Surgical Approaches for Fractures and Injuries of the Pelvic Ring
|
|
|
- Lester Carpenter
- 5 years ago
- Views:
Transcription
1 Surgical Approaches for Fractures and Injuries of the Pelvic Ring Mara L. Schenker, MD Emory University / Grady Hospital Created by Steven A. Olson, MD in 2004 and Kyle Dickson, MD in 2004 First revised by Rafael Neiman, MD and Sean Nork in 2007 Second Revision by James C. Krieg, MD in 2009 and Sean Nork, MD in 2010 Third Revision by Mara Schenker and Clifford Jones in 2016
2 Goals Indications: non-operative vs. operative Acute management Definitive management Surgical approaches Reduction Fixation
3 Pelvic Ring Stability Biomechanical stability = ability to support a physiological load, and is dependent on an intact posterior sacroiliac ligamentous complex for load transfer from axial to appendicular skeleton
4 Pelvic Ring Instability Biomechanical Instability Posterior ring injuries frequently lead to instability Anterior ring injuries MAY lead to instability, and are often associated with posterior ring injuries Tile Classification based on instability May lead to hemodynamic instability If untreated, may lead to permanent disability from pelvis mobility
5 Assessing Stability Is there deformity? Is there posterior ring involvement? Are there associated injuries? Is there displacement with stress examination?

6 eformity: Predicts Instability

7 Posterior ring injury: ligamentous and bony injury predict instability


8 Associated injuries predict instability: L5 transverse process fracture; ischial spine avulsion, lateral sacral avulsion



9 Stress examination: external rotation, internal rotation, lower extremity push-pull while taking AP, inlet and outlet projections
 stance views are")

10 Stress examination: flamingo (single-leg) stance views are beneficial in diagnosing occult pelvic ring ligamentous injuries
11 Describing Instability Refer to previous lecture on Classification Tile Classification A stable B partially stable C unstable
12 Resuscitation Mobilization Operative Indications Just as stabilizing long bones helps in mobilization of polytrauma patients Preventing long term functional impairment Malunion can affect function (bladder, dyspareunia, sitting imbalance, leg length inequality, mechanical low back pain) and quality of life
13 Non-Operative Indications Lateral impaction type injuries, without cephalad displacement or excessive hemipelvis rotation Pubic symphyseal widening < 2.5 cm Without associated SI injury Assuming no motion with stress or mobilization This number is not absolute, so other evidence of instability (like SI injury) must be ruled out
14 Non-Operative Treatment: TILE A Stable injuries can generally WBAT Serial radiographs Displacement requires reassessment of stability and consideration given to operative treatment
15 Non-Operative Treatment: TILE B Partially stable injuries can be treated nonoperatively if deformity is minimal Weight bearing should be restricted (TTWB) on side of posterior ring injury Serial radiographs Displacement requires reassessment of stability and consideration given to operative treatment
16 Resuscitation, Containment, Angiography ACUTE MANAGEMENT
17 An unstable pelvic ring injury may allow hemorrhage to collect in the true pelvis. There is no longer a constraint to tamponade. Volume is best estimated by a hemi-elliptical sphere. (Stover, J Trauma, 2006
18 ATLS Protocol Airway maintenance with cervical spine protection Breathing and ventilation Circulation with hemorrhage control Disability: Neurologic status Exposure/environment control: undress patient but prevent hypothemia
19 Physical Examination Open wounds Degloving injuries Blood at the urethral meatus Perineal and scrotal ecchymosis Neurologic deficiency

20 OPEN WOUNDS Perineum, anterior pelvis, vagina, rectum Aggressive debridement and closure Consider diverting colostomy

21 15% incidence Blood at meatus Urologic Injuries Bladder ruptures are usually repaired Urethral injuries can be repaired on a delayed basis Foleys or tunneled suprapubic catheters are preferred to avoid surgical site contamination
22 Hemorrhage Management AP pelvis with an understanding of the mechanism of injury helps determine whether the pelvis is a source of bleeding in the hemodynamically unstable patient APC injuries have increased need for blood transfusion (Burgess J Trauma 1990)
23 Methods of Hemorrhage Control Pelvic containment Binder Sheet External fixation Angiography Laparotomy, with or without packing


24 BEFORE Sheet AFTER Sheet
25 Pelvic Binders Commercially available. Placed over the TROCHANTERS and not over the abdomen.
26 External Fixation Location AIIS Clinical Application Resuscitative Iliac crest Augmentative C-clamp Definitive
27 External Fixation: AIIS frames Advantages: Thought to be biomechanically superior to crest frames Patients can sit



28 Fluoro dependent: Starting point on obturator outlet Pins placed on iliac oblique and obturator inlet views Incisions directed toward final anticipated location Can leave in sheet and cut a hole

29
 Aim: 30 to 45 degrees (from lateral to")
30 ASIS Ex Fix Pin Placement Fluoro dependent: 3 to 5 cm posterior to the ASIS Along gluteus medius pillar Incisions directed toward final anticipated pin location Pin entry at the junction of the lateral 2/3 and medial 1/3 of the iliac crest (lateral overhang of the crest) Aim: 30 to 45 degrees (from lateral to medial)

31 External fixation: C-Clamp Better posterior pelvic ring stabilization Allows abdominal access Can be combined with pelvic packing


32 External Fixation: C-Clamp Similar starting point to iliosacral screw Allows for maximum compression Can be identified without fluoro in experienced hands


33 Caution! Avoid over-compression in sacral fractures
34 Pelvic Packing Direct retroperitoneal packing, Pfannenstiel approach Combine with mechanical stabilization (internal versus external) May decrease need for transfusion, make angiography more efficient, and decrease mortality; requires additional OR trips and may increase incidence of abdominal compartment syndrome
35 Angiography Arterial bleeding Selective embolization is preferable to minimize ischemic complications Successful embolization rates for arterial injuries: % Early angiography within minutes improves mortality
36 Management Summary: Hemodynamically Unstable Injuries Biffl et al, Evolution of a mutlidisciplinary clinical pathway for the management of unstable patients with pelvic fractures. JOT, elements: Immediate trauma surgeon availability (+ Ortho!) Early simultaneous blood and coagulation products Prompt diagnosis & treatment of life threatening injuries Stabilization of the pelvic girdle Timely pelvic angiography and embolization Changes: Patients more severely injured (52% vs 35% SBP < 90) DPL phased out for U/S Pelvic binders and C-clamps replaced traditional ex fix
37 Management Summary: Hemodynamically Unstable Injuries Biffl et al, Evolution of a mutlidisciplinary clinical pathway for the management of unstable patients with pelvic fractures. JOT, 2001 Mortality decreased from 31% to 15% Exsanguination death from 9% to 1% MOF from 12% to 1% Death (<24 hours) from 16% to 5% The evolution of a multidisciplinary clinical pathway, coordinating the resources of a level 1 trauma center and directed by joint decision making between trauma surgeons and orthopedic traumatologists, has resulted in improved patient survival. The primary benefits appear to be in reducing early deaths from exsanguination and late deaths from multiple organ failure.
38 Summary: Acute Management Play well with others (general surgery, urology, interventional radiology, neurosurgery) Understand the fracture pattern Do something (sheet, binder, ex fix, c-clamp) Combine knowledge of the fracture, the patients condition, and the physical exam to decide on the next step
39 Approaches, Reduction, Fixation DEFINITIVE MANAGEMENT
40 Principles of Definitive Operative Treatment Primary goal: prevent malunion With complete disruption of the posterior ring, anterior fixation alone is inadequate With instability of the posterior ring and cephalad displacement, posterior fixation should be supplemented with anterior fixation (ORIF or ex fix)
41 Biomechanics of Pelvic Fixation No clinical comparison studies exist Experimental biomechanical data exist In general, it seems that more points/planes of fixation provide better stability How much stability is enough is injury dependant
42 Preoperative Planning Consider patient-related factors: resuscitation, coordination of care (trauma surgeon, intensivist, neurosurgery, urology, gynecology), examine soft tissues, is it safe to position prone if needed? Consider timing: reduction may be easier (particularly for percutaneous fixation) in first hours; risk of second hit in days 2-5 (particularly for open surgery)
43 Preoperative Planning Intraoperative imaging Radiolucent table Fluoroscopy Radiologic Technician and Surgeon understand C- arm views necessary Reduction tools Traction Pelvic manipulator (e.g. femoral distractor) Specialized clamps
44 Preoperative Planning Implants needed Extra-long screws Cannulated screws, often extra-long with appropriate instruments Specialized plates for contourability (reconstruction plates) External fixation
45 Surgical Approach: Anterior Pelvic Ring Pfannenstiel approach Exposure of symphysis pubis and pubic bones Longitudinal incision along the fascia of the linea alba Elevate rectus subperiosteally, protect the bladder with a malleable retractor Kain, Tornetta Op Tech Orthop
46 Surgical Approach: Anterior Pelvic Ring Stoppa extension Exposes symphysis to SI joint along pelvic brim Care taken laterally, as the corona mortis tends to be 6 cm lateral to the pubic symphysis (anastamosis between obturator and external iliac vessels)
47 Surgical Approach: Posterior Pelvic Ring Lateral window of the ilioinguinal approach Exposure of sacroiliac joint anteriorly Avoid injury to the L5 nerve root with retractor placement anteriorly along the sacrum
48 Surgical Approach: Posterior Pelvic Ring Paramedian approach Exposure of sacrum and posterior ilium Sacral fractures Iliac fracture dislocations of the SI joint (crescent fracture) Allows simultaneous reduction and lumbopelvic fixation when necessary
49 Reduction and Fixation: Symphysis Weber clamp placed through drill holes anteriorly Kain, Tornetta Op Tech Orthop

50 Reduction and Fixation: Symphysis Jungbluth clamp with screws

51 Reduction and Fixation: Symphysis Pelvic reconstruction plate Commonly 6 hole plate Variable directions of screws

52 Reduction and Fixation: Ramus Pelvic reconstruction plate


53 Reduction and Fixation: Ramus Medullary screw fixation: antegrade or retrograde Fluoroscopic views: obturator outlet and inlet
54 Biomechanics of Pelvic Fixation: Anterior Fixation Anterior plating superior to external fixation in internal/external rotation Neither technique very effective at control of vertical displacement Anterior fixation can protect posterior fixation from failure
55 Biomechanics of Pelvic Fixation: Anterior Fixation Two hole symphyseal plate inadequate Retrograde pubic screw higher failure rate than antegrade
56 Reduction and Fixation: SI joint fracture-dislocation Jungbluth clamp Anterior provisional or definitive plating

57 Reduction and Fixation: SI joint fracture-dislocation

 Fully threaded for improved fixation Knowledge of anatomy")
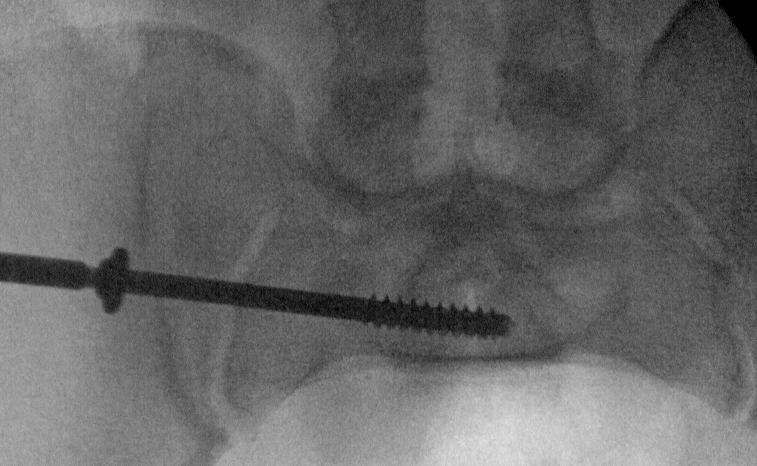
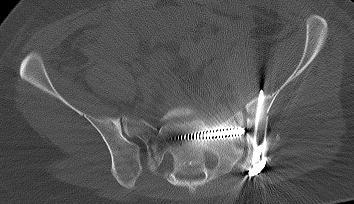
58 Reduction and Fixation: Percutaneous SI screw Cannulated for ease of placement Partially threaded for reduction (6.5 mm, 7.3 mm, or 8.0 mm) Fully threaded for improved fixation Knowledge of anatomy and imaging is essential Be aware of sacral dysmorphism



59 Inlet Outlet Cannulated drill allows predictable small changes in trajectory



60

61 20 degree rollover view to assess screw down to bone


62 Reduction and Fixation: Posterior plate Crescent fractures

63
64 Reduction and Fixation: Sacral Fracture Indirect reduction Anterior ring reduction Traction Distractor
65 Reduction and Fixation: Sacral Fracture Direct reduction Posterior exposure Clamp application (Pointed Weber clamps) Can decompress as well if needed Can perform lumbopelvic fixation if needed


66 Reduction and Fixation: Sacral Fracture Iliosacral screws Upper 2 sacral segments Fully threaded screws Know morphology, anatomy

67 Reduction and Fixation: Sacral Fractures Lumbopelvic fixation Vertical control Can be useful in unstable H or Y type sacral fracture and sacral fractures in the setting of severe dysmorphism Transiliac plating
68 Biomechanics of Pelvic Fixation: Posterior Fixation Options include single SI screw, multiple SI screws, double plating of SI joint, transiliac plate of sacral fracture, or plate plus SI screw for sacral fracture or SI dislocation Any of the above are more stable than single SI screw in unstable injuries
69 Biomechanics of Pelvic Fixation: Lumbopelvic fixation Posterior Fixation Lumbopelvic dissociation (unstable Y, H, or U type sacral fractures) Sacral fractures with significant instability Can provide axial (vertical) stability that is not as dependant on fracture reduction/stability
70 Post-Operative Protocol Mobilize when systemic and physiologic status allow Any complete disruption of posterior ring should be immobilized with touch-down weightbearing for 10 to 12 weeks Incomplete posterior ring disruptions can typically be allowed full weightbearing as tolerated
71 Outcomes Pain common Improvement occurs for at least a year in most patients Neurologic injury most common predictor of poor outcome
72 Outcomes SI dislocations have poor tolerance for residual displacement Sacral fractures have more tolerance for displacement, but parameters poorly understood Injury Severity Score and fracture type do not correlate with functional outcome
73 Conclusions: Pelvic Ring Injury Complex constellation of injuries Treatment based on comprehensive understanding of potential pelvic ring instability, displacement, and associated injuries Surgical techniques for reduction and stabilization continue to evolve
74 For questions or comments, please send to
The Acute Management of Pelvic Ring Injuries
 The Acute Management of Pelvic Ring Injuries Brian J Ladner, MD North Oaks Medical Center Original Author: Kyle F. Dickson, MD; Created March 2004 Sean E. Nork, MD; Revised December 2010 New Author: October
The Acute Management of Pelvic Ring Injuries Brian J Ladner, MD North Oaks Medical Center Original Author: Kyle F. Dickson, MD; Created March 2004 Sean E. Nork, MD; Revised December 2010 New Author: October
Pelvic Injuries. Chapter 21
 Chapter 21 Introduction Injuries of the pelvis are an uncommon, but potentially lethal, battlefield injury. Blunt injuries may be associated with major hemorrhage and early mortality. Death within the
Chapter 21 Introduction Injuries of the pelvis are an uncommon, but potentially lethal, battlefield injury. Blunt injuries may be associated with major hemorrhage and early mortality. Death within the
Pelvic fractures. Dr Raymond Yean, MBBS Surgical SRMO
 Pelvic fractures Dr Raymond Yean, MBBS Surgical SRMO PELVIC FRACTURES Pelvic fracture account for 2-8% all skeletal injuries Associated with High energy trauma Soft tissue injuries and blood loss. Shock,
Pelvic fractures Dr Raymond Yean, MBBS Surgical SRMO PELVIC FRACTURES Pelvic fracture account for 2-8% all skeletal injuries Associated with High energy trauma Soft tissue injuries and blood loss. Shock,
Iliosacral Screws Indications. What Injuries Are Amenable? CRPFPP Indications Injured Zones 11/18/2013
 Iliosacral Screws Indications ML Chip Routt Jr MD UT Houston Orthopedics Houston, Texas What Injuries Are Amenable? Sacroiliac Sacral Iliac Combination CRPFPP Indications Injured Zones SI Joint Sacral
Iliosacral Screws Indications ML Chip Routt Jr MD UT Houston Orthopedics Houston, Texas What Injuries Are Amenable? Sacroiliac Sacral Iliac Combination CRPFPP Indications Injured Zones SI Joint Sacral
10/2/2018. Acute Management of Pelvic Injuries. Learning Objectives. 17 yo male ped struck by truck
 17 yo male ped struck by truck Acute Management of Pelvic Injuries David Volgas, MD CoxHealth University of Missouri HD unstable Open pelvic wound superior gluteal fold through rectum to scrotum Open rami
17 yo male ped struck by truck Acute Management of Pelvic Injuries David Volgas, MD CoxHealth University of Missouri HD unstable Open pelvic wound superior gluteal fold through rectum to scrotum Open rami
Hassan R. Mir, MD, MBA, FACS
 DISCLOSURES Hassan R. Mir, MD, MBA, FACS Paid Consultant for a Company or Supplier Smith & Nephew Zimmer Biomet Trice Medical Stock or Stock Options Core Orthopaedics OrthoGrid Systems Research Support
DISCLOSURES Hassan R. Mir, MD, MBA, FACS Paid Consultant for a Company or Supplier Smith & Nephew Zimmer Biomet Trice Medical Stock or Stock Options Core Orthopaedics OrthoGrid Systems Research Support
Pelvic Fractures. AOCP National Course Belfast City Hospital. 11 th June D Swain BSc; FRCSI; FRCS (Orth.)
") Pelvic Fractures AOCP National Course Belfast City Hospital 11 th June 2010 Who s this bloke? Consultant orthopaedic surgeon RVH Trained in Belfast, England and Toronto Interests - pelvic and acetabular
Pelvic Fractures AOCP National Course Belfast City Hospital 11 th June 2010 Who s this bloke? Consultant orthopaedic surgeon RVH Trained in Belfast, England and Toronto Interests - pelvic and acetabular
THE INITIAL MANAGEMENT OF PELVIC AND ACETABULAR TRAUMA LOUIS LEBLOND MD FRCSC DEPT OF ORTHOPAEDICS THE MONCTON HOSPITAL - L HÔPITAL DE MONCTON
 THE INITIAL MANAGEMENT OF PELVIC AND ACETABULAR TRAUMA LOUIS LEBLOND MD FRCSC DEPT OF ORTHOPAEDICS THE MONCTON HOSPITAL - L HÔPITAL DE MONCTON DISCLOSURES + BACKGROUND No. Centre de formation médicale
THE INITIAL MANAGEMENT OF PELVIC AND ACETABULAR TRAUMA LOUIS LEBLOND MD FRCSC DEPT OF ORTHOPAEDICS THE MONCTON HOSPITAL - L HÔPITAL DE MONCTON DISCLOSURES + BACKGROUND No. Centre de formation médicale
Anterior Pelvic Plating and Sacroiliac Joint Fixation in Unstable Pelvic Ring Injuries
 Original Article http://dx.doi.org/10.3349/ymj.2012.53.2.422 pissn: 0513-5796, eissn: 1976-2437 Yonsei Med J 53(2):422-426, 2012 Anterior Pelvic Plating and Sacroiliac Joint Fixation in Unstable Pelvic
Original Article http://dx.doi.org/10.3349/ymj.2012.53.2.422 pissn: 0513-5796, eissn: 1976-2437 Yonsei Med J 53(2):422-426, 2012 Anterior Pelvic Plating and Sacroiliac Joint Fixation in Unstable Pelvic
West Yorkshire Major Trauma Network Clinical Guidelines 2015
 WYMTN: Pelvic fracture with urogenital trauma KEY RECOMMENDATIONS 1. During the initial exploratory survey / secondary survey, a. The external urethral meatus and the transurethral bladder catheter (if
WYMTN: Pelvic fracture with urogenital trauma KEY RECOMMENDATIONS 1. During the initial exploratory survey / secondary survey, a. The external urethral meatus and the transurethral bladder catheter (if
Pelvis injuries Fractures of the femur (proximal,shaft) Dr Tamás Bodzay
 Dr Tamás Bodzay") Pelvis injuries Fractures of the femur (proximal,shaft) Dr Tamás Bodzay Pelvis anatomy Pelvis function - axial load bearing - protection: abdominal, pelvic structures Pelvic injury mechanism Falling from
Pelvis injuries Fractures of the femur (proximal,shaft) Dr Tamás Bodzay Pelvis anatomy Pelvis function - axial load bearing - protection: abdominal, pelvic structures Pelvic injury mechanism Falling from
Initial Management of Pelvic Injuries
 Initial Management of Pelvic Injuries Olav Røise, MD, PhD Chairman Division of Neuroscience and Skeletal Medicine Ullevål University Hospital Trauma treatment Represent a chain of health services in which
Initial Management of Pelvic Injuries Olav Røise, MD, PhD Chairman Division of Neuroscience and Skeletal Medicine Ullevål University Hospital Trauma treatment Represent a chain of health services in which
Initial Pelvic Fracture Management. Patrick M Reilly MD FACS February 27, 2010
 Initial Pelvic Fracture Management Patrick M Reilly MD FACS February 27, 2010 John Pryor MD Field Triage* * Step One : Physiology * Step Two : Anatomy * Step Three : Mechanism * Step Four : Co-Morbid Conditions
Initial Pelvic Fracture Management Patrick M Reilly MD FACS February 27, 2010 John Pryor MD Field Triage* * Step One : Physiology * Step Two : Anatomy * Step Three : Mechanism * Step Four : Co-Morbid Conditions
RADIOLOGY OF THE NORMAL ACETABULUM. X-ray X-ray X-ray. Figure. Figure ILIAC OBLIQUE VIEW OBTURATOR OBLIQUE VIEW AP VIEW
 RADIOLOGY OF THE NORMAL ACETABULUM Six radiological landmarks should be recognized on the Anterior Posterior radiograph: 1. Posterior wall of the acetabulum 2. Anterior wall of the acetabulum 3. Roof /
RADIOLOGY OF THE NORMAL ACETABULUM Six radiological landmarks should be recognized on the Anterior Posterior radiograph: 1. Posterior wall of the acetabulum 2. Anterior wall of the acetabulum 3. Roof /
The Lower Limb. Anatomy RHS 241 Lecture 2 Dr. Einas Al-Eisa
 The Lower Limb Anatomy RHS 241 Lecture 2 Dr. Einas Al-Eisa The bony pelvis Protective osseofibrous ring for the pelvic viscera Transfer of forces to: acetabulum & head of femur (when standing) ischial
The Lower Limb Anatomy RHS 241 Lecture 2 Dr. Einas Al-Eisa The bony pelvis Protective osseofibrous ring for the pelvic viscera Transfer of forces to: acetabulum & head of femur (when standing) ischial
DISTRACTION EXTERNAL FIXATIONS OF PELVIC FRACTURES CAUSED BY A LATERAL COMPRESSION
 DOI: 10.5272/jimab.2011171.161 Journal of IMAB - Annual Proceeding (Scientific Papers) 2011, vol. 17, book 1 DISTRACTION EXTERNAL FIXATIONS OF PELVIC FRACTURES CAUSED BY A LATERAL COMPRESSION Pavlin Apostolov,
DOI: 10.5272/jimab.2011171.161 Journal of IMAB - Annual Proceeding (Scientific Papers) 2011, vol. 17, book 1 DISTRACTION EXTERNAL FIXATIONS OF PELVIC FRACTURES CAUSED BY A LATERAL COMPRESSION Pavlin Apostolov,
Table 2. First Generated List of Expert Responses. Likert-Type Scale. Category or Criterion. Rationale or Comments (1) (2) (3) (4)
 (2) (3) (4)") Table 2. First Generated List of Expert Responses. Likert-Type Scale Category or Criterion Anatomical Structures and Features Skeletal Structures and Features (1) (2) (3) (4) Rationale or Comments 1. Bones
Table 2. First Generated List of Expert Responses. Likert-Type Scale Category or Criterion Anatomical Structures and Features Skeletal Structures and Features (1) (2) (3) (4) Rationale or Comments 1. Bones
LAB Notes#1. Ahmad Ar'ar. Eslam
 LAB Notes#1 Ahmad Ar'ar Eslam 1 P a g e Anatomy lab Notes Lower limb bones :- Pelvic girdle: It's the connection between the axial skeleton and the lower limb; it's made up of one bone called the HIP BONE
LAB Notes#1 Ahmad Ar'ar Eslam 1 P a g e Anatomy lab Notes Lower limb bones :- Pelvic girdle: It's the connection between the axial skeleton and the lower limb; it's made up of one bone called the HIP BONE
Unstable fractures of the pelvis treated with a trapezoid compression frame
 Acta Orthop Scand 55, 325-329, 1984 Unstable fractures of the pelvis treated with a trapezoid compression frame Sixteen patients with unstable pelvic fractures were treated by early reduction and fixation
Acta Orthop Scand 55, 325-329, 1984 Unstable fractures of the pelvis treated with a trapezoid compression frame Sixteen patients with unstable pelvic fractures were treated by early reduction and fixation
Intracanal Sacral Nerve Impingement Following Percutaneous Iliosacral Screw Pelvic Fixation
 texas orthopaedic journal CASE REPORT Intracanal Sacral Nerve Impingement Following Percutaneous Iliosacral Screw Pelvic Fixation Michael L. Brennan, MD; John M. Hamilton, MD; Christopher D. Chaput, MD;
texas orthopaedic journal CASE REPORT Intracanal Sacral Nerve Impingement Following Percutaneous Iliosacral Screw Pelvic Fixation Michael L. Brennan, MD; John M. Hamilton, MD; Christopher D. Chaput, MD;
Is there a clinical benefit of additional tension band wiring in plate fixation of the symphysis?
 Park et al. BMC Musculoskeletal Disorders (2017) 18:40 DOI 10.1186/s12891-017-1418-3 RESEARCH ARTICLE Open Access Is there a clinical benefit of additional tension band wiring in plate fixation of the
Park et al. BMC Musculoskeletal Disorders (2017) 18:40 DOI 10.1186/s12891-017-1418-3 RESEARCH ARTICLE Open Access Is there a clinical benefit of additional tension band wiring in plate fixation of the
Clinical Module. Pelvic Injury Trauma. Princess Alexandra Hospital Emergency Department. 1 Introduction
 Princess Alexandra Hospital Emergency Department Clinical Module Trauma Review Officers: Katherine Isoardi / Glenn Ryan Version no: 2 Review date: Aug 2015 Key Words: Pelvic Trauma, Pelvic Injury, Pelvic
Princess Alexandra Hospital Emergency Department Clinical Module Trauma Review Officers: Katherine Isoardi / Glenn Ryan Version no: 2 Review date: Aug 2015 Key Words: Pelvic Trauma, Pelvic Injury, Pelvic
Damage Control in Abdominal and Pelvic Injuries
 Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
Skeletal System Module 13: The Pelvic Girdle and Pelvis
 OpenStax-CNX module: m47993 1 Skeletal System Module 13: The Pelvic Girdle and Pelvis Donna Browne Based on The Pelvic Girdle and Pelvis by OpenStax College This work is produced by OpenStax-CNX and licensed
OpenStax-CNX module: m47993 1 Skeletal System Module 13: The Pelvic Girdle and Pelvis Donna Browne Based on The Pelvic Girdle and Pelvis by OpenStax College This work is produced by OpenStax-CNX and licensed
Copyright 2003 Pearson Education, Inc. publishing as Benjamin Cummings. Dr. Nabil Khouri MD, MSc, Ph.D
 Dr. Nabil Khouri MD, MSc, Ph.D Pelvic Girdle (Hip) Organization of the Lower Limb It is divided into: The Gluteal region The thigh The knee The leg The ankle The foot The thigh and the leg have compartments
Dr. Nabil Khouri MD, MSc, Ph.D Pelvic Girdle (Hip) Organization of the Lower Limb It is divided into: The Gluteal region The thigh The knee The leg The ankle The foot The thigh and the leg have compartments
Access Pelvic Fixator
 Access Pelvic Fixator Attila Poka, MD Director, Orthopedic Trauma Service Grant Medical Center Columbus, OH Patents Pending CONTENTS 1 Introduction...Page 2 Equipment Required...Page 3 Design Rationale...Page
Access Pelvic Fixator Attila Poka, MD Director, Orthopedic Trauma Service Grant Medical Center Columbus, OH Patents Pending CONTENTS 1 Introduction...Page 2 Equipment Required...Page 3 Design Rationale...Page
PELVIC RING FRACTURES: SHOULD THEY BE FIXED?
 REVIEW ARTICLE PELVIC RING FRACTURES: SHOULD THEY BE FIXED? MARVIN TILE From the Sunnybrook Medical Centre, Toronto The management of traumatic disruption of the pelvic ring has become a focus of interest,
REVIEW ARTICLE PELVIC RING FRACTURES: SHOULD THEY BE FIXED? MARVIN TILE From the Sunnybrook Medical Centre, Toronto The management of traumatic disruption of the pelvic ring has become a focus of interest,
Anatomy & Physiology Pelvic Girdles 10.1 General Information
 Anatomy & Physiology Pelvic Girdles 10.1 General Information ICan2Ed, Inc. In human anatomy, the pelvis (plural pelves or pelvises) is the lower part of. The area of the body that is between the abdomen
Anatomy & Physiology Pelvic Girdles 10.1 General Information ICan2Ed, Inc. In human anatomy, the pelvis (plural pelves or pelvises) is the lower part of. The area of the body that is between the abdomen
EVOS MINI with IM Nailing
 Case Series Dr. John A. Scolaro EVOS MINI with IM Nailing A series of studies Introduction Intramedullary nailing has become the standard for many long bone fractures. Fracture reduction prior to nail
Case Series Dr. John A. Scolaro EVOS MINI with IM Nailing A series of studies Introduction Intramedullary nailing has become the standard for many long bone fractures. Fracture reduction prior to nail
5/31/2018. Ipsilateral Femoral Neck And Shaft Fractures. Ipsilateral Neck-Shaft Fractures Introduction. Ipsilateral Neck-Shaft Fractures Introduction
 Ipsilateral Femoral Neck And Shaft Fractures Exchange Nailing For Non- Union Donald Wiss MD Cedars-Sinai Medical Center Los Angeles, California Introduction Uncommon Injury Invariably High Energy Trauma
Ipsilateral Femoral Neck And Shaft Fractures Exchange Nailing For Non- Union Donald Wiss MD Cedars-Sinai Medical Center Los Angeles, California Introduction Uncommon Injury Invariably High Energy Trauma
- Acute Management of Pelvic Fractures - Damage Control Orthopaedics. High- energy Fractures
 Controversies in Orthopaedic Trauma Surgery Eric G. Meinberg, MD Assistant Clinical Professor UCSF/SFGH Orthopaedic Trauma InsKtute - Acute Management of Pelvic Fractures - Damage Control Orthopaedics
Controversies in Orthopaedic Trauma Surgery Eric G. Meinberg, MD Assistant Clinical Professor UCSF/SFGH Orthopaedic Trauma InsKtute - Acute Management of Pelvic Fractures - Damage Control Orthopaedics
Emergent Management of Pelvic Ring Fractures with Use of Circumferential Compression
 This is an enhanced PDF from The Journal of Bone and Joint Surgery The PDF of the article you requested follows this cover page. Emergent Management of Pelvic Ring Fractures with Use of Circumferential
This is an enhanced PDF from The Journal of Bone and Joint Surgery The PDF of the article you requested follows this cover page. Emergent Management of Pelvic Ring Fractures with Use of Circumferential
First practical session. Bones of the gluteal region
 First practical session 2017 Bones of the gluteal region The Hip bone The hip bone is made of: 1 The ilium: superior in position 2 The ischium:postero-inferior in position 3 The pubis: antero-inferior
First practical session 2017 Bones of the gluteal region The Hip bone The hip bone is made of: 1 The ilium: superior in position 2 The ischium:postero-inferior in position 3 The pubis: antero-inferior
Stoppa Approach for Anterior Plate Fixation in Unstable Pelvic Ring Injury
 Original rticle Clinics in Orthopedic Surgery 2016;8:243-248 http://dx.doi.org/10.4055/cios.2016.8.3.243 Stoppa pproach for nterior Plate Fixation in Unstable Pelvic Ring Injury Hyoung-Keun Oh, MD, Suk
Original rticle Clinics in Orthopedic Surgery 2016;8:243-248 http://dx.doi.org/10.4055/cios.2016.8.3.243 Stoppa pproach for nterior Plate Fixation in Unstable Pelvic Ring Injury Hyoung-Keun Oh, MD, Suk
Triple Pelvic Osteotomy
 Triple Pelvic Osteotomy Peter Templeton and Peter V. Giannoudis 2 Indications Acetabular dysplasia with point loading, lateral migration, and painful limp. Hip joint should be reasonably congruent in abduction
Triple Pelvic Osteotomy Peter Templeton and Peter V. Giannoudis 2 Indications Acetabular dysplasia with point loading, lateral migration, and painful limp. Hip joint should be reasonably congruent in abduction
FUNCTIONAL ANATOMY AND EXAM OF THE HIP, GROIN AND THIGH
 FUNCTIONAL ANATOMY AND EXAM OF THE HIP, GROIN AND THIGH Peter G Gerbino, MD, FACSM Orthopedic Surgeon Monterey Joint Replacement and Sports Medicine Monterey, CA TPC, San Diego, 2017 The lecturer has no
FUNCTIONAL ANATOMY AND EXAM OF THE HIP, GROIN AND THIGH Peter G Gerbino, MD, FACSM Orthopedic Surgeon Monterey Joint Replacement and Sports Medicine Monterey, CA TPC, San Diego, 2017 The lecturer has no
7/23/2018 DESCRIBING THE FRACTURE. Pattern Open vs closed Location BASIC PRINCIPLES OF FRACTURE MANAGEMENT. Anjan R. Shah MD July 21, 2018.
 BASIC PRINCIPLES OF FRACTURE MANAGEMENT Anjan R. Shah MD July 21, 2018 DESCRIBING THE FRACTURE Pattern Open vs closed Location POLL OPEN HOW WOULD YOU DESCRIBE THIS FRACTURE PATTERN? 1 Spiral 2 Transverse
BASIC PRINCIPLES OF FRACTURE MANAGEMENT Anjan R. Shah MD July 21, 2018 DESCRIBING THE FRACTURE Pattern Open vs closed Location POLL OPEN HOW WOULD YOU DESCRIBE THIS FRACTURE PATTERN? 1 Spiral 2 Transverse
Surgical Care at the District Hospital. EMERGENCY & ESSENTIAL SURGICAL CARE
 Surgical Care at the District Hospital 1 18 Orthopedic Trauma Key Points 2 18.1 Upper Extremity Injuries Clavicle Fractures Diagnose fractures from the history and by physical examination Treat with a
Surgical Care at the District Hospital 1 18 Orthopedic Trauma Key Points 2 18.1 Upper Extremity Injuries Clavicle Fractures Diagnose fractures from the history and by physical examination Treat with a
ATLS: Initial Assessment and Management. SAUSHEC Medical Student Lecture Series
 ATLS: Initial Assessment and Management SAUSHEC Medical Student Lecture Series Objectives Identify sequence of priorities in assessing the multiply injured patient Apply principles outlined in primary
ATLS: Initial Assessment and Management SAUSHEC Medical Student Lecture Series Objectives Identify sequence of priorities in assessing the multiply injured patient Apply principles outlined in primary
No disclosures relevant to this topic Acknowledgement: some clinical pictures were obtained from the OTA fracture lecture series and AO fracture
 CALCANEUS FRACTURES No disclosures relevant to this topic Acknowledgement: some clinical pictures were obtained from the OTA fracture lecture series and AO fracture lecture series INCIDENCE 2% of all fractures
CALCANEUS FRACTURES No disclosures relevant to this topic Acknowledgement: some clinical pictures were obtained from the OTA fracture lecture series and AO fracture lecture series INCIDENCE 2% of all fractures
Guidelines and Protocols
 TITLE: PELVIC TRAUMA PURPOSE: Develop a protocol of care that will insure rapid identification and treatment of these patients PROCESS: I. CARE OF PATIENTS WITH PELVIC TRAUMA A. Patients in hemorrhagic
TITLE: PELVIC TRAUMA PURPOSE: Develop a protocol of care that will insure rapid identification and treatment of these patients PROCESS: I. CARE OF PATIENTS WITH PELVIC TRAUMA A. Patients in hemorrhagic
Anterior Stabilisation of Sacroilliac Joint for Complex Pelvic Injuries
 CSE REPORT - Sacroilliac Joint Pelvic Injuries Malaysian Journal of Medical Sciences, Vol. 16, No. 3, July - September 2009 CSE REPORT nterior Stabilisation of Sacroilliac Joint for Complex Pelvic Injuries
CSE REPORT - Sacroilliac Joint Pelvic Injuries Malaysian Journal of Medical Sciences, Vol. 16, No. 3, July - September 2009 CSE REPORT nterior Stabilisation of Sacroilliac Joint for Complex Pelvic Injuries
Management of Bleeding Pelvic Fractures
 Management of Bleeding Pelvic Fractures Clay Cothren Burlew, MD FACS Professor of Surgery Program Director, SCC and TACS Fellowships Director, Surgical Intensive Care Unit Denver Health Medical Center/University
Management of Bleeding Pelvic Fractures Clay Cothren Burlew, MD FACS Professor of Surgery Program Director, SCC and TACS Fellowships Director, Surgical Intensive Care Unit Denver Health Medical Center/University
Ali Bakir Al-Hilli. Senior Lecturer Orthopedics and Trauma/ College of Medicine / Baghdad University. THE IRAQI POSTGRADUATE MEDICAL JOURNAL 525
 CLOSED THE IRAQI REDUCTION POSTGRADUATE FOR MEDICAL SACROILIAC JOURNAL DISRUPTION Evaluation of Closed Reduction and Percutaneous Iliosacral Cannulated Screw Fixation for Sacroiliac Disruption or Sacral
CLOSED THE IRAQI REDUCTION POSTGRADUATE FOR MEDICAL SACROILIAC JOURNAL DISRUPTION Evaluation of Closed Reduction and Percutaneous Iliosacral Cannulated Screw Fixation for Sacroiliac Disruption or Sacral
Pelvic Implants and Instruments. A dedicated system for reconstructive pelvic and acetabular surgery.
 Pelvic Implants and Instruments. A dedicated system for reconstructive pelvic and acetabular surgery. Surgical Technique This publication is not intended for distribution in the USA. Instruments and implants
Pelvic Implants and Instruments. A dedicated system for reconstructive pelvic and acetabular surgery. Surgical Technique This publication is not intended for distribution in the USA. Instruments and implants
C. Bones of the Pelvic Girdle
 C. Bones of the Pelvic Girdle 1. 2 coxal bones (a.k.a hip bones): -bony pelvis is made up of hip bones, sacrum, & coccyx -pelvic bones are large & heavy & attach to the axial skeleton via sacrum/coccyx
C. Bones of the Pelvic Girdle 1. 2 coxal bones (a.k.a hip bones): -bony pelvis is made up of hip bones, sacrum, & coccyx -pelvic bones are large & heavy & attach to the axial skeleton via sacrum/coccyx
The functional outcome of surgically treated unstable pelvic ring fractures by open reduction, internal fixation
 Original Research Medical Journal of Islamic Republic of Iran, Vol. 25, No. 2, Aug 2011, pp. 87-93 The functional outcome of surgically treated unstable pelvic ring fractures by open reduction, internal
Original Research Medical Journal of Islamic Republic of Iran, Vol. 25, No. 2, Aug 2011, pp. 87-93 The functional outcome of surgically treated unstable pelvic ring fractures by open reduction, internal
NOTES FROM GUTMAN LECTURE 10/26 Use this outline to study from. As you go through Gutman s lecture, fill in the topics.
 NOTES FROM GUTMAN LECTURE 10/26 Use this outline to study from. As you go through Gutman s lecture, fill in the topics. Anatomy above the arcuate line Skin Camper s fascia Scarpa s fascia External oblique
NOTES FROM GUTMAN LECTURE 10/26 Use this outline to study from. As you go through Gutman s lecture, fill in the topics. Anatomy above the arcuate line Skin Camper s fascia Scarpa s fascia External oblique
Percutaneous Ilio-Sacral Screw Fixation in Supine Position under Fluoroscopy Guidance.
 Percutaneous Ilio-Sacral Screw Fixation in Supine Position under Fluoroscopy Guidance. Shrestha D, Dhoju D, Shrestha R, Sharma V ABSTRACT Background Department of Orthopaedic and Truamtology Dhulikhel
Percutaneous Ilio-Sacral Screw Fixation in Supine Position under Fluoroscopy Guidance. Shrestha D, Dhoju D, Shrestha R, Sharma V ABSTRACT Background Department of Orthopaedic and Truamtology Dhulikhel
UBC Department of Urologic Sciences Lecture Series. Urological Trauma
 UBC Department of Urologic Sciences Lecture Series Urological Trauma Disclaimer: This is a lot of information to cover and we are unlikely to cover it all today These slides are to be utilized for your
UBC Department of Urologic Sciences Lecture Series Urological Trauma Disclaimer: This is a lot of information to cover and we are unlikely to cover it all today These slides are to be utilized for your
Classification of Pelvis and Aetabulum Injuries
 Introduction The earliest attempt at classifying pelvic ring injuries was made by Bucholz where he described three groups essentially defining anteroposterior injuries of later classification systems.[1]
Introduction The earliest attempt at classifying pelvic ring injuries was made by Bucholz where he described three groups essentially defining anteroposterior injuries of later classification systems.[1]
Crescent Fracture-Dislocation of the Sacroiliac Joint: Use of Iliosacral Screws
 Med. J. Cairo Univ., Vol. 85, No. 5, September: 1815-1819, 2017 www.medicaljournalofcairouniversity.net Crescent Fracture-Dislocation of the Sacroiliac Joint: Use of Iliosacral Screws SHERIF A. KHALED,
Med. J. Cairo Univ., Vol. 85, No. 5, September: 1815-1819, 2017 www.medicaljournalofcairouniversity.net Crescent Fracture-Dislocation of the Sacroiliac Joint: Use of Iliosacral Screws SHERIF A. KHALED,
Magnetic Resonance Imaging for the Evaluation of Ligamentous Injury in the Pelvis: A Prospective Case-Controlled Study
 ORIGINAL ARTICLE Magnetic Resonance Imaging for the Evaluation of ous Injury in the Pelvis: A Prospective Case-Controlled Study Joshua L. Gary, MD,* Michael Mulligan, MD, Kelley Banagan, MD,* Marcus F.
ORIGINAL ARTICLE Magnetic Resonance Imaging for the Evaluation of ous Injury in the Pelvis: A Prospective Case-Controlled Study Joshua L. Gary, MD,* Michael Mulligan, MD, Kelley Banagan, MD,* Marcus F.
Kyle F. Dickson, M.D. M.B.A. I Need a Special Table to Treat Some Acetabular Fractures. I Prefer a Special Table to Treat Most Acetabular Fractures
 Kyle F. Dickson, M.D. M.B.A. Professor Baylor College of Medicine Southwest Orthopaedic Group, Houston, Texas kyledickson99@gmail.com cell 713-208-4168 I Need a Special Table to Treat Some Acetabular Fractures
Kyle F. Dickson, M.D. M.B.A. Professor Baylor College of Medicine Southwest Orthopaedic Group, Houston, Texas kyledickson99@gmail.com cell 713-208-4168 I Need a Special Table to Treat Some Acetabular Fractures
Disclosures. Sacroiliac Joint (SIJ) Pain. Modified Triplanar Fluoroscopic Approach in Percutaneous Fixation of Sacroiliac Joint 5/12/2017
 Pain. Modified Triplanar Fluoroscopic Approach in Percutaneous Fixation of Sacroiliac Joint 5/12/2017") Modified Triplanar Fluoroscopic Approach in Percutaneous Fixation of Sacroiliac Joint J.E. Barrett, M.D. Atlanta Medical Center Atlanta Trauma Symposium 22 April 2017 Disclosures None Sacroiliac Joint
Modified Triplanar Fluoroscopic Approach in Percutaneous Fixation of Sacroiliac Joint J.E. Barrett, M.D. Atlanta Medical Center Atlanta Trauma Symposium 22 April 2017 Disclosures None Sacroiliac Joint
Management of Pelvic Fracture
 Management of Pelvis Fracture with Hemodynamic Instability James W. Davis MD Professor of Clinical Surgery, UCSF/Fresno Chief of Trauma Management of Pelvic Fracture How NOT to do it The basics Evaluation
Management of Pelvis Fracture with Hemodynamic Instability James W. Davis MD Professor of Clinical Surgery, UCSF/Fresno Chief of Trauma Management of Pelvic Fracture How NOT to do it The basics Evaluation
PELVIS & SACRUM Dr. Jamila El-Medany Dr. Essam Eldin Salama
 PELVIS & SACRUM Dr. Jamila El-Medany Dr. Essam Eldin Salama Learning Objectives At the end of the lecture, the students should be able to : Describe the bony structures of the pelvis. Describe in detail
PELVIS & SACRUM Dr. Jamila El-Medany Dr. Essam Eldin Salama Learning Objectives At the end of the lecture, the students should be able to : Describe the bony structures of the pelvis. Describe in detail
Clinical comparative analysis on unstable pelvic fractures in the treatment with percutaneous sacroiliac screws and
 European Review for Medical and Pharmacological Sciences Clinical comparative analysis on unstable pelvic fractures in the treatment with percutaneous sacroiliac screws and sacroiliac joint anterior plate
European Review for Medical and Pharmacological Sciences Clinical comparative analysis on unstable pelvic fractures in the treatment with percutaneous sacroiliac screws and sacroiliac joint anterior plate
Pelvic Fixation. Disclosures 5/19/2017. Rationale for Lumbo-pelvic Fixation
 Pelvic Fixation Joseph M Zavatsky, MD Spine & Scoliosis Specialists Tampa, FL Disclosures Consultant - DePuy Synthes Spine, Zimmer Biomet, Amendia, Stryker Stock - Innovative Surgical Solutions, Vivex
Pelvic Fixation Joseph M Zavatsky, MD Spine & Scoliosis Specialists Tampa, FL Disclosures Consultant - DePuy Synthes Spine, Zimmer Biomet, Amendia, Stryker Stock - Innovative Surgical Solutions, Vivex
2. List the 8 pelvic spaces: list one procedure or dissection which involves entering that space.
 Name: Anatomy Quiz: Pre / Post 1. In making a pfannensteil incision you would traverse through the following layers: a) Skin, Camper s fascia, Scarpa s fascia, external oblique aponeurosis, internal oblique
Name: Anatomy Quiz: Pre / Post 1. In making a pfannensteil incision you would traverse through the following layers: a) Skin, Camper s fascia, Scarpa s fascia, external oblique aponeurosis, internal oblique
Vasu Pai FRACS, MCh, MS, Nat Board Ortho Surgeon Gisborne
 Vasu Pai FRACS, MCh, MS, Nat Board Ortho Surgeon Gisborne FRACTURE MANAGEMENT I Simple closed fracture : Complete or Incomplete Stable or unstable II Open fracture III Multiple fracture IV Polytrauma Fractures
Vasu Pai FRACS, MCh, MS, Nat Board Ortho Surgeon Gisborne FRACTURE MANAGEMENT I Simple closed fracture : Complete or Incomplete Stable or unstable II Open fracture III Multiple fracture IV Polytrauma Fractures
Fractures and dislocations around elbow in adult
 Lec: 3 Fractures and dislocations around elbow in adult These include fractures of distal humerus, fracture of the capitulum, fracture of the radial head, fracture of the olecranon & dislocation of the
Lec: 3 Fractures and dislocations around elbow in adult These include fractures of distal humerus, fracture of the capitulum, fracture of the radial head, fracture of the olecranon & dislocation of the
Midfoot - Reduction & Fixation - ORIF - screw fixation - AO Surgery Reference. ORIF - screw fixation
 Midfoot - TMT (Lisfranc) injury 1. Diagnosis ORIF - screw fixation Authors Mechanism of the injury Tarso-metatarsal (Lisfranc) injuries may be caused by direct or indirect forces. Direct forces include
Midfoot - TMT (Lisfranc) injury 1. Diagnosis ORIF - screw fixation Authors Mechanism of the injury Tarso-metatarsal (Lisfranc) injuries may be caused by direct or indirect forces. Direct forces include
ROTATIONAL PILON FRACTURES
 CHAPTER 31 ROTATIONAL PILON FRACTURES George S. Gumann, DPM The opinions and commentary of the author should not be construed as refl ecting offi cial U.S. Army Medical Department policy. Pilon injuries
CHAPTER 31 ROTATIONAL PILON FRACTURES George S. Gumann, DPM The opinions and commentary of the author should not be construed as refl ecting offi cial U.S. Army Medical Department policy. Pilon injuries
OBJECTIVES: Define basic assessments skills needed to identify orthopedic injuries. Differentiate when an orthopedic injury is a medical emergency
 1 2 How to Triage Orthopaedic Care David W. Gray, M.D. OBJECTIVES: Define basic assessments skills needed to identify orthopedic injuries Differentiate when an orthopedic injury is a medical emergency
1 2 How to Triage Orthopaedic Care David W. Gray, M.D. OBJECTIVES: Define basic assessments skills needed to identify orthopedic injuries Differentiate when an orthopedic injury is a medical emergency
TREATMENT OF PUBIC DISJUNCTION IN YOUNG-BURGUESS TYPE II AND III PELVIC RING FRACTURES
 Rev. Med. Chir. Soc. Med. Nat., Iaşi 2016 vol. 120, no. 1 SURGERY ORIGINAL PAPERS TREATMENT OF PUBIC DISJUNCTION IN YOUNG-BURGUESS TYPE II AND III PELVIC RING FRACTURES R.I. Malancea 1, R. Malancea 2,
Rev. Med. Chir. Soc. Med. Nat., Iaşi 2016 vol. 120, no. 1 SURGERY ORIGINAL PAPERS TREATMENT OF PUBIC DISJUNCTION IN YOUNG-BURGUESS TYPE II AND III PELVIC RING FRACTURES R.I. Malancea 1, R. Malancea 2,
Delayed Presentation of Traumatic Bladder Injury: A case report and review of current treatment trends
 ISPUB.COM The Internet Journal of Urology Volume 5 Number 1 Delayed Presentation of Traumatic Bladder Injury: A case report and review of current treatment trends S Deem, C Lavender, S Agarwal Citation
ISPUB.COM The Internet Journal of Urology Volume 5 Number 1 Delayed Presentation of Traumatic Bladder Injury: A case report and review of current treatment trends S Deem, C Lavender, S Agarwal Citation
Information within the handout. Brief Introduction Anatomy & Biomechanics Assessment & Diagnosis Treatment through Muscle Energy
 Manual Medicine Diagnosis and Treatment for Somatic Dysfunction of the Pelvis Through Muscle Energy Greenman s Priciples of Manual Medicine (5 th Ed.)- Lisa DeStefano,DO Speaker disclosure I declare I
Manual Medicine Diagnosis and Treatment for Somatic Dysfunction of the Pelvis Through Muscle Energy Greenman s Priciples of Manual Medicine (5 th Ed.)- Lisa DeStefano,DO Speaker disclosure I declare I
Observation on closed reduction and internal fixation with external fixation in treating unstable pelvic fracture.
 Biomedical Research 2017; 28 (15): 6911-6915 ISSN 0970-938X www.biomedres.info Observation on closed reduction and internal fixation with external fixation in treating unstable pelvic fracture. Wei-Zhou
Biomedical Research 2017; 28 (15): 6911-6915 ISSN 0970-938X www.biomedres.info Observation on closed reduction and internal fixation with external fixation in treating unstable pelvic fracture. Wei-Zhou
AcUMEDr. LoCKING CLAVICLE PLATE SYSTEM
 AcUMEDr LoCKING CLAVICLE PLATE SYSTEM LoCKING CLAVICLE PLATE SYSTEM Since 1988 Acumed has been designing solutions to the demanding situations facing orthopedic surgeons, hospitals and their patients.
AcUMEDr LoCKING CLAVICLE PLATE SYSTEM LoCKING CLAVICLE PLATE SYSTEM Since 1988 Acumed has been designing solutions to the demanding situations facing orthopedic surgeons, hospitals and their patients.
Bony Anatomy. Femur. Femoral Head Femoral Neck Greater Trochanter Lesser Trochanter Intertrochanteric Crest Intertrochanteric Line Gluteal Tuberosity
 Hip Anatomy Bony Anatomy Femur Femoral Head Femoral Neck Greater Trochanter Lesser Trochanter Intertrochanteric Crest Intertrochanteric Line Gluteal Tuberosity Bony Anatomy Pelvic Girdle Acetabulum 3 bones
Hip Anatomy Bony Anatomy Femur Femoral Head Femoral Neck Greater Trochanter Lesser Trochanter Intertrochanteric Crest Intertrochanteric Line Gluteal Tuberosity Bony Anatomy Pelvic Girdle Acetabulum 3 bones
Dorsal Cervical Surgeries and Techniques
 Dorsal Cervical Approaches Dorsal Cervical Surgeries and Techniques Gregory R. Trost, MD Professor and Vice Chair of Neurological Surgery University of Wisconsin-Madison Advantages Straightforward Easily
Dorsal Cervical Approaches Dorsal Cervical Surgeries and Techniques Gregory R. Trost, MD Professor and Vice Chair of Neurological Surgery University of Wisconsin-Madison Advantages Straightforward Easily
Treatment of Unstable Pelvic Ring Injuries
 REVIEW RTICLE Hip Pelvis 26(2): 79-83, 2014 http://dx.doi.org/10.5371/hp.2014.26.2.79 Print ISSN 2287-3260 Online ISSN 2287-3279 Treatment of Unstable Pelvic Ring Injuries Weon-Yoo Kim, MD Department of
REVIEW RTICLE Hip Pelvis 26(2): 79-83, 2014 http://dx.doi.org/10.5371/hp.2014.26.2.79 Print ISSN 2287-3260 Online ISSN 2287-3279 Treatment of Unstable Pelvic Ring Injuries Weon-Yoo Kim, MD Department of
Slide Read the tables it is about the difference between male & female pelvis.
 I didn t include the slides, this is only what the doctor read or said because he skipped a lot of things because we took it previously, very important to go back to the slides (*there is an edited version)
I didn t include the slides, this is only what the doctor read or said because he skipped a lot of things because we took it previously, very important to go back to the slides (*there is an edited version)
Lesson 24. A & P Hip
 Lesson 24 A & P Hip 1 Aims of the Session This session will allow candidates to have an understanding of the bony prominences and soft tissues of the hip 2 Learning Outcomes By the end of the lesson the
Lesson 24 A & P Hip 1 Aims of the Session This session will allow candidates to have an understanding of the bony prominences and soft tissues of the hip 2 Learning Outcomes By the end of the lesson the
Advantages of MISS. Disclosures. Thoracolumbar Trauma: Minimally Invasive Techniques. Minimal Invasive Spine Surgery 11/8/2013.
 3 rd Annual UCSF Techniques in Complex Spine Surgery Program Thoracolumbar Trauma: Minimally Invasive Techniques Research Support: Stryker Disclosures Murat Pekmezci, MD Assistant Clinical Professor UCSF/SFGH
3 rd Annual UCSF Techniques in Complex Spine Surgery Program Thoracolumbar Trauma: Minimally Invasive Techniques Research Support: Stryker Disclosures Murat Pekmezci, MD Assistant Clinical Professor UCSF/SFGH
Outcome of Surgical Treatment of AO Type C Pelvic Ring Injury
 ORIGINAL ARTICLE Hip Pelvis 26(4): 269-274, 2014 http://dx.doi.org/10.5371/hp.2014.26.4.269 Print ISSN 2287-3260 Online ISSN 2287-3279 Outcome of Surgical Treatment of AO Type C Pelvic Ring Injury Do Hyeon
ORIGINAL ARTICLE Hip Pelvis 26(4): 269-274, 2014 http://dx.doi.org/10.5371/hp.2014.26.4.269 Print ISSN 2287-3260 Online ISSN 2287-3279 Outcome of Surgical Treatment of AO Type C Pelvic Ring Injury Do Hyeon
The Treatment of Pelvic Discontinuity During Acetabular Revision
 The Journal of Arthroplasty Vol. 20 No. 4 Suppl. 2 2005 The Treatment of Pelvic Discontinuity During Acetabular Revision Scott M. Sporer, MD, MS,*y Michael O Rourke, MD,z and Wayne G. Paprosky, MD, FACS*y
The Journal of Arthroplasty Vol. 20 No. 4 Suppl. 2 2005 The Treatment of Pelvic Discontinuity During Acetabular Revision Scott M. Sporer, MD, MS,*y Michael O Rourke, MD,z and Wayne G. Paprosky, MD, FACS*y
Pelvic Trauma. Ø Pelvis: The most important area of the body. Ø Pelvic injuries often represent multisystem
 Pelvic Trauma Jim Holliman, M.D. FACEP Associate Professor of Surgery / Emergency Medicine Director, Center for International Emergency Medicine M.S. Hershey Medical Center Penn State University Hershey,
Pelvic Trauma Jim Holliman, M.D. FACEP Associate Professor of Surgery / Emergency Medicine Director, Center for International Emergency Medicine M.S. Hershey Medical Center Penn State University Hershey,
The Hip Joint. Shenequia Howard David Rivera
 The Hip Joint Shenequia Howard David Rivera Topics Of Discussion Movement Bony Anatomy Ligamentous Anatomy Muscular Anatomy Origin/Insertion/Action/Innervation Common Injuries MOVEMENT Flexion Extension
The Hip Joint Shenequia Howard David Rivera Topics Of Discussion Movement Bony Anatomy Ligamentous Anatomy Muscular Anatomy Origin/Insertion/Action/Innervation Common Injuries MOVEMENT Flexion Extension
Introduction to Anatomy. Dr. Maher Hadidi. Tala Ar ar. Mar/10th/2013
 Sheet Introduction to Anatomy Dr. Maher Hadidi Tala Ar ar 15 Mar/10th/2013 Lower limb The skeleton of the lower limb is the lower appendicular skeleton which consists of 2 parts: 1- Pelvic girdle. 2- Bones
Sheet Introduction to Anatomy Dr. Maher Hadidi Tala Ar ar 15 Mar/10th/2013 Lower limb The skeleton of the lower limb is the lower appendicular skeleton which consists of 2 parts: 1- Pelvic girdle. 2- Bones
Figure 1 - Hip and Pelvis
 Hip Figure 1 - Hip and Pelvis The terms hip and pelvis are frequently used interchangeably, but strictly speaking, the pelvis is a girdle of bones and the hip is a joint. The pelvis consists of The sacrum
Hip Figure 1 - Hip and Pelvis The terms hip and pelvis are frequently used interchangeably, but strictly speaking, the pelvis is a girdle of bones and the hip is a joint. The pelvis consists of The sacrum
Index. B Backslap technique depth assessment, 82, 83 diaphysis distal trocar, 82 83
 Index A Acromial impingement, 75, 76 Aequalis intramedullary locking avascular necrosis, 95 central humeral head, 78, 80 clinical and functional outcomes, 95, 96 design, 77, 79 perioperative complications,
Index A Acromial impingement, 75, 76 Aequalis intramedullary locking avascular necrosis, 95 central humeral head, 78, 80 clinical and functional outcomes, 95, 96 design, 77, 79 perioperative complications,
Spinal Cord Injuries: The Basics. Kadre Sneddon POS Rounds October 1, 2003
 Spinal Cord Injuries: The Basics Kadre Sneddon POS Rounds October 1, 2003 Anatomy Dorsal columntouch, vibration Corticospinal tract- UMN Anterior horn-lmn Spinothalamic tractpain, temperature (contralateral)
Spinal Cord Injuries: The Basics Kadre Sneddon POS Rounds October 1, 2003 Anatomy Dorsal columntouch, vibration Corticospinal tract- UMN Anterior horn-lmn Spinothalamic tractpain, temperature (contralateral)
Percutaneous screw fixation for sacral & sacro iliac joint injuries: Case series
 2017; 3(4): 669-674 ISSN: 2395-1958 IJOS 2017; 3(4): 669-674 2017 IJOS www.orthopaper.com Received: 04-08-2017 Accepted: 05-09-2017 Dr. Ramprasath DR Associate Professor, Department of Orthopaedic Surgery,
2017; 3(4): 669-674 ISSN: 2395-1958 IJOS 2017; 3(4): 669-674 2017 IJOS www.orthopaper.com Received: 04-08-2017 Accepted: 05-09-2017 Dr. Ramprasath DR Associate Professor, Department of Orthopaedic Surgery,
Evaluation Tools and Outcomes after Osteosynthesis of Unstable Type B and C Pelvic Ring Injuries
 305/, p. 305 320 Evaluation Tools and Outcomes after Osteosynthesis of Unstable Type B and C Pelvic Ring Injuries Nástroje pro zhodnocení a výsledky po osteosyntéze nestabilního poranění pánevního kruhu
305/, p. 305 320 Evaluation Tools and Outcomes after Osteosynthesis of Unstable Type B and C Pelvic Ring Injuries Nástroje pro zhodnocení a výsledky po osteosyntéze nestabilního poranění pánevního kruhu
CURRENT TREATMENT OPTIONS
 CURRENT TREATMENT OPTIONS Fix single column or both: Always fix both. A study by Svend-Hansen corroborated the poor results associated with isolated medial malleolar fixation in bimalleolar ankle fractures.
CURRENT TREATMENT OPTIONS Fix single column or both: Always fix both. A study by Svend-Hansen corroborated the poor results associated with isolated medial malleolar fixation in bimalleolar ankle fractures.
THE HIP. Cooler than cool, the pinnacle of what is "it". Beyond all trends and conventional coolness.
 THE HIP Cooler than cool, the pinnacle of what is "it". Beyond all trends and conventional coolness. Objectives Hip anatomy Causes of hip pain Hip exam Anatomy Bones Ilium Anterior Superior Iliac Spine
THE HIP Cooler than cool, the pinnacle of what is "it". Beyond all trends and conventional coolness. Objectives Hip anatomy Causes of hip pain Hip exam Anatomy Bones Ilium Anterior Superior Iliac Spine
Minimally invasive treatment for anterior pelvic ring injuries with modified pedicle screw-rod fixation: a retrospective study
 Hung et al. Journal of Orthopaedic Surgery and Research (2018) 13:238 https://doi.org/10.1186/s13018-018-0945-4 RESEARCH ARTICLE Open Access Minimally invasive treatment for anterior pelvic ring injuries
Hung et al. Journal of Orthopaedic Surgery and Research (2018) 13:238 https://doi.org/10.1186/s13018-018-0945-4 RESEARCH ARTICLE Open Access Minimally invasive treatment for anterior pelvic ring injuries
Using the Starr Frame and Da Vinci surgery system for pelvic fracture and sacral nerve injury
 https://doi.org/10.1186/s13018-018-1040-6 TECHNICAL NOTE Open Access Using the Starr Frame and Da Vinci surgery system for pelvic fracture and sacral nerve injury Ye Peng 1, Wei Zhang 1, Gongzi Zhang 1,
https://doi.org/10.1186/s13018-018-1040-6 TECHNICAL NOTE Open Access Using the Starr Frame and Da Vinci surgery system for pelvic fracture and sacral nerve injury Ye Peng 1, Wei Zhang 1, Gongzi Zhang 1,
Pelvic Implants and Instruments. A dedicated system for reconstructive pelvic and acetabular surgery.
 Pelvic Implants and Instruments. A dedicated system for reconstructive pelvic and acetabular surgery. Surgical Technique This publication is not intended for distribution in the USA. Instruments and implants
Pelvic Implants and Instruments. A dedicated system for reconstructive pelvic and acetabular surgery. Surgical Technique This publication is not intended for distribution in the USA. Instruments and implants
IMAGING OF PELVIC FRACTURES AND ASSOCIATED INJURIES C. Craig Blackmore, MD, MPH
 IMAGING OF PELVIC FRACTURES AND ASSOCIATED INJURIES C. Craig Blackmore, MD, MPH Introduction Pelvic fractures occur in approximately 113,000 persons in the United States each year [1], and have a major
IMAGING OF PELVIC FRACTURES AND ASSOCIATED INJURIES C. Craig Blackmore, MD, MPH Introduction Pelvic fractures occur in approximately 113,000 persons in the United States each year [1], and have a major
Functional outcome of acetabular fracture fixation by modified Stoppa s approach
 International Journal of Research in Orthopaedics http://www.ijoro.org Original Research Article DOI: http://dx.doi.org/10.18203/issn.2455-4510.intjresorthop20185343 Functional outcome of acetabular fracture
International Journal of Research in Orthopaedics http://www.ijoro.org Original Research Article DOI: http://dx.doi.org/10.18203/issn.2455-4510.intjresorthop20185343 Functional outcome of acetabular fracture
Kaan Yücel M.D., Ph.D. 14.January.2014 Tuesday
 Kaan Yücel M.D., Ph.D. 14.January.2014 Tuesday Sexual differences are related mainly 1. Heavier build and larger muscles of most men 2. Adaptation of the pelvis (particularly the lesser pelvis) in women
Kaan Yücel M.D., Ph.D. 14.January.2014 Tuesday Sexual differences are related mainly 1. Heavier build and larger muscles of most men 2. Adaptation of the pelvis (particularly the lesser pelvis) in women
Subaxial Cervical Spine Trauma
 Subaxial Cervical Spine Trauma Pooria Salari, MD Assistant Professor Of Orthopaedics Department of Orthopaedic Surgery St. Louis University School of Medicine St. Louis, Missouri, USA Initial Evaluation
Subaxial Cervical Spine Trauma Pooria Salari, MD Assistant Professor Of Orthopaedics Department of Orthopaedic Surgery St. Louis University School of Medicine St. Louis, Missouri, USA Initial Evaluation
Clinical aspects in urogenital injuries
 Clinical aspects in urogenital injuries Rolf Wahlqvist Oslo Urological University Clinic Aker University Hospital Nordic Rad.2008 1 Urogenital injuries in trauma patients Renal injury Ureteral injury (infrequent/iatrogenic)
Clinical aspects in urogenital injuries Rolf Wahlqvist Oslo Urological University Clinic Aker University Hospital Nordic Rad.2008 1 Urogenital injuries in trauma patients Renal injury Ureteral injury (infrequent/iatrogenic)
Guido Barbagli. Center for Reconstructive ti Urethral lsurgery
 Guido Barbagli Center for Reconstructive ti Urethral lsurgery Arezzo - Italy E-mail: guido@rdn.it Website: www.urethralcenter.it Dedicated to Ruggero Lenzi, teacher and friend. His passing was a great
Guido Barbagli Center for Reconstructive ti Urethral lsurgery Arezzo - Italy E-mail: guido@rdn.it Website: www.urethralcenter.it Dedicated to Ruggero Lenzi, teacher and friend. His passing was a great
PREVIEW ONLY. What is the pelvis? The Pelvis. The Pelvis. The fundamentals: ANATOMY of the SIJ and PELVIS. The basic structure of the pelvis
 The fundamentals: ANATOMY of the SIJ and PELVIS Presented by: Taso Lambridis BSc (Physiotherapy) MSc (Sports Medicine) Suite 3, 104 Spofforth Street Tel: (02) 8969 6300 info@spinalsynergy.com.au Cremorne,
The fundamentals: ANATOMY of the SIJ and PELVIS Presented by: Taso Lambridis BSc (Physiotherapy) MSc (Sports Medicine) Suite 3, 104 Spofforth Street Tel: (02) 8969 6300 info@spinalsynergy.com.au Cremorne,
PediLoc 3.5mm and 4.5mm Bowed Femur Plate Surgical Technique
 PediLoc 3.5mm and 4.5mm Bowed Femur Plate Surgical Technique 2957 Bow Broch_REV_B.indd 1 2/10/11 12:47 PM Surgical Technique Bowed Femur Plate The technique description herein is made available to the
PediLoc 3.5mm and 4.5mm Bowed Femur Plate Surgical Technique 2957 Bow Broch_REV_B.indd 1 2/10/11 12:47 PM Surgical Technique Bowed Femur Plate The technique description herein is made available to the
How to Triage Orthopaedic Care. David W. Gray, M.D.
 How to Triage Orthopaedic Care David W. Gray, M.D. OBJECTIVES: Define basic assessments skills needed to identify orthopedic injuries Differentiate when an orthopedic injury is a medical emergency Determine
How to Triage Orthopaedic Care David W. Gray, M.D. OBJECTIVES: Define basic assessments skills needed to identify orthopedic injuries Differentiate when an orthopedic injury is a medical emergency Determine