Tremor. Mario Zappia. Università degli Studi di Catania
|
|
|
- Sheila Hodge
- 5 years ago
- Views:
Transcription

1 Tremor Mario Zappia Università degli Studi di Catania
2 Tremor: Definition Rhythmical, Involuntary, Oscillatory movement of a body part Classification of Dyskinesias Based on Rhythmicity Rhythmical Dyskinesias: Tremor Clonus Myorhythmia (Myoclonus) (Dystonic Dyskinesias) Not- Rhythmical Dyskinesias: Chorea Athetosis Dystonic Dyskinesias Ballisms Tics and Stereotypes Myoclonus
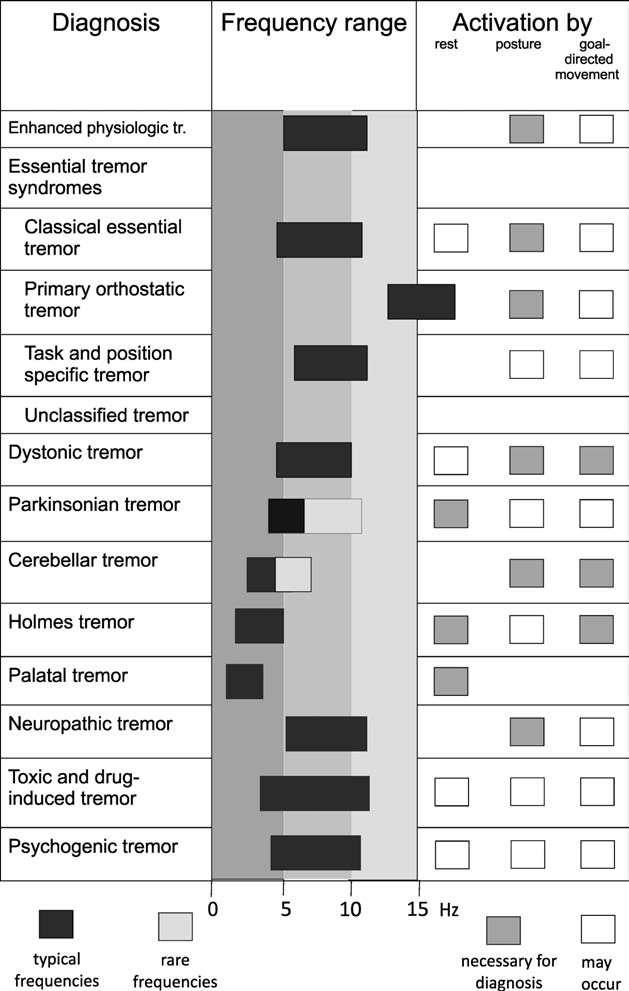
3 Clinical Assessment of Tremor Syndromes Topography: Head (Chin, Face, Tongue, Palate), Limbs (Distal, Proximal), Trunk Activation Condition: rest, action, goal-direction, posture, task Rhithmicity Characteristics: Amplitude and Frequency (Low < 4 Hz, High > 7 Hz), Modulation Associated Movements: mirrors and dystonic outflows Adapted from: 1998 Consensus Statement of the Movement Disorder Society
4 Clinical Assessment of Tremor Syndromes Specific examinations for assessment of: Akinesia/bradykinesia Muscle tone (including Froment s sign for the upper and lower extremity and coactivation sign for psychogenic tremor) Postural abnormalities Dystonia Cerebellar signs Pyramidal signs Neuropathic signs Systemic signs (thyrotoxicosis and so forth) Gait and stance (orthostatic tremor) 1998 Consensus Statement of the Movement Disorder Society
5 Clinical Assessment of Tremor Syndromes Specific data from the medical history: Onset of tremor Family history of neurologic diseases (especially tremor) Alcohol sensitivity Sequence of spread of tremor (including symmetry and laterality) Associated diseases (restless legs, polyneuropathy) Medication Drug abuse 1998 Consensus Statement of the Movement Disorder Society
6
7 Essential Tremor Classical and Controversial Clinical Aspects

8 Mov Disord 2010
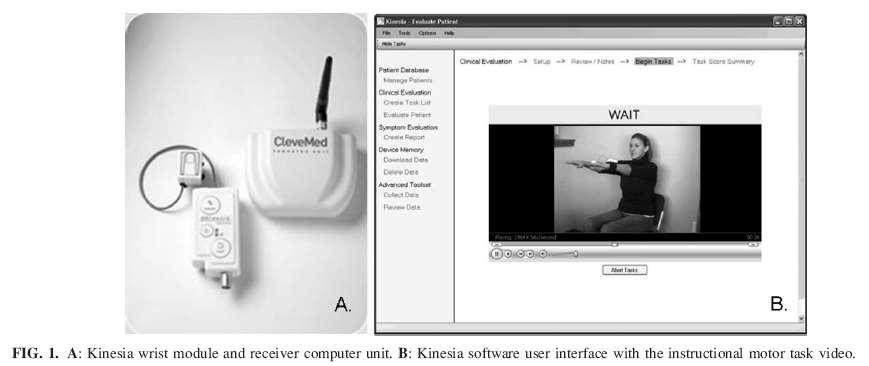
9 P.G. (66 years old) History Tremor since 2007 RBD Examination Mild bradykinesia/rigidity upper limbs R>L Arms tremor at rest R>L Chin tremor at rest Brain MRI Subcortical vascular lesions Single-axial accelerometer Tremor at rest frequency: 4.4 Hz Spect DaT-SCAN Normal Last Visit: October No Changes.

10 Follow-up:11.1 years (range, 8-25 years)
11
12 Polygraphic recording of cervical tremor when seated. The patient looks straight ahead in A, counts backward in B Alternate pattern
13
14 S.M. (73 years old). Family History Consanguineous parents Father s sister: head and vocal tremor Two brothers: unspecified Motor Neurone Disease; unspecified Sensitive Axonal Polyneuropathy History 15 years ago: head and vocal tremor. Instability during walking Brain MRI: n.t.r. Spect DaT-SCAN: normal Blink reflex recovery cicle: enhanced R2 inhibition Genetics: negative SCA1-2-3 Patient Third Brother.
15
16 Essential Tremor Pathophysiological Aspects

17 Glassy, eosinophilic swellings in the molecular layer adjacent to Purkinje cell bodies.
18
19

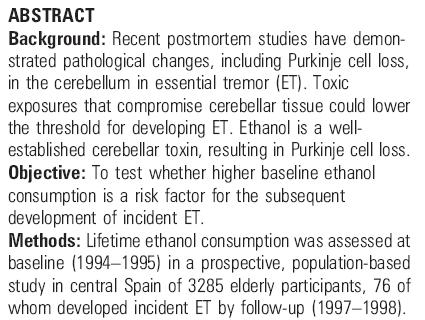
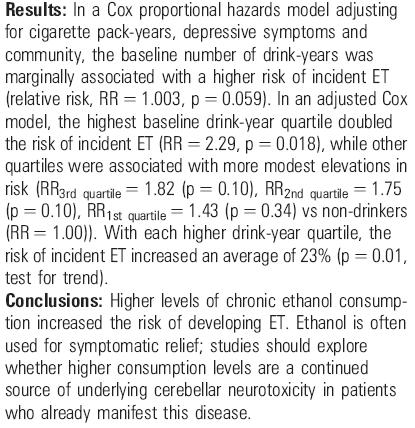
20 Is ET really caused by Alcohol Consumption? possibility that participants who developed incident ET between the baseline and follow-up evaluations had preclinical ET at baseline % of the incident cases of ET had no baseline in-person clinical evaluation, so a diagnosis of ET at the time of enrollment was excluded using only the analysis of handwriting samples, with possible initial misdiagnosis and then overestimation of the incident cases at the time of follow-up.
21
22
23 Moderate Alcohol Consumption and Neuroprotection Compared with abstention, consumption of 1 to 6 drinks weekly was associated with a lower risk of incident dementia. Mukamal KJ et al., JAMA 2003 OR 1,4 1,2 1 0,8 0,6 0,4 0,2 0 J-Shape effect 1,22 0,65 0,46 0,69 <1 1 to 6 7 to Weekly alcohol consumption (drinks) A 34-year follow-up prospective population study showed wine and spirits may display opposite associations with dementia. Thus, at least part of the association for wine may be explained by components other than ethanol. Mehlig K, Am J Epidemiol 2008
24
25 Red Wine Resveratrol Protective Effect Resveratrol is a polyphenolic compound derived from grapes and red wine Produces the inhibition of microglial activation and the subsequent reduction of proinflammatory factor release Resveratrol-mediated neuroprotection has been attributed to the inhibition of NADPH oxidase Protectes dopaminergic neurons against lipopolysaccharide (LPS)-induced neurotoxicity in concentration and timedependent manners. Zhang F, Mol Pharmacol 2010
26 Essential Tremor Assessments
27
28
29 Other Tremors Clinical Examples
30 D.V. (50 years old) History Family history for gait disorders History Onset in 2010 with deflection of mood and anxiety Pain in the neck and right shoulder with associated tremor of the hand Examination Lateralization of the trunk to the right Right laterocollis Deficit of postural reflexes Hypophonia Hypomimia Rest tremor of the right upper limb Postural tremor of the upper limbs (right>left) Moderate rigidity of the upper limbs (right>left) Moderate bradykinesia of the upper limbs (right>left) Peak-of-dose Distonia/Athetosis of the right foot

31 Brain MRI Scan Axial T1 Axial T2 Axial Flair

32 Brain CT Scan
33 Q.A. (55 years old) Family Hystory Family history of involuntar movements: a son with deflection of mood, anxiety, motor and vocal tics. Hystory Onset in 2010 with generalized weakness and bradikinesia, right hand tremor. Three years ago: tinnitus treated with flunarizine. In 2010 improvement after stopping treatment with flunarizine. Two years ago: muscle cramps in the left hand and bilateral plantar introversion, not correlated with exercise. Improvement after muscle strain. Examination Hypomimia Reduced pendular movements Slight postural and kinetic asymmetric tremor of the upper limbs Moderate rigidity of the trunk and upper limbs Slight bradikinesia of all four limbs Hyperreflexia of the deep tendon reflexes in all four limbs

34 Brain CT Scan
35 Movement disorders accounted for 55% of the total symptomatic patients
36 Hereditary motor-sensory neuropathy and movement disorders. Cardoso FE, Jankovic J. Muscle Nerve Sep;16(9): S.S. (54 years old) Hystory Age 40: lower limbs weakness, unsteadiness, gait disturbance
37 B.E. (55 years old) History 5 years ago writing trouble with tremor October 2010: tinglings to the left limbs Neurological examination Hypoactive deep tendon reflexes Not-elicitable plantar reflexes Mild action tremor and writing tremor Rhynopharynx Cyst Blood Exam: Anti-Chlamidia Pneumoniae IgA/IgG, NSE (low) (anti-hcv neg.) CSF exam: proteins (high) EMG: sensitive-motor neuropathy SSEP lower limbs: central conduction time (high) VEP: left P100 latency (high) MTS: Upper limbs: MEPS latency (high); Left lower limb: central motor conduction time (high)

38 Brain MRI Scan

39
40
41 R.R. (69 years old) History Ischemic Heart Disease In 2010 sudden weakness right limbs and dysarthria. Remission after days. Examination Weakness of lower facial muscles on the right side Spastic gait to the right Pseudo-rhythmical distal athetosis on the right hand with abnormal posture and loss of proprioception ( thalamic hand )

42 Brain MRI Scan


43 Myoclonic dystonia with predominating myoclonus and thalamic hand associating dystonic posture and slow, pseudo-athetoid movements, both related to controlateral lesions in the Vim and Vc nuclei of the Thalamus.
44 S.G. (60 years old) History Hypertension Neurosensorial hypoacusis Depression treated with neuroleptics and antidepressants Onset since 2 years ago with left hand tremor Neurological examination Left upper limb rest tremor and slight bilateral postural tremor characterized by disappearance after distraction.
45
Presented by Joanna O Leary, MD Providence St. Vincent Medical Center Movement Disorder Department
 Presented by Joanna O Leary, MD Providence St. Vincent Medical Center Movement Disorder Department Hyperkinetic movement disorders Increase in muscle movements causing involuntary motion Tremor Dystonia
Presented by Joanna O Leary, MD Providence St. Vincent Medical Center Movement Disorder Department Hyperkinetic movement disorders Increase in muscle movements causing involuntary motion Tremor Dystonia
Disorders of Movement M A R T I N H A R L E Y N E U R O L O G Y
 Disorders of Movement M A R T I N H A R L E Y N E U R O L O G Y Educational Objectives Improved history taking in patients with movement disorders. Develop a systematic approach to observing and describing
Disorders of Movement M A R T I N H A R L E Y N E U R O L O G Y Educational Objectives Improved history taking in patients with movement disorders. Develop a systematic approach to observing and describing
Tremor 101. Objectives 9/30/2015. Importance of tremors
 Tremor 101 Umer Akbar, MD Assistant Professor, Brown University Movement Disorders Program, Rhode Island Hospital & Butler Hospital Objectives Recognize and describe the qualities of common types of tremor
Tremor 101 Umer Akbar, MD Assistant Professor, Brown University Movement Disorders Program, Rhode Island Hospital & Butler Hospital Objectives Recognize and describe the qualities of common types of tremor
Professor Tim Anderson
 Professor Tim Anderson Neurologist University of Otago Christchurch 11:00-11:55 WS #91: Shakes Jerks and Spasms - Recognition and Differential Diagnosis 12:05-13:00 WS #102: Shakes Jerks and Spasms - Recognition
Professor Tim Anderson Neurologist University of Otago Christchurch 11:00-11:55 WS #91: Shakes Jerks and Spasms - Recognition and Differential Diagnosis 12:05-13:00 WS #102: Shakes Jerks and Spasms - Recognition
Professor Tim Anderson
 Professor Tim Anderson Neurologist University of Otago Christchurch 11:00-11:55 WS #91: Shakes Jerks and Spasms - Recognition and Differential Diagnosis 12:05-13:00 WS #102: Shakes Jerks and Spasms - Recognition
Professor Tim Anderson Neurologist University of Otago Christchurch 11:00-11:55 WS #91: Shakes Jerks and Spasms - Recognition and Differential Diagnosis 12:05-13:00 WS #102: Shakes Jerks and Spasms - Recognition
An Approach to Patients with Movement Disorders
 An Approach to Patients with Movement Disorders Joaquim Ferreira, MD, PhD Laboratory of Clinical Pharmacology and Therapeutics Faculty of Medicine University of Lisbon EDUCATIONAL TOOLS MDS video library
An Approach to Patients with Movement Disorders Joaquim Ferreira, MD, PhD Laboratory of Clinical Pharmacology and Therapeutics Faculty of Medicine University of Lisbon EDUCATIONAL TOOLS MDS video library
Types of involuntary movements
 Tremor Types of involuntary movements Dystonia Chorea Myoclonus Tics Tremor Rhythmic shaking of muscles that produces an oscillating movement Parkinsonian tremor Rest tremor > posture > kinetic Re-emergent
Tremor Types of involuntary movements Dystonia Chorea Myoclonus Tics Tremor Rhythmic shaking of muscles that produces an oscillating movement Parkinsonian tremor Rest tremor > posture > kinetic Re-emergent
DIFFERENTIAL DIAGNOSIS SARAH MARRINAN
 Parkinson s Academy Registrar Masterclass Sheffield DIFFERENTIAL DIAGNOSIS SARAH MARRINAN 17 th September 2014 Objectives Importance of age in diagnosis Diagnostic challenges Brain Bank criteria Differential
Parkinson s Academy Registrar Masterclass Sheffield DIFFERENTIAL DIAGNOSIS SARAH MARRINAN 17 th September 2014 Objectives Importance of age in diagnosis Diagnostic challenges Brain Bank criteria Differential
Differential Diagnosis of Hypokinetic Movement Disorders
 Differential Diagnosis of Hypokinetic Movement Disorders Dr Donald Grosset Consultant Neurologist - Honorary Professor Institute of Neurological Sciences - Glasgow University Hypokinetic Parkinson's Disease
Differential Diagnosis of Hypokinetic Movement Disorders Dr Donald Grosset Consultant Neurologist - Honorary Professor Institute of Neurological Sciences - Glasgow University Hypokinetic Parkinson's Disease
Movement disorders in childhood: assessment and diagnosis. Lucinda Carr
 Movement disorders in childhood: assessment and diagnosis Lucinda Carr Movement disorders in childhood: Assessment Classification Causes Diagnosis Presentation of movement disorders in childhood: Concerns
Movement disorders in childhood: assessment and diagnosis Lucinda Carr Movement disorders in childhood: Assessment Classification Causes Diagnosis Presentation of movement disorders in childhood: Concerns
Evaluation of Parkinson s Patients and Primary Care Providers
 Evaluation of Parkinson s Patients and Primary Care Providers 2018 Movement Disorders Half Day Symposium Elise Anderson MD Medical Co-Director, PBSI Movement Disorders 6/28/2018 1 Disclosures GE Speaker,
Evaluation of Parkinson s Patients and Primary Care Providers 2018 Movement Disorders Half Day Symposium Elise Anderson MD Medical Co-Director, PBSI Movement Disorders 6/28/2018 1 Disclosures GE Speaker,
STEADY YOUR APPROACH TO TREMOR (OVERVIEW OF DIFFERENTIAL DIAGNOSIS)
") STEADY YOUR APPROACH TO TREMOR (OVERVIEW OF DIFFERENTIAL DIAGNOSIS) Karen M. Thomas D.O. Diplomate, ABPN Director of Movement Disorders Program Director of Comprehensive Parkinson s Disease Program Sentara
STEADY YOUR APPROACH TO TREMOR (OVERVIEW OF DIFFERENTIAL DIAGNOSIS) Karen M. Thomas D.O. Diplomate, ABPN Director of Movement Disorders Program Director of Comprehensive Parkinson s Disease Program Sentara
III./3.1. Movement disorders with akinetic rigid symptoms
 III./3.1. Movement disorders with akinetic rigid symptoms III./3.1.1. Parkinson s disease Parkinson s disease (PD) is the second most common neurodegenerative disorder worldwide after Alzheimer s disease.
III./3.1. Movement disorders with akinetic rigid symptoms III./3.1.1. Parkinson s disease Parkinson s disease (PD) is the second most common neurodegenerative disorder worldwide after Alzheimer s disease.
Movement Disorders. Psychology 372 Physiological Psychology. Background. Myasthenia Gravis. Many Types
 Background Movement Disorders Psychology 372 Physiological Psychology Steven E. Meier, Ph.D. Listen to the audio lecture while viewing these slides Early Studies Found some patients with progressive weakness
Background Movement Disorders Psychology 372 Physiological Psychology Steven E. Meier, Ph.D. Listen to the audio lecture while viewing these slides Early Studies Found some patients with progressive weakness
Hyperkinetic movement disorders are. Hyperkinetic Movement Disorders. Cases in Movement Disorders. James case. About Tom
 Hyperkinetic Movement Disorders Sarah Furtado, MD, PhD, FRCPC James case A mother brings her son James, 10, to your office because of repetitive sniffing sounds and repetitive eye blinking. This sniffing
Hyperkinetic Movement Disorders Sarah Furtado, MD, PhD, FRCPC James case A mother brings her son James, 10, to your office because of repetitive sniffing sounds and repetitive eye blinking. This sniffing
Phenomenology of Movement Disorders
 Phenomenology of Movement Disorders Raja Mehanna MD Anatomical reasoning Anatomical reasoning Phenomenological reasoning Abnormal movement Hypokinetic Hyperkinetic Ataxia Video 1 But there is a tremor!
Phenomenology of Movement Disorders Raja Mehanna MD Anatomical reasoning Anatomical reasoning Phenomenological reasoning Abnormal movement Hypokinetic Hyperkinetic Ataxia Video 1 But there is a tremor!
Involuntary Movements in Children and Adolescents: Is it Seizure, Tic or Something Else?
 Involuntary Movements in Children and Adolescents: Is it Seizure, Tic or Something Else? California Association of Nurse Practitioners Monterey, March 22, 2013 Julie Sprague-McRae, MS, RN, PPCNP-BC Ruth
Involuntary Movements in Children and Adolescents: Is it Seizure, Tic or Something Else? California Association of Nurse Practitioners Monterey, March 22, 2013 Julie Sprague-McRae, MS, RN, PPCNP-BC Ruth
Department of Neurology, Rigshospitalet, 9 Blegdamsvej, PAULSON, O.B. Involuntary Movements. Tohoku J. Exp. Med., 1990, 161,
 Tohoku J. Exp. Med., 1990, 161, Suppl., 21-27 Involuntary Movements OLAF B. PAULSON Department of Neurology, Rigshospitalet, 9 Blegdamsvej, DK-2100, Copenhagen, Denmark PAULSON, O.B. Involuntary Movements.
Tohoku J. Exp. Med., 1990, 161, Suppl., 21-27 Involuntary Movements OLAF B. PAULSON Department of Neurology, Rigshospitalet, 9 Blegdamsvej, DK-2100, Copenhagen, Denmark PAULSON, O.B. Involuntary Movements.
The Neurologic Examination. John W. Engstrom, M.D. University of California San Francisco School of Medicine
 The Neurologic Examination John W. Engstrom, M.D. University of California San Francisco School of Medicine Overview The Neurologic Examination Mental status demonstration/questions Cranial nerves demonstration/questions
The Neurologic Examination John W. Engstrom, M.D. University of California San Francisco School of Medicine Overview The Neurologic Examination Mental status demonstration/questions Cranial nerves demonstration/questions
Neurological Examination
 Neurological Examination Charles University in Prague 1st Medical Faculty and General University Hospital Neurological examination: Why important? clinical history taking and bedside examination: classical
Neurological Examination Charles University in Prague 1st Medical Faculty and General University Hospital Neurological examination: Why important? clinical history taking and bedside examination: classical
Parkinson s Disease in the Elderly A Physicians perspective. Dr John Coyle
 Parkinson s Disease in the Elderly A Physicians perspective Dr John Coyle Overview Introduction Epidemiology and aetiology Pathogenesis Diagnosis and clinical features Treatment Psychological issues/ non
Parkinson s Disease in the Elderly A Physicians perspective Dr John Coyle Overview Introduction Epidemiology and aetiology Pathogenesis Diagnosis and clinical features Treatment Psychological issues/ non
VL VA BASAL GANGLIA. FUNCTIONAl COMPONENTS. Function Component Deficits Start/initiation Basal Ganglia Spontan movements
 BASAL GANGLIA Chris Cohan, Ph.D. Dept. of Pathology/Anat Sci University at Buffalo I) Overview How do Basal Ganglia affect movement Basal ganglia enhance cortical motor activity and facilitate movement.
BASAL GANGLIA Chris Cohan, Ph.D. Dept. of Pathology/Anat Sci University at Buffalo I) Overview How do Basal Ganglia affect movement Basal ganglia enhance cortical motor activity and facilitate movement.
Movement Disorders Will Garrett, M.D Assistant Professor of Neurology
 Movement Disorders Will Garrett, M.D Assistant Professor of Neurology I. The Basal Ganglia The basal ganglia are composed of several structures including the caudate and putamen (collectively called the
Movement Disorders Will Garrett, M.D Assistant Professor of Neurology I. The Basal Ganglia The basal ganglia are composed of several structures including the caudate and putamen (collectively called the
Movement Disorders. Eric Kraus, MD! Neurology!
 Movement Disorders Eric Kraus, MD! Neurology! Classify Bradykinesia! Tic! Myoclonus! Tremor! Dystonia! Athetosis! Chorea! Ballismus! Case 1 This 64 year-old female has had progression of a tremor over
Movement Disorders Eric Kraus, MD! Neurology! Classify Bradykinesia! Tic! Myoclonus! Tremor! Dystonia! Athetosis! Chorea! Ballismus! Case 1 This 64 year-old female has had progression of a tremor over
ID # COMPLETED: YES.. 1 DATE NO... 5 NEUROLOGICAL EXAM
 ID # COMPLETED: YES.. 1 DATE NO... 5 NEUROLOGICAL EXAM VIDEOTAPED: YES.. 1 NO... 5 COMMENT: NEUROLOGICAL EXAM "Normal, Abnormal, Other, Can't execute or Missing for each question. Always complete specify
ID # COMPLETED: YES.. 1 DATE NO... 5 NEUROLOGICAL EXAM VIDEOTAPED: YES.. 1 NO... 5 COMMENT: NEUROLOGICAL EXAM "Normal, Abnormal, Other, Can't execute or Missing for each question. Always complete specify
Tremor What is tremor? What causes tremor? What are the characteristics of tremor? What are the different categories of tremor?
 Tremor What is tremor? Tremor is an unintentional, somewhat rhythmic, muscle movement involving to-and-fro movements (oscillations) of one or more parts of the body. It is the most common of all involuntary
Tremor What is tremor? Tremor is an unintentional, somewhat rhythmic, muscle movement involving to-and-fro movements (oscillations) of one or more parts of the body. It is the most common of all involuntary
Parkinson Disease. Lorraine Kalia, MD, PhD, FRCPC. Presented by: Ontario s Geriatric Steering Committee
 Parkinson Disease Lorraine Kalia, MD, PhD, FRCPC Key Learnings Parkinson Disease (L. Kalia) Key Learnings Parkinson disease is the most common but not the only cause of parkinsonism Parkinson disease is
Parkinson Disease Lorraine Kalia, MD, PhD, FRCPC Key Learnings Parkinson Disease (L. Kalia) Key Learnings Parkinson disease is the most common but not the only cause of parkinsonism Parkinson disease is
Movement Disorders- Parkinson s Disease. Fahed Saada, MD March 8 th, th Family Medicine Refresher Course St.
 Movement Disorders- Parkinson s Disease Fahed Saada, MD March 8 th, 2019 48 th Family Medicine Refresher Course St. Joseph s Health Disclosure ACADIA Pharmaceuticals Objectives Review the classification
Movement Disorders- Parkinson s Disease Fahed Saada, MD March 8 th, 2019 48 th Family Medicine Refresher Course St. Joseph s Health Disclosure ACADIA Pharmaceuticals Objectives Review the classification
Parkinson s Disease. Sirilak yimcharoen
 Parkinson s Disease Sirilak yimcharoen EPIDEMIOLOGY ~1% of people over 55 years Age range 35 85 years peak age of onset is in the early 60s ~5% of cases characterized by an earlier age of onset (typically
Parkinson s Disease Sirilak yimcharoen EPIDEMIOLOGY ~1% of people over 55 years Age range 35 85 years peak age of onset is in the early 60s ~5% of cases characterized by an earlier age of onset (typically
Evolution of a concept: Apraxia/higher level gait disorder. ataxia v. apraxia gait = limb apraxia. low, middle, high gait disturbance levels
 Case #1 81-year-old woman Gait Imbalance: Two Unusual Cases in Older Patients February 2008: 3 years of gradually progressive gait imbalance no vertigo, dizziness or paresthesias etiology unclear on examination
Case #1 81-year-old woman Gait Imbalance: Two Unusual Cases in Older Patients February 2008: 3 years of gradually progressive gait imbalance no vertigo, dizziness or paresthesias etiology unclear on examination
CN V! touch! pain! Touch! P/T!
 CN V! touch! pain! Touch! P/T! Visual Pathways! L! R! B! A! C! D! LT! E! F! RT! G! hypothalamospinal! and! ALS! Vestibular Pathways! 1. Posture/Balance!!falling! 2. Head Position! 3. Eye-Head Movements
CN V! touch! pain! Touch! P/T! Visual Pathways! L! R! B! A! C! D! LT! E! F! RT! G! hypothalamospinal! and! ALS! Vestibular Pathways! 1. Posture/Balance!!falling! 2. Head Position! 3. Eye-Head Movements
Parkinson s Disease and other related movement disorders a video guide to diagnosis
 Parkinson s Disease and other related movement disorders a video guide to diagnosis Parkinson s Disease Masterclass November 2017 Dr Frank Phelan MidYorkshire Hospitals NHS Trust Ideopathic Parkinson s
Parkinson s Disease and other related movement disorders a video guide to diagnosis Parkinson s Disease Masterclass November 2017 Dr Frank Phelan MidYorkshire Hospitals NHS Trust Ideopathic Parkinson s
CONTRIBUTORS The American Academy of Neurology Institute.
 Several of these multiple-choice questions were originally published in Continuum: Lifelong Learning in Neurology Movement Disorders, Volume 22, Issue 4, August 2016 based on the content in the issue developed
Several of these multiple-choice questions were originally published in Continuum: Lifelong Learning in Neurology Movement Disorders, Volume 22, Issue 4, August 2016 based on the content in the issue developed
University of Manitoba - MPT: Neurological Clinical Skills Checklist
 Name: Site: Assessment Skills Observed Performed Becoming A. Gross motor function i. Describe movement strategies (quality, devices, timeliness, independence): supine sidelying sit stand supine long sitting
Name: Site: Assessment Skills Observed Performed Becoming A. Gross motor function i. Describe movement strategies (quality, devices, timeliness, independence): supine sidelying sit stand supine long sitting
Headway Victoria Epilepsy and Parkinson s Centre
 Headway Victoria Epilepsy and Parkinson s Centre Parkinson s Overview and Medication Shannon Oatway Community Education/ Awareness Coordinator What is Parkinson s Disease? The basics It is a chronic and
Headway Victoria Epilepsy and Parkinson s Centre Parkinson s Overview and Medication Shannon Oatway Community Education/ Awareness Coordinator What is Parkinson s Disease? The basics It is a chronic and
Functional Distinctions
 Functional Distinctions FUNCTION COMPONENT DEFICITS Start Basal Ganglia Spontaneous Movements Move UMN/LMN Cerebral Cortex Brainstem, Spinal cord Roots/peripheral nerves Plan Cerebellum Ataxia Adjust Cerebellum
Functional Distinctions FUNCTION COMPONENT DEFICITS Start Basal Ganglia Spontaneous Movements Move UMN/LMN Cerebral Cortex Brainstem, Spinal cord Roots/peripheral nerves Plan Cerebellum Ataxia Adjust Cerebellum
Joint Session with ACOFP and Mayo Clinic. Parkinson's Disease: 5 Pearls. Jay Van Gerpen, MD
 Joint Session with ACOFP and Mayo Clinic Parkinson's Disease: 5 Pearls Jay Van Gerpen, MD Parkinson s Disease: 5 Pearls J.A. van Gerpen, MD Sections of Movement Disorders and Clinical Neurophysiology
Joint Session with ACOFP and Mayo Clinic Parkinson's Disease: 5 Pearls Jay Van Gerpen, MD Parkinson s Disease: 5 Pearls J.A. van Gerpen, MD Sections of Movement Disorders and Clinical Neurophysiology
MOVEMENT DISORDERS UPDATE H. MURRAY TODD, M.D., F.A.A.N.
 MOVEMENT DISORDERS UPDATE H. MURRAY TODD, M.D., F.A.A.N. Movement Disorders Hypokinesia : decreased voluntary and automatic movements Hyperkinesia : excessive movements HYPOKINESIAS Parkinson s disease
MOVEMENT DISORDERS UPDATE H. MURRAY TODD, M.D., F.A.A.N. Movement Disorders Hypokinesia : decreased voluntary and automatic movements Hyperkinesia : excessive movements HYPOKINESIAS Parkinson s disease
PARKINS ON CENTER. Parkinson s Disease: Diagnosis and Management. Learning Objectives: Recognition of PD OHSU. Disclosure Information
 OHSU PARKINS ON CENTER Parkinson s Disease: Diagnosis and Management for Every MD Disclosure Information Grants/Research Support: National Parkinson Foundation, NIH, Michael J. Fox Foundation Consultant:
OHSU PARKINS ON CENTER Parkinson s Disease: Diagnosis and Management for Every MD Disclosure Information Grants/Research Support: National Parkinson Foundation, NIH, Michael J. Fox Foundation Consultant:
Neurophysiological study of tremor: How to do it in clinical practice
 3 rd Congress of the European Academy of Neurology Amsterdam, The Netherlands, June 24 27, 2017 Hands-on Course 8 MDS-ES/EAN: Neurophysiological study of tremor - Level 1 Neurophysiological study of tremor:
3 rd Congress of the European Academy of Neurology Amsterdam, The Netherlands, June 24 27, 2017 Hands-on Course 8 MDS-ES/EAN: Neurophysiological study of tremor - Level 1 Neurophysiological study of tremor:
Form B3L: UPDRS Part III Motor Examination 1
 Initial Visit Packet NACC Uniform Data Set (UDS) LBD MODULE Form B3L: UPDRS Part III Motor Examination 1 ADC name: Subject ID: Form date: / / Visit #: Examiner s initials: INSTRUCTIONS: This form is to
Initial Visit Packet NACC Uniform Data Set (UDS) LBD MODULE Form B3L: UPDRS Part III Motor Examination 1 ADC name: Subject ID: Form date: / / Visit #: Examiner s initials: INSTRUCTIONS: This form is to
ASHI691: Why We Fall Apart: The Neuroscience and Neurophysiology of Aging. Dr. Olav E. Krigolson Lecture 5: PARKINSONS DISEASE
 ASHI691: Why We Fall Apart: The Neuroscience and Neurophysiology of Aging Dr. Olav E. Krigolson krigolson@uvic.ca Lecture 5: PARKINSONS DISEASE The Basal Ganglia Primary motor cortex Execution of movement
ASHI691: Why We Fall Apart: The Neuroscience and Neurophysiology of Aging Dr. Olav E. Krigolson krigolson@uvic.ca Lecture 5: PARKINSONS DISEASE The Basal Ganglia Primary motor cortex Execution of movement
HISTORY TAKING ON NERVOUS SYSTEM. Dr. Amitesh Aggarwal
 HISTORY TAKING ON NERVOUS SYSTEM Dr. Amitesh Aggarwal General points History of neurological symptoms should also be taken from patient and close relative or friend Memory loss, intoxication, aphasia Patient
HISTORY TAKING ON NERVOUS SYSTEM Dr. Amitesh Aggarwal General points History of neurological symptoms should also be taken from patient and close relative or friend Memory loss, intoxication, aphasia Patient
Neuro Exam Explained
 Neuro Exam Explained Michael Nelson M.D. Providence Neurological Specialties East Primary Care Conference October 26 rd, 2017 Michael Nelson M.D. Medical School: University of Missouri-Columbia Residency:
Neuro Exam Explained Michael Nelson M.D. Providence Neurological Specialties East Primary Care Conference October 26 rd, 2017 Michael Nelson M.D. Medical School: University of Missouri-Columbia Residency:
1/29/18 TREMOR. Tremor definition. Classification of tremors. International Congress of Parkinson's Disease and Movement Disorders
 TREMOR International Congress of Parkinson's Disease and Movement Disorders 5-9 Oct 2018 Hong Kong www.movementdisorders.org Prof Pille Taba University of Tartu, Estonia 3 February 2018, Bordeaux MDS-ES
TREMOR International Congress of Parkinson's Disease and Movement Disorders 5-9 Oct 2018 Hong Kong www.movementdisorders.org Prof Pille Taba University of Tartu, Estonia 3 February 2018, Bordeaux MDS-ES
Strick Lecture 4 March 29, 2006 Page 1
 Strick Lecture 4 March 29, 2006 Page 1 Basal Ganglia OUTLINE- I. Structures included in the basal ganglia II. III. IV. Skeleton diagram of Basal Ganglia Loops with cortex Similarity with Cerebellar Loops
Strick Lecture 4 March 29, 2006 Page 1 Basal Ganglia OUTLINE- I. Structures included in the basal ganglia II. III. IV. Skeleton diagram of Basal Ganglia Loops with cortex Similarity with Cerebellar Loops
Deep Brain Stimulation: Indications and Ethical Applications
 Deep Brain Stimulation Overview Kara D. Beasley, DO, MBe, FACOS Boulder Neurosurgical and Spine Associates (303) 562-1372 Deep Brain Stimulation: Indications and Ethical Applications Instrument of Change
Deep Brain Stimulation Overview Kara D. Beasley, DO, MBe, FACOS Boulder Neurosurgical and Spine Associates (303) 562-1372 Deep Brain Stimulation: Indications and Ethical Applications Instrument of Change
Gait Disorders. Nicholas J. Silvestri, MD
 Gait Disorders Nicholas J. Silvestri, MD Disclosures NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS TO REPORT Learning Objectives Explain the normal development of gait Describe various gait
Gait Disorders Nicholas J. Silvestri, MD Disclosures NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS TO REPORT Learning Objectives Explain the normal development of gait Describe various gait
Evaluation and Management of Parkinson s Disease in the Older Patient
 Evaluation and Management of Parkinson s Disease in the Older Patient David A. Hinkle, MD, PhD Comprehensive Movement Disorders Clinic Pittsburgh Institute for Neurodegenerative Diseases University of
Evaluation and Management of Parkinson s Disease in the Older Patient David A. Hinkle, MD, PhD Comprehensive Movement Disorders Clinic Pittsburgh Institute for Neurodegenerative Diseases University of
2/18/ yo man with history of mild developmental delay and chorea of unclear etiology, with new complaints of speech difficulty
 18 yo man with history of mild developmental delay and chorea of unclear etiology, with new complaints of speech difficulty Audrey Foster-Barber UCSF Child Neurology February 18, 2011 Several years of
18 yo man with history of mild developmental delay and chorea of unclear etiology, with new complaints of speech difficulty Audrey Foster-Barber UCSF Child Neurology February 18, 2011 Several years of
Clinical Caveats for Functional Disorders. Kalpesh Jivan Division of Neurology Department of Neurosciences
 Clinical Caveats for Functional Disorders Kalpesh Jivan Division of Neurology Department of Neurosciences How common are functional symptoms? ± ⅓ of new neurological outpatients Definitions Conversion(functional)
Clinical Caveats for Functional Disorders Kalpesh Jivan Division of Neurology Department of Neurosciences How common are functional symptoms? ± ⅓ of new neurological outpatients Definitions Conversion(functional)
An approach to movement disorders. Kailash Bhatia, DM, FRCP Professor of Clinical Neurology Institute of Neurology Queen Square, London
 An approach to movement disorders Kailash Bhatia, DM, FRCP Professor of Clinical Neurology Institute of Neurology Queen Square, London Neurology Diagnosis Two main questions: What parts of the nervous
An approach to movement disorders Kailash Bhatia, DM, FRCP Professor of Clinical Neurology Institute of Neurology Queen Square, London Neurology Diagnosis Two main questions: What parts of the nervous
Approach to Tremor in Older Adults
 Neurology Primer Approach to Tremor in Older Adults Joel S. Hurwitz, MB, FRCPC, FRCP (London), Associate Professor, Department of Medicine (Division of Geriatric Medicine), University of Western Ontario,
Neurology Primer Approach to Tremor in Older Adults Joel S. Hurwitz, MB, FRCPC, FRCP (London), Associate Professor, Department of Medicine (Division of Geriatric Medicine), University of Western Ontario,
Patient selection for surgery: Hyperkinetic movement disorders
 Patient selection for surgery: Hyperkinetic movement disorders Alfons Schnitzler, MD, PhD Dept. of Neurology, Movement Disorder and Neuromodulation, Heinrich-Heine-University Düsseldorf, Germany Hyperkinetic
Patient selection for surgery: Hyperkinetic movement disorders Alfons Schnitzler, MD, PhD Dept. of Neurology, Movement Disorder and Neuromodulation, Heinrich-Heine-University Düsseldorf, Germany Hyperkinetic
10/13/2017. Disclosures. Deep Brain Stimulation in the Treatment of Movement Disorders. Deep Brain Stimulation: Objectives.
 Deep Brain Stimulation in the Treatment of Movement Disorders Disclosures None Eleanor K Orehek, M.D. Movement Disorders Specialist Noran Neurological Clinic 1 2 Objectives To provide an overview of deep
Deep Brain Stimulation in the Treatment of Movement Disorders Disclosures None Eleanor K Orehek, M.D. Movement Disorders Specialist Noran Neurological Clinic 1 2 Objectives To provide an overview of deep
Dr. Farah Nabil Abbas. MBChB, MSc, PhD
 Dr. Farah Nabil Abbas MBChB, MSc, PhD The Basal Ganglia *Functions in association with motor cortex and corticospinal pathways. *Regarded as accessory motor system besides cerebellum. *Receive most of
Dr. Farah Nabil Abbas MBChB, MSc, PhD The Basal Ganglia *Functions in association with motor cortex and corticospinal pathways. *Regarded as accessory motor system besides cerebellum. *Receive most of
Neurologic Examination
 John W. Engstrom, MD October 16, 2015 Neurologic Examination Overview The Neurologic Examination Neurologic Examination John W. Engstrom, M.D. Dept. of Neurology University of California, San Francisco
John W. Engstrom, MD October 16, 2015 Neurologic Examination Overview The Neurologic Examination Neurologic Examination John W. Engstrom, M.D. Dept. of Neurology University of California, San Francisco
Brain and Central Nervous System Cancers
 Brain and Central Nervous System Cancers NICE guidance link: https://www.nice.org.uk/guidance/ta121 Clinical presentation of brain tumours History and Examination Consider immediate referral Management
Brain and Central Nervous System Cancers NICE guidance link: https://www.nice.org.uk/guidance/ta121 Clinical presentation of brain tumours History and Examination Consider immediate referral Management
The Neurologic Examination: High-Yield Strategies
 The Neurologic Examination: High-Yield Strategies S. Andrew Josephson, MD Assistant Professor, Department of Neurology Divisions of Neurovascular and Behavioral Neurology University of California San Francisco
The Neurologic Examination: High-Yield Strategies S. Andrew Josephson, MD Assistant Professor, Department of Neurology Divisions of Neurovascular and Behavioral Neurology University of California San Francisco
The motor regulator. 1) Basal ganglia/nucleus
 Basal ganglia/nucleus") The motor regulator 1) Basal ganglia/nucleus Neural structures involved in the control of movement Basal Ganglia - Components of the basal ganglia - Function of the basal ganglia - Connection and circuits
The motor regulator 1) Basal ganglia/nucleus Neural structures involved in the control of movement Basal Ganglia - Components of the basal ganglia - Function of the basal ganglia - Connection and circuits
Approach to a Neurologic Diagnosis
 Approach to a Neurologic Diagnosis Neurologic Diagnosis History Physical & Neurological Examination Ancillary Procedures 3 Questions Asked Focal neurologic deficits Increased intracranial pressure Signs
Approach to a Neurologic Diagnosis Neurologic Diagnosis History Physical & Neurological Examination Ancillary Procedures 3 Questions Asked Focal neurologic deficits Increased intracranial pressure Signs
Misdiagnosis in cervical spondylosis myelopathy.
 Journal of the International Society of Head and Neck Trauma (ISHANT) Case report Misdiagnosis in cervical spondylosis myelopathy. Dr. Reinel A. Junco Martin. Neurosurgeon. Assistant professor Miguel Enriquez
Journal of the International Society of Head and Neck Trauma (ISHANT) Case report Misdiagnosis in cervical spondylosis myelopathy. Dr. Reinel A. Junco Martin. Neurosurgeon. Assistant professor Miguel Enriquez
The Neurologic Examination: High-Yield Strategies
 The Neurologic Examination: High-Yield Strategies S. Andrew Josephson, MD Examination Approach Two types of neurologic examinations 1. Screening Examination 2. Testing Hypotheses Select high-yield tests
The Neurologic Examination: High-Yield Strategies S. Andrew Josephson, MD Examination Approach Two types of neurologic examinations 1. Screening Examination 2. Testing Hypotheses Select high-yield tests
Hypokinetic Movement Disorders
 Hypokinetic Movement Disorders Ariane Park, MD, MPH Assistant Professor-Clinical Division of Neurology The Ohio State University Wexner Medical Center Hypokinetic movement disorders Diminished voluntary
Hypokinetic Movement Disorders Ariane Park, MD, MPH Assistant Professor-Clinical Division of Neurology The Ohio State University Wexner Medical Center Hypokinetic movement disorders Diminished voluntary
ID # COMPLETED: YES 1 DATE NO 2
 ID # COMPLETED: YES 1 DATE NO 2 NEUROLOGICAL EXAM "Normal, Abnormal, Other, Can't execute or Missing for each question. If you circle "Abnormal" or Other, also check the appropriate reason why or explain
ID # COMPLETED: YES 1 DATE NO 2 NEUROLOGICAL EXAM "Normal, Abnormal, Other, Can't execute or Missing for each question. If you circle "Abnormal" or Other, also check the appropriate reason why or explain
U n i f i e d P a r k i n s o n s D i s e a s e R a t i n g S c a l e ( U P D R S )
") Patient last name:................................. Date of birth:.... /.... /........ Patient first name:................................. Date:.... /.... /........ U n i f i e d P a r k i n s o n s D
Patient last name:................................. Date of birth:.... /.... /........ Patient first name:................................. Date:.... /.... /........ U n i f i e d P a r k i n s o n s D
How to Think like a Neurologist Review of Exam Process and Assessment Findings
 Lehigh Valley Health Network LVHN Scholarly Works Neurology Update for the Non-Neurologist 2013 Neurology Update for the Non-Neurologist Feb 20th, 5:10 PM - 5:40 PM How to Think like a Neurologist Review
Lehigh Valley Health Network LVHN Scholarly Works Neurology Update for the Non-Neurologist 2013 Neurology Update for the Non-Neurologist Feb 20th, 5:10 PM - 5:40 PM How to Think like a Neurologist Review
Basal ganglia Sujata Sofat, class of 2009
 Basal ganglia Sujata Sofat, class of 2009 Basal ganglia Objectives Describe the function of the Basal Ganglia in movement Define the BG components and their locations Describe the motor loop of the BG
Basal ganglia Sujata Sofat, class of 2009 Basal ganglia Objectives Describe the function of the Basal Ganglia in movement Define the BG components and their locations Describe the motor loop of the BG
Reflexes. Dr. Baizer
 Reflexes Dr. Baizer 1 Learning objectives: reflexes Students will be able to describe: 1. The clinical importance of testing reflexes. 2. The essential components of spinal reflexes. 3.The stretch reflex.
Reflexes Dr. Baizer 1 Learning objectives: reflexes Students will be able to describe: 1. The clinical importance of testing reflexes. 2. The essential components of spinal reflexes. 3.The stretch reflex.
3) Approach to Ataxia - Dr. Zana
 Approach to Ataxia - Dr. Zana") 3) Approach to Ataxia - Dr. Zana Introduction Ataxia is derived from Greek word a -not, taxis -orderly, (not orderly/ not in order) Ataxia is the inability to make smooth, accurate and coordinated movements
3) Approach to Ataxia - Dr. Zana Introduction Ataxia is derived from Greek word a -not, taxis -orderly, (not orderly/ not in order) Ataxia is the inability to make smooth, accurate and coordinated movements
High Yield Neurological Examination
 High Yield Neurological Examination Vanja Douglas, MD Sara & Evan Williams Foundation Endowed Neurohospitalist Chair Director, Neurohospitalist Division Associate Professor of Clinical Neurology UCSF Department
High Yield Neurological Examination Vanja Douglas, MD Sara & Evan Williams Foundation Endowed Neurohospitalist Chair Director, Neurohospitalist Division Associate Professor of Clinical Neurology UCSF Department
Optimizing Clinical Communication in Parkinson s Disease:
 Optimizing Clinical Communication in Parkinson s Disease:,Strategies for improving communication between you and your neurologist PFNCA Symposium March 25, 2017 Pritha Ghosh, MD Assistant Professor of
Optimizing Clinical Communication in Parkinson s Disease:,Strategies for improving communication between you and your neurologist PFNCA Symposium March 25, 2017 Pritha Ghosh, MD Assistant Professor of
Shake It Off: Recognizing & Treating Movement Disorders
 Ooi Phaik Yee Annual scientific meeting College of Medicine, Academy of Medicine of Malaysia 12 th November 2017 Shake It Off: Recognizing & Treating Movement Disorders MOVEMENT DISORDER A group of symptoms
Ooi Phaik Yee Annual scientific meeting College of Medicine, Academy of Medicine of Malaysia 12 th November 2017 Shake It Off: Recognizing & Treating Movement Disorders MOVEMENT DISORDER A group of symptoms
The NIHSS score is 4 (considering 2 pts for the ataxia involving upper and lower limbs.
 Neuroscience case 5 1. Speech comprehension, ability to speak, and word use were normal in Mr. Washburn, indicating that aphasia (cortical language problem) was not involved. However, he did have a problem
Neuroscience case 5 1. Speech comprehension, ability to speak, and word use were normal in Mr. Washburn, indicating that aphasia (cortical language problem) was not involved. However, he did have a problem
Dr Barry Snow. Neurologist Auckland District Health Board
 Dr Barry Snow Neurologist Auckland District Health Board Dystonia and Parkinson s disease Barry Snow Gowers 1888: Tetanoid chorea Dystonia a movement disorder characterized by sustained or intermittent
Dr Barry Snow Neurologist Auckland District Health Board Dystonia and Parkinson s disease Barry Snow Gowers 1888: Tetanoid chorea Dystonia a movement disorder characterized by sustained or intermittent
Enhanced Primary Care Pathway: Parkinson s Disease
 Enhanced Primary Care Pathway: Parkinson s Disease 1. Focused summary of PD relevant to primary care Parkinson s Disease (PD) and Essential tremor (ET) are two of the most common movement disorders encountered
Enhanced Primary Care Pathway: Parkinson s Disease 1. Focused summary of PD relevant to primary care Parkinson s Disease (PD) and Essential tremor (ET) are two of the most common movement disorders encountered
Unit VIII Problem 5 Physiology: Cerebellum
 Unit VIII Problem 5 Physiology: Cerebellum - The word cerebellum means: the small brain. Note that the cerebellum is not completely separated into 2 hemispheres (they are not clearly demarcated) the vermis
Unit VIII Problem 5 Physiology: Cerebellum - The word cerebellum means: the small brain. Note that the cerebellum is not completely separated into 2 hemispheres (they are not clearly demarcated) the vermis
A Hypothesis Driven Approach to the Neurological Exam
 A Hypothesis Driven Approach to the Neurological Exam Vanja Douglas, MD Assistant Clinical Professor UCSF Department of Neurology Disclosures None 1 Purpose of Neuro Exam Screen asymptomatic patients Screen
A Hypothesis Driven Approach to the Neurological Exam Vanja Douglas, MD Assistant Clinical Professor UCSF Department of Neurology Disclosures None 1 Purpose of Neuro Exam Screen asymptomatic patients Screen
Overview. Overview. Parkinson s disease. Secondary Parkinsonism. Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits
 Overview Overview Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits The differential diagnosis of Parkinson s disease Primary vs. Secondary Parkinsonism Proteinopathies:
Overview Overview Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits The differential diagnosis of Parkinson s disease Primary vs. Secondary Parkinsonism Proteinopathies:
Subthalamic Nucleus Deep Brain Stimulation (STN-DBS)
") Subthalamic Nucleus Deep Brain Stimulation (STN-DBS) A Neurosurgical Treatment for Parkinson s Disease Parkinson s Disease Parkinson s disease is a common neurodegenerative disorder that affects about
Subthalamic Nucleus Deep Brain Stimulation (STN-DBS) A Neurosurgical Treatment for Parkinson s Disease Parkinson s Disease Parkinson s disease is a common neurodegenerative disorder that affects about
Clinical Learning Exercise #1
 Clinical Learning Exercise #1 Exercise: We are going to assume nothing is wrong with the peripheral nervous system and attempt to identify the central nervous system anatomical location for the following
Clinical Learning Exercise #1 Exercise: We are going to assume nothing is wrong with the peripheral nervous system and attempt to identify the central nervous system anatomical location for the following
Parkinson s Disease WHERE HAVE WE BEEN, WHERE ARE WE HEADING? CHARLECE HUGHES D.O.
 Parkinson s Disease WHERE HAVE WE BEEN, WHERE ARE WE HEADING? CHARLECE HUGHES D.O. Parkinson s Epidemiology AFFECTS 1% OF POPULATION OVER 65 MEAN AGE OF ONSET 65 MEN:WOMEN 1.5:1 IDIOPATHIC:HEREDITARY 90:10
Parkinson s Disease WHERE HAVE WE BEEN, WHERE ARE WE HEADING? CHARLECE HUGHES D.O. Parkinson s Epidemiology AFFECTS 1% OF POPULATION OVER 65 MEAN AGE OF ONSET 65 MEN:WOMEN 1.5:1 IDIOPATHIC:HEREDITARY 90:10
2/20/18. History of Parkinson s. What is happening in the brain? DOPAMINE! Epidemiology. Parkinson s Disease. It s much more than tremor
 Parkinson s Disease History of Parkinson s It s much more than tremor Laura Dixon, DNP, MPA, APRN, FNP-BC University of Louisville Department of Neurology Movement Disorders Division Parkinson s Disease
Parkinson s Disease History of Parkinson s It s much more than tremor Laura Dixon, DNP, MPA, APRN, FNP-BC University of Louisville Department of Neurology Movement Disorders Division Parkinson s Disease
Understanding. Tremor. Christy, diagnosed with essential tremor in childhood, with her husband, Ben.
 Understanding Tremor Christy, diagnosed with essential tremor in childhood, with her husband, Ben. What Is Tremor? A tremor is the repetitive, involuntary, rhythmic trembling of one or more parts of the
Understanding Tremor Christy, diagnosed with essential tremor in childhood, with her husband, Ben. What Is Tremor? A tremor is the repetitive, involuntary, rhythmic trembling of one or more parts of the
Moving fast or moving slow: an overview of Movement Disorders
 Moving fast or moving slow: an overview of Movement Disorders Mini Medical School October 25, 2018 Heather Rigby, MD, FRCPC 2014 MFMER slide-1 2014 MFMER slide-2 Basal Ganglia Dysfunction - Movement Disorders
Moving fast or moving slow: an overview of Movement Disorders Mini Medical School October 25, 2018 Heather Rigby, MD, FRCPC 2014 MFMER slide-1 2014 MFMER slide-2 Basal Ganglia Dysfunction - Movement Disorders
The High-Yield Neurologic Examination
 The High-Yield Neurologic Examination S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Chair, Department of Neurology Director, Neurohospitalist
The High-Yield Neurologic Examination S. Andrew Josephson MD Carmen Castro Franceschi and Gladyne K. Mitchell Neurohospitalist Distinguished Professor Chair, Department of Neurology Director, Neurohospitalist
Year 2 MBChB Clinical Skills Session Examination of the Motor System
 Year 2 MBChB Clinical Skills Session Examination of the Motor System Reviewed & ratified by: o o o o Dr D Smith Consultant Neurologist Dr R Davies Consultant Neurologist Dr B Michael Neurology Clinical
Year 2 MBChB Clinical Skills Session Examination of the Motor System Reviewed & ratified by: o o o o Dr D Smith Consultant Neurologist Dr R Davies Consultant Neurologist Dr B Michael Neurology Clinical
Data Collection Worksheets
 Data Collection Worksheets PhenX Measure: Antipsychotic Medication Extrapyramidal Side Effects (#661600) PhenX Protocol: Antipsychotic Medication Extrapyramidal Side Effects (#661601) Date of Interview/Examination/Bioassay
Data Collection Worksheets PhenX Measure: Antipsychotic Medication Extrapyramidal Side Effects (#661600) PhenX Protocol: Antipsychotic Medication Extrapyramidal Side Effects (#661601) Date of Interview/Examination/Bioassay
Dystonia: Title. A real pain in the neck. in All the Wrong Places
 Focus on CME at the University of Western Ontario Dystonia: Title in All the Wrong Places A real pain in the neck By Mandar Jog, MD, FRCPC and; Mary Jenkins, MD, FRCPC What is dystonia? Dystonia is a neurologic
Focus on CME at the University of Western Ontario Dystonia: Title in All the Wrong Places A real pain in the neck By Mandar Jog, MD, FRCPC and; Mary Jenkins, MD, FRCPC What is dystonia? Dystonia is a neurologic
Chapter 4 NEUROLOGY PROBLEMS. Thomas O. Crawford. The Neurology of Ataxia Telangiectasia
 NEUROLOGY PROBLEMS Thomas O. Crawford The Neurology of Ataxia Telangiectasia The neurology of A-T is incredibly complicated. Those who have the disease, family members, therapists, and neurologists who
NEUROLOGY PROBLEMS Thomas O. Crawford The Neurology of Ataxia Telangiectasia The neurology of A-T is incredibly complicated. Those who have the disease, family members, therapists, and neurologists who
Infant Reflexes and Stereotypies. Chapter 9
 Infant Reflexes and Stereotypies Chapter 9 Infant reflexes and stereotypies are very important in the process of development Importance of Infant Reflexes Reflexive movements occur during the last 4 months
Infant Reflexes and Stereotypies Chapter 9 Infant reflexes and stereotypies are very important in the process of development Importance of Infant Reflexes Reflexive movements occur during the last 4 months
PARKINSON S DISEASE: current aspects of ETIOLOGY, DIAGNOSIS and TREATMENT. Dilek Ince Gunal, MD Assoc. Prof
 PARKINSON S DISEASE: current aspects of ETIOLOGY, DIAGNOSIS and TREATMENT Dilek Ince Gunal, MD Assoc. Prof Definition Clinical symptoms: Pathogenesis: Etiology: Neurodegenerative syndrome with chronic,
PARKINSON S DISEASE: current aspects of ETIOLOGY, DIAGNOSIS and TREATMENT Dilek Ince Gunal, MD Assoc. Prof Definition Clinical symptoms: Pathogenesis: Etiology: Neurodegenerative syndrome with chronic,
Disorders of gait and balance
 Disorders of gait and balance clinical assessment and classification Evžen Růžička Charles University in Prague 1st Medical Faculty and General University Hospital handout additional videos and photos
Disorders of gait and balance clinical assessment and classification Evžen Růžička Charles University in Prague 1st Medical Faculty and General University Hospital handout additional videos and photos
Parkinson s Disease. Prevalence. Mark S. Baron, M.D. Cardinal Features. Clinical Characteristics. Not Just a Movement Disorder
 Prevalence Parkinson s Disease Mark S. Baron, M.D. Associate Professor of Neurology Movement Disorders Section VCU School of Medicine Common disorder Approaching 1% by 65 yrs of age, 2% by 80 yrs of age
Prevalence Parkinson s Disease Mark S. Baron, M.D. Associate Professor of Neurology Movement Disorders Section VCU School of Medicine Common disorder Approaching 1% by 65 yrs of age, 2% by 80 yrs of age
Electrodiagnostics for Back & Neck Pain. Steven Andersen, MD Providence Physiatry Clinic
 Electrodiagnostics for Back & Neck Pain Steven Andersen, MD Providence Physiatry Clinic Electrodiagnostics Electromyography (EMG) Needle EMG exam (NEE) Nerve conduction studies (NCS) Motor Sensory Late
Electrodiagnostics for Back & Neck Pain Steven Andersen, MD Providence Physiatry Clinic Electrodiagnostics Electromyography (EMG) Needle EMG exam (NEE) Nerve conduction studies (NCS) Motor Sensory Late
Deep Brain Stimulation for Parkinson s Disease & Essential Tremor
 Deep Brain Stimulation for Parkinson s Disease & Essential Tremor Albert Fenoy, MD Assistant Professor University of Texas at Houston, Health Science Center Current US Approvals Essential Tremor and Parkinsonian
Deep Brain Stimulation for Parkinson s Disease & Essential Tremor Albert Fenoy, MD Assistant Professor University of Texas at Houston, Health Science Center Current US Approvals Essential Tremor and Parkinsonian
PARKINSON S DISEASE. Nigrostriatal Dopaminergic Neurons 5/11/16 CARDINAL FEATURES OF PARKINSON S DISEASE. Parkinson s disease
 5/11/16 PARKINSON S DISEASE Parkinson s disease Prevalence increases with age (starts 40s60s) Seen in all ethnic groups, M:F about 1.5:1 Second most common neurodegenerative disease Genetics role greater
5/11/16 PARKINSON S DISEASE Parkinson s disease Prevalence increases with age (starts 40s60s) Seen in all ethnic groups, M:F about 1.5:1 Second most common neurodegenerative disease Genetics role greater
BRAIN STEM CASE HISTORIES CASE HISTORY VII
 463 Brain stem Case history BRAIN STEM CASE HISTORIES CASE HISTORY VII A 60 year old man with hypertension wakes one morning with trouble walking. He is feeling dizzy and is sick to his stomach. His wife
463 Brain stem Case history BRAIN STEM CASE HISTORIES CASE HISTORY VII A 60 year old man with hypertension wakes one morning with trouble walking. He is feeling dizzy and is sick to his stomach. His wife
Sensory Trick in Task Specific Upper Limb Dystonia (ULD)
") UNIVERSITÀ DEGLI STUDI DI CAGLIARI Dipartimento di Scienze Mediche e Sanità Pubblica Scuola di Specializzazione in Neurologia Direttore: Prof. Giovanni Defazio Sensory Trick in Task Specific Upper Limb
UNIVERSITÀ DEGLI STUDI DI CAGLIARI Dipartimento di Scienze Mediche e Sanità Pubblica Scuola di Specializzazione in Neurologia Direttore: Prof. Giovanni Defazio Sensory Trick in Task Specific Upper Limb