ACUTE CORONARY SYNDROME
|
|
|
- Rudolf Bryant
- 5 years ago
- Views:
Transcription







1 12 LEAD ECG INTERPRETATION in ACUTE CORONARY SYNDROME WAYNE W RUPPERT, CVT, CCCC, NREMT P Cardiovascular C di l Clinical Cli i l Coordinator C di t Bayfront Health Dade City Dade City, FL Education Specialist St. Joseph s Hospital Tampa, FL Curriculum Development: Didactic Materials: Practical Electrocardiography by Galen Wagner, MD and Henry J. L. Marriott, MD Practical Electrophysiology by Richard Fogoros, MD 70+ current Medical Journal article citations: primary sources NEJM, JACC, JAMA, AHA Circulation, + others CASE STUDIES from St. Joseph s Hospital CARDIAC CATH LAB 1997 TODAY PowerPoint presentation converted to TEXTBOOK in Wayne W Ruppert, CVT, CCCC, NREMT-P Cardiovascular Clinical Coordinator, Bayfront Health Dade City BarnesandNoble.com Amazon.com wayne.ruppert@bayfronthealth.com 1








2 TEXTBOOK REVIEWED BY: Joseph P. Ornato, MD, FACP, FACEP, FACC, Professor and Chairman, Department of Emergency Medicine, Medical College of Virginia Virginia Commonwealth University Humberto Coto, MD, FACP, FACC, Chief of Cardiology, St. Joseph s Hospital Matthew Glover, MD, FACP, FACC, Interventional Cardiologist, St. Joseph s Hospital Xavier Prida, Pid MD, FACP, FACC, Interventional ti lcardiologist, i St. Joseph s Hospital Charles Sand, MD, FACP, FACEP, Emergency Department Physician, St. Joseph s Hospital 2










3 3








4 4











5 5






. 6")


6 ACUTE MITRAL VALVE RUPTURE USUALLY OCCURS 7-10 DAYS POST EXTENSIV (e.g.: INFERIOR POSTERIOR LATERAL MI). 6









7 7








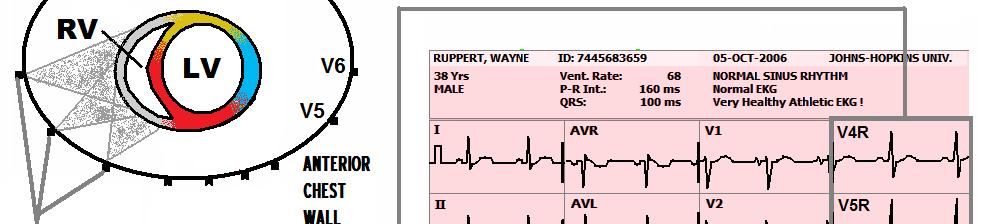
8 The 12 Lead ECG To SEE the RIGHT VENTRICLE and the POSTERIOR WALL, you must do an 18 LEAD ECG! The standard 12 Lead ECG has TWO The significant 18 Lead BLIND ECG SPOTS: - RIGHT VENTRICLE - POSTERIOR WALL of Left Ventricle 8


 an INVALUABLE ASSET for ALL MEDICAL PROFESSIONALS who")
9 To do this with a STANDARD 12 Lead ECG machine, FIRST, do you 12 Lead ECG in the traditional manner, and then you will REPOSITION the CHEST LEADS like this.... INDICATIONS for an 18 LEAD ECG include whenever you see: - INFERIOR WALL STEMI - ST DEPRESSION in any of the ANTERIOR LEADS (V1 V4) an INVALUABLE ASSET for ALL MEDICAL PROFESSIONALS who provide direct care to STEMI patients! 9










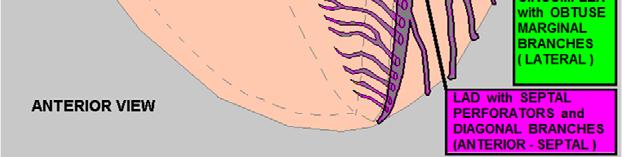
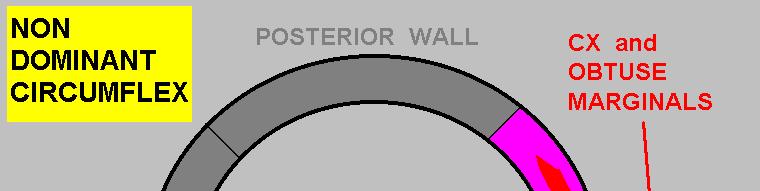
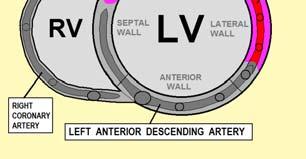
10 Which Coronary Artery typically Supplies the ANTERIOR WALL? 10




11 11


, CONSIDER the possibility of POSTERIOR WALL")

12 POSTERIOR WALL MI usually accompanies INFERIOR and/or LATERAL WALL MI!!! POSTERIOR WALL MI usually accompanies INFERIOR and/or LATERAL WALL MI!!!.... On rare occasions, we see isolated cases of POSTERIOR WALL MI Whenever your patient s ECG exhibits ST DEPRESSION in any of the ANTERIOR LEADS (V1-V4), CONSIDER the possibility of POSTERIOR WALL STEMI!!... To DIGANOSE Posterior Wall STEMI, we should see LEADS V7 V9!! 12




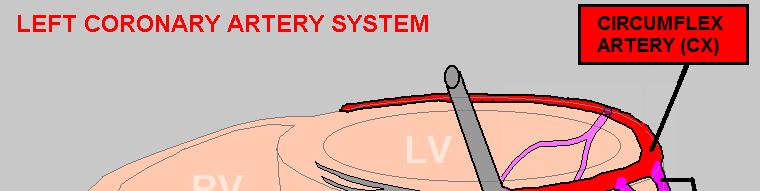



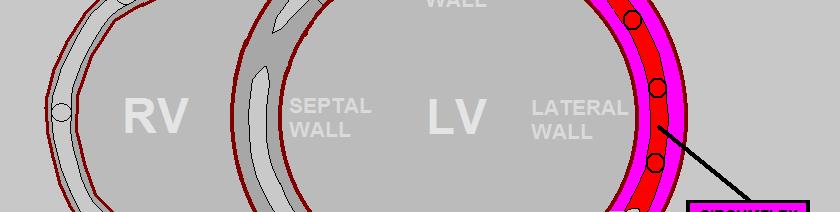

13 Which Coronary Artery typically Supplies the LATERAL WALL? 13










14 14







15 When LEAD AVR shows ST Elevation: - STEMI: consider occlusion of the Left Main Coronary Artery. : 15




16 When LEAD AVR shows ST Elevation: - STEMI: consider occlusion of the Left Main Coronary Artery. - NSTEMI and Unstable Angina consider LMCA Occlusion or TRIPLE VESSEL DISEASE Which CORONARY ARTERY usually supplies the INFERIOR WALL? 16


17 Because the RCA feeds the INFERIOR WALL in 75-80% of the population, AND it also feeds the RIGHT VENTRICLE, in every case of INFERIOR WALL MI, there is a high probability that RIGHT VENTRICULAR MI is ALSO present!!! IN EVERY CASE of INFERIOR WALL STEMI You must first RULE OUT RIGHT VENTRICULAR MI BEFORE giving any: - NITROGLYCERIN - Dieuretics NITROGLYCERIN is a CLASS III CONTRINDICATION in RIGHT VENTRICULAR MI!!* So when you see INFERIOR WALL STEMI..... It WILL precipitate PROFOUND HYPOTENSION! * A.H.A. ACLS




18 18



19 INFERIOR WALL STEMI --- summary: 75-80% caused by RCA OCCLUSION, think: - minimal LV Pump failure - Right Ventricular MI -- EXTREME sensitivity to NITRATES : 10-15% caused by CIRCUMFLEX OCCLUSION, think: - PROFOUND PUMP FAILURE - CARDIOGENIC SHOCK - PULMONARY EDEMA - CARDIAC ARREST 19





20 20





21 21








22 37 y/o male Chief Complaint: Lightheadedness, Palpitations, Shortness of Breath HPI: Sudden onset of above symptoms approx. 1 hour ago PMH: HTN (non compliant) 22


 -LOOK FOR DELTA WAVES Physician correctly")


23 37 y/o male PE: Alert, oriented, restless, cool, pale, dry skin. PERL, No JVD, Lungs clear. Abd soft non tender, Extremities: WNL, no edema Meds: None, NKDA VS: BP 106/50, P 180, R 26, SAO2 93% -NOTE IRREGULARITY OF RHYTHM - (SUGGESTIVE of A-FIB) -LOOK FOR DELTA WAVES Physician correctly identified Atrial Fibrillation with Rapid Ventricular Response. However did NOT identify the Wolff- Parkinson-White component. Patient was given Diltiazem promptly converted to - VENTRICULAR FIBRILLATION. 23



 -LOOK FOR DELTA")

 FOR")

24 CHARACTERISTICS of W-P-W with Afib & RVR: - WIDE COMPLEX TACHYCARDIA - IRREGULARLY IRREGULAR R R INTERVALS!! -NOTE IRREGULARITY OF RHYTHM - (SUGGESTIVE of A-FIB) -LOOK FOR DELTA WAVES NO AV NODAL BLOCKERS ( e.g. ADENOSINE, CALCIUM CHANNEL BLOCKERS) FOR WIDE COMPLEX TACHYCARDIAS THAT COULD BE ATRIAL FIBRILLATION with Pre-Excitation i (W-P-W W) 24








25 25











26 26







27 27






28 28





29 QT CORRECTION FORMULAS: Bazett s Fredericia Framingham Rautaharju QTc=QT/ RR QTc=QT/(RR)1/3 QTc=QT+0.154(1 RR) QTc=656/(1+HR/100) 29
 *P. Rautaharju, et al, Standardization and Interpretation of the ECG, Part IV JACC2009;53, no. 11:982 991 You get dispatched to a grocery store for seizures.")

30 ECG Indicators of Long QT Syndrome: QTc 460ms or longer in females* QTc 450ms or longer in males* T wave alterans U waves >100% of the T wave U waves merged with T waves U waves >0.1mv (1mm on standard calibrated ECG) *P. Rautaharju, et al, Standardization and Interpretation of the ECG, Part IV JACC2009;53, no. 11: You get dispatched to a grocery store for seizures. You find a 22 year old female alert and oriented to person, place and time. Witnesses describe a brief grand-mal seizure, then woke up and was alert. She has a history of seizures, and is on Cerebyx. WHEN LQTS IS SUSPECTED, TAKE THE FOLLOWING PRECAUTIONS.... WHEN THE QUICK PEEK METHOD for QT INTERAL EVALUATION IS APPLIED TO THE ABOVE ECG, WHAT IS THE RESULT? Etiology of Long QT Syndromes: Congenital (14 known subtypes) Genetic mutation results in abnormalities of cellular ion channels Acquired Drug Induced Metabolic/electrolyte induced Very low energy diets / anorexia CNS & Autonomic nervous system disorders Miscellaneous Coronary Artery Disease Mitral Valve Prolapse 30



31 If patient has a PROLONGED Q-T INTERVAL, AVOID DRUGS THAT LENGTHEN THE Q-T. Such drugs include: -Amiodarone -Ritalin -Procainamide -Benadryl -Levaquin -Haloperidol -Erythromycin -Thorazine -Norpace -Propulcid -Tequin..... AND MANY MORE & 31



32 When ECG Indicators of Long QT Synrome are present: Obtain a thorough patient history, to rule out incidence of syncope and family history of sudden death/ near sudden death. Evaluate patient s meds list for meds that prolong the QT Interval. Rule out hypothermia Rule out CVA Evaluate the patient s electrolyte levels, and MONITOR PATIENT S ECG FOR RUNS OF TORSADES Consider expert consult (electrophysiologist) to rule out LQTS Q: What is the ideal medication to treat Torsades? A: Magnesium Sulfate, 1 2 grams over 5 60 minutes (AHA ACLS) HERNANDO COUNTY FIRE RESCUE PROTOCOL: Torsades Mag Sulphate (9.21) 2 gm IV over 10 minuntes 32




33 15 year old male, suffered sudden cardiac arrest. Successful out of hospital resuscitation with CPR / AED. His ECG is shown below: EP STUDY REVEALS ABNORMAL AFTER DEPOLARIZATION. PATIENT RECEIVED ICD. ABSOLUTELY NO DRUGS THAT PROLONG THE Q-T INTERVAL!! 33







34 34



35 35
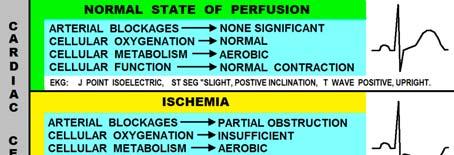







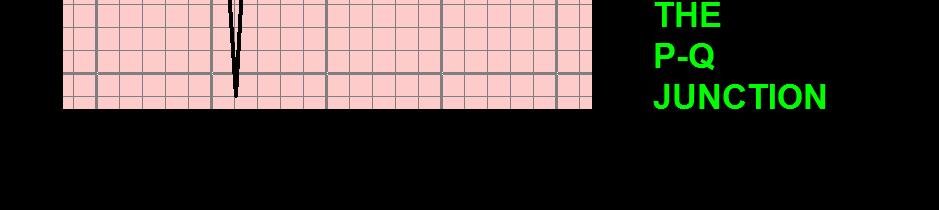
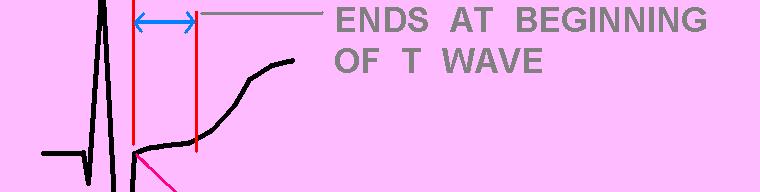
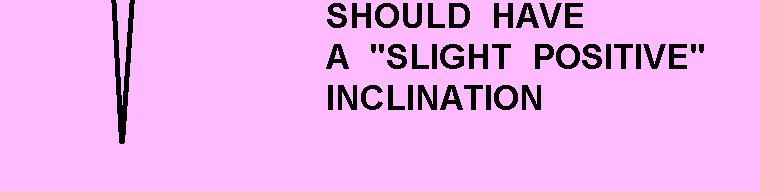
36 CHANGES ASSOCIATED WITH CELLULAR PERFUSION INVOLVING THE: QRS J point ST Segment T wave BOOK PAGE: 70 36




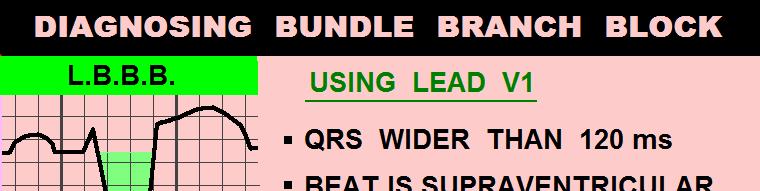
37 ECG EVALUATION for ACS: STEP 1: EVALUATE WIDTH of QRS IF THE QRS IS TOO WIDE ( GREATER THAN 120 ms ) BOOK PAGE: IS the QRS morphology: LEFT BUNDLE BRANCH BLOCK OR RIGHT BUNDLE BRANCH BLOCK????? 37








38 WIDE QRS COMPLEXES ALTER THE J POINTS ST SEGMENTS T WAVES Of the ECG... BOOK PAGE: 74 38

 :")




39 IF THE QRS COMPLEXES ON THE EKG ARE OF NORMAL WIDTH (<120 ms) : BOOK PAGE: 80 ALL KINDS of WEIRD ST SEGMENT and T WAVE VARIATIONS.... ALL CAN SPELL T R O U B L E. IF IT S NOT NORMAL, it s ABNORMAL! BOOK PAGE: 83 39




40 ECG COMPUTER DOES NOT NOTICE THE CONVEX J T APEX SEGMENTS! 40









41 HYPERACUTE T WAVES BOOK PAGE: 88 41









42 Cath Lab findings: Wayne W Ruppert, CVT, CCCC, NREMT-P Cardiovascular Clinical Coordinator, Bayfront Health Dade City wayne.ruppert@bayfronthealth.com 42
No.")
43 ECG CRITERIA for DIAGNOSIS of STEMI: (ST J POINT) *LEADS V2 and V3: MALES AGE 40 and up 20mm 2.0 (MALES LESS THAN mm) FEMALES 1.5 mm ALL OTHER LEADS: 1.0 mm or more, in TWO or more CONTIGUOUS LEADS * P. Rautaharju et al, Standardization and Interpretation of the ECG, JACC 2009;(53)No.11: ST SEGMENT ELEVATION: Reciprocal S T Segment Depression may or may not be present during AMI. The presence of S T Depression on an EKG which exhibits significant S T elevation is a fairly reliable indicator that AMI is the diagnosis. 3 COMMON PATTERNS of ST SEGMENT ELEVATION From ACUTE MI: However the lack of Reciprocal S T Depression DOES NOT rule out AMI. 43










44 44







45 HCFD PROTOCOL CARDIOGENIC SHOCK: Dopamine drip: (400 mg/250cc/d5w or premix bag) start 5 mcg/kg/min and titrate to achieve a blood pressure of 100 systolic. Max of 20 mcg/kg/min 45


46 46






47 THERE ARE TWO IMPORTANT CLUES that the patient s BLOCKAGE is in the PROXIMAL LEFT ANTERIOR DESCENDING ARTERY: 1. When ST elevation is noted in leads I and avl in cases of ANTERIOR WALL STEMI, it is a good indicator that the FIRST DIAGONAL BRANCH is included in the zone of infarction. RECIPROCAL ST DEPRESSION in the INFERIOR LEADS (II, III, and/or avf) is an indication that the LAD is blocked proximal to the FIRST DIAGONAL BRANCH. [1] [1] Use of the Electrocardiogram in Acute Myocardial Infarction, Zimetbaum, et al, NEJM 348:






48 PLUS: EXTENSION OF THROMBUS LOAD INTO THE LEFT MAIN CORONARY ARTERY.... WHO SHOULD GO TO THE CATH LAB FIRST? And.... WHAT WOULD YOU DO WITH THE PATIENT WHO DID NOT GO TO THE CATH LAB? 48









49 PATIENT A: PATIENT B: ST ELEVATION in Lead AVR With STEMI..... THINK LEFT MAIN CORONARY ARTERY OCCLUSION! 49









50 Despite the dismal mortality rate associated with STEMI from total LMCA occlusion, this patient t survived and was later discharged. His EF is estimated at approximately 30%. He received an ICD, and is currently stable. 50







51 INFERIOR WALL MI: ALWAYS RULE OUT RIGHT VENTRICULAR MI BEFORE GIVING ANY NITRATES!! 51




52 52






53 53







54 If this patient becomes HYPOTENSIVE









55 55









56 BRUGADA SYNDROME and Other Infarction Mimics 56







57 TEST QUESTION # 32 57








58 58





59 My top two reasons for giving everything in life the best I have to offer. 59
ACUTE CORONARY SYNDROME
 12 LEAD ECG INTERPRETATION in ACUTE CORONARY SYNDROME WAYNE W RUPPERT, CVT, CCCC, NREMT-P Cardiovascular Clinical Coordinator Bayfront Health Seven Rivers Crystal River, FL Education Specialist St. Joseph
12 LEAD ECG INTERPRETATION in ACUTE CORONARY SYNDROME WAYNE W RUPPERT, CVT, CCCC, NREMT-P Cardiovascular Clinical Coordinator Bayfront Health Seven Rivers Crystal River, FL Education Specialist St. Joseph
STAT 12 Lead ECG Workshop: Basics & ACS
 STAT 12 Lead ECG Workshop: Basics & ACS Part 2: Acute Coronary Syndrome WAYNE W RUPPERT, CVT, CCCC, NREMT-P Cardiovascular Coordinator Bayfront Health Seven Rivers Crystal River, Florida Interventional
STAT 12 Lead ECG Workshop: Basics & ACS Part 2: Acute Coronary Syndrome WAYNE W RUPPERT, CVT, CCCC, NREMT-P Cardiovascular Coordinator Bayfront Health Seven Rivers Crystal River, Florida Interventional
Wayne Ruppert and Dr. James Irwin, St Joseph s Hospital, Tampa, FL 2006
 The EMS 12 Lead 101 Wayne W Ruppert, CVT, CCCC, NREMT-P Interventional Cardiovascular Technologist Cardiovascular Coordinator Bayfront Health Seven Rivers Welcome! Wayne Ruppert and Dr. James Irwin, St
The EMS 12 Lead 101 Wayne W Ruppert, CVT, CCCC, NREMT-P Interventional Cardiovascular Technologist Cardiovascular Coordinator Bayfront Health Seven Rivers Welcome! Wayne Ruppert and Dr. James Irwin, St
A walk through a STEMI
 A walk through a STEMI M.M. s Story Kim Robison Ashley Corcoran Situation M.M. is an 82 year old male brought in by private vehicle on 10/22/17 to the Emergency Department Pt. c/o left arm numbness, pain
A walk through a STEMI M.M. s Story Kim Robison Ashley Corcoran Situation M.M. is an 82 year old male brought in by private vehicle on 10/22/17 to the Emergency Department Pt. c/o left arm numbness, pain
12 Lead ECGs: Ischemia, Injury & Infarction. Kevin Handke NRP, FP-C, CCP, CMTE STEMI Coordinator Flight Paramedic
 12 Lead ECGs: Ischemia, Injury & Infarction Kevin Handke NRP, FP-C, CCP, CMTE STEMI Coordinator Flight Paramedic None Disclosures Objectives Upon completion of this program the learner will be able to
12 Lead ECGs: Ischemia, Injury & Infarction Kevin Handke NRP, FP-C, CCP, CMTE STEMI Coordinator Flight Paramedic None Disclosures Objectives Upon completion of this program the learner will be able to
Observation Medicine ECG Instructor Workshop session 2 Serial 12 Lead ECG Interpretation
 American College of Cardiology 20 th Congress 2017 Observation Medicine ECG Instructor Workshop session 2 Serial 12 Lead ECG Interpretation Part 1 By: Wayne W Ruppert, CVT, CCCC, NREMT-P This curriculum
American College of Cardiology 20 th Congress 2017 Observation Medicine ECG Instructor Workshop session 2 Serial 12 Lead ECG Interpretation Part 1 By: Wayne W Ruppert, CVT, CCCC, NREMT-P This curriculum
All About STEMIs. Presented By: Brittney Urvand, RN, BSN, CCCC. Essentia Health Fargo Cardiovascular Program Manager.
 All About STEMIs Presented By: Brittney Urvand, RN, BSN, CCCC Essentia Health Fargo Cardiovascular Program Manager Updated 10/2/2018 None Disclosures Objectives Identify signs and symptoms of a heart attack
All About STEMIs Presented By: Brittney Urvand, RN, BSN, CCCC Essentia Health Fargo Cardiovascular Program Manager Updated 10/2/2018 None Disclosures Objectives Identify signs and symptoms of a heart attack
Huseng Vefali MD St. Luke s University Health Network Department of Cardiology
 Huseng Vefali MD St. Luke s University Health Network Department of Cardiology Learning Objectives Establish Consistent Approach to Interpreting ECGs Review Essential Cases for Paramedics and first responders
Huseng Vefali MD St. Luke s University Health Network Department of Cardiology Learning Objectives Establish Consistent Approach to Interpreting ECGs Review Essential Cases for Paramedics and first responders
ECG Basics Sonia Samtani 7/2017 UCI Resident Lecture Series
 ECG Basics Sonia Samtani 7/2017 UCI Resident Lecture Series Agenda I. Introduction II.The Conduction System III.ECG Basics IV.Cardiac Emergencies V.Summary The Conduction System Lead Placement avf Precordial
ECG Basics Sonia Samtani 7/2017 UCI Resident Lecture Series Agenda I. Introduction II.The Conduction System III.ECG Basics IV.Cardiac Emergencies V.Summary The Conduction System Lead Placement avf Precordial
12 Lead ECG Interpretation
 12 Lead ECG Interpretation Julie Zimmerman, MSN, RN, CNS, CCRN Significant increase in mortality for every 15 minutes of delay! N Engl J Med 2007;357:1631-1638 Who should get a 12-lead ECG? Also include
12 Lead ECG Interpretation Julie Zimmerman, MSN, RN, CNS, CCRN Significant increase in mortality for every 15 minutes of delay! N Engl J Med 2007;357:1631-1638 Who should get a 12-lead ECG? Also include
SIMPLY ECGs. Dr William Dooley
 SIMPLY ECGs Dr William Dooley Content Basic ECG interpretation pattern Some common (examined) abnormalities Presenting ECGs in context Setting up an ECG Setting up an ECG 1 V1-4 th Right intercostal space
SIMPLY ECGs Dr William Dooley Content Basic ECG interpretation pattern Some common (examined) abnormalities Presenting ECGs in context Setting up an ECG Setting up an ECG 1 V1-4 th Right intercostal space
REtrive. REpeat. RElearn Design by. Test-Enhanced Learning based ECG practice E-book
 Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning based ECG practice E-book REtrive REpeat RElearn Design by S I T T I N U N T H A N G J U I P E E R I Y A W A
Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning Test-Enhanced Learning based ECG practice E-book REtrive REpeat RElearn Design by S I T T I N U N T H A N G J U I P E E R I Y A W A
10 ECGs No Practitioner Can Afford to Miss. Objectives
 10 ECGs No Practitioner Can Afford to Miss Mary L. Dohrmann, MD Professor of Clinical Medicine Division of Cardiovascular Medicine University of Missouri School of Medicine No disclosures Objectives 1.
10 ECGs No Practitioner Can Afford to Miss Mary L. Dohrmann, MD Professor of Clinical Medicine Division of Cardiovascular Medicine University of Missouri School of Medicine No disclosures Objectives 1.
Case-Based Practical ECG Interpretation for the Generalist
 Case-Based Practical ECG Interpretation for the Generalist Paul D. Varosy, MD, FACC, FAHA, FHRS Director of Cardiac Electrophysiology VA Eastern Colorado Health Care System Associate Professor of Medicine
Case-Based Practical ECG Interpretation for the Generalist Paul D. Varosy, MD, FACC, FAHA, FHRS Director of Cardiac Electrophysiology VA Eastern Colorado Health Care System Associate Professor of Medicine
Arrhythmic Complications of MI. Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine
 Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
Case #1. 73 y/o man with h/o HTN and CHF admitted with dizziness and SOB Treated for CHF exacerbation with Lasix Now HR 136
 Tachycardias Case #1 73 y/o man with h/o HTN and CHF admitted with dizziness and SOB Treated for CHF exacerbation with Lasix Now HR 136 Initial Assessment Check Telemetry screen if pt on tele Telemetry
Tachycardias Case #1 73 y/o man with h/o HTN and CHF admitted with dizziness and SOB Treated for CHF exacerbation with Lasix Now HR 136 Initial Assessment Check Telemetry screen if pt on tele Telemetry
ECGs: Everything a finalist needs to know. Dr Amy Coulden As part of the Simply Finals series
 ECGs: Everything a finalist needs to know Dr Amy Coulden As part of the Simply Finals series Aims and objectives To be able to interpret basic ECG abnormalities To be able to recognise commonly tested
ECGs: Everything a finalist needs to know Dr Amy Coulden As part of the Simply Finals series Aims and objectives To be able to interpret basic ECG abnormalities To be able to recognise commonly tested
2009 Unit-Based Competencies
 2009 Unit-Based Competencies Alameda County Medical Center Highland Hospital Emergency Department Janis Farnholtz Provinse, RN, MS, CNS, CEN, ED Clinical Nurse Specialist Nurses play a pivotal role in
2009 Unit-Based Competencies Alameda County Medical Center Highland Hospital Emergency Department Janis Farnholtz Provinse, RN, MS, CNS, CEN, ED Clinical Nurse Specialist Nurses play a pivotal role in
12 Lead Electrocardiogram (ECG) PFN: SOMACL17. Terminal Learning Objective. References
 PFN: SOMACL17. Terminal Learning Objective. References") 12 Lead Electrocardiogram (ECG) PFN: SOMACL17 Slide 1 Terminal Learning Objective Action: Communicate knowledge of 12 Lead Electrocardiogram (ECG) Condition: Given a lecture in a classroom environment
12 Lead Electrocardiogram (ECG) PFN: SOMACL17 Slide 1 Terminal Learning Objective Action: Communicate knowledge of 12 Lead Electrocardiogram (ECG) Condition: Given a lecture in a classroom environment
SIMPLY ECGs. Dr William Dooley
 SIMPLY ECGs Dr William Dooley 1 No anatomy just interpretation 2 Setting up an ECG 3 Setting up an ECG 1 V1-4 th Right intercostal space at sternal border 2 V2-4 th Left intercostal space at sternal border
SIMPLY ECGs Dr William Dooley 1 No anatomy just interpretation 2 Setting up an ECG 3 Setting up an ECG 1 V1-4 th Right intercostal space at sternal border 2 V2-4 th Left intercostal space at sternal border
The Electrocardiogram part II. Dr. Adelina Vlad, MD PhD
 The Electrocardiogram part II Dr. Adelina Vlad, MD PhD Basic Interpretation of the ECG 1) Evaluate calibration 2) Calculate rate 3) Determine rhythm 4) Determine QRS axis 5) Measure intervals 6) Analyze
The Electrocardiogram part II Dr. Adelina Vlad, MD PhD Basic Interpretation of the ECG 1) Evaluate calibration 2) Calculate rate 3) Determine rhythm 4) Determine QRS axis 5) Measure intervals 6) Analyze
The Fundamentals of 12 Lead EKG. ECG Recording. J Point. Reviewing the Cardiac Conductive System. Dr. E. Joe Sasin, MD Rusty Powers, NRP
 The Fundamentals of 12 Lead EKG Dr. E. Joe Sasin, MD Rusty Powers, NRP SA Node Intranodal Pathways AV Junction AV Fibers Bundle of His Septum Bundle Branches Purkinje System Reviewing the Cardiac Conductive
The Fundamentals of 12 Lead EKG Dr. E. Joe Sasin, MD Rusty Powers, NRP SA Node Intranodal Pathways AV Junction AV Fibers Bundle of His Septum Bundle Branches Purkinje System Reviewing the Cardiac Conductive
2/1/2013. Poisoning pitfalls. The original pitfall
 The original pitfall Poisoning pitfalls Craig Smollin MD Associate Medical Director, California Poison Control System - SF Division Assistant Professor of Emergency Medicine, UCSF What will we talk about?
The original pitfall Poisoning pitfalls Craig Smollin MD Associate Medical Director, California Poison Control System - SF Division Assistant Professor of Emergency Medicine, UCSF What will we talk about?
Masqueraders of STEMI
 Masqueraders of STEMI Steven M. Costa, M.D. Assistant Professor Department of Medicine Division of Cardiology Scott & White Memorial Hospital and Clinic Texas A&M University Health Science Center Disclosures
Masqueraders of STEMI Steven M. Costa, M.D. Assistant Professor Department of Medicine Division of Cardiology Scott & White Memorial Hospital and Clinic Texas A&M University Health Science Center Disclosures
Common Codes for ICD-10
 Common Codes for ICD-10 Specialty: Cardiology *Always utilize more specific codes first. ABNORMALITIES OF HEART RHYTHM ICD-9-CM Codes: 427.81, 427.89, 785.0, 785.1, 785.3 R00.0 Tachycardia, unspecified
Common Codes for ICD-10 Specialty: Cardiology *Always utilize more specific codes first. ABNORMALITIES OF HEART RHYTHM ICD-9-CM Codes: 427.81, 427.89, 785.0, 785.1, 785.3 R00.0 Tachycardia, unspecified
Preface: Wang s Viewpoints
 AHA/ACCF/HRS Recommendations for the Standardization and Interpretation of the Electrocardiogram: Part IV, Ischemia and Infarction Presented by: WANG, TZONG LUEN, MD, PhD, JM, FACC, FESC, FCAPSC Professor,
AHA/ACCF/HRS Recommendations for the Standardization and Interpretation of the Electrocardiogram: Part IV, Ischemia and Infarction Presented by: WANG, TZONG LUEN, MD, PhD, JM, FACC, FESC, FCAPSC Professor,
Basic electrocardiography reading. R3 lee wei-chieh
 Basic electrocardiography reading R3 lee wei-chieh The Normal Conduction System Lead Placement avf Limb Leads Precordial Leads Interpretation Rate Rhythm Interval Axis Chamber abnormality QRST change What
Basic electrocardiography reading R3 lee wei-chieh The Normal Conduction System Lead Placement avf Limb Leads Precordial Leads Interpretation Rate Rhythm Interval Axis Chamber abnormality QRST change What
Disclosure. 3. ST depression indicative of ischemia is most commonly observed in leads: 1. V1-V2. 2. I and avl 3. V
 Interpreting Stress Induced Ischemia by ECG, Bundle Branch Block & Arrhythmias Disclosure Gregory S Thomas MD, MPH Medical Director, MemorialCare Heart & Vascular Institute, Long Beach Memorial Astellas
Interpreting Stress Induced Ischemia by ECG, Bundle Branch Block & Arrhythmias Disclosure Gregory S Thomas MD, MPH Medical Director, MemorialCare Heart & Vascular Institute, Long Beach Memorial Astellas
Arrhythmias. Sarah B. Murthi Department of Surgery University of Maryland Medical School R. Adams Cowley Shock Trauma Center
 Arrhythmias Sarah B. Murthi Department of Surgery University of Maryland Medical School R. Adams Cowley Shock Trauma Center 2012 Clinical Congress Presenter Disclosure Slide American College of Surgeons
Arrhythmias Sarah B. Murthi Department of Surgery University of Maryland Medical School R. Adams Cowley Shock Trauma Center 2012 Clinical Congress Presenter Disclosure Slide American College of Surgeons
Family Medicine for English language students of Medical University of Lodz ECG. Jakub Dorożyński
 Family Medicine for English language students of Medical University of Lodz ECG Jakub Dorożyński Parts of an ECG The standard ECG has 12 leads: six of them are considered limb leads because they are placed
Family Medicine for English language students of Medical University of Lodz ECG Jakub Dorożyński Parts of an ECG The standard ECG has 12 leads: six of them are considered limb leads because they are placed
ECG in coronary artery disease. By Sura Boonrat Central Chest Institute
 ECG in coronary artery disease By Sura Boonrat Central Chest Institute EKG P wave = Atrium activation PR interval QRS = Ventricle activation T wave= repolarization J-point EKG QT interval Abnormal repolarization
ECG in coronary artery disease By Sura Boonrat Central Chest Institute EKG P wave = Atrium activation PR interval QRS = Ventricle activation T wave= repolarization J-point EKG QT interval Abnormal repolarization
Atherosclerotic Heart Disease: Coronary Vessels, EKG Localization of STEMI and Complications/Derivatives for USMLE Step One
 Atherosclerotic Heart Disease: Coronary Vessels, EKG Localization of STEMI and Complications/Derivatives for USMLE Step One Howard J. Sachs, MD Associate Professor of Medicine University of Massachusetts
Atherosclerotic Heart Disease: Coronary Vessels, EKG Localization of STEMI and Complications/Derivatives for USMLE Step One Howard J. Sachs, MD Associate Professor of Medicine University of Massachusetts
Please check your answers with correct statements in answer pages after the ECG cases.
 ECG Cases ECG Case 1 Springer International Publishing AG, part of Springer Nature 2018 S. Okutucu, A. Oto, Interpreting ECGs in Clinical Practice, In Clinical Practice, https://doi.org/10.1007/978-3-319-90557-0
ECG Cases ECG Case 1 Springer International Publishing AG, part of Springer Nature 2018 S. Okutucu, A. Oto, Interpreting ECGs in Clinical Practice, In Clinical Practice, https://doi.org/10.1007/978-3-319-90557-0
Hot Topics in Cardiac Arrest. Should the patient go To the Cath Lab?
 Hot Topics in Cardiac Arrest Should the patient go To the Cath Lab? Tim Russert 1950-2008 Host of NBC s Meet the Press Sudden Cardiac Arrest : Autopsy showed plaque rupture in his LAD ( per LA Times,
Hot Topics in Cardiac Arrest Should the patient go To the Cath Lab? Tim Russert 1950-2008 Host of NBC s Meet the Press Sudden Cardiac Arrest : Autopsy showed plaque rupture in his LAD ( per LA Times,
Unknown ECGs for the Clinician
 Unknown ECGs for the Clinician 2016 Bryan Heart Fall Cardiology Conference Andrew Merliss, MD, FACC, CDRS, FHRS Director of Cardiac Arrhythmia Service Bryan Heart Disclaimer Advisory Board for Medtronic
Unknown ECGs for the Clinician 2016 Bryan Heart Fall Cardiology Conference Andrew Merliss, MD, FACC, CDRS, FHRS Director of Cardiac Arrhythmia Service Bryan Heart Disclaimer Advisory Board for Medtronic
Section V. Objectives
 Section V Landscape of an MI Objectives At the conclusion of this presentation the participant will be able to Outline a systematic approach to 12 lead ECG interpretation Demonstrate the process for determining
Section V Landscape of an MI Objectives At the conclusion of this presentation the participant will be able to Outline a systematic approach to 12 lead ECG interpretation Demonstrate the process for determining
Myocardial Infarction. Reading Assignment (p66-78 in Outline )
") Myocardial Infarction Reading Assignment (p66-78 in Outline ) Objectives 1. Why do ST segments go up or down in ischemia? 2. STEMI locations and culprit vessels 3. Why 15-lead ECGs? 4. What s up with avr?
Myocardial Infarction Reading Assignment (p66-78 in Outline ) Objectives 1. Why do ST segments go up or down in ischemia? 2. STEMI locations and culprit vessels 3. Why 15-lead ECGs? 4. What s up with avr?
Acute Coronary Syndromes Unstable Angina Non ST segment Elevation MI (NSTEMI) ST segment Elevation MI (STEMI)
 ST segment Elevation MI (STEMI)") Leanna R. Miller, RN, MN, CCRN-CSC, PCCN-CMC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Evaluate common abnormalities that mimic myocardial infarction. Identify
Leanna R. Miller, RN, MN, CCRN-CSC, PCCN-CMC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Evaluate common abnormalities that mimic myocardial infarction. Identify
Ekg pra pr c a tice D.HAMMOUDI.MD
 Ekg practice D.HAMMOUDI.MD Anatomy Revisited RCA (Right Coronary Artery) Right ventricle Inferior wall of LV Posterior wall of LV (75%) SA Node (60%) AV Node (>80%) LCA (Left Coronary Artery) Septal wall
Ekg practice D.HAMMOUDI.MD Anatomy Revisited RCA (Right Coronary Artery) Right ventricle Inferior wall of LV Posterior wall of LV (75%) SA Node (60%) AV Node (>80%) LCA (Left Coronary Artery) Septal wall
12 Lead ECG Interpretation: Color Coding for MI s
 12 Lead ECG Interpretation: Color Coding for MI s Anna E. Story, RN, MS Director, Continuing Professional Education Critical Care Nurse Online Instructional Designer 2004 Anna Story 1 Objectives review
12 Lead ECG Interpretation: Color Coding for MI s Anna E. Story, RN, MS Director, Continuing Professional Education Critical Care Nurse Online Instructional Designer 2004 Anna Story 1 Objectives review
Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016
 Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016 Disclosures: EKG Workshop Louis Mancano, MD Speaker has no disclosures
Pennsylvania Academy of Family Physicians Foundation & UPMC 43rd Refresher Course in Family Medicine CME Conference March 10-13, 2016 Disclosures: EKG Workshop Louis Mancano, MD Speaker has no disclosures
Initial Evaluation and Early Stabilization: Best Practices for the AF Patient Wayne Ruppert, CVT, CCCC, NREMT-P
 Initial Evaluation and Early Stabilization: Best Practices for the AF Patient Wayne Ruppert, CVT, CCCC, NREMT-P Cardiovascular Coordinator Bayfront Health Dade City This presentation is available for download
Initial Evaluation and Early Stabilization: Best Practices for the AF Patient Wayne Ruppert, CVT, CCCC, NREMT-P Cardiovascular Coordinator Bayfront Health Dade City This presentation is available for download
Rhythm Control: Is There a Role for the PCP? Blake Norris, MD, FACC BHHI Primary Care Symposium February 28, 2014
 Rhythm Control: Is There a Role for the PCP? Blake Norris, MD, FACC BHHI Primary Care Symposium February 28, 2014 Financial disclosures Consultant Medtronic 3 reasons to evaluate and treat arrhythmias
Rhythm Control: Is There a Role for the PCP? Blake Norris, MD, FACC BHHI Primary Care Symposium February 28, 2014 Financial disclosures Consultant Medtronic 3 reasons to evaluate and treat arrhythmias
Electrocardiography. Hilal Al Saffar College of Medicine,Baghdad University
 Electrocardiography Hilal Al Saffar College of Medicine,Baghdad University Which of the following is True 1. PR interval, represent the time taken for the impulse to travel from SA node to AV nose. 2.
Electrocardiography Hilal Al Saffar College of Medicine,Baghdad University Which of the following is True 1. PR interval, represent the time taken for the impulse to travel from SA node to AV nose. 2.
12 Lead ECG Interpretation: The Basics and Beyond
 12 Lead ECG Interpretation: The Basics and Beyond Cindy Weston, DNP, RN, CCRN, CNS-CC, FNP-BC Assistant Professor Texas A&M University College of Nursing cweston@tamhsc.edu Objectives Review the basics
12 Lead ECG Interpretation: The Basics and Beyond Cindy Weston, DNP, RN, CCRN, CNS-CC, FNP-BC Assistant Professor Texas A&M University College of Nursing cweston@tamhsc.edu Objectives Review the basics
By the end of this lecture, you will be able to: Understand the 12 lead ECG in relation to the coronary circulation and myocardium Perform an ECG
 By the end of this lecture, you will be able to: Understand the 12 lead ECG in relation to the coronary circulation and myocardium Perform an ECG recording Identify the ECG changes that occur in the presence
By the end of this lecture, you will be able to: Understand the 12 lead ECG in relation to the coronary circulation and myocardium Perform an ECG recording Identify the ECG changes that occur in the presence
You Don t Want to Miss This One! Focus on can t miss EKG tracings
 You Don t Want to Miss This One! Focus on can t miss EKG tracings Renaissance St. Louis Grand Hotel Convention Center October 23, 2014 David K. Tan, M.D., EMT-T, FAAEM EMS Section Chief, Division of Emergency
You Don t Want to Miss This One! Focus on can t miss EKG tracings Renaissance St. Louis Grand Hotel Convention Center October 23, 2014 David K. Tan, M.D., EMT-T, FAAEM EMS Section Chief, Division of Emergency
Cardiology III 1/22/2019. Disclosures - none. But first. Objectives. Ischemia EKG s. And second
 Disclosures - none Cardiology III Matthew K Hysell, MD Spectrum Health Lakeland St Joseph, MI 1 2 Objectives Review specific high-yield EKG patterns Ischemia Ischemia mimics Electrolytes Review Cardiac/CV
Disclosures - none Cardiology III Matthew K Hysell, MD Spectrum Health Lakeland St Joseph, MI 1 2 Objectives Review specific high-yield EKG patterns Ischemia Ischemia mimics Electrolytes Review Cardiac/CV
Sudden cardiac death: Primary and secondary prevention
 Sudden cardiac death: Primary and secondary prevention By Kai Chi Chan Penultimate Year Medical Student St George s University of London at UNic Sheba Medical Centre Definition Sudden cardiac arrest (SCA)
Sudden cardiac death: Primary and secondary prevention By Kai Chi Chan Penultimate Year Medical Student St George s University of London at UNic Sheba Medical Centre Definition Sudden cardiac arrest (SCA)
12 Lead EKG. The Basics
 12 Lead EKG The Basics Objectives Demonstrate proper 12 EKG lead placement Determine electrical axis Identify ST and T wave changes as they relate to myocardial ischemia Describe possible complications
12 Lead EKG The Basics Objectives Demonstrate proper 12 EKG lead placement Determine electrical axis Identify ST and T wave changes as they relate to myocardial ischemia Describe possible complications
12 LEAD EKG BASICS. By: Steven Jones, NREMT P CLEMC
 12 LEAD EKG BASICS By: Steven Jones, NREMT P CLEMC ECG Review Waves and Intervals P wave: the sequential activation (depolarization) of the right and left atria QRS complex: right and left ventricular
12 LEAD EKG BASICS By: Steven Jones, NREMT P CLEMC ECG Review Waves and Intervals P wave: the sequential activation (depolarization) of the right and left atria QRS complex: right and left ventricular
Understanding the 12-lead ECG, part II
 Bundle-branch blocks Understanding the 12-lead ECG, part II Most common electrocardiogram (ECG) abnormality Appears as a wider than normal S complex Occurs when one of the two bundle branches can t conduct
Bundle-branch blocks Understanding the 12-lead ECG, part II Most common electrocardiogram (ECG) abnormality Appears as a wider than normal S complex Occurs when one of the two bundle branches can t conduct
ECG Interpretation Made Easy
 ECG Interpretation Made Easy Dr. A Tageldien Abdellah, MSc MD EBSC Lecturer of Cardiology- Hull University Hull York Medical School 2007-2008 ECG Interpretation Made Easy Synopsis Benefits Objectives Process
ECG Interpretation Made Easy Dr. A Tageldien Abdellah, MSc MD EBSC Lecturer of Cardiology- Hull University Hull York Medical School 2007-2008 ECG Interpretation Made Easy Synopsis Benefits Objectives Process
MWLCEMS SYSTEM Continuing Education Packet Management of the Acute MI Patient
 MWLCEMS SYSTEM Continuing Education Packet Management of the Acute MI Patient In this CE we will discuss the patient presenting with an acute ST-Elevation Myocardial Infarction (STEMI) Definition: Myocardial
MWLCEMS SYSTEM Continuing Education Packet Management of the Acute MI Patient In this CE we will discuss the patient presenting with an acute ST-Elevation Myocardial Infarction (STEMI) Definition: Myocardial
McHenry Western Lake County EMS System Optional CE for EMT-B, Paramedics and PHRN s Bradycardia and Treatments Optional #7 2018
 McHenry Western Lake County EMS System Optional CE for EMT-B, Paramedics and PHRN s Bradycardia and Treatments Optional #7 2018 This month we will be looking at a specific ECG Rhythm and its treatments
McHenry Western Lake County EMS System Optional CE for EMT-B, Paramedics and PHRN s Bradycardia and Treatments Optional #7 2018 This month we will be looking at a specific ECG Rhythm and its treatments
The most common. hospitalized patients. hypotension due to. filling time Rate control in ICU patients may be difficult as many drugs cause hypotension
 Arrhythmias in the critically ill ICU patients: Approach for rapid recognition & management Objectives Be able to identify and manage: Atrial fibrillation with a rapid ventricular response Atrial flutter
Arrhythmias in the critically ill ICU patients: Approach for rapid recognition & management Objectives Be able to identify and manage: Atrial fibrillation with a rapid ventricular response Atrial flutter
ECG pre-reading manual. Created for the North West Regional EMET training program
 ECG pre-reading manual Created for the North West Regional EMET training program Author:- Dr Juan Carlos Ascencio-Lane juan.ascencio-lane@ths.tas.gov.au 1 Disclaimer This handbook has been created for
ECG pre-reading manual Created for the North West Regional EMET training program Author:- Dr Juan Carlos Ascencio-Lane juan.ascencio-lane@ths.tas.gov.au 1 Disclaimer This handbook has been created for
Acute Coronary Syndromes. Disclosures
 Acute Coronary Syndromes Disclosures I work for Virginia Garcia Memorial Health Center, Beaverton, OR. Jon Tardiff, BS, PA-C OHSU Clinical Assistant Professor And I am a medical editor for Jones & Bartlett
Acute Coronary Syndromes Disclosures I work for Virginia Garcia Memorial Health Center, Beaverton, OR. Jon Tardiff, BS, PA-C OHSU Clinical Assistant Professor And I am a medical editor for Jones & Bartlett
Electrical System Overview Electrocardiograms Action Potentials 12-Lead Positioning Values To Memorize Calculating Rates
 Electrocardiograms Electrical System Overview James Lamberg 2/ 74 Action Potentials 12-Lead Positioning 3/ 74 4/ 74 Values To Memorize Inherent Rates SA: 60 to 100 AV: 40 to 60 Ventricles: 20 to 40 Normal
Electrocardiograms Electrical System Overview James Lamberg 2/ 74 Action Potentials 12-Lead Positioning 3/ 74 4/ 74 Values To Memorize Inherent Rates SA: 60 to 100 AV: 40 to 60 Ventricles: 20 to 40 Normal
Difficult Data Definitions and Scenario s
 Difficult Data Definitions and Scenario s Presenter Disclosure Information Cornelia Anderson BSN, RN To following relationships exist related to this presentation: No Disclosures Objectives Discuss key
Difficult Data Definitions and Scenario s Presenter Disclosure Information Cornelia Anderson BSN, RN To following relationships exist related to this presentation: No Disclosures Objectives Discuss key
Chapter 9. Learning Objectives. Learning Objectives 9/11/2012. Cardiac Arrhythmias. Define electrical therapy
 Chapter 9 Cardiac Arrhythmias Learning Objectives Define electrical therapy Explain why electrical therapy is preferred initial therapy over drug administration for cardiac arrest and some arrhythmias
Chapter 9 Cardiac Arrhythmias Learning Objectives Define electrical therapy Explain why electrical therapy is preferred initial therapy over drug administration for cardiac arrest and some arrhythmias
It is what you will see most in practice and what you need to know thoroughly.
 Acute Myocardial Infarction: Pre-hospital Issues 2 CEUs By: Michelle E. Duffelmeyer, MD INTRODUCTION An in depth review of the pathophysiology, symptomatology, and treatment modalities for acute MI. It
Acute Myocardial Infarction: Pre-hospital Issues 2 CEUs By: Michelle E. Duffelmeyer, MD INTRODUCTION An in depth review of the pathophysiology, symptomatology, and treatment modalities for acute MI. It
Nathan Cade, MD Brandon Fainstad, MD Andrew Prouse, MD
 Nathan Cade, MD Brandon Fainstad, MD Andrew Prouse, MD OBJECTIVES 1. Identify the basic electrophysiology of the four causes of wide complex tachycardia. 2. Develop a simple framework for acute management
Nathan Cade, MD Brandon Fainstad, MD Andrew Prouse, MD OBJECTIVES 1. Identify the basic electrophysiology of the four causes of wide complex tachycardia. 2. Develop a simple framework for acute management
Electrocardiography for Healthcare Professionals. Chapter 14 Basic 12-Lead ECG Interpretation
 Electrocardiography for Healthcare Professionals Chapter 14 Basic 12-Lead ECG Interpretation 2012 The Companies, Inc. All rights reserved. Learning Outcomes 14.1 Discuss the anatomic views seen on a 12-lead
Electrocardiography for Healthcare Professionals Chapter 14 Basic 12-Lead ECG Interpretation 2012 The Companies, Inc. All rights reserved. Learning Outcomes 14.1 Discuss the anatomic views seen on a 12-lead
ECG Cases and Questions. Ashish Sadhu, MD, FHRS, FACC Electrophysiology/Cardiology
 ECG Cases and Questions Ashish Sadhu, MD, FHRS, FACC Electrophysiology/Cardiology 32 yo female Life Insurance Physical 56 yo male with chest pain Terminology Injury ST elevation Ischemia T wave inversion
ECG Cases and Questions Ashish Sadhu, MD, FHRS, FACC Electrophysiology/Cardiology 32 yo female Life Insurance Physical 56 yo male with chest pain Terminology Injury ST elevation Ischemia T wave inversion
CORONARY ARTERIES. LAD Anterior wall of the left vent Lateral wall of left vent Anterior 2/3 of interventricluar septum R & L bundle branches
 CORONARY ARTERIES RCA Right atrium Right ventricle SA node 55% AV node 90% Posterior wall of left ventricle in 90% Posterior third of interventricular septum 90% LAD Anterior wall of the left vent Lateral
CORONARY ARTERIES RCA Right atrium Right ventricle SA node 55% AV node 90% Posterior wall of left ventricle in 90% Posterior third of interventricular septum 90% LAD Anterior wall of the left vent Lateral
ECG CONVENTIONS AND INTERVALS
 1 ECG Waveforms and Intervals ECG waveforms labeled alphabetically P wave== represents atrial depolarization QRS complex=ventricular depolarization ST-T-U complex (ST segment, T wave, and U wave)== V repolarization.
1 ECG Waveforms and Intervals ECG waveforms labeled alphabetically P wave== represents atrial depolarization QRS complex=ventricular depolarization ST-T-U complex (ST segment, T wave, and U wave)== V repolarization.
EKG Competency for Agency
 EKG Competency for Agency Name: Date: Agency: 1. The upper chambers of the heart are known as the: a. Atria b. Ventricles c. Mitral Valve d. Aortic Valve 2. The lower chambers of the heart are known as
EKG Competency for Agency Name: Date: Agency: 1. The upper chambers of the heart are known as the: a. Atria b. Ventricles c. Mitral Valve d. Aortic Valve 2. The lower chambers of the heart are known as
Treatment of Arrhythmias in the Emergency Setting
 Treatment of Arrhythmias in the Emergency Setting Zian H. Tseng, M.D. Assistant Professor of Medicine Cardiac Electrophysiology Section Cardiology Division University of California, San Francisco There
Treatment of Arrhythmias in the Emergency Setting Zian H. Tseng, M.D. Assistant Professor of Medicine Cardiac Electrophysiology Section Cardiology Division University of California, San Francisco There
Other 12-Lead ECG Findings
 Other 12-Lead ECG Findings Left Atrial Enlargement Left atrial enlargement is illustrated by increased P wave duration in lead II, top ECG, and by the prominent negative P terminal force in lead V1, bottom
Other 12-Lead ECG Findings Left Atrial Enlargement Left atrial enlargement is illustrated by increased P wave duration in lead II, top ECG, and by the prominent negative P terminal force in lead V1, bottom
Cardiac Ischemia ECG Workshop
 Cardiac Ischemia ECG Workshop Classic, Confusing, and Confounding Patterns Amal Mattu, MD, NE Professor and Vice Chair Department of Emergency Medicine University of Maryland School of Medicine amalmattu@comcast.net
Cardiac Ischemia ECG Workshop Classic, Confusing, and Confounding Patterns Amal Mattu, MD, NE Professor and Vice Chair Department of Emergency Medicine University of Maryland School of Medicine amalmattu@comcast.net
ELECTROCARDIOGRAPH. General. Heart Rate. Starship Children s Health Clinical Guideline
 General Heart Rate QRS Axis T Wave Axis PR Interval according to Heart Rate & Age P Wave Duration and Amplitude QRS Duration according to Age QT Interval R & S voltages according to Lead & Age R/S ratio
General Heart Rate QRS Axis T Wave Axis PR Interval according to Heart Rate & Age P Wave Duration and Amplitude QRS Duration according to Age QT Interval R & S voltages according to Lead & Age R/S ratio
FANS Long QT Syndrome Investigation Protocol (including suspected mutation carriers)
") Clinical Features FANS Long QT Syndrome Investigation Protocol (including suspected mutation carriers) History Syncope or presyncope compatible with ventricular tachyarrhythmia, especially relating to
Clinical Features FANS Long QT Syndrome Investigation Protocol (including suspected mutation carriers) History Syncope or presyncope compatible with ventricular tachyarrhythmia, especially relating to
QT Interval: The Proper Measurement Techniques.
 In the name of God Shiraz E-Medical Journal Vol. 11, No. 2, April 2010 http://semj.sums.ac.ir/vol11/apr2010/88044.htm QT Interval: The Proper Measurement Techniques. Basamad Z*. * Assistant Professor,
In the name of God Shiraz E-Medical Journal Vol. 11, No. 2, April 2010 http://semj.sums.ac.ir/vol11/apr2010/88044.htm QT Interval: The Proper Measurement Techniques. Basamad Z*. * Assistant Professor,
ECG Workshop. Carolyn Shepherd And Anya Horne UWE Principles of Cardiac Care
 ECG Workshop Carolyn Shepherd And Anya Horne UWE Principles of Cardiac Care ECG workshop case study1 44 Year old male. Reports SOB, Lethargy, tiredness. PMH: Hypertension, nil else. What tests? What treatment?
ECG Workshop Carolyn Shepherd And Anya Horne UWE Principles of Cardiac Care ECG workshop case study1 44 Year old male. Reports SOB, Lethargy, tiredness. PMH: Hypertension, nil else. What tests? What treatment?
Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition
 Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition Table of Contents Volume 1 Chapter 1: Cardiovascular Anatomy and Physiology Basic Cardiac
Cardiovascular Nursing Practice: A Comprehensive Resource Manual and Study Guide for Clinical Nurses 2 nd Edition Table of Contents Volume 1 Chapter 1: Cardiovascular Anatomy and Physiology Basic Cardiac
12-Lead ECG Interpretation. Kathy Kuznar, RN, ANP
 12-Lead ECG Interpretation Kathy Kuznar, RN, ANP The 12-Lead ECG Objectives Identify the normal morphology and features of the 12- lead ECG. Perform systematic analysis of the 12-lead ECG. Recognize abnormalities
12-Lead ECG Interpretation Kathy Kuznar, RN, ANP The 12-Lead ECG Objectives Identify the normal morphology and features of the 12- lead ECG. Perform systematic analysis of the 12-lead ECG. Recognize abnormalities
BEDSIDE ECG INTERPRETATION
 BEDSIDE ECG INTERPRETATION Presented by: Ryan Dean, RN, MSN, CCRN, CCNS, CFRN Flight Nurse 2017 Based on presentations originally by Gennifer DePaoli, RN Objectives Hospital policies Electrical conduction
BEDSIDE ECG INTERPRETATION Presented by: Ryan Dean, RN, MSN, CCRN, CCNS, CFRN Flight Nurse 2017 Based on presentations originally by Gennifer DePaoli, RN Objectives Hospital policies Electrical conduction
MICS OF MYOCARDIAL ISCHEMIA AND INFARCTION REVISED FOR LAS VEGAS
 ECG MIMICS OF MYOCARDIAL ISCHEMIA AND INFARCTION 102.06.05 Tzong-Luen Wang MD, PhD, JM, FESC, FACC Professor. Medical School, Fu-Jen Catholic University Chief, Emergency Department, Shin-Kong Wu Ho-Su
ECG MIMICS OF MYOCARDIAL ISCHEMIA AND INFARCTION 102.06.05 Tzong-Luen Wang MD, PhD, JM, FESC, FACC Professor. Medical School, Fu-Jen Catholic University Chief, Emergency Department, Shin-Kong Wu Ho-Su
Understanding basics of EKG
 Understanding basics of EKG By Alula A.(R III) www.le.ac.uk Topic for discussion Understanding of cellular electrophysiology Basics Rate Rhythm Axis Intervals P wave QRS ST/T wave Abnormal EKGs Understanding
Understanding basics of EKG By Alula A.(R III) www.le.ac.uk Topic for discussion Understanding of cellular electrophysiology Basics Rate Rhythm Axis Intervals P wave QRS ST/T wave Abnormal EKGs Understanding
Ischemic heart disease
 Ischemic heart disease Introduction In > 90% of cases: the cause is: reduced coronary blood flow secondary to: obstructive atherosclerotic vascular disease so most of the time it is called: coronary artery
Ischemic heart disease Introduction In > 90% of cases: the cause is: reduced coronary blood flow secondary to: obstructive atherosclerotic vascular disease so most of the time it is called: coronary artery
ACLS Prep. Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep.
 November, 2013 ACLS Prep Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep. ACLS Prep Preparation is key to a successful ACLS experience.
November, 2013 ACLS Prep Preparation is key to a successful ACLS experience. Please complete the ACLS Pretest and Please complete this ACLS Prep. ACLS Prep Preparation is key to a successful ACLS experience.
WE ARE STEMI HUNTERS. LearningObjectives. I have no relevant disclosures. Myth: Jennifer Carlquist PA-C, ER CAQ
 WE ARE STEMI HUNTERS Jennifer Carlquist PA-C, ER CAQ Salinas Valley Memorial, ER Central Coast Cardiology, Specializing in EP LearningObjectives How to use pattern recognition to detect ischemia Triage
WE ARE STEMI HUNTERS Jennifer Carlquist PA-C, ER CAQ Salinas Valley Memorial, ER Central Coast Cardiology, Specializing in EP LearningObjectives How to use pattern recognition to detect ischemia Triage
A Review of Cardiac Pathophysiology and EKG. Jamie Dyson PT, DPT Kathy Swanick PT, DPT, OCS
 A Review of Cardiac Pathophysiology and EKG Jamie Dyson PT, DPT Kathy Swanick PT, DPT, OCS Cardiac Pathophysiology Coronary Artery Disease Congestive Heart Failure Valvular Heart Disease Athletic Heart
A Review of Cardiac Pathophysiology and EKG Jamie Dyson PT, DPT Kathy Swanick PT, DPT, OCS Cardiac Pathophysiology Coronary Artery Disease Congestive Heart Failure Valvular Heart Disease Athletic Heart
12 Lead ECG Workshop. Virginia Hass, DNP, FNP-C, PA-C Kim Newlin, CNS, ANP-C, FPCNA. California Association of Nurse Practitioners March 18, 2016
 12 Lead ECG Workshop Virginia Hass, DNP, FNP-C, PA-C Kim Newlin, CNS, ANP-C, FPCNA California Association of Nurse Practitioners March 18, 2016 Learning Objectives Identify key changes on the ECG which
12 Lead ECG Workshop Virginia Hass, DNP, FNP-C, PA-C Kim Newlin, CNS, ANP-C, FPCNA California Association of Nurse Practitioners March 18, 2016 Learning Objectives Identify key changes on the ECG which
CAN T MISS ECG FINDINGS L. THOMAS RICHARDS, MD ASSISTANT PROFESSOR OF EMERGENCY MEDICINE
 Topics in Emergency Medicine 2010 CAN T MISS ECG FINDINGS L. THOMAS RICHARDS, MD ASSISTANT PROFESSOR OF EMERGENCY MEDICINE OBJECTIVES Examine three common presentations to the ED which compel the EM provider
Topics in Emergency Medicine 2010 CAN T MISS ECG FINDINGS L. THOMAS RICHARDS, MD ASSISTANT PROFESSOR OF EMERGENCY MEDICINE OBJECTIVES Examine three common presentations to the ED which compel the EM provider
CASE 10. What would the ST segment of this ECG look like? On which leads would you see this ST segment change? What does the T wave represent?
 CASE 10 A 57-year-old man presents to the emergency center with complaints of chest pain with radiation to the left arm and jaw. He reports feeling anxious, diaphoretic, and short of breath. His past history
CASE 10 A 57-year-old man presents to the emergency center with complaints of chest pain with radiation to the left arm and jaw. He reports feeling anxious, diaphoretic, and short of breath. His past history
15 16 September Seminar W10O. ECG for General Practice
 15 16 September 2012 Seminar W10O ECG for General Practice Speaker: Ms Natasha Eaton ECG for General Practice Speaker: Natasha Eaton Cardiac CNC Executive Representative Electrocardiography The graphic
15 16 September 2012 Seminar W10O ECG for General Practice Speaker: Ms Natasha Eaton ECG for General Practice Speaker: Natasha Eaton Cardiac CNC Executive Representative Electrocardiography The graphic
Hanna K. Al-Makhamreh, M.D., FACC Interventional Cardiologist
 Hanna K. Al-Makhamreh, M.D., FACC Interventional Cardiologist Introduction. Basic Life Support (BLS). Advanced Cardiac Life Support (ACLS). Cardiovascular diseases (CVDs) are the number one cause of death
Hanna K. Al-Makhamreh, M.D., FACC Interventional Cardiologist Introduction. Basic Life Support (BLS). Advanced Cardiac Life Support (ACLS). Cardiovascular diseases (CVDs) are the number one cause of death
Dysrhythmias 11/7/2017. Disclosures. 3 reasons to evaluate and treat dysrhythmias. None. Eliminate symptoms and improve hemodynamics
 Dysrhythmias CYDNEY STEWART MD, FACC NOVEMBER 3, 2017 Disclosures None 3 reasons to evaluate and treat dysrhythmias Eliminate symptoms and improve hemodynamics Prevent imminent death/hemodynamic compromise
Dysrhythmias CYDNEY STEWART MD, FACC NOVEMBER 3, 2017 Disclosures None 3 reasons to evaluate and treat dysrhythmias Eliminate symptoms and improve hemodynamics Prevent imminent death/hemodynamic compromise
DR QAZI IMTIAZ RASOOL OBJECTIVES
 PRACTICAL ELECTROCARDIOGRAPHY DR QAZI IMTIAZ RASOOL OBJECTIVES Recording of electrical events in heart Established electrode pattern results in specific tracing pattern Health of heart i. e. Anatomical
PRACTICAL ELECTROCARDIOGRAPHY DR QAZI IMTIAZ RASOOL OBJECTIVES Recording of electrical events in heart Established electrode pattern results in specific tracing pattern Health of heart i. e. Anatomical
2) Heart Arrhythmias 2 - Dr. Abdullah Sharif
 Heart Arrhythmias 2 - Dr. Abdullah Sharif") 2) Heart Arrhythmias 2 - Dr. Abdullah Sharif Rhythms from the Sinus Node Sinus Tachycardia: HR > 100 b/m Causes: o Withdrawal of vagal tone & Sympathetic stimulation (exercise, fight or flight) o Fever
2) Heart Arrhythmias 2 - Dr. Abdullah Sharif Rhythms from the Sinus Node Sinus Tachycardia: HR > 100 b/m Causes: o Withdrawal of vagal tone & Sympathetic stimulation (exercise, fight or flight) o Fever
Case 1. Case 2. Case 3
 Case 1 The correct answer is D. Occasionally, the Brugada syndrome can present similar morphologies to A and also change depending on the lead position but in the Brugada pattern the r is wider and ST
Case 1 The correct answer is D. Occasionally, the Brugada syndrome can present similar morphologies to A and also change depending on the lead position but in the Brugada pattern the r is wider and ST
12 Lead Acquisition and Interpretation APRIL 23 11:00 AM
 12 Lead Acquisition and Interpretation APRIL 23 11:00 AM Presented by : Jennifer Robson, Prehospital Care Specialist Dr. Don Eby, Local Medical Director Objectives Upon completion of this webinar, you
12 Lead Acquisition and Interpretation APRIL 23 11:00 AM Presented by : Jennifer Robson, Prehospital Care Specialist Dr. Don Eby, Local Medical Director Objectives Upon completion of this webinar, you
Study methodology for screening candidates to athletes risk
 1. Periodical Evaluations: each 2 years. Study methodology for screening candidates to athletes risk 2. Personal history: Personal history of murmur in childhood; dizziness, syncope, palpitations, intolerance
1. Periodical Evaluations: each 2 years. Study methodology for screening candidates to athletes risk 2. Personal history: Personal history of murmur in childhood; dizziness, syncope, palpitations, intolerance
Ablative Therapy for Ventricular Tachycardia
 Ablative Therapy for Ventricular Tachycardia Nitish Badhwar, MD, FACC, FHRS 2 nd Annual UC Davis Heart and Vascular Center Cardiovascular Nurse / Technologist Symposium May 5, 2012 Disclosures Research
Ablative Therapy for Ventricular Tachycardia Nitish Badhwar, MD, FACC, FHRS 2 nd Annual UC Davis Heart and Vascular Center Cardiovascular Nurse / Technologist Symposium May 5, 2012 Disclosures Research
A few new tools for better detection and understanding of STEMIs in the field.
 A few new tools for better detection and understanding of STEMIs in the field. Let s talk, prep and placement. Try to shoot for quality, consistency and no artifact! (looking sometimes for 1 or 2 mm changes)
A few new tools for better detection and understanding of STEMIs in the field. Let s talk, prep and placement. Try to shoot for quality, consistency and no artifact! (looking sometimes for 1 or 2 mm changes)
CRC 431 ECG Basics. Bill Pruitt, MBA, RRT, CPFT, AE-C
 CRC 431 ECG Basics Bill Pruitt, MBA, RRT, CPFT, AE-C Resources White s 5 th ed. Ch 6 Electrocardiography Einthoven s Triangle Chest leads and limb leads Egan s 10 th ed. Ch 17 Interpreting the Electrocardiogram
CRC 431 ECG Basics Bill Pruitt, MBA, RRT, CPFT, AE-C Resources White s 5 th ed. Ch 6 Electrocardiography Einthoven s Triangle Chest leads and limb leads Egan s 10 th ed. Ch 17 Interpreting the Electrocardiogram
EMT. Chapter 14 Review
 EMT Chapter 14 Review Review 1. All of the following are common signs and symptoms of cardiac ischemia, EXCEPT: A. headache. B. chest pressure. C. shortness of breath. D. anxiety or restlessness. Review
EMT Chapter 14 Review Review 1. All of the following are common signs and symptoms of cardiac ischemia, EXCEPT: A. headache. B. chest pressure. C. shortness of breath. D. anxiety or restlessness. Review