15 Years Of Clinical Trials In ARDS: What Progress Have We Made?
|
|
|
- Jared French
- 5 years ago
- Views:
Transcription
1 15 Years Of Clinical Trials In ARDS: What Progress Have We Made? Niall D. Ferguson, MD, FRCPC, MSc Head of Critical Care Medicine University Health Network & Mount Sinai Hospital Senior Scientist, Toronto General Research Institute Associate Professor, Depts of Medicine & Physiology, Institute of Health Policy, Management and Evaluation Interdepartmental Division of Critical Care Medicine University of Toronto
2 1952: Copenhagen Polio Epidemic First month 31 patients with respiratory paralysis 27 patients died (87%)
3

4 Bjørn Ibsen The tank respirator (negativepressure) did not provide adequate ventilation An elevated CO 2 was indicative of CO 2 retention, and not, as the epidemiologists thought, of metabolic alkalosis Early application of positivepressure ventilation
5 Hand ventilator used in the Copenhagen polio epidemic of 1952 by hundreds of ventilators

6 Mortality July 1952 March 1953 Months
7 AUGUST 26 TH 1952 Birth of mechanical ventilation and intensive care unit
8

9
10 Advances in Mechanical Ventilators Improvements in technical aspects of ventilators Flow delivery Exhalation valves Microprocessor-controlled ventilators Improved monitors and monitoring Better triggering, cycling Better flow delivery systems New modes of ventilation IMV, HFV, PC-IRV, PSV, APRV, PAV, NAVA,..

11 Iatrogenic Consequences of Ventilation: First, do no harm!
12
13
14


15 Observational Mortality Rate since 1994 = 40-45%

16

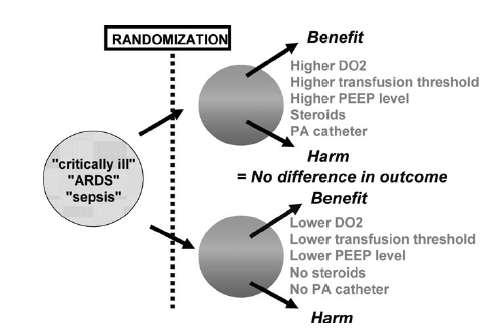
17 RCTs: Absolutely Necessary

18


19

20
21 Survival Curve
22 Why Randomise? ALLOCATION CONCEALMENT Minimise allocation bias, selection bias Balances known and unknown prognostic (confounding) factors, including time Facilitates statistical hypothesis testing, maximize statistical power
23 Alternatives to RCTs We should just carefully analyse observational data but of course we need to avoid complicated statistics.
24 Problematic RCTs Dumb idea Wrong patients Incorrect protocolization of therapy
25
26 Poor Quality RCTs Inadequate concealment Unbalanced cointerventions Loss to follow-up Lack of intention-to-treat analysis Lack of blinding Bad luck Table 1 not balanced Stopped early



27 P-values are necessary but insufficient the reader must estimate the prior probability that the research hypothesis is true

28
29
30 Interpreting RCT Results I already knew that I don t believe it
31 ARDS Network High Stretch V T : 11.8 P PLAT : RR: 18 V MIN : 13 PEEP: 8 Low Stretch V T : 6.2 ml/kg P PLAT : 25 cm H 2 O RR: 29 V MIN : 13 L/min PEEP: 9 cm H 2 O Mortality 40% Mortality 31% N Engl J Med :1301-8
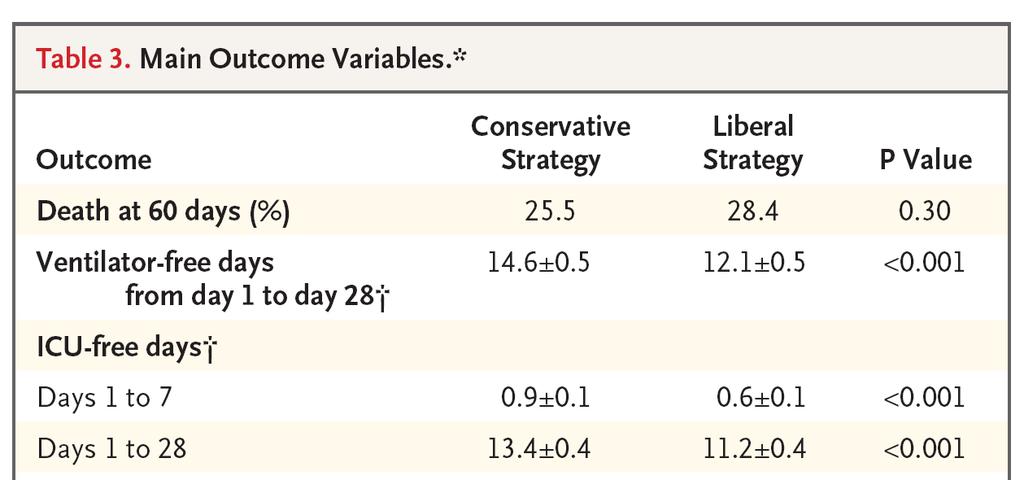
32 FACCT


33 28-day Mortality: 24% - Nimbex 33% - Placebo p=0.05

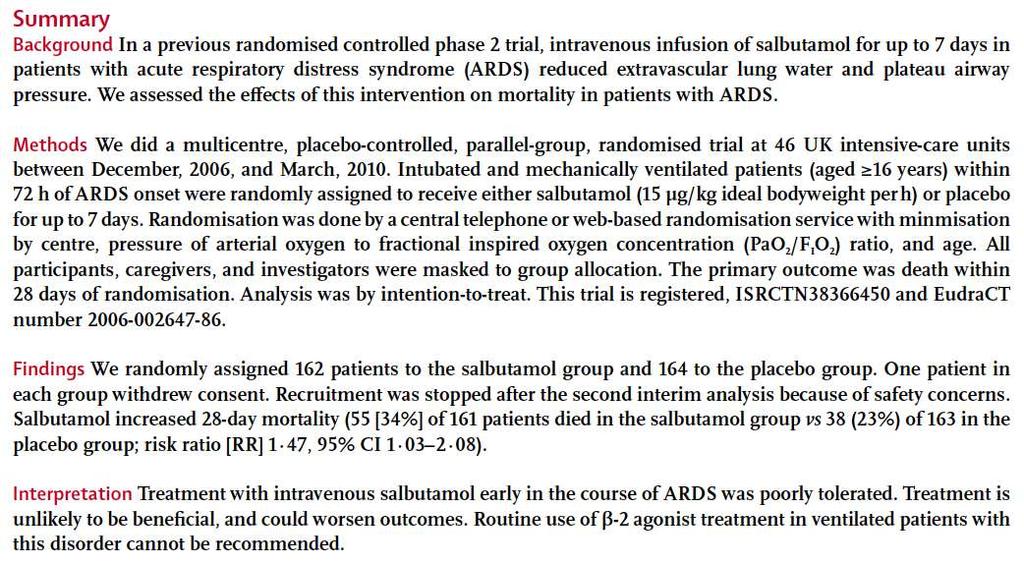

34 28-day mortality: 34% Salbutamol 23% Placebo RR 1.47 ( )

35 What They Found ICU Mortality: RR 0.85 ( )



36 28-day Mortality: 16% vs. 33%; p<0.001
37

38 How has practice changed? Has the evidence been a factor?


39 Mechanical ventilation practice has changed significantly from 1998 to 2004
40 Patients in 103 Repeat ICUs patients in 103 Repeat ICUs Literature Review Practice-change Hypotheses
41 Hypotheses: ARDS Decreased tidal volumes in ALI/ARDS A minimal increase in PEEP No significant increase in PC mode use No significant increase in prone ventilation
42 20 Tidal volume (ml/kg ABW) P < ± ± 1.8 (8.8 ml/kg PBW) ARDS
43 PEEP (cm of water) ± ± p=0.02 ARDS


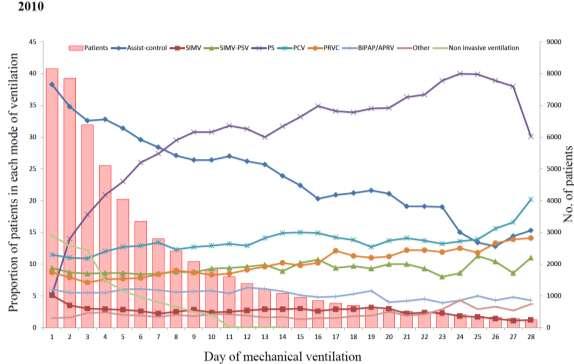
44 3 rd International Study of Mechanical Ventilation ( 2010) Countries 37 ICUs 520 Patients 8.152
45


46 Tidal Volume (ml/kg ABW) in ARDS Means & %age
47
48 Where do we go from here?

49

50 clinicaltrials.gov current ARDS studies
51 Reliable and Valid Definitions are ESSENTIAL to Conduct and Interpret Clinical Research

52 Berlin Definition of ARDS
53 Distribution of patients across categories of ARDS ARDS 22% % 27% Mortality Mild 50% 32% Mortality Moderate 45% Mortality Severe

54 AECC Limitations Berlin Modifications No definition of acute ALI/ARDS confusion Inconsistency of PaO 2 /F I O 2 ratio Effect of PEEP Effect of F I O 2 CXR has poor reliability PAWP & ARDS can coexist Risk factors not included No Acute definition onset defined of acute ALI/ARDS eliminated confusion 3 mutually exclusive grades of Inconsistency ARDS of PaO 2 /F I O 2 ratio Inconsistency of PaO 2 /F I O 2 ratio Effect of PEEP Minumum PEEP required F I O 2 effect reduced with Severe Effect of F I O 2 CXR clarified + examples PAWP removed CXR has poor reliability PAWP & ARDS can coexist Risk factors included Risk factors not included


55
56 The importance of recognising ARDS
57 From Ware & Matthay NEJM 2000
58

59 Importance of Specificity in RCTs Specific Test Non-Specific Test Other Diseases
60 60
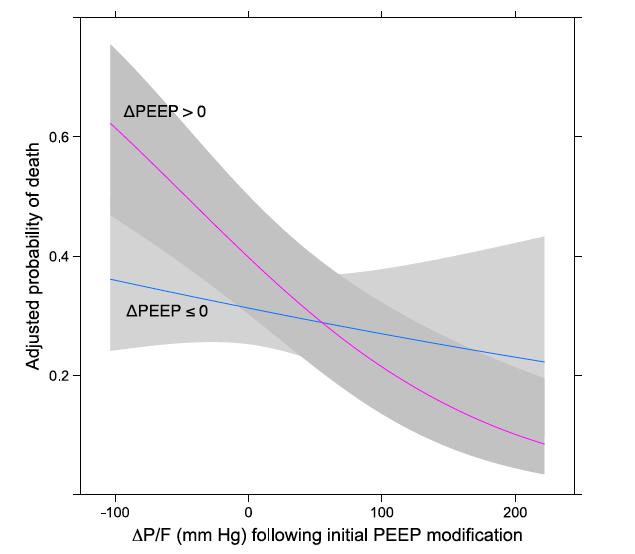
61 Enriching a Trial Population Goligher EC et al. Am J Respir Crit Care Med; 2015 In Press A. Conventional enrolment design épeep ARDS pa ents Randomize êpeep B. Conventional restricted (severity-based) enrolment design épeep ARDS pa ents Exclude less severely ill pa ents based on baseline P/F Randomize êpeep C. Novel restricted (response-based) enrolment design #1 épeep Responders Randomize Eligible pa ents Response assessment êpeep Non-responders Exclude
62 Study population randomized Original Trial ARDS P/F < 150 ARDS with positive O 2 response* Control group mortality 40% 49% 40% Treatment group mortality Hypothesized effect size Number required to be randomized (α = 0.05 and β = 0.2) Proportion of patients with P/F < threshold for inclusion Frequency of positive response to PEEP Total number of ARDS patients required to be evaluated 36% 43% 32% 4% 6% 8% n/a 56% n/a n/a n/a 54%** Goligher EC et al. Am J Respir Crit Care Med; 2015 In Press


63 ARMA & ALVEOLI Trials Latent Class Modeling 63

64 The Future of ARDS Trials?

65 New Monitoring Devices Electrical Impedance Tomography Extravascular Lung Water measurement Specific Elastance measurement PET Scanning Lung Ultrasound



66 New Therapeutic Devices New modes of ventilation NAVA PAV BiLevel / APRV ASV ECMO ECCO2R

67 Novel Applications ARDS Prevention PEEP Settings and Titration Transpulmonary pressure Staircase recruitment Noninvasive ventilation Neurmuscular blockers Spontaneous breathing in ARDS
68 New Therapeutics & Diagnostics Steroids Mesenchymal stem cells Specific anti-inflammatories Anti Tissue Factor Ab Biomarkers srage VEGF strem Ang2

69 Challenge Translational Medicine There is a translational block leading to a disconnect between basic science success and negative clinical trials
70 Opportunity Translational Medicine We need to make periodic revisions to our syndromic definitions Gradually incorporating more basic science into them Maintain the genotype-phenotype link We need a large detailed observational study of acute respiratory failure to further inform ARDS definitions We need to work collaboratively together on large international RCTs based on sound physiology

71

72 Every science begins as philosophy and ends as art Will Durant

73 October Sheraton Centre Hotel, Toronto
Outline. Basic principles of lung protective ventilation. The challenging areas. Small tidal volumes Recruitment
 ARDS beyond 6/kg Gordon D. Rubenfeld, MD MSc Professor of Medicine, University of Toronto Chief, Program in Trauma, Emergency, and Critical Care Sunnybrook Health Sciences Centre Outline Basic principles
ARDS beyond 6/kg Gordon D. Rubenfeld, MD MSc Professor of Medicine, University of Toronto Chief, Program in Trauma, Emergency, and Critical Care Sunnybrook Health Sciences Centre Outline Basic principles
Landmark articles on ventilation
 Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
Recognizing and Correcting Patient-Ventilator Dysynchrony
 2019 KRCS Annual State Education Seminar Recognizing and Correcting Patient-Ventilator Dysynchrony Eric Kriner BS,RRT Pulmonary Critical Care Clinical Specialist MedStar Washington Hospital Center Washington,
2019 KRCS Annual State Education Seminar Recognizing and Correcting Patient-Ventilator Dysynchrony Eric Kriner BS,RRT Pulmonary Critical Care Clinical Specialist MedStar Washington Hospital Center Washington,
Management of Severe ARDS: Current Canadian Practice
 Management of Severe ARDS: Current Canadian Practice Erick Duan MD FRCPC Clinical Scholar, Department of Medicine, Division of Critical Care, McMaster University Intensivist, St. Joseph's Healthcare Hamilton
Management of Severe ARDS: Current Canadian Practice Erick Duan MD FRCPC Clinical Scholar, Department of Medicine, Division of Critical Care, McMaster University Intensivist, St. Joseph's Healthcare Hamilton
ARDS: The Evidence. Topics. New definition Breaths: Little or Big? Wet or Dry? Moving or Still? Upside down or Right side up?
 ARDS: The Evidence Todd M Bull MD Professor of Medicine Division of Pulmonary Sciences and Critical Care Division of Cardiology Director Pulmonary Vascular Disease Center Director Center for Lungs and
ARDS: The Evidence Todd M Bull MD Professor of Medicine Division of Pulmonary Sciences and Critical Care Division of Cardiology Director Pulmonary Vascular Disease Center Director Center for Lungs and
Oxygenation Failure. Increase FiO2. Titrate end-expiratory pressure. Adjust duty cycle to increase MAP. Patient Positioning. Inhaled Vasodilators
 Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
Phenotyping of ARDS and non ARDS Patients
 Critical Care Canada Forum 2018 Sheraton Toronto, Toronto, Canada November 8, 2018; 11:05h 11:25h Phenotyping of and non Patients Berlin & Kigali, RALE score, Reclassification, Driving Pressure and Mechanical
Critical Care Canada Forum 2018 Sheraton Toronto, Toronto, Canada November 8, 2018; 11:05h 11:25h Phenotyping of and non Patients Berlin & Kigali, RALE score, Reclassification, Driving Pressure and Mechanical
Acute Lung Injury/ARDS. Disclosures. Overview. Acute Respiratory Failure 5/30/2014. Research funding: NIH, UCSF CTSI, Glaxo Smith Kline
 Disclosures Acute Respiratory Failure Carolyn S. Calfee, MD MAS UCSF Critical Care Medicine and Trauma CME May 30, 2014 Research funding: NIH, UCSF CTSI, Glaxo Smith Kline Medical advisory boards: Cerus
Disclosures Acute Respiratory Failure Carolyn S. Calfee, MD MAS UCSF Critical Care Medicine and Trauma CME May 30, 2014 Research funding: NIH, UCSF CTSI, Glaxo Smith Kline Medical advisory boards: Cerus
Ventilator ECMO Interactions
 Ventilator ECMO Interactions Lorenzo Del Sorbo, MD CCCF Toronto, October 2 nd 2017 Disclosure Relevant relationships with commercial entities: none Potential for conflicts within this presentation: none
Ventilator ECMO Interactions Lorenzo Del Sorbo, MD CCCF Toronto, October 2 nd 2017 Disclosure Relevant relationships with commercial entities: none Potential for conflicts within this presentation: none
ARDS: an update 6 th March A. Hakeem Al Hashim, MD, FRCP SQUH
 ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
ARDS and Ventilators PG26 Update in Surgical Critical Care October 9, 2013
 ARDS and Ventilators PG26 Update in Surgical Critical Care October 9, 2013 Pauline K. Park MD, FACS, FCCM University of Michigan School of Medicine Ann Arbor, MI OVERVIEW New Berlin definition of ARDS
ARDS and Ventilators PG26 Update in Surgical Critical Care October 9, 2013 Pauline K. Park MD, FACS, FCCM University of Michigan School of Medicine Ann Arbor, MI OVERVIEW New Berlin definition of ARDS
Pro: Early use of VV ECMO for ARDS
 Pro: Early use of VV ECMO for ARDS Kyle J. Rehder, MD, FCCP Associate Professor Division of Pediatric Critical Care Medicine Department of Pediatrics Duke Children s Hospital The ventilator is slowly killing
Pro: Early use of VV ECMO for ARDS Kyle J. Rehder, MD, FCCP Associate Professor Division of Pediatric Critical Care Medicine Department of Pediatrics Duke Children s Hospital The ventilator is slowly killing
Extubation Failure & Delay in Brain-Injured Patients
 Extubation Failure & Delay in Brain-Injured Patients Niall D. Ferguson, MD, FRCPC, MSc Director, Critical Care Medicine University Health Network & Mount Sinai Hospital Associate Professor of Medicine
Extubation Failure & Delay in Brain-Injured Patients Niall D. Ferguson, MD, FRCPC, MSc Director, Critical Care Medicine University Health Network & Mount Sinai Hospital Associate Professor of Medicine
The Berlin Definition: Does it fix anything?
 The Berlin Definition: Does it fix anything? Gordon D. Rubenfeld, MD MSc Professor of Medicine, University of Toronto Chief, Program in Trauma, Emergency, and Critical Care Sunnybrook Health Sciences Centre
The Berlin Definition: Does it fix anything? Gordon D. Rubenfeld, MD MSc Professor of Medicine, University of Toronto Chief, Program in Trauma, Emergency, and Critical Care Sunnybrook Health Sciences Centre
Neuromuscular Blockade in ARDS
 Neuromuscular Blockade in ARDS Maureen O. Meade, MD, FRCPC Critical care consultant, Hamilton Health Sciences Professor of Medicine, McMaster University www.oscillatetrial.com Disclosures None Possible
Neuromuscular Blockade in ARDS Maureen O. Meade, MD, FRCPC Critical care consultant, Hamilton Health Sciences Professor of Medicine, McMaster University www.oscillatetrial.com Disclosures None Possible
ARDS and treatment strategies
 ARDS and treatment strategies Geoff Bellingan Medical Director University College Hospital ARDS: Definitions History of predisposing condition Refractory hypoxaemia of acute onset PaO 2 /FiO 2 ratio:
ARDS and treatment strategies Geoff Bellingan Medical Director University College Hospital ARDS: Definitions History of predisposing condition Refractory hypoxaemia of acute onset PaO 2 /FiO 2 ratio:
ARDS Assisted ventilation and prone position. ICU Fellowship Training Radboudumc
 ARDS Assisted ventilation and prone position ICU Fellowship Training Radboudumc Fig. 1 Physiological mechanisms controlling respiratory drive and clinical consequences of inappropriate respiratory drive
ARDS Assisted ventilation and prone position ICU Fellowship Training Radboudumc Fig. 1 Physiological mechanisms controlling respiratory drive and clinical consequences of inappropriate respiratory drive
The new ARDS definitions: what does it mean?
 The new ARDS definitions: what does it mean? Richard Beale 7 th September 2012 METHODS ESICM convened an international panel of experts, with representation of ATS and SCCM The objectives were to update
The new ARDS definitions: what does it mean? Richard Beale 7 th September 2012 METHODS ESICM convened an international panel of experts, with representation of ATS and SCCM The objectives were to update
Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye
 Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye Steroids in ARDS: conclusion Give low-dose steroids if indicated for another problem
Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye Steroids in ARDS: conclusion Give low-dose steroids if indicated for another problem
CLINICAL VIGNETTE 2016; 2:3
 CLINICAL VIGNETTE 2016; 2:3 Editor-in-Chief: Olufemi E. Idowu. Neurological surgery Division, Department of Surgery, LASUCOM/LASUTH, Ikeja, Lagos, Nigeria. Copyright- Frontiers of Ikeja Surgery, 2016;
CLINICAL VIGNETTE 2016; 2:3 Editor-in-Chief: Olufemi E. Idowu. Neurological surgery Division, Department of Surgery, LASUCOM/LASUTH, Ikeja, Lagos, Nigeria. Copyright- Frontiers of Ikeja Surgery, 2016;
PAEDIATRIC RESPIRATORY FAILURE. Tang Swee Fong Department of Paediatrics University Kebangsaan Malaysia Medical Centre
 PAEDIATRIC RESPIRATORY FAILURE Tang Swee Fong Department of Paediatrics University Kebangsaan Malaysia Medical Centre Outline of lecture Bronchiolitis Bronchopulmonary dysplasia Asthma ARDS Bronchiolitis
PAEDIATRIC RESPIRATORY FAILURE Tang Swee Fong Department of Paediatrics University Kebangsaan Malaysia Medical Centre Outline of lecture Bronchiolitis Bronchopulmonary dysplasia Asthma ARDS Bronchiolitis
Experience with Low Flow ECCO2R device on a CRRT platform : CO2 removal
 Experience with Low Flow ECCO2R device on a CRRT platform : CO2 removal Alain Combes, MD, PhD, Hôpital Pitié-Salpêtrière, AP-HP Inserm UMRS 1166, ican, Institute of Cardiometabolism and Nutrition Pierre
Experience with Low Flow ECCO2R device on a CRRT platform : CO2 removal Alain Combes, MD, PhD, Hôpital Pitié-Salpêtrière, AP-HP Inserm UMRS 1166, ican, Institute of Cardiometabolism and Nutrition Pierre
Ventilatory Management of ARDS. Alexei Ortiz Milan; MD, MSc
 Ventilatory Management of ARDS Alexei Ortiz Milan; MD, MSc 2017 Outline Ventilatory management of ARDS Protected Ventilatory Strategy Use of NMB Selection of PEEP Driving pressure Lung Recruitment Prone
Ventilatory Management of ARDS Alexei Ortiz Milan; MD, MSc 2017 Outline Ventilatory management of ARDS Protected Ventilatory Strategy Use of NMB Selection of PEEP Driving pressure Lung Recruitment Prone
Biomarkers for ARDS not so simple. John Laffey. Critical Illness and Injury Research Centre St Michael s Hospital, University of Toronto, CANADA
 Biomarkers for ARDS not so simple John Laffey Critical Illness and Injury Research Centre St Michael s Hospital, University of Toronto, CANADA Berlin ARDS definition - 2012 Mild Moderate Severe Acute Onset
Biomarkers for ARDS not so simple John Laffey Critical Illness and Injury Research Centre St Michael s Hospital, University of Toronto, CANADA Berlin ARDS definition - 2012 Mild Moderate Severe Acute Onset
Year in Review: Critical Care Medicine
 Year in Review: Critical Care Medicine No disclosures Eric J. Seeley, M.D. Assistant Professor of Medicine Division of Pulmonary and Critical Care Medicine Why I Selected These Studies High quality studies
Year in Review: Critical Care Medicine No disclosures Eric J. Seeley, M.D. Assistant Professor of Medicine Division of Pulmonary and Critical Care Medicine Why I Selected These Studies High quality studies
APRV: An Update CHLOE STEINSHOUER, MD PULMONARY & SLEEP CONSULTANTS OF KANSAS 04/06/2017
 APRV: An Update CHLOE STEINSHOUER, MD PULMONARY & SLEEP CONSULTANTS OF KANSAS 04/06/2017 Disclosures No conflicts of interest Objectives Attendees will be able to: Define the mechanism of APRV Describe
APRV: An Update CHLOE STEINSHOUER, MD PULMONARY & SLEEP CONSULTANTS OF KANSAS 04/06/2017 Disclosures No conflicts of interest Objectives Attendees will be able to: Define the mechanism of APRV Describe
Potential Conflicts of Interest
 Potential Conflicts of Interest Patient Ventilator Synchrony, PAV and NAVA! Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts 4-27-09 WSRC Received research
Potential Conflicts of Interest Patient Ventilator Synchrony, PAV and NAVA! Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts 4-27-09 WSRC Received research
Proportional Assist Ventilation (PAV) (NAVA) Younes ARRD 1992;145:114. Ventilator output :Triggering, Cycling Control of flow, rise time and pressure
 (NAVA) Younes ARRD 1992;145:114. Ventilator output :Triggering, Cycling Control of flow, rise time and pressure") Conflict of Interest Disclosure Robert M Kacmarek Unconventional Techniques Using Your ICU Ventilator!" 5-5-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston,
Conflict of Interest Disclosure Robert M Kacmarek Unconventional Techniques Using Your ICU Ventilator!" 5-5-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston,
Analyzing Lung protective ventilation F Javier Belda MD, PhD Sº de Anestesiología y Reanimación. Hospital Clinico Universitario Valencia (Spain)
") Analyzing Lung protective ventilation F Javier Belda MD, PhD Sº de Anestesiología y Reanimación Hospital Clinico Universitario Valencia (Spain) ALI/ARDS Report of the American-European consensus conference
Analyzing Lung protective ventilation F Javier Belda MD, PhD Sº de Anestesiología y Reanimación Hospital Clinico Universitario Valencia (Spain) ALI/ARDS Report of the American-European consensus conference
Part 2 of park s Ventilator and ARDS slides for syllabus
 Part 2 of park s Ventilator and ARDS slides for syllabus Early Neuromuscular Blockade Question 4 The early use of cis-atracurium in severe ARDS is: A. Contraindicated in patients with diabetes B. Associated
Part 2 of park s Ventilator and ARDS slides for syllabus Early Neuromuscular Blockade Question 4 The early use of cis-atracurium in severe ARDS is: A. Contraindicated in patients with diabetes B. Associated
ARDS and Lung Protection
 ARDS and Lung Protection Kristina Sullivan, MD Associate Professor University of California, San Francisco Department of Anesthesia and Perioperative Care Division of Critical Care Medicine Overview Low
ARDS and Lung Protection Kristina Sullivan, MD Associate Professor University of California, San Francisco Department of Anesthesia and Perioperative Care Division of Critical Care Medicine Overview Low
Difficult Ventilation in ARDS Patients
 Thank you for viewing this presentation. We would like to remind you that this material is the property of the author. It is provided to you by the ERS for your personal use only, as submitted by the author.
Thank you for viewing this presentation. We would like to remind you that this material is the property of the author. It is provided to you by the ERS for your personal use only, as submitted by the author.
Application of Lung Protective Ventilation MUST Begin Immediately After Intubation
 Conflict of Interest Disclosure Robert M Kacmarek Managing Severe Hypoxemia!" 9-28-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts I disclose
Conflict of Interest Disclosure Robert M Kacmarek Managing Severe Hypoxemia!" 9-28-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts I disclose
Inhaled nitric oxide: clinical evidence for use in adults
 Inhaled nitric oxide: clinical evidence for use in adults Neill Adhikari Critical Care Medicine Sunnybrook Health Sciences Centre and University of Toronto 31 October 2014 Conflict of interest Ikaria provided
Inhaled nitric oxide: clinical evidence for use in adults Neill Adhikari Critical Care Medicine Sunnybrook Health Sciences Centre and University of Toronto 31 October 2014 Conflict of interest Ikaria provided
NIV in hypoxemic patients
 NIV in hypoxemic patients Massimo Antonelli, MD Dept. of Intensive Care & Anesthesiology Università Cattolica del Sacro Cuore Rome - Italy Conflict of interest (research grants and consultations): Maquet
NIV in hypoxemic patients Massimo Antonelli, MD Dept. of Intensive Care & Anesthesiology Università Cattolica del Sacro Cuore Rome - Italy Conflict of interest (research grants and consultations): Maquet
ACUTE RESPIRATORY DISTRESS SYNDROME
 ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
Wet Lungs Dry lungs Impact on Outcome in ARDS. Charlie Phillips MD Division of PCCM OHSU 2009
 Wet Lungs Dry lungs Impact on Outcome in ARDS Charlie Phillips MD Division of PCCM OHSU 2009 Today s talk Pathophysiology of ARDS The case for dry Targeting EVLW Disclosures Advisor for Pulsion Medical
Wet Lungs Dry lungs Impact on Outcome in ARDS Charlie Phillips MD Division of PCCM OHSU 2009 Today s talk Pathophysiology of ARDS The case for dry Targeting EVLW Disclosures Advisor for Pulsion Medical
Ventilator curves. Fellowonderwijs 2 feb 2012
 Ventilator curves Fellowonderwijs 2 feb 2012 Mechanical ventilation Supported Ventilator affects patients respiratory drive Monitor interaction patient - ventilator Controlled Monitor interatcion patient
Ventilator curves Fellowonderwijs 2 feb 2012 Mechanical ventilation Supported Ventilator affects patients respiratory drive Monitor interaction patient - ventilator Controlled Monitor interatcion patient
Sub-category: Intensive Care for Respiratory Distress
 Course n : Course 3 Title: RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE Sub-category: Intensive Care for Respiratory Distress Topic: Acute Respiratory Distress
Course n : Course 3 Title: RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE Sub-category: Intensive Care for Respiratory Distress Topic: Acute Respiratory Distress
Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor
 Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
THE ACUTE RESPIRATORY DISTRESS SYNDROME. Daniel Brockman, DO
 THE ACUTE RESPIRATORY DISTRESS SYNDROME Daniel Brockman, DO Objectives Describe the history and evolution of the diagnosis of ARDS Review the diagnostic criteria for ARDS Discuss the primary interventions
THE ACUTE RESPIRATORY DISTRESS SYNDROME Daniel Brockman, DO Objectives Describe the history and evolution of the diagnosis of ARDS Review the diagnostic criteria for ARDS Discuss the primary interventions
CSIM annual meeting Acute respiratory failure. Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018
 CSIM annual meeting - 2018 Acute respiratory failure Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018 NRGH affiliated with UBC medicine Disclosures None relevant to this presentation. Also no
CSIM annual meeting - 2018 Acute respiratory failure Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018 NRGH affiliated with UBC medicine Disclosures None relevant to this presentation. Also no
ARDS Management Protocol
 ARDS Management Protocol February 2018 ARDS Criteria Onset Within 1 week of a known clinical insult or new or worsening respiratory symptoms Bilateral opacities not fully explained by effusions, lobar/lung
ARDS Management Protocol February 2018 ARDS Criteria Onset Within 1 week of a known clinical insult or new or worsening respiratory symptoms Bilateral opacities not fully explained by effusions, lobar/lung
Best of Pulmonary Jennifer R. Hucks, MD University of South Carolina School of Medicine
 Best of Pulmonary 2012-2013 Jennifer R. Hucks, MD University of South Carolina School of Medicine Topics ARDS- Berlin Definition Prone Positioning For ARDS Lung Protective Ventilation In Patients Without
Best of Pulmonary 2012-2013 Jennifer R. Hucks, MD University of South Carolina School of Medicine Topics ARDS- Berlin Definition Prone Positioning For ARDS Lung Protective Ventilation In Patients Without
Airway pressure release ventilation (APRV) in PICU: Current evidence. Chor Yek Kee Sarawak General Hospital
 in PICU: Current evidence. Chor Yek Kee Sarawak General Hospital") Airway pressure release ventilation (APRV) in PICU: Current evidence Chor Yek Kee Sarawak General Hospital Outline Brief introduction of APRV History of APRV Common confusion in APRV Features of APRV and
Airway pressure release ventilation (APRV) in PICU: Current evidence Chor Yek Kee Sarawak General Hospital Outline Brief introduction of APRV History of APRV Common confusion in APRV Features of APRV and
Steroids for ARDS. Clinical Problem. Management
 Steroids for ARDS James Beck Clinical Problem A 60 year old lady re-presented to ICU with respiratory failure. She had previously been admitted for fluid management and electrolyte correction having presented
Steroids for ARDS James Beck Clinical Problem A 60 year old lady re-presented to ICU with respiratory failure. She had previously been admitted for fluid management and electrolyte correction having presented
Ventilator Dyssynchrony - Recognition, implications, and management
 Ventilator Dyssynchrony - Recognition, implications, and management Gavin M Joynt Dept of Anaesthesia & Intensive Care The Chinese University of Hong Kong Dyssynchrony Uncoupling of mechanical delivered
Ventilator Dyssynchrony - Recognition, implications, and management Gavin M Joynt Dept of Anaesthesia & Intensive Care The Chinese University of Hong Kong Dyssynchrony Uncoupling of mechanical delivered
Adjunct Therapies for Pediatric ARDS: Where are the Data?
 Adjunct Therapies for Pediatric ARDS: Where are the Data? Alexandre T. Rotta, MD, FCCM Professor of Pediatrics, Linsalata Family Endowed Chair in Pediatric Critical Care and Emergency Medicine Rainbow
Adjunct Therapies for Pediatric ARDS: Where are the Data? Alexandre T. Rotta, MD, FCCM Professor of Pediatrics, Linsalata Family Endowed Chair in Pediatric Critical Care and Emergency Medicine Rainbow
Weaning and extubation in PICU An evidence-based approach
 Weaning and extubation in PICU An evidence-based approach Suchada Sritippayawan, MD. Div. Pulmonology & Crit Care Dept. Pediatrics Faculty of Medicine Chulalongkorn University Kanokporn Udomittipong, MD.
Weaning and extubation in PICU An evidence-based approach Suchada Sritippayawan, MD. Div. Pulmonology & Crit Care Dept. Pediatrics Faculty of Medicine Chulalongkorn University Kanokporn Udomittipong, MD.
Patient-Ventilator Synchrony and Impact on Outcome
 Variables Controlled during Mechanical Ventilation Patient-Ventilator Synchrony and Impact on Outcome 9-30-17 Cox Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts
Variables Controlled during Mechanical Ventilation Patient-Ventilator Synchrony and Impact on Outcome 9-30-17 Cox Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts
Patient Asynchrony and Its Impact on Patient Outcome
 Patient Asynchrony and Its Impact on Patient Outcome 5-14-18 CSRC Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts Conflict of Interest Disclosure Robert
Patient Asynchrony and Its Impact on Patient Outcome 5-14-18 CSRC Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts Conflict of Interest Disclosure Robert
What s New About Proning?
 1 What s New About Proning? J. Brady Scott, MSc, RRT-ACCS, AE-C, FAARC Director of Clinical Education and Assistant Professor Department of Cardiopulmonary Sciences Division of Respiratory Care Rush University
1 What s New About Proning? J. Brady Scott, MSc, RRT-ACCS, AE-C, FAARC Director of Clinical Education and Assistant Professor Department of Cardiopulmonary Sciences Division of Respiratory Care Rush University
The Berlin definition met our needs: yes
 Intensive Care Med (2016) 42:643 647 DOI 10.1007/s00134-016-4286-7 EDITORIAL The Berlin definition met our needs: yes Lorenzo Del Sorbo 1,2, V. Marco Ranieri 3 and Niall D. Ferguson 1,2,4* 2016 Springer-Verlag
Intensive Care Med (2016) 42:643 647 DOI 10.1007/s00134-016-4286-7 EDITORIAL The Berlin definition met our needs: yes Lorenzo Del Sorbo 1,2, V. Marco Ranieri 3 and Niall D. Ferguson 1,2,4* 2016 Springer-Verlag
Test Bank Pilbeam's Mechanical Ventilation Physiological and Clinical Applications 6th Edition Cairo
 Instant dowload and all chapters Test Bank Pilbeam's Mechanical Ventilation Physiological and Clinical Applications 6th Edition Cairo https://testbanklab.com/download/test-bank-pilbeams-mechanical-ventilation-physiologicalclinical-applications-6th-edition-cairo/
Instant dowload and all chapters Test Bank Pilbeam's Mechanical Ventilation Physiological and Clinical Applications 6th Edition Cairo https://testbanklab.com/download/test-bank-pilbeams-mechanical-ventilation-physiologicalclinical-applications-6th-edition-cairo/
Protective ventilation for ALL patients
 Protective ventilation for ALL patients PAOLO PELOSI, MD, FERS Department of Surgical Sciences and Integrated Diagnostics (DISC), San Martino Policlinico Hospital IRCCS for Oncology, University of Genoa,
Protective ventilation for ALL patients PAOLO PELOSI, MD, FERS Department of Surgical Sciences and Integrated Diagnostics (DISC), San Martino Policlinico Hospital IRCCS for Oncology, University of Genoa,
Clinical syndrome of severe dyspnea of rapid onset, hypoxemia, and diffuse pulmonary infiltrates leading to respiratory failure.
 Yuanlin Song, M.D. Clinical syndrome of severe dyspnea of rapid onset, hypoxemia, and diffuse pulmonary infiltrates leading to respiratory failure. Pneumonia Trauma SARS PaO2/fiO2
Yuanlin Song, M.D. Clinical syndrome of severe dyspnea of rapid onset, hypoxemia, and diffuse pulmonary infiltrates leading to respiratory failure. Pneumonia Trauma SARS PaO2/fiO2
The use of proning in the management of Acute Respiratory Distress Syndrome
 Case 3 The use of proning in the management of Acute Respiratory Distress Syndrome Clinical Problem This expanded case summary has been chosen to explore the rationale and evidence behind the use of proning
Case 3 The use of proning in the management of Acute Respiratory Distress Syndrome Clinical Problem This expanded case summary has been chosen to explore the rationale and evidence behind the use of proning
Outcomes From Severe ARDS Managed Without ECMO. Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016
 Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
Case discussion Acute severe asthma during pregnancy. J.G. van der Hoeven
 Case discussion Acute severe asthma during pregnancy J.G. van der Hoeven Case (1) 32-year-old female - gravida 3 - para 2 Previous medical history - asthma Pregnant (33 w) Acute onset fever with wheezing
Case discussion Acute severe asthma during pregnancy J.G. van der Hoeven Case (1) 32-year-old female - gravida 3 - para 2 Previous medical history - asthma Pregnant (33 w) Acute onset fever with wheezing
Breathing: Conventional. Matter?
 Breathing: Conventional Ventilation Does the Mode Matter? Brian K. Walsh, RRT NPS, FAARC Director of Respiratory Care Children s Medical Center Dallas Disclosure Research relationships: Maquet NAVA GE
Breathing: Conventional Ventilation Does the Mode Matter? Brian K. Walsh, RRT NPS, FAARC Director of Respiratory Care Children s Medical Center Dallas Disclosure Research relationships: Maquet NAVA GE
The Association Between Oxygenation Thresholds and Mortality During Extracorporeal Life Support
 The Association Between Oxygenation Thresholds and Mortality During Extracorporeal Life Support Laveena Munshi, MD, MSc November 1, 2016 Critical Care Canada Forum Interdepartmental Division of Critical
The Association Between Oxygenation Thresholds and Mortality During Extracorporeal Life Support Laveena Munshi, MD, MSc November 1, 2016 Critical Care Canada Forum Interdepartmental Division of Critical
Respiratory Care at 65
 Respiratory Care at 65 Dean Hess Assistant Director of Respiratory Care Massachusetts General Hospital Associate Professor of Anesthesia Harvard Medical School Editor in Chief, RESPIRATORY CARE Disclosures
Respiratory Care at 65 Dean Hess Assistant Director of Respiratory Care Massachusetts General Hospital Associate Professor of Anesthesia Harvard Medical School Editor in Chief, RESPIRATORY CARE Disclosures
The Impact of Patient-Ventilator. Karen J Bosma, MD, FRCPC Critical Care Medicine and Respirology
 Achieving Restful Ventilation: The Impact of Patient-Ventilator Interaction on Sleep Karen J Bosma, MD, FRCPC Critical Care Medicine and Respirology Disclosure Statement I have received a research grant
Achieving Restful Ventilation: The Impact of Patient-Ventilator Interaction on Sleep Karen J Bosma, MD, FRCPC Critical Care Medicine and Respirology Disclosure Statement I have received a research grant
Mechanical Ventilation in COPD patients
 Mechanical Ventilation in COPD patients Θεόδωρος Βασιλακόπουλος Καθηγητής Πνευμονολογίας-Εντατικής Θεραπείας Εθνικό & Καποδιστριακό Πανεπιστήμιο Αθηνών Νοσοκομείο «ο Ευαγγελισμός» Adjunct Professor, McGill
Mechanical Ventilation in COPD patients Θεόδωρος Βασιλακόπουλος Καθηγητής Πνευμονολογίας-Εντατικής Θεραπείας Εθνικό & Καποδιστριακό Πανεπιστήμιο Αθηνών Νοσοκομείο «ο Ευαγγελισμός» Adjunct Professor, McGill
Mechanical Ventilation of the Patient with Neuromuscular Disease
 Mechanical Ventilation of the Patient with Neuromuscular Disease Dean Hess PhD RRT Associate Professor of Anesthesia, Harvard Medical School Assistant Director of Respiratory Care, Massachusetts General
Mechanical Ventilation of the Patient with Neuromuscular Disease Dean Hess PhD RRT Associate Professor of Anesthesia, Harvard Medical School Assistant Director of Respiratory Care, Massachusetts General
Daniel Hadfield Critical Care Nurse NIHR / HEE Clinical Doctoral Research Fellow King s College Hospital
 Daniel Hadfield Critical Care Nurse NIHR / HEE Clinical Doctoral Research Fellow King s College Hospital Baby 2 Moving house Funding??????? Baby 1 NHS support Me My research Baby 2 Moving house Funding???????
Daniel Hadfield Critical Care Nurse NIHR / HEE Clinical Doctoral Research Fellow King s College Hospital Baby 2 Moving house Funding??????? Baby 1 NHS support Me My research Baby 2 Moving house Funding???????
Mechanical Ventilation in Post-Op VSD Problems Encountered and Treatment Solutions in Developing Countries
 Mechanical Ventilation in Post-Op VSD Problems Encountered and Treatment Solutions in Developing Countries Casey Culbertson MD Cardiac Intensivist Disclosure #1 Unfortunately Nothing financial Disclosure
Mechanical Ventilation in Post-Op VSD Problems Encountered and Treatment Solutions in Developing Countries Casey Culbertson MD Cardiac Intensivist Disclosure #1 Unfortunately Nothing financial Disclosure
Is ARDS Important to Recognize?
 Is ARDS Important to Recognize? Lorraine B. Ware MD Vanderbilt University Financial Disclosures: research funding from Boehringer Ingelheim, Global Blood Therapeutics Why diagnose ARDS? -initiate specific
Is ARDS Important to Recognize? Lorraine B. Ware MD Vanderbilt University Financial Disclosures: research funding from Boehringer Ingelheim, Global Blood Therapeutics Why diagnose ARDS? -initiate specific
Seminar. Current Concepts
 Seminar Current Concepts In ARDS What I think is possible to cover in 40 minutes- Definition Management Ventilatory strategies Conventional LPV Rescue therapy Non Ventilatory strategies Definition and
Seminar Current Concepts In ARDS What I think is possible to cover in 40 minutes- Definition Management Ventilatory strategies Conventional LPV Rescue therapy Non Ventilatory strategies Definition and
Breathing life into new therapies: Updates on treatment for severe respiratory failure. Whitney Gannon, MSN ACNP-BC
 Breathing life into new therapies: Updates on treatment for severe respiratory failure Whitney Gannon, MSN ACNP-BC Overview Definition of ARDS Clinical signs and symptoms Causes Pathophysiology Management
Breathing life into new therapies: Updates on treatment for severe respiratory failure Whitney Gannon, MSN ACNP-BC Overview Definition of ARDS Clinical signs and symptoms Causes Pathophysiology Management
Journal Club American Journal of Respiratory and Critical Care Medicine. Zhang Junyi
 Journal Club 2018 American Journal of Respiratory and Critical Care Medicine Zhang Junyi 2018.11.23 Background Mechanical Ventilation A life-saving technique used worldwide 15 million patients annually
Journal Club 2018 American Journal of Respiratory and Critical Care Medicine Zhang Junyi 2018.11.23 Background Mechanical Ventilation A life-saving technique used worldwide 15 million patients annually
ECMO/ECCO 2 R in Acute Respiratory Failure
 ECMO/ECCO 2 R in Acute Respiratory Failure Alain Combes, MD, PhD, Hôpital Pitié-Salpêtrière, AP-HP Inserm UMRS 1166, ican, Institute of Cardiometabolism and Nutrition Sorbonne Pierre et Marie Curie University,
ECMO/ECCO 2 R in Acute Respiratory Failure Alain Combes, MD, PhD, Hôpital Pitié-Salpêtrière, AP-HP Inserm UMRS 1166, ican, Institute of Cardiometabolism and Nutrition Sorbonne Pierre et Marie Curie University,
Ventilation update Anaesthesia departmental PGME. Tuesday 10 th December Dr Alastair Glossop Consultant Anaesthesia and Critical Care
 Ventilation update Anaesthesia departmental PGME Tuesday 10 th December Dr Alastair Glossop Consultant Anaesthesia and Critical Care What s fashionable in ICU ventilation? Acute respiratory distress syndrome
Ventilation update Anaesthesia departmental PGME Tuesday 10 th December Dr Alastair Glossop Consultant Anaesthesia and Critical Care What s fashionable in ICU ventilation? Acute respiratory distress syndrome
Year in Review Intensive Care Training Program Radboud University Medical Centre Nijmegen
 Year in Review 2013 Intensive Care Training Program Radboud University Medical Centre Nijmegen Contents ARDS Ventilator associated pneumonia Tracheostomy and endotracheal intubation Enteral feeding Fluid
Year in Review 2013 Intensive Care Training Program Radboud University Medical Centre Nijmegen Contents ARDS Ventilator associated pneumonia Tracheostomy and endotracheal intubation Enteral feeding Fluid
The GOLD Study. Goal of Open Lung Ventilation in Donors. Michael A. Matthay M.D. and Lorraine B. Ware, MD. Disclosures
 The GOLD Study Goal of Open Lung Ventilation in Donors Michael A. Matthay M.D. and Lorraine B. Ware, MD Disclosures Research grants from the NHLBI, FDA & Industry - R37 HL51856 - R01 HL126176 - HL 110969
The GOLD Study Goal of Open Lung Ventilation in Donors Michael A. Matthay M.D. and Lorraine B. Ware, MD Disclosures Research grants from the NHLBI, FDA & Industry - R37 HL51856 - R01 HL126176 - HL 110969
Tracking lung recruitment and regional tidal volume at the bedside. Antonio Pesenti
 Tracking lung recruitment and regional tidal volume at the bedside Antonio Pesenti Conflicts of Interest Maquet: Received research support and consultation fees Drager: Received research support and consultation
Tracking lung recruitment and regional tidal volume at the bedside Antonio Pesenti Conflicts of Interest Maquet: Received research support and consultation fees Drager: Received research support and consultation
ARDS A Brief Overview. Lucas Pitts, M.D. Assistant Professor of Medicine Pulmonary and Critical Care Medicine University of Kansas School of Medicine
 ARDS A Brief Overview Lucas Pitts, M.D. Assistant Professor of Medicine Pulmonary and Critical Care Medicine University of Kansas School of Medicine Outline Definition of ARDS Epidemiology of ARDS Pathophysiology
ARDS A Brief Overview Lucas Pitts, M.D. Assistant Professor of Medicine Pulmonary and Critical Care Medicine University of Kansas School of Medicine Outline Definition of ARDS Epidemiology of ARDS Pathophysiology
Mechanical Ventilation 1. Shari McKeown, RRT Respiratory Services - VGH
 Mechanical Ventilation 1 Shari McKeown, RRT Respiratory Services - VGH Objectives Describe indications for mcvent Describe types of breaths and modes of ventilation Describe compliance and resistance and
Mechanical Ventilation 1 Shari McKeown, RRT Respiratory Services - VGH Objectives Describe indications for mcvent Describe types of breaths and modes of ventilation Describe compliance and resistance and
Concerns and Controversial Issues in NPPV. Concerns and Controversial Issues in Noninvasive Positive Pressure Ventilation
 : Common Therapy in Daily Practice Concerns and Controversial Issues in Noninvasive Positive Pressure Ventilation Rongchang Chen Guangzhou Institute of Respiratory Disease as the first choice of mechanical
: Common Therapy in Daily Practice Concerns and Controversial Issues in Noninvasive Positive Pressure Ventilation Rongchang Chen Guangzhou Institute of Respiratory Disease as the first choice of mechanical
Veno-Venous ECMO Support. Chris Cropsey, MD Sept. 21, 2015
 Veno-Venous ECMO Support Chris Cropsey, MD Sept. 21, 2015 Objectives List indications and contraindications for ECMO Describe hemodynamics and oxygenation on ECMO Discuss evidence for ECMO outcomes Identify
Veno-Venous ECMO Support Chris Cropsey, MD Sept. 21, 2015 Objectives List indications and contraindications for ECMO Describe hemodynamics and oxygenation on ECMO Discuss evidence for ECMO outcomes Identify
OSCAR & OSCILLATE. & the Future of High Frequency Oscillatory Ventilation (HFOV)
") & & the Future of High Frequency Oscillatory Ventilation (HFOV) www.philippelefevre.com What do we know already? Sud S et al. BMJ 2010 & Multi-centre randomised controlled trials of HFOV verses current
& & the Future of High Frequency Oscillatory Ventilation (HFOV) www.philippelefevre.com What do we know already? Sud S et al. BMJ 2010 & Multi-centre randomised controlled trials of HFOV verses current
Deep vein thrombosis and its prevention in critically ill adults Attia J, Ray J G, Cook D J, Douketis J, Ginsberg J S, Geerts W H
 Deep vein thrombosis and its prevention in critically ill adults Attia J, Ray J G, Cook D J, Douketis J, Ginsberg J S, Geerts W H Authors' objectives To systematically review the incidence of deep vein
Deep vein thrombosis and its prevention in critically ill adults Attia J, Ray J G, Cook D J, Douketis J, Ginsberg J S, Geerts W H Authors' objectives To systematically review the incidence of deep vein
Cardiorespiratory Physiotherapy Tutoring Services 2017
 VENTILATOR HYPERINFLATION ***This document is intended to be used as an information resource only it is not intended to be used as a policy document/practice guideline. Before incorporating the use of
VENTILATOR HYPERINFLATION ***This document is intended to be used as an information resource only it is not intended to be used as a policy document/practice guideline. Before incorporating the use of
Mechanical Ventilation Principles and Practices
 Mechanical Ventilation Principles and Practices Dr LAU Chun Wing Arthur Department of Intensive Care Pamela Youde Nethersole Eastern Hospital 6 October 2009 In this lecture, you will learn Major concepts
Mechanical Ventilation Principles and Practices Dr LAU Chun Wing Arthur Department of Intensive Care Pamela Youde Nethersole Eastern Hospital 6 October 2009 In this lecture, you will learn Major concepts
Physiology to Improve RCTs
 Physiology to Improve RCTs Brian Kavanagh Hospital for Sick Children University of Toronto 1 Conflicts of Interest No financial conflict of interest with the subject matter of this talk Where s the Interest
Physiology to Improve RCTs Brian Kavanagh Hospital for Sick Children University of Toronto 1 Conflicts of Interest No financial conflict of interest with the subject matter of this talk Where s the Interest
Patient Ventilator Interactions. Patient-Ventilator Interactions. Assisted vs Controlled MV. Ventilatory Muscle Fatigue Recovery
 Patient Ventilator Interactions Patient-Ventilator Interactions Neil MacIntyre MD Duke Uni versity Medi cal Center Durham NC, USA Newer a pproaches to improving intera ctions Assisted vs Controlled MV
Patient Ventilator Interactions Patient-Ventilator Interactions Neil MacIntyre MD Duke Uni versity Medi cal Center Durham NC, USA Newer a pproaches to improving intera ctions Assisted vs Controlled MV
Bi-Level Therapy: Boosting Comfort & Compliance in Apnea Patients
 Bi-Level Therapy: Boosting Comfort & Compliance in Apnea Patients Objectives Describe nocturnal ventilation characteristics that may indicate underlying conditions and benefits of bilevel therapy for specific
Bi-Level Therapy: Boosting Comfort & Compliance in Apnea Patients Objectives Describe nocturnal ventilation characteristics that may indicate underlying conditions and benefits of bilevel therapy for specific
APRV Ventilation Mode
 APRV Ventilation Mode Airway Pressure Release Ventilation A Type of CPAP Continuous Positive Airway Pressure (CPAP) with an intermittent release phase. Patient cycles between two levels of CPAP higher
APRV Ventilation Mode Airway Pressure Release Ventilation A Type of CPAP Continuous Positive Airway Pressure (CPAP) with an intermittent release phase. Patient cycles between two levels of CPAP higher
INTELLiVENT -ASV insight. Alexandra Geiger CAS, Dr. Marc Wysocki, Head of Medical Research Hamilton Medical
 INTELLiVENT -ASV insight Alexandra Geiger CAS, Dr. Marc Wysocki, Head of Medical Research Hamilton Medical First Automation of HAMILTON MEDICAL 1998 Adaptive Support Ventilation (ASV) ASV optimize VT and
INTELLiVENT -ASV insight Alexandra Geiger CAS, Dr. Marc Wysocki, Head of Medical Research Hamilton Medical First Automation of HAMILTON MEDICAL 1998 Adaptive Support Ventilation (ASV) ASV optimize VT and
New Modes to Enhance Synchrony & Dietrich Henzler MD, PhD, FRCPC Division of Critical Care
 New Modes to Enhance Synchrony & Dietrich Henzler MD, PhD, FRCPC Division of Critical Care Disclosure Conflicts of Interest 2001-2011 Research Grants & Payments (cost reimbursements, speaker fees) Draeger
New Modes to Enhance Synchrony & Dietrich Henzler MD, PhD, FRCPC Division of Critical Care Disclosure Conflicts of Interest 2001-2011 Research Grants & Payments (cost reimbursements, speaker fees) Draeger
GUIDELINES ON THE MANAGEMENT OF ACUTE RESPIRATORY DISTRESS SYNDROME
 GUIDELINES ON THE MANAGEMENT OF ACUTE RESPIRATORY DISTRESS SYNDROME Version 1 July 2018 CONTENTS Executive Summary 3 List of Contributors 4 List of Abbreviations 5 Introduction 7 Technical Summary 9 Corticosteroids
GUIDELINES ON THE MANAGEMENT OF ACUTE RESPIRATORY DISTRESS SYNDROME Version 1 July 2018 CONTENTS Executive Summary 3 List of Contributors 4 List of Abbreviations 5 Introduction 7 Technical Summary 9 Corticosteroids
Novel pharmacotherapy in ARDS
 Novel pharmacotherapy in ARDS Danny McAuley Royal Victoria Hospital and Queen s University of Belfast Critical Care Cananda Forum October 2012 Disclosures GSK; consultancy and participate in research funded
Novel pharmacotherapy in ARDS Danny McAuley Royal Victoria Hospital and Queen s University of Belfast Critical Care Cananda Forum October 2012 Disclosures GSK; consultancy and participate in research funded
Mechanical ventilation in the emergency department
 Mechanical ventilation in the emergency department Intubation and mechanical ventilation are often needed in emergency treatment. A ENGELBRECHT, MB ChB, MMed (Fam Med), Dip PEC, DA Head, Emergency Medicine
Mechanical ventilation in the emergency department Intubation and mechanical ventilation are often needed in emergency treatment. A ENGELBRECHT, MB ChB, MMed (Fam Med), Dip PEC, DA Head, Emergency Medicine
New and Future Trends in EMS. Ron Brown, MD, FACEP Paramedic Lecture Series 2018
 New and Future Trends in EMS Ron Brown, MD, FACEP Paramedic Lecture Series 2018 New technologies and protocols DSD Mechanical Compression ITD BiPAP Ultrasound Double Sequential Defibrillation Two defibrillators
New and Future Trends in EMS Ron Brown, MD, FACEP Paramedic Lecture Series 2018 New technologies and protocols DSD Mechanical Compression ITD BiPAP Ultrasound Double Sequential Defibrillation Two defibrillators
What is Acute Respiratory Distress Syndrome? Acute Respiratory Distress Syndrome (ARDS)
") Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Acute Respiratory Distress Syndrome (ARDS) What is Acute Respiratory Distress Syndrome?
 What is Acute Respiratory Distress Syndrome?") Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Comparison of the SpO 2 /FIO 2 Ratio and the PaO 2 /FIO 2 Ratio in Patients With Acute Lung Injury or ARDS*
 CHEST Original Research Comparison of the SpO 2 /FIO 2 Ratio and the PaO 2 /FIO 2 Ratio in Patients With Acute Lung Injury or ARDS* Todd W. Rice, MD, MSc; Arthur P. Wheeler, MD, FCCP; Gordon R. Bernard,
CHEST Original Research Comparison of the SpO 2 /FIO 2 Ratio and the PaO 2 /FIO 2 Ratio in Patients With Acute Lung Injury or ARDS* Todd W. Rice, MD, MSc; Arthur P. Wheeler, MD, FCCP; Gordon R. Bernard,
Fluid restriction is superior in acute lung injury and ARDS
 TAKE-HOME POINTS FROM LECTURES BY CLEVELAND CLINIC AND VISITING FACULTY MEDICAL GRAND ROUNDS CME CREDIT HERBERT P. WIEDEMANN, MD Chairman, Department of Pulmonary, Allergy, and Critical Care Medicine,
TAKE-HOME POINTS FROM LECTURES BY CLEVELAND CLINIC AND VISITING FACULTY MEDICAL GRAND ROUNDS CME CREDIT HERBERT P. WIEDEMANN, MD Chairman, Department of Pulmonary, Allergy, and Critical Care Medicine,
Oregon Health and Science University Portland, Oregon USA
 Classifying ARDS The Role of EVLW Ch l Philli MD Charles Phillips MD Oregon Health and Science University Portland, Oregon USA Incidence High ARDS 2013 150,000 200,000 per year in US alone. Mortality persists
Classifying ARDS The Role of EVLW Ch l Philli MD Charles Phillips MD Oregon Health and Science University Portland, Oregon USA Incidence High ARDS 2013 150,000 200,000 per year in US alone. Mortality persists