HFOV IN THE NON-RECRUITABLE LUNG
|
|
|
- Rodney Short
- 5 years ago
- Views:
Transcription
1 HFOV IN THE NON-RECRUITABLE LUNG HFOV IN THE NON-RECRUITABLE LUNG PPHN Pulmonary hypoplasia after PPROM Congenital diaphragmatic hernia Pulmonary interstitial emphysema / cystic lung disease 1
2 30 Mean airway pressure (cm H 2 O) Bay 1 PPHN 0 APPROACH TO TREATMENT OF PPHN Confirmation of the diagnosis (clinical + ECHO) Treatment for the underlying lung disease Ventilatory support ± Exogenous surfactant ± Antibiotics Circulatory support Adjunctive treatment for PPHN Definitive treatment for PPHN 2
3 Circulatory support and adjunctive therapy in PPHN Circulatory support Increasing systemic BP may reduce R L shunt through the ductus arteriosus Possible agents: dobutamine ± noradrenaline or? milrinone Avoid agents that reduce systemic blood pressure (e.g. tolazoline) Do not volume overload Adjunctive therapy Heavy sedation and muscle relaxation until stable Correction of: Hypoglycaemia Hypocalcaemia Hypomagnesemia Polycythaemia or anaemia Fluid bolus increased systemic blood pressure decreased R to L ductal shunt 30 Mean airway pressure (cm H 2 O)
4 Ventilatory support in PPHN Most infants with significant PPHN benefit from intubation and ventilation Should apply ventilation so as to: Achieve normocapnia and ph Optimise lung volume and avoid ventilator-induced lung injury FRC (end-expiratory lung volume) is an important determinant of pulmonary blood flow For parenchymal disease + PPHN, high frequency ventilation is recommended, as FRC may remain poor on conventional ventilation For pulmonary hypoplasia + PPHN, high frequency ventilation is recommended, as overdistension and/or ventilator-induced lung injury worsen PPHN For idiopathic PPHN, conventional ventilation is preferred Ventilatory support in PPHN Relationship between lung volume and PVR Simmons Circ Res
5 Ventilatory support in PPHN Relationship between lung volume and PVR Simmons Circ Res 1961 Recruitment manoeuvre to 28 cm H 2 O higher PVR oxygenation worse 30 Mean airway pressure (cm H 2 O)

6 Mean airway pressure (cm H 2 O) Post-recruitment oxygenation better at same P AW pre-post ductal difference less 0 HFOV and ino in PPHN Kinsella et al J Pediatr

7 HFOV and ino in hypoxic respiratory failure in PICU Dobyns et al Crit Care Med 2002 Bay 2 Pulmonary hypoplasia 7
8 Preterm infants with extreme PPROM RWH Melbourne Membrane rupture <24 weeks Minimal latent period 14 days Everest et al ADCF&N 2007 Preterm infants with extreme PPROM RHH Hobart Membrane rupture <25 weeks Minimal latent period 14 days Gestation at birth 24 weeks If needing intubation: Conventionally ventilated (Babylog or Neopuff) Surfactant given Early transition to HFOV (Sensormedics) if: Remaining in FiO 2 > 0.4 Respiratory acidosis, ph < 7.25 ino only used for refractory hypoxia Aiyappan et al PSANZ abstract, JCPH
9 Preterm infants with extreme PPROM RHH Hobart infants born alive 4 infants on CPAP from the outset (2 intubated beyond 1 st week) 16 infants intubated on day 1 9 stabilised on CMV 7 infants had refractory hypoxic respiratory failure on CMV and had early transition to HFOV (mean age 2 hrs) Aiyappan et al PSANZ abstract, JCPH 2010 Extreme PPROM RHH Hobart Infants with refractory hypoxia on CMV (n=7) P AW FiO 2 P AW (cm H 2 O) FiO Pre HFOV 6 hrs post-hfov Pre HFOV 6 hrs post-hfov ph pco 2 ph Pre HFOV 6 hrs post-hfov Pre HFOV 6 hrs post-hfov PCO 2 (mm Hg) 9
 frequency 10-12 Hz wait for an effect gentle stepwise recruitment only if oxygenation")
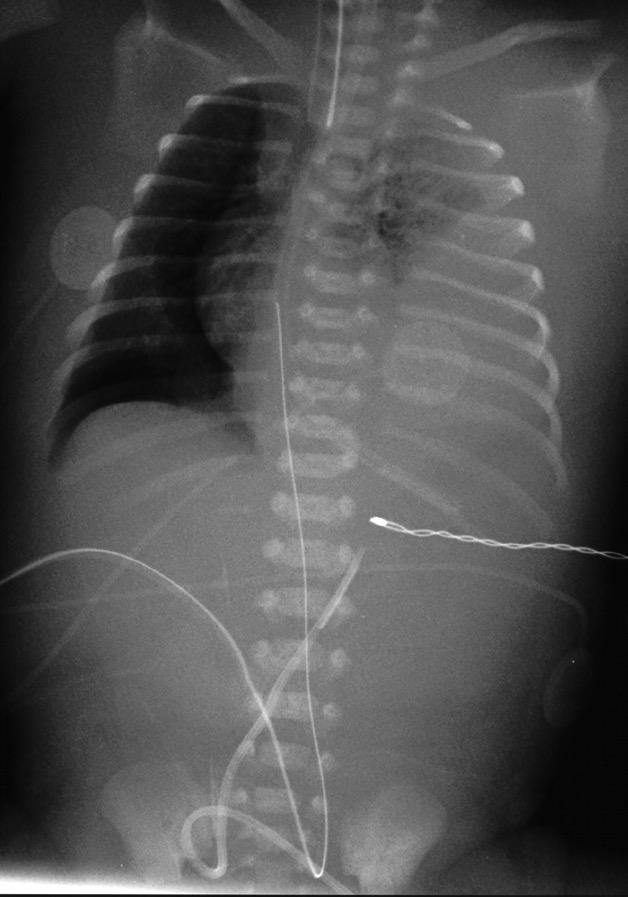
10 HFOV in pulmonary hypoplasia Pulmonary hypoplasia Small but often biochemically mature lung Structurally immaturity, high susceptibility to barotrauma High pulmonary vascular resistance APPROACH: Early transition to HFOV if failing on CMV Low pressure strategy initial P AW cm H 2 O ( P AW on CMV) frequency Hz wait for an effect gentle stepwise recruitment only if oxygenation remains poor and lung parenchyma is opacified Initially allow minimal or no spontaneous respiration sedation and muscle relaxation Treat co-existing PPHN with ino if failing to oxygenate after time on HFOV Pulmonary hypoplasia with L lung opacification 10

11 Pulmonary hypoplasia with overdistension Extreme PPROM RHH Hobart Infants with refractory hypoxia on CMV (n=7) P AW FiO 2 P AW (cm H 2 O) FiO Pre HFOV 6 hrs post-hfov Pre HFOV 6 hrs post-hfov ph pco 2 ph Pre HFOV 6 hrs post-hfov Pre HFOV 6 hrs post-hfov PCO 2 (mm Hg) 11
12 Extreme PPROM RHH Hobart Infants with refractory hypoxia on CMV (n=7) P AW FiO 2 P AW (cm H 2 O) FiO Pre HFOV 6 hrs post-hfov Pre HFOV 6 hrs post-hfov ph pco 2 ph Pre HFOV 6 hrs post-hfov Pre HFOV 6 hrs post-hfov PCO 2 (mm Hg) Preterm infants with extreme PPROM RHH Hobart infants born alive (24-31 weeks) Early HFOV in 7/20 (35%) None died on day 1 All survived to discharge One death post-discharge (PVL) Aiyappan et al PSANZ abstract, JCPH

13 Preterm infants with extreme PPROM Royal North Shore Membrane rupture 24 weeks Minimal latent period 14 days Shah & Kluckow JCPH 2011 Bay 3 L CDH 13
14 HFOV in CDH for many, the management of the newborn with CDH is more emotional than scientific. Glick, Irish & Holm Clin Perinatol 1996 HFOV in CDH unlike the other neonatal pulmonary diseases, CDH does not represent a recruitable lung and attempts to use a high mean airway pressure are likely to cause pulmonary damage. Bohn AJRCCM


15 The CDH lung Kotecha et al Eur Respir J 2012 The CDH lung vasculature Levin J Pediatr


16 HFOV in CDH The evidence HFOV in CDH 16


17 HFOV in CDH HFOV in CDH Bohn AJRCCM
18 Ventilation in CDH Tracy et al J Pediatr Surg 2010 HFOV in CDH Management practices Routine CS delivery? Intubation at delivery? NG tube at delivery? Acceptable gas exchange Pre-ductal SpO2 Post-ductal SpO2 ph Bohn 2001 NS Yes Yes >85% 70% 7.3 ERS Taskforce 2012 No Yes Yes >85% NS 7.2 Euro Consortium 2010 No Yes Yes >85% 70% 7.2 Tracy 2010 No Yes Yes >85% 7.25 Migliazza 2007 Yes Yes Yes >85% NS NS RWH-RCH No Yes Yes >85% (70%) 7.2 NA: not applicable, NS: not stated 18
19 HFOV in CDH Management practices Acceptable gas exchange Routine CS Intubation at NG tube at CMV delivery? settings delivery? HFOV delivery? settings Pre-ductal Muscle SpO2 Post-ductal SpO2 ph Max ino use ECMO use Max PIP PEEP range deltap I:E freq relaxants Bohn 2001 NS Yes Paw Yes >85% 70% 7.3 Bohn cm H2O NS NS NS Not routine Restricted Restricted (6%) ERS Taskforce 2012 No Yes Yes >85% NS 7.2 ERS Taskforce cm H2O <5 cm H2O 17 NS NS NS Not routine NS NS Euro Consortium 2010 No Yes Yes >85% 70% 7.2 Euro Consortium cm H2O 2-5 cm H2O :1* 10 Hz Not routine Liberal Liberal (25-30%) Tracy 2010 No Yes Yes >85% 7.25 Tracy cm H2O NS 22+ NS NS NS Not routine Liberal (40%) Liberal (23%) Migliazza Migliazza NA YesNA Yes NA Yes 1:2* 10 Hz >85% Routine Liberal NS (30%) Restricted NS (<5%) RWH-RCH RWH-RCH 25 cm H2O 3-5 Nocm H2O Yes Yes 1:2 10 Hz >85% Liberal Liberal (70%) (60%) Restricted 7.2 (<5%) NA: not applicable, NS: not stated; *Sensormedics oscillator; 1:2 with Sensormedics, other oscillators and HFJV also used HFOV in CDH The VICI trial HFOV (n=80) compared with CMV (n=91) Prenatally diagnosed CDH Mx according to Euro Consortium protocol Of 80 managed on HFOV initially, 48 crossed over to CMV or ECMO On intention-to-treat analysis: No difference in survival free of oxygen at 28 days Less treatment failures in CMV group Shorter duration of ventilation in CMV group Snoek et al EAPS abstract





20 L CDH immediately post-op L CDH day 1 post-op L CDH day 2 post-op L CDH day 3 post-op L CDH day 4 post-op L CDH showing early overdistention and cystic change 20

21 L CDH gross overinflation of the L lung HFOV in CDH Migliazza J Pediatr Surg
22 Therapies for CDH at RCH Melbourne TIME EPOCH ECMO HFO/JV ino PGE May May 2003-end % 0% 0% 0% 9% 13% 0% 0% 11% 52% 48% 0% 7% 46% 36% 0% 3% 73% 72% 68% 5% 83% 60% 70% RCH CDH Survival N=124 liveborn infants Antenatal diagnosis 65% Left 80% Rt 20% Survival (all) 76% Survival (excluding major anomalies) 78% Slide courtesy of Dr. Michael Stewart 22


23 29 weeks, day 11, on nasal CPAP resp acidosis and increasing FiO 2 Bay 4 Cystic lung disease / PIE Jet ventilation experience at RCH 28/40, day 25, pre- jet ventilation, FiO hours after HFJV, FiO

24 Preterm infants with cystic PIE RHH Hobart Median (IQR) or n (%) Squires et al Neonatology 2013 HFOV in cystic lung disease / PIE PLAN: Use the oscillator in a manner that allows the cysts to empty more effectively with each oscillatory cycle Ultimate aim is to encourage gas to resorb from the interstitium, and airspaces to then re-expand APPROACH: Use an oscillator with active expiration 24
25 Comparison of pressure waveforms between oscillators Harcourt et al Pediatr Crit Care Med 2014 HFOV in cystic lung disease / PIE PLAN: Use the oscillator in a manner that allows the cysts to empty more effectively with each oscillatory cycle Ultimate aim is to encourage gas to resorb from the interstitium, and airspaces to then re-expand APPROACH: Use an oscillator with active expiration Low pressure strategy P AW cm H 2 O the lowest possible P AW whilst maintaining oxygenation no recruitment manoeuvres accept high FiO 2 Frequency 5 Hz = low frequency high frequency ventilation beware hypocarbia Initially allow no spontaneous respiration sedation and muscle relaxation allow spontaneous breathing once PIE improved (usually only 2-3 days) Positioning good lung uppermost 25





26 Unilateral cystic lung disease Before low pressure, low frequency HFOV 24 hrs P AW 11, freq 5 Hz FiO hrs P AW 7, freq 5 Hz FiO Unilateral cystic lung disease 84 hrs P AW 7, freq 5 Hz FiO hrs P AW 7, freq 12 FiO



27 Bilateral cystic lung disease 24 weeks, day 15 transferred to HFOV day 18, P AW 12, freq 5 Hz FiO day 21, P AW 10, freq 5 Hz FiO Bilateral cystic lung disease Squires et al Neonatology

28 Preterm infants with cystic PIE RHH Hobart Squires et al Neonatology 2013 HFOV IN THE NON-RECRUITABLE LUNG Summary Use (or avoidance) of recruitment manoeuvres should take into account: degree of parenchymal disease susceptibility of the lung to barotrauma state of the pulmonary vasculature A low pressure strategy with time dependent recruitment can be very effective if aggressive recruitment is contraindicated Low frequency HFOV (freq = 5) can help to decompress overdistended lung regions 28
USE OF INHALED NITRIC OXIDE IN THE NICU East Bay Newborn Specialists Guideline Prepared by P Joe, G Dudell, A D Harlingue Revised 7/9/2014
 USE OF INHALED NITRIC OXIDE IN THE NICU East Bay Newborn Specialists Guideline Prepared by P Joe, G Dudell, A D Harlingue Revised 7/9/2014 ino for Late Preterm and Term Infants with Severe PPHN Background:
USE OF INHALED NITRIC OXIDE IN THE NICU East Bay Newborn Specialists Guideline Prepared by P Joe, G Dudell, A D Harlingue Revised 7/9/2014 ino for Late Preterm and Term Infants with Severe PPHN Background:
Management of Respiratory Disease in the Term Infant
 Management of Respiratory Disease in the Term Infant David Tingay 1. Neonatal Research, Murdoch Children s Research Institute, Melbourne 2. Neonatology, Royal Children s Hospital 3. Dept of Paediatrics,
Management of Respiratory Disease in the Term Infant David Tingay 1. Neonatal Research, Murdoch Children s Research Institute, Melbourne 2. Neonatology, Royal Children s Hospital 3. Dept of Paediatrics,
Three Decades of Managing Congenital Diaphragmatic Hernia
 Three Decades of Managing Congenital Diaphragmatic Hernia Desmond Bohn The Department of Critical Care Medicine The Hospital for Sick Children, Toronto Robert E Gross Congenital Diaphragmatic Hernia 1960-80
Three Decades of Managing Congenital Diaphragmatic Hernia Desmond Bohn The Department of Critical Care Medicine The Hospital for Sick Children, Toronto Robert E Gross Congenital Diaphragmatic Hernia 1960-80
CPAP failure in preterm infants: incidence, predictors and consequences
 CPAP failure in preterm infants: incidence, predictors and consequences SUPPLEMENTAL TEXT METHODS Study setting The Royal Hobart Hospital has an 11-bed combined Neonatal and Paediatric Intensive Care Unit
CPAP failure in preterm infants: incidence, predictors and consequences SUPPLEMENTAL TEXT METHODS Study setting The Royal Hobart Hospital has an 11-bed combined Neonatal and Paediatric Intensive Care Unit
PPHN (see also ECMO guideline)
") Children s Acute Transport Service Clinical Guidelines PPHN (see also ECMO guideline) Document Control Information Author P Brooke E.Randle Author Position Medical Student Consultant Document Owner E.
Children s Acute Transport Service Clinical Guidelines PPHN (see also ECMO guideline) Document Control Information Author P Brooke E.Randle Author Position Medical Student Consultant Document Owner E.
The Blue Baby. Network Stabilisation of the Term Infant Study Day 15 th March 2017 Joanna Behrsin
 The Blue Baby Network Stabilisation of the Term Infant Study Day 15 th March 2017 Joanna Behrsin Session Structure Definitions and assessment of cyanosis Causes of blue baby Structured approach to assessing
The Blue Baby Network Stabilisation of the Term Infant Study Day 15 th March 2017 Joanna Behrsin Session Structure Definitions and assessment of cyanosis Causes of blue baby Structured approach to assessing
Cardiorespiratory Interactions:
 Cardiorespiratory Interactions: The Heart - Lung Connection Jon N. Meliones, MD, MS, FCCM Professor of Pediatrics Duke University Medical Director PCVICU Optimizing CRI Cardiorespiratory Economics O2:
Cardiorespiratory Interactions: The Heart - Lung Connection Jon N. Meliones, MD, MS, FCCM Professor of Pediatrics Duke University Medical Director PCVICU Optimizing CRI Cardiorespiratory Economics O2:
6/25/2013. Pulmonary Hypoplasia in Congenital Defects. Joshua E. Petrikin, MD Assistant Professor Pediatrics June 28 th, 2013
 Pulmonary Hypoplasia in Congenital Defects Joshua E. Petrikin, MD Assistant Professor Pediatrics June 28 th, 2013 I have no financial conflicts of interest to disclose Case 1 39 wk infant with born via
Pulmonary Hypoplasia in Congenital Defects Joshua E. Petrikin, MD Assistant Professor Pediatrics June 28 th, 2013 I have no financial conflicts of interest to disclose Case 1 39 wk infant with born via
Provide guidelines for the management of mechanical ventilation in infants <34 weeks gestation.
 Page 1 of 5 PURPOSE: Provide guidelines for the management of mechanical ventilation in infants
Page 1 of 5 PURPOSE: Provide guidelines for the management of mechanical ventilation in infants
Extracorporeal Membrane Oxygenation (ECMO) Referrals
 Referrals") Children s Acute Transport Service Clinical Guideline Extracorporeal Membrane Oxygenation (ECMO) Referrals Document Control Information Author ECMO/CATS Author Position Service Coordinator Document Owner
Children s Acute Transport Service Clinical Guideline Extracorporeal Membrane Oxygenation (ECMO) Referrals Document Control Information Author ECMO/CATS Author Position Service Coordinator Document Owner
HFOV Case Study 3.6kg MAS Instructor Copy
 HFOV Case Study 3.6kg MAS Instructor Copy Color key: Black Patient case Blue RN/RCP collaboration Red MD consult Green - Critical Thinking Inquiry Green italics CT answers ABG: ph/pco2/po2/base A 35 year-old
HFOV Case Study 3.6kg MAS Instructor Copy Color key: Black Patient case Blue RN/RCP collaboration Red MD consult Green - Critical Thinking Inquiry Green italics CT answers ABG: ph/pco2/po2/base A 35 year-old
Dr. AM MAALIM KPA 2018
 Dr. AM MAALIM KPA 2018 Journey Towards Lung protection Goals of lung protection Strategies Summary Conclusion Before 1960: Oxygen; impact assessed clinically. The 1960s:President JFK, Ventilators mortality;
Dr. AM MAALIM KPA 2018 Journey Towards Lung protection Goals of lung protection Strategies Summary Conclusion Before 1960: Oxygen; impact assessed clinically. The 1960s:President JFK, Ventilators mortality;
** SURFACTANT THERAPY**
 ** SURFACTANT THERAPY** Full Title of Guideline: Surfactant Therapy Author (include email and role): Stephen Wardle (V4) Reviewed by Dushyant Batra Consultant Neonatologist Division & Speciality: Division:
** SURFACTANT THERAPY** Full Title of Guideline: Surfactant Therapy Author (include email and role): Stephen Wardle (V4) Reviewed by Dushyant Batra Consultant Neonatologist Division & Speciality: Division:
SWISS SOCIETY OF NEONATOLOGY. Supercarbia in an infant with meconium aspiration syndrome
 SWISS SOCIETY OF NEONATOLOGY Supercarbia in an infant with meconium aspiration syndrome January 2006 2 Wilhelm C, Frey B, Department of Intensive Care and Neonatology, University Children s Hospital Zurich,
SWISS SOCIETY OF NEONATOLOGY Supercarbia in an infant with meconium aspiration syndrome January 2006 2 Wilhelm C, Frey B, Department of Intensive Care and Neonatology, University Children s Hospital Zurich,
Lung Wit and Wisdom. Understanding Oxygenation and Ventilation in the Neonate. Jennifer Habert, BHS-RT, RRT-NPS, C-NPT Willow Creek Women s Hospital
 Lung Wit and Wisdom Understanding Oxygenation and Ventilation in the Neonate Jennifer Habert, BHS-RT, RRT-NPS, C-NPT Willow Creek Women s Hospital Objectives To review acid base balance and ABG interpretation
Lung Wit and Wisdom Understanding Oxygenation and Ventilation in the Neonate Jennifer Habert, BHS-RT, RRT-NPS, C-NPT Willow Creek Women s Hospital Objectives To review acid base balance and ABG interpretation
Congenital diaphragmatic hernia: a systematic review and summary of best-evidence practice strategies
 STATE OF THE ART Congenital diaphragmatic hernia: a systematic review and summary of best-evidence practice strategies JW Logan 1, HE Rice 2, RN Goldberg 1 and CM Cotten 1 (2007) 27, 535 549 r 2007 Nature
STATE OF THE ART Congenital diaphragmatic hernia: a systematic review and summary of best-evidence practice strategies JW Logan 1, HE Rice 2, RN Goldberg 1 and CM Cotten 1 (2007) 27, 535 549 r 2007 Nature
1
 1 2 3 RIFAI 5 6 Dublin cohort, retrospective review. Milrinone was commenced at an initial dose of 0.50 μg/kg/minute up to 0.75 μg/kg/minute and was continued depending on clinical response. No loading
1 2 3 RIFAI 5 6 Dublin cohort, retrospective review. Milrinone was commenced at an initial dose of 0.50 μg/kg/minute up to 0.75 μg/kg/minute and was continued depending on clinical response. No loading
Hypoxic Respiratory Failure in the Newborn. Question and Answer
 Hypoxic Respiratory Failure in the Newborn Question and Answer Question: When administering nitric oxide to premature babies what is considered safe or common practice in terms of length of treatment?
Hypoxic Respiratory Failure in the Newborn Question and Answer Question: When administering nitric oxide to premature babies what is considered safe or common practice in terms of length of treatment?
Earlier Use of Inhaled Nitric Oxide in Term and Near-Term Neonates With Hypoxic Respiratory Failure (HRF) and Pulmonary Hypertension (PH)
 and Pulmonary Hypertension (PH)") Earlier Use of Inhaled Nitric Oxide in Term and Near-Term Neonates With Hypoxic Respiratory Failure (HRF) and Pulmonary Hypertension (PH) 2013 Ikaria, Inc. 1 Disclosure Information This program is sponsored
Earlier Use of Inhaled Nitric Oxide in Term and Near-Term Neonates With Hypoxic Respiratory Failure (HRF) and Pulmonary Hypertension (PH) 2013 Ikaria, Inc. 1 Disclosure Information This program is sponsored
Congenital Diaphragmatic Hernia Evidence Based Management
 Congenital Diaphragmatic Hernia Evidence Based Management Saima Aftab MD PSA Chief Neonatology Director Fetal Care Center NCH Director National Victor Center Affiliate Faculty Brigham and Women s Hospital
Congenital Diaphragmatic Hernia Evidence Based Management Saima Aftab MD PSA Chief Neonatology Director Fetal Care Center NCH Director National Victor Center Affiliate Faculty Brigham and Women s Hospital
Simulation 08: Cyanotic Preterm Infant in Respiratory Distress
 Flow Chart Simulation 08: Cyanotic Preterm Infant in Respiratory Distress Opening Scenario Section 1 Type: DM As staff therapist assigned to a Level 2 NICU in a 250 bed rural medical center you are called
Flow Chart Simulation 08: Cyanotic Preterm Infant in Respiratory Distress Opening Scenario Section 1 Type: DM As staff therapist assigned to a Level 2 NICU in a 250 bed rural medical center you are called
Hyaline membrane disease. By : Dr. Ch Sarishma Peadiatric Pg
 Hyaline membrane disease By : Dr. Ch Sarishma Peadiatric Pg Also called Respiratory distress syndrome. It occurs primarily in premature infants; its incidence is inversely related to gestational age and
Hyaline membrane disease By : Dr. Ch Sarishma Peadiatric Pg Also called Respiratory distress syndrome. It occurs primarily in premature infants; its incidence is inversely related to gestational age and
PERSISTENT PULMONARY HYPERTENSION OF THE NEWBORN East Bay Newborn Specialists Guideline Prepared by L Truong 12/15/2015
 PERSISTENT PULMONARY HYPERTENSION OF THE NEWBORN East Bay Newborn Specialists Guideline Prepared by L Truong 12/15/2015 Background: Persistent pulmonary hypertension of the newborn occurs in ~2 per 1,000
PERSISTENT PULMONARY HYPERTENSION OF THE NEWBORN East Bay Newborn Specialists Guideline Prepared by L Truong 12/15/2015 Background: Persistent pulmonary hypertension of the newborn occurs in ~2 per 1,000
Surfactant Administration
 Approved by: Surfactant Administration Gail Cameron Senior Director Operations, Maternal, Neonatal & Child Health Programs Dr. Paul Byrne Medical Director, Neonatology Neonatal Policy & Procedures Manual
Approved by: Surfactant Administration Gail Cameron Senior Director Operations, Maternal, Neonatal & Child Health Programs Dr. Paul Byrne Medical Director, Neonatology Neonatal Policy & Procedures Manual
Objectives. Apnea Definition and Pitfalls. Pathophysiology of Apnea. Apnea of Prematurity and hypoxemia episodes 5/18/2015
 Apnea of Prematurity and hypoxemia episodes Deepak Jain MD Care of Sick Newborn Conference May 2015 Objectives Differentiating between apnea and hypoxemia episodes. Pathophysiology Diagnosis of apnea and
Apnea of Prematurity and hypoxemia episodes Deepak Jain MD Care of Sick Newborn Conference May 2015 Objectives Differentiating between apnea and hypoxemia episodes. Pathophysiology Diagnosis of apnea and
Neonatal/Pediatric Cardiopulmonary Care. Persistent Pulmonary Hypertension of the Neonate (PPHN) PPHN. Other. Other Diseases
 PPHN. Other. Other Diseases") Neonatal/Pediatric Cardiopulmonary Care Other Diseases Persistent Pulmonary Hypertension of the Neonate (PPHN) PPHN 3 Also known as Persistent Fetal Circulation (PFC) Seen most frequently in term, post-term
Neonatal/Pediatric Cardiopulmonary Care Other Diseases Persistent Pulmonary Hypertension of the Neonate (PPHN) PPHN 3 Also known as Persistent Fetal Circulation (PFC) Seen most frequently in term, post-term
APPENDIX VI HFOV Quick Guide
 APPENDIX VI HFOV Quick Guide Overall goal: Maintain PH in the target range at the minimum tidal volume. This is achieved by favoring higher frequencies over lower P (amplitude). This goal is also promoted
APPENDIX VI HFOV Quick Guide Overall goal: Maintain PH in the target range at the minimum tidal volume. This is achieved by favoring higher frequencies over lower P (amplitude). This goal is also promoted
Scope: This guideline is aimed at all Health Care Professionals involved in the care of infants within the Neonatal Service.
 Persistent Pulmonary Hypertension of the Newborn (PPHN) University Hospitals of Leicester NHS NHS Trust June 2018 June 2021 Scope: This guideline is aimed at all Health Care Professionals involved in the
Persistent Pulmonary Hypertension of the Newborn (PPHN) University Hospitals of Leicester NHS NHS Trust June 2018 June 2021 Scope: This guideline is aimed at all Health Care Professionals involved in the
The Art and Science of Weaning from Mechanical Ventilation
 The Art and Science of Weaning from Mechanical Ventilation Shekhar T. Venkataraman M.D. Professor Departments of Critical Care Medicine and Pediatrics University of Pittsburgh School of Medicine Some definitions
The Art and Science of Weaning from Mechanical Ventilation Shekhar T. Venkataraman M.D. Professor Departments of Critical Care Medicine and Pediatrics University of Pittsburgh School of Medicine Some definitions
Nitric Resource Manual
 Nitric Resource Manual OBJECTIVES Describe the biologic basis for inhaled nitric oxide therapy Describe the indications for inhaled nitric oxide therapy Describe the potential hazards, side effects and
Nitric Resource Manual OBJECTIVES Describe the biologic basis for inhaled nitric oxide therapy Describe the indications for inhaled nitric oxide therapy Describe the potential hazards, side effects and
OSCAR & OSCILLATE. & the Future of High Frequency Oscillatory Ventilation (HFOV)
") & & the Future of High Frequency Oscillatory Ventilation (HFOV) www.philippelefevre.com What do we know already? Sud S et al. BMJ 2010 & Multi-centre randomised controlled trials of HFOV verses current
& & the Future of High Frequency Oscillatory Ventilation (HFOV) www.philippelefevre.com What do we know already? Sud S et al. BMJ 2010 & Multi-centre randomised controlled trials of HFOV verses current
Minimizing Lung Damage During Respiratory Support
 Minimizing Lung Damage During Respiratory Support University of Miami Jackson Memorial Medical Center Care of the Sick Newborn 15 Eduardo Bancalari MD University of Miami Miller School of Medicine Jackson
Minimizing Lung Damage During Respiratory Support University of Miami Jackson Memorial Medical Center Care of the Sick Newborn 15 Eduardo Bancalari MD University of Miami Miller School of Medicine Jackson
CONTINUOUS POSITIVE AIRWAY PRESSURE (CPAP) DEFINITION
 DEFINITION") CONTINUOUS POSITIVE AIRWAY PRESSURE (CPAP) DEFINITION Method of maintaining low pressure distension of lungs during inspiration and expiration when infant breathing spontaneously Benefits Improves oxygenation
CONTINUOUS POSITIVE AIRWAY PRESSURE (CPAP) DEFINITION Method of maintaining low pressure distension of lungs during inspiration and expiration when infant breathing spontaneously Benefits Improves oxygenation
ritical Care Review Early Intervention in Respiratory Distress Syndrome Stephen Minton, MD, Dale Gerstmann, MD, Ronald Stoddard, MD
 ritical Care Review CURRENT APPLICATIONS AND ECONOMICS Early Intervention in Respiratory Distress Syndrome Stephen Minton, MD, Dale Gerstmann, MD, Ronald Stoddard, MD Introduction Since its availability
ritical Care Review CURRENT APPLICATIONS AND ECONOMICS Early Intervention in Respiratory Distress Syndrome Stephen Minton, MD, Dale Gerstmann, MD, Ronald Stoddard, MD Introduction Since its availability
ARDS: an update 6 th March A. Hakeem Al Hashim, MD, FRCP SQUH
 ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
Newborn Life Support. NLS guidance.
 Kelly Harvey, ANNP NWNODN, previously Wythenshawe Hospital has shared this presentation with the understanding that it is for personal use following your attendance at the 8th Annual Senior Neonatal Nursing
Kelly Harvey, ANNP NWNODN, previously Wythenshawe Hospital has shared this presentation with the understanding that it is for personal use following your attendance at the 8th Annual Senior Neonatal Nursing
Delivery Room Resuscitation of Newborns with Congenital Anomalies
 Delivery Room Resuscitation of Newborns with Congenital Anomalies Anne Ades, MD, MSEd Director of Neonatal Education The Children s Hospital of Philadelphia Associate Professor of Clinical Pediatrics Perelman
Delivery Room Resuscitation of Newborns with Congenital Anomalies Anne Ades, MD, MSEd Director of Neonatal Education The Children s Hospital of Philadelphia Associate Professor of Clinical Pediatrics Perelman
5 Million neonatal deaths each year worldwide. 20% caused by neonatal asphyxia. Improvement of the outcome of 1 million newborns every year
 1 5 Million neonatal deaths each year worldwide 20% caused by neonatal asphyxia Improvement of the outcome of 1 million newborns every year International Liaison Committee on Resuscitation (ILCOR) American
1 5 Million neonatal deaths each year worldwide 20% caused by neonatal asphyxia Improvement of the outcome of 1 million newborns every year International Liaison Committee on Resuscitation (ILCOR) American
SWISS SOCIETY OF NEONATOLOGY. Preterm infant with. pulmonary hypertension and hypopituitarism
 SWISS SOCIETY OF NEONATOLOGY Preterm infant with pulmonary hypertension and hypopituitarism November 2007 2 Pilgrim S, Stocker M, Neonatal and Pediatric Intensiv Care Unit, Children s Hospital of Lucerne,
SWISS SOCIETY OF NEONATOLOGY Preterm infant with pulmonary hypertension and hypopituitarism November 2007 2 Pilgrim S, Stocker M, Neonatal and Pediatric Intensiv Care Unit, Children s Hospital of Lucerne,
1. Which of the following arterial blood gas results indicate metabolic acidosis?
 B10 Baby s Breath: Ventilation Strategies and Blood Gas Interpretation Mary Beth Bodin, DNP, CRNP, NNP-BC Assistant Professor School of Nursing, University of Alabama at Birmingham Neonatal Nurse Practitioner
B10 Baby s Breath: Ventilation Strategies and Blood Gas Interpretation Mary Beth Bodin, DNP, CRNP, NNP-BC Assistant Professor School of Nursing, University of Alabama at Birmingham Neonatal Nurse Practitioner
Simulation 3: Post-term Baby in Labor and Delivery
 Simulation 3: Post-term Baby in Labor and Delivery Opening Scenario (Links to Section 1) You are an evening-shift respiratory therapist in a large hospital with a level III neonatal unit. You are paged
Simulation 3: Post-term Baby in Labor and Delivery Opening Scenario (Links to Section 1) You are an evening-shift respiratory therapist in a large hospital with a level III neonatal unit. You are paged
INTRODUCTION The effect of CPAP works on lung mechanics to improve oxygenation (PaO 2
 2 Effects of CPAP INTRODUCTION The effect of CPAP works on lung mechanics to improve oxygenation (PaO 2 ). The effect on CO 2 is only secondary to the primary process of improvement in lung volume and
2 Effects of CPAP INTRODUCTION The effect of CPAP works on lung mechanics to improve oxygenation (PaO 2 ). The effect on CO 2 is only secondary to the primary process of improvement in lung volume and
Dr. Roberta Keller has nothing to disclose.
 Vascular reactivity and onary hypertension in congenital diaphragmatic hernia Roberta L. Keller, MD UCSF Benioff Children s Hospital March 12, 211 Dr. Roberta Keller has nothing to disclose. Outline Lung
Vascular reactivity and onary hypertension in congenital diaphragmatic hernia Roberta L. Keller, MD UCSF Benioff Children s Hospital March 12, 211 Dr. Roberta Keller has nothing to disclose. Outline Lung
Mechanical Ventilation: Disease-Specific Strategies
 23 Mechanical Ventilation: DiseaseSpecific Strategies Bradley A. Yoder, MD When noninvasive respiratory support is insufficient to achieve adequate gas exchange, insertion of an endotracheal tube and mechanical
23 Mechanical Ventilation: DiseaseSpecific Strategies Bradley A. Yoder, MD When noninvasive respiratory support is insufficient to achieve adequate gas exchange, insertion of an endotracheal tube and mechanical
Non Invasive Ventilation In Preterm Infants. Manuel Sanchez Luna Hospital General Universitario Gregorio Marañón Complutense University Madrid
 Non Invasive Ventilation In Preterm Infants Manuel Sanchez Luna Hospital General Universitario Gregorio Marañón Complutense University Madrid Summary Noninvasive ventilation begings in the delivery room
Non Invasive Ventilation In Preterm Infants Manuel Sanchez Luna Hospital General Universitario Gregorio Marañón Complutense University Madrid Summary Noninvasive ventilation begings in the delivery room
Usefulness of DuoPAP in the treatment of very low birth weight preterm infants with neonatal respiratory distress syndrome
 European Review for Medical and Pharmacological Sciences 2015; 19: 573-577 Usefulness of DuoPAP in the treatment of very low birth weight preterm infants with neonatal respiratory distress syndrome B.
European Review for Medical and Pharmacological Sciences 2015; 19: 573-577 Usefulness of DuoPAP in the treatment of very low birth weight preterm infants with neonatal respiratory distress syndrome B.
SWISS SOCIETY OF NEONATOLOGY. Selective bronchial intubation for unilateral PIE
 SWISS SOCIETY OF NEONATOLOGY Selective bronchial intubation for unilateral PIE October 2000 2 Berger TM, Jöhr M, Neonatal and Pediatric Intensive Care Unit (BTM), Kinderspital Luzern, Department of Anesthesiology
SWISS SOCIETY OF NEONATOLOGY Selective bronchial intubation for unilateral PIE October 2000 2 Berger TM, Jöhr M, Neonatal and Pediatric Intensive Care Unit (BTM), Kinderspital Luzern, Department of Anesthesiology
Kugelman A, Riskin A, Said W, Shoris I, Mor F, Bader D.
 Heated, Humidified High-Flow Nasal Cannula (HHHFNC) vs. Nasal Intermittent Positive Pressure Ventilation (NIPPV) for the Primary Treatment of RDS, A Randomized, Controlled, Prospective, Pilot Study Kugelman
Heated, Humidified High-Flow Nasal Cannula (HHHFNC) vs. Nasal Intermittent Positive Pressure Ventilation (NIPPV) for the Primary Treatment of RDS, A Randomized, Controlled, Prospective, Pilot Study Kugelman
Noah Hillman M.D. IPOKRaTES Conference Guadalajaira, Mexico August 23, 2018
 Postnatal Steroids Use for Bronchopulmonary Dysplasia in 2018 + = Noah Hillman M.D. IPOKRaTES Conference Guadalajaira, Mexico August 23, 2018 AAP Policy Statement - 2002 This statement is intended for
Postnatal Steroids Use for Bronchopulmonary Dysplasia in 2018 + = Noah Hillman M.D. IPOKRaTES Conference Guadalajaira, Mexico August 23, 2018 AAP Policy Statement - 2002 This statement is intended for
AEROSURF Phase 2 Program Update Investor Conference Call
 AEROSURF Phase 2 Program Update Investor Conference Call November 12, 2015 Forward Looking Statement To the extent that statements in this presentation are not strictly historical, including statements
AEROSURF Phase 2 Program Update Investor Conference Call November 12, 2015 Forward Looking Statement To the extent that statements in this presentation are not strictly historical, including statements
Stabilization and Transportation guidelines for Neonates and infants with Heart disease:
 Stabilization and Transportation guidelines for Neonates and infants with Heart disease: Background: Referral Pediatric Cardiac Units, frequently receive neonates and infants referred and transported from
Stabilization and Transportation guidelines for Neonates and infants with Heart disease: Background: Referral Pediatric Cardiac Units, frequently receive neonates and infants referred and transported from
9/5/2018. Conflicts of Interests. Pediatric Acute Respiratory Distress Syndrome. Objectives ARDS ARDS. Definitions. None
 Pediatric Acute Respiratory Distress Syndrome Conflicts of Interests Diane C Lipscomb, MD Director Inpatient Pediatric Medical Director Mercy Springfield Associate Clerkship Clinical Director University
Pediatric Acute Respiratory Distress Syndrome Conflicts of Interests Diane C Lipscomb, MD Director Inpatient Pediatric Medical Director Mercy Springfield Associate Clerkship Clinical Director University
The CDH Study Group A possible model for multi disciplinary collaboration?
 The CDH Study Group A possible model for multi disciplinary collaboration? Krisa P. Van Meurs, MD Stanford University Palo Alto, California Kevin P. Lally, MD University of Texas Houston Houston, Texas
The CDH Study Group A possible model for multi disciplinary collaboration? Krisa P. Van Meurs, MD Stanford University Palo Alto, California Kevin P. Lally, MD University of Texas Houston Houston, Texas
Management of refractory ARDS. Saurabh maji
 Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
B13. Baby s Breath: Ventilation Strategies and Blood Gas Interpretation. Session Summary. Session Objectives. Test Questions.
 B13 Baby s Breath: Ventilation Strategies and Blood Gas Interpretation Karen Wright, PhD, NNP-BC DNP NNP Program Director Rush University, Chicago, IL The speaker has signed a disclosure form and indicated
B13 Baby s Breath: Ventilation Strategies and Blood Gas Interpretation Karen Wright, PhD, NNP-BC DNP NNP Program Director Rush University, Chicago, IL The speaker has signed a disclosure form and indicated
EPNV-Montreux 2018: Preliminary Educational and Scientific Program
 EPNV-Montreux 2018: Preliminary Educational and Scientific Program April 25-26, 2018: Pre-Conference Workshops Wednesday (April 25): 09 00 18 00 Thursday (April 26): 08 00 12 00 April 26-28, 2018: Main
EPNV-Montreux 2018: Preliminary Educational and Scientific Program April 25-26, 2018: Pre-Conference Workshops Wednesday (April 25): 09 00 18 00 Thursday (April 26): 08 00 12 00 April 26-28, 2018: Main
Assessing Initial Response to High-Frequency Jet Ventilation in Premature Infants With Hypercapnic Respiratory Failure
 Assessing Initial Response to High-Frequency Jet Ventilation in Premature Infants With Hypercapnic Respiratory Failure Craig R Wheeler RRT-NPS, Craig D Smallwood RRT, Iris O Donnell RRT-NPS, Daniel Gagner
Assessing Initial Response to High-Frequency Jet Ventilation in Premature Infants With Hypercapnic Respiratory Failure Craig R Wheeler RRT-NPS, Craig D Smallwood RRT, Iris O Donnell RRT-NPS, Daniel Gagner
Disclosures. Learning Objectives. Mechanical Ventilation of Infants with Severe BPD: An Interdisciplinary Approach 3/10/2017
 Mechanical Ventilation of Infants with Severe BPD: An Interdisciplinary Approach Steven H. Abman, MD Professor, Department of Pediatrics Director, Pediatric Heart Lung Center University of Colorado School
Mechanical Ventilation of Infants with Severe BPD: An Interdisciplinary Approach Steven H. Abman, MD Professor, Department of Pediatrics Director, Pediatric Heart Lung Center University of Colorado School
GASTRO-INTESTINAL. NEC Necrotisiing Enterocolitis
 GASTRO-INTESTINAL NEC Necrotisiing Enterocolitis BACKGROUND: This is a spectrum of disease comprising ischaemia and infection affecting the intestine of, predominantly, low birth weight, premature neonates.
GASTRO-INTESTINAL NEC Necrotisiing Enterocolitis BACKGROUND: This is a spectrum of disease comprising ischaemia and infection affecting the intestine of, predominantly, low birth weight, premature neonates.
An Overview of Bronchopulmonary Dysplasia and Chronic Lung Disease in Infancy
 An Overview of Bronchopulmonary Dysplasia and Chronic Lung Disease in Infancy Housekeeping: I have no financial disclosures Learning objectives: Develop an understanding of bronchopulmonary dysplasia (BPD)
An Overview of Bronchopulmonary Dysplasia and Chronic Lung Disease in Infancy Housekeeping: I have no financial disclosures Learning objectives: Develop an understanding of bronchopulmonary dysplasia (BPD)
Presented By : Kamlah Olaimat
 Presented By : Kamlah Olaimat 18\7\2010 Transient Tachpnea of the Definition:- newborn (TTN) TTN is a benign disease of near term or term infant who display respiratory distress shortly after delivery.
Presented By : Kamlah Olaimat 18\7\2010 Transient Tachpnea of the Definition:- newborn (TTN) TTN is a benign disease of near term or term infant who display respiratory distress shortly after delivery.
Volume Guarantee Initiation and ongoing clinical management of an infant supported by Volume Guarantee A Case Study
 D-32084-2011 Volume Guarantee Initiation and ongoing clinical management of an infant supported by Volume Guarantee A Case Study Robert DiBlasi RRT-NPS, FAARC Respiratory Care Manager of Research & Quality
D-32084-2011 Volume Guarantee Initiation and ongoing clinical management of an infant supported by Volume Guarantee A Case Study Robert DiBlasi RRT-NPS, FAARC Respiratory Care Manager of Research & Quality
Congenital Diaphragmatic Hernia: Update on Regional Experience
 Khalid Al-Umran, CABP; Saleem Khawaja, FRCS; Adekunle H. Dawodu, FRCP(Ed); Abdulatif Al-Arfj, Fachartz From the Departments of Pediatrics (Drs. Al-Umran and Dawodu), and Surgery (Drs. Khawaja and Al-Arfaj),
Khalid Al-Umran, CABP; Saleem Khawaja, FRCS; Adekunle H. Dawodu, FRCP(Ed); Abdulatif Al-Arfj, Fachartz From the Departments of Pediatrics (Drs. Al-Umran and Dawodu), and Surgery (Drs. Khawaja and Al-Arfaj),
Congenital Diaphragmatic Hernia information for parents. David M Notrica MD FACS FAAP Pediatric Surgeons of Phoenix
 Congenital Diaphragmatic Hernia information for parents David M Notrica MD FACS FAAP Pediatric Surgeons of Phoenix CDH Congenital absence of a portion of the diaphragm allowing abdominal contents to migrate
Congenital Diaphragmatic Hernia information for parents David M Notrica MD FACS FAAP Pediatric Surgeons of Phoenix CDH Congenital absence of a portion of the diaphragm allowing abdominal contents to migrate
ARDS: MANAGEMENT UPDATE
 ARDS: MANAGEMENT UPDATE Tanıl Kendirli, Assoc. Prof. Ankara University School of Medicine, Pediatric Critical Care Medicine The AECC Definition Timing Acute onset, within 48-72 hours Oxygenation ALI PaO2/FiO2
ARDS: MANAGEMENT UPDATE Tanıl Kendirli, Assoc. Prof. Ankara University School of Medicine, Pediatric Critical Care Medicine The AECC Definition Timing Acute onset, within 48-72 hours Oxygenation ALI PaO2/FiO2
N orthway et first described bronchopulmonary
 F6 ORIGINAL ARTICLE Does sustained lung inflation at resuscitation reduce lung injury in the preterm infant? A E Harling, M W Beresford, G S Vince, M Bates, C W Yoxall... See end of article for authors
F6 ORIGINAL ARTICLE Does sustained lung inflation at resuscitation reduce lung injury in the preterm infant? A E Harling, M W Beresford, G S Vince, M Bates, C W Yoxall... See end of article for authors
Key Words: congenital diaphragmatic hernia, consensus guidelines, evidence review, management
 The Canadian Congenital Diaphragmatic Hernia Collaborative Evidence and Consensus- Based National Clinical Management Guideline The Canadian CDH Collaborative Short Title: Canadian CDH Collaborative Guidelines
The Canadian Congenital Diaphragmatic Hernia Collaborative Evidence and Consensus- Based National Clinical Management Guideline The Canadian CDH Collaborative Short Title: Canadian CDH Collaborative Guidelines
End tidal carbon dioxide (ETCO2) and peripheral pulse oximetry (SpO2) trends and right-to-left shunting in neonates undergoing
 and peripheral pulse oximetry (SpO2) trends and right-to-left shunting in neonates undergoing") End tidal carbon dioxide (ETCO2) and peripheral pulse oximetry (SpO2) trends and right-to-left shunting in neonates undergoing non cardiac surgery under general anesthesia C. Goonasekera, G. Kunst, M.
End tidal carbon dioxide (ETCO2) and peripheral pulse oximetry (SpO2) trends and right-to-left shunting in neonates undergoing non cardiac surgery under general anesthesia C. Goonasekera, G. Kunst, M.
Persistent Pulmonary Hypertension of the Newborn
 Persistent Pulmonary Hypertension of the Newborn Lon-Yen Tsao Division of Neonatology, Department of Pediatrics Changhua Christian Hospital, Changhua, Taiwan, R.O.C. Introduction: Persistent pulmonary
Persistent Pulmonary Hypertension of the Newborn Lon-Yen Tsao Division of Neonatology, Department of Pediatrics Changhua Christian Hospital, Changhua, Taiwan, R.O.C. Introduction: Persistent pulmonary
Bubble CPAP for Respiratory Distress Syndrome in Preterm Infants
 R E S E A R C H P A P E R Bubble CPAP for Respiratory Distress Syndrome in Preterm Infants JAGDISH KOTI*, SRINIVAS MURKI, PRAMOD GADDAM, ANUPAMA REDDY AND M DASARADHA RAMI REDDY From Fernandez Hospital
R E S E A R C H P A P E R Bubble CPAP for Respiratory Distress Syndrome in Preterm Infants JAGDISH KOTI*, SRINIVAS MURKI, PRAMOD GADDAM, ANUPAMA REDDY AND M DASARADHA RAMI REDDY From Fernandez Hospital
ARDS and Ventilators PG26 Update in Surgical Critical Care October 9, 2013
 ARDS and Ventilators PG26 Update in Surgical Critical Care October 9, 2013 Pauline K. Park MD, FACS, FCCM University of Michigan School of Medicine Ann Arbor, MI OVERVIEW New Berlin definition of ARDS
ARDS and Ventilators PG26 Update in Surgical Critical Care October 9, 2013 Pauline K. Park MD, FACS, FCCM University of Michigan School of Medicine Ann Arbor, MI OVERVIEW New Berlin definition of ARDS
HFOV Case Study 14 year old Instructor Copy
 HFOV Case Study 14 year old Instructor Copy Color key: Black Patient case Blue RN/RCP collaboration Red MD consult Green - Critical Thinking Inquiry Green italics CT answers ABG format: ph/pco2/po2/base
HFOV Case Study 14 year old Instructor Copy Color key: Black Patient case Blue RN/RCP collaboration Red MD consult Green - Critical Thinking Inquiry Green italics CT answers ABG format: ph/pco2/po2/base
BPD. Neonatal/Pediatric Cardiopulmonary Care. Disease. Bronchopulmonary Dysplasia. Baby Jane
 1 Neonatal/Pediatric Cardiopulmonary Care Disease 2 Bronchopulmonary Dysplasia 3 is a 33-day-old prematurely born girl who weighs 1420 g. At birth, her estimated gestational age was 28 weeks. Her initial
1 Neonatal/Pediatric Cardiopulmonary Care Disease 2 Bronchopulmonary Dysplasia 3 is a 33-day-old prematurely born girl who weighs 1420 g. At birth, her estimated gestational age was 28 weeks. Her initial
When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영
 When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영 The Korean Society of Cardiology COI Disclosure Eun-Young Choi The author have no financial conflicts of interest to disclose
When is Risky to Apply Oxygen for Congenital Heart Disease 부천세종병원 소아청소년과최은영 The Korean Society of Cardiology COI Disclosure Eun-Young Choi The author have no financial conflicts of interest to disclose
11 th Annual Congress Turkish Thoracic Society. Mechanical Ventilation in Acute Hypoxemic Respiratory Failure
 11 th Annual Congress Turkish Thoracic Society Mechanical Ventilation in Acute Hypoxemic Respiratory Failure Lluis Blanch MD PhD Senior Critical Care Center Scientific Director Corporació Parc Taulí Universitat
11 th Annual Congress Turkish Thoracic Society Mechanical Ventilation in Acute Hypoxemic Respiratory Failure Lluis Blanch MD PhD Senior Critical Care Center Scientific Director Corporació Parc Taulí Universitat
10/16/2017. Review the indications for ECMO in patients with. Respiratory failure Cardiac failure Cardiorespiratory failure
 Review the indications for ECMO in patients with Respiratory failure Cardiac failure Cardiorespiratory failure 1 Extracorporeal membrane lung and/or cardiac support. A support therapy, in no way definitive.
Review the indications for ECMO in patients with Respiratory failure Cardiac failure Cardiorespiratory failure 1 Extracorporeal membrane lung and/or cardiac support. A support therapy, in no way definitive.
NEONATAL CLINICAL PRACTICE GUIDELINE
 NEONATAL CLINICAL PRACTICE GUIDELINE Title: Integrated Evaluation of Neonatal Hemodynamics (IENH) and Targeted Echocardiogram Approval Date: January 2015 Approved by: Neonatal Patient Care Teams, HSC &
NEONATAL CLINICAL PRACTICE GUIDELINE Title: Integrated Evaluation of Neonatal Hemodynamics (IENH) and Targeted Echocardiogram Approval Date: January 2015 Approved by: Neonatal Patient Care Teams, HSC &
Outcomes From Severe ARDS Managed Without ECMO. Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016
 Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
Handling Common Problems & Pitfalls During. Oxygen desaturation in patients receiving mechanical ventilation ACUTE SEVERE RESPIRATORY FAILURE
 Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1.
Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1.
GE Healthcare. Non Invasive Ventilation (NIV) For the Engström Ventilator. Relief, Relax, Recovery
 For the Engström Ventilator. Relief, Relax, Recovery") GE Healthcare Non Invasive Ventilation (NIV) For the Engström Ventilator Relief, Relax, Recovery COPD is currently the fourth leading cause of death in the world, and further increases in the prevalence
GE Healthcare Non Invasive Ventilation (NIV) For the Engström Ventilator Relief, Relax, Recovery COPD is currently the fourth leading cause of death in the world, and further increases in the prevalence
Oxygenation Failure. Increase FiO2. Titrate end-expiratory pressure. Adjust duty cycle to increase MAP. Patient Positioning. Inhaled Vasodilators
 Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
Duct Dependant Congenital Heart Disease
 Children s Acute Transport Service Clinical Guidelines Duct Dependant Congenital Heart Disease This guideline has been agreed by both NTS & CATS Document Control Information Author CATS/NTS Author Position
Children s Acute Transport Service Clinical Guidelines Duct Dependant Congenital Heart Disease This guideline has been agreed by both NTS & CATS Document Control Information Author CATS/NTS Author Position
ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate. Carolyn Calfee, MD MAS Mark Eisner, MD MPH
 ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate Carolyn Calfee, MD MAS Mark Eisner, MD MPH June 3, 2010 Case Presentation Setting: Community hospital, November 2009 29 year old woman with
ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate Carolyn Calfee, MD MAS Mark Eisner, MD MPH June 3, 2010 Case Presentation Setting: Community hospital, November 2009 29 year old woman with
TRAINING NEONATOLOGY SILVANA PARIS
 TRAINING ON NEONATOLOGY SILVANA PARIS RESUSCITATION IN DELIVERY ROOM INTRODUCTION THE GLOBAL RESUSCITATION BURDEN IN NEWBORN 136 MILL NEWBORN BABIES EACH YEAR (WHO WORLD REPORT) 5-8 MILL NEWBORN INFANTS
TRAINING ON NEONATOLOGY SILVANA PARIS RESUSCITATION IN DELIVERY ROOM INTRODUCTION THE GLOBAL RESUSCITATION BURDEN IN NEWBORN 136 MILL NEWBORN BABIES EACH YEAR (WHO WORLD REPORT) 5-8 MILL NEWBORN INFANTS
NEONATAL CLINICAL PRACTICE GUIDELINE
 NEONATAL CLINICAL PRACTICE GUIDELINE Title: Brain Oxygen Monitoring in Newborns Using Near Infrared Spectroscopy (NIRS) Approval Date: Pages: June 2016 Approved by: Neonatal Patient Care Teams, HSC & SBH
NEONATAL CLINICAL PRACTICE GUIDELINE Title: Brain Oxygen Monitoring in Newborns Using Near Infrared Spectroscopy (NIRS) Approval Date: Pages: June 2016 Approved by: Neonatal Patient Care Teams, HSC & SBH
APRV Ventilation Mode
 APRV Ventilation Mode Airway Pressure Release Ventilation A Type of CPAP Continuous Positive Airway Pressure (CPAP) with an intermittent release phase. Patient cycles between two levels of CPAP higher
APRV Ventilation Mode Airway Pressure Release Ventilation A Type of CPAP Continuous Positive Airway Pressure (CPAP) with an intermittent release phase. Patient cycles between two levels of CPAP higher
Review of Neonatal Respiratory Problems
 Review of Neonatal Respiratory Problems Respiratory Distress Occurs in about 7% of infants Clinical presentation includes: Apnea Cyanosis Grunting Inspiratory stridor Nasal flaring Poor feeding Tachypnea
Review of Neonatal Respiratory Problems Respiratory Distress Occurs in about 7% of infants Clinical presentation includes: Apnea Cyanosis Grunting Inspiratory stridor Nasal flaring Poor feeding Tachypnea
1st Annual Clinical Simulation Conference
 1st Annual Clinical Simulation Conference Newborns with Acute Respiratory Distress: Diagnosis and Management Ma Teresa C. Ambat, MD Assistant Professor Division of Neonatology, Department of Pediatrics
1st Annual Clinical Simulation Conference Newborns with Acute Respiratory Distress: Diagnosis and Management Ma Teresa C. Ambat, MD Assistant Professor Division of Neonatology, Department of Pediatrics
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv
 Rv") ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
Mechanical Ventilation & Cardiopulmonary Interactions: Clinical Application in Non- Conventional Circulations. Eric M. Graham, MD
 Mechanical Ventilation & Cardiopulmonary Interactions: Clinical Application in Non- Conventional Circulations Eric M. Graham, MD Background Heart & lungs work to meet oxygen demands Imbalance between supply
Mechanical Ventilation & Cardiopulmonary Interactions: Clinical Application in Non- Conventional Circulations Eric M. Graham, MD Background Heart & lungs work to meet oxygen demands Imbalance between supply
Aim: Reduction in the rate of CLD in ELBW infants (<1000 grams) by 30% from its baseline of 72 % by January 2016.
 by 30% from its baseline of 72 % by January 2016.") LIVE (Less Invasive Ventilation of ELBW infants) HEALTHY WVU Children s Hospital, Morgantown, WV, USA Rebecca Tilley, RN; Jamie Karr, RT; Tiffany Blosser, RN; Christy Dixon, RT; Melinda Connolly, ANP;
LIVE (Less Invasive Ventilation of ELBW infants) HEALTHY WVU Children s Hospital, Morgantown, WV, USA Rebecca Tilley, RN; Jamie Karr, RT; Tiffany Blosser, RN; Christy Dixon, RT; Melinda Connolly, ANP;
Landmark articles on ventilation
 Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
State of Florida Systemic Supportive Care Guidelines. Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology
 State of Florida Systemic Supportive Care Guidelines Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology I. FEN 1. What intravenous fluids should be initiated upon admission
State of Florida Systemic Supportive Care Guidelines Michael D. Weiss, M.D. Associate Professor of Pediatrics Division of Neonatology I. FEN 1. What intravenous fluids should be initiated upon admission
ADMISSION/DISCHARGE FORM FOR INFANTS BORN IN 2019 DO NOT mail or fax this form to the CPQCC Data Center. This form is for internal use ONLY.
 1 Any eligible inborn infant who dies in the delivery room or at any other location in your hospital within 12 hours after birth and prior to admission to the NICU is defined as a "Delivery Room Death."
1 Any eligible inborn infant who dies in the delivery room or at any other location in your hospital within 12 hours after birth and prior to admission to the NICU is defined as a "Delivery Room Death."
TREATMENT OF SEVERE MECONIUM ASPIRATION SYNDROME
 TREATMENT OF SEVERE MECONIUM ASPIRATION SYNDROME WITH DILUTE SURFACTANT LAVAGE Hung-Yang Chang, Chyong-Hsin Hsu, Hsin-An Kao, Han-Yang Hung, Jui-Hsing Chang, Chun-Chih Peng, and Wai-Tim Jim Background
TREATMENT OF SEVERE MECONIUM ASPIRATION SYNDROME WITH DILUTE SURFACTANT LAVAGE Hung-Yang Chang, Chyong-Hsin Hsu, Hsin-An Kao, Han-Yang Hung, Jui-Hsing Chang, Chun-Chih Peng, and Wai-Tim Jim Background
Yorkshire & Humber Neonatal ODN (South) Clinical Guideline
 Clinical Guideline") Yorkshire & Humber Neonatal ODN (South) Clinical Guideline Title: Ventilation Author: Dr Cath Smith updated September 2017, written by Dr Elizabeth Pilling May 2011 Date written: May 2011 Review date:
Yorkshire & Humber Neonatal ODN (South) Clinical Guideline Title: Ventilation Author: Dr Cath Smith updated September 2017, written by Dr Elizabeth Pilling May 2011 Date written: May 2011 Review date:
Quality Improvement Approaches to BPD. Jay P. Goldsmith, M.D. Tulane University New Orleans, Louisiana
 Quality Improvement Approaches to BPD Jay P. Goldsmith, M.D. Tulane University New Orleans, Louisiana goldsmith.jay@gmail.com No conflicts of interest to declare There is nothing more dangerous to the
Quality Improvement Approaches to BPD Jay P. Goldsmith, M.D. Tulane University New Orleans, Louisiana goldsmith.jay@gmail.com No conflicts of interest to declare There is nothing more dangerous to the
Learning Objectives. 1. Indications versus contra-indications 2. CPAP versus NiVS 3. Clinical evidence
 Learning Objectives 1. Indications versus contra-indications 2. CPAP versus NiVS 3. Clinical evidence Pre-hospital Non-invasive vventilatory support Marc Gillis, MD Imelda Bonheiden Our goal out there
Learning Objectives 1. Indications versus contra-indications 2. CPAP versus NiVS 3. Clinical evidence Pre-hospital Non-invasive vventilatory support Marc Gillis, MD Imelda Bonheiden Our goal out there
Ventilatory Management of ARDS. Alexei Ortiz Milan; MD, MSc
 Ventilatory Management of ARDS Alexei Ortiz Milan; MD, MSc 2017 Outline Ventilatory management of ARDS Protected Ventilatory Strategy Use of NMB Selection of PEEP Driving pressure Lung Recruitment Prone
Ventilatory Management of ARDS Alexei Ortiz Milan; MD, MSc 2017 Outline Ventilatory management of ARDS Protected Ventilatory Strategy Use of NMB Selection of PEEP Driving pressure Lung Recruitment Prone
Mechanical Ventilation 1. Shari McKeown, RRT Respiratory Services - VGH
 Mechanical Ventilation 1 Shari McKeown, RRT Respiratory Services - VGH Objectives Describe indications for mcvent Describe types of breaths and modes of ventilation Describe compliance and resistance and
Mechanical Ventilation 1 Shari McKeown, RRT Respiratory Services - VGH Objectives Describe indications for mcvent Describe types of breaths and modes of ventilation Describe compliance and resistance and