Timing of Surgery for Cervical Spine Anomalies
|
|
|
- Lora Phelps
- 5 years ago
- Views:
Transcription

1 Timing of Surgery for Cervical Spine Anomalies Ilkka Helenius, MD, PhD Professor and Chairman Department of Pediatric Orthopedic Surgery University of Turku and Turku University Hospital, Finland
2 Disclosures IH: Consultant and Grants to Institution from Medtronic
3 Pathology of Cervical Spine Instability Occipitocervical (Down) Atlantoaxial (Os odontoideum) Subaxial (Klippel-Feil, Diastrophic dysplasia, Larsen syndrome) Deformity Cervical kyphosis (Congenital, Neurofibromatosis) Spinal stenosis Achondroplasia
 Instability (Down, 22q11.")
4 Cervical Spine Instability Occipitocervical instability (C0/C1) Basilar invagination: Tip of dens above level of foramen magnum (McRae line) (Chamberlain WE. Yale J Biol Med 1939;11:487-96) Instability (Down, 22q11.2 Deletion syndrome): >1 mm of translation at the occipitoatlantal articulation (measured from the anterior surface of the occipital condyles to the posterior surface of the anterior arch of the atlas) (Wiesel SW. Spine 1979;4: ) Atlantoaxial instability (C1/C2) Atlantoaxial distance 5 mm (Locke GR, AJR 1966;97:135-40) Space available for cord (SAC) < 13mm (Spierings and Braakman, JBJS Br 1982;64-B:422-8) Os odontoideum, skeletal dysplasias such as spondyloepiphyseal dysplasia Subaxial instability Vertebral bodyhypoplasia (congenital, diastrophic dysplasia) Klippel-Feil with block vertebrae Vertebral dysplasia and erosion (Neurofibromatosis) Postlaminectomy (without instrumentation)
 Protocol in children skeletal dysplasia General anaesthesia or sedation.")
5 Flexion-Extension MR images Bony landmarks often difficult skeletal dysplasia Flexion-extension MR images diagnostic and safe (MacKenzie et al. JPO 2013) Protocol in children skeletal dysplasia General anaesthesia or sedation. Radiologist and anesthesiologist available T1+T2 sagittal, axial in neutral position (external auditory meatus at the level of shoulders) If no cord compression / airway considerations continue with dynamic MRI Flexion: Padding under occiput Padding under shoulders Findings Space available for cord, critical value less than 13 mm Cord encroachment, signal changes Soft tissue mass not shown in plain filmas or CT scan (Morquio) (Dede et al. JBJS 2013)

 Occipitocervical fusion before the age of 2 years (Hale et al.")

6 C Spine Instrumentation before 2 yrs 1.7-yr-old with NF1 Courtesy of Dr. Firoz Miyangi Cervical kyphosis in NF1 (Helenius I et al. JBJS 2016) Anatomic dimensions on CT more important than age (Lastikka et al. JCO 2017, in press) Occipitocervical fusion before the age of 2 years (Hale et al. Child Nerv Syst 2017;33: ) 10 infants with traumatic C0/C1 instability or C2 fx 10 infants with congenital instability (3 with Down sdr, 3 with skeletal dysplasia, 4 with congenital anomaly Complications: transversal sinus injury (1), worsening neurology (2), all fused C1 lateral mass, C2 pedicle or translaminar screws can often be used; strut graft useful (rib, iliac)

7 Osteotomy classification of Cervical Spine Ames CP et al. J Neurosurg Spine 2013;19:

8 Hemivertebra Resection (C Spine) Hemivertebra Resection in the Cervical Spine. Ruf M et al. Spine. 30(4): , February 15, Traditional treatment for C spine hemi: Posterior in situ with/o instrumentation (Hensinger RN. Clin Orthop 1991) 1st description of cervical hemi resection by Deburge and Briard JBJS 1981 (C7, four staged surgery) Above C7 (in the vertebral artery area) described by Harms and Ruf (Spine 2005) Combined posteroanterior or posteroanteroposterior approach Three children, one developed C5 nerve palsy Harms and Ruf advocated early hemi resection to prevent compensatory curves Indications Head tilt, prevention of compensatory curves if fully segmented hemi

9 Technical aspects of Hemivertebra Resection Hemivertebra Resection in the Cervical Spine. Ruf M et al. Spine. 30(4): , February 15, Posterior exposure Hemilamina excision with facet joint above and below Nerve root exposure, divisions of nerve root vertebral artery connections Resection of posterior wall for transverse foramen Anterior exposure Disc above and below excised Hemicorpus resected piecemiel Transverse process resected with anterior wall of transverse foramen and exposure of vertebral artery Anterior closure of resection with plate, if necessary posterior instrumentation with C2 pedicle and lateral mass screw
 Natural course of a cervical congenital scoliosis in a boy with hemivertebrae C3a and C7a at the left side.")
10 Timing and Effects of C Spine Deformity Harms and Ruf advocated early hemi resection to prevent compensatory curves, age ranged 4.4 to 14.9 in three patients (Spine 2005). Anatomic dimensions need to be satisfactory for implant placement (Lastikka et al. JCO 2017) Natural course of a cervical congenital scoliosis in a boy with hemivertebrae C3a and C7a at the left side. At the age of 2 years, the thoracic spine was completely straight (A). At the age of 14 years, there was a compensatory, now structural curve of 79[degrees] at the thoracic spine (B). Ruf et al. Spine

")


11 Craniocervical Junction Hemi Described on adult patient (Ruf et al. Spine 2015) Visualization of basilar & vertebral arteries preoperatively Transoral resection + posterior compression 5

 58% scoliosis correction with hemivertebrectomy Neck tilt: 20 11 One")
12 Cervicothoracic Juntion Hemivertebra Present with head tilt, shoulder imbalance Typically outside vertebral artery area Recent case series of 18 children (aged 5.5 to 15.2 yrs) with hemis between C7 and T4 (Chen et al. Spine 2017, Jul 11, epub) 58% scoliosis correction with hemivertebrectomy Neck tilt: One Horner sdr, one radicular pain 20% pedicle screw malposition risk 5




13 Klippel-Feil Instability Instability presents typically at adult age Contact sports denied Single level ACIF vs. posterior based instrumentation 5





14 Correction of Congenital Kyphosis >10yrs When neuro st + MR ok Postponing until rigid a+p fixation reliable is an option 5
15 Chondrodysplasia punctata 5-yr-old boy Mid-cervical kyphosis and stenosis Associated myelopathy Custom-made collar since 1-yr-old Neurosurgical plan: Anterior decompression via C4 corpectomy and plate with postop Halo immobilization
16 Immediate Postoperative MRI Anterior corpectomy + biodegradable plate No suitable halo body jacket available Fixation failed and resulted into full tetraplegia + respiratory arrest (T2 sag MRI)
17 Posterior Decompression & C0-T2 Instr Regained standing and eating but remains tetraparetic


18 Posterior decompression and C0-T4 fix Non-union at 1.5 years postop, no anterior column support? Combined approach revision with anterior support

19 At 4-yr Follow-Up Union N. Pakkasjärvi; M. Mattila; V. Remes; I. Helenius; Scandinavian Journal of Surgery 2013;102:
 Anterior and posterior elements may become detached (Katz et al. JPO 2005) Guidelines missing for treatment Combined approach preferred (Madera et al.")
20 Larsen s syndrome Connective tissue disorder Congenital joint dislocations Progressive cervical kyphosis and risk of neuro deficit with minor trauma (Johnston et al. JBJS 1996) Anterior and posterior elements may become detached (Katz et al. JPO 2005) Guidelines missing for treatment Combined approach preferred (Madera et al. J Neurosurg Ped 2008)


21 Case from Literature Madera M et al. J Neurosurg Ped 2008 Apr;1:320-4
 Close follow-up 4 mths Custom made collar 4-6kk-> >60 º AP fusion Fiberoscopic intubation for all")
22 Spontaneous Correction in Diastrophic Dysplasia Kyphosis <60º resolving (Remes et al., Spine 1999) Close follow-up 4 mths Custom made collar 4-6kk-> >60 º AP fusion Fiberoscopic intubation for all procedures (tracheomalacia) 1-yr-old 4-yr-old


 Cervical kyphosis")


23 Implications in Early onset scoliosis treatment 1 v 3 v Traction EOS typically highly progressive in Diastrophic Dysplasia (Remes et al. Spine 2002) Cervical kyphosis prevents Glisson traction during casting of scoliosis Use underarm traction instead. Cervical kyphosis resolves by continued growth if less than 60 deg (Remes et al. Spine 1999)

 Atlantoaxial distance (AAD) 5 mm (Locke GR, AJR")
24 Os Odontoideum Os odontoideum Bone (os), tooth (odontoideum), latin (Giacomini, Gior R Acad Med Torino 1886) Lack of continuity between the odontoid process and the body of C2 (axis) An independent ossicle with smooth cortical margins separated from a shorthened axis Ossiculum terminale=non-union of secondary ossification center, not associated with C1/C2 instability Clinical Presentation Asymptomatic Neurologic deficits: Brainstem or spinal cord compression Two main anatomical types Orthotopic: Ossicle associated with C1 anterior arch Dystopic: Ossicle migrated towards clivus, functionally fused to the basion Idiopathic and associated with syndromes Down syndrome, skeletal dysplasia Atlantoaxial instability (C1/C2) Atlantoaxial distance (AAD) 5 mm (Locke GR, AJR 1966;97:135-40) Anterior, posterior or combined Measured betweenposterior border of anterior arch (C1) vs. Posterior border of body of axis Os odontoideum with C1/C2 instability Ossiculum terminale

25 Radiographic findings Lack of continuity between the odontoid process and the body of C2 (axis) An independent ossicle with smooth cortical margins separated from a shorthened axis Enlarged anterior arch of C1 Jigsaw sign = articulation between anterior arch and the os Two main anatomical types (Fielding et al. JBJS 1980) Orthotopic: Ossicle associated with C1 anterior arch Dystopic: Ossicle fused to the basion Atlantoaxial instability (C1/C2) Atlantoaxial distance (AAD) 5 mm (Locke GR, AJR 1966;97:135-40) Space available for cord (SAC) <13mm Canal encroachment Bony Reactive synovitis Orthotopic Dystopic Reactive synovitis causing compression
26 Etiology Embryology 4th occipital sclerotome (proatlas) apical cap of dens and apical ligament 1st spinal sclerotome (C1) rest of dens 2nd spinal sclerotome (C2) axis body & arches Congenital Fusion failure between the dens and body of atlas Traumatic History of trauma common in os odontoideum Etiology varies (Sankar et al. Spine 2006) Atlantoaxial instability (C1/C2) Atlantoaxial distance (AAD) 5 mm (Locke GR, AJR 1966;97:135-40) Space available for cord (SAC) <13mm Canal encroachment Bony Reactive synovitis Arvin et al. Neurosurgery 2010
27 Conservative treatment 20 patients treated conservatively (Spierings and Braakman JBJS Br 1982) 15 patients without neurologic deficits, FU 6.5 years, none developed neurologic deficits 4 patients with transient cord signs, no deterioration Minor trauma associated with Sudden death (Michaels et al JBJS 1969; Dempster et al. Am J Forensic Med 1990) Quadriplegia, serious neurologic deficits, worsening of neurology (Clements et al. Injury 1995; Choi et al Ped Radiology 2005; Klimo et al JNS 2008) Spinal cord atrophy (Fielding et al. JBJS 1980) Cerebellar infarction (Sasaki et al. Spine 2000) Minimum requirements for conservative treatment Normal cord morphology Minimum SAC >13 mm 10% risk of myelopathy with SAC<13mm (Spiering and Braakman JBJS Br 1982) Conservative treatment includes Stable, yearly flexion-extension radiographs MR images every 5 years to prevent signal changes No contact sports Requires further investigations!


28 Preoperative considerations C1/C2 instability AAD>4 mm, SAC<13mm 10% risk of myelopathy with SAC<13mm (Fieding JBJS Br 1982) C1-C2 vs. C0-C2 spinal fusion Down patients with dysplastic C0/C1 joints? Preoperative imaging MR angiography: Vertebral arteries CT: Bifid C1 posterior elements Use of intraoperative navigation Preoperative traction (Hedequist et al. 2016) Fixation points Occiput C1 posterior elements, lateral mass C2 posterior elements, pedicle Transarticular screws Dysplastic C0/C1 joints Effect of preop traction on alignment (El-Barr et al. J Neurosurg Ped 2016)



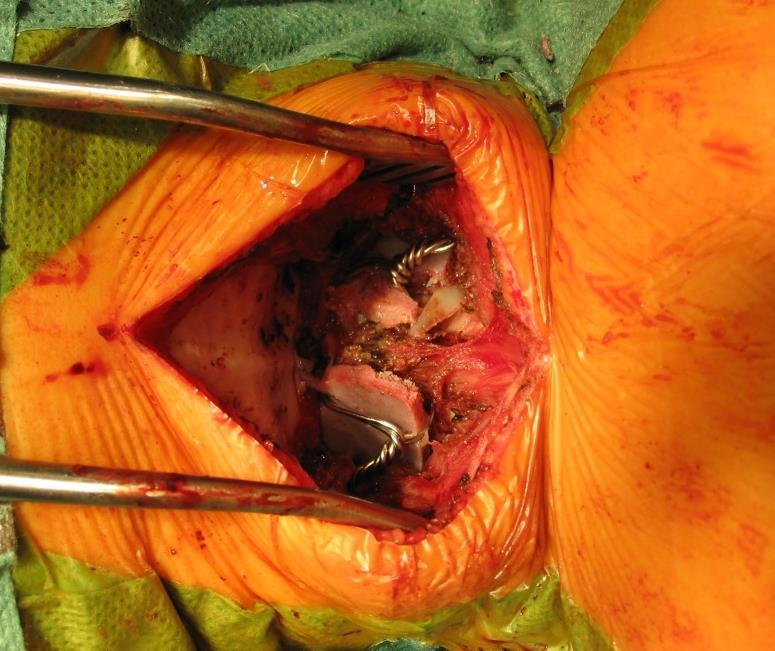
29 Brooks-Jenkins wiring Spondyloepiphyseal dysplasia 4-yr-old girl Odontoid hypoplasia AAD 8mm or SAC 9mm


")


30 Harms technique (C1 lateral mass, C2 pedicle)
 14 non-rigid (mostly wiring), 14 rigid (Harms or hooks) Risk of non-union higher in non-rigid 6/14 vs. 0/14 (p=0.")
31 Rigid fixation improves fusion rates 28 children with skeletal dysplasia and C1/C2 instability (Helenius ym. JBJS 2015) 14 non-rigid (mostly wiring), 14 rigid (Harms or hooks) Risk of non-union higher in non-rigid 6/14 vs. 0/14 (p=0.0057) Two vertebral artery lesions with attempted C2 pedicle screw placement

 C2 free hand Intraoperative O-arm to confirm reduction, implant placement Avoid C0/C1 fusion Halo body")
32 Author s current practice Preoperative evaluation MR: signal changes, cord morphology, anatomy of arteries (dominant vertebral artery?) Intraoperative traction Halo kg traction Harms technique C1 navigated + exposure of lateral mass (C2 sacrifice) C2 free hand Intraoperative O-arm to confirm reduction, implant placement Avoid C0/C1 fusion Halo body jacket 2-3 months Custom made collar 3 months Contact sports not allowed 5-yr-old girl, head tilt, neck pain

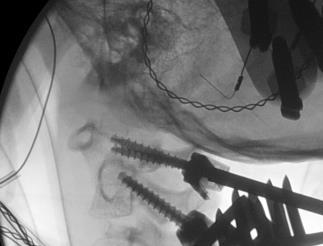
33 Intraoperative traction Make sure cervical alignment is acceptable with fluoroscopy


34 Implant placement




35 Intraoperative O-arm Implant placement Space available for cord Alignment of os odontoideum of axis, avoid over/undercorrection

36 Conclusions Early surgery may prevent compensatory curves Anatomical dimensions need to be evaluated preoperatively If neurological status OK, postpone surgery until school age to allow stable, segmental, rigid fixation Ongoing study on Os Odontoideum by the Pediatric Cervical Spine Study Group Idiopathic vs. non-idiopathic children Conservative treatment Operative treatment Contact or
May have excessive movement in the unfused segment to compensate. Flexion extension better preserved than lateral bend or rotation
 IV CONGENITAL SPINE KLIPPEL FLAIL SYNDROME Prevalence 0.60% Mainly around upper 3 vertebrae [75%] Commonest: C2 3 Lower Cervical spine fusion may be associated with syndromes: Fetal alcohol syndrome Goldenhar
IV CONGENITAL SPINE KLIPPEL FLAIL SYNDROME Prevalence 0.60% Mainly around upper 3 vertebrae [75%] Commonest: C2 3 Lower Cervical spine fusion may be associated with syndromes: Fetal alcohol syndrome Goldenhar
Common fracture & dislocation of the cervical spine. Theerachai Apivatthakakul Department of Orthopaedic Chiangmai University
 Common fracture & dislocation of the cervical spine Theerachai Apivatthakakul Department of Orthopaedic Chiangmai University Objective Anatomy Mechanism and type of injury PE.and radiographic evaluation
Common fracture & dislocation of the cervical spine Theerachai Apivatthakakul Department of Orthopaedic Chiangmai University Objective Anatomy Mechanism and type of injury PE.and radiographic evaluation
Cervical Spine Disorder in Children
 Cervical Spine Disorder in Children Embryology of Vertebra Para axial Mesoderm 42~44, 42~44 somite 4 occipital somite 8 cervical somite 12 thoracic somite 5 lumbar somite 10 sacral somite 5 coccyx somite
Cervical Spine Disorder in Children Embryology of Vertebra Para axial Mesoderm 42~44, 42~44 somite 4 occipital somite 8 cervical somite 12 thoracic somite 5 lumbar somite 10 sacral somite 5 coccyx somite
Subaxial Cervical Spine Trauma
 Subaxial Cervical Spine Trauma Pooria Salari, MD Assistant Professor Of Orthopaedics Department of Orthopaedic Surgery St. Louis University School of Medicine St. Louis, Missouri, USA Initial Evaluation
Subaxial Cervical Spine Trauma Pooria Salari, MD Assistant Professor Of Orthopaedics Department of Orthopaedic Surgery St. Louis University School of Medicine St. Louis, Missouri, USA Initial Evaluation
Involvement of the spine is common in rheumatoid. Incidence been reported to be 85% radiologically but only 30% have neurological signs and symptoms.
 RHEUMATOID SPINE Involvement of the spine is common in rheumatoid. Incidence been reported to be 85% radiologically but only 30% have neurological signs and symptoms. When neurology is present it may manifest
RHEUMATOID SPINE Involvement of the spine is common in rheumatoid. Incidence been reported to be 85% radiologically but only 30% have neurological signs and symptoms. When neurology is present it may manifest
Congenital Spine Deformity: Surgical Treatment Options. Spine Masters. Fri May , 4:10-4:25 Paul Sponseller MD
 Congenital Spine Deformity: Surgical Treatment Options Spine Masters Fri May19 2017, 4:10-4:25 Paul Sponseller MD Disclosures Medical Education Reviews JBJS Depuy Synthes Spine: Research, royalties Globus:
Congenital Spine Deformity: Surgical Treatment Options Spine Masters Fri May19 2017, 4:10-4:25 Paul Sponseller MD Disclosures Medical Education Reviews JBJS Depuy Synthes Spine: Research, royalties Globus:
SUBAXIAL CERVICAL SPINE TRAUMA- DIAGNOSIS AND MANAGEMENT
 SUBAXIAL CERVICAL SPINE TRAUMA- DIAGNOSIS AND MANAGEMENT 1 Anatomy 3 columns- Anterior, middle and Posterior Anterior- ALL, Anterior 2/3 rd body & disc. Middle- Posterior 1/3 rd of body & disc, PLL Posterior-
SUBAXIAL CERVICAL SPINE TRAUMA- DIAGNOSIS AND MANAGEMENT 1 Anatomy 3 columns- Anterior, middle and Posterior Anterior- ALL, Anterior 2/3 rd body & disc. Middle- Posterior 1/3 rd of body & disc, PLL Posterior-
Cranial Vertebral Junction Anatomy and Pathology
 Cranial Vertebral Junction Anatomy and Pathology October 2016 Mary Scanlon MD FACR Goals and Objective Goal-Understand CVJ anatomy & pathology Objective-After attending this lecture you will be able to
Cranial Vertebral Junction Anatomy and Pathology October 2016 Mary Scanlon MD FACR Goals and Objective Goal-Understand CVJ anatomy & pathology Objective-After attending this lecture you will be able to
Imaging of Cervical Spine Trauma Tudor H Hughes, M.D.
 Imaging of Cervical Spine Trauma Tudor H Hughes, M.D. General Considerations Most spinal fractures are due to a single episode of major trauma. Fatigue fractures of the spine are unusual except in the
Imaging of Cervical Spine Trauma Tudor H Hughes, M.D. General Considerations Most spinal fractures are due to a single episode of major trauma. Fatigue fractures of the spine are unusual except in the
Cervicothoracic Congenital Scoliosis: Treatment of shoulder balance and head tilt
 Cervicothoracic Congenital Scoliosis: Treatment of shoulder balance and head tilt David L. Skaggs, MD, MMM Professor and Chief of Orthopaedic Surgery University of Southern California Children s Hospital
Cervicothoracic Congenital Scoliosis: Treatment of shoulder balance and head tilt David L. Skaggs, MD, MMM Professor and Chief of Orthopaedic Surgery University of Southern California Children s Hospital
Subaxial (C3 7) cervical instability in children may
 cervical instability in children may") clinical article J Neurosurg Spine 24:892 896, 2016 Management of subaxial cervical instability in very young or small-for-age children using a static single-screw anterior cervical plate: indications,
clinical article J Neurosurg Spine 24:892 896, 2016 Management of subaxial cervical instability in very young or small-for-age children using a static single-screw anterior cervical plate: indications,
Case report. Open Access. Abstract
 Open Access Case report Orthotopic ossiculum terminale persistens and atlantoaxial instability in a child less than 12 years of age: a case report and review of the literature Ashwin Viswanathan 1, William
Open Access Case report Orthotopic ossiculum terminale persistens and atlantoaxial instability in a child less than 12 years of age: a case report and review of the literature Ashwin Viswanathan 1, William
Subaxial Cervical Spine Trauma. Introduction. Anatomic Considerations 7/23/2018
 Subaxial Cervical Spine Trauma Sheyan J. Armaghani, MD Florida Orthopedic Institute Assistant Professor USF Dept of Orthopedics Introduction Trauma to the cervical spine accounts for 5 of all spine injuries
Subaxial Cervical Spine Trauma Sheyan J. Armaghani, MD Florida Orthopedic Institute Assistant Professor USF Dept of Orthopedics Introduction Trauma to the cervical spine accounts for 5 of all spine injuries
Dorsal Cervical Surgeries and Techniques
 Dorsal Cervical Approaches Dorsal Cervical Surgeries and Techniques Gregory R. Trost, MD Professor and Vice Chair of Neurological Surgery University of Wisconsin-Madison Advantages Straightforward Easily
Dorsal Cervical Approaches Dorsal Cervical Surgeries and Techniques Gregory R. Trost, MD Professor and Vice Chair of Neurological Surgery University of Wisconsin-Madison Advantages Straightforward Easily
Subaxial Cervical Spine Trauma Dr Hesarikia BUMS
 Subaxial Cervical Spine Trauma Dr. Hesarikia BUMS Subaxial Cervical Spine From C3-C7 ROM Majority of cervical flexion Lateral bending Approximately 50% rotation Ligamentous Anatomy Anterior ALL, PLL, intervertebral
Subaxial Cervical Spine Trauma Dr. Hesarikia BUMS Subaxial Cervical Spine From C3-C7 ROM Majority of cervical flexion Lateral bending Approximately 50% rotation Ligamentous Anatomy Anterior ALL, PLL, intervertebral
A Review of the Diagnosis and Treatment of Atlantoaxial Dislocations
 Global Spine Journal Review Article 197 A Review of the Diagnosis and Treatment of Atlantoaxial Dislocations Sun Y. Yang 1 Anthony J. Boniello 1 Caroline E. Poorman 1 Andy L. Chang 1 Shenglin Wang 2 Peter
Global Spine Journal Review Article 197 A Review of the Diagnosis and Treatment of Atlantoaxial Dislocations Sun Y. Yang 1 Anthony J. Boniello 1 Caroline E. Poorman 1 Andy L. Chang 1 Shenglin Wang 2 Peter
Pediatric cervical spine injuries with neurological deficits, treatment options, and potential for recovery
 SICOT J 2017, 3, 53 Ó The Authors, published by EDP Sciences, 2017 DOI: 10.1051/sicotj/2017035 Available online at: www.sicot-j.org CASE REPORT OPEN ACCESS Pediatric cervical spine injuries with neurological
SICOT J 2017, 3, 53 Ó The Authors, published by EDP Sciences, 2017 DOI: 10.1051/sicotj/2017035 Available online at: www.sicot-j.org CASE REPORT OPEN ACCESS Pediatric cervical spine injuries with neurological
Management of severe cervical kyphosis in a patient with Larsen syndrome
 J Neurosurg Pediatrics 1:320 324, 2008 Management of severe cervical kyphosis in a patient with Larsen syndrome Case report MARCI MADERA, M.D., 1 ALVIN CRAWFORD, M.D., 2 AND FRANCESCO T. MANGANO, D.O.
J Neurosurg Pediatrics 1:320 324, 2008 Management of severe cervical kyphosis in a patient with Larsen syndrome Case report MARCI MADERA, M.D., 1 ALVIN CRAWFORD, M.D., 2 AND FRANCESCO T. MANGANO, D.O.
Surgical management of combined fracture of atlas associated with fracture of axis vertebrae (CAAF): Case Series
: Case Series") Romanian Neurosurgery (2015) XXIX 3: 335-341 335 Surgical management of combined fracture of atlas associated with fracture of axis vertebrae (CAAF): Case Series Guru Dutta Satyarthee, Gaurang Vaghani,
Romanian Neurosurgery (2015) XXIX 3: 335-341 335 Surgical management of combined fracture of atlas associated with fracture of axis vertebrae (CAAF): Case Series Guru Dutta Satyarthee, Gaurang Vaghani,
NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE
 NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedures overview of direct C1 lateral mass screw procedure for cervical spine stabilisation Introduction
NATIONAL INSTITUTE FOR CLINICAL EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedures overview of direct C1 lateral mass screw procedure for cervical spine stabilisation Introduction
A study of indications and assessment of fusion rates for atlantoaxial subluxation
 International Surgery Journal Reddy AM et al. Int Surg J. 2016 Feb;3(1):211-216 http://www.ijsurgery.com pissn 2349-3305 eissn 2349-2902 Research Article DOI: http://dx.doi.org/10.18203/2349-2902.isj20160228
International Surgery Journal Reddy AM et al. Int Surg J. 2016 Feb;3(1):211-216 http://www.ijsurgery.com pissn 2349-3305 eissn 2349-2902 Research Article DOI: http://dx.doi.org/10.18203/2349-2902.isj20160228
Management Of Posttraumatic Spinal Instability (Neurosurgical Topics, No 3) READ ONLINE
 READ ONLINE") Management Of Posttraumatic Spinal Instability (Neurosurgical Topics, No 3) READ ONLINE If you are searching for a ebook Management of Posttraumatic Spinal Instability (Neurosurgical Topics, No 3) in pdf
Management Of Posttraumatic Spinal Instability (Neurosurgical Topics, No 3) READ ONLINE If you are searching for a ebook Management of Posttraumatic Spinal Instability (Neurosurgical Topics, No 3) in pdf
Spinal Cord Injuries: The Basics. Kadre Sneddon POS Rounds October 1, 2003
 Spinal Cord Injuries: The Basics Kadre Sneddon POS Rounds October 1, 2003 Anatomy Dorsal columntouch, vibration Corticospinal tract- UMN Anterior horn-lmn Spinothalamic tractpain, temperature (contralateral)
Spinal Cord Injuries: The Basics Kadre Sneddon POS Rounds October 1, 2003 Anatomy Dorsal columntouch, vibration Corticospinal tract- UMN Anterior horn-lmn Spinothalamic tractpain, temperature (contralateral)
International Journal of Pharma and Bio Sciences
 Original Research Article Anatomy and Allied sciences International Journal of Pharma and Bio Sciences ISSN 0975-6299 SCREENING FOR ANOMALIES IN OCCIPITO-CERVICAL JUNCTION USING CRANIOMETRY IN COMPUTED
Original Research Article Anatomy and Allied sciences International Journal of Pharma and Bio Sciences ISSN 0975-6299 SCREENING FOR ANOMALIES IN OCCIPITO-CERVICAL JUNCTION USING CRANIOMETRY IN COMPUTED
8/31/2018 IMPORTANT CONSIDERATIONS. Signalment History Symmetry Progression of signs Painful vs non-painful SURGICAL CONSIDERATIONS
 IMPORTANT CONSIDERATIONS Signalment History Symmetry Progression of signs Painful vs non-painful SURGICAL CONSIDERATIONS Specific region of TL spine Differences in size and shape of articular processes
IMPORTANT CONSIDERATIONS Signalment History Symmetry Progression of signs Painful vs non-painful SURGICAL CONSIDERATIONS Specific region of TL spine Differences in size and shape of articular processes
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 4,000 116,000 120M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 4,000 116,000 120M Open access books available International authors and editors Downloads Our
The craniocervical junction
 Anver Jameel, MD The craniocervical junction A biomechanical and anatomical unit that extends from the skull base to C2 Includes the clivus, foramen magnum and contiguous occipital bone, the occipital
Anver Jameel, MD The craniocervical junction A biomechanical and anatomical unit that extends from the skull base to C2 Includes the clivus, foramen magnum and contiguous occipital bone, the occipital
Module 1: Basic Comprehensive Course
 The Hellenic Spine Society organize 5 modules according to the following program, which is based on the Eurospine program Module 1: Basic Comprehensive Course SESSION1: SPINE THE BIGGER PICTURE Evidence
The Hellenic Spine Society organize 5 modules according to the following program, which is based on the Eurospine program Module 1: Basic Comprehensive Course SESSION1: SPINE THE BIGGER PICTURE Evidence
2. The vertebral arch is composed of pedicles (projecting from the body) and laminae (uniting arch posteriorly).
 and laminae (uniting arch posteriorly).") VERTEBRAL COLUMN 2018zillmusom I. VERTEBRAL COLUMN - functions to support weight of body and protect spinal cord while permitting movements of trunk and providing for muscle attachments. A. Typical vertebra
VERTEBRAL COLUMN 2018zillmusom I. VERTEBRAL COLUMN - functions to support weight of body and protect spinal cord while permitting movements of trunk and providing for muscle attachments. A. Typical vertebra
Key Primary CPT Codes: Refer to pages: 7-9 Last Review Date: October 2016 Medical Coverage Guideline Number:
 National Imaging Associates, Inc. Clinical guidelines CERVICAL SPINE SURGERY: ANTERI CERVICAL DECOMPRESSION WITH FUSION CERVICAL POSTERI DECOMPRESSION WITH FUSION CERVICAL ARTIFICIAL DISC CERVICAL POSTERI
National Imaging Associates, Inc. Clinical guidelines CERVICAL SPINE SURGERY: ANTERI CERVICAL DECOMPRESSION WITH FUSION CERVICAL POSTERI DECOMPRESSION WITH FUSION CERVICAL ARTIFICIAL DISC CERVICAL POSTERI
Radiology of Cervical Spine Trauma. Cervical Spine Trauma. Imaging Standards. Canadian C. Spine Rule 11/28/2016
 Radiology of Cervical Spine Trauma Dr. Steven J. Gould, D.C. Board Certified Chiropractic Radiologist Cleveland Chiropractic College, KC. MO. Radiology Residency at CCC, KC Cervical Spine Trauma Vertebral
Radiology of Cervical Spine Trauma Dr. Steven J. Gould, D.C. Board Certified Chiropractic Radiologist Cleveland Chiropractic College, KC. MO. Radiology Residency at CCC, KC Cervical Spine Trauma Vertebral
Spinal Deformity Pathologies and Treatments
 Spinal Deformity Pathologies and Treatments Scoliosis Spinal Deformity 3-dimensional deformity affecting all 3 planes Can be difficult to visualize with 2-dimensional radiographs Kyphosis Deformity affecting
Spinal Deformity Pathologies and Treatments Scoliosis Spinal Deformity 3-dimensional deformity affecting all 3 planes Can be difficult to visualize with 2-dimensional radiographs Kyphosis Deformity affecting
Prognosis of neurological deficits associated with upper cervical spine injuries
 Paraplegia (1995) 33, 195-202 1995 International Medical Society of Paraplegia All rights reserved 0031-1758/95 $9.00 Prognosis of neurological deficits associated with upper cervical spine injuries Y
Paraplegia (1995) 33, 195-202 1995 International Medical Society of Paraplegia All rights reserved 0031-1758/95 $9.00 Prognosis of neurological deficits associated with upper cervical spine injuries Y
Odontoid process fracture in 2 year old child: a rare case report
 Romanian Neurosurgery Volume XXXI Number 4 2017 October-December Article Odontoid process fracture in 2 year old child: a rare case report Prajapati Hanuman Prasad, Singh Deepak Kumar, Singh Rakesh Kumar,
Romanian Neurosurgery Volume XXXI Number 4 2017 October-December Article Odontoid process fracture in 2 year old child: a rare case report Prajapati Hanuman Prasad, Singh Deepak Kumar, Singh Rakesh Kumar,
APPLYING BOTH ANTERIOR AND POSTERIOR APPROACH FOR MID CERVICAL TRAUMA: CASE REPORT
 APPLYING BOTH ANTERIOR AND POSTERIOR APPROACH FOR MID CERVICAL TRAUMA: CASE REPORT Dr. Sunil Pahari *1, Prof. Dr. Lu Hou Gen 2, Prof. Dr. Liu Jun 3 and Prof. Dr. Zhi Yu Sun 4 1,2,3,4Department of Orthopaedic
APPLYING BOTH ANTERIOR AND POSTERIOR APPROACH FOR MID CERVICAL TRAUMA: CASE REPORT Dr. Sunil Pahari *1, Prof. Dr. Lu Hou Gen 2, Prof. Dr. Liu Jun 3 and Prof. Dr. Zhi Yu Sun 4 1,2,3,4Department of Orthopaedic
CTQ 6/24/2018. Age-Related Disc Degeneration. Age-Related Disc Degeneration. Acknowledgement. Cervical Spondylosis. Key Points.
 Acknowledgement Thank you to A. Jay Khanna, MD for providing many of the images and slides Francis H. Shen, MD Warren G. Stamp Endowed Professor Division Head, Spine Division Co-Director, Spine Center
Acknowledgement Thank you to A. Jay Khanna, MD for providing many of the images and slides Francis H. Shen, MD Warren G. Stamp Endowed Professor Division Head, Spine Division Co-Director, Spine Center
ELY ASHKENAZI Israel Spine Center at Assuta Hospital Tel Aviv, Israel
 nterior cervical decompression using the Hybrid Decompression Fixation technique, a combination of corpectomies and or discectomies, in the management of multilevel cervical myelopathy J ORTHOP TRUM SURG
nterior cervical decompression using the Hybrid Decompression Fixation technique, a combination of corpectomies and or discectomies, in the management of multilevel cervical myelopathy J ORTHOP TRUM SURG
Comprehension of the common spine disorder.
 Objectives Comprehension of the common spine disorder. Disc degeneration/hernia. Spinal stenosis. Common spinal deformity (Spondylolisthesis, Scoliosis). Osteoporotic fracture. Anatomy Anatomy Anatomy
Objectives Comprehension of the common spine disorder. Disc degeneration/hernia. Spinal stenosis. Common spinal deformity (Spondylolisthesis, Scoliosis). Osteoporotic fracture. Anatomy Anatomy Anatomy
Congenital deformity of the spine-therapy. Werner Lack*, Georg Grabmeier**
 Congenital deformity of the spine-therapy Werner Lack*, Georg Grabmeier** *free spine surgeons of Austria, **SMZ-East, Vienna Conservative therapy in clear cases of progression (2 hemi vertebrae, unilateral
Congenital deformity of the spine-therapy Werner Lack*, Georg Grabmeier** *free spine surgeons of Austria, **SMZ-East, Vienna Conservative therapy in clear cases of progression (2 hemi vertebrae, unilateral
Ligaments of the vertebral column:
 In the last lecture we started talking about the joints in the vertebral column, and we said that there are two types of joints between adjacent vertebrae: 1. Between the bodies of the vertebrae; which
In the last lecture we started talking about the joints in the vertebral column, and we said that there are two types of joints between adjacent vertebrae: 1. Between the bodies of the vertebrae; which
Surgical Management of Congenital Cervical Kyphosis
 n Feature Article Surgical Management of Congenital Cervical Kyphosis Zhimin He, MD; Yang Liu, MD; Feng Xue, MD; Haijun Xiao, MD; Wen Yuan, MD; Deyu Chen, MD abstract Full article available online at Healio.com/Orthopedics.
n Feature Article Surgical Management of Congenital Cervical Kyphosis Zhimin He, MD; Yang Liu, MD; Feng Xue, MD; Haijun Xiao, MD; Wen Yuan, MD; Deyu Chen, MD abstract Full article available online at Healio.com/Orthopedics.
Rick C. Sasso MD Professor Chief of Spine Surgery Clinical Orthopaedic Surgery Indiana University School of Medicine
 Cervical Myelopathy: Anterior Surgery is Best Rick C. Sasso MD Professor Chief of Surgery Clinical Orthopaedic Surgery University School of Medicine Disclosure: Research support-medtronic, Stryker, AO,
Cervical Myelopathy: Anterior Surgery is Best Rick C. Sasso MD Professor Chief of Surgery Clinical Orthopaedic Surgery University School of Medicine Disclosure: Research support-medtronic, Stryker, AO,
UPPER CERVICAL MYELOPATHY WITH METATROPIC DYSPLASIA
 UPPER CERVICAL MYELOPATHY WITH METATROPIC DYSPLASIA REPORT OF 4 SURGICAL CASES Yujiro Takeshita*, Kota Miyoshi**, Tomoaki Kitagawa** *Department of Orthopaedic and Spine Surgery, University of Tokyo, Japan
UPPER CERVICAL MYELOPATHY WITH METATROPIC DYSPLASIA REPORT OF 4 SURGICAL CASES Yujiro Takeshita*, Kota Miyoshi**, Tomoaki Kitagawa** *Department of Orthopaedic and Spine Surgery, University of Tokyo, Japan
Case Report A Case of Delayed Myelopathy Caused by Atlantoaxial Subluxation without Fracture
 Case Reports in Orthopedics Volume 2013, Article ID 421087, 4 pages http://dx.doi.org/10.1155/2013/421087 Case Report A Case of Delayed Myelopathy Caused by Atlantoaxial Subluxation without Fracture Ryo
Case Reports in Orthopedics Volume 2013, Article ID 421087, 4 pages http://dx.doi.org/10.1155/2013/421087 Case Report A Case of Delayed Myelopathy Caused by Atlantoaxial Subluxation without Fracture Ryo
What Every Spine Surgeon Should Know About Neurosurgical Issues
 What Every Spine Surgeon Should Know About Neurosurgical Issues Amer Samdani, MD Chief of Surgery Shriners Hospitals for Children Philadelphia, PA Objectives Main intraspinal lesions Chiari malformation
What Every Spine Surgeon Should Know About Neurosurgical Issues Amer Samdani, MD Chief of Surgery Shriners Hospitals for Children Philadelphia, PA Objectives Main intraspinal lesions Chiari malformation
Asymmetric T5 Pedicle Subtraction Osteotomy (PSO) for complex posttraumatic deformity
 for complex posttraumatic deformity") Eur Spine J (2013) 22:2130 2135 DOI 10.1007/s00586-013-2942-y OPEN OPERATING THEATRE (OOT) Asymmetric T5 Pedicle Subtraction Osteotomy (PSO) for complex posttraumatic deformity Ibrahim Obeid Fethi Laouissat
Eur Spine J (2013) 22:2130 2135 DOI 10.1007/s00586-013-2942-y OPEN OPERATING THEATRE (OOT) Asymmetric T5 Pedicle Subtraction Osteotomy (PSO) for complex posttraumatic deformity Ibrahim Obeid Fethi Laouissat
Occipital-Cervical-Thoracic Fixation Techniques
 Occipital-Cervical-Thoracic Fixation Techniques Neill M. Wright, M.D. Herbert Lourie Professor of Neurological Surgery Professor of Orthopaedic Surgery Washington University School of Medicine Disclosures
Occipital-Cervical-Thoracic Fixation Techniques Neill M. Wright, M.D. Herbert Lourie Professor of Neurological Surgery Professor of Orthopaedic Surgery Washington University School of Medicine Disclosures
Posterior cervical fusion in children
 Posterior cervical fusion in children JOE M. MCWHORTER, M.D., EBEN ALEXANDER, JR., M.D., COURTLAND H. DAVIS, JR., M.D., AND DAVID L. KELLY, JR., M.D. Section on Neurosurgery, Department of Surgery, Bowman
Posterior cervical fusion in children JOE M. MCWHORTER, M.D., EBEN ALEXANDER, JR., M.D., COURTLAND H. DAVIS, JR., M.D., AND DAVID L. KELLY, JR., M.D. Section on Neurosurgery, Department of Surgery, Bowman
Inferior view of the skull showing foramina (Atlas of Human Anatomy, 5th edition, Plate 12)
") Section 1 Head and Neck Skull, Basal View Incisive foramen Choanae Foramen ovale Foramen lacerum Foramen spinosum Carotid canal Jugular fossa Mastoid process Inferior view of the skull showing foramina
Section 1 Head and Neck Skull, Basal View Incisive foramen Choanae Foramen ovale Foramen lacerum Foramen spinosum Carotid canal Jugular fossa Mastoid process Inferior view of the skull showing foramina
Scoliosis: Orthopaedic Perspectives
 Scoliosis: Orthopaedic Perspectives Scott B. Rosenfeld, MD Division of Pediatric Orthopaedic Surgery Texas Children s Hospital Page 0 xxx00.#####.ppt 9/23/2012 8:26:24 AM I have no disclosures Disclosures
Scoliosis: Orthopaedic Perspectives Scott B. Rosenfeld, MD Division of Pediatric Orthopaedic Surgery Texas Children s Hospital Page 0 xxx00.#####.ppt 9/23/2012 8:26:24 AM I have no disclosures Disclosures
Imaging of Cervical Spine Trauma
 Imaging of Cervical Spine Trauma C Craig Blackmore, MD, MPH Professor of Radiology and Adjunct Professor of Health Services University of Washington, Harborview Medical Center Salary support: AHRQ grant
Imaging of Cervical Spine Trauma C Craig Blackmore, MD, MPH Professor of Radiology and Adjunct Professor of Health Services University of Washington, Harborview Medical Center Salary support: AHRQ grant
LUMBAR SPINAL STENOSIS
 LUMBAR SPINAL STENOSIS Always occurs in the mobile segment. Factors play role in Stenosis Pre existing congenital or developmental narrowing of the lumbar spinal canal Translation of one anatomic segment
LUMBAR SPINAL STENOSIS Always occurs in the mobile segment. Factors play role in Stenosis Pre existing congenital or developmental narrowing of the lumbar spinal canal Translation of one anatomic segment
Musculoskeletal Development and Sports Injuries in Pediatric Patients
 Dynamic Chiropractic October 21, 2010, Vol. 28, Issue 22 Musculoskeletal Development and Sports Injuries in Pediatric Patients By Deborah Pate, DC, DACBR Physical activity is extremely important for everyone,
Dynamic Chiropractic October 21, 2010, Vol. 28, Issue 22 Musculoskeletal Development and Sports Injuries in Pediatric Patients By Deborah Pate, DC, DACBR Physical activity is extremely important for everyone,
Malformations of the cranio-cervical junction: basilar impression Gonzalo Bertullo 1, Viviana Cabrera 2
 Malformations of the cranio-cervical junction: basilar impression Gonzalo Bertullo 1, Viviana Cabrera 2 Abstract Cranio-cervical junction abnormalities are a rare combination of congenital or acquired
Malformations of the cranio-cervical junction: basilar impression Gonzalo Bertullo 1, Viviana Cabrera 2 Abstract Cranio-cervical junction abnormalities are a rare combination of congenital or acquired
Objectives. Comprehension of the common spine disorder
 Objectives Comprehension of the common spine disorder Disc degeneration/hernia Spinal stenosis Common spinal deformity (Spondylolisthesis, Scoliosis) Osteoporotic fracture Destructive spinal lesions Anatomy
Objectives Comprehension of the common spine disorder Disc degeneration/hernia Spinal stenosis Common spinal deformity (Spondylolisthesis, Scoliosis) Osteoporotic fracture Destructive spinal lesions Anatomy
Infantile developmental thoracolumbar kyphosis with segmental subluxation of the spine
 Infantile developmental thoracolumbar kyphosis with segmental subluxation of the spine A. I. Tsirikos, M. J. McMaster From The Royal Hospital for Sick Children, Edinburgh, Scotland We report five children
Infantile developmental thoracolumbar kyphosis with segmental subluxation of the spine A. I. Tsirikos, M. J. McMaster From The Royal Hospital for Sick Children, Edinburgh, Scotland We report five children
Copyright 2010 Pearson Education, Inc.
 E. VERTEBRAL COLUMN 1. The vertebral column extends from the skull to the pelvis and forms the vertical axis of the skeleton. 2. The vertebral column is composed of vertebrae that are separated by intervertebral
E. VERTEBRAL COLUMN 1. The vertebral column extends from the skull to the pelvis and forms the vertical axis of the skeleton. 2. The vertebral column is composed of vertebrae that are separated by intervertebral
Idiopathic scoliosis Scoliosis Deformities I 06
 What is Idiopathic scoliosis? 80-90% of all scolioses are idiopathic, the rest are neuromuscular or congenital scolioses with manifest primary diseases responsible for the scoliotic pathogenesis. This
What is Idiopathic scoliosis? 80-90% of all scolioses are idiopathic, the rest are neuromuscular or congenital scolioses with manifest primary diseases responsible for the scoliotic pathogenesis. This
Mitsuhiro Hashimto 1), Masashi Yamazaki 2), Macondo Mochizuki 3), Masatsune Yamagata 1), Yoshikazu Ikeda 1), Fumitake Nakajima 1)
, Masashi Yamazaki 2), Macondo Mochizuki 3), Masatsune Yamagata 1), Yoshikazu Ikeda 1), Fumitake Nakajima 1)") Long-term results of anterior cervical corpectomy and arthrodesis for cervical degenerative diseases with more than ten years of follow-up Mitsuhiro Hashimto 1), Masashi Yamazaki 2), Macondo Mochizuki
Long-term results of anterior cervical corpectomy and arthrodesis for cervical degenerative diseases with more than ten years of follow-up Mitsuhiro Hashimto 1), Masashi Yamazaki 2), Macondo Mochizuki
Neck Pain: Help! Eric M. Massicotte, MD, MSc, MBA, FRCSC Associate Professor University of Toronto
 Neck Pain: Help! Eric M. Massicotte, MD, MSc, MBA, FRCSC Associate Professor University of Toronto Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied,
Neck Pain: Help! Eric M. Massicotte, MD, MSc, MBA, FRCSC Associate Professor University of Toronto Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied,
Cervical Hyperextension and Scoliosis in Muscular Dystrophy: Case Report and Literature Review
 Cronicon OPEN ACCESS ORTHOPAEDICS Review Article Cervical Hyperextension and Scoliosis in Muscular Dystrophy: Case Report and Literature Review Yu Wang, Hong Liu, Chunde Li, Hong Li and Xiaodong Yi* Department
Cronicon OPEN ACCESS ORTHOPAEDICS Review Article Cervical Hyperextension and Scoliosis in Muscular Dystrophy: Case Report and Literature Review Yu Wang, Hong Liu, Chunde Li, Hong Li and Xiaodong Yi* Department
VERTEBRAL COLUMN VERTEBRAL COLUMN
 VERTEBRAL COLUMN FUNCTIONS: 1) Support weight - transmits weight to pelvis and lower limbs 2) Houses and protects spinal cord - spinal nerves leave cord between vertebrae 3) Permits movements - *clinical
VERTEBRAL COLUMN FUNCTIONS: 1) Support weight - transmits weight to pelvis and lower limbs 2) Houses and protects spinal cord - spinal nerves leave cord between vertebrae 3) Permits movements - *clinical
ESSENTIALS OF PLAIN FILM INTERPRETATION: SPINE DR ASIF SAIFUDDIN
 ESSENTIALS OF PLAIN FILM INTERPRETATION: SPINE DR ASIF SAIFUDDIN Consultant Musculoskeletal Radiologist Royal National Orthopaedic Hospital Stanmore,UK. INTRODUCTION 2 INTRODUCTION 3 INTRODUCTION Spinal
ESSENTIALS OF PLAIN FILM INTERPRETATION: SPINE DR ASIF SAIFUDDIN Consultant Musculoskeletal Radiologist Royal National Orthopaedic Hospital Stanmore,UK. INTRODUCTION 2 INTRODUCTION 3 INTRODUCTION Spinal
MDCT and MRI evaluation of cervical spine trauma
 Insights Imaging (2014) 5:67 75 DOI 10.1007/s13244-013-0304-2 PICTORIAL REVIEW MDCT and MRI evaluation of cervical spine trauma Michael Utz & Shadab Khan & Daniel O Connor & Stephen Meyers Received: 10
Insights Imaging (2014) 5:67 75 DOI 10.1007/s13244-013-0304-2 PICTORIAL REVIEW MDCT and MRI evaluation of cervical spine trauma Michael Utz & Shadab Khan & Daniel O Connor & Stephen Meyers Received: 10
Ossification of the posterior longitudinal ligament
 J Neurosurg Spine 19:431 435, 2013 AANS, 2013 Upper cervical cord compression due to a C-1 posterior arch in a patient with ossification of the posterior longitudinal ligament and a kyphotic cervical spine
J Neurosurg Spine 19:431 435, 2013 AANS, 2013 Upper cervical cord compression due to a C-1 posterior arch in a patient with ossification of the posterior longitudinal ligament and a kyphotic cervical spine
You have 24 vertebrae in your spinal column. Two are special enough to be individually named.
 You have 24 vertebrae in your spinal column. Two are special enough to be individually named. Your atlas (C01) and axis (C02) are very important vertebrae. Without them, head and neck movement would be
You have 24 vertebrae in your spinal column. Two are special enough to be individually named. Your atlas (C01) and axis (C02) are very important vertebrae. Without them, head and neck movement would be
Upper Cervical Spine - Occult Injury and Trigger for CT Exam
 Upper Cervical Spine - Occult Injury and Trigger for CT Exam Main Menu Introduction Clinical clearance of C-SpineC Radiographic evaluation Norms for C-spineC Triggers for CT exam: Odontoid Lateral view
Upper Cervical Spine - Occult Injury and Trigger for CT Exam Main Menu Introduction Clinical clearance of C-SpineC Radiographic evaluation Norms for C-spineC Triggers for CT exam: Odontoid Lateral view
Outline. Epidemiology Indications for C-spine imaging Modalities Interpretation Types of fractures
 C-Spine Plain Films Outline Epidemiology Indications for C-spine imaging Modalities Interpretation Types of fractures Epidemiology 7000-10000 c-spine injuries treated each year Additional 5000 die at the
C-Spine Plain Films Outline Epidemiology Indications for C-spine imaging Modalities Interpretation Types of fractures Epidemiology 7000-10000 c-spine injuries treated each year Additional 5000 die at the
Os odontoideum is an anatomical abnormality in
 Neurosurg Focus 31 (6):E10, 2011 Incidental os odontoideum: current management strategies Paul Klimo Jr., M.D., M.P.H., 1 Valerie Coon, M.D., 2 and Douglas Brockmeyer, M.D. 2 1 Semmes-Murphey Neurologic
Neurosurg Focus 31 (6):E10, 2011 Incidental os odontoideum: current management strategies Paul Klimo Jr., M.D., M.P.H., 1 Valerie Coon, M.D., 2 and Douglas Brockmeyer, M.D. 2 1 Semmes-Murphey Neurologic
Injuries to the lower cervical spine are common in
 One stage anterior-posterior approach for traumatic atlantoaxial instability combined with subaxial cervical spinal cord injury WANG Chang-sheng, LIU Mou-jun, LIN Jian-hua*, XU Wei-hong and LUO Hong-bin
One stage anterior-posterior approach for traumatic atlantoaxial instability combined with subaxial cervical spinal cord injury WANG Chang-sheng, LIU Mou-jun, LIN Jian-hua*, XU Wei-hong and LUO Hong-bin
SCIWORA Rozlyn McTeer BSN, RN, CEN Pediatric Trauma Coordinator Trauma Services OBJECTIVES DEFINITION 11/8/2017. Identify SCIWORA.
 SCIWORA Rozlyn McTeer BSN, RN, CEN Pediatric Trauma Coordinator Trauma Services Identify SCIWORA. OBJECTIVES Identify the population at risk. To identify anatomic and physiologic reasons for SCIWORA. To
SCIWORA Rozlyn McTeer BSN, RN, CEN Pediatric Trauma Coordinator Trauma Services Identify SCIWORA. OBJECTIVES Identify the population at risk. To identify anatomic and physiologic reasons for SCIWORA. To
AXIAL SKELETON FORM THE VERTICAL AXIS OF THE BODY CONSISTS OF 80 BONES INCLUDES BONES OF HEAD, VERTEBRAL COLUMN, RIBS,STERNUM
 AXIAL SKELETON FORM THE VERTICAL AXIS OF THE BODY CONSISTS OF 80 BONES INCLUDES BONES OF HEAD, VERTEBRAL COLUMN, RIBS,STERNUM APPENDICULAR SKELETON BONES OF THE FREE APPENDAGES & THEIR POINTS OF ATTACHMENTS
AXIAL SKELETON FORM THE VERTICAL AXIS OF THE BODY CONSISTS OF 80 BONES INCLUDES BONES OF HEAD, VERTEBRAL COLUMN, RIBS,STERNUM APPENDICULAR SKELETON BONES OF THE FREE APPENDAGES & THEIR POINTS OF ATTACHMENTS
Atlantoaxial joint distraction as a treatment for basilar invagination: A report of an experience with 11 cases
 Original Article Atlantoaxial joint distraction as a treatment for basilar invagination: A report of an experience with 11 cases Atul Goel, Abhidha Shah Department of Neurosurgery, King Edward 7 th Memorial
Original Article Atlantoaxial joint distraction as a treatment for basilar invagination: A report of an experience with 11 cases Atul Goel, Abhidha Shah Department of Neurosurgery, King Edward 7 th Memorial
Treatment of thoracolumbar burst fractures by vertebral shortening
 Eur Spine J (2002) 11 :8 12 DOI 10.1007/s005860000214 TECHNICAL INNOVATION Alejandro Reyes-Sanchez Luis M. Rosales Victor P. Miramontes Dario E. Garin Treatment of thoracolumbar burst fractures by vertebral
Eur Spine J (2002) 11 :8 12 DOI 10.1007/s005860000214 TECHNICAL INNOVATION Alejandro Reyes-Sanchez Luis M. Rosales Victor P. Miramontes Dario E. Garin Treatment of thoracolumbar burst fractures by vertebral
Spine Surgery: Techniques, Complication Avoidance, and Management. 2 Volume Set
 Spine Surgery: Techniques, Complication Avoidance, and Management. 2 Volume Set Benzel, E ISBN-13: 9781437705874 Table of Contents SECTION 1 - HISTORY 1 - History 2 - History of Spine Instrumentation -
Spine Surgery: Techniques, Complication Avoidance, and Management. 2 Volume Set Benzel, E ISBN-13: 9781437705874 Table of Contents SECTION 1 - HISTORY 1 - History 2 - History of Spine Instrumentation -
Imaging of Trauma to the Spine. Orthopedic Diplomate Program University of Bridgeport College of Chiropractic
 Imaging of Trauma to the Spine Orthopedic Diplomate Program University of Bridgeport College of Chiropractic Jefferson Fracture Yee, LL: The Jefferson Fracture, Radiology Cases in Pediatric Emergency Medicine.
Imaging of Trauma to the Spine Orthopedic Diplomate Program University of Bridgeport College of Chiropractic Jefferson Fracture Yee, LL: The Jefferson Fracture, Radiology Cases in Pediatric Emergency Medicine.
Formation defects Scoliosis Deformities I 07 1
 What is congenital scoliosis? Congenital scoliosis is a spinal deformity with lateral deviation and rotation of the spinal column, where congenital dysfunctions in embryonal vertebra development cause
What is congenital scoliosis? Congenital scoliosis is a spinal deformity with lateral deviation and rotation of the spinal column, where congenital dysfunctions in embryonal vertebra development cause
Complex Spine Symposium January 12th, Balgrist University Hospital
 DEGENERATIVE CERVICAL MYELOPATHY CLINICAL DECISION MAKING Prof. Dr. Mazda Farshad Chair of Orthopedic Surgery Chief of Spine Surgery Medical Director CERVICAL MYELOPATHY - CAUSES degenerative cervical
DEGENERATIVE CERVICAL MYELOPATHY CLINICAL DECISION MAKING Prof. Dr. Mazda Farshad Chair of Orthopedic Surgery Chief of Spine Surgery Medical Director CERVICAL MYELOPATHY - CAUSES degenerative cervical
ESCOME Pre-Course Outline (v1.09)
") ESCOME Pre-Course Outline (v1.09) 1. Basics of Spinal Disorders Introduction to Spinal Surgery Spinal Anatomy Introduction to Vertebral Anatomical Concepts Anatomy and Function of Joints and Ligaments
ESCOME Pre-Course Outline (v1.09) 1. Basics of Spinal Disorders Introduction to Spinal Surgery Spinal Anatomy Introduction to Vertebral Anatomical Concepts Anatomy and Function of Joints and Ligaments
Spondylolysis. Lysis (Greek λύσις, lýsis from lýein "to separate") refers to the breaking down.
 refers to the breaking down.") Spondylolysis Lysis (Greek λύσις, lýsis from lýein "to separate") refers to the breaking down. Thomas J Kishen Spine Surgeon Sparsh Hospital for Advanced Surgeries Bangalore Spondylolysis Defect in the
Spondylolysis Lysis (Greek λύσις, lýsis from lýein "to separate") refers to the breaking down. Thomas J Kishen Spine Surgeon Sparsh Hospital for Advanced Surgeries Bangalore Spondylolysis Defect in the
Adult Spinal Deformity Robert Hart. Dept. Orthopaedics and Rehab OHSU
 Adult Spinal Deformity 2010 Robert Hart Dept. Orthopaedics and Rehab OHSU What is Adult Spinal Deformity? Untreated Idiopathic Scoliosis Flat Back Syndrome Adjacent Segment Stenosis Non-Union Degenerative
Adult Spinal Deformity 2010 Robert Hart Dept. Orthopaedics and Rehab OHSU What is Adult Spinal Deformity? Untreated Idiopathic Scoliosis Flat Back Syndrome Adjacent Segment Stenosis Non-Union Degenerative
An anatomic consideration of C2 vertebrae artery groove variation for individual screw implantation in axis
 Eur Spine J (2013) 22:1547 1552 DOI 10.1007/s00586-013-2779-4 ORIGINAL ARTICLE An anatomic consideration of C2 vertebrae artery groove variation for individual screw implantation in axis Janhua Wang Hong
Eur Spine J (2013) 22:1547 1552 DOI 10.1007/s00586-013-2779-4 ORIGINAL ARTICLE An anatomic consideration of C2 vertebrae artery groove variation for individual screw implantation in axis Janhua Wang Hong
PEDIATRIC CERVICAL SPINE DEFORMITY.
 PEDIATRIC CERVICAL SPINE DEFORMITY www.fisiokinesiterapia.biz DEVELOPMENT EACH VERTEBRAE DEVELOP FROM THE CAUDAL AND CRANIAL ½ OF 2 SCLEROTOMES C1 and C2 primitive centrum fuse to form odontoid process
PEDIATRIC CERVICAL SPINE DEFORMITY www.fisiokinesiterapia.biz DEVELOPMENT EACH VERTEBRAE DEVELOP FROM THE CAUDAL AND CRANIAL ½ OF 2 SCLEROTOMES C1 and C2 primitive centrum fuse to form odontoid process
ACDF. Anterior Cervical Discectomy and Fusion. An introduction to
 An introduction to ACDF Anterior Cervical Discectomy and Fusion This booklet provides general information on ACDF. It is not meant to replace any personal conversations that you might wish to have with
An introduction to ACDF Anterior Cervical Discectomy and Fusion This booklet provides general information on ACDF. It is not meant to replace any personal conversations that you might wish to have with
Vertebral Column. Backbone consists of 26 vertebrae. Five vertebral regions. Cervical
 Vertebral Column Backbone consists of 26 vertebrae. Five vertebral regions Cervical vertebrae (7) in the neck. Thoracic vertebrae (12) in the thorax. Lumbar vertebrae (5) in the lower back. Sacrum (5,
Vertebral Column Backbone consists of 26 vertebrae. Five vertebral regions Cervical vertebrae (7) in the neck. Thoracic vertebrae (12) in the thorax. Lumbar vertebrae (5) in the lower back. Sacrum (5,
CASE REPORT. Tadanori Ogata 1*, Tadao Morino 1, Masayuki Hino 2 and Hiromasa Miura 2
 Ogata et al. Journal of Medical Case Reports 2012, 6:171 JOURNAL OF MEDICAL CASE REPORTS CASE REPORT Open Access Cervical myelopathy caused by atlantoaxial instability in a patient with an os odontoideum
Ogata et al. Journal of Medical Case Reports 2012, 6:171 JOURNAL OF MEDICAL CASE REPORTS CASE REPORT Open Access Cervical myelopathy caused by atlantoaxial instability in a patient with an os odontoideum
What is an osteotomy? Bony resection designed to increase flexibility of spine or alteration of alignment
 Spinal osteotomies Nicholas D. Fletcher, MD Assistant Professor of Orthopedics Director of Spinal Quality/Outcomes Emory University Department of Orthopedics Children s Healthcare of Atlanta Atlanta, GA
Spinal osteotomies Nicholas D. Fletcher, MD Assistant Professor of Orthopedics Director of Spinal Quality/Outcomes Emory University Department of Orthopedics Children s Healthcare of Atlanta Atlanta, GA
Symptomatic atlantoaxial instability in Down syndrome
 J Neurosurg (Pediatrics 3) 103:231 237, 2005 Symptomatic atlantoaxial instability in Down syndrome ALI NADER-SEPAHI, F.R.C.S. (SN), ADRIAN T. H. CASEY, F.R.C.S., RICHARD HAYWARD, F.R.C.S., H. ALAN CROCKARD,
J Neurosurg (Pediatrics 3) 103:231 237, 2005 Symptomatic atlantoaxial instability in Down syndrome ALI NADER-SEPAHI, F.R.C.S. (SN), ADRIAN T. H. CASEY, F.R.C.S., RICHARD HAYWARD, F.R.C.S., H. ALAN CROCKARD,
Classification of Thoracolumbar Spine Injuries
 Classification of Thoracolumbar Spine Injuries Guillem Saló Bru 1 IMAS. Hospitals del Mar i de l Esperança. ICATME. Institut Universitari Dexeus USP. UNIVERSITAT AUTÒNOMA DE BARCELONA Objectives of classification
Classification of Thoracolumbar Spine Injuries Guillem Saló Bru 1 IMAS. Hospitals del Mar i de l Esperança. ICATME. Institut Universitari Dexeus USP. UNIVERSITAT AUTÒNOMA DE BARCELONA Objectives of classification
River North Pain Management Consultants, S.C., Axel Vargas, M.D., Regional Anesthesiology and Interventional Pain Management.
 River North Pain Management Consultants, S.C., Axel Vargas, M.D., Regional Anesthesiology and Interventional Pain Management. Chicago, Illinois, 60611 Phone: (888) 951-6471 Fax: (888) 961-6471 Clinical
River North Pain Management Consultants, S.C., Axel Vargas, M.D., Regional Anesthesiology and Interventional Pain Management. Chicago, Illinois, 60611 Phone: (888) 951-6471 Fax: (888) 961-6471 Clinical
A rare case of spinal injury: bilateral facet dislocation without fracture at the lumbosacral joint
 J Orthop Sci (2012) 17:189 193 DOI 10.1007/s00776-011-0082-y CASE REPORT A rare case of spinal injury: bilateral facet dislocation without fracture at the lumbosacral joint Kei Shinohara Shigeru Soshi
J Orthop Sci (2012) 17:189 193 DOI 10.1007/s00776-011-0082-y CASE REPORT A rare case of spinal injury: bilateral facet dislocation without fracture at the lumbosacral joint Kei Shinohara Shigeru Soshi
Focal Correction of Severe Fixed Kyphosis with Single Level Posterior Ponte Osteotomy and Interbody Fusion
 Open Access Case Report DOI: 10.7759/cureus.653 Focal Correction of Severe Fixed Kyphosis with Single Level Posterior Ponte Osteotomy and Interbody Fusion Seth S. Molloy 1, Faiz U. Ahmad 2, Griffin R.
Open Access Case Report DOI: 10.7759/cureus.653 Focal Correction of Severe Fixed Kyphosis with Single Level Posterior Ponte Osteotomy and Interbody Fusion Seth S. Molloy 1, Faiz U. Ahmad 2, Griffin R.
Cervical Osteotomies: Choosing the Right Surgical Approach
 Cervical Osteotomies: Choosing the Right Surgical Approach Todd J. Albert, MD Surgeon-in-Chief and Medical Director Korein-Wilson Professor Hospital for Special Surgery Chairman, Department of Orthopaedic
Cervical Osteotomies: Choosing the Right Surgical Approach Todd J. Albert, MD Surgeon-in-Chief and Medical Director Korein-Wilson Professor Hospital for Special Surgery Chairman, Department of Orthopaedic
SPORC 2017 EOS/Congenital Talk
 SPORC 2017 EOS/Congenital Talk Early Onset / Congenital Spine Deformity What Do We Know? What Are We Doing? Charles E Johnston MD TSRHC Dallas Tx Disclosures : Medtronic, Elsevier EOSD / Congenital Untreated
SPORC 2017 EOS/Congenital Talk Early Onset / Congenital Spine Deformity What Do We Know? What Are We Doing? Charles E Johnston MD TSRHC Dallas Tx Disclosures : Medtronic, Elsevier EOSD / Congenital Untreated
PATIENT: DOB: TODAY S DATE:
 1. I have been strongly advised to carefully read and consider this operative permit. I realize that it is important that I understand this material. I also understand that if certain sections are not
1. I have been strongly advised to carefully read and consider this operative permit. I realize that it is important that I understand this material. I also understand that if certain sections are not
Technique Guide. C1/C2 Access System. Percutaneous transarticular screw fixation.
 Technique Guide C1/C2 Access System. Percutaneous transarticular screw fixation. C1/C2 Access System Table of Contents General introduction 2 Indications/Contraindications 2 Image intensifier-assisted
Technique Guide C1/C2 Access System. Percutaneous transarticular screw fixation. C1/C2 Access System Table of Contents General introduction 2 Indications/Contraindications 2 Image intensifier-assisted
Laminar hook instrumentation in the cervical spine. An experimental study on the relation of hooks to the spinal cord
 Eur Spine J (2001) 10 :340 344 DOI 10.1007/s005860100251 ORIGINAL ARTICLE T. Fagerström R. Hedlund P. Bancel R. Robert B. Dupas Laminar hook instrumentation in the cervical spine. An experimental study
Eur Spine J (2001) 10 :340 344 DOI 10.1007/s005860100251 ORIGINAL ARTICLE T. Fagerström R. Hedlund P. Bancel R. Robert B. Dupas Laminar hook instrumentation in the cervical spine. An experimental study
Rheumatoid Arthritis and the Cervical Spine. Radiology Rounds November 21, 2006 Derek Haaland
 Rheumatoid Arthritis and the Cervical Spine Radiology Rounds November 21, 2006 Derek Haaland Laiho et al. Semin Arthritis Rheum. 2004:34;267. Laiho et al. Semin Arthritis Rheum. 2004:34;267. *Shen et al.
Rheumatoid Arthritis and the Cervical Spine Radiology Rounds November 21, 2006 Derek Haaland Laiho et al. Semin Arthritis Rheum. 2004:34;267. Laiho et al. Semin Arthritis Rheum. 2004:34;267. *Shen et al.
Management of Bone and Spinal Cord in Spinal Surgery.
 Management of Bone and Spinal Cord in Spinal Surgery. G. Saló, PhD, MD. Senior Consultant Spine Unit. Hospital del Mar. Barcelona. Ass. Prof. Universitat Autònoma de Barcelona. Introduction The management
Management of Bone and Spinal Cord in Spinal Surgery. G. Saló, PhD, MD. Senior Consultant Spine Unit. Hospital del Mar. Barcelona. Ass. Prof. Universitat Autònoma de Barcelona. Introduction The management
M ASTER S T ECHNIQUES: VCR & GROWING R ODS
 M ASTER S T ECHNIQUES: VCR & GROWING R ODS LAWRENCE G. LENKE, MD The Jerome J. Gilden Distinguished Professor of Orthopaedic Surgery Professor of Neurological Surgery Chief, Spinal Surgery Co-Director,
M ASTER S T ECHNIQUES: VCR & GROWING R ODS LAWRENCE G. LENKE, MD The Jerome J. Gilden Distinguished Professor of Orthopaedic Surgery Professor of Neurological Surgery Chief, Spinal Surgery Co-Director,