Lacunar Infarct. Dr. Tapas Kumar Banerjee Medical Director & Chief Consultant Neurologist National Neurosciences Centre Calcutta
|
|
|
- Aubrey Short
- 5 years ago
- Views:
Transcription
1 Lacunar Infarct Dr. Tapas Kumar Banerjee Medical Director & Chief Consultant Neurologist National Neurosciences Centre Calcutta

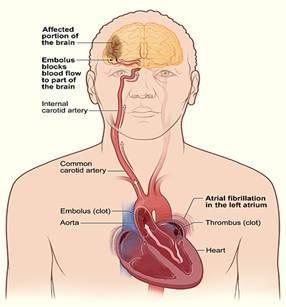
2 Aetiologies of Ischemic Stroke Atherothrombo-embolic Cardio-embolic

3 Aetiologies of Ischemic Stroke (contd) Lacunar infarction Miscellaneous Blood disorders Other non-atheromatous disease of vessel wall- SLE, PAN, Wegener s granulomatosis, etc Cryptogenic or Embolic stroke of unknown source (ESUS)
4
5 Lacunar infarct Are small, discrete, often irregular subcortical infarcts, ranging usually from 3mm to 1.5 cm in size (definitely 2cm). Caused by occlusion of a single penetrating branch of a large cerebral artery. These branches arise at acute angles from large arteries of the circle of Willis, stem of the middle cerebral artery, or the basilar artery. The gliotic infarct area removed by macrophages leaving tiny cavities or lacunes ; hence the name lacunar infarct.
6 Lacunar infarct (contd) Most commonly located in putamen (37%), pons (16%), thalamus (14%), caudate nucleus (10%), posterior limb of internal capsule (10%). Less common in anterior limb of internal capsule and cerebellum. Rarely exist in cerebral peduncles, pyramids, and subcortical white matter. NOT found in cerebral and cerebellar cortices. D/D: Dilated Virchow-Robin spaces- round or linear, < 3mm and located in lower basal ganglia region.
7 Symptoms and signs Classical Lacunar Syndromes - if located mostly at internal capsule or pons where clinically eloquent ascending and descending neural tracts are concentrated. Lacunar infarcts manifested with other types of neurological deficits. Cognitive decline- from strategically located single infarct in basal ganglia Clinically silent
8 Classic Lacunar Syndromes Fisher CM. Neurology 1982;32: Pure motor stroke/hemiparesis (commonest; 33-45%) Ataxic hemiparesis (2 nd commonest) Pure sensory stroke Mixed sensorimotor stroke Dysarthria-clumsy hand syndrome Hemiplegia/ hemiparesis that typically affects the contralateral face, arm, or leg Contralateral weakness with hemi-ataxia Conralateral persistent numbness or paresthesia Contralateral hemiplegia/ hemiparesis with hemisensory impairment Dysarthria with clumsiness of hand, especially during writing; probably a variant of ataxic hemiparesis
9 Classic Lacunar Syndromes(contd) No visual field defect No visuo-spatial disturbance No aphasia No brain-stem dysfunction, such as vertigo, diplopia, deafness, tinnitus, nystagmus, stance and gait ataxia No drowsiness
10 Other clinical manifestations of lacunar infarcts Dysphagia, dysarthria, even mutism with mild facial weakness. No limb paresis Often bilateral with pseudo-bulbar palsy and emotional incontinence Non-pyramidal hemimotor syndrome- hemi-parkinsonism, hemichorea, clumsiness, slight increased resistance to passive movement Ipsilateral 3 rd cranial nerve palsy with contralateral hemiparesis (Weber s syndrome) Ipsilateral 6 th cranial nerve palsy/ internuclear opthalmoplegia/ conjugate-gaze palsy with contralateral hemiparesis
11 Lacunar infarct in thalamus or in caudate nucleus Abulia- decreased activity, lack of motivation, long delays in response to commands Cognitive decline- strategic infarct dementia Fluctuating alertness

12 Lesion sites in lacunar syndromes

13 Lesion sites in lacunar syndromes (contd)
14 Risk factors for lacunar infarction Age Gender Hypertension Diabetes mellitus Smoking Obesity (body mass index 30kg/ m 2 ) Dyslipidemia Cardiac valvular disease
15 Pathology & pathophysiology of lacunar infarction Two types of pathology: 1. Segmental arterial disorganisation or lipohyalinosis 2. Atheroma either at the mouth or along the length of penetrating arteries
16 Risk factors for lacunar infarction (contd) If pathology is lipohyalinosis: 1. Age 2. Hypertension 3. Diabetes mellitus If pathology is microatheroma: 1. Hypertension 2. Diabetes mellitus 3. Hypercholesterolemia 4. Smoking 5. Male gender 6. Obesity
17 Risk factors for lacunar infarcts Hypertension: prerequisite for the development of lacunar infarction, with OR of The nature of cerebral small-vessel disease has been changed by more effective treatment of hypertension in the population during the last decade. Diabetes mellitus: another major risk factor in lacunar infarction with OR of Obesity: BMI 30kg/ m 2 is also an independent risk factor associated with lacunar infarcts. Hypercholeterolemia: risk factor for microatheroma but not for lipohyalinosis
18 Risk factors for incident lacunes In Rotterdam Scan Study (RSS): the incident lacunes (3-20 mm) are associated with age, female sex, and baseline carotid atherosclerosis. In Leukoaraiosis And Disability Study (LADIS): the incident lacunes (3-10 mm) were associated with WMH load, systolic BP, and low highdensity lipoprotein (HDL) cholesterol levels. There were unexpected associations with high diastolic BP and high LDL cholesterol as factors protecting against incident lacunes. This disparity between the above studies is because individual with small lacunes and with at least some degree of WMH were only included in the 2 nd study.

19 Investigations MRI scan of brain in: T2-wt, FLAIR, T1-wt, DWI and ADC sequences

20 Figure Different shapes of lacunae-sized infarcts(a, B) On diffusion-weighted MRI, small single lacunar infarcts are observed in the left thalamus and left corona radiata. Dong Woo Ryu et al. Neurology 2012;78: Copyright 2012 by AAN Enterprises, Inc.

21 Investigations (contd) MR-angiography/ CT-angiography of intra-cranial and extra-cranial arteries
22 Treatment & prevention THROMBOLYSIS: IV t-pa was found to be as effective a treatment in acute lacunar stroke as in non-lacunar strokes. Current consensus guidelines do not distinguish between ischemic stroke subtypes in terms of t-pa efficacy. CONTROL OF HYPERTENSION: Reduction of systolic BP< 130 to prevent lacunar stroke. BP management may have be more cautiously made in patients with advanced age, a long history of hypertension, extensive WMH, or cognitive dysfunction. ROLE OF STATINS: Statins may increase the risk of bleeding, but this may be outweighed by reduction of ischemic stroke risk. So current guideline for statin use applicable in lacunar stroke as in other types.
23 Treatment & prevention (contd) ANTIPLATELETS: Currently aspirin, aspirin plus dipyridamole and clopidogrel are the acceptable options. Among patients with recent lacunar stroke, the addition of clopidogrel to aspirin does not significantly reduce the risk of recurrent stroke; on the contrary significantly increase the risk of bleeding and death. CONTROL OF DIABETES MELLITUS AVOIDANCE OF SMOKING WEIGHT REDUCTION
24 Outcome of lacunar infarct In lacunar infarcts, the rate of recovery is normally rapid, quite naturally because the primary lesion is small. Mortality was lowest in patients with lacunar stroke, intermediate in athero-thrombotic stroke and highest in cardio-embolic stroke. Small-artery occlusion subgroups were 3 times more likely to be alive at 2 years than those with cardio-embolism.
25 Outcome of lacunar infarct (contd) Risk of recurrent stroke: 1. The average rate of recurrent stroke at 1 year in all studies was 7 7% (range 2 12%) whereas the cumulative rate at 4 5 years was 22 4% (range 15 28%). 2. In most studies the risk of recurrent stroke after the first year was about 4 6% per year. 3. The annual rate of stroke recurrence decreased from about 5% during the first 5 years, to less than 1% between 5 and 10 years after the first stroke.
26 Outcome of lacunar infarct (contd) Prognosis for patients with lacunar infarct is more favorable in terms of survival and disability than for those with other stroke subtypes during the first few years, which is probably explained simply by the small lesion size. But there is progressive accumulation of silent multiple lacunar infarcts over the years. At 10 years after onset, a third or less of patients are still alive and free of recurrent stroke, but a large proportion of survivors are disabled, and have either some amount of cognitive impairment or are frankly demented (vascular dementia-parkinsonism)
27 Vascular Dementia Large-vessel vascular dementia Hemorrhagic vascular dementia Ischemic hypo-perfusive vascular dementia Subcortical ischemic vascular dementia (SIVD)
28 Subcortical ischemic vascular dementia (SIVD) Two core pathological features are: 1. Multiple lacunar infarcts (etat lacunaire) 2. Binswanger s disease

29 Multiple lacunar infarcts

30 Binswanger s disease Binswanger s disease is due to incomplete infarction or diffuse ischemia. Pathologically, there is demyelination as well as axonal and oligodendrocyte loss with sparing of the U- fibres. Cerebral MRI shows diffuse white matter hyperintensities with sparing of the U-fibres.
00190-4) Copyright 2002 Elsevier Ltd Terms")
31 Figure 1 The Lancet Neurology , DOI: ( /S (02) ) Copyright 2002 Elsevier Ltd Terms and Conditions
00190-4) Copyright 2002 Elsevier Ltd Terms")
32 Figure 2 The Lancet Neurology , DOI: ( /S (02) ) Copyright 2002 Elsevier Ltd Terms and Conditions
33 Pharmacotherapy for vascular dementia Risk factor modification (hypertension, diabetes mellitus, etc) is mandatory Cognition, stabilization of global functioning, behavior: donepezil, rivastigmine, galantamine, memantine Depression, anxiety: SSRI (tricylcic antidepressants discouraged owing to anticholinergic effects including orthostatic hypotension) Agitation, disruptive behavior: atypical antipsychotics Probably modest efficacy in vascular dementia: piracetam, aspirin, citicoline, pentoxiphyllin, etc
34 Conclusion Recent long-term prospective studies have changed our views of lacunar infarcts. Once thought benign and innocuous vascular lesions, lacunar infarct is now regarded as important markers of cerebral small-vessel disease with a high risk of unfavorable outcome with time. Asymptomatic progression of cerebral small-vessel disease is several times more common than new strokes, and is likely to be detrimental to brain function. Risk factor modification plays a central part in therapeutic intevention of lacunar infarcts.

35
Stroke School for Internists Part 1
 Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
Stroke School for Internists Part 1 November 4, 2017 Dr. Albert Jin Dr. Gurpreet Jaswal Disclosures I receive a stipend for my role as Medical Director of the Stroke Network of SEO I have no commercial
TIA AND STROKE. Topics/Order of the day 1. Topics/Order of the day 2 01/08/2012
 Charles Ashton Medical Director TIA AND STROKE Topics/Order of the day 1 What Works? Clinical features of TIA inc the difference between Carotid and Vertebral territories When is a TIA not a TIA TIA management
Charles Ashton Medical Director TIA AND STROKE Topics/Order of the day 1 What Works? Clinical features of TIA inc the difference between Carotid and Vertebral territories When is a TIA not a TIA TIA management
Neuroanatomy of a Stroke. Joni Clark, MD Professor of Neurology Barrow Neurologic Institute
 Neuroanatomy of a Stroke Joni Clark, MD Professor of Neurology Barrow Neurologic Institute No disclosures Stroke case presentations Review signs and symptoms Review pertinent exam findings Identify the
Neuroanatomy of a Stroke Joni Clark, MD Professor of Neurology Barrow Neurologic Institute No disclosures Stroke case presentations Review signs and symptoms Review pertinent exam findings Identify the
CVA. Alison Atwater PA-C
 CVA Alison Atwater PA-C Types of CVAs Ischemic strokes 80% of strokes 2/3 are thrombotic 1/3 are embolic emboli from the heart or arteries feeding the brain such as carotids, vertebral and basilar etc
CVA Alison Atwater PA-C Types of CVAs Ischemic strokes 80% of strokes 2/3 are thrombotic 1/3 are embolic emboli from the heart or arteries feeding the brain such as carotids, vertebral and basilar etc
Key Clinical Concepts
 Cerebrovascular Review and General Vascular Syndromes, Including Those That Impact Dizziness Key Clinical Concepts Basic Review of Cerebrovascular Circulation Circulation to the brain is divided into anterior
Cerebrovascular Review and General Vascular Syndromes, Including Those That Impact Dizziness Key Clinical Concepts Basic Review of Cerebrovascular Circulation Circulation to the brain is divided into anterior
Small Vessel Stroke. Domenico Inzitari Careggi University Hospital Florence (Italy)
") Small Vessel Stroke Domenico Inzitari Careggi University Hospital Florence (Italy) Topics Lacunar stroke The small vessel conundrum Small and large Conclusions Fisher s lacunar syndromes Pure motor hemiparesis
Small Vessel Stroke Domenico Inzitari Careggi University Hospital Florence (Italy) Topics Lacunar stroke The small vessel conundrum Small and large Conclusions Fisher s lacunar syndromes Pure motor hemiparesis
Essentials of Clinical MR, 2 nd edition. 14. Ischemia and Infarction II
 14. Ischemia and Infarction II Lacunar infarcts are small deep parenchymal lesions involving the basal ganglia, internal capsule, thalamus, and brainstem. The vascular supply of these areas includes the
14. Ischemia and Infarction II Lacunar infarcts are small deep parenchymal lesions involving the basal ganglia, internal capsule, thalamus, and brainstem. The vascular supply of these areas includes the
Acute stroke. Ischaemic stroke. Characteristics. Temporal classification. Clinical features. Interpretation of Emergency Head CT
 Ischaemic stroke Characteristics Stroke is the third most common cause of death in the UK, and the leading cause of disability. 80% of strokes are ischaemic Large vessel occlusive atheromatous disease
Ischaemic stroke Characteristics Stroke is the third most common cause of death in the UK, and the leading cause of disability. 80% of strokes are ischaemic Large vessel occlusive atheromatous disease
[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]
![[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]](/thumbs/89/98619893.jpg "[(PHY-3a) Initials of MD reviewing films] [(PHY-3b) Initials of 2 nd opinion MD]") 2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
2015 PHYSICIAN SIGN-OFF (1) STUDY NO (PHY-1) CASE, PER PHYSICIAN REVIEW 1=yes 2=no [strictly meets case definition] (PHY-1a) CASE, IN PHYSICIAN S OPINION 1=yes 2=no (PHY-2) (PHY-3) [based on all available
Stroke/TIA. Tom Bedwell
 Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
CEREBRO VASCULAR ACCIDENTS
 CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
/ / / / / / Hospital Abstraction: Stroke/TIA. Participant ID: Hospital Code: Multi-Ethnic Study of Atherosclerosis
 Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes. Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville
 Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville Disclosure Statement of Financial Interest Within the
Overview of Stroke: Etiologies, Demographics, Syndromes, and Outcomes Alex Abou-Chebl, MD, FSVIN Medical Director, Stroke Baptist Health Louisville Disclosure Statement of Financial Interest Within the
The NIHSS score is 4 (considering 2 pts for the ataxia involving upper and lower limbs.
 Neuroscience case 5 1. Speech comprehension, ability to speak, and word use were normal in Mr. Washburn, indicating that aphasia (cortical language problem) was not involved. However, he did have a problem
Neuroscience case 5 1. Speech comprehension, ability to speak, and word use were normal in Mr. Washburn, indicating that aphasia (cortical language problem) was not involved. However, he did have a problem
Cerebrovascular Disorders. Blood, Brain, and Energy. Blood Supply to the Brain 2/14/11
 Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
Nicolas Bianchi M.D. May 15th, 2012
 Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
Posterior Circulation Stroke
 Posterior Circulation Stroke Brett Kissela, MD, MS Professor and Chair Department of Neurology and Rehabilitation Medicine Senior Associate Dean of Clinical Research University of Cincinnati College of
Posterior Circulation Stroke Brett Kissela, MD, MS Professor and Chair Department of Neurology and Rehabilitation Medicine Senior Associate Dean of Clinical Research University of Cincinnati College of
8/24/2015. It is divided into an a. Anterior limb b. Posterior limb c. Genu (or knee)
") Joint Commission Technical Advisory Panel (TAP) for Comprehensive Stroke Centers no monetary benefits Debbie Summers, MSN, RN, ACNS-BC, CNRN, SCRN, FAHA, ANVP Evaluates the structures of the internal capsule
Joint Commission Technical Advisory Panel (TAP) for Comprehensive Stroke Centers no monetary benefits Debbie Summers, MSN, RN, ACNS-BC, CNRN, SCRN, FAHA, ANVP Evaluates the structures of the internal capsule
Stroke: clinical presentations, symptoms and signs
 Stroke: clinical presentations, symptoms and signs Professor Peter Sandercock University of Edinburgh EAN teaching course Burkina Faso 8 th November 2017 Clinical diagnosis is important to Ensure stroke
Stroke: clinical presentations, symptoms and signs Professor Peter Sandercock University of Edinburgh EAN teaching course Burkina Faso 8 th November 2017 Clinical diagnosis is important to Ensure stroke
University Journal of Medicine and Medical Sciences
 ISSN 2455-2852 Volume 2 Issue 5 2016 Case report -Opalski's syndrome A rare variant of lateral medullary syndrome in TAKAYASUS ARTERITIS SHANKAR GANESH N NAINAR Department of Neurology, MADRAS MEDICAL
ISSN 2455-2852 Volume 2 Issue 5 2016 Case report -Opalski's syndrome A rare variant of lateral medullary syndrome in TAKAYASUS ARTERITIS SHANKAR GANESH N NAINAR Department of Neurology, MADRAS MEDICAL
Inside Your Patient s Brain Michelle Peterson, APRN, CNP Centracare Stroke and Vascular Neurology
 Inside Your Patient s Brain Michelle Peterson, APRN, CNP Centracare Stroke and Vascular Neurology Activity Everyone stand up, raise your right hand, tell your neighbors your name 1 What part of the brain
Inside Your Patient s Brain Michelle Peterson, APRN, CNP Centracare Stroke and Vascular Neurology Activity Everyone stand up, raise your right hand, tell your neighbors your name 1 What part of the brain
Cerebral small vessel disease
 Cerebral small vessel disease What is it? What are the clinical syndromes? How do we diagnose it? What is the pathophysiology? New insights from genetics? Possible therapies? Small Vessel disease Changes
Cerebral small vessel disease What is it? What are the clinical syndromes? How do we diagnose it? What is the pathophysiology? New insights from genetics? Possible therapies? Small Vessel disease Changes
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
Alan Barber Professor of Clinical Neurology University of Auckland Presented with Non-fluent dysphasia R facial weakness Background Ischaemic heart disease Hypertension Hyperlipidemia L MCA branch
Vascular Dementia. Laura Pedelty, PhD MD The University of Illinois at Chicago and Jesse Brown VA Medical Center
 Vascular Dementia Laura Pedelty, PhD MD The University of Illinois at Chicago and Jesse Brown VA Medical Center none Disclosures Objectives To review the definition of Vascular Cognitive Impairment (VCI);
Vascular Dementia Laura Pedelty, PhD MD The University of Illinois at Chicago and Jesse Brown VA Medical Center none Disclosures Objectives To review the definition of Vascular Cognitive Impairment (VCI);
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Blood Supply. Allen Chung, class of 2013
 Blood Supply Allen Chung, class of 2013 Objectives Understand the importance of the cerebral circulation. Understand stroke and the types of vascular problems that cause it. Understand ischemic penumbra
Blood Supply Allen Chung, class of 2013 Objectives Understand the importance of the cerebral circulation. Understand stroke and the types of vascular problems that cause it. Understand ischemic penumbra
The Epidemiology of Stroke and Vascular Risk Factors in Cognitive Aging
 The Epidemiology of Stroke and Vascular Risk Factors in Cognitive Aging REBECCA F. GOTTESMAN, MD PHD ASSOCIATE PROFESSOR OF NEUROLOGY AND EPIDEMIOLOGY JOHNS HOPKINS UNIVERSITY OCTOBER 20, 2014 Outline
The Epidemiology of Stroke and Vascular Risk Factors in Cognitive Aging REBECCA F. GOTTESMAN, MD PHD ASSOCIATE PROFESSOR OF NEUROLOGY AND EPIDEMIOLOGY JOHNS HOPKINS UNIVERSITY OCTOBER 20, 2014 Outline
Spinal Cord: Clinical Applications. Dr. Stuart Inglis
 Spinal Cord: Clinical Applications Dr. Stuart Inglis Tabes dorsalis, also known as syphilitic myelopathy, is a slow degeneration (specifically, demyelination) of the nerves in the dorsal funiculus of the
Spinal Cord: Clinical Applications Dr. Stuart Inglis Tabes dorsalis, also known as syphilitic myelopathy, is a slow degeneration (specifically, demyelination) of the nerves in the dorsal funiculus of the
the face department, Geneva University Hospitals and University of Geneva, Rue Micheli-du-Crest
 Final article published in Journal of Neurology 2009 Jun;256(6):1017-8. http://dx.doi.org/10.1007/s00415-009-5041-6. Sixth cranial nerve palsy and contralateral hemiparesis (Raymond s syndrome) sparing
Final article published in Journal of Neurology 2009 Jun;256(6):1017-8. http://dx.doi.org/10.1007/s00415-009-5041-6. Sixth cranial nerve palsy and contralateral hemiparesis (Raymond s syndrome) sparing
CMS Limitations Guide - Radiology Services
 CMS Limitations Guide - Radiology Services Starting October 1, 2015, CMS will update their existing medical necessity limitations on tests and procedures to correspond to ICD-10 codes. This limitations
CMS Limitations Guide - Radiology Services Starting October 1, 2015, CMS will update their existing medical necessity limitations on tests and procedures to correspond to ICD-10 codes. This limitations
Pure motor hemiparesis (PMH) and ataxic hemiparesis
 and ataxic hemiparesis") Somatosensory Evoked Potentials in Lacunar Syndromes of Pure Motor and Ataxic Hemiparesis 09 Michael A. Kelly, MD, Stuart J. Perlik, MD, and Morris A. Fisher, MD Syndromes of hemlparetic lacunar infarction
Somatosensory Evoked Potentials in Lacunar Syndromes of Pure Motor and Ataxic Hemiparesis 09 Michael A. Kelly, MD, Stuart J. Perlik, MD, and Morris A. Fisher, MD Syndromes of hemlparetic lacunar infarction
Speakers. 2015, American Heart Association 1
 Speakers Lee Schwamm, MD, FAHA Executive Vice Chairman of Neurology, Massachusetts General Hospital Director, Stroke Service and Medical Director, MGH TeleHealth, Massachusetts General Hospital Director,
Speakers Lee Schwamm, MD, FAHA Executive Vice Chairman of Neurology, Massachusetts General Hospital Director, Stroke Service and Medical Director, MGH TeleHealth, Massachusetts General Hospital Director,
Disclosure Statement: Dr. Knoefel has nothing to disclose
 Stroke Janice E. Knoefel, MD, MPH Professor of Medicine & Neurology University of New Mexico Geriatrics/Extended Care (retired) New Mexico VA Healthcare System Albuquerque, NM Disclosure Statement: Dr.
Stroke Janice E. Knoefel, MD, MPH Professor of Medicine & Neurology University of New Mexico Geriatrics/Extended Care (retired) New Mexico VA Healthcare System Albuquerque, NM Disclosure Statement: Dr.
Brain Attacks and Acute Stroke Management
 Brain Attacks and Acute Stroke Management WWW.RN.ORG Reviewed January, 2017, Expires January, 2019 Provider Information and Specifics available on our Website Unauthorized Distribution Prohibited 2017
Brain Attacks and Acute Stroke Management WWW.RN.ORG Reviewed January, 2017, Expires January, 2019 Provider Information and Specifics available on our Website Unauthorized Distribution Prohibited 2017
Functional Distinctions
 Functional Distinctions FUNCTION COMPONENT DEFICITS Start Basal Ganglia Spontaneous Movements Move UMN/LMN Cerebral Cortex Brainstem, Spinal cord Roots/peripheral nerves Plan Cerebellum Ataxia Adjust Cerebellum
Functional Distinctions FUNCTION COMPONENT DEFICITS Start Basal Ganglia Spontaneous Movements Move UMN/LMN Cerebral Cortex Brainstem, Spinal cord Roots/peripheral nerves Plan Cerebellum Ataxia Adjust Cerebellum
Cerebrovascular Disease
 Cerebrovascular Disease I. INTRODUCTION Cerebrovascular disease (CVD) includes all disorders in which an area of the brain is transiently or permanently affected by ischemia or bleeding and one or more
Cerebrovascular Disease I. INTRODUCTION Cerebrovascular disease (CVD) includes all disorders in which an area of the brain is transiently or permanently affected by ischemia or bleeding and one or more
Diagnosis and management of non-alzheimer dementias. Melissa Yu, M.D. Department of Neurology
 Diagnosis and management of non-alzheimer dementias Melissa Yu, M.D. Department of Neurology AGENDA Introduction When to think of alternate diagnoses Other forms of dementia Other reasons for confusion
Diagnosis and management of non-alzheimer dementias Melissa Yu, M.D. Department of Neurology AGENDA Introduction When to think of alternate diagnoses Other forms of dementia Other reasons for confusion
Assessing the Stroke Patient. Arlene Boudreaux, MSN, RN, CCRN, CNRN
 Assessing the Stroke Patient Arlene Boudreaux, MSN, RN, CCRN, CNRN Cincinnati Pre-Hospital Stroke Scale May be done by EMS o One of many o F facial droop on one side o A arm drift (hold a pizza box, close
Assessing the Stroke Patient Arlene Boudreaux, MSN, RN, CCRN, CNRN Cincinnati Pre-Hospital Stroke Scale May be done by EMS o One of many o F facial droop on one side o A arm drift (hold a pizza box, close
TACLS-Chapter-2-Body-Structure.pdf Essential Resources
 Stroke Network 1. http://www.strokebestpractices.ca/wp-content/uploads/2016/01/ TACLS-Chapter-2-Body-Structure.pdf Essential Resources Stroke Rehabilitation Unit Orientation Module 1: Pathophysiology of
Stroke Network 1. http://www.strokebestpractices.ca/wp-content/uploads/2016/01/ TACLS-Chapter-2-Body-Structure.pdf Essential Resources Stroke Rehabilitation Unit Orientation Module 1: Pathophysiology of
How to Think like a Neurologist Review of Exam Process and Assessment Findings
 Lehigh Valley Health Network LVHN Scholarly Works Neurology Update for the Non-Neurologist 2013 Neurology Update for the Non-Neurologist Feb 20th, 5:10 PM - 5:40 PM How to Think like a Neurologist Review
Lehigh Valley Health Network LVHN Scholarly Works Neurology Update for the Non-Neurologist 2013 Neurology Update for the Non-Neurologist Feb 20th, 5:10 PM - 5:40 PM How to Think like a Neurologist Review
Stroke - Intracranial hemorrhage. Dr. Amitesh Aggarwal Associate Professor Department of Medicine
 Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Research Article Corticospinal Tract Change during Motor Recovery in Patients with Medulla Infarct: A Diffusion Tensor Imaging Study
 BioMed Research International, Article ID 524096, 5 pages http://dx.doi.org/10.1155/2014/524096 Research Article Corticospinal Tract Change during Motor Recovery in Patients with Medulla Infarct: A Diffusion
BioMed Research International, Article ID 524096, 5 pages http://dx.doi.org/10.1155/2014/524096 Research Article Corticospinal Tract Change during Motor Recovery in Patients with Medulla Infarct: A Diffusion
Permanent foramen ovale: when to close?
 Permanent foramen ovale: when to close? Pierre Amarenco INSERM U-698 and Denis Diderot University - Paris VII Department of Neurology and Stroke Center Bichat hospital, Paris, France PFO - Pathology TEE
Permanent foramen ovale: when to close? Pierre Amarenco INSERM U-698 and Denis Diderot University - Paris VII Department of Neurology and Stroke Center Bichat hospital, Paris, France PFO - Pathology TEE
Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis
/intracranial atherosclerosis") Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis Tim Mikesell, D.O. Oct 22, 2016 Stroke facts Despite progress in decreasing stroke incidence and mortality, stroke
Management of intracranial atherosclerotic stenosis (ICAS)/intracranial atherosclerosis Tim Mikesell, D.O. Oct 22, 2016 Stroke facts Despite progress in decreasing stroke incidence and mortality, stroke
TIAs and posterior circulation problems
 TIAs and posterior circulation problems A/Professor Helen Dewey Head, Stroke Service Austin Health Austin Health How many strokes and TIAs are out there? depends on the definition! ~60,000 strokes in
TIAs and posterior circulation problems A/Professor Helen Dewey Head, Stroke Service Austin Health Austin Health How many strokes and TIAs are out there? depends on the definition! ~60,000 strokes in
HYPERTENSIVE ENCEPHALOPATHY
 HYPERTENSIVE ENCEPHALOPATHY Reversible posterior leukoencephalopathy syndrome Cause Renal disease Pheochromocytoma Disseminated vasculitis Eclampsia Acute toxemia Medications & illicit drugs (cocaine)
HYPERTENSIVE ENCEPHALOPATHY Reversible posterior leukoencephalopathy syndrome Cause Renal disease Pheochromocytoma Disseminated vasculitis Eclampsia Acute toxemia Medications & illicit drugs (cocaine)
FILE / PERIVENTRICULAR MICROVASCULAR ISCHEMIC CHANGES EBOOK
 07 June, 2018 FILE / PERIVENTRICULAR MICROVASCULAR ISCHEMIC CHANGES EBOOK Document Filetype: PDF 365.11 KB 0 FILE / PERIVENTRICULAR MICROVASCULAR ISCHEMIC CHANGES EBOOK I recently had a MRI last week with
07 June, 2018 FILE / PERIVENTRICULAR MICROVASCULAR ISCHEMIC CHANGES EBOOK Document Filetype: PDF 365.11 KB 0 FILE / PERIVENTRICULAR MICROVASCULAR ISCHEMIC CHANGES EBOOK I recently had a MRI last week with
 CLINICAL FEATURES THAT SUPPORT ATHEROSCLEROTIC STROKE 1. cerebral cortical impairment (aphasia, neglect, restricted motor involvement, etc.) or brain stem or cerebellar dysfunction 2. lacunar clinical
CLINICAL FEATURES THAT SUPPORT ATHEROSCLEROTIC STROKE 1. cerebral cortical impairment (aphasia, neglect, restricted motor involvement, etc.) or brain stem or cerebellar dysfunction 2. lacunar clinical
Cryptogenic Strokes: Evaluation and Management
 Cryptogenic Strokes: Evaluation and Management 77 yo man with hypertension and hyperlipidemia developed onset of left hemiparesis and right gaze preference, last seen normal at 10:00 AM Brought to ZSFG
Cryptogenic Strokes: Evaluation and Management 77 yo man with hypertension and hyperlipidemia developed onset of left hemiparesis and right gaze preference, last seen normal at 10:00 AM Brought to ZSFG
Stroke 101. Maine Cardiovascular Health Summit. Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013
 Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
Stroke 101 Maine Cardiovascular Health Summit Eileen Hawkins, RN, MSN, CNRN Pen Bay Stroke Program Coordinator November 7, 2013 Stroke Statistics Definition of stroke Risk factors Warning signs Treatment
PRESERVE: How intensively should we treat blood pressure in established cerebral small vessel disease? Guide to assessing MRI scans
 PRESERVE: How intensively should we treat blood pressure in established cerebral small vessel disease? Guide to assessing MRI scans Inclusion Criteria Clinical syndrome Patients must have clinical evidence
PRESERVE: How intensively should we treat blood pressure in established cerebral small vessel disease? Guide to assessing MRI scans Inclusion Criteria Clinical syndrome Patients must have clinical evidence
Imaging Acute Stroke and Cerebral Ischemia
 Department of Radiology University of California San Diego Imaging Acute Stroke and Cerebral Ischemia John R. Hesselink, M.D. Causes of Stroke Arterial stenosis Thrombosis Embolism Dissection Hypotension
Department of Radiology University of California San Diego Imaging Acute Stroke and Cerebral Ischemia John R. Hesselink, M.D. Causes of Stroke Arterial stenosis Thrombosis Embolism Dissection Hypotension
Approach to a Neurologic Diagnosis
 Approach to a Neurologic Diagnosis Neurologic Diagnosis History Physical & Neurological Examination Ancillary Procedures 3 Questions Asked Focal neurologic deficits Increased intracranial pressure Signs
Approach to a Neurologic Diagnosis Neurologic Diagnosis History Physical & Neurological Examination Ancillary Procedures 3 Questions Asked Focal neurologic deficits Increased intracranial pressure Signs
Raluca Pavaloiu et al. - Clinical, Epidemiological and Etiopathogenic Study of Ischemic Stroke
 Original Paper Clinical, Epidemiological and Etiopathogenic Study of Ischemic Stroke RALUCA PAVALOIU 1, L. MOGOANTA 2 1 Department of Neurology, Hospital of Neuropsychiatry Craiova, Romania 2 Department
Original Paper Clinical, Epidemiological and Etiopathogenic Study of Ischemic Stroke RALUCA PAVALOIU 1, L. MOGOANTA 2 1 Department of Neurology, Hospital of Neuropsychiatry Craiova, Romania 2 Department
INSTITUTE OF NEUROSURGERY & DEPARTMENT OF PICU
 CEREBRAL BYPASS An Innovative Treatment for Arteritis INSTITUTE OF NEUROSURGERY & DEPARTMENT OF PICU CASE 1 q 1 year old girl -recurrent seizure, right side limb weakness, excessive cry and irritability.
CEREBRAL BYPASS An Innovative Treatment for Arteritis INSTITUTE OF NEUROSURGERY & DEPARTMENT OF PICU CASE 1 q 1 year old girl -recurrent seizure, right side limb weakness, excessive cry and irritability.
Appendix 2C - Stroke Services in Fife
 Appendix 2C - Stroke Services in Fife Stroke and TIA Management Guidance for GPs The aim of this document is to; Inform GPs of acute stroke services in Fife Summarise who to admit and describe acute management
Appendix 2C - Stroke Services in Fife Stroke and TIA Management Guidance for GPs The aim of this document is to; Inform GPs of acute stroke services in Fife Summarise who to admit and describe acute management
Disorders of language and speech. Samuel Komoly MD PhD DHAS Professor and Chairman Department of Neurology
 Disorders of language and speech Samuel Komoly MD PhD DHAS Professor and Chairman Department of Neurology http://neurology.pote.hu major categories disorders of language and speech cortical types aphasias
Disorders of language and speech Samuel Komoly MD PhD DHAS Professor and Chairman Department of Neurology http://neurology.pote.hu major categories disorders of language and speech cortical types aphasias
The Importance of Middle Cerebral Artery Stenosis In Patients With A Lacunar Infarction In The Carotid Artery Territory
 The Importance of Middle Cerebral Artery Stenosis In Patients With A Lacunar Infarction In The Carotid Artery Territory Oh Young Bang, M.D., Jeong Hoon Cho, M.D., Ji Hoe Heo, M.D., Dong Ik Kim, M.D.* Department
The Importance of Middle Cerebral Artery Stenosis In Patients With A Lacunar Infarction In The Carotid Artery Territory Oh Young Bang, M.D., Jeong Hoon Cho, M.D., Ji Hoe Heo, M.D., Dong Ik Kim, M.D.* Department
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine
 Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
Size Matters: Differentiating Large Vessel Occlusion (LVO) and Small Vessel Occlusion (SVO) in Stroke
 and Small Vessel Occlusion (SVO) in Stroke") Size Matters: Differentiating Large Vessel Occlusion (LVO) and Small Vessel Occlusion (SVO) in Stroke Charles E. Romero, M.D. UPMC Hamot Great Lakes Neurosurgery & Neurointervention Case 1 83 yo RH F with
Size Matters: Differentiating Large Vessel Occlusion (LVO) and Small Vessel Occlusion (SVO) in Stroke Charles E. Romero, M.D. UPMC Hamot Great Lakes Neurosurgery & Neurointervention Case 1 83 yo RH F with
Dr Ben Turner. Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital
 Stroke Management Dr Ben Turner Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital Introduction Stroke is the major cause of disability in the developed
Stroke Management Dr Ben Turner Consultant Neurologist and Honorary Senior Lecturer Barts and The London NHS Trust London Bridge Hospital Introduction Stroke is the major cause of disability in the developed
Silent Infarction in Patients with First-ever Stroke
 221 Silent Infarction in Patients with First-ever Stroke Cheung-Ter Ong 1, Wen-Pin Chen 2, Sheng-Feng Sung 1, Chi-Shun Wu 1, and Yung-Chu Hsu 1 Abstract- Background / Purpose: Silent infarcts (SIs) are
221 Silent Infarction in Patients with First-ever Stroke Cheung-Ter Ong 1, Wen-Pin Chen 2, Sheng-Feng Sung 1, Chi-Shun Wu 1, and Yung-Chu Hsu 1 Abstract- Background / Purpose: Silent infarcts (SIs) are
CN V! touch! pain! Touch! P/T!
 CN V! touch! pain! Touch! P/T! Visual Pathways! L! R! B! A! C! D! LT! E! F! RT! G! hypothalamospinal! and! ALS! Vestibular Pathways! 1. Posture/Balance!!falling! 2. Head Position! 3. Eye-Head Movements
CN V! touch! pain! Touch! P/T! Visual Pathways! L! R! B! A! C! D! LT! E! F! RT! G! hypothalamospinal! and! ALS! Vestibular Pathways! 1. Posture/Balance!!falling! 2. Head Position! 3. Eye-Head Movements
Acute stroke imaging
 Acute stroke imaging Aims Imaging modalities and differences Why image acute stroke Clinical correlation to imaging appearance What is stroke Classic definition: acute focal injury to the central nervous
Acute stroke imaging Aims Imaging modalities and differences Why image acute stroke Clinical correlation to imaging appearance What is stroke Classic definition: acute focal injury to the central nervous
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination pulse 80/min reg, BP 160/95
STROKE UPDATE ANTHEA PARRY MAY 2010
 STROKE UPDATE ANTHEA PARRY MAY 2010 Delivery of stroke care Clinical presentations Management Health Care for London plan 8 HASU (hyperacute) units 20 stroke units TIA services Hyperacute stroke units
STROKE UPDATE ANTHEA PARRY MAY 2010 Delivery of stroke care Clinical presentations Management Health Care for London plan 8 HASU (hyperacute) units 20 stroke units TIA services Hyperacute stroke units
An Introduc+on to Stroke
 An Introduc+on to Stroke Elizabeth Huntoon MS, MD Assistant Professor Department of Physical Medicine and Rehabilita>on Vanderbilt University School of Medicine Defini+on Sudden focal neurologic deficit
An Introduc+on to Stroke Elizabeth Huntoon MS, MD Assistant Professor Department of Physical Medicine and Rehabilita>on Vanderbilt University School of Medicine Defini+on Sudden focal neurologic deficit
Lab 2. we will look into several angled horizontal sections ( orbitomeatal plane ) i.e passing from the orbit into the ear
 i.e passing from the orbit into the ear") we will look into several angled horizontal sections ( orbitomeatal plane ) i.e passing from the orbit into the ear Figure I page 76 : looking at the key on the left side this section passed through the
we will look into several angled horizontal sections ( orbitomeatal plane ) i.e passing from the orbit into the ear Figure I page 76 : looking at the key on the left side this section passed through the
Principles Arteries & Veins of the CNS LO14
 Principles Arteries & Veins of the CNS LO14 14. Identify (on cadaver specimens, models and diagrams) and name the principal arteries and veins of the CNS: Why is it important to understand blood supply
Principles Arteries & Veins of the CNS LO14 14. Identify (on cadaver specimens, models and diagrams) and name the principal arteries and veins of the CNS: Why is it important to understand blood supply
Stroke & the Emergency Department. Dr. Barry Moynihan, March 2 nd, 2012
 Stroke & the Emergency Department Dr. Barry Moynihan, March 2 nd, 2012 Outline Primer Stroke anatomy & clinical syndromes Diagnosing stroke Anterior / Posterior Thrombolysis Haemorrhage The London model
Stroke & the Emergency Department Dr. Barry Moynihan, March 2 nd, 2012 Outline Primer Stroke anatomy & clinical syndromes Diagnosing stroke Anterior / Posterior Thrombolysis Haemorrhage The London model
Demyelinating Diseases of the Brain
 Department of Radiology University of California San Diego Demyelinating Diseases of the Brain John R. Hesselink, M.D. T1-Weighted Images Normal White Matter Contents Axons with envelope of myelin Neuroglia
Department of Radiology University of California San Diego Demyelinating Diseases of the Brain John R. Hesselink, M.D. T1-Weighted Images Normal White Matter Contents Axons with envelope of myelin Neuroglia
IV. Cerebrovascular diseases
 IV. Cerebrovascular diseases - Cerebrovascular disease denotes brain disorders caused by pathologic processes involving the blood vessels. - The three main pathogenic mechanisms are: 1. Thrombotic occlusion
IV. Cerebrovascular diseases - Cerebrovascular disease denotes brain disorders caused by pathologic processes involving the blood vessels. - The three main pathogenic mechanisms are: 1. Thrombotic occlusion
Carotid Embolectomy and Endarterectomy for Symptomatic Complete Occlusion of the Carotid Artery as a Rescue Therapy in Acute Ischemic Stroke
 This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivs 3.0 License (www.karger.com/oa-license), applicable to the online version of the article
This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivs 3.0 License (www.karger.com/oa-license), applicable to the online version of the article
Marc Norman, Ph.D. - Do Not Use without Permission 1. Cerebrovascular Accidents. Marc Norman, Ph.D. Department of Psychiatry
 Cerebrovascular Accidents Marc Norman, Ph.D. Department of Psychiatry Neuropsychiatry and Behavioral Medicine Neuropsychology Clinical Training Seminar 1 5 http://www.nlm.nih.gov/medlineplus/ency/images/ency/fullsize/18009.jpg
Cerebrovascular Accidents Marc Norman, Ph.D. Department of Psychiatry Neuropsychiatry and Behavioral Medicine Neuropsychology Clinical Training Seminar 1 5 http://www.nlm.nih.gov/medlineplus/ency/images/ency/fullsize/18009.jpg
PFO closure group total no. PFO closure group no. of males
 Suppl Table. Characteristics of the five trials included in this meta-analysis. Trial name Device used for Definition of medical Primary Endpoint group total no. group no. of males group age (yrs) group
Suppl Table. Characteristics of the five trials included in this meta-analysis. Trial name Device used for Definition of medical Primary Endpoint group total no. group no. of males group age (yrs) group
General Sensory Pathways of the Trunk and Limbs
 General Sensory Pathways of the Trunk and Limbs Lecture Objectives Describe gracile and cuneate tracts and pathways for conscious proprioception, touch, pressure and vibration from the limbs and trunk.
General Sensory Pathways of the Trunk and Limbs Lecture Objectives Describe gracile and cuneate tracts and pathways for conscious proprioception, touch, pressure and vibration from the limbs and trunk.
Vertebrobasilar Insufficiency
 Equilibrium Res Vol. (3) Vertebrobasilar Insufficiency Toshiaki Yamanaka Department of Otolaryngology-Head and Neck Surgery, Nara Medical University School of Medicine Vertebrobasilar insufficiency (VBI)
Equilibrium Res Vol. (3) Vertebrobasilar Insufficiency Toshiaki Yamanaka Department of Otolaryngology-Head and Neck Surgery, Nara Medical University School of Medicine Vertebrobasilar insufficiency (VBI)
IMAGING IN ACUTE ISCHEMIC STROKE
 IMAGING IN ACUTE ISCHEMIC STROKE Timo Krings MD, PhD, FRCP (C) Professor of Radiology & Surgery Braley Chair of Neuroradiology, Chief and Program Director of Diagnostic and Interventional Neuroradiology;
IMAGING IN ACUTE ISCHEMIC STROKE Timo Krings MD, PhD, FRCP (C) Professor of Radiology & Surgery Braley Chair of Neuroradiology, Chief and Program Director of Diagnostic and Interventional Neuroradiology;
Vague Neurological Conditions
 Vague Neurological Conditions Dr. John Lefebre, MD, FRCPC Chief Regional Medical Director Europe, India, South Africa, Middle East and Turkey Canada 2014 2 3 4 Agenda Dr. John Lefebre, M.D., FRCPC 1. TIA
Vague Neurological Conditions Dr. John Lefebre, MD, FRCPC Chief Regional Medical Director Europe, India, South Africa, Middle East and Turkey Canada 2014 2 3 4 Agenda Dr. John Lefebre, M.D., FRCPC 1. TIA
Differential Diagnosis of Hypokinetic Movement Disorders
 Differential Diagnosis of Hypokinetic Movement Disorders Dr Donald Grosset Consultant Neurologist - Honorary Professor Institute of Neurological Sciences - Glasgow University Hypokinetic Parkinson's Disease
Differential Diagnosis of Hypokinetic Movement Disorders Dr Donald Grosset Consultant Neurologist - Honorary Professor Institute of Neurological Sciences - Glasgow University Hypokinetic Parkinson's Disease
Symptoms of small vessel strokes. Small Vessel stroke. What is this? Treatment. Large Vessel stroke 6/1/2018
 Stroke Stroke Megan Stevens MD Vascular Neurology SUDDEN Maximal at onset Lateralized weakness, lateralized numbness, vision loss (one eye or portion of field in both eyes), double vision, slurred speech,
Stroke Stroke Megan Stevens MD Vascular Neurology SUDDEN Maximal at onset Lateralized weakness, lateralized numbness, vision loss (one eye or portion of field in both eyes), double vision, slurred speech,
United Council for Neurologic Subspecialties Geriatric Neurology Written Examination Content Outline
 United Council for Neurologic Subspecialties Geriatric Neurology Written Examination Content Outline REV 3/24/09 The UCNS Geriatric Neurology examination was established to determine the level of competence
United Council for Neurologic Subspecialties Geriatric Neurology Written Examination Content Outline REV 3/24/09 The UCNS Geriatric Neurology examination was established to determine the level of competence
CT and MR Imaging in Young Stroke Patients
 CT and MR Imaging in Young Stroke Patients Ashfaq A. Razzaq,Behram A. Khan,Shahid Baig ( Department of Neurology, Aga Khan University Hospital, Karachi. ) Abstract Pages with reference to book, From 66
CT and MR Imaging in Young Stroke Patients Ashfaq A. Razzaq,Behram A. Khan,Shahid Baig ( Department of Neurology, Aga Khan University Hospital, Karachi. ) Abstract Pages with reference to book, From 66
Cerebrovascular Disease
 Neuropathology lecture series Cerebrovascular Disease Physiology of cerebral blood flow Brain makes up only 2% of body weight Percentage of cardiac output: 15-20% Percentage of O 2 consumption (resting):
Neuropathology lecture series Cerebrovascular Disease Physiology of cerebral blood flow Brain makes up only 2% of body weight Percentage of cardiac output: 15-20% Percentage of O 2 consumption (resting):
Table 1: Baseline characteristics of 108 isolated vertigo patients Clinical or laboratory variable n (%) Female 67 (62%)
 Female 67 (62%)") 4. Results The 108 patients who fulfilled the inclusion and exclusion criteria were analyzed. Baseline demographic and epidemiological characteristics of the patients are given in Table 1. Table 1: Baseline
4. Results The 108 patients who fulfilled the inclusion and exclusion criteria were analyzed. Baseline demographic and epidemiological characteristics of the patients are given in Table 1. Table 1: Baseline
Turkish Title: Akut Eş Zamanlı Subkortikal Infarktların Neden Olduğu Progresif Bulber Paralizi ile Prezente olan CADASIL Olgusu
 DOI: Manuscript Type: Case Report Turkish Title: Akut Eş Zamanlı Subkortikal Infarktların Neden Olduğu Progresif Bulber Paralizi ile Prezente olan CADASIL Olgusu Turkish Running Head: Eş Zamanlı İnfartlarla
DOI: Manuscript Type: Case Report Turkish Title: Akut Eş Zamanlı Subkortikal Infarktların Neden Olduğu Progresif Bulber Paralizi ile Prezente olan CADASIL Olgusu Turkish Running Head: Eş Zamanlı İnfartlarla
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for
 Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
Recanalization of Chronic Carotid Artery Occlusion Objective Improvement Of Cerebral Perfusion
 Recanalization of Chronic Carotid Artery Occlusion Objective Improvement Of Cerebral Perfusion Paul Hsien-Li Kao, MD Assistant Professor National Taiwan University Medical School and Hospital ICA stenting
Recanalization of Chronic Carotid Artery Occlusion Objective Improvement Of Cerebral Perfusion Paul Hsien-Li Kao, MD Assistant Professor National Taiwan University Medical School and Hospital ICA stenting
Pharmacy STROKE. Anne Kinnear Lead Pharmacist NHS Lothian. Educational Solutions for Workforce Development
 STROKE Anne Kinnear Lead Pharmacist NHS Lothian Aim To update pharmacists on Stroke: the disease and its management and explore ways to implement pharmaceutical care for this patient group as part of normal
STROKE Anne Kinnear Lead Pharmacist NHS Lothian Aim To update pharmacists on Stroke: the disease and its management and explore ways to implement pharmaceutical care for this patient group as part of normal
Cerebral Vascular Diseases. Nabila Hamdi MD, PhD
 Cerebral Vascular Diseases Nabila Hamdi MD, PhD Outline I. Stroke statistics II. Cerebral circulation III. Clinical symptoms of stroke IV. Pathogenesis of cerebral infarcts (Stroke) 1. Ischemic - Thrombotic
Cerebral Vascular Diseases Nabila Hamdi MD, PhD Outline I. Stroke statistics II. Cerebral circulation III. Clinical symptoms of stroke IV. Pathogenesis of cerebral infarcts (Stroke) 1. Ischemic - Thrombotic
10/13/2017. AllinaHealthSystems. Stroke Recognition Sandra K Hanson, MD Medical Director United Hospital Stroke Program
 Agenda Stroke Recognition Sandra K Hanson, MD Medical Director United Hospital Stroke Program Vascular anatomy NIH Stroke Scale Recognizing the hard to recognize Distinguishing stroke mimics 1 Symptoms
Agenda Stroke Recognition Sandra K Hanson, MD Medical Director United Hospital Stroke Program Vascular anatomy NIH Stroke Scale Recognizing the hard to recognize Distinguishing stroke mimics 1 Symptoms
Ischemic Stroke in Critically Ill Patients with Malignancy
 Ischemic Stroke in Critically Ill Patients with Malignancy Jeong-Am Ryu 1, Oh Young Bang 2, Daesang Lee 1, Jinkyeong Park 1, Jeong Hoon Yang 1, Gee Young Suh 1, Joongbum Cho 1, Chi Ryang Chung 1, Chi-Min
Ischemic Stroke in Critically Ill Patients with Malignancy Jeong-Am Ryu 1, Oh Young Bang 2, Daesang Lee 1, Jinkyeong Park 1, Jeong Hoon Yang 1, Gee Young Suh 1, Joongbum Cho 1, Chi Ryang Chung 1, Chi-Min
Current Clinical Trials for Stroke Survivors in NJ and Philadelphia Areas
 Current Clinical Trials for Survivors in NJ and Philadelphia Areas For more information go to https://clinicaltrials.gov/ and search for the title in search box Condition / Disease 1. Spatial Neglect and
Current Clinical Trials for Survivors in NJ and Philadelphia Areas For more information go to https://clinicaltrials.gov/ and search for the title in search box Condition / Disease 1. Spatial Neglect and
Management and Investigation of Ischemic Stroke By Etiology
 Management and Investigation of Ischemic Stroke By Etiology Andrew M. Demchuk MD FRCPC Director, Calgary Stroke Program Deputy Dept Head, Clinical Neurosciences Heart and Stroke Foundation Chair in Stroke
Management and Investigation of Ischemic Stroke By Etiology Andrew M. Demchuk MD FRCPC Director, Calgary Stroke Program Deputy Dept Head, Clinical Neurosciences Heart and Stroke Foundation Chair in Stroke
Identifying Cerebrovascular Disorders. Wengui Yu, MD, PhD Department of Neurology, University of California, Irvine
 Identifying Cerebrovascular Disorders Wengui Yu, MD, PhD Department of Neurology, University of California, Irvine Objectives Review different types of cerebrovascular disorders. Briefly discuss etiology,
Identifying Cerebrovascular Disorders Wengui Yu, MD, PhD Department of Neurology, University of California, Irvine Objectives Review different types of cerebrovascular disorders. Briefly discuss etiology,
Patent Foramen Ovale and Cryptogenic Stroke: Do We Finally Have Closure? Christopher Streib, MD, MS
 Patent Foramen Ovale and Cryptogenic Stroke: Do We Finally Have Closure? Christopher Streib, MD, MS 11-8-18 Outline 1. Background 2. Anatomy of patent foramen ovale (PFO) 3. Relationship between PFO and
Patent Foramen Ovale and Cryptogenic Stroke: Do We Finally Have Closure? Christopher Streib, MD, MS 11-8-18 Outline 1. Background 2. Anatomy of patent foramen ovale (PFO) 3. Relationship between PFO and
MRI OF THE THALAMUS. Mohammed J. Zafar, MD, FAAN Kalamazoo, MI
 1 MRI OF THE THALAMUS Mohammed J. Zafar, MD, FAAN Kalamazoo, MI Objectives: The thalamic nuclei can be involved in a wide variety of conditions. A systematic imaging approach would be useful for narrowing
1 MRI OF THE THALAMUS Mohammed J. Zafar, MD, FAAN Kalamazoo, MI Objectives: The thalamic nuclei can be involved in a wide variety of conditions. A systematic imaging approach would be useful for narrowing
It s Always a Stroke; Except For When It s Not..
 It s Always a Stroke; Except For When It s Not.. TREVOR PHINNEY, D.O. Disclosures No Relevant Disclosures 1 Objectives Discuss variables of differential diagnosis for stroke Review when to TPA and when
It s Always a Stroke; Except For When It s Not.. TREVOR PHINNEY, D.O. Disclosures No Relevant Disclosures 1 Objectives Discuss variables of differential diagnosis for stroke Review when to TPA and when
GENERAL PRINCIPLES OF NEUROLOGY- John W. Day, M.D., Ph.D.
 I. TAKE HOME POINTS FOR THIS LECTURE A. Localizing the disease is the first step in diagnosing a neurological disorder. B. Time course of the disease (acute, subacute, or chronic) indicates the pathophysiological
I. TAKE HOME POINTS FOR THIS LECTURE A. Localizing the disease is the first step in diagnosing a neurological disorder. B. Time course of the disease (acute, subacute, or chronic) indicates the pathophysiological