Adrenal Mass. Cynthia Kwong SUNY Downstate Medical Center Grand Rounds October 13, 2016
|
|
|
- Kelley Holland
- 5 years ago
- Views:
Transcription
1 Adrenal Mass Cynthia Kwong SUNY Downstate Medical Center Grand Rounds October 13, 2016
2 Case Presentation 65F found to have a 4cm left adrenal mass in 2012 now presents with 6.7cm left adrenal mass PMHx: HTN, arthritis, obstructive sleep apnea, morbid obesity PSHx: lap cholecystectomy, lap appendectomy, radical TAH-BSO, right total knee replacement Previous functional adrenal mass workup negative History of endometrial adenocarcinoma s/p radial TAH-BSO ECHO: EF 55-60% Underwent robot-assisted laparoscopic left adrenalectomy Pathology: myelolipoma
3
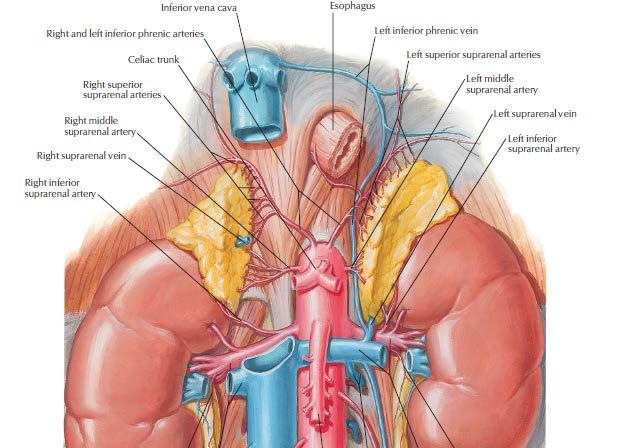
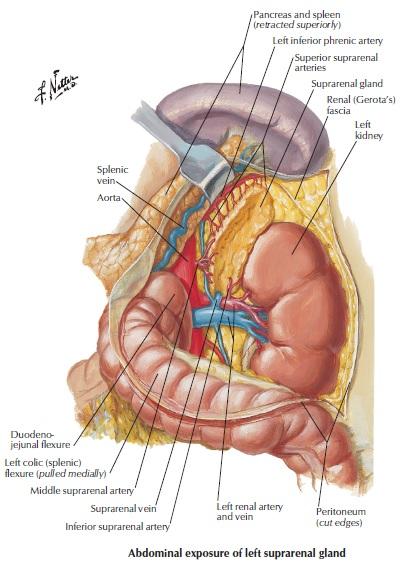
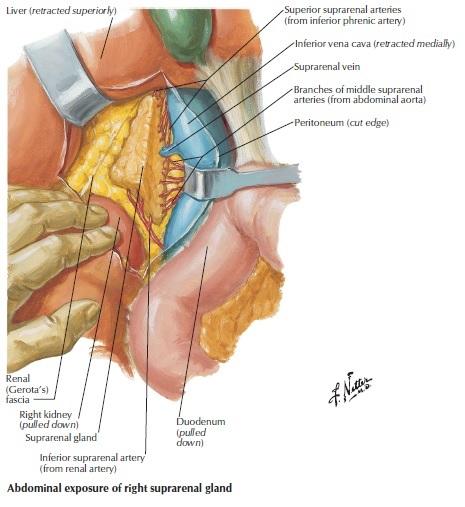
4 Adrenal Anatomy Arterial Supply Superior suprarenal artery branches off of the inferior phrenic artery Middle suprarenal artery branches off of the aorta Inferior suprarenal artery branches off of the renal artery Venous Drainage Right suprarenal vein drains into IVC Left suprarenal vein joins inferior phrenic vein and drains into left renal vein Lymph Drainage Drains into lumbar (aortic and caval) nodes
5
6
7
8 Physiology
9
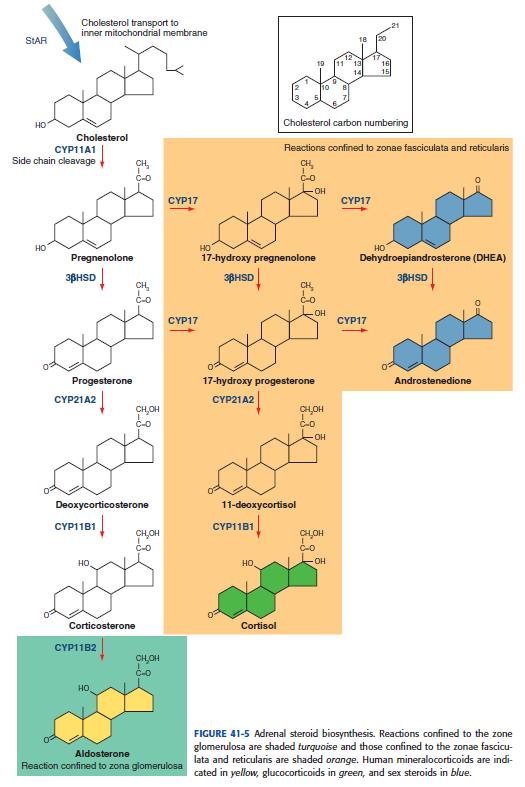
10 Glucocorticoids Corticotropin releasing factor (CRF) > Adrenocorticotropic hormone (ACTH) secretion (anterior pituitary gland) > Glucocorticoid secretion (cortisol) Stress response Enhances effect of catecholamine signaling on arterial smooth muscle cells Increases cardiac contractility and vascular tone Anti-inflammatory and immunosuppressive Reduces circulating lymphocyte and eosinophil counts Increases neutrophil counts Histamine release suppressed Cytokine and immunoglobulin production decreased
11 Glucocorticoids Catabolic state Upregulation of gluconeogenesis Inhibition of glucose uptake by peripheral tissues Stimulation of lipolysis Insulin resistance
12 Mineralocorticoids Zone Glomerulosa Regulated by renin-angiotensinaldosterone axis Angiotensinogen -> angiotensin I - > angiotensin II Stimulates aldosterone release Downregulation Hypokalemia Increased sodium delivery to distal tubule Aldosterone Acts on renal distal convoluted tubule Promotes sodium and chloride retention Potassium and hydrogen ions secreted into urine Expansion of extracellular fluid volume
13 Adrenal Sex Steroids Androstenedione, DHEA, DHEA-S Physiological effects are generally weak in comparison to gonadal sex steroids Development of secondary sexual characteristics
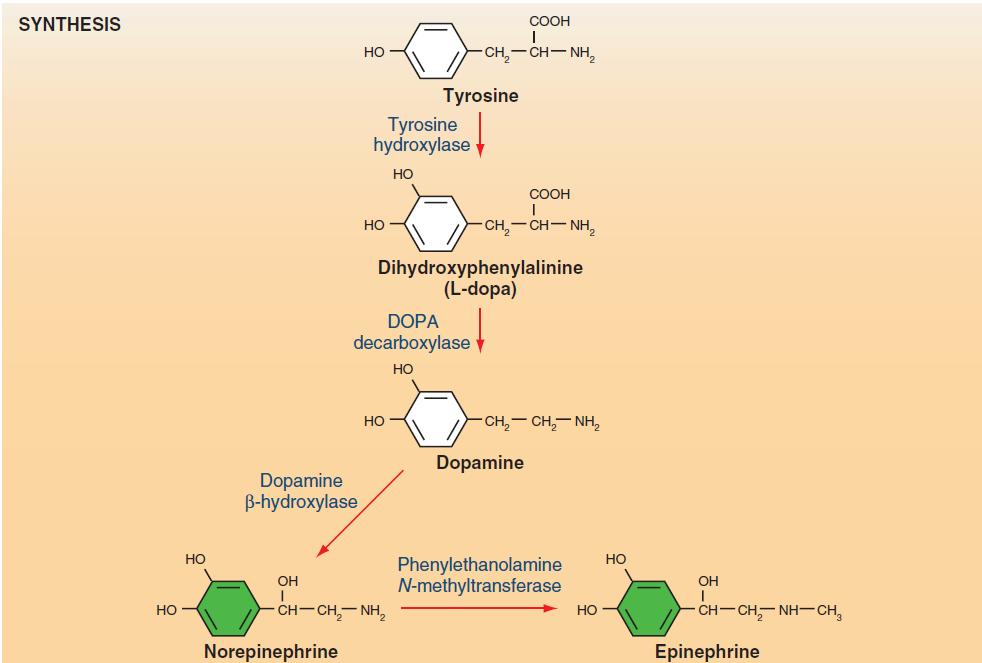
14 Catecholamines

15 Adrenal Masses
16 Adrenal Masses Functional Cortisol producing adenoma (Cushing s syndrome) Aldosteronoma (Conn s syndrome) Pheochromocytoma Malignant Adrenocortical carcinoma Metastatic lesion Other Adrenal cyst Ganglioneuroma Myelolipoma
17 Adrenal Masses Functional Cortisol producing adenoma (Cushing s syndrome) Aldosteronoma (Conn s syndrome) Pheochromocytoma Malignant Adrenocortical carcinoma Metastatic lesion Other Adrenal cyst Ganglioneuroma Myelolipoma


18 Cortisol-Producing Adenomas
19 Cortisol-Producing Adenomas History findings Fatigue, depression, sleep disturbances Weight gain Menstrual irregularities Hypertension Glucose intolerance Easy bruising Osteoporosis / fracture with minimal trauma Physical exam findings Central obesity Supraclavicular fat accumulation Dorsocervical fat pat Facial plethora Thinned skin Purple and wide (>1cm) striae Acne Ecchymoses Hirsutism Proximal muscle weakness or wasting
20 Cortisol-Producing Adenomas Goal: demonstrate 3 pathophysiologic derangements of Cushing syndrome Loss of normal diurnal pattern with abnormally high late-night cortisol secretion (late-night salivary cortisol test) Failure to discontinue the production of cortisol despite absence of ACTH stimulation (dexamethasone suppression test) Excess production of cortisol (24-hr UFC test)
21 Adrenal Masses Functional Cortisol producing adenoma (Cushing s syndrome) Aldosteronoma (Conn s syndrome) Pheochromocytoma Malignant Adrenocortical carcinoma Metastatic lesion Other Adrenal cyst Ganglioneuroma Myelolipoma
22 Aldosteronoma Conn s syndrome Hypertension, hypokalemia History: Muscle cramping and weakness Headaches Intermittent or periodic paralysis Polydipsia, polyuria, nocturia Drug refractory hypertension (need of >3 agents)
23 Aldosteronoma
24 Aldosteronoma Aldosterone renin ratio (ARR) > 20 Plasma aldosterone concentration (PAC) Plasma renin activity (PRA) Salt loading confirmation test Positive if aldosterone remains elevated
25 Aldosteronoma Adrenal Venous Sampling Indication: older patients, morphologically abnormal glands bilaterally, unilateral microadenomas Corrected aldosterone/cortisol ratio of >4:1 = unilateral source of aldosterone excess
26 Aldosteronoma Treatment Medical management: spironolactone, eplerenone Surgical management: laparoscopic adrenalectomy
27 Adrenal Masses Functional Cortisol producing adenoma (Cushing s syndrome) Aldosteronoma (Conn s syndrome) Pheochromocytoma Malignant Adrenocortical carcinoma Metastatic lesion Other Adrenal cyst Ganglioneuroma Myelolipoma
28 Pheochromocytoma Found in % of hypertensive patients History Severe hypertension Tachycardia, palpitations Cardiac arrhythmias Anxiety attacks Weight loss Sweating Family history of pheochromocytoma, MEN type 2, VHL
29

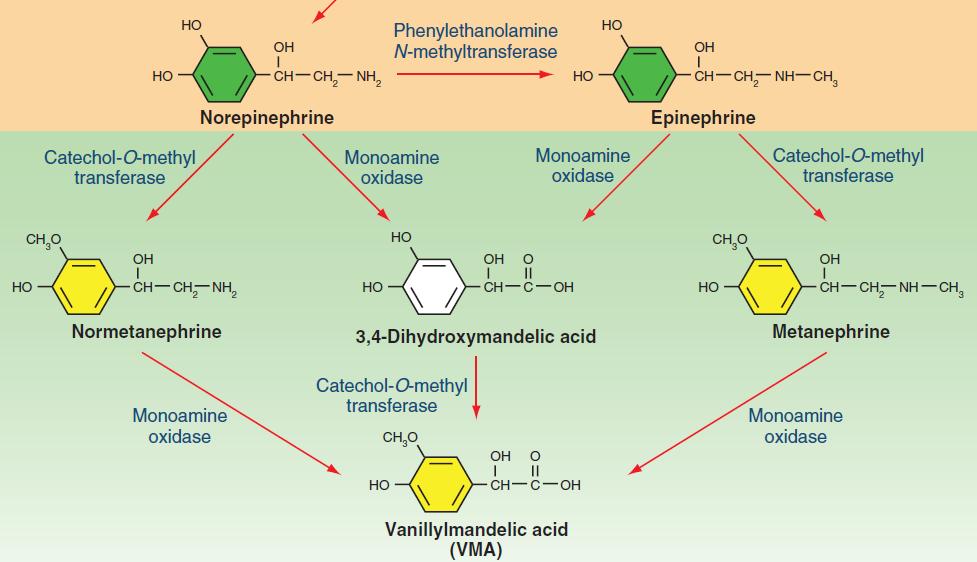
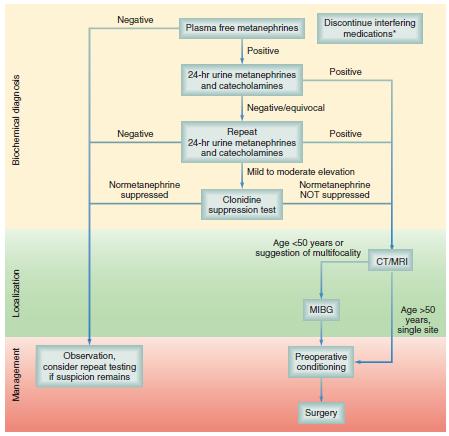
30 Pheochromocytoma Biochemical Evaluation 24-hour urine collection - catecholamines and total/fractionated metanephrines Plasma fractionated metanephrines and normetanephirines Genetic Testing RET, VHL, subunits of succinate dehydrogenase genes
31
32 Pheochromocytoma Pre-operative management Phenoxybenzamine 10mg BID: alpha-adrenergic (long-acting) blockage for 1-3 weeks Other meds: doxazosin, metyrosine (alpha-methyltyrosine) Beta-blockade Indications: persistent tachycardia, extra-systoles, arrhythmias Can only be given in setting of adequate alpha-adrenergic blockade Propranolol 10-40mg q6-8hr Calcium channel blockers can be used for preoperative and intraoperative blood pressure control Encourage liberal fluid and salt intact
33 Pheochromocytoma Intra-operative management Arterial line and central line for monitoring Hypertension : nitroprusside, nicardipine, nitroglycerin, phentolamine Tachyarrhythmia : esmolol Ventricular arrhythmia : lidocaine Hypotension after pheochromocytoma removed -> crystalloid and alpha-adrenergic agonists
34 Adrenal Masses Functional Cortisol producing adenoma (Cushing s syndrome) Aldosteronoma (Conn s syndrome) Pheochromocytoma Malignant Adrenocortical carcinoma Metastatic lesion Other Adrenal cyst Ganglioneuroma Myelolipoma
35 Adrenocortical Carcinoma Rare tumor, annual incidence approximately 1 : 1,000,000 Ages 40-50, no gender predilection >50% are functional cortisol, aldosterone, sex steroids CT features: heterogeneity, irregular borders, central necrosis, invasion of adjacent structures Treatment: radical open resection with en bloc resection of adjacent organs and/or regional lymphadenectomy Local recurrence and metastases typically occur within 2 years Chemotherapy : mitotane
36 Adrenal Masses Functional Cortisol producing adenoma (Cushing s syndrome) Aldosteronoma (Conn s syndrome) Pheochromocytoma Malignant Adrenocortical carcinoma Metastatic lesion Other Adrenal cyst Ganglioneuroma Myelolipoma
37 Metastatic lesion Cancers that metastasize to the adrenal gland Lung cancer Breast cancer Melanoma Renal carcinoma Adrenal matastatectomy is rarely indicated. Patients with bilateral adrenal metastatic lesions should undergo evaluation for adrenal insufficiency
38 Adrenal Masses Functional Cortisol producing adenoma (Cushing s syndrome) Aldosteronoma (Conn s syndrome) Pheochromocytoma Malignant Adrenocortical carcinoma Metastatic lesion Other Adrenal cyst Ganglioneuroma: rare, benign, asymptomatic tumor of neural crest origin Myelolipoma
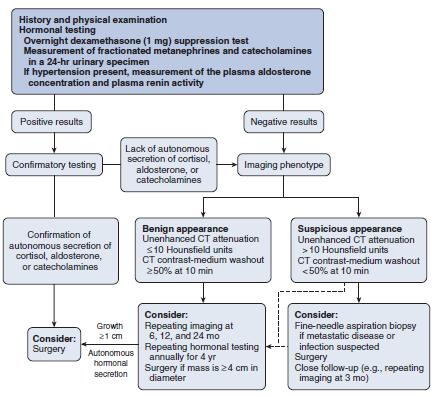
39 Adrenal Incidentaloma Incidence 8.7% (autopsy series) Answer 3 questions: Is it functional? Does it have radiologic characteristics suggestive of a malignant lesion? Does the patient have a history of malignancy? RULE OUT pheochromocytoma prior to any attempted resection or biopsy
40 Adrenal Incidentaloma
41 Adrenal Incidentaloma If incidentaloma does not fulfill criteria for surgical resection: Radiologic re-evaluation at 3-6 months, then annually for 1-2 years Hormonal evaluation at time of diagnosis, then annually for 5 years
42 A 36 year old man has an abdominal CT scan after a motor vehicle crash. No injuries are found, but his blood pressure is 160/100 mm Hg. The CT scan shows a 3cm adrenal mass. Appropriate initial biochemical evaluation should include all of the following EXCEPT A. plasma metanephrines B. plasma aldosterone level C. low-dose overnight dexamethasone suppression test D. plasma renin level E. serum adrenocorticotropic hormone level
43 A 36 year old man has an abdominal CT scan after a motor vehicle crash. No injuries are found, but his blood pressure is 160/100 mm Hg. The CT scan shows a 3cm adrenal mass. Appropriate initial biochemical evaluation should include all of the following EXCEPT A. plasma metanephrines B. plasma aldosterone level C. low-dose overnight dexamethasone suppression test D. plasma renin level E. serum adrenocorticotropic hormone level
44 References AACE/AAES Adrenal Incidentaloma Guidelines, Endocr Pract. 2009;15(Suppl 1) Sabiston Chapter 41 Fischer s Mastery of Surgery Chapter 44: Adrenalectomy Open and Minimally Invasive Cameron Current Surgical Therapy. Adrenal Incidentaloma Netter s Atlas of Human Anatomy. Plate 310, 320 Townsend and Evers: Atlas of General Surgical Techniques. Chapter 8: Adrenals Anterior, Posterior (Open and Laparoscopic)
ADRENAL INCIDENTALOMA. Jamii St. Julien
 ADRENAL INCIDENTALOMA Jamii St. Julien Outline Definition Differential Evaluation Treatment Follow up Questions Case Definition The phenomenon of detecting an otherwise unsuspected adrenal mass on radiologic
ADRENAL INCIDENTALOMA Jamii St. Julien Outline Definition Differential Evaluation Treatment Follow up Questions Case Definition The phenomenon of detecting an otherwise unsuspected adrenal mass on radiologic
Endocrine. Endocrine as it relates to the kidney. Sarah Elfering, MD University of Minnesota
 Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
The Work-up and Treatment of Adrenal Nodules
 The Work-up and Treatment of Adrenal Nodules Lawrence Andrew Drew Shirley, MD, MS, FACS Assistant Professor of Surgical-Clinical Department of Surgery Division of Surgical Oncology The Ohio State University
The Work-up and Treatment of Adrenal Nodules Lawrence Andrew Drew Shirley, MD, MS, FACS Assistant Professor of Surgical-Clinical Department of Surgery Division of Surgical Oncology The Ohio State University
Approach to Adrenal Incidentaloma. Alice Y.Y. Cheng, MD, FRCP
 Approach to Adrenal Incidentaloma Alice Y.Y. Cheng, MD, FRCP Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
Approach to Adrenal Incidentaloma Alice Y.Y. Cheng, MD, FRCP Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone
 Disease of the Adrenals 1 Zona Glomerulosa Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone leads to salt
Disease of the Adrenals 1 Zona Glomerulosa Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone leads to salt
Case Based Urology Learning Program
 Case Based Urology Learning Program Resident s Corner: UROLOGY Case Number 4 CBULP 2010 004 Case Based Urology Learning Program Editor: Associate Editors: Manager: Case Contributors: Steven C. Campbell,
Case Based Urology Learning Program Resident s Corner: UROLOGY Case Number 4 CBULP 2010 004 Case Based Urology Learning Program Editor: Associate Editors: Manager: Case Contributors: Steven C. Campbell,
Pheochromocytoma AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGY ILLINOIS CHAPTER OCTOBER 13, 2018
 Pheochromocytoma AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGY ILLINOIS CHAPTER OCTOBER 13, 2018 Steven A. De Jong, M.D., FACS, FACE Professor and Vice Chair of Surgery Chief, Division of General Surgery
Pheochromocytoma AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGY ILLINOIS CHAPTER OCTOBER 13, 2018 Steven A. De Jong, M.D., FACS, FACE Professor and Vice Chair of Surgery Chief, Division of General Surgery
Endocrine MR. Jan 30, 2015 Michael LaFata, MD
 Endocrine MR Jan 30, 2015 Michael LaFata, MD Brief case 55-year-old female in ED PMH: HTN, DM2, HLD, GERD CC: Epigastric/LUQ abdominal pain, N/V x2 days AF, HR 103, BP 155/85, room air CMP: Na 133, K 3.6,
Endocrine MR Jan 30, 2015 Michael LaFata, MD Brief case 55-year-old female in ED PMH: HTN, DM2, HLD, GERD CC: Epigastric/LUQ abdominal pain, N/V x2 days AF, HR 103, BP 155/85, room air CMP: Na 133, K 3.6,
THE HIGHS AND LOWS OF ADRENAL GLAND PATHOLOGY
 THE HIGHS AND LOWS OF ADRENAL GLAND PATHOLOGY Symptoms of Adrenal Gland Disorders 2 Depends on whether it is making too much or too little hormone And on what you Google! Symptoms include obesity, skin
THE HIGHS AND LOWS OF ADRENAL GLAND PATHOLOGY Symptoms of Adrenal Gland Disorders 2 Depends on whether it is making too much or too little hormone And on what you Google! Symptoms include obesity, skin
How to Recognize Adrenal Disease
 How to Recognize Adrenal Disease CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi
How to Recognize Adrenal Disease CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi
COPYRIGHTED MATERIAL. Adrenal Imaging. 1.1 Introduction. Khaled M. Elsayes 1, Isaac R. Francis 1, Melvyn Korobkin 1 and Gerard M.
 1 Adrenal Imaging Khaled M. Elsayes 1, Isaac R. Francis 1, Melvyn Korobkin 1 and Gerard M. Doherty 2 1 Department of Radiology, University of Michigan 2 Department of Radiology and Surgery, University
1 Adrenal Imaging Khaled M. Elsayes 1, Isaac R. Francis 1, Melvyn Korobkin 1 and Gerard M. Doherty 2 1 Department of Radiology, University of Michigan 2 Department of Radiology and Surgery, University
Adrenal gland Incidentaloma
 Adrenal gland Incidentaloma Topic review 17 sep 2008 Anatomy 1 Anatomical consideration Blood supply Artery: small branches from Inf. phrenic, renal artery and aorta Vein: Rt : medial aspect to IVC Lt
Adrenal gland Incidentaloma Topic review 17 sep 2008 Anatomy 1 Anatomical consideration Blood supply Artery: small branches from Inf. phrenic, renal artery and aorta Vein: Rt : medial aspect to IVC Lt
The Adrenal Glands. I. Normal adrenal gland A. Gross & microscopic B. Hormone synthesis, regulation & measurement. II.
 The Adrenal Glands Thomas Jacobs, M.D. Diane Hamele-Bena, M.D. I. Normal adrenal gland A. Gross & microscopic B. Hormone synthesis, regulation & measurement II. Hypoadrenalism III. Hyperadrenalism; Adrenal
The Adrenal Glands Thomas Jacobs, M.D. Diane Hamele-Bena, M.D. I. Normal adrenal gland A. Gross & microscopic B. Hormone synthesis, regulation & measurement II. Hypoadrenalism III. Hyperadrenalism; Adrenal
Diseases of the Adrenal gland
 Diseases of the Adrenal gland Adrenal insufficiency Cushing disease vs syndrome Pheochromocytoma Hyperaldostronism What are the layers of the adrenal gland?? And what does each layer produce?? What are
Diseases of the Adrenal gland Adrenal insufficiency Cushing disease vs syndrome Pheochromocytoma Hyperaldostronism What are the layers of the adrenal gland?? And what does each layer produce?? What are
Adrenal incidentaloma
 Adrenal incidentaloma Prevalence 5% post-mortem series 4% CT series 6-20% CT series in patients with Hx extra-adrenal malignancy Commoner with increasing age Associated with adrenal hyperfunction in 15%
Adrenal incidentaloma Prevalence 5% post-mortem series 4% CT series 6-20% CT series in patients with Hx extra-adrenal malignancy Commoner with increasing age Associated with adrenal hyperfunction in 15%
AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA
 AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2016 Mayo Foundation for Medical Education and Research.
AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2016 Mayo Foundation for Medical Education and Research.
Pituitary Gland Disorders
 Pituitary Gland Disorders 1 2 (GH-RH) (CRH) (TRH) (TRH) (GTRH) (GTRH) 3 Classification of pituitary disorders: 1. Hypersecretory diseases: a. Acromegaly and gigantism: Usually caused by (GH)-secreting
Pituitary Gland Disorders 1 2 (GH-RH) (CRH) (TRH) (TRH) (GTRH) (GTRH) 3 Classification of pituitary disorders: 1. Hypersecretory diseases: a. Acromegaly and gigantism: Usually caused by (GH)-secreting
AVS and IPSS: The Basics and the Pearls
 AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2018 Mayo Foundation for Medical Education and Research.
AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2018 Mayo Foundation for Medical Education and Research.
The Management of adrenal incidentaloma
 The Management of adrenal incidentaloma Dimitrios Linos, MD Director of Surgery, Hygeia Hospital, Athens, Greece Consultant in Surgery, Massachusetts General Hospital, Boston, USA 8 th Postgraduate Course
The Management of adrenal incidentaloma Dimitrios Linos, MD Director of Surgery, Hygeia Hospital, Athens, Greece Consultant in Surgery, Massachusetts General Hospital, Boston, USA 8 th Postgraduate Course
THE FACTS YOU NEED TO KNOW
 PHEOCHROMOCYTOMA THE FACTS YOU NEED TO KNOW Pheochromocytoma is a part of the pheochromocytoma and paraganglioma group of syndromes. A pheochromocytoma is a tumor arising in the adrenal gland medulla.
PHEOCHROMOCYTOMA THE FACTS YOU NEED TO KNOW Pheochromocytoma is a part of the pheochromocytoma and paraganglioma group of syndromes. A pheochromocytoma is a tumor arising in the adrenal gland medulla.
The endocrine system is made up of a complex group of glands that secrete hormones.
 1 10. Endocrinology I MEDCHEM 535 Diagnostic Medicinal Chemistry Endocrinology The endocrine system is made up of a complex group of glands that secrete hormones. These hormones control reproduction, metabolism,
1 10. Endocrinology I MEDCHEM 535 Diagnostic Medicinal Chemistry Endocrinology The endocrine system is made up of a complex group of glands that secrete hormones. These hormones control reproduction, metabolism,
ADRENAL LESIONS 10/09/2012. Adrenal + lesion. Introduction. Common causes. Anatomy. Financial disclosure. Dr. Boraiah Sreeharsha. Nothing to declare
 ADRENAL LESIONS Financial disclosure Nothing to declare Dr. Boraiah Sreeharsha MBBS;FRCR;FRCPSC Introduction Adrenal + lesion Adrenal lesions are common 9% of the population Increase in the detection rate
ADRENAL LESIONS Financial disclosure Nothing to declare Dr. Boraiah Sreeharsha MBBS;FRCR;FRCPSC Introduction Adrenal + lesion Adrenal lesions are common 9% of the population Increase in the detection rate
27 F with new onset hypertension and weight gain. Rajesh Jain Endorama 10/01/2015
 27 F with new onset hypertension and weight gain Rajesh Jain Endorama 10/01/2015 HPI 27 F with hypertension x 1 year BP 130-140/90 while on amlodipine 5 mg daily She also reports weight gain, 7 LB, mainly
27 F with new onset hypertension and weight gain Rajesh Jain Endorama 10/01/2015 HPI 27 F with hypertension x 1 year BP 130-140/90 while on amlodipine 5 mg daily She also reports weight gain, 7 LB, mainly
RECURRENT ADRENAL DISEASE. Megan Applewhite Endorama 2/19/2015 SR , SC
 RECURRENT ADRENAL DISEASE Megan Applewhite Endorama 2/19/2015 SR 2412318, SC 3421561 Category: Adrenal Attendings: Angelos & Grogan PATIENT #1 36yo woman with a hx of Cushing s Syndrome and right adrenalectomy
RECURRENT ADRENAL DISEASE Megan Applewhite Endorama 2/19/2015 SR 2412318, SC 3421561 Category: Adrenal Attendings: Angelos & Grogan PATIENT #1 36yo woman with a hx of Cushing s Syndrome and right adrenalectomy
PHEOCHROMOCYTOMA. Anita Chiu, MD Kings County Hospital Center January 13, 2011
 PHEOCHROMOCYTOMA Anita Chiu, MD Kings County Hospital Center January 13, 2011 Case Presentation 62 year old female from Grenada with longstanding HTN, DM, CRI Complaints of palpitations for years Abdominal
PHEOCHROMOCYTOMA Anita Chiu, MD Kings County Hospital Center January 13, 2011 Case Presentation 62 year old female from Grenada with longstanding HTN, DM, CRI Complaints of palpitations for years Abdominal
Adrenal incidentaloma guideline for Northern Endocrine Network
 Adrenal incidentaloma guideline for Northern Endocrine Network Definition of adrenal incidentaloma Adrenal mass detected on an imaging study done for indications that are not related to an adrenal problem
Adrenal incidentaloma guideline for Northern Endocrine Network Definition of adrenal incidentaloma Adrenal mass detected on an imaging study done for indications that are not related to an adrenal problem
Adrenal gland And Pancreas
 Adrenal gland And Pancreas Structure Cortex Glucocorticoids Effects Control of secretion Mineralocorticoids Effects Control of secretion Sex steroids Medulla Catecholamines Adrenal cortex 80% of an adrenal
Adrenal gland And Pancreas Structure Cortex Glucocorticoids Effects Control of secretion Mineralocorticoids Effects Control of secretion Sex steroids Medulla Catecholamines Adrenal cortex 80% of an adrenal
Evaluation of Thyroid Nodules
 Evaluation of Thyroid Nodules Stephan Kowalyk, MD January 25 28, 2018 1 Primary goal Exclude malignancy Incidental thyroid nodules If found on CT, MRI, PET scan, carotid Doppler ULTRASOUND!! January 25
Evaluation of Thyroid Nodules Stephan Kowalyk, MD January 25 28, 2018 1 Primary goal Exclude malignancy Incidental thyroid nodules If found on CT, MRI, PET scan, carotid Doppler ULTRASOUND!! January 25
ADRENAL MEDULLARY DISORDERS: PHAEOCHROMOCYTOMAS AND MORE
 ADRENAL MEDULLARY DISORDERS: PHAEOCHROMOCYTOMAS AND MORE DR ANJU SAHDEV READER AND CONSULTANT RADIOLOGIST QUEEN MARY UNIVERSITY AND ST BARTHOLOMEW S HOSPITAL BARTS HEALTH, LONDON, UK DISCLOSURE OF CONFLICT
ADRENAL MEDULLARY DISORDERS: PHAEOCHROMOCYTOMAS AND MORE DR ANJU SAHDEV READER AND CONSULTANT RADIOLOGIST QUEEN MARY UNIVERSITY AND ST BARTHOLOMEW S HOSPITAL BARTS HEALTH, LONDON, UK DISCLOSURE OF CONFLICT
Primary Aldosteronism
 Primary Aldosteronism Odelia Cooper, MD Assistant Professor of Medicine Division of Endocrinology, Diabetes, and Metabolism Cedars-Sinai Medical Center HYPERTENSION CENTER Barriers to diagnosing primary
Primary Aldosteronism Odelia Cooper, MD Assistant Professor of Medicine Division of Endocrinology, Diabetes, and Metabolism Cedars-Sinai Medical Center HYPERTENSION CENTER Barriers to diagnosing primary
Year 2004 Paper two: Questions supplied by Megan 1
 Year 2004 Paper two: Questions supplied by Megan 1 QUESTION 96 A 32yo woman if found to have high blood pressure (180/105mmHg) at an insurance medical examination. She is asymptomatic. Clinical examination
Year 2004 Paper two: Questions supplied by Megan 1 QUESTION 96 A 32yo woman if found to have high blood pressure (180/105mmHg) at an insurance medical examination. She is asymptomatic. Clinical examination
Incidental Adrenal Nodules Differential Diagnosis
 Adrenal Stuff Richard J. Auchus, MD, PhD, FACE Division of Metabolism, Endocrinology & Diabetes Departments of Internal Medicine & Pharmacology University of Michigan/VA Ann Arbor Incidental Adrenal Nodules
Adrenal Stuff Richard J. Auchus, MD, PhD, FACE Division of Metabolism, Endocrinology & Diabetes Departments of Internal Medicine & Pharmacology University of Michigan/VA Ann Arbor Incidental Adrenal Nodules
Nephtali R. Gomez, M.D. To The Incidental Adrenal Mass
 Nephtali R. Gomez, M.D. To The Incidental Adrenal Mass The Complete Idiot s Guide to The Incidental Adrenal Mass Defini:on Any adrenal mass 1cm or more in diameter discovered on a radiologic exam performed
Nephtali R. Gomez, M.D. To The Incidental Adrenal Mass The Complete Idiot s Guide to The Incidental Adrenal Mass Defini:on Any adrenal mass 1cm or more in diameter discovered on a radiologic exam performed
Daniela Faivovich K., MS VII Universidad de Chile Gillian Lieberman, MD Harvard Medical School
 Daniela Faivovich K., MS VII Universidad de Chile Gillian Lieberman, MD Harvard Medical School May 21st, 2010 56 year old male patient History of hypertension, hyperlipidemia and insulin-resistance 2009:
Daniela Faivovich K., MS VII Universidad de Chile Gillian Lieberman, MD Harvard Medical School May 21st, 2010 56 year old male patient History of hypertension, hyperlipidemia and insulin-resistance 2009:
Cortisol levels. Naturally produced by the adrenal Cortisol
 1 + 2 Cortisol levels asleep awake Naturally produced by the adrenal Cortisol Man made tablets, injections, creams & inhalers Cortisone Hydrocortisone Prednisone Prednisolone Betamethasone Methylprednisolone
1 + 2 Cortisol levels asleep awake Naturally produced by the adrenal Cortisol Man made tablets, injections, creams & inhalers Cortisone Hydrocortisone Prednisone Prednisolone Betamethasone Methylprednisolone
CUSHING SYNDROME Dr. Muhammad Sarfraz
 Indep Rev Jul-Dec 2018;20(7-12) CUSHING SYNDROME Dr. Muhammad Sarfraz IR-655 Abstract: It is defined as clinical condition in which there are increased free circulating glucocorticoides casused by excessive
Indep Rev Jul-Dec 2018;20(7-12) CUSHING SYNDROME Dr. Muhammad Sarfraz IR-655 Abstract: It is defined as clinical condition in which there are increased free circulating glucocorticoides casused by excessive
CPY 605 ADVANCED ENDOCRINOLOGY
 CPY 605 ADVANCED ENDOCRINOLOGY THE ADRENAL CORTEX PRESENTED BY WAINDIM NYIAMBAM YVONNE HS09A187 INTRODUCTION Two adrenal glands lie on top of each kidney. Each gland between 6 and 8g in weight is composed
CPY 605 ADVANCED ENDOCRINOLOGY THE ADRENAL CORTEX PRESENTED BY WAINDIM NYIAMBAM YVONNE HS09A187 INTRODUCTION Two adrenal glands lie on top of each kidney. Each gland between 6 and 8g in weight is composed
Morbidity & Mortality. Mark H. Tseng MD SUNY Downstate Medical Center Lutheran Medical Center December 16, 2005
 Morbidity & Mortality Mark H. Tseng MD SUNY Downstate Medical Center Lutheran Medical Center December 16, 2005 Case presentation Pt is a xx year old Asian woman who present to the ED with cc of epigastric
Morbidity & Mortality Mark H. Tseng MD SUNY Downstate Medical Center Lutheran Medical Center December 16, 2005 Case presentation Pt is a xx year old Asian woman who present to the ED with cc of epigastric
74. Hormone synthesis in the adrenal cortex. The glucocorticoids: biosynthesis, regulation, effects. Adrenal cortex is vital for life!
 74. Hormone synthesis in the adrenal cortex. The glucocorticoids: biosynthesis, regulation, effects. Adrenal cortex is vital for life! 5 g each Zona glomerulosa : Mineralocorticoids ALDOSTERON Zona fasciculata:
74. Hormone synthesis in the adrenal cortex. The glucocorticoids: biosynthesis, regulation, effects. Adrenal cortex is vital for life! 5 g each Zona glomerulosa : Mineralocorticoids ALDOSTERON Zona fasciculata:
How to approach resistant hypertension. Teh-Li Huo, M.D., Ph.D.
 How to approach resistant hypertension Teh-Li Huo, M.D., Ph.D. BP goals No risk factors:
How to approach resistant hypertension Teh-Li Huo, M.D., Ph.D. BP goals No risk factors:
Updates in primary hyperaldosteronism and the rule
 Updates in primary hyperaldosteronism and the 20-50 rule I. David Weiner, M.D. Professor of Medicine and Physiology and Functional Genomics University of Florida College of Medicine and NF/SGVHS The 20-50
Updates in primary hyperaldosteronism and the 20-50 rule I. David Weiner, M.D. Professor of Medicine and Physiology and Functional Genomics University of Florida College of Medicine and NF/SGVHS The 20-50
MILD HYPERCORTISOLISM DUE TO ADRENAL ADENOMA: IS IT REALLY SUBCLINICAL?
 MILD HYPERCORTISOLISM DUE TO ADRENAL ADENOMA: IS IT REALLY SUBCLINICAL? Alice C. Levine, MD Professor of Medicine Division of Endocrinology, Diabetes and Bone Diseases Georgia-AACE 2017 Annual Meeting
MILD HYPERCORTISOLISM DUE TO ADRENAL ADENOMA: IS IT REALLY SUBCLINICAL? Alice C. Levine, MD Professor of Medicine Division of Endocrinology, Diabetes and Bone Diseases Georgia-AACE 2017 Annual Meeting
Pathophysiology of Adrenal Disorders
 Pathophysiology of Adrenal Disorders PHCL 415 Hadeel Alkofide April 2010 Some slides adapted from Rania Aljizani MSc 1 Learning Objectives Describe the roles of the various zones of the adrenal cortex
Pathophysiology of Adrenal Disorders PHCL 415 Hadeel Alkofide April 2010 Some slides adapted from Rania Aljizani MSc 1 Learning Objectives Describe the roles of the various zones of the adrenal cortex
ADRENAL GLAND. Introduction 4/21/2009. Among most important and vital endocrine organ. Small bilateral yellowish retroperitoneal organ
 Introduction Among most important and vital endocrine organ ADRENAL GLAND D.Hammoudi.MD Small bilateral yellowish retroperitoneal organ Lies just above kidney in gerota s fascia 2 1 The Adrenal Gland Anatomy
Introduction Among most important and vital endocrine organ ADRENAL GLAND D.Hammoudi.MD Small bilateral yellowish retroperitoneal organ Lies just above kidney in gerota s fascia 2 1 The Adrenal Gland Anatomy
PITUITARY: JUST THE BASICS PART 2 THE PATIENT
 PITUITARY: JUST THE BASICS PART 2 THE PATIENT DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and
PITUITARY: JUST THE BASICS PART 2 THE PATIENT DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and
Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences. Endocrinology. (Review) Year 5 Internal Medicine
 Year 5 Internal Medicine") Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences Endocrinology (Review) Year 5 Internal Medicine Presented by: Dr. Mona Arekat Prepared by: Ali Jassim Alhashli Case (1):
Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical Sciences Endocrinology (Review) Year 5 Internal Medicine Presented by: Dr. Mona Arekat Prepared by: Ali Jassim Alhashli Case (1):
Adrenal Incidentaloma Management
 Adrenal Incidentaloma Management Full Title of Guideline: Author Management of Incidentally-discovered Adrenal Lesions ( Incidentalomas ) Mr David Chadwick Consultant Endocrine Surgeon david.chadwick2@nuh.nhs.uk
Adrenal Incidentaloma Management Full Title of Guideline: Author Management of Incidentally-discovered Adrenal Lesions ( Incidentalomas ) Mr David Chadwick Consultant Endocrine Surgeon david.chadwick2@nuh.nhs.uk
Assistant Professor of Endocrinology
 Pathophysiology Of Adrenal Disorder Dr.Rezvan Salehidoost Assistant Professor of Endocrinology Pathophysiology Of Adrenal Disorder The adrenal glands lie at the superior pole of each kidney and are composed
Pathophysiology Of Adrenal Disorder Dr.Rezvan Salehidoost Assistant Professor of Endocrinology Pathophysiology Of Adrenal Disorder The adrenal glands lie at the superior pole of each kidney and are composed
Upon completion, participants should be able to:
 Learning Objectives Upon completion, participants should be able to: Describe the causes of secondary hypertension and the prevalence of primary aldosteronism Discuss the diagnostic approach to primary
Learning Objectives Upon completion, participants should be able to: Describe the causes of secondary hypertension and the prevalence of primary aldosteronism Discuss the diagnostic approach to primary
October 13, Surgical Nuances to Managing Cushing s Disease. Cortisol Regulation. Cushing s Syndrome Excess Cortisol. Sandeep Kunwar, M.D.
 Surgical Nuances to Managing Cushing s Disease Cortisol Regulation Sandeep Kunwar, M.D. Surgical Director, California Center for Pituitary Disorders Associate Clinical Professor, University of California,
Surgical Nuances to Managing Cushing s Disease Cortisol Regulation Sandeep Kunwar, M.D. Surgical Director, California Center for Pituitary Disorders Associate Clinical Professor, University of California,
adrenal and parathyroid glands Done by jehad abdel aziz
 15-11-09 prof. muhammed khammash adrenal and parathyroid glands Done by jehad abdel aziz The adrenal glands:- Anatomy:- The adrenal glands are flattened, yellowish structures that weigh less than 10g in
15-11-09 prof. muhammed khammash adrenal and parathyroid glands Done by jehad abdel aziz The adrenal glands:- Anatomy:- The adrenal glands are flattened, yellowish structures that weigh less than 10g in
Dimitrios Linos, M.D., Ph.D. Professor of Surgery National & Kapodistrian University of Athens
 Dimitrios Linos, M.D., Ph.D. Professor of Surgery National & Kapodistrian University of Athens What is an adrenal incidentaloma? An adrenal incidentaloma is defined as an adrenal tumor initially diagnosed
Dimitrios Linos, M.D., Ph.D. Professor of Surgery National & Kapodistrian University of Athens What is an adrenal incidentaloma? An adrenal incidentaloma is defined as an adrenal tumor initially diagnosed
Endocrine Topic Review. Sethanant Sethakarun, MD
 Endocrine Topic Review Sethanant Sethakarun, MD Definition Cushing's syndrome comprises a large group of signs and symptoms that reflect prolonged and in appropriately high exposure of tissue to glucocorticoids
Endocrine Topic Review Sethanant Sethakarun, MD Definition Cushing's syndrome comprises a large group of signs and symptoms that reflect prolonged and in appropriately high exposure of tissue to glucocorticoids
Systemic Hypertension Dr ahmed almutairi Assistant professor Internal medicine dept
 Systemic Hypertension Dr ahmed almutairi Assistant professor Internal medicine dept Continents 1- introduction 2- classification/definition 3- classification/etiology 4-etiology in both categories 5- complications
Systemic Hypertension Dr ahmed almutairi Assistant professor Internal medicine dept Continents 1- introduction 2- classification/definition 3- classification/etiology 4-etiology in both categories 5- complications
C h a p t e r 3 8 Cushing s Syndrome : Current Concepts in Diagnosis and Management
 C h a p t e r 3 8 Cushing s Syndrome : Current Concepts in Diagnosis and Management Padma S Menon Professor of Endocrinology, Seth G S Medical College & KEM Hospital, Mumbai A clinical syndrome resulting
C h a p t e r 3 8 Cushing s Syndrome : Current Concepts in Diagnosis and Management Padma S Menon Professor of Endocrinology, Seth G S Medical College & KEM Hospital, Mumbai A clinical syndrome resulting
Indications for Surgical Removal of Adrenal Glands
 The adrenal glands are orange-colored endocrine glands which are located on the top of both kidneys. The adrenal glands are triangular shaped and measure about one-half inch in height and 3 inches in length.
The adrenal glands are orange-colored endocrine glands which are located on the top of both kidneys. The adrenal glands are triangular shaped and measure about one-half inch in height and 3 inches in length.
Endocrinology and VHL: The adrenal and the pancreas
 Overview Endocrinology and VHL: The adrenal and the pancreas LAUREN FISHBEIN MD, PHD UNIVERSITY OF COLORADO SCHOOL OF MEDICINE DIVISION OF ENDOCRINOLOGY, METABOLISM AND DIABETES DIVISION OF BIOMEDICAL
Overview Endocrinology and VHL: The adrenal and the pancreas LAUREN FISHBEIN MD, PHD UNIVERSITY OF COLORADO SCHOOL OF MEDICINE DIVISION OF ENDOCRINOLOGY, METABOLISM AND DIABETES DIVISION OF BIOMEDICAL
Where in the adrenal cortex is cortisol produced? How do glucocorticoids inhibit prostaglandin production?
 CASE 35 A 36-year-old woman presents to her gynecologist with complaints of amenorrhea and hirsutism. She has also noticed an increase in her weight (especially in the trunk region) and easy fatigability.
CASE 35 A 36-year-old woman presents to her gynecologist with complaints of amenorrhea and hirsutism. She has also noticed an increase in her weight (especially in the trunk region) and easy fatigability.
The Case of the Adrenal Mass
 The Case of the Adrenal Mass Functional Adrenal Tumors Patricia Leung 10.2.14 Kings County Hospital Case presentation 62 year old F PMH: HTN, DM, arthritis PSH: none Meds: Metoprolol, Nifedipine, Losartan,
The Case of the Adrenal Mass Functional Adrenal Tumors Patricia Leung 10.2.14 Kings County Hospital Case presentation 62 year old F PMH: HTN, DM, arthritis PSH: none Meds: Metoprolol, Nifedipine, Losartan,
John Sutton, DO, FACOI, FACE, CCD. Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989
 John Sutton, DO, FACOI, FACE, CCD Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989 Gonadal Physiology and Disease 3 No Disclosures Gonadal Axis Hypothalamic-pituitary-gonadal Feedback mechanisms
John Sutton, DO, FACOI, FACE, CCD Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989 Gonadal Physiology and Disease 3 No Disclosures Gonadal Axis Hypothalamic-pituitary-gonadal Feedback mechanisms
ENDOCRINOLOGY 3. R. A. Benacka, MD, PhD, prof. Department of Pathophysiology Medical faculty, Safarik University, Košice
 Academic lectures for general medicine 3rd year 2005/2006, 2013/2014 ENDOCRINOLOGY 3 R. A. Benacka, MD, PhD, prof. Department of Pathophysiology Medical faculty, Safarik University, Košice Figures and
Academic lectures for general medicine 3rd year 2005/2006, 2013/2014 ENDOCRINOLOGY 3 R. A. Benacka, MD, PhD, prof. Department of Pathophysiology Medical faculty, Safarik University, Košice Figures and
Adrenocorticosteroids
 Adrenocorticosteroids Divided into those having: 1. Important effects on intermediary metabolism and immune function = glucocorticoids (cortisol). 2. Salt-retaining activity = mineralocorticoids (aldosterone).
Adrenocorticosteroids Divided into those having: 1. Important effects on intermediary metabolism and immune function = glucocorticoids (cortisol). 2. Salt-retaining activity = mineralocorticoids (aldosterone).
Endocrine Hypertension
 Endocrine Hypertension 1 No Disclosures Endocrine Hypertension Objectives: 1. Understand Endocrine disorders causing hypertension 2. Understand clinical presentation of Pheochromocytoma and Hyperaldosteronism
Endocrine Hypertension 1 No Disclosures Endocrine Hypertension Objectives: 1. Understand Endocrine disorders causing hypertension 2. Understand clinical presentation of Pheochromocytoma and Hyperaldosteronism
SECONDARY HYPERTENSION
 SECONDARY HYPERTENSION Grand round for Medical student 25 October 2013 By Rungnapa Laortanakul, MD. OUTLINE Overview of HT Secondary HT Resistance HT Primary aldosteronism Pheochromocytoma Cushing s syndrome
SECONDARY HYPERTENSION Grand round for Medical student 25 October 2013 By Rungnapa Laortanakul, MD. OUTLINE Overview of HT Secondary HT Resistance HT Primary aldosteronism Pheochromocytoma Cushing s syndrome
Pharmacology of Corticosteroids
 Pharmacology of Corticosteroids Dr. Aliah Alshanwani Dept. of Pharmacology College of Medicine, KSU Feb 2018 1 The Corticosteroids are steroid hormones produced by the adrenal cortex. They consist of two
Pharmacology of Corticosteroids Dr. Aliah Alshanwani Dept. of Pharmacology College of Medicine, KSU Feb 2018 1 The Corticosteroids are steroid hormones produced by the adrenal cortex. They consist of two
Corticosteroids. Abdulmoein Al-Agha, FRCPCH Professor of Pediatric Endocrinology, King Abdulaziz University Hospital,
 Corticosteroids Abdulmoein Al-Agha, FRCPCH Professor of Pediatric Endocrinology, King Abdulaziz University Hospital, http://aagha.kau.edu.sa History 1855 Addison's disease 1856 Adrenal glands essential
Corticosteroids Abdulmoein Al-Agha, FRCPCH Professor of Pediatric Endocrinology, King Abdulaziz University Hospital, http://aagha.kau.edu.sa History 1855 Addison's disease 1856 Adrenal glands essential
Management of adrenal incidentalomas
 31 Management of adrenal incidentalomas KEVIN MURTAGH, NANA MUHAMMAD AND MAREK MILLER The return of a scan result with reference to an incidental finding of an adrenal mass is a common scenario. 1 The
31 Management of adrenal incidentalomas KEVIN MURTAGH, NANA MUHAMMAD AND MAREK MILLER The return of a scan result with reference to an incidental finding of an adrenal mass is a common scenario. 1 The
PROBLEMS WITH REGULATION AND METABOLISM. Objectives A & P 8/11/2011
 PROBLEMS WITH REGULATION AND METABOLISM Lemone and Burke Chapters 18-20 Objectives Review A & P Recall age related changes Identify diagnostic tests Describe etiology, pathophysiology, clinical manifestation,
PROBLEMS WITH REGULATION AND METABOLISM Lemone and Burke Chapters 18-20 Objectives Review A & P Recall age related changes Identify diagnostic tests Describe etiology, pathophysiology, clinical manifestation,
Heart Failure (HF) Treatment
 Treatment") Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Heart Failure (HF) Treatment Heart Failure (HF) Complex, progressive disorder. The heart is unable to pump sufficient blood to meet the needs of the body. Its cardinal symptoms are dyspnea, fatigue, and
Karim Said. 41 year old farmer. Referred from the Uro-surgery Department because of uncontrolled hypertension prior to Lt. partial nephrectomy
 Case Presentation Karim Said Cardiology Departement Cairo University 41 year old farmer Referred from the Uro-surgery Department because of uncontrolled hypertension prior to Lt. partial nephrectomy ١
Case Presentation Karim Said Cardiology Departement Cairo University 41 year old farmer Referred from the Uro-surgery Department because of uncontrolled hypertension prior to Lt. partial nephrectomy ١
Adrenal Incidentalomas. G Stephen DeCherney, MD, MPH Clinical Professor of Medicine Division of Endocrinology UNC School of Medicine
 Adrenal Incidentalomas G Stephen DeCherney, MD, MPH Clinical Professor of Medicine Division of Endocrinology UNC School of Medicine Disclosures No financial, investment, or consulting relationship with
Adrenal Incidentalomas G Stephen DeCherney, MD, MPH Clinical Professor of Medicine Division of Endocrinology UNC School of Medicine Disclosures No financial, investment, or consulting relationship with
Secondary Hypertension: A Real World Approach
 Secondary Hypertension: A Real World Approach Evan Brittain, MD December 7, 2012 Kingston, Jamaica Disclosures None Real World Causes Renovascular Hypertension Endocrine Obstructive Sleep Apnea Pseudosecondary
Secondary Hypertension: A Real World Approach Evan Brittain, MD December 7, 2012 Kingston, Jamaica Disclosures None Real World Causes Renovascular Hypertension Endocrine Obstructive Sleep Apnea Pseudosecondary
Incidental adrenal masses A primary care approach
 CLINICAL Incidental adrenal masses A primary care approach Rasha Gendy, Prem Rashid Background The common use of cross-sectional imaging for the investigation of abdominal and thoracic illness has resulted
CLINICAL Incidental adrenal masses A primary care approach Rasha Gendy, Prem Rashid Background The common use of cross-sectional imaging for the investigation of abdominal and thoracic illness has resulted
Endocrine Tumors Part II. Jim Perry, PhD, DVM, DACVIM (Oncology), DACVS-SA
, DACVS-SA") Endocrine Tumors Part II Jim Perry, PhD, DVM, DACVIM (Oncology), DACVS-SA Adrenal Tumors: Adrenal tumors in veterinary patients can be challenging both to diagnose and to treat. An additional conundrum
Endocrine Tumors Part II Jim Perry, PhD, DVM, DACVIM (Oncology), DACVS-SA Adrenal Tumors: Adrenal tumors in veterinary patients can be challenging both to diagnose and to treat. An additional conundrum
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs
 Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
Introductory Clinical Pharmacology Chapter 41 Antihypertensive Drugs Blood Pressure Normal = sys
The Pathological l Basis of Disease
 Endocrine Diseases The Pathological l Basis of Disease - Graduate Course CMM5001 Qiao Li, MD, PhD Faculty of Medicine University of Ottawa qiaoli@uottawa.ca Outline Endocrine System Adrenal Gland Anatomy
Endocrine Diseases The Pathological l Basis of Disease - Graduate Course CMM5001 Qiao Li, MD, PhD Faculty of Medicine University of Ottawa qiaoli@uottawa.ca Outline Endocrine System Adrenal Gland Anatomy
Updates in primary hyperaldosteronism and the rule
 Updates in primary hyperaldosteronism and the 20-50 rule I. David Weiner, M.D. C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University of
Updates in primary hyperaldosteronism and the 20-50 rule I. David Weiner, M.D. C. Craig and Audrae Tisher Chair in Nephrology Professor of Medicine and Physiology and Functional Genomics University of
Personal data. Age : 63 Gender : male
 Personal data Age : 63 Gender : male Chief complain No specific symptom or discomfort A hepatic mass, found by abdominal sonography of routine health exam on 88-12-08 Past history 1984-3-3 Old CVA with
Personal data Age : 63 Gender : male Chief complain No specific symptom or discomfort A hepatic mass, found by abdominal sonography of routine health exam on 88-12-08 Past history 1984-3-3 Old CVA with
Cushing s Syndrome. Diagnosis. GuidelineCentral.com. Key Points. Diagnosis
 Cushing s Syndrome Consultant: Endocrine Society of Cushing s Syndrome Clinical Practice Guideline Writing Committee Key Points GuidelineCentral.com Key Points The most common cause of Cushing s syndrome
Cushing s Syndrome Consultant: Endocrine Society of Cushing s Syndrome Clinical Practice Guideline Writing Committee Key Points GuidelineCentral.com Key Points The most common cause of Cushing s syndrome
THE ADRENAL (SUPRARENAL) GLANDS
 GLANDS") THE ADRENAL (SUPRARENAL) GLANDS They are two glands, present above the kidneys. One adrenal gland is sufficient for human beings/mammals (example: we also have two kidneys but one is sufficient). The Adrenal
THE ADRENAL (SUPRARENAL) GLANDS They are two glands, present above the kidneys. One adrenal gland is sufficient for human beings/mammals (example: we also have two kidneys but one is sufficient). The Adrenal
Adrenal Steroid Hormones (Chapter 15) I. glucocorticoids cortisol corticosterone
 I. glucocorticoids cortisol corticosterone") Adrenal Steroid Hormones (Chapter 15) I. glucocorticoids cortisol corticosterone II. mineralocorticoids i id aldosterone III. androgenic steroids dehydroepiandrosterone testosterone IV. estrogenic steroids
Adrenal Steroid Hormones (Chapter 15) I. glucocorticoids cortisol corticosterone II. mineralocorticoids i id aldosterone III. androgenic steroids dehydroepiandrosterone testosterone IV. estrogenic steroids
Corticosteroids. Hawler Medical University College of Medicine Department of Pharmacology and Biophysics Dr.Susan Abdulkadir Farhadi MSc Pharmacology
 Corticosteroids Hawler Medical University College of Medicine Department of Pharmacology and Biophysics Dr.Susan Abdulkadir Farhadi MSc Pharmacology Objectives By the end of this lecture you should be
Corticosteroids Hawler Medical University College of Medicine Department of Pharmacology and Biophysics Dr.Susan Abdulkadir Farhadi MSc Pharmacology Objectives By the end of this lecture you should be
Pituitary Adenomas: Evaluation and Management. Fawn M. Wolf, MD 10/27/17
 Pituitary Adenomas: Evaluation and Management Fawn M. Wolf, MD 10/27/17 Over 18,000 pituitaries examined at autopsy: -10.6% contained adenomas (1.5-27%) -Frequency similar for men and women and across
Pituitary Adenomas: Evaluation and Management Fawn M. Wolf, MD 10/27/17 Over 18,000 pituitaries examined at autopsy: -10.6% contained adenomas (1.5-27%) -Frequency similar for men and women and across
The Evaluation of the Incidental Adrenal Mass and Not-So-Incidental Adrenal Hormone Excess
 The Evaluation of the Incidental Adrenal Mass and Not-So-Incidental Adrenal Hormone Excess Richard J. Auchus, MD, PhD, FACE Depts. Internal Medicine/MEND & Pharmacology Endocrinology Fellowship Program
The Evaluation of the Incidental Adrenal Mass and Not-So-Incidental Adrenal Hormone Excess Richard J. Auchus, MD, PhD, FACE Depts. Internal Medicine/MEND & Pharmacology Endocrinology Fellowship Program
ABSITE Review. RTC Conference Christina Bailey January 15, 2009
 ABSITE Review RTC Conference Christina Bailey January 15, 2009 How It s Broken Down? 220 questions Junior level (PGY 1 and 2) Exam 60% Basic Science 40% Clinical Management Senior Level (PGY 3-5) exam
ABSITE Review RTC Conference Christina Bailey January 15, 2009 How It s Broken Down? 220 questions Junior level (PGY 1 and 2) Exam 60% Basic Science 40% Clinical Management Senior Level (PGY 3-5) exam
Endocrine Testing. Alice Y.Y. Cheng, MD, FRCP October 14, 2015
 Endocrine Testing Alice Y.Y. Cheng, MD, FRCP October 14, 2015 Disclosure No disclosures relevant to the content of this workshop Learning Objectives By the end of this workshop, you will be able to: 1.
Endocrine Testing Alice Y.Y. Cheng, MD, FRCP October 14, 2015 Disclosure No disclosures relevant to the content of this workshop Learning Objectives By the end of this workshop, you will be able to: 1.
Aldosterone synthase inhibitors. John McMurray BHF Cardiovascular Research Centre University of Glasgow
 Aldosterone synthase inhibitors John McMurray BHF Cardiovascular Research Centre University of Glasgow Inhibition of aldosterone synthesis is hypothesized to be of benefit to patients with cardiovascular
Aldosterone synthase inhibitors John McMurray BHF Cardiovascular Research Centre University of Glasgow Inhibition of aldosterone synthesis is hypothesized to be of benefit to patients with cardiovascular
CUSHING S SYNDROME THE FACTS YOU NEED TO KNOW
 CUSHING S SYNDROME THE FACTS YOU NEED TO KNOW Written by: Paul Margulies, MD, FACE, FACP, Medical Director, NADF. Clinical Associate Professor of Medicine, Zucker School of Medicine at Hofstra/Northwell.
CUSHING S SYNDROME THE FACTS YOU NEED TO KNOW Written by: Paul Margulies, MD, FACE, FACP, Medical Director, NADF. Clinical Associate Professor of Medicine, Zucker School of Medicine at Hofstra/Northwell.
The adrenal gland consists of the cortex & the medulla. Medulla secretes epinephrine, whereas cortex synthesizes & secretes two major classes of
 Adrenocorticosteroids Dr. Entisar Al-Mukhtar The adrenal gland consists of the cortex & the medulla. Medulla secretes epinephrine, whereas cortex synthesizes & secretes two major classes of steroid hormones:
Adrenocorticosteroids Dr. Entisar Al-Mukhtar The adrenal gland consists of the cortex & the medulla. Medulla secretes epinephrine, whereas cortex synthesizes & secretes two major classes of steroid hormones:
Primary Aldosteronism: screening, diagnosis and therapy
 Primary Aldosteronism: screening, diagnosis and therapy Jacques W.M. Lenders, internist DEPT. OF INTERNAL MEDICINE, RADBOUD UNIVERSITY NIJMEGEN MEDICAL CENTER, NIJMEGEN,THE NETHERLANDS DEPT. OF INTERNAL
Primary Aldosteronism: screening, diagnosis and therapy Jacques W.M. Lenders, internist DEPT. OF INTERNAL MEDICINE, RADBOUD UNIVERSITY NIJMEGEN MEDICAL CENTER, NIJMEGEN,THE NETHERLANDS DEPT. OF INTERNAL
ULTIMATE BEAUTY OF BIOCHEMISTRY. Dr. Veena Bhaskar S Gowda Dept of Biochemistry 30 th Nov 2017
 ULTIMATE BEAUTY OF BIOCHEMISTRY Dr. Veena Bhaskar S Gowda Dept of Biochemistry 30 th Nov 2017 SUSPECTED CASE OF CUSHING S SYNDROME Clinical features Moon face Obesity Hypertension Hunch back Abdominal
ULTIMATE BEAUTY OF BIOCHEMISTRY Dr. Veena Bhaskar S Gowda Dept of Biochemistry 30 th Nov 2017 SUSPECTED CASE OF CUSHING S SYNDROME Clinical features Moon face Obesity Hypertension Hunch back Abdominal
The Endocrine System Part II
 The Endocrine System Part II Thyroid gland Parathyroid glands Regulation of blood Calcium level Adrenal gland Exocrine part of pancreas (Islets of Langerhans) Thyroid Gland Located in the anterior neck
The Endocrine System Part II Thyroid gland Parathyroid glands Regulation of blood Calcium level Adrenal gland Exocrine part of pancreas (Islets of Langerhans) Thyroid Gland Located in the anterior neck
in Primary Care (Part 2) Jonathan R. Anolik, MD, FACP, FACE Lewis Katz School of Medicine at Temple University
 Jonathan R. Anolik, MD, FACP, FACE Lewis Katz School of Medicine at Temple University") Common Endocrine Problems Seen in Primary Care (Part 2) Lecture #34 Jonathan R. Anolik, MD, FACP, FACE Lewis Katz School of Medicine at Temple University None Conflict of Interest Topics to be Covered
Common Endocrine Problems Seen in Primary Care (Part 2) Lecture #34 Jonathan R. Anolik, MD, FACP, FACE Lewis Katz School of Medicine at Temple University None Conflict of Interest Topics to be Covered
Potassium regulation. -Kidney is a major regulator for potassium Homeostasis.
 Potassium regulation. -Kidney is a major regulator for potassium Homeostasis. Normal potassium intake, distribution, and output from the body. Effects of severe hyperkalemia Partial depolarization of cell
Potassium regulation. -Kidney is a major regulator for potassium Homeostasis. Normal potassium intake, distribution, and output from the body. Effects of severe hyperkalemia Partial depolarization of cell
Read the following article and answer the questions that follow. Refer to the Keys section to check your answers.
 ENGLISH 183 READING PRACTICE - Pheochromocytoma Read the following article and answer the questions that follow. Refer to the Keys section to check your answers. Pheochromocytoma is a tumor on the medulla
ENGLISH 183 READING PRACTICE - Pheochromocytoma Read the following article and answer the questions that follow. Refer to the Keys section to check your answers. Pheochromocytoma is a tumor on the medulla
Subclinical Cushing s Syndrome
 Subclinical Cushing s Syndrome AACE 26th Annual Scientific & Clinical Congress Associate Clinical Professor of Medicine and Clinical Chief University of Miami Miller Scholl of Medicine Miami, Florida aayala2@miami.edu
Subclinical Cushing s Syndrome AACE 26th Annual Scientific & Clinical Congress Associate Clinical Professor of Medicine and Clinical Chief University of Miami Miller Scholl of Medicine Miami, Florida aayala2@miami.edu
PTA/OTA 106 Unit 2 Lecture 4 Introduction to the Endocrine System
 PTA/OTA 106 Unit 2 Lecture 4 Introduction to the Endocrine System 1 Anterior Pituitary or Adenohypophysis Corticotrophs Adrenocorticotropic hormone (ACTH) Hypothalamic Control Corticotropic releasing hormone
PTA/OTA 106 Unit 2 Lecture 4 Introduction to the Endocrine System 1 Anterior Pituitary or Adenohypophysis Corticotrophs Adrenocorticotropic hormone (ACTH) Hypothalamic Control Corticotropic releasing hormone
Adrenal and retropetionium
 Adrenal and retropetionium Disorders of the Adrenal Cortex Hyperaldosteronism: Hyperaldosteronism may be secondary to stimulation of the renin-angiotensin system from renal artery stenosis and to low-flow
Adrenal and retropetionium Disorders of the Adrenal Cortex Hyperaldosteronism: Hyperaldosteronism may be secondary to stimulation of the renin-angiotensin system from renal artery stenosis and to low-flow
Pituitary, Parathyroid Pheochromocytomas & Paragangliomas: The 4 Ps of NETs
 Pituitary, Parathyroid Pheochromocytomas & Paragangliomas: The 4 Ps of NETs Shereen Ezzat, MD, FRCP(C), FACP Professor Of Medicine & Oncology Head, Endocrine Oncology Princess Margaret Hospital/University
Pituitary, Parathyroid Pheochromocytomas & Paragangliomas: The 4 Ps of NETs Shereen Ezzat, MD, FRCP(C), FACP Professor Of Medicine & Oncology Head, Endocrine Oncology Princess Margaret Hospital/University
Hypertension Update Warwick Jaffe Interventional Cardiologist Ascot Hospital
 Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment
Hypertension Update 2008 Warwick Jaffe Interventional Cardiologist Ascot Hospital Definition of Hypertension Continuous variable At some point the risk becomes high enough to justify treatment Treatment