Venothrombotic Events: The Subtle Killer
|
|
|
- Preston McDaniel
- 5 years ago
- Views:
Transcription

1 Venothrombotic Events: The Subtle Killer

2 Disclosure Statement No financial or professional conflicts to report
3 Learner Objectives Review risk factors, symptoms and subgroups of VTE Recognize medications utilized to treat VTE, indications and contraindications Utilize most current evidence-based guidelines for prevention and duration of treatment therapy
4


5 Pulmonary Embolism Thrombosis (VTE) that originates in the venous system and embolizes to the pulmonary arterial circulation DVT in veins of leg above the knee (>90%) DVT elsewhere (pelvic, arm, calf veins, etc.) Cardiac thrombi Air embolism. Fat embolism.
6 Epidemiology Third most common acute cardiovascular disease After coronary ischemia and stroke Rate is 98 (nonfatal) and 107 (fatal) events per 100,000 persons in USA (650,000 yr) Over 300,000 hospitalizations and 50,000 deaths per year
7 Mortality increases with age and male sex 40% (idiopathic PE's) have increased incidence of developing overt cancer 10-20% of persons with PE have genetic thrombophilic disorders Patients with PE are at increased risk (>1.5X) of death within 6 months of diagnosis



8
 Systemically normotensive (systolic BP 90 mmhg) RV dysfunction Myocardial necrosis Systemically normotensive (systolic BP 90 mmhg) No")
9 Definitions Massive PE Submassive PE Minor/Nonmassive PE High risk Moderate/intermediate risk Low risk Sustained hypotension (systolic BP <90 mmhg for 15 min) Inotropic support Pulseless Persistent profound bradycardia (HR <40 bpm with signs or symptoms of shock) Systemically normotensive (systolic BP 90 mmhg) RV dysfunction Myocardial necrosis Systemically normotensive (systolic BP 90 mmhg) No RV dysfunction No myocardial necrosis RV dysfunction RV/LV ratio > 0.9 or RV systolic dysfunction on echo RV/LV ratio > 0.9 on CT Elevation of BNP (>90 pg/ml) Elevation of NTpro-BNP (>500 pg/ml) ECG changes: new complete or incomplete RBBB anteroseptal ST elevation or depression anteroseptal T-wave inversion Jaff et al. Circulation 2011;123(16): Jaff et al. Circulation 2011;123(16):
10 Predisposing Factors History of DVT, Concurrent DVT >95% of patients with PE; PE occurs in >50% of cases with confirmed DVT Obesity ~40% Cancer ~30% Heart Failure ~35% Surgery - ~20% (> 60 minutes) Fracture ~20% (pelvic/femur) Smoking (> 25 cigarettes/day) Shock Air Travel - particularly >3100 miles
11 Predisposing Factors- con t. Intake of (high doses of) Estrogen Especially in smokers on OCP Estrogen replacement therapy (ERT): increase risk ~1.2-2X in current users Factor V Leiden patients on OCPs may have >30X increased risk of thromboembolism Trauma Pregnancy: peri- and post-partum
12 Predisposing Factors- con t. Hypercoagulable States Factor V Leiden - Resistance to Activated Protein C (~12% of PE cases) Factor II (Prothrombin) 20210A mutation - (~10% of PE cases) It was discovered in 1996 that a specific change in the genetic code causes the body to produce an excess of the prothrombin protein. Protein C, S or Antithrombin III Deficiency Low levels of tissue factor pathway inhibitor (TFPI)

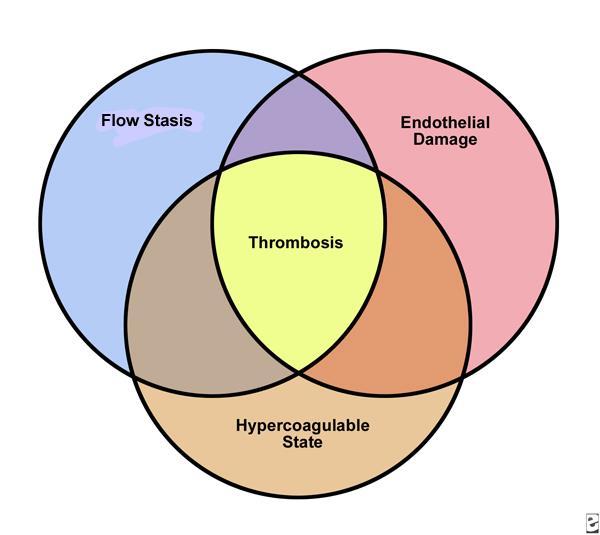
13 Rudolf Virchow
14
15 High Risk for Fatal Outcome Cancer Heart Failure Chronic underlying lung disease Recurrent PE Elevated troponin (T or I) Pulmonary Hypertension (P-HTN) BNP elevated brain natriuretic peptide or N- terminal pro-brain natriuretic peptide (NTproBNP) predicts RV dysfunction and mortality RV thrombus -have a higher 14-day mortality and three-month mortality Overall, few patients have recurrent emboli, particularly after initiation of therapy

16 How to Determine Risk Registry of 1,416 patients Mortality rate: 1.9% if RV/LV ratio < % if RV/LV ratio 0.9 Fremont et al. CHEST 2008;133:

17 How to Determine Risk Retrospective analysis of 120 patients with hemodynamically stable PE based on chest CT PE-related mortality at 3 months: 17% if RV/LV 1.5 8% if 1.0 RV/LV < 1.5 0% if RV/LV < 1.0 Van der Meer et al. Radiology 2005; 235:

18 How to Determine Risk Retrospective analysis of 63 patients with chest CT Adverse event rate at 30 days: 80.3% if RV/LV ratio > % if RV/LV ratio 0.9 Quiroz et. al. Circulation. 2004;109:
19 Pathogenesis Clot forms at distal site, usually in distal veins in the leg or in pelvic veins Clots migrate to pulmonary vasculature Most clots lodge in pulmonary arterioles or segmental arteries Lodging at pulmonary artery bifurcation leads to "saddle" embolism Lodged thrombi release vasoconstrictors Serotonin Thrombin Endothelin
20 Pathogenesis con t. Release of these vasoconstrictors causes diffuse pulmonary vascular constriction P-HTN follows and can cause right heart failure, JVD not sensitive in acute P-HTN Alveolar Dead Space Vascular blockade (full or partial) leads to unperfused areas of lung These areas are called dead space (ventilated but not perfused) Alveolar dead space increases in PE in proportion to severity of vascular blockade
21 Pathophysiology Obstruction RV Pressure Load Neuro-hormonal Decreased RV CPP VO2 Ischemia Wall stress RV Decompensation Increase RV Volume Septal Shift Pericardial Restriction Decrease RV Output COP / MAP Decrease LV Distensiblity Decreased LV Preload
22 Clinical Presentation Symptoms are non-specific, not very sensitive; high suspicion must be maintained Pleuritic chest pain in absence of dyspnea is common first presentation Dyspnea 77% (A-a gradient) Tachypnea 70% Chest Pain 55% (usually pleuritic) Tachycardia 43% Cyanosis 18% Hemoptysis 13% Syncope 10%
23 Symptoms con t. Cough 43% Leg Swelling 33% Leg Pain 30% Palpitations 12% Wheezing 10% Angina-like pain 5% Sudden cardiac arrest with pulseless electrical activity Some have NO SYMPTOMS

24

25
26 Differential Diagnosis Myocardial Infarction Pneumonia Pulmonary Edema / Heart Failure Asthma, COPD Exacerbation Pneumothorax/rib fracture Musculoskeletal Pain, Costochondritis Dissecting Thoracic Aneurysm Anxiety / Panic Attack
27 Pulmonary Embolism Prediction Rules Suspicion should be high if ANY risk factors or symptoms/signs are present >70% of patients who die of PE are not suspected of having it Only ~35% of patients suspected of having PE actually have it PE testing is less reliable in older persons than in younger persons Age is a major risk factor, particularly with underlying predisposing conditions
28 Wells Score Clinical symptoms of DVT (leg swelling, pain with palpation) 3.0 Traditional clinical probability assessment (Wells criteria) Other diagnosis less likely than pulmonary embolism 3.0 Heart rate > Immobilization ( 3 days) or surgery in the previous four weeks 1.5 Previous DVT/PE 1.5 Hemoptysis 1.0 Malignancy 1.0 High >6.0 Moderate 2.0 to 6.0 Low <2.0 Simplified clinical probability assessment (Modified Wells criteria) PE likely >4.0 PE unlikely 4.0
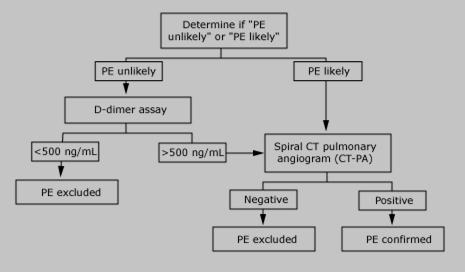
29 Diagnostic Algorithm
30 Diagnostic Evaluation Low clinical probability: high sensitivity D-dimer (level <500µg/L) to rule out PE Lower extremity venous ultrasound (US) to rule in DVT Helical CT angiography or V/Q scanning Contrast angiography MRA
31 Routine Laboratory Tests Electrolytes, complete blood count, coagulation parameters (PT, aptt) ECG with right sided leads All patients should have an Arterial Blood Gas (ABG, preferably on room air) A PaO2 between 85 and 105 mmhg exists in approximately 18 percent of patients with PE Normal A-a gradient found in <6% of patients with PE High Sensitivity D-Dimer Test Lower extremity venous US with doppler measurements
32 D-Dimer Artifact Arterial thrombosis DVT/PE MI CAD CVA Malignancy Pregnancy Surgery Trauma DIC Afib Limb ischemia Renal failure Liver disease SIRS/Sepsis Sickle Cell
33 ECG Changes Most common ECG is normal sinus rhythm: Sinus Tachycardia extremely common Right Axis Deviation; Q in III, inverted T in III Right sided leads should be evaluated
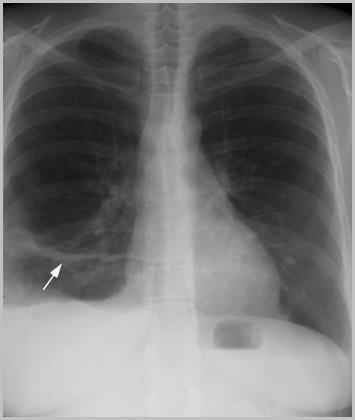
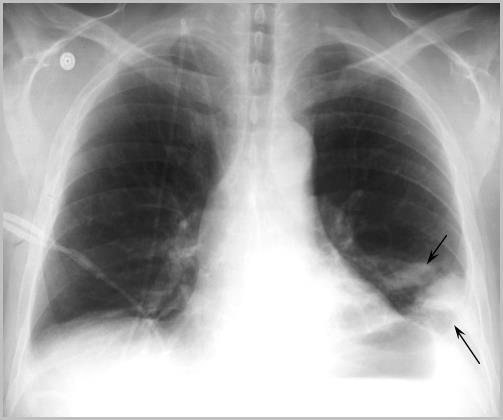

34 CXR Atelectasis Hampton s Hump Prominent PA
35 Ventilation-Perfusion (V/Q) Scans High probability scans identify only ~50% of patients with PE overall About 60% of V/Q scans will be indeterminant (intermediate + low probability) Of intermediate probability scans, ~33% occur with angiographically proven PE Conclude: normal test rules out PE in ~98% of cases Note that low probability test still has ~15-25% chance of PE However, there were no deaths due to PE within 6 months in a study of 536 patients with low probability scans

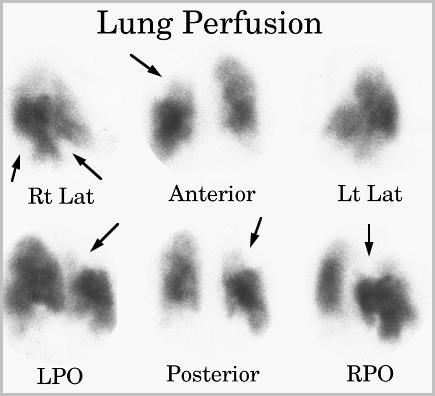
36 V/Q with Large Defect
37 Lower Extremity Doppler US To evaluate for DVT as possible cause of PE or to help rule in PE Up to 40% of patients with DVT without PE symptoms will HAVE a PE by angiography Pelvis blinded area A positive US with abnormal V/Q rules IN a PE

38 Venous Ultrasound A subtotal occlusive thrombus in the right popliteal vein is shown in this color Doppler image.
39 Helical (Spiral) Computed Tomography Helical CT scanning produces volumetric two-dimensional image of lung This is accomplished by giving IV contrast agent and rotating detector around the patient PE appears as a filling defect that may be central, eccentric or mural The embolism may completely or partially occlude the vessel
40 Helical (Spiral) Computed Tomography (CT) Reported sensitivity 83% in PIOPED II specificity 96% in PIOPED II N Engl J Med Jun 1;354(22): Test is very quick, requires IV contrast and careful interpretation and is costly Helical CT increases the diagnosis of PE and reduce angiography

41 Helical (Spiral) Computed Tomography (CT)
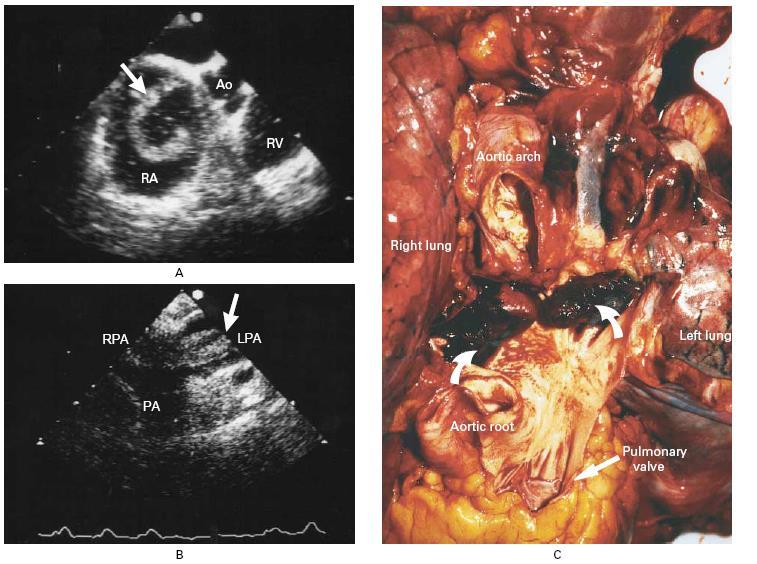
42 Echocardiography-Two Fold
43 Pulmonary Angiography This has been the gold standard for diagnosis but it is highly invasive May be morbid with worsening shortness of breath, artery perforation The pulmonary catheter may also be used therapeutically (angioplasty) Positive result is a filling defect or sharp cutoff in a pulmonary artery branch Angiography can be avoided in most patients by using other tests


44 Contrast Pulmonary Angiography
45 Magnetic Resonance Angiography (MRA) Techniques for use of MRA for diagnosing PE are evolving rapidly Estimated sensitivity ~80% (~100% for larger emboli), specificity 95% Non-invasive with little morbidity Dynamic gadolinium enhancement is used, allowing high quality images Strongly consider prior to standard invasive pulmonary angiography

 MRA")
46 Magnetic Resonance Angiography (MRA) MRA after resolution
47 Heparin Induced Thrombocytopenia (HIT) 1-5% patient exposed develop syndrome (bovine>porcine) 50% of platelets in 5-10 days after exposure Hep AB positive Serotonin Release Assay (SRA) positive VTE/arterial thrombosis in 50 % of HIT patients

48 Antithrombotic Therapy and Prevention of Thrombosis: ACCP Evidence-Based Clinical Practice Guidelines, 10th ed-2016
49 Clotting Cascade
50 Interpretation of Recommendations Grade Recom Method Evidence B vs B Implication 1A Strong RCT no limit High quality OW Apply to most pts 1B Strong RCT some limits Moderate OW Apply to most pts 1C Strong Observ Low/very low OW Apply to most data may change 2A Weak Observ High Balan ced 2B Weak Observ Moderate Balan ced Circumstan ces vital New data change plan 2C Weak Observ/ case Low Balan ced Other plans may be >/=
51 Scoring Systems-Padua Predication Score
52 Risk for Bleeding Chest 2012

53
54 Prevention of VTE in Non Surgical Patient Increased risk of thrombosis (scoring systems), LMWH, LDUH, BID/TID (Grade 1B) Low risk of thrombosis, no use of pharm or mech prophylaxis (Grade 1B) None for patient who are bleeding or high risk for bleeding (Grade 1B)
55 Critically Ill Patients No need for US screening (2C) Suggest use of LMWH/LDUH over none (2B) Bleeding or risk of bleeding suggest mech (2C) When bleeding risk decreases, suggest that pharm be started (2C)
56 Prevention of VTE Nonorthopedic Surgery Very low risk for VTE-no need for pharm (1B) or mech (2C) use early mobility Low risk, mech over pharm (2C) Mod risk for VTE and not at risk for bleeding, LMWH/LDUH (2B), mech (2C) over no use Mod risk VTE and high risk for bleeding, mech over pharm (2C)
57 High risk for VTE not at risk for bleeding, LMWH/LDUH over none (1B) and mech (2C) High risk for VTE, risk for major bleeding, mech and then start pharm when risk over (2C) IVC should not be used for primary prevention (2C) No serial US screen (2C)
58 Case A 44-year-old man is evaluated in follow-up for an episode of unprovoked left proximal leg deep venous thrombosis 3 months ago. Following initial anticoagulation with lowmolecular-weight heparin, he began treatment with warfarin. INR testing done every 3 to 4 weeks has shown a stable therapeutic INR. He has mild left leg discomfort after a long day of standing, but it does not limit his activity level. He tolerates warfarin well. Family history is unremarkable, and he takes no other medications. Which of the following is the most appropriate management? A. Continue anticoagulation indefinitely B. Discontinue warfarin in another 3 months C. Discontinue warfarin now D. Discontinue warfarin and perform thrombophilia testing
59 Objectives Recognize subgroups of VTE Review medications for VTE anticoagulation Learn guidelines for duration of therapy Understand differences in therapy based on type of VTE
60 Subgroups of VTE Cancer-associated vs No cancer Provoked vs Unprovoked Proximal vs Distal DVT Upper extremity vs Lower extremity DVT
61 VTE and No Cancer Use NOAC preferred! (Grade 2B) Rivaroxaban, apixaban No bridging needed Dabigatran, edoxaban Start with parenteral anticoagulation x5 days If contraindications to NOAC, then use VKA therapy (warfarin) (Grade 2C) Overlap with parenteral anticoagulation x5 days, And INR >2 for 24 hours
62 Contraindications to NOACs Extreme BMI (>40) CrCl <30 Patient who doesn t like idea of no known reversal agent/strategy (except Dabigatran) Significant increased risk of bleeding
63
64 Cancer-Associated Thrombosis Use LMWH (Grade 2C) Enoxaparin 1 mg/kg/dose BID
65 Provoking Transient Risk Factors for VTE Surgery Estrogen therapy Pregnancy Leg injury Flight >8h
66 Location of VTE Lower extremity DVT Proximal Popliteal or more proximal veins Distal Calf veins Upper extremity DVT Proximal Axillary or more proximal veins Catheter-associated
67 Duration of Therapy Proximal DVT or PE Isolated Distal DVT Cancerassociated Upper extremity DVT Provoked 3 months (Grade 1B) Low bleeding risk Extended therapy (first VTE - Grade 2B, second VTE - Grade 1B) Unprovoked Mod bleeding risk Extended therapy (first VTE - Grade 2B, second VTE - Grade 2B) High bleeding risk 3 months (first VTE - Grade 1B, second VTE - Grade 2B) Mild symptoms or high bleeding risk Serial imaging x2 weeks (Grade 2C) Extending thrombus Severe symptoms or risk for extension Anticoagulate (Grade 2C) Extended therapy (Grade 1B) Anticoagulate (Grade 2C) Anticoagulate (Grade 1B, 2C)
68 Special Considerations for Upper Extremity DVT Proximal Catheterassociated Anticoagulate Catheter functional? Yes No Catheter still needed? Yes No Remove and anticoagulate x3 months Leave catheter in and anticoagulate
69 Risk Factors for Bleeding on Anticoagulant Therapy Age >65 Age >75 Previous bleeding Cancer Metastatic cancer Renal failure Liver failure Thrombocytopenia Previous stroke Diabetes Anemia Antiplatelet therapy Poor anticoagulant control Comorbidity and reduced functional capacity Recent surgery Frequent falls Alcohol abuse NSAID use Low risk Moderate risk High risk 0 risk factors 1 risk factor 2 risk factors
70 Risk Factors for Extension of Distal DVT Positive D-dimer Extensive thrombus >5cm long, involves multiple veins, >7mm diameter Thrombus close to proximal veins No reversible provoking factor Active cancer History of VTE Inpatient status
71 What if my patient stops anticoagulation? Aspirin is NOT a reasonable alternative to anticoagulation for extended therapy Much less effective at preventing recurrent VTE However, aspirin is better than nothing (Grade 2B)
72 Recurrent DVT on Anticoagulation If on therapeutic warfarin or NOAC, then switch to enoxaparin temporarily (minimum 1 month) (Grade 2C) Is this really recurrent VTE? Is my patient compliant with therapy? Is there underlying malignancy? If on enoxaparin and compliant, then increase the dose by 25-33% (Grade 2C)
73 Case Revisited A 44-year-old man is evaluated in follow-up for an episode of unprovoked left proximal leg deep venous thrombosis 3 months ago. Following initial anticoagulation with low-molecular-weight heparin, he began treatment with warfarin. INR testing done every 3 to 4 weeks has shown a stable therapeutic INR. He has mild left leg discomfort after a long day of standing, but it does not limit his activity level. He tolerates warfarin well. Family history is unremarkable, and he takes no other medications. Which of the following is the most appropriate management? A. Continue anticoagulation indefinitely B. Discontinue warfarin in another 3 months C. Discontinue warfarin now D. Discontinue warfarin and perform thrombophilia testing

74 Duration of Therapy Proximal DVT or PE Isolated Distal DVT Cancerassociated Upper extremity DVT Provoked Unprovoked Mild symptoms or high bleeding risk Severe symptoms or risk for extension Extended therapy Anticoagulat e 3 months Low to moderate bleeding risk High bleeding risk Serial imaging x2 weeks Anticoagulate Extended therapy 3 months Extending thrombus Anticoagulate
75 Case Revisited A 44-year-old man is evaluated in follow-up for an episode of unprovoked left proximal leg deep venous thrombosis 3 months ago. Following initial anticoagulation with low-molecular-weight heparin, he began treatment with warfarin. INR testing done every 3 to 4 weeks has shown a stable therapeutic INR. He has mild left leg discomfort after a long day of standing, but it does not limit his activity level. He tolerates warfarin well. Family history is unremarkable, and he takes no other medications. Which of the following is the most appropriate management? A. Continue anticoagulation indefinitely B. Discontinue warfarin in another 3 months C. Discontinue warfarin now D. Discontinue warfarin and perform thrombophilia testing
76 Summary NOACs are preferred over warfarin for anticoagulation Except if VTE is cancer-associated, then use enoxaparin Duration of therapy is usually 3 months, with extended therapy based on risk factors for recurrent VTE
77 Key changes to recommendations in the 9th edition to the 10th edition include: Non-vitamin K antagonist oral anticoagulants (NOACs) are suggested over warfarin for initial and long-term treatment of VTE in patients without cancer. Routine use of compression stockings is out to prevent postthrombotic syndrome in acute DVT. New isolated subsegmental pulmonary embolism treatment recommendations. The 10th edition suggests which patients diagnosed with isolated subsegmental pulmonary embolism (SSPE) should, and should not, receive anticoagulant therapy.
78 Betrixaban 2018!!! First oral approved VTE prophylaxis in adult patients hospitalized for an acute medical illness who are at risk due to moderate or severe restricted mobility and other risk factors for VTE. Efficacy was measured in 7,441 Fewer events were observed in patients receiving betrixaban (4.4%) compared with enoxaparin (6%) The most common adverse reactions ( 5%) with betrixaban were related to bleeding.
79 54% of patients receiving betrixaban experienced at least one adverse reaction compared with 52% taking enoxaparin. The frequency of patients reporting serious adverse reactions was similar between betrixaban (18%) and enoxaparin (17%). The most frequent reason for treatment discontinuation was bleeding, with an incidence rate for all bleeding episodes of 2.4% and 1.2% for betrixaban and enoxaparin, respectively. The incidence rate for major bleeding episodes was 0.67% and 0.57% for betrixaban and enoxaparin, respectively.
80 HESTIA Criteria-Don t Leave Home Without it Hemodynamically unstable Thrombolysis or embolectomy needed Active risk or significant risk of bleeding Oxygen required to keep saturation > 94% for > 24 hours Pulmonary embolism during anticoagulation therapy IV pain medications within the last 24 hours Medical or social issues that require in-hospital stay Creatinine clearance < 30 ml/min Severe liver dysfunction Pregnancy History of HIT If any question illicits a YES the patient cannot be treated as an outpatient
81 Thrombolytic Therapy Usually given to patients with echocardiographic evidence of right heart strain / failure Massive PE Fibrin-specific agents, which include alteplase (tpa), reteplase and tenecteplase Non fibrin-specific agent - streptokinase is not widely used in the United States but is still used elsewhere because of its lower cost.

82 CT Pre and Post Lytic Therapy


83 Ultrasound Accelerated Thrombosis

84 Ultrasound Accelerated Thrombosis

85
86 Treatment of High Risk Patients The ULTIMA Trial ULTrasound Accelerated ThrombolysIs of PulMonAry Embolism Hypothesis: Ultrasound-assisted, catheter-directed thrombolysis is superior to treatment with heparin alone for reversing RV enlargement within 24 hours 87

87 Treatment of High Risk Patients The ULTIMA Trial Enrollment Criteria Symptoms < 14 days No hemodynamic collapse at presentation No active bleeding Acute symptomatic PE confirmed by contrast-enhanced chest CT with embolus located in at least one main or proximal lower lobe pulmonary artery RV/LV ratio > 1 on echocardiography 88

88 Treatment of High Risk Patients The ULTIMA Trial Right Ventricular Dysfunction Nils Kutcher, ACC.13
89 Systemic Lytics vs EKOS JACC 2016 Systemic Lytics v Heparin EKOS v Heparin Total Lytics Dose 100mg 20.7mg (12.2mg) Mortality 5.9% -> 4.3% 1/29 -> 0/30 RV Size Improved Improved RV Function Improved Improved Major Bleeding 20% 0/30 ICH 3% 0/30

90 Treatment of High Risk Patients

91 The Aphorisms of Hippocrates In acute diseases,,, coldness of the extremities,, is a very bad sign.
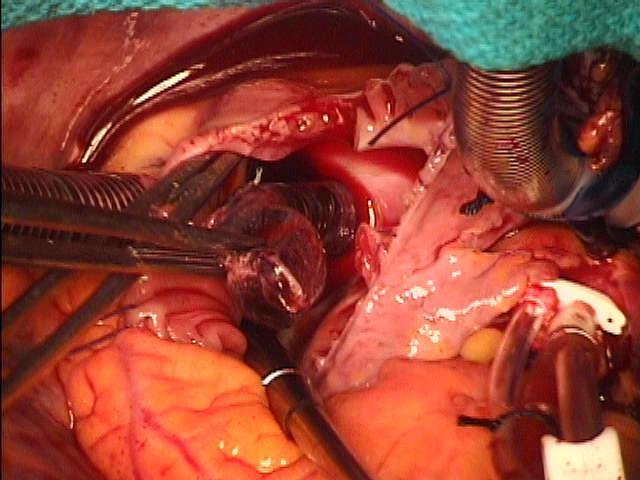
92 Thrombectomy Surgical thrombectomy only in very selective cases Perioperative mortality is 25-50% Massive pulmonary embolism where thrombolysis contraindicated
93

94
95 IVC Filter Placement Generally reserved for patients with recurrent PE on anti-coagulation May also be used for patients in whom anti-coagulation is contraindicated Can be used as adjunct in massive PE where thrombolysis is not an option IVC filters are being used for PE prophylaxis in select groups of patients
96 IVC Filter Placement Complications rare but include Complications related to the insertion process (eg, bleeding, venous thrombosis at the insertion site). Filter misplacement. Filter migration. Filter erosion and perforation of the IVC wall. IVC obstruction due to filter thrombosis.

97
98 VTE in Children Epidemiology Not until 1990 s was there serious study in children cases/10,000 by % increase Incidence peaks in < 1 year and then very low rates until early adolescence Cause Thrombin inhibitors are low until 6 m Arterial caths (prophylactic heparin decreases incidence from 40% to < 8%) Central lines can account for 45% of VTE Surgery and immobilization (though very low) Malignancy (and associate central cath) Inherited clotting disorders Congenital heart disease-prosthetic valves

99 Sequential Compression Devices
100 60 sec cycles 22% effective solo therapy 53% effective with dual therapy Most effective on surgical, cancer patients 35% misused 75% patient compliance Legs exercises and ambulation more effective EARLY MOBILITY!!!!!

101 LEGS EXERCISES
102
103 Activations 2016
104 Conclusions VTE is common among surgical and critically ill patient Assessment of VTE and bleeding risk should be done on all patients Mechanical and pharm regimens have been proven to be effective for prophylaxis
105
106 Ancora Imparo Michelangelo age 87
Venothrombotic Events: The Subtle Killer
 Venothrombotic Events: The Subtle Killer Disclosure Statement No financial or professional conflicts to report Learner Objectives Review risk factors, symptoms and subgroups of VTE Recognize medications
Venothrombotic Events: The Subtle Killer Disclosure Statement No financial or professional conflicts to report Learner Objectives Review risk factors, symptoms and subgroups of VTE Recognize medications
9/30/2017. Venothrombotic Events: The Subtle Killer. Disclosure Statement. Learner Objectives
 Venothrombotic Events: The Subtle Killer Disclosure Statement No financial or professional conflicts to report Learner Objectives Review risk factors, symptoms and subgroups of VTE Recognize medications
Venothrombotic Events: The Subtle Killer Disclosure Statement No financial or professional conflicts to report Learner Objectives Review risk factors, symptoms and subgroups of VTE Recognize medications
PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT
: DIAGNOSIS AND TREATMENT") PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT OBJECTIVE: To provide a diagnostic algorithm and treatment options for patients with acute pulmonary embolism (PE). BACKGROUND: Venous thromboembolism (VTE)
PULMONARY EMBOLISM (PE): DIAGNOSIS AND TREATMENT OBJECTIVE: To provide a diagnostic algorithm and treatment options for patients with acute pulmonary embolism (PE). BACKGROUND: Venous thromboembolism (VTE)
Pulmonary Embolism. Pulmonary Embolism. Pulmonary Embolism. PE - Clinical
 Pulmonary embolus - a practical approach to investigation and treatment Sam Janes Wellcome Senior Fellow and Respiratory Physician, University College London Background Diagnosis Treatment Common: 50 cases
Pulmonary embolus - a practical approach to investigation and treatment Sam Janes Wellcome Senior Fellow and Respiratory Physician, University College London Background Diagnosis Treatment Common: 50 cases
PE and DVT. Dr Anzo William Adiga WatsApp or Call Medical Officer/RHEMA MEDICAL GROUP
 PE and DVT Dr Anzo William Adiga WatsApp or Call +256777363201 Medical Officer/RHEMA MEDICAL GROUP OBJECTIVES DEFINE DVT AND P.E PATHOPHYSIOLOGY OF DVT CLINICAL PRESENTATION OF DVT/PE INVESTIGATE DVT MANAGEMENT
PE and DVT Dr Anzo William Adiga WatsApp or Call +256777363201 Medical Officer/RHEMA MEDICAL GROUP OBJECTIVES DEFINE DVT AND P.E PATHOPHYSIOLOGY OF DVT CLINICAL PRESENTATION OF DVT/PE INVESTIGATE DVT MANAGEMENT
Acute Pulmonary Embolism and Deep Vein Thrombosis. Barbara LeVarge MD Beth Israel Deaconess Medical Center Pulmonary Hypertension Center COPYRIGHT
 Acute Pulmonary Embolism and Deep Vein Thrombosis Barbara LeVarge MD Beth Israel Deaconess Medical Center Pulmonary Hypertension Center Acute PE and DVT No disclosures. Acute PE and DVT Learning objectives
Acute Pulmonary Embolism and Deep Vein Thrombosis Barbara LeVarge MD Beth Israel Deaconess Medical Center Pulmonary Hypertension Center Acute PE and DVT No disclosures. Acute PE and DVT Learning objectives
Venous Thrombosis. Magnitude of the Problem. DVT 2 Million PE 600,000. Death 60,000. Estimated Cost of VTE Care $1.5 Billion/year.
 Venous Thrombosis Magnitude of the Problem DVT 2 Million Postthrombotic Syndrome 800,000 PE 600,000 Death 60,000 Silent PE 1 Million Pulmonary Hypertension 30,000 Estimated Cost of VTE Care $1.5 Billion/year
Venous Thrombosis Magnitude of the Problem DVT 2 Million Postthrombotic Syndrome 800,000 PE 600,000 Death 60,000 Silent PE 1 Million Pulmonary Hypertension 30,000 Estimated Cost of VTE Care $1.5 Billion/year
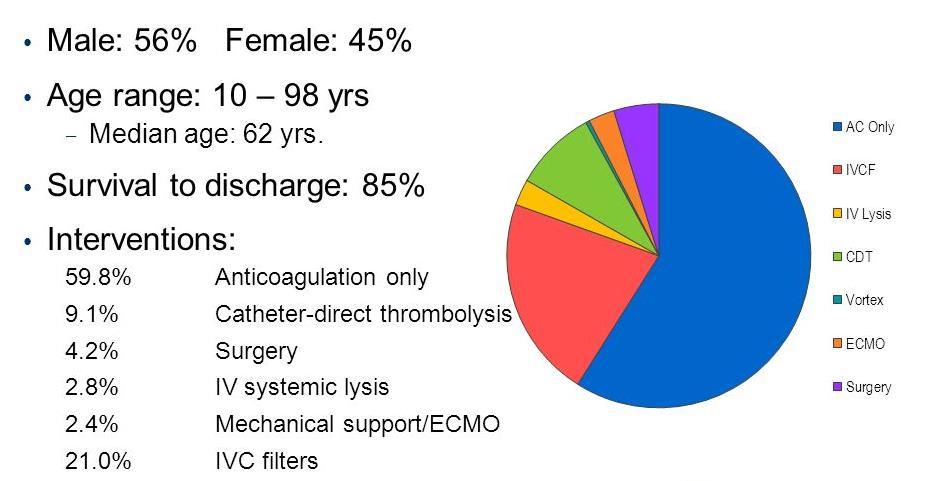
Single Center 4 year series of 114 consecutive patients treated for massive and submassive PE. Mark Goodwin, MD
 Single Center 4 year series of 114 consecutive patients treated for massive and submassive PE Mark Goodwin, MD Disclosure Speaker name:... I have the following potential conflicts of interest to report:
Single Center 4 year series of 114 consecutive patients treated for massive and submassive PE Mark Goodwin, MD Disclosure Speaker name:... I have the following potential conflicts of interest to report:
Dr. Rami M. Adil Al-Hayali Assistant Professor in Medicine
 Dr. Rami M. Adil Al-Hayali Assistant Professor in Medicine Venous thromboembolism: pulmonary embolism (PE) deep vein thrombosis (DVT) 1% of all patients admitted to hospital 5% of in-hospital mortality
Dr. Rami M. Adil Al-Hayali Assistant Professor in Medicine Venous thromboembolism: pulmonary embolism (PE) deep vein thrombosis (DVT) 1% of all patients admitted to hospital 5% of in-hospital mortality
Mabel Labrada, MD Miami VA Medical Center
 Mabel Labrada, MD Miami VA Medical Center *1-Treatment for acute DVT with underlying malignancy is for 3 months. *2-Treatment of provoked acute proximal DVT can be stopped after 3months of treatment and
Mabel Labrada, MD Miami VA Medical Center *1-Treatment for acute DVT with underlying malignancy is for 3 months. *2-Treatment of provoked acute proximal DVT can be stopped after 3months of treatment and
Pulmonary Thromboembolism
 Pulmonary Thromboembolism James Allen, MD Epidemiology of Pulmonary Embolism 1,500,000 new cases per year in the United States Often asymptomatic 300,000 deaths per year DVT or PE present in 10% of ICU
Pulmonary Thromboembolism James Allen, MD Epidemiology of Pulmonary Embolism 1,500,000 new cases per year in the United States Often asymptomatic 300,000 deaths per year DVT or PE present in 10% of ICU
Disclosures. DVT: Diagnosis and Treatment. Questions To Ask. Dr. Susanna Shin - DVT: Diagnosis and Treatment. Acute Venous Thromboembolism (VTE) None
 None") Disclosures DVT: Diagnosis and Treatment None Susanna Shin, MD, FACS Assistant Professor University of Washington Acute Venous Thromboembolism (VTE) Deep Venous Thrombosis (DVT) Pulmonary Embolism (PE)
Disclosures DVT: Diagnosis and Treatment None Susanna Shin, MD, FACS Assistant Professor University of Washington Acute Venous Thromboembolism (VTE) Deep Venous Thrombosis (DVT) Pulmonary Embolism (PE)
Thrombolysis in PE. Outline. Disclosure. Overview on Pulmonary Embolism. Hot Topics in Emergency Medicine 2012 Midyear Clinical Meeting
 Disclosure Thrombolysis in PE Daniel P. Hays, PharmD, BCPS, FASHP reports no relevant financial relationships. Daniel P. Hays, PharmD, BCPS, FASHP Outline 55 YOF presents to ED with SOB PMH of DVT + noncompliance
Disclosure Thrombolysis in PE Daniel P. Hays, PharmD, BCPS, FASHP reports no relevant financial relationships. Daniel P. Hays, PharmD, BCPS, FASHP Outline 55 YOF presents to ED with SOB PMH of DVT + noncompliance
Venous Thromboembolic Disease Update
 Canadian Society of Internal Medicine Annual Meeting Calgary, Alberta, October 2014 Venous Thromboembolic Disease Update Benjamin Bell, MD FRCPC James Douketis, MD FRCPC On Behalf of Thrombosis Canada
Canadian Society of Internal Medicine Annual Meeting Calgary, Alberta, October 2014 Venous Thromboembolic Disease Update Benjamin Bell, MD FRCPC James Douketis, MD FRCPC On Behalf of Thrombosis Canada
DEEP VEIN THROMBOSIS (DVT): TREATMENT
: TREATMENT") DEEP VEIN THROMBOSIS (DVT): TREATMENT OBJECTIVE: To provide an evidence-based approach to treatment of patients presenting with deep vein thrombosis (DVT). BACKGROUND: An estimated 45,000 patients in Canada
DEEP VEIN THROMBOSIS (DVT): TREATMENT OBJECTIVE: To provide an evidence-based approach to treatment of patients presenting with deep vein thrombosis (DVT). BACKGROUND: An estimated 45,000 patients in Canada
Understanding Best Practices in Anticoagulation Therapy in Patients with Venous Thromboembolism. Rajat Deo, MD, MTR
 Understanding Best Practices in Anticoagulation Therapy in Patients with Venous Thromboembolism Rajat Deo, MD, MTR Director of Translational Research in Cardiac Arrhythmias Division of Cardiovascular Medicine
Understanding Best Practices in Anticoagulation Therapy in Patients with Venous Thromboembolism Rajat Deo, MD, MTR Director of Translational Research in Cardiac Arrhythmias Division of Cardiovascular Medicine
Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis. Prof. Ralf R.Kolvenbach MD,PhD,FEBVS
 Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis Prof. Ralf R.Kolvenbach MD,PhD,FEBVS Catheter-based thrombolysis Local administration of lytic agent Higher local
Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis Prof. Ralf R.Kolvenbach MD,PhD,FEBVS Catheter-based thrombolysis Local administration of lytic agent Higher local
Epidemiology. Update on Pulmonary Embolism. Keys to PE Management 5/5/2014. Diagnosis. Risk stratification. Treatment
 Update on Pulmonary Embolism Steven M. Dean, DO, FACP, RPVI Program Director- Vascular Medicine Associate Professor of Internal Medicine Division of Cardiovascular Medicine The Ohio State University Keys
Update on Pulmonary Embolism Steven M. Dean, DO, FACP, RPVI Program Director- Vascular Medicine Associate Professor of Internal Medicine Division of Cardiovascular Medicine The Ohio State University Keys
Jessica Bryan, Natalia Evans, Karlyn Henderson, & Whitney Parks
 Jessica Bryan, Natalia Evans, Karlyn Henderson, & Whitney Parks 1. What is the most common cause of death in hospitalized patients? 1. Hospital-acquired infection 2. Pulmonary embolism 3. Myocardial infarction
Jessica Bryan, Natalia Evans, Karlyn Henderson, & Whitney Parks 1. What is the most common cause of death in hospitalized patients? 1. Hospital-acquired infection 2. Pulmonary embolism 3. Myocardial infarction
Venous thromboembolic diseases: diagnosis, management and thrombophilia testing (2012) NICE guideline CG144
 NICE guideline CG144") Venous thromboembolic diseases: diagnosis, management and thrombophilia testing (2012) NICE guideline CG144 Appendix A: Summary of new evidence from Summary of evidence from previous year Diagnosis Diagnostic
Venous thromboembolic diseases: diagnosis, management and thrombophilia testing (2012) NICE guideline CG144 Appendix A: Summary of new evidence from Summary of evidence from previous year Diagnosis Diagnostic
Pathology of pulmonary vascular disease. Dr.Ashraf Abdelfatah Deyab. Assistant Professor of Pathology Faculty of Medicine Almajma ah University
 Pathology of pulmonary vascular disease Dr.Ashraf Abdelfatah Deyab Assistant Professor of Pathology Faculty of Medicine Almajma ah University Pulmonary vascular disease Type of pulmonary circulation: Types
Pathology of pulmonary vascular disease Dr.Ashraf Abdelfatah Deyab Assistant Professor of Pathology Faculty of Medicine Almajma ah University Pulmonary vascular disease Type of pulmonary circulation: Types
Disclosures. Objectives
 BRIGHAM AND WOMEN S HOSPITAL Treatment of Massive and Submassive Pulmonary Embolism Gregory Piazza, MD, MS Assistant Professor of Medicine Harvard Medical School Staff Physician, Cardiovascular Division
BRIGHAM AND WOMEN S HOSPITAL Treatment of Massive and Submassive Pulmonary Embolism Gregory Piazza, MD, MS Assistant Professor of Medicine Harvard Medical School Staff Physician, Cardiovascular Division
Diagnosis and Treatment of Deep Venous Thrombosis and Pulmonary Embolism
 Agency for Healthcare Research and Quality Evidence Report/Technology Assessment Diagnosis and Treatment of Deep Venous Thrombosis and Pulmonary Embolism Summary Number 68 Overview Venous thromboembolism
Agency for Healthcare Research and Quality Evidence Report/Technology Assessment Diagnosis and Treatment of Deep Venous Thrombosis and Pulmonary Embolism Summary Number 68 Overview Venous thromboembolism
VENOUS THROMBOEMBOLISM AND CORONARY ARTERY DISEASE: IS THERE A LINK?
 VENOUS THROMBOEMBOLISM AND CORONARY ARTERY DISEASE: IS THERE A LINK? Ayman El-Menyar (1), MD, Hassan Al-Thani (2),MD (1)Clinical Research Consultant, (2) Head of Vascular Surgery, Hamad General Hospital
VENOUS THROMBOEMBOLISM AND CORONARY ARTERY DISEASE: IS THERE A LINK? Ayman El-Menyar (1), MD, Hassan Al-Thani (2),MD (1)Clinical Research Consultant, (2) Head of Vascular Surgery, Hamad General Hospital
October 2017 Pulmonary Embolism
 October 2017 Pulmonary Embolism Prof. Ahmed BaHammam, FRCP, FCCP Professor of Medicine College of Medicine King Saud University 1 Objectives Epidemiology Pathophysiology Diagnosis Massive PE Treatment
October 2017 Pulmonary Embolism Prof. Ahmed BaHammam, FRCP, FCCP Professor of Medicine College of Medicine King Saud University 1 Objectives Epidemiology Pathophysiology Diagnosis Massive PE Treatment
Cover Page. The handle holds various files of this Leiden University dissertation.
 Cover Page The handle http://hdl.handle.net/1887/21764 holds various files of this Leiden University dissertation. Author: Mos, Inge Christina Maria Title: A more granular view on pulmonary embolism Issue
Cover Page The handle http://hdl.handle.net/1887/21764 holds various files of this Leiden University dissertation. Author: Mos, Inge Christina Maria Title: A more granular view on pulmonary embolism Issue
Risk factors for DVT. Venous thrombosis & pulmonary embolism. Anticoagulation (cont d) Diagnosis 1/5/2018. Ahmed Mahmoud, MD
 Diagnosis 1/5/2018. Ahmed Mahmoud, MD") Risk factors for DVT Venous thrombosis & pulmonary embolism Ahmed Mahmoud, MD Surgery ; post op especially for long cases, pelvic operations (THR), Trauma ; long bone fractures, pelvic fractures (posterior
Risk factors for DVT Venous thrombosis & pulmonary embolism Ahmed Mahmoud, MD Surgery ; post op especially for long cases, pelvic operations (THR), Trauma ; long bone fractures, pelvic fractures (posterior
Venous thrombosis & pulmonary embolism. Ahmed Mahmoud, MD
 Venous thrombosis & pulmonary embolism Ahmed Mahmoud, MD Risk factors for DVT Surgery ; post op especially for long cases, pelvic operations (THR), Trauma ; long bone fractures, pelvic fractures (posterior
Venous thrombosis & pulmonary embolism Ahmed Mahmoud, MD Risk factors for DVT Surgery ; post op especially for long cases, pelvic operations (THR), Trauma ; long bone fractures, pelvic fractures (posterior
CURRENT & FUTURE THERAPEUTIC MANAGEMENT OF VENOUS THROMBOEMBOLISM. Gordon Lowe Professor of Vascular Medicine University of Glasgow
 CURRENT & FUTURE THERAPEUTIC MANAGEMENT OF VENOUS THROMBOEMBOLISM Gordon Lowe Professor of Vascular Medicine University of Glasgow VENOUS THROMBOEMBOLISM Common cause of death and disability 50% hospital-acquired
CURRENT & FUTURE THERAPEUTIC MANAGEMENT OF VENOUS THROMBOEMBOLISM Gordon Lowe Professor of Vascular Medicine University of Glasgow VENOUS THROMBOEMBOLISM Common cause of death and disability 50% hospital-acquired
Updates in Diagnosis & Management of VTE
 Updates in Diagnosis & Management of VTE TRACY MINICHIELLO, MD CHIEF, ANTICOAGULATION& THROMBOSIS SERVICE-SAN FRANCISCO VAMC PROFESSOR OF MEDICINE UNIVERSITY OF CALIFORNIA, SAN FRANCISCO Financial Disclosures-NONE
Updates in Diagnosis & Management of VTE TRACY MINICHIELLO, MD CHIEF, ANTICOAGULATION& THROMBOSIS SERVICE-SAN FRANCISCO VAMC PROFESSOR OF MEDICINE UNIVERSITY OF CALIFORNIA, SAN FRANCISCO Financial Disclosures-NONE
PULMONARY EMBOLISM -CASE REPORT-
 University Goce Delcev, Faculty of Medical sciences, Stip University Clinic of Cardiology, Skopje R. Of Macedonia PULMONARY EMBOLISM -CASE REPORT- Gordana Kamceva MD mr.sci Acknowledgment Marija Vavlukis
University Goce Delcev, Faculty of Medical sciences, Stip University Clinic of Cardiology, Skopje R. Of Macedonia PULMONARY EMBOLISM -CASE REPORT- Gordana Kamceva MD mr.sci Acknowledgment Marija Vavlukis
Epidemiology: Incidence VTE: Mortality Morbidity Risk Factors: Acute Chronic : Genetic
 Submassive PE Pulmonary Embolism Epidemiology: Incidence VTE: 100-200/100,000 = 3rd most frequent cardiovascular disease Symptomatic DVT complicated by PE = 40-50% Sudden fatal PE = 34% Intermediate-risk
Submassive PE Pulmonary Embolism Epidemiology: Incidence VTE: 100-200/100,000 = 3rd most frequent cardiovascular disease Symptomatic DVT complicated by PE = 40-50% Sudden fatal PE = 34% Intermediate-risk
Deep Vein Thrombosis and Pulmonary Embolism: Patient Information
 Deep Vein Thrombosis and Pulmonary Embolism: Patient Information A Deep Vein Thrombosis (DVT) and a Pulmonary Embolism (PE) are both disorders of unwanted blood clotting. Unwanted blood clots can occur
Deep Vein Thrombosis and Pulmonary Embolism: Patient Information A Deep Vein Thrombosis (DVT) and a Pulmonary Embolism (PE) are both disorders of unwanted blood clotting. Unwanted blood clots can occur
Epidermiology Early pulmonary embolism
 Epidermiology Early pulmonary embolism Sitang Nirattisaikul Faculty of Medicine, Prince of Songkla University 3 rd most common cause of cardiovascular death in the United States, following ischemic heart
Epidermiology Early pulmonary embolism Sitang Nirattisaikul Faculty of Medicine, Prince of Songkla University 3 rd most common cause of cardiovascular death in the United States, following ischemic heart
Heart Health ESC Guidelines on the diagnosis and management of acute pulmonary embolism
 Heart Health Open Access Received: Oct 22, 2014 Accepted: Dec 01, 2014 Published: Dec 05, 2014 http://dx.doi.org/10.14437/hhoa-1-105 Review Jiri Widimsky, Heart Health Open Access 2014, 1:1 2014 ESC Guidelines
Heart Health Open Access Received: Oct 22, 2014 Accepted: Dec 01, 2014 Published: Dec 05, 2014 http://dx.doi.org/10.14437/hhoa-1-105 Review Jiri Widimsky, Heart Health Open Access 2014, 1:1 2014 ESC Guidelines
Venous thrombosis is common and often occurs spontaneously, but it also frequently accompanies medical and surgical conditions, both in the community
 Venous Thrombosis Venous Thrombosis It occurs mainly in the deep veins of the leg (deep vein thrombosis, DVT), from which parts of the clot frequently embolize to the lungs (pulmonary embolism, PE). Fewer
Venous Thrombosis Venous Thrombosis It occurs mainly in the deep veins of the leg (deep vein thrombosis, DVT), from which parts of the clot frequently embolize to the lungs (pulmonary embolism, PE). Fewer
Massive and Submassive Pulmonary Embolism: 2017 Update and Future Directions
 Massive and Submassive Pulmonary Embolism: 2017 Update and Future Directions Kush R Desai, MD Assistant Professor of Radiology Northwestern University Feinberg School of Medicine Chicago, IL Disclosures
Massive and Submassive Pulmonary Embolism: 2017 Update and Future Directions Kush R Desai, MD Assistant Professor of Radiology Northwestern University Feinberg School of Medicine Chicago, IL Disclosures
Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis. Prof. Ralf R.Kolvenbach MD,PhD,FEBVS
 Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis Prof. Ralf R.Kolvenbach MD,PhD,FEBVS Conflict of Interest BTG Standard PE therapy ANTICOAGULATION (AC) HEPARIN
Innovative Endovascular Approach to Pulmonary Embolism by Ultrasound Enhanced Thrombolysis Prof. Ralf R.Kolvenbach MD,PhD,FEBVS Conflict of Interest BTG Standard PE therapy ANTICOAGULATION (AC) HEPARIN
Use of EKOS Catheter in the management of Venous Mr. Manoj Niverthi, Mr. Sarang Pujari, and Ms. Nupur Dandavate, The GTF Group
 Use of EKOS Catheter in the management of Venous Thromboembolism @ Mr. Manoj Niverthi, Mr. Sarang Pujari, and Ms. Nupur Dandavate, The GTF Group Introduction Georgia Thrombosis Forum (GTF, www.gtfonline.net)
Use of EKOS Catheter in the management of Venous Thromboembolism @ Mr. Manoj Niverthi, Mr. Sarang Pujari, and Ms. Nupur Dandavate, The GTF Group Introduction Georgia Thrombosis Forum (GTF, www.gtfonline.net)
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC
 Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC 1 st workshop: update to VTE guidelines in 2016 2 nd workshop: VTE controversies + new horizons André Roussin MD, FRCP, CSPQ CHUM
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC 1 st workshop: update to VTE guidelines in 2016 2 nd workshop: VTE controversies + new horizons André Roussin MD, FRCP, CSPQ CHUM
How long to continue anticoagulation after DVT?
 How long to continue anticoagulation after DVT? Dr. Nihar Ranjan Pradhan M.S., DNB (Vascular Surgery), FVES(UK) Consultant Vascular Surgeon Apollo Hospital, Jubilee Hills, Hyderabad (Formerly Faculty in
How long to continue anticoagulation after DVT? Dr. Nihar Ranjan Pradhan M.S., DNB (Vascular Surgery), FVES(UK) Consultant Vascular Surgeon Apollo Hospital, Jubilee Hills, Hyderabad (Formerly Faculty in
Updates in Medical Management of Pulmonary Embolism and Deep Vein Thrombosis. By: Justin Youtsey, Elliott Reiff, William Montgomery, Grant Finlan
 Updates in Medical Management of Pulmonary Embolism and Deep Vein Thrombosis By: Justin Youtsey, Elliott Reiff, William Montgomery, Grant Finlan Objectives Describe the prevalence of PE and DVT as it relates
Updates in Medical Management of Pulmonary Embolism and Deep Vein Thrombosis By: Justin Youtsey, Elliott Reiff, William Montgomery, Grant Finlan Objectives Describe the prevalence of PE and DVT as it relates
Dr. Riaz JanMohamed Consultant Haematologist The Hillingdon Hospital Foundation Trust
 MANAGEMENT OF PATIENTS WITH DEEP VEIN THROMBOSIS (DVT) IN THE COMMUNITY SETTING & ANTICOAGULATION CLINICS THE PAST, PRESENT AND THE FUTURE Dr. Riaz JanMohamed Consultant Haematologist The Hillingdon Hospital
MANAGEMENT OF PATIENTS WITH DEEP VEIN THROMBOSIS (DVT) IN THE COMMUNITY SETTING & ANTICOAGULATION CLINICS THE PAST, PRESENT AND THE FUTURE Dr. Riaz JanMohamed Consultant Haematologist The Hillingdon Hospital
Acute and long-term treatment of PE. Cecilia Becattini University of Perugia
 Acute and long-term treatment of PE Cecilia Becattini University of Perugia Acute and long-term treatment of VTE What is the optimal acute phase treatment for the patient? Intravenous thrombolysis One
Acute and long-term treatment of PE Cecilia Becattini University of Perugia Acute and long-term treatment of VTE What is the optimal acute phase treatment for the patient? Intravenous thrombolysis One
Approach to Thrombosis
 Approach to Thrombosis Theera Ruchutrakool, M.D. Division of Hematology Department of Medicine Siriraj Hospital Faculty of Medicine Mahidol University Approach to Thrombosis Thrombosis: thrombus formation
Approach to Thrombosis Theera Ruchutrakool, M.D. Division of Hematology Department of Medicine Siriraj Hospital Faculty of Medicine Mahidol University Approach to Thrombosis Thrombosis: thrombus formation
Acute and long-term treatment of VTE. Cecilia Becattini University of Perugia
 Acute and long-term treatment of VTE Cecilia Becattini University of Perugia Acute and long-term treatment of VTE The goals The acute PE phase After the acute phase Treatment for VTE Goals of acute treatment
Acute and long-term treatment of VTE Cecilia Becattini University of Perugia Acute and long-term treatment of VTE The goals The acute PE phase After the acute phase Treatment for VTE Goals of acute treatment
Management of Acute Pulmonary Embolism. Judith Hurdman Consultant Respiratory Physician
 Management of Acute Pulmonary Embolism Judith Hurdman Consultant Respiratory Physician Judith.hurdman@sth.nhs.uk Overview Risk Stratification Who can be managed as an outpatient? To thrombolyse or not
Management of Acute Pulmonary Embolism Judith Hurdman Consultant Respiratory Physician Judith.hurdman@sth.nhs.uk Overview Risk Stratification Who can be managed as an outpatient? To thrombolyse or not
UC SF. Division of General Internal Medicine UNIVERSITY OF CALIFORNIA SAN FRANCISCO, DIVISION OF HOSPITAL MEDICINE
 Updates in the Management of Venous Thromboembolism Margaret C. Fang, MD, MPH Associate Professor of Medicine UCSF Division of Hospital Medicine Medical Director, Anticoagulation Clinic Venous Thromboembolism
Updates in the Management of Venous Thromboembolism Margaret C. Fang, MD, MPH Associate Professor of Medicine UCSF Division of Hospital Medicine Medical Director, Anticoagulation Clinic Venous Thromboembolism
Asif Serajian DO FACC FSCAI
 Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Anticoagulation and Antiplatelet update: A case based approach Asif Serajian DO FACC FSCAI No disclosures relevant to this talk Objectives 1. Discuss the indication for antiplatelet therapy for cardiac
Updates in Management of Pulmonary Embolism (PE) David Ming, MD Duke Hospital Medicine July 24, 2017 Hilton Head, SC
 David Ming, MD Duke Hospital Medicine July 24, 2017 Hilton Head, SC") Updates in Management of Pulmonary Embolism (PE) David Ming, MD Duke Hospital Medicine July 24, 2017 Hilton Head, SC Objectives Highlight clinical features and presentation of acute PE Analyze strategies
Updates in Management of Pulmonary Embolism (PE) David Ming, MD Duke Hospital Medicine July 24, 2017 Hilton Head, SC Objectives Highlight clinical features and presentation of acute PE Analyze strategies
DVT - initial management NSCCG
 Background information Information resources for patients and carers Updates to this care map Synonyms Below knee DVT and bleeding risks Patient with confirmed DVT Scan confirms superficial thrombophlebitis
Background information Information resources for patients and carers Updates to this care map Synonyms Below knee DVT and bleeding risks Patient with confirmed DVT Scan confirms superficial thrombophlebitis
VENOUS THROMBOEMBOLISM: DURATION OF TREATMENT
 VENOUS THROMBOEMBOLISM: DURATION OF TREATMENT OBJECTIVE: To provide guidance on the recommended duration of anticoagulant therapy for venous thromboembolism (VTE). BACKGROUND: Recurrent episodes of VTE
VENOUS THROMBOEMBOLISM: DURATION OF TREATMENT OBJECTIVE: To provide guidance on the recommended duration of anticoagulant therapy for venous thromboembolism (VTE). BACKGROUND: Recurrent episodes of VTE
Proper Diagnosis of Venous Thromboembolism (VTE)
") Proper Diagnosis of Venous Thromboembolism (VTE) Whal Lee, M.D. Seoul National University Hospital Department of Radiology 2 nd EFORT Asia Symposium, 3 rd November 2010, Taipei DVT - Risk Factors Previous
Proper Diagnosis of Venous Thromboembolism (VTE) Whal Lee, M.D. Seoul National University Hospital Department of Radiology 2 nd EFORT Asia Symposium, 3 rd November 2010, Taipei DVT - Risk Factors Previous
With All the New Drugs, This is How I Treat Acute DVT and Superficial Phlebitis
 BRIGHAM AND WOMEN S HOSPITAL With All the New Drugs, This is How I Treat Acute DVT and Superficial Phlebitis Gregory Piazza, MD, MS Division of Cardiovascular Medicine Brigham and Women s Hospital April
BRIGHAM AND WOMEN S HOSPITAL With All the New Drugs, This is How I Treat Acute DVT and Superficial Phlebitis Gregory Piazza, MD, MS Division of Cardiovascular Medicine Brigham and Women s Hospital April
REVIEW ON PULMONARY EMBOLISM
 REVIEW ON PULMONARY EMBOLISM * Shashi Kumar Yadav, Prof. Xiao Wei, Roshan Kumar Yadav, Sanjay Kumar Verma and Deepika Dhakal * Department of Medicine, Clinical College of Yangtze University, The first
REVIEW ON PULMONARY EMBOLISM * Shashi Kumar Yadav, Prof. Xiao Wei, Roshan Kumar Yadav, Sanjay Kumar Verma and Deepika Dhakal * Department of Medicine, Clinical College of Yangtze University, The first
CHAPTER 2 VENOUS THROMBOEMBOLISM
 CHAPTER 2 VENOUS THROMBOEMBOLISM Objectives Venous Thromboembolism (VTE) Prevalence Patho-physiology Risk Factors Diagnosis Pulmonary Embolism (PE) Management of DVT/PE Prevention VTE Patho-physiology
CHAPTER 2 VENOUS THROMBOEMBOLISM Objectives Venous Thromboembolism (VTE) Prevalence Patho-physiology Risk Factors Diagnosis Pulmonary Embolism (PE) Management of DVT/PE Prevention VTE Patho-physiology
10/8/2012. Disclosures. Making Sense of AT9: Review of the 2012 ACCP Antithrombotic Guidelines. Goals and Objectives. Outline
 Disclosures Making Sense of AT9: Review of the 2012 ACCP Antithrombotic Guidelines No relevant conflicts of interest related to the topic presented. Cyndy Brocklebank, PharmD, CDE Chronic Disease Management
Disclosures Making Sense of AT9: Review of the 2012 ACCP Antithrombotic Guidelines No relevant conflicts of interest related to the topic presented. Cyndy Brocklebank, PharmD, CDE Chronic Disease Management
Management of Pulmonary Embolism. Michael Hooper, M.D., MSc Associate Professor, Pulmonary and Critical Care Medicine Eastern Virginia Medical School
 Management of Pulmonary Embolism Michael Hooper, M.D., MSc Associate Professor, Pulmonary and Critical Care Medicine Eastern Virginia Medical School I have no conflicts of interest to report. VTE Overview
Management of Pulmonary Embolism Michael Hooper, M.D., MSc Associate Professor, Pulmonary and Critical Care Medicine Eastern Virginia Medical School I have no conflicts of interest to report. VTE Overview
What is New in Acute Pulmonary Embolism? Interventional Treatment. Prof. Nils Kucher University Hospital Bern Switzerland
 What is New in Acute Pulmonary Embolism? Interventional Treatment Prof. Nils Kucher University Hospital Bern Switzerland nils.kucher@insel.ch Disclosure of Interest Dr. Kucher received research grants
What is New in Acute Pulmonary Embolism? Interventional Treatment Prof. Nils Kucher University Hospital Bern Switzerland nils.kucher@insel.ch Disclosure of Interest Dr. Kucher received research grants
A 50-year-old woman with syncope
 Hira Shahzad 1, Ali Bin Sarwar Zubairi 2 1 Medical College, Aga Khan University Hospital, Karachi 2 Department of Medicine, Aga Khan University Hospital, Karachi, Pakistan Ali Bin Sarwar Zubairi Associate
Hira Shahzad 1, Ali Bin Sarwar Zubairi 2 1 Medical College, Aga Khan University Hospital, Karachi 2 Department of Medicine, Aga Khan University Hospital, Karachi, Pakistan Ali Bin Sarwar Zubairi Associate
Is Thrombolysis Only for a Crisis?
 Is Thrombolysis Only for a Crisis? December 19, 2017 Is Thrombolysis Only for a Crisis? Indications for Thrombolytic Therapy in Patients with Acute Pulmonary Embolism Case Scenario A 28 year old woman
Is Thrombolysis Only for a Crisis? December 19, 2017 Is Thrombolysis Only for a Crisis? Indications for Thrombolytic Therapy in Patients with Acute Pulmonary Embolism Case Scenario A 28 year old woman
Updates in venous thromboembolism. Cecilia Becattini University of Perugia
 Updates in venous thromboembolism Cecilia Becattini University of Perugia News for VTE Diagnosis Treatment the acute phase the agents Pulmonary embolism: diagnosis Vein ultrasonography Meta-analysis 15
Updates in venous thromboembolism Cecilia Becattini University of Perugia News for VTE Diagnosis Treatment the acute phase the agents Pulmonary embolism: diagnosis Vein ultrasonography Meta-analysis 15
INDICATIONS FOR THROMBO-PROPHYLAXIS AND WHEN TO STOP ANTICOAGULATION BEFORE ELECTIVE SURGERY
 INDICATIONS FOR THROMBO-PROPHYLAXIS AND WHEN TO STOP ANTICOAGULATION BEFORE ELECTIVE SURGERY N.E. Pearce INTRODUCTION Preventable death Cause of morbidity and mortality Risk factors Pulmonary embolism
INDICATIONS FOR THROMBO-PROPHYLAXIS AND WHEN TO STOP ANTICOAGULATION BEFORE ELECTIVE SURGERY N.E. Pearce INTRODUCTION Preventable death Cause of morbidity and mortality Risk factors Pulmonary embolism
Chapter 1. Introduction
 Chapter 1 Introduction Introduction 9 Even though the first reports on venous thromboembolism date back to the 13 th century and the mechanism of acute pulmonary embolism (PE) was unraveled almost 150
Chapter 1 Introduction Introduction 9 Even though the first reports on venous thromboembolism date back to the 13 th century and the mechanism of acute pulmonary embolism (PE) was unraveled almost 150
Ultrasound-enhanced, catheter-directed thrombolysis for pulmonary embolism
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Ultrasound-enhanced, catheter-directed thrombolysis for pulmonary embolism A pulmonary embolism (PE) is
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Ultrasound-enhanced, catheter-directed thrombolysis for pulmonary embolism A pulmonary embolism (PE) is
Updates in Diagnosis & Management of VTE
 Updates in Diagnosis & Management of VTE Financial Disclosures-NONE TRACY MINICHIELLO, MD CHIEF, ANTICOAGULATION& THROMBOSIS SERVICE- SAN FRANCISCO VAMC PROFESSOR OF MEDICINE UNIVERSITY OF CALIFORNIA,
Updates in Diagnosis & Management of VTE Financial Disclosures-NONE TRACY MINICHIELLO, MD CHIEF, ANTICOAGULATION& THROMBOSIS SERVICE- SAN FRANCISCO VAMC PROFESSOR OF MEDICINE UNIVERSITY OF CALIFORNIA,
Pulmonary Embolism. Thoracic radiologist Helena Lauri
 Pulmonary Embolism Thoracic radiologist Helena Lauri 8.5.2017 Statistics 1-2 out of 1000 adults annually are diagnosed with deep vein thrombosis (DVT) and/or pulmonary embolism (PE) About half of patients
Pulmonary Embolism Thoracic radiologist Helena Lauri 8.5.2017 Statistics 1-2 out of 1000 adults annually are diagnosed with deep vein thrombosis (DVT) and/or pulmonary embolism (PE) About half of patients
COMMITTEE FOR PROPRIETARY MEDICINAL PRODUCTS (CPMP)
") The European Agency for the Evaluation of Medicinal Products Evaluation of Medicines for Human Use London, 16 December 1999 COMMITTEE FOR PROPRIETARY MEDICINAL PRODUCTS (CPMP) NOTE FOR GUIDANCE ON CLINICAL
The European Agency for the Evaluation of Medicinal Products Evaluation of Medicines for Human Use London, 16 December 1999 COMMITTEE FOR PROPRIETARY MEDICINAL PRODUCTS (CPMP) NOTE FOR GUIDANCE ON CLINICAL
Challenges in Anticoagulation and Thromboembolism
 Challenges in Anticoagulation and Thromboembolism Ethan Cumbler M.D. Assistant Professor of Medicine Hospitalist Medicine Section University of Colorado Denver May 2010 No Conflicts of Interest Objectives
Challenges in Anticoagulation and Thromboembolism Ethan Cumbler M.D. Assistant Professor of Medicine Hospitalist Medicine Section University of Colorado Denver May 2010 No Conflicts of Interest Objectives
8/16/2012. Pulmonary Embolism
 Pulmonary Embolism Rita M. Williams, NP-C, PA PeaceHealth Medical Group, Pulmonary & Critical Care Pulmonary Embolism Acute pulmonary embolism (PE) is a common and frequently fatal disease Clinical presentation
Pulmonary Embolism Rita M. Williams, NP-C, PA PeaceHealth Medical Group, Pulmonary & Critical Care Pulmonary Embolism Acute pulmonary embolism (PE) is a common and frequently fatal disease Clinical presentation
Diagnosis and management of pulmonary embolism
 Follow the link from the online version of this article to obtain certified continuing medical education credits bmj.com Respiratory Medicine updates from BMJ Group are at bmj.com/specialties/respiratory-medicine
Follow the link from the online version of this article to obtain certified continuing medical education credits bmj.com Respiratory Medicine updates from BMJ Group are at bmj.com/specialties/respiratory-medicine
Pulmonary embolism. Paweł Balsam
 Pulmonary embolism Paweł Balsam Venous thromboembolism (VTE) Pulmonary embolism (PE) and deep vein thrombosis (DVT) are two clinical presentations of veonus thromboembolism Pulmonary embolism A pulmonary
Pulmonary embolism Paweł Balsam Venous thromboembolism (VTE) Pulmonary embolism (PE) and deep vein thrombosis (DVT) are two clinical presentations of veonus thromboembolism Pulmonary embolism A pulmonary
Handbook for Venous Thromboembolism
 Handbook for Venous Thromboembolism Gregory Piazza Benjamin Hohlfelder Samuel Z. Goldhaber Handbook for Venous Thromboembolism Gregory Piazza Cardiovascular Division Harvard Medical School Brigham and
Handbook for Venous Thromboembolism Gregory Piazza Benjamin Hohlfelder Samuel Z. Goldhaber Handbook for Venous Thromboembolism Gregory Piazza Cardiovascular Division Harvard Medical School Brigham and
DVT and Pulmonary Embolus. Dr Piers Blombery BSc(Biomed), MBBS (Hons), FRACP, FRCPA Consultant Haematologist Peter MacCallum Cancer Centre
, MBBS (Hons), FRACP, FRCPA Consultant Haematologist Peter MacCallum Cancer Centre") DVT and Pulmonary Embolus Dr Piers Blombery BSc(Biomed), MBBS (Hons), FRACP, FRCPA Consultant Haematologist Peter MacCallum Cancer Centre Overview Structure of deep and superficial venous system of upper
DVT and Pulmonary Embolus Dr Piers Blombery BSc(Biomed), MBBS (Hons), FRACP, FRCPA Consultant Haematologist Peter MacCallum Cancer Centre Overview Structure of deep and superficial venous system of upper
DEEP VENOUS THROMBOSIS A PRACTICAL APPROACH TO IMPROVING CLINICAL OUTCOMES
 DEEP VENOUS THROMBOSIS A PRACTICAL APPROACH TO IMPROVING CLINICAL OUTCOMES Jose M. Borromeo M.D. Vascular Surgeon Iowa Heart Center Disclosures: AstraZeneca Pharmaceuticals Cook CVRx LeMaitre Vascular,
DEEP VENOUS THROMBOSIS A PRACTICAL APPROACH TO IMPROVING CLINICAL OUTCOMES Jose M. Borromeo M.D. Vascular Surgeon Iowa Heart Center Disclosures: AstraZeneca Pharmaceuticals Cook CVRx LeMaitre Vascular,
The Treatment of Venous Thromboembolism (VTE): Has Warfarin Met Its Match? Michael P. Gulseth, Pharm. D., BCPS, FASHP Program Director for
: Has Warfarin Met Its Match? Michael P. Gulseth, Pharm. D., BCPS, FASHP Program Director for") The Treatment of Venous Thromboembolism (VTE): Has Warfarin Met Its Match? Michael P. Gulseth, Pharm. D., BCPS, FASHP Program Director for Anticoagulation Services Sanford USD Medical Center Sioux Falls,
The Treatment of Venous Thromboembolism (VTE): Has Warfarin Met Its Match? Michael P. Gulseth, Pharm. D., BCPS, FASHP Program Director for Anticoagulation Services Sanford USD Medical Center Sioux Falls,
Mark H. Meissner, MD Peter Gloviczki Professor of Venous & Lymphatic Disorders University of Washington School of Medicine
 Pulmonary Embolism Response Teams Not So Fast Early Interventions is a House of Cards Mark H. Meissner, MD Peter Gloviczki Professor of Venous & Lymphatic Disorders University of Washington School of Medicine
Pulmonary Embolism Response Teams Not So Fast Early Interventions is a House of Cards Mark H. Meissner, MD Peter Gloviczki Professor of Venous & Lymphatic Disorders University of Washington School of Medicine
THROMBOSIS RISK FACTOR ASSESSMENT
 Name: Procedure: Doctor: Date: THROMBOSIS RISK FACTOR ASSESSMENT CHOOSE ALL THAT APPLY EACH RISK FACTOR REPRESENTS 1 POINT Age 41 60 years Minor Surgery Planned History of Prior Major Surgery (< 1 month)
Name: Procedure: Doctor: Date: THROMBOSIS RISK FACTOR ASSESSMENT CHOOSE ALL THAT APPLY EACH RISK FACTOR REPRESENTS 1 POINT Age 41 60 years Minor Surgery Planned History of Prior Major Surgery (< 1 month)
This chapter will describe the effectiveness of antithrombotic
 Antithrombotic Therapy for Venous Thromboembolic Disease The Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy Harry R. Büller, MD, Chair; Giancarlo Agnelli, MD; Russel D. Hull, MBBS,
Antithrombotic Therapy for Venous Thromboembolic Disease The Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy Harry R. Büller, MD, Chair; Giancarlo Agnelli, MD; Russel D. Hull, MBBS,
Diagnosis and Treatment of Pulmonary Embolism: High-Tech versus Low- Tech, which way to go?
 Diagnosis and Treatment of Pulmonary Embolism: High-Tech versus Low- Tech, which way to go? Philip S. Wells MD, FRCPC, MSc Professor Chair and Chief, Department of Medicine, University of Ottawa DISCLOSURE
Diagnosis and Treatment of Pulmonary Embolism: High-Tech versus Low- Tech, which way to go? Philip S. Wells MD, FRCPC, MSc Professor Chair and Chief, Department of Medicine, University of Ottawa DISCLOSURE
Pulmonary embolism - the great masquerader
 Pulmonary embolism - the great masquerader V.N. Karazin Kharkov National University Department of Internal Medicine Associate professor Makharynska О.S., MD, PhD 2016 Pulmonary embolism (PE) is a blockage
Pulmonary embolism - the great masquerader V.N. Karazin Kharkov National University Department of Internal Medicine Associate professor Makharynska О.S., MD, PhD 2016 Pulmonary embolism (PE) is a blockage
Objectives. Venous Thromboembolism (VTE) Prophylaxis. Case VTE WHY DO IT? Question: Who Is At Risk?
 Prophylaxis. Case VTE WHY DO IT? Question: Who Is At Risk?") Objectives Venous Thromboembolism (VTE) Prophylaxis Rishi Garg, MD Department of Medicine Identify patients at risk for VTE Options for VTE prophylaxis Current Recommendations (based on The Seventh ACCP
Objectives Venous Thromboembolism (VTE) Prophylaxis Rishi Garg, MD Department of Medicine Identify patients at risk for VTE Options for VTE prophylaxis Current Recommendations (based on The Seventh ACCP
Treatment Options and How They Work
 Treatment Options and How They Work Robin Offord Director of Clinical Pharmacy UCL Hospitals NHS Foundation Trust robin.offord@uclh.nhs.uk Introducing the term anticoagulant... What they do Inhibit the
Treatment Options and How They Work Robin Offord Director of Clinical Pharmacy UCL Hospitals NHS Foundation Trust robin.offord@uclh.nhs.uk Introducing the term anticoagulant... What they do Inhibit the
Implications from the ACCP 2012 Consensus Guidelines for the Management of Thrombosis: a case based approach
 Implications from the ACCP 2012 Consensus Guidelines for the Management of Thrombosis: a case based approach Prof. I. Baumgartner Head Clinical and Interventional Angiology About the ACCP guidelines Widely
Implications from the ACCP 2012 Consensus Guidelines for the Management of Thrombosis: a case based approach Prof. I. Baumgartner Head Clinical and Interventional Angiology About the ACCP guidelines Widely
Slide 1. Slide 2. Slide 3. Outline of This Presentation
 Slide 1 Current Approaches to Venous Thromboembolism Prevention in Orthopedic Patients Hujefa Vora, MD Maria Fox, RN June 9, 2017 Slide 2 Slide 3 Outline of This Presentation Pathophysiology of venous
Slide 1 Current Approaches to Venous Thromboembolism Prevention in Orthopedic Patients Hujefa Vora, MD Maria Fox, RN June 9, 2017 Slide 2 Slide 3 Outline of This Presentation Pathophysiology of venous
Radiologic Features of The Pulmonary Embolus
 January 2003 Radiologic Features of The Pulmonary Embolus Travis McGlothin HMSIII Mr. J is a 51 y.o. male who presented to the BIDMC ED w/ acute onset of: Lft. Hemiparesis slurred speech mild dyspnea mild
January 2003 Radiologic Features of The Pulmonary Embolus Travis McGlothin HMSIII Mr. J is a 51 y.o. male who presented to the BIDMC ED w/ acute onset of: Lft. Hemiparesis slurred speech mild dyspnea mild
Case. Case. Management of Pulmonary Embolism in the ICU
 Management of Pulmonary Embolism in the ICU Todd M Bull, M.D. Associate Professor of Medicine Division of Pulmonary Sciences and Critical Care Medicine Pulmonary Hypertension Center University of Colorado
Management of Pulmonary Embolism in the ICU Todd M Bull, M.D. Associate Professor of Medicine Division of Pulmonary Sciences and Critical Care Medicine Pulmonary Hypertension Center University of Colorado
Pulmonary embolism. Paweł Balsam MD, PhD
 Pulmonary embolism Paweł Balsam MD, PhD Venous thromboembolism (VTE) Pulmonary embolism (PE) and deep vein thrombosis (DVT) are two clinical presentations of veonus thromboembolism Pulmonary embolism A
Pulmonary embolism Paweł Balsam MD, PhD Venous thromboembolism (VTE) Pulmonary embolism (PE) and deep vein thrombosis (DVT) are two clinical presentations of veonus thromboembolism Pulmonary embolism A
CARDIAC PROBLEMS IN PREGNANCY
 CARDIAC PROBLEMS IN PREGNANCY LAS VEGAS, NEVADA, USA 27 February 1 March 2016 SUCCESSFUL TREATMENT WITH RECOMBINANT TISSUE PLASMINOGEN ACTIVATOR OF MASSIVE PULMONARY EMBOLISM IN THE 16 TH WEEK OF PREGNANCY
CARDIAC PROBLEMS IN PREGNANCY LAS VEGAS, NEVADA, USA 27 February 1 March 2016 SUCCESSFUL TREATMENT WITH RECOMBINANT TISSUE PLASMINOGEN ACTIVATOR OF MASSIVE PULMONARY EMBOLISM IN THE 16 TH WEEK OF PREGNANCY
Duration of Anticoagulant Therapy. Linda R. Kelly PharmD, PhC, CACP September 17, 2016
 Duration of Anticoagulant Therapy Linda R. Kelly PharmD, PhC, CACP September 17, 2016 Conflicts of Interest No conflicts of interest to report Objectives At the end of the program participants will be
Duration of Anticoagulant Therapy Linda R. Kelly PharmD, PhC, CACP September 17, 2016 Conflicts of Interest No conflicts of interest to report Objectives At the end of the program participants will be
University Journal of Medicine and Medical Specialities
 University Journal of Medicine and Medical Specialities Volume 1 Issue 1 2015 An unusual case of SADDLE Pulmonary Thrombo Embolism Boopathirajan P Jayanthi R Stanley Medical College Abstract: Pulmonary
University Journal of Medicine and Medical Specialities Volume 1 Issue 1 2015 An unusual case of SADDLE Pulmonary Thrombo Embolism Boopathirajan P Jayanthi R Stanley Medical College Abstract: Pulmonary
DVT PROPHYLAXIS IN HOSPITALIZED MEDICAL PATIENTS SAURABH MAJI SR (PULMONARY,MEDICINE)
") DVT PROPHYLAXIS IN HOSPITALIZED MEDICAL PATIENTS SAURABH MAJI SR (PULMONARY,MEDICINE) Introduction VTE (DVT/PE) is an important complication in hospitalized patients Hospitalization for acute medical illness
DVT PROPHYLAXIS IN HOSPITALIZED MEDICAL PATIENTS SAURABH MAJI SR (PULMONARY,MEDICINE) Introduction VTE (DVT/PE) is an important complication in hospitalized patients Hospitalization for acute medical illness
Managing Perioperative Anticoagulation. Edie Shen MD
 Managing Perioperative Anticoagulation Edie Shen MD Anticoagulation VKA Warfarin (Coumadin) DOACs Direct Thrombin Inhibitor Dabigatran (Pradaxa) Factor Xa Inhibitor Rivaroxaban(Xarelto) Apixaban(Eliquis)
Managing Perioperative Anticoagulation Edie Shen MD Anticoagulation VKA Warfarin (Coumadin) DOACs Direct Thrombin Inhibitor Dabigatran (Pradaxa) Factor Xa Inhibitor Rivaroxaban(Xarelto) Apixaban(Eliquis)
RISK STRATIFICATION OF PATIENTS WITH ACUTE SYMPTOMATIC PULMONARY EMBOLISM. David Jiménez, MD, PhD, FCCP Ramón y Cajal Hospital, IRYCIS Madrid, Spain
 RISK STRATIFICATION OF PATIENTS WITH ACUTE SYMPTOMATIC PULMONARY EMBOLISM David Jiménez, MD, PhD, FCCP Ramón y Cajal Hospital, IRYCIS Madrid, Spain Potential Conflicts of Interest Financial conflicts of
RISK STRATIFICATION OF PATIENTS WITH ACUTE SYMPTOMATIC PULMONARY EMBOLISM David Jiménez, MD, PhD, FCCP Ramón y Cajal Hospital, IRYCIS Madrid, Spain Potential Conflicts of Interest Financial conflicts of
Management of Massive and Sub-Massive Pulmonary Embolism
 Management of Massive and Sub-Massive Pulmonary Embolism M. Montero-Baker, MD L Leon Jr., MD, RVT, FACS Tucson Medical Center Vascular and Endovascular Surgery Section CASE PRESENTATION 54 YEAR- OLD CAUCASIAN
Management of Massive and Sub-Massive Pulmonary Embolism M. Montero-Baker, MD L Leon Jr., MD, RVT, FACS Tucson Medical Center Vascular and Endovascular Surgery Section CASE PRESENTATION 54 YEAR- OLD CAUCASIAN
Medical Patients: A Population at Risk
 Case Vignette A 68-year-old woman with obesity was admitted to the Medical Service with COPD and pneumonia and was treated with oral corticosteroids, bronchodilators, and antibiotics. She responded well
Case Vignette A 68-year-old woman with obesity was admitted to the Medical Service with COPD and pneumonia and was treated with oral corticosteroids, bronchodilators, and antibiotics. She responded well
Misunderstandings of Venous thromboembolism prophylaxis
 Misunderstandings of Venous thromboembolism prophylaxis Veerendra Chadachan Senior Consultant Dept of General Medicine (Vascular Medicine and Hypertension) Tan Tock Seng Hospital, Singapore Case scenario
Misunderstandings of Venous thromboembolism prophylaxis Veerendra Chadachan Senior Consultant Dept of General Medicine (Vascular Medicine and Hypertension) Tan Tock Seng Hospital, Singapore Case scenario
Clinical Guide - Suspected PE (Reviewed 2006)
") Clinical Guide - Suspected (Reviewed 2006) Principal Developer: B. Geerts Secondary Developers: C. Demers, C. Kearon Background Investigation of patients with suspected pulmonary emboli () remains problematic
Clinical Guide - Suspected (Reviewed 2006) Principal Developer: B. Geerts Secondary Developers: C. Demers, C. Kearon Background Investigation of patients with suspected pulmonary emboli () remains problematic
Venous Thromboembolism Prophylaxis
 Approved by: Venous Thromboembolism Prophylaxis Vice President and Chief Medical Officer; and Vice President and Chief Operating Officer Corporate Policy & Procedures Manual Number: Date Approved January
Approved by: Venous Thromboembolism Prophylaxis Vice President and Chief Medical Officer; and Vice President and Chief Operating Officer Corporate Policy & Procedures Manual Number: Date Approved January
Low Molecular Weight Heparin for Prevention and Treatment of Venous Thromboembolic Disorders
 SURGICAL GRAND ROUNDS March 17 th, 2007 Low Molecular Weight Heparin for Prevention and Treatment of Venous Thromboembolic Disorders Guillermo Escobar, M.D. LMWH vs UFH Jayer s sales pitch: FALSE LMW is
SURGICAL GRAND ROUNDS March 17 th, 2007 Low Molecular Weight Heparin for Prevention and Treatment of Venous Thromboembolic Disorders Guillermo Escobar, M.D. LMWH vs UFH Jayer s sales pitch: FALSE LMW is