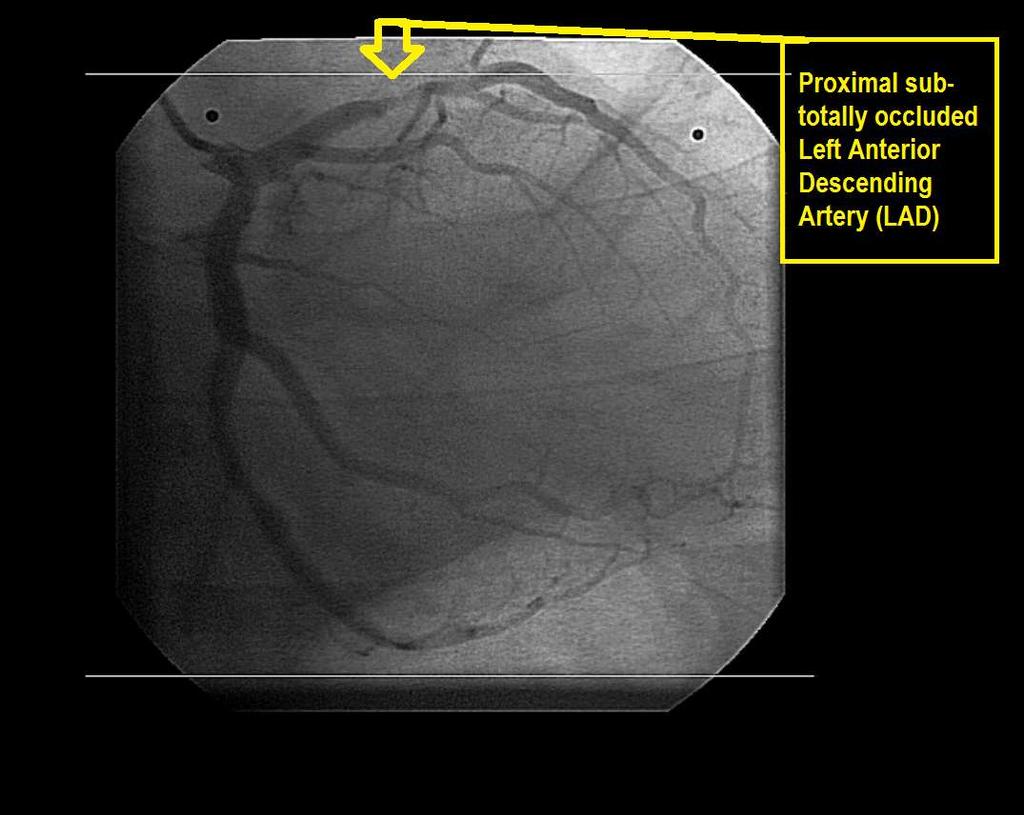
160

161

162 ECG COMPUTER DOES NOT NOTICE THE CONVEX J-T APEX SEGMENTS!
163
164

165
166 ECG Patterns associated with EARLY PHASE MI: J-T Apex abnormalities Dynamic ST-T Wave Changes on Serial ECGs

167




168 3. Dynmamic ST-T Wave Changes in Serial ECGs. Recorded at SRRMC 1 st ECG 2 nd ECG 1 st ECG 2 nd ECG

169 Acute In-Stent Thrombus Proximal LAD
170

171 T waves should not be HYPERACUTE
172 HYPERACUTE T Waves may indicate: Early phase Acute MI Transmural ischemia (usually seen in one region of the ECG) Hyperkalemia (seen globally across ECG) Hypertrophy
 and just after (normal) the")
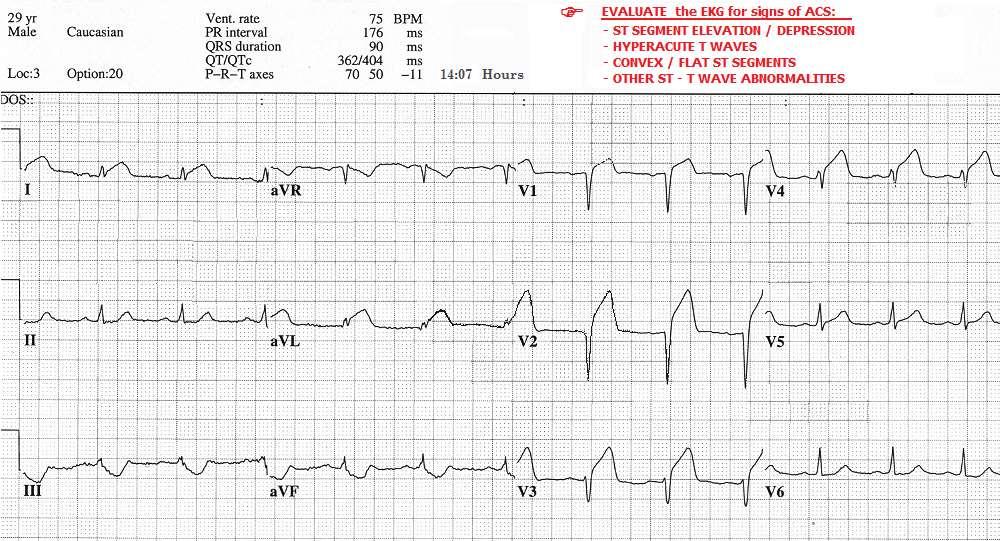
 artery.")
173 HYPERACUTE T WAVES ECG waveforms obtained just before (hyperacute) and just after (normal) the critical blockage was stented in this patient s Proximal Left Anterior Descending (LAD) artery.
174 Helpful Clue: Hyper-Acute T Waves GLOBAL Hyper-acute T Waves (in leads viewing multiple myocardial regions / arterial distributions) favors HYPERKALEMIA

175
176 Helpful Clue: Hyper-Acute T Waves GLOBAL Hyper-acute T Waves (in leads viewing multiple myocardial regions / arterial distributions) favors HYPERKALEMIA Hyper-acute T Wave noted in ONE ARTERIAL DISTRIBUTION ( Anterior / Lateral / Inferior ) favors TRANSMURAL ISCHEMIA / Early Phase Acute MI

177

178

179


180 Cath Lab findings:
181 Dynamic ST-T Wave Changes: Other than HEART RATE related variations (which affect intervals), J Points, ST- Segments and T Waves SHOULD NOT CHANGE.
182 Dynamic ST-T Wave Changes: Other than HEART RATE related variations (which affect intervals), J Points, ST- Segments and T Waves SHOULD NOT CHANGE. When changes to J Points, ST-Segments and/or T waves are NOTED, consider EVOLVING MYOCARDIAL ISCHEMIA and/or EARLY PHASE MI, until proven otherwise.

183 46 year old male Exertional dyspnea X several weeks Intermittent chest pressure X last 3 hours. Currently pain free.

184 46 year old male: ECG 1 Chest pressure has returned, 5 on 1-10 scale. 2 nd ECG obtained due to change in symptoms :

185
186


187 ST-Segment Depression 7:59 am 8:08 am
188 Cath Lab Angiography:

189 NOWHERE, NEW MEXICO, 1994
190
191 ECG CRITERIA for DIAGNOSIS of STEMI: (ST J POINT) *LEADS V2 and V3: MALES AGE 40 and up mm (MALES LESS THAN mm) FEMALES mm ALL OTHER LEADS: 1.0 mm or more, in TWO or more CONTIGUOUS LEADS * P. Rautaharju et al, Standardization and Interpretation of the ECG, JACC 2009;(53)No.11:

192 ST SEGMENT ELEVATION: 3 COMMON PATTERNS of ST SEGMENT ELEVATION From ACUTE MI:

193
194 Reciprocal S-T Segment Depression may or may not be present during AMI. The presence of S-T Depression on an EKG which exhibits significant S-T elevation is a fairly reliable indicator that AMI is the diagnosis. However the lack of Reciprocal S-T Depression DOES NOT rule out AMI.

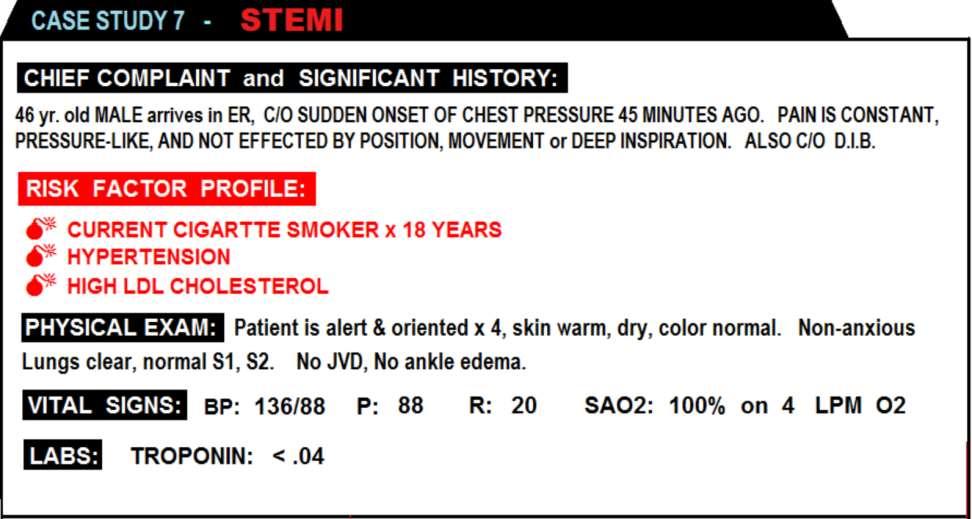
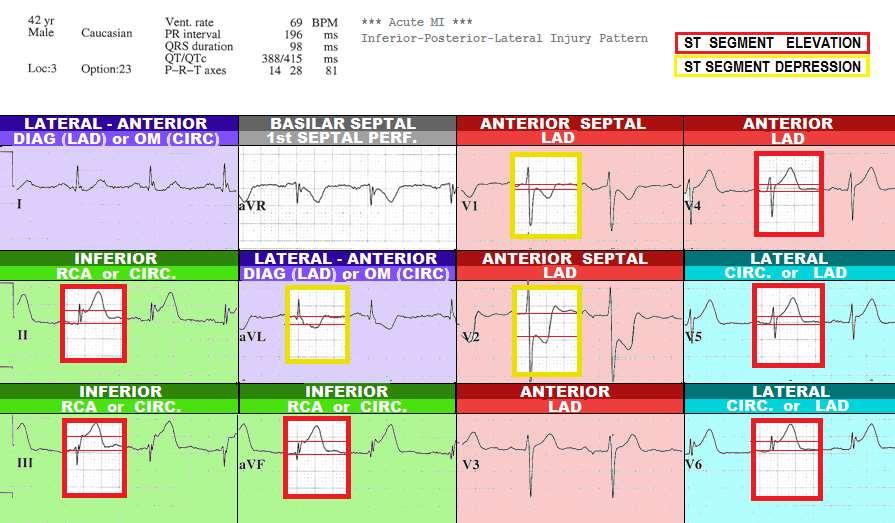
195 STEMI CASE STUDIES

196
197 INVALUABLE ASSET for ALL MEDICAL PROFESSIONALS who provide direct care to STEMI patients!

198 The 12 Lead ECG becomes your crystal ball!!

199
200 STEMI CASE STUDIES
201 STEMI Case Studies, excerpts from 12 Lead ECG Interpretation in ACS with Case Studies from the Cardiac Cath Lab.

202

203
204
205 Note: There is NO Reciprocal ST Depression on this STEMI ECG!
206
207
208

209

210

211
212 ANTICIPATED COMPLICATIONS of ANTERIOR-SEPTAL WALL STEMI & POSSIBLE INDICATED INTERVENTIONS: - CARDIAC ARREST BCLS / ACLS - CARDIAC DYSRHYTHMIAS (VT / VF) ACLS (antiarrhythmics) - PUMP FAILURE with INOTROPE THERAPY: CARDIOGENIC SHOCK -DOPAMINE / DOBUTAMINE / LEVOPHED - INTRA-AORTIC BALLOON PUMP (use caution with fluid challenges due to PULMONARY EDEMA) - PULMONARY EDEMA - CPAP - ET INTUBATION (use caution with dieuretics due to pump failure and hypotension) - 3rd DEGREE HEART BLOCK - NOT RESPONSIVE TO ATROPINE TRANSCUTANEOUS or TRANSVENOUS PACING



213

214

215

216

217
218




219 CASE PROGRESSION: As the patient was being prepared for transport to the Cardiac Cath Lab, she experienced an episode of Ventricular Fibrillation.

220

221
222

223
224 - Reciprocal ST Depression is NOW PRESENT - Additional ST Elevation is present in Leads I, AVL
225 = +

226
227 = +
228

229
230 ANTICIPATED COMPLICATIONS of ANTERIOR-SEPTAL WALL STEMI & POSSIBLE INDICATED INTERVENTIONS: - CARDIAC ARREST BCLS / ACLS - CARDIAC DYSRHYTHMIAS (VT / VF) ACLS (antiarrhythmics) - PUMP FAILURE with INOTROPE THERAPY: CARDIOGENIC SHOCK -DOPAMINE / DOBUTAMINE / LEVOPHED - INTRA-AORTIC BALLOON PUMP (use caution with fluid challenges due to PULMONARY EDEMA) - PULMONARY EDEMA - CPAP - ET INTUBATION (use caution with dieuretics due to pump failure and hypotension) - 3rd DEGREE HEART BLOCK - NOT RESPONSIVE TO ATROPINE TRANSCUTANEOUS or TRANSVENOUS PACING

231 WHILE AWAITING THE CATH TEAM, THE PATIENT BEGAN VOMITING. SKIN BECAME ASHEN & DIAPHORETIC. REPEAT BP = 50/30. -WHAT THERAPEUTIC INTERVENTIONS SHOULD BE IMPLMENTED AT THIS POINT?


232

233

234 WHO SHOULD GO TO THE CATH LAB FIRST? And.... WHAT WOULD YOU DO WITH THE PATIENT WHO DID NOT GO TO THE CATH LAB?



235
236 PATIENT A: PATIENT B:


237


238


239


240 Despite the dismal mortality rate associated with STEMI from total LMCA occlusion, this patient survived and was later discharged. His EF is estimated at approximately 30%. He received an ICD, and is currently stable.

241
242
243
244
245

246
247

248
249 ANTICIPATED COMPLICATIONS of INFERIOR WALL STEMI secondary to RCA Occlusion & POSSIBLE INDICATED INTERVENTIONS: - CARDIAC ARREST BCLS / ACLS - CARDIAC DYSRHYTHMIAS (VT / VF) ACLS (antiarrhythmics) - SINUS BRADYCARDIA ATROPINE 0.5mg, REPEAT as needed UP TO 3mg. (follow ACLS and/or UNIT protocols) - HEART BLOCKS (1st, 2nd & 3rd Degree HB) ATROPINE 0.5mg, REPEAT as needed UP TO 3mg, Transcutaneous Pacing, (follow ACLS and/or UNIT - RIGHT VENTRICULAR MYOCARDIAL INFARCTION protocols) - The standard 12 Lead ECG does NOT view the Right Ventricle. - You must do a RIGHT-SIDED ECG to see if RV MI is present. - Do NOT give any Inferior Wall STEMI patient NITRATES or DIURETICS until RV MI has been RULED OUT. - POSTERIOR WALL INFARCTION - POSTERIOR WALL MI presents on the 12 Lead ECG as ST DEPRESSION in Leads V1 - V3. - POSTERIOR WALL MI is NOT PRESENT

250

251

252

253

254
255 IN EVERY CASE of INFERIOR WALL STEMI You must first RULE OUT RIGHT VENTRICULAR MI BEFORE giving any: - NITROGLYCERIN - Diuretics
256 Nitroglycerin & Diuretics are CLASS III CONTRINDICATED in RIGHT VENTRICULAR MI!!* They precipitate SEVERE HYPOTENSION * A.H.A. ACLS 2010 / 2015

257
258 ANTICIPATED COMPLICATIONS of INFERIOR - RIGHT VENRICULAR WALL STEMI secondary to PROXIMAL RCA Occlusion & POSSIBLE INDICATED INTERVENTIONS: - CARDIAC ARREST BCLS / ACLS - CARDIAC DYSRHYTHMIAS (VT / VF) ACLS (antiarrhythmics) - SINUS BRADYCARDIA ATROPINE 0.5mg, REPEAT as needed UP TO 3mg. (follow ACLS and/or UNIT protocols) - HEART BLOCKS (1st, 2nd & 3rd Degree HB) ATROPINE 0.5mg, REPEAT as needed UP TO 3mg, Transcutaneous Pacing, (follow ACLS and/or UNIT protocols) - RIGHT VENTRICULAR MYOCARDIAL INFARCTION - NITRATES and DIURETICS are CONTRA- INDICATED. - TREAT HYPOTENSION WITH FLUIDS. (It is Not uncommon to give ml of NORMAL SALINE to stabilize BP. - POSTERIOR WALL INFARCTION - POSTERIOR WALL MI presents on the 12 Lead ECG as ST DEPRESSION in Leads V1 - V3. - POSTERIOR WALL MI is NOT PRESENT ON THIS ECG.
259 If this patient becomes HYPOTENSIVE.....

260


261


262

263
264


265
266


267




268

269
270 Case Study- January y/o female complaining of L arm pain, and minimal chest pain EMS 12 Lead ECGs show ST Depression in Anterior Leads V1-V4. There is NO ST Elevation

271
272 Initial Exam in ED Upon arrival in ED, 12 Lead ECG confirmed EMS findings: ST Depression in Leads V1-V4.

273
274 Causes of ST Depression V1-V4 Anterior Wall ischemia Anterior Wall NSTEMI (partial wall thickness myocardial infarction) Posterior Wall STEMI
275 Posterior Wall STEMI. Does not show ST elevation on standard 12 lead ECG because NONE of the 12 leads view the Posterior Wall directly.
276 Posterior Wall STEMI. Often shows NO ST Elevation on the standard 12 Lead ECG. Will show up on standard 12 Lead ECG as ST Depression (Reciprocal) in Leads V1-V3 (sometimes V4-V6, too).
277 V1-V3 see the Posterior Wall ONLY through RECIPROCAL changes (ST Depression)
278
279 Posterior Wall STEMI. To see ST Elevation from a Posterior Wall STEMI, you must place ECG leads on the patient s back
280 Continued Exam in the ED. Upon noting ST Depression in Anterior Leads V1-V4, ED Paramedic Gary Polizzi place three leads on the patient s back. Gary used the lead wires for V4, V5 and V6, with placement as shown here: The Posterior Lead ECG is seen on the next slide

281
282 STEMI Alert! Upon seeing Significant ST Elevation in TWO or more CONTIGUOUS LEADS, the ED physician diagnosed Posterior Wall STEMI, a STEMI Alert was issued, and the patient was taken immediately to the cardiac cath lab, where the following images were obtained.

283

284

285
286 SUMMARY Whenever ST Depression is noted in Anterior Leads (V1-V4), it could indicate that Acute Posterior Wall STEMI is present. To rule-out Posterior Wall STEMI, a posterior lead ECG (V7 V9) must be obtained. In THIS CASE, Posterior Wall STEMI was diagnosed via Posterior Lead ECG. STEMI Alert was issued, with a Door-to-PCI time of 53 minutes!

287

288 Evaluating the ECG for ACS:
289 Wide QRS present: QRSd > 120ms Determine RIGHT vs. LEFT Bundle Branch Block Pattern

290 Simple Turn Signal Method...

291 Terminal Phase of QRS Method...

292

293

294 From: Rapid Interpretation of ECGs by Dale Dubin, MD

295
296

297

298
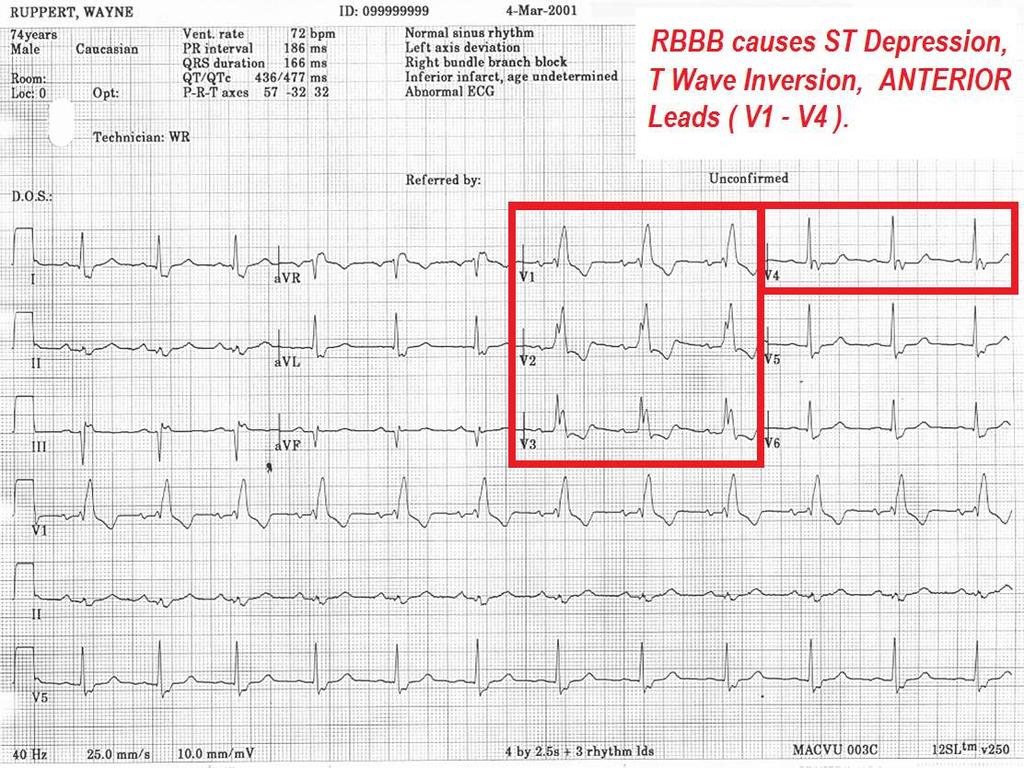
299 Wide QRS present: (QRSd > 120ms) When RIGHT Bundle Branch Block pattern is present: Precordial Leads typically demonstrate ST Depression and T wave Inversion
300
301 Wide QRS present: (QRSd > 120ms) When RIGHT Bundle Branch Block pattern is present: Precordial Leads typically demonstrate ST Depression and T wave Inversion DOES NOT MASK STEMI; when ST Elevation is noted, CONSIDER STEMI!!

302

303

304
305 Wide QRS present: (QRSd > 120ms) When LBBB QRS pattern is present:
306 Wide QRS present: (QRSd > 120ms) When LBBB QRS pattern is present: ST-Segment Elevation is typically noted in Precordial Leads
307 Wide QRS present: (QRSd > 120ms) When LBBB QRS pattern is present: ST-Segment Elevation is typically noted in Precordial Leads Can cause up to 5mm of J Point Elevation in normally calibrated ECG (1mm=10mv)
308 Wide QRS present: (QRSd > 120ms) When LBBB QRS pattern is present: ST-Segment Elevation is typically noted in Precordial Leads Can cause up to 5mm of J Point Elevation in normally calibrated ECG (1mm=10mv) Does NOT typically cause ST elevation in INFERIOR Leads (II, III and AVF).
309 Diagnosis of STEMI with LBBB pattern: 2013 ACC/AHA Guideline for Management of STEMI ST Elevation of 0.1mv (1mm) or more in leads with Positive Deflection QRS complexes
310 Diagnosis of STEMI with LBBB pattern: 2013 ACC/AHA Guideline for Management of STEMI ST Elevation of 0.1mv (1mm) or more in leads with Positive Deflection QRS complexes ST Elevation of 0.5mv (5mm) or more in leads with Negative Deflection QRS complexes
311 Diagnosis of STEMI with LBBB pattern: 2013 ACC/AHA Guideline for Management of STEMI ST Elevation of 0.1mv (1mm) or more in leads with Positive Deflection QRS complexes ST Elevation of 0.5mv (5mm) or more in leads with Negative Deflection QRS complexes ST Segment Changes as compared with those of older ECGs with LBBB
312 Diagnosis of STEMI with LBBB pattern: 2013 ACC/AHA Guideline for Management of STEMI ST Elevation of 0.1mv (1mm) or more in leads with Positive Deflection QRS complexes ST Elevation of 0.5mv (5mm) or more in leads with Negative Deflection QRS complexes ST Segment Changes as compared with those of older ECGs with LBBB Convex ST Segment

313

314

315
316 Electrocardiographic Diagnosis of Evolving Acute Myocardial Infarction in the Presence of Left Bundle-Branch Block Birnbaum et al, N Engl J Med 1996; 334:
317 Be advised that in patients with Left Bundle Branch Block Combined with Ventricular Hypertrophy, The J Point elevation can exceed 0.5 mv (5mm) above the iso-electric line in patients without ACS.
318


319

320

321 STEMI Assistant: an Emergency Crash Cart Interactive Reference Manual - free Download STEMI Assistant Information Video
322 Helpful STEMI ECG Resources [1] Use of the Electrocardiogram in Acute Myocardial Infarction, Zimetbaum, et al, NEJM 348: Abnormal ST Elevation Criteria: ACC/AHA 2009 Standardization and Interpretation of the ECG, Part VI Acute Ischemia and Infarction, Galen Wagner, et al ECG in STEMI excellent powerpoint quick reference, in-depth material
323 Helpful STEMI ECG Resources Download Non-ED STEMI Protocol - example Download STEMI Alert ED Physicians Order Set

324

325

326

327

328
329 Classic Wellen s Syndrome: Characteristic T wave changes Biphasic T waves Inverted T waves History of anginal chest pain Normal or minimally elevated cardiac markers ECG without Q waves, without significant ST-segment elevation, and with normal precordial R-wave progression
330 Wellen s Syndrome ETIOLOGY: Critical Lesion, Proximal LAD Coronary Artery Vasospasm Cocaine use (vasospasm) Increased myocardial oxygen demand Generalized Hypoxia / anemia / low H&H
331 Wellen s Syndrome EPIDEMIOLOGY & PROGNOSIS: Present in 14-18% of patients admitted with unstable angina 75% patients not treated developed extensive Anterior MI within 3 weeks. Median Average time from presentation to Acute Myocardial Infarction 8 days Sources: H Wellens et. Al, Am Heart J 1982; v103(4)
332 Wellen s Syndrome Case Study 33 y/o male Chief complaint sharp, pleuritic quality chest pain, intermittent, recent history lower respiratory infection with productive cough. ED physician attributed the ST elevation in precordial leads to early repolarization, due to patient age, gender, race (African American) and concave nature of ST-segments.

333 Wellen s Syndrome Case Study

334 Wellen s Syndrome Case Study
335 DYNAMIC ST-T Wave Changes ARE PRESENT!! NOW is the time for the STAT CALL to the CARDIOLOGIST!!!!

336 Wellen s Syndrome Case Study

337 Wellen s Syndrome Case Study

338 Wellen s Syndrome Case Study

339 Wellen s Syndrome Case Study
340 Additional Resources: Wellen s Syndrome, NEJM case study

341

342

343 Some less common, less reliable possible indicators of ACS:
344 Long QT Syndrome

345

346
347 Determining the QTc Manual calculation: QT CORRECTION FORMULAS: Bazett s Fredericia Framingham Rautaharju QTc=QT/ RR QTc=QT/(RR)1/3 QTc=QT+0.154(1-RR) QTp=656/(1+HR/100)

348

349
350

351 Determining the QT / QTc Method 1 12 Lead ECG Report:
352 Determining the QTc Method 4, Use a Smartphone App: iphone Android m.medsam.qtccalculator&hl=en

353 There s an APP for that!

354 Determining the QTc Method 3, Use a Web-based App:

355 SOURCE: ACC/AHA/HRS Recommendations for Standardization and Interpretation of the ECG, Part IV: The ST Segment, T and U Waves, and the QT Interval Rautaharju et al 2009

356 WHEN THE QUICK PEEK METHOD for QT INTERAL EVALUATION IS APPLIED TO THE ABOVE ECG, WHAT IS THE RESULT?

357 Dysrhythmia Associated with Mortality, Triggered by LQTS: Torsades de Pointes Torsades de Pointes (TdP) HEMODYNAMICS: Decreased to NO Cardiac Output Often patient PULSELESS during episode Patients often report SYNCOPE when TdP self-terminates. May DETERIORATE into VENTRICULAR FIBRILLATION and CARDIAC ARREST. ( Sudden Death )


358 ECG Characteristics of TdP: The QRS Pattern of Torsades de Pointes resembles..... a piece of Twisted Ribbon!
359 Evolving MI & Old MI

360

361

362
363
364

365

366

367 The NORMAL ECG R wave amplitude (size) gradually increases from V1 through V6....

368 The NORMAL ECG In V3 or V4, the QRS complex becomes Biphasic.
 is a common")
369 Poor R Wave Progression.... Anterior Wall necrosis ( old MI ) is a common cause of Poor R Wave Progression.
370 EVOLVING STEMI: -ST SEGMENTS DROP -Q WAVES FORM -R WAVE PROGRESSION CHANGES IN PRECORDIAL LEADS.
371 EVOLVING STEMI: -ST SEGMENTS DROP -Q WAVES FORM -R WAVE PROGRESSION CHANGES IN PRECORDIAL LEADS.

372

373 ACUTE ANTERIOR WALL STEMI

374 EVOLVING ANTERIOR WALL STEMI

375 FULLY EVOLVED ANTERIOR WALL MI
376 Additional Materials:

377

378

379

380

381

382

383

384

385

386

387

388

389

390

391

392 ACUTE MITRAL VALVE RUPTURE USUALLY OCCURS 7-10 DAYS POST EXTENSIVE MI (e.g.: INFERIOR POSTERIOR LATERAL MI).
393

394

395

396

397
398 Practice ECGs...
399 Let s review ECG abnormality(ies)? 2. Possible diagnosis? 3. Action / Intervention?
. 3. Action / Intervention? STAT CATH LAB vs STAT Thrombolytics.")
400 1. ECG abnormality(ies)? ST Elevation Leads I, AVR AVL, V1, V2, V3, V4, V5 & V6. ST Depression II, III and AVF 2. Possible diagnosis? Acute Anterolateral Wall STEMI secondary to Left Main Coronary Artery occlusion (widowmaker MI). 3. Action / Intervention? STAT CATH LAB vs STAT Thrombolytics. Prepare for Cardiac Arrest

401 1. ECG abnormality(ies)? 2. Possible diagnosis? 3. Action / Intervention?

402 1. ECG abnormality(ies)? ST Depression V1-V4 2. Possible diagnosis? Anterior ischemia vs. Posterior wall STEMI 3. Action / Intervention? Posterior ECG (V7-V9)
403 1. ECG abnormality(ies)? 2. Possible diagnosis? 3. Action / Intervention?
404 1. ECG abnormality(ies)? ST Elevation, Leads II,III & AVF 2. Possible diagnosis? Inferior Wall STEMI 3. Action / Intervention? 1. Do R-sided ECG, prepare for Atropine administration, external pacing, cardiac arrest, STAT cath lab visit!

405 What leads show signs of possible ACS?

406 12 Lead ECG shows ISCHEMIC CHANGES Lateral Wall:
407 1. ECG abnormality(ies)? 2. Possible diagnosis? 3. Action / Intervention?
408 1. ECG abnormality(ies)? ST Elevation Lead AVR, Global ST Depression (I, II, III, AVL, AVF, V2, V3, V4, V5, V6) 2. Possible diagnosis? possible LMCA or 3x vessel disease. 3. Action / Intervention? Troponins, Continuous ST monitoring, cath lab visit STAT or ASAP (based on sympt.)
409 1. ECG abnormality(ies)? 2. Possible diagnosis? 3. Action / Intervention?
410 1. ECG abnormality(ies)? Inferior (II, III, AVF) ST Depr (ischemia?), I & AVL T wave inversion, V5 ST Depr 2. Possible diagnosis? Inferior / Lateral ischemia 3. Action / Intervention? Serial ECGs / Troponins, additional diagnostic testing, cath lab
411 Your thoughts, ideas, comments and feedback are welcome...
412 Author s correspondence information: Wayne W Ruppert Wayneruppert@bayfronthealth.com Office: Cell:

413 My top two reasons for giving everything in life the best I have to offer.
STAT 12 Lead ECG Workshop: Basics & ACS
 STAT 12 Lead ECG Workshop: Basics & ACS Part 2: Acute Coronary Syndrome WAYNE W RUPPERT, CVT, CCCC, NREMT-P Cardiovascular Coordinator Bayfront Health Seven Rivers Crystal River, Florida Interventional
STAT 12 Lead ECG Workshop: Basics & ACS Part 2: Acute Coronary Syndrome WAYNE W RUPPERT, CVT, CCCC, NREMT-P Cardiovascular Coordinator Bayfront Health Seven Rivers Crystal River, Florida Interventional
ACUTE CORONARY SYNDROME
 12 LEAD ECG INTERPRETATION in ACUTE CORONARY SYNDROME WAYNE W RUPPERT, CVT, CCCC, NREMT-P Cardiovascular Clinical Coordinator Bayfront Health Seven Rivers Crystal River, FL Education Specialist St. Joseph
12 LEAD ECG INTERPRETATION in ACUTE CORONARY SYNDROME WAYNE W RUPPERT, CVT, CCCC, NREMT-P Cardiovascular Clinical Coordinator Bayfront Health Seven Rivers Crystal River, FL Education Specialist St. Joseph
Observation Medicine ECG Instructor Workshop session 2 Serial 12 Lead ECG Interpretation
 American College of Cardiology 20 th Congress 2017 Observation Medicine ECG Instructor Workshop session 2 Serial 12 Lead ECG Interpretation Part 1 By: Wayne W Ruppert, CVT, CCCC, NREMT-P This curriculum
American College of Cardiology 20 th Congress 2017 Observation Medicine ECG Instructor Workshop session 2 Serial 12 Lead ECG Interpretation Part 1 By: Wayne W Ruppert, CVT, CCCC, NREMT-P This curriculum
ACUTE CORONARY SYNDROME
 12 LEAD ECG INTERPRETATION in ACUTE CORONARY SYNDROME WAYNE W RUPPERT, CVT, CCCC, NREMT P Cardiovascular C di l Clinical Cli i l Coordinator C di t Bayfront Health Dade City Dade City, FL Education Specialist
12 LEAD ECG INTERPRETATION in ACUTE CORONARY SYNDROME WAYNE W RUPPERT, CVT, CCCC, NREMT P Cardiovascular C di l Clinical Cli i l Coordinator C di t Bayfront Health Dade City Dade City, FL Education Specialist
12 Lead ECG Interpretation
 12 Lead ECG Interpretation Julie Zimmerman, MSN, RN, CNS, CCRN Significant increase in mortality for every 15 minutes of delay! N Engl J Med 2007;357:1631-1638 Who should get a 12-lead ECG? Also include
12 Lead ECG Interpretation Julie Zimmerman, MSN, RN, CNS, CCRN Significant increase in mortality for every 15 minutes of delay! N Engl J Med 2007;357:1631-1638 Who should get a 12-lead ECG? Also include
All About STEMIs. Presented By: Brittney Urvand, RN, BSN, CCCC. Essentia Health Fargo Cardiovascular Program Manager.
 All About STEMIs Presented By: Brittney Urvand, RN, BSN, CCCC Essentia Health Fargo Cardiovascular Program Manager Updated 10/2/2018 None Disclosures Objectives Identify signs and symptoms of a heart attack
All About STEMIs Presented By: Brittney Urvand, RN, BSN, CCCC Essentia Health Fargo Cardiovascular Program Manager Updated 10/2/2018 None Disclosures Objectives Identify signs and symptoms of a heart attack
12 Lead EKG. The Basics
 12 Lead EKG The Basics Objectives Demonstrate proper 12 EKG lead placement Determine electrical axis Identify ST and T wave changes as they relate to myocardial ischemia Describe possible complications
12 Lead EKG The Basics Objectives Demonstrate proper 12 EKG lead placement Determine electrical axis Identify ST and T wave changes as they relate to myocardial ischemia Describe possible complications
12 Lead Electrocardiogram (ECG) PFN: SOMACL17. Terminal Learning Objective. References
 PFN: SOMACL17. Terminal Learning Objective. References") 12 Lead Electrocardiogram (ECG) PFN: SOMACL17 Slide 1 Terminal Learning Objective Action: Communicate knowledge of 12 Lead Electrocardiogram (ECG) Condition: Given a lecture in a classroom environment
12 Lead Electrocardiogram (ECG) PFN: SOMACL17 Slide 1 Terminal Learning Objective Action: Communicate knowledge of 12 Lead Electrocardiogram (ECG) Condition: Given a lecture in a classroom environment
The Fundamentals of 12 Lead EKG. ECG Recording. J Point. Reviewing the Cardiac Conductive System. Dr. E. Joe Sasin, MD Rusty Powers, NRP
 The Fundamentals of 12 Lead EKG Dr. E. Joe Sasin, MD Rusty Powers, NRP SA Node Intranodal Pathways AV Junction AV Fibers Bundle of His Septum Bundle Branches Purkinje System Reviewing the Cardiac Conductive
The Fundamentals of 12 Lead EKG Dr. E. Joe Sasin, MD Rusty Powers, NRP SA Node Intranodal Pathways AV Junction AV Fibers Bundle of His Septum Bundle Branches Purkinje System Reviewing the Cardiac Conductive
REtrive. REpeat. RElearn Design by. Test-Enhanced Learning based ECG practice E-book
 Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning based ECG practice E-book REtrive REpeat RElearn Design by S I T T I N U N T H A N G J U I P E E R I Y A W A
Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning based ECG practice E-book REtrive REpeat RElearn Design by S I T T I N U N T H A N G J U I P E E R I Y A W A
Family Medicine for English language students of Medical University of Lodz ECG. Jakub Dorożyński
 Family Medicine for English language students of Medical University of Lodz ECG Jakub Dorożyński Parts of an ECG The standard ECG has 12 leads: six of them are considered limb leads because they are placed
Family Medicine for English language students of Medical University of Lodz ECG Jakub Dorożyński Parts of an ECG The standard ECG has 12 leads: six of them are considered limb leads because they are placed
12 Lead ECG Interpretation: Color Coding for MI s
 12 Lead ECG Interpretation: Color Coding for MI s Anna E. Story, RN, MS Director, Continuing Professional Education Critical Care Nurse Online Instructional Designer 2004 Anna Story 1 Objectives review
12 Lead ECG Interpretation: Color Coding for MI s Anna E. Story, RN, MS Director, Continuing Professional Education Critical Care Nurse Online Instructional Designer 2004 Anna Story 1 Objectives review
By the end of this lecture, you will be able to: Understand the 12 lead ECG in relation to the coronary circulation and myocardium Perform an ECG
 By the end of this lecture, you will be able to: Understand the 12 lead ECG in relation to the coronary circulation and myocardium Perform an ECG recording Identify the ECG changes that occur in the presence
By the end of this lecture, you will be able to: Understand the 12 lead ECG in relation to the coronary circulation and myocardium Perform an ECG recording Identify the ECG changes that occur in the presence
12-Lead ECG Interpretation. Kathy Kuznar, RN, ANP
 12-Lead ECG Interpretation Kathy Kuznar, RN, ANP The 12-Lead ECG Objectives Identify the normal morphology and features of the 12- lead ECG. Perform systematic analysis of the 12-lead ECG. Recognize abnormalities
12-Lead ECG Interpretation Kathy Kuznar, RN, ANP The 12-Lead ECG Objectives Identify the normal morphology and features of the 12- lead ECG. Perform systematic analysis of the 12-lead ECG. Recognize abnormalities
12 LEAD EKG BASICS. By: Steven Jones, NREMT P CLEMC
 12 LEAD EKG BASICS By: Steven Jones, NREMT P CLEMC ECG Review Waves and Intervals P wave: the sequential activation (depolarization) of the right and left atria QRS complex: right and left ventricular
12 LEAD EKG BASICS By: Steven Jones, NREMT P CLEMC ECG Review Waves and Intervals P wave: the sequential activation (depolarization) of the right and left atria QRS complex: right and left ventricular
ECG Basics Sonia Samtani 7/2017 UCI Resident Lecture Series
 ECG Basics Sonia Samtani 7/2017 UCI Resident Lecture Series Agenda I. Introduction II.The Conduction System III.ECG Basics IV.Cardiac Emergencies V.Summary The Conduction System Lead Placement avf Precordial
ECG Basics Sonia Samtani 7/2017 UCI Resident Lecture Series Agenda I. Introduction II.The Conduction System III.ECG Basics IV.Cardiac Emergencies V.Summary The Conduction System Lead Placement avf Precordial
Section V. Objectives
 Section V Landscape of an MI Objectives At the conclusion of this presentation the participant will be able to Outline a systematic approach to 12 lead ECG interpretation Demonstrate the process for determining
Section V Landscape of an MI Objectives At the conclusion of this presentation the participant will be able to Outline a systematic approach to 12 lead ECG interpretation Demonstrate the process for determining
Ekg pra pr c a tice D.HAMMOUDI.MD
 Ekg practice D.HAMMOUDI.MD Anatomy Revisited RCA (Right Coronary Artery) Right ventricle Inferior wall of LV Posterior wall of LV (75%) SA Node (60%) AV Node (>80%) LCA (Left Coronary Artery) Septal wall
Ekg practice D.HAMMOUDI.MD Anatomy Revisited RCA (Right Coronary Artery) Right ventricle Inferior wall of LV Posterior wall of LV (75%) SA Node (60%) AV Node (>80%) LCA (Left Coronary Artery) Septal wall
Acute Coronary Syndromes. Disclosures
 Acute Coronary Syndromes Disclosures I work for Virginia Garcia Memorial Health Center, Beaverton, OR. Jon Tardiff, BS, PA-C OHSU Clinical Assistant Professor And I am a medical editor for Jones & Bartlett
Acute Coronary Syndromes Disclosures I work for Virginia Garcia Memorial Health Center, Beaverton, OR. Jon Tardiff, BS, PA-C OHSU Clinical Assistant Professor And I am a medical editor for Jones & Bartlett
Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016
 Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016 Disclosures: EKG Workshop Louis Mancano, MD Speaker has no disclosures
Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016 Disclosures: EKG Workshop Louis Mancano, MD Speaker has no disclosures
A few new tools for better detection and understanding of STEMIs in the field.
 A few new tools for better detection and understanding of STEMIs in the field. Let s talk, prep and placement. Try to shoot for quality, consistency and no artifact! (looking sometimes for 1 or 2 mm changes)
A few new tools for better detection and understanding of STEMIs in the field. Let s talk, prep and placement. Try to shoot for quality, consistency and no artifact! (looking sometimes for 1 or 2 mm changes)
ECG in coronary artery disease. By Sura Boonrat Central Chest Institute
 ECG in coronary artery disease By Sura Boonrat Central Chest Institute EKG P wave = Atrium activation PR interval QRS = Ventricle activation T wave= repolarization J-point EKG QT interval Abnormal repolarization
ECG in coronary artery disease By Sura Boonrat Central Chest Institute EKG P wave = Atrium activation PR interval QRS = Ventricle activation T wave= repolarization J-point EKG QT interval Abnormal repolarization
ECG Workshop. Nezar Amir
 ECG Workshop Nezar Amir Myocardial Ischemia ECG Infarct ECG in STEMI is dynamic & evolving Common causes of ST shift Infarct Localisation Left main artery occlusion: o diffuse ST-depression with ST elevation
ECG Workshop Nezar Amir Myocardial Ischemia ECG Infarct ECG in STEMI is dynamic & evolving Common causes of ST shift Infarct Localisation Left main artery occlusion: o diffuse ST-depression with ST elevation
Myocardial Infarction. Reading Assignment (p66-78 in Outline )
") Myocardial Infarction Reading Assignment (p66-78 in Outline ) Objectives 1. Why do ST segments go up or down in ischemia? 2. STEMI locations and culprit vessels 3. Why 15-lead ECGs? 4. What s up with avr?
Myocardial Infarction Reading Assignment (p66-78 in Outline ) Objectives 1. Why do ST segments go up or down in ischemia? 2. STEMI locations and culprit vessels 3. Why 15-lead ECGs? 4. What s up with avr?
Basic electrocardiography reading. R3 lee wei-chieh
 Basic electrocardiography reading R3 lee wei-chieh The Normal Conduction System Lead Placement avf Limb Leads Precordial Leads Interpretation Rate Rhythm Interval Axis Chamber abnormality QRST change What
Basic electrocardiography reading R3 lee wei-chieh The Normal Conduction System Lead Placement avf Limb Leads Precordial Leads Interpretation Rate Rhythm Interval Axis Chamber abnormality QRST change What
12 Lead ECGs: Ischemia, Injury & Infarction. Kevin Handke NRP, FP-C, CCP, CMTE STEMI Coordinator Flight Paramedic
 12 Lead ECGs: Ischemia, Injury & Infarction Kevin Handke NRP, FP-C, CCP, CMTE STEMI Coordinator Flight Paramedic None Disclosures Objectives Upon completion of this program the learner will be able to
12 Lead ECGs: Ischemia, Injury & Infarction Kevin Handke NRP, FP-C, CCP, CMTE STEMI Coordinator Flight Paramedic None Disclosures Objectives Upon completion of this program the learner will be able to
Huseng Vefali MD St. Luke s University Health Network Department of Cardiology
 Huseng Vefali MD St. Luke s University Health Network Department of Cardiology Learning Objectives Establish Consistent Approach to Interpreting ECGs Review Essential Cases for Paramedics and first responders
Huseng Vefali MD St. Luke s University Health Network Department of Cardiology Learning Objectives Establish Consistent Approach to Interpreting ECGs Review Essential Cases for Paramedics and first responders
Acute Coronary Syndromes Unstable Angina Non ST segment Elevation MI (NSTEMI) ST segment Elevation MI (STEMI)
 ST segment Elevation MI (STEMI)") Leanna R. Miller, RN, MN, CCRN-CSC, PCCN-CMC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Evaluate common abnormalities that mimic myocardial infarction. Identify
Leanna R. Miller, RN, MN, CCRN-CSC, PCCN-CMC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Evaluate common abnormalities that mimic myocardial infarction. Identify
Relax and Learn At the Farm 2012
 Relax and Learn At the Farm 2012 Session 2: 12 Lead ECG Fundamentals 101 Cynthia Webner DNP, RN, CCNS, CCRN-CMC, CHFN Though for Today Mastery is not something that strikes in an instant, like a thunderbolt,
Relax and Learn At the Farm 2012 Session 2: 12 Lead ECG Fundamentals 101 Cynthia Webner DNP, RN, CCNS, CCRN-CMC, CHFN Though for Today Mastery is not something that strikes in an instant, like a thunderbolt,
ECGs: Everything a finalist needs to know. Dr Amy Coulden As part of the Simply Finals series
 ECGs: Everything a finalist needs to know Dr Amy Coulden As part of the Simply Finals series Aims and objectives To be able to interpret basic ECG abnormalities To be able to recognise commonly tested
ECGs: Everything a finalist needs to know Dr Amy Coulden As part of the Simply Finals series Aims and objectives To be able to interpret basic ECG abnormalities To be able to recognise commonly tested
Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition
 Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition Table of Contents Volume 1 Chapter 1: Cardiovascular Anatomy and Physiology Basic Cardiac
Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition Table of Contents Volume 1 Chapter 1: Cardiovascular Anatomy and Physiology Basic Cardiac
12 Lead ECG. Presented by Rebecca Sevigny BSN, RN Professional Practice & Development Dept.
 12 Lead ECG Presented by Rebecca Sevigny BSN, RN Professional Practice & Development Dept. Two Main Coronary Arteries RCA LCA which branches into Left Anterior Descending Circumflex Artery Two Main Coronary
12 Lead ECG Presented by Rebecca Sevigny BSN, RN Professional Practice & Development Dept. Two Main Coronary Arteries RCA LCA which branches into Left Anterior Descending Circumflex Artery Two Main Coronary
10 ECGs No Practitioner Can Afford to Miss. Objectives
 10 ECGs No Practitioner Can Afford to Miss Mary L. Dohrmann, MD Professor of Clinical Medicine Division of Cardiovascular Medicine University of Missouri School of Medicine No disclosures Objectives 1.
10 ECGs No Practitioner Can Afford to Miss Mary L. Dohrmann, MD Professor of Clinical Medicine Division of Cardiovascular Medicine University of Missouri School of Medicine No disclosures Objectives 1.
12 Lead ECG Skills: Building Confidence for Clinical Practice. Presented By: Cynthia Webner, BSN, RN, CCRN-CMC. Karen Marzlin, BSN, RN,CCRN-CMC
 12 Lead ECG Skills: Building Confidence for Clinical Practice NTI 2009 Preconference Session 803 Presented By: Karen Marzlin, BSN, RN,CCRN-CMC 1 12 Lead ECG Fundamentals: The Starting Place for Linking
12 Lead ECG Skills: Building Confidence for Clinical Practice NTI 2009 Preconference Session 803 Presented By: Karen Marzlin, BSN, RN,CCRN-CMC 1 12 Lead ECG Fundamentals: The Starting Place for Linking
Please check your answers with correct statements in answer pages after the ECG cases.
 ECG Cases ECG Case 1 Springer International Publishing AG, part of Springer Nature 2018 S. Okutucu, A. Oto, Interpreting ECGs in Clinical Practice, In Clinical Practice, https://doi.org/10.1007/978-3-319-90557-0
ECG Cases ECG Case 1 Springer International Publishing AG, part of Springer Nature 2018 S. Okutucu, A. Oto, Interpreting ECGs in Clinical Practice, In Clinical Practice, https://doi.org/10.1007/978-3-319-90557-0
Understanding the 12-lead ECG, part II
 Bundle-branch blocks Understanding the 12-lead ECG, part II Most common electrocardiogram (ECG) abnormality Appears as a wider than normal S complex Occurs when one of the two bundle branches can t conduct
Bundle-branch blocks Understanding the 12-lead ECG, part II Most common electrocardiogram (ECG) abnormality Appears as a wider than normal S complex Occurs when one of the two bundle branches can t conduct
The Electrocardiogram part II. Dr. Adelina Vlad, MD PhD
 The Electrocardiogram part II Dr. Adelina Vlad, MD PhD Basic Interpretation of the ECG 1) Evaluate calibration 2) Calculate rate 3) Determine rhythm 4) Determine QRS axis 5) Measure intervals 6) Analyze
The Electrocardiogram part II Dr. Adelina Vlad, MD PhD Basic Interpretation of the ECG 1) Evaluate calibration 2) Calculate rate 3) Determine rhythm 4) Determine QRS axis 5) Measure intervals 6) Analyze
Preface: Wang s Viewpoints
 AHA/ACCF/HRS Recommendations for the Standardization and Interpretation of the Electrocardiogram: Part IV, Ischemia and Infarction Presented by: WANG, TZONG LUEN, MD, PhD, JM, FACC, FESC, FCAPSC Professor,
AHA/ACCF/HRS Recommendations for the Standardization and Interpretation of the Electrocardiogram: Part IV, Ischemia and Infarction Presented by: WANG, TZONG LUEN, MD, PhD, JM, FACC, FESC, FCAPSC Professor,
ECG Interpretation. Introduction to Cardiac Telemetry. Michael Peters, RN, CCRN, CFRN CALSTAR Air Medical Services
 ECG Interpretation Introduction to Cardiac Telemetry Michael Peters, RN, CCRN, CFRN CALSTAR Air Medical Services Disclosures Nothing to disclose Objectives Describe the electrical conduction pathway in
ECG Interpretation Introduction to Cardiac Telemetry Michael Peters, RN, CCRN, CFRN CALSTAR Air Medical Services Disclosures Nothing to disclose Objectives Describe the electrical conduction pathway in
Electrocardiogram ECG. Hilal Al Saffar FRCP FACC College of medicine,baghdad University
 Electrocardiogram ECG Hilal Al Saffar FRCP FACC College of medicine,baghdad University Tuesday 29 October 2013 ECG introduction Wednesday 30 October 2013 Abnormal ECG ( ischemia, chamber hypertrophy, heart
Electrocardiogram ECG Hilal Al Saffar FRCP FACC College of medicine,baghdad University Tuesday 29 October 2013 ECG introduction Wednesday 30 October 2013 Abnormal ECG ( ischemia, chamber hypertrophy, heart
Arrhythmic Complications of MI. Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine
 Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
2009 Unit-Based Competencies
 2009 Unit-Based Competencies Alameda County Medical Center Highland Hospital Emergency Department Janis Farnholtz Provinse, RN, MS, CNS, CEN, ED Clinical Nurse Specialist Nurses play a pivotal role in
2009 Unit-Based Competencies Alameda County Medical Center Highland Hospital Emergency Department Janis Farnholtz Provinse, RN, MS, CNS, CEN, ED Clinical Nurse Specialist Nurses play a pivotal role in
Marcin Dada, MD December 03, 2013
 STEMI Imposters Marcin Dada, MD December 03, 2013 Marcin Dada, MD Associate Director, Chest Pain Center Hartford Hospital, Hartford, CT Member, AHA Mission Lifeline Steering Committee Outline of Topics
STEMI Imposters Marcin Dada, MD December 03, 2013 Marcin Dada, MD Associate Director, Chest Pain Center Hartford Hospital, Hartford, CT Member, AHA Mission Lifeline Steering Committee Outline of Topics
12 Lead Acquisition and Interpretation APRIL 23 11:00 AM
 12 Lead Acquisition and Interpretation APRIL 23 11:00 AM Presented by : Jennifer Robson, Prehospital Care Specialist Dr. Don Eby, Local Medical Director Objectives Upon completion of this webinar, you
12 Lead Acquisition and Interpretation APRIL 23 11:00 AM Presented by : Jennifer Robson, Prehospital Care Specialist Dr. Don Eby, Local Medical Director Objectives Upon completion of this webinar, you
Study methodology for screening candidates to athletes risk
 1. Periodical Evaluations: each 2 years. Study methodology for screening candidates to athletes risk 2. Personal history: Personal history of murmur in childhood; dizziness, syncope, palpitations, intolerance
1. Periodical Evaluations: each 2 years. Study methodology for screening candidates to athletes risk 2. Personal history: Personal history of murmur in childhood; dizziness, syncope, palpitations, intolerance
15 16 September Seminar W10O. ECG for General Practice
 15 16 September 2012 Seminar W10O ECG for General Practice Speaker: Ms Natasha Eaton ECG for General Practice Speaker: Natasha Eaton Cardiac CNC Executive Representative Electrocardiography The graphic
15 16 September 2012 Seminar W10O ECG for General Practice Speaker: Ms Natasha Eaton ECG for General Practice Speaker: Natasha Eaton Cardiac CNC Executive Representative Electrocardiography The graphic
Electrocardiography for Healthcare Professionals. Chapter 14 Basic 12-Lead ECG Interpretation
 Electrocardiography for Healthcare Professionals Chapter 14 Basic 12-Lead ECG Interpretation 2012 The Companies, Inc. All rights reserved. Learning Outcomes 14.1 Discuss the anatomic views seen on a 12-lead
Electrocardiography for Healthcare Professionals Chapter 14 Basic 12-Lead ECG Interpretation 2012 The Companies, Inc. All rights reserved. Learning Outcomes 14.1 Discuss the anatomic views seen on a 12-lead
BEDSIDE ECG INTERPRETATION
 BEDSIDE ECG INTERPRETATION Presented by: Ryan Dean, RN, MSN, CCRN, CCNS, CFRN Flight Nurse 2017 Based on presentations originally by Gennifer DePaoli, RN Objectives Hospital policies Electrical conduction
BEDSIDE ECG INTERPRETATION Presented by: Ryan Dean, RN, MSN, CCRN, CCNS, CFRN Flight Nurse 2017 Based on presentations originally by Gennifer DePaoli, RN Objectives Hospital policies Electrical conduction
Understanding basics of EKG
 Understanding basics of EKG By Alula A.(R III) www.le.ac.uk Topic for discussion Understanding of cellular electrophysiology Basics Rate Rhythm Axis Intervals P wave QRS ST/T wave Abnormal EKGs Understanding
Understanding basics of EKG By Alula A.(R III) www.le.ac.uk Topic for discussion Understanding of cellular electrophysiology Basics Rate Rhythm Axis Intervals P wave QRS ST/T wave Abnormal EKGs Understanding
ECG Interpretation Cat Williams, DVM DACVIM (Cardiology)
") ECG Interpretation Cat Williams, DVM DACVIM (Cardiology) Providing the best quality care and service for the patient, the client, and the referring veterinarian. GOAL: Reduce Anxiety about ECGs Back to
ECG Interpretation Cat Williams, DVM DACVIM (Cardiology) Providing the best quality care and service for the patient, the client, and the referring veterinarian. GOAL: Reduce Anxiety about ECGs Back to
ECG Cases and Questions. Ashish Sadhu, MD, FHRS, FACC Electrophysiology/Cardiology
 ECG Cases and Questions Ashish Sadhu, MD, FHRS, FACC Electrophysiology/Cardiology 32 yo female Life Insurance Physical 56 yo male with chest pain Terminology Injury ST elevation Ischemia T wave inversion
ECG Cases and Questions Ashish Sadhu, MD, FHRS, FACC Electrophysiology/Cardiology 32 yo female Life Insurance Physical 56 yo male with chest pain Terminology Injury ST elevation Ischemia T wave inversion
UNDERSTANDING YOUR ECG: A REVIEW
 UNDERSTANDING YOUR ECG: A REVIEW Health professionals use the electrocardiograph (ECG) rhythm strip to systematically analyse the cardiac rhythm. Before the systematic process of ECG analysis is described
UNDERSTANDING YOUR ECG: A REVIEW Health professionals use the electrocardiograph (ECG) rhythm strip to systematically analyse the cardiac rhythm. Before the systematic process of ECG analysis is described
12 Lead EKG Chapter 4 Worksheet
 Match the following using the word bank. 1. A form of arteriosclerosis in which the thickening and hardening of the vessels walls are caused by an accumulation of fatty deposits in the innermost lining
Match the following using the word bank. 1. A form of arteriosclerosis in which the thickening and hardening of the vessels walls are caused by an accumulation of fatty deposits in the innermost lining
Electrical System Overview Electrocardiograms Action Potentials 12-Lead Positioning Values To Memorize Calculating Rates
 Electrocardiograms Electrical System Overview James Lamberg 2/ 74 Action Potentials 12-Lead Positioning 3/ 74 4/ 74 Values To Memorize Inherent Rates SA: 60 to 100 AV: 40 to 60 Ventricles: 20 to 40 Normal
Electrocardiograms Electrical System Overview James Lamberg 2/ 74 Action Potentials 12-Lead Positioning 3/ 74 4/ 74 Values To Memorize Inherent Rates SA: 60 to 100 AV: 40 to 60 Ventricles: 20 to 40 Normal
Cardiovascular Disorders Lecture 3 Coronar Artery Diseases
 Cardiovascular Disorders Lecture 3 Coronar Artery Diseases By Prof. El Sayed Abdel Fattah Eid Lecturer of Internal Medicine Delta University Coronary Heart Diseases It is the leading cause of death in
Cardiovascular Disorders Lecture 3 Coronar Artery Diseases By Prof. El Sayed Abdel Fattah Eid Lecturer of Internal Medicine Delta University Coronary Heart Diseases It is the leading cause of death in
Chapter 76 Acute Coronary Syndromes Part A
 Chapter 76 Acute Coronary Syndromes Part A Episode Overview: 1. Define Stable Angina, UA, AMI 2. Describe the pathophysiology of AMI 3. What are the components of prehospital management of AMI 4. List
Chapter 76 Acute Coronary Syndromes Part A Episode Overview: 1. Define Stable Angina, UA, AMI 2. Describe the pathophysiology of AMI 3. What are the components of prehospital management of AMI 4. List
Acute Coronary Syndrome. Emergency Department Updated Jan. 2017
 Acute Coronary Syndrome Emergency Department Updated Jan. 2017 Goals and Objectives To reduce mortality and morbidity for people who have cardiovascular disease, with a focus on those who experience an
Acute Coronary Syndrome Emergency Department Updated Jan. 2017 Goals and Objectives To reduce mortality and morbidity for people who have cardiovascular disease, with a focus on those who experience an
ECG ABNORMALITIES D R. T AM A R A AL Q U D AH
 ECG ABNORMALITIES D R. T AM A R A AL Q U D AH When we interpret an ECG we compare it instantaneously with the normal ECG and normal variants stored in our memory; these memories are stored visually in
ECG ABNORMALITIES D R. T AM A R A AL Q U D AH When we interpret an ECG we compare it instantaneously with the normal ECG and normal variants stored in our memory; these memories are stored visually in
12 Lead ECG Interpretation: The Basics and Beyond
 12 Lead ECG Interpretation: The Basics and Beyond Cindy Weston, DNP, RN, CCRN, CNS-CC, FNP-BC Assistant Professor Texas A&M University College of Nursing cweston@tamhsc.edu Objectives Review the basics
12 Lead ECG Interpretation: The Basics and Beyond Cindy Weston, DNP, RN, CCRN, CNS-CC, FNP-BC Assistant Professor Texas A&M University College of Nursing cweston@tamhsc.edu Objectives Review the basics
SIMPLY ECGs. Dr William Dooley
 SIMPLY ECGs Dr William Dooley Content Basic ECG interpretation pattern Some common (examined) abnormalities Presenting ECGs in context Setting up an ECG Setting up an ECG 1 V1-4 th Right intercostal space
SIMPLY ECGs Dr William Dooley Content Basic ECG interpretation pattern Some common (examined) abnormalities Presenting ECGs in context Setting up an ECG Setting up an ECG 1 V1-4 th Right intercostal space
Masqueraders of STEMI
 Masqueraders of STEMI Steven M. Costa, M.D. Assistant Professor Department of Medicine Division of Cardiology Scott & White Memorial Hospital and Clinic Texas A&M University Health Science Center Disclosures
Masqueraders of STEMI Steven M. Costa, M.D. Assistant Professor Department of Medicine Division of Cardiology Scott & White Memorial Hospital and Clinic Texas A&M University Health Science Center Disclosures
Hot Topics in Cardiac Arrest. Should the patient go To the Cath Lab?
 Hot Topics in Cardiac Arrest Should the patient go To the Cath Lab? Tim Russert 1950-2008 Host of NBC s Meet the Press Sudden Cardiac Arrest : Autopsy showed plaque rupture in his LAD ( per LA Times,
Hot Topics in Cardiac Arrest Should the patient go To the Cath Lab? Tim Russert 1950-2008 Host of NBC s Meet the Press Sudden Cardiac Arrest : Autopsy showed plaque rupture in his LAD ( per LA Times,
DR QAZI IMTIAZ RASOOL OBJECTIVES
 PRACTICAL ELECTROCARDIOGRAPHY DR QAZI IMTIAZ RASOOL OBJECTIVES Recording of electrical events in heart Established electrode pattern results in specific tracing pattern Health of heart i. e. Anatomical
PRACTICAL ELECTROCARDIOGRAPHY DR QAZI IMTIAZ RASOOL OBJECTIVES Recording of electrical events in heart Established electrode pattern results in specific tracing pattern Health of heart i. e. Anatomical
A walk through a STEMI
 A walk through a STEMI M.M. s Story Kim Robison Ashley Corcoran Situation M.M. is an 82 year old male brought in by private vehicle on 10/22/17 to the Emergency Department Pt. c/o left arm numbness, pain
A walk through a STEMI M.M. s Story Kim Robison Ashley Corcoran Situation M.M. is an 82 year old male brought in by private vehicle on 10/22/17 to the Emergency Department Pt. c/o left arm numbness, pain
Goals: Widen Your Understanding of the Wide QRS!
 Goals: Widen Your Understanding of the Wide QRS! 1. Describe an approach to diagnosis of LBBB 2. Describe the predictive value of New LBBB 3. Describe the ST segment changes that are diagnostic of AMI
Goals: Widen Your Understanding of the Wide QRS! 1. Describe an approach to diagnosis of LBBB 2. Describe the predictive value of New LBBB 3. Describe the ST segment changes that are diagnostic of AMI
Cardiac Ischemia ECG Workshop
 Cardiac Ischemia ECG Workshop Classic, Confusing, and Confounding Patterns Amal Mattu, MD, NE Professor and Vice Chair Department of Emergency Medicine University of Maryland School of Medicine amalmattu@comcast.net
Cardiac Ischemia ECG Workshop Classic, Confusing, and Confounding Patterns Amal Mattu, MD, NE Professor and Vice Chair Department of Emergency Medicine University of Maryland School of Medicine amalmattu@comcast.net
Comments or Questions? me:
 Comments or Questions? Email me: amalmattu@comcast.net Interested in short video tutorials on electrocardiography? Check out www.ecgweekly.com Subscription fee < cost of a cup of coffee/week Covers every
Comments or Questions? Email me: amalmattu@comcast.net Interested in short video tutorials on electrocardiography? Check out www.ecgweekly.com Subscription fee < cost of a cup of coffee/week Covers every
Introduction to Electrocardiography
 Introduction to Electrocardiography Class Objectives: Introduction to ECG monitoring Discuss principles of interpretation Identify the components and measurements of the ECG ECG analysis ECG Monitoring
Introduction to Electrocardiography Class Objectives: Introduction to ECG monitoring Discuss principles of interpretation Identify the components and measurements of the ECG ECG analysis ECG Monitoring
2017 EKG Workshop Advanced. Family Medicine Review Course Lou Mancano, MD, FAAFP Reading Health System Family and Community Medicine Reading, PA
 2017 EKG Workshop Advanced Family Medicine Review Course Lou Mancano, MD, FAAFP Reading Health System Family and Community Medicine Reading, PA Part II - Objective Describe a useful approach to interpreting
2017 EKG Workshop Advanced Family Medicine Review Course Lou Mancano, MD, FAAFP Reading Health System Family and Community Medicine Reading, PA Part II - Objective Describe a useful approach to interpreting
Ischemic heart disease
 Ischemic heart disease Introduction In > 90% of cases: the cause is: reduced coronary blood flow secondary to: obstructive atherosclerotic vascular disease so most of the time it is called: coronary artery
Ischemic heart disease Introduction In > 90% of cases: the cause is: reduced coronary blood flow secondary to: obstructive atherosclerotic vascular disease so most of the time it is called: coronary artery
3/4/2018. March Martina Frost, PA C Desert Cardiology. Electricity moving towards/away from electrode create downward/upward directions of waves
 March 2018 Martina Frost, PA C Desert Cardiology Electricity moving towards/away from electrode create downward/upward directions of waves Frontal view Limb leads: I, II, III, avl, avf, (avr) Horizontal
March 2018 Martina Frost, PA C Desert Cardiology Electricity moving towards/away from electrode create downward/upward directions of waves Frontal view Limb leads: I, II, III, avl, avf, (avr) Horizontal
June 2009 CE. Site code # E-1209
 1 June 2009 CE Site code # 107200E-1209 Region X SOP Review ACS, Asystole/PEA, Bradycardia, VF/Pulseless VT, Conscious Sedation, Region X Field Triage Criteria Prepared by: Sharon Hopkins, RN, BSN, EMT-P
1 June 2009 CE Site code # 107200E-1209 Region X SOP Review ACS, Asystole/PEA, Bradycardia, VF/Pulseless VT, Conscious Sedation, Region X Field Triage Criteria Prepared by: Sharon Hopkins, RN, BSN, EMT-P
Hanna K. Al-Makhamreh, M.D., FACC Interventional Cardiologist
 Hanna K. Al-Makhamreh, M.D., FACC Interventional Cardiologist Introduction. Basic Life Support (BLS). Advanced Cardiac Life Support (ACLS). Cardiovascular diseases (CVDs) are the number one cause of death
Hanna K. Al-Makhamreh, M.D., FACC Interventional Cardiologist Introduction. Basic Life Support (BLS). Advanced Cardiac Life Support (ACLS). Cardiovascular diseases (CVDs) are the number one cause of death
Difficult Data Definitions and Scenario s
 Difficult Data Definitions and Scenario s Presenter Disclosure Information Cornelia Anderson BSN, RN To following relationships exist related to this presentation: No Disclosures Objectives Discuss key
Difficult Data Definitions and Scenario s Presenter Disclosure Information Cornelia Anderson BSN, RN To following relationships exist related to this presentation: No Disclosures Objectives Discuss key
WE ARE STEMI HUNTERS. LearningObjectives. I have no relevant disclosures. Myth: Jennifer Carlquist PA-C, ER CAQ
 WE ARE STEMI HUNTERS Jennifer Carlquist PA-C, ER CAQ Salinas Valley Memorial, ER Central Coast Cardiology, Specializing in EP LearningObjectives How to use pattern recognition to detect ischemia Triage
WE ARE STEMI HUNTERS Jennifer Carlquist PA-C, ER CAQ Salinas Valley Memorial, ER Central Coast Cardiology, Specializing in EP LearningObjectives How to use pattern recognition to detect ischemia Triage
Appendix D Output Code and Interpretation of Analysis
 Appendix D Output Code and Interpretation of Analysis 8 Arrhythmia Code No. Description 8002 Marked rhythm irregularity 8110 Sinus rhythm 8102 Sinus arrhythmia 8108 Marked sinus arrhythmia 8120 Sinus tachycardia
Appendix D Output Code and Interpretation of Analysis 8 Arrhythmia Code No. Description 8002 Marked rhythm irregularity 8110 Sinus rhythm 8102 Sinus arrhythmia 8108 Marked sinus arrhythmia 8120 Sinus tachycardia
CORONARY ARTERIES HEART
 CARDIAC/ECG MODULE THE HEART CORONARY ARTERIES FIBRILLATING HEART CORONARY ARTERIES HEART PRACTICE RHYTHMS PRACTICE RHYTHMS ELECTRICAL CONDUCTION SA Node (60 100) Primary pacemaker AV Node (40 60) ***Creates
CARDIAC/ECG MODULE THE HEART CORONARY ARTERIES FIBRILLATING HEART CORONARY ARTERIES HEART PRACTICE RHYTHMS PRACTICE RHYTHMS ELECTRICAL CONDUCTION SA Node (60 100) Primary pacemaker AV Node (40 60) ***Creates
Office ECG Interpretation
 Office ECG Interpretation Jason Evanchan, DO Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center Outline of topics High risk ischemia T wave
Office ECG Interpretation Jason Evanchan, DO Assistant Professor of Medicine Division of Cardiovascular Medicine The Ohio State University Wexner Medical Center Outline of topics High risk ischemia T wave
Chapter 3 for 12 Lead Training -Precourse-
 ONTARIO BASE HOSPITAL GROUP Chapter 3 for 12 Lead Training -Precourse- Ontario Base Hospital Group Education Subcommittee 2008 TIME IS MUSCLE ONTARIO BASE HOSPITAL GROUP Introduction and Purpose Introduction
ONTARIO BASE HOSPITAL GROUP Chapter 3 for 12 Lead Training -Precourse- Ontario Base Hospital Group Education Subcommittee 2008 TIME IS MUSCLE ONTARIO BASE HOSPITAL GROUP Introduction and Purpose Introduction
5- The normal electrocardiogram (ECG)
") 5- The (ECG) Introduction Electrocardiography is a process of recording electrical activities of heart muscle at skin surface. The electrical current spreads into the tissues surrounding the heart, a small
5- The (ECG) Introduction Electrocardiography is a process of recording electrical activities of heart muscle at skin surface. The electrical current spreads into the tissues surrounding the heart, a small
BASIC CONCEPT OF ECG
 BASIC CONCEPT OF ECG Electrocardiogram The electrocardiogram (ECG) is a recording of cardiac electrical activity. The electrical activity is readily detected by electrodes attached to the skin. After the
BASIC CONCEPT OF ECG Electrocardiogram The electrocardiogram (ECG) is a recording of cardiac electrical activity. The electrical activity is readily detected by electrodes attached to the skin. After the
IHCP bulletin INDIANA HEALTH COVERAGE PROGRAMS BT JANUARY 24, 2012
 IHCP bulletin INDIANA HEALTH COVERAGE PROGRAMS BT201203 JANUARY 24, 2012 The IHCP to reimburse implantable cardioverter defibrillators separately from outpatient implantation Effective March 1, 2012, the
IHCP bulletin INDIANA HEALTH COVERAGE PROGRAMS BT201203 JANUARY 24, 2012 The IHCP to reimburse implantable cardioverter defibrillators separately from outpatient implantation Effective March 1, 2012, the
ECG pre-reading manual. Created for the North West Regional EMET training program
 ECG pre-reading manual Created for the North West Regional EMET training program Author:- Dr Juan Carlos Ascencio-Lane juan.ascencio-lane@ths.tas.gov.au 1 Disclaimer This handbook has been created for
ECG pre-reading manual Created for the North West Regional EMET training program Author:- Dr Juan Carlos Ascencio-Lane juan.ascencio-lane@ths.tas.gov.au 1 Disclaimer This handbook has been created for
How to Read an Athlete s ECG. Sanjay Sharma BSc (Hons), MD, FRCP, FESC
, MD, FRCP, FESC") How to Read an Athlete s ECG Sanjay Sharma BSc (Hons), MD, FRCP, FESC Athlete s EKG Vagotonia Sinus bradycardia Sinus arrhythmia First degree AVB ST-elevation Tall T waves Increased chamber size Left ventricular
How to Read an Athlete s ECG Sanjay Sharma BSc (Hons), MD, FRCP, FESC Athlete s EKG Vagotonia Sinus bradycardia Sinus arrhythmia First degree AVB ST-elevation Tall T waves Increased chamber size Left ventricular
Review Packet EKG Competency This packet is a review of the information you will need to know for the proctored EKG competency test.
 Review Packet EKG Competency 2015 This packet is a review of the information you will need to know for the proctored EKG competency test. Normal Sinus Rhythm Rhythm: Regular Ventricular Rate: 60-100 bpm
Review Packet EKG Competency 2015 This packet is a review of the information you will need to know for the proctored EKG competency test. Normal Sinus Rhythm Rhythm: Regular Ventricular Rate: 60-100 bpm
also aid the clinician in recognizing both the obvious and subtle abnormalities that may help guide therapy.
 Karen Lieberman, MS, CRNP f the many diagnostic tools used to screen for and evaluate cardiac abnormalities, the 12-lead electrocardiogram (ECG) is among the most basic. This inexpensive and noninvasive
Karen Lieberman, MS, CRNP f the many diagnostic tools used to screen for and evaluate cardiac abnormalities, the 12-lead electrocardiogram (ECG) is among the most basic. This inexpensive and noninvasive
EKG Competency for Agency
 EKG Competency for Agency Name: Date: Agency: 1. The upper chambers of the heart are known as the: a. Atria b. Ventricles c. Mitral Valve d. Aortic Valve 2. The lower chambers of the heart are known as
EKG Competency for Agency Name: Date: Agency: 1. The upper chambers of the heart are known as the: a. Atria b. Ventricles c. Mitral Valve d. Aortic Valve 2. The lower chambers of the heart are known as
McHenry Western Lake County EMS System Optional CE for EMT-B, Paramedics and PHRN s Bradycardia and Treatments Optional #7 2018
 McHenry Western Lake County EMS System Optional CE for EMT-B, Paramedics and PHRN s Bradycardia and Treatments Optional #7 2018 This month we will be looking at a specific ECG Rhythm and its treatments
McHenry Western Lake County EMS System Optional CE for EMT-B, Paramedics and PHRN s Bradycardia and Treatments Optional #7 2018 This month we will be looking at a specific ECG Rhythm and its treatments
INTERPRETAZIONE ECG NEL PAZIENTE CON SOSPETTO STEMI
 INTERPRETAZIONE ECG NEL PAZIENTE CON SOSPETTO STEMI Giacomo Veronese Scuola di Specializzazione Medicina d Emergenza e Urgenza Università Milano-Bicocca Siete d accordo se vi propongo per una relazione..
INTERPRETAZIONE ECG NEL PAZIENTE CON SOSPETTO STEMI Giacomo Veronese Scuola di Specializzazione Medicina d Emergenza e Urgenza Università Milano-Bicocca Siete d accordo se vi propongo per una relazione..
Cardiac Emergencies. A Review of Cardiac Compromise. Lawrence L. Lambert
 Cardiac Emergencies A Review of Cardiac Compromise Lawrence L. Lambert 1 Cardiac Emergencies Objectives: Following successful completion of this training session, the student should be able to: 1. Describe
Cardiac Emergencies A Review of Cardiac Compromise Lawrence L. Lambert 1 Cardiac Emergencies Objectives: Following successful completion of this training session, the student should be able to: 1. Describe
Acute Coronary Syndromes
 Overview Acute Coronary Syndromes Rabeea Aboufakher, MD, FACC, FSCAI Section Chief of Cardiology Altru Health System Grand Forks, ND Epidemiology Pathophysiology Clinical features and diagnosis STEMI management
Overview Acute Coronary Syndromes Rabeea Aboufakher, MD, FACC, FSCAI Section Chief of Cardiology Altru Health System Grand Forks, ND Epidemiology Pathophysiology Clinical features and diagnosis STEMI management
Electrocardiography. Hilal Al Saffar College of Medicine,Baghdad University
 Electrocardiography Hilal Al Saffar College of Medicine,Baghdad University Which of the following is True 1. PR interval, represent the time taken for the impulse to travel from SA node to AV nose. 2.
Electrocardiography Hilal Al Saffar College of Medicine,Baghdad University Which of the following is True 1. PR interval, represent the time taken for the impulse to travel from SA node to AV nose. 2.
Other 12-Lead ECG Findings
 Other 12-Lead ECG Findings Left Atrial Enlargement Left atrial enlargement is illustrated by increased P wave duration in lead II, top ECG, and by the prominent negative P terminal force in lead V1, bottom
Other 12-Lead ECG Findings Left Atrial Enlargement Left atrial enlargement is illustrated by increased P wave duration in lead II, top ECG, and by the prominent negative P terminal force in lead V1, bottom
ECG S: A CASE-BASED APPROACH December 6,
 ECG S: A CASE-BASED APPROACH December 6, 2018 1 Faculty Disclosure Faculty: Lorne Gula MD, FRCPC Professor, Western University Cardiologist, Hearth Rhythm Specialist Director, Electrophysiology Laboratory,
ECG S: A CASE-BASED APPROACH December 6, 2018 1 Faculty Disclosure Faculty: Lorne Gula MD, FRCPC Professor, Western University Cardiologist, Hearth Rhythm Specialist Director, Electrophysiology Laboratory,
UPDATE ON THE MANAGEMENTACUTE CORONARY SYNDROME. DR JULES KABAHIZI, Psc (Rwa) Lt Col CHIEF CONSULTANT RMH/KFH 28 JUNE18
 Lt Col CHIEF CONSULTANT RMH/KFH 28 JUNE18") UPDATE ON THE MANAGEMENTACUTE CORONARY SYNDROME DR JULES KABAHIZI, Psc (Rwa) Lt Col CHIEF CONSULTANT RMH/KFH 28 JUNE18 INTRODUCTION The clinical entities that comprise acute coronary syndromes (ACS)-ST-segment
UPDATE ON THE MANAGEMENTACUTE CORONARY SYNDROME DR JULES KABAHIZI, Psc (Rwa) Lt Col CHIEF CONSULTANT RMH/KFH 28 JUNE18 INTRODUCTION The clinical entities that comprise acute coronary syndromes (ACS)-ST-segment
Common Codes for ICD-10
 Common Codes for ICD-10 Specialty: Cardiology *Always utilize more specific codes first. ABNORMALITIES OF HEART RHYTHM ICD-9-CM Codes: 427.81, 427.89, 785.0, 785.1, 785.3 R00.0 Tachycardia, unspecified
Common Codes for ICD-10 Specialty: Cardiology *Always utilize more specific codes first. ABNORMALITIES OF HEART RHYTHM ICD-9-CM Codes: 427.81, 427.89, 785.0, 785.1, 785.3 R00.0 Tachycardia, unspecified
DAY1_CARDIOVASCULAR PRACTICE QUESTIONS
 DAY1_CARDIOVASCULAR PRACTICE QUESTIONS 1 P age 1. A 59-year-old male is admitted complaining of chest pain and dyspnea. ST elevation and T-wave inversion were seen on the ECG in V2, V3, and V4. IV thrombolytic
DAY1_CARDIOVASCULAR PRACTICE QUESTIONS 1 P age 1. A 59-year-old male is admitted complaining of chest pain and dyspnea. ST elevation and T-wave inversion were seen on the ECG in V2, V3, and V4. IV thrombolytic
DEPARTMENT NAME PRE-PARTICIPATION SCREENING THE SPORTS PHYSICAL
 PRE-PARTICIPATION SCREENING THE SPORTS PHYSICAL Michele Krenek, MSN, RN, FNP-C TCHAPP Conference, Houston, TX April 4, 2019 PRE-PARTICIPATION SPORTS SCREENING According to the AHA the definition of the
PRE-PARTICIPATION SCREENING THE SPORTS PHYSICAL Michele Krenek, MSN, RN, FNP-C TCHAPP Conference, Houston, TX April 4, 2019 PRE-PARTICIPATION SPORTS SCREENING According to the AHA the definition of the
Introduction to ECG Gary Martin, M.D.
 Brief review of basic concepts Introduction to ECG Gary Martin, M.D. The electrical activity of the heart is caused by a sequence of rapid ionic movements across cell membranes resulting first in depolarization
Brief review of basic concepts Introduction to ECG Gary Martin, M.D. The electrical activity of the heart is caused by a sequence of rapid ionic movements across cell membranes resulting first in depolarization