When and how to perform a secondary hypertension work up? Docteur Cédric RAFAT Urgences Néphrologiques et Transplantation rénale Hôpital TENON
|
|
|
- Clarissa Walters
- 5 years ago
- Views:
Transcription


1 When and how to perform a secondary hypertension work up? Docteur Cédric RAFAT Urgences Néphrologiques et Transplantation rénale Hôpital TENON
2 Conflict of interest None related to the topic

3 When to look for secondary hypertension?.why look for secondary hypertension AHT avec SAP > 180 and/or DAP > 130 Severe AHT? Accelerated AHT or «malignant hypertension» Resistant AHT Young patient < 30 yo Curable AHT? Hypokalemia JNC7, ESH, HAS Recommendations
4 Causes of AHT II AHT Drug / toxic associated AHT Sleep apnea syndrome Primary hyperaldosteronism Renal vascular disease Pheochromocytoma/paraganglioma Cushing disease Chronic kidney disease Genetic AHT
 Licorice Grapefruit Serotonine/ norepinephrin recapture inhibitor Café EPO Anti-VEGF therapy Estrogen based contraception Farese NEJM 1991, Grossman Eur J")
5 Drug/toxic associated AHT Drug causing AHT Toxic related AHT Anti HTA drug interaction NSAID Cocaine +/- NSAID Glucocorticoids Phenythelamine Ketoconazole CNI inhibitors (ciclosporine ++) Licorice Grapefruit Serotonine/ norepinephrin recapture inhibitor Café EPO Anti-VEGF therapy Estrogen based contraception Farese NEJM 1991, Grossman Eur J Pharmaco 2015
6 Causes of AHT II AHT Drug / toxic associated AHT Sleep apnea syndrome Primary hyperaldosteronism Renal vascular disease Pheochromocytoma/PGL Cushing disease Chronic kidney disease Genetic AHT


7 Obstructive sleep apnea and AHT: an epidemiological conundrum Obstructive sleep apnea Arterial hypertension AHT /OSA patients : 35-80%, «Dose-effect» AHI>30 AHT>67% OSA/ AHT patients: ~40%, «Dose-effect» Resistant AHT OSA 65% Nieto JAMA 2000 Gonzaga Hypertension 2011
8 Obstructive sleep apnea and AHT The physiopathological chain reaction Systemic inflammation Heart rate OSA Hypoxemia Hypercapnia Oxydative stress Endothelial dysfunction Σ nerve & RAAS activation Peripheral arterial resistance Arterial stiffness AHT Cai Hypertension Research

9 OSA as a common cause of AHT Age > 50 y Neck circumference Snoring Pedrosa Hypertension 2011
10 Causes of AHT II AHT Drug / toxic associated AHT Sleep apnea syndrome Primary hyperaldosteronism Renal vascular disease Pheochromocytoma/PGL Cushing disease Chronic kidney disease Genetic AHT


11 Primary hyperaldosteronism 12% < 1% 10,5 % Rossi JACC 2006 Gordon Clin Exp Pharmaco 1993 Mulatero JCEM 2004 The prevalence of PA is on the rise The likeliness of PA increases with the severity of AHT Resistent AHT SBP > 180 mmhg Severe consequences Adenoma 10 mm Widespread use of Aldostérone/rénine ratio
12 Primary hyperaldosteronism PA cannot be ruled out on the basis of normokalemia Rossi JACC 2006






13 Primary hyperaldosteronism : diagnostic strategy 1. Wash out of anti AHT drug interference 2 weeks Beta blocker Diuretics Angiotensinogen Renin Renin inhibitor Normokalemia restored Normalt salt intakes 6 weeks Angiotensinogen I ACE Angiotensinogen II Sartan 2 weeks 2 weeks ACE inhibitor Kalemia Aldosterone 6 weeks Spironolactone Mineralocorticoid inhibitor

14 Primary hyperaldosteronism : diagnostic strategy 1. Aldosterone/ renin ratio (ARR) Morning > 2 h wake, sitting 2. Urine aldosterone / 24 h 3. Sodium loading test Direct renin = Renin C +++ Better standardized Plasma renin activity = PRA +/- Time consuming Adrenal CT with CI Surgery if signs of malignancy 1.< 55 yo AND 2. Cleared for surgery Adrenal venous catheter sampling Drug therapy if no lateralization Surgery if lateralized
 Cort adrenal vein / Cort inferior vena cava > 2")

15 Primary hyperaldosteronism : Adrenal venous catheterism sampling Selectivity criteria : cortisol sampling (Cort) Cort adrenal vein / Cort inferior vena cava > 2 Lateralization : cortisol and aldosterone (Ald sampling) Aldo/Cort dominant side /Aldo/Cort non dominant side > 4 Steichen Curr Opin in endoc 2016 Giachetti trends in metabo 2008


16 Adrenal venous sampling.to avoid : Primary hyperaldosteronism in a 63 yo patient. Das G Endoc Diabetes & Metabo 2015
17 Causes of AHT II AHT Drug / toxic associated AHT Sleep apnea syndrome Primary hyperaldosteronism Renal vascular disease Pheochromocytoma/PGL Cushing disease Chronic kidney disease Genetic AHT
 No CV Risk Factors +/- Carotid FMD, other middle")

18 Renal vascular disease 65 yo Caucasian Multiple CV Risk Factors +/- Ischemic cardiomyopathy, peripheral vascular disease yo Female (90%) No CV Risk Factors +/- Carotid FMD, other middle sized vessels (35% 2) Relationship with coronary dissection Renal atheromatous stenosis Renal fibromuscular dysplasia Courtesy of Dr E. Vidal-Petiot, HEGP Presad Am j cardiol 2015 Olin Circulation 2012

19 Renal Artery Stenting with a a special focus on the CORAL and ASTRAL trials ASTRAL CORAL Primary outcome Renal function The occurrence of a major cardiovascular or renal event Enrolment protocol Uncontrolled or refractory AHT Unexplained renal dysfunction «Substantial» RAS 750 patients SAP>155 mmhg 2 antihypertensive medications. SAR > 60% 947 patients Death HR: 0.90; p=0.61 HR: 0.80; p=0.20 Major cardiov events HR= 0.94; p= 0.88 HR= 0.97; p=0.88. Renal events HR= 0.97; p=0.88 Progressive renal insufficiency. HR= 0.86; p = 0.34 Blood pressure Revascularization: 141 ± 26/73 ± 12 Medical: 141 ± 25/70 ± 13 ns Systolic BP decreased in: Revascularization: 15.6 ± 25.8 Medical: 16.2 ±21.2 ; p=0.03



20 Ongoing controversies White Cath and cardio int 2010 Serac semin in vasc Surg 2011




21 When should renal revascularization should be contemplated? Initial diagnostic work-up «Flash» pulmonary Edema GFR / ACE inhibitor Multidrug resistance & significant RAS Follow-up Accelerated renal dysfunction Renal atrophy?? Beware!! Renal atrophy Significant proteinuria Distal renal vascular disease Rooke circulation 2011



22 Renal Fibromuscular dysplasia : typical and less typical presentations PHACTR1 variant?? Estrogens? Others? Multifocal Monofocal Renal vascular Aneurysm 30% Renal vascular Dissection 10% Other localization? Plouin Neph Ther 2015 Kadian Dodov JACC 2016 Kiando Plos genet 2016

23 Diagnostic screening strategy in renal fibromuscular dysplasia Renal doppler US AHT young F CT scan or angio MRI Negative exam AND strong suspicion Cervical FMD Renal infarct Abdominal bruit Negative exam AND strong suspicion Positive exam Renal angiography Angioplasty Positive exam Positive exam Cervico-cerebrovascular CT or MRI
24 Causes of AHT II AHT Drug / toxic associated AHT Sleep apnea syndrome Primary hyperaldosteronism Renal vascular disease Pheochromocytoma/PGL Cushing disease Chronic kidney disease Genetic AHT

25 Pheochromocytoma/PGL when to look for it? Rare cause of AHT 0,1-0,6% AHT patients Headache 60 90% Palpitations 50 70% Sweating 55 75% Pallor 40 45% Nausea 20 40% Flushing 10 20% Weight loss 20 40% Tiredness 25 40% Psychological symptoms 20-40% Sustained hypertension 50 60% Paroxysmal hypertension 10-30% Orthostatic hypotension 10 50% Hyperglycaemia 40% Family history Incidentaloma Young patients Clinical signs & Paroxysmal AHT (after anesthesia/surgery ++) Refractory AHT Hyperglycemia Lenders Lancet 2005
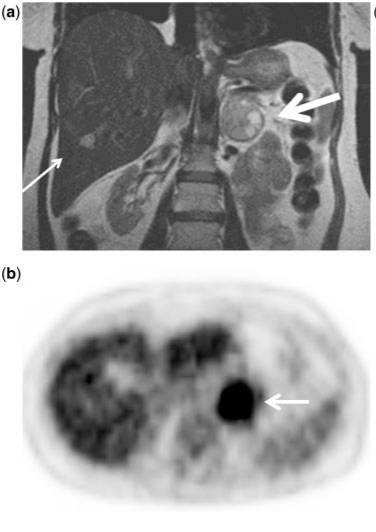
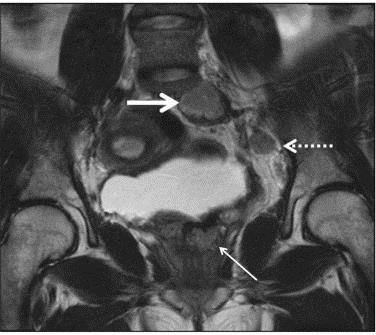
26 Pheochromocytoma/PGL where to look for it? 10% extra adrenal 10% malignant Baez Cancer imaging 2012


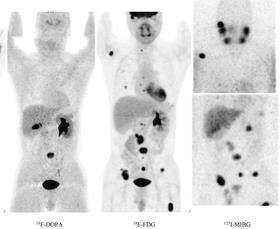
27 Pheochromocytoma/PGL, how to look for it? Urinary free metanephrines and normetanephrines MN+NMN/CreatU < 0,354 µmol/mmol Plasma free metanephrines and normetanephrines Anatomical imaging CT scan ++ or MRI Functional imaging 123 MIBG, 18 FDG PET Life long follow up Surgery Genetic testing NF1, VHL, RET, SDHB,SDHC ou SDHD.. Familial/sporadic Benign/malignant
28 Causes of AHT II AHT Drug / toxic associated AHT Sleep apnea syndrome Primary hyperaldosteronism Renal vascular disease Pheochromocytoma/PGL Cushing disease Chronic kidney disease Genetic AHT


29 Hypercortisolism : who should undergo testing and how? Rare cause of AHT i= / 10 6 p per Y Cushing syndrome Incidentaloma Young patients with unusual features Osteoporosis HTA 24 hour urinary free cortisol X 2 Cyclical Cushing syndrome, pregnancy Late night salivary cortisol X 2 Incidentaloma 1 mg overnight DXM suppression test Stage IV/V CKD


 Confirmation of")

30 How to perform testing for Cushing s syndrome Urinary free cortisol X 2 Late night salivary cortisol X 2 1 mg overnight DXM suppression test Longer low dose suppression test (2mg/48 h) Exclude non-cushing related clinical hypercortisolism Morbid obesity Alcohol Depression Poorly controled DM Exclude non-cushing related biological hypercortisolism Physical stress, surgery Exclude drugs which interfere with GC metabolism (CYP3A4) Confirmation of Cushing syndrome Expert endocrinologist Reference centre ACTH dependent/independent Cushing syndrome Complications and treatment Wong W J of radio 2016 Lim An ped J endoc dis 2014
Secondary Hypertension: A Real World Approach
 Secondary Hypertension: A Real World Approach Evan Brittain, MD December 7, 2012 Kingston, Jamaica Disclosures None Real World Causes Renovascular Hypertension Endocrine Obstructive Sleep Apnea Pseudosecondary
Secondary Hypertension: A Real World Approach Evan Brittain, MD December 7, 2012 Kingston, Jamaica Disclosures None Real World Causes Renovascular Hypertension Endocrine Obstructive Sleep Apnea Pseudosecondary
How to Recognize Adrenal Disease
 How to Recognize Adrenal Disease CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi
How to Recognize Adrenal Disease CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi
How do I investigate suspected secondary hypertension? Marie Freel RCP Update in Medicine 23 rd November 2016
 How do I investigate suspected secondary hypertension? Marie Freel RCP Update in Medicine 23 rd November 2016 World beaters..! Michel Joffres et al. BMJ Open 2013;3:e003423 Hypertension often poorly controlled
How do I investigate suspected secondary hypertension? Marie Freel RCP Update in Medicine 23 rd November 2016 World beaters..! Michel Joffres et al. BMJ Open 2013;3:e003423 Hypertension often poorly controlled
Endocrine. Endocrine as it relates to the kidney. Sarah Elfering, MD University of Minnesota
 Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
Approach to patient with hypertension. Dr. Amitesh Aggarwal
 Approach to patient with hypertension Dr. Amitesh Aggarwal Definition A systolic blood pressure ( SBP) >139 mmhg and/or A diastolic (DBP) >89 mmhg. Based on the average of two or more properly measured,
Approach to patient with hypertension Dr. Amitesh Aggarwal Definition A systolic blood pressure ( SBP) >139 mmhg and/or A diastolic (DBP) >89 mmhg. Based on the average of two or more properly measured,
Primary Aldosteronism: screening, diagnosis and therapy
 Primary Aldosteronism: screening, diagnosis and therapy Jacques W.M. Lenders, internist DEPT. OF INTERNAL MEDICINE, RADBOUD UNIVERSITY NIJMEGEN MEDICAL CENTER, NIJMEGEN,THE NETHERLANDS DEPT. OF INTERNAL
Primary Aldosteronism: screening, diagnosis and therapy Jacques W.M. Lenders, internist DEPT. OF INTERNAL MEDICINE, RADBOUD UNIVERSITY NIJMEGEN MEDICAL CENTER, NIJMEGEN,THE NETHERLANDS DEPT. OF INTERNAL
Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone
 Disease of the Adrenals 1 Zona Glomerulosa Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone leads to salt
Disease of the Adrenals 1 Zona Glomerulosa Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone leads to salt
SECONDARY HYPERTENSION
 SECONDARY HYPERTENSION Grand round for Medical student 25 October 2013 By Rungnapa Laortanakul, MD. OUTLINE Overview of HT Secondary HT Resistance HT Primary aldosteronism Pheochromocytoma Cushing s syndrome
SECONDARY HYPERTENSION Grand round for Medical student 25 October 2013 By Rungnapa Laortanakul, MD. OUTLINE Overview of HT Secondary HT Resistance HT Primary aldosteronism Pheochromocytoma Cushing s syndrome
RESISTENT HYPERTENSION. Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University
 RESISTENT HYPERTENSION Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University Resistant Hypertension Blood pressure remaining above goal in spite of concurrent use of 3 antihypertensive
RESISTENT HYPERTENSION Dr. Helmy Bakr Professor and Head of Cardiology Dept. Mansoura University Resistant Hypertension Blood pressure remaining above goal in spite of concurrent use of 3 antihypertensive
Primary Aldosteronism
 Primary Aldosteronism Odelia Cooper, MD Assistant Professor of Medicine Division of Endocrinology, Diabetes, and Metabolism Cedars-Sinai Medical Center HYPERTENSION CENTER Barriers to diagnosing primary
Primary Aldosteronism Odelia Cooper, MD Assistant Professor of Medicine Division of Endocrinology, Diabetes, and Metabolism Cedars-Sinai Medical Center HYPERTENSION CENTER Barriers to diagnosing primary
How to approach resistant hypertension. Teh-Li Huo, M.D., Ph.D.
 How to approach resistant hypertension Teh-Li Huo, M.D., Ph.D. BP goals No risk factors:
How to approach resistant hypertension Teh-Li Huo, M.D., Ph.D. BP goals No risk factors:
A CASE OF HYPERTENSION AND ACUTE RENAL FAILURE OBJECTIVES
 A CASE OF HYPERTENSION AND ACUTE RENAL FAILURE Maricel Pilapil-Pureza WLA Nephrology OBJECTIVES After the presentation, the attendee will be able to: 1. Discuss when to suspect for secondary causes of
A CASE OF HYPERTENSION AND ACUTE RENAL FAILURE Maricel Pilapil-Pureza WLA Nephrology OBJECTIVES After the presentation, the attendee will be able to: 1. Discuss when to suspect for secondary causes of
Treating Hypertension from
 Treating Hypertension from Initiation to Resistance: A Case Study Approach Michelle Krause, MD Division of Nephrology University of Arkansas for Medical Sciences Central Arkansas Veteran s Healthcare System
Treating Hypertension from Initiation to Resistance: A Case Study Approach Michelle Krause, MD Division of Nephrology University of Arkansas for Medical Sciences Central Arkansas Veteran s Healthcare System
Current Role of Renal Artery Stenting in Patients with Renal Artery Stenosis
 Current Role of Renal Artery Stenting in Patients with Renal Artery Stenosis Young-Guk Ko, M.D. Severance Cardiovascular Hospital, Yonsei University College of Medicine, Seoul, Korea Etiology Fibromuscular
Current Role of Renal Artery Stenting in Patients with Renal Artery Stenosis Young-Guk Ko, M.D. Severance Cardiovascular Hospital, Yonsei University College of Medicine, Seoul, Korea Etiology Fibromuscular
Approach to Adrenal Incidentaloma. Alice Y.Y. Cheng, MD, FRCP
 Approach to Adrenal Incidentaloma Alice Y.Y. Cheng, MD, FRCP Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
Approach to Adrenal Incidentaloma Alice Y.Y. Cheng, MD, FRCP Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
Systemic Hypertension Dr ahmed almutairi Assistant professor Internal medicine dept
 Systemic Hypertension Dr ahmed almutairi Assistant professor Internal medicine dept Continents 1- introduction 2- classification/definition 3- classification/etiology 4-etiology in both categories 5- complications
Systemic Hypertension Dr ahmed almutairi Assistant professor Internal medicine dept Continents 1- introduction 2- classification/definition 3- classification/etiology 4-etiology in both categories 5- complications
Jared Moore, MD, FACP
 Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
The European Consensus on Fibromuscular Dysplasia
 The European Consensus on Fibromuscular Dysplasia Alexandre Persu, M.D.-PhD Cardiology Department Cliniques Universitaires Saint-Luc Catholic University of Louvain Brussels, Belgium Eur J Clin Invest.
The European Consensus on Fibromuscular Dysplasia Alexandre Persu, M.D.-PhD Cardiology Department Cliniques Universitaires Saint-Luc Catholic University of Louvain Brussels, Belgium Eur J Clin Invest.
Hypertension in the very old. Objectives: Clinical Perspective
 Harvard Medical School Hypertension in the very old Ihab Hajjar, MD, MS, AGSF Associate Director, CV Research Lab Assistant Professor of Medicine, Harvard Medical School Objectives: Describe the clinical
Harvard Medical School Hypertension in the very old Ihab Hajjar, MD, MS, AGSF Associate Director, CV Research Lab Assistant Professor of Medicine, Harvard Medical School Objectives: Describe the clinical
Duplex Ultrasound of the Renal Arteries. Duplex Ultrasound. In the Beginning
 Duplex Ultrasound of the Renal Arteries DIMENSIONS IN HEART AND VASCULAR CARE 2013 PENN STATE HEART AND VASCULAR INSTITUTE ROBERT G. ATNIP MD PROFESSOR OF SURGERY AND RADIOLOGY Duplex Ultrasound Developed
Duplex Ultrasound of the Renal Arteries DIMENSIONS IN HEART AND VASCULAR CARE 2013 PENN STATE HEART AND VASCULAR INSTITUTE ROBERT G. ATNIP MD PROFESSOR OF SURGERY AND RADIOLOGY Duplex Ultrasound Developed
Management of Hypertension. M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine
 Division of Nephrology University of Missouri School of Medicine") Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Pharmacologic Management of Hypertension
 Current Concepts In Management of Fernando Vega, MD Secondary - Definition Renovascular Disease (The kidney doesn t get impressed by blood pressure) Renovascular stenosis Renal artery stenosis Fibromuscular
Current Concepts In Management of Fernando Vega, MD Secondary - Definition Renovascular Disease (The kidney doesn t get impressed by blood pressure) Renovascular stenosis Renal artery stenosis Fibromuscular
Adrenal incidentaloma guideline for Northern Endocrine Network
 Adrenal incidentaloma guideline for Northern Endocrine Network Definition of adrenal incidentaloma Adrenal mass detected on an imaging study done for indications that are not related to an adrenal problem
Adrenal incidentaloma guideline for Northern Endocrine Network Definition of adrenal incidentaloma Adrenal mass detected on an imaging study done for indications that are not related to an adrenal problem
Coral Trials: A personal experience that challenges its results in patients with uncontrolled blood pressure.
 Coral Trials: A personal experience that challenges its results in patients with uncontrolled blood pressure.. Dr. Javier Ruiz Aburto, FACS, FICS Assistant Professor Ponce School of Medicine Puerto Rico
Coral Trials: A personal experience that challenges its results in patients with uncontrolled blood pressure.. Dr. Javier Ruiz Aburto, FACS, FICS Assistant Professor Ponce School of Medicine Puerto Rico
Renal artery stenosis
 Renal artery stenosis Dr. Alexander Woywodt Consultant Renal Physician, Royal Preston Hospital Preston, 31.10.2007 Menu anatomy of the renal arteries diseases of the large renal arteries atherosclerotic
Renal artery stenosis Dr. Alexander Woywodt Consultant Renal Physician, Royal Preston Hospital Preston, 31.10.2007 Menu anatomy of the renal arteries diseases of the large renal arteries atherosclerotic
Renal Intervention. Douglas E. Drachman, MD, FSCAI Division of Cardiology Vascular Medicine Section December 9, 2014
 Renal Intervention Douglas E. Drachman, MD, FSCAI Division of Cardiology Vascular Medicine Section December 9, 2014 Disclosure Information Douglas E. Drachman, MD, FACC Abbott Vascular, Inc.: Advisory
Renal Intervention Douglas E. Drachman, MD, FSCAI Division of Cardiology Vascular Medicine Section December 9, 2014 Disclosure Information Douglas E. Drachman, MD, FACC Abbott Vascular, Inc.: Advisory
Year 2004 Paper two: Questions supplied by Megan 1
 Year 2004 Paper two: Questions supplied by Megan 1 QUESTION 96 A 32yo woman if found to have high blood pressure (180/105mmHg) at an insurance medical examination. She is asymptomatic. Clinical examination
Year 2004 Paper two: Questions supplied by Megan 1 QUESTION 96 A 32yo woman if found to have high blood pressure (180/105mmHg) at an insurance medical examination. She is asymptomatic. Clinical examination
Endocrine Hypertension
 Endocrine Hypertension 1 No Disclosures Endocrine Hypertension Objectives: 1. Understand Endocrine disorders causing hypertension 2. Understand clinical presentation of Pheochromocytoma and Hyperaldosteronism
Endocrine Hypertension 1 No Disclosures Endocrine Hypertension Objectives: 1. Understand Endocrine disorders causing hypertension 2. Understand clinical presentation of Pheochromocytoma and Hyperaldosteronism
Audience Response. Hypertension. Case: Mr. J. Measuring BP. Non-pharmacologic intervention. Case: Mr. J. Session ID: HTN411
 Audience Response http://rwpoll.com OR App downloads: Hypertension Chris Knight, MD cknight@uw.edu http://tiny.cc/rwiphone http://tiny.cc/rwdroid Session ID: HTN411 Case: Mr. J 52 y/o male patient comes
Audience Response http://rwpoll.com OR App downloads: Hypertension Chris Knight, MD cknight@uw.edu http://tiny.cc/rwiphone http://tiny.cc/rwdroid Session ID: HTN411 Case: Mr. J 52 y/o male patient comes
27 F with new onset hypertension and weight gain. Rajesh Jain Endorama 10/01/2015
 27 F with new onset hypertension and weight gain Rajesh Jain Endorama 10/01/2015 HPI 27 F with hypertension x 1 year BP 130-140/90 while on amlodipine 5 mg daily She also reports weight gain, 7 LB, mainly
27 F with new onset hypertension and weight gain Rajesh Jain Endorama 10/01/2015 HPI 27 F with hypertension x 1 year BP 130-140/90 while on amlodipine 5 mg daily She also reports weight gain, 7 LB, mainly
Renal Artery Disease. None > 65,000,000. Learning objectives: Renal Artery Disease
 Renal Artery Disease Robert D. McBane, M.D. Division of Cardiology Mayo Clinic Rochester Financial Disclosure Information Renal Artery Disease Robert McBane, MD None To appreciate: Learning objectives:
Renal Artery Disease Robert D. McBane, M.D. Division of Cardiology Mayo Clinic Rochester Financial Disclosure Information Renal Artery Disease Robert McBane, MD None To appreciate: Learning objectives:
ADRENAL INCIDENTALOMA. Jamii St. Julien
 ADRENAL INCIDENTALOMA Jamii St. Julien Outline Definition Differential Evaluation Treatment Follow up Questions Case Definition The phenomenon of detecting an otherwise unsuspected adrenal mass on radiologic
ADRENAL INCIDENTALOMA Jamii St. Julien Outline Definition Differential Evaluation Treatment Follow up Questions Case Definition The phenomenon of detecting an otherwise unsuspected adrenal mass on radiologic
Life After CORAL: What Did CORAL Prove? David Paul Slovut, MD, PhD Co-director TAVR, Dir of Advanced Intervention
 Life After CORAL: What Did CORAL Prove? David Paul Slovut, MD, PhD Co-director TAVR, Dir of Advanced Intervention No Relationships to Disclose The Need for Modern Renal Trials Increased rate of RAS diagnosis
Life After CORAL: What Did CORAL Prove? David Paul Slovut, MD, PhD Co-director TAVR, Dir of Advanced Intervention No Relationships to Disclose The Need for Modern Renal Trials Increased rate of RAS diagnosis
Hypertension: Who and How (and Why) to Investigate. Jessica Triay Andy Levy
 to Investigate. Jessica Triay Andy Levy") Hypertension: Who and How (and Why) to Investigate Jessica Triay Andy Levy What I'm not going to talk about Most Common: Renal Disease Renal USS Likely to be normal if bloods and urine normal Renal artery
Hypertension: Who and How (and Why) to Investigate Jessica Triay Andy Levy What I'm not going to talk about Most Common: Renal Disease Renal USS Likely to be normal if bloods and urine normal Renal artery
Hypertension Update. Objectives 4/28/2015. Beverly J. Mathis, D.O. OOA May 2015
 Hypertension Update Beverly J. Mathis, D.O. OOA May 2015 Objectives Learn new recommendations for BP treatment goals Approach to hypertension in the office Use of hypertensive drugs, and how to tailor
Hypertension Update Beverly J. Mathis, D.O. OOA May 2015 Objectives Learn new recommendations for BP treatment goals Approach to hypertension in the office Use of hypertensive drugs, and how to tailor
Hypertension Management Controversies in the Elderly Patient
 Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Chronic Pediatric Hypertension
 Chronic Pediatric Hypertension Nephrology Grand Round 3/13/2015 Mahmoud Kallash M.D Outline Definition of hypertension (HTN) Challenges in diagnosing HTN Epidemiology Causes and evaluation of HTN Management
Chronic Pediatric Hypertension Nephrology Grand Round 3/13/2015 Mahmoud Kallash M.D Outline Definition of hypertension (HTN) Challenges in diagnosing HTN Epidemiology Causes and evaluation of HTN Management
COMPLEX HYPERTENSION. Anita Ralstin, FNP-BC Next Step Health Consultant, LLC
 COMPLEX HYPERTENSION Anita Ralstin, FNP-BC Next Step Health Consultant, LLC Incidence Of Hypertension About 70 million American adults have high blood pressure. About 33% of the population Only 52% have
COMPLEX HYPERTENSION Anita Ralstin, FNP-BC Next Step Health Consultant, LLC Incidence Of Hypertension About 70 million American adults have high blood pressure. About 33% of the population Only 52% have
Adrenal Mass. Cynthia Kwong SUNY Downstate Medical Center Grand Rounds October 13, 2016
 Adrenal Mass Cynthia Kwong SUNY Downstate Medical Center Grand Rounds October 13, 2016 Case Presentation 65F found to have a 4cm left adrenal mass in 2012 now presents with 6.7cm left adrenal mass PMHx:
Adrenal Mass Cynthia Kwong SUNY Downstate Medical Center Grand Rounds October 13, 2016 Case Presentation 65F found to have a 4cm left adrenal mass in 2012 now presents with 6.7cm left adrenal mass PMHx:
ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ. Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH
 ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH Hypertension Co-Morbidities HTN Commonly Clusters with Other Risk
ΑΡΥΙΚΗ ΠΡΟΔΓΓΙΗ ΤΠΔΡΣΑΙΚΟΤ ΑΘΔΝΟΤ Μ.Β.Παπαβαζιλείοσ Καρδιολόγος FESC - Γιεσθύνηρια ιζμανόγλειον ΓΝΑ Clinical Hypertension Specialist ESH Hypertension Co-Morbidities HTN Commonly Clusters with Other Risk
Hypertension The normal radial artery blood pressures in adults are: Systolic arterial pressure: 100 to 140 mmhg. Diastolic arterial pressure: 60 to
 Hypertension The normal radial artery blood pressures in adults are: Systolic arterial pressure: 100 to 140 mmhg. Diastolic arterial pressure: 60 to 90 mmhg. These pressures are called Normal blood pressure
Hypertension The normal radial artery blood pressures in adults are: Systolic arterial pressure: 100 to 140 mmhg. Diastolic arterial pressure: 60 to 90 mmhg. These pressures are called Normal blood pressure
Cardiac Pathophysiology
 Cardiac Pathophysiology Evaluation Components Medical history Physical examination Routine laboratory tests Optional tests Medical History Duration and classification of hypertension. Patient history of
Cardiac Pathophysiology Evaluation Components Medical history Physical examination Routine laboratory tests Optional tests Medical History Duration and classification of hypertension. Patient history of
The Work-up and Treatment of Adrenal Nodules
 The Work-up and Treatment of Adrenal Nodules Lawrence Andrew Drew Shirley, MD, MS, FACS Assistant Professor of Surgical-Clinical Department of Surgery Division of Surgical Oncology The Ohio State University
The Work-up and Treatment of Adrenal Nodules Lawrence Andrew Drew Shirley, MD, MS, FACS Assistant Professor of Surgical-Clinical Department of Surgery Division of Surgical Oncology The Ohio State University
Hypertension Update Warwick Jaffe Interventional Cardiologist Ascot Hospital
 Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Objectives. JNC 7 Is Nice But What s Up With JNC 8? Why Do We Care? Hypertension Background: Prevalence
 JNC 7 Is Nice But What s Up With JNC 8? 37 th Annual CAPA Conference October 4 th 2013 Ignacio de Artola, Jr. M.D. Assistant Professor of Clinical Family Medicine Medical Director, Primary Care Physician
JNC 7 Is Nice But What s Up With JNC 8? 37 th Annual CAPA Conference October 4 th 2013 Ignacio de Artola, Jr. M.D. Assistant Professor of Clinical Family Medicine Medical Director, Primary Care Physician
Adrenal Incidentaloma Management
 Adrenal Incidentaloma Management Full Title of Guideline: Author Management of Incidentally-discovered Adrenal Lesions ( Incidentalomas ) Mr David Chadwick Consultant Endocrine Surgeon david.chadwick2@nuh.nhs.uk
Adrenal Incidentaloma Management Full Title of Guideline: Author Management of Incidentally-discovered Adrenal Lesions ( Incidentalomas ) Mr David Chadwick Consultant Endocrine Surgeon david.chadwick2@nuh.nhs.uk
Secondary hypertension is defined as being
 Canadian Coalation for High Blood Pressure Prevention and Control Coalition Canadienne pour la Prévention et le Contrôle de l Hypertension Artérielle Secondary Hypertension: Diagnosis and Management Options
Canadian Coalation for High Blood Pressure Prevention and Control Coalition Canadienne pour la Prévention et le Contrôle de l Hypertension Artérielle Secondary Hypertension: Diagnosis and Management Options
Difficult-to-Control & Resistant Hypertension. Anthony Viera, MD, MPH, FAHA Professor and Chair
 Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
Updates in primary hyperaldosteronism and the rule
 Updates in primary hyperaldosteronism and the 20-50 rule I. David Weiner, M.D. Professor of Medicine and Physiology and Functional Genomics University of Florida College of Medicine and NF/SGVHS The 20-50
Updates in primary hyperaldosteronism and the 20-50 rule I. David Weiner, M.D. Professor of Medicine and Physiology and Functional Genomics University of Florida College of Medicine and NF/SGVHS The 20-50
Renal Artery Stenting
 Renal Artery Stenting J.P. Reilly, MD, FSCAI Ochsner Medical Center Speaker s bureau: Astra Zeneca and Lilly/Diachi Sankyo Prevalence of RAS is high in cath population. Renal artery intervention can help
Renal Artery Stenting J.P. Reilly, MD, FSCAI Ochsner Medical Center Speaker s bureau: Astra Zeneca and Lilly/Diachi Sankyo Prevalence of RAS is high in cath population. Renal artery intervention can help
SAURIN GANDHI, AZCOM Evidence-Based Guideline for the Management of High Blood Pressure in Adults (JNC 8)
") 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults (JNC 8) Background HTN is the most common condition seen in primary care and leads to MI, stroke, renal failure, and death
2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults (JNC 8) Background HTN is the most common condition seen in primary care and leads to MI, stroke, renal failure, and death
Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences. Endocrinology. (Review) Year 5 Internal Medicine
 Year 5 Internal Medicine") Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences Endocrinology (Review) Year 5 Internal Medicine Presented by: Dr. Mona Arekat Prepared by: Ali Jassim Alhashli Case (1):
Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences Endocrinology (Review) Year 5 Internal Medicine Presented by: Dr. Mona Arekat Prepared by: Ali Jassim Alhashli Case (1):
Endocrine hypertensionmolecules. Marie Freel Caledonian Endocrine Society Meeting 29 th November 2015
 Endocrine hypertensionmolecules and genes Marie Freel Caledonian Endocrine Society Meeting 29 th November 2015 Plan Mineralocorticoid hypertension Myths surrounding Primary Aldosteronism (PA) New developments
Endocrine hypertensionmolecules and genes Marie Freel Caledonian Endocrine Society Meeting 29 th November 2015 Plan Mineralocorticoid hypertension Myths surrounding Primary Aldosteronism (PA) New developments
2 Arterial Hypertension
 2 Arterial Hypertension Daniel A. Duprez CONTENTS KEY POINTS INTRODUCTION DEFINITION EPIDEMIOLOGY OF HYPERTENSION MECHANISMS OF HYPERTENSION ETIOLOGY OF HYPERTENSION COMPLICATED MANAGEMENT PROBLEMS IN
2 Arterial Hypertension Daniel A. Duprez CONTENTS KEY POINTS INTRODUCTION DEFINITION EPIDEMIOLOGY OF HYPERTENSION MECHANISMS OF HYPERTENSION ETIOLOGY OF HYPERTENSION COMPLICATED MANAGEMENT PROBLEMS IN
Hypertension Update Background
 Hypertension Update Background Overview Aaron J. Friedberg, MD Assistant Professor, Clinical Division of General Internal Medicine The Ohio State University Wexner Medical Center Management Guideline Comparison
Hypertension Update Background Overview Aaron J. Friedberg, MD Assistant Professor, Clinical Division of General Internal Medicine The Ohio State University Wexner Medical Center Management Guideline Comparison
Southern Derbyshire Shared Care Pathology Guidelines. Secondary Hypertension
 Southern Derbyshire Shared Care Pathology Guidelines Secondary Hypertension Purpose of Guideline This guideline covers the investigation and referral criteria of patients with suspected secondary causes
Southern Derbyshire Shared Care Pathology Guidelines Secondary Hypertension Purpose of Guideline This guideline covers the investigation and referral criteria of patients with suspected secondary causes
Endocrine MR. Jan 30, 2015 Michael LaFata, MD
 Endocrine MR Jan 30, 2015 Michael LaFata, MD Brief case 55-year-old female in ED PMH: HTN, DM2, HLD, GERD CC: Epigastric/LUQ abdominal pain, N/V x2 days AF, HR 103, BP 155/85, room air CMP: Na 133, K 3.6,
Endocrine MR Jan 30, 2015 Michael LaFata, MD Brief case 55-year-old female in ED PMH: HTN, DM2, HLD, GERD CC: Epigastric/LUQ abdominal pain, N/V x2 days AF, HR 103, BP 155/85, room air CMP: Na 133, K 3.6,
Diseases of the Adrenal gland
 Diseases of the Adrenal gland Adrenal insufficiency Cushing disease vs syndrome Pheochromocytoma Hyperaldostronism What are the layers of the adrenal gland?? And what does each layer produce?? What are
Diseases of the Adrenal gland Adrenal insufficiency Cushing disease vs syndrome Pheochromocytoma Hyperaldostronism What are the layers of the adrenal gland?? And what does each layer produce?? What are
Secondary hypertension How to approach?
 Secondary hypertension How to approach? Tomáš Seeman Department of Pediatrics and Transplantation Center, University Hospital Motol, 2 nd Faculty of Medicine, Charles University Prague, Czech Republic
Secondary hypertension How to approach? Tomáš Seeman Department of Pediatrics and Transplantation Center, University Hospital Motol, 2 nd Faculty of Medicine, Charles University Prague, Czech Republic
Hypertension Update. Aaron J. Friedberg, MD
 Hypertension Update Aaron J. Friedberg, MD Assistant Professor, Clinical Division of General Internal Medicine The Ohio State University Wexner Medical Center Background Diagnosis Management Overview Guideline
Hypertension Update Aaron J. Friedberg, MD Assistant Professor, Clinical Division of General Internal Medicine The Ohio State University Wexner Medical Center Background Diagnosis Management Overview Guideline
Hypertension Cases. Katharine Dahl, MD January 10, 2017
 Hypertension Cases Katharine Dahl, MD January 10, 2017 Dr. Dahl arrives late for her AHD hypertension lecture and you are asked to present the epidemiology of hypertension until she arrives. Which of the
Hypertension Cases Katharine Dahl, MD January 10, 2017 Dr. Dahl arrives late for her AHD hypertension lecture and you are asked to present the epidemiology of hypertension until she arrives. Which of the
Clarification of hypertension Diagnosis of primary hyperaldosteronism
 Nr. 1/2010 Clarification of hypertension Diagnosis of primary hyperaldosteronism Marc Beineke The significance of the /renin ratio (ARR) in the diagnosis of normoalaemic and hypokalaemic primary hyperaldosteronism,
Nr. 1/2010 Clarification of hypertension Diagnosis of primary hyperaldosteronism Marc Beineke The significance of the /renin ratio (ARR) in the diagnosis of normoalaemic and hypokalaemic primary hyperaldosteronism,
Circulation. Blood Pressure and Antihypertensive Medications. Venous Return. Arterial flow. Regulation of Cardiac Output.
 Circulation Blood Pressure and Antihypertensive Medications Two systems Pulmonary (low pressure) Systemic (high pressure) Aorta 120 mmhg Large arteries 110 mmhg Arterioles 40 mmhg Arteriolar capillaries
Circulation Blood Pressure and Antihypertensive Medications Two systems Pulmonary (low pressure) Systemic (high pressure) Aorta 120 mmhg Large arteries 110 mmhg Arterioles 40 mmhg Arteriolar capillaries
Diagnostic et prise en charge des phéochromocytomes (PH) et paragangliomes (PG)
 et paragangliomes (PG)") Diagnostic et prise en charge des phéochromocytomes (PH) et paragangliomes (PG) PF Plouin, L Amar et AP Gimenez-Roqueplo COMETE, ENS@T et HEGP/Université Paris-Descartes Chromaffin tumors: PH and PG PH
Diagnostic et prise en charge des phéochromocytomes (PH) et paragangliomes (PG) PF Plouin, L Amar et AP Gimenez-Roqueplo COMETE, ENS@T et HEGP/Université Paris-Descartes Chromaffin tumors: PH and PG PH
My favorite hypertensive patients. Entertaining you is Friedrich C. Luft
 My favorite hypertensive patients Entertaining you is Friedrich C. Luft 37 year-old woman with fairly severe hypertension Negative family history, normal pregnancy Receives HCTZ, Amlodipine, and Valsartan
My favorite hypertensive patients Entertaining you is Friedrich C. Luft 37 year-old woman with fairly severe hypertension Negative family history, normal pregnancy Receives HCTZ, Amlodipine, and Valsartan
Σύγτρονη θεραπεία της ανθεκτικής σπέρτασης
 Σύγτρονη θεραπεία της ανθεκτικής σπέρτασης Κώζηας Τζιούθης Α Παν/κή Καρ/κή Κλινική Ιπποκράηειο Γ.Ν.Α. Resistant or Refractory to treatment Hypertension Office BP>140/90 or 130/80 mm Hg in patients with
Σύγτρονη θεραπεία της ανθεκτικής σπέρτασης Κώζηας Τζιούθης Α Παν/κή Καρ/κή Κλινική Ιπποκράηειο Γ.Ν.Α. Resistant or Refractory to treatment Hypertension Office BP>140/90 or 130/80 mm Hg in patients with
Blood Pressure Treatment in 2018
 Blood Pressure Treatment in 2018 Jay D. Geoghagan, MD, FACC Disclosures: None 1 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/ APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management
Blood Pressure Treatment in 2018 Jay D. Geoghagan, MD, FACC Disclosures: None 1 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/ APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management
Update in Pheochromocytoma/Paraganglioma: Focus on Diagnosis and Management
 Update in Pheochromocytoma/Paraganglioma: Focus on Diagnosis and Management Ohk-Hyun Ryu, MD. Associate Professor, Department of Internal Medicine Division of Endocrinology and Metabolism College of Medicine,
Update in Pheochromocytoma/Paraganglioma: Focus on Diagnosis and Management Ohk-Hyun Ryu, MD. Associate Professor, Department of Internal Medicine Division of Endocrinology and Metabolism College of Medicine,
JESFC 2016 FLASH ACTUALITÉ HTA Bilan étiologique de l'hta : dosages hormonaux toujours avant l'imagerie?
 JESFC 2016 FLASH ACTUALITÉ HTA Bilan étiologique de l'hta : dosages hormonaux toujours avant l'imagerie? Etiology of hypertension : hormonal assays always before imaging? 16 JANVIER 2016 Bernard CHAMONTIN
JESFC 2016 FLASH ACTUALITÉ HTA Bilan étiologique de l'hta : dosages hormonaux toujours avant l'imagerie? Etiology of hypertension : hormonal assays always before imaging? 16 JANVIER 2016 Bernard CHAMONTIN
Difficult to Control HTN: It is not all the same. Structured approach to evaluation and treatment
 Difficult to Control HTN: It is not all the same. Structured approach to evaluation and treatment Dmitri Vasin M.D. Nephrologist and ASH certified clinical hypertension specialist Bremerton, WA, USA Johnson
Difficult to Control HTN: It is not all the same. Structured approach to evaluation and treatment Dmitri Vasin M.D. Nephrologist and ASH certified clinical hypertension specialist Bremerton, WA, USA Johnson
Joshua M. Crasner,DO,FACC,FACOI
 Joshua M. Crasner,DO,FACC,FACOI 50 million people USA SBP>115 incr risk CAD/CVA Q 20mm incr=2x risk JNC-8 almost changed aggressive Tx Pseudo-HTN Hypertension 2015 2 Most common HBP( > 90 %)--multifactorial
Joshua M. Crasner,DO,FACC,FACOI 50 million people USA SBP>115 incr risk CAD/CVA Q 20mm incr=2x risk JNC-8 almost changed aggressive Tx Pseudo-HTN Hypertension 2015 2 Most common HBP( > 90 %)--multifactorial
Hypertension. Most important public health problem in developed countries
 Hypertension Strategy for Continued Success in Treatment for the 21st Century November 15, 2005 Arnold B. Meshkov, M.D. Associate Professor of Medicine Temple University School of Medicine Philadelphia,
Hypertension Strategy for Continued Success in Treatment for the 21st Century November 15, 2005 Arnold B. Meshkov, M.D. Associate Professor of Medicine Temple University School of Medicine Philadelphia,
A case of hypokalemia MIHO TAGAWA FIRST DEPARTMENT OF MEDICINE NARA MEDICAL UNIVERSITY
 A case of hypokalemia MIHO TAGAWA FIRST DEPARTMENT OF MEDICINE NARA MEDICAL UNIVERSITY Case 57 y.o. male CC: Weakness HPI: About 20 years ago, he developed bilateral lower extremity weakness. Laboratory
A case of hypokalemia MIHO TAGAWA FIRST DEPARTMENT OF MEDICINE NARA MEDICAL UNIVERSITY Case 57 y.o. male CC: Weakness HPI: About 20 years ago, he developed bilateral lower extremity weakness. Laboratory
Fibromuscular Dysplasia. Miranda Forrest Baker College
 Fibromuscular Dysplasia Miranda Forrest Baker College Overview Case Study Patient Information Exam Images Findings FMD Types Signs and Symptoms Treatment Case Study Patient Information Female 57 years
Fibromuscular Dysplasia Miranda Forrest Baker College Overview Case Study Patient Information Exam Images Findings FMD Types Signs and Symptoms Treatment Case Study Patient Information Female 57 years
HYPERTENSIVE VASCULAR DISEASE
 HYPERTENSIVE VASCULAR DISEASE Cutoffs in diagnosing hypertension in clinical practice sustained diastolic pressures >90 mm Hg, or sustained systolic pressures >140 mm Hg Malignant hypertension A small
HYPERTENSIVE VASCULAR DISEASE Cutoffs in diagnosing hypertension in clinical practice sustained diastolic pressures >90 mm Hg, or sustained systolic pressures >140 mm Hg Malignant hypertension A small
Upon completion, participants should be able to:
 Learning Objectives Upon completion, participants should be able to: Describe the causes of secondary hypertension and the prevalence of primary aldosteronism Discuss the diagnostic approach to primary
Learning Objectives Upon completion, participants should be able to: Describe the causes of secondary hypertension and the prevalence of primary aldosteronism Discuss the diagnostic approach to primary
Renovascular hypertension in children and adolescents
 Renovascular hypertension in children and adolescents M I E C Z Y S L AW L I T W I N D E P T. O F N E P H R O LO G Y & A R T E R I A L H Y P E R T E N S I O N T H E C H I L D R E N S M E M O R I A L H
Renovascular hypertension in children and adolescents M I E C Z Y S L AW L I T W I N D E P T. O F N E P H R O LO G Y & A R T E R I A L H Y P E R T E N S I O N T H E C H I L D R E N S M E M O R I A L H
AVS and IPSS: The Basics and the Pearls
 AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2018 Mayo Foundation for Medical Education and Research.
AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2018 Mayo Foundation for Medical Education and Research.
HYPERTENSION IN CKD. LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL
 HYPERTENSION IN CKD LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL Stages in Progression of Chronic Kidney Disease and Therapeutic Strategies Complications Normal Increased risk Damage GFR
HYPERTENSION IN CKD LEENA ONGAJYOOTH, M.D., Dr.med RENAL UNIT SIRIRAJ HOSPITAL Stages in Progression of Chronic Kidney Disease and Therapeutic Strategies Complications Normal Increased risk Damage GFR
Updates in primary hyperaldosteronism and the rule
 Updates in primary hyperaldosteronism and the 20-50 rule I. David Weiner, M.D. C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University of
Updates in primary hyperaldosteronism and the 20-50 rule I. David Weiner, M.D. C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University of
Incidental Adrenal Nodules Differential Diagnosis
 Adrenal Stuff Richard J. Auchus, MD, PhD, FACE Division of Metabolism, Endocrinology & Diabetes Departments of Internal Medicine & Pharmacology University of Michigan/VA Ann Arbor Incidental Adrenal Nodules
Adrenal Stuff Richard J. Auchus, MD, PhD, FACE Division of Metabolism, Endocrinology & Diabetes Departments of Internal Medicine & Pharmacology University of Michigan/VA Ann Arbor Incidental Adrenal Nodules
AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA
 AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2016 Mayo Foundation for Medical Education and Research.
AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2016 Mayo Foundation for Medical Education and Research.
USMLE PREP LECTURE SERIES Lecture 2.2
 USMLE PREP LECTURE SERIES Lecture 2.2 Elite Medical Prep Guide for Ben Gurion Students from Day 1 to Test day Last Updated: January 17, 2019. Delivered: January 17, 2019 Objectives 5 month planning Flashcards:
USMLE PREP LECTURE SERIES Lecture 2.2 Elite Medical Prep Guide for Ben Gurion Students from Day 1 to Test day Last Updated: January 17, 2019. Delivered: January 17, 2019 Objectives 5 month planning Flashcards:
Renal Artery Denervation New Concepts in Hypertension Treatment
 Renal Artery Denervation New Concepts in Hypertension Treatment Istanbul Course of Interventional Cardiology J. Weil Medizinische Klinik II Kardiologie, Angiologie und internistische Intensivmedizin Universitätsklinikum,
Renal Artery Denervation New Concepts in Hypertension Treatment Istanbul Course of Interventional Cardiology J. Weil Medizinische Klinik II Kardiologie, Angiologie und internistische Intensivmedizin Universitätsklinikum,
 Hypertension Epidemiology 6% of deaths worldwide Defined as any of the following: systolic blood pressure 140 mmhg, diastolic blood pressure 90 mmhg, taking antihypertensive medications Pulse pressure=
Hypertension Epidemiology 6% of deaths worldwide Defined as any of the following: systolic blood pressure 140 mmhg, diastolic blood pressure 90 mmhg, taking antihypertensive medications Pulse pressure=
Genetic factors. A number of genetic factors or interactions between genes play a major role in essential hypertension.
 Hypertension Blood pressure is a measurement of the force against the walls of your arteries as your heart pumps blood through your body. Hypertension is another term used to describe high blood pressure.
Hypertension Blood pressure is a measurement of the force against the walls of your arteries as your heart pumps blood through your body. Hypertension is another term used to describe high blood pressure.
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014
 HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
Fibromuscular Dysplasia (FMD) of the renal arteries Angiographic features and therapeutic options
 of the renal arteries Angiographic features and therapeutic options") Fibromuscular Dysplasia (FMD) of the renal arteries Angiographic features and therapeutic options Poster No.: C-0630 Congress: ECR 2012 Type: Educational Exhibit Authors: K. I. Ringe, B. Meyer, F. Wacker,
Fibromuscular Dysplasia (FMD) of the renal arteries Angiographic features and therapeutic options Poster No.: C-0630 Congress: ECR 2012 Type: Educational Exhibit Authors: K. I. Ringe, B. Meyer, F. Wacker,
- Dr Alia Shatnawi. 1 P a g e
 - 1 مها أبو عجمية - - - Dr Alia Shatnawi 1 P a g e A Skippable Intr0 Blood pressure normally decreases during the night. Absence of this phenomenon is called (nondipping) Wikipedia: Circadian rhythm....
- 1 مها أبو عجمية - - - Dr Alia Shatnawi 1 P a g e A Skippable Intr0 Blood pressure normally decreases during the night. Absence of this phenomenon is called (nondipping) Wikipedia: Circadian rhythm....
Primary aldosteronism clinical practice guidelines: a re-appraisal The Management of Primary Aldosteronism
 Primary aldosteronism clinical practice guidelines: a re-appraisal The Management of Primary Aldosteronism Prof. FRANCO MANTERO Division of Endocrinology University of Padua Italy Case Detection, Diagnosis
Primary aldosteronism clinical practice guidelines: a re-appraisal The Management of Primary Aldosteronism Prof. FRANCO MANTERO Division of Endocrinology University of Padua Italy Case Detection, Diagnosis
Hypertension Update. Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy
 Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
John Sutton, DO, FACOI, FACE, CCD. Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989
 John Sutton, DO, FACOI, FACE, CCD Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989 Gonadal Physiology and Disease 3 No Disclosures Gonadal Axis Hypothalamic-pituitary-gonadal Feedback mechanisms
John Sutton, DO, FACOI, FACE, CCD Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989 Gonadal Physiology and Disease 3 No Disclosures Gonadal Axis Hypothalamic-pituitary-gonadal Feedback mechanisms
Special Lecture 11/08/2013. Hypertension Dr. HN Mayrovitz
 Special Lecture 11/08/2013 Hypertension Dr. HN Mayrovitz Arterial Blood Pressure (ABP) Major Factors Summarized Sympathetic Hormones Arteriole MAP ~ Q x TPR + f (V / C) SV x HR Renal SBP Hypertension =
Special Lecture 11/08/2013 Hypertension Dr. HN Mayrovitz Arterial Blood Pressure (ABP) Major Factors Summarized Sympathetic Hormones Arteriole MAP ~ Q x TPR + f (V / C) SV x HR Renal SBP Hypertension =
Coronary Artery Manifestations of Fibromuscular Dysplasia: Infrequent and Easily Missed
 Coronary Artery Manifestations of Fibromuscular Dysplasia: Infrequent and Easily Missed Jeffrey W Olin, D.O., F.A.C.C., F.A.H.A. Professor of Medicine (Cardiology) Director of Vascular Medicine & Vascular
Coronary Artery Manifestations of Fibromuscular Dysplasia: Infrequent and Easily Missed Jeffrey W Olin, D.O., F.A.C.C., F.A.H.A. Professor of Medicine (Cardiology) Director of Vascular Medicine & Vascular
The endocrine system is made up of a complex group of glands that secrete hormones.
 1 10. Endocrinology I MEDCHEM 535 Diagnostic Medicinal Chemistry Endocrinology The endocrine system is made up of a complex group of glands that secrete hormones. These hormones control reproduction, metabolism,
1 10. Endocrinology I MEDCHEM 535 Diagnostic Medicinal Chemistry Endocrinology The endocrine system is made up of a complex group of glands that secrete hormones. These hormones control reproduction, metabolism,
Case Based Urology Learning Program
 Case Based Urology Learning Program Resident s Corner: UROLOGY Case Number 4 CBULP 2010 004 Case Based Urology Learning Program Editor: Associate Editors: Manager: Case Contributors: Steven C. Campbell,
Case Based Urology Learning Program Resident s Corner: UROLOGY Case Number 4 CBULP 2010 004 Case Based Urology Learning Program Editor: Associate Editors: Manager: Case Contributors: Steven C. Campbell,
LXIV: DRUGS: 4. RAS BLOCKADE
 LXIV: DRUGS: 4. RAS BLOCKADE ACE Inhibitors Components of RAS Actions of Angiotensin i II Indications for ACEIs Contraindications RAS blockade in hypertension RAS blockade in CAD RAS blockade in HF Limitations
LXIV: DRUGS: 4. RAS BLOCKADE ACE Inhibitors Components of RAS Actions of Angiotensin i II Indications for ACEIs Contraindications RAS blockade in hypertension RAS blockade in CAD RAS blockade in HF Limitations
The Management of adrenal incidentaloma
 The Management of adrenal incidentaloma Dimitrios Linos, MD Director of Surgery, Hygeia Hospital, Athens, Greece Consultant in Surgery, Massachusetts General Hospital, Boston, USA 8 th Postgraduate Course
The Management of adrenal incidentaloma Dimitrios Linos, MD Director of Surgery, Hygeia Hospital, Athens, Greece Consultant in Surgery, Massachusetts General Hospital, Boston, USA 8 th Postgraduate Course
DISCLOSURES OUTLINE OUTLINE 9/29/2014 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE
 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
Michael Meuse, M.D. Vascular and Interventional Radiology
 Michael Meuse, M.D. Vascular and Interventional Radiology Which patient would likely benefit from renal artery revascularization? Patient A- 60 y/o male with 20 year hx of htn; on 2 drug therapy for 10
Michael Meuse, M.D. Vascular and Interventional Radiology Which patient would likely benefit from renal artery revascularization? Patient A- 60 y/o male with 20 year hx of htn; on 2 drug therapy for 10