COMMON MSK CONDITIONS IN BABIES. Introduction to Paediatric Physiotherapy June 2017 By Linda Walsh
|
|
|
- Everett Randall
- 6 years ago
- Views:
Transcription
1 COMMON MSK CONDITIONS IN BABIES Introduction to Paediatric Physiotherapy June 2017 By Linda Walsh
2 OBJECTIVES Overview of: Congenital Talipes Equinovarus (CTEV) Developmental Hip Dysplasia (DDH) Plagiocephaly/Torticollis Obstetric Brachial Plexus Palsy (OBPP)
3 "THE ART OF SIMPLICITY IS A PUZZLE OF COMPLEXITY" Douglas Horton
4 SYSTEMATIC APPROACH
5 SYSTEMATIC ASSESSMENT ORTHOPAEDIC S'S Stiffness Symmetry Skeletal Dysplasia Symptoms Systemic signs Look Move Feel Functional context "P (REMS) PAEDIATRIC REGIONAL EXAM OF MSK SYSTEM

6 CONGENITAL TALIPES EQUINOVARUS Aetiology Pathology Clinical assessment Pirani score Ponseti treatment

7 TYPES OF TALIPES
 Equinus (percutaneous heel cord")
8 CTEV "CAVE" deformity Cavus Adduction (navicular) Varus (calcaneus) Equinus (percutaneous heel cord tenotomy)




9 "CAVE" DEFORMITY Cavus Adduction Varus Equinus

10 BACKGROUND 1:1000 live births Affects girls >boys 3-4% if FH on one side 30% chance if FH from both parents Bony deformity Increased pull of tibialis posterior, gastro-soleus and long toe flexors Muscles are smaller in size and shorter Thick and Taut ligaments
11 ASSESSMENT THE PIRANI SCORE: 6 CLINICAL SIGNS MIDFOOT SCORE HINDFOOT SCORE Curved lateral border Medial crease Position of the talar head Posterior Crease Rigid Equinus Empty Heel

12 PIRANI SCORE CURVED LATERAL BORDER

13 MEDIAL CREASE

14 LATERAL HEAD OF TALUS

15 POSTERIOR CREASE

16 RIGID EQUINUS

17 EMPTY HEEL

18 PONSETI TECHNIQUE Gold standard for treatment at all ages Foot is moved and stretched Plaster cast from toe to thigh Approx 6 casts Achilles tenotomy Boots and Bar until age 4-5

19 CTEV TREATMENT



20 PONSETI CASTING


 until the age")
21 TO MAINTAIN CORRECTION o Foot abduction brace o 3 months 23 hours o Night time and nap time (minimum hours) until the age of 4-5
22 OTHER DIFFERENTIALS.

23 METATARSUS ADDUCTUS Curved Lateral Border Medial crease Forefoot abduction ROM
24 CALCANEOVALGUS Normal hindfoot Rests in valgus Look at range of plantar flexion If restricted PF, ensure no empty heel Need to rule out vertical talus Rx=plantar flexion stretches with supination and inversion


25 CONGENITAL VERTICAL TALUS Very rare Hindfoot Valgus heel Empty heel Posterior crease Midfoot will present with rocker bottom

26 DESCRIBE THE FOOT

27 DESCRIBE THE FOOT

28 DESCRIBE THE FOOT
29 DEVELOPMENTAL HIP DYSPLASIA

30 DDH Aetiology Pathology Clinical assessment Ultrasound techniques XR assessment Treatment Case discussion
 Can affect the labrum, capsule, soft tissues Most common orthopaedic disorder in")
31 WHAT IS DDH A spectrum of conditions Can refer to subluxation or dislocation Can occur from conception, birth or subsequently Can affect osseous structures (acetabulum/prox femur) Can affect the labrum, capsule, soft tissues Most common orthopaedic disorder in new-borns

32 AETIOLOGY Dysplasia; 1 per 100 Dislocation; 1 per 1000 Bilateral in 20% of cases Genetic factors 12 times increased risk in 1st degree relatives Lower rates in African communities Packaging

33 DEVELOPMENT OF THE HIP 3rd trimester; the femoral head grows more rapidly than acetabular cartilage and so by birth the femoral head is less than 50% covered. Acetabular cartilage then develops faster than the femoral head, to allow more coverage.

34 PATHOLOGY NEW BORN Poor ossification of acetabulum Femoral head can glide in and out of acetabulum Socket shallow with loss of supero-lateral acetabulum Poor restraint to postero-lateral dislocation
35 EXAMINATION Is the hip dislocated? If dislocated is it reducible? If not dislocated is it dislocatable? Is it an older child? General exam e.g Mm/skeletal dysplasia, foot abnormalities, Spinal dysraphism

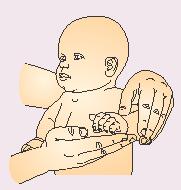
36 CLINICAL EXAMINATION OF BABIES Barlow Test: Hips flexed Thigh adducted Push posterially in line with the shaft of femur(pistoling) Positive sign is femoral head dislocating posteriorly. Ortolani s test: Hips examined 1 at a time Flex hips and knees to 90 degrees Thigh abducted with adduction pressure on greater trochanter Positive sign is a palpable and audible clunk as the hip reduces.


37 ORTOLANI AND BARLOW

38
39 CLINICAL EXAM 100% specific but <60% sensitivity (Scandinavian countries) Accurate within the first few days of life Experience of clinicians



40 CLINICAL EXAMINATION THE OLDER CHILD Galleazi test Skin creases Range of motion Barlow test Ortolani test Gait- waddling Lordosis Reduced Abduction Toe walking (especially unilaterally)
 Anatomy according to age; what is the maturation")
41 ULTRASOUND METHODS Graf (Europe) Terjesen (RLH/Scandinavian) Harcke (States) Anatomy according to age; what is the maturation curve

42 X-RAY MEASUREMENT Hilgenreiner s Line femoral head below Perkin s Line femoral head medial Shenton s Line continuous Reverse Shenton s continuous
43 GOALS OF RX Reduction Retention Maturation

44 PAVLIK HARNESS RX < 6 months and reducible hip flexion 50 abd 6 Weeks 95% cases resolve > 6 months, failure rate = 50% Not for tetralogic / neuromuscular hips Complications AVN due extreme abduction Femoral nerve injury


45 OTHER TREATMENT OPTIONS 6 months 18 months?adductor tenotomy?traction?eua arthrogram Closed reduction 6 months 24 months / irreducible Failure of closed treatment Persistent subluxation Surgical approach

46 CASE DISCUSSION 9 month female Brought into A&E by mother Noticed not walking on left leg Noticed left leg shorter by 2cm Born at term, normal delivery and development 3 older children, first child had DDH Did not attend / have hip screening
47 TORTICOLLIS
48 TORTICOLLIS Descriptive term- neck rotation and side flexion Not a specific diagnosis but a sign of an underlying disorder Not always muscular in origin- exclude differentials! 3rd most common MSK condition of childhood Muscular torticollis incidence is 0.3-2% Males > females

49 BALLOCK AND SONG children with torticollis 18% had a non-muscular aetiology Of which 30% had Klippel-Feil anomalies Underlying neurological disorder in 51% (ocular 23%, OBPI 17%, CNS lesions 11% Inflammatory C1-C2 rotary subluxations Clavicle fracture Paroxysmal torticollis
50 CONGENITAL TORTICOLLIS Postural/Packaging Mechanical stresses Muscular (Sternocleidomastoid tightness +/- fibrosis) Unknown aetiology Sternocleidomastoid Tumour Benign soft fluid filled tumour 8-16mm/fibrotic thickening/haematoma, most apparent a few weeks after birth. Resolves approx 5-21 months after birth The type of torticollis is predictive of the time to resolution.
51 ASSESSMENT Subjective acute onset, unwell child, trauma Head shape analysis (80-90% have plagiocephaly) Facial asymmetries Resting/preferential postures & assessment of symmetry Neck skin folds Passive Neck ROM Active Neck Rom Visual eye tracking and eye movements Head control Lateral Head Righting on the contralateral side (strength) General neurodevelopment screen i.e. milestones, movements, tone etc Upper limb dominance Spine/skeletal alignment Palpation SCM tumour (USS) Other lumps! Hip Ax
52 RED FLAGS Ocular Motor Asymmetry (nystagmus, strabismus) Palpable Masses Asymmetrical head positioning due to abnormal muscle tone, muscle tone imbalance, absence of SCM contracture Palpable skeletal Anomalies or asymmetries (congenital scoliosis) Delayed development and integration of primitive reflexes Presence of pathological reflexes (clonus, tremors) Absence of Movement of any extremity Presence of any hand or leg dominance
53 TREATMENT Neck PROM/stretches: Formally e.g. every nappy change Informally: carrying, prone, positioning, feeding etc Neck AROM Visual attraction Asymmetric handling to activate weak muscles Use head righting reactions Prone Positioning Correlates with AIMs Facilitate development of symmetrical normal movement & milestones e.g. midline play, reaching, rolling, avoidance of functional neglect Environmental adaptations: position of cot, play gym etc. Educate about plagiocephaly
54 PROGNOSIS Variable, Dependent on age, severity, type and compliance (Cheng et al., 2001) Physio before < month of age = 98% success rate in 2.5 months Intervention > 1 month up to 3 months = 89% success rate in 6 months of physio Physio at >6 months to 12 months = 10 months & less success (20% success rate)petronic et al., (2010) Boys had longer treatment duration < 3 months= 100% (Demirbilek et al % after 3 months Tatli et al. (2006) 94% resolve if treated before 24 weeks Watemberg et al. (2016). At age 2 years, 78% had no evidence of torticollis; ; 3.3% had torticollis of the same severity as at diagnosis; 18.3% had improved.
55 PHYSIO IS GREAT!!:-) Ryu et al. (2016) Physiotherapy was the only factor influencing complete resolution Only patient age correlated with non-resolution Ohman, Nilsson and Beckung (2010) Resolution was quicker with a physiotherapy-administered stretching programme v parent-administered stretching programme 0.9. months v 3.0 months to achieve good ROM 2.5 months v 4.5 months to achieve symmetrical head position
56 PLAGIOCEPHALY
57 NORMAL NEONATAL HEADS

58 PROGRESSION OF HEAD SHAPE A period of rapid head growth Reflective of brain growth Plagiocephaly at birth is not predictive for plagiocephaly at 7 weeks.

59 DEFORMATIONAL MOULDING
60 OBSERVATIONAL AX Parallelogram shaped skull Flattening of R or L side occiput Ipsilateral frontal bossing Facial asymmetries Orbital bulging Ipsilateral ear displacement anteriorly Mandibular/maxillary deformation
61 OBSERVATION
62 PREVALENCE Approx 5% pre back to sleep 20-30% now Cranial asymmetries 13% singletons 56% of twins 67-90% if have CMT
63 RISK FACTORS Restrictive uterine environment Big baby, big head, mulitparity, small maternal pelvis, malformed uterus, increased uterine/abdo tone, oligohydramnious/polyhydramnious, breech presentation, primiparity CMT Advanced maternal age Developmental delay Back to Sleep /lack of prone play/equipment - car seats Prematurity. In last 10 weeks of pregnancy, calvarial bones stiffness increases 5 to 10 fold

64 DIFFERENTIALS Plagiocephaly vs brachcephaly vs scaphycephaly vs craniosynostosis Craniosynostosis: Premature fusion of one of more cranial sutures Single or multiple suture fusions


65 BRACHYCEPHALY & SCAPHYCEPHALY
66 TREATMENT Counterpositioning (Active repositioning to reduce preference) Facilitate active head turn e.g. through feeding, positioning, handling Environmental adaptation Facilitate normal symmetrical development & milestones Tummy time (Back to Sleep). Helmet???
67 PROGNOSIS R.E PLAGIOCEPHALY Complete correction in 77% of conservative treatment (Steinbrenner et al 2015) Risk factors for failure: poor compliance, older babies, prolonged torticollis, developmental delay, initial severity Criteria for correction: diagonal difference of less than 5mm and/or cranial ratio of less than 0.85 by 18 months. Complete correction in 94% with helmet therapy Recommendation: Favour conservative Rx as a first choice if there are minimal risk factors Dependent on age, severity, compliance, & presence of torticollis

68 OBSTETRIC BRACHIAL PLEXUS PALSY ( B I RTH RELATED B RAC H I A L P L E X U S PA L S Y)

69 OBPP OBJECTIVES Aetiology Pathology Clinical assessment Treatment
70 WHAT IS BRBPP Umbrella term Refers to injury noted in the perinatal period to all or a portion of the brachial plexus 2 main risk factors: Birth Weight and Breech presentation Injuries affecting the upper brachial plexus are classically termed Erb palsies Injuries associated with the lower plexus are traditionally termed Klumpke palsies.
71 AETIOLOGY Always a Tearing Force Large babies (more than 4kg) Possible forceps or ventouse assistance Upper plexus injury, most commonly to the C5 and C6, and occasionally to the C7 roots, but never the lower nerve roots. Small babies (less than 3kg) Breech presentation-requiring excessive extension of the head & manipulation of the hand and arm which exerts traction on both the upper and lower roots. This may cause rupture or avulsion of any, or all of the roots

72 Associated with a 100-fold increased risk of brachial plexus injury SHOULDER DYSTOCIA
73 OBPP Incidence varies from 0.42 per 1000 live births (Evans-Jones, 2003) to per 1000 live births (Pondaag et al, 2004). Occasionally bilateral + Prognostic factor; Rapid return of motor function Various assessment tools and classification systems Narrakas classification Mallet classification Assisting Hand Assessment Toronto score Gilbert Raimondi assessment tools


74 THE BRACHIAL PLEXUS
;")
75 TYPES OF INJURY Avulsion ; nerve is torn from where it attaches to the spinal cord Rupture is when the nerve is torn A neuroma forms when torn nerve fibres have attempted to re-grow and heal themselves, but scar tissue has grown in and around the injury Axonotmesis occurs when nerve fibres are ruptured, but the nerve covering is intact - recovery by nerve growth takes time (1mm per day); Neuropraxis occurs when the nerve has been damaged but is intact - nerve fibres recover on their own and recovery should occur within 3 months.
76 NERVE INJURY
77 AIMS OF PHYSIOTHERAPY To maintain full and equal passive range of movement in all joints and full soft tissue length in the upper limb To encourage active movements and improve strength and endurance against gravity To be aware of any sensory deficit and advise appropriately To introduce developmental activities at an age appropriate time To advise and educate parents on appropriate management.

78 APCP REFERRAL PATHWAY WITHIN FIRST 24 HOURS FOLLOWING BIRTH ASSESS: Does the baby move both arms equally? Observe spontaneous movements in supine and side-lying Compare left and right sides Assess for Horner s sign. If abnormalities observed.. BEFORE DISCHARGE FROM HOSPITAL: X-ray of humerus or clavicle if fractured, arrange pain relief and orthopaedic follow-up Check for phrenic nerve palsy Physiotherapy referral for initial advice re. handling and positioning; Refer to paediatric physiotherapy.
79 WITHIN 1 WEEK OF RECEIVING REFERRAL Complete baseline assessment using Toronto scoring Check passive range of movement Check parent handling and teach stretches Provide information on Erbs Palsy Group Arrange follow-up at 8 weeks or sooner
80 BY 8 WEEK REVIEW Refer for specialist opinion if Toronto score <3.5 If there is FULL RECOVERY; Discharge INCOMPLETE RECOVERY; Continue to monitor active and passive range of movement Monitor and advise on child s development Refer to Occupational Therapy & Community Paediatrician if appropriate Advice to school if required Direct intervention if surgery planned. Goals should focus on minimizing bony deformities and joint contracture, while optimising functional outcomes.









81 EXERCISES



82 POSITIONING
83 "CONSISTENCY IS MORE VALUABLE THAN TALENT"

84 QUERIES???
Hip Dysplasia for the Primary Care Physician George Gantsoudes, MD. November 4, 2017
 Hip Dysplasia for the Primary Care Physician George Gantsoudes, MD November 4, 2017 Introduction Developmental Dysplasia of the Hip DDH - preferred term Teratologic hips Subluxation Dislocation-usually
Hip Dysplasia for the Primary Care Physician George Gantsoudes, MD November 4, 2017 Introduction Developmental Dysplasia of the Hip DDH - preferred term Teratologic hips Subluxation Dislocation-usually
Clinical Guidance. Neonatal Manual Chapter 10: Musculoskeletal problems
 Clinical Guidance Neonatal Manual Chapter 10: Musculoskeletal problems Summary This manual contains clinical guidelines developed by the Neonatal Unit multidisciplinary team over recent years. This chapter
Clinical Guidance Neonatal Manual Chapter 10: Musculoskeletal problems Summary This manual contains clinical guidelines developed by the Neonatal Unit multidisciplinary team over recent years. This chapter
DDH. Abnormal hip development Traditionally CDH (congenital dysplasia of the hip) Today DDH(developmental dysplasia of the hip)
 Today DDH(developmental dysplasia of the hip)") DDH Update on Screening Kathryn A Keeler, MD Assistant Professor University of Missouri-Kansas City School of Medicine, Department of Orthopaedic Surgery and Department of Pediatrics Children s Mercy Kansas
DDH Update on Screening Kathryn A Keeler, MD Assistant Professor University of Missouri-Kansas City School of Medicine, Department of Orthopaedic Surgery and Department of Pediatrics Children s Mercy Kansas
Clinical Practice & Referral Guideline - Developmental Dysplasia of the Hip
 Clinical Practice & Referral Guideline - Developmental Dysplasia of the Hip *This guideline was developed from the American Academy of Pediatrics Clinical Practice Guideline: Early Detection of Developmental
Clinical Practice & Referral Guideline - Developmental Dysplasia of the Hip *This guideline was developed from the American Academy of Pediatrics Clinical Practice Guideline: Early Detection of Developmental
Yorkshire and Humber Neonatal ODN (South) Clinical Guideline
 Clinical Guideline") Yorkshire and Humber Neonatal ODN (South) Clinical Guideline Title: Author: NEONATAL BRACHIAL PLEXUS INJURY Rebecca Musson Date written: January 2011, reviewed January 2016 Review date: January 2019 This
Yorkshire and Humber Neonatal ODN (South) Clinical Guideline Title: Author: NEONATAL BRACHIAL PLEXUS INJURY Rebecca Musson Date written: January 2011, reviewed January 2016 Review date: January 2019 This
Childhood hip conditions. Belen Carsi Paediatric Orthopaedic Consultant
 Childhood hip conditions Belen Carsi Paediatric Orthopaedic Consultant Developmental Dysplasia of the Hip Legg-Calve-Perthes disease Slipped Capital femoral epiphysis Limp Arthritis Developmental Dysplasia
Childhood hip conditions Belen Carsi Paediatric Orthopaedic Consultant Developmental Dysplasia of the Hip Legg-Calve-Perthes disease Slipped Capital femoral epiphysis Limp Arthritis Developmental Dysplasia
Four weeks of Intrauterine life
 Objective Congenital & Developmental Malformation Overview of Musculoskeletal dev. Abnormal pattern of dev. Common upper & lower ext. abnormalities READ : SPINE and more information in text book Definition
Objective Congenital & Developmental Malformation Overview of Musculoskeletal dev. Abnormal pattern of dev. Common upper & lower ext. abnormalities READ : SPINE and more information in text book Definition
Hip Joint DX 612 Orthopedics and Neurology
 Hip Joint DX 612 Orthopedics and Neurology James J. Lehman, DC, MBA, DABCO University of Bridgeport College of Chiropractic Hip Anatomy Palpation Point tenderness Edema Symmetry Hip ROM Hip Contracture
Hip Joint DX 612 Orthopedics and Neurology James J. Lehman, DC, MBA, DABCO University of Bridgeport College of Chiropractic Hip Anatomy Palpation Point tenderness Edema Symmetry Hip ROM Hip Contracture
Hip Anatomy. Hip Joint DX 612 Orthopedics and Neurology. Hip ROM. Palpation
 Hip Joint DX 612 Orthopedics and Neurology Hip Anatomy James J. Lehman, DC, MBA, DABCO University of Bridgeport College of Chiropractic Palpation Hip ROM Point tenderness Edema Symmetry Hip Contracture
Hip Joint DX 612 Orthopedics and Neurology Hip Anatomy James J. Lehman, DC, MBA, DABCO University of Bridgeport College of Chiropractic Palpation Hip ROM Point tenderness Edema Symmetry Hip Contracture
International Journal of Biological & Medical Research
 Int J Biol Med Res. 2013; 4(1): 2986-2990 Int J Biol Med Res Volume 3, Issue 1, Jan 2012 www.biomedscidirect.com BioMedSciDirect Publications Contents lists available at BioMedSciDirect Publications International
Int J Biol Med Res. 2013; 4(1): 2986-2990 Int J Biol Med Res Volume 3, Issue 1, Jan 2012 www.biomedscidirect.com BioMedSciDirect Publications Contents lists available at BioMedSciDirect Publications International
CLINICAL GUIDELINES ID TAG Developmental Dysplasia of hips Regional Guideline Mr Aidan Cosgrove. Title:
 Title: Author: Designation: Speciality / Division: Directorate: CLINICAL GUIDELINES ID TAG Developmental Dysplasia of hips Regional Guideline Mr Aidan Cosgrove Paediatric Orthopaedics Orthopaedic Orthopaedics
Title: Author: Designation: Speciality / Division: Directorate: CLINICAL GUIDELINES ID TAG Developmental Dysplasia of hips Regional Guideline Mr Aidan Cosgrove Paediatric Orthopaedics Orthopaedic Orthopaedics
Foot and Ankle Natalie Stork, MD
 Foot and Ankle Natalie Stork, MD Assistant Professor University of Missouri-Kansas City School of Medicine, Department of Orthopaedic Surgery and Department of Pediatrics Children s Mercy Kansas City,
Foot and Ankle Natalie Stork, MD Assistant Professor University of Missouri-Kansas City School of Medicine, Department of Orthopaedic Surgery and Department of Pediatrics Children s Mercy Kansas City,
Developmental Dysplasia of the Hip
 Developmental Dysplasia of the Hip Abnormal relationship of femoral head to the acetabulum Formerly known as congenital hip dislocation Believed to be developmental Most dislocations are evident at births
Developmental Dysplasia of the Hip Abnormal relationship of femoral head to the acetabulum Formerly known as congenital hip dislocation Believed to be developmental Most dislocations are evident at births
Metatarsus adductus, Skew foot, Club foot 성균관대학교삼성창원병원 장현정
 Metatarsus adductus, Skew foot, Club foot 성균관대학교삼성창원병원 장현정 Metatarsus adductus Epidemiology and Etiology 0.1-12% with higher number for multiple birth Deformation and compression from intrauterine crowding
Metatarsus adductus, Skew foot, Club foot 성균관대학교삼성창원병원 장현정 Metatarsus adductus Epidemiology and Etiology 0.1-12% with higher number for multiple birth Deformation and compression from intrauterine crowding
The Hip Baby?? Baby Hippie??
 In Need of a Title? The Hip Baby?? Baby Hippie?? Review of Developmental Dysplasia of the Hip in the Newborn OCR Symposium 2018 Ryan L. Hartman, MD Specialty: Pediatric and Sports Orthopaedics 23 month
In Need of a Title? The Hip Baby?? Baby Hippie?? Review of Developmental Dysplasia of the Hip in the Newborn OCR Symposium 2018 Ryan L. Hartman, MD Specialty: Pediatric and Sports Orthopaedics 23 month
PAEDIATRIC ORTHOPAEDICS BRENT WEATHERHEAD, MD, FRCSC PAEDIATRIC ORTHOPAEDIC SURGEON MEDICAL DIRECTOR, REBALANCE
 PAEDIATRIC ORTHOPAEDICS BRENT WEATHERHEAD, MD, FRCSC PAEDIATRIC ORTHOPAEDIC SURGEON MEDICAL DIRECTOR, REBALANCE DISCLOSURES I HAVE NO INDUSTRY CONFLICTS TO DECLARE I AM AN ORTHOPAEDIC SURGEON TRAINED IN
PAEDIATRIC ORTHOPAEDICS BRENT WEATHERHEAD, MD, FRCSC PAEDIATRIC ORTHOPAEDIC SURGEON MEDICAL DIRECTOR, REBALANCE DISCLOSURES I HAVE NO INDUSTRY CONFLICTS TO DECLARE I AM AN ORTHOPAEDIC SURGEON TRAINED IN
Pediatric Orthopedics: ``To Refer or Not to Refer``
 Pediatric Orthopedics: ``To Refer or Not to Refer`` Thierry E. Benaroch, MD, FRCS(C) McGill University Health Centre Intoeing Knock knees Bowlegs Flatfeet Toe walking Knee pain Hip click Intoeing Objectives
Pediatric Orthopedics: ``To Refer or Not to Refer`` Thierry E. Benaroch, MD, FRCS(C) McGill University Health Centre Intoeing Knock knees Bowlegs Flatfeet Toe walking Knee pain Hip click Intoeing Objectives
9/24/2015. Neonatal Orthopaedics - The Top 10 Diagnosis You Will or May See. Learning Objectives. Orthopaedic Diagnoses in Intensive Care Nursery
 Neonatal Orthopaedics - The Top 10 Diagnosis You Will or May See Learning Objectives Dale E. Jarka MD,CM, FRCSC Division of Orthopaedic Surgery The Children s Mercy Hospitals and Clinics To be cognizant
Neonatal Orthopaedics - The Top 10 Diagnosis You Will or May See Learning Objectives Dale E. Jarka MD,CM, FRCSC Division of Orthopaedic Surgery The Children s Mercy Hospitals and Clinics To be cognizant
Hip Dysplasia David S. Feldman, MD
 Hip Dysplasia David S. Feldman, MD Chief of Pediatric Orthopedic Surgery Professor of Orthopedic Surgery & Pediatrics NYU Langone Medical Center & NYU Hospital for Joint Diseases Overview Hip dysplasia
Hip Dysplasia David S. Feldman, MD Chief of Pediatric Orthopedic Surgery Professor of Orthopedic Surgery & Pediatrics NYU Langone Medical Center & NYU Hospital for Joint Diseases Overview Hip dysplasia
Obstetric Brachial Plexus Injuries. Surgery department grand rounds Bassam MJ Addas, FRCSC Neurological Surgery, KAUH
 Obstetric Brachial Plexus Injuries. Surgery department grand rounds Bassam MJ Addas, FRCSC Neurological Surgery, KAUH Definition Obstetric versus birth palsy Obstetric versus congenital palsy Not all birth
Obstetric Brachial Plexus Injuries. Surgery department grand rounds Bassam MJ Addas, FRCSC Neurological Surgery, KAUH Definition Obstetric versus birth palsy Obstetric versus congenital palsy Not all birth
Developmental Dysplasia of the Hip, (DDH) including Femoral and Pelvic Osteotomy
 including Femoral and Pelvic Osteotomy") Developmental Dysplasia of the Hip, (DDH) including Femoral and Pelvic Osteotomy Leicester Children s Hospital Information for Patients, Parents and Carers DRAFT What is developmental dysplasia of the
Developmental Dysplasia of the Hip, (DDH) including Femoral and Pelvic Osteotomy Leicester Children s Hospital Information for Patients, Parents and Carers DRAFT What is developmental dysplasia of the
Society for Pediatric Radiology 2015 Hands on Session. DDH: Pitfalls and Practical Tips
 Society for Pediatric Radiology 2015 Hands on Session DDH: Pitfalls and Practical Tips Michael A. DiPietro, M.D. John F. Holt Collegiate Professor of Radiology Professor of Pediatrics and Communicable
Society for Pediatric Radiology 2015 Hands on Session DDH: Pitfalls and Practical Tips Michael A. DiPietro, M.D. John F. Holt Collegiate Professor of Radiology Professor of Pediatrics and Communicable
Case Developmental dysplasia of hip
 Case 13303 Developmental dysplasia of hip Hidayatullah Hamidi, Sahar Maroof French medical institute for children, Kabul, Afghanistan Email: Hedayatullah.hamidi@gmail.com Maroofsahar1@gmail.com French
Case 13303 Developmental dysplasia of hip Hidayatullah Hamidi, Sahar Maroof French medical institute for children, Kabul, Afghanistan Email: Hedayatullah.hamidi@gmail.com Maroofsahar1@gmail.com French
Developmental Dysplasia of the Hip
 1 Developmental Dysplasia of the Hip Developmental dysplasia of the hip (DDH) or otherwise known as congenital dislocation of the hip (CDH) is a developmental (ongoing) process, which can often go undetected
1 Developmental Dysplasia of the Hip Developmental dysplasia of the hip (DDH) or otherwise known as congenital dislocation of the hip (CDH) is a developmental (ongoing) process, which can often go undetected
Ponseti Treatment Method for Idiopathic Clubfoot Continuing Education Module
 Ponseti Treatment Method for Idiopathic Clubfoot Continuing Education Module Michelle J. Hall, CPO, BSE 1 Ignacio V. Ponseti, MD 2 1. Certified Prosthetist Orthotist at American Prosthetics & Orthotics,
Ponseti Treatment Method for Idiopathic Clubfoot Continuing Education Module Michelle J. Hall, CPO, BSE 1 Ignacio V. Ponseti, MD 2 1. Certified Prosthetist Orthotist at American Prosthetics & Orthotics,
Intoeing: When to Worry? Sukhdeep K. Dulai SPORC 2018
 Intoeing: When to Worry? Sukhdeep K. Dulai SPORC 2018 What is it? Intoeing: When to worry? Why isn t it always cause for worry? What are the benign causes of intoeing? What are the pathologic causes of
Intoeing: When to Worry? Sukhdeep K. Dulai SPORC 2018 What is it? Intoeing: When to worry? Why isn t it always cause for worry? What are the benign causes of intoeing? What are the pathologic causes of
1. Discuss some common pediatric problems seen in the clinic. Diagnosis Clinical examination (at birth and subsequent well-baby examinations)
") 1 Pediatric Orthopaedics for Primary Care Providers 2 Disclosure Statement No conflicts related to this presentation 3 4 Goals 1. Discuss some common pediatric problems seen in the clinic 2. Examination
1 Pediatric Orthopaedics for Primary Care Providers 2 Disclosure Statement No conflicts related to this presentation 3 4 Goals 1. Discuss some common pediatric problems seen in the clinic 2. Examination
In-toeing and Out-toeing
 In-toeing and Out-toeing What is all the fuss about? Natalie Stork, MD Assistant Professor University of Missouri-Kansas City School of Medicine, Department of Orthopaedic Surgery and Department of Pediatrics
In-toeing and Out-toeing What is all the fuss about? Natalie Stork, MD Assistant Professor University of Missouri-Kansas City School of Medicine, Department of Orthopaedic Surgery and Department of Pediatrics
DDH: Pathology Diagnosis, and Treatment before Walking Age
 DDH: Pathology Diagnosis, and Treatment before Walking Age 영남의대 김세동 Ⅰ. Terminology of hip dysplasia a. Congenital dysplasia or dislocation of the hip(cdh): Hippocrates Congenital -Existing at Birth but
DDH: Pathology Diagnosis, and Treatment before Walking Age 영남의대 김세동 Ⅰ. Terminology of hip dysplasia a. Congenital dysplasia or dislocation of the hip(cdh): Hippocrates Congenital -Existing at Birth but
Friday Teaching. Bones
 Friday Teaching Bones Regarding slipped femoral capital epiphysis It represents Salter Harris type V injury 20% are bilateral There is slight widening of the joint space Slip is typically posteromedial
Friday Teaching Bones Regarding slipped femoral capital epiphysis It represents Salter Harris type V injury 20% are bilateral There is slight widening of the joint space Slip is typically posteromedial
Scar Engorged veins. Size of the foot [In clubfoot, small foot]
![Scar Engorged veins. Size of the foot [In clubfoot, small foot]](/thumbs/78/77722241.jpg "Scar Engorged veins. Size of the foot [In clubfoot, small foot]") 6. FOOT HISTORY Pain: Walking, Running Foot wear problem Swelling; tingly feeling Deformity Stiffness Disability: At work; recreation; night; walk; ADL, Sports Previous Rx Comorbidities Smoke, Sugar, Steroid
6. FOOT HISTORY Pain: Walking, Running Foot wear problem Swelling; tingly feeling Deformity Stiffness Disability: At work; recreation; night; walk; ADL, Sports Previous Rx Comorbidities Smoke, Sugar, Steroid
Guidelines, Policies and Statements. Statement on the Use of Ultrasound in the Diagnosis of Developmental Hip Dysplasia and Dislocation
 Guidelines, Policies and Statements Statement on the Use of Ultrasound in the Diagnosis of Developmental Hip Dysplasia and Dislocation Approved by Council June 2018 Disclaimer and Copyright The ASUM Standards
Guidelines, Policies and Statements Statement on the Use of Ultrasound in the Diagnosis of Developmental Hip Dysplasia and Dislocation Approved by Council June 2018 Disclaimer and Copyright The ASUM Standards
Surgical Care at the District Hospital. EMERGENCY & ESSENTIAL SURGICAL CARE
 Surgical Care at the District Hospital 1 18 Orthopedic Trauma Key Points 2 18.1 Upper Extremity Injuries Clavicle Fractures Diagnose fractures from the history and by physical examination Treat with a
Surgical Care at the District Hospital 1 18 Orthopedic Trauma Key Points 2 18.1 Upper Extremity Injuries Clavicle Fractures Diagnose fractures from the history and by physical examination Treat with a
Prevention Diagnosis
 Prevention and Management of Positional Skull Deformities in Infants John Persing, MD, Hector James, MD, Jack Swanson, MD, John Kattwinkel, MD, Committee on Practice and Ambulatory Medicine, Section on
Prevention and Management of Positional Skull Deformities in Infants John Persing, MD, Hector James, MD, Jack Swanson, MD, John Kattwinkel, MD, Committee on Practice and Ambulatory Medicine, Section on
Evaluation of Gait Mechanics Using Computerized Plantar Surface Pressure Analysis and it s Relation to Common Musculoskeletal Problems
 Evaluation of Gait Mechanics Using Computerized Plantar Surface Pressure Analysis and it s Relation to Common Musculoskeletal Problems Laws of Physics effecting gait Ground Reaction Forces Friction Stored
Evaluation of Gait Mechanics Using Computerized Plantar Surface Pressure Analysis and it s Relation to Common Musculoskeletal Problems Laws of Physics effecting gait Ground Reaction Forces Friction Stored
Ultrasound Scanning of Neonatal Hips
 Ultrasound Scanning of Neonatal Hips Dr. Dickson S F Tsang Associate Consultant Queen Mary Hospital Why? How? What? Outline IAAHS 2nd April, 2011 Outline Why? Why performing hip ultrasound (USG)? Why USG?
Ultrasound Scanning of Neonatal Hips Dr. Dickson S F Tsang Associate Consultant Queen Mary Hospital Why? How? What? Outline IAAHS 2nd April, 2011 Outline Why? Why performing hip ultrasound (USG)? Why USG?
Conservative management of idiopathic clubfoot: Kite versus Ponseti method
 Journal of Orthopaedic Surgery 2009;17(1):67-71 Conservative management of idiopathic clubfoot: Kite versus Ponseti method AV Sanghvi, 1 VK Mittal 2 1 Department of Orthopaedics, Government Medical College
Journal of Orthopaedic Surgery 2009;17(1):67-71 Conservative management of idiopathic clubfoot: Kite versus Ponseti method AV Sanghvi, 1 VK Mittal 2 1 Department of Orthopaedics, Government Medical College
What is a Hip Dysplasia?
 What is a Hip Dysplasia? Hip dysplasia, developmental dysplasia of the hip (DDH)[1] or congenital dysplasia of the hip (CDH)[2] is a congenital or acquired deformation or misalignment of the hip joint.
What is a Hip Dysplasia? Hip dysplasia, developmental dysplasia of the hip (DDH)[1] or congenital dysplasia of the hip (CDH)[2] is a congenital or acquired deformation or misalignment of the hip joint.
Foot Disorders, from the cradle to the grave
 Foot Disorders, from the cradle to the grave A O ADEDAPO MBBS, FRCS, FRCS(Tr/Orth) Consultant Orthopaedic Surgeon James Cook University Hospital Middlesbrough, U.K. General Overview. General Orthopaedic
Foot Disorders, from the cradle to the grave A O ADEDAPO MBBS, FRCS, FRCS(Tr/Orth) Consultant Orthopaedic Surgeon James Cook University Hospital Middlesbrough, U.K. General Overview. General Orthopaedic
Effects of Immobilization. N24 Pedi Musculoskeletal Spring 2012, Week 14. Cabrillo ADN/C. Madsen RN, MSN 1. Physical effects on other systems
 Common Orthopedic Problems of Children Congenital Acquired Bones Neuromuscular Physical effects on other systems Pulmonary Cardiac Skin integrity Elimination GI GU 1 4 General Nursing Considerations any
Common Orthopedic Problems of Children Congenital Acquired Bones Neuromuscular Physical effects on other systems Pulmonary Cardiac Skin integrity Elimination GI GU 1 4 General Nursing Considerations any
FACTS 1. Most need only Gastro aponeurotic release [in positive Silverskiold test]
![FACTS 1. Most need only Gastro aponeurotic release [in positive Silverskiold test]](/thumbs/83/88335212.jpg "FACTS 1. Most need only Gastro aponeurotic release [in positive Silverskiold test]") FOOT IN CEREBRAL PALSY GAIT IN CEREBRAL PALSY I True Equinus II Jump gait III Apparent Equinus IV Crouch gait Group I True Equinus Extended hip and knee Equinus at ankle II Jump Gait [commonest] Equinus
FOOT IN CEREBRAL PALSY GAIT IN CEREBRAL PALSY I True Equinus II Jump gait III Apparent Equinus IV Crouch gait Group I True Equinus Extended hip and knee Equinus at ankle II Jump Gait [commonest] Equinus
Peggers Super Summaries: Paediatric Hip
 EMBRYOLOGY Development o Mesenchymal stem cells cartilage blood supply bone Dates o 6/40 Limb development o 8-11/40 hip development (acetabulum and hip formed from one bone splitting by apoptosis) o 16/40
EMBRYOLOGY Development o Mesenchymal stem cells cartilage blood supply bone Dates o 6/40 Limb development o 8-11/40 hip development (acetabulum and hip formed from one bone splitting by apoptosis) o 16/40
BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY
 BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY B.Resseque, D.P.M. ARCH HEIGHT OFF WEIGHTBEARING Evaluate arch height by placing a ruler from the heel to the first metatarsal head Compare arch
BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY B.Resseque, D.P.M. ARCH HEIGHT OFF WEIGHTBEARING Evaluate arch height by placing a ruler from the heel to the first metatarsal head Compare arch
Copyright 2004, Yoshiyuki Shiratori. All right reserved.
 Ankle and Leg Evaluation 1. History Chief Complaint: A. What happened? B. Is it a sharp or dull pain? C. How long have you had the pain? D. Can you pinpoint the pain? E. Do you have any numbness or tingling?
Ankle and Leg Evaluation 1. History Chief Complaint: A. What happened? B. Is it a sharp or dull pain? C. How long have you had the pain? D. Can you pinpoint the pain? E. Do you have any numbness or tingling?
COMMON MUSCULOSKELETAL PROBLEMS GROWTH AND DEVELOPMENT PATHOLOGIC VS. NORMAL
 COMMON MUSCULOSKELETAL PROBLEMS GROWTH AND DEVELOPMENT PATHOLOGIC VS. NORMAL Clifford L. Craig, M.D. M2 Musculoskeletal Fall 2008 I. ANGULAR AND TORSIONAL DEFORMITIES OF THE LOWER LIMBS Examination Relaxed,
COMMON MUSCULOSKELETAL PROBLEMS GROWTH AND DEVELOPMENT PATHOLOGIC VS. NORMAL Clifford L. Craig, M.D. M2 Musculoskeletal Fall 2008 I. ANGULAR AND TORSIONAL DEFORMITIES OF THE LOWER LIMBS Examination Relaxed,
LECTURE 8: DEVELOPMENTAL ORTHOPAEDICS. Paediatric MS History o Reason for referral o Past history
 LECTURE 8: DEVELOPMENTAL ORTHOPAEDICS Paediatric MS History o Reason for referral o Past history Antenatal history Birth history (term? Premmy? Breech? Complications?). Medical history/investigations/tests
LECTURE 8: DEVELOPMENTAL ORTHOPAEDICS Paediatric MS History o Reason for referral o Past history Antenatal history Birth history (term? Premmy? Breech? Complications?). Medical history/investigations/tests
BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY 2017
 BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY 2017 B. RESSEQUE, D.P.M., D.A.B.P.O. Professor, N.Y. College of Podiatric Medicine ARCH HEIGHT OFF WEIGHTBEARING Evaluate arch height by placing
BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY 2017 B. RESSEQUE, D.P.M., D.A.B.P.O. Professor, N.Y. College of Podiatric Medicine ARCH HEIGHT OFF WEIGHTBEARING Evaluate arch height by placing
Financial Disclosure. The authors have not received any financial support for the preparation of this work.
 Persistent Clubfoot Deformity Following Treatment by the Ponseti Method W.B. Lehman, M.D. Alice Chu, M.D. New York Ponseti Clubfoot Center Department of Pediatric Orthopaedic Surgery Financial Disclosure
Persistent Clubfoot Deformity Following Treatment by the Ponseti Method W.B. Lehman, M.D. Alice Chu, M.D. New York Ponseti Clubfoot Center Department of Pediatric Orthopaedic Surgery Financial Disclosure
RN(EC) ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT ***
 ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT ***") HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age of patient - Certain conditions are more prevalent in particular age groups (Hip pain in children may refer to the knee from Legg-Calve-Perthes
HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age of patient - Certain conditions are more prevalent in particular age groups (Hip pain in children may refer to the knee from Legg-Calve-Perthes
Developmental Dysplasia of the Hip From Birth to Six Months
 From Birth to Six Months James T. Guille, MD, Peter D. Pizzutillo, MD, and G. Dean MacEwen, MD Abstract The term developmental dysplasia or dislocation of the hip (DDH) refers to the complete spectrum
From Birth to Six Months James T. Guille, MD, Peter D. Pizzutillo, MD, and G. Dean MacEwen, MD Abstract The term developmental dysplasia or dislocation of the hip (DDH) refers to the complete spectrum
Musculoskeletal Examination
 Musculoskeletal Examination Statement of Goals Know how to perform a complete musculoskeletal examination. Learning Objectives A. Describe the anatomy of the musculoskeletal system including the bony structures,
Musculoskeletal Examination Statement of Goals Know how to perform a complete musculoskeletal examination. Learning Objectives A. Describe the anatomy of the musculoskeletal system including the bony structures,
Radiological Sequelae of developmental dysplasia of the hip: a Review
 Radiological Sequelae of developmental dysplasia of the hip: a Review Poster No.: P-0037 Congress: ESSR 2012 Type: Scientific Exhibit Authors: S. G. Flanagan, J. Sarkodieh, K. Mcdonald, M. Ramachandran,
Radiological Sequelae of developmental dysplasia of the hip: a Review Poster No.: P-0037 Congress: ESSR 2012 Type: Scientific Exhibit Authors: S. G. Flanagan, J. Sarkodieh, K. Mcdonald, M. Ramachandran,
Balanced Body Movement Principles
 Balanced Body Movement Principles How the Body Works and How to Train it. Module 3: Lower Body Strength and Power Developing Strength, Endurance and Power The lower body is our primary source of strength,
Balanced Body Movement Principles How the Body Works and How to Train it. Module 3: Lower Body Strength and Power Developing Strength, Endurance and Power The lower body is our primary source of strength,
A Patient s Guide to Clubfoot
 A Patient s Guide to Clubfoot 651 Old Country Road Plainview, NY 11803 Phone: 5166818822 Fax: 5166813332 p.lettieri@aol.com DISCLAIMER: The information in this booklet is compiled from a variety of sources.
A Patient s Guide to Clubfoot 651 Old Country Road Plainview, NY 11803 Phone: 5166818822 Fax: 5166813332 p.lettieri@aol.com DISCLAIMER: The information in this booklet is compiled from a variety of sources.
Department of Neurosurgery. Differentiating Craniosynostosis from Positional Plagiocephaly
 Department of Neurosurgery Differentiating Craniosynostosis from Positional Plagiocephaly The number of infants with head shape deformities has risen over the past several years, likely due to increased
Department of Neurosurgery Differentiating Craniosynostosis from Positional Plagiocephaly The number of infants with head shape deformities has risen over the past several years, likely due to increased
Treatment of congenital subluxation and dislocation of the hip by knee splint harness
 Prosthetics and Orthotics International, 1994,18, 34-39 Treatment of congenital subluxation and dislocation of the hip by knee splint harness M. FUKUSHIMA Fukushima Orthopaedic Clinic, Hiroshima City,
Prosthetics and Orthotics International, 1994,18, 34-39 Treatment of congenital subluxation and dislocation of the hip by knee splint harness M. FUKUSHIMA Fukushima Orthopaedic Clinic, Hiroshima City,
Pediatric Orthopaedic Surgery and the HMSNs
 Reviewed and accepted by the 2011-2012 Neuromuscular Committee of the American Association of Neuromuscular & Electrodiagnostic Medicine Certified for CME credit 10/2011 05/2020 Reviewed 10/2017 by the
Reviewed and accepted by the 2011-2012 Neuromuscular Committee of the American Association of Neuromuscular & Electrodiagnostic Medicine Certified for CME credit 10/2011 05/2020 Reviewed 10/2017 by the
A Patient s Guide to Rotational Deformities in Children
 A Patient s Guide to Rotational Deformities in Children 2350 Royal Boulevard Suite 200 Elgin, IL 60123 Phone: 847.931.5300 Fax: 847.931.9072 DISCLAIMER: The information in this booklet is compiled from
A Patient s Guide to Rotational Deformities in Children 2350 Royal Boulevard Suite 200 Elgin, IL 60123 Phone: 847.931.5300 Fax: 847.931.9072 DISCLAIMER: The information in this booklet is compiled from
HIP DYSPLASIA AND HYPOTONIA CAN STANDING IN ABDUCTION HELP?
 HIP DYSPLASIA AND HYPOTONIA CAN STANDING IN ABDUCTION HELP? Written by: MARY MILES, PT, DPT, ATP THIS CASE STUDY IS SPONSORED BY ALTIMATE MEDICAL Standing with hips in abduction has evolved as the new
HIP DYSPLASIA AND HYPOTONIA CAN STANDING IN ABDUCTION HELP? Written by: MARY MILES, PT, DPT, ATP THIS CASE STUDY IS SPONSORED BY ALTIMATE MEDICAL Standing with hips in abduction has evolved as the new
Evaluation of three ultrasound techniques used for the diagnosis of developmental dysplasia of the hip (DDH)
") Evaluation of three ultrasound techniques used for the diagnosis of developmental dysplasia of the hip (DDH) Poster No.: C-2049 Congress: ECR 2012 Type: Scientific Exhibit Authors: E. M. D. B. Pacheco,
Evaluation of three ultrasound techniques used for the diagnosis of developmental dysplasia of the hip (DDH) Poster No.: C-2049 Congress: ECR 2012 Type: Scientific Exhibit Authors: E. M. D. B. Pacheco,
A Syndrome (Pattern) Approach to Low Back Pain. History
 Approach to Low Back Pain. History") A Syndrome (Pattern) Approach to Low Back Pain Hamilton Hall MD FRCSC Professor, Department of Surgery, University of Toronto Medical Director, CBI Health Group Executive Director, Canadian Spine Society
A Syndrome (Pattern) Approach to Low Back Pain Hamilton Hall MD FRCSC Professor, Department of Surgery, University of Toronto Medical Director, CBI Health Group Executive Director, Canadian Spine Society
Lecture Notes The LocomotorSystem. W. P. Howlett 2017
 Lecture Notes The LocomotorSystem W. P. Howlett 2017 Symptoms Main Symptoms Pain Stiffness Swelling Weakness The History Joints: involved Pain: onset, precipitating& relievingfactors Stiffness: pattern
Lecture Notes The LocomotorSystem W. P. Howlett 2017 Symptoms Main Symptoms Pain Stiffness Swelling Weakness The History Joints: involved Pain: onset, precipitating& relievingfactors Stiffness: pattern
Treatment of DDH before Walking Age 고려대학안암병원
 Treatment of DDH before Walking Age 이 순혁 고려대학안암병원 Subluxated Hip Always to deg. hip The more, the earlier Even in 2nd Decade Dysplastic Hip Eventually to osteoarthritis but later Etiology of end-stage
Treatment of DDH before Walking Age 이 순혁 고려대학안암병원 Subluxated Hip Always to deg. hip The more, the earlier Even in 2nd Decade Dysplastic Hip Eventually to osteoarthritis but later Etiology of end-stage
Orthopedics - Dr. Ahmad - Lecture 2 - Injuries of the Upper Limb
 The shoulder and the upper arm Fractures of the clavicle 1. Fall on the shoulder. 2. Fall on outstretched hand. In mid shaft fractures, the outer fragment is pulled down by the weight of the arm and the
The shoulder and the upper arm Fractures of the clavicle 1. Fall on the shoulder. 2. Fall on outstretched hand. In mid shaft fractures, the outer fragment is pulled down by the weight of the arm and the
Dropfoot - Video Gait Analysis - Craig A. Camasta, DPM, FACFAS Atlanta, Georgia, USA
 Equinus, Pes Cavus and Dropfoot - Video Gait Analysis - Craig A. Camasta, DPM, FACFAS Atlanta, Georgia, USA Equinus = Toe Walker Soft Tissue Static fixed contracture Dynamic spastic, hypertonic Bone Procurvatum,,
Equinus, Pes Cavus and Dropfoot - Video Gait Analysis - Craig A. Camasta, DPM, FACFAS Atlanta, Georgia, USA Equinus = Toe Walker Soft Tissue Static fixed contracture Dynamic spastic, hypertonic Bone Procurvatum,,
Evaluation of three ultrasound techniques used for the diagnosis of developmental dysplasia of the hip (DDH)
") Evaluation of three ultrasound techniques used for the diagnosis of developmental dysplasia of the hip (DDH) Poster No.: C-2049 Congress: ECR 2012 Type: Scientific Exhibit Authors: E. M. D. B. Pacheco,
Evaluation of three ultrasound techniques used for the diagnosis of developmental dysplasia of the hip (DDH) Poster No.: C-2049 Congress: ECR 2012 Type: Scientific Exhibit Authors: E. M. D. B. Pacheco,
Case Presentations The Child with a Limp
 Case Presentations The Child with a Limp Douglas G. Armstrong, M.D. Professor, PennState Hershey College of Medicine Division Head, Pediatric Orthopaedics Dept. of Orthopaedics and Rehabilitation PennState
Case Presentations The Child with a Limp Douglas G. Armstrong, M.D. Professor, PennState Hershey College of Medicine Division Head, Pediatric Orthopaedics Dept. of Orthopaedics and Rehabilitation PennState
Deformity and Pain in Foot of Neuromuscular Disease
 Deformity and Pain in Foot of Neuromuscular Disease CHA 의과학대학재활의학과김민영 (2012.11.10 제 4 회대한발의학회 ) Neuromuscular Diseases & Foot Deformity : almost Pain : infrequent Non-ambulatory, Ambulatory Neuromuscular
Deformity and Pain in Foot of Neuromuscular Disease CHA 의과학대학재활의학과김민영 (2012.11.10 제 4 회대한발의학회 ) Neuromuscular Diseases & Foot Deformity : almost Pain : infrequent Non-ambulatory, Ambulatory Neuromuscular
Human Anatomy - Problem Drill 06: The Skeletal System Axial Skeleton & Articualtions
 Human Anatomy - Problem Drill 06: The Skeletal System Axial Skeleton & Articualtions Question No. 1 of 10 Instructions: (1) Read the problem and answer choices carefully, (2) Work the problems on paper
Human Anatomy - Problem Drill 06: The Skeletal System Axial Skeleton & Articualtions Question No. 1 of 10 Instructions: (1) Read the problem and answer choices carefully, (2) Work the problems on paper
Normal development & reflex
 Normal development & reflex Definition of Development : acquisition & refinement of skills 1 대근육운동발달 2 소근육운동발달 3 대인관계및사회성발달 4 적응능력혹은비언어성발달 5 의사소통및언어발달 6 학습, 청각, 시각의발달 Department of Rehabilitation Medicine,
Normal development & reflex Definition of Development : acquisition & refinement of skills 1 대근육운동발달 2 소근육운동발달 3 대인관계및사회성발달 4 적응능력혹은비언어성발달 5 의사소통및언어발달 6 학습, 청각, 시각의발달 Department of Rehabilitation Medicine,
Understanding Leg Anatomy and Function THE UPPER LEG
 Understanding Leg Anatomy and Function THE UPPER LEG The long thigh bone is the femur. It connects to the pelvis to form the hip joint and then extends down to meet the tibia (shin bone) at the knee joint.
Understanding Leg Anatomy and Function THE UPPER LEG The long thigh bone is the femur. It connects to the pelvis to form the hip joint and then extends down to meet the tibia (shin bone) at the knee joint.
Radiographic Assessment of Pediatric Foot Alignment: Self-Assessment Module
 1.5 CME AJR Integrative Imaging LIFELONG LEARNING FOR RADIOLOGY Radiographic Assessment of Pediatric Foot Alignment: Self-Assessment Module Mahesh M. Thapa 1,2, Sumit Pruthi 1,2, Felix S. Chew 2 ABSTRACT
1.5 CME AJR Integrative Imaging LIFELONG LEARNING FOR RADIOLOGY Radiographic Assessment of Pediatric Foot Alignment: Self-Assessment Module Mahesh M. Thapa 1,2, Sumit Pruthi 1,2, Felix S. Chew 2 ABSTRACT
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Abductor hallucis tendon procedures, for hallux varus, 536 537 Acetabular disorders, intoeing in, 551 553 Akron dome osteotomy, for cavus deformities,
Note: Page numbers of article titles are in boldface type. A Abductor hallucis tendon procedures, for hallux varus, 536 537 Acetabular disorders, intoeing in, 551 553 Akron dome osteotomy, for cavus deformities,
L side 65% Torticollis, Plagiocephaly, Metatarsus varus Flat foot.
 DEVELOPMENTAL DISLOCATION OF THE HIP [DDH] Older terminology was Congenital dislocation of the hip. DDH means developmental dysplasia of the hip. DDH is better than CDH as dislocation is not always congenital.
DEVELOPMENTAL DISLOCATION OF THE HIP [DDH] Older terminology was Congenital dislocation of the hip. DDH means developmental dysplasia of the hip. DDH is better than CDH as dislocation is not always congenital.
Case Report Ipsilateral Hip Dysplasia in Patients with Sacral Hemiagenesis: A Report of Two Cases
 Case Reports in Orthopedics Volume 2015, Article ID 854151, 4 pages http://dx.doi.org/10.1155/2015/854151 Case Report Ipsilateral Hip Dysplasia in Patients with Sacral Hemiagenesis: A Report of Two Cases
Case Reports in Orthopedics Volume 2015, Article ID 854151, 4 pages http://dx.doi.org/10.1155/2015/854151 Case Report Ipsilateral Hip Dysplasia in Patients with Sacral Hemiagenesis: A Report of Two Cases
Musculoskeletal Examination Benchmarks
 Musculoskeletal Examination Benchmarks _ The approach to examining the musculoskeletal system is the same no matter what joint or limb is being examined. The affected and contralateral region should both
Musculoskeletal Examination Benchmarks _ The approach to examining the musculoskeletal system is the same no matter what joint or limb is being examined. The affected and contralateral region should both
A Patient s Guide to Adult-Acquired Flatfoot Deformity
 A Patient s Guide to Adult-Acquired Flatfoot Deformity Glendale Adventist Medical Center 1509 Wilson Terrace Glendale, CA 91206 Phone: (818) 409-8000 DISCLAIMER: The information in this booklet is compiled
A Patient s Guide to Adult-Acquired Flatfoot Deformity Glendale Adventist Medical Center 1509 Wilson Terrace Glendale, CA 91206 Phone: (818) 409-8000 DISCLAIMER: The information in this booklet is compiled
Foot and Ankle Physical Exam. The Big Picture: - Gait analysis - Exam standing - Exam sitting - Provocative maneuvers
 Foot and Ankle Physical Exam The Big Picture: - Gait analysis - Exam standing - Exam sitting - Provocative maneuvers 1. Gait analysis Physical Exam 2. Examination Standing Alignment Swelling 3. Examination
Foot and Ankle Physical Exam The Big Picture: - Gait analysis - Exam standing - Exam sitting - Provocative maneuvers 1. Gait analysis Physical Exam 2. Examination Standing Alignment Swelling 3. Examination
Adult Hip Dysplasia David S. Feldman, MD
 Adult Hip Dysplasia David S. Feldman, MD Chief of Pediatric Orthopedic Surgery Professor of Orthopedic Surgery & Pediatrics NYU Langone Medical Center & NYU Hospital for Joint Diseases Overview Adult hip
Adult Hip Dysplasia David S. Feldman, MD Chief of Pediatric Orthopedic Surgery Professor of Orthopedic Surgery & Pediatrics NYU Langone Medical Center & NYU Hospital for Joint Diseases Overview Adult hip
Toe-Walking. Benign Variant or Scourge of Bipedal Locomotion? Definition. Physical Exam. Absent Heel Strike 2/28/2011
 Toe-Walking Benign Variant or Scourge of Bipedal Locomotion? Definition Absent Heel Strike +/- Equinus Thoughout Gait Cycle +/- Knee Hyperextension +/- Hip Flexion Physical Exam +/- Equinus Contracture
Toe-Walking Benign Variant or Scourge of Bipedal Locomotion? Definition Absent Heel Strike +/- Equinus Thoughout Gait Cycle +/- Knee Hyperextension +/- Hip Flexion Physical Exam +/- Equinus Contracture
Where should you palpate the pulse of different arteries in the lower limb?
 Where should you palpate the pulse of different arteries in the lower limb? The femoral artery In the femoral triangle, its pulse is easily felt just inferior to the inguinal ligament midway between the
Where should you palpate the pulse of different arteries in the lower limb? The femoral artery In the femoral triangle, its pulse is easily felt just inferior to the inguinal ligament midway between the
General appearance examination
 Childhood athletic participation has dramatically increased over the past twenty years. Children are being introduced to organised sports at increasingly immature stages of physical development. It is
Childhood athletic participation has dramatically increased over the past twenty years. Children are being introduced to organised sports at increasingly immature stages of physical development. It is
AND PARACLINICAL INVESTIGATIONS
 Jurnal Medical Aradean (Arad Medical Journal) CONGENITAL DISLOCATION OF THE HIP: CLINICAL AND PARACLINICAL INVESTIGATIONS Violeta Oriţă, Marius Bucur Constantinescu, Beatrice Frumuşeanu, Mihaela Golumbeanu
Jurnal Medical Aradean (Arad Medical Journal) CONGENITAL DISLOCATION OF THE HIP: CLINICAL AND PARACLINICAL INVESTIGATIONS Violeta Oriţă, Marius Bucur Constantinescu, Beatrice Frumuşeanu, Mihaela Golumbeanu
Anatomy and evaluation of the ankle.
 Anatomy and evaluation of the ankle www.fisiokinesiterapia.biz Ankle Anatomical Structures Tibia Fibular Talus Tibia This is the strongest largest bone of the lower leg. It bears weight and the bone creates
Anatomy and evaluation of the ankle www.fisiokinesiterapia.biz Ankle Anatomical Structures Tibia Fibular Talus Tibia This is the strongest largest bone of the lower leg. It bears weight and the bone creates
CHRONIC FOOT PROBLEMS FOOT and ANKLE BASICS
 CHRONIC FOOT PROBLEMS FOOT and ANKLE BASICS ABC s of Comprehensive Musculoskeletal Care December 1 st, 2007 Stephen Pinney MD Chief, UCSF Foot and Ankle Service Chronic problems typically occur gradually
CHRONIC FOOT PROBLEMS FOOT and ANKLE BASICS ABC s of Comprehensive Musculoskeletal Care December 1 st, 2007 Stephen Pinney MD Chief, UCSF Foot and Ankle Service Chronic problems typically occur gradually
DEVELOPMENTAL DYSPLASIA OF THE HIP CURRENT TRENDS APLLIED IN ARAD
 DEVELOPMENTAL DYSPLASIA OF THE HIP CURRENT TRENDS APLLIED IN ARAD PAVEL Adrian Ionel 1, BOIA Eugen Sorin 2, 1 PhD, Victor Babes University of Medicine and Pharmacy, Timisoara, Romania 2 Prof., PhD, MD,
DEVELOPMENTAL DYSPLASIA OF THE HIP CURRENT TRENDS APLLIED IN ARAD PAVEL Adrian Ionel 1, BOIA Eugen Sorin 2, 1 PhD, Victor Babes University of Medicine and Pharmacy, Timisoara, Romania 2 Prof., PhD, MD,
What Happens to the Paediatric Flat Foot? Peter J Briggs Freeman Hospital Newcastle upon Tyne
 What Happens to the Paediatric Flat Foot? Peter J Briggs Freeman Hospital Newcastle upon Tyne We don t know!! Population Studies 2300 children aged 4-13 years Shoe wearers Flat foot 8.6% Non-shoe wearers
What Happens to the Paediatric Flat Foot? Peter J Briggs Freeman Hospital Newcastle upon Tyne We don t know!! Population Studies 2300 children aged 4-13 years Shoe wearers Flat foot 8.6% Non-shoe wearers
ANKLE PLANTAR FLEXION
 ANKLE PLANTAR FLEXION Evaluation and Measurements By Isabelle Devreux 1 Ankle Plantar Flexion: Gastrocnemius and Soleus ROM: 0 to 40-45 A. Soleus: Origin: Posterior of head of fibula and proximal1/3 of
ANKLE PLANTAR FLEXION Evaluation and Measurements By Isabelle Devreux 1 Ankle Plantar Flexion: Gastrocnemius and Soleus ROM: 0 to 40-45 A. Soleus: Origin: Posterior of head of fibula and proximal1/3 of
10/26/2017. Comprehensive & Coordinated Orthopaedic Management of Children with CP. Objectives. It s all about function. Robert Bruce, MD Sayan De, MD
 Comprehensive & Coordinated Orthopaedic Management of Children with CP Robert Bruce, MD Sayan De, MD Objectives Understand varying levels of intervention are available to optimize function of children
Comprehensive & Coordinated Orthopaedic Management of Children with CP Robert Bruce, MD Sayan De, MD Objectives Understand varying levels of intervention are available to optimize function of children
Paediatric Foot Disorders. Foot Disorders
 Paediatric B Milne FRACS (Orth) Paediatric Orthopaedic Fellow Anatomy Bones of the foot Valgus Deviation of the distal body part away from the midline Varus Deviation of the distal body part towards the
Paediatric B Milne FRACS (Orth) Paediatric Orthopaedic Fellow Anatomy Bones of the foot Valgus Deviation of the distal body part away from the midline Varus Deviation of the distal body part towards the
Paul Allan Regional Clinical Lead - South. Lumbar Spine. Assessment & Differential Diagnosis
 Paul Allan Regional Clinical Lead - South Lumbar Spine Assessment & Differential Diagnosis Aims Refresh lumbar spine anatomy Red flags Discuss common pathologies seen in general practice Subjective and
Paul Allan Regional Clinical Lead - South Lumbar Spine Assessment & Differential Diagnosis Aims Refresh lumbar spine anatomy Red flags Discuss common pathologies seen in general practice Subjective and
POSTURAL ANALYSIS. Posture is the attitude of the body. Good Posture = maximum efficiency with minimum effort
 POSTURAL ANALYSIS A Postural Analysis should be undertaken on a client prior to each occasion a treatment is performed. It can vary from an extensive total body analysis to just a specific problem area.
POSTURAL ANALYSIS A Postural Analysis should be undertaken on a client prior to each occasion a treatment is performed. It can vary from an extensive total body analysis to just a specific problem area.
CHANGES IN ANKLE MUSCULAR STRENGTH AFTER ANTERIOR TIBIALIS TENDON TRANSFER IN CHILDREN WITH CLUBFEET DEFORMITIES: A PROSPECTIVE STUDY
 CHANGES IN ANKLE MUSCULAR STRENGTH AFTER ANTERIOR TIBIALIS TENDON TRANSFER IN CHILDREN WITH CLUBFEET DEFORMITIES: A PROSPECTIVE STUDY Aaron Lyles, MD c, Hank White, PT, PhD a, J.J. Wallace, MS a, Sam Augsburger,
CHANGES IN ANKLE MUSCULAR STRENGTH AFTER ANTERIOR TIBIALIS TENDON TRANSFER IN CHILDREN WITH CLUBFEET DEFORMITIES: A PROSPECTIVE STUDY Aaron Lyles, MD c, Hank White, PT, PhD a, J.J. Wallace, MS a, Sam Augsburger,
PTA Applied Kinesiology 1
 Western Technical College 10524156 PTA Applied Kinesiology 1 Course Outcome Summary Course Information Description Career Cluster Instructional Level Total Credits 4.00 Introduces basic principles of musculoskeletal
Western Technical College 10524156 PTA Applied Kinesiology 1 Course Outcome Summary Course Information Description Career Cluster Instructional Level Total Credits 4.00 Introduces basic principles of musculoskeletal
APPLICATION OF THE MOVEMENT SYSTEMS MODEL TO THE MANAGEMENT COMMON HIP PATHOLOGIES
 APPLICATION OF THE MOVEMENT SYSTEMS MODEL TO THE MANAGEMENT COMMON HIP PATHOLOGIES Tracy Porter, PT, DPT Des Moines University Department of Physical Therapy Objectives Review current literature related
APPLICATION OF THE MOVEMENT SYSTEMS MODEL TO THE MANAGEMENT COMMON HIP PATHOLOGIES Tracy Porter, PT, DPT Des Moines University Department of Physical Therapy Objectives Review current literature related
ORDER OF VERBAL EXAMS
 ORDER OF VERBAL EXAMS The students are able to register for the exam on the NEPTUN system. The students pick two titles, from the title list available at the beginning of the Semester. This list can be
ORDER OF VERBAL EXAMS The students are able to register for the exam on the NEPTUN system. The students pick two titles, from the title list available at the beginning of the Semester. This list can be
The Pelvic Equilibrium Theory Part 2
 The Pelvic Equilibrium Theory Part 2 Understanding the abnormal motion patterns associated with The Pelvic Equilibrium Theory and Leg length Inequality. Aims of this section! To discuss the abnormal motion
The Pelvic Equilibrium Theory Part 2 Understanding the abnormal motion patterns associated with The Pelvic Equilibrium Theory and Leg length Inequality. Aims of this section! To discuss the abnormal motion
Evaluating Movement Posture Disorganization
 Evaluating Movement Posture Disorganization A Criteria-Based Reference Format for Observing & Analyzing Motor Behavior in Children with Learning Disabilities By W. Michael Magrun, MS, OTR 3 R D E D I T
Evaluating Movement Posture Disorganization A Criteria-Based Reference Format for Observing & Analyzing Motor Behavior in Children with Learning Disabilities By W. Michael Magrun, MS, OTR 3 R D E D I T
Other Congenital and Developmental Diseases of the Foot. Department of Orthopedic Surgery St. Vincent s s Hospital, The Catholic University
 Other Congenital and Developmental Diseases of the Foot Department of Orthopedic Surgery St. Vincent s s Hospital, The Catholic University Contents Metatarsus Adductus Skewfoot Hallux Valgus Hallux Valgus
Other Congenital and Developmental Diseases of the Foot Department of Orthopedic Surgery St. Vincent s s Hospital, The Catholic University Contents Metatarsus Adductus Skewfoot Hallux Valgus Hallux Valgus
Physical Examination of the Foot & Ankle
 Inspection Standing, feet straight forward facing toward examiner Swelling Deformity Flatfoot (pes planus and hindfoot valgus) High arch (pes cavus and hindfoot varus) Peek-a-boo heel Varus Too many toes
Inspection Standing, feet straight forward facing toward examiner Swelling Deformity Flatfoot (pes planus and hindfoot valgus) High arch (pes cavus and hindfoot varus) Peek-a-boo heel Varus Too many toes