How to Triage Orthopaedic Care. David W. Gray, M.D.
|
|
|
- Marjory Fox
- 6 years ago
- Views:
Transcription
1 How to Triage Orthopaedic Care David W. Gray, M.D.
2 OBJECTIVES: Define basic assessments skills needed to identify orthopedic injuries Differentiate when an orthopedic injury is a medical emergency Determine best level of care, when to refer to a higher level medical care, and which healthcare professional is the most appropriate (ER, UCC, PCP, or Specialist)
3 Skeletal Trauma 10 to 15 % of all Childhood Injuries Physeal Injuries are ~ 15% of all Skeletal Injuries
4 Immediate Referral for Musculoskeletal Injuries Suspected Spinal Cord Injury Obvious Deformity - extremity is bent or bowed Dislocation of Joint Open Laceration Neurologic Injury Vascular Injury - be able to assess pulses and color of extremity
5 Immediate Referral for Musculoskeletal Injuries Neurologic Injury - especially loss of motor function Tingling or Numbness in a single extremity after injury is not an uncommon complaint - reassess and know how to do a Neurologic Exam of an Extremity - you have to develop your skills Assess by Doing a Motor and Sensory Examination Light touch, Pin prick ( use a paper clip)
6 Immediate Referral for Musculoskeletal Injuries Neurologic Injury Assess by Doing a Motor and Sensory Examination Light touch, Pin prick, and 2 point Discrimination Paper Clip helpful for Pin Prick and 2 point discrimination 2 Point Discrimination very helpful for hand injuries and lacerations
7 Immediate Referral for Musculoskeletal Injuries Vascular Injury - be able to assess pulses and color of extremity Capillary refill is variable If the environment is cold and having difficulty with vascular exam warm the extremity
8 Immediate Referral for Musculoskeletal Injuries Compartment Syndrome is swelling with in a Muscular Compartment that closes off the capillary flow to the soft tissue of that compartment The Muscle Compartment is very firm, tense and painful to touch. This is a surgical emergency and needs immediate evaluation Can be associated with fractures, crush injuries or vascular injuries, or after extreme exertion
9 Immediate Referral for Musculoskeletal Injuries This is a surgical emergency and needs immediate evaluation It can happen acutely within an hour of injury or develop over several hours after injury Most commonly seen in leg (below the knee ) and forearm
10 Immediate Referral for Musculoskeletal Injuries Compartment Syndrome Pain out of Proportion - First sign is Pain on Passive Range of Motion Extreme Pain on Passive Motion of the Muscles in that Compartment - example severe pain on movement of fingers or toes after injury to the leg or forearm above Pulses are Intact early on! Neurologic Exam is Intact early on! (May have some some tingling ) The Muscle Compartment is very firm, tense and painful to touch.
11 Delayed Referral for Medical Evaluation Persistent Swelling Persistent Loss of Range of Motion Difficulty with Ambulation Persistent Pain Constitutional Symptoms - fever, weight loss
12 The History How, When and Where? Swelling? Ability to Ambulate? Did you hear or feel a Pop? Did you Relocate an Injured part?
13 Extremity Examination Learn How to Examine an Extremity Know the Vascular and Neurologic Examination - Study Know the Extremity Anatomy - Bone, Muscle, Ligament, Nerve, Vascular Dont be afraid to Reassess and Repeat your Examination Stay Calm
14 Physical Exam Visual Inspection for Swelling, Discoloration, Bruising, and Obvious Deformity? Open Laceration or Wound? Range of Motion - can the injured area move - either with the patient moving it or examiner? Stability of the Joint - may or may not be able to assess
15 Physical Exam Tenderness : Where is the maximal tenderness - over the Bone, Ligaments, Muscle or Joint? Is the Patient able to Weight Bear? Neurovascular Exam of the Extremity Are they able to Move the Injured Area
16 The Physical Exam Have the patient demonstrate the area of maximal tenderness Use one finger to localize tenderness Is the tenderness located over the bone or the soft tissues? Compare the 2 sides looking for swelling
17 Orthopaedic Assessment Palpate for Tenderness Deformity Evaluate Neurologic Status Evaluate the Vascular Status Assess the Soft Tissue Injury Understand the Mechanism of Injury

18 Rang s Childrens Fractures Orthopaedic Resources

19 Extremity ExaminationResources Hoppenfeld Physical Examination of Spine and Extremities

20 Extremity Examination Resources Hoppenfeld - Orthpaedic Neurology

21 Extremity Examination Resources Ciba Collection of Medical Illustrations Volume 8 Part 1 Anatomy, Physiology and Metabolic Disorders by Frank Netter
22 Skeletally Immature Patients Possess Unique Characteristics Compared to the Adults The Closer to Skeletal Maturity the more the Injury Patterns Mimic Adults
 than girls (11 to 12) 3.")
23 Unique Anatomy For Children and Implications for Injury Physis ( Growth Plates ) 1. Adds longitudinal growth of the bone 2. Peak height velocity occurs later in boys (13 to 14) than girls (11 to 12) 3. Periods of rapid growth put children at risk for injury as growth plates narrow near the end of growth

24 Orthopedic Anatomy Parts of a growing bone» Epiphysis» Physis» Metaphysis» Diaphysis

25 Anatomy Epiphysis Physis Metaphysis Diaphysis

26 Apophysis 1. Growth Area of bone where a muscle tendon attaches 2. Highest risk of injury during peak growth rate 3. Best Known - Tibial Tubercle - Osgood Schlatter Apophysis


27 Tibial Tubercle is an Apophysis- Osgood Schlatter is inflammation of the tibial tubercle - Apophysitis
28 Injury Terms: Fractures Fracture - Broken, Break, Crack etc. Open - soft tissue envelope open allowing contamination of bone to dirt and bacteria Closed - soft tissue envelope intact - no communication to outside world Comminuted - multiple pieces Compound - we do not use this term - it was primarily used to indicate an open fracture in older literature
29 Injury Terms: Sprain vs Strain 2 9
30 Sprains Severity: Grade I - min. structural disruption Grade II - partial disruption Grade III - complete disruption 3 0

31 Strain vs. Avulsion Fracture Site of Injury - know your Anatomy - Avulsion Injuries Hurt on the Bone Ischial Apophysis Avulsion - pulled away by Hamstring Origin

32 Pelvic Avulsion Fractures» Often preceding symptoms» Multiple Apophyseal Sites in the Pelvis» Sometimes occult» Disabling and can be slow to heal ASIS Lesser Trochanter AIIS Ischial Apophysi
 Pelvic")


33 Anterior Inferior Iliac Spine (Apophysis) Pelvic Avulsion Fracture the Rectus Femoris Muscle has its origin here - one of the 4 muscles that constitute the Quadriceps

34 Physeal Fracture Patterns 3 4
 IV. Through V. EveRything Ruined www.niams.nih.gov/.")
35 Salter Harris Classification System I. Separation II. Above III. Lower (below) IV. Through V. EveRything Ruined

36 Salter II Fracture Distal Radius

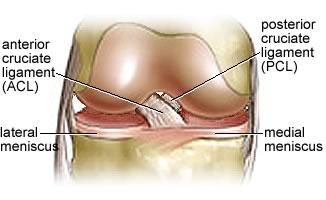
37 Knee Anatomy 3 7
38 Physeal Anatomy and Knee Ligaments Insertion Sites in Children May Create Unique Injuries 3 8
39 Salter I Fracture Distal Femur Fracture at Distal Femoral Physis (Growth Plate) as seen on Stress Film - the Physis Failed in this case instead of the Medial Collateral Ligament Tearing 3 9


40 Salter I Fracture Distal Femur How would you know to refer? Exam will show Swelling at the Joint - Large Joint Effusion Tender on the Femur - Directly on the Bone Unable to bear weight 4 0

41 Radius and Ulna Fractures Deformity - Bowing of Arm Open area that may represent an Open Fracture

42 Radius and/or Ulna Fractures» This was an open fracture» Immediate Referral» Often will see Dark Blood and Fat Globules in the Blood Oozing from Wound» Splint and Send

43 Supracondylar Fractures» Most common type is Fall on Outstretched Elbow» Marked Swelling around the Elbow» Splint with long arm splint with comfortable position.

44 Supracondylar Humerus Fracture» Marked Swelling around Elbow» May Have Ecchymosis Anteriorly from the Proximal humerus tearing thru the Brachialis Muscle and Coming up to the Skin» May even have Dimpling or Puckering of the Skin - which has been pulled back into the fracture» Refer Immediately» Splint in Position of Slight Flexion - 20 to 45 degrees

45 Supracondylar Humerus» General Typical age range 1-10 years Males > females by 2:1 Peak incidence: 5 to 8 years Approximately 1% are open concurrent forearm fractures in ~5%

46 Supracondylar Humerus» Arterial Injury: Pink hand Be highly suspicious of entrapment especially if: Anterior puckering Anterior medial ecchymosis Median nerve injury
47 Supracondylar Humerus Fracture» Examination Always check for palpable pulses (Doppler pulse may be present in spite of complete of occlusion of the brachial artery) Check compartments Surgeons should Always document detailed neurovascular examination before any treatment!!


48 Supracondylar Humerus Type III» Arterial Injury» Brachial Artery Occluded» Reconstituted Flow by Collaterals Distally
49 Supracondylar Humerus Fracture» Neurologic Examination Nerve injury is present in about 8% Of this 8% Radial nerve 40% Median nerve (complete) 35% Ulnar nerve 22% (but most common with flexion supracondylar) Anterior interosseous nerve is actually the most common (but requires detailed neuro exam)

50 Deformity This is a Femoral Shaft Fracture Note the Bowing of the Thigh Splint the Extremity If there are No Pulses and there is an Obvious Deformity Gently Straighten the Extremity and Splint prior to Transport For Example if the Extremity is Rotated more than 90 degrees For Example if the extremity is Bent more than 45 degrees and Floppy (Unstable)

51 If the fingers do not li or they cross over it indicates angular or rotational deformity of the bone Symmetric Hand Closure For finger and Hand I look for Symmetric Fl Cascade

52 Patellar Dislocation Referral Needed to Assess for any occult Fractures that are Intra- Articular Referral Does not have to be Immediate if the Patella is Reduced

53 Anterior Thigh Femoral Artery Femoral Nerve - Quadriceps Saphenous Nerve end branch of Femoral Nerve Obturator Nerve - supplies Adductor Muscles and Sensory Branches to Hip - Reason for Referred pain from Hip to Thigh and Knee

54 Medial Thigh Obturator Nerve - Medial Compartment of Thigh to supply the Adductor Muscles It also sends Sensory Branches to Hip - This is the Reason for Referred pain from Hip to Thigh and Knee

55 Posterior Thigh Sciatic Nerve - Posterior Compartment of Thigh Supplies Hamstring Muscles Branches to Common Peroneal and Tibial Nerve Near Knee

56 Anterior Lateral Leg Common Peroneal wraps around Fibular Neck Divides into: Superficial Peroneal Nerve - Lateral Compartment of Leg to Supply Peroneal Muscles - Everts Foot Deep Peroneal Nerve - Anterior Compartment of Leg to Supply Dorsiflexion Foot and Toes

57 Posterior Leg Tibial Nerve - Posterior Compartment of the Leg - also called Posterior Tibial Nerve - supplies the Flexors of the Foot and Toes - Plantar Flexion

58 Posterior Leg Femoral Artery becomes the Popliteal Artery - moving from Anterior Compartment of Thigh to Posterior Compartment on Medial Side of Distal Femur Popliteal Artery Splits into Anterior Tibial Artery Posterior Tibial Artery Peroneal Artery

59 Anterior Leg Popliteal Artery Splits into Anterior Tibial Artery which pierces the Intermuscular Septum from Posteriorly to Enter the Anterior Compartment It becomes the Dorsalis Pedis Artery at the Foot

60 Posterior Leg Popliteal Artery Splits into Popliteal Artery Splits into Anterior Tibial Artery Posterior Tibial Artery Peroneal Artery Posterior Tibial Artery is Palpable behind Medial Malleolus

61 Upper Extremity Brachial Artery Radial Artery Ulnar Artery Axillary Nerve Musculocutaneous Nerve Radial Nerve Ulnar Nerve Median Nerve

62 Dorsal Forearm Radial Nerve Motor Function Extensors of Wrist Extensors of MCP Joints of Hand Thumb Extension

63 Volar Forearm Median Nerve Motor Function Flexion of Thumb Flexion Radial Side of Wrist Flexion of Fingers Anterior Interosseous Nerve - branch of Median Nerve flexion IP of Thumb and DIP of Index

64 Volar Forearm Ulnar Nerve Motor Function Abduction Index Finger Flexion of DIP of Small Finger Flexion Ulnar Side of Wrist Intrinsics of Hand

65 Hand and Finger Assessment

66 Hand Sensory Innervation
OBJECTIVES: Define basic assessments skills needed to identify orthopedic injuries. Differentiate when an orthopedic injury is a medical emergency
 1 2 How to Triage Orthopaedic Care David W. Gray, M.D. OBJECTIVES: Define basic assessments skills needed to identify orthopedic injuries Differentiate when an orthopedic injury is a medical emergency
1 2 How to Triage Orthopaedic Care David W. Gray, M.D. OBJECTIVES: Define basic assessments skills needed to identify orthopedic injuries Differentiate when an orthopedic injury is a medical emergency
Upper Extremity Fractures
 Upper Extremity Fractures Ranie Whatley, RN,FNP-C David W. Gray, MD Skeletal Trauma 10 to 15 % of all Childhood Injuries Physeal (Growth Plate) Injuries are ~ 15% of all Skeletal Injuries Orthopaedic Assessment
Upper Extremity Fractures Ranie Whatley, RN,FNP-C David W. Gray, MD Skeletal Trauma 10 to 15 % of all Childhood Injuries Physeal (Growth Plate) Injuries are ~ 15% of all Skeletal Injuries Orthopaedic Assessment
Pediatric Fractures. Objectives. Epiphyseal Complex. Anatomy and Physiology. Ligaments. Bony matrix
 1 Pediatric Fractures Nicholas White, MD Assistant Professor of Pediatrics Eastern Virginia Medical School Attending, Pediatric Emergency Department Children s Hospital of The King s Daughters Objectives
1 Pediatric Fractures Nicholas White, MD Assistant Professor of Pediatrics Eastern Virginia Medical School Attending, Pediatric Emergency Department Children s Hospital of The King s Daughters Objectives
Surgical Care at the District Hospital. EMERGENCY & ESSENTIAL SURGICAL CARE
 Surgical Care at the District Hospital 1 18 Orthopedic Trauma Key Points 2 18.1 Upper Extremity Injuries Clavicle Fractures Diagnose fractures from the history and by physical examination Treat with a
Surgical Care at the District Hospital 1 18 Orthopedic Trauma Key Points 2 18.1 Upper Extremity Injuries Clavicle Fractures Diagnose fractures from the history and by physical examination Treat with a
Year 2004 Paper one: Questions supplied by Megan
 QUESTION 47 A 58yo man is noted to have a right foot drop three days following a right total hip replacement. On examination there is weakness of right ankle dorsiflexion and toe extension (grade 4/5).
QUESTION 47 A 58yo man is noted to have a right foot drop three days following a right total hip replacement. On examination there is weakness of right ankle dorsiflexion and toe extension (grade 4/5).
PEM GUIDE CHILDHOOD FRACTURES
 PEM GUIDE CHILDHOOD FRACTURES INTRODUCTION Skeletal injuries account for 10-15% of all injuries in children; 20% of those are fractures, 3 out of 4 fractures affect the physis or growth plate. Always consider
PEM GUIDE CHILDHOOD FRACTURES INTRODUCTION Skeletal injuries account for 10-15% of all injuries in children; 20% of those are fractures, 3 out of 4 fractures affect the physis or growth plate. Always consider
Chapter 29 Orthopaedic Injuries Principles of Splinting Types of Muscles
 1 2 3 4 5 6 7 Chapter 29 Orthopaedic Injuries Principles of Splinting Types of Muscles Striated Skeletal Smooth Anatomy and Physiology of the Musculoskeletal System Skeletal System Skeletal System Functions
1 2 3 4 5 6 7 Chapter 29 Orthopaedic Injuries Principles of Splinting Types of Muscles Striated Skeletal Smooth Anatomy and Physiology of the Musculoskeletal System Skeletal System Skeletal System Functions
Where should you palpate the pulse of different arteries in the lower limb?
 Where should you palpate the pulse of different arteries in the lower limb? The femoral artery In the femoral triangle, its pulse is easily felt just inferior to the inguinal ligament midway between the
Where should you palpate the pulse of different arteries in the lower limb? The femoral artery In the femoral triangle, its pulse is easily felt just inferior to the inguinal ligament midway between the
1 Chapter 29 Orthopaedic Injuries Principles of Splinting 2 Types of Muscles. Striated Skeletal. Smooth
 1 Chapter 29 Orthopaedic Injuries Principles of Splinting 2 Types of Muscles Striated Skeletal Smooth 3 Anatomy and Physiology of the Musculoskeletal System 4 Skeletal System 5 Skeletal System Functions
1 Chapter 29 Orthopaedic Injuries Principles of Splinting 2 Types of Muscles Striated Skeletal Smooth 3 Anatomy and Physiology of the Musculoskeletal System 4 Skeletal System 5 Skeletal System Functions
The Lower Limb II. Anatomy RHS 241 Lecture 3 Dr. Einas Al-Eisa
 The Lower Limb II Anatomy RHS 241 Lecture 3 Dr. Einas Al-Eisa Tibia The larger & medial bone of the leg Functions: Attachment of muscles Transfer of weight from femur to skeleton of the foot Articulations
The Lower Limb II Anatomy RHS 241 Lecture 3 Dr. Einas Al-Eisa Tibia The larger & medial bone of the leg Functions: Attachment of muscles Transfer of weight from femur to skeleton of the foot Articulations
FOOSH It sounded like a fun thing at the time!
 FOOSH It sounded like a fun thing at the time! Evaluating acute hand and wrist injuries Larry Collins, MPAS, PA-C, ATC, DFAAPA Assistant Professor, Physician Assistant Program Assistant Professor, Department
FOOSH It sounded like a fun thing at the time! Evaluating acute hand and wrist injuries Larry Collins, MPAS, PA-C, ATC, DFAAPA Assistant Professor, Physician Assistant Program Assistant Professor, Department
EMERGENCY PITFALLS IN ORTHOPAEDIC TRAUMA. Thierry E. Benaroch, MD, FRCS MCH Trauma Rounds February 9, 2009
 EMERGENCY PITFALLS IN ORTHOPAEDIC TRAUMA Thierry E. Benaroch, MD, FRCS MCH Trauma Rounds February 9, 2009 MORAL OF THE STORY Fracture distal radius and intact ulna W/O radius fracture will most likely
EMERGENCY PITFALLS IN ORTHOPAEDIC TRAUMA Thierry E. Benaroch, MD, FRCS MCH Trauma Rounds February 9, 2009 MORAL OF THE STORY Fracture distal radius and intact ulna W/O radius fracture will most likely
7/1/2012. Repetitive valgus stresses cause microfractures in the apophyseal cartilage (weak link) Common in year olds
 Common in year olds") 1 2 3 4 5 6 7 When growing pains are not growing pains David W. Gray,M.D. Medical Director Orthopedics Differential Diagnosis Fracture Ligament Injury Disloclation Cartilage Injury Apophysitis Inflammation
1 2 3 4 5 6 7 When growing pains are not growing pains David W. Gray,M.D. Medical Director Orthopedics Differential Diagnosis Fracture Ligament Injury Disloclation Cartilage Injury Apophysitis Inflammation
FOOSH It sounded like a fun thing at the time!
 FOOSH It sounded like a fun thing at the time! Evaluating acute hand and wrist injuries Larry Collins, MPAS, PA-C, ATC, DFAAPA Assistant Professor, Physician Assistant Program Assistant Professor, Department
FOOSH It sounded like a fun thing at the time! Evaluating acute hand and wrist injuries Larry Collins, MPAS, PA-C, ATC, DFAAPA Assistant Professor, Physician Assistant Program Assistant Professor, Department
AMERICAN RED CROSS FIRST AID RESPONDING TO EMERGENCIES FOURTH EDITION Copyright 2006 by The American National Red Cross All rights reserved.
 Musculoskeletal injuries are most commonly caused by Mechanical forms of energy. Chemicals. Electrical energy. Heat Mechanical energy produces direct, indirect, twisting and contracting forces. Can be
Musculoskeletal injuries are most commonly caused by Mechanical forms of energy. Chemicals. Electrical energy. Heat Mechanical energy produces direct, indirect, twisting and contracting forces. Can be
The arm: *For images refer back to the slides
 The arm: *For images refer back to the slides Muscles of the arm: deltoid, triceps (which is located at the back of the arm), biceps and brachialis (it lies under the biceps), brachioradialis (it lies
The arm: *For images refer back to the slides Muscles of the arm: deltoid, triceps (which is located at the back of the arm), biceps and brachialis (it lies under the biceps), brachioradialis (it lies
Contents of the Posterior Fascial Compartment of the Thigh
 Contents of the Posterior Fascial Compartment of the Thigh 1-Muscles: B i c e p s f e m o r i s S e m i t e n d i n o s u s S e m i m e m b r a n o s u s a small part of the adductor magnus (h a m s t
Contents of the Posterior Fascial Compartment of the Thigh 1-Muscles: B i c e p s f e m o r i s S e m i t e n d i n o s u s S e m i m e m b r a n o s u s a small part of the adductor magnus (h a m s t
Apply this knowledge into proper management strategies and referrals
 1 2 3 Lower Extremity Injuries Jason Kennedy, M.D. Disclosures I have no financial/ industry disclosures. Objectives Identify common lower extremity injury patterns in the child and adolescent Apply this
1 2 3 Lower Extremity Injuries Jason Kennedy, M.D. Disclosures I have no financial/ industry disclosures. Objectives Identify common lower extremity injury patterns in the child and adolescent Apply this
SMALL GROUP SESSION 16 January 8 th or 10 th Shoulder pain case/ Touch workshop/ Upper and Lower Extremity Examination
 SMALL GROUP SESSION 16 January 8 th or 10 th Shoulder pain case/ Touch workshop/ Upper and Lower Extremity Examination Suggested Readings: Opatrny L. The Healing Touch. Ann Int Med 2002; 137:1003. http://www.annals.org/cgi/reprint/137/12/1003.pdf
SMALL GROUP SESSION 16 January 8 th or 10 th Shoulder pain case/ Touch workshop/ Upper and Lower Extremity Examination Suggested Readings: Opatrny L. The Healing Touch. Ann Int Med 2002; 137:1003. http://www.annals.org/cgi/reprint/137/12/1003.pdf
Injuries to the Hands and Feet
 Injuries to the Hands and Feet Chapter 26 Injuries to the Hands and Feet Introduction Combat injuries to the hands and feet differ from those of the arms and legs in terms of mortality and morbidity. Death
Injuries to the Hands and Feet Chapter 26 Injuries to the Hands and Feet Introduction Combat injuries to the hands and feet differ from those of the arms and legs in terms of mortality and morbidity. Death
Common Orthopaedic Injuries in Children
 Common Orthopaedic Injuries in Children Rakesh P. Mashru, M.D. Division of Orthopaedic Trauma Cooper University Hospital Cooper Medical School of Rowan University December 1, 2017 1 Learning Objectives
Common Orthopaedic Injuries in Children Rakesh P. Mashru, M.D. Division of Orthopaedic Trauma Cooper University Hospital Cooper Medical School of Rowan University December 1, 2017 1 Learning Objectives
Common Apophyseal Problems in the Athlete
 Disclosure Common Apophyseal Problems in the Athlete Mark Halstead, MD November 19, 2009 Faculty Disclosure Information In the past 12 months, I have no relevant financial relationships with the manufacturer
Disclosure Common Apophyseal Problems in the Athlete Mark Halstead, MD November 19, 2009 Faculty Disclosure Information In the past 12 months, I have no relevant financial relationships with the manufacturer
Practice Changes I Hope You Make
 Is that Bad? What PCPs (& Parents) Need to Know about Fractures Aharon Z. Gladstein, MD Pediatric Orthopaedics & Sports Medicine Texas Children s Hospital Assistant Professor, Orthopaedics Baylor College
Is that Bad? What PCPs (& Parents) Need to Know about Fractures Aharon Z. Gladstein, MD Pediatric Orthopaedics & Sports Medicine Texas Children s Hospital Assistant Professor, Orthopaedics Baylor College
Peripheral Vascular Examination. Dr. Gary Mumaugh Western Physical Assessment
 Peripheral Vascular Examination Dr. Gary Mumaugh Western Physical Assessment Competencies 1. Inspection of upper extremity for: size symmetry swelling venous pattern color Texture nail beds Competencies
Peripheral Vascular Examination Dr. Gary Mumaugh Western Physical Assessment Competencies 1. Inspection of upper extremity for: size symmetry swelling venous pattern color Texture nail beds Competencies
musculoskeletal system anatomy nerves of the lower limb 2 done by: Dina sawadha & mohammad abukabeer
 musculoskeletal system anatomy nerves of the lower limb 2 done by: Dina sawadha & mohammad abukabeer #Sacral plexus : emerges from the ventral rami of the spinal segments L4 - S4 and provides motor and
musculoskeletal system anatomy nerves of the lower limb 2 done by: Dina sawadha & mohammad abukabeer #Sacral plexus : emerges from the ventral rami of the spinal segments L4 - S4 and provides motor and
CASE ONE CASE ONE. RADIAL HEAD FRACTURE Mason Classification. RADIAL HEAD FRACTURE Mechanism of Injury. RADIAL HEAD FRACTURE Imaging
 CASE ONE An eighteen year old female falls during a basketball game, striking her elbow on the court. She presents to your office that day with a painful, swollen elbow that she is unable to flex or extend
CASE ONE An eighteen year old female falls during a basketball game, striking her elbow on the court. She presents to your office that day with a painful, swollen elbow that she is unable to flex or extend
*the Arm* -the arm extends from the shoulder joint (proximal), to the elbow joint (distal) - it has one bone ; the humerus which is a long bone
, to the elbow joint (distal) - it has one bone ; the humerus which is a long bone") *the Arm* -the arm extends from the shoulder joint (proximal), to the elbow joint (distal) - it has one bone ; the humerus which is a long bone - muscles in the arm : *brachialis muscle *Biceps brachii
*the Arm* -the arm extends from the shoulder joint (proximal), to the elbow joint (distal) - it has one bone ; the humerus which is a long bone - muscles in the arm : *brachialis muscle *Biceps brachii
Fractures and dislocations around elbow in adult
 Lec: 3 Fractures and dislocations around elbow in adult These include fractures of distal humerus, fracture of the capitulum, fracture of the radial head, fracture of the olecranon & dislocation of the
Lec: 3 Fractures and dislocations around elbow in adult These include fractures of distal humerus, fracture of the capitulum, fracture of the radial head, fracture of the olecranon & dislocation of the
Disclosures Head to Toe: Common Sports Injuries in Kids
 Disclosures Head to Toe: Common Sports Injuries in Kids None R. Jay Lee MD Director Pediatric Orthopaedic Fellowship Assistant Professor Pediatric Orthopaedics Johns Hopkins / Bloomberg Children s Objectives
Disclosures Head to Toe: Common Sports Injuries in Kids None R. Jay Lee MD Director Pediatric Orthopaedic Fellowship Assistant Professor Pediatric Orthopaedics Johns Hopkins / Bloomberg Children s Objectives
1-Muscles: 2-Blood supply: Branches of the profunda femoris artery. 3-Nerve supply: Sciatic nerve
 1-Muscles: B i c e p s f e m o r i s S e m i t e n d i n o s u s S e m i m e m b r a n o s u s a small part of the adductor magnus (h a m s t r i n g p a r t o r i s c h i a l p a r t ) 2-Blood supply:
1-Muscles: B i c e p s f e m o r i s S e m i t e n d i n o s u s S e m i m e m b r a n o s u s a small part of the adductor magnus (h a m s t r i n g p a r t o r i s c h i a l p a r t ) 2-Blood supply:
Lower Limb Nerves. Clinical Anatomy
 Lower Limb Nerves Clinical Anatomy Lumbar Plexus Ventral rami L1 L4 Supplies: Abdominal wall External genitalia Anteromedial thigh Major nerves.. Lumbar Plexus Nerves relation to psoas m. : Obturator n.
Lower Limb Nerves Clinical Anatomy Lumbar Plexus Ventral rami L1 L4 Supplies: Abdominal wall External genitalia Anteromedial thigh Major nerves.. Lumbar Plexus Nerves relation to psoas m. : Obturator n.
On the Field Management of Pediatric Trauma
 On the Field Management of Pediatric Trauma Kyle Nagle, MD MPH University of Colorado Department of Orthopedics Children s Hospital Colorado Orthopedics Institute Disclosures I have no conflicts of interest
On the Field Management of Pediatric Trauma Kyle Nagle, MD MPH University of Colorado Department of Orthopedics Children s Hospital Colorado Orthopedics Institute Disclosures I have no conflicts of interest
Muscles of the lower extremities. Dr. Nabil khouri MD, MSc, Ph.D
 Muscles of the lower extremities Dr. Nabil khouri MD, MSc, Ph.D Posterior leg Popliteal fossa Boundaries Biceps femoris (superior-lateral) Semitendinosis and semimembranosis (superior-medial) Gastrocnemius
Muscles of the lower extremities Dr. Nabil khouri MD, MSc, Ph.D Posterior leg Popliteal fossa Boundaries Biceps femoris (superior-lateral) Semitendinosis and semimembranosis (superior-medial) Gastrocnemius
ANATYOMY OF The thigh
 ANATYOMY OF The thigh 1- Lateral cutaneous nerve of the thigh Ι) Skin of the thigh Anterior view 2- Femoral branch of the genitofemoral nerve 5- Intermediate cutaneous nerve of the thigh 1, 2 and 3 are
ANATYOMY OF The thigh 1- Lateral cutaneous nerve of the thigh Ι) Skin of the thigh Anterior view 2- Femoral branch of the genitofemoral nerve 5- Intermediate cutaneous nerve of the thigh 1, 2 and 3 are
Case. 5 year old with 2 weeks leg pain and now refusing to walk + Fevers, lower leg swelling, warmth Denies and history of trauma or wounds
 Case 5 year old with 2 weeks leg pain and now refusing to walk + Fevers, lower leg swelling, warmth Denies and history of trauma or wounds Exam I: Swelling over entire tibia extending to foot P: Tenderness
Case 5 year old with 2 weeks leg pain and now refusing to walk + Fevers, lower leg swelling, warmth Denies and history of trauma or wounds Exam I: Swelling over entire tibia extending to foot P: Tenderness
Leg. Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology
 Leg Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Skin of the Leg Cutaneous Nerves Medially: The saphenous nerve, a branch of the femoral nerve supplies the skin on the medial surface
Leg Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Skin of the Leg Cutaneous Nerves Medially: The saphenous nerve, a branch of the femoral nerve supplies the skin on the medial surface
The Lower Limb VI: The Leg. Anatomy RHS 241 Lecture 6 Dr. Einas Al-Eisa
 The Lower Limb VI: The Leg Anatomy RHS 241 Lecture 6 Dr. Einas Al-Eisa Muscles of the leg Posterior compartment (superficial & deep): primary plantar flexors of the foot flexors of the toes Anterior compartment:
The Lower Limb VI: The Leg Anatomy RHS 241 Lecture 6 Dr. Einas Al-Eisa Muscles of the leg Posterior compartment (superficial & deep): primary plantar flexors of the foot flexors of the toes Anterior compartment:
The Lower Limb. Anatomy RHS 241 Lecture 2 Dr. Einas Al-Eisa
 The Lower Limb Anatomy RHS 241 Lecture 2 Dr. Einas Al-Eisa The bony pelvis Protective osseofibrous ring for the pelvic viscera Transfer of forces to: acetabulum & head of femur (when standing) ischial
The Lower Limb Anatomy RHS 241 Lecture 2 Dr. Einas Al-Eisa The bony pelvis Protective osseofibrous ring for the pelvic viscera Transfer of forces to: acetabulum & head of femur (when standing) ischial
Fascial Compartments of the Upper Arm
 Fascial Compartments of the Upper Arm The upper arm is enclosed in a sheath of deep fascia and has two fascial septa: 1- Medial fascial septum (medial intermuscular septum): attached to the medial supracondylar
Fascial Compartments of the Upper Arm The upper arm is enclosed in a sheath of deep fascia and has two fascial septa: 1- Medial fascial septum (medial intermuscular septum): attached to the medial supracondylar
The Knee. Clarification of Terms. Osteology of the Knee 7/28/2013. The knee consists of: The tibiofemoral joint Patellofemoral joint
 The Knee Clarification of Terms The knee consists of: The tibiofemoral joint Patellofemoral joint Mansfield, p273 Osteology of the Knee Distal Femur Proximal tibia and fibula Patella 1 Osteology of the
The Knee Clarification of Terms The knee consists of: The tibiofemoral joint Patellofemoral joint Mansfield, p273 Osteology of the Knee Distal Femur Proximal tibia and fibula Patella 1 Osteology of the
Nerves of Upper limb. Dr. Brijendra Singh Professor & Head Department of Anatomy AIIMS Rishikesh
 Nerves of Upper limb Dr. Brijendra Singh Professor & Head Department of Anatomy AIIMS Rishikesh 1 Objectives Origin, course & relation of median & ulnar nerves. Motor & sensory distribution Carpal tunnel
Nerves of Upper limb Dr. Brijendra Singh Professor & Head Department of Anatomy AIIMS Rishikesh 1 Objectives Origin, course & relation of median & ulnar nerves. Motor & sensory distribution Carpal tunnel
Copyright 2003 Pearson Education, Inc. publishing as Benjamin Cummings. Dr. Nabil Khouri MD, MSc, Ph.D
 Dr. Nabil Khouri MD, MSc, Ph.D Pelvic Girdle (Hip) Organization of the Lower Limb It is divided into: The Gluteal region The thigh The knee The leg The ankle The foot The thigh and the leg have compartments
Dr. Nabil Khouri MD, MSc, Ph.D Pelvic Girdle (Hip) Organization of the Lower Limb It is divided into: The Gluteal region The thigh The knee The leg The ankle The foot The thigh and the leg have compartments
Sick Call Screener Course
 Sick Call Screener Course Musculoskeletal System Upper Extremities (2.7) 2.7-2-1 Enabling Objectives 1.46 Utilize the knowledge of musculoskeletal system anatomy while assessing a patient with a musculoskeletal
Sick Call Screener Course Musculoskeletal System Upper Extremities (2.7) 2.7-2-1 Enabling Objectives 1.46 Utilize the knowledge of musculoskeletal system anatomy while assessing a patient with a musculoskeletal
Practical 1 Worksheet
 Practical 1 Worksheet ANATOMICAL TERMS 1. Use the word bank to fill in the missing words. reference side stand body arms palms anatomical forward All anatomical terms have a(n) point which is called the
Practical 1 Worksheet ANATOMICAL TERMS 1. Use the word bank to fill in the missing words. reference side stand body arms palms anatomical forward All anatomical terms have a(n) point which is called the
Hand Anatomy A Patient's Guide to Hand Anatomy
 Hand Anatomy A Patient's Guide to Hand Anatomy Introduction Few structures of the human anatomy are as unique as the hand. The hand needs to be mobile in order to position the fingers and thumb. Adequate
Hand Anatomy A Patient's Guide to Hand Anatomy Introduction Few structures of the human anatomy are as unique as the hand. The hand needs to be mobile in order to position the fingers and thumb. Adequate
Physical Examination of the Knee
 History: Pain Traumatic vs. atraumatic Acute vs Chronic Mechanism of injury Swelling, catching, instability Previous evaluation and treatment General Setup Examine standing, sitting and supine Evaluate
History: Pain Traumatic vs. atraumatic Acute vs Chronic Mechanism of injury Swelling, catching, instability Previous evaluation and treatment General Setup Examine standing, sitting and supine Evaluate
Disclosure. Pediatric Orthopedic Emergencies. I have no actual or potential conflict of interest in relation to this program or presentation.
 Pediatric Orthopedic Emergencies Robin Pearce MSN, RN-BC Trauma Performance Improvement Manager Henrico Doctors Hospital, Forest Disclosure I have no actual or potential conflict of interest in relation
Pediatric Orthopedic Emergencies Robin Pearce MSN, RN-BC Trauma Performance Improvement Manager Henrico Doctors Hospital, Forest Disclosure I have no actual or potential conflict of interest in relation
The thigh. Prof. Oluwadiya KS
 The thigh Prof. Oluwadiya KS www.oluwadiya.com The Thigh: Boundaries The thigh is the region of the lower limb that is approximately between the hip and knee joints Anteriorly, it is separated from the
The thigh Prof. Oluwadiya KS www.oluwadiya.com The Thigh: Boundaries The thigh is the region of the lower limb that is approximately between the hip and knee joints Anteriorly, it is separated from the
THE LOWER EXTREMITY EXAM FOR THE FAMILY PRACTITIONER
 THE LOWER EXTREMITY EXAM FOR THE FAMILY PRACTITIONER Melinda A. Scott, D.O. Orthopedic Associates of Dayton Board Certified in Primary Care Sports Medicine GOALS Identify landmarks necessary for exam of
THE LOWER EXTREMITY EXAM FOR THE FAMILY PRACTITIONER Melinda A. Scott, D.O. Orthopedic Associates of Dayton Board Certified in Primary Care Sports Medicine GOALS Identify landmarks necessary for exam of
Bone Injuries and Treatment. Fractures and Dislocations
 Bone Injuries and Treatment Fractures and Dislocations Bellwork Research the small bones in the foot and wrist. Draw them in your notes. State Standards 16) Understand principles of and successfully perform
Bone Injuries and Treatment Fractures and Dislocations Bellwork Research the small bones in the foot and wrist. Draw them in your notes. State Standards 16) Understand principles of and successfully perform
region of the upper limb between the shoulder and the elbow Superiorly communicates with the axilla.
 1 region of the upper limb between the shoulder and the elbow Superiorly communicates with the axilla. Inferiorly, a number of important structures pass between arm & forearm through cubital fossa. 2 medial
1 region of the upper limb between the shoulder and the elbow Superiorly communicates with the axilla. Inferiorly, a number of important structures pass between arm & forearm through cubital fossa. 2 medial
SMALL GROUP SESSION 16 January 8 th or 10 th. Shoulder pain case/ Touch workshop/ Upper and Lower Extremity Examination
 SMALL GROUP SESSION 16 January 8 th or 10 th Shoulder pain case/ Touch workshop/ Upper and Lower Extremity Examination Suggested Readings: Opatrny L. The Healing Touch. Ann Int Med 2002; 137:1003. http://www.annals.org/cgi/reprint/137/12/1003.pdf
SMALL GROUP SESSION 16 January 8 th or 10 th Shoulder pain case/ Touch workshop/ Upper and Lower Extremity Examination Suggested Readings: Opatrny L. The Healing Touch. Ann Int Med 2002; 137:1003. http://www.annals.org/cgi/reprint/137/12/1003.pdf
Mohammad Ashraf. Abdulrahman Al-Hanbali. Ahmad Salman. 1 P a g e
 - 7 Mohammad Ashraf Abdulrahman Al-Hanbali Ahmad Salman 1 P a g e Structures under the cover of Gluteus Maximus: 1-Bones: Ileum, Femur (Head, greater trochanter and gluteal tuberosity), Ischium (ischial
- 7 Mohammad Ashraf Abdulrahman Al-Hanbali Ahmad Salman 1 P a g e Structures under the cover of Gluteus Maximus: 1-Bones: Ileum, Femur (Head, greater trochanter and gluteal tuberosity), Ischium (ischial
Gluteal region DR. GITANJALI KHORWAL
 Gluteal region DR. GITANJALI KHORWAL Gluteal region The transitional area between the trunk and the lower extremity. The gluteal region includes the rounded, posterior buttocks and the laterally placed
Gluteal region DR. GITANJALI KHORWAL Gluteal region The transitional area between the trunk and the lower extremity. The gluteal region includes the rounded, posterior buttocks and the laterally placed
Muscle Testing of Knee Extensors. Yasser Moh. Aneis, PhD, MSc., PT. Lecturer of Physical Therapy Basic Sciences Department
 Muscle Testing of Knee Extensors Yasser Moh. Aneis, PhD, MSc., PT. Lecturer of Physical Therapy Basic Sciences Department Muscle Testing of Knee Extensors othe Primary muscle Quadriceps Femoris -Rectus
Muscle Testing of Knee Extensors Yasser Moh. Aneis, PhD, MSc., PT. Lecturer of Physical Therapy Basic Sciences Department Muscle Testing of Knee Extensors othe Primary muscle Quadriceps Femoris -Rectus
The Leg. Prof. Oluwadiya KS
 The Leg Prof. Oluwadiya KS www.oluwadiya.sitesled.com Compartments of the leg 4 Four Compartments: 1. Anterior compartment Deep fibular nerve Dorsiflexes the foot and toes 2. Lateral Compartment Superficial
The Leg Prof. Oluwadiya KS www.oluwadiya.sitesled.com Compartments of the leg 4 Four Compartments: 1. Anterior compartment Deep fibular nerve Dorsiflexes the foot and toes 2. Lateral Compartment Superficial
rotation of the hip Flexion of the knee Iliac fossa of iliac Lesser trochanter Femoral nerve Flexion of the thigh at the hip shaft of tibia
 Anatomy of the lower limb Anterior & medial compartments of the thigh Dr. Hayder The fascia lata encloses the entire thigh like a sleeve/stocking. Three intramuscular fascial septa (lateral, medial, and
Anatomy of the lower limb Anterior & medial compartments of the thigh Dr. Hayder The fascia lata encloses the entire thigh like a sleeve/stocking. Three intramuscular fascial septa (lateral, medial, and
Compartment Syndrome
 Compartment Syndrome Chapter 34 Compartment Syndrome Introduction Compartment syndrome may occur with an injury to any fascial compartment. The fascial defect caused by the injury may not be adequate to
Compartment Syndrome Chapter 34 Compartment Syndrome Introduction Compartment syndrome may occur with an injury to any fascial compartment. The fascial defect caused by the injury may not be adequate to
Upper Extremity Injury Management. Jonathan Pirie MD, Med, FRCPC, FAAP
 Upper Extremity Injury Management Jonathan Pirie MD, Med, FRCPC, FAAP Learning Objectives At the end of this session, you will be able to manage common fractures of the: 1. Humerus 2. Elbow 3. Forearm
Upper Extremity Injury Management Jonathan Pirie MD, Med, FRCPC, FAAP Learning Objectives At the end of this session, you will be able to manage common fractures of the: 1. Humerus 2. Elbow 3. Forearm
1. A worker falls from a height and lands on his feet. Radiographs reveal a fracture of the sustentaculum tali. The muscle passing immediately
 1. A worker falls from a height and lands on his feet. Radiographs reveal a fracture of the sustentaculum tali. The muscle passing immediately beneath it that would be adversely affected is the: fibularis
1. A worker falls from a height and lands on his feet. Radiographs reveal a fracture of the sustentaculum tali. The muscle passing immediately beneath it that would be adversely affected is the: fibularis
Gross Anatomy Coloring Book Series. Lower Extremity Arteries
 Gross Anatomy Coloring Book Series Lower Extremity Arteries 1 Femoral Artery and Associated Branches For the life of the flesh is in the blood. Leviticus 17:11 Femoral Artery and Associated Branches After
Gross Anatomy Coloring Book Series Lower Extremity Arteries 1 Femoral Artery and Associated Branches For the life of the flesh is in the blood. Leviticus 17:11 Femoral Artery and Associated Branches After
4/28/2010. Fractures. Normal Bone and Normal Ossification Bone Terms. Epiphysis Epiphyseal Plate (physis) Metaphysis
 Metaphysis") Fractures Normal Bone and Normal Ossification Bone Terms Epiphysis Epiphyseal Plate (physis) Metaphysis Diaphysis 1 Fracture Classifications A. Longitudinal B. Transverse C. Oblique D. Spiral E. Incomplete
Fractures Normal Bone and Normal Ossification Bone Terms Epiphysis Epiphyseal Plate (physis) Metaphysis Diaphysis 1 Fracture Classifications A. Longitudinal B. Transverse C. Oblique D. Spiral E. Incomplete
Therapeutic Foot Care Certificate Program Part I: Online Home Study Program
 Therapeutic Foot Care Certificate Program Part I: Online Home Study Program 1 Anatomy And Terminology Of The Lower Extremity Joan E. Edelstein, MA, PT, FISPO Associate Professor of Clinical Physical Therapy
Therapeutic Foot Care Certificate Program Part I: Online Home Study Program 1 Anatomy And Terminology Of The Lower Extremity Joan E. Edelstein, MA, PT, FISPO Associate Professor of Clinical Physical Therapy
Musculoskeletal Examination
 Musculoskeletal Examination Statement of Goals Know how to perform a complete musculoskeletal examination. Learning Objectives A. Describe the anatomy of the musculoskeletal system including the bony structures,
Musculoskeletal Examination Statement of Goals Know how to perform a complete musculoskeletal examination. Learning Objectives A. Describe the anatomy of the musculoskeletal system including the bony structures,
5.1 Identify, describe the attachments of and deduce the actions of the muscles of the thigh:
 5.1 Identify, describe the attachments of and deduce the actions of the muscles of the thigh: Anterior group Proximal attachment Distal attachment Sartorius ASIS» Upper part of shaft tibia (middle surface)»
5.1 Identify, describe the attachments of and deduce the actions of the muscles of the thigh: Anterior group Proximal attachment Distal attachment Sartorius ASIS» Upper part of shaft tibia (middle surface)»
Chapter 30 - Musculoskeletal_Trauma
 Introduction to Emergency Medical Care 1 OBJECTIVES 30.1 Define key terms introduced in this chapter. Slides 11 12, 19 20, 22 23, 37 30.2 Describe the anatomy of elements of the musculoskeletal system.
Introduction to Emergency Medical Care 1 OBJECTIVES 30.1 Define key terms introduced in this chapter. Slides 11 12, 19 20, 22 23, 37 30.2 Describe the anatomy of elements of the musculoskeletal system.
Human Anatomy and Physiology I Laboratory Spinal and Peripheral Nerves and Reflexes
 Human Anatomy and Physiology I Laboratory Spinal and Peripheral Nerves and Reflexes 1 This lab involves the second section of the exercise Spinal Cord, Spinal Nerves, and the Autonomic Nervous System,
Human Anatomy and Physiology I Laboratory Spinal and Peripheral Nerves and Reflexes 1 This lab involves the second section of the exercise Spinal Cord, Spinal Nerves, and the Autonomic Nervous System,
Slides of Anatomy. Spring Dr. Maher Hadidi, University of Jordan
 Slides of Anatomy Please note : These slides are Dr. Maher Hadidi s slides of spring 2016 and were edited by the Premed Academic Team to fit the slides of spring 2019. Spring 2019 Dr. Maher Hadidi, University
Slides of Anatomy Please note : These slides are Dr. Maher Hadidi s slides of spring 2016 and were edited by the Premed Academic Team to fit the slides of spring 2019. Spring 2019 Dr. Maher Hadidi, University
Anatomy MCQs Week 13
 Anatomy MCQs Week 13 1. Posterior to the medial malleolus of the ankle: The neurovascular bundle lies between Tibialis Posterior and Flexor Digitorum Longus The tendon of Tibialis Posterior inserts into
Anatomy MCQs Week 13 1. Posterior to the medial malleolus of the ankle: The neurovascular bundle lies between Tibialis Posterior and Flexor Digitorum Longus The tendon of Tibialis Posterior inserts into
Human Anatomy Biology 255
 Human Anatomy Biology 255 Exam #4 Please place your name and I.D. number on the back of the last page of this exam. You must answer all questions on this exam. Because statistics demonstrate that, on average,
Human Anatomy Biology 255 Exam #4 Please place your name and I.D. number on the back of the last page of this exam. You must answer all questions on this exam. Because statistics demonstrate that, on average,
Lower Extremity Dislocations: Management and Triage on the Field
 Lower Extremity Dislocations: Management and Triage on the Field Scott J Tarantino, MD Towson Orthopaedic Associates, Towson, MD None Disclsures Purpose To provide you with knowledge which may guide you
Lower Extremity Dislocations: Management and Triage on the Field Scott J Tarantino, MD Towson Orthopaedic Associates, Towson, MD None Disclsures Purpose To provide you with knowledge which may guide you
Understanding Leg Anatomy and Function THE UPPER LEG
 Understanding Leg Anatomy and Function THE UPPER LEG The long thigh bone is the femur. It connects to the pelvis to form the hip joint and then extends down to meet the tibia (shin bone) at the knee joint.
Understanding Leg Anatomy and Function THE UPPER LEG The long thigh bone is the femur. It connects to the pelvis to form the hip joint and then extends down to meet the tibia (shin bone) at the knee joint.
ANATYOMY OF The thigh
 ANATYOMY OF The thigh 1- Lateral cutaneous nerve of the thigh Ι) Skin of the thigh Anterior view 2- Femoral branch of the genitofemoral nerve 1, 2 and 3 are From the lumber plexus 5- Intermediate cutaneous
ANATYOMY OF The thigh 1- Lateral cutaneous nerve of the thigh Ι) Skin of the thigh Anterior view 2- Femoral branch of the genitofemoral nerve 1, 2 and 3 are From the lumber plexus 5- Intermediate cutaneous
Running Injuries in Children and Adolescents
 Running Injuries in Children and Adolescents Cook Children s SPORTS Symposium July 2, 2014 Running Injuries Overuse injuries Acute injuries Anatomic conditions 1 Overuse Injuries Pain that cannot be tied
Running Injuries in Children and Adolescents Cook Children s SPORTS Symposium July 2, 2014 Running Injuries Overuse injuries Acute injuries Anatomic conditions 1 Overuse Injuries Pain that cannot be tied
HUMAN BODY COURSE LOWER LIMB NERVES AND VESSELS
 HUMAN BODY COURSE LOWER LIMB NERVES AND VESSELS October 22, 2010 D. LOWER LIMB MUSCLES 2. Lower limb compartments ANTERIOR THIGH COMPARTMENT General lfunction: Hip flexion, knee extension, other motions
HUMAN BODY COURSE LOWER LIMB NERVES AND VESSELS October 22, 2010 D. LOWER LIMB MUSCLES 2. Lower limb compartments ANTERIOR THIGH COMPARTMENT General lfunction: Hip flexion, knee extension, other motions
KNEE DISLOCATION. The most common injury will be an anterior dislocation, and this usually results from a hyperextension mechanism.
 KNEE DISLOCATION Introduction Dislocation of the knee is a severe injury associated with major soft tissue injury and a high incidence of damage to the popliteal artery. There is displacement of the tibia
KNEE DISLOCATION Introduction Dislocation of the knee is a severe injury associated with major soft tissue injury and a high incidence of damage to the popliteal artery. There is displacement of the tibia
A Patient s Guide to Elbow Anatomy
 A Patient s Guide to Elbow Anatomy Iain is a specialist in musculoskeletal imaging and the diagnosis of musculoskeletal pain. This information is provided with the hope that you can better understand and
A Patient s Guide to Elbow Anatomy Iain is a specialist in musculoskeletal imaging and the diagnosis of musculoskeletal pain. This information is provided with the hope that you can better understand and
ANATYOMY OF The thigh
 ANATYOMY OF The thigh 1- Lateral cutaneous nerve of the thigh Ι) Skin of the thigh Anterior view 2- Femoral branch of the genitofemoral nerve 5- Intermediate cutaneous nerve of the thigh 1, 2 and 3 are
ANATYOMY OF The thigh 1- Lateral cutaneous nerve of the thigh Ι) Skin of the thigh Anterior view 2- Femoral branch of the genitofemoral nerve 5- Intermediate cutaneous nerve of the thigh 1, 2 and 3 are
FUNCTIONAL ANATOMY AND EXAM OF THE HIP, GROIN AND THIGH
 FUNCTIONAL ANATOMY AND EXAM OF THE HIP, GROIN AND THIGH Peter G Gerbino, MD, FACSM Orthopedic Surgeon Monterey Joint Replacement and Sports Medicine Monterey, CA TPC, San Diego, 2017 The lecturer has no
FUNCTIONAL ANATOMY AND EXAM OF THE HIP, GROIN AND THIGH Peter G Gerbino, MD, FACSM Orthopedic Surgeon Monterey Joint Replacement and Sports Medicine Monterey, CA TPC, San Diego, 2017 The lecturer has no
Elbow. Chapter 2 LISTEN. Mechanism of Injury (If Applicable) Pain
 Pain") Chapter 2 Elbow LISTEN Mechanism of Injury (If Applicable) Patient usually remembers their position at the time of injury Certain mechanisms of injury result in characteristic patterns Fall on outstretched
Chapter 2 Elbow LISTEN Mechanism of Injury (If Applicable) Patient usually remembers their position at the time of injury Certain mechanisms of injury result in characteristic patterns Fall on outstretched
General Concepts. Growth Around the Knee. Topics. Evaluation
 General Concepts Knee Injuries in Skeletally Immature Athletes Zachary Stinson, M.D. Increased rate and ability of healing Higher strength of ligaments compared to growth plates Continued growth Children
General Concepts Knee Injuries in Skeletally Immature Athletes Zachary Stinson, M.D. Increased rate and ability of healing Higher strength of ligaments compared to growth plates Continued growth Children
Elbow Anatomy, Growth and Physical Exam. Donna M. Pacicca, MD Section of Sports Medicine Division of Orthopaedic Surgery Children s Mercy Hospital
 Elbow Anatomy, Growth and Physical Exam Donna M. Pacicca, MD Section of Sports Medicine Division of Orthopaedic Surgery Children s Mercy Hospital Contributing Factors to Elbow Injury The elbow is affected
Elbow Anatomy, Growth and Physical Exam Donna M. Pacicca, MD Section of Sports Medicine Division of Orthopaedic Surgery Children s Mercy Hospital Contributing Factors to Elbow Injury The elbow is affected
A Patient s Guide to Nursemaid's Elbow in Children. PHYSIO.coza
 A Patient s Guide to Nursemaid's Elbow in Children SANDTON MEDICLINIC 011 706 7495 FAIRWAYS LIFE HOSPITAL 011 875 1827 ST STITHIANS 082 378 9642 JEPPE BOYS HIGH SCHOOL 084 816 5457 JOHANNESBURG, SANDTON@PHYSIO.CO.ZA
A Patient s Guide to Nursemaid's Elbow in Children SANDTON MEDICLINIC 011 706 7495 FAIRWAYS LIFE HOSPITAL 011 875 1827 ST STITHIANS 082 378 9642 JEPPE BOYS HIGH SCHOOL 084 816 5457 JOHANNESBURG, SANDTON@PHYSIO.CO.ZA
Nursing Management: Musculoskeletal Trauma and Orthopedic Surgery. By: Aun Lauriz E. Macuja SAC_SN4
 Nursing Management: Musculoskeletal Trauma and Orthopedic Surgery By: Aun Lauriz E. Macuja SAC_SN4 The most common cause of musculoskeletal injuries is a traumatic event resulting in fracture, dislocation,
Nursing Management: Musculoskeletal Trauma and Orthopedic Surgery By: Aun Lauriz E. Macuja SAC_SN4 The most common cause of musculoskeletal injuries is a traumatic event resulting in fracture, dislocation,
Phase II Health Sciences as Applied to Coaching.
 Phase II Health Sciences as Applied to Coaching www.topform.us Overview What is going to be covered today is.. Skeletal System Muscular System Most common injuries to know about in your sport Part One:
Phase II Health Sciences as Applied to Coaching www.topform.us Overview What is going to be covered today is.. Skeletal System Muscular System Most common injuries to know about in your sport Part One:
lower limb Anterior Compartment: lecture 3 The deep fascia ( fascia lata) divides the thigh into 3 compartments:
 divides the thigh into 3 compartments:") lower limb lecture 3 The deep fascia ( fascia lata) divides the thigh into 3 compartments: 1. Anterior Extensor compartment 2. Medial Adductor compartment 3. Posterior Flexor compartment Anterior Compartment:
lower limb lecture 3 The deep fascia ( fascia lata) divides the thigh into 3 compartments: 1. Anterior Extensor compartment 2. Medial Adductor compartment 3. Posterior Flexor compartment Anterior Compartment:
Anterior and Medial compartments of the thigh. Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology
 Anterior and Medial compartments of the thigh Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Terms Related to Movements Movement Flexion Extension Abduction Adduction Medial (internal)
Anterior and Medial compartments of the thigh Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Terms Related to Movements Movement Flexion Extension Abduction Adduction Medial (internal)
Muscles of the Hip 1. Tensor Fasciae Latae O: iliac crest I: lateral femoral condyle Action: abducts the thigh Nerve: gluteal nerve
 Muscles of the Hip 1. Tensor Fasciae Latae O: iliac crest I: lateral femoral condyle Action: abducts the thigh Nerve: gluteal nerve 2. Gluteus Maximus O: ilium I: femur Action: abduct the thigh Nerve:
Muscles of the Hip 1. Tensor Fasciae Latae O: iliac crest I: lateral femoral condyle Action: abducts the thigh Nerve: gluteal nerve 2. Gluteus Maximus O: ilium I: femur Action: abduct the thigh Nerve:
MUSCULOSKELETAL LOWER LIMB
 MUSCULOSKELETAL LOWER LIMB Spinal Cord Lumbar and Sacral Regions Spinal cord Dorsal root ganglion Conus medullaris Cauda equina Dorsal root ganglion of the fifth lumbar nerve End of subarachnoid space
MUSCULOSKELETAL LOWER LIMB Spinal Cord Lumbar and Sacral Regions Spinal cord Dorsal root ganglion Conus medullaris Cauda equina Dorsal root ganglion of the fifth lumbar nerve End of subarachnoid space
Artery 1 Head and Thoracic Arteries. Arrange the parts in the order blood flows through them.
 Artery 1 Head and Thoracic Arteries 1. Given the following parts of the aorta: 1. abdominal aorta 2. aortic arch 3. ascending aorta 4. thoracic aorta Arrange the parts in the order blood flows through
Artery 1 Head and Thoracic Arteries 1. Given the following parts of the aorta: 1. abdominal aorta 2. aortic arch 3. ascending aorta 4. thoracic aorta Arrange the parts in the order blood flows through
Basic Care of Common Fractures Utku Kandemir, MD
 Basic Care of Common Fractures Utku Kandemir, MD Assistant Clinical Professor Trauma & Sports Medicine Dept. of Orthopaedic Surgery UCSF / SFGH History Physical Exam Radiology Treatment History Acute trauma
Basic Care of Common Fractures Utku Kandemir, MD Assistant Clinical Professor Trauma & Sports Medicine Dept. of Orthopaedic Surgery UCSF / SFGH History Physical Exam Radiology Treatment History Acute trauma
RN(EC) ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT ***
 ENC(C) GNC(C) MN ACNP *** MECHANISM OF INJURY.. MOST IMPORTANT ***") HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age of patient - Certain conditions are more prevalent in particular age groups (Hip pain in children may refer to the knee from Legg-Calve-Perthes
HISTORY *** MECHANISM OF INJURY.. MOST IMPORTANT *** Age of patient - Certain conditions are more prevalent in particular age groups (Hip pain in children may refer to the knee from Legg-Calve-Perthes
Disclosure. Learning ObjecAves. A Quick Review. Pediatric Fractures. The Developing Bone
 How to Bend but not Break Managing Pediatric Orthopedic Injuries in the Emergency Department Disclosure Nothing to disclosure No conflict of interest related to this topic Adam Cheng, MD, FRCPC Division
How to Bend but not Break Managing Pediatric Orthopedic Injuries in the Emergency Department Disclosure Nothing to disclosure No conflict of interest related to this topic Adam Cheng, MD, FRCPC Division
Caring for Muscle and Bone Injuries From Brady s First Responder (8 th Edition) 54 Questions
 54 Questions") Caring for Muscle and Bone Injuries From Brady s First Responder (8 th Edition) 54 Questions 1. What is caused by overexerting or tearing of a muscle? p. 375 A.) Dislocation B.) Sprain C.) Fracture *D.)
Caring for Muscle and Bone Injuries From Brady s First Responder (8 th Edition) 54 Questions 1. What is caused by overexerting or tearing of a muscle? p. 375 A.) Dislocation B.) Sprain C.) Fracture *D.)
Functional anatomy and variability of the blood vessels of the upper and lower limbs. Anastasia Bendelic Human Anatomy Departament
 Functional anatomy and variability of the blood vessels of the upper and lower limbs Anastasia Bendelic Human Anatomy Departament Plan: 1. Variations of the branching pattern of the aortic arch 2. Arterial
Functional anatomy and variability of the blood vessels of the upper and lower limbs Anastasia Bendelic Human Anatomy Departament Plan: 1. Variations of the branching pattern of the aortic arch 2. Arterial
Lecture 08 THIGH MUSCLES ANTERIOR COMPARTMENT. Dr Farooq Khan Aurakzai. Dated:
 Lecture 08 THIGH MUSCLES ANTERIOR COMPARTMENT BY Dr Farooq Khan Aurakzai Dated: 11.02.2017 INTRODUCTION to the thigh Muscles. The musculature of the thigh can be split into three sections by intermuscular
Lecture 08 THIGH MUSCLES ANTERIOR COMPARTMENT BY Dr Farooq Khan Aurakzai Dated: 11.02.2017 INTRODUCTION to the thigh Muscles. The musculature of the thigh can be split into three sections by intermuscular
Balanced Body Movement Principles
 Balanced Body Movement Principles How the Body Works and How to Train it. Module 3: Lower Body Strength and Power Developing Strength, Endurance and Power The lower body is our primary source of strength,
Balanced Body Movement Principles How the Body Works and How to Train it. Module 3: Lower Body Strength and Power Developing Strength, Endurance and Power The lower body is our primary source of strength,
Lecture 10 Arteries and veins of the upper limb
 Lecture 10 Arteries and veins of the upper limb 1. Identify the Subclavian, axillary, brachial (deep and superficial), radial and ulnar arteries and superficial/deep palmar arches 2. Describe the major
Lecture 10 Arteries and veins of the upper limb 1. Identify the Subclavian, axillary, brachial (deep and superficial), radial and ulnar arteries and superficial/deep palmar arches 2. Describe the major
The Muscular System. Chapter 10 Part D. PowerPoint Lecture Slides prepared by Karen Dunbar Kareiva Ivy Tech Community College
 Chapter 10 Part D The Muscular System Annie Leibovitz/Contact Press Images PowerPoint Lecture Slides prepared by Karen Dunbar Kareiva Ivy Tech Community College Table 10.14: Muscles Crossing the Hip and
Chapter 10 Part D The Muscular System Annie Leibovitz/Contact Press Images PowerPoint Lecture Slides prepared by Karen Dunbar Kareiva Ivy Tech Community College Table 10.14: Muscles Crossing the Hip and