A Nightmare. R Dulgheru, CHU Liege
|
|
|
- Lillian Mills
- 5 years ago
- Views:
Transcription

1 A Nightmare R Dulgheru, CHU Liege



2 Faculty disclosure Raluca Dulgheru I have no financial relationships to disclose.
3 MB, 57 years old male 18/03/2016 to the ER for altered mental status, First weight name - last loss, name denutrition, fall with mild cranial trauma Recent medical history: Bentall procedure for acute aortic dissection type Stanford A 14/12/2015 Several post-operative complications: Reintervention for acute bleeeding at the anasthomosis between the St Jude mechanical valve and the Dacron tube 15/12/2015 Cardiac arrest on the 16/12/2016 due to a pulss less VT (post op AMI, metabolic acidosis and hyperkalemia) Reversible acute renal failure with anuria, needing CVVH followed by HD, left renal artery dissection and occlusion Left hospital on the 01/02/2016 after 1 month and 1/2 (revalidation clinic)
4 18/03/2016 Clinical examination at hospital admission: Blood tests at hospital admission: confusion cachexia BP=113/83, HR=87 regular no dyspnea no detectable heart murmur peripheral cyanosis peripheral oedema 10.8 g/dl Hb (normochromicnormocytic anemia) 6400 WBC PLT INR=2.0 creat 0.99 mg/dl albumine 29g/l (low) CRP 30.9 mg/l (high) altered hepatic tests high ferritine levels





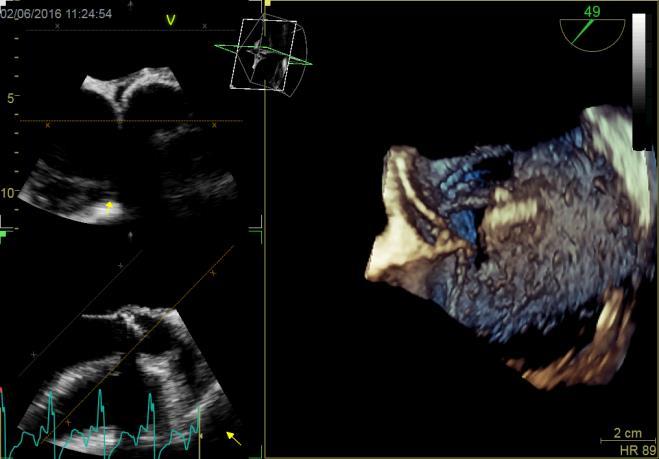
5 TTE evaluation 24/03/2016:
6 TTE evaluation 24/03/2016: LVOT=2.4 EOA=2.2 cm² MG =2 mmhg SVi=22ml/m² LVEF=33% What is your diagnosis?
7 TTE evaluation 24/03/2016: LVOT=2.4 EOA=2.2 cm² MG =2 mmhg SVi=22ml/m² LVEF=33% Mechanical aortic valve prosthesis with normal function (no PVL, no obstruction, no mismatch EOA=2.2 cm²) Dilated ischemic cardiomyopathy with moderate LV systolic dysfunction severe secondary MR probable PHT (estimated spap 51 mmhg)
8 What would you do next? A. Perform a TOE as soon as possible B. Perform blood cultures C. Perform a cerebral CT scan D. Just follow up the patient clinically
9 Should we suspect IE? high risk patient for IE ( patients with prosthetic valve and prosthetic material have higher risk of IE, higher mortality from EI and develop more often complications ) immunocompromised patient (difficult post operatory period, heart failure with reduced LVEF, NYHA III-IV, cachexia) Clinical & biological features: inflammatory syndrome of unknown cause no fever reported no other clinical signs of IE (no new cardiac murmur, no splinter hemorrhages, etc ) non specific symptoms (weight loss, altered mental status) confusion (possible cerebral embolization?)

10 High risk patient + red flags ESC Guidelines on IE, EHJ 2009



11 YES ESC Guidelines on IE, EHJ 2015

12 TOE evaluation 25/03/2016: What is your Diagnosis?
13 How do you interpret the TOE? A. Positive for IE B. Negative for IE C. I do not know

14 TOE evaluation 25/03/2016: No abnormality No peri-aortic oedema/thickening No sign of IE
15 29/03/2016: Patient not doing well Chills Back pain Altered mental status Inability to eat (parenteral nutrition) Clinical signs of infection of the central venous line line removed on the 29 th Persistent inflammatory syndrome (CRP 35 on the 19 th then 178 on the 31/03/2016) Finally BC asked
16 State of facts on the 31/3/2016: 2 Blood cultures + for Staph aureus (ATB sensibility not known yet) on the 29th and 30/03/2016 Negative findings on TOE 25 th /03/2016 Inflammatory syndrome aggravating At risk patient for EI (recent Bentall procedure) Clinical examination: unremarkable for IE Context of central venous line infection What is your diagnosis? 1 MAJOR CRITERION 1 minor criterion
17 What complementary exams to ask at this point? 1. Repeat TOE in 5 to 7 days 2. Repeat TTE immediately followed by TOE if TTE negative 3. Ask for ophtalmological exam (Roth s spots) 4. Blood cultures until - 5. Brain MRI and maybe MRI of the dorsal spine
18 2 nd TOE evaluation 06/04/2016 What is your diagnosis?
19 2 nd TOE evaluation 06/04/2016 Report: MV IE confirmation P2 vegetation (13.5 mm length) No perforation mild SMR Aortic prosthesis of normal function peri-aortic thickening, ask for a PET CT
 only?")
20 Definite diagnosis made on the 6 th /04/ major criteria + 1 minor, type? What is your diagnosis? Left sided Native valve (mitral) only? Nosocomial Active ESC Guidelines on IE, EHJ 2009
21 State of the facts on the 06 th /4/2016 Endocarditis team discussion ( in between 2 patients ) : MV IE, without signs of IE of the aortic prosthesis/conduit (highly unlikely since it is a Staph aureus + immunocompromised patient) +blood cultures persistent after central venous catheter removal (red flag, should have done a TTE/TOE ASAP, especially if Staph aureus!!!) TO DOs: brain CMR to exclude cerebral emboli (confusion) demand PET CT (to exclude/confirm AV endocarditis since ATB regimen differs; look for spondylodiscites since he has back pain) continue to perform blood cultures until


22 If the two TOEs would have been compared TOE 25/03/2016: TOE 06/04/2016: + AV prosthesis IE Systematic image acquisition is important for further comparisons


23 Pet CT results available 15/04/2016 (: 9 days lost) suspected IE of the AV, not of the aortic conduit Possible septic emboli in the liver Hyper metabolism at the level of the right vertebral bodies L4-L5 (confirmed spondylodiscites by MRI) 15/04/2016 : subacute ischemic lesion in the right MCA territory Frontal left ischemic sequellae No evidence of aneurisms, no signs of hemorrhage
24 Methicillin susceptible Staph aureus left side valves endocarditis of the native mitral valve vegetation 1.35 cm, highly mobile, high embolic risk, evidence of emboli in the brain, vertebral bodies, and possible liver and of the prosthetic aortic valve (echocardiographic and PET CT evidence of peri-aortic prosthetic abcess) Nosocomial? Active What is your final diagnosis?

25 Prognosis assessment: ESC Guidelines on IE, EHJ 2015


26 Is surgery indicated at this point?
27 What does the surgeon say? 1. High risk surgery for many reasons 2. Frail patient (heart failure, denutriton, immunocompromised)





28 At follow up 06/2016
29 The fails 1. Should have asked for blood cultures sooner because in the suspected case of IE the final diagnosis is based on clinical manifestations, BC and imaging evidence 2. Should have asked for a TTE immediately after +BC for Staph aureus, followed by a TOE 3. Should have compared the two TOEs to detect early PVE (changes treatment, prognosis) not wait for the PET CT results 4. Should have been systematic in TOE image acquisition 5. Should have been more aggressive in our research for emboli 6. Should have discussed the case in the Endocarditis team earlier
30 The learning 1. Lower clinical threshold in suspecting IE in immunocompromised patients 2. The modified Duke should be used as a diagnostic guide but clinical judgment is important (Duke criteria have a diminished sensitivity in PVE) 3. TOE has a high sensitivity to detect IE but nevertheless lower than 100%, PET-CT have helped the diagnosis if done earlier 4. Strict aseptic measurements during hospitalization (high risk patient for IE) to avoid nosocomial IE 5. Endocarditis team discussion is important
Case-based session. Infective Endocarditis. Applying the new guidelines. A case of large vegetation with neurological complication.
 Case-based session. Infective Endocarditis. Applying the new guidelines. A case of large vegetation with neurological complication. María Nazarena Pizzi Hospital Universitari Vall d Hebron Barcelona. I
Case-based session. Infective Endocarditis. Applying the new guidelines. A case of large vegetation with neurological complication. María Nazarena Pizzi Hospital Universitari Vall d Hebron Barcelona. I
DICE Session. The endocarditis team. Bernard Iung Bichat Hospital, Paris Diderot University Paris, France
 DICE Session. The endocarditis team Bernard Iung Bichat Hospital, Paris Diderot University Paris, France Faculty disclosure First name - last name I disclose the following financial relationships: Consultant
DICE Session. The endocarditis team Bernard Iung Bichat Hospital, Paris Diderot University Paris, France Faculty disclosure First name - last name I disclose the following financial relationships: Consultant
Challenging clinical situation
 Challenging clinical situation A young patient with prosthetic aortic valve endocarditis Gilbert Habib La Timone Hospital Marseille - France October 25 th 2014 Case report History of the disease Clinical
Challenging clinical situation A young patient with prosthetic aortic valve endocarditis Gilbert Habib La Timone Hospital Marseille - France October 25 th 2014 Case report History of the disease Clinical
IE with cerebral hemorrhage
 IE with cerebral hemorrhage Gilbert Habib / Patrizio Lancellotti La Timone Hospital Marseille - France Palermo, 26 April 2018 Case report: aortic bioprosthetic IE History of the disease 75 year-old man
IE with cerebral hemorrhage Gilbert Habib / Patrizio Lancellotti La Timone Hospital Marseille - France Palermo, 26 April 2018 Case report: aortic bioprosthetic IE History of the disease 75 year-old man
Diagnostic strategy. Dr Pilar Tornos Hospital Vall d Hebron Barcelona
 Diagnostic strategy Dr Pilar Tornos Hospital Vall d Hebron Barcelona Faculty disclosure Pilar Tornos I disclose the following financial relationships: Paid speaker for Recordati, Edwards. Diagnosis of
Diagnostic strategy Dr Pilar Tornos Hospital Vall d Hebron Barcelona Faculty disclosure Pilar Tornos I disclose the following financial relationships: Paid speaker for Recordati, Edwards. Diagnosis of
General management of infective endocarditis
 General management of infective endocarditis Team approach in infective endocarditis Gilbert Habib La Timone Hospital Marseille - France Eurovalves Barcelona 2017 The echolab «Heart Team" Infective Endocarditis
General management of infective endocarditis Team approach in infective endocarditis Gilbert Habib La Timone Hospital Marseille - France Eurovalves Barcelona 2017 The echolab «Heart Team" Infective Endocarditis
What is Your Diagnosis?
 What is Your Diagnosis? A STORM R Dulgheru, Liege, Belgium Faculty disclosure Raluca Dulgheru I have no financial relationships to disclose. Case presentation 52 years old male Ongoing oppressive chest
What is Your Diagnosis? A STORM R Dulgheru, Liege, Belgium Faculty disclosure Raluca Dulgheru I have no financial relationships to disclose. Case presentation 52 years old male Ongoing oppressive chest
Heart on Fire: Infective Endocarditis. Objectives. Disclosure 8/27/2018. Mary McGreal DNP, RN, ANP-c, CCRN
 Heart on Fire: Infective Endocarditis Mary McGreal DNP, RN, ANP-c, CCRN Objectives Discuss the incidence of infective endocarditis? Discuss the pathogenesis of infective endocarditis? Discuss clinical
Heart on Fire: Infective Endocarditis Mary McGreal DNP, RN, ANP-c, CCRN Objectives Discuss the incidence of infective endocarditis? Discuss the pathogenesis of infective endocarditis? Discuss clinical
Apport des recommandations européennes
 Apport des recommandations européennes Gilbert Habib Cardiology Department- La Timone Marseille - France Bordeaux le 28 Juin 2011 Infective Endocarditis: a changing disease new high-risk subgroups IVDA
Apport des recommandations européennes Gilbert Habib Cardiology Department- La Timone Marseille - France Bordeaux le 28 Juin 2011 Infective Endocarditis: a changing disease new high-risk subgroups IVDA
Update on the prevention, diagnosis and management of Infective Endocarditis (IE)
") Update on the prevention, diagnosis and management of Infective Endocarditis (IE) Dr.Ahmed Yahya Mohammed Alarhabi MD, MsC,FcUSM,FACC,MAHA Consultant Interventional Cardiologist Head of Cardiac Center
Update on the prevention, diagnosis and management of Infective Endocarditis (IE) Dr.Ahmed Yahya Mohammed Alarhabi MD, MsC,FcUSM,FACC,MAHA Consultant Interventional Cardiologist Head of Cardiac Center
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Kang D-H, Kim Y-J, Kim S-H, et al. Early surgery versus conventional
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Kang D-H, Kim Y-J, Kim S-H, et al. Early surgery versus conventional
Pulmonary Embolism Is it the Greatest Danger in Deep Vein Thrombosis?
 Difficult issues in Deep Vein Thrombosis: Pulmonary Embolism Is it the Greatest Danger in Deep Vein Thrombosis? Raluca Dulgheru; C Gherghinescu; B Dorobat; H Muresan; R Darabont; M Cinteza; D Vinereanu
Difficult issues in Deep Vein Thrombosis: Pulmonary Embolism Is it the Greatest Danger in Deep Vein Thrombosis? Raluca Dulgheru; C Gherghinescu; B Dorobat; H Muresan; R Darabont; M Cinteza; D Vinereanu
PRINCIPLES OF ENDOCARDITIS
 015 // Endocarditis CONTENTS 140 Principles of Endocarditis 141 Native Valve Endocarditis 143 Complications of Native Valve Endocarditis 145 Right Heart Endocarditis 145 Prosthetic Valve Endocarditis 146
015 // Endocarditis CONTENTS 140 Principles of Endocarditis 141 Native Valve Endocarditis 143 Complications of Native Valve Endocarditis 145 Right Heart Endocarditis 145 Prosthetic Valve Endocarditis 146
PROSTHETIC VALVE ENDOCARDITIS Dr Bernard Prendergast DM FRCP EUROVALVE CONGRESS MADRID NOVEMBER 2013
 PROSTHETIC VALVE ENDOCARDITIS Dr Bernard Prendergast DM FRCP EUROVALVE CONGRESS MADRID NOVEMBER 2013 Prosthetic Valve Endocarditis A Dangerous Disease Affects 1-6% of prosthetic valves Mechanical and biological
PROSTHETIC VALVE ENDOCARDITIS Dr Bernard Prendergast DM FRCP EUROVALVE CONGRESS MADRID NOVEMBER 2013 Prosthetic Valve Endocarditis A Dangerous Disease Affects 1-6% of prosthetic valves Mechanical and biological
April 16, 09:00-09:15 중앙대학교 윤신원
 April 16, 09:00-09:15 중앙대학교 윤신원 When to perform Echocardiography in IE? Vegetations?(pathologic Whatever the level hallmark) of suspicion Intracardiac abscess? Confirm or R/O at the Earliest opportunity.
April 16, 09:00-09:15 중앙대학교 윤신원 When to perform Echocardiography in IE? Vegetations?(pathologic Whatever the level hallmark) of suspicion Intracardiac abscess? Confirm or R/O at the Earliest opportunity.
The changing landscape of infective endocarditis (IE)in congenital heart disease (CHD)
in congenital heart disease (CHD)") The changing landscape of infective endocarditis (IE)in congenital heart disease (CHD) Rekwan Sittiwangkul,MD Department of Pediatrics. Chiang Mai University Hospital, 24 th March 2018 Infective endocarditis
The changing landscape of infective endocarditis (IE)in congenital heart disease (CHD) Rekwan Sittiwangkul,MD Department of Pediatrics. Chiang Mai University Hospital, 24 th March 2018 Infective endocarditis
Daniel C. DeSimone, MD Assistant Professor of Medicine
 Daniel C. DeSimone, MD Assistant Professor of Medicine Faculty photo will be placed here Desimone.Daniel@mayo.edu 2015 MFMER 3543652-1 Infective Endocarditis Mayo School of Continuous Professional Development
Daniel C. DeSimone, MD Assistant Professor of Medicine Faculty photo will be placed here Desimone.Daniel@mayo.edu 2015 MFMER 3543652-1 Infective Endocarditis Mayo School of Continuous Professional Development
SONOGRAPHER & NURSE LED VALVE CLINICS
 SONOGRAPHER & NURSE LED VALVE CLINICS Frequency of visits and alerts AORTIC STENOSIS V max > 4.0 m/s or EOA < 1.0 cm 2 V max 3.5 4.0 m/s + Ca+ V max 3.0 4.0 m/s or EOA 1.0-1.5 cm 2 V max 2.5 3.0 m/s every
SONOGRAPHER & NURSE LED VALVE CLINICS Frequency of visits and alerts AORTIC STENOSIS V max > 4.0 m/s or EOA < 1.0 cm 2 V max 3.5 4.0 m/s + Ca+ V max 3.0 4.0 m/s or EOA 1.0-1.5 cm 2 V max 2.5 3.0 m/s every
Endocarditis in the elderly
 Endocarditis in the elderly Gilbert Habib Département de Cardiologie - Timone Marseille Eurovalves Barcelona 2017 Endocarditis in the octogenarian Gilbert Habib Département de Cardiologie - Timone Marseille
Endocarditis in the elderly Gilbert Habib Département de Cardiologie - Timone Marseille Eurovalves Barcelona 2017 Endocarditis in the octogenarian Gilbert Habib Département de Cardiologie - Timone Marseille
Echocardiographic Evaluation of Aortic Valve Prosthesis
 Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co-Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co-Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
Endocarditis and Its Complications: The Role of Echocardiography
 Endocarditis and Its Complications: The Role of Echocardiography Pravin Patil, MD FACC FASE Associate Professor of Medicine Director, Cardiovascular Disease Training Program Lewis Katz School of Medicine
Endocarditis and Its Complications: The Role of Echocardiography Pravin Patil, MD FACC FASE Associate Professor of Medicine Director, Cardiovascular Disease Training Program Lewis Katz School of Medicine
Infective Endocarditis Empirical therapy Antibiotic Guidelines. Contents
 Infective Endocarditis Empirical therapy Antibiotic Guidelines Classification: Clinical Guideline Lead Author: Antibiotic Steering Group Additional author(s): as above Authors Division: Division of Clinical
Infective Endocarditis Empirical therapy Antibiotic Guidelines Classification: Clinical Guideline Lead Author: Antibiotic Steering Group Additional author(s): as above Authors Division: Division of Clinical
Exercise Testing/Echocardiography in Asymptomatic AS
 Exercise Testing/Echocardiography in Asymptomatic AS Raluca Dulgheru, MD Heart Valve Clinic, University of Liège, CHU Sart Tilman, BELGIUM Disclosure related to this presentation: None VALVULAR HEART DISEASE
Exercise Testing/Echocardiography in Asymptomatic AS Raluca Dulgheru, MD Heart Valve Clinic, University of Liège, CHU Sart Tilman, BELGIUM Disclosure related to this presentation: None VALVULAR HEART DISEASE
Acute Valve Regurgitation Catherine M. Otto, MD J. Ward Kennedy-Hamilton Endowed Chair in Cardiology University of Washington, Seattle
 Acute Valve Regurgitation Catherine M. Otto, MD J. Ward Kennedy-Hamilton Endowed Chair in Cardiology University of Washington, Seattle No conflicts of interest Acute Aortic Regurgitation Causes aortic
Acute Valve Regurgitation Catherine M. Otto, MD J. Ward Kennedy-Hamilton Endowed Chair in Cardiology University of Washington, Seattle No conflicts of interest Acute Aortic Regurgitation Causes aortic
Surgical Indications of Infective Endocarditis in Children
 2016 Annual Spring Scientific Conference of the KSC April 15-16, 2016 Surgical Indications of Infective Endocarditis in Children Cheul Lee, MD Pediatric and Congenital Cardiac Surgery Seoul St. Mary s
2016 Annual Spring Scientific Conference of the KSC April 15-16, 2016 Surgical Indications of Infective Endocarditis in Children Cheul Lee, MD Pediatric and Congenital Cardiac Surgery Seoul St. Mary s
How does Pulmonary Hypertension Affect the Decision to Intervene in Mitral Valve Disease? NO DISCLOSURE
 How does Pulmonary Hypertension Affect the Decision to Intervene in Mitral Valve Disease? Prof. Patrizio LANCELLOTTI, MD, PhD GIGA Cardiovascular Sciences, Heart Valve Clinic, University of Liège, CHU
How does Pulmonary Hypertension Affect the Decision to Intervene in Mitral Valve Disease? Prof. Patrizio LANCELLOTTI, MD, PhD GIGA Cardiovascular Sciences, Heart Valve Clinic, University of Liège, CHU
Michael Stander, Pharm.D.
 Michael Stander, Pharm.D. Endocarditis: Goals Epidemiology Presentation of acute and subacute. Diagnosis: What is Dukes Criteria and how do we approach the diagnosis of endocarditis? Treatment: Understand
Michael Stander, Pharm.D. Endocarditis: Goals Epidemiology Presentation of acute and subacute. Diagnosis: What is Dukes Criteria and how do we approach the diagnosis of endocarditis? Treatment: Understand
Prosthetic valve dysfunction: stenosis or regurgitation
 Prosthetic valve dysfunction: stenosis or regurgitation Jean G. Dumesnil MD, FRCP(C), FACC, FASE(Hon) Quebec Heart and Lung Institute, Québec, Québec No disclosures Possible Causes of High Gradients in
Prosthetic valve dysfunction: stenosis or regurgitation Jean G. Dumesnil MD, FRCP(C), FACC, FASE(Hon) Quebec Heart and Lung Institute, Québec, Québec No disclosures Possible Causes of High Gradients in
Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis?
 EuroValves 2015, Nice Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis? Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE FESC Canada Research Chair in Valvular Heart Diseases Université LAVAL Disclosure
EuroValves 2015, Nice Prosthesis-Patient Mismatch or Prosthetic Valve Stenosis? Philippe Pibarot, DVM, PhD, FACC, FAHA, FASE FESC Canada Research Chair in Valvular Heart Diseases Université LAVAL Disclosure
Exercise PHT in valvular heart disease. Julien Magne CHU Limoges, France
 Exercise PHT in valvular heart disease Julien Magne CHU Limoges, France Faculty disclosure Julien Magne I disclose the following financial relationships: I have no financial relationships to disclose.
Exercise PHT in valvular heart disease Julien Magne CHU Limoges, France Faculty disclosure Julien Magne I disclose the following financial relationships: I have no financial relationships to disclose.
Detailed Order Request Checklists for Cardiology
 Next Generation Solutions Detailed Order Request Checklists for Cardiology 8600 West Bryn Mawr Avenue South Tower Suite 800 Chicago, IL 60631 www.aimspecialtyhealth.com Appropriate.Safe.Affordable 2018
Next Generation Solutions Detailed Order Request Checklists for Cardiology 8600 West Bryn Mawr Avenue South Tower Suite 800 Chicago, IL 60631 www.aimspecialtyhealth.com Appropriate.Safe.Affordable 2018
Echocardiographic Evaluation of Aortic Valve Prosthesis
 Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Co Director, Echocardiography, Director, Interventional Cardiology Research, Beaumont Health System
Echocardiographic Evaluation of Aortic Valve Prosthesis
 Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Director, Interventional Cardiology Research, Beaumont Health System Associate Professor of Medicine,
Echocardiographic Evaluation of Aortic Valve Prosthesis Amr E Abbas, MD, FACC, FASE, FSCAI, FSVM, RPVI Director, Interventional Cardiology Research, Beaumont Health System Associate Professor of Medicine,
Dr Babak Tamizi far MD. Assistant Professor Of Internal Medicine Al-Zahra Hospital Isfahan University Of Medical Sciences
 Dr Babak Tamizi far MD. Assistant Professor Of Internal Medicine Al-Zahra Hospital Isfahan University Of Medical Sciences ١ ٢ ٣ A 57-year-old man presents with new-onset fever, shortness of breath, lower
Dr Babak Tamizi far MD. Assistant Professor Of Internal Medicine Al-Zahra Hospital Isfahan University Of Medical Sciences ١ ٢ ٣ A 57-year-old man presents with new-onset fever, shortness of breath, lower
[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]
![[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]](/thumbs/89/98619893.jpg "[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]") 2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
More acute cardiology
 Case 1 RC 86, Male More acute cardiology Dr John Chambers Consultant Cardiologist A&E: SOB at rest. No chest pain. Exertional SOB for 6/12. PMHx: HT Rx: Ramipril 5mg od Examination: Afebrile, HR = 105,
Case 1 RC 86, Male More acute cardiology Dr John Chambers Consultant Cardiologist A&E: SOB at rest. No chest pain. Exertional SOB for 6/12. PMHx: HT Rx: Ramipril 5mg od Examination: Afebrile, HR = 105,
Aortic Stenosis and TAVR TARUN NAGRANI, MD INTERVENTIONAL AND ENDOVASCULAR CARDIOLOGIST, SOMC
 Aortic Stenosis and TAVR TARUN NAGRANI, MD INTERVENTIONAL AND ENDOVASCULAR CARDIOLOGIST, SOMC No Financial Disclosures Aortic Stenosis AS is an insidious disease with a long latency period followed by
Aortic Stenosis and TAVR TARUN NAGRANI, MD INTERVENTIONAL AND ENDOVASCULAR CARDIOLOGIST, SOMC No Financial Disclosures Aortic Stenosis AS is an insidious disease with a long latency period followed by
Indications chirurgicales dans l endocardite infectieuse
 Indications chirurgicales dans l endocardite infectieuse Bruno Hoen ICE AEPEI Agenda Indications of surgery in IE: current guidelines Impact of early valve surgery (EVS) on the prognosis of IE: is the
Indications chirurgicales dans l endocardite infectieuse Bruno Hoen ICE AEPEI Agenda Indications of surgery in IE: current guidelines Impact of early valve surgery (EVS) on the prognosis of IE: is the
March yr. old male, newspaper writer, with worsening dyspnea /orthopnea past few months
 Case 1 March 2016 59 yr. old male, newspaper writer, with worsening dyspnea /orthopnea past few months PMH diabetes, celiac disease Reports chest discomfort, positional coughing and pedal edema last 10
Case 1 March 2016 59 yr. old male, newspaper writer, with worsening dyspnea /orthopnea past few months PMH diabetes, celiac disease Reports chest discomfort, positional coughing and pedal edema last 10
10/16/2014. CCRN Review - Cardiovascular. CCRN Review - Cardiovascular. CCRN Review - Cardiovascular
 Hypertrophic (IHSS) Diagnosis Chest x ray cardiomegaly Electrocardiography LV hypertrophy, ST segment T was changes, Q waves in inferior & precordial leads Atrial & ventricular dysrhythmias Hypertrophic
Hypertrophic (IHSS) Diagnosis Chest x ray cardiomegaly Electrocardiography LV hypertrophy, ST segment T was changes, Q waves in inferior & precordial leads Atrial & ventricular dysrhythmias Hypertrophic
25 different brand names >44 different models Sizes mm
 Types of Prosthetic Valves BIOLOGIC STENTED Porcine xenograft Pericardial xenograft STENTLESS Porcine xenograft Pericardial xenograft Homograft (allograft) Autograft PERCUTANEOUS MECHANICAL Bileaflet Single
Types of Prosthetic Valves BIOLOGIC STENTED Porcine xenograft Pericardial xenograft STENTLESS Porcine xenograft Pericardial xenograft Homograft (allograft) Autograft PERCUTANEOUS MECHANICAL Bileaflet Single
TREATMENT OF ENDOCARDITIS: Destruction and Reconstruction of the Fibrous Skeleton. Gösta B. Pettersson, M.D., Ph.D. No relationships to disclose!
 TREATMENT OF ENDOCARDITIS: Destruction and Reconstruction of the Fibrous Skeleton Gösta B. Pettersson, M.D., Ph.D. The Cleveland Clinic Foundation No relationships to disclose! Adult Cardiac Surgery Symposium
TREATMENT OF ENDOCARDITIS: Destruction and Reconstruction of the Fibrous Skeleton Gösta B. Pettersson, M.D., Ph.D. The Cleveland Clinic Foundation No relationships to disclose! Adult Cardiac Surgery Symposium
Pregnancy and Heart Disease Sharon L. Roble, MD Echo Hawaii 2016
 1 Pregnancy and Heart Disease Sharon L. Roble, MD Echo Hawaii 2016 DISCLOSURES I have no disclosures relevant to today s talk 2 Cardiovascular Effects of Pregnancy Anatomic Ventricular muscle mass increases
1 Pregnancy and Heart Disease Sharon L. Roble, MD Echo Hawaii 2016 DISCLOSURES I have no disclosures relevant to today s talk 2 Cardiovascular Effects of Pregnancy Anatomic Ventricular muscle mass increases
TCTAP C-217 Bilateral Pulmonary Arterio Venus Fistula Managed by Vascular Plugs and Coil Manotosh Panja 1 1 BelleVue Clinic, India
 S450 JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY, VOL. 65, NO. 17, SUPPL S, 2015 Case Summary. Aneurysm at LVOT is a rare complication after Bentall operation and the aneurysm may increase in size. In
S450 JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY, VOL. 65, NO. 17, SUPPL S, 2015 Case Summary. Aneurysm at LVOT is a rare complication after Bentall operation and the aneurysm may increase in size. In
A new way to look at the aortic valve
 The aortic valve: impedance, misfits and bulges Felix J. Rogers, DO, FASE Oakwood Southshore Medical Center January 24, 2010 A new way to look at the aortic valve Aortic stenosis patients with the same
The aortic valve: impedance, misfits and bulges Felix J. Rogers, DO, FASE Oakwood Southshore Medical Center January 24, 2010 A new way to look at the aortic valve Aortic stenosis patients with the same
Rest and Exercise Echocardiography in Hypertrophic Cardiomyopathy: Determinants of Exercise Peak Gradient and Predictors of Outcome
 Rest and Exercise Echocardiography in Hypertrophic Cardiomyopathy: Determinants of Exercise Peak Gradient and Predictors of Outcome G. Deswarte, AS. Polge, N. Lamblin, A. Millaire, M. Richardson, C. Bauters,
Rest and Exercise Echocardiography in Hypertrophic Cardiomyopathy: Determinants of Exercise Peak Gradient and Predictors of Outcome G. Deswarte, AS. Polge, N. Lamblin, A. Millaire, M. Richardson, C. Bauters,
Blank DISCLOSURES 1/17/2017 COMPLEX VALVE CASES CHALLENGES IN EVALUATING AND MANAGING MULTIVALVULAR HEART DISEASE ECHO HAWAII 1/23/17 NONE
 Blank COMPLEX VALVE CASES ECHO HAWAII 1/23/17 1 David A. Orsinelli, MD, FACC, FASE Professor, Internal Medicine Director, Structural Heart Imaging The Ohio State University Division of Cardiovascular Medicine
Blank COMPLEX VALVE CASES ECHO HAWAII 1/23/17 1 David A. Orsinelli, MD, FACC, FASE Professor, Internal Medicine Director, Structural Heart Imaging The Ohio State University Division of Cardiovascular Medicine
Dobutamine Stress testing In Low Flow, Low EF, Low Gradient Aortic Stenosis Case Studies
 Dobutamine Stress testing In Low Flow, Low EF, Low Gradient Aortic Stenosis Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and
Dobutamine Stress testing In Low Flow, Low EF, Low Gradient Aortic Stenosis Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and
7. Echocardiography Appropriate Use Criteria (by Indication)
") Criteria for Echocardiography 1133 7. Echocardiography Criteria (by ) Table 1. TTE for General Evaluation of Cardiac Structure and Function Suspected Cardiac Etiology General With TTE 1. Symptoms or conditions
Criteria for Echocardiography 1133 7. Echocardiography Criteria (by ) Table 1. TTE for General Evaluation of Cardiac Structure and Function Suspected Cardiac Etiology General With TTE 1. Symptoms or conditions
Dysfunction of transcatheter mitral valve prosthesis. Early valve degeneration or thrombosis - that is the question.
 Dysfunction of transcatheter mitral valve prosthesis. Early valve degeneration or thrombosis - that is the question. Böhm A., Hricak V., Tomasovic B., Bena M., Postulka J. The National Institute of, Department
Dysfunction of transcatheter mitral valve prosthesis. Early valve degeneration or thrombosis - that is the question. Böhm A., Hricak V., Tomasovic B., Bena M., Postulka J. The National Institute of, Department
Μαρία Μπόνου Διευθύντρια ΕΣΥ, ΓΝΑ Λαϊκό
 Μαρία Μπόνου Διευθύντρια ΕΣΥ, ΓΝΑ Λαϊκό Diastolic HF DD: Diastolic Dysfunction DHF: Diastolic HF HFpEF: HF with preserved EF DD Pathophysiologic condition: impaired relaxation, LV compliance, LV filling
Μαρία Μπόνου Διευθύντρια ΕΣΥ, ΓΝΑ Λαϊκό Diastolic HF DD: Diastolic Dysfunction DHF: Diastolic HF HFpEF: HF with preserved EF DD Pathophysiologic condition: impaired relaxation, LV compliance, LV filling
Case Studies in Complex Endocarditis
 Case Studies in Complex Endocarditis Vera H. Rigolin, MD Professor of Medicine Northwestern University Feinberg School of Medicine Medical Director, Echocardiography Laboratory Northwestern Memorial Hospital
Case Studies in Complex Endocarditis Vera H. Rigolin, MD Professor of Medicine Northwestern University Feinberg School of Medicine Medical Director, Echocardiography Laboratory Northwestern Memorial Hospital
History. 2D echo before TAVI. 88 female Hypertensive - hyperlipidemic History of LOC syncope Echo: severe AS AV gradient 90 mmhg Good LV LVH
 History 88 female Hypertensive - hyperlipidemic History of LOC syncope Echo: severe AS AV gradient 90 mmhg Good LV LVH 2D echo before TAVI LHC: Normal cors Pre severe calcification LVOT calcification
History 88 female Hypertensive - hyperlipidemic History of LOC syncope Echo: severe AS AV gradient 90 mmhg Good LV LVH 2D echo before TAVI LHC: Normal cors Pre severe calcification LVOT calcification
ASE 2011 Appropriate Use Criteria for Echocardiography
 ASE 2011 Appropriate Use Criteria for Echocardiography Table 1. TTE for General Evaluation of Cardiac Structure and Function 1 2 Suspected Cardiac Etiology General With TTE Symptoms or conditions potentially
ASE 2011 Appropriate Use Criteria for Echocardiography Table 1. TTE for General Evaluation of Cardiac Structure and Function 1 2 Suspected Cardiac Etiology General With TTE Symptoms or conditions potentially
New murmur: acute valvular regurgitations. A.Pasquet, MD,PhD. UCL -Cliniques Saint Luc
 New murmur: acute valvular regurgitations. A.Pasquet, MD,PhD UCL -Cliniques Saint Luc Acute valvular regurgitation Clinical case Mr Dupont, a 53 y old men, without any particular medical history On Thursday
New murmur: acute valvular regurgitations. A.Pasquet, MD,PhD UCL -Cliniques Saint Luc Acute valvular regurgitation Clinical case Mr Dupont, a 53 y old men, without any particular medical history On Thursday
Infected cardiac-implantable electronic devices: diagnosis, and treatment
 Infected cardiac-implantable electronic devices: diagnosis, and treatment The incidence of infection following implantation of cardiac implantable electronic devices (CIEDs) is increasing at a faster rate
Infected cardiac-implantable electronic devices: diagnosis, and treatment The incidence of infection following implantation of cardiac implantable electronic devices (CIEDs) is increasing at a faster rate
Section 1: Initial Evaluation for Valvular Heart Disease Table 1: Initial Evaluation of an Asymptomatic Patient
 Section 1: Initial Evaluation for Valvular Heart Disease Table 1: Initial Evaluation of an Asymptomatic Patient Indication 1. Unexplained murmur or abnormal heart sounds 2. Reasonable suspicion of valvular
Section 1: Initial Evaluation for Valvular Heart Disease Table 1: Initial Evaluation of an Asymptomatic Patient Indication 1. Unexplained murmur or abnormal heart sounds 2. Reasonable suspicion of valvular
Cases of Abnormal Prosthetic Valves
 Cases of Abnormal Prosthetic Valves Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echcoardiography Associate Director, Cardiology
Cases of Abnormal Prosthetic Valves Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echcoardiography Associate Director, Cardiology
Clinical Indications for Echocardiography
 Clinical Indications for Echocardiography Echocardiography is widely utilised and potential applications are increasing with advances in technology. The aim of this document is two-fold: 1) To define clinical
Clinical Indications for Echocardiography Echocardiography is widely utilised and potential applications are increasing with advances in technology. The aim of this document is two-fold: 1) To define clinical
Looking Outside the Box: Incidental Extracardiac Finding in Echo
 Looking Outside the Box: Incidental Extracardiac Finding in Echo Dr. Aijaz Shah Head of Division, Adult Echocardiography Laboratory Prince Sultan Cardiac Centre Riyadh Case 1 17 year old boy presented
Looking Outside the Box: Incidental Extracardiac Finding in Echo Dr. Aijaz Shah Head of Division, Adult Echocardiography Laboratory Prince Sultan Cardiac Centre Riyadh Case 1 17 year old boy presented
You Won t Believe What I Saw on. Disclosures. Goals. Dimensions 2013 October 18 th Michael Pfeiffer, MD. No Financial Disclosures
 You Won t Believe What I Saw on that ECHO! Dimensions 2013 October 18 th Michael Pfeiffer, MD Disclosures No Financial Disclosures Goals Review unusual and unique echocardiographic images. Briefly present
You Won t Believe What I Saw on that ECHO! Dimensions 2013 October 18 th Michael Pfeiffer, MD Disclosures No Financial Disclosures Goals Review unusual and unique echocardiographic images. Briefly present
Mechanical versus bioprosthetic valve. Intern: Supervisor: VS
 Mechanical versus bioprosthetic valve Intern: Supervisor: VS Patient basic data ID: N102110716 Name: Age: 64 years old Sex: male Occupation: Admission date: 0960528 Chief complaint Exertional dyspnea for
Mechanical versus bioprosthetic valve Intern: Supervisor: VS Patient basic data ID: N102110716 Name: Age: 64 years old Sex: male Occupation: Admission date: 0960528 Chief complaint Exertional dyspnea for
TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central
 TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University 1 Disclosure Chiesi Pharma- Consultant
TAVR-Update Andrzej Boguszewski MD, FACC, FSCAI Vice Chairman, Cardiology Mid-Michigan Health Associate Professor Michigan State University, Central Michigan University 1 Disclosure Chiesi Pharma- Consultant
VALVULAR HEART DISEASE
 VALVULAR HEART DISEASE Stenosis: failure of a valve to open completely, obstructing forward flow. - almost always due to a chronic process (e.g., calcification or valve scarring). Insufficiency : failure
VALVULAR HEART DISEASE Stenosis: failure of a valve to open completely, obstructing forward flow. - almost always due to a chronic process (e.g., calcification or valve scarring). Insufficiency : failure
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know
 Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
Aortic Valve Practice Guidelines: What Has Changed and What You Need to Know James F. Burke, MD Program Director Cardiovascular Disease Fellowship Lankenau Medical Center Disclosure Dr. Burke has no conflicts
RF & RHD Workshop 22 nd March MANAGEMENT of RHEUMATIC HEART DISEASE in PREGNANCY. Dr Dorothy Radford
 RF & RHD Workshop 22 nd March 2016 MANAGEMENT of RHEUMATIC HEART DISEASE in PREGNANCY Dr Dorothy Radford PREGNANCY PHYSIOLOGY Increased cardiac output 30%-50% Increased blood volume 30%-50% Increased heart
RF & RHD Workshop 22 nd March 2016 MANAGEMENT of RHEUMATIC HEART DISEASE in PREGNANCY Dr Dorothy Radford PREGNANCY PHYSIOLOGY Increased cardiac output 30%-50% Increased blood volume 30%-50% Increased heart
Diagnostic approach to cardiac amyloidosis: A case report
 Diagnostic approach to cardiac amyloidosis: A case report Georgia Vogiatzi, MD, MSc, PhD 1 st Cardiology Department, Hippokration Hospital, Athens Medical School Disclosures I have no relevant relationships
Diagnostic approach to cardiac amyloidosis: A case report Georgia Vogiatzi, MD, MSc, PhD 1 st Cardiology Department, Hippokration Hospital, Athens Medical School Disclosures I have no relevant relationships
The Challenge of Managing Staphylococcus aureus Bacteremia
 The Challenge of Managing Staphylococcus aureus Bacteremia M A R G A R E T G R A Y B S P F C S H P C L I N I C A L P R A C T I C E M A N A G E R N O R T H / I D P H A R M A C I S T A L B E R T A H E A
The Challenge of Managing Staphylococcus aureus Bacteremia M A R G A R E T G R A Y B S P F C S H P C L I N I C A L P R A C T I C E M A N A G E R N O R T H / I D P H A R M A C I S T A L B E R T A H E A
Focused. se with 2008 F. lar Heart Diseas. date. ents With Valvul. Upd. gement of Patie. lines for Manag. HA 2006 Guidel ACC/AH. Fig.
 ACC/AH HA 2006 Guidel nic severe AI (Fig. 4). ned by age, ay also be helpful nd echo. For AI, ollow up may be or MRI rather than mension; SD, end lines for Manag gement of Patie Upd ents With Valvul date
ACC/AH HA 2006 Guidel nic severe AI (Fig. 4). ned by age, ay also be helpful nd echo. For AI, ollow up may be or MRI rather than mension; SD, end lines for Manag gement of Patie Upd ents With Valvul date
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease Etiology General Principles Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
BASIC KNOWLEDGE ABOUT INFECTIVE ENDOCARDITIS FOR CLINICIAN
 BASIC KNOWLEDGE ABOUT INFECTIVE ENDOCARDITIS FOR CLINICIAN When should I suspect infective endocarditis? Antibiotic regimen Patient care after completion of treatment Prophylactic Regimens Prosthetic Valve
BASIC KNOWLEDGE ABOUT INFECTIVE ENDOCARDITIS FOR CLINICIAN When should I suspect infective endocarditis? Antibiotic regimen Patient care after completion of treatment Prophylactic Regimens Prosthetic Valve
ASE Guidelines on Aortic Regurgitation What Do I Measure? Case Studies
 ASE Guidelines on Aortic Regurgitation What Do I Measure? Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and Chairman, Department
ASE Guidelines on Aortic Regurgitation What Do I Measure? Case Studies Mitral Regurgitation The New ASE Guidelines: Role of 2D/3D and CMR William A. Zoghbi MD, FASE, MACC Professor and Chairman, Department
ACUTE CENTRAL PERIFERALEMBOLISM
 EAE TEACHING COURSE 2010 Belgrade, Serbia October 22-23, 2010 ACUTE CENTRAL and PERIFERALEMBOLISM Maria João Andrade Lisbon, PT BACKGROUND Stroke is a leading cause of mortality and long-term disability
EAE TEACHING COURSE 2010 Belgrade, Serbia October 22-23, 2010 ACUTE CENTRAL and PERIFERALEMBOLISM Maria João Andrade Lisbon, PT BACKGROUND Stroke is a leading cause of mortality and long-term disability
Cardiology III 1/22/2019. Disclosures - none. But first. Objectives. Ischemia EKG s. And second
 Disclosures - none Cardiology III Matthew K Hysell, MD Spectrum Health Lakeland St Joseph, MI 1 2 Objectives Review specific high-yield EKG patterns Ischemia Ischemia mimics Electrolytes Review Cardiac/CV
Disclosures - none Cardiology III Matthew K Hysell, MD Spectrum Health Lakeland St Joseph, MI 1 2 Objectives Review specific high-yield EKG patterns Ischemia Ischemia mimics Electrolytes Review Cardiac/CV
Supplementary Online Content
 Supplementary Online Content Inohara T, Manandhar P, Kosinski A, et al. Association of renin-angiotensin inhibitor treatment with mortality and heart failure readmission in patients with transcatheter
Supplementary Online Content Inohara T, Manandhar P, Kosinski A, et al. Association of renin-angiotensin inhibitor treatment with mortality and heart failure readmission in patients with transcatheter
USE OF BALLOON VALVOTOMY AS BRIDGE TO SURGERY FOR SEVERE HIGH RISK MITRAL STENOSIS
 USE OF BALLOON VALVOTOMY AS BRIDGE TO SURGERY FOR SEVERE HIGH RISK MITRAL STENOSIS Prof. Gerald Yonga MBChB, MMed, MBA, FRCP(Edin),FESC, FACC Aga Khan University Hospital Nairobi, Kenya. RHEUMATIC HEART
USE OF BALLOON VALVOTOMY AS BRIDGE TO SURGERY FOR SEVERE HIGH RISK MITRAL STENOSIS Prof. Gerald Yonga MBChB, MMed, MBA, FRCP(Edin),FESC, FACC Aga Khan University Hospital Nairobi, Kenya. RHEUMATIC HEART
Cardiothoracic and Cardiothoracic Surgery ICD-10-CM 2014: Reference Mapping Card
 2014: Reference Mapping Card 162.3 Malignant neoplasm upper lobe lung 162.5 Malignant neoplasm lower lobe lung 162.9 lung/bronchus 396.2 396.3 Mitral insufficiency, aortic stenosis Mitral aortic valve
2014: Reference Mapping Card 162.3 Malignant neoplasm upper lobe lung 162.5 Malignant neoplasm lower lobe lung 162.9 lung/bronchus 396.2 396.3 Mitral insufficiency, aortic stenosis Mitral aortic valve
APOLLO TMVR Trial Update: Case Presentation
 APOLLO TMVR Trial Update: Case Presentation Anelechi Anyanwu, MD, MSc, FRCS-CTh Professor and Vice-Chairman Department of Cardiovascular Surgery Icahn School of Medicine at Mount Sinai New York, NY Disclosure
APOLLO TMVR Trial Update: Case Presentation Anelechi Anyanwu, MD, MSc, FRCS-CTh Professor and Vice-Chairman Department of Cardiovascular Surgery Icahn School of Medicine at Mount Sinai New York, NY Disclosure
Emergency Intraoperative Echocardiography
 Emergency Intraoperative Echocardiography Justiaan Swanevelder Department of Anaesthesia, Glenfield Hospital University Hospitals of Leicester NHS Trust, UK Carl Gustav Jung (1875-1961) Your vision will
Emergency Intraoperative Echocardiography Justiaan Swanevelder Department of Anaesthesia, Glenfield Hospital University Hospitals of Leicester NHS Trust, UK Carl Gustav Jung (1875-1961) Your vision will
Ejection across stenotic aortic valve requires a systolic pressure gradient between the LV and aorta. This places a pressure load on the LV.
 Valvular Heart Disease General Principles Etiology Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Valvular Heart Disease General Principles Etiology Cellular and molecular mechanism of valve damage Structural pathology Functional pathology - stenosis/regurgitation Loading conditions - pressure/volume
Tips & tricks on how to treat an acute heart failure patient with low cardiac output and diuretic resistance
 Tips & tricks on how to treat an acute heart failure patient with low cardiac output and diuretic resistance J. Parissis Attikon University Hospital, Athens, Greece Disclosures ALARM investigator received
Tips & tricks on how to treat an acute heart failure patient with low cardiac output and diuretic resistance J. Parissis Attikon University Hospital, Athens, Greece Disclosures ALARM investigator received
Ian T. Meredith AM. MBBS, PhD, FRACP, FCSANZ, FACC, FAPSIC. Monash HEART, Monash Health & Monash University Melbourne, Australia
 Two-Year Outcomes With the Fully Repositionable and Retrievable Lotus Transcatheter Aortic Replacement Valve in 120 High-Risk Surgical Patients With Severe Aortic Stenosis: Results From the REPRISE II
Two-Year Outcomes With the Fully Repositionable and Retrievable Lotus Transcatheter Aortic Replacement Valve in 120 High-Risk Surgical Patients With Severe Aortic Stenosis: Results From the REPRISE II
Echocardiographic Evaluation of Mitral Valve Prostheses
 Echocardiographic Evaluation of Mitral Valve Prostheses Dennis A. Tighe, M.D., FACC, FACP, FASE Cardiovascular Medicine University of Massachusetts Medical School Worcester, MA www.asecho.org 1 Nishimura
Echocardiographic Evaluation of Mitral Valve Prostheses Dennis A. Tighe, M.D., FACC, FACP, FASE Cardiovascular Medicine University of Massachusetts Medical School Worcester, MA www.asecho.org 1 Nishimura
Anaesthesia for non-cardiac surgery in patients left ventricular outflow tract obstruction (LVOTO)
") Anaesthesia for non-cardiac surgery in patients left ventricular outflow tract obstruction (LVOTO) Dr. Siân Jaggar Consultant Anaesthetist Royal Brompton Hospital London UK Congenital Cardiac Services
Anaesthesia for non-cardiac surgery in patients left ventricular outflow tract obstruction (LVOTO) Dr. Siân Jaggar Consultant Anaesthetist Royal Brompton Hospital London UK Congenital Cardiac Services
HIGHLIGHT SESSION. Imaging. J. L. Zamorano Gomez (Madrid, ES) Disclosures: Speaker Philips
 Disclosures: Speaker Philips") Imaging. J. L. Zamorano Gomez (Madrid, ES) Disclosures: Speaker Philips Agenda ECHO Diagnosis & Prognosis : Functional MR Severity Aortic Stenosis CT How to select pts for TAVI Adding prognostic info to
Imaging. J. L. Zamorano Gomez (Madrid, ES) Disclosures: Speaker Philips Agenda ECHO Diagnosis & Prognosis : Functional MR Severity Aortic Stenosis CT How to select pts for TAVI Adding prognostic info to
ECG Workshop. Nezar Amir
 ECG Workshop Nezar Amir Myocardial Ischemia ECG Infarct ECG in STEMI is dynamic & evolving Common causes of ST shift Infarct Localisation Left main artery occlusion: o diffuse ST-depression with ST elevation
ECG Workshop Nezar Amir Myocardial Ischemia ECG Infarct ECG in STEMI is dynamic & evolving Common causes of ST shift Infarct Localisation Left main artery occlusion: o diffuse ST-depression with ST elevation
Natural History and Echo Evaluation of Aortic Stenosis
 Natural History and Echo Evaluation of Aortic Stenosis Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM AORTIC STENOSIS First valvular disease
Natural History and Echo Evaluation of Aortic Stenosis Prof. Patrizio LANCELLOTTI, MD, PhD Heart Valve Clinic, University of Liège, CHU Sart Tilman, Liège, BELGIUM AORTIC STENOSIS First valvular disease
Valvular Imaging Optimizing Data Acquisition and Interpretation
 Valvular Imaging Optimizing Data Acquisition and Interpretation Suhny Abbara, MD Director Cardiovascular Imaging Section, Massachusetts General Hospital Assistant Professor, Harvard Medical School Sabbara@Partners.org
Valvular Imaging Optimizing Data Acquisition and Interpretation Suhny Abbara, MD Director Cardiovascular Imaging Section, Massachusetts General Hospital Assistant Professor, Harvard Medical School Sabbara@Partners.org
Managing Hypertrophic Cardiomyopathy with Imaging. Gisela C. Mueller University of Michigan Department of Radiology
 Managing Hypertrophic Cardiomyopathy with Imaging Gisela C. Mueller University of Michigan Department of Radiology Disclosures Gadolinium contrast material for cardiac MRI Acronyms Afib CAD Atrial fibrillation
Managing Hypertrophic Cardiomyopathy with Imaging Gisela C. Mueller University of Michigan Department of Radiology Disclosures Gadolinium contrast material for cardiac MRI Acronyms Afib CAD Atrial fibrillation
Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials
 Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials Pregnancy and Congenital Heart Disease Case Review Heidi M. Connolly, M.D. Professor of Medicine Chair for Education
Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials Pregnancy and Congenital Heart Disease Case Review Heidi M. Connolly, M.D. Professor of Medicine Chair for Education
Endocardites infectieuses Des recommandations à la pratique Quelles explorations en 2017?
 Endocardites infectieuses Des recommandations à la pratique Quelles explorations en 2017? 1 Pr Xavier Duval Conflict of interest to declare None Case History 62-year old man Bentall intervention in 2005
Endocardites infectieuses Des recommandations à la pratique Quelles explorations en 2017? 1 Pr Xavier Duval Conflict of interest to declare None Case History 62-year old man Bentall intervention in 2005
CEREBRO VASCULAR ACCIDENTS
 CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
A RARE CASE OF SEPTIC SHOCK SECONDARY TO PRIMARY STERNOCLAVICULAR JOINT SEPTIC ARTHRITIS
 A RARE CASE OF SEPTIC SHOCK SECONDARY TO PRIMARY STERNOCLAVICULAR JOINT SEPTIC ARTHRITIS Dr Ehab F. Girgis & Dr Daniel S.Z.M. Boctor National Health Service, UK TAKE HOME MESSAGES 1. SCJ Septic Arthritis
A RARE CASE OF SEPTIC SHOCK SECONDARY TO PRIMARY STERNOCLAVICULAR JOINT SEPTIC ARTHRITIS Dr Ehab F. Girgis & Dr Daniel S.Z.M. Boctor National Health Service, UK TAKE HOME MESSAGES 1. SCJ Septic Arthritis
DISCLOSURE. Echocardiography in Systemic Diseases: Questions. Relevant Financial Relationship(s) None. Off Label Usage None 5/7/2018
 None. Off Label Usage None 5/7/2018") Echocardiography in Systemic Diseases: Questions Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate
Echocardiography in Systemic Diseases: Questions Sunil Mankad, MD, FACC, FCCP, FASE Associate Professor of Medicine Mayo Clinic College of Medicine Director, Transesophageal Echocardiography Associate
Role of Stress Echo in Valvular Heart Disease. Satoshi Nakatani Osaka University Graduate School of Medicine Osaka, Japan
 Role of Stress Echo in Valvular Heart Disease Satoshi Nakatani Osaka University Graduate School of Medicine Osaka, Japan Exercise echocardiography Dobutamine echocardiography Usefulness of exercise echo
Role of Stress Echo in Valvular Heart Disease Satoshi Nakatani Osaka University Graduate School of Medicine Osaka, Japan Exercise echocardiography Dobutamine echocardiography Usefulness of exercise echo
Echo Emergencies. Outline. Michael H. Picard, MD Massachusetts General Hospital Harvard Medical School No disclosures
 Echo Emergencies Michael H. Picard, MD Massachusetts General Hospital Harvard Medical School No disclosures Outline Common emergency / on call scenarios Tamponade Pulmonary embolism/rv strain Cardiogenic
Echo Emergencies Michael H. Picard, MD Massachusetts General Hospital Harvard Medical School No disclosures Outline Common emergency / on call scenarios Tamponade Pulmonary embolism/rv strain Cardiogenic
MITRAL (Mitral Implantation of TRAnscatheter valves)
") MITRAL (Mitral Implantation of TRAnscatheter valves) 30-Day Outcomes of Transcatheter MV Replacement in Patients With Severe Mitral Valve Disease Secondary to Mitral Annular Calcification or Failed Annuloplasty
MITRAL (Mitral Implantation of TRAnscatheter valves) 30-Day Outcomes of Transcatheter MV Replacement in Patients With Severe Mitral Valve Disease Secondary to Mitral Annular Calcification or Failed Annuloplasty
Valve Disease in the Pregnant Patient
 Valve Disease in the Pregnant Patient Julie B. Damp, MD December 6, 2012 VanderbiltHeart.com If single, do not allow marriage. If fertile, do not allow pregnancy. If pregnant, do not allow delivery. If
Valve Disease in the Pregnant Patient Julie B. Damp, MD December 6, 2012 VanderbiltHeart.com If single, do not allow marriage. If fertile, do not allow pregnancy. If pregnant, do not allow delivery. If
P = 4V 2. IVC Dimensions 10/20/2014. Comprehensive Hemodynamic Evaluation by Doppler Echocardiography. The Simplified Bernoulli Equation
 Comprehensive Hemodynamic Evaluation by Doppler Echocardiography Itzhak Kronzon, MD North Shore LIJ/ Lenox Hill Hospital New York, NY Disclosure: Philips Healthcare St. Jude Medical The Simplified Bernoulli
Comprehensive Hemodynamic Evaluation by Doppler Echocardiography Itzhak Kronzon, MD North Shore LIJ/ Lenox Hill Hospital New York, NY Disclosure: Philips Healthcare St. Jude Medical The Simplified Bernoulli
Right-Sided Bacterial Endocarditis
 New Concepts in the Treatment of the Uncontrollable Infection Agustin Arbulu, M.D., Ali Kafi, M.D., Norman W. Thorns, M.D., and Robert F. Wilson, M.D. ABSTRACT Our experience with 25 patients with right-sided
New Concepts in the Treatment of the Uncontrollable Infection Agustin Arbulu, M.D., Ali Kafi, M.D., Norman W. Thorns, M.D., and Robert F. Wilson, M.D. ABSTRACT Our experience with 25 patients with right-sided