Cholecystectomy. Sarah Forsyth
|
|
|
- Carmella Johnson
- 6 years ago
- Views:
Transcription
1 Cholecystectomy Sarah Forsyth

2 History of Cholecystectomy
3 First open cholecystectomy 1882 by Carl Langenbuch in Germany First lap cholecystectomy 1987, Philip Mouret (Gynaecologist) in Lyon, France 1990, Francois Dubois (French surgeon) published a case series
4 Anatomy
5 Gall bladder Pear shaped viscous, stores & concentrates bile secreted by the liver 50ml capacity 3 parts: Fundus Body Neck n Hartmann s pouch Lies in the GB fossa on visceral surface of R lobe of liver, adjacent to quadrate lobe


6 Gall bladder Relations: Liver, ant abdo wall, duodenum, TV colon Surface anatomy Fundus projects below lower border of liver, touches ant abdo wall n Tip 9 th CC n Lateral border R rectus sheath n Transpyloric plane crosses the R costal margin
7 Histology Wall composed of fibromuscular tissue Non striated muscle cells composed in circular, longitudinal & oblique fashion Mucosa: single layer of simple columnar epithelium n Secrete mucous, no goblet cells Spiral valves of Heister: neck and cystic duct, spiral folds of mucosa
 Diameter 2-3mm 3 major modes of entry into CHD Variations: Cystic duct joins")
8 Cystic duct Passes down & back to join the CHD to form the CBD Length 2-3cm (Last s), 2-8cm (Jamieson s) Diameter 2-3mm 3 major modes of entry into CHD Variations: Cystic duct joins RHD
9 Cystic artery Main blood supply to GB In addition to small vessels from hepatic bed Branch of RHA R side of RHD Passes behind cystic duct to reach neck of GB Branches into ant & post cystic art Variations: Branch of CHA/LHA/GDA 25% of people arises on L side of duct system, crosses in front of duct to reach GB
10 Calot s triangle Triangle formed by: Liver Cystic duct CHD Cystic artery usually found within the triangle
11 Describing the operation What is the aim of a laparoscopic cholecystectomy?
12 To not cause a bile duct injury!
13 Check your set up IOC booked II table Laparoscopic stack with 30 degree scope Port sizes/types Hook diathermy/sucker/clip applicator/concord or RO/graspers (ratchet)/endocatch/drain Sutures
14 Patient positioning Time out/iv Abx/DVT prophylaxis/cc/diathermy plate & set to 30 coag/0 cut Supine L arm in, R arm out Prep from nipple line Drape Superior & lateral drape position Suitable for conversion to open Laparoscopic set up Screen on patients right side
15 Access 15 blade Subumbilical incision Identify cicatrix Incision in linea alba 0 vicryl stay suture 10mm Hasson port Pneumoperitoneum Pressure 12mmHg Position patient reverse trendelenburg/r side up
16 Access Ports introduced under direct vision LA marcain 0.5% w adrenaline 1 x 10mm epigastric port 2 x 5mm R flank/ruq
 & retracts cranially Hartmann s pouch grasped and retracted")
17 Assistant and surgeon on left side of patient Assistant grasps fundus with toothed forcep (ratchet) & retracts cranially Hartmann s pouch grasped and retracted laterally

18 Identify critical structures

19 Identify critical structures

20 Identify critical structures

21 Dissection Peritoneum over medial/lateral edges of GB divided Peritoneum over hepatocystic triangle divided
22 Establish critical view of safety Clear hepatocystic triangle of fat and fibrous tissue Diathermy/sucker/blunt dissection Create window between duct & artery/artery and liver Dissect the GB off the cystic plate Cystic artery Clip x 3 and divide with scissors Cystic duct Clip proximally Incision in duct with scissors to perform IOC
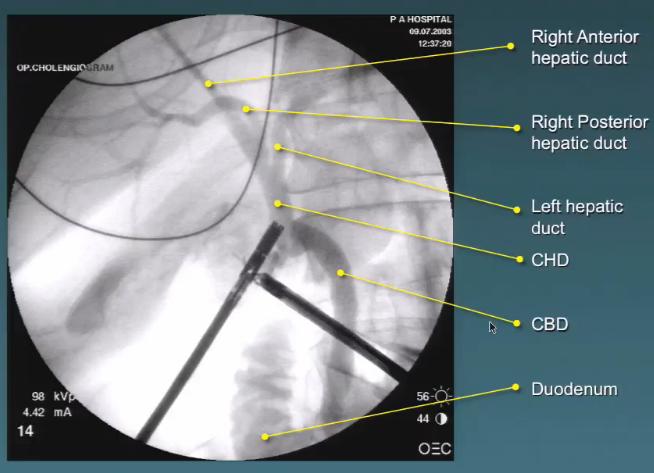
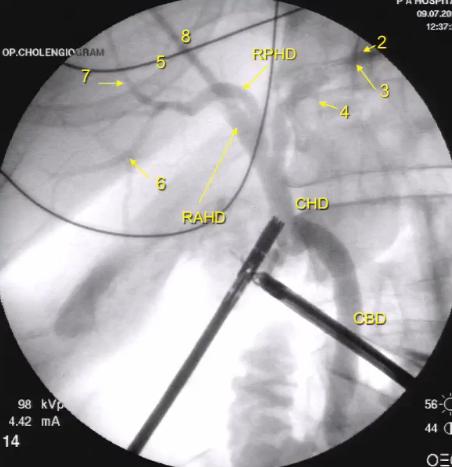
23 IOC 5 things 1. Filling defects 2. Free flow into duodenum 3. Tapering of CBD into duodenum 4. R & L hepatic ducts/intrahepatic biliary tree 5. Size of cystic duct/cbd
24 IOC Concord needle or Reddick Olsen (4Fr ureteric catheter) 20ml syringe with NS to catheter and insert into duct (L port) Clamp over catheter & ensure free flow of NS without leak Level and raise table for II Place clip to secure ratchet grasper on GB Attach 20ml syringe of contrast (omnipaque) to catheter ensuring no bubbles Mayo to cover II Shot to establish position, then save images at 3 frames/ second Slow injection of contrast to observe filling of CBD
25 IOC
26 Finish dissection Place 3 clips distally on cystic duct and divide between clips If any concern about cystic duct stump, apply endoloop Dissect rest of GB off liver bed with hook diathermy Move laparoscope to epigastric port, insert endocatch bag, place GB in bag and secure suture externally
27 Post dissection Inspect GB fossa for bleeding/bile leak Haemostasis with diathermy if required Level patient, irrigation and lavage Desufflate Remove bag/gb through umbilical port incision 10mm jackson pratt drain if necessary Closure: 0 vicryl fascia 3-0 monocryl subcuticular to skin Dress with steri strips/opsite dressing

28 Strasberg critical view of safety (CVS) Rationale and Use of the Critical View of Safety in Laparoscopic Cholecystectomy Steven M Strasberg, MD, FACS, L Michael Brunt, MD, FACS
29 CVS Three requirements 1. Calot s triangle must be cleared of fat and fibrous tissue 2. The lowest part of the GB must be separated from the cystic plate 3. Two structures, and only two, should be seen entering the GB
30 CVS Figure 3. Difference between 2 windows and critical view of safety (CVS). (A) Dissection has led to the creation of 2 windows, 1 between the cystic duct and artery and 1 between the artery and the liver (arrows). This dissection does not fulfill the criteria of CVS because the cystic plate cannot be clearly identified. (B) CVS. Arrow points to whitish clearly identified cystic plate.
31 CVS Figure 4. Different appearances of the cystic plate. (A) Critical view of safety (CVS) is seen from in front of the gallbladder as usually shown. The cystic plate is very thin. (B) CVS is seen with the gallbladder reflected to the left so that a posterior view of the triangle of Calot is shown. The cystic plate is thicker and whitish. Both views fulfill criteria for CVS.
32 IOC Routine vs Selective Routine: Anatomy Stones Early ID of injury Routine skill

33 Routine IOC
34
Surface Anatomy. Location Shape Weight Role of Five Surfaces Borders Fissures Lobes Peritoneal Lig
 The Liver Functions Bile production and secretion Detoxification Storage of glycogen Protein synthesis Production of heparin and bile pigments Erythropoiesis (in fetus) Surface Anatomy Location Shape Weight
The Liver Functions Bile production and secretion Detoxification Storage of glycogen Protein synthesis Production of heparin and bile pigments Erythropoiesis (in fetus) Surface Anatomy Location Shape Weight
Complication of Laparoscopic Cholecystectomy
 Complication of Laparoscopic Cholecystectomy R.K.Mishra What to do if something goes wrong There is not a single laparoscopic surgeon in the world who has not damaged CBD Complications Early Common bile
Complication of Laparoscopic Cholecystectomy R.K.Mishra What to do if something goes wrong There is not a single laparoscopic surgeon in the world who has not damaged CBD Complications Early Common bile
Pancreas & Biliary System. Dr. Vohra & Dr. Jamila
 Pancreas & Biliary System Dr. Vohra & Dr. Jamila 1 Objectives At the end of the lecture, the student should be able to describe the: Location, surface anatomy, parts, relations & peritoneal reflection
Pancreas & Biliary System Dr. Vohra & Dr. Jamila 1 Objectives At the end of the lecture, the student should be able to describe the: Location, surface anatomy, parts, relations & peritoneal reflection
Clinical Anatomy of the Biliary Apparatus: Relations & Variations
 Clinical Anatomy of the Biliary Apparatus: Relations & Variations Handout download: http://www.oucom.ohiou.edu/dbms-witmer/gs-rpac.htm 27 March 2007 Lawrence M. Witmer, PhD Professor of Anatomy Department
Clinical Anatomy of the Biliary Apparatus: Relations & Variations Handout download: http://www.oucom.ohiou.edu/dbms-witmer/gs-rpac.htm 27 March 2007 Lawrence M. Witmer, PhD Professor of Anatomy Department
Accessory Glands of Digestive System
 Accessory Glands of Digestive System The liver The liver is soft and pliable and occupies the upper part of the abdominal cavity just beneath the diaphragm. The greater part of the liver is situated under
Accessory Glands of Digestive System The liver The liver is soft and pliable and occupies the upper part of the abdominal cavity just beneath the diaphragm. The greater part of the liver is situated under
Retrieval of Gallbladder through Subxiphoid V/S Supraumbilical Port in Laparoscopic Cholecystectomy.
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 17, Issue 8 Ver. 4 (August. 2018), PP 36-41 www.iosrjournals.org Retrieval of Gallbladder through Subxiphoid
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 17, Issue 8 Ver. 4 (August. 2018), PP 36-41 www.iosrjournals.org Retrieval of Gallbladder through Subxiphoid
Duodenum retroperitoneal
 Duodenum retroperitoneal C shaped Initial region out of stomach into small intestine RETROperitoneal viscus Superior 1 st part duodenal cap ; moves upwards and backwards to lie on the R crura medial to
Duodenum retroperitoneal C shaped Initial region out of stomach into small intestine RETROperitoneal viscus Superior 1 st part duodenal cap ; moves upwards and backwards to lie on the R crura medial to
My Patient Has Abdominal Pain PoCUS of the Biliary Tract and the Urinary Tract
 My Patient Has Abdominal Pain PoCUS of the Biliary Tract and the Urinary Tract Objectives PoCUS for Biliary Disease PoCUS for Renal Colic PoCUS for Urinary Retention Biliary Disease A patient presents
My Patient Has Abdominal Pain PoCUS of the Biliary Tract and the Urinary Tract Objectives PoCUS for Biliary Disease PoCUS for Renal Colic PoCUS for Urinary Retention Biliary Disease A patient presents
The Physician as Medical Illustrator
 The Physician as Medical Illustrator Francois Luks Arlet Kurkchubasche Division of Pediatric Surgery Wednesday, December 9, 2015 Week 5 A good picture is worth a 1,000 bad ones How to illustrate an operation
The Physician as Medical Illustrator Francois Luks Arlet Kurkchubasche Division of Pediatric Surgery Wednesday, December 9, 2015 Week 5 A good picture is worth a 1,000 bad ones How to illustrate an operation
Pancreas and Biliary System
 Pancreas and Biliary System Please view our Editing File before studying this lecture to check for any changes. Color Code Important Doctors Notes Notes/Extra explanation Objectives At the end of the lecture,
Pancreas and Biliary System Please view our Editing File before studying this lecture to check for any changes. Color Code Important Doctors Notes Notes/Extra explanation Objectives At the end of the lecture,
INGUINAL HERNIA REPAIR PROCEDURE GUIDE
 ROOM CONFIGURATION The following figure shows an overhead view of the recommended OR configuration for a da Vinci Inguinal Hernia Repair (Figure 1). NOTE: Configuration of the operating room suite is dependent
ROOM CONFIGURATION The following figure shows an overhead view of the recommended OR configuration for a da Vinci Inguinal Hernia Repair (Figure 1). NOTE: Configuration of the operating room suite is dependent
JMSCR Volume 03 Issue 05 Page May 2015
 www.jmscr.igmpublication.org Impact Factor 3.79 ISSN (e)-2347-176x Comparison of 3-Port Versus 4-Port Laproscopic Cholecystectomy- A Prospective Comparative Study Authors Shekhar Gogna 1, Priya Goyal 2,
www.jmscr.igmpublication.org Impact Factor 3.79 ISSN (e)-2347-176x Comparison of 3-Port Versus 4-Port Laproscopic Cholecystectomy- A Prospective Comparative Study Authors Shekhar Gogna 1, Priya Goyal 2,
Lecture 01 Internal surface of anterolateral abdominal wall. BY Dr Farooq Khan Aurakzai
 Lecture 01 Internal surface of anterolateral abdominal wall BY Dr Farooq Khan Aurakzai Dated: 21.12.2017 Internal surface of the anterolateral abdominal wall The internal ( posterior ) surface of the anterolateral
Lecture 01 Internal surface of anterolateral abdominal wall BY Dr Farooq Khan Aurakzai Dated: 21.12.2017 Internal surface of the anterolateral abdominal wall The internal ( posterior ) surface of the anterolateral
Management of biliary injury after laparoscopic cholecystectomy N. Dayes Kings County Hospital Center & Long Island College Hospital 8/19/2010
 Management of biliary injury after laparoscopic cholecystectomy N. Dayes Kings County Hospital Center & Long Island College Hospital 8/19/2010 Case Presentation 30 y.o. woman with 2 weeks of RUQ abdominal
Management of biliary injury after laparoscopic cholecystectomy N. Dayes Kings County Hospital Center & Long Island College Hospital 8/19/2010 Case Presentation 30 y.o. woman with 2 weeks of RUQ abdominal
Laparoscopic Cholecystectomy: Challenges faced by beginners our perspective
 Open Access Archives of Surgery and Clinical Research Research Article ISSN 2576-9537 Laparoscopic Cholecystectomy: Challenges faced by beginners our perspective Kunal Chowdhary, Gurinder Kaur, Kapil Sindhu,
Open Access Archives of Surgery and Clinical Research Research Article ISSN 2576-9537 Laparoscopic Cholecystectomy: Challenges faced by beginners our perspective Kunal Chowdhary, Gurinder Kaur, Kapil Sindhu,
Bile Duct Injury during Lap Chole. Bile Duct Injury during cholecystectomy TOPICS. 1. Prevalence, mechanisms, prevention and diagnosis
 Bile Duct Injury during cholecystectomy Catherine HUBERT Jean-Fran François GIGOT Benoît t NAVEZ Division of Hepato-Biliary Biliary-Pancreatic Surgery Department of Abdominal Surgery and Transplantation
Bile Duct Injury during cholecystectomy Catherine HUBERT Jean-Fran François GIGOT Benoît t NAVEZ Division of Hepato-Biliary Biliary-Pancreatic Surgery Department of Abdominal Surgery and Transplantation
DISCHARGE DIAGNOSES: End stage renal disease secondary to rapidly progressive glomerulonephritis.
 DISCHARGE SUMMARY DISCHARGE DIAGNOSES: End stage renal disease secondary to rapidly progressive glomerulonephritis. OPERATIONS/PROCEDURES: Living related renal transplantation. HISTORY: For full details
DISCHARGE SUMMARY DISCHARGE DIAGNOSES: End stage renal disease secondary to rapidly progressive glomerulonephritis. OPERATIONS/PROCEDURES: Living related renal transplantation. HISTORY: For full details
Endoscopic Component Separation November Philip Omotosho, MD Assistant Professor of Surgery Duke University School of Medicine
 Endoscopic Component Separation November 2014 Philip Omotosho, MD Assistant Professor of Surgery Duke University School of Medicine Abdominal Wall Anatomy External Oblique Rectus Abdominus Internal Oblique
Endoscopic Component Separation November 2014 Philip Omotosho, MD Assistant Professor of Surgery Duke University School of Medicine Abdominal Wall Anatomy External Oblique Rectus Abdominus Internal Oblique
Laparoscopic Subtotal Cholecystectomy for Difficult Acute Calculous Cholecystitis
 Journal of Surgery 2017; 5(6): 111-117 http://www.sciencepublishinggroup.com/j/js doi: 10.11648/j.js.20170506.15 ISSN: 2330-0914 (Print); ISSN: 2330-0930 (Online) Laparoscopic Subtotal Cholecystectomy
Journal of Surgery 2017; 5(6): 111-117 http://www.sciencepublishinggroup.com/j/js doi: 10.11648/j.js.20170506.15 ISSN: 2330-0914 (Print); ISSN: 2330-0930 (Online) Laparoscopic Subtotal Cholecystectomy
-12. -Renad Habahbeh. -Dr Mohammad mohtasib
 -12 -Renad Habahbeh - -Dr Mohammad mohtasib The Gallbladder -The gallbladder has a body, a fundus (a rounded end), a neck, Hartmann s pouch before the neck and a cystic duct that meets the common hepatic
-12 -Renad Habahbeh - -Dr Mohammad mohtasib The Gallbladder -The gallbladder has a body, a fundus (a rounded end), a neck, Hartmann s pouch before the neck and a cystic duct that meets the common hepatic
Biliary Anatomy in Living-related Liver Transplantation
 The 5th IHPBA Congress - Istanbul Biliary Anatomy in Living-related Liver Transplantation biliary trees hilar plate Assessment for Vascular Anatomy 1. 3DCT portal vein hepatic vein hepatic artery 2. No
The 5th IHPBA Congress - Istanbul Biliary Anatomy in Living-related Liver Transplantation biliary trees hilar plate Assessment for Vascular Anatomy 1. 3DCT portal vein hepatic vein hepatic artery 2. No
Biology Human Anatomy Abdominal and Pelvic Cavities
 Biology 351 - Human Anatomy Abdominal and Pelvic Cavities Please place your name and I.D. number on the back of the last page of this exam. You must answer all questions on this exam. Because statistics
Biology 351 - Human Anatomy Abdominal and Pelvic Cavities Please place your name and I.D. number on the back of the last page of this exam. You must answer all questions on this exam. Because statistics
Tor Chiu. Deep Inferior Epigastric Artery Perforator Flap 161
 18 Deep Inferior Epigastric Artery Perforator Flap Tor Chiu Deep Inferior Epigastric Artery Perforator Flap 161 Deep Inferior Epigastric Artery Perforator Flap FLAP TERRITORY The deep inferior epigastric
18 Deep Inferior Epigastric Artery Perforator Flap Tor Chiu Deep Inferior Epigastric Artery Perforator Flap 161 Deep Inferior Epigastric Artery Perforator Flap FLAP TERRITORY The deep inferior epigastric
Alexander C Vlantis. Total Laryngectomy 57
 07 Total Laryngectomy Alexander C Vlantis Total Laryngectomy 57 Total Laryngectomy STEP 1 INCISION AND POSITION OF STOMA A superiorly based apron flap incision is marked with the horizontal limb placed
07 Total Laryngectomy Alexander C Vlantis Total Laryngectomy 57 Total Laryngectomy STEP 1 INCISION AND POSITION OF STOMA A superiorly based apron flap incision is marked with the horizontal limb placed
Anatomy: Know Your Abdomen
 Anatomy: Know Your Abdomen Glossary Abdomen - part of the body below the thorax (chest cavity); separated by the diaphragm. Anterior - towards the front of the body. For example, the umbilicus is anterior
Anatomy: Know Your Abdomen Glossary Abdomen - part of the body below the thorax (chest cavity); separated by the diaphragm. Anterior - towards the front of the body. For example, the umbilicus is anterior
Digestive Anatomy Lab
 Digestive Anatomy Lab In-Lab Exercises I have included the word list in this document. Any descrepencies between this document and the wordlist, you should default to this document. There is a lot of repetition
Digestive Anatomy Lab In-Lab Exercises I have included the word list in this document. Any descrepencies between this document and the wordlist, you should default to this document. There is a lot of repetition
Cystotomy Laboratory Simulation
 Kelli Braun MD, Robert Stager MD, Chadburn Ray MD, Bunja Rungruang MD Medical College of Georgia at Augusta University Note: This model can be used for Open Cystotomy Repair or Laparoscopic Cystotomy Repair.
Kelli Braun MD, Robert Stager MD, Chadburn Ray MD, Bunja Rungruang MD Medical College of Georgia at Augusta University Note: This model can be used for Open Cystotomy Repair or Laparoscopic Cystotomy Repair.
This presentation will discuss the anatomy of the anterior abdominal wall as it pertains to gynaecological and obstetric surgery.
 This presentation will discuss the anatomy of the anterior abdominal wall as it pertains to gynaecological and obstetric surgery. 1 The border of the anterior abdominal wall is defined superiorly by the
This presentation will discuss the anatomy of the anterior abdominal wall as it pertains to gynaecological and obstetric surgery. 1 The border of the anterior abdominal wall is defined superiorly by the
Liver o The liver is the largest gland in the body and has a wide variety of functions. - It s an accessory organ of GIT
 بسم رلاهللا You don t need to refer to the slides, we included everything here In this lecture we will talk about Liver & Gallbladder Liver o The liver is the largest gland in the body and has a wide variety
بسم رلاهللا You don t need to refer to the slides, we included everything here In this lecture we will talk about Liver & Gallbladder Liver o The liver is the largest gland in the body and has a wide variety
4/9/2018 OBJECTIVES PANCREAOTO BILIARY ULTRASOUND: BEYOND CHOLECYSTITIS
 PANCREAOTO BILIARY ULTRASOUND: BEYOND CHOLECYSTITIS Jean Yves Sewah Kaiser Permanente West Los Angeles 1 OBJECTIVES Discuss the role of ultrasound in the evaluation of the gallbladder, biliary tree and
PANCREAOTO BILIARY ULTRASOUND: BEYOND CHOLECYSTITIS Jean Yves Sewah Kaiser Permanente West Los Angeles 1 OBJECTIVES Discuss the role of ultrasound in the evaluation of the gallbladder, biliary tree and
Done by: nisreen obeidat
 Sheet: liver and pancreas Done by: nisreen obeidat Embryology of the liver The liver develops in the ventral mesentery of the foregut and divides the ventral mesentery :into 1)lesser omentum (between the
Sheet: liver and pancreas Done by: nisreen obeidat Embryology of the liver The liver develops in the ventral mesentery of the foregut and divides the ventral mesentery :into 1)lesser omentum (between the
Umbilicus Saving Three-Port Laparoscopic Cholecystectomy
 Article ID: WMC001882 ISSN 2046-1690 Umbilicus Saving Three-Port Laparoscopic Cholecystectomy Corresponding Author: Dr. Masahiko Hirota, MD, PhD, Departments of Surgery, Kumamoto Regional Medical Center
Article ID: WMC001882 ISSN 2046-1690 Umbilicus Saving Three-Port Laparoscopic Cholecystectomy Corresponding Author: Dr. Masahiko Hirota, MD, PhD, Departments of Surgery, Kumamoto Regional Medical Center
Minimally Invasive. TEM Instrument System for Transanal Endoscopic Microsurgery
 TEM Minimally Invasive TEM Instrument System for Transanal Endoscopic Microsurgery The only complete system for transanal endoscopic microsurgery Unique autoclavable stereoscope for 3-D visualization of
TEM Minimally Invasive TEM Instrument System for Transanal Endoscopic Microsurgery The only complete system for transanal endoscopic microsurgery Unique autoclavable stereoscope for 3-D visualization of
Anatomy of the liver and pancreas
 Anatomy of the liver and pancreas Prof. Abdulameer Al-Nuaimi E-mail: a.al-nuaimi@sheffield.ac.uk abdulameerh@yahoo.com Liver Aorta Pulm. Trunk Rt. At, Duct. Art. Lt. Ven. Rt. Ven. Internal Posterior
Anatomy of the liver and pancreas Prof. Abdulameer Al-Nuaimi E-mail: a.al-nuaimi@sheffield.ac.uk abdulameerh@yahoo.com Liver Aorta Pulm. Trunk Rt. At, Duct. Art. Lt. Ven. Rt. Ven. Internal Posterior
Colorectal procedure guide
 Colorectal procedure guide Illustrations by Lisa Clark Biodesign ADVANCED TISSUE REPAIR cookmedical.com 2 INDEX Anal fistula repair Using the Biodesign plug with no button.... 4 Anal fistula repair Using
Colorectal procedure guide Illustrations by Lisa Clark Biodesign ADVANCED TISSUE REPAIR cookmedical.com 2 INDEX Anal fistula repair Using the Biodesign plug with no button.... 4 Anal fistula repair Using
The abdominal Esophagus, Stomach and the Duodenum. Prof. Oluwadiya KS
 The abdominal Esophagus, Stomach and the Duodenum Prof. Oluwadiya KS www.oluwadiya.com Viscera of the abdomen Abdominal esophagus: Terminal part of the esophagus The stomach Intestines: Small and Large
The abdominal Esophagus, Stomach and the Duodenum Prof. Oluwadiya KS www.oluwadiya.com Viscera of the abdomen Abdominal esophagus: Terminal part of the esophagus The stomach Intestines: Small and Large
Case Report. XCM Biologic Tissue Matrix. Components separation using sandwich technique for reconstruction of abdominal wall defect.
 Case Report XCM Biologic Tissue Matrix. Components separation using sandwich technique for reconstruction of abdominal wall defect. XCM Biologic Tissue Matrix. Components separation using sandwich technique
Case Report XCM Biologic Tissue Matrix. Components separation using sandwich technique for reconstruction of abdominal wall defect. XCM Biologic Tissue Matrix. Components separation using sandwich technique
Lecture 02 Anatomy of the LIVER
 Lecture 02 Anatomy of the LIVER BY Dr Farooq Khan Aurakzai Dated: 02.01.2018 Introduction to Liver Largest gland in the body. 2 nd largest organ of the body. Weight approximately 1500 gm, and is roughly
Lecture 02 Anatomy of the LIVER BY Dr Farooq Khan Aurakzai Dated: 02.01.2018 Introduction to Liver Largest gland in the body. 2 nd largest organ of the body. Weight approximately 1500 gm, and is roughly
5. COMMON APPROACHES. Each of the described approaches is also demonstrated on supplementary videos, please see Appendix 2.
 5. COMMON APPROACHES Each of the described approaches is also demonstrated on supplementary videos, please see Appendix 2. 5.1. LATERAL SUPRAORBITAL APPROACH The most common craniotomy approach used in
5. COMMON APPROACHES Each of the described approaches is also demonstrated on supplementary videos, please see Appendix 2. 5.1. LATERAL SUPRAORBITAL APPROACH The most common craniotomy approach used in
CHILD HYDROCELE OPERATION. COPYRIGHT M.H.EDWARDS 2005 FILE NAME SW-CHHY OPERATION NO 037 SURGEON... Last updated
 CHILD HYDROCELE OPERATION COPYRIGHT M.H.EDWARDS 2005 FILE NAME SW-CHHY OPERATION NO 037 SURGEON... Last updated 30 12 05 CHILD HYDROCELE OPERATION GRADE 4 (SEVERE) THESE S COVER MALE PATIENT LESS THAN
CHILD HYDROCELE OPERATION COPYRIGHT M.H.EDWARDS 2005 FILE NAME SW-CHHY OPERATION NO 037 SURGEON... Last updated 30 12 05 CHILD HYDROCELE OPERATION GRADE 4 (SEVERE) THESE S COVER MALE PATIENT LESS THAN
8 A SIMPLE FISTULA REPAIR, STEP BY STEP
 8 A SIMPLE FISTULA REPAIR, STEP BY STEP The first step is to suture the labia to the thighs and cover the anus with a swab (Figure 31). Figure 31 The labia are sutured to the thighs and the anus is covered
8 A SIMPLE FISTULA REPAIR, STEP BY STEP The first step is to suture the labia to the thighs and cover the anus with a swab (Figure 31). Figure 31 The labia are sutured to the thighs and the anus is covered
Breast conservation surgery and sentinal node biopsy: Dr R Botha Moderator: Dr E Osman
 Breast conservation surgery and sentinal node biopsy: Dr R Botha Moderator: Dr E Osman Breast anatomy: Breast conserving surgery: The aim of wide local excision is to remove all invasive and in situ
Breast conservation surgery and sentinal node biopsy: Dr R Botha Moderator: Dr E Osman Breast anatomy: Breast conserving surgery: The aim of wide local excision is to remove all invasive and in situ
RECTAL INJURY IN UROLOGIC SURGERY. Inadvertent rectal injury from a urologic procedure is often subtle but has serious postoperative consequences.
 RECTAL INJURY IN 27 UROLOGIC SURGERY Inadvertent rectal injury from a urologic procedure is often subtle but has serious postoperative consequences. With good mechanical bowel preparation plus antibiotic
RECTAL INJURY IN 27 UROLOGIC SURGERY Inadvertent rectal injury from a urologic procedure is often subtle but has serious postoperative consequences. With good mechanical bowel preparation plus antibiotic
Current Perspective of Laparoscopic Cholecystectomy for Acute Cholecystitis
 The Egyptian Journal of Hospital Medicine (July 2018) Vol. 72 (7), Page 4885-4893 Current Perspective of Laparoscopic Cholecystectomy for Acute Cholecystitis Abdelghany Mahmoud AlShamy, Karim Fahmy Abd
The Egyptian Journal of Hospital Medicine (July 2018) Vol. 72 (7), Page 4885-4893 Current Perspective of Laparoscopic Cholecystectomy for Acute Cholecystitis Abdelghany Mahmoud AlShamy, Karim Fahmy Abd
د. عصام طارق. Objectives:
 GI anatomy Lecture: 5 د. عصام طارق Objectives: To describe anatomy of stomach, duodenum & pancreas. To list their main relations. To define their blood & nerve supply. To list their lymph drainage. To
GI anatomy Lecture: 5 د. عصام طارق Objectives: To describe anatomy of stomach, duodenum & pancreas. To list their main relations. To define their blood & nerve supply. To list their lymph drainage. To
COMPLICATIONS OF LAPAROSCOPIC CHOLECYSTECTOMY AT ISRA UNIVERSITY HOSPITAL, HYDERABAD
 Original Article COMPLICATIONS OF LAPAROSCOPIC CHOLECYSTECTOMY AT ISRA UNIVERSITY HOSPITAL, HYDERABAD Waseem Memon 1, Tariq Wahab Khanzada 2, Abdul Samad 3, M. Hussain Laghari 4 ABSTRACT Objective: The
Original Article COMPLICATIONS OF LAPAROSCOPIC CHOLECYSTECTOMY AT ISRA UNIVERSITY HOSPITAL, HYDERABAD Waseem Memon 1, Tariq Wahab Khanzada 2, Abdul Samad 3, M. Hussain Laghari 4 ABSTRACT Objective: The
INGROWING TOE NAIL REQUIREMENTS A. Instruments to be autoclaved and packed B. Disposables C. Solutions PROCEDURE
 INGROWING TOE NAIL Pages with reference to book, From 21 To 23 Irfan Daudi ( Department of Surgery, Aga Khan University of Health Sciences, Stadium Road, Karachi. ) The condition of in growing toe nail
INGROWING TOE NAIL Pages with reference to book, From 21 To 23 Irfan Daudi ( Department of Surgery, Aga Khan University of Health Sciences, Stadium Road, Karachi. ) The condition of in growing toe nail
Department of Urology, Columbia University School of Medicine, New York, NY
 Laparoscopic Partial Nephrectomy Jaime Landman, MD Associate Professor of Urology Director of Minimally Invasive Urology Columbia University Department of Urology Department of Urology, Columbia University
Laparoscopic Partial Nephrectomy Jaime Landman, MD Associate Professor of Urology Director of Minimally Invasive Urology Columbia University Department of Urology Department of Urology, Columbia University
To describe the liver. To list main structures in porta hepatis.
 GI anatomy Lecture: 6 د. عصام طارق Objectives: To describe the liver. To list main structures in porta hepatis. To define portal system & portosystemic anastomosis. To list parts of biliary system. To
GI anatomy Lecture: 6 د. عصام طارق Objectives: To describe the liver. To list main structures in porta hepatis. To define portal system & portosystemic anastomosis. To list parts of biliary system. To
Cholecystitis is defined as nonspecific inflammation of the gallbladder with or without cholelithiasis. Types: calculous and acalculous.
 Cholecystitis is defined as nonspecific inflammation of the gallbladder with or without cholelithiasis. Types: calculous and acalculous. Anatomy of the gallbladder The gallbladder, a pear-shaped reservoir
Cholecystitis is defined as nonspecific inflammation of the gallbladder with or without cholelithiasis. Types: calculous and acalculous. Anatomy of the gallbladder The gallbladder, a pear-shaped reservoir
5 IN THEATRE. The anaesthetic
 5 IN THEATRE The anaesthetic Spinal anaesthesia is the preferred method for all fistula cases (Figure 5.1). Many surgeons give spinal anaesthesia themselves. Bupivacaine 0.5% in glucose (Marcain Heavy)
5 IN THEATRE The anaesthetic Spinal anaesthesia is the preferred method for all fistula cases (Figure 5.1). Many surgeons give spinal anaesthesia themselves. Bupivacaine 0.5% in glucose (Marcain Heavy)
Abdominal ultrasound:
 Abdominal ultrasound: Non-traumatic acute abdomen Wittanee Na-ChiangMai, MD Department of Radiology ChiangMai University 26/04/2017 Contents Technique of examination Normal anatomy Emergency conditions
Abdominal ultrasound: Non-traumatic acute abdomen Wittanee Na-ChiangMai, MD Department of Radiology ChiangMai University 26/04/2017 Contents Technique of examination Normal anatomy Emergency conditions
The Digestive System. Chapter 16. Introduction. Overview of Digestive System. Histological Organization. Movement and Mixing of Digestive Materials
 The Digestive System Chapter 16 Introduction Structure of the digestive system A tube that extends from mouth to anus Accessory organs are attached Functions include Ingestion Movement Digestion Absorption
The Digestive System Chapter 16 Introduction Structure of the digestive system A tube that extends from mouth to anus Accessory organs are attached Functions include Ingestion Movement Digestion Absorption
The Digestive System. Chapter 25
 The Digestive System Chapter 25 Introduction Structure of the digestive system A tube that extends from mouth to anus Accessory organs are attached Functions include Ingestion Movement Digestion Absorption
The Digestive System Chapter 25 Introduction Structure of the digestive system A tube that extends from mouth to anus Accessory organs are attached Functions include Ingestion Movement Digestion Absorption
ABDOMINAL WALL & RECTUS SHEATH
 ABDOMINAL WALL & RECTUS SHEATH Learning Objectives Describe the anatomy, innervation and functions of the muscles of the anterior, lateral and posterior abdominal walls. Discuss their functional relations
ABDOMINAL WALL & RECTUS SHEATH Learning Objectives Describe the anatomy, innervation and functions of the muscles of the anterior, lateral and posterior abdominal walls. Discuss their functional relations
The Digestive System
 The Digestive System Identify the Structure and Function. Mesentery of the Large Intestine The mesentery functions to connect the visceral organs to the abdominal wall. Identify the Structure. Nasal Cavity
The Digestive System Identify the Structure and Function. Mesentery of the Large Intestine The mesentery functions to connect the visceral organs to the abdominal wall. Identify the Structure. Nasal Cavity
Alexander C Vlantis. Selective Neck Dissection 33
 05 Modified Radical Neck Dissection Type II Alexander C Vlantis Selective Neck Dissection 33 Modified Radical Neck Dissection Type II INCISION Various incisions can be used for a neck dissection. The incision
05 Modified Radical Neck Dissection Type II Alexander C Vlantis Selective Neck Dissection 33 Modified Radical Neck Dissection Type II INCISION Various incisions can be used for a neck dissection. The incision
Bile Duct Injuries. Dr. Bennet Rajmohan, MRCS (Eng), MRCS Ed Consultant General & Laparoscopic Surgeon Apollo Speciality Hospitals Madurai, India
, MRCS Ed Consultant General & Laparoscopic Surgeon Apollo Speciality Hospitals Madurai, India") Bile Duct Injuries Dr. Bennet Rajmohan, MRCS (Eng), MRCS Ed Consultant General & Laparoscopic Surgeon Apollo Speciality Hospitals Madurai, India Introduction Bile duct injury (BDI) rare but potentially
Bile Duct Injuries Dr. Bennet Rajmohan, MRCS (Eng), MRCS Ed Consultant General & Laparoscopic Surgeon Apollo Speciality Hospitals Madurai, India Introduction Bile duct injury (BDI) rare but potentially
ADVANCED LAPAROSCOPIC PANCREAS SURGERY A HANDS-ON WORKSHOP
 ADVANCED LAPAROSCOPIC PANCREAS SURGERY A HANDS-ON WORKSHOP 3-4 November 2017 at the AMC in Amsterdam Organizing committee: Mo Abu Hilal, Professor of Surgery at Southampton University Marc Besselink, Professor
ADVANCED LAPAROSCOPIC PANCREAS SURGERY A HANDS-ON WORKSHOP 3-4 November 2017 at the AMC in Amsterdam Organizing committee: Mo Abu Hilal, Professor of Surgery at Southampton University Marc Besselink, Professor
Block 3: DISSECTION 2 CELIAC TRUNK, JEJUNUM/ILEUM, LARGE INTESTINE, DUODENUM, PANCREAS, PORTAL VEIN; MOBILIZATION OF THE LIVER
 1 Block 3: DISSECTION 2 CELIAC TRUNK, JEJUNUM/ILEUM, LARGE INTESTINE, DUODENUM, PANCREAS, PORTAL VEIN; MOBILIZATION OF THE LIVER Attempt to complete as much as you can of the dissection explained in the
1 Block 3: DISSECTION 2 CELIAC TRUNK, JEJUNUM/ILEUM, LARGE INTESTINE, DUODENUM, PANCREAS, PORTAL VEIN; MOBILIZATION OF THE LIVER Attempt to complete as much as you can of the dissection explained in the
Early vs delayed laparoscopic cholecystectomy for acute cholecystitis
 Original articles Surg Endosc (2004) 18:1323 1327 DOI:10.1007/s00464-003-9230-6 Ó Springer Science+Business Media, Inc. 2004 Early vs delayed laparoscopic cholecystectomy for acute cholecystitis A prospective
Original articles Surg Endosc (2004) 18:1323 1327 DOI:10.1007/s00464-003-9230-6 Ó Springer Science+Business Media, Inc. 2004 Early vs delayed laparoscopic cholecystectomy for acute cholecystitis A prospective
WHICH LYMPH NODES SHOULD BE
 Y.K.: 82 Y.O. WOMAN WITH ANEMIA No GI symptoms. Chronic AF taking coumadin: INR=2.1. HCT=24. Anemia persists despite Rx. Colonoscopy: tumor in ascending colon. Bx: adenocarcinoma. Rx: Laparoscopic right
Y.K.: 82 Y.O. WOMAN WITH ANEMIA No GI symptoms. Chronic AF taking coumadin: INR=2.1. HCT=24. Anemia persists despite Rx. Colonoscopy: tumor in ascending colon. Bx: adenocarcinoma. Rx: Laparoscopic right
GI anatomy Lecture: 2 د. عصام طارق
 GI anatomy Lecture: 2 د. عصام طارق Objectives: To define rectus sheath. To describe anatomy of inguinal canal. To relates types of inguinal hernia to the region. To explore spermatic cord. Rectus Abdominis
GI anatomy Lecture: 2 د. عصام طارق Objectives: To define rectus sheath. To describe anatomy of inguinal canal. To relates types of inguinal hernia to the region. To explore spermatic cord. Rectus Abdominis
Modified Radical Mastectomy
 Modified Radical Mastectomy Valerie L. Staradub, MD, and Monica Morrow, MD S urgical management options for breast cancer include modified radical mastectomy (MRM), MRM with immediate reconstruction, and
Modified Radical Mastectomy Valerie L. Staradub, MD, and Monica Morrow, MD S urgical management options for breast cancer include modified radical mastectomy (MRM), MRM with immediate reconstruction, and
Common Bile Duct Injury: Recognition and Management
 Common Bile Duct Injury: Recognition and Management Jaime A Pineda, MD Division of Transplantation Department of Surgery University of Vermont Medical Center No disclosure Is This Going to Happen to Me
Common Bile Duct Injury: Recognition and Management Jaime A Pineda, MD Division of Transplantation Department of Surgery University of Vermont Medical Center No disclosure Is This Going to Happen to Me
The Whipple Operation Illustrations
 The Whipple Operation Illustrations Fig. 1. Illustration of the sixstep pancreaticoduodenectomy (Whipple operation) as described in a number of recent text books by Dr. Evans. The operation is divided
The Whipple Operation Illustrations Fig. 1. Illustration of the sixstep pancreaticoduodenectomy (Whipple operation) as described in a number of recent text books by Dr. Evans. The operation is divided
BY DR NOMAN ULLAH WAZIR
 BY DR NOMAN ULLAH WAZIR The stomach (from ancient Greek word stomachos, stoma means mouth) is a muscular, hollow and the most dilated part of the GIT. It starts from the point where esophagus ends. It
BY DR NOMAN ULLAH WAZIR The stomach (from ancient Greek word stomachos, stoma means mouth) is a muscular, hollow and the most dilated part of the GIT. It starts from the point where esophagus ends. It
Anatomy of the Large Intestine
 Large intestine Anatomy of the Large Intestine 2 Large Intestine Extends from ileocecal valve to anus Length = 1.5-2.5m = 5 feet Regions Cecum = 2.5-3 inch Appendix= 3-5 inch Colon Ascending= 5 inch Transverse=
Large intestine Anatomy of the Large Intestine 2 Large Intestine Extends from ileocecal valve to anus Length = 1.5-2.5m = 5 feet Regions Cecum = 2.5-3 inch Appendix= 3-5 inch Colon Ascending= 5 inch Transverse=
THE ORAL CAVITY
 THE ORAL CAVITY WALL OF ABDOMEN (ANTERIOR) The paraumbilical vein drains into the portal vein and then through the liver. This is an important clinical connection. THE ABDOMINAL VISCERA The small
THE ORAL CAVITY WALL OF ABDOMEN (ANTERIOR) The paraumbilical vein drains into the portal vein and then through the liver. This is an important clinical connection. THE ABDOMINAL VISCERA The small
ABDOMINAL WALL HAEMATOMA COMPLICATING LAPAROSCOPIC CHOLECYSTECTOMY
 HPB Surgery, 1994, Vol. 7, pp. 291-296 Reprints available directly from the publisher Photocopying permitted by license only (C) 1994 Harwood Academic Publishers GmbH Printed in the United States of America
HPB Surgery, 1994, Vol. 7, pp. 291-296 Reprints available directly from the publisher Photocopying permitted by license only (C) 1994 Harwood Academic Publishers GmbH Printed in the United States of America
Gross Anatomy ABDOMEN/SESSION 1 Dr. Firas M. Ghazi
 Anterior Abdominal Wall Structure, muscles and surface anatomy Curricular Objectives By the end of this session students are expected to: Practical 1. Identify the hip and distinguish the three bones forming
Anterior Abdominal Wall Structure, muscles and surface anatomy Curricular Objectives By the end of this session students are expected to: Practical 1. Identify the hip and distinguish the three bones forming
The Digestive System Laboratory
 The Digestive System Laboratory 1 The Digestive Tract The alimentary canal is a continuous tube stretching from the mouth to the anus. Liver Gallbladder Small intestine Anus Parotid, sublingual, and submaxillary
The Digestive System Laboratory 1 The Digestive Tract The alimentary canal is a continuous tube stretching from the mouth to the anus. Liver Gallbladder Small intestine Anus Parotid, sublingual, and submaxillary
Biliary Ultrasonography Kathleen O Brien MD MPH RDMS Kaiser Permanente South Sacramento
 Biliary Ultrasonography Kathleen O Brien MD MPH RDMS Kaiser Permanente South Sacramento https://www.google.com/search?sa=g&hl=en&q=public+disclosure&tbm=isch&tbs=simg:caqsigeahwelekju2aqaaawlelcmpwgaygpgcamskpib_1qnza7ai
Biliary Ultrasonography Kathleen O Brien MD MPH RDMS Kaiser Permanente South Sacramento https://www.google.com/search?sa=g&hl=en&q=public+disclosure&tbm=isch&tbs=simg:caqsigeahwelekju2aqaaawlelcmpwgaygpgcamskpib_1qnza7ai
LECTURE 5. Anatomy of the heart
 LECTURE 5. Anatomy of the heart Main components of the CVS: Heart Blood circulatory system arterial compartment haemomicrocirculatory (=microvascular) compartment venous compartment Lymphatic circulatory
LECTURE 5. Anatomy of the heart Main components of the CVS: Heart Blood circulatory system arterial compartment haemomicrocirculatory (=microvascular) compartment venous compartment Lymphatic circulatory
Robotic Surgery for Upper Tract Urothelial Carcinoma. Li-Ming Su, MD
 Robotic Surgery for Upper Tract Urothelial Carcinoma Li-Ming Su, MD David A. Cofrin Professor of Urology, Associate Chairman of Clinical Affairs, Chief, Division of Robotic and Minimally Invasive Urologic
Robotic Surgery for Upper Tract Urothelial Carcinoma Li-Ming Su, MD David A. Cofrin Professor of Urology, Associate Chairman of Clinical Affairs, Chief, Division of Robotic and Minimally Invasive Urologic
Urinary System Laboratory
 Urinary System Laboratory 1 Adrenal gland Organs of The Urinary System Renal artery and vein Kidney Ureter Urinary bladder Figure 26.1 2 Urethra Functions of the urinary system organs: Urethra expels urine
Urinary System Laboratory 1 Adrenal gland Organs of The Urinary System Renal artery and vein Kidney Ureter Urinary bladder Figure 26.1 2 Urethra Functions of the urinary system organs: Urethra expels urine
Laparoscopic Cholecystectomy in Acute Cholecystitis :An Experience with 100 cases
 ORIGINALARTICLE Laparoscopic Cholecystectomy in Acute Cholecystitis :An Experience with 100 cases Rajni Bhardwaj, M.R.Attri, Shahnawaz Ahangar Abstract This study was undertaken to evaluate our experience
ORIGINALARTICLE Laparoscopic Cholecystectomy in Acute Cholecystitis :An Experience with 100 cases Rajni Bhardwaj, M.R.Attri, Shahnawaz Ahangar Abstract This study was undertaken to evaluate our experience
Table of Contents: CARPAL TUNNEL RELEASE SURGICAL TECHNIQUE Knife Assembly... Page 6 VERSION 2.2
 www.s2ssurgical.com Table of Contents: Preparation... Page 1 Dissection... Page 2 Tunneling... Page 3 Release... Page 4 Closure... Page 6 Knife Assembly... Page 6 CARPAL TUNNEL RELEASE SURGICAL TECHNIQUE
www.s2ssurgical.com Table of Contents: Preparation... Page 1 Dissection... Page 2 Tunneling... Page 3 Release... Page 4 Closure... Page 6 Knife Assembly... Page 6 CARPAL TUNNEL RELEASE SURGICAL TECHNIQUE
The peritoneum. Prof. Oluwadiya KS, MBBS, FMCS(Orthop) Website:
 Website:") The peritoneum Prof. Oluwadiya KS, MBBS, FMCS(Orthop) Website: http://oluwadiya.com The peritoneum Serous membrane that lines the abdominopelvic cavity and invests the viscera The largest serous membrane
The peritoneum Prof. Oluwadiya KS, MBBS, FMCS(Orthop) Website: http://oluwadiya.com The peritoneum Serous membrane that lines the abdominopelvic cavity and invests the viscera The largest serous membrane
Jhia Anjela D. Rivera 1 1. BS Biology, Department of Biology, College of Science, Polytechnic University of the Philippines
 DIGESTIVE SYSTEM Jhia Anjela D. Rivera 1 1 BS Biology, Department of Biology, College of Science, Polytechnic University of the Philippines DIGESTIVE SYSTEM Consists of the digestive tract (gastrointestinal
DIGESTIVE SYSTEM Jhia Anjela D. Rivera 1 1 BS Biology, Department of Biology, College of Science, Polytechnic University of the Philippines DIGESTIVE SYSTEM Consists of the digestive tract (gastrointestinal
Common Bile Duct (CBD)
") Liver Last time we talked about the liver and the doctor started by revising some information about it: It has five surfaces. It reaches the 5 th intercostal space ; some books write that it reaches the
Liver Last time we talked about the liver and the doctor started by revising some information about it: It has five surfaces. It reaches the 5 th intercostal space ; some books write that it reaches the
The Digestive System and Body Metabolism
 14 PART B The Digestive System and Body Metabolism PowerPoint Lecture Slide Presentation by Jerry L. Cook, Sam Houston University ESSENTIALS OF HUMAN ANATOMY & PHYSIOLOGY EIGHTH EDITION ELAINE N. MARIEB
14 PART B The Digestive System and Body Metabolism PowerPoint Lecture Slide Presentation by Jerry L. Cook, Sam Houston University ESSENTIALS OF HUMAN ANATOMY & PHYSIOLOGY EIGHTH EDITION ELAINE N. MARIEB
Ventral Hernia Repair
 Ventral Hernia Repair Ventrio ST Hernia Patch Ventrio Hernia Patch Technique Guide Open and Laparoscopic Ventral Hernia Repair SOFT TISSUE REPAIR Right Procedure. Right Product. Right Outcome. This Technique
Ventral Hernia Repair Ventrio ST Hernia Patch Ventrio Hernia Patch Technique Guide Open and Laparoscopic Ventral Hernia Repair SOFT TISSUE REPAIR Right Procedure. Right Product. Right Outcome. This Technique
Needlescopic cholecystectomy: prospective study of 150 patients
 ORIGINAL ARTICLE ECS Lai M Fok ASH Chan Needlescopic cholecystectomy: prospective study of patients!"#$%&'()*+,-./3467 Objective. To evaluate the feasibility and safety of cholecystectomy using miniaturised
ORIGINAL ARTICLE ECS Lai M Fok ASH Chan Needlescopic cholecystectomy: prospective study of patients!"#$%&'()*+,-./3467 Objective. To evaluate the feasibility and safety of cholecystectomy using miniaturised
Chapter 2. Simple Nephrectomy. Please Give Three Tips for Laparoscopic Simple Nephrectomy. Dr. de la Rosette
 Chapter 2 Simple Nephrectomy Please Give Three Tips for Laparoscopic Simple Nephrectomy............. 39 How Does One Find the Renal Hilum during Transperitoneal Laparoscopic Nephrectomy?.................
Chapter 2 Simple Nephrectomy Please Give Three Tips for Laparoscopic Simple Nephrectomy............. 39 How Does One Find the Renal Hilum during Transperitoneal Laparoscopic Nephrectomy?.................
Manual on Preparation of Tissue for Neonatal Skills Course. Version 1.0_2018. Prepared by: Haitham Dagash. MBBS, FRCSEd (Paed)
") Manual on Preparation of Tissue for Neonatal Skills Course Version 1.0_2018 Prepared by: Haitham Dagash MBBS, FRCSEd (Paed) University of Leicester and Leicester Infirmary Hospital Prof.Kokila Lakhoo PhD,FRCS(ENG+EDIN),FCS(SA),FCS(SA:PAED),MRCPCH,MBCHB
Manual on Preparation of Tissue for Neonatal Skills Course Version 1.0_2018 Prepared by: Haitham Dagash MBBS, FRCSEd (Paed) University of Leicester and Leicester Infirmary Hospital Prof.Kokila Lakhoo PhD,FRCS(ENG+EDIN),FCS(SA),FCS(SA:PAED),MRCPCH,MBCHB
Laboratory exercises for abdominal organs
 Laboratory exercises for abdominal organs Slide #77 (C007- H- 107A). Pancreas, dog. pancreatic islets CENTROACINAR CELLS ARE THE BEGINNING CELLS OF THE INTERCALATED DUCTS THAT DRAIN THE SECRETORY ACINI
Laboratory exercises for abdominal organs Slide #77 (C007- H- 107A). Pancreas, dog. pancreatic islets CENTROACINAR CELLS ARE THE BEGINNING CELLS OF THE INTERCALATED DUCTS THAT DRAIN THE SECRETORY ACINI
Urinary Bladder. Prof. Imran Qureshi
 Urinary Bladder Prof. Imran Qureshi Urinary Bladder It develops from the upper end of the urogenital sinus, which is continuous with the allantois. The allantois degenerates and forms a fibrous cord in
Urinary Bladder Prof. Imran Qureshi Urinary Bladder It develops from the upper end of the urogenital sinus, which is continuous with the allantois. The allantois degenerates and forms a fibrous cord in
Small Plicae Circularis. Short Closely packed together. Sparse, completely absent at distal part Lymphoid Nodule
 Intestines Differences Between Jejunum and Ileum Types Jejunum Ileum Color Deeper red Paler pink Calibre Bigger Smaller Thickness of wall Thick and Heavy Thin and Lighter Vascularity Highly vascularised
Intestines Differences Between Jejunum and Ileum Types Jejunum Ileum Color Deeper red Paler pink Calibre Bigger Smaller Thickness of wall Thick and Heavy Thin and Lighter Vascularity Highly vascularised
Exploring Anatomy: the Human Abdomen
 Exploring Anatomy: the Human Abdomen PERITONEUM AND PERITONEAL CAVITY PERITONEUM The peritoneum is a thin serous membrane that lines the abdominal cavity and covers, in variable amounts, the viscera within
Exploring Anatomy: the Human Abdomen PERITONEUM AND PERITONEAL CAVITY PERITONEUM The peritoneum is a thin serous membrane that lines the abdominal cavity and covers, in variable amounts, the viscera within
ANTERIOR CERVICAL TRIANGLE (Fig. 2.1 )
") 2 Neck Anatomy ANTERIOR CERVICAL TRIANGLE (Fig. 2.1 ) The boundaries are: Lateral: sternocleidomastoid muscle Superior: inferior border of the mandible Medial: anterior midline of the neck This large triangle
2 Neck Anatomy ANTERIOR CERVICAL TRIANGLE (Fig. 2.1 ) The boundaries are: Lateral: sternocleidomastoid muscle Superior: inferior border of the mandible Medial: anterior midline of the neck This large triangle
ISSN X (Print) Research Article. *Corresponding author Jitendra Singh Yadav
 Research Article. *Corresponding author Jitendra Singh Yadav") Scholars Journal of Applied Medical Sciences (SJAMS) Sch. J. App. Med. Sci., 2014; 2(3B):966-970 Scholars Academic and Scientific Publisher (An International Publisher for Academic and Scientific Resources)
Scholars Journal of Applied Medical Sciences (SJAMS) Sch. J. App. Med. Sci., 2014; 2(3B):966-970 Scholars Academic and Scientific Publisher (An International Publisher for Academic and Scientific Resources)
Surgical anatomy of the biliary tract
 HPB, 2008; 10: 7276 REVIEW ARTICLE Surgical anatomy of the biliary tract DENIS CASTAING Centre hépato-biliaire, Hôpital Paul Brousse, Assistance Publique- Hôpitaux de Paris, Université Paris XI, Paris,
HPB, 2008; 10: 7276 REVIEW ARTICLE Surgical anatomy of the biliary tract DENIS CASTAING Centre hépato-biliaire, Hôpital Paul Brousse, Assistance Publique- Hôpitaux de Paris, Université Paris XI, Paris,
ABDOMEN - GI. Duodenum
 TALA SALEH ABDOMEN - GI Duodenum - Notice the shape of the duodenum, it looks like capital G shape tube which extends from the pyloroduodenal junction to the duodenojejunal junction. - It is 10 inches
TALA SALEH ABDOMEN - GI Duodenum - Notice the shape of the duodenum, it looks like capital G shape tube which extends from the pyloroduodenal junction to the duodenojejunal junction. - It is 10 inches
EndoRelease ENDOSCOPIC CUBITAL TUNNEL RELEASE SYSTEM
 EndoRelease ENDOSCOPIC CUBITAL TUNNEL RELEASE SYSTEM SURGICAL TECHNIQUE Up p e r Ex t r e m i t y So l u t i o n s ENDOSCOPIC CUBITAL TUNNEL RELEASE SYSTEM Description: The EndoRelease Endoscopic Cubital
EndoRelease ENDOSCOPIC CUBITAL TUNNEL RELEASE SYSTEM SURGICAL TECHNIQUE Up p e r Ex t r e m i t y So l u t i o n s ENDOSCOPIC CUBITAL TUNNEL RELEASE SYSTEM Description: The EndoRelease Endoscopic Cubital
Peritoneal Dialysis Catheter Placement. Peritoneal Dialysis Catheter Placement. Peritoneal Dialysis Catheter Placement
 ASDIN Advanced Techniques Pre-course Feb. 24, 2012 New Orleans, La Randall L. Rasmussen, MD Special thank you to Drs. Rajeev Narayan, San Antonio, Tx and Hemant Dhingra, Fresno Ca for lending me slides
ASDIN Advanced Techniques Pre-course Feb. 24, 2012 New Orleans, La Randall L. Rasmussen, MD Special thank you to Drs. Rajeev Narayan, San Antonio, Tx and Hemant Dhingra, Fresno Ca for lending me slides
7/11/17. The Surgeon s Operative Report: Tools and Tips to Enhance Abstraction. Stopwoundinfection.com. Impact to Healthcare
 1. Scott, R. Douglas. The Direct Medical Costs of Healthcare-Associated Infections in U.S. Hospitals and the Benefits of Prevention. March 2009. http://www.cdc.gov/hai/pdfs/hai/scott_costpaper.pdf. 2.
1. Scott, R. Douglas. The Direct Medical Costs of Healthcare-Associated Infections in U.S. Hospitals and the Benefits of Prevention. March 2009. http://www.cdc.gov/hai/pdfs/hai/scott_costpaper.pdf. 2.
CHEST DRAIN PROTOCOL
 CHEST DRAIN PROTOCOL Rationale The pleural membranes have an important role in effective lung expansion. The visceral pleura is a thin, smooth, serous membrane covering the surface of the lungs and is
CHEST DRAIN PROTOCOL Rationale The pleural membranes have an important role in effective lung expansion. The visceral pleura is a thin, smooth, serous membrane covering the surface of the lungs and is
Laparoscopic total mesorectal excision (TME) with electric hook for rectal cancer
 with electric hook for rectal cancer") Technical Note Page 1 of 8 Laparoscopic total mesorectal excision (TME) with electric hook for rectal cancer Gong Chen, Rong-Xin Zhang, Zhi-Tao Xiao Department of Colorectal Surgery, Sun Yat-sen University
Technical Note Page 1 of 8 Laparoscopic total mesorectal excision (TME) with electric hook for rectal cancer Gong Chen, Rong-Xin Zhang, Zhi-Tao Xiao Department of Colorectal Surgery, Sun Yat-sen University