The Acute Management of Pelvic Ring Injuries
|
|
|
- Tyler Brooks
- 5 years ago
- Views:
Transcription

1 The Acute Management of Pelvic Ring Injuries Brian J Ladner, MD North Oaks Medical Center Original Author: Kyle F. Dickson, MD; Created March 2004 Sean E. Nork, MD; Revised December 2010 New Author: October 2017
2 Conflicts of Interest I have no conflicts of interest to report.

3 High energy Morbidity/Mortality Hemorrhage Pelvic Ring Injuries
4 An unstable pelvic injury may allow hemorrhage to collect in the true pelvis as there is no longer a constraint which allows tamponade. The volume was traditionally assumed to be a cylinder with a volume of 4/3π r 3, However Pelvic Ring Injuries Best estimated by a hemi-elliptical sphere (Stover et al, J Trauma, 2006)
5 Primary survey: ABC s Airway maintenance with cervical spine protection Breathing and ventilation Circulation with hemorrhage control Disability: Neurologic status Exposure/environment control: undress patient but prevent hypothemia
6 Considerations for Transfer or Care at a Specialized Center: Pelvic Fractures Significant posterior pelvis instability/displacement on the initial AP X- ray (indicates potential need for ORIF) Bladder/urethra injury Open pelvic fractures Lateral directed force with fractures through iliac wing, sacral ala or foramina Open book with anterior displacement > 2.5 cm (value of 2.5 centimeters somewhat arbitrary and controversial with regards to reliability)

7 Physical Exam Degloving injuries Limb shortening Limb rotation Open wounds Swelling & hematoma


8 Radiographic Hemodynamic Defining Pelvic Stability??? Biomechanical (Tile & Hearn) Mechanical Able to withstand normal physiological forces without abnormal deformation

9 Single examiner Use fluoro if available Best in experienced hands Stable or Unstable?
10 Radiographic Signs of Instability Sacroiliac displacement of 5 mm in any plane Posterior fracture gap (rather than impaction) Avulsion of fifth lumbar transverse process, lateral border of sacrum (sacrotuberous ligament), or ischial spine (sacrospinous ligament)
11 Open Pelvic Injuries Open wounds extending to the colon, rectum, or perineum: strongly consider early diverting colostomy Soft-tissue wounds should be aggressively debrided Early repair of vaginal lacerations to minimize subsequent pelvic abscess
12 15% incidence Urologic Injuries Blood at meatus or high riding prostate Eventual swelling of scrotum and labia (occasional arterial bleeder requiring surgery) Retrograde urethrogram indicated in pelvic injured patients
13 Urologic Injuries Intraperitoneal & extraperitoneal bladder ruptures are usually repaired A foley catheter is preferred If a supra-pubic catheter it used, it should be tunneled to prevent anterior wound contamination Urethral injuries are usually repaired on a delayed basis
")

14 Sources of Hemorrhage External (open wounds) Internal: Chest Long bones Abdominal Retroperitoneal
15 Sources of Hemorrhage External (open wounds) Internal: Chest Long bones Abdominal Retroperitoneal Chest x-ray Physical exam, swelling DPL, ultrasound, FAST CT scan, direct look
16 Shock vs Hemodynamic Instability Definitions Confusing Potentially based on multiple factors & measures Lactate Base Deficit SBP < 90 mmhg Ongoing drop in Hematrocrit Response to fluid challenge
17 Pelvic Fractures & Hemorrhage Fracture pattern associated with risk of vascular injury (Young & Burgess) External rotation and vertical shear injury patterns at higher risk for a vascular injury that internal rotation patterns APC & VS (antero-posterior compression and vertical shear) at increased risk of hemorrhage Injury patterns that are tensile to N-V structures at increased risk (eg iliac wing fractures with GSN extension) Dalal et al, JT, 1989 Burgess et al, JT, 1990 Whitbeck et al, JOT, 1997 Switzer et al, JOT, 2000 Eastridge et al, JT, 2002

18 Lateral Compression (LC) Anteroposterior Compression (APC) Vertical Shear (VS) Pelvic Fractures & Hemorrhage: Young and Burgess Classification ER & VS > IR APC & VS at increased risk
19 Hemorrhage Control: Methods Pelvic Containment Sheet Pelvic Binder External Fixation Angiography Laparotomy Pelvic Packing




20 Supine 2 Wrappers Placement Apply Clamper 30 Seconds Circumferential Sheeting 4 1 Routt et al, JOT,


21 Sheet Application
22 Sheet Application Before
23 After
24


25 Pelvic Binders Commercially available. Placed over the TROCHANTERS and not over the abdomen.
26 Location External Fixation Clinical Application AIIS Resuscitative ASIS Augmentative C-clamp Definitive
27 Biomechanics of External Fixation: Anterior External Fixation Open book injuries with posterior ligaments (hinge) intact: All designs work C-type injury patterns No designs work well (but AIIS frames help more than ASIS frames)
28 Biomechanics of External Fixation: Considerations Pin size Number of pins Frame design Frame location

29 Placed at the iliac crests bilaterally Not a good vector for controlling the pelvis ASIS Frames

30 Placed at the AIIS bilaterally At least biomechanically equivalent, thought to be superior to ASIS frames Patients can sit Kim et al, CORR, 1999 AIIS Frames

31 Placed at the AIIS bilaterally At least biomechanically equivalent, thought to be superior to ASIS frames Patients can sit Kim et al, CORR, 1999 AIIS Frames
32 Indications for External Fixation Resuscitative (hemorrhage control, stability) To decrease pain in polytraumatized patients? As an adjunct to ORIF Definitive treatment (Rare!) Distraction frame Can t ORIF the pelvis
33 Indications for External Fixation Resuscitative (hemorrhage control, stability) To decrease pain in polytraumatized patients? As an adjunct to ORIF Definitive treatment (Rare!) Distraction frame Can t ORIF the pelvis

34
35


36

37
38 Indications for External Fixation Resuscitative (hemorrhage control, stability) To decrease pain in polytraumatized patients? As an adjunct to ORIF Definitive treatment (Rare!) Distraction frame Can t ORIF the pelvis Theoretical and a marginal indication, but there is literature support Barei, D. P.; Shafer, B. L.; Beingessner, D. M.; Gardner, M. J.; Nork, S. E.; and Routt, M. L.: The impact of open reduction internal fixation on acute pain management in unstable pelvic ring injuries. J Trauma, 68(4): , 2010.
39 Indications for External Fixation Resuscitative (hemorrhage control, stability) To decrease pain in polytraumatized patients? As an adjunct to ORIF Definitive treatment (Rare!) Distraction frame Can t ORIF the pelvis

40

41

42

43 Indications for External Fixation Resuscitative (hemorrhage control, stability) To decrease pain in polytraumatized patients? As an adjunct to ORIF Definitive treatment (Rare!) Distraction frame If can t ORIF the pelvis



44

45


46



47

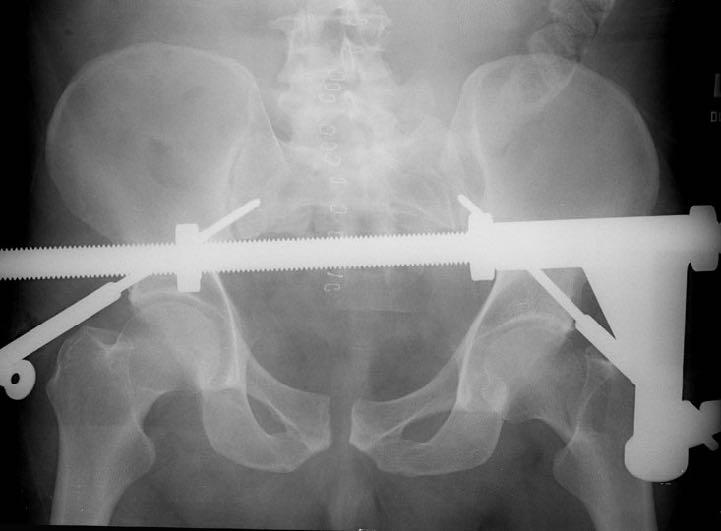
48 Anti-shock Clamp (C-clamp) Better posterior pelvis stabilization Allows abdominal access Consider application with fluoro or in the OR to prevent poor pin placement Can be combined with pelvic packing Ertel, W et al, JOT, 2001

49 Anti-shock Clamp (C-clamp) Better posterior pelvis stabilization Allows abdominal access Consider application with fluoro or in the OR to prevent poor pin placement Can be combined with pelvic packing

50 Anti-shock Clamp (C-clamp) Better posterior pelvis stabilization Allows abdominal access Consider application with fluoro or in the OR to prevent poor pin placement Can be combined with pelvic packing

51 Anti-shock Clamp (C-clamp) Better posterior pelvis stabilization Allows abdominal access Consider application with fluoro or in the OR to prevent poor pin placement Can be combined with pelvic packing


52 Emergent Application



53 Pelvic Packing Ertel, W et al, JOT, 2001 Pohlemann et al, Giannoudis et al,
54 Role of Angiography??? Valuable for arterial only Estimated at 5-15% Timing (early vs late?) Institution dependent
55 Role of Angiography??? Fracture pattern may predict effectiveness Contrast CT suggests Effective in retrospective studies!!!
56 Arterial vs Venous vs Cancellous Unstable posterior ring association Associated fracture extension into notch Role of angiography Vascular Injuries Cryer et al, JT, 1988 O Neill et al, CORR, 1996 Goldstein et al, JT, 1994


57

58 Acute Hemipelvectomy.
 Life")
59 Acute Hemipelvectomy. Rarely required (thankfully) Life saving indications only

60 si um N o Fr rt id h ay Oa, N ks ov T em rau be ma r3 S, 2 ym 01 po 7 Acute Hemipelvectomy.
61 Retrospective evidence suggests Hypotensive with stable pelvic pattern Proceed to Laparotomy (85% with abdominal hemorrhage) Hypotensive with unstable pelvic pattern Proceed to Angio (59% with positive angio) Eastridge et al, JT, 2002 Contrast enhanced CT very suggestive of arterial source (40 fold likelihood ratio) (PPV and NPV of 80%, 98%) Stephen et al, JT, 1999

62 Example of a protocol for management
63 Example of a protocol for management Hypovolemic shock and no response to fluids (+) DPL: 1. Laparotomy (+/- packing with ex fix) 2. Angio (-) DPL: 1. Sheet/binder/ex-fix (some still crash lap) 2. Angio Hypovolemic shock with response to fluids (++) DPL: 1. Laparotomy (+/- packing with ex fix) 2. Ex Fix 3. Angio (+) DPL: 1. Ex Fix 2. Laparotomy 3. Angio (-) DPL: 1. Sheet/binder 2. Angio 3. Ex Fix
64 Example of a protocol for management
65 Protocol for Management Biffl et al, Evolution of a mutlidisciplinary clinical pathway for the management of unstable patients with pelvic fractures. JOT, elements: Immediate trauma surgeon availability (+ Ortho!) Early simultaneous blood and coagulation products Prompt diagnosis & treatment of life threatening injuries Stabilization of the pelvic girdle Timely pelvic angiography and embolization Changes: Patients more severely injured (52% vs 35% SBP < 90) DPL phased out for U/S Pelvic binders and C-clamps replaced traditional ex fix
66 Protocol for Management Biffl et al, Evolution of a mutlidisciplinary clinical pathway for the management of unstable patients with pelvic fractures. JOT, 2001 Mortality decreased from 31% to 15% Exsanguination death from 9% to 1% MOF from 12% to 1% Death (<24 hours) from 16% to 5% The evolution of a multidisciplinary clinical pathway, coordinating the resources of a level 1 trauma center and directed by joint decision making between trauma surgeons and orthopedic traumatologists, has resulted in improved patient survival. The primary benefits appear to be in reducing early deaths from exsanguination and late deaths from multiple organ failure.




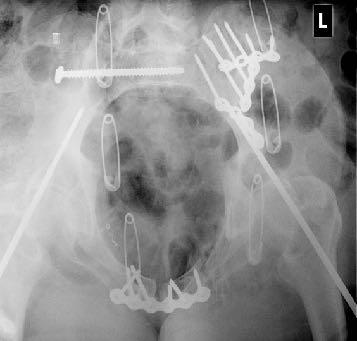
67 Immediate Percutaneous Fixation From Chip Routt, MD
68 Summary: Acute Management Play well with others (general surgery, urology, interventional radiology, neurosurgery) Understand the fracture pattern Do something (sheet, binder, ex fix, c-clamp) Combine knowledge of the fracture, the patients condition, and the physical exam to decide on the next step

69 Thank You!
Surgical Approaches for Fractures and Injuries of the Pelvic Ring
 Surgical Approaches for Fractures and Injuries of the Pelvic Ring Mara L. Schenker, MD Emory University / Grady Hospital Created by Steven A. Olson, MD in 2004 and Kyle Dickson, MD in 2004 First revised
Surgical Approaches for Fractures and Injuries of the Pelvic Ring Mara L. Schenker, MD Emory University / Grady Hospital Created by Steven A. Olson, MD in 2004 and Kyle Dickson, MD in 2004 First revised
Pelvic fractures. Dr Raymond Yean, MBBS Surgical SRMO
 Pelvic fractures Dr Raymond Yean, MBBS Surgical SRMO PELVIC FRACTURES Pelvic fracture account for 2-8% all skeletal injuries Associated with High energy trauma Soft tissue injuries and blood loss. Shock,
Pelvic fractures Dr Raymond Yean, MBBS Surgical SRMO PELVIC FRACTURES Pelvic fracture account for 2-8% all skeletal injuries Associated with High energy trauma Soft tissue injuries and blood loss. Shock,
Pelvic Injuries. Chapter 21
 Chapter 21 Introduction Injuries of the pelvis are an uncommon, but potentially lethal, battlefield injury. Blunt injuries may be associated with major hemorrhage and early mortality. Death within the
Chapter 21 Introduction Injuries of the pelvis are an uncommon, but potentially lethal, battlefield injury. Blunt injuries may be associated with major hemorrhage and early mortality. Death within the
10/2/2018. Acute Management of Pelvic Injuries. Learning Objectives. 17 yo male ped struck by truck
 17 yo male ped struck by truck Acute Management of Pelvic Injuries David Volgas, MD CoxHealth University of Missouri HD unstable Open pelvic wound superior gluteal fold through rectum to scrotum Open rami
17 yo male ped struck by truck Acute Management of Pelvic Injuries David Volgas, MD CoxHealth University of Missouri HD unstable Open pelvic wound superior gluteal fold through rectum to scrotum Open rami
THE INITIAL MANAGEMENT OF PELVIC AND ACETABULAR TRAUMA LOUIS LEBLOND MD FRCSC DEPT OF ORTHOPAEDICS THE MONCTON HOSPITAL - L HÔPITAL DE MONCTON
 THE INITIAL MANAGEMENT OF PELVIC AND ACETABULAR TRAUMA LOUIS LEBLOND MD FRCSC DEPT OF ORTHOPAEDICS THE MONCTON HOSPITAL - L HÔPITAL DE MONCTON DISCLOSURES + BACKGROUND No. Centre de formation médicale
THE INITIAL MANAGEMENT OF PELVIC AND ACETABULAR TRAUMA LOUIS LEBLOND MD FRCSC DEPT OF ORTHOPAEDICS THE MONCTON HOSPITAL - L HÔPITAL DE MONCTON DISCLOSURES + BACKGROUND No. Centre de formation médicale
Pelvic Fractures. AOCP National Course Belfast City Hospital. 11 th June D Swain BSc; FRCSI; FRCS (Orth.)
") Pelvic Fractures AOCP National Course Belfast City Hospital 11 th June 2010 Who s this bloke? Consultant orthopaedic surgeon RVH Trained in Belfast, England and Toronto Interests - pelvic and acetabular
Pelvic Fractures AOCP National Course Belfast City Hospital 11 th June 2010 Who s this bloke? Consultant orthopaedic surgeon RVH Trained in Belfast, England and Toronto Interests - pelvic and acetabular
Initial Management of Pelvic Injuries
 Initial Management of Pelvic Injuries Olav Røise, MD, PhD Chairman Division of Neuroscience and Skeletal Medicine Ullevål University Hospital Trauma treatment Represent a chain of health services in which
Initial Management of Pelvic Injuries Olav Røise, MD, PhD Chairman Division of Neuroscience and Skeletal Medicine Ullevål University Hospital Trauma treatment Represent a chain of health services in which
Initial Pelvic Fracture Management. Patrick M Reilly MD FACS February 27, 2010
 Initial Pelvic Fracture Management Patrick M Reilly MD FACS February 27, 2010 John Pryor MD Field Triage* * Step One : Physiology * Step Two : Anatomy * Step Three : Mechanism * Step Four : Co-Morbid Conditions
Initial Pelvic Fracture Management Patrick M Reilly MD FACS February 27, 2010 John Pryor MD Field Triage* * Step One : Physiology * Step Two : Anatomy * Step Three : Mechanism * Step Four : Co-Morbid Conditions
Management of Bleeding Pelvic Fractures
 Management of Bleeding Pelvic Fractures Clay Cothren Burlew, MD FACS Professor of Surgery Program Director, SCC and TACS Fellowships Director, Surgical Intensive Care Unit Denver Health Medical Center/University
Management of Bleeding Pelvic Fractures Clay Cothren Burlew, MD FACS Professor of Surgery Program Director, SCC and TACS Fellowships Director, Surgical Intensive Care Unit Denver Health Medical Center/University
Damage Control in Abdominal and Pelvic Injuries
 Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
Damage Control in Abdominal and Pelvic Injuries Raul Coimbra, MD, PhD, FACS The Monroe E. Trout Professor of Surgery Surgeon-in Chief UCSD Medical Center Hillcrest Campus Executive Vice-Chairman Department
West Yorkshire Major Trauma Network Clinical Guidelines 2015
 WYMTN: Pelvic fracture with urogenital trauma KEY RECOMMENDATIONS 1. During the initial exploratory survey / secondary survey, a. The external urethral meatus and the transurethral bladder catheter (if
WYMTN: Pelvic fracture with urogenital trauma KEY RECOMMENDATIONS 1. During the initial exploratory survey / secondary survey, a. The external urethral meatus and the transurethral bladder catheter (if
Management of Pelvic Fracture
 Management of Pelvis Fracture with Hemodynamic Instability James W. Davis MD Professor of Clinical Surgery, UCSF/Fresno Chief of Trauma Management of Pelvic Fracture How NOT to do it The basics Evaluation
Management of Pelvis Fracture with Hemodynamic Instability James W. Davis MD Professor of Clinical Surgery, UCSF/Fresno Chief of Trauma Management of Pelvic Fracture How NOT to do it The basics Evaluation
Guidelines and Protocols
 TITLE: PELVIC TRAUMA PURPOSE: Develop a protocol of care that will insure rapid identification and treatment of these patients PROCESS: I. CARE OF PATIENTS WITH PELVIC TRAUMA A. Patients in hemorrhagic
TITLE: PELVIC TRAUMA PURPOSE: Develop a protocol of care that will insure rapid identification and treatment of these patients PROCESS: I. CARE OF PATIENTS WITH PELVIC TRAUMA A. Patients in hemorrhagic
Haemodynamic deterioration in lateral compression pelvic fracture after prehospital pelvic circumferential compression device application
 Haemodynamic deterioration in lateral compression pelvic fracture after prehospital pelvic circumferential compression device application Authors Alan A Garner Retrieval consultant CareFlight Northmead,
Haemodynamic deterioration in lateral compression pelvic fracture after prehospital pelvic circumferential compression device application Authors Alan A Garner Retrieval consultant CareFlight Northmead,
Hassan R. Mir, MD, MBA, FACS
 DISCLOSURES Hassan R. Mir, MD, MBA, FACS Paid Consultant for a Company or Supplier Smith & Nephew Zimmer Biomet Trice Medical Stock or Stock Options Core Orthopaedics OrthoGrid Systems Research Support
DISCLOSURES Hassan R. Mir, MD, MBA, FACS Paid Consultant for a Company or Supplier Smith & Nephew Zimmer Biomet Trice Medical Stock or Stock Options Core Orthopaedics OrthoGrid Systems Research Support
UBC Department of Urologic Sciences Lecture Series. Urological Trauma
 UBC Department of Urologic Sciences Lecture Series Urological Trauma Disclaimer: This is a lot of information to cover and we are unlikely to cover it all today These slides are to be utilized for your
UBC Department of Urologic Sciences Lecture Series Urological Trauma Disclaimer: This is a lot of information to cover and we are unlikely to cover it all today These slides are to be utilized for your
Pelvic Fracture Care (CPG ID: 34) Provides a brief review for the stabilization and treatment of pelvic fractures sustained in combat casualties.
 Provides a brief review for the stabilization and treatment of pelvic fractures sustained in combat casualties.") JOINT TRAUMA SYS TEM CLINICAL PRACTIC E GUIDELINE (JTS CPG ) Pelvic Fracture Care (CPG ID: 34) Provides a brief review for the stabilization and treatment of pelvic fractures sustained in combat casualties.
JOINT TRAUMA SYS TEM CLINICAL PRACTIC E GUIDELINE (JTS CPG ) Pelvic Fracture Care (CPG ID: 34) Provides a brief review for the stabilization and treatment of pelvic fractures sustained in combat casualties.
Clinical aspects in urogenital injuries
 Clinical aspects in urogenital injuries Rolf Wahlqvist Oslo Urological University Clinic Aker University Hospital Nordic Rad.2008 1 Urogenital injuries in trauma patients Renal injury Ureteral injury (infrequent/iatrogenic)
Clinical aspects in urogenital injuries Rolf Wahlqvist Oslo Urological University Clinic Aker University Hospital Nordic Rad.2008 1 Urogenital injuries in trauma patients Renal injury Ureteral injury (infrequent/iatrogenic)
Bladder Trauma Data Collection Sheet
 Bladder Trauma Data Collection Sheet If there was no traumatic injury with PENETRATION of the bladder DO NOT proceed Date of injury: / / Time of injury: Date of hospital arrival: / / Time of hospital arrival:
Bladder Trauma Data Collection Sheet If there was no traumatic injury with PENETRATION of the bladder DO NOT proceed Date of injury: / / Time of injury: Date of hospital arrival: / / Time of hospital arrival:
Clinical Module. Pelvic Injury Trauma. Princess Alexandra Hospital Emergency Department. 1 Introduction
 Princess Alexandra Hospital Emergency Department Clinical Module Trauma Review Officers: Katherine Isoardi / Glenn Ryan Version no: 2 Review date: Aug 2015 Key Words: Pelvic Trauma, Pelvic Injury, Pelvic
Princess Alexandra Hospital Emergency Department Clinical Module Trauma Review Officers: Katherine Isoardi / Glenn Ryan Version no: 2 Review date: Aug 2015 Key Words: Pelvic Trauma, Pelvic Injury, Pelvic
Canadian Undergraduate Urology Curriculum (CanUUC): Genitourinary Trauma. Last reviewed June 2014
: Genitourinary Trauma. Last reviewed June 2014") Canadian Undergraduate Urology Curriculum (CanUUC): Genitourinary Trauma Last reviewed June 2014 Session Objectives 1. Recognize hematuria as the cardinal symptom of urinary tract trauma. 1. Outline the
Canadian Undergraduate Urology Curriculum (CanUUC): Genitourinary Trauma Last reviewed June 2014 Session Objectives 1. Recognize hematuria as the cardinal symptom of urinary tract trauma. 1. Outline the
Northern Trauma Network. Management of Haemodynamically Unstable Patients with Pelvic Injury
 Management of Haemodynamically Unstable Patients with Pelvic Injury Northern Trauma Network This guideline focuses on the assessment of haemodynamic instability related to haemorrhage associated with a
Management of Haemodynamically Unstable Patients with Pelvic Injury Northern Trauma Network This guideline focuses on the assessment of haemodynamic instability related to haemorrhage associated with a
Classification, management and outcomes of severe pelvic ring fractures
 Classification, management and outcomes of severe pelvic ring fractures School of Public Health and Preventive Medicine, Monash University The Alfred Hospital, Royal Melbourne Hospital, Epworth Health
Classification, management and outcomes of severe pelvic ring fractures School of Public Health and Preventive Medicine, Monash University The Alfred Hospital, Royal Melbourne Hospital, Epworth Health
Trauma. Neck trauma zones. Neck Injuries 1/3/2018. Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure
 Trauma 45 minutes highest points Ahmed Mahmoud, MD Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure Neck trauma zones Airway ;Rapid sequence intubation Breathing ;Needle
Trauma 45 minutes highest points Ahmed Mahmoud, MD Basic principles A ; Airway B ; Breathing C ; Circulation D ; Disability E ; Exposure Neck trauma zones Airway ;Rapid sequence intubation Breathing ;Needle
ATLS: Initial Assessment and Management. SAUSHEC Medical Student Lecture Series
 ATLS: Initial Assessment and Management SAUSHEC Medical Student Lecture Series Objectives Identify sequence of priorities in assessing the multiply injured patient Apply principles outlined in primary
ATLS: Initial Assessment and Management SAUSHEC Medical Student Lecture Series Objectives Identify sequence of priorities in assessing the multiply injured patient Apply principles outlined in primary
CORE STANDARDS STANDARDS USED IN TARN REPORTS
 CORE STANDARDS Time to CT Scan BEST PRACTICE TARIFF SECTION 4.10 MAJOR TRAUMA 7 If the patient is admitted directly to the MTC or transferred as an emergency, the patient must be received by a trauma team
CORE STANDARDS Time to CT Scan BEST PRACTICE TARIFF SECTION 4.10 MAJOR TRAUMA 7 If the patient is admitted directly to the MTC or transferred as an emergency, the patient must be received by a trauma team
Pelvis injuries Fractures of the femur (proximal,shaft) Dr Tamás Bodzay
 Dr Tamás Bodzay") Pelvis injuries Fractures of the femur (proximal,shaft) Dr Tamás Bodzay Pelvis anatomy Pelvis function - axial load bearing - protection: abdominal, pelvic structures Pelvic injury mechanism Falling from
Pelvis injuries Fractures of the femur (proximal,shaft) Dr Tamás Bodzay Pelvis anatomy Pelvis function - axial load bearing - protection: abdominal, pelvic structures Pelvic injury mechanism Falling from
Access Pelvic Fixator
 Access Pelvic Fixator Attila Poka, MD Director, Orthopedic Trauma Service Grant Medical Center Columbus, OH Patents Pending CONTENTS 1 Introduction...Page 2 Equipment Required...Page 3 Design Rationale...Page
Access Pelvic Fixator Attila Poka, MD Director, Orthopedic Trauma Service Grant Medical Center Columbus, OH Patents Pending CONTENTS 1 Introduction...Page 2 Equipment Required...Page 3 Design Rationale...Page
Renal Trauma: Management Options
 Renal Trauma: Management Options Immediate surgical repair Nephrectomy Conservative management Alonso RC et al. Kidney in Danger: CT Findings of Blunt and Penetrating Renal Trauma. RadioGraphics 2009;
Renal Trauma: Management Options Immediate surgical repair Nephrectomy Conservative management Alonso RC et al. Kidney in Danger: CT Findings of Blunt and Penetrating Renal Trauma. RadioGraphics 2009;
IMAGING OF PELVIC FRACTURES AND ASSOCIATED INJURIES C. Craig Blackmore, MD, MPH
 IMAGING OF PELVIC FRACTURES AND ASSOCIATED INJURIES C. Craig Blackmore, MD, MPH Introduction Pelvic fractures occur in approximately 113,000 persons in the United States each year [1], and have a major
IMAGING OF PELVIC FRACTURES AND ASSOCIATED INJURIES C. Craig Blackmore, MD, MPH Introduction Pelvic fractures occur in approximately 113,000 persons in the United States each year [1], and have a major
Surgical Care at the District Hospital. EMERGENCY & ESSENTIAL SURGICAL CARE
 Surgical Care at the District Hospital 1 17 Orthopedic Techniques Key Points 2 17.1 Traction Use an appropriate method of traction to treat fractures of the extremities and cervical spine Apply extremity
Surgical Care at the District Hospital 1 17 Orthopedic Techniques Key Points 2 17.1 Traction Use an appropriate method of traction to treat fractures of the extremities and cervical spine Apply extremity
T-PODResponder Pelvic Stabilization Device
 T-PODResponder Pelvic Stabilization Device Training Session Pyng Medical Corp. 1-604-303-7964 2014 Pyng Medical Corp. August 2014 PM-176a Why T-PODResponder? Pelvic fractures have a mortality rate of 5%
T-PODResponder Pelvic Stabilization Device Training Session Pyng Medical Corp. 1-604-303-7964 2014 Pyng Medical Corp. August 2014 PM-176a Why T-PODResponder? Pelvic fractures have a mortality rate of 5%
Center for Reconstructive Urethral Surgery Guido Barbagli Center for Reconstructive Urethral Surgery Arezzo - Italy
 Guido Barbagli Arezzo - Italy E-mail: guido@rdn.it Website: www.urethralcenter.it 23 rd ANNUAL EAU CONGRESS Sub-plenary Session on Male urinary incontinence 26 29 March 2008 Milan Italy Incontinence following
Guido Barbagli Arezzo - Italy E-mail: guido@rdn.it Website: www.urethralcenter.it 23 rd ANNUAL EAU CONGRESS Sub-plenary Session on Male urinary incontinence 26 29 March 2008 Milan Italy Incontinence following
Genitourinary Trauma Introduction GU Trauma overlooked
 Genitourinary Trauma Introduction GU Trauma overlooked 10-20% of all injured patients Long term morbidity Impotence Incontinence Life-threatening injuries first Urethral Injury Plan Bladder Injury Kidney
Genitourinary Trauma Introduction GU Trauma overlooked 10-20% of all injured patients Long term morbidity Impotence Incontinence Life-threatening injuries first Urethral Injury Plan Bladder Injury Kidney
Pelvic Trauma. Ø Pelvis: The most important area of the body. Ø Pelvic injuries often represent multisystem
 Pelvic Trauma Jim Holliman, M.D. FACEP Associate Professor of Surgery / Emergency Medicine Director, Center for International Emergency Medicine M.S. Hershey Medical Center Penn State University Hershey,
Pelvic Trauma Jim Holliman, M.D. FACEP Associate Professor of Surgery / Emergency Medicine Director, Center for International Emergency Medicine M.S. Hershey Medical Center Penn State University Hershey,
SUBAXIAL CERVICAL SPINE TRAUMA- DIAGNOSIS AND MANAGEMENT
 SUBAXIAL CERVICAL SPINE TRAUMA- DIAGNOSIS AND MANAGEMENT 1 Anatomy 3 columns- Anterior, middle and Posterior Anterior- ALL, Anterior 2/3 rd body & disc. Middle- Posterior 1/3 rd of body & disc, PLL Posterior-
SUBAXIAL CERVICAL SPINE TRAUMA- DIAGNOSIS AND MANAGEMENT 1 Anatomy 3 columns- Anterior, middle and Posterior Anterior- ALL, Anterior 2/3 rd body & disc. Middle- Posterior 1/3 rd of body & disc, PLL Posterior-
Delayed Presentation of Traumatic Bladder Injury: A case report and review of current treatment trends
 ISPUB.COM The Internet Journal of Urology Volume 5 Number 1 Delayed Presentation of Traumatic Bladder Injury: A case report and review of current treatment trends S Deem, C Lavender, S Agarwal Citation
ISPUB.COM The Internet Journal of Urology Volume 5 Number 1 Delayed Presentation of Traumatic Bladder Injury: A case report and review of current treatment trends S Deem, C Lavender, S Agarwal Citation
RESUSCITATION IN TRAUMA. Important things I have learnt
 RESUSCITATION IN TRAUMA Important things I have learnt Trauma resuscitation through the decades What was hot and now is not 1970s 1980s 1990s 2000s Now 1977 Fluids Summary Dogs subjected to arterial hemorrhage
RESUSCITATION IN TRAUMA Important things I have learnt Trauma resuscitation through the decades What was hot and now is not 1970s 1980s 1990s 2000s Now 1977 Fluids Summary Dogs subjected to arterial hemorrhage
Abdominal Trauma. Nat Krairojananan M.D., FRCST Department of Trauma and Emergency Medicine Phramongkutklao Hospital
 Abdominal Trauma Nat Krairojananan M.D., FRCST Department of Trauma and Emergency Medicine Phramongkutklao Hospital overview Quick review abdominal anatomy Review of mechanism of injury Review of investigation
Abdominal Trauma Nat Krairojananan M.D., FRCST Department of Trauma and Emergency Medicine Phramongkutklao Hospital overview Quick review abdominal anatomy Review of mechanism of injury Review of investigation
Emergent Management of Pelvic Ring Fractures with Use of Circumferential Compression
 This is an enhanced PDF from The Journal of Bone and Joint Surgery The PDF of the article you requested follows this cover page. Emergent Management of Pelvic Ring Fractures with Use of Circumferential
This is an enhanced PDF from The Journal of Bone and Joint Surgery The PDF of the article you requested follows this cover page. Emergent Management of Pelvic Ring Fractures with Use of Circumferential
Table 2. First Generated List of Expert Responses. Likert-Type Scale. Category or Criterion. Rationale or Comments (1) (2) (3) (4)
 (2) (3) (4)") Table 2. First Generated List of Expert Responses. Likert-Type Scale Category or Criterion Anatomical Structures and Features Skeletal Structures and Features (1) (2) (3) (4) Rationale or Comments 1. Bones
Table 2. First Generated List of Expert Responses. Likert-Type Scale Category or Criterion Anatomical Structures and Features Skeletal Structures and Features (1) (2) (3) (4) Rationale or Comments 1. Bones
Guido Barbagli. Center for Reconstructive ti Urethral lsurgery
 Guido Barbagli Center for Reconstructive ti Urethral lsurgery Arezzo - Italy E-mail: guido@rdn.it Website: www.urethralcenter.it Dedicated to Ruggero Lenzi, teacher and friend. His passing was a great
Guido Barbagli Center for Reconstructive ti Urethral lsurgery Arezzo - Italy E-mail: guido@rdn.it Website: www.urethralcenter.it Dedicated to Ruggero Lenzi, teacher and friend. His passing was a great
Ali Bakir Al-Hilli. Senior Lecturer Orthopedics and Trauma/ College of Medicine / Baghdad University. THE IRAQI POSTGRADUATE MEDICAL JOURNAL 525
 CLOSED THE IRAQI REDUCTION POSTGRADUATE FOR MEDICAL SACROILIAC JOURNAL DISRUPTION Evaluation of Closed Reduction and Percutaneous Iliosacral Cannulated Screw Fixation for Sacroiliac Disruption or Sacral
CLOSED THE IRAQI REDUCTION POSTGRADUATE FOR MEDICAL SACROILIAC JOURNAL DISRUPTION Evaluation of Closed Reduction and Percutaneous Iliosacral Cannulated Screw Fixation for Sacroiliac Disruption or Sacral
DISTRACTION EXTERNAL FIXATIONS OF PELVIC FRACTURES CAUSED BY A LATERAL COMPRESSION
 DOI: 10.5272/jimab.2011171.161 Journal of IMAB - Annual Proceeding (Scientific Papers) 2011, vol. 17, book 1 DISTRACTION EXTERNAL FIXATIONS OF PELVIC FRACTURES CAUSED BY A LATERAL COMPRESSION Pavlin Apostolov,
DOI: 10.5272/jimab.2011171.161 Journal of IMAB - Annual Proceeding (Scientific Papers) 2011, vol. 17, book 1 DISTRACTION EXTERNAL FIXATIONS OF PELVIC FRACTURES CAUSED BY A LATERAL COMPRESSION Pavlin Apostolov,
Financial Disclosure. Objectives 9/24/2018
 Hemorrhage and Transfusion Adjuncts in the Setting of Damage Control Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Adjunct Professor of Orthopedics and Neurosurgery, University
Hemorrhage and Transfusion Adjuncts in the Setting of Damage Control Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Adjunct Professor of Orthopedics and Neurosurgery, University
Iliosacral Screws Indications. What Injuries Are Amenable? CRPFPP Indications Injured Zones 11/18/2013
 Iliosacral Screws Indications ML Chip Routt Jr MD UT Houston Orthopedics Houston, Texas What Injuries Are Amenable? Sacroiliac Sacral Iliac Combination CRPFPP Indications Injured Zones SI Joint Sacral
Iliosacral Screws Indications ML Chip Routt Jr MD UT Houston Orthopedics Houston, Texas What Injuries Are Amenable? Sacroiliac Sacral Iliac Combination CRPFPP Indications Injured Zones SI Joint Sacral
MANAGEMENT OF SOLID ORGAN INJURIES
 MANAGEMENT OF SOLID ORGAN INJURIES Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Director of Surgical Critical Care, Harborview Medical Center Introduction Solid organ injury
MANAGEMENT OF SOLID ORGAN INJURIES Joseph Cuschieri, MD FACS Professor of Surgery, University of Washington Director of Surgical Critical Care, Harborview Medical Center Introduction Solid organ injury
Muscle spasm Diminished bowel sounds Nausea/vomiting
 3 4 5 6 7 8 9 0 Chapter 8: Abdomen and Genitalia Injuries Abdominal Injuries Abdomen is major body cavity extending from to pelvis. Contains organs that make up digestive, urinary, and genitourinary systems.
3 4 5 6 7 8 9 0 Chapter 8: Abdomen and Genitalia Injuries Abdominal Injuries Abdomen is major body cavity extending from to pelvis. Contains organs that make up digestive, urinary, and genitourinary systems.
2. Blunt abdominal Trauma
 Abdominal Trauma 1. Evaluation and management depends on: a. Mechanism (Blunt versus Penetrating) b. Injury complex in addition to abdomen c. Haemodynamic stability assessment: i. Classically patient s
Abdominal Trauma 1. Evaluation and management depends on: a. Mechanism (Blunt versus Penetrating) b. Injury complex in addition to abdomen c. Haemodynamic stability assessment: i. Classically patient s
PELVIC RING FRACTURES: SHOULD THEY BE FIXED?
 REVIEW ARTICLE PELVIC RING FRACTURES: SHOULD THEY BE FIXED? MARVIN TILE From the Sunnybrook Medical Centre, Toronto The management of traumatic disruption of the pelvic ring has become a focus of interest,
REVIEW ARTICLE PELVIC RING FRACTURES: SHOULD THEY BE FIXED? MARVIN TILE From the Sunnybrook Medical Centre, Toronto The management of traumatic disruption of the pelvic ring has become a focus of interest,
First practical session. Bones of the gluteal region
 First practical session 2017 Bones of the gluteal region The Hip bone The hip bone is made of: 1 The ilium: superior in position 2 The ischium:postero-inferior in position 3 The pubis: antero-inferior
First practical session 2017 Bones of the gluteal region The Hip bone The hip bone is made of: 1 The ilium: superior in position 2 The ischium:postero-inferior in position 3 The pubis: antero-inferior
ABC of Emergency Radiology
 ABC of Emergency Radiology It is possible for the non-specialist to interpret pelvic radiographs accurately Important anatomical considerations THE PELVIS P A Driscoll, R Ross, D A Nicholson FIG i-line
ABC of Emergency Radiology It is possible for the non-specialist to interpret pelvic radiographs accurately Important anatomical considerations THE PELVIS P A Driscoll, R Ross, D A Nicholson FIG i-line
Crescent Fracture-Dislocation of the Sacroiliac Joint: Use of Iliosacral Screws
 Med. J. Cairo Univ., Vol. 85, No. 5, September: 1815-1819, 2017 www.medicaljournalofcairouniversity.net Crescent Fracture-Dislocation of the Sacroiliac Joint: Use of Iliosacral Screws SHERIF A. KHALED,
Med. J. Cairo Univ., Vol. 85, No. 5, September: 1815-1819, 2017 www.medicaljournalofcairouniversity.net Crescent Fracture-Dislocation of the Sacroiliac Joint: Use of Iliosacral Screws SHERIF A. KHALED,
Fractures of the Thoracic and Lumbar Spine
 A spinal fracture is a serious injury. Nader M. Hebela, MD Fellow of the American Academy of Orthopaedic Surgeons http://orthodoc.aaos.org/hebela Cleveland Clinic Abu Dhabi Cleveland Clinic Abu Dhabi Neurological
A spinal fracture is a serious injury. Nader M. Hebela, MD Fellow of the American Academy of Orthopaedic Surgeons http://orthodoc.aaos.org/hebela Cleveland Clinic Abu Dhabi Cleveland Clinic Abu Dhabi Neurological
Major Trauma Scenarios. Ballarat Health Services Emergency Medicine Training Hub
 Major Trauma Scenarios Ballarat Health Services Emergency Medicine Training Hub Trauma Scenario 1 You receive a phone call from the ambulance service. They have a 27 yr old male involved in a MCA, he is
Major Trauma Scenarios Ballarat Health Services Emergency Medicine Training Hub Trauma Scenario 1 You receive a phone call from the ambulance service. They have a 27 yr old male involved in a MCA, he is
Activity Three: Where s the Bleeding?
 Activity Three: Where s the Bleeding? There are five main sites of potentially fatal bleeding in trauma, remembered by the phrase on the floor and four more. On the floor refers to losing blood externally
Activity Three: Where s the Bleeding? There are five main sites of potentially fatal bleeding in trauma, remembered by the phrase on the floor and four more. On the floor refers to losing blood externally
Orthopedic Injury Coding. Bryant Oliphant 10:20
 Orthopedic Injury Coding Bryant Oliphant 10:20 Orthopaedic Trauma in MTQIP Bryant Oliphant, MD, MBA, MSc Research Investigator bryantol@med.umich.edu @BonezNQuality DEPARTMENT OF ORTHOPAEDIC SURGERY None
Orthopedic Injury Coding Bryant Oliphant 10:20 Orthopaedic Trauma in MTQIP Bryant Oliphant, MD, MBA, MSc Research Investigator bryantol@med.umich.edu @BonezNQuality DEPARTMENT OF ORTHOPAEDIC SURGERY None
RADIOLOGY OF THE NORMAL ACETABULUM. X-ray X-ray X-ray. Figure. Figure ILIAC OBLIQUE VIEW OBTURATOR OBLIQUE VIEW AP VIEW
 RADIOLOGY OF THE NORMAL ACETABULUM Six radiological landmarks should be recognized on the Anterior Posterior radiograph: 1. Posterior wall of the acetabulum 2. Anterior wall of the acetabulum 3. Roof /
RADIOLOGY OF THE NORMAL ACETABULUM Six radiological landmarks should be recognized on the Anterior Posterior radiograph: 1. Posterior wall of the acetabulum 2. Anterior wall of the acetabulum 3. Roof /
High-energy pelvic fractures are
 Review Article Management of Hemorrhage in Life-threatening Pelvic Fracture David J. Hak, MD, MBA Wade R. Smith, MD Takashi Suzuki, MD Abstract Emergent life-saving treatment is required for high-energy
Review Article Management of Hemorrhage in Life-threatening Pelvic Fracture David J. Hak, MD, MBA Wade R. Smith, MD Takashi Suzuki, MD Abstract Emergent life-saving treatment is required for high-energy
Classification of Pelvis and Aetabulum Injuries
 Introduction The earliest attempt at classifying pelvic ring injuries was made by Bucholz where he described three groups essentially defining anteroposterior injuries of later classification systems.[1]
Introduction The earliest attempt at classifying pelvic ring injuries was made by Bucholz where he described three groups essentially defining anteroposterior injuries of later classification systems.[1]
- Acute Management of Pelvic Fractures - Damage Control Orthopaedics. High- energy Fractures
 Controversies in Orthopaedic Trauma Surgery Eric G. Meinberg, MD Assistant Clinical Professor UCSF/SFGH Orthopaedic Trauma InsKtute - Acute Management of Pelvic Fractures - Damage Control Orthopaedics
Controversies in Orthopaedic Trauma Surgery Eric G. Meinberg, MD Assistant Clinical Professor UCSF/SFGH Orthopaedic Trauma InsKtute - Acute Management of Pelvic Fractures - Damage Control Orthopaedics
PELVIS & SACRUM Dr. Jamila El-Medany Dr. Essam Eldin Salama
 PELVIS & SACRUM Dr. Jamila El-Medany Dr. Essam Eldin Salama Learning Objectives At the end of the lecture, the students should be able to : Describe the bony structures of the pelvis. Describe in detail
PELVIS & SACRUM Dr. Jamila El-Medany Dr. Essam Eldin Salama Learning Objectives At the end of the lecture, the students should be able to : Describe the bony structures of the pelvis. Describe in detail
utility of Plain Film Pelvic Radiographs in Blunt Trauma Patients in the Emergency Department
 utility of Plain Film Pelvic Radiographs in Blunt Trauma Patients in the Emergency Department AMAL KAMIL OBAID, M.D., ANDREW BARLEBEN, M.D., DIANA PORRAL, B.S., STEPHANIE LUSH, M.S.N., MARIANNE CINAT,
utility of Plain Film Pelvic Radiographs in Blunt Trauma Patients in the Emergency Department AMAL KAMIL OBAID, M.D., ANDREW BARLEBEN, M.D., DIANA PORRAL, B.S., STEPHANIE LUSH, M.S.N., MARIANNE CINAT,
Unstable fractures of the pelvis treated with a trapezoid compression frame
 Acta Orthop Scand 55, 325-329, 1984 Unstable fractures of the pelvis treated with a trapezoid compression frame Sixteen patients with unstable pelvic fractures were treated by early reduction and fixation
Acta Orthop Scand 55, 325-329, 1984 Unstable fractures of the pelvis treated with a trapezoid compression frame Sixteen patients with unstable pelvic fractures were treated by early reduction and fixation
Bleeding pelvic fractures: updates and controversies in acute phase management
 Hong Kong Journal of Emergency Medicine Bleeding pelvic fractures: updates and controversies in acute phase management CH Lai and CW Kam Background: The management of patients with haemodynamic instability
Hong Kong Journal of Emergency Medicine Bleeding pelvic fractures: updates and controversies in acute phase management CH Lai and CW Kam Background: The management of patients with haemodynamic instability
SPECIAL DIAGNOSTIC STUDIES IN BLUNT TRAUMA OLEH : Prof.DR.Dr Abdul Rasyid SpRad (K),Ph.D Dr.Evo Elidar Sp.Rad
,Ph.D Dr.Evo Elidar Sp.Rad") SPECIAL DIAGNOSTIC STUDIES IN BLUNT TRAUMA OLEH : Prof.DR.Dr Abdul Rasyid SpRad (K),Ph.D Dr.Evo Elidar Sp.Rad Trauma Emergency Room layout Ideally the trauma emergency room is centrally located to provide
SPECIAL DIAGNOSTIC STUDIES IN BLUNT TRAUMA OLEH : Prof.DR.Dr Abdul Rasyid SpRad (K),Ph.D Dr.Evo Elidar Sp.Rad Trauma Emergency Room layout Ideally the trauma emergency room is centrally located to provide
Imaging in the Trauma Patient
 Imaging in the Trauma Patient David A. Spain, MD Department of Surgery Stanford University Pan Scan Instead of Clinical Exam? 1 Granted, some patients don t need CT scan Platinum Package Stanford Special
Imaging in the Trauma Patient David A. Spain, MD Department of Surgery Stanford University Pan Scan Instead of Clinical Exam? 1 Granted, some patients don t need CT scan Platinum Package Stanford Special
Emergency Room Resuscitation of the Unstable Trauma Patient
 Emergency Room Resuscitation of the Unstable Trauma Patient Goals of trauma resuscitation Maintain: Systemic oxygenation Systemic perfusion Neurologic function Approach to unstable trauma patient Primary
Emergency Room Resuscitation of the Unstable Trauma Patient Goals of trauma resuscitation Maintain: Systemic oxygenation Systemic perfusion Neurologic function Approach to unstable trauma patient Primary
THE HIP. Cooler than cool, the pinnacle of what is "it". Beyond all trends and conventional coolness.
 THE HIP Cooler than cool, the pinnacle of what is "it". Beyond all trends and conventional coolness. Objectives Hip anatomy Causes of hip pain Hip exam Anatomy Bones Ilium Anterior Superior Iliac Spine
THE HIP Cooler than cool, the pinnacle of what is "it". Beyond all trends and conventional coolness. Objectives Hip anatomy Causes of hip pain Hip exam Anatomy Bones Ilium Anterior Superior Iliac Spine
Kaan Yücel M.D., Ph.D. 14.January.2014 Tuesday
 Kaan Yücel M.D., Ph.D. 14.January.2014 Tuesday Sexual differences are related mainly 1. Heavier build and larger muscles of most men 2. Adaptation of the pelvis (particularly the lesser pelvis) in women
Kaan Yücel M.D., Ph.D. 14.January.2014 Tuesday Sexual differences are related mainly 1. Heavier build and larger muscles of most men 2. Adaptation of the pelvis (particularly the lesser pelvis) in women
Algorithms for managing the common trauma patient
 ALGORITHMS Algorithms for managing the common trauma patient J John, MB ChB Department of Urology, Frere Hospital, East London Hospital Complex, East London, South Africa Corresponding author: J John (jeffveenajohn@gmail.com)
ALGORITHMS Algorithms for managing the common trauma patient J John, MB ChB Department of Urology, Frere Hospital, East London Hospital Complex, East London, South Africa Corresponding author: J John (jeffveenajohn@gmail.com)
M-AFRAKHTEH. MD OCT.2017 SHOHADA HOSPITAL TAJRISH
 Unrestricted M-AFRAKHTEH. MD OCT.2017 SHOHADA HOSPITAL TAJRISH Patients at imminent risk of exsanguination Manual aortic compression Resuscitative endovascular balloon occlusion of the aorta Uterine tourniquet
Unrestricted M-AFRAKHTEH. MD OCT.2017 SHOHADA HOSPITAL TAJRISH Patients at imminent risk of exsanguination Manual aortic compression Resuscitative endovascular balloon occlusion of the aorta Uterine tourniquet
Analysis of the Importance of Sacroiliac Joint Fractures as a Prognostic Factor of the Patients with Pelvic Fractures
 ORIGINARL ARTICLE J Trauma Inj 2018;31(1):6-11 http://doi.org/10.20408/jti.2018.31.1.6 JOURNAL OF TRAUMA AND INJURY Analysis of the Importance of Sacroiliac Joint Fractures as a Prognostic Factor of the
ORIGINARL ARTICLE J Trauma Inj 2018;31(1):6-11 http://doi.org/10.20408/jti.2018.31.1.6 JOURNAL OF TRAUMA AND INJURY Analysis of the Importance of Sacroiliac Joint Fractures as a Prognostic Factor of the
APPROACH TO TRAUMA. Dr E.Memary Anesthesiologist Assistant Professor of SBMU
 APPROACH TO TRAUMA Dr E.Memary Anesthesiologist Assistant Professor of SBMU Objectives Describe the initial approach to the injured patient, including the primary and secondary surveys. Identify the types
APPROACH TO TRAUMA Dr E.Memary Anesthesiologist Assistant Professor of SBMU Objectives Describe the initial approach to the injured patient, including the primary and secondary surveys. Identify the types
Anatomy & Physiology Pelvic Girdles 10.1 General Information
 Anatomy & Physiology Pelvic Girdles 10.1 General Information ICan2Ed, Inc. In human anatomy, the pelvis (plural pelves or pelvises) is the lower part of. The area of the body that is between the abdomen
Anatomy & Physiology Pelvic Girdles 10.1 General Information ICan2Ed, Inc. In human anatomy, the pelvis (plural pelves or pelvises) is the lower part of. The area of the body that is between the abdomen
Spinal Trauma. Dr T G Kruger
 Spinal Trauma Dr T G Kruger Epidemiology Spine injury in 6% of trauma patients Multiple levels involved in 20% of cases 80% of spinal cord injury patients have concurrent other system injuries 41% have
Spinal Trauma Dr T G Kruger Epidemiology Spine injury in 6% of trauma patients Multiple levels involved in 20% of cases 80% of spinal cord injury patients have concurrent other system injuries 41% have
Intracanal Sacral Nerve Impingement Following Percutaneous Iliosacral Screw Pelvic Fixation
 texas orthopaedic journal CASE REPORT Intracanal Sacral Nerve Impingement Following Percutaneous Iliosacral Screw Pelvic Fixation Michael L. Brennan, MD; John M. Hamilton, MD; Christopher D. Chaput, MD;
texas orthopaedic journal CASE REPORT Intracanal Sacral Nerve Impingement Following Percutaneous Iliosacral Screw Pelvic Fixation Michael L. Brennan, MD; John M. Hamilton, MD; Christopher D. Chaput, MD;
Subaxial Cervical Spine Trauma. Introduction. Anatomic Considerations 7/23/2018
 Subaxial Cervical Spine Trauma Sheyan J. Armaghani, MD Florida Orthopedic Institute Assistant Professor USF Dept of Orthopedics Introduction Trauma to the cervical spine accounts for 5 of all spine injuries
Subaxial Cervical Spine Trauma Sheyan J. Armaghani, MD Florida Orthopedic Institute Assistant Professor USF Dept of Orthopedics Introduction Trauma to the cervical spine accounts for 5 of all spine injuries
Imaging of Cervical Spine Trauma Tudor H Hughes, M.D.
 Imaging of Cervical Spine Trauma Tudor H Hughes, M.D. General Considerations Most spinal fractures are due to a single episode of major trauma. Fatigue fractures of the spine are unusual except in the
Imaging of Cervical Spine Trauma Tudor H Hughes, M.D. General Considerations Most spinal fractures are due to a single episode of major trauma. Fatigue fractures of the spine are unusual except in the
Abdomen and Genitalia Injuries. Chapter 28
 Abdomen and Genitalia Injuries Chapter 28 Hollow Organs in the Abdominal Cavity Signs of Peritonitis Abdominal pain Tenderness Muscle spasm Diminished bowel sounds Nausea/vomiting Distention Solid Organs
Abdomen and Genitalia Injuries Chapter 28 Hollow Organs in the Abdominal Cavity Signs of Peritonitis Abdominal pain Tenderness Muscle spasm Diminished bowel sounds Nausea/vomiting Distention Solid Organs
Treatment of Unstable Pelvic Ring Injuries
 REVIEW RTICLE Hip Pelvis 26(2): 79-83, 2014 http://dx.doi.org/10.5371/hp.2014.26.2.79 Print ISSN 2287-3260 Online ISSN 2287-3279 Treatment of Unstable Pelvic Ring Injuries Weon-Yoo Kim, MD Department of
REVIEW RTICLE Hip Pelvis 26(2): 79-83, 2014 http://dx.doi.org/10.5371/hp.2014.26.2.79 Print ISSN 2287-3260 Online ISSN 2287-3279 Treatment of Unstable Pelvic Ring Injuries Weon-Yoo Kim, MD Department of
PEDIATRIC TRAUMA I: ABDOMINAL TRAUMA BURNS. December 19, 2012
 PEDIATRIC TRAUMA I: ABDOMINAL TRAUMA BURNS Niel F. Miele,, M.D. December 19, 2012 EPIDEMIOLOGY Major Trauma responsible for
PEDIATRIC TRAUMA I: ABDOMINAL TRAUMA BURNS Niel F. Miele,, M.D. December 19, 2012 EPIDEMIOLOGY Major Trauma responsible for
Magnetic Resonance Imaging for the Evaluation of Ligamentous Injury in the Pelvis: A Prospective Case-Controlled Study
 ORIGINAL ARTICLE Magnetic Resonance Imaging for the Evaluation of ous Injury in the Pelvis: A Prospective Case-Controlled Study Joshua L. Gary, MD,* Michael Mulligan, MD, Kelley Banagan, MD,* Marcus F.
ORIGINAL ARTICLE Magnetic Resonance Imaging for the Evaluation of ous Injury in the Pelvis: A Prospective Case-Controlled Study Joshua L. Gary, MD,* Michael Mulligan, MD, Kelley Banagan, MD,* Marcus F.
Hemorrhage Control. Chapter 6
 Chapter 6 The hemorrhage that take[s] place when a main artery is divided is usually so rapid and so copious that the wounded man dies before help can reach him. Colonel H. M. Gray, 1919 Stop the Bleeding!
Chapter 6 The hemorrhage that take[s] place when a main artery is divided is usually so rapid and so copious that the wounded man dies before help can reach him. Colonel H. M. Gray, 1919 Stop the Bleeding!
Anterior Stabilisation of Sacroilliac Joint for Complex Pelvic Injuries
 CSE REPORT - Sacroilliac Joint Pelvic Injuries Malaysian Journal of Medical Sciences, Vol. 16, No. 3, July - September 2009 CSE REPORT nterior Stabilisation of Sacroilliac Joint for Complex Pelvic Injuries
CSE REPORT - Sacroilliac Joint Pelvic Injuries Malaysian Journal of Medical Sciences, Vol. 16, No. 3, July - September 2009 CSE REPORT nterior Stabilisation of Sacroilliac Joint for Complex Pelvic Injuries
PENETRATING COLON TRAUMA: THE CURRENT EVIDENCE
 PENETRATING COLON TRAUMA: THE CURRENT EVIDENCE Samuel Hawkins MD CASE PRESENTATION 22M BIBEMS s/p multiple GSW ABCs intact Normotensive, non-tachycardic Secondary Survey: 4 truncal bullet holes L superior
PENETRATING COLON TRAUMA: THE CURRENT EVIDENCE Samuel Hawkins MD CASE PRESENTATION 22M BIBEMS s/p multiple GSW ABCs intact Normotensive, non-tachycardic Secondary Survey: 4 truncal bullet holes L superior
John Kiefer, BS, DVM Resident in Small Animal Surgery. The Veterinary Forum, Leesburg, VA October 18 th, 2015
 John Kiefer, BS, DVM Resident in Small Animal Surgery The Veterinary Forum, Leesburg, VA October 18 th, 2015 www.vscvets.com Facebook.com/AnimalSurgeons Hind Limb Trauma Why this topic matters to you Triaging
John Kiefer, BS, DVM Resident in Small Animal Surgery The Veterinary Forum, Leesburg, VA October 18 th, 2015 www.vscvets.com Facebook.com/AnimalSurgeons Hind Limb Trauma Why this topic matters to you Triaging
We have reviewed this material in accordance with U.S. Copyright Law and have tried to maximize your ability to
 Author(s): Patrick Carter, Daniel Wachter, Rockefeller Oteng, Carl Seger, 2009-2010. License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution
Author(s): Patrick Carter, Daniel Wachter, Rockefeller Oteng, Carl Seger, 2009-2010. License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution
ROLE OF COMPUTED TOMOGRAPHY AND 3D RECONSTRUCTIONS IN PELVIC RIM AND ACETABULAR FRACTURES Somasekhar R 1, A. V. K. Adithya 2, Kalra V.
 ROLE OF COMPUTED TOMOGRAPHY AND 3D RECONSTRUCTIONS IN PELVIC RIM AND ACETABULAR FRACTURES Somasekhar R 1, A. V. K. Adithya 2, Kalra V. B 3 HOW TO CITE THIS ARTICLE: Somasekhar R, A. V. K. Adithya, Kalra
ROLE OF COMPUTED TOMOGRAPHY AND 3D RECONSTRUCTIONS IN PELVIC RIM AND ACETABULAR FRACTURES Somasekhar R 1, A. V. K. Adithya 2, Kalra V. B 3 HOW TO CITE THIS ARTICLE: Somasekhar R, A. V. K. Adithya, Kalra
Anterior Pelvic Plating and Sacroiliac Joint Fixation in Unstable Pelvic Ring Injuries
 Original Article http://dx.doi.org/10.3349/ymj.2012.53.2.422 pissn: 0513-5796, eissn: 1976-2437 Yonsei Med J 53(2):422-426, 2012 Anterior Pelvic Plating and Sacroiliac Joint Fixation in Unstable Pelvic
Original Article http://dx.doi.org/10.3349/ymj.2012.53.2.422 pissn: 0513-5796, eissn: 1976-2437 Yonsei Med J 53(2):422-426, 2012 Anterior Pelvic Plating and Sacroiliac Joint Fixation in Unstable Pelvic
Percutaneous Ilio-Sacral Screw Fixation in Supine Position under Fluoroscopy Guidance.
 Percutaneous Ilio-Sacral Screw Fixation in Supine Position under Fluoroscopy Guidance. Shrestha D, Dhoju D, Shrestha R, Sharma V ABSTRACT Background Department of Orthopaedic and Truamtology Dhulikhel
Percutaneous Ilio-Sacral Screw Fixation in Supine Position under Fluoroscopy Guidance. Shrestha D, Dhoju D, Shrestha R, Sharma V ABSTRACT Background Department of Orthopaedic and Truamtology Dhulikhel
Trauma Alert Step 2 Additions
 Trauma Alert Step 2 Additions MANGLED, DEGLOVED OR PULSELESS EXTREMITY PELVIC INJURY WITH HIGH-RISK MECHANISM OF INJURY Many thanks to Paramedic FTO Justin Bramlette for assembling this training presentation
Trauma Alert Step 2 Additions MANGLED, DEGLOVED OR PULSELESS EXTREMITY PELVIC INJURY WITH HIGH-RISK MECHANISM OF INJURY Many thanks to Paramedic FTO Justin Bramlette for assembling this training presentation
Noninvasive Reduction of Open-Book Pelvic Fractures by Circumferential Compression
 Journal of Orthopaedic Trauma Vol. 16, No. 6, pp. 367 373 2002 Lippincott Williams & Wilkins, Inc., Philadelphia Noninvasive Reduction of Open-Book Pelvic Fractures by Circumferential Compression Michael
Journal of Orthopaedic Trauma Vol. 16, No. 6, pp. 367 373 2002 Lippincott Williams & Wilkins, Inc., Philadelphia Noninvasive Reduction of Open-Book Pelvic Fractures by Circumferential Compression Michael
Pelvic ring fractures: what to expect
 Pelvic ring fractures: what to expect Poster No.: C-0690 Congress: ECR 2014 Type: Educational Exhibit Authors: A. L. Popirtac, I. G. Filimon ; Cluj-Napoca, Cl/RO, Cluj-Napoca/ RO Keywords: Trauma, Diagnostic
Pelvic ring fractures: what to expect Poster No.: C-0690 Congress: ECR 2014 Type: Educational Exhibit Authors: A. L. Popirtac, I. G. Filimon ; Cluj-Napoca, Cl/RO, Cluj-Napoca/ RO Keywords: Trauma, Diagnostic
Pelvic ring fractures: what to expect
 Pelvic ring fractures: what to expect Poster No.: C-0690 Congress: ECR 2014 Type: Educational Exhibit Authors: A. L. Popirtac, I. G. Filimon ; Cluj-Napoca, Cl/RO, Cluj-Napoca/ RO Keywords: Trauma, Diagnostic
Pelvic ring fractures: what to expect Poster No.: C-0690 Congress: ECR 2014 Type: Educational Exhibit Authors: A. L. Popirtac, I. G. Filimon ; Cluj-Napoca, Cl/RO, Cluj-Napoca/ RO Keywords: Trauma, Diagnostic
5/31/2018. Ipsilateral Femoral Neck And Shaft Fractures. Ipsilateral Neck-Shaft Fractures Introduction. Ipsilateral Neck-Shaft Fractures Introduction
 Ipsilateral Femoral Neck And Shaft Fractures Exchange Nailing For Non- Union Donald Wiss MD Cedars-Sinai Medical Center Los Angeles, California Introduction Uncommon Injury Invariably High Energy Trauma
Ipsilateral Femoral Neck And Shaft Fractures Exchange Nailing For Non- Union Donald Wiss MD Cedars-Sinai Medical Center Los Angeles, California Introduction Uncommon Injury Invariably High Energy Trauma
Clinical comparative analysis on unstable pelvic fractures in the treatment with percutaneous sacroiliac screws and
 European Review for Medical and Pharmacological Sciences Clinical comparative analysis on unstable pelvic fractures in the treatment with percutaneous sacroiliac screws and sacroiliac joint anterior plate
European Review for Medical and Pharmacological Sciences Clinical comparative analysis on unstable pelvic fractures in the treatment with percutaneous sacroiliac screws and sacroiliac joint anterior plate
Preperitoneal pelvic packing in patients with hemodynamic instability due to severe pelvic fracture: early experience in a Korean trauma center
 Jang et al. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine (2016) 24:3 DOI 10.1186/s13049-016-0196-5 ORIGINAL RESEARCH Open Access Preperitoneal pelvic packing in patients with hemodynamic
Jang et al. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine (2016) 24:3 DOI 10.1186/s13049-016-0196-5 ORIGINAL RESEARCH Open Access Preperitoneal pelvic packing in patients with hemodynamic
SPINE EVALUATION AND CLEARANCE Basic Principles
 SPINE EVALUATION AND CLEARANCE Basic Principles General 1. Entire spine is immobilized during primary survey. 2. Radiographic clearance of the spine is not required before emergent surgical procedures.
SPINE EVALUATION AND CLEARANCE Basic Principles General 1. Entire spine is immobilized during primary survey. 2. Radiographic clearance of the spine is not required before emergent surgical procedures.