Radiology of Cervical Spine Trauma. Cervical Spine Trauma. Imaging Standards. Canadian C. Spine Rule 11/28/2016
|
|
|
- Matilda Williamson
- 6 years ago
- Views:
Transcription

1 Radiology of Cervical Spine Trauma Dr. Steven J. Gould, D.C. Board Certified Chiropractic Radiologist Cleveland Chiropractic College, KC. MO. Radiology Residency at CCC, KC Cervical Spine Trauma Vertebral column fractures account for 3-6% of all skeletal injuries, mostly in people between yrs and 80% are male. More injuries in thoracic and lumbar regions, but the cervical area has greater potential risk for spinal cord injury. Auto accidents, sports, and falls from heights Imaging Standards Written clinical need for imaging Quality diagnostic images Written radiographic report (not a note in SOAP notes). Check lists are not supported. Incorporation of imaging report in the patient file Canadian C. Spine Rule National Emergency X-Radiography Utilization Study (NEXUS) 1



, anterior")
, dural reflection (6), posterior")
, nuchal ligament")
2 Anatomy Anatomy Anatomy; C.T. Anatomy; MRI Normal anatomy in 43-year-old woman. Sagittal T2-weighted MR image (TR/TE, 4500/117) obtained on 0.3-T MR scanner shows normal apical ligament (1), anterior occipitoatlantal membrane (2), anterior atlantoaxial membrane (3), anterior longitudinal ligament (4), tectorial membrane (5), dural reflection (6), posterior occipitoatlantal membrane (7), posterior atlantoaxial membrane (8), nuchal ligament (9), flaval ligaments (10), area of interspinous ligaments (11), and supraspinous ligament (12). 2









3 Technical Notes Lateral Cervical-- 40inch FFD. Post. Arch C1 over nameplate Technical Notes APOM --patient positioning APLC-- pt. Positioning/tube tilt/collimation Technical Notes REMOVE CLOTHING AND JEWLREY Technical Notes Two views perpendicular---minimum 3



. Measure: At the level of C3, Adam s Apple from front to back.")

4 CERVICAL SPINE POSITIONING PROCEDURES Neutral Lateral Cervical: FFD: 72, kvp: 70,mA: 200 Sec: **Time or mas depends on measurement of patient. Measure in cm. Tube Tilt: None Patient position: Erect with face directed forward. No flexion of chin. Central Ray: C3, just below and behind angle of mandible Measure: Across traps, side to side at level of C7. Breathing: Hold or exhale and hold, to lower shoulders. Misc..; Weights maybe needed to lower shoulders. Neutral Lateral Cervical A-P Lower Cervical: FFD: 40, kvp: 70, ma: 100 Sec: **Time or mas will depend on measurement of the patient. Measure in cm. Tube Tilt: 15 degrees cephalad Patient position: Erect or supine, Anterior to Posterior, Chin elevated slightly. Central Ray: At C3/C4, or the Thyroid (Adam s Apple). Measure: At the level of C3, Adam s Apple from front to back. Breathing: Hold or exhale and hold. AP Lower Cervical A-P Open Mouth: FFD: 40,kVp: 70,mA: 100 Sec: **Time or mas will depend on measurement of the patient. Measure in cm. Tube Tilt: None Patient position: Erect or supine in AP. Mouth open with mastoid process and upper incisor line parallel to floor (central ray). Central Ray: At C1/C2. Through the middle of open mouth Measure: At the level of C3, As for the AP Lower Cervical Breathing: Hold 4






5 A-P Open Mouth Flexion Lateral Cervical: FFD: 72, kvp: 70,mA: 200 Sec: **Time or mas depends on measurement of patient. Measure in cm. Tube Tilt: None Patient position: Erect in lateral position. Chin tucked and head and neck flexed forward to patient tolerance. Done following Cleared Cervical spine. Motion is done by the patient. Central Ray: C3 Measure: Across traps, side to side at level of C7. Breathing: Hold or exhale and hold, to lower shoulders. Misc.; Weights maybe needed to lower shoulders. Flexion Lateral Cervical ***When assisting the patent with positioning. Do not push on the patient s head. This movement is to be done to patient tolerance. Extension Lateral Cervical: FFD: 72, kvp: 70, ma: 200 Sec:**Time or mas depends on measurement of patient. Measure in cm. Tube Tilt: None Patient position: Erect in lateral position. Chin elevated and head and neck extended backward to patient tolerance. Central Ray: C3 Measure: Across traps, side to side at level of C7. Breathing: Hold or exhale and hold, to lower shoulders. Misc.; Weights maybe needed to lower shoulders. Extension Lateral Cervical Left Posterior Oblique Cervical FFD: 72, kvp: 70, ma: 200 Sec: **Time or mas depends on measurement of patient. Measure in cm. Tube Tilt: 15 degrees Cephalad for posterior oblique. Caudal tube tilt for anterior oblique. Patient position: Erect in 45 degree oblique position. Central Ray: C3 Measure: Across traps, side to side at level of C7. SAME AS LATERAL. Breathing: Hold or exhale and hold, to lower shoulders. Misc.; Weights maybe needed to lower shoulders. 5

 Cervical FFD: 72, kvp: 70, ma: 200 Sec: **Time or mas depends on measurement of patient.")



 FFD: 40, kvp: 70, ma: 100 Sec: **Time or mas depends on measurement of patient.")
6 Cervical Oblique Projections Left Posterior Oblique (LPO) shown here. Patient s shoulders and body are rotated 45 degrees. Head is positioned with sagittal plan parallel to film. Chin is slightly elevated to project mandible off of spine. Posterior oblique image demonstrates the opposite side intervertebral foramen (IVF). Anterior obliques show the same side IVFs. Right Posterior Oblique (RPO) Cervical FFD: 72, kvp: 70, ma: 200 Sec: **Time or mas depends on measurement of patient. Measure in cm. Tube Tilt: 15 degrees Cephalad for posterior obls. Caudal tube tilt for anterior obls. Patient position: Erect in an oblique position of 45 degrees rotation. Central Ray: C3 Measure: Across traps, side to side at level of C7. SAME AS LATERAL Breathing: same as for LPO Right Posterior Oblique Cervical Cervical Spine Optional Projections: Swim-Lateral Cervicothoracic projection; Demonstrates the level of C7/T1. AP Open Mouth Lateral Bending Aids in Evaluation of upper cervical stability Pillars Projections; Demonstrate the articular pillars and facet joint spaces. AP Pillars Projections (Left Pillars shown) FFD: 40, kvp: 70, ma: 100 Sec: **Time or mas depends on measurement of patient. Measure in cm. Tube Tilt: 35 degrees Caudal for AP and Cephalad T.T. for PA. Patient position: Erect or supine in AP or PA position. Turn head/face away from side being imaged. Central Ray: C3 Measure: Anterior to posterior with tube tilt. Breathing: Hold or exhale and hold. AP Pillars Projection (left shown) Must do both sides, just as for the oblique projections 6







7 Swim Lateral Cervicothoracic Spot Projection FFD: 40, kvp: 80, ma: 300 Sec: **Time or mas depends on measurement of patient. Measure in cm. Figure technique as a Lateral Lumbar Tube Tilt: None or 10 degree caudal. Patient position: Erect in lateral position. Central Ray: C7/T1, top of clavicle. Measure: Mid-clavicle to shoulder against bucky, to include shoulder. Breathing: Hold or exhale and hold, to lower shoulders. Swim Lateral Cervicothoracic spot projection Patient position: Erect in lateral position. Arm closest to bucky elevated and shoulder away from bucky is lowered, to unsuperimpose the shoulders. Rotation of patient away from the lateral position should be minimized to maintain a lateral view. Breathing: Hold or exhale and hold, to lower shoulders. Additional special projections Swim Lateral Cervicothoracic Spot Projection Compensating filter is necessary of the cervical region, to prevent gross overexposure. The image must be sufficiently exposed however to view the C7/T1 level. 7









8 Lateral cervical with decreased KVP for better demonstration of prevertebral soft tissues. MVC MVC 25 yoa Female Seen at hospital released Chiro. office limited mobilitiy and pain Films obtained. Findings? MVC Lines of Mensuration Chamberlain line Odontoid < 3mm above line McRae line Odontoid below line 8










9 Basilar Impression Lines of Mensuration McGregor s line odontoid < 4.5 mm above Ranawat method C2 pedicle 17mm below the C1 line Apparent Basilar Impression Projectional distortion Signs of Segmental Instability Fanning of spinous processes Loss of parallelism of facet surfaces Disc angle of >11 degrees relative to adjacent discs Anterolisthesis or Retro. of > 3.5mm. ADI > 3mm 9







10 Signs of Segmental Instability Signs of Segmental Instability Angulation between segements >11 degrees Foreman and Croft Whiplash Injuries, pg 147 Arcual kyphosis due to muscle spasm Angular kyphosis due to ligament injury Yochum and Rowe, Essentials of Skeletal Radiology, pg442 Signs of Segmental Instability Soft tissue Injury Flexion/Extension evaluation = instability on flexion at C4/C5. Yochum and Rowe, Essentials of Skeletal Radiology, pg




")



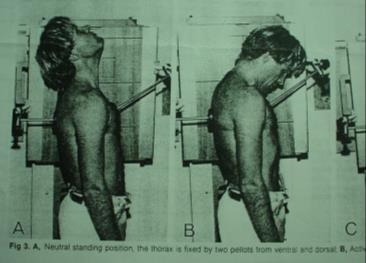
11 Template Analysis Template Analysis Template Analysis Template Analysis C3/C4 Flex C5/C6 Ext C4/C5 Ext Lucent Cleft noted on Extension only Functional Radiographic Diagnosis of the Cervical Spine: Flexion/Extension Dvorak, Froehlich, Penning, Baumgartner, Panjabi, SPINE, Vol. 13, No healthy patients and 31 patients with cervical spine pain and soft tissue injury were studied. Active flexion/extension =19 hypermobile segments and 60 hypomobile segments Passive (forced/stressed) flexion/extension = 31 hypermobile segments and 43 hypomobile segments Immobilized the upper thorax to gain truer motion in the cervical region, without thoracic spine involvement. Used variation of film overlay methods to measure relative segmental positions on flexion/extension films. Functional Radiographic Diagnosis of the Cervical Spine: Flexion/Extension Dvorak, Froehlich, Penning, Baumgartner, Panjabi, SPINE, Vol. 13, No







12 Functional Radiographic Diagnosis of the Cervical Spine: Flexion/Extension Dvorak, Froehlich, Penning, Baumgartner, Panjabi, SPINE, Vol. 13, No Reliability of functional x-ray analysis of cervical vertebrae flexion and Extension. Schops P, Stabler A, et.al. Unfallchirurg 1999 Jul;102(7): Passive functional radiographs of the cervical spine in flexion and extension were taken of 20 patients with painful limitation of mobility of the cervical spine and 20 subjects, similar in sex and age, without complaints. Five physicians measured the angles of segmental mobility in a blind study. The results of the study prove that the evaluation method by Penning shows usable, and,for segments C3/C4 to C6/C7, significant selectivity. The correlation between the five reviewers showed good to very good results The measured values, however, have to be considered, in connection with the appropriate clinical symptoms, as still "normal" or "functionally disordered" in the context of segmental hypo-/hypermobility. Paankhenamun 12
Digital Motion X-ray Cervical Spine
 NAME OF PATIENT: CASE STUDY 4 DATE OF REPORT: DATE OF EXAMINATION: REFERRING PHYSICIAN: TESTING FACILITY: Digital Motion X-ray Cervical Spine 1. In the neutral lateral projection: Shows reversal of the
NAME OF PATIENT: CASE STUDY 4 DATE OF REPORT: DATE OF EXAMINATION: REFERRING PHYSICIAN: TESTING FACILITY: Digital Motion X-ray Cervical Spine 1. In the neutral lateral projection: Shows reversal of the
DIAGNOSTIC VIDEOFLUOROSCOPY IMPRESSIONS and BIOMECHANICS REPORT
 P.O. Box 6743 New Albany, IN 47151-6743 (812) 945-5515 (812) 945-5632 Fax WWW.KMX.CC DIAGNOSTIC VIDEOFLUOROSCOPY IMPRESSIONS and BIOMECHANICS REPORT Patient Name: Lubna Ibriham Date of Digitization and
P.O. Box 6743 New Albany, IN 47151-6743 (812) 945-5515 (812) 945-5632 Fax WWW.KMX.CC DIAGNOSTIC VIDEOFLUOROSCOPY IMPRESSIONS and BIOMECHANICS REPORT Patient Name: Lubna Ibriham Date of Digitization and
LESSON ASSIGNMENT. Positioning for Exams of the Spine. After completing this lesson, you should be able to identify:
 LESSON ASSIGNMENT LESSON 4 Positioning for Exams of the Spine. LESSON ASSIGNMENT Paragraphs 4-1 through 4-15. LESSON OBJECTIVES After completing this lesson, you should be able to identify: 4-1. Identify
LESSON ASSIGNMENT LESSON 4 Positioning for Exams of the Spine. LESSON ASSIGNMENT Paragraphs 4-1 through 4-15. LESSON OBJECTIVES After completing this lesson, you should be able to identify: 4-1. Identify
PREPARED FOR. Marsha Eichhorn DATE OF INJURY : N/A DATE OF ANALYSIS : 12/14/2016 DATE OF IMAGES : 12/8/2016. REFERRING DOCTOR : Dr.
 Accent on Health Chiropractic 405 Firemans Ave PREPARED FOR Marsha Eichhorn DATE OF INJURY : N/A DATE OF ANALYSIS : 12/14/2016 DATE OF IMAGES : 12/8/2016 REFERRING DOCTOR : Dr. David Bohn This report contains
Accent on Health Chiropractic 405 Firemans Ave PREPARED FOR Marsha Eichhorn DATE OF INJURY : N/A DATE OF ANALYSIS : 12/14/2016 DATE OF IMAGES : 12/8/2016 REFERRING DOCTOR : Dr. David Bohn This report contains
How to Determine the Severity of a Spinal Sprain Outline
 Spinal Trauma How to Determine the Severity of a Spinal Sprain Outline Instructor: Dr. Jeffrey A. Cronk, DC, CICE Director of Education, Spinal Kinetics. CICE, American Board of Independent Medical Examiners.
Spinal Trauma How to Determine the Severity of a Spinal Sprain Outline Instructor: Dr. Jeffrey A. Cronk, DC, CICE Director of Education, Spinal Kinetics. CICE, American Board of Independent Medical Examiners.
INDEPENDENT LEARNING: DISC HERNIATION IN THE NATIONAL FOOTBALL LEAGUE: ANATOMICAL FACTORS TO CONSIDER IN REVIEW
 INDEPENDENT LEARNING: DISC HERNIATION IN THE NATIONAL FOOTBALL LEAGUE: ANATOMICAL FACTORS TO CONSIDER IN REVIEW CDC REPORT - CAUSES OF DISABILITY, 2005 REVIEW QUESTIONS ABOUT DISC HERNIATION IN THE NATIONAL
INDEPENDENT LEARNING: DISC HERNIATION IN THE NATIONAL FOOTBALL LEAGUE: ANATOMICAL FACTORS TO CONSIDER IN REVIEW CDC REPORT - CAUSES OF DISABILITY, 2005 REVIEW QUESTIONS ABOUT DISC HERNIATION IN THE NATIONAL
Upper Cervical Spine - Occult Injury and Trigger for CT Exam
 Upper Cervical Spine - Occult Injury and Trigger for CT Exam Main Menu Introduction Clinical clearance of C-SpineC Radiographic evaluation Norms for C-spineC Triggers for CT exam: Odontoid Lateral view
Upper Cervical Spine - Occult Injury and Trigger for CT Exam Main Menu Introduction Clinical clearance of C-SpineC Radiographic evaluation Norms for C-spineC Triggers for CT exam: Odontoid Lateral view
VERTEBRAL COLUMN VERTEBRAL COLUMN
 VERTEBRAL COLUMN FUNCTIONS: 1) Support weight - transmits weight to pelvis and lower limbs 2) Houses and protects spinal cord - spinal nerves leave cord between vertebrae 3) Permits movements - *clinical
VERTEBRAL COLUMN FUNCTIONS: 1) Support weight - transmits weight to pelvis and lower limbs 2) Houses and protects spinal cord - spinal nerves leave cord between vertebrae 3) Permits movements - *clinical
Radiographic Instability Report
 Prepared for: Bad Spine Insurance #: Gender: Male Date of Birth: 8/7/1954 Address: Evaluation Date: 6/29/2013 Date X-Ray Taken: 6/29/2013 Prepared by: Modern Chiropractic Someplace Drive Somewhere Cityville,
Prepared for: Bad Spine Insurance #: Gender: Male Date of Birth: 8/7/1954 Address: Evaluation Date: 6/29/2013 Date X-Ray Taken: 6/29/2013 Prepared by: Modern Chiropractic Someplace Drive Somewhere Cityville,
Spine, October 1, 2003; 28(19): Eythor Kristjansson, Gunnar Leivseth, Paul Brinckmann, Wolfgang Frobin
: Eythor Kristjansson, Gunnar Leivseth, Paul Brinckmann, Wolfgang Frobin") Increased Sagittal Plane Segmental Motion in the Lower Cervical Spine in Women With Chronic Whiplash-Associated Disorders, Grades I-II: A Case-Control Study Using a New Measurement Protocol 1 Spine, October
Increased Sagittal Plane Segmental Motion in the Lower Cervical Spine in Women With Chronic Whiplash-Associated Disorders, Grades I-II: A Case-Control Study Using a New Measurement Protocol 1 Spine, October
Country Health SA Medical Imaging
 Country Health SA Medical Imaging REMOTE OPERATORS POSITIONING GUIDE Contents Image Evaluation Page 4 Positioning Guides Section 1 - THORAX 1.1 Chest Page 5 1.2 Bedside Chest Page 7 1.3 Ribs Page 8 Section
Country Health SA Medical Imaging REMOTE OPERATORS POSITIONING GUIDE Contents Image Evaluation Page 4 Positioning Guides Section 1 - THORAX 1.1 Chest Page 5 1.2 Bedside Chest Page 7 1.3 Ribs Page 8 Section
Clarification of Terms
 Clarification of Terms The Spine, Spinal Column, and Vertebral Column are synonymous terms referring to the bony components housing the spinal cord Spinal Cord = made of nervous tissue Facet = a small,
Clarification of Terms The Spine, Spinal Column, and Vertebral Column are synonymous terms referring to the bony components housing the spinal cord Spinal Cord = made of nervous tissue Facet = a small,
Clarification of Terms
 Clarification of Terms The Spine, Spinal Column, and Vertebral Column are synonymous terms referring to the bony components housing the spinal cord Spinal Cord = made of nervous tissue Facet = a small,
Clarification of Terms The Spine, Spinal Column, and Vertebral Column are synonymous terms referring to the bony components housing the spinal cord Spinal Cord = made of nervous tissue Facet = a small,
Human Anatomy - Problem Drill 06: The Skeletal System Axial Skeleton & Articualtions
 Human Anatomy - Problem Drill 06: The Skeletal System Axial Skeleton & Articualtions Question No. 1 of 10 Instructions: (1) Read the problem and answer choices carefully, (2) Work the problems on paper
Human Anatomy - Problem Drill 06: The Skeletal System Axial Skeleton & Articualtions Question No. 1 of 10 Instructions: (1) Read the problem and answer choices carefully, (2) Work the problems on paper
'Objective Spinal Motion Unit Assessment through AMA Precision Compliant Procedures' Computer Aided Radiographic Mensuration Analysis
 PATIENT'S NAME: New, Patient REFERRED BY: Dr. Example, DC DATE OF FILMS: 12/21/2011 DOB: 0/00/0000 AGE: D.O.S. 'Objective Spinal Motion Unit Assessment through AMA Precision Compliant Procedures' Computer
PATIENT'S NAME: New, Patient REFERRED BY: Dr. Example, DC DATE OF FILMS: 12/21/2011 DOB: 0/00/0000 AGE: D.O.S. 'Objective Spinal Motion Unit Assessment through AMA Precision Compliant Procedures' Computer
Imaging of Cervical Spine Trauma Tudor H Hughes, M.D.
 Imaging of Cervical Spine Trauma Tudor H Hughes, M.D. General Considerations Most spinal fractures are due to a single episode of major trauma. Fatigue fractures of the spine are unusual except in the
Imaging of Cervical Spine Trauma Tudor H Hughes, M.D. General Considerations Most spinal fractures are due to a single episode of major trauma. Fatigue fractures of the spine are unusual except in the
Mechanism of Injury, Trauma, Subluxation and Instability Outline
 Spinal Trauma Instructor: Dr. Jeffrey A. Cronk, DC, CICE Director of Education, Spinal Kinetics. CICE, American Board of Independent Medical Examiners. Mechanism of Injury is just something that you must
Spinal Trauma Instructor: Dr. Jeffrey A. Cronk, DC, CICE Director of Education, Spinal Kinetics. CICE, American Board of Independent Medical Examiners. Mechanism of Injury is just something that you must
Dr Ajit Singh Moderator Dr P S Chandra Dr Rajender Kumar
 BIOMECHANICS OF SPINE Dr Ajit Singh Moderator Dr P S Chandra Dr Rajender Kumar What is biomechanics? Biomechanics is the study of the consequences of application of external force on the spine Primary
BIOMECHANICS OF SPINE Dr Ajit Singh Moderator Dr P S Chandra Dr Rajender Kumar What is biomechanics? Biomechanics is the study of the consequences of application of external force on the spine Primary
Anterior Cervical Subluxation: An Unstable Position
 275 Anterior Cervical Subluxation: An Unstable Position, 1 A. T. Scher1 The radioiogic signs of cervical anterior subluxation are subtle. Even when recognized, the injury may not be considered significant.
275 Anterior Cervical Subluxation: An Unstable Position, 1 A. T. Scher1 The radioiogic signs of cervical anterior subluxation are subtle. Even when recognized, the injury may not be considered significant.
2. The vertebral arch is composed of pedicles (projecting from the body) and laminae (uniting arch posteriorly).
 and laminae (uniting arch posteriorly).") VERTEBRAL COLUMN 2018zillmusom I. VERTEBRAL COLUMN - functions to support weight of body and protect spinal cord while permitting movements of trunk and providing for muscle attachments. A. Typical vertebra
VERTEBRAL COLUMN 2018zillmusom I. VERTEBRAL COLUMN - functions to support weight of body and protect spinal cord while permitting movements of trunk and providing for muscle attachments. A. Typical vertebra
Clarification of Terms
 Clarification of Terms The Spine, Spinal Column, and Vertebral Column are synonymous terms referring to the bony components housing the spinal cord Spinal Cord = made of nervous tissue Facet = a small,
Clarification of Terms The Spine, Spinal Column, and Vertebral Column are synonymous terms referring to the bony components housing the spinal cord Spinal Cord = made of nervous tissue Facet = a small,
Subaxial Cervical Spine Trauma. Introduction. Anatomic Considerations 7/23/2018
 Subaxial Cervical Spine Trauma Sheyan J. Armaghani, MD Florida Orthopedic Institute Assistant Professor USF Dept of Orthopedics Introduction Trauma to the cervical spine accounts for 5 of all spine injuries
Subaxial Cervical Spine Trauma Sheyan J. Armaghani, MD Florida Orthopedic Institute Assistant Professor USF Dept of Orthopedics Introduction Trauma to the cervical spine accounts for 5 of all spine injuries
The vault bones Frontal Parietals Occiput Temporals Sphenoid Ethmoid
 The Vertebral Column Head, Neck and Spine Bones of the head Some consider the bones of the head in terms of the vault bones and the facial bones hanging off the front of them The vault bones Frontal Parietals
The Vertebral Column Head, Neck and Spine Bones of the head Some consider the bones of the head in terms of the vault bones and the facial bones hanging off the front of them The vault bones Frontal Parietals
3 Movements of the Trunk. Flexion Rotation Extension
 3 Movements of the Trunk Flexion Rotation Extension 1 TRUNK FLEXION 2 TRUNK FLEXION: Rectus Abdominalis O: Crest of Pubis & ligaments covering front of symphysis pubis. I: By «3 portions into cartilages
3 Movements of the Trunk Flexion Rotation Extension 1 TRUNK FLEXION 2 TRUNK FLEXION: Rectus Abdominalis O: Crest of Pubis & ligaments covering front of symphysis pubis. I: By «3 portions into cartilages
The Trunk and Spinal Column Kinesiology Cuneyt Mirzanli Istanbul Gelisim University
 The Trunk and Spinal Column Kinesiology Cuneyt Mirzanli Istanbul Gelisim University The Trunk and Spinal Column Vertebral column 24 articulating vertebrae 31 pairs of spinal nerves Abdominal muscles some
The Trunk and Spinal Column Kinesiology Cuneyt Mirzanli Istanbul Gelisim University The Trunk and Spinal Column Vertebral column 24 articulating vertebrae 31 pairs of spinal nerves Abdominal muscles some
Thoracic and Lumbar Spine Anatomy.
 Thoracic and Lumbar Spine Anatomy www.fisiokinesiterapia.biz Thoracic Vertebrae Bodies Pedicles Laminae Spinous Processes Transverse Processes Inferior & Superior Facets Distinguishing Feature Costal Fovea
Thoracic and Lumbar Spine Anatomy www.fisiokinesiterapia.biz Thoracic Vertebrae Bodies Pedicles Laminae Spinous Processes Transverse Processes Inferior & Superior Facets Distinguishing Feature Costal Fovea
May have excessive movement in the unfused segment to compensate. Flexion extension better preserved than lateral bend or rotation
 IV CONGENITAL SPINE KLIPPEL FLAIL SYNDROME Prevalence 0.60% Mainly around upper 3 vertebrae [75%] Commonest: C2 3 Lower Cervical spine fusion may be associated with syndromes: Fetal alcohol syndrome Goldenhar
IV CONGENITAL SPINE KLIPPEL FLAIL SYNDROME Prevalence 0.60% Mainly around upper 3 vertebrae [75%] Commonest: C2 3 Lower Cervical spine fusion may be associated with syndromes: Fetal alcohol syndrome Goldenhar
OMT Without An OMT Table Workshop. Dennis Dowling, DO FAAO Ann Habenicht, DO FAAO FACOFP
 OMT Without An OMT Table Workshop Dennis Dowling, DO FAAO Ann Habenicht, DO FAAO FACOFP Cervical Somatic Dysfunction (C5 SR RR) - Seated 1. Patient position: seated. 2. Physician position: standing facing
OMT Without An OMT Table Workshop Dennis Dowling, DO FAAO Ann Habenicht, DO FAAO FACOFP Cervical Somatic Dysfunction (C5 SR RR) - Seated 1. Patient position: seated. 2. Physician position: standing facing
Human Anatomy and Physiology - Problem Drill 07: The Skeletal System Axial Skeleton
 Human Anatomy and Physiology - Problem Drill 07: The Skeletal System Axial Skeleton Question No. 1 of 10 Which of the following statements about the axial skeleton is correct? Question #01 A. The axial
Human Anatomy and Physiology - Problem Drill 07: The Skeletal System Axial Skeleton Question No. 1 of 10 Which of the following statements about the axial skeleton is correct? Question #01 A. The axial
Bony Thorax. Anatomy and Procedures of the Bony Thorax Edited by M. Rhodes
 Bony Thorax Anatomy and Procedures of the Bony Thorax 10-526-191 Edited by M. Rhodes Anatomy Review Bony Thorax Formed by Sternum 12 pairs of ribs 12 thoracic vertebrae Conical in shape Narrow at top Posterior
Bony Thorax Anatomy and Procedures of the Bony Thorax 10-526-191 Edited by M. Rhodes Anatomy Review Bony Thorax Formed by Sternum 12 pairs of ribs 12 thoracic vertebrae Conical in shape Narrow at top Posterior
Raymond Wiegand, D.C. Spine Rehabilitation Institute of Missouri
 2D Pattern matching of frontal plane radiograph to 3D model identifies structural and functional deficiencies of the spinal pelvic system in consideration of mechanical spine pain (AKA Spine distortion
2D Pattern matching of frontal plane radiograph to 3D model identifies structural and functional deficiencies of the spinal pelvic system in consideration of mechanical spine pain (AKA Spine distortion
Subaxial Cervical Spine Trauma Dr Hesarikia BUMS
 Subaxial Cervical Spine Trauma Dr. Hesarikia BUMS Subaxial Cervical Spine From C3-C7 ROM Majority of cervical flexion Lateral bending Approximately 50% rotation Ligamentous Anatomy Anterior ALL, PLL, intervertebral
Subaxial Cervical Spine Trauma Dr. Hesarikia BUMS Subaxial Cervical Spine From C3-C7 ROM Majority of cervical flexion Lateral bending Approximately 50% rotation Ligamentous Anatomy Anterior ALL, PLL, intervertebral
THE VERTEBRAL COLUMN. Average adult length: In male: about 70 cms. In female: about 65 cms.
 THE VERTEBRAL COLUMN Average adult length: In male: about 70 cms. In female: about 65 cms. 1 Vertebral Column (Regions and Curvatures) Curvatures of the vertebral column: A. Primary curvature: C-shaped;
THE VERTEBRAL COLUMN Average adult length: In male: about 70 cms. In female: about 65 cms. 1 Vertebral Column (Regions and Curvatures) Curvatures of the vertebral column: A. Primary curvature: C-shaped;
VIRGINIA ORTHOPEDIC MANUAL PHYSICAL THERAPY INSTITUTE TECHNIQUE MANUAL
 VIRGINIA ORTHOPEDIC MANUAL PHYSICAL THERAPY INSTITUTE TECHNIQUE MANUAL Lumbar and Thoracic Spine Lumbar AROM Assessment -Patient Positioning: Standing, appropriately undressed so that the lumbar and thoracic
VIRGINIA ORTHOPEDIC MANUAL PHYSICAL THERAPY INSTITUTE TECHNIQUE MANUAL Lumbar and Thoracic Spine Lumbar AROM Assessment -Patient Positioning: Standing, appropriately undressed so that the lumbar and thoracic
River North Pain Management Consultants, S.C., Axel Vargas, M.D., Regional Anesthesiology and Interventional Pain Management.
 River North Pain Management Consultants, S.C., Axel Vargas, M.D., Regional Anesthesiology and Interventional Pain Management. Chicago, Illinois, 60611 Phone: (888) 951-6471 Fax: (888) 961-6471 Clinical
River North Pain Management Consultants, S.C., Axel Vargas, M.D., Regional Anesthesiology and Interventional Pain Management. Chicago, Illinois, 60611 Phone: (888) 951-6471 Fax: (888) 961-6471 Clinical
Outline. Epidemiology Indications for C-spine imaging Modalities Interpretation Types of fractures
 C-Spine Plain Films Outline Epidemiology Indications for C-spine imaging Modalities Interpretation Types of fractures Epidemiology 7000-10000 c-spine injuries treated each year Additional 5000 die at the
C-Spine Plain Films Outline Epidemiology Indications for C-spine imaging Modalities Interpretation Types of fractures Epidemiology 7000-10000 c-spine injuries treated each year Additional 5000 die at the
PREOPERATIVE RETROLISTHESIS IS A RISK FACTOR OF LUMBAR DISC HERNIATION AFTER FENESTRATION WITHOUT DISCECTOMY
 PREOPERATIVE RETROLISTHESIS IS A RISK FACTOR OF LUMBAR DISC HERNIATION AFTER FENESTRATION WITHOUT DISCECTOMY Shota Takenaka*, Noboru Hosono, Yoshihiro Mukai, Kosuke Tateishi, Takeshi Fuji Osaka Kosei-nenkin
PREOPERATIVE RETROLISTHESIS IS A RISK FACTOR OF LUMBAR DISC HERNIATION AFTER FENESTRATION WITHOUT DISCECTOMY Shota Takenaka*, Noboru Hosono, Yoshihiro Mukai, Kosuke Tateishi, Takeshi Fuji Osaka Kosei-nenkin
Posture. Kinesiology RHS 341 Lecture 10 Dr. Einas Al-Eisa
 Posture Kinesiology RHS 341 Lecture 10 Dr. Einas Al-Eisa Posture = body alignment = the relative arrangement of parts of the body Changes with the positions and movements of the body throughout the day
Posture Kinesiology RHS 341 Lecture 10 Dr. Einas Al-Eisa Posture = body alignment = the relative arrangement of parts of the body Changes with the positions and movements of the body throughout the day
It consist of two components: the outer, laminar fibrous container (or annulus), and the inner, semifluid mass (the nucleus pulposus).
, and the inner, semifluid mass (the nucleus pulposus).") Lumbar Spine The lumbar vertebrae are the last five vertebrae of the vertebral column. They are particularly large and heavy when compared with the vertebrae of the cervical or thoracicc spine. Their bodies
Lumbar Spine The lumbar vertebrae are the last five vertebrae of the vertebral column. They are particularly large and heavy when compared with the vertebrae of the cervical or thoracicc spine. Their bodies
Fluoroscopically Guided Cervical Prolotherapy for Instability with Blinded Pre and Post Radiographic Reading
 Centeno et al Prolotherapy for Cervical Instability 67 Pain Physician. 2005;8:67-72, ISSN 1533-3159 A Case Series Fluoroscopically Guided Cervical Prolotherapy for Instability with Blinded Pre and Post
Centeno et al Prolotherapy for Cervical Instability 67 Pain Physician. 2005;8:67-72, ISSN 1533-3159 A Case Series Fluoroscopically Guided Cervical Prolotherapy for Instability with Blinded Pre and Post
Comprehension of the common spine disorder.
 Objectives Comprehension of the common spine disorder. Disc degeneration/hernia. Spinal stenosis. Common spinal deformity (Spondylolisthesis, Scoliosis). Osteoporotic fracture. Anatomy Anatomy Anatomy
Objectives Comprehension of the common spine disorder. Disc degeneration/hernia. Spinal stenosis. Common spinal deformity (Spondylolisthesis, Scoliosis). Osteoporotic fracture. Anatomy Anatomy Anatomy
Radiology Positioning Practical Test #2 Table (By Jung Park):
:") Radiology Positioning Practical Test #2 Table (By Jung Park): (Lower Extremity): patient is fully gowned / no artifacts / properly shielded (exposure for femur and below : hold still, don t move ) (exposure
Radiology Positioning Practical Test #2 Table (By Jung Park): (Lower Extremity): patient is fully gowned / no artifacts / properly shielded (exposure for femur and below : hold still, don t move ) (exposure
Cervical Spine Anatomy and Biomechanics. Typical Cervical Vertebra C3 6. Typical Cervical Vertebra Anterior 10/5/2017
 Cervical Spine Anatomy and Biomechanics Typical Cervical Vertebra C3 6 Small, relatively broad body Bifid SpinousProcess Long and narrow laminae Spinal Canal: large, triangular; remarkably consistent dimensions
Cervical Spine Anatomy and Biomechanics Typical Cervical Vertebra C3 6 Small, relatively broad body Bifid SpinousProcess Long and narrow laminae Spinal Canal: large, triangular; remarkably consistent dimensions
Structure and Function of the Vertebral Column
 Structure and Function of the Vertebral Column Posture Vertebral Alignment Does it really matter? Yes it does! Postural Curves The vertebral column has a series of counterbalancing curves posterior anterior
Structure and Function of the Vertebral Column Posture Vertebral Alignment Does it really matter? Yes it does! Postural Curves The vertebral column has a series of counterbalancing curves posterior anterior
P V S MEMORIAL HOSPITAL LTD.
 SHOULDER XRAYS Instability Series o True AP (Grashey s) o Axillary o Stryker Notch view o True AP in Internal rotation o Scapular Y view o West Point view for Bony Bankart ( looks like modif axillary view)
SHOULDER XRAYS Instability Series o True AP (Grashey s) o Axillary o Stryker Notch view o True AP in Internal rotation o Scapular Y view o West Point view for Bony Bankart ( looks like modif axillary view)
Fractures of the thoracic and lumbar spine and thoracolumbar transition
 Most spinal column injuries occur in the thoracolumbar transition, the area between the lower thoracic spine and the upper lumbar spine; over half of all vertebral fractures involve the 12 th thoracic
Most spinal column injuries occur in the thoracolumbar transition, the area between the lower thoracic spine and the upper lumbar spine; over half of all vertebral fractures involve the 12 th thoracic
SUBAXIAL CERVICAL SPINE TRAUMA- DIAGNOSIS AND MANAGEMENT
 SUBAXIAL CERVICAL SPINE TRAUMA- DIAGNOSIS AND MANAGEMENT 1 Anatomy 3 columns- Anterior, middle and Posterior Anterior- ALL, Anterior 2/3 rd body & disc. Middle- Posterior 1/3 rd of body & disc, PLL Posterior-
SUBAXIAL CERVICAL SPINE TRAUMA- DIAGNOSIS AND MANAGEMENT 1 Anatomy 3 columns- Anterior, middle and Posterior Anterior- ALL, Anterior 2/3 rd body & disc. Middle- Posterior 1/3 rd of body & disc, PLL Posterior-
CERVICAL SPINE: Radiographs and MRI Cases
 www.jprad.com Radiology reports with recommendations & clinical information - $30 per region, x-ray - $50 per MRI - Medpay Monthly Newsletter 700 East Redlands Blvd, Redlands CA 92373 909.353.9348 jpedley299@yahoo.com
www.jprad.com Radiology reports with recommendations & clinical information - $30 per region, x-ray - $50 per MRI - Medpay Monthly Newsletter 700 East Redlands Blvd, Redlands CA 92373 909.353.9348 jpedley299@yahoo.com
Ligaments of the vertebral column:
 In the last lecture we started talking about the joints in the vertebral column, and we said that there are two types of joints between adjacent vertebrae: 1. Between the bodies of the vertebrae; which
In the last lecture we started talking about the joints in the vertebral column, and we said that there are two types of joints between adjacent vertebrae: 1. Between the bodies of the vertebrae; which
WEEKEND 1 CERVICAL SPINE
 Virginia Orthopedic Manual Physical Therapy Institute - Technique Manual WEEKEND 1 CERVICAL SPINE Cervical Active Range of Motion Testing Rotation CT Flexion Mid Cervical Flexion Extension Side-Bending
Virginia Orthopedic Manual Physical Therapy Institute - Technique Manual WEEKEND 1 CERVICAL SPINE Cervical Active Range of Motion Testing Rotation CT Flexion Mid Cervical Flexion Extension Side-Bending
VERTEBRAL COLUMN ANATOMY IN CNS COURSE
 VERTEBRAL COLUMN ANATOMY IN CNS COURSE Vertebral body Sections of the spine Atlas (C1) Axis (C2) What type of joint is formed between atlas and axis? Pivot joint What name is given to a fracture of both
VERTEBRAL COLUMN ANATOMY IN CNS COURSE Vertebral body Sections of the spine Atlas (C1) Axis (C2) What type of joint is formed between atlas and axis? Pivot joint What name is given to a fracture of both
Proteus XR/f Patient positioning guide
 Proteus XR/f Patient positioning guide PROTEUS XR/F Now a single digital x-ray room accommodates nearly all your radiographic studies. With extended tube coverage and wireless detectors, Proteus XR/f gives
Proteus XR/f Patient positioning guide PROTEUS XR/F Now a single digital x-ray room accommodates nearly all your radiographic studies. With extended tube coverage and wireless detectors, Proteus XR/f gives
Types of Body Movements
 Types of Body Movements Bởi: OpenStaxCollege Synovial joints allow the body a tremendous range of movements. Each movement at a synovial joint results from the contraction or relaxation of the muscles
Types of Body Movements Bởi: OpenStaxCollege Synovial joints allow the body a tremendous range of movements. Each movement at a synovial joint results from the contraction or relaxation of the muscles
Cervical Spine Exercise and Manual Therapy for the Autonomous Practitioner
 Cervical Spine Exercise and Manual Therapy for the Autonomous Practitioner Eric Chaconas PT, PhD, DPT, FAAOMPT Assistant Professor and Assistant Program Director Doctor of Physical Therapy Program Eric
Cervical Spine Exercise and Manual Therapy for the Autonomous Practitioner Eric Chaconas PT, PhD, DPT, FAAOMPT Assistant Professor and Assistant Program Director Doctor of Physical Therapy Program Eric
The Back. Anatomy RHS 241 Lecture 9 Dr. Einas Al-Eisa
 The Back Anatomy RHS 241 Lecture 9 Dr. Einas Al-Eisa The spine has to meet 2 functions Strength Mobility Stability of the vertebral column is provided by: Deep intrinsic muscles of the back Ligaments
The Back Anatomy RHS 241 Lecture 9 Dr. Einas Al-Eisa The spine has to meet 2 functions Strength Mobility Stability of the vertebral column is provided by: Deep intrinsic muscles of the back Ligaments
Anatomy notes-thorax.
 Anatomy notes-thorax. Thorax: the part extending from the root of the neck to the abdomen. Parts of the thorax: - Thoracic cage (bones). - Thoracic wall. - Thoracic cavity. ** The thoracic cavity is covered
Anatomy notes-thorax. Thorax: the part extending from the root of the neck to the abdomen. Parts of the thorax: - Thoracic cage (bones). - Thoracic wall. - Thoracic cavity. ** The thoracic cavity is covered
Anatomy and Physiology II. Spine
 Anatomy and Physiology II Spine Bones and Other Structures Vertibrae Contains Cervical, Thoracic, Lumbar, Sacral and Coccygeal regions We use Capital letters to refer to these (C, T, L, S, and Co) and
Anatomy and Physiology II Spine Bones and Other Structures Vertibrae Contains Cervical, Thoracic, Lumbar, Sacral and Coccygeal regions We use Capital letters to refer to these (C, T, L, S, and Co) and
Chiropractic Glossary
 Chiropractic Glossary Anatomy Articulation: A joint formed where two or more bones in the body meet. Your foot bone, for example, forms an articulation with your leg bone. You call that articulation an
Chiropractic Glossary Anatomy Articulation: A joint formed where two or more bones in the body meet. Your foot bone, for example, forms an articulation with your leg bone. You call that articulation an
OMT Without The Table Saroj Misra, DO, FACOFP and Marissa Rogers, DO
 OMT Without The Table Saroj Misra, DO, FACOFP and Marissa Rogers, DO Why bother? May not always have the table present Patient may not be able to lay prone or supine Some techniques may be easier to accomplish
OMT Without The Table Saroj Misra, DO, FACOFP and Marissa Rogers, DO Why bother? May not always have the table present Patient may not be able to lay prone or supine Some techniques may be easier to accomplish
Cervical Spine Injury Guidelines
 6/15/2018 Cervical Spine Injury Guidelines Benjamin Oshlag, MD, CAQSM Assistant Professor of Emergency Medicine Assistant Professor of Sports Medicine Columbia University Medical Center Nothing to Disclose
6/15/2018 Cervical Spine Injury Guidelines Benjamin Oshlag, MD, CAQSM Assistant Professor of Emergency Medicine Assistant Professor of Sports Medicine Columbia University Medical Center Nothing to Disclose
Thoracolumbar Spine Fractures
 Thoracolumbar Spine Fractures C. Craig Blackmore, MD, MPH Professor of Radiology Adjunct Professor of Health Services Harborview Injury Prevention and Research Center University of Washington Outline Who
Thoracolumbar Spine Fractures C. Craig Blackmore, MD, MPH Professor of Radiology Adjunct Professor of Health Services Harborview Injury Prevention and Research Center University of Washington Outline Who
3/10/17 Spinal a Injury 1
 Spinal Injury 1 'Paralysed' Watmough vows he'll have the backbone for Game Two after treatment for neck injury Watmough will have cortisone injected into his spine this morning to speed up the recovery
Spinal Injury 1 'Paralysed' Watmough vows he'll have the backbone for Game Two after treatment for neck injury Watmough will have cortisone injected into his spine this morning to speed up the recovery
2017 COS ANNUAL MEETING AND EXHIBITION HOME EXERCISES
 UPPER BODY Push Up From a push up position. Lower whole body down to floor. Press up to return to start position. Maintain abdominal hollow and neutral spinal alignment throughout movement. Note: Perform
UPPER BODY Push Up From a push up position. Lower whole body down to floor. Press up to return to start position. Maintain abdominal hollow and neutral spinal alignment throughout movement. Note: Perform
Thoracolumbar Anatomy Eric Shamus Catherine Patla Objectives
 1 2 Thoracolumbar Anatomy Eric Shamus Catherine Patla Objectives List the muscular and ligamentous attachments of the thoracic and lumbar spine Describe how the muscles affect the spine and upper extremity
1 2 Thoracolumbar Anatomy Eric Shamus Catherine Patla Objectives List the muscular and ligamentous attachments of the thoracic and lumbar spine Describe how the muscles affect the spine and upper extremity
Ultimate Spinal Analysis PA USA-XRAY ( )
") Page: 1 Spine Atlas Angle 7.24 S Atlas Angle 21.67 S The Atlas Angle is a measurement of the stability of the Atlas. The Atlas Plane Line is compared to true horizontal. Any increase or decrease of this
Page: 1 Spine Atlas Angle 7.24 S Atlas Angle 21.67 S The Atlas Angle is a measurement of the stability of the Atlas. The Atlas Plane Line is compared to true horizontal. Any increase or decrease of this
Passive Intervertebral Mobilization
 Passive Intervertebral Mobilization Terry Rose DPT, FAAOMPT, Cert, MDT Guide to Physical Therapy Practice Section 4D-Impairment/Connective Tissue Dysfunction Section 4E,4F,4G,4H,4I,4J Impaired Joint Mobility
Passive Intervertebral Mobilization Terry Rose DPT, FAAOMPT, Cert, MDT Guide to Physical Therapy Practice Section 4D-Impairment/Connective Tissue Dysfunction Section 4E,4F,4G,4H,4I,4J Impaired Joint Mobility
Evidence- Based Examination of the Lumbar Spine Presented by Chad Cook, PT, PhD, MBA, FAAOMPT Practice Sessions/Skill Check- offs
 Evidence- Based Examination of the Lumbar Spine Presented by Chad Cook, PT, PhD, MBA, FAAOMPT Practice Sessions/Skill Check- offs Chapter Five: Movement Examination of the Lumbar Spine Time) (45 minutes
Evidence- Based Examination of the Lumbar Spine Presented by Chad Cook, PT, PhD, MBA, FAAOMPT Practice Sessions/Skill Check- offs Chapter Five: Movement Examination of the Lumbar Spine Time) (45 minutes
Thoracic Spine Applied Anatomy. Jason Zafereo, PT, OCS, FAAOMPT
 Thoracic Spine Applied Anatomy Jason Zafereo, PT, OCS, FAAOMPT Clinical i l Orthopedic Rehabilitation ti Education Objectives Discuss concepts relevant to thoracic pain of red flag origin Discuss concepts
Thoracic Spine Applied Anatomy Jason Zafereo, PT, OCS, FAAOMPT Clinical i l Orthopedic Rehabilitation ti Education Objectives Discuss concepts relevant to thoracic pain of red flag origin Discuss concepts
Objectives. Comprehension of the common spine disorder
 Objectives Comprehension of the common spine disorder Disc degeneration/hernia Spinal stenosis Common spinal deformity (Spondylolisthesis, Scoliosis) Osteoporotic fracture Destructive spinal lesions Anatomy
Objectives Comprehension of the common spine disorder Disc degeneration/hernia Spinal stenosis Common spinal deformity (Spondylolisthesis, Scoliosis) Osteoporotic fracture Destructive spinal lesions Anatomy
Subaxial Cervical Spine Trauma
 Subaxial Cervical Spine Trauma Pooria Salari, MD Assistant Professor Of Orthopaedics Department of Orthopaedic Surgery St. Louis University School of Medicine St. Louis, Missouri, USA Initial Evaluation
Subaxial Cervical Spine Trauma Pooria Salari, MD Assistant Professor Of Orthopaedics Department of Orthopaedic Surgery St. Louis University School of Medicine St. Louis, Missouri, USA Initial Evaluation
REVIEW QUESTIONS ON VERTEBRAE, SPINAL CORD, SPINAL NERVES
 REVIEW QUESTIONS ON VERTEBRAE, SPINAL CORD, SPINAL NERVES 1. A 28-year-old-women presented to the hospital emergency room with intense lower back spasms in the context of coughing during an upper respiratory
REVIEW QUESTIONS ON VERTEBRAE, SPINAL CORD, SPINAL NERVES 1. A 28-year-old-women presented to the hospital emergency room with intense lower back spasms in the context of coughing during an upper respiratory
The trunk and spinal column. Functions of Spine. Bones 6/5/2017. Chapter 10. Consider the complexity of functions. 33 bones of the spine
 The trunk and spinal column Chapter 10 Functions of Spine Consider the complexity of functions provides stability to a cylinder permits movement in all directions supports structures of considerable weight
The trunk and spinal column Chapter 10 Functions of Spine Consider the complexity of functions provides stability to a cylinder permits movement in all directions supports structures of considerable weight
Case Report: CASE REPORT OF FACET ARTHROPATHY INDUCED NERVE ROOT COMPRESSION RESULTING IN MOTOR WEAKNESS AND PAIN
 Cox Technic Case Report #100 published at www.coxtechnic.com (sent October 2011 on 10/11/11 ) 1 Case Report: CASE REPORT OF FACET ARTHROPATHY INDUCED NERVE ROOT COMPRESSION RESULTING IN MOTOR WEAKNESS
Cox Technic Case Report #100 published at www.coxtechnic.com (sent October 2011 on 10/11/11 ) 1 Case Report: CASE REPORT OF FACET ARTHROPATHY INDUCED NERVE ROOT COMPRESSION RESULTING IN MOTOR WEAKNESS
1/15/2012. Cervical Spine Trauma. Who to Image. Who to Image. Who to Image. Who to Image. Trauma Cx Spine Protocols NEXUS. CCR and Nexus CCR CCR
 Trauma Cx Spine Protocols Cervical Spine Trauma Issues The clinically negative Cx-spine Does everyone need a CT Dr. Tudor H. Hughes M.D., FRCR Department of Radiology University of California School of
Trauma Cx Spine Protocols Cervical Spine Trauma Issues The clinically negative Cx-spine Does everyone need a CT Dr. Tudor H. Hughes M.D., FRCR Department of Radiology University of California School of
Whiplash Associated Disorders (WAD) Instability & Case Studies
 Instability & Case Studies") Whiplash Associated Disorders (WAD) Instability & Case Studies Steven G. Yeomans, DC, FACO 404 Eureka Street Ripon, WI 64971-0263 920-748-3644 (Ph) 920-748-3642 (Fax) sgyeomansdc@gmail.com www.yeomansdc.com
Whiplash Associated Disorders (WAD) Instability & Case Studies Steven G. Yeomans, DC, FACO 404 Eureka Street Ripon, WI 64971-0263 920-748-3644 (Ph) 920-748-3642 (Fax) sgyeomansdc@gmail.com www.yeomansdc.com
factor for identifying unstable thoracolumbar fractures. There are clinical and radiological criteria
 NMJ-Vol :2/ Issue:1/ Jan June 2013 Case Report Medical Sciences Progressive subluxation of thoracic wedge compression fracture with unidentified PLC injury Dr.Thalluri.Gopala krishnaiah* Dr.Voleti.Surya
NMJ-Vol :2/ Issue:1/ Jan June 2013 Case Report Medical Sciences Progressive subluxation of thoracic wedge compression fracture with unidentified PLC injury Dr.Thalluri.Gopala krishnaiah* Dr.Voleti.Surya
Routine Guide EXAMINATION PROJECTION CASSETTE SIZE NOTES PRINT ORIENTATION. 14x17 CW* 14x17LW 14x17LW. 14x17LW 14x17LW 14x17LW
 EXAMINATION PROJECTION CASSETTE SIZE NOTES PRINT ORIENTATION A-C Joints without weights with weights 14x17 CW* One 14x17 divided; both shoulders on one exposure. *If part does not fit, do 10x12s CW. Both
EXAMINATION PROJECTION CASSETTE SIZE NOTES PRINT ORIENTATION A-C Joints without weights with weights 14x17 CW* One 14x17 divided; both shoulders on one exposure. *If part does not fit, do 10x12s CW. Both
The Thoracic Cage ANATOMY 2: THORACIC CAGE AND VERTEBRAL COLUMN
 ANATOMY 2: THORACIC CAGE AND VERTEBRAL COLUMN PSK 4U Mr. S. Kelly North Grenville DHS The Thoracic Cage 7 true ribs 3 false ribs 2 floating ribs Clavicle = collarbone Manubrium Sternum Xiphoid Process
ANATOMY 2: THORACIC CAGE AND VERTEBRAL COLUMN PSK 4U Mr. S. Kelly North Grenville DHS The Thoracic Cage 7 true ribs 3 false ribs 2 floating ribs Clavicle = collarbone Manubrium Sternum Xiphoid Process
Imaging Decision Making: Recommended Radiographic Projections
 WSCC Clinics Protocol Adopted: 3/05 Imaging Decision Making: Recommended Radiographic Projections This document lists the routine, supplemental and alternative projections performed in the Diagnostic Imaging
WSCC Clinics Protocol Adopted: 3/05 Imaging Decision Making: Recommended Radiographic Projections This document lists the routine, supplemental and alternative projections performed in the Diagnostic Imaging
102 Results RESULTS. Age Mean=S.D Range 42= years -84 years Number % <30 years years >50 years
 102 Results RESULTS A total of 50 cases were studied 39 males and 11females.Their age ranged between 16 years and 84 years (mean 42years). T1 and T2WI were acquired for all cases in sagittal and axial
102 Results RESULTS A total of 50 cases were studied 39 males and 11females.Their age ranged between 16 years and 84 years (mean 42years). T1 and T2WI were acquired for all cases in sagittal and axial
Thoracic Spine Applied Anatomy. Jason Zafereo, PT, OCS, FAAOMPT
 Thoracic Spine Applied Anatomy Jason Zafereo, PT, OCS, FAAOMPT Clinical i l Orthopedic Rehabilitation ti Education 1 Objectives Discuss red flag signs for the thoracic region Apply key concepts from the
Thoracic Spine Applied Anatomy Jason Zafereo, PT, OCS, FAAOMPT Clinical i l Orthopedic Rehabilitation ti Education 1 Objectives Discuss red flag signs for the thoracic region Apply key concepts from the
Hands PA; Obl. Lat.; Norgaard s Thumb AP; Lat. PA. PA; Lat.: Obls.; Elongated PA with ulnar deviation
 Projections Region Basic projections Additional / Modified projections Upper Limbs Hands PA; Obl. Lat.; Norgaard s Thumb ; Lat. PA Fingers PA; Lat. Wrist PA; Lat. Obls. Scaphoid Lunate Trapezium Triquetral
Projections Region Basic projections Additional / Modified projections Upper Limbs Hands PA; Obl. Lat.; Norgaard s Thumb ; Lat. PA Fingers PA; Lat. Wrist PA; Lat. Obls. Scaphoid Lunate Trapezium Triquetral
Back To Chiropractic CE Seminars Back to Basics: X-Ray ~ 5 Hours
 Back To Chiropractic CE Seminars Back to Basics: X-Ray ~ 5 Hours Welcome to Back To Chiropractic Online CE exams: This course counts toward your California Board of Chiropractic Examiners CE & your Radiography
Back To Chiropractic CE Seminars Back to Basics: X-Ray ~ 5 Hours Welcome to Back To Chiropractic Online CE exams: This course counts toward your California Board of Chiropractic Examiners CE & your Radiography
Vertebral Column. Backbone consists of 26 vertebrae. Five vertebral regions. Cervical
 Vertebral Column Backbone consists of 26 vertebrae. Five vertebral regions Cervical vertebrae (7) in the neck. Thoracic vertebrae (12) in the thorax. Lumbar vertebrae (5) in the lower back. Sacrum (5,
Vertebral Column Backbone consists of 26 vertebrae. Five vertebral regions Cervical vertebrae (7) in the neck. Thoracic vertebrae (12) in the thorax. Lumbar vertebrae (5) in the lower back. Sacrum (5,
THE OSTEOPATHIC WORKSHOP: NECK PAIN
 THE OSTEOPATHIC WORKSHOP: NECK PAIN Trevine R. Albert, D.O. M.S. Family Medicine Neuromusculoskeletal Medicine PGY-3 2018 FSACOFP Convention DISCLOSURES There are no actual or potential personal, financial
THE OSTEOPATHIC WORKSHOP: NECK PAIN Trevine R. Albert, D.O. M.S. Family Medicine Neuromusculoskeletal Medicine PGY-3 2018 FSACOFP Convention DISCLOSURES There are no actual or potential personal, financial
THE PRO-POSTURE NECK EXERCISER
 EXERCISE INSTRUCTIONS FOR THE PRO-POSTURE NECK EXERCISER The following are a list of six different exercises that can be performed with the Pro- Posture Neck Exerciser. 1) Basic Pro-Posture Neck Pump Exercise
EXERCISE INSTRUCTIONS FOR THE PRO-POSTURE NECK EXERCISER The following are a list of six different exercises that can be performed with the Pro- Posture Neck Exerciser. 1) Basic Pro-Posture Neck Pump Exercise
Cervical Spine: Pearls and Pitfalls
 Cervical Spine: Pearls and Pitfalls Presenters Dr. Rob Donkin Functional Anatomy Current research Cervical Radiculopathy Dr. Gert Ferreira Red flags Case Study Kinesio Taping Chris Neethling Gonstead adjusting
Cervical Spine: Pearls and Pitfalls Presenters Dr. Rob Donkin Functional Anatomy Current research Cervical Radiculopathy Dr. Gert Ferreira Red flags Case Study Kinesio Taping Chris Neethling Gonstead adjusting
Anatomy. Anatomy deals with the structure of the human body, and includes a precise language on body positions and relationships between body parts.
 Anatomy deals with the structure of the human body, and includes a precise language on body positions and relationships between body parts. Proper instruction on safe and efficient exercise technique requires
Anatomy deals with the structure of the human body, and includes a precise language on body positions and relationships between body parts. Proper instruction on safe and efficient exercise technique requires
Blair Radiology Exam Examination Packet
 Blair Radiology Exam Examination Packet This packet is made of up five sections: Examiner s Instructions, Applicant Requirements, Analysis Rubric, Overall Result and Comments and Exam Form. The Exam Form
Blair Radiology Exam Examination Packet This packet is made of up five sections: Examiner s Instructions, Applicant Requirements, Analysis Rubric, Overall Result and Comments and Exam Form. The Exam Form
Imaging of Trauma to the Spine. Orthopedic Diplomate Program University of Bridgeport College of Chiropractic
 Imaging of Trauma to the Spine Orthopedic Diplomate Program University of Bridgeport College of Chiropractic Jefferson Fracture Yee, LL: The Jefferson Fracture, Radiology Cases in Pediatric Emergency Medicine.
Imaging of Trauma to the Spine Orthopedic Diplomate Program University of Bridgeport College of Chiropractic Jefferson Fracture Yee, LL: The Jefferson Fracture, Radiology Cases in Pediatric Emergency Medicine.
CLINICAL EXAM IMAGING AND TREATMENT OF THE NECK
 Arbeitsgruppe Pferd Advanced applications of ultrasound imaging in horses Bonn Germany sept.2010 CLINICAL EXAM IMAGING AND TREATMENT OF THE NECK Philippe HEILES DVM MSc Les Bréviaires France philippeheiles@equineclinic.fr
Arbeitsgruppe Pferd Advanced applications of ultrasound imaging in horses Bonn Germany sept.2010 CLINICAL EXAM IMAGING AND TREATMENT OF THE NECK Philippe HEILES DVM MSc Les Bréviaires France philippeheiles@equineclinic.fr
The Swimmer s Shoulder: An Osteopathic Approach
 The Swimmer s Shoulder: An Osteopathic Approach Mary Solomon, D.O. Rainbow Babies and Children s Hospital Cleveland, OH 440-914-7865 1 I have no relevant relationships/affiliations with any proprietary
The Swimmer s Shoulder: An Osteopathic Approach Mary Solomon, D.O. Rainbow Babies and Children s Hospital Cleveland, OH 440-914-7865 1 I have no relevant relationships/affiliations with any proprietary
Manual Muscle Testing. Yasser Moh. Aneis, PhD, MSc., PT. Lecturer of Physical Therapy Basic Sciences Department
 Manual Muscle Testing Yasser Moh. Aneis, PhD, MSc., PT. Lecturer of Physical Therapy Basic Sciences Department Manual Muscle Testing Evaluation of the function and strength of individual muscles and muscles
Manual Muscle Testing Yasser Moh. Aneis, PhD, MSc., PT. Lecturer of Physical Therapy Basic Sciences Department Manual Muscle Testing Evaluation of the function and strength of individual muscles and muscles
Chapter 7. Skeletal System
 Chapter 7 Skeletal System 1 Skull A. The skull is made up of 22 bones: 8 cranial bones, 13 facial bones, and the mandible. B. The Cranium encloses and protects the brain, provides attachments for muscles,
Chapter 7 Skeletal System 1 Skull A. The skull is made up of 22 bones: 8 cranial bones, 13 facial bones, and the mandible. B. The Cranium encloses and protects the brain, provides attachments for muscles,
Transitioning to the Suboccipital Triangle. Suboccipital Triangle
 Transitioning to the Suboccipital Triangle Syllabus p. 14-15 Suboccipital Triangle Borders -Rectus capitis posterior major -Obliquus capitis superior -Obliquus capitis inferior Contents -Vertebral artery
Transitioning to the Suboccipital Triangle Syllabus p. 14-15 Suboccipital Triangle Borders -Rectus capitis posterior major -Obliquus capitis superior -Obliquus capitis inferior Contents -Vertebral artery
Anatomy and Physiology II. Review Spine and Neck
 Anatomy and Physiology II Review Spine and Neck Spine regions How many cervical vertibrae are there? 7 The curvature is the cervical region posterior? Concave posterior How many thoracic? And curvature?
Anatomy and Physiology II Review Spine and Neck Spine regions How many cervical vertibrae are there? 7 The curvature is the cervical region posterior? Concave posterior How many thoracic? And curvature?
Spine Metrics. SPINAL BIOMECHANICAL ENGINEERING STUDY X-Ray Study for Alteration of Motion Segment Integrity (AOMSI)
") Spine Metrics Corporate: Billing Inquiries: Tech Support: 520 Huber Park Court, Weldon Spring, MO 63304 520 Huber Park Court, Weldon Spring, MO 63304 636-329-8774 smsubmitfiles@gmail.com Date: 05-03-15
Spine Metrics Corporate: Billing Inquiries: Tech Support: 520 Huber Park Court, Weldon Spring, MO 63304 520 Huber Park Court, Weldon Spring, MO 63304 636-329-8774 smsubmitfiles@gmail.com Date: 05-03-15
MEDICAL IMAGING OF THE VERTEBRAE
 MEDICAL IMAGING OF THE VERTEBRAE Vertebrae are your friends Matthew Harper MS-IV LECTURE OBJECTIVES INTRODUCE THE MOST COMMON MODALITIES OF MEDICAL IMAGING AND BASIC TECHNIQUES FOR READING THESE IMAGES
MEDICAL IMAGING OF THE VERTEBRAE Vertebrae are your friends Matthew Harper MS-IV LECTURE OBJECTIVES INTRODUCE THE MOST COMMON MODALITIES OF MEDICAL IMAGING AND BASIC TECHNIQUES FOR READING THESE IMAGES
Adaptive Radiography: Tips and Tricks
 Adaptive Radiography: Tips and Tricks WCEC 20 th Student Educator Radiographer Conference Dennis Bowman, RT(R), CRT (R)(F) Community Hospital of the Monterey Peninsula (CHOMP) - Staff Radiographer Owner/Consultant
Adaptive Radiography: Tips and Tricks WCEC 20 th Student Educator Radiographer Conference Dennis Bowman, RT(R), CRT (R)(F) Community Hospital of the Monterey Peninsula (CHOMP) - Staff Radiographer Owner/Consultant
LUMBAR SPINAL STENOSIS
 LUMBAR SPINAL STENOSIS Always occurs in the mobile segment. Factors play role in Stenosis Pre existing congenital or developmental narrowing of the lumbar spinal canal Translation of one anatomic segment
LUMBAR SPINAL STENOSIS Always occurs in the mobile segment. Factors play role in Stenosis Pre existing congenital or developmental narrowing of the lumbar spinal canal Translation of one anatomic segment