Management of Chronic Lateral Ligament Instability
|
|
|
- Carol Ross
- 5 years ago
- Views:
Transcription
1 Management of Chronic Lateral Ligament Instability

2 Bony Anatomy Curved trochlear surface of talus produces a cone-shaped articulation whose apex is directed medially; thus the fan-shaped deltoid is all that is needed for support medially A larger area of movement and the subtalar joint articulation laterally dictates more soft tissue involvement to produce stability, thus, more commonly injured
3 The lateral ligaments should include not only the ATFL, CFL, and PTFL of the tibiotalar joint, but should also include the subtalar joint which is supported by the CFL, inferior extensor retinaculum, the lateral talocalcaneal ligament, the cervical ligament, and the interosseous talocalcaneal ligament Note: the CFL is included in both these joints and is crucial to the proper biomechanics of both joints Anatomy of Ligaments
4 ATFL - originates at the distal anterior fibula and inserts on the body of the talus just anterior to the articular facet (not unto the talar neck) ATFL - Makes an angle of approximately 75 with the floor from its fibular origin Anatomy of Ligaments

5 PTFL - originates from the medial surface of the lateral malleolus and courses medially in a horizontal manner to nearly the entire posterior lip of the talus Anatomy of Ligaments

6 CFL - originates from the anterior border of the distal lateral malleolus just below the origin of the ATFL and courses medially, posteriorly, and inferiorly from its fibular origin. It s attachment on the calcaneus blends with the peroneal tendon sheath and inserts on a small tubercle posterior and superior to the the peroneal tubercle. It runs approximately 10 to 45 posterior to the line of the longitudinal axis of the fibula Burks and Morgan showed ATFL and CFL had adjacent attachments on the anterior distal fibula 8 to 10 mm from the tip Anatomy of Ligaments
7 Anatomy of Ligaments Inferior extensor retinaculum is composed of 3 (lateral, intermediate, and medial); the CFL, LTCL, and the lateral root constitutes the superficial ligamentous support of the subtalar joint Lateral talocalcaneal ligamentoriginates from the lateral wall of the calcaneus just anterior to the calcaneal origin of the CFL and inserts on the body of the talus just inferior to the ATFL. This often blends with the CFL and ATFL (arcuate type) Cervical ligament- lies in the sinus tarsi and connects the neck of the talus to the superior surface of the calcaneus Interosseous talocalcaneal ligament located at the most medial aspect of the sinus tarsi and extends from a ridge at the sulcus tali
8 The angle of CFL and ATFL in the sagittal plane averages 105 ; this is clinically important in both the etiology of instability and for reconstruction Passing from dorsiflexion to plantarflexion causes a moment in time in which there may be decreased stability At 105 this is unusual, however, with an anatomical variant that displays a larger angle, there may be a larger interval of vulnerablity Ligament Anatomy
9 Biomechanics of Ligaments CFL is parallel to the subtalar joint axis in the sagittal plane; as the ankle is dorsi and plantar flexed, CFL and subtalar relationship does not change CFL is designed to allow motion in two joints simultaneously Neutral position, CFL is angulated posteriorly; in dorsiflexion it is brought in line with the fibula and becomes a true collateral ligament CFL in plantar flexion becomes parallel with the ground, and thus provides little support with resisting inversion ATFL is in line with fibula when the ankle is plantar flexed: collateral ligament ATFL in dorsiflexion positions the ligament horizontal to the ground and provides little resistance to inversion



10 Biomechanics of Ligaments Relationship in neutral Relationship in plantarflexion Relationship in dorsiflexion
11 Biomechanics of Ligaments PTFL is maximally stressed in dorsiflexion and prevents external rotation in dorsiflexion Attarin et al. ATFL has a lower load to failure than the CFL (CFL times greater) However, the ATFL is capable of undergoing greater strain which allows for the internal rotation of the talus during plantar flexion The ATFL inhibits internal rotation primarily; in plantar flexion it also prevents adduction CFL prohibits adduction and acts almost independently in the neutral and dorsiflexed positions. In plantar flexion it prevents adduction in conjunction with the ATFL
12 Biomechanics in Injury Forced dorsiflexion, PTFL ruptures Forced internal rotation ATFL ruptures followed by injury to the PTFL Extreme external rotation produces disruption of the deep deltoid lig. Adduction forces in neutral and dorsiflexion positions cause disruption of the CFL whereas in plantar flexion the ATFL is primarily injured Kjaersgaard-Anderson et al. cutting of CFL increased talocalcaneal rotation by 20% and increased tibiotalar adduction by 61%-77%


13 Biomechanics: Subtalar motion Allows the leg to undergo an additional amount of internal and external rotation Joint moves around a single inclined axis and functions essentially like a hinge connecting the talus and calcaneus The axis in the transverse plane deviates approx. 23 medial to long axis of foot, and in the horizontal plane, the axis is approx. 41 to the floor


14 Biomechanics: Subtalar Motion CFL and subtalar joint relationship: subtalar deviates from medial to lateral as it passes from dorsal to plantar direction Axis is defined from head of talus to lateral calcaneus, and forms a cone shape motion with its apex intersecting with the calcaneal attachment site of the CFL This cone shape arc and the position of the CFL allows unrestricted motion of the ankle and subtalar joint
15 Biomechanics: Subtalar Motion Two boards attached with a 45 hinge illustrates a one to one relationship of torque. A more horizontal hinge creates more rotation of the horizontal member (acts much like a torque converter)
16 Biomechanics: Subtalar Motion To prevent the horizontal member from participating in the displacement, it can be divided into 2 members: a short proximal segment and long distal segment The distal segment remains stationary by pivoting with the short segment (the transverse tarsal joint): this short segment acts just like the subtalar joint
17 Biomechanics: Subtalar Motion Conversion of the distal segment into rays will create an anatomical foot model where external rotation of the leg causes inversion of the heel, elevation of the medial side of foot, and depression of lateral side Clinical: Patients with pes planus have a more horizontal subtalar joint so that with little leg rotation, they have more supination and pronation
18 Epidemiology Acute sprains account for 16%-21% for all athletic injuries Lateral injuries account for 85% of all ankle sprains 10%-30% of all acute sprains result in chronic symptomatology Instability can be thought of in two ways: functional and mechanical Functional = subjective complaint with proprioceptive disorder that is rehab able Mechanical = objective instability that is determined by anterior drawer and talar tilt stress tests and often requires surgical intervention O Donaghue classification most commonly used: Grade I, II, III
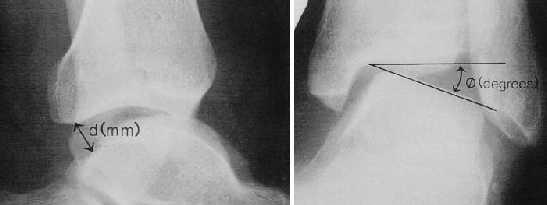
19 Exam Anterior drawer test- performed in relaxed plantar flexion Talar tilt test performed in neutral with hindfoot locked Freeman described modified Romberg s test performed on injured and uninjured leg (positive = proprioceptive defects, rehab) Telos stress test: 1) anterior draw > 10mm and talar tilt > 9. 2) difference of anterior drawer of symptomatic ankle from asymptomatic should be > 3mm. 3) difference b/n talar tilt of symptomatic versus asymptomatic should be > 3. Karlsson et al. found > 90% sensitivity, specificity, and predictive values with above criteria

20 Telos stress test
21 Treatment Conservative management should be attempted first Peroneal strengthening, coordination training, and aggressive PT Failure of conservative management is variable Surgical treatment can be broken into three groups: 1) delayed primary repair (Brostrom Repair) 2) Tenodesis procedures (Watson-Jones, Chrisman-Snook, Lee, Evans, Elmslie) 3) Anatomic reconstruction Varus hindfoot deformities should be repaired prior to any of the above procedures Kibler et al. found intra-articular problems in 83% of ankles scoped prior to performing modified Brostrom (indication to scope before procedure)
22 Surgical Classification Stability determined by talar tilt and anterior drawer test: type I negative and Type II positive Type I receive functional treatment Type II positive anterior drawer and/or talar tilt: split into Group I and Group II Group I = non-athlete or older and get functional treatment Group II = young athlete which gets broken into Type A and Type B Type A = negative stress X-ray get functional treatment Type B = positive tibiotalar stress x-ray (tilt > 15 and anterior draw > 1cm gets surgical treatment
23 Direct repair (Brostrom type procedure) Originally described in 1966 to repair ATFL and CFL if disrupted Many modifications have been introduced since then Not indicated for patients with: 1. Generalized hypermobility 2. Long-standing ligamentous insufficiency (>10 years) 3. Patients with previous ligamentous surgery to the ankle 4. Obese patients > 225 Gould et al. in 1980 described the modification of advancement of inferior retinaculum to address subtalar instability Karlson modification was to simply imbricate the attenuated ligament during the direct repair
24 Once through skin, enter the anterolateral capsule at the plafond and then dissect distally to expose the ATFL. If ligament is simply attenuated imbricate. Address the CFL by opening the peroneal sheath and judge the quality of the ligament. May be able to simply imbricate or suture to bone. If ligaments are attenuated and scarred to capsule, they may be elevated subperiosteally to recreate the ligament Before closure, the inferior extensor retinaculum is imbricated or sutured to the periosteum over the fibula Brostrom-Gould
25 Keller et al. Lateral Ankle Instability and the Brostrom-Gould Procedure. The Journal of Foot and Ankle Surgery. 36(6): patients followed for 67 months after above procedure 5 presented with acute on chronic, 2 patients were elite athletes with severe acute injury, and 37 were chronic (5 lost to follow up) Results were rated as poor, fair, good, excellent (good and excellent back to normal ADL s and athletic activity) 2.5% poor, 0 fair, 12.8% good, and 84.6% excellent
26 Tenodesis Procedures
27 Watson-Jones brevis used to reconstruct the ATFL; prevents inversion of the foot and restricts subtalar motion Persistent subjective instabiltiy 20%-90% Watson-Jones
28 Bahr et al. Biomechanics of Ankle Ligament Reconstruction. An In-Vitro Comparison of the Brostrom Repair, Watson- Jones Reconstruction, and a New Anatomic Reconstruction Technique. AJSM: July/Aug, First cadaveric model that allowed measurement of ligament force and simultaneous joint motion 8 cadavers were used and ankles were put through 3 rotations (dorsiplantar flexion, supination-pronation, and internal-external rotation) and three translations (anterior-posterior, medial-lateral, and joint compression-distraction) Force and motion recorded in unloaded and loaded state at dorsiflexion, neutral, plantar flexion, pronation, and supination Motion and force recorded during application of anterior translation and during talar tilt Testing was performed in specimens with ligaments intact, sectioned ATFL and then sectioned CFL, and then with above mentioned reconstructions
29 Bahr et al. Biomechanics of Ankle Ligament Reconstruction. An In-Vitro Comparison of the Brostrom Repair, Watson- Jones Reconstruction, and a New Anatomic Reconstruction Technique. AJSM: July/Aug, ATFL stress increased with increasing plantar flexion in compression mode while CFL was unchanged 15 of supination increases stress in CFL and posterior grafts, however, different than normal (Watson-Jones was associated with reduction in total joint plantar flexion and internal rotation) Anterior translation remained at an increased injury level after Brostrom repair No changes in ATFL force in intact and grafts during anterior drawer and talar tilt and there was no difference b/n intact ankle and posterior grafts of any reconstruction during an anterior drawer An increase in posterior graft force was seen during talar tilt after Watson-Jones
30 Bahr et al. Biomechanics of Ankle Ligament Reconstruction. An In-Vitro Comparison of the Brostrom Repair, Watson- Jones Reconstruction, and a New Anatomic Reconstruction Technique. AJSM: July/Aug, All three reconstructions significantly reduced the laxity demonstrated when the ATFL and CFL were sectioned Joint motion was restricted after Watson-Jones procedure The graft force patterns of the Brostrom and anatomic reconstruction resembled those recorded in normal ankle
31 Sugimoto et al. Long-Term Results of Watson-Jones Tenodesis of the Ankle. JBJS 80A: November ankles followed for mean duration of 13 years 8 months 27 had manual examination while 6 were phone interviewed Pre op were evaluated by rating system of Good et al. Post op were evaluated by rating scale of Good et al. and American Orthopaedic Foot and Ankle Society Circumference of calf, goniometric measurement of hindfoot and sagittal motion, and manual strength testing to foot eversion were compared
32 Sugimoto et al. Long-Term Results of Watson-Jones Tenodesis of the Ankle. JBJS 80A: November excellent, 11 good, 3 fair, and one poor 9 with mild restriction of sagittal motion 14 had mild or moderate restriction of hindfoot and seven had difficulty squatting Weakness of peroneals was not detected, however, all but two demonstrated atrophy of calf muscles
33 Evans Evans routed brevis into lateral malleolus, prevents inversion and restricts subtalar motion Subjective instability 20%-33% Persistent anterior drawer is found 45%-60%
34 Chrisman-Snook split brevis graft (modification of the elmslie) designed to replace both ATFL and CFL and to prevent inversion and anterior translation; restricts subtalar motion Subjective instability 13%-30% Chrisman-Snook
35 Snook et al, Long Term Results of the Chrisman-Snook Operation for Reconstruction of the Lateral Ligaments of the Ankle. JBJS 67-A: Jan year follow up of 48 of 60 ankles originally performed 36 had complete evaluation, 12 had phone conversation 4 ratings had to be met : 1) elimination of patient-perceived instability 2)restoration of function, both occupational and recreational 3) maintenance of a near-normal range of motion of the ankle in all directions 4) lack of sensory changes consequent to surgical manipulation of sural nerve Stated loss of < 20 of inversion is not associated with functional limitations, however, reported on 3 patients known to have > 20 loss and limited inversion (not reported as failures in this study)
36 Snook et al, Long Term Results of the Chrisman-Snook Operation for Reconstruction of the Lateral Ligaments of the Ankle. JBJS 67-A: Jan Original description is to pass graft from anterior to posterior through fibula at the level of the tibiotalar joint The graft is then passed distally over the longus and remaining brevis and pulled into a trough in the lateral calcaneus where CFL inserts. Original description was to sew back into base of the fifth but now recommends sewing into leading anterior hole of the fibula Modifications: 1. Drill hole in calcaneus instead of trap door 2.suture into anterior fibula instead base of fifth 3. Mild rather than forced eversion of the foot while graft is sutured in place to eliminate painful limitation of inversion.
37 Snook et al, Long Term Results of the Chrisman-Snook Operation for Reconstruction of the Lateral Ligaments of the Ankle. JBJS 67-A: Jan Results: largest loss in motion was 20 inversion in two patients without functional complaints, 45 ankles had excellent or good results, 3 had unsatisfactory result 3 unsatisfactory results were recurrence of lateral ankle instability all secondary to severe injury Believe this reconstruction is vital to restore tibiotalar and subtalar stability (referenced that the Brostrom repair only fixes the ATFL and most people with chronic instability have both ATFL and CFL tears)
38 Snook et al, Long Term Results of the Chrisman-Snook Operation for Reconstruction of the Lateral Ligaments of the Ankle. JBJS 67-A: Jan
39 Modified Chrisman-Snook Procedure Used in generalized ligamentous laxity, failed imbrication or tenodesis or in athletes with long history of laxity(>10 years of instability) Long lateral incision 11 cm proximal curving at the tip of fibula and ending in the vicinity of the calcaneocuboid joint The peroneal retinaculum is split except for the superior part in line with the incision Arthrotomy is made just proximal to the superior border of the ATFL The peroneal sheath is opened distal to fibula to prepare the tendons for transfer Subperiosteal dissect deep to peroneal tendons to locate calcaneal drill hole site Harvest half of brevis starting distally and ending proximal 2-3 cm
40 Modified Chrisman-Snook Procedure First drill hole is placed in lateral neck of talus and the second is in the distal anterior fibula directing this anterior to posterior at level of tibiotalar joint The third hole goes from the posterior fibula to the anterior distal fibula near the tip where the CFL originates The final two holes are made in the calcaneus to replicate insertion of the CFL The graft starts in talus to fibula anterior to posterior then back into fibula and into calcaneus No anterior directed force or eversion and sew old ATFL to grafts
41 Split brevis graft that is used to anatomically reconstruct the CFL and the ATFL Easy to harvest, good biomechanical testing Bigger incision than Brostrom and may therefore have slightly higher nerve complication Colville
42 Colville et al. Reconstruction of the lateral ankle ligament. A biomechanical analysis. AJSM; 20(5) Cadaveric analysis on 15 ankles comparing the Evans, Chrisman- Snook, Watson-Jones, and a new anatomic repair Believe that symptoms are a result of excessive anterior talar translocation, internal rotation, and talar tilt. The above and subtalar motion were evaluated and compared. Isometry of bone tunnels were compared from 20 dorsiflexion to 30 plantarflexion All grafts were tensioned with the ankle in eversion and neutral dorsi/plantar flexion
43 Colville et al. Reconstruction of the lateral ankle ligament. A biomechanical analysis. AJSM; 20(5) Isometry Evans - 5% decrease change of graft. Watson-Jones graft from fifth meta. to posterior fibula decreased 5% while graft from anterior fibula to talus increased 17%. Chrisman-Snook graft from base of fifth to anterior fibula increased 15% while graft posterior fibula to calcaneus decreased 24%. Anatomic graft from anterior fibula to talus increased 6% while graft from posterior fibula to calcaneus decreased 10%.
44 Colville et al. Reconstruction of the lateral ankle ligament. A biomechanical analysis. AJSM: 20(5), Biomechanical Testing Watson-Jones and anatomic repair had limitation of internal rotation while C-S and Evans displayed a lack of restricting internal rotation C-S and Evans allowed significant greater anterior translocation, while W-J and anatomic were similar to intact ligaments Talar tilt was significantly greater with the W-J and Evans while C-S and anatomic were similar to each other and similar to intact ligaments Anatomic repair allowed statistically similar subtalar motion compared to intact ligaments, while all three tenodesis reconstructions significantly had decreased subtalar motion compared to normal.
45 Colville et al. Reconstruction of the lateral ankle ligament. A biomechanical analysis. AJSM; 20(5) Evans: restored internal rotation however anterior translocation and tilt were poorly controlled and subtalar motion was restricted Chrisman-Snook: did well especially with limiting the talar tilt, but restricted subtalar motion Watson-Jones: most effective in reducing anterior translocation and internal rotation, however had significant increase in talar tilt and restricted subtalar motion Anatomic: mechanics were restored most closely and subtalar motion was not limited
46 Burk and Morgan Anatomical reconstruction with graft material (autograft or allograft) Good biomechanical testing Again bigger incision
47 Plantaris tendon is used and routed medial to lateral through the calcaneus and used to reconstruct both the CFL and the ATFL Good reconstruction, bad for harvesting Anderson
V E R I TAS MGH 1811 MGH 1811 V E R I TAS. *Gerber JP. Persistent disability with ankle sprains. Foot Ankle Int 19: , 1998.
 MGH 1811 Management of Ankle Instability Richard J. de Asla, M.D. V E R I TAS MGH 1811 I have no potential conflicts with this presentation. V E R I TAS It s just a sprain Lateral Ankle Sprains Most common
MGH 1811 Management of Ankle Instability Richard J. de Asla, M.D. V E R I TAS MGH 1811 I have no potential conflicts with this presentation. V E R I TAS It s just a sprain Lateral Ankle Sprains Most common
Copyright 2004, Yoshiyuki Shiratori. All right reserved.
 Ankle and Leg Evaluation 1. History Chief Complaint: A. What happened? B. Is it a sharp or dull pain? C. How long have you had the pain? D. Can you pinpoint the pain? E. Do you have any numbness or tingling?
Ankle and Leg Evaluation 1. History Chief Complaint: A. What happened? B. Is it a sharp or dull pain? C. How long have you had the pain? D. Can you pinpoint the pain? E. Do you have any numbness or tingling?
BIOMECHANICS OF ANKLE FRACTURES
 BIOMECHANICS OF ANKLE FRACTURES William R Reinus, MD MBA FACR Significance of Ankle Fractures Most common weight-bearing Fx 70% of all Fxs Incidence is increasing Bimodal distribution Men 15-24 Women over
BIOMECHANICS OF ANKLE FRACTURES William R Reinus, MD MBA FACR Significance of Ankle Fractures Most common weight-bearing Fx 70% of all Fxs Incidence is increasing Bimodal distribution Men 15-24 Women over
Ankle Pain After a Sprain.
 Ankle Pain After a Sprain www.fisiokinesiterapia.biz Anterior Drawer Stress Test Talar Tilt Talar Tilt (CFL) Difficult to isolate from subtalar ROM Slight plantar flexion (dorsi = relative subtalar isolation)
Ankle Pain After a Sprain www.fisiokinesiterapia.biz Anterior Drawer Stress Test Talar Tilt Talar Tilt (CFL) Difficult to isolate from subtalar ROM Slight plantar flexion (dorsi = relative subtalar isolation)
Ligament lesions of the ankle. Marc C. Attinger
 Ligament lesions of the ankle Marc C. Attinger Anatomy Mechanism of injury Each lig with its function during ROM in dorsiflexion/er ATFL slack, CFL tight in plantarflexion/ir CFL slack, ATFL tight Acute
Ligament lesions of the ankle Marc C. Attinger Anatomy Mechanism of injury Each lig with its function during ROM in dorsiflexion/er ATFL slack, CFL tight in plantarflexion/ir CFL slack, ATFL tight Acute
SURGICAL AND APPLIED ANATOMY
 Página 1 de 9 Copyright 2001 Lippincott Williams & Wilkins Bucholz, Robert W., Heckman, James D. Rockwood & Green's Fractures in Adults, 5th Edition SURGICAL AND APPLIED ANATOMY Part of "47 - ANKLE FRACTURES"
Página 1 de 9 Copyright 2001 Lippincott Williams & Wilkins Bucholz, Robert W., Heckman, James D. Rockwood & Green's Fractures in Adults, 5th Edition SURGICAL AND APPLIED ANATOMY Part of "47 - ANKLE FRACTURES"
Mary Lloyd Ireland, M.D. Associate Professor University of Kentucky Dept. of Orthopaedic Surgery and Sports Medicine Lexington, Kentucky
 Common Ankle Injuries: Diagnosis and Treatment Mary Lloyd Ireland, M.D. Associate Professor University of Kentucky Dept. of Orthopaedic Surgery and Sports Medicine Lexington, Kentucky Disclaimer Slide
Common Ankle Injuries: Diagnosis and Treatment Mary Lloyd Ireland, M.D. Associate Professor University of Kentucky Dept. of Orthopaedic Surgery and Sports Medicine Lexington, Kentucky Disclaimer Slide
Clin Podiatr Med Surg 19 (2002) Index
 Index") Clin Podiatr Med Surg 19 (2002) 335 344 Index Note: Page numbers of article titles are in bold face type. A Accessory soleus muscle, magnetic resonance imaging of, 300 Achilles tendon injury of, magnetic
Clin Podiatr Med Surg 19 (2002) 335 344 Index Note: Page numbers of article titles are in bold face type. A Accessory soleus muscle, magnetic resonance imaging of, 300 Achilles tendon injury of, magnetic
The Lower Limb VII: The Ankle & Foot. Anatomy RHS 241 Lecture 7 Dr. Einas Al-Eisa
 The Lower Limb VII: The Ankle & Foot Anatomy RHS 241 Lecture 7 Dr. Einas Al-Eisa Ankle joint Synovial, hinge joint Allow movement of the foot in the sagittal plane only (1 degree of freedom): dorsiflexion:
The Lower Limb VII: The Ankle & Foot Anatomy RHS 241 Lecture 7 Dr. Einas Al-Eisa Ankle joint Synovial, hinge joint Allow movement of the foot in the sagittal plane only (1 degree of freedom): dorsiflexion:
Introduction. The primary function of the ankle and foot is to absorb shock and impart thrust to the body during walking.
 The ankle 1 Introduction The primary function of the ankle and foot is to absorb shock and impart thrust to the body during walking. OSTEOLOGRY The term ankle refers primarily to the talocrural joint,
The ankle 1 Introduction The primary function of the ankle and foot is to absorb shock and impart thrust to the body during walking. OSTEOLOGRY The term ankle refers primarily to the talocrural joint,
Clarification of Terms
 Clarification of Terms The plantar aspect of the foot refers to the role or its bottom The dorsal aspect refers to the top or its superior portion The ankle and foot perform three main functions: 1. shock
Clarification of Terms The plantar aspect of the foot refers to the role or its bottom The dorsal aspect refers to the top or its superior portion The ankle and foot perform three main functions: 1. shock
Bio-Tenodesis Screw Fixation
 Bio-Tenodesis Screw Fixation in Tendon Enhanced Ankle Ligament Reconstruction Surgical Technique Kevin O'Shea, M.D. with contributions from Thomas Clanton, M.D., and William McGarvey, M.D. Bio-Tenodesis
Bio-Tenodesis Screw Fixation in Tendon Enhanced Ankle Ligament Reconstruction Surgical Technique Kevin O'Shea, M.D. with contributions from Thomas Clanton, M.D., and William McGarvey, M.D. Bio-Tenodesis
Outline. Ankle/Foot Anatomy Ankle Sprains Ottawa Ankle Rules DDx: The Sprain That Wasn t
 Ankle Injuries Outline Ankle/Foot Anatomy Ankle Sprains Ottawa Ankle Rules DDx: The Sprain That Wasn t Anatomy: Ankle Mortise Bony Anatomy Lateral Ligament Complex Medial Ligament Complex Ankle Sprains
Ankle Injuries Outline Ankle/Foot Anatomy Ankle Sprains Ottawa Ankle Rules DDx: The Sprain That Wasn t Anatomy: Ankle Mortise Bony Anatomy Lateral Ligament Complex Medial Ligament Complex Ankle Sprains
X-Ray Rounds: (Plain) Radiographic Evaluation of the Ankle.
 Radiographic Evaluation of the Ankle.") X-Ray Rounds: (Plain) Radiographic Evaluation of the Ankle www.fisiokinesiterapia.biz Anatomy Complex hinge joint Articulations among: Fibula Tibia Talus Tibial plafond Distal tibial articular surface
X-Ray Rounds: (Plain) Radiographic Evaluation of the Ankle www.fisiokinesiterapia.biz Anatomy Complex hinge joint Articulations among: Fibula Tibia Talus Tibial plafond Distal tibial articular surface
Anatomy of Foot and Ankle
 Anatomy of Foot and Ankle Surface anatomy of the ankle & foot Surface anatomy of the ankle & foot Medial orientation point medial malleous sustentaculum tali tuberosity of navicular TA muscle TP muscle
Anatomy of Foot and Ankle Surface anatomy of the ankle & foot Surface anatomy of the ankle & foot Medial orientation point medial malleous sustentaculum tali tuberosity of navicular TA muscle TP muscle
Physical Examination of the Foot & Ankle
 Inspection Standing, feet straight forward facing toward examiner Swelling Deformity Flatfoot (pes planus and hindfoot valgus) High arch (pes cavus and hindfoot varus) Peek-a-boo heel Varus Too many toes
Inspection Standing, feet straight forward facing toward examiner Swelling Deformity Flatfoot (pes planus and hindfoot valgus) High arch (pes cavus and hindfoot varus) Peek-a-boo heel Varus Too many toes
Anatomy and evaluation of the ankle.
 Anatomy and evaluation of the ankle www.fisiokinesiterapia.biz Ankle Anatomical Structures Tibia Fibular Talus Tibia This is the strongest largest bone of the lower leg. It bears weight and the bone creates
Anatomy and evaluation of the ankle www.fisiokinesiterapia.biz Ankle Anatomical Structures Tibia Fibular Talus Tibia This is the strongest largest bone of the lower leg. It bears weight and the bone creates
Technique for Single-Graft Lateral Ankle Stabilization: A Cadaveric Biomechanical Study
 The Foot and Ankle Online Journal Official publication of the International Foot & Ankle Foundation Technique for Single-Graft Lateral Ankle Stabilization: A Cadaveric Biomechanical Study by Craig E Clifford,
The Foot and Ankle Online Journal Official publication of the International Foot & Ankle Foundation Technique for Single-Graft Lateral Ankle Stabilization: A Cadaveric Biomechanical Study by Craig E Clifford,
FACTS 1. Most need only Gastro aponeurotic release [in positive Silverskiold test]
![FACTS 1. Most need only Gastro aponeurotic release [in positive Silverskiold test]](/thumbs/83/88335212.jpg "FACTS 1. Most need only Gastro aponeurotic release [in positive Silverskiold test]") FOOT IN CEREBRAL PALSY GAIT IN CEREBRAL PALSY I True Equinus II Jump gait III Apparent Equinus IV Crouch gait Group I True Equinus Extended hip and knee Equinus at ankle II Jump Gait [commonest] Equinus
FOOT IN CEREBRAL PALSY GAIT IN CEREBRAL PALSY I True Equinus II Jump gait III Apparent Equinus IV Crouch gait Group I True Equinus Extended hip and knee Equinus at ankle II Jump Gait [commonest] Equinus
Sports Injuries of the Foot and Ankle Dominic Nielsen. Parkside Hospital Ashtead Hospital St George s
 Sports Injuries of the Foot and Ankle Dominic Nielsen Parkside Hospital Ashtead Hospital St George s Themes Ankle instability Ankle impingement Stress fractures 5 th MT fractures Peroneal subluxation Ankle
Sports Injuries of the Foot and Ankle Dominic Nielsen Parkside Hospital Ashtead Hospital St George s Themes Ankle instability Ankle impingement Stress fractures 5 th MT fractures Peroneal subluxation Ankle
Scar Engorged veins. Size of the foot [In clubfoot, small foot]
![Scar Engorged veins. Size of the foot [In clubfoot, small foot]](/thumbs/78/77722241.jpg "Scar Engorged veins. Size of the foot [In clubfoot, small foot]") 6. FOOT HISTORY Pain: Walking, Running Foot wear problem Swelling; tingly feeling Deformity Stiffness Disability: At work; recreation; night; walk; ADL, Sports Previous Rx Comorbidities Smoke, Sugar, Steroid
6. FOOT HISTORY Pain: Walking, Running Foot wear problem Swelling; tingly feeling Deformity Stiffness Disability: At work; recreation; night; walk; ADL, Sports Previous Rx Comorbidities Smoke, Sugar, Steroid
Leg. Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology
 Leg Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Skin of the Leg Cutaneous Nerves Medially: The saphenous nerve, a branch of the femoral nerve supplies the skin on the medial surface
Leg Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Skin of the Leg Cutaneous Nerves Medially: The saphenous nerve, a branch of the femoral nerve supplies the skin on the medial surface
Therapeutic Foot Care Certificate Program Part I: Online Home Study Program
 Therapeutic Foot Care Certificate Program Part I: Online Home Study Program 1 Anatomy And Terminology Of The Lower Extremity Joan E. Edelstein, MA, PT, FISPO Associate Professor of Clinical Physical Therapy
Therapeutic Foot Care Certificate Program Part I: Online Home Study Program 1 Anatomy And Terminology Of The Lower Extremity Joan E. Edelstein, MA, PT, FISPO Associate Professor of Clinical Physical Therapy
Peggers Super Summaries: Foot Injuries
 Lisfranc Injury ANATOMY Roman arch with recessed 2 nd MT base AP medial side of intermediate cuneiform to 2 nd MT base Oblique medial side of lateral cuneiform with 3 rd MT base and 4 th with medial boarder
Lisfranc Injury ANATOMY Roman arch with recessed 2 nd MT base AP medial side of intermediate cuneiform to 2 nd MT base Oblique medial side of lateral cuneiform with 3 rd MT base and 4 th with medial boarder
Evidence-Based Examination of the Foot Presented by Alexis Wright, PT, PhD, DPT, FAAOMPT Practice Sessions/Skill Check-offs
 Evidence-Based Examination of the Foot Presented by Alexis Wright, PT, PhD, DPT, FAAOMPT Practice Sessions/Skill Check-offs Module Five: Movement Assessment of the Foot/Ankle (1 hour CEU Time) Skilled
Evidence-Based Examination of the Foot Presented by Alexis Wright, PT, PhD, DPT, FAAOMPT Practice Sessions/Skill Check-offs Module Five: Movement Assessment of the Foot/Ankle (1 hour CEU Time) Skilled
5.1 Identify, describe the attachments of and deduce the actions of the muscles of the thigh:
 5.1 Identify, describe the attachments of and deduce the actions of the muscles of the thigh: Anterior group Proximal attachment Distal attachment Sartorius ASIS» Upper part of shaft tibia (middle surface)»
5.1 Identify, describe the attachments of and deduce the actions of the muscles of the thigh: Anterior group Proximal attachment Distal attachment Sartorius ASIS» Upper part of shaft tibia (middle surface)»
Ankle Tendons in Athletes. Laura W. Bancroft, M.D.
 Ankle Tendons in Athletes Laura W. Bancroft, M.D. Outline Protocols Normal Anatomy Tendinopathy, partial and complete tears Posterior tibial, Flexor Hallucis Longus, Achilles, Peroneal and Anterior Tibial
Ankle Tendons in Athletes Laura W. Bancroft, M.D. Outline Protocols Normal Anatomy Tendinopathy, partial and complete tears Posterior tibial, Flexor Hallucis Longus, Achilles, Peroneal and Anterior Tibial
Index. Clin Sports Med 23 (2004) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Clin Sports Med 23 (2004) 169 173 Index Note: Page numbers of article titles are in boldface type. A Achilles enthesopathy, calcaneal spur with, 133 clinical presentation of, 135 136 definition of, 131
Clin Sports Med 23 (2004) 169 173 Index Note: Page numbers of article titles are in boldface type. A Achilles enthesopathy, calcaneal spur with, 133 clinical presentation of, 135 136 definition of, 131
Joints and muscles of the foot. Architecture of the foot. Sándor Katz M.D.,Ph.D.
 Joints and muscles of the foot. Architecture of the foot. Sándor Katz M.D.,Ph.D. Ankle (talocrural) joint type: hinge Talocrural joint - medial collateral ligament Medial collateral = deltoid ligament
Joints and muscles of the foot. Architecture of the foot. Sándor Katz M.D.,Ph.D. Ankle (talocrural) joint type: hinge Talocrural joint - medial collateral ligament Medial collateral = deltoid ligament
The Leg. Prof. Oluwadiya KS
 The Leg Prof. Oluwadiya KS www.oluwadiya.sitesled.com Compartments of the leg 4 Four Compartments: 1. Anterior compartment Deep fibular nerve Dorsiflexes the foot and toes 2. Lateral Compartment Superficial
The Leg Prof. Oluwadiya KS www.oluwadiya.sitesled.com Compartments of the leg 4 Four Compartments: 1. Anterior compartment Deep fibular nerve Dorsiflexes the foot and toes 2. Lateral Compartment Superficial
Pelvic cavity. Gross anatomy of the lower limb. Walking. Sándor Katz M.D.,Ph.D.
 Pelvic cavity. Gross anatomy of the lower limb. Walking. Sándor Katz M.D.,Ph.D. Lower limb Pelvic girdle Free lower extremity Hip bone Definitive fusion of the Y- shaped growth plate occurs 16th -18th
Pelvic cavity. Gross anatomy of the lower limb. Walking. Sándor Katz M.D.,Ph.D. Lower limb Pelvic girdle Free lower extremity Hip bone Definitive fusion of the Y- shaped growth plate occurs 16th -18th
Sports Injuries of the Ankle and Ankle Arthritis. Mr Amit Amin Consultant Foot and Ankle Surgeon Parkside Hospital
 Sports Injuries of the Ankle and Ankle Arthritis Mr Amit Amin Consultant Foot and Ankle Surgeon Parkside Hospital Impingement Painful mechanical limitation of full ankle movement secondary to osseous
Sports Injuries of the Ankle and Ankle Arthritis Mr Amit Amin Consultant Foot and Ankle Surgeon Parkside Hospital Impingement Painful mechanical limitation of full ankle movement secondary to osseous
Donald Stewart, MD. Lateral ligament injuries Chronic lateral ligament instability Syndesmosis Injuries
 Donald Stewart, MD Arlington Orthopedic Associates Lateral ligament injuries Chronic lateral ligament instability Syndesmosis Injuries Anatomy Mechanism of Injury Classification Diagnostic Tests Management
Donald Stewart, MD Arlington Orthopedic Associates Lateral ligament injuries Chronic lateral ligament instability Syndesmosis Injuries Anatomy Mechanism of Injury Classification Diagnostic Tests Management
5 COMMON INJURIES IN THE FOOT & ANKLE
 5 COMMON INJURIES IN THE FOOT & ANKLE MICHAEL P. CLARE, MD FLORIDA ORTHOPAEDIC INSTITUTE TAMPA, FL USA MECHANISM OF INJURY HOW DID IT HAPPEN? HIGH ENERGY VS LOW ENERGY DIRECTION OF FORCES INVOLVED LIVING
5 COMMON INJURIES IN THE FOOT & ANKLE MICHAEL P. CLARE, MD FLORIDA ORTHOPAEDIC INSTITUTE TAMPA, FL USA MECHANISM OF INJURY HOW DID IT HAPPEN? HIGH ENERGY VS LOW ENERGY DIRECTION OF FORCES INVOLVED LIVING
ANKLE PLANTAR FLEXION
 ANKLE PLANTAR FLEXION Evaluation and Measurements By Isabelle Devreux 1 Ankle Plantar Flexion: Gastrocnemius and Soleus ROM: 0 to 40-45 A. Soleus: Origin: Posterior of head of fibula and proximal1/3 of
ANKLE PLANTAR FLEXION Evaluation and Measurements By Isabelle Devreux 1 Ankle Plantar Flexion: Gastrocnemius and Soleus ROM: 0 to 40-45 A. Soleus: Origin: Posterior of head of fibula and proximal1/3 of
Recognizing common injuries to the lower extremity
 Recognizing common injuries to the lower extremity Bones Femur Patella Tibia Tibial Tuberosity Medial Malleolus Fibula Lateral Malleolus Bones Tarsals Talus Calcaneus Metatarsals Phalanges Joints - Knee
Recognizing common injuries to the lower extremity Bones Femur Patella Tibia Tibial Tuberosity Medial Malleolus Fibula Lateral Malleolus Bones Tarsals Talus Calcaneus Metatarsals Phalanges Joints - Knee
Extraarticular Lateral Ankle Impingement
 Extraarticular Lateral Ankle Impingement Poster No.: C-1282 Congress: ECR 2016 Type: Educational Exhibit Authors: C. Cevikol; Keywords: Trauma, Diagnostic procedure, MR, CT, Musculoskeletal system, Musculoskeletal
Extraarticular Lateral Ankle Impingement Poster No.: C-1282 Congress: ECR 2016 Type: Educational Exhibit Authors: C. Cevikol; Keywords: Trauma, Diagnostic procedure, MR, CT, Musculoskeletal system, Musculoskeletal
ANKLE JOINT ANATOMY 3. TALRSALS = (FOOT BONES) Fibula. Frances Daly MSc 1 CALCANEUS 2. TALUS 3. NAVICULAR 4. CUBOID 5.
 Fibula. Frances Daly MSc 1 CALCANEUS 2. TALUS 3. NAVICULAR 4. CUBOID 5.") ANKLE JOINT ANATOMY The ankle joint is a synovial joint of the hinge type. The joint is formed by the distal end of the tibia and medial malleolus, the fibula and lateral malleolus and talus bone. It is
ANKLE JOINT ANATOMY The ankle joint is a synovial joint of the hinge type. The joint is formed by the distal end of the tibia and medial malleolus, the fibula and lateral malleolus and talus bone. It is
Influence of bone morphology and injured ligament of the ankle on ankle stress radiographs
 Influence of bone morphology and injured ligament of the ankle on ankle stress radiographs Gye Wang Lee, MD, Chin Youb Chung, MD, Moon Seok Park, MD Seung Yeol Lee, MD, Myung Ki Chung, MD, Byung Chae Jo,
Influence of bone morphology and injured ligament of the ankle on ankle stress radiographs Gye Wang Lee, MD, Chin Youb Chung, MD, Moon Seok Park, MD Seung Yeol Lee, MD, Myung Ki Chung, MD, Byung Chae Jo,
OTM Lecture Gait and Somatic Dysfunction of the Lower Extremity
 OTM Lecture Gait and Somatic Dysfunction of the Lower Extremity Somatic Dysfunction Tenderness Asymmetry Range of Motion Tissue Texture Changes Any one of which must be present to diagnosis somatic dysfunction.
OTM Lecture Gait and Somatic Dysfunction of the Lower Extremity Somatic Dysfunction Tenderness Asymmetry Range of Motion Tissue Texture Changes Any one of which must be present to diagnosis somatic dysfunction.
Modified Brostrom-Evans-Gould technique for recurrent lateral ankle ligament instability
 Journal of Orthopaedic Surgery 2007;15(3):306-10 Modified Brostrom-Evans-Gould technique for recurrent lateral ankle ligament instability ZD Ng, S Das De Department of Orthopaedic Surgery, National University
Journal of Orthopaedic Surgery 2007;15(3):306-10 Modified Brostrom-Evans-Gould technique for recurrent lateral ankle ligament instability ZD Ng, S Das De Department of Orthopaedic Surgery, National University
Modified Brostrom-Gould Technique
 Surgical Technique Modified Brostrom-Gould Technique Modified Brostrom-Gould Technique for Lateral Ankle Ligament Reconstruction Modified Brostrom-Gould Technique for Lateral Ankle Ligament Reconstruction
Surgical Technique Modified Brostrom-Gould Technique Modified Brostrom-Gould Technique for Lateral Ankle Ligament Reconstruction Modified Brostrom-Gould Technique for Lateral Ankle Ligament Reconstruction
The Dance Hall by Vincent van Gogh,1888
 The Dance Hall by Vincent van Gogh,1888 Articulations of the pelvic girdle Lumbosacral joints, sacroiliac joints & pubic symphysis The remaining joints of the lower limb Hip joint Knee joint Tibiofibular
The Dance Hall by Vincent van Gogh,1888 Articulations of the pelvic girdle Lumbosacral joints, sacroiliac joints & pubic symphysis The remaining joints of the lower limb Hip joint Knee joint Tibiofibular
Posterior Tibialis Tendon Dysfunction & Repair
 1 Posterior Tibialis Tendon Dysfunction & Repair Surgical Indications and Considerations Anatomical Considerations: The posterior tibialis muscle arises from the interosseous membrane and the adjacent
1 Posterior Tibialis Tendon Dysfunction & Repair Surgical Indications and Considerations Anatomical Considerations: The posterior tibialis muscle arises from the interosseous membrane and the adjacent
Section Three: The Leg, Ankle, and Foot Lecture: Review of Clinical Anatomy, Patterns of Dysfunction and Injury, and
 Section Three: The Leg, Ankle, and Foot Lecture: Review of Clinical Anatomy, Patterns of Dysfunction and Injury, and Treatment Implications for the Leg, Ankle, and Foot Levels I and II Demonstration and
Section Three: The Leg, Ankle, and Foot Lecture: Review of Clinical Anatomy, Patterns of Dysfunction and Injury, and Treatment Implications for the Leg, Ankle, and Foot Levels I and II Demonstration and
UvA-DARE (Digital Academic Repository) Treatment of osteochondral defects of the talus van Bergen, C.J.A. Link to publication
 Treatment of osteochondral defects of the talus van Bergen, C.J.A. Link to publication") UvA-DARE (Digital Academic Repository) Treatment of osteochondral defects of the talus van Bergen, C.J.A. Link to publication Citation for published version (APA): van Bergen, C. J. A. (2014). Treatment
UvA-DARE (Digital Academic Repository) Treatment of osteochondral defects of the talus van Bergen, C.J.A. Link to publication Citation for published version (APA): van Bergen, C. J. A. (2014). Treatment
First & second layers of muscles of the sole
 The FOOT First & second layers of muscles of the sole introduction The muscles acting on the foot can be divided into two distinct groups; extrinsic and intrinsic muscles. The extrinsic muscles arise from
The FOOT First & second layers of muscles of the sole introduction The muscles acting on the foot can be divided into two distinct groups; extrinsic and intrinsic muscles. The extrinsic muscles arise from
Feet First. Michael K. Cooper, DO FACOFP Family Practice/OMM St John Clinic - Claremore OOA 2018 Annual Convention
 Feet First Michael K. Cooper, DO FACOFP Family Practice/OMM St John Clinic - Claremore OOA 2018 Annual Convention Disclaimer I have no conflict of interest. I am not on any pharmaceutical company payroll
Feet First Michael K. Cooper, DO FACOFP Family Practice/OMM St John Clinic - Claremore OOA 2018 Annual Convention Disclaimer I have no conflict of interest. I am not on any pharmaceutical company payroll
What is Kinesiology? Basic Biomechanics. Mechanics
 What is Kinesiology? The study of movement, but this definition is too broad Brings together anatomy, physiology, physics, geometry and relates them to human movement Lippert pg 3 Basic Biomechanics the
What is Kinesiology? The study of movement, but this definition is too broad Brings together anatomy, physiology, physics, geometry and relates them to human movement Lippert pg 3 Basic Biomechanics the
Ankle Ligament Injury: Don t Worry- It s Only a Sprain Wes Jackson MD Orthopaedic Foot & Ankle
 Ankle Ligament Injury: Don t Worry- It s Only a Sprain Wes Jackson MD Orthopaedic Foot & Ankle Outline I. Epidemiology II. Classification and Types of Sprains III. Anatomy IV. Clinical Assessment and Imaging
Ankle Ligament Injury: Don t Worry- It s Only a Sprain Wes Jackson MD Orthopaedic Foot & Ankle Outline I. Epidemiology II. Classification and Types of Sprains III. Anatomy IV. Clinical Assessment and Imaging
11/2/17. Lateral Collateral Complex Medial Collateral Complex Distal Tibiofibular Syndesmosis Spring Ligament
 Andrew J Grainger Leeds, UK Lateral Collateral Complex ial Collateral Complex Distal Tibiofibular Syndesmosis Spring Ligament Brief anatomy review Scan tips and tricks Pathological appearances andrewgrainger@nhs.net
Andrew J Grainger Leeds, UK Lateral Collateral Complex ial Collateral Complex Distal Tibiofibular Syndesmosis Spring Ligament Brief anatomy review Scan tips and tricks Pathological appearances andrewgrainger@nhs.net
Arthroscopy Of the Ankle.
 Arthroscopy Of the Ankle www.fisiokinesiterapia.biz Ankle Arthroscopy Anatomy Patient setup Portal placement Procedures Complications Anatomy Portals Anterior Anteromedial Anterolateral Anterocentral Posterior
Arthroscopy Of the Ankle www.fisiokinesiterapia.biz Ankle Arthroscopy Anatomy Patient setup Portal placement Procedures Complications Anatomy Portals Anterior Anteromedial Anterolateral Anterocentral Posterior
We investigated a new method of stress
 SUBTALAR STRESS RADIOGRAPHY USING FORCED DORSIFLEXION AND SUPINATION TOMOO ISHII, SHUMPEI MIYAGAWA, TORU FUKUBAYASHI, KOICHIRO HAYASHI From the University of Tsukuba, Japan We investigated a new method
SUBTALAR STRESS RADIOGRAPHY USING FORCED DORSIFLEXION AND SUPINATION TOMOO ISHII, SHUMPEI MIYAGAWA, TORU FUKUBAYASHI, KOICHIRO HAYASHI From the University of Tsukuba, Japan We investigated a new method
Prevention and Treatment of Injuries. Anatomy. Anatomy. Tibia: the second longest bone in the body
 Prevention and Treatment of Injuries The Ankle and Lower Leg Westfield High School Houston, Texas Anatomy Tibia: the second longest bone in the body Serves as the principle weight-bearing bone of the leg.
Prevention and Treatment of Injuries The Ankle and Lower Leg Westfield High School Houston, Texas Anatomy Tibia: the second longest bone in the body Serves as the principle weight-bearing bone of the leg.
(v) Chronic ankle instability
 Chronic ankle instability") (v) Chronic ankle instability Hiro Tanaka Lyndon Mason Abstract Injuries to the ligaments of the ankle are common, especially in athletes. Symptomatic ankle instability develops in as many as 10e40% following
(v) Chronic ankle instability Hiro Tanaka Lyndon Mason Abstract Injuries to the ligaments of the ankle are common, especially in athletes. Symptomatic ankle instability develops in as many as 10e40% following
Musculoskeletal Ultrasound Technical Guidelines. VI. Ankle
 European Society of MusculoSkeletal Radiology Musculoskeletal Ultrasound Technical Guidelines VI. Ankle Ian Beggs, UK Stefano Bianchi, Switzerland Angel Bueno, Spain Michel Cohen, France Michel Court-Payen,
European Society of MusculoSkeletal Radiology Musculoskeletal Ultrasound Technical Guidelines VI. Ankle Ian Beggs, UK Stefano Bianchi, Switzerland Angel Bueno, Spain Michel Cohen, France Michel Court-Payen,
Main Menu. Ankle and Foot Joints click here. The Power is in Your Hands
 1 The Ankle and Foot Joints click here Main Menu Copyright HandsOn Therapy Schools 2009 K.8 http://www.handsonlineeducation.com/classes/k8/k8entry.htm[3/27/18, 1:40:03 PM] Ankle and Foot Joint 26 bones
1 The Ankle and Foot Joints click here Main Menu Copyright HandsOn Therapy Schools 2009 K.8 http://www.handsonlineeducation.com/classes/k8/k8entry.htm[3/27/18, 1:40:03 PM] Ankle and Foot Joint 26 bones
Understanding Leg Anatomy and Function THE UPPER LEG
 Understanding Leg Anatomy and Function THE UPPER LEG The long thigh bone is the femur. It connects to the pelvis to form the hip joint and then extends down to meet the tibia (shin bone) at the knee joint.
Understanding Leg Anatomy and Function THE UPPER LEG The long thigh bone is the femur. It connects to the pelvis to form the hip joint and then extends down to meet the tibia (shin bone) at the knee joint.
Ankle Sprains and Their Imitators
 Ankle Sprains and Their Imitators Mark Halstead, MD Dr. Mark Halstead is the Associate Professor of the Departments of Orthopedics and Pediatrics at Washington University School of Medicine; Director of
Ankle Sprains and Their Imitators Mark Halstead, MD Dr. Mark Halstead is the Associate Professor of the Departments of Orthopedics and Pediatrics at Washington University School of Medicine; Director of
CHAPTER 8: THE BIOMECHANICS OF THE HUMAN LOWER EXTREMITY
 CHAPTER 8: THE BIOMECHANICS OF THE HUMAN LOWER EXTREMITY _ 1. The hip joint is the articulation between the and the. A. femur, acetabulum B. femur, spine C. femur, tibia _ 2. Which of the following is
CHAPTER 8: THE BIOMECHANICS OF THE HUMAN LOWER EXTREMITY _ 1. The hip joint is the articulation between the and the. A. femur, acetabulum B. femur, spine C. femur, tibia _ 2. Which of the following is
17/10/2017. Foot and Ankle
 17/10/2017 Alicia M. Yochum RN, DC, DACBR, RMSK Foot and Ankle Plantar Fasciitis Hallux Valgus Deformity Achilles Tendinosis Posterior Tibialis Tendon tendinopathy Stress Fracture Ligamentous tearing Turf
17/10/2017 Alicia M. Yochum RN, DC, DACBR, RMSK Foot and Ankle Plantar Fasciitis Hallux Valgus Deformity Achilles Tendinosis Posterior Tibialis Tendon tendinopathy Stress Fracture Ligamentous tearing Turf
Elbow Elbow Anatomy. Flexion extension. Pronation Supination. Anatomy. Anatomy. Romina Astifidis, MS., PT., CHT
 Elbow Elbow Anatomy Romina Astifidis, MS., PT., CHT Curtis National Hand Center Baltimore, MD October 6-8, 2017 Link between the arm and forearm to position the hand in space Not just a hinge Elbow = 70%
Elbow Elbow Anatomy Romina Astifidis, MS., PT., CHT Curtis National Hand Center Baltimore, MD October 6-8, 2017 Link between the arm and forearm to position the hand in space Not just a hinge Elbow = 70%
Biokinesiology of the Ankle Complex
 Rehabilitation Considerations Following Ankle Fracture: Impact on Gait & Closed Kinetic Chain Function Disclosures David Nolan, PT, DPT, MS, OCS, SCS, CSCS I have no actual or potential conflict of interest
Rehabilitation Considerations Following Ankle Fracture: Impact on Gait & Closed Kinetic Chain Function Disclosures David Nolan, PT, DPT, MS, OCS, SCS, CSCS I have no actual or potential conflict of interest
BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY
 BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY B.Resseque, D.P.M. ARCH HEIGHT OFF WEIGHTBEARING Evaluate arch height by placing a ruler from the heel to the first metatarsal head Compare arch
BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY B.Resseque, D.P.M. ARCH HEIGHT OFF WEIGHTBEARING Evaluate arch height by placing a ruler from the heel to the first metatarsal head Compare arch
TENDON TRANSFER IN CAVUS FOOT
 TENDON TRANSFER IN CAVUS FOOT Cavovarus deformity is defined by fixed equinus of the forefoot on the hindfoot, resulting in a pathologic elevation of the longitudinal arch, with either a fixed or flexible
TENDON TRANSFER IN CAVUS FOOT Cavovarus deformity is defined by fixed equinus of the forefoot on the hindfoot, resulting in a pathologic elevation of the longitudinal arch, with either a fixed or flexible
Contents of the Posterior Fascial Compartment of the Thigh
 Contents of the Posterior Fascial Compartment of the Thigh 1-Muscles: B i c e p s f e m o r i s S e m i t e n d i n o s u s S e m i m e m b r a n o s u s a small part of the adductor magnus (h a m s t
Contents of the Posterior Fascial Compartment of the Thigh 1-Muscles: B i c e p s f e m o r i s S e m i t e n d i n o s u s S e m i m e m b r a n o s u s a small part of the adductor magnus (h a m s t
CHAPTER 80 BASIC CONSIDERATIONS
 Página 1 de 32 Copyright 2001 Lippincott Williams & Wilkins Loeser, John D. Bonica's Management of Pain, 3rd Edition CHAPTER 80 BASIC CONSIDERATIONS Part of "CHAPTER 80 - Pain in the Leg, Ankle, and Foot"
Página 1 de 32 Copyright 2001 Lippincott Williams & Wilkins Loeser, John D. Bonica's Management of Pain, 3rd Edition CHAPTER 80 BASIC CONSIDERATIONS Part of "CHAPTER 80 - Pain in the Leg, Ankle, and Foot"
Ankle Injuries: Anatomical and Biomechanical Considerations Necessary for the Development of an Injury Prevention Program
 0196-6011 /80/0103-0171$02.00/0 THE JOURNAL OF ORTHOPAEDIC AND SPORTS PHYSICAL THERAPY Copyright O 1980 by The Orthopaedic and Sports Medicine Sections of the American Physical Therapy Association Ankle
0196-6011 /80/0103-0171$02.00/0 THE JOURNAL OF ORTHOPAEDIC AND SPORTS PHYSICAL THERAPY Copyright O 1980 by The Orthopaedic and Sports Medicine Sections of the American Physical Therapy Association Ankle
Craig S. Radnay, M.D. 1/27/2016. Access to the Talus for Treatment of Osteochondral Lesions. Epidemiology of OLT. Treatment of OLT
 Access to the Talus for Treatment of Osteochondral Lesions Craig S. Radnay, MD, MPH ISK Institute for Orthopaedics and Sports Medicine NYU/Hospital for Joint Diseases Tampa, FL January 23, 2016 Epidemiology
Access to the Talus for Treatment of Osteochondral Lesions Craig S. Radnay, MD, MPH ISK Institute for Orthopaedics and Sports Medicine NYU/Hospital for Joint Diseases Tampa, FL January 23, 2016 Epidemiology
EDL EHL. Extensor Hallucis Longus L5 Extensor Digitorum longus L5,1 Peroneus Tertius L5 1 Extensor Digitorum Brevis S1,2 [like intrinsic muscle]
![EDL EHL. Extensor Hallucis Longus L5 Extensor Digitorum longus L5,1 Peroneus Tertius L5 1 Extensor Digitorum Brevis S1,2 [like intrinsic muscle]](/thumbs/78/77875930.jpg "EDL EHL. Extensor Hallucis Longus L5 Extensor Digitorum longus L5,1 Peroneus Tertius L5 1 Extensor Digitorum Brevis S1,2 [like intrinsic muscle]") ANATOMY OF ANKLE AND FOOT Lateral aspect: [Dorsal medial to lateral= dorsal under extensor retinaculum] Tibialis Anterior EHL Artery [Dorsal pedal A] and Anterior tibial N EDL Peroneus Tertius Behind the
ANATOMY OF ANKLE AND FOOT Lateral aspect: [Dorsal medial to lateral= dorsal under extensor retinaculum] Tibialis Anterior EHL Artery [Dorsal pedal A] and Anterior tibial N EDL Peroneus Tertius Behind the
بسم هللا الرحمن الرحيم
 بسم هللا الرحمن الرحيم Laboratory RHS 221 Manual Muscle Testing Theory 1 hour practical 2 hours Dr. Ali Aldali, MS, PT Department of Physical Therapy King Saud University Talocrural and Subtalar Joint
بسم هللا الرحمن الرحيم Laboratory RHS 221 Manual Muscle Testing Theory 1 hour practical 2 hours Dr. Ali Aldali, MS, PT Department of Physical Therapy King Saud University Talocrural and Subtalar Joint
Tarsal Coalition On MR
 Tarsal Coalition On MR By William Renner, M.D. This and other topics will be discussed in Tarsal coalition is a congenital anomaly with fusion of the tarsal bones. The fusion may be bony, fibrous or cartilaginous.
Tarsal Coalition On MR By William Renner, M.D. This and other topics will be discussed in Tarsal coalition is a congenital anomaly with fusion of the tarsal bones. The fusion may be bony, fibrous or cartilaginous.
What is the most frequently sprained ligament with inversion ankle sprains? 1/30/2014
 What is the most frequently sprained ligament with inversion ankle sprains? A. Anterior Talofibular B. Anterior Tibiofibular C. Calcaniofibular D. Posterior Talofibular E. Deltoid Lateral ligaments of
What is the most frequently sprained ligament with inversion ankle sprains? A. Anterior Talofibular B. Anterior Tibiofibular C. Calcaniofibular D. Posterior Talofibular E. Deltoid Lateral ligaments of
The Language of Anatomy. (Anatomical Terminology)
") The Language of Anatomy (Anatomical Terminology) Terms of Position The anatomical position is a fixed position of the body (cadaver) taken as if the body is standing (erect) looking forward with the upper
The Language of Anatomy (Anatomical Terminology) Terms of Position The anatomical position is a fixed position of the body (cadaver) taken as if the body is standing (erect) looking forward with the upper
THE LOWER EXTREMITY EXAM FOR THE FAMILY PRACTITIONER
 THE LOWER EXTREMITY EXAM FOR THE FAMILY PRACTITIONER Melinda A. Scott, D.O. Orthopedic Associates of Dayton Board Certified in Primary Care Sports Medicine GOALS Identify landmarks necessary for exam of
THE LOWER EXTREMITY EXAM FOR THE FAMILY PRACTITIONER Melinda A. Scott, D.O. Orthopedic Associates of Dayton Board Certified in Primary Care Sports Medicine GOALS Identify landmarks necessary for exam of
Biology 325 Fall 2003
 Name: pre-lab exercise due at beginning of your lab session Matching a. fibrous joints b. cartilaginous joints c. synovial joints 1. exhibit a joint cavity 2. types are sutures and syndesmoses 3. bones
Name: pre-lab exercise due at beginning of your lab session Matching a. fibrous joints b. cartilaginous joints c. synovial joints 1. exhibit a joint cavity 2. types are sutures and syndesmoses 3. bones
BLUE SKY SCHOOL OF PROFESSIONAL MASSAGE AND THERAPEUTIC BODYWORK Musculoskeletal Anatomy & Kinesiology KNEE & ANKLE MUSCLES
 BLUE SKY SCHOOL OF PROFESSIONAL MASSAGE AND THERAPEUTIC BODYWORK Musculoskeletal Anatomy & Kinesiology KNEE & ANKLE MUSCLES MSAK201-I Session 3 1) REVIEW a) THIGH, LEG, ANKLE & FOOT i) Tibia Medial Malleolus
BLUE SKY SCHOOL OF PROFESSIONAL MASSAGE AND THERAPEUTIC BODYWORK Musculoskeletal Anatomy & Kinesiology KNEE & ANKLE MUSCLES MSAK201-I Session 3 1) REVIEW a) THIGH, LEG, ANKLE & FOOT i) Tibia Medial Malleolus
Surgery-Ortho. Fractures of the tibia and fibula. Management. Treatment of low energy fractures. Fifth stage. Lec-6 د.
 Fifth stage Lec-6 د. مثنى Surgery-Ortho 28/4/2016 Indirect force: (low energy) Fractures of the tibia and fibula Twisting: spiral fractures of both bones Angulatory: oblique fractures with butterfly segment.
Fifth stage Lec-6 د. مثنى Surgery-Ortho 28/4/2016 Indirect force: (low energy) Fractures of the tibia and fibula Twisting: spiral fractures of both bones Angulatory: oblique fractures with butterfly segment.
Managing Tibialis Posterior Tendon Injuries
 Managing Tibialis Posterior Tendon Injuries by Thomas C. Michaud, DC Published April 1, 2015 by Dynamic Chiropractic Magazine Tibialis posterior is the deepest, strongest, and most central muscle of the
Managing Tibialis Posterior Tendon Injuries by Thomas C. Michaud, DC Published April 1, 2015 by Dynamic Chiropractic Magazine Tibialis posterior is the deepest, strongest, and most central muscle of the
Lateral TTC Plate SURGICAL TECHNIQUE
 MAXLOCK EXTREME Lateral TTC Plate SURGICAL TECHNIQUE Contents Overview 2 Exposure 3 Surgical Technique 4 Implants and Instruments 10 11 Proper surgical procedures and techniques are the responsibility
MAXLOCK EXTREME Lateral TTC Plate SURGICAL TECHNIQUE Contents Overview 2 Exposure 3 Surgical Technique 4 Implants and Instruments 10 11 Proper surgical procedures and techniques are the responsibility
High Ankle Sprains: Diagnosis & Treatment
 High Ankle Sprains: Diagnosis & Treatment Mark J. Mendeszoon, DPM, FACFAS, FACFAOM Precision Orthopaedic Specialties University Regional Hospitals Advanced Foot & Ankle Fellowship- Director It Is Only
High Ankle Sprains: Diagnosis & Treatment Mark J. Mendeszoon, DPM, FACFAS, FACFAOM Precision Orthopaedic Specialties University Regional Hospitals Advanced Foot & Ankle Fellowship- Director It Is Only
 P R E S E N T S Dr. Mufa T. Ghadiali is skilled in all aspects of General Surgery. His General Surgery Services include: General Surgery Advanced Laparoscopic Surgery Surgical Oncology Gastrointestinal
P R E S E N T S Dr. Mufa T. Ghadiali is skilled in all aspects of General Surgery. His General Surgery Services include: General Surgery Advanced Laparoscopic Surgery Surgical Oncology Gastrointestinal
Human Anatomy - Problem Drill 06: The Skeletal System Axial Skeleton & Articualtions
 Human Anatomy - Problem Drill 06: The Skeletal System Axial Skeleton & Articualtions Question No. 1 of 10 Instructions: (1) Read the problem and answer choices carefully, (2) Work the problems on paper
Human Anatomy - Problem Drill 06: The Skeletal System Axial Skeleton & Articualtions Question No. 1 of 10 Instructions: (1) Read the problem and answer choices carefully, (2) Work the problems on paper
Results of Calcaneal Osteotomy & Flexor Digitorum Longus transfer in Stage II Acquired Flatfoot Deformity
 Results of Calcaneal Osteotomy & Flexor Digitorum Longus transfer in Stage II Acquired Flatfoot Deformity Mr Amit Chauhan Mr Prasad Karpe Ms Maire-claire Killen Mr Rajiv Limaye University Hospital of North
Results of Calcaneal Osteotomy & Flexor Digitorum Longus transfer in Stage II Acquired Flatfoot Deformity Mr Amit Chauhan Mr Prasad Karpe Ms Maire-claire Killen Mr Rajiv Limaye University Hospital of North
Clinical evaluation where no obvious fracture a. Squeeze test
 7:43 am The Syndesmotic Injury: From Subtle to Severe Robert B. Anderson, MD Chief, Foot and Ankle Carolinas Medical Center OrthoCarolina (Charlotte, North Carolina) 7:30-8:25 am Symposium 1: Management
7:43 am The Syndesmotic Injury: From Subtle to Severe Robert B. Anderson, MD Chief, Foot and Ankle Carolinas Medical Center OrthoCarolina (Charlotte, North Carolina) 7:30-8:25 am Symposium 1: Management
Anterior Impingement
 Anterior Impingement Ziali Sivardeen BMedSci, (MRCS), AFRCS, FRCS (Tr & Orth) Consultant Trauma and Orthopaedic Surgeon (Shoulder, Knee and Sports Injuries) Aims Causes of Anterior Ankle Pain Ankle Impingement
Anterior Impingement Ziali Sivardeen BMedSci, (MRCS), AFRCS, FRCS (Tr & Orth) Consultant Trauma and Orthopaedic Surgeon (Shoulder, Knee and Sports Injuries) Aims Causes of Anterior Ankle Pain Ankle Impingement
SUB-TALAR AND TRIPLE ARTHRODESIS
 SUB-TALAR AND TRIPLE ARTHRODESIS J de Halleux With the members of Education Committee INDICATIONS ARTHRITIS OF THE SUB-TALAR AND/OR MID-TARSAL JOINTS RIGID VARUS OR VALGUS DEFORMITY OF THE HIND-FOOT COALITIONS
SUB-TALAR AND TRIPLE ARTHRODESIS J de Halleux With the members of Education Committee INDICATIONS ARTHRITIS OF THE SUB-TALAR AND/OR MID-TARSAL JOINTS RIGID VARUS OR VALGUS DEFORMITY OF THE HIND-FOOT COALITIONS
The University Of Jordan Faculty Of Medicine FOOT. Dr.Ahmed Salman Assistant Prof. of Anatomy. The University Of Jordan
 The University Of Jordan Faculty Of Medicine FOOT Dr.Ahmed Salman Assistant Prof. of Anatomy. The University Of Jordan Tarsal Tunnel Syndrome Due to compression of Tibial nerve as it travels through the
The University Of Jordan Faculty Of Medicine FOOT Dr.Ahmed Salman Assistant Prof. of Anatomy. The University Of Jordan Tarsal Tunnel Syndrome Due to compression of Tibial nerve as it travels through the
Determining Sensitive and Accurate Measures for Detecting Balance Deficits Associated with Functional Ankle Instability
 Virginia Commonwealth University VCU Scholars Compass Theses and Dissertations Graduate School 2009 Determining Sensitive and Accurate Measures for Detecting Balance Deficits Associated with Functional
Virginia Commonwealth University VCU Scholars Compass Theses and Dissertations Graduate School 2009 Determining Sensitive and Accurate Measures for Detecting Balance Deficits Associated with Functional
حسام أبو عوض. - Ahmad. 1 P a g e
 - 9 حسام أبو عوض - - Ahmad 1 P a g e In the last lecture, we finished discussing the superficial part of the posterior compartment and the popliteus muscle of the deep layer[reminder: The entire posterior
- 9 حسام أبو عوض - - Ahmad 1 P a g e In the last lecture, we finished discussing the superficial part of the posterior compartment and the popliteus muscle of the deep layer[reminder: The entire posterior
A Patient s Guide to Ankle Anatomy
 A Patient s Guide to Ankle Anatomy 245 North College Lafayette, LA 70506 Phone: 337.232.5301 Fax: 337.237.6504 DISCLAIMER: The information in this booklet is compiled from a variety of sources. It may
A Patient s Guide to Ankle Anatomy 245 North College Lafayette, LA 70506 Phone: 337.232.5301 Fax: 337.237.6504 DISCLAIMER: The information in this booklet is compiled from a variety of sources. It may
Disclosures. Syndesmosis Injury. Syndesmosis Ligaments. Objectives. Mark M. Casillas, M.D.
 Disclosures Syndesmosis Injury No relevant disclosures Mark M. Casillas, M.D. 1 Objectives Syndesmosis Ligaments Understand the syndesmosis anatomy and function Classify syndesmosis injuries Describe treatment
Disclosures Syndesmosis Injury No relevant disclosures Mark M. Casillas, M.D. 1 Objectives Syndesmosis Ligaments Understand the syndesmosis anatomy and function Classify syndesmosis injuries Describe treatment
A Patient s Guide to Ankle Anatomy
 A Patient s Guide to Ankle Anatomy 1436 Exchange Street Middlebury, VT 05753 Phone: 802-388-3194 Fax: 802-388-4881 cvo@champlainvalleyortho.com DISCLAIMER: The information in this booklet is compiled from
A Patient s Guide to Ankle Anatomy 1436 Exchange Street Middlebury, VT 05753 Phone: 802-388-3194 Fax: 802-388-4881 cvo@champlainvalleyortho.com DISCLAIMER: The information in this booklet is compiled from
The Elbow and the cubital fossa. Prof Oluwadiya Kehinde
 The Elbow and the cubital fossa Prof Oluwadiya Kehinde www.oluwadiya.com Elbow and Forearm Anatomy The elbow joint is formed by the humerus, radius, and the ulna Bony anatomy of the elbow Distal Humerus
The Elbow and the cubital fossa Prof Oluwadiya Kehinde www.oluwadiya.com Elbow and Forearm Anatomy The elbow joint is formed by the humerus, radius, and the ulna Bony anatomy of the elbow Distal Humerus
Surgical Technique Guide
 Guide CAUTION: Federal Law (USA) restricts this device to sale by or on the order of a physician. INDICATIONS FOR USE The Align Anterior Ankle Fusion Plate is intended to facilitate arthrodesis of the
Guide CAUTION: Federal Law (USA) restricts this device to sale by or on the order of a physician. INDICATIONS FOR USE The Align Anterior Ankle Fusion Plate is intended to facilitate arthrodesis of the
BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY 2017
 BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY 2017 B. RESSEQUE, D.P.M., D.A.B.P.O. Professor, N.Y. College of Podiatric Medicine ARCH HEIGHT OFF WEIGHTBEARING Evaluate arch height by placing
BIOMECHANICAL EXAMINATION OF THE PEDIATRIC LOWER EXTREMITY 2017 B. RESSEQUE, D.P.M., D.A.B.P.O. Professor, N.Y. College of Podiatric Medicine ARCH HEIGHT OFF WEIGHTBEARING Evaluate arch height by placing
Unraveling the Mystery of Ankle Pain #4: Medial Ligament Sprains
 Unraveling the Mystery of Ankle Pain #4: Medial Ligament Sprains 1 Instructor: Ben Benjamin, Ph.D. 2 1 Instructor: Ben Benjamin, Ph.D. 3 Webinar Goals Explore the Assessment and Treatment of Medial Ankle
Unraveling the Mystery of Ankle Pain #4: Medial Ligament Sprains 1 Instructor: Ben Benjamin, Ph.D. 2 1 Instructor: Ben Benjamin, Ph.D. 3 Webinar Goals Explore the Assessment and Treatment of Medial Ankle
Review relevant anatomy of the foot and ankle. Learn the approach to examining the foot and ankle
 Objectives Review relevant anatomy of the foot and ankle Learn the approach to examining the foot and ankle Learn the basics of diagnosis and treatment of ankle sprains Overview of other common causes
Objectives Review relevant anatomy of the foot and ankle Learn the approach to examining the foot and ankle Learn the basics of diagnosis and treatment of ankle sprains Overview of other common causes
Cavus Foot: Subtle and Not-So-Subtle AOFAS Resident Review Course September 28, 2013
 Cavus Foot: Subtle and Not-So-Subtle Course September 28, 2013 Matthew M. Roberts, MD Associate Professor of Clinical Orthopaedic Surgery Co-Chief, Foot and Ankle Service Hospital for Special Surgery Disclosure
Cavus Foot: Subtle and Not-So-Subtle Course September 28, 2013 Matthew M. Roberts, MD Associate Professor of Clinical Orthopaedic Surgery Co-Chief, Foot and Ankle Service Hospital for Special Surgery Disclosure