Mr Patrick Gladding. Specialist General Cardiology and Internal Medicine Auckland
|
|
|
- Ralf Sharp
- 5 years ago
- Views:
Transcription

1 Mr Patrick Gladding Specialist General Cardiology and Internal Medicine Auckland 16:30-17:25 WS #60: Individualising Hypertension Treatment - Intensive or Not? 17:35-18:30 WS #72: Individualising Hypertension Treatment - Intensive or Not? (Repeated)
2 Individualising Hypertension Treatment: Intensive or not? Dr. Patrick Gladding, MBChB, FRACP, PhD Ascot Cardiology
 and monitoring (mhealth) Targets SPRINT trial Lifestyle interventions (Functional Foods) Genomics and Personalised")
3 Hypertension update Outline New Guidelines Definitions and treatment thresholds Global risk, investigations (Pulse wave velocity) and monitoring (mhealth) Targets SPRINT trial Lifestyle interventions (Functional Foods) Genomics and Personalised Care



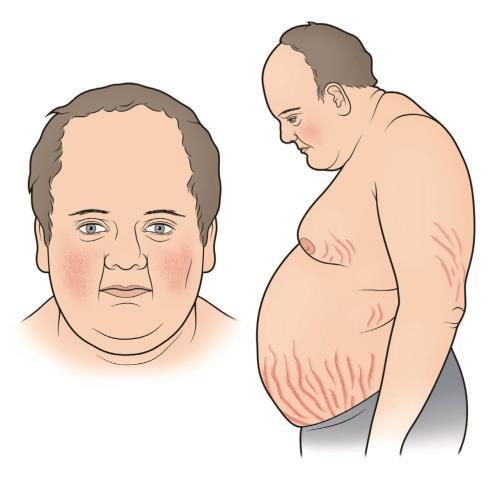






4 Secondary causes of Hypertension Aortic coarctation Cushings syndrome

5
6


7

8 Office BP White coat hypertension Ambulatory 24-hr BP (ABPM) Masked hypertension Home blood pressure monitoring Increased granularity White coat hypertension Feedback Dietary/Lifestyle and drug n=1 trials Adherence Personal control JAMA. 2014;312(8): patients 9mmHg SBP reduction with self-mx

9


10
11


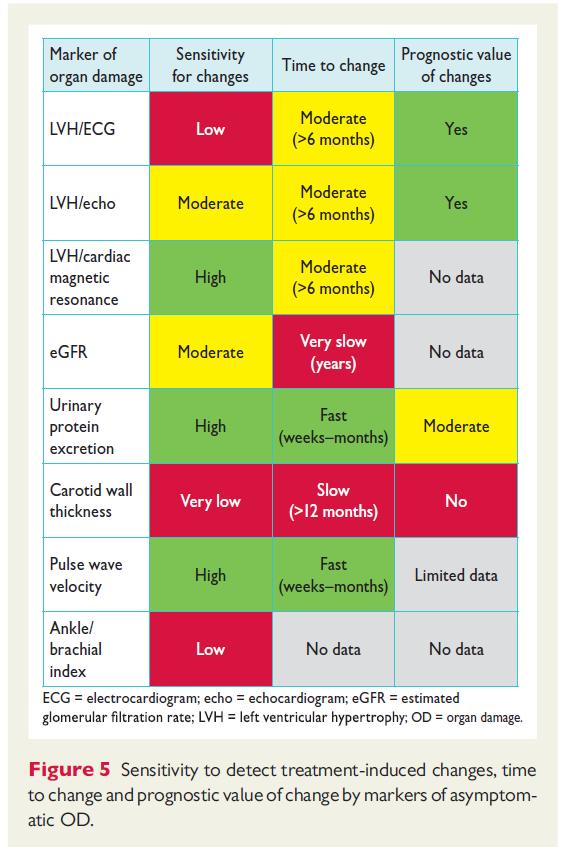
12 2 emerging techniques in echo to improve detection of end-organ damage: 1) LV strain; Deformation of the LV vs EF 2) LV mass


13

")

14 Hypertension update 76 yr old man Supine HTN orthostatic hypotension (~50mmHg) Arterial stiffness indicates lower central BP 14



15
16 JNC 8 Goal for people > 60 yrs should be a SBP < 150, DBP < 90
17 1466 older men and women For fit elderly patients, a high DBP (>90 mm Hg) was associated with a 50% increase in mortality The ultimate goal is personalized treatment so that we can avoid overtreatment of the frail, and undertreatment of the fit. By contrast, for frail elderly patients, a low DBP was associated with a 50% increased risk of dying during 15 year follow-up period

 occurred in 5.")
18 9361 patients (age, 50) with SBP of 130 to 180 mm Hg and high cardiovascular (CV) risk One or more: CV disease, CKD EGFR ml/minute/1.73 m2, 10-year Framingham CV risk 15%, or age 75 Patients with diabetes and stroke were excluded. Patients were randomized to either intensive or standard treatment (systolic BP targets, 120 or 140 mm Hg, respectively) The trial was terminated early after median follow-up of 3.3 years The primary composite outcome (MACE) occurred in 5.2% of intensivetreatment patients and 6.8% of standard-treatment patients (P<0.001)
19 First, the results should not be considered a mandate for people to run out and get treated so their blood pressures are below 120. Second, the potential benefits of lowering blood pressure must be weighed against harms. Third, we need more information about the balance of risks and benefits for each person so that the choice can be personalized.

 and less than 80 mmhg")
20 The ideal blood pressure for most people is likely to be below 120 mmhg systolic and 75 mmhg diastolic. The 2017 AHA/ACC guideline s recommended treatment goal is to reach office BP levels of less than 130mmHg (systolic) and less than 80 mmhg (diastolic) if pharmacotherapy is commenced.





21
22 Personalised Hypertension Management 80 year old woman seen in clinic. Presenting symptom of presyncope and palpitations. Office BP 190/90 on an ACEi/thiazide combination (Inhibace plus) as well as bisoprolol 2.5mg od. She takes ASA and a statin, has no T2DM, total cholesterol of 3.9, an HDL of 1.3 mmol/l. Creatinine 82 umol/l, caucasian, nonsmoker. Is she well treated? Should treatment be intensified? Is the SPRINT trial relevant? Is there an app for that????


23
24 Insert title of presentation here ABPM shows average BP 135/80 with a precipitous drop at around 1400 (see attached) to BP 105/66, when she often feels unwell. Diastolic BP <65mmHg is BAD
25 Personalised Hypertension Management 80 year old woman seen in clinic. Presenting symptom of presyncope and palpitations. Office BP 190/90 on an ACEi/thiazide combination (Inhibace plus) as well as bisoprolol 2.5mg od. She takes ASA and a statin, has no T2DM, total cholesterol of 3.9, an HDL of 1.3 mmol/l. Creatinine 82 umol/l, caucasian, nonsmoker. Is she well treated? NO. She is overtreated. Should treatment be intensified? NO Is the SPRINT trial relevant? YES and NO SPRINT score calculator NNT 267, NNH 30.
26 Personalised Hypertension Management 80 year old woman seen in clinic. Presenting symptom of presyncope and palpitations. Office BP 190/90 on an ACEi/thiazide combination (Inhibace plus) as well as bisoprolol 2.5mg od. She takes ASA and a statin, has no T2DM, total cholesterol of 3.9, an HDL of 1.3 mmol/l. Creatinine 82 umol/l, caucasian, nonsmoker. Inhibace + is halved I m a different person!


27 ios Android

28 Guidelines take with a grain of salt Increased risk of CV events with very low salt intake Guidelines based on averaging population N Engl J Med


29 Renal denervation therapy SYMPLICITY-3: Renal denervation therapy doesn t work, for unselected patients with HTN Renal artery stenosis

30 Age directed vs Renin directed Rx Individualise Rx based on other comorbidities Spironolactone for Resistant HTN

31


32 J Clin Pharmacol 1994;34:



33 Gladding et al. Personalized Medicine Journal. June 2015,Vol. 12, No. 3, Pages
34
35 Personalised Medicine in practice 35






36 Era of Mobile Health 36


37 Advanced ECG WiFi based ECG Ultraportable, $3,500 Deconvolutes ECG components Advanced pattern recognition, artificial intelligence ECG biological age 37

38 Advanced ECG for general practice Sensitive, high sampling frequency, accurate.
39 Case 43 year old man with dyspnoea, BP 220/140


40 Case



41 British Journal of General Practice 2007; 57: BMJ 1996;312:222 41
42 A-ECG LVSD Sensitivity 93-95%, Specificity 95% Southern X reimbursed


43
44 Conclusion Hypertension is common, often called the Silent Killer Requires personalised Care taking into account Global risk Age and comordities Guidelines not always applicable to the individual patient Emerging technologies for investigation of end-organ disease Lifestyle, diet, prevention paramount Functional foods Feedback, mhealth, Internet of Things (IoT) Limited new drug treatments, or procedures though these will be targeted Emerging role of genomics (not yet fully advocated)
45 Interactive Session: Hypertension and Personalised Care Dr. Patrick Gladding, MBChB, FRACP, PhD

46 Case: 26 year old with HTN on home BP monitor Ubiquitous home BP monitoring Checked BP on friend s mother s home BP machine Measurement high ABPM 169/101 No other PMHx Maternal Grandparents had HTN, Gfather had ESRF and HD Normal diet, no illicit drugs Mother did not have pre-eclampsia Normal FBC, Cr, TSH. 46
47 Case: 26 year old with HTN on home BP monitor What investigations would you order? 1. Urinalysis sediment, microalbumin/cr ratio 2. Renin/Aldosterone levels 3. Echocardiogram 4. Renal artery USS 5. All of the above 47
48 Case: 26 year old with HTN on home BP monitor What investigations would you order? 1. Urinalysis sediment, microalbumin/cr ratio 2. Renin/Aldosterone levels 3. Echocardiogram 4. Renal artery USS 5. All of the above 48
49 Case: 26 year old with HTN on home BP monitor Differential diagnosis for his age Secondary hypertension much more likely from structural reasons e.g. coarctation, PCKD, but acute renal injury, nephritis but also endocrine (hyperaldosteronism) FHx PCKD? Hereditary HTN 49

50 Case: Value of ubiquitous home BP monitoring Checked BP on friend s mother s home BP machine Measurement high ABPM 169/101 USS right renal hydronephrosis ACEi -?nephrectomy 50
51 Case: 56 year old man with longstanding hypertension 56 year old man with longstanding hypertension GORD, dyslipidaemia, TIA 2014?, abnormal LFTs - 3-4L beer/day Palmar desquamation reaction to indapamide ABPM average BP 145/87, whilst on Candesartan 16mg od Renal USS no renal artery stenosis, post void residual 80mls Echocardiogram: Mild basal septal hypertrophy Renin 744 (4 46), Aldosterone 134 (60 1,000) on ARB
52 Case: 56 year old man with longstanding hypertension
53 Case: 56 year old man How would you manage him? 1. Renin directed Rx - Bb 2. Add bendrofluazide 3. Add amlodipine 4. Counsel regarding EtOH 5. 1 or 3, and 4 Spironolactone for Resistant 53 HTN
54 Case: 56 year old man How would you manage him? 1. Renin directed Rx - Bb 2. Add bendrofluazide 3. Add amlodipine 4. Counsel regarding EtOH 5. 1 or 3, and 4 54 Spironolactone for Resistant HTN
55 Case: 56 year old man with longstanding hypertension Renin is a red herring, cannot be relied upon whilst taking antihtn meds, especially RAAS blockers Renin is also elevated in chronic EtOH Indapamide is a thiazide-like diuretic, as is bendrofluazide?class effect with desquamation Age on the cusp of the NICE guidelines so could get ACEi (<55yrs) or CCHB (>55yrs) however the big problem is in the ABPM

56 Case: Value of 24hr ABPM and diurnal measures Focus on alcohol Worrying diastolic nadir 40mmHg

57 Case: 56 year old man abstaining from alcohol
58 Case: 61 year old GP 61 year old GP, Hx of HTN on Rx 12L ECG normal AECG abnormal/cad and biological age Coronary angiogram mild-moderate CAD 58 Journal of Hypertension 2014, 32:
59 Case 61 year old GP What are the red arrows pointing to? 1.Acute coffee intake 2.Conn syndrome 3.Work stress 4.Normal diurnal variation 5.Phaeochromocytoma
60 Case: 61 year old GP What are the red arrows pointing to? 1.Acute coffee intake 2.Conn syndrome 3.Work stress 4.Normal diurnal variation 5.Phaeochromocytoma



61 Case 61 year old GP Work stress is associated with HTN Concurrent CAD Rx to lower target? Manage causes of stress, mindfulness 61 Journal of Hypertension 2014, 32:
62 Case: 56 year old wife of GP Emotional stress ABPM BP 166/97 (Grade II HTN) Was on Amlodipine 5mg Drug withheld 2 weeks: Renin 22, Aldo N Green mussel extract, celery extract J Clin Hypertens (Greenwich) Jan; 16(1): Journal of Hypertension 2014, 32:
63 Case: 56 year old wife of GP What is the next course of action? 1.Increase dose of CCHB 2.Bb 3.ACEi or ARB 4.Diuretic 5.Spirinolactone 63 Spironolactone for Resistant HTN
64 Case: 56 year old wife of GP What is the next course of action? 1.Increase dose of CCHB 2.Bb 3.ACEi or ARB 4.Diuretic 5.Spirinolactone 64 Spironolactone for Resistant HTN
. 2014 Jan; 16(1): 54 62.")
65 Case 56 year old wife of GP Emotional stress Was on Amlodipine 5mg ABPM BP 166/97 Renin 22, Aldo N Green mussel extract, celery extract Px Chlorthalidone 12.5mg od Pranayama Pranayama J Clin Hypertens (Greenwich) Jan; 16(1): Journal of Hypertension 2014, 32:
66 Case: 48 year old woman 48 year old woman with depression on Venlafaxine 225mg Mild dyslipidaemia Prior Hx of right sided breast cancer, partial mastectomy FHx of premature stroke Office BP 145/99 Normal Cr, ECG, renin/aldosterone ratio 66
67 Case: 48 year old woman How would you better define risk in view of BP? Advanced lipids Lp(a) CIMT CAC ETT CTCA 67
68 Case: 48 year old woman How would you better define risk in view of BP? Advanced lipids Lp(a) CIMT CAC ETT CTCA 68
69 Case: 48 year old woman What is the cause of her mild hypertension? 69

70 Case: Drug induced HTN 48 year old woman with depression started Venlafaxine, BP 145/99 Genomics indicated ADE WiFi BP max 133/95 70
71 Case:29 year old woman 29 year old woman, otherwise well, father adopted Normal weight, no EtOH No added salt, good sleep quality Office BP 140/90 on OCP 71 Journal of Hypertension 2009, 27:
72 What would you do next? 1. Stop the OCP, alternative Rx and retest her BP hr ABPM 3. Renin/Aldosterone 4. Renal USS 5. Renal denervation therapy
73 What would you do next? 1. Stop the OCP, alternative Rx and retest her BP hr ABPM 3. Renin/Aldosterone 4. Renal USS 5. Renal denervation therapy


74 Case: Incidental genomics 29 year old woman, otherwise well, father adopted Office BP 140/90 on OCP ABPM 132/85 deltaf508 carrier Genetic counselling Prenatal screening 3-4 cups of coffee per day associated with increased risk of MI and HTN in poor metabolisers Journal of Hypertension 2009, 27:
75 Case 54 year old man 54 year old man presents with MI HTN with known hypertensive retinopathy, mild-mod LVH on Echo BP 217/119 in 2014, started on Felodipine 10mg od Smoker Occasional methaphetamine user BP 170/90 on chlorthalidone 12.5mg od Moderate CAD on coronary angiography ASA/Ticagrelor/Statin/Bb/Chlorthalidone

76 Case 54 year old man - Potassium Renin <2 (4 46), Aldosterone 600 (60 1,000) Felodipine 10mg od Losartan + Thiazide 3.5 MI 3.4 F/up clinic Chlorthalidone stopped Atypical CP, dyspnoea Admitted to hospital TnI <15 K supp Atypical CP, dyspnoea Admitted to hospital Dx GORD Spironolactone Took P went to ED 2.9
77 Case: 54 year old man What is the diagnosis? 1.Acute coffee intake 2.Surreptitious thiazide use 3.Conn syndrome 4.Methaphetamine related hypokalaemia 5.Phaeochromocytoma

78 Case: Conn Syndrome What is the diagnosis? 1.Acute coffee intake 2.Surreptitious thiazide use 3.Conn syndrome Saline suppression test Renal vein sampling 4.Methaphetamine related hypokalaemia 5.Phaeochromocytoma
79 Thank you
Hypertension Management Controversies in the Elderly Patient
 Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Management of Hypertension and Consequences of non-compliance. Colin Edwards
 Management of Hypertension and Consequences of non-compliance Colin Edwards CARDIOLOGIST AHG May 2016 Outline 1. Consequences of poorly controlled hypertension 2. BP targets and anti-hypertensive drugs
Management of Hypertension and Consequences of non-compliance Colin Edwards CARDIOLOGIST AHG May 2016 Outline 1. Consequences of poorly controlled hypertension 2. BP targets and anti-hypertensive drugs
Hypertension diagnosis (see detail document) Diabetic. Target less than 130/80mmHg
 Diabetic. Target less than 130/80mmHg") Hypertension diagnosis (see detail document) Non-diabetic Diabetic Very elderly (older than 80 years) Target less than 140/90mmHg Target less than 130/80mmHg Consider SBP target less than 150mmHg Non-diabetic
Hypertension diagnosis (see detail document) Non-diabetic Diabetic Very elderly (older than 80 years) Target less than 140/90mmHg Target less than 130/80mmHg Consider SBP target less than 150mmHg Non-diabetic
Hypertension in 2015: SPRINT-ing ahead of JNC-8. MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic
 Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Jared Moore, MD, FACP
 Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Difficult-to-Control & Resistant Hypertension. Anthony Viera, MD, MPH, FAHA Professor and Chair
 Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
Hypertension and Cardiovascular Disease
 Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
Hypertension Pharmacotherapy: A Practical Approach
 Hypertension Pharmacotherapy: A Practical Approach Ronald Victor, MD Burns & Allen Chair in Cardiology Director, The Hypertension Center Associate Director, The Heart Institute Hypertension Center 1. 2.
Hypertension Pharmacotherapy: A Practical Approach Ronald Victor, MD Burns & Allen Chair in Cardiology Director, The Hypertension Center Associate Director, The Heart Institute Hypertension Center 1. 2.
Personalised Medicine in Practice. Dr. Patrick Gladding MBChB, PhD Cardiologist, NSH
 Personalised Medicine in Practice Dr. Patrick Gladding MBChB, PhD Cardiologist, NSH 1 Challenges of medicine in 21 st C Increasing demand Aging population Constrained, limited resources Inefficiency and
Personalised Medicine in Practice Dr. Patrick Gladding MBChB, PhD Cardiologist, NSH 1 Challenges of medicine in 21 st C Increasing demand Aging population Constrained, limited resources Inefficiency and
4/4/17 HYPERTENSION TARGETS: WHAT DO WE DO NOW? SET THE STAGE BP IN CLINICAL TRIALS?
 HYPERTENSION TARGETS: WHAT DO WE DO NOW? MICHAEL LEFEVRE, MD, MSPH PROFESSOR AND VICE CHAIR DEPARTMENT OF FAMILY AND COMMUNITY MEDICINE UNIVERSITY OF MISSOURI 4/4/17 DISCLOSURE: MEMBER OF THE JNC 8 PANEL
HYPERTENSION TARGETS: WHAT DO WE DO NOW? MICHAEL LEFEVRE, MD, MSPH PROFESSOR AND VICE CHAIR DEPARTMENT OF FAMILY AND COMMUNITY MEDICINE UNIVERSITY OF MISSOURI 4/4/17 DISCLOSURE: MEMBER OF THE JNC 8 PANEL
Hypertension Update. Mayo Clinic 90 th Annual Clinical Reviews November 2 nd and 16 th, 2016
 Mayo Clinic 90 th Annual Clinical Reviews November 2 nd and 16 th, 2016 Hypertension Update Vincent J. Canzanello, M.D. Consultant, Division of Nephrology and Hypertension Professor or Medicine College
Mayo Clinic 90 th Annual Clinical Reviews November 2 nd and 16 th, 2016 Hypertension Update Vincent J. Canzanello, M.D. Consultant, Division of Nephrology and Hypertension Professor or Medicine College
HYPERTENSION CHAT with Colin and Ted AUG 2015
 HYPERTENSION CHAT with Colin and Ted AUG 2015 INTRODUCTION Hypertension has challenged famous physicians for centuries. 1733 - Clergyman Stephen Hales made the 1 st published measurement of blood pressure
HYPERTENSION CHAT with Colin and Ted AUG 2015 INTRODUCTION Hypertension has challenged famous physicians for centuries. 1733 - Clergyman Stephen Hales made the 1 st published measurement of blood pressure
RESISTANT HYPERTENSION
 RESISTANT HYPERTENSION John D. Bisognano, MD PhD Professor of Medicine / Cardiology President-Elect, American Society of Hypertension Director, Outpatient Cardiology University of Rochester RESISTANT HYPERTENSION
RESISTANT HYPERTENSION John D. Bisognano, MD PhD Professor of Medicine / Cardiology President-Elect, American Society of Hypertension Director, Outpatient Cardiology University of Rochester RESISTANT HYPERTENSION
MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure. No relevant financial relationships. Blood Pressure and Risk
 MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
Management of Lipid Disorders and Hypertension: Implications of the New Guidelines
 Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Colin Edwards. Cardiologist Auckland Heart Group Waitemata Health
 Colin Edwards Cardiologist Auckland Heart Group Waitemata Health August 2011 BP MEASUREMENTS measured seated mean of 2 or BP recordings at least 2 visits 2 x risk of developing true hypertension Size of
Colin Edwards Cardiologist Auckland Heart Group Waitemata Health August 2011 BP MEASUREMENTS measured seated mean of 2 or BP recordings at least 2 visits 2 x risk of developing true hypertension Size of
Patrick Kay, General and Interventional Cardiologist Auckland or healthpoint.co.nz
 Patrick Kay, General and Interventional Cardiologist Auckland ipatkay@hotmail.com or healthpoint.co.nz Rotorua 2015 Rotorua 2015 Graphical example of true mean and variation, and of regression to the
Patrick Kay, General and Interventional Cardiologist Auckland ipatkay@hotmail.com or healthpoint.co.nz Rotorua 2015 Rotorua 2015 Graphical example of true mean and variation, and of regression to the
Hypertension in the Era of ACC/AHA: Practice Changing Evidence and Recommendations
 Hypertension in the Era of ACC/AHA: Practice Changing Evidence and Recommendations Gerald W. Smetana, M.D., MACP Division of General Medicine Beth Israel Deaconess Medical Center Professor of Medicine
Hypertension in the Era of ACC/AHA: Practice Changing Evidence and Recommendations Gerald W. Smetana, M.D., MACP Division of General Medicine Beth Israel Deaconess Medical Center Professor of Medicine
Treating Hypertension in 2018: What Makes the Most Sense Today?
 Treating Hypertension in 2018: What Makes the Most Sense Today? Daniel Blanchard, MD Professor of Medicine UC San Diego Cardiovascular Center La Jolla, California 1 2 Speaker Disclosures Consultant and/or
Treating Hypertension in 2018: What Makes the Most Sense Today? Daniel Blanchard, MD Professor of Medicine UC San Diego Cardiovascular Center La Jolla, California 1 2 Speaker Disclosures Consultant and/or
Managing Hypertension in 2016
 Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
Todd S. Perlstein, MD FIFTH ANNUAL SYMPOSIUM
 Todd S. Perlstein, MD FIFTH ANNUAL SYMPOSIUM Faculty Disclosure I have no financial interest to disclose No off-label use of medications will be discussed FIFTH ANNUAL SYMPOSIUM Recognize changes between
Todd S. Perlstein, MD FIFTH ANNUAL SYMPOSIUM Faculty Disclosure I have no financial interest to disclose No off-label use of medications will be discussed FIFTH ANNUAL SYMPOSIUM Recognize changes between
Egyptian Hypertension Guidelines
 Egyptian Hypertension Guidelines 2014 Egyptian Hypertension Guidelines Dalia R. ElRemissy, MD Lecturer of Cardiovascular Medicine Cairo University Why Egyptian Guidelines? Guidelines developed for rich
Egyptian Hypertension Guidelines 2014 Egyptian Hypertension Guidelines Dalia R. ElRemissy, MD Lecturer of Cardiovascular Medicine Cairo University Why Egyptian Guidelines? Guidelines developed for rich
DISCLOSURES OUTLINE OUTLINE 9/29/2014 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE
 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
Personalised Cardiovascular medicine: Integrating therapeutics and diagnostics. Dr. Patrick Gladding, MBChB, PhD Cardiologist, WDHB
 Personalised Cardiovascular medicine: Integrating therapeutics and diagnostics Dr. Patrick Gladding, MBChB, PhD Cardiologist, WDHB 2 3 4 Era of Mobile Health 5 Wireless Telemedicine 6 Increased sensitivity
Personalised Cardiovascular medicine: Integrating therapeutics and diagnostics Dr. Patrick Gladding, MBChB, PhD Cardiologist, WDHB 2 3 4 Era of Mobile Health 5 Wireless Telemedicine 6 Increased sensitivity
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
How do we diagnose hypertension today? Presentation Subtitle
 How do we diagnose hypertension today? Presentation Subtitle Renata Cífková Case 1 JM, a 64-year-old lady referred to our center because of undesirable effects of her antihypertensive medication Personal
How do we diagnose hypertension today? Presentation Subtitle Renata Cífková Case 1 JM, a 64-year-old lady referred to our center because of undesirable effects of her antihypertensive medication Personal
CKD & HT. Anne-Marie Angus
 CKD & HT Anne-Marie Angus Hypertension definitions Persisting BP >140/90 and HBPM >135/85 Stage 1 >140/90 (HBPM >135/85) Stage 2 >160/100 (HBPM >150/90) Severe >180/100 White coat HT Why treat? A major
CKD & HT Anne-Marie Angus Hypertension definitions Persisting BP >140/90 and HBPM >135/85 Stage 1 >140/90 (HBPM >135/85) Stage 2 >160/100 (HBPM >150/90) Severe >180/100 White coat HT Why treat? A major
Colin Edwards. Cardiologist Auckland Heart Group Waitemata Health
 Colin Edwards Cardiologist Auckland Heart Group Waitemata Health AUG 2012 Introduction Case Summary BP MEASUREMENTS measured seated mean of 2 BP recordings per visit at least 2 visits Diet Exercise Weight
Colin Edwards Cardiologist Auckland Heart Group Waitemata Health AUG 2012 Introduction Case Summary BP MEASUREMENTS measured seated mean of 2 BP recordings per visit at least 2 visits Diet Exercise Weight
HYPERTENSION. Introduction. Colin Edwards Cardiologist AHG and WDHB
 HYPERTENSION Introduction Colin Edwards Cardiologist AHG and WDHB June 2014 Disclosures FIONA STEWART Advisory Board Pfizer, AstraZeneca Meetings - AstraZeneca, MSD COLIN EDWARDS Meetings - AstraZeneca
HYPERTENSION Introduction Colin Edwards Cardiologist AHG and WDHB June 2014 Disclosures FIONA STEWART Advisory Board Pfizer, AstraZeneca Meetings - AstraZeneca, MSD COLIN EDWARDS Meetings - AstraZeneca
New Hypertension Guidelines. Kofi Osei, MD
 New Hypertension Guidelines Kofi Osei, MD None Disclosures Objectives The new blood pressure definitions and cardiovascular risk The role to time and location in the diagnosis of hypertension Apply evidence-based
New Hypertension Guidelines Kofi Osei, MD None Disclosures Objectives The new blood pressure definitions and cardiovascular risk The role to time and location in the diagnosis of hypertension Apply evidence-based
Hypertension Update. Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy
 Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
We are delighted to have Dr. Roetzheim with us today to discuss Managing Hypertension in Older Adult Patients.
 Richard Roetzheim, MD, MSPH is Professor and Chair, Department of Family Medicine at the University of South Florida Morsani College of Medicine. Dr. Roetzheim has considerable experience leading NIH funded
Richard Roetzheim, MD, MSPH is Professor and Chair, Department of Family Medicine at the University of South Florida Morsani College of Medicine. Dr. Roetzheim has considerable experience leading NIH funded
Practical Aspects of Hypertension: Simple Strategies to Help You and Your Patients Meet Guideline Blood Pressure Targets
 Practical Aspects of Hypertension: Simple Strategies to Help You and Your Patients Meet Guideline Blood Pressure Targets Robert J. Herman University of Calgary herman@ucalgary.ca Conflict of Interest Disclosure
Practical Aspects of Hypertension: Simple Strategies to Help You and Your Patients Meet Guideline Blood Pressure Targets Robert J. Herman University of Calgary herman@ucalgary.ca Conflict of Interest Disclosure
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Objectives. Describe results and implications of recent landmark hypertension trials
 Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
Hypertension Putting the Guidelines into Practice
 Hypertension 2017 Putting the Guidelines into Practice Disclosures Relationships with commercial interests: Grants/Research Support: Speakers Bureau/Honoraria: Consulting Fees: Data Safety and Monitoring:
Hypertension 2017 Putting the Guidelines into Practice Disclosures Relationships with commercial interests: Grants/Research Support: Speakers Bureau/Honoraria: Consulting Fees: Data Safety and Monitoring:
Hypertension 2015: Recent Evidence that Will Change Your Practice
 Hypertension 2015: Recent Evidence that Will Change Your Practice Gerald W. Smetana, M.D. Division of General Medicine Beth Israel Deaconess Medical Center Professor of Medicine Harvard Medical School
Hypertension 2015: Recent Evidence that Will Change Your Practice Gerald W. Smetana, M.D. Division of General Medicine Beth Israel Deaconess Medical Center Professor of Medicine Harvard Medical School
Disclosures. Learning Objectives. Hypertension: a sprint to the finish Ontario Pharmacists Association 1
 Disclosures I have no current or past relationships with commercial entities I have received a speaker s fee from the Ontario Pharmacists Association for this learning activity Laura Tsang PharmD Sunnybrook
Disclosures I have no current or past relationships with commercial entities I have received a speaker s fee from the Ontario Pharmacists Association for this learning activity Laura Tsang PharmD Sunnybrook
Preventing and Treating High Blood Pressure
 Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Younger adults with a family history of premature artherosclerotic disease should have their cardiovascular risk factors measured.
 Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
Appendix 2A - Guidance on Management of Hypertension Measurement of blood pressure All adults from 40 years should have blood pressure measured as part of opportunistic cardiovascular risk assessment.
Hypertension Update Clinical Controversies Regarding Age and Race
 Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Modern Management of Hypertension
 Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
Hypertension Putting the Guidelines into Practice
 Hypertension 2017 Putting the Guidelines into Practice Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or
Hypertension 2017 Putting the Guidelines into Practice Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or
MANAGEMENT OF HYPERTENSION: TREATMENT THRESHOLDS AND MEDICATION SELECTION
 Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
What s In the New Hypertension Guidelines?
 American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
Hypertension in the very old. Objectives: Clinical Perspective
 Harvard Medical School Hypertension in the very old Ihab Hajjar, MD, MS, AGSF Associate Director, CV Research Lab Assistant Professor of Medicine, Harvard Medical School Objectives: Describe the clinical
Harvard Medical School Hypertension in the very old Ihab Hajjar, MD, MS, AGSF Associate Director, CV Research Lab Assistant Professor of Medicine, Harvard Medical School Objectives: Describe the clinical
DISCLOSURE PHARMACIST OBJECTIVES 9/30/2014 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES. I have nothing to disclose.
 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
JNC 8 -Controversies. Sagren Naidoo Nephrologist CMJAH
 JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
Update in Hypertension
 Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Treating Hypertension from
 Treating Hypertension from Initiation to Resistance: A Case Study Approach Michelle Krause, MD Division of Nephrology University of Arkansas for Medical Sciences Central Arkansas Veteran s Healthcare System
Treating Hypertension from Initiation to Resistance: A Case Study Approach Michelle Krause, MD Division of Nephrology University of Arkansas for Medical Sciences Central Arkansas Veteran s Healthcare System
New Lipid Guidelines. PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids.
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
New Hypertension Guideline Recommendations for Adults July 7, :45-9:30am
 Advances in Cardiovascular Disease 30 th Annual Convention and Reunion UERM-CMAA, Inc. Annual Convention and Scientific Meeting July 5-8, 2018 New Hypertension Guideline Recommendations for Adults July
Advances in Cardiovascular Disease 30 th Annual Convention and Reunion UERM-CMAA, Inc. Annual Convention and Scientific Meeting July 5-8, 2018 New Hypertension Guideline Recommendations for Adults July
New Hypertension Guidelines: Why the change? Neil Brummond, M.D. Avera Medical Group Internal Medicine Sioux Falls, SD
 New Hypertension Guidelines: Why the change? Neil Brummond, M.D. Avera Medical Group Internal Medicine Sioux Falls, SD None Disclosures Objectives Understand trend in blood pressure clinical practice guidelines
New Hypertension Guidelines: Why the change? Neil Brummond, M.D. Avera Medical Group Internal Medicine Sioux Falls, SD None Disclosures Objectives Understand trend in blood pressure clinical practice guidelines
Hypertension in Geriatrics. Dr. Allen Liu Consultant Nephrologist 10 September 2016
 Hypertension in Geriatrics Dr. Allen Liu Consultant Nephrologist 10 September 2016 Annual mortality (%) Cardiovascular Mortality Rates are Higher among Dialysis Patients 100 10 1 0.1 0.01 0.001 25-34
Hypertension in Geriatrics Dr. Allen Liu Consultant Nephrologist 10 September 2016 Annual mortality (%) Cardiovascular Mortality Rates are Higher among Dialysis Patients 100 10 1 0.1 0.01 0.001 25-34
Overview. NOT A REPETION OF LOCAL GUIDELINE Dr Diviash Thakrar
 Overview 1. Why hypertension is important? 2. What are basic principles in treatment? 3. Different ways of measuring 4. Hypercholesterolemia NOT A REPETION OF LOCAL GUIDELINE CVD risk factors? Non modifiable
Overview 1. Why hypertension is important? 2. What are basic principles in treatment? 3. Different ways of measuring 4. Hypercholesterolemia NOT A REPETION OF LOCAL GUIDELINE CVD risk factors? Non modifiable
Hypertension and the 2017 Guidelines Meeting the Targets in Small Groups. Lisa Ivy APRN
 Hypertension and the 2017 Guidelines Meeting the Targets in Small Groups Lisa Ivy APRN The 2017 Guideline is an Update to JNC7 New information regarding BP related risk of CVD Ambulatory BP monitoring
Hypertension and the 2017 Guidelines Meeting the Targets in Small Groups Lisa Ivy APRN The 2017 Guideline is an Update to JNC7 New information regarding BP related risk of CVD Ambulatory BP monitoring
Modern Management of Hypertension: Where Do We Draw the Line?
 Modern Management of Hypertension: Where Do We Draw the Line? Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Blood Pressure
Modern Management of Hypertension: Where Do We Draw the Line? Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Blood Pressure
Managing Hypertension in 2018
 MANAGING HYPERTENSION IN 2018 How Do We Work With Conflicting Data and Conflicting Guidelines? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School
MANAGING HYPERTENSION IN 2018 How Do We Work With Conflicting Data and Conflicting Guidelines? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School
Incidental Findings; Management of patients presenting with high BP. Phil Swales
 Incidental Findings; Management of patients presenting with high BP Phil Swales Consultant Physician Acute & General Medicine University Hospitals of Leicester NHS Trust Objectives The approach to an incidental
Incidental Findings; Management of patients presenting with high BP Phil Swales Consultant Physician Acute & General Medicine University Hospitals of Leicester NHS Trust Objectives The approach to an incidental
Approach to Management of Hypertension. Prof. Abdulkareem Al-Suwaida, MD, FRCPC, MSc
 Approach to Management of Hypertension Prof. Abdulkareem Al-Suwaida, MD, FRCPC, MSc 442-2018 Objectives of The Lecture Hypertension in KSA New definitions of hypertension Understand how to diagnose hypertension
Approach to Management of Hypertension Prof. Abdulkareem Al-Suwaida, MD, FRCPC, MSc 442-2018 Objectives of The Lecture Hypertension in KSA New definitions of hypertension Understand how to diagnose hypertension
Combination Therapy for Hypertension
 Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
How do I investigate suspected secondary hypertension? Marie Freel RCP Update in Medicine 23 rd November 2016
 How do I investigate suspected secondary hypertension? Marie Freel RCP Update in Medicine 23 rd November 2016 World beaters..! Michel Joffres et al. BMJ Open 2013;3:e003423 Hypertension often poorly controlled
How do I investigate suspected secondary hypertension? Marie Freel RCP Update in Medicine 23 rd November 2016 World beaters..! Michel Joffres et al. BMJ Open 2013;3:e003423 Hypertension often poorly controlled
Hypertension Update. Aaron J. Friedberg, MD
 Hypertension Update Aaron J. Friedberg, MD Assistant Professor, Clinical Division of General Internal Medicine The Ohio State University Wexner Medical Center Background Diagnosis Management Overview Guideline
Hypertension Update Aaron J. Friedberg, MD Assistant Professor, Clinical Division of General Internal Medicine The Ohio State University Wexner Medical Center Background Diagnosis Management Overview Guideline
HTN talk_l Davis_ /28/2018
 1 2 GUIDELINES PUBLISHED AHEAD OF PRINT NOV 13, 2017 = SAME DAY AS PUBLIC PRESENTATION LESLIE L DAVIS, PHD, RN, ANP-BC, FPCNA, FAANP, FAHA The New Guidelines Have Been Published! Whelton PK, Carey RM,
1 2 GUIDELINES PUBLISHED AHEAD OF PRINT NOV 13, 2017 = SAME DAY AS PUBLIC PRESENTATION LESLIE L DAVIS, PHD, RN, ANP-BC, FPCNA, FAANP, FAHA The New Guidelines Have Been Published! Whelton PK, Carey RM,
Hypertension CHAPTER-I CARDIOVASCULAR SYSTEM. Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati
 CHAPTER-I CARDIOVASCULAR SYSTEM Hypertension SUB: PHARMACOTHERAPEUTICS-I CODE:T0820006 Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati Hypertension
CHAPTER-I CARDIOVASCULAR SYSTEM Hypertension SUB: PHARMACOTHERAPEUTICS-I CODE:T0820006 Dr. K T NAIK Pharm.D Associate Professor Department of Pharm.D Krishna Teja Pharmacy College, Tirupati Hypertension
hypertension Head of prevention and control of CVD disease office Ministry of heath
 hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
hypertension t. Samavat MD,Cadiologist,MPH Head of prevention and control of CVD disease office Ministry of heath RECOMMENDATIONS FOR HYPERTENSION DIAGNOSIS, ASSESSMENT, AND TREATMENT Definition of hypertension
Hypertension Controversies: SPRINTing to New Goals
 Hypertension Controversies: SPRINTing to New Goals Diana Isaacs, PharmD, BCPS, BC-ADM, CDE Clinical Pharmacy Specialist Cleveland Clinic Lauren Wolfe, PharmD Primary Care Clinical Specialist Cleveland
Hypertension Controversies: SPRINTing to New Goals Diana Isaacs, PharmD, BCPS, BC-ADM, CDE Clinical Pharmacy Specialist Cleveland Clinic Lauren Wolfe, PharmD Primary Care Clinical Specialist Cleveland
5.2 Key priorities for implementation
 5.2 Key priorities for implementation From the full set of recommendations, the GDG selected ten key priorities for implementation. The criteria used for selecting these recommendations are listed in detail
5.2 Key priorities for implementation From the full set of recommendations, the GDG selected ten key priorities for implementation. The criteria used for selecting these recommendations are listed in detail
Evaluation and Management of Hypertension in Women. Vesna D. Garovic, M.D. Moscow, Russia, December 2016
 Evaluation and Management of Hypertension in Women Vesna D. Garovic, M.D. Moscow, Russia, December 2016 2016 MFMER 3508058-1 Women are not small men There is nothing as powerful as an idea whose time has
Evaluation and Management of Hypertension in Women Vesna D. Garovic, M.D. Moscow, Russia, December 2016 2016 MFMER 3508058-1 Women are not small men There is nothing as powerful as an idea whose time has
Hypertension Update Warwick Jaffe Interventional Cardiologist Ascot Hospital
 Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Adult Blood Pressure Clinician Guide June 2018
 Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Adult Blood Pressure Clinician Guide June 2018 Adult Blood Pressure Clinician Guide June 2018 Introduction This Clinician Guide is based on the 2018
Kaiser Permanente National CLINICAL PRACTICE GUIDELINES Adult Blood Pressure Clinician Guide June 2018 Adult Blood Pressure Clinician Guide June 2018 Introduction This Clinician Guide is based on the 2018
DEPARTMENT OF GENERAL MEDICINE WELCOMES
 DEPARTMENT OF GENERAL MEDICINE WELCOMES 1 Dr.Mohamed Omar Shariff, 2 nd Year Post Graduate, Department of General Medicine. DR.B.R.Ambedkar Medical College & Hospital. 2 INTRODUCTION Leading cause of global
DEPARTMENT OF GENERAL MEDICINE WELCOMES 1 Dr.Mohamed Omar Shariff, 2 nd Year Post Graduate, Department of General Medicine. DR.B.R.Ambedkar Medical College & Hospital. 2 INTRODUCTION Leading cause of global
Talking about blood pressure
 Talking about blood pressure Mrs Khan 56 BP 158/99 BMI 32 Total cholesterol 5.4 (HDL 0.8) HbA1c 43 She has been promising to do more exercise and eat more healthily for the last 2 years but her weight
Talking about blood pressure Mrs Khan 56 BP 158/99 BMI 32 Total cholesterol 5.4 (HDL 0.8) HbA1c 43 She has been promising to do more exercise and eat more healthily for the last 2 years but her weight
Approach to patient with hypertension. Dr. Amitesh Aggarwal
 Approach to patient with hypertension Dr. Amitesh Aggarwal Definition A systolic blood pressure ( SBP) >139 mmhg and/or A diastolic (DBP) >89 mmhg. Based on the average of two or more properly measured,
Approach to patient with hypertension Dr. Amitesh Aggarwal Definition A systolic blood pressure ( SBP) >139 mmhg and/or A diastolic (DBP) >89 mmhg. Based on the average of two or more properly measured,
Hypertension (JNC-8)
") Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
RESISTENT HYPERTENSION. Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University
 RESISTENT HYPERTENSION Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University Resistant Hypertension Blood pressure remaining above goal in spite of concurrent use of 3 antihypertensive
RESISTENT HYPERTENSION Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University Resistant Hypertension Blood pressure remaining above goal in spite of concurrent use of 3 antihypertensive
Hypertension Update. Faculty/Presenter Disclosure
 Hypertension Update Who Gives a CHEP About Targets? Faculty/Presenter Disclosure Presenter: Raj Padwal Relationships that may introduce potential bias and/or conflict of interest: Grants/Research Support:
Hypertension Update Who Gives a CHEP About Targets? Faculty/Presenter Disclosure Presenter: Raj Padwal Relationships that may introduce potential bias and/or conflict of interest: Grants/Research Support:
Hypertension Update Background
 Hypertension Update Background Overview Aaron J. Friedberg, MD Assistant Professor, Clinical Division of General Internal Medicine The Ohio State University Wexner Medical Center Management Guideline Comparison
Hypertension Update Background Overview Aaron J. Friedberg, MD Assistant Professor, Clinical Division of General Internal Medicine The Ohio State University Wexner Medical Center Management Guideline Comparison
Hypertension: What s new since JNC 7. Harold M. Szerlip, MD, FACP, FCCP, FASN, FNKF
 Hypertension: What s new since JNC 7 Harold M. Szerlip, MD, FACP, FCCP, FASN, FNKF Disclosures Spectral Diagnostics Site investigator Eli Lilly Site investigator ACP IM ITE writing committee NBME Step
Hypertension: What s new since JNC 7 Harold M. Szerlip, MD, FACP, FCCP, FASN, FNKF Disclosures Spectral Diagnostics Site investigator Eli Lilly Site investigator ACP IM ITE writing committee NBME Step
Update on Current Trends in Hypertension Management
 Friday General Session Update on Current Trends in Hypertension Management Shawna Nesbitt, MD Associate Dean, Minority Student Affairs Associate Professor, Department of Internal Medicine Office of Student
Friday General Session Update on Current Trends in Hypertension Management Shawna Nesbitt, MD Associate Dean, Minority Student Affairs Associate Professor, Department of Internal Medicine Office of Student
Management of Hypertension in Women
 Management of Hypertension in Women Eliseo J. Pérez-Stable MD Professor of Medicine DGIM, Department of Medicine July 1, 2013 Declaration of full disclosure: No conflict of interest (I have never been
Management of Hypertension in Women Eliseo J. Pérez-Stable MD Professor of Medicine DGIM, Department of Medicine July 1, 2013 Declaration of full disclosure: No conflict of interest (I have never been
Hypertension: JNC-7. Southern California University of Health Sciences Physician Assistant Program
 Hypertension: JNC-7 Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! Reference Card
Hypertension: JNC-7 Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! Reference Card
The State of Hypertension in NZ in 2010 personal view
 The State of Hypertension in NZ in 2010 personal view Patient referred to medical clinic Dear Dr, Please see this man with resistant hypertension 50 year old European male Blood Pressure on current meds
The State of Hypertension in NZ in 2010 personal view Patient referred to medical clinic Dear Dr, Please see this man with resistant hypertension 50 year old European male Blood Pressure on current meds
Management of Hypertension
 Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Clinical Practice Guidelines Management of Hypertension Definition and classification of blood pressure levels (mmhg) Category Systolic Diastolic Normal
Hypertension. Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute
 Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Updates in Cardiovascular Recommendations for Diabetic Patients
 Updates in Cardiovascular Recommendations for Diabetic Patients Chris Tawwater, Pharm.D., BCPS Clinical Pharmacist, Abilene Regional Medical Center Assistant Professor, Adult Medicine Division Pharmacotherapy
Updates in Cardiovascular Recommendations for Diabetic Patients Chris Tawwater, Pharm.D., BCPS Clinical Pharmacist, Abilene Regional Medical Center Assistant Professor, Adult Medicine Division Pharmacotherapy
Brent M. Egan, MD Professor of Medicine USCSOM Greenville
 Contemporary Management of Uncontrolled and Treatment Resistant Hypertension Brent M. Egan, MD Professor of Medicine USCSOM Greenville Disclosures (past 3 years): Honoraria: BCBSSC, Medtronic Grant Support:
Contemporary Management of Uncontrolled and Treatment Resistant Hypertension Brent M. Egan, MD Professor of Medicine USCSOM Greenville Disclosures (past 3 years): Honoraria: BCBSSC, Medtronic Grant Support:
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005
 VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
Difficult to Treat Hypertension
 Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Management of Hypertension. M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine
 Division of Nephrology University of Missouri School of Medicine") Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Blood Pressure. Michelle Bertram- Nephrology- OBH
 Blood Pressure Michelle Bertram- Nephrology- OBH Hypertension- how common? 29-30% white adults 46-51% uncontrolled Diagnosis Two or more properly measured BP s after an initial screen NICE guidelines also
Blood Pressure Michelle Bertram- Nephrology- OBH Hypertension- how common? 29-30% white adults 46-51% uncontrolled Diagnosis Two or more properly measured BP s after an initial screen NICE guidelines also
Cardiovascular risk factor appraisal art or science?
 Cardiovascular risk factor appraisal art or science? Prof. Philip MacCarthy BSc MBChB (Hons) PhD FRCP Consultant Cardiologist Bupa Cromwell Hospital Clinics: Wednesday & Friday PM/Evening What are we trying
Cardiovascular risk factor appraisal art or science? Prof. Philip MacCarthy BSc MBChB (Hons) PhD FRCP Consultant Cardiologist Bupa Cromwell Hospital Clinics: Wednesday & Friday PM/Evening What are we trying
MPharmProgramme. Hypertension (HTN)
") MPharmProgramme Hypertension (HTN) Slide 1 of 30 Overview Definition Prevalence Type Causes Diagnosis Management Patients perspective Slide 2 of 30 Definition It is not a disease! So what is it? What two
MPharmProgramme Hypertension (HTN) Slide 1 of 30 Overview Definition Prevalence Type Causes Diagnosis Management Patients perspective Slide 2 of 30 Definition It is not a disease! So what is it? What two
Treating Hypertension in Individuals with Diabetes
 Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Treating Hypertension in Individuals with Diabetes Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any
Hypertension in the Elderly. John Puxty Division of Geriatrics Center for Studies in Aging and Health, Providence Care
 Hypertension in the Elderly John Puxty Division of Geriatrics Center for Studies in Aging and Health, Providence Care Learning Objectives Review evidence for treatment of hypertension in elderly Consider
Hypertension in the Elderly John Puxty Division of Geriatrics Center for Studies in Aging and Health, Providence Care Learning Objectives Review evidence for treatment of hypertension in elderly Consider
Prevention of Heart Failure: What s New with Hypertension
 Prevention of Heart Failure: What s New with Hypertension Ali AlMasood Prince Sultan Cardiac Center Riyadh 3ed Saudi Heart Failure conference, Jeddah, 13 December 2014 Background 20-30% of Saudi adults
Prevention of Heart Failure: What s New with Hypertension Ali AlMasood Prince Sultan Cardiac Center Riyadh 3ed Saudi Heart Failure conference, Jeddah, 13 December 2014 Background 20-30% of Saudi adults
JNC Evidence-Based Guidelines for the Management of High Blood Pressure in Adults
 JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
Preventing Cardiovascular Disease Stroke Primary Prevention Guidelines. John Potter Professor Ageing & Stroke Medicine University of East Anglia
 Preventing Cardiovascular Disease Stroke Primary Prevention Guidelines John Potter Professor Ageing & Stroke Medicine University of East Anglia Preventing Cardiovascular Disease Stroke Primary Prevention
Preventing Cardiovascular Disease Stroke Primary Prevention Guidelines John Potter Professor Ageing & Stroke Medicine University of East Anglia Preventing Cardiovascular Disease Stroke Primary Prevention